Submitted:
07 June 2025
Posted:
09 June 2025
You are already at the latest version
Abstract
Background/Objectives: We investigated the potential protective effect of dietary curcumin in curry meals against the risk of cognitive decline and incident neurocognitive disorder (mild cognitive impairment and dementia) in the population-based Singapore Longitudinal Ageing cohort study. Methods: Curry consumption was categorised as ‘never or rarely’, ‘occasionally’: <once/month, ‘often’: >once/month to <once/week, ‘very often’: >once/week, or ‘daily’. Among 2920 participants (mean age 65.5 ± SD 7.1) who were free of stroke, Parkinson disease, or traumatic brain injury at baseline, cognitive decline (MMSE drop ≥2) was assessed at 3-5 year (mean 4.5) follow up. Risk of incident MCI or dementia was assessed at follow up among 2446 participants who were free of MCI and dementia at baseline. Results: Higher levels of curry consumption were associated with a decreasing linear trend of cognitive decline (p=0.037). Controlling for baseline confounders, OR relative to ‘never or rare’ consumption decreased from 0.73 for occasional consumption to 0.66 for daily consumption (p linear trend=0.15); the OR for ‘often’ consuming curry was 0.68, 95%CI=0.48-0.95. The cumulated incidence of MCI-dementia decreased from 13.1% in those who never or rarely consumed curry to 3.6% in those who daily consumed curry (linear p<0.001). The adjusted OR across levels of curry consumption showed a significant linear trend (p=0.021) from OR=0.61 (p<0.05) for occasional consumption to OR=0.21 (p<0.001) for daily consumption. Conclusions: Dietary curcumin through curry consumption is associated with a dose-dependent decrease in incidence of cognitive decline and MCI-dementia in this Asian population of community-dwelling older adults.
Keywords:
cucumin
; curry
; neurocognitive disorder
; population-based study
1. Introduction
Numerous laboratory studies have documented the potent antioxidant, anti-inflammatory, antimicrobial, antiviral, anti-neoplastic and anti-aging activities of curcumin, a polyphenolic compound isolated from the roots of Curcuma longa [1,2,3]. Its therapeutic potential is intensively investigated in over 100 clinical trials for chronic diseases including cancers, diabetes, obesity, cardiovascular, pulmonary, neurological and autoimmune diseases [1].
Dementia is a devastating cognitive disorder due to brain neurodegeneration characterized by underlying β amyloid and tau pathology, cerebral microvascular disease, and neuro-inflammation. Experimental evidence strongly suggest that curcumin has the potential to prevent accelerated cognitive decline in humans [4]. Curcumin has the ability to cross the blood–brain barrier. In neural tissues, curcumin binds to β amyloid (Aβ) and tau, inhibiting Aβ aggregation and modulate tau processing [5,6,7,8,9]. Animal studies show that curcumin decreases brain Aβ deposition and plaque load in transgenic mouse models of AD [10,11]. Its protective effect against microvascular brain pathology is evidenced by experimental data showing its anti-platelet and anti-diabetic activities, as well as cardio-protective activities ameliorating cardiac hypertrophy and chronic heart failure [12,13,14,15,16,17,18,19]. Additionally, there is ample evidence of its potent anti-inflammatory activity attenuating neuro-inflammation. Animal studies also show that curcumin improves cognitive function [20,21]. Finally, a limited number of randomized controlled trials in humans suggest that curcumin could be safely and effectively used to slow cognitive decline [4,22,23,24,25,26].
Turmeric, from which curcumin is extracted, is used widely as a coloring agent and traditional Indian and Chinese medicine. As a food additive, it is the predominant source of curcumin in Asian diets. In the form of the Indian spice, turmeric is consumed in curry meals by millions of people in sub-continental India, South East Asia and other parts of the world. Only a limited number of naturalistic studies have investigated the potential cognitive benefits of dietary food source(s) of curcumin in humans. We first showed in a population-based observational study of community-dwelling middle-aged and older adults that there was a cross-sectional association of curry consumption with higher global cognitive performance score on the Mini-Mental State Examination (MMSE) [27]. Subsequent longitudinal observations in the Singapore Longitudinal Ageing Study (SLAS) follow up cohort showed that the consumption of dietary curcumin was associated with the maintenance over time of higher functioning on attention, working memory, vis[29,30uospatial constructional ability, language and executive function. The effect sizes ranged from 0.13 and 0.30 in sub-groups of participants [28].
