
Submitted:
06 June 2025
Posted:
09 June 2025
You are already at the latest version
Abstract
Background: In 2016, the neonatal resuscitation program (NRP) withdrew its recommendation to perform endotracheal suctioning in non-vigorous neonates born through meconium-stained amniotic fluid (MSAF). The objective of this study is to compare outcomes in non-vigorous neonates born through MSAF before and after the change in NRP’s recommendations. Methods: This is a retrospective cohort study in a single center assessing all neonates ≥34 weeks of gestation with MSAF in 2010-2015 (pre-implementation of new guidelines) and 2017-2022 (post-implementation of new guidelines). Results: Neonates receiving tracheal suctioning were more likely to be diagnosed with MAS (29.3% vs. 19.7%; P=0.03) and PPHN (8.9% vs. 2.5%; P=0.003), and more likely to receive surfactant (7.6% vs. 3.2%; P=0.03). Conclusion: In our institution, non-vigorous neonates born via MSAF after the change in NRP guidelines were less likely to be diagnosed with MAS and PPHN and were less likely to receive surfactant. Our study supports current NRP guidelines.
Keywords:
meconium aspiration syndrome
; meconium-stained amniotic fluid
; neonatal resuscitation
1. Introduction
Meconium-stained amniotic fluid (MSAF) can occur in up to 25% of all pregnancies, which often causes meconium aspiration syndrome (MAS), a potentially devastating outcome that can lead to surfactant inactivation, persistent pulmonary hypertension of the newborn (PPHN) or hypoxic respiratory failure (HRF) requiring mechanical ventilation in up to 50% of affected patients, and death in 5-12% (up to 40%) of affected patients [1,2]
Delivery room management of MSAF has evolved over the last two decades [3]. Prior to 2016, the neonatal resuscitation program (NRP) recommended intubating neonates to suction meconium below the level of the glottis in non-vigorous neonates [4]. However, in its two most recent editions, the NRP withdrew that recommendation since several small, randomized studies including non-vigorous newborns born via MSAF concluded that there is no benefit to tracheal suction as it delays initiation of positive pressure ventilation (PPV) [5]. An ovine study from our large animal lab at University at Buffalo, where meconium aspiration was induced in asphyxiated newborn lambs showed improved ventilation and oxygenation in lambs that received tracheal suctioning [6].
After the change in NRP guidelines in 2015, a retrospective review by Kalra et. al. observed a higher incidence of adverse outcomes such as MAS, PPHN, and need for mechanical ventilation in their institute [1]. Two other studies found no difference in MAS incidence or death rates before or after a change in guidelines [7,8].
There is an ongoing debate about how to manage neonates born through MSAF due to conflicting results.
We hypothesized that the incidence of MAS and NICU admissions for respiratory distress would be similar between non-vigorous and vigorous infants born through MSAF in the no-suction era and the prior routine-suction era. We conducted an individual chart review of all infants born through MSAF during both periods/ epochs.
2. Materials and Methods
This is a single-center retrospective cohort study in a level IV 64-bed regional perinatal center. A chart review was conducted on all neonates born at ≥34 weeks of gestation during the years 2010-2015 and 2017-2022. All neonates admitted to mother-baby unit (MBU) and neonatal intensive care unit (NICU) were included.
This study was approved by the Institutional Review Board of the State University of New York at Buffalo, John R. Oishei Children’s Hospital (IRB ID STUDY00006961. For patients admitted to the NICU, data was extracted from our NICU’s Neodata database using a query function. Charts were reviewed individually to confirm data. For patients admitted to the MBU, delivery and admission notes of non-vigorous patients born via MSAF were reviewed.
Neonates born in 2016 were excluded from the analysis due to the transition period following the 2016 changes to the NRP guidelines. During this time, providers were still undergoing training, leading to inconsistencies and overlap in the use of suction versus no-suction practices of the endotracheal tube using a meconium aspirator. We excluded neonates born ≤34 weeks of gestation, vigorous neonates, neonates with chromosomal, genetic, cardiac or fatal anomalies. We also excluded neonates that were not managed per existing NRP guidelines at the time of birth (non-vigorous neonates born via MSAF that did not receive tracheal suctioning prior to 2016, and non-vigorous neonates born via MSAF that did receive tracheal suctioning after 2016 change in guidelines) (Figure 1).