This report presents the results of longitudinal analysis of the association of curry consumption with the risk of cognitive decline and incident neurocognitive disorder (mild cognitive impairment and dementia) from 4.5 years of follow up of community-dwelling older adults in the SLAS prospective cohort study.
2. Materials and Methods
2.1. Study Design and Participants
Details of the SLAS study design and methodology are described in previous publications [29,30]. Briefly, the SLAS cohort included Singapore citizens who were residents in study locations and aged ≥55years at recruitment, excluding individuals who were unable to participate due to severe physical or mental disability. The SLAS included two combined population cohorts: SLAS-1 recruited 2804 participants in South-East Singapore from Sep 2003 to Dec 2004, and SLAS-2 recruited 3270 participants in South-West Singapore from Mar 2009 to Jun 2013. First wave follow-up visits and assessments were conducted at approximately 3–5 (mean 4.5) years after baseline assessment: Mar 2005–Sep 2007 for SLAS-1, and Jan 2013–Aug 2018 for SLAS-2.
The study was approved by National University of Singapore Institutional Review Board (Protocol Code: 04–140), in accordance with the relevant guidelines and regulations of the Declaration of Helsinki and the Belmont Report. All participants gave written informed consent to participate in the study.
2.2. Measurements
An extensive range of socio-demographic, lifestyle, behavioral, psychological, medical and health data at baseline were collected by trained nurses from face-to-face questionnaire interviews during home visits and clinical and physiological measurements performed in a local study site.
2.2.1. Curry Consumption
At baseline and follow up interviews, the frequency of consumption of curry were asked and categorized as never or rarely (<once a year), occasionally (at least once/year to less than once/month), often (at least once/month to less than once/week, very often (at least once a week) or daily. An additional question asked whether curry consumption had remained mostly unchanged or have changed. Data indicating consistent responses at baseline and follow up interviews were used to assign participants unequivocally to the highest and the lowest consumption category. Participants who consistently reported ‘occasional’ or ‘often’ consumption frequencies at both baseline and follow up were also assigned as such to the appropriate category. For inconsistent responses that differed by one response category between baseline and follow up, we used the higher consumption response to assign to the nearest ‘occasional’ or ‘often’ categories. For more widely inconsistent responses, we used the average response score to assign them to the nearest response category, either ‘occasional’ or ‘often’.
2.2.2. Diagnosis of Neurocognitive Disorder (MCI and Dementia)
Cases of MCI and dementia were determined from two-staged procedure of cognitive screening and assessment, followed by consensus diagnosis based on DSM-V criteria performed by a three-member expert panel of geriatricians and psychiatrists.
Cognitive screening was performed using the locally modified and validated English, Chinese and Malay translated versions of Mini-Mental State Examination (MMSE), with appropriate education- and ethnic-stratified cut-offs [31,32]. Subjective cognitive complaint was ascertained from self-report (“Do you feel you have more problems with memory than most?” and informant reports (IQCODE) of memory and cognitive problems [33,34].
Post screening cognitive assessment was performed using Clinical Dementia Scale (CDR) and a battery of neurocognitive tests which included attention (digit span forward and backward) and spatial span forward and backward, memory (Rey Auditory Verbal Learning Test immediate and delayed recall, visual reproduction immediate and delayed recall), executive function (Symbol Digit Modality Test, Design Fluency and Trail Making Test Part B, language (categorical verbal fluency) and visuospatial abilities (block design). Details of the neurocognitive tests and their normative values have been described in a previous publication [35,36].
MCI diagnosis was based on published criteria [37]: (1) subjective memory and cognitive difficulties, or IQCODE score >3.3; (2) objective cognitive impairment in 1 or more domains: MMSE global score ranging from 24 to 27, or a decline of MMSE ≥2 points from baseline; and at least one neurocognitive domain (attention, memory, executive function, language or visuospatial abilities) score 1 to 2 standard deviations (SDs) less than the age and education-adjusted mean values, or drop from baseline of 0.5 SD during follow-up assessments; (3) Clinical Dementia Scale (CDR) global score ≥0.5 [38]; (4) essentially independent in performing Basic Activities of Daily Living (BADL); and (5) not demented.