3. Results
Five hundred and eight patients were included in this report, 225 in the group prior to change in guidelines and 283 after. The incidence of birth via MSAF was similar between the two groups (11.2% in 2010-2015 vs. 11.5% in 2017-2022; P=0.44). The baseline patient characteristics were similar between the two groups (Table 1).
No difference in incidence of NICU admission was noted, as shown in Table 2. Additionally, no statistically significant difference was observed in incidence of endotracheal intubation, use of mechanical ventilation, use of non-invasive ventilation, use of continuous positive airway pressure (CPAP), use of oxygen, use of inhaled nitric oxide (iNO), However, there seemed to be a trend of increased use of invasive mechanical ventilation and non-invasive respiratory support when endotracheal suctioning was performed.
Furthermore, a significantly higher incidence of meconium aspiration syndrome (before 2016: 29.3% vs. after 2016: 19.7%; P=0.03) and persistent pulmonary hypertension of the newborn (before 2016: 8.9% vs. after 2016: 2.5%; P=0.003) was noted in the epoch prior to NRP guideline changes. There was also a significant higher incidence of surfactant administration in these non-vigorous patients born through meconium prior with endotracheal suctioning prior to 2016 (before change: 7.6% vs. after change: 3.2%; P=0.03) (Table 2).
4. Discussion
The neonatal resuscitation approach to MSAF has evolved over the last couple few decades. The 7th edition of the NRP guidelines (2015) eliminated routine endotracheal suctioning for non-vigorous infants born through meconium-stained amniotic fluid (MSAF), recommending that resuscitation follow the same principles as for births with clear fluid. Initial steps should occur under a radiant warmer, with positive pressure ventilation initiated if the infant is apneic or the heart rate is <100 bpm. The revised recommendation was guided by the intent to reduce intubation-related risks and minimize delays in initiating PPV, given the lack of evidence supporting the benefit of routine tracheal suctioning. The 8th edition (2021) reaffirmed these recommendations, emphasizing that routine intrapartum suctioning offers no advantage.
In our institution, non-vigorous neonates born through MSAF who received tracheal suctioning in the delivery room had a significantly higher incidence of MAS (29.3% vs. 19.7%; P=0.03) and PPHN (8.9% vs 2.5%; P=0.003) and were more likely to require surfactant (7.6% vs. 3.2%; P=0.03).
Since the change in guidelines, we observed a decreasing trend in requiring CPAP support (5.8% vs. 2.5%; P=0.06), mechanical ventilation (24.9% vs. 19.1%; P=0.12) and days on ventilator support (5.31 ± 2.36 vs. 4.62 ± 0.65; P=0.65). There was no difference in requiring extracorporeal membrane oxygenation (ECMO), or incidence of death before or after the change in NRP guidelines (0.4% vs. 1.1%; P=0.45). Length of stay was similar between the groups (17.96 ± 1.88 prior to guidelines change vs. 14.53 ± 1.44 after 2016; P=0.14). Based on these results, our study supports the current NRP guidelines.
The optimal management of non-vigorous infants born through MSAF remains debated. Two meta-analyses of four RCTs found no significant difference in MAS incidence or mortality between tracheal suction and no-suction approaches [9,10]. However, one trial indicated a potential increase in MAS (41.3% to 57.1%) in the no-suction group (p=0.052) [11]. A regional study (CPQCC) and a national database (Vermont Oxford Network) reported declining MAS rates following the NRP 7th edition guidelines [12,13]. We observed comparable results in our center.
Post-guideline implementation, Aldhafeeri et al. reported no significant changes in MAS rates or complications related to MAS [14]. Myers et al. showed improved 1-minute Apgar scores and reduced respiratory support needs with no notable change in NICU admission rates [15]. Oommenn et al. noted fewer NICU admissions since change in guidelines [16]. Chiruvolu et al. documented increased respiratory NICU admissions, mechanical ventilation, oxygen therapy, and surfactant use, with a non-significant rise in MAS (5% to 11%) [17].