Diagnosis of dementia required (1) evidence of objective cognitive deficit (MMSE total score ≤23, or neurocognitive domain score that was 2 SDs less than the mean values (age and education stratified), and (2) presence of functional disability (needing help with at least 1 BADL activities or Clinical Dementia Rating (CDR) global score ≥1). Participants who did not meet the criteria for MCI or dementia were classified as cognitively normal (CN).
Cognitive decline was defined by a drop of MMSE score at follow up of 2 or more points from baseline.
2.2.3. Covariates
Measurements of potential confounding risk factors included sex, age (single years), ethnicity (Chinese versus non-Chinese, that includes Malay, Indian and Other), and education (None, 1-6 years, >6 years). Health behavioral factors included smoking (never, past smoker, current smoker), alcohol (≥once/week), and physical activity score, social activity score and productive activity score which were calculated from the number and frequencies of usual participation in 18 different categories of physical, social, and productive activities [30]. Cardio-metabolic factors included central obesity (waist circumference ≥80cm in women and ≥90cm in men) [39]. Hypertension was defined by systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg [40], or a self-report history of hypertension diagnosis and treatment, verified by recorded names of drugs shown on medication packages. Diabetes was defined by fasting blood glucose concentrations of ≥5.6 mmol/L [41] or a self-report history of diabetes diagnosis and treatment. Dyslipidaemia was defined as either triglyceride levels of ≥1.7 mmol/L or high-density lipoprotein cholesterol <1 mmol/L in men and <1.3 mmol/L in women [42]. Prevalent cardiovascular disease included self-report histories of stroke, coronary disease, myocardial infarct, or heart failure. Depressive symptoms were assessed by the locally translated and validated version of the 15-item Geriatric Depression Scale (GDS) [43].
2.3. Analysis
In the original cohort of 6074 participants, a total of 5035 participants were free of stroke, Parkinson disease, or traumatic brain injury and had available data on curry intake. Longitudinal analyses were performed on data for cognitive decline in 2920 participants with data available for MMSE at follow up (432 who showed cognitive decline and 2489 who did not show cognitive decline). See flow chart in Figure 1. After excluding 101 participants who had dementia, 626 participants who had MCI, and 149 with unknown neurocognitive status, there were 4159 cognitive normal participants at baseline. Longitudinal data analysis for incident MCI or dementia involved 2446 participants who were free of MCI and dementia at baseline and provided available data on NCD status at follow up.
We used ANOVA tests for continuous variables and chi-squared tests for categorical variables to examine differences in baseline characteristics between participants who exhibited cognitive decline or progressed to NCD at follow-up and those who did not. The odds ratio (OR) with their 95% confidence intervals (CIs) of associations of curry intake with cognitive decline or incident NCD was estimated in binary logistic regression models adjusting for the baseline co-variables, as described above. Data analysis was performed using IBM-SPSS version 25. All statistical significance tests were two-sided, and an α-level of 0.05 was considered significant.
3. Results
The mean (±SD) age of the 2920 study participants was 65.5 (±7.1) years, and 65.2% were women. Participants who reported higher levels of curry consumption were more likely to be younger, men, of non-Chinese (Malay, Indian) ethnicity, better educated, had higher levels of social and productive (mentally stimulating) activity, more central obesity, diabetes, and had lower GDS depression scores (Table 1). Greater frequency of curry consumption was significantly associated with higher mean levels of MMSE global cognition.
3.1. Cognitive Decline
Curry consumption was inversely associated with cognitive decline. (Table 2 and Table 3) Increasing levels of curry consumption was associated with decreased likelihood of cognitive decline, from 18.7% in those who never or rarely consumed curry to 12.8% who consumed curry daily, p for linear trend=0.037. Controlling for the influence of baseline confounders, the adjusted OR of association showed a similar linear trend of association from 0.73 to 0.66 (p=0.15). (Table 3 and Figure 2) The lowered OR of association with cognitive decline was significant for often consuming curry (OR=0.68, 95%CI=0.48-0.95) compared to never or rarely consuming curry.