These differences between various centers may be due to multiple reasons. Different time frames of the two epochs with difference in prenatal, labor and delivery, as well as NICU care and management. Concomitant changes like delayed cord clamping and umbilical cord milking could have played a role. Differences in the resources, patient population and skill sets among the providers may have played a role. Additionally, classifying a baby as non-vigorous can be very subjective.
The large animal study in an ovine model from our lab showed that tracheal suctioning reduced aspirated meconium density and improved oxygenation but delayed PPV initiation by ~100 seconds. Not spending time for tracheal suctioning and directly giving PPV could have been the reason we saw significantly less MAS and PPHN cases in our unit [6]. Clearing the larger airways before meconium reaches the lungs during initial breaths seems like a reasonable step in neonatal resuscitation. However, if deep gasping efforts before apnea have already caused in utero aspiration, this intervention may be ineffective. Additionally, intubation and tracheal suctioning can delay resuscitation, potentially worsening hypoxic-ischemic injury in a compromised newborn.
Our current study has limitations. It is a single-center study with a relatively small sample size. The two-year gap between epochs may have introduced variability in acuity and management styles. We conducted a detailed chart review of all infants with MSAF, applying strict MAS criteria, which may have excluded mild cases. However, consistent guidelines were used across epochs to minimize misclassification with transient tachypnea or other transitional disorders.
5. Conclusion
Based on the improved outcomes of the non-vigorous infants born through meconium in our center, we support the change in NRP guidelines of no routine tracheal suctioning. Large-scale multicenter randomized-controlled clinical trials may be needed to identify the best approach in managing non-vigorous neonates born through MSAF.
Author Contributions
Conceptualization, H.A., P.C. and M.R.; methodology, H.A.; software, H.A.; validation, H.A. and M.R.; formal analysis, H.A. and M.R.; investigation, H.A.; resources, H.A.; data curation, H.A, J.S..; writing—original draft preparation, H.A.; writing—review and editing, H.A., P.C. and M.R.; visualization, H.A.; supervision, M.R.; project administration, H.A. All authors have read and agreed to the published version of the manuscript.
Funding
PC is supported by the following grants: R01HD104909, 1UM1TR005296-01
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of SUNY University at Buffalo IRB (UBIRB) (IRB ID STUDY00006961, approved on 12/12/2022).
Informed Consent Statement
Patient consent was waived. The use or disclosure of protected health information involves no more than a minimal risk to the privacy of individuals, based on, at least, the presence of the following elements: 1) Patient identifiers were protected from improper use and disclosure; 2) Patient identifiers were discarded and destroyed in an appropriate manner after the data collection process; and, 3) Adequate written assurances that the protected health information will not be reused or disclosed to any other person or entity, except as required by law, for authorized oversight of the research study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CPAP | Continuous positive airway pressure |
| PPV | Positive Pressure Ventilation |
| ECMO | Extracorporeal membrane oxygenation |
| ETT | Endotracheal tube |
| iNO | Inhaled nitric oxide |
| IQR | Interquartile range |
| MAS | Meconium aspiration syndrome |
| MSAF | Meconium-stained amniotic fluid |
| NICU | Neonatal intensive care unit |
| NRP | Neonatal resuscitation program |
| PPHN | Persistent pulmonary hypertension of the newborn |
| SEM | Standard error of mean |
References
- Kalra, V.; et al. Neonatal outcomes of non-vigorous neonates with meconium-stained amniotic fluid before and after change in tracheal suctioning recommendation. J Perinatol 2022, 42, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Yurdakok, M. Meconium aspiration syndrome: do we know? Turk J Pediatr 2011, 53, 121–129. [Google Scholar] [PubMed]
- Rawat, M.; et al. Approach to Infants Born Through Meconium Stained Amniotic Fluid: Evolution Based on Evidence? Am J Perinatol 2018, 35, 815–822. [Google Scholar] [PubMed]
- Gupta, A.; Lee, H.C. Revisiting the Latest NRP Guidelines for Meconium: Searching for Clarity in a Murky Situation. Hosp Pediatr 2020, 10, 300–302. [Google Scholar] [CrossRef] [PubMed]
- Textbook of Neonatal Resuscitation; Weiner, G.M., Zaichkin, J., Eds.; American Academy of Pediatrics.
- Lakshminrusimha, S.; et al. Tracheal suctioning improves gas exchange but not hemodynamics in asphyxiated lambs with meconium aspiration. Pediatr Res 2015, 77, 347–55. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, M.; et al. Neonatal Outcomes since the Implementation of No Routine Endotracheal Suctioning of Meconium-Stained Nonvigorous Neonates. Am J Perinatol 2024, 41, 1366–1372. [Google Scholar] [CrossRef] [PubMed]
- Phattraprayoon, N.; Tangamornsuksan, W.; Ungtrakul, T. Outcomes of endotracheal suctioning in non-vigorous neonates born through meconium-stained amniotic fluid: a systematic review and meta-analysis. Arch Dis Child Fetal Neonatal Ed 2021, 106, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Dikou, M.; et al. Routine Tracheal Intubation and Meconium Suctioning in Non-Vigorous Neonates with Meconium-Stained Amniotic Fluid: A Systematic Review and Meta-Analysis. Diagnostics (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Trevisanuto, D.; et al. Tracheal suctioning of meconium at birth for non-vigorous infants: a systematic review and meta-analysis. Resuscitation 2020, 149, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.N.; et al. Effect of endotracheal suctioning just after birth in non-vigorous infants born through meconium stained amniotic fluid: A randomized controlled trial. Clinical Epidemiology and Global Health 2018. [Google Scholar] [CrossRef]
- Edwards, E.M.; et al. NICU Admissions for Meconium Aspiration Syndrome before and after a National Resuscitation Program Suctioning Guideline Change. Children (Basel) 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Kalra, V.K.; et al. Change in neonatal resuscitation guidelines and trends in incidence of meconium aspiration syndrome in California. J Perinatol 2020, 40, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Aldhafeeri, F.M.; et