3.2. Incident MCI-Dementia
Among the 2446 participants who were cognitively normal at baseline, an increasing level of curry consumption was inversely associated with the risk of incident MCI-dementia, p for linear trend<0.001. (Table 2) The cumulated incidence of MCI-dementia decreased from 13.1% in those who never or rarely consumed curry to 3.6% in those who daily consumed curry. (Table 4 and Figure 2) Controlling for the influence of baseline confounders, the adjusted OR across increasing levels of curry consumption showed a significant linear trend (p=0.021), OR=0.61 (p<0.05) for occasional consumption compared to OR=0.21 (p<0.001) for daily consumption.
4. Discussion
Results from animal studies consistently demonstrate the positive effects of curcumin and its analogues on cognition. In senescence accelerated mouse (SAM)-prone 8 (SAMP8) mice, intragastric administration of curcumin (20 or 50 mg/kg) for 25 days had a dose-dependent effect on decreased latency in the Morris Water Maze (MWM), whereby mice given the highest dose had the same latency as that reported with the control group SAMR1 mice [21]. Qi Chen and colleagues [45] investigated the cognitive effects of J147, a structural analog of curcumin in young Sprague Dawley (SD) rats and C57BL/6 mice. In young SD rats, J147 facilitated long-term potentiation (LTP) induction in the hippocampus, and improved performance in a novel object recognition test. J147 supplemented C57BL/6 mice demonstrated a significant improvement in spatial memory in novel object location (NOL), short-term memory on the Y-maze, and fewer errors than control mice on the retention test portion of the Barnes maze.
Randomized trials of curcumin for improving cognition in non-demented elderly has generated mixed results. In a randomized, double-blind, placebo-controlled trial of 60 non-demented adults aged 60-85 years, a lipid curcumin formulation improved working memory after both acute and chronic administration. Subjects on curcumin did significantly better on the digit vigilance task after acute treatment. Subjects on both the acute and chronic curcumin treatment had significantly better performance on the serial 3 subtraction task than their counterparts on placebo [23].
Rainey-Smith et al. [46] assessed the efficacy of curcumin in non-demented elderly in a 48-week randomized placebo-controlled, double-blind study. There was a significant difference in cognition measures observed at 24-week whence the subjects in the curcumin group did significantly better on the Montreal Cognitive Assessment (MoCA) compared to the placebo group. However, there was no significant between-group difference at 48 weeks when the intervention was completed. These results suggest that curcumin is a promising therapeutic agent for cognitive decline although the findings remain inconclusive at this time.
Studies have demonstrated the Alzheimer disease-modifying effects of curcumin [2]. In mice with Alzheimer’s disease (APP/PS1 double knockout model), 6-month curcumin diet was associated with better working and long-term memory performance on Morris water maze in a dose-dependent manner. The mice also showed a reduction in brain amyloid beta 42 (Aβ42) aggregates and better clearance of the dissolved aggregates. There was a significantly higher number of autophagosomes [47,48] in the CA1 region of the curcumin groups along with an increased expression of Beclin 1 and downregulation of the PI3K/Akt/mTOR signaling pathway [49]. Curcumin could protect neuron-like PC12 rat cells and umbilical endothelial cells against Aβ through the inhibition of oxidative damage and tau hyperphosphorylation [50], promote Aβ uptake from macrophages of AD patients [51], and reduce fibril formation and extension dose-dependently, also destabilizing preformed Aβ fibrils [52,53,54]. Furthermore, curcumin decreases levels of Aβ-induced radical oxygen species [55] and inhibits amyloid precursor protein (APP) cleavage [56]. Of note, in rat hippocampal slices treated with Aβ oligomers, curcumin restores synaptic plasticity by enhancing long-term potentiation [57]. Since curcumin clears Aβ and tau and promotes autophagosomes in the brain, this might also be a future target for clinical investigations.