al. Have the 2015 Neonatal Resuscitation Program Guidelines changed the management and outcome of infants born through meconium-stained amniotic fluid? Ann Saudi Med 2019, 39, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Myers, P.; Gupta, A.G. Impact of the Revised NRP Meconium Aspiration Guidelines on Term Infant Outcomes. Hosp Pediatr 2020, 10, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Oommen, V.I.; et al. Resuscitation of non-vigorous neonates born through meconium-stained amniotic fluid: post policy change impact analysis. Arch Dis Child Fetal Neonatal Ed 2021, 106, 324–326. [Google Scholar] [CrossRef] [PubMed]
- Chiruvolu, A.; et al. Delivery Room Management of Meconium-Stained Newborns and Respiratory Support. Pediatrics 2018, 142. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Inclusion/Exclusion criteria.
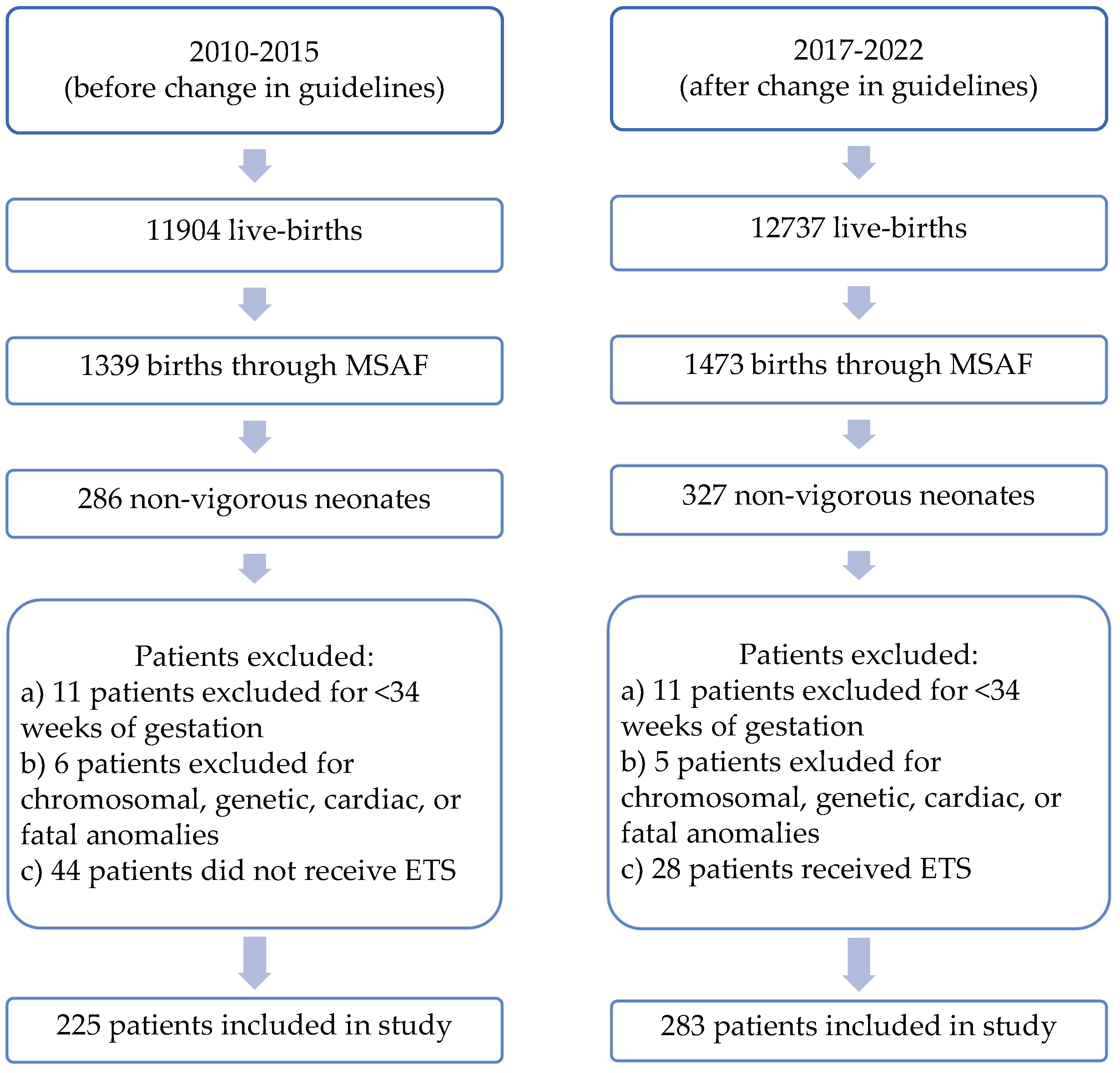

Table 1.
Patient characteristics.
| Characteristics | 2010-2015 | 2017-2022 | P-value |
|---|---|---|---|
| Infants born through MSAF | 1339 | 1473 | - |
| MSAF patients that were born non-vigorous (%) | 225 (16.8%) | 283 (19.2%) | 0.71 |
| Gestational age | 39 3/7 ± 2 days | 38 6/7 ± 6 days | 0.13 |
| Birth weight (kg) | 3.28 ± 0.69 | 3.27 ± 0.65 | 0.77 |
| Male gender | 120 (53%) | 133 (47%) | 0.16 |
| Multiple gestation | 2 (0.9%) | 6 (2.1%) | 0.28 |
| Apgar score 1 minute [Median (IQR)] | 4(2-6) | 3(2-5) | 0.32 |
| Apgar score 5 minute [Median (IQR)] | 7(6-8) | 7(6-8) | 0.08 |
| Apgar score 10 minute [Median (IQR)] | 8(7-8) | 8(6-8) | 0.21 |
| Cord pH | 7.16 ± 0.13 | 7.19 ± 0.12 | 0.07 |
| C-section | 132 (58.7%) | 166 (58.7%) | 0.99 |
| Vaginal delivery | 93 (41.3%) | 117 (41.3%) | |
| General anesthesia for delivery | 36 (16%) | 40 (14%) | 0.57 |
| Spinal/Epidural anesthesia for delivery | 119 (53%) | 153 (54%) |
Table 2.