Strengths and limitations. In this study, real-world observations of the cognitive benefits in humans are achieved in a large population-based cohort of community-dwelling older adults followed-up for a mean of 4.5 years. The follow up duration is relatively short. While this is appropriate for estimating adequate numbers of persons progressing from normal cognition to incident MCI, the number of incident cases of dementia was small, and should be accomplished with longer periods of follow up. The observed estimates of risk associated with exposure to curry consumption are likely to be underestimated due to survival bias. This is because the study selectively followed up participants with relatively healthy risk factor profile and favourable cognitive status. A notable strength is that incident cases of MCI and dementia were determined using rigorous clinical assessment and consensus panel diagnosis. One should cautiously generalize the findings to other populations, considering that the study was conducted in a population of Asian ethnicity with higher levels of curry consumption. Nevertheless, it is interesting to surmise that populations with relatively lower prevalence and modest levels of curry consumption could experience similar cognitive benefits, given that the significant effects were observed at moderate levels of curry consumption. A non-linear dose-dependent effect of curcumin exposure is plausible and interesting because laboratory evidence has documented a pronounced hermetic effect of curcumin on diverse biological processes, exhibiting biphasic dose-responses, with low doses having stronger effects than high doses for some effects [58]. This has also been observed with higher cognitive performance at relatively lower levels of curry consumption in a previous study [28].
Our results support the cognitive benefits of curcumin from natural dietary food sources in humans. They suggest that increased consumption of curcumin in a turmeric-rich diet could enhance population health by reducing the rate of cognitive decline and risk of developing MCI or dementia. Further studies should be conducted to replicate these findings in other similarly exposed populations.
Author Contributions
Conceptualization, T.P.N., Y.L.; methodology, T.P.N., Y.L.; formal analysis, T.P.N., Y.L.; investigation, Y.L., Q.G., X.G., T.S.L., W.S.L., P.Y., C.Y.C., I.R., T.M.L, K.B.Y.; data curation, T.P.N., Y.L.; writing—original draft preparation, T.P.N., Y.L.; writing—review and editing, T.P.N., Y.L., T.S.L., W.S.L., P.Y., C.Y.C., I.R., T.M.L, K.B.Y., Q.G., X.G.; visualization, T.P.N.; project administration, Q.G., X.G., and K.B.Y.; funding acquisition, T.P.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Agency for Science, Technology and Research (A*STAR) Biomedical Research Council, grant number BMRC/08/1/21/19/567 and the National Medical Research Council, grant numbers NMRC/1108/2007 and NMRC/CIRG/1409/2014.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of National University of Singapore (protocol code 04-140).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank the following voluntary welfare organizations for their support: Geylang East Home for the Aged, Presbyterian Community Services, St Luke’s Eldercare Services, Thye Hua Kwan Moral Society (Moral Neighbourhood Links), Yuhua Neighbourhood Link, Henderson Senior Citizens’ Home, NTUC Eldercare Co-op Ltd., Thong Kheng Seniors Activity Centre (Queenstown Centre) and Redhill Moral Seniors Activity Centre.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| Aβ | β amyloid |
| MMSE | Mini-Mental State Examination |
| SLAS | Singapore Longitudinal Ageing Study |
| CDR | Clinical Dementia Scale |
| SD | standard deviation |
| BADL | Basic Activities of Daily Living |
| CN | cognitively normal |
| GDS | Geriatric Depression Scale |
| OR | odds ratio |
| CI | confidence interval |
| SAM | senescence accelerated mouse |
| MWM | Morris Water Maze |
| SD | Sprague Dawley |
| LTP | long-term potentiation |
| NOL | novel object location |
| MoCA | Montreal Cognitive Assessment |
| APP | amyloid precursor protein |
References
- Salehi B, Stojanović-Radić Z, Matejić J, Sharifi-Rad M, Anil Kumar NV, Martins N, et al. The therapeutic potential of curcumin: A review of clinical trials. European Journal of Medicinal Chemistry. 2019;163:527-45. [CrossRef]
- Nicoliche T, Bartolomeo CS, Lemes RMR, Pereira GC, Nunes TA, Oliveira RB, et al. Antiviral, anti-inflammatory and antioxidant effects of curcumin and curcuminoids in SH-SY5Y cells infected by SARS-CoV-2. Scientific Reports. 2024;14(1):10696. [CrossRef]
- Fu Y-S, Chen T-H, Weng L, Huang L, Lai D, Weng C-F. Pharmacological properties and underlying mechanisms of curcumin and prospects in medicinal potential. Biomedicine & Pharmacotherapy. 2021;141:111888. [CrossRef]
- Sarker MR, Franks SF. Efficacy of curcumin for age-associated cognitive decline: a narrative review of preclinical and clinical studies. GeroScience. 2018;40(2):73-95. Epub 2018/04/22. PubMed PubMed Central PMCID: PMCPMC5964053. [CrossRef] [PubMed]
- Zang W-B, Wei H-L, Zhang W-W, Ma W, Li J, Yao Y. Curcumin hybrid molecules for the treatment of Alzheimer’s disease: Structure and pharmacological activities. European Journal of Medicinal Chemistry. 2024;265:116070. [CrossRef]
- Lo Cascio F, Puangmalai N, Ellsworth A, Bucchieri F, Pace A, Palumbo Piccionello A, et al. Toxic Tau Oligomers Modulated by Novel Curcumin Derivatives. Scientific Reports. 2019;9(1):19011. [CrossRef]
- Benameur T, Giacomucci G, Panaro MA, Ruggiero M, Trotta T, Monda V, et al. New Promising Therapeutic Avenues of Curcumin in Brain Diseases. Molecules (Basel, Switzerland). 2021;27(1). Epub 2022/01/12. PubMed PubMed Central PMCID: PMCPMC8746812. [CrossRef] [PubMed]
- Chen M, Du ZY, Zheng X, Li DL, Zhou RP, Zhang K. Use of curcumin in diagnosis, prevention, and treatment of Alzheimer’s disease. Neural regeneration research. 2018;13(4):742-52. Epub 2018/05/04. PubMed PubMed Central PMCID: PMCPMC5950688. [CrossRef] [PubMed]
- Askarizadeh A, Barreto GE, Henney NC, Majeed M, Sahebkar A. Neuroprotection by curcumin: A review on brain delivery strategies. International journal of pharmaceutics. 2020;585:119476. Epub 2020/05/31. [CrossRef] [PubMed]
- Pradeep H, Yenisetti SC, Rajini PS, Muralidhara M. Chapter 16 - Neuroprotective Propensity of Curcumin: Evidence in Animal Models, Mechanisms, and Its Potential Therapeutic Value. In: Farooqui T, Farooqui AA, editors. Curcumin for Neurological and Psychiatric Disorders: Academic Press; 2019. p. 301-23.
- Zhang C, Browne A, Child D, Tanzi RE. Curcumin Decreases Amyloid-β Peptide Levels by Attenuating the Maturation of Amyloid-β Precursor Protein*. Journal of Biological Chemistry. 2010;285(37):28472-80. [CrossRef]
- Bozkurt O, Kocaadam-Bozkurt B, Yildiran H. Effects of curcumin, a bioactive component of turmeric, on type 2 diabetes mellitus and its complications: an updated review. Food & Function. 2022;13(23):11999-2010. [CrossRef]
- Tabeshpour J, Hashemzaei M, Sahebkar A. The regulatory role of curcumin on platelet functions. Journal of cellular biochemistry. 2018;119(11):8713-22. Epub 2018/08/12. [CrossRef] [PubMed]