Outcomes for non-vigorous patients born through MSAF.
| Outcomes for non-vigorous patients born through MSAF | 2010-2015 (n=225) |
2017-2022 (n=283) |
Odds Ratio (95% CI) |
P-value |
|---|---|---|---|---|
| Patients admitted to NICU | 179 (80%) | 241 (85%) | 0.68 (0.43-1.08) | 0.10 |
| Patients admitted to Newborn Nursery | 46 (20%) | 42 (15%) | 1.47 (0.93-2.34) | 0.10 |
| Non-vigorous patients diagnosed with MAS | 66 (29.3%) | 59 (19.7%) | 1.58 (1.05-2.36) | 0.03* |
| Non-vigorous patients diagnosed with PPHN | 20 (8.9%) | 7 (2.5%) | 3.85 (1.60-9.27) | 0.003* |
| Non-vigorous patients who received iNO | 10 (4.4%) | 16 (5.7%) | 0.78 (0.35-1.75) | 0.54 |
| Non-vigorous patients who required ETT | 73 (32.4%) | 103 (36.4%) | 0.83 (0.58-1.21) | 0.35 |
| Non-vigorous patients who required chest compressions | 15 (6.7%) | 14 (4.9%) | 1.37 (0.65-2.91) | 0.41 |
| Non-vigorous patients who required epinephrine | 4 (1.8%) | 6 (2.1%) | 0.84 (0.23-3.00) | 0.78 |
| Non-vigorous patients who required surfactant | 17 (7.6%) | 9 (3.2%) | 2.49 (1.09-5.69) | 0.03* |
| Patients who required supplemental O2 | 69 (30.7%) | 80 (28.3%) | 1.12 (0.76-1.65) | 0.56 |
| Patients who required CPAP support | 13 (5.8%) | 7 (2.5%) | 2.42 (0.95-6.17) | 0.06 |
| Patients who required non-invasive ventilation support | 19 (8.4%) | 20 (6.7%) | 1.21 (0.63-2.33) | 0.56 |
| Patients who required conventional ventilator support | 45 (20%) | 44 (14.7%) | 1.36 (0.86-2.15) | 0.19 |
| Patients who required High Frequency Jet ventilator support | 1 (0.4%) | 2 (0.7%) | 0.63 (0.06-6.96) | 0.70 |
| Patients who required High Frequency Oscillator ventilator support | 10 (4.4%) | 8 (2.8%) | 1.60 (0.62-4.12) | 0.33 |
| Patients who required mechanical ventilation | 56 (24.9%) | 54 (19.1%) | 1.41 (0.92-2.15) | 0.12 |
| Mean ventilator days [per patient] ± SEM | 2.27 ± 0.3 | 2.26 ± 0.32 | 0.98 | |
| Median ventilator days [per patient] (IQR) | 2 (1-2) | 2 (1-3) | ||
| Patients who required non-invasive mechanical ventilation (%) | 101 (44.9%) | 107 (37.8%) | 1.34 (0.94-1.91) | 0.11 |
| Mean days on non-invasive respiratory support [per patient] ± SEM | 5.31 ± 2.36 | 4.62 ± 0.65 | 0.65 | |
| Median days on non-invasive respiratory support [per patient] (IQR) | 2 (1-4) | 2 (1-5) | ||
| Number of patients requiring ECMO | 0 (0%) | 2 (0.4%) | 0.25 (0.01-5.26) | 0.37 |
| Number of patient deaths (%) | 1 (0.4%) | 3 (1.1%) | 0.42 (0.04-4.03) | 0.45 |
| Length of stay | 17.96 ± 1.88 | 14.53 ± 1.44 | 0.14 | |
| *p-value <0.05 | ||||
| CPAP: Continuous positive airway pressure. ECMO: Extracorporeal membrane oxygenation. ETT: Endotracheal Tube. iNO: inhaled nitric oxide. IQR: Interquartile range. MAS: Meconium aspiration syndrome. MSAF: Meconium-stained amniotic fluid. NICU: Neonatal intensive care unit. PPHN: Persistent pulmonary hypertension of the newborn. SEM: Standard error of mean. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