- Li H, Sureda A, Devkota HP, Pittalà V, Barreca D, Silva AS, et al. Curcumin, the golden spice in treating cardiovascular diseases. Biotechnology advances. 2020;38:107343. Epub 2019/02/05. [CrossRef] [PubMed]
- Bai X-J, Hao J-T, Wang J, Zhang W-F, Yan C-P, Zhao J-H, et al. Curcumin inhibits cardiac hypertrophy and improves cardiovascular function via enhanced Na+/Ca2+ exchanger expression after transverse abdominal aortic constriction in rats. Pharmacological Reports. 2018;70(1):60-8. [CrossRef]
- Cox FF, Misiou A, Vierkant A, Ale-Agha N, Grandoch M, Haendeler J, et al. Protective Effects of Curcumin in Cardiovascular Diseases-Impact on Oxidative Stress and Mitochondria. Cells. 2022;11(3). Epub 2022/02/16. PubMed PubMed Central PMCID: PMCPMC8833931. [CrossRef] [PubMed]
- Saeidinia A, Keihanian F, Butler AE, Bagheri RK, Atkin SL, Sahebkar A. Curcumin in heart failure: A choice for complementary therapy? Pharmacological Research. 2018;131:112-9. [CrossRef]
- Hussain Y, Abdullah, Khan F, Alsharif KF, Alzahrani KJ, Saso L, et al. Regulatory Effects of Curcumin on Platelets: An Update and Future Directions. Biomedicines. 2022;10(12). Epub 2022/12/24. PubMed PubMed Central PMCID: PMCPMC9775400. [CrossRef] [PubMed]
- Marton LT, Pescinini-e-Salzedas LM, Camargo MEC, Barbalho SM, Haber JFdS, Sinatora RV, et al. The Effects of Curcumin on Diabetes Mellitus: A Systematic Review. Frontiers in Endocrinology. 2021;12. [CrossRef]
- Fan L, Zhang Z. Therapeutic potential of curcumin on the cognitive decline in animal models of Alzheimer’s disease: a systematic review and meta-analysis. Naunyn-Schmiedeberg’s Archives of Pharmacology. 2024;397(7):4499-509. [CrossRef]
- Sun CY, Qi SS, Zhou P, Cui HR, Chen SX, Dai KY, et al. Neurobiological and pharmacological validity of curcumin in ameliorating memory performance of senescence-accelerated mice. Pharmacology, biochemistry, and behavior. 2013;105:76-82. Epub 2013/02/14. [CrossRef] [PubMed]
- Hishikawa N, Takahashi Y, Amakusa Y, Tanno Y, Tuji Y, Niwa H, et al. Effects of turmeric on Alzheimer’s disease with behavioral and psychological symptoms of dementia. Ayu. 2012;33(4):499-504. Epub 2013/06/01. PubMed PubMed Central PMCID: PMCPMC3665200. [CrossRef] [PubMed]
- Cox KH, Pipingas A, Scholey AB. Investigation of the effects of solid lipid curcumin on cognition and mood in a healthy older population. Journal of psychopharmacology (Oxford, England). 2015;29(5):642-51. Epub 2014/10/04. [CrossRef] [PubMed]
- Rainey-Smith SR, Brown BM, Sohrabi HR, Shah T, Goozee KG, Gupta VB, et al. Curcumin and cognition: a randomised, placebo-controlled, double-blind study of community-dwelling older adults. The British journal of nutrition. 2016;115(12):2106-13. Epub 2016/04/23. [CrossRef] [PubMed]
- Cox KHM, White DJ, Pipingas A, Poorun K, Scholey A. Further Evidence of Benefits to Mood and Working Memory from Lipidated Curcumin in Healthy Older People: A 12-Week, Double-Blind, Placebo-Controlled, Partial Replication Study. Nutrients. 2020;12(6). Epub 2020/06/10. PubMed PubMed Central PMCID: PMCPMC7352411. [CrossRef] [PubMed]
- Das SS, Gopal PM, Thomas JV, Mohan MC, Thomas SC, Maliakel BP, et al. Influence of CurQfen(®)-curcumin on cognitive impairment: a randomized, double-blinded, placebo-controlled, 3-arm, 3-sequence comparative study. Frontiers in dementia. 2023;2:1222708. Epub 2024/07/31. PubMed PubMed Central PMCID: PMCPMC11285547. [CrossRef] [PubMed]
- Ng TP, Chiam PC, Lee T, Chua HC, Lim L, Kua EH. Curry consumption and cognitive function in the elderly. American journal of epidemiology. 2006;164(9):898-906. Epub 2006/07/28. [CrossRef] [PubMed]
- Ng TP, Nyunt MSZ, Gao Q, Gwee X, Chua DQL, Yap KB. Curcumin-Rich Curry Consumption and Neurocognitive Function from 4.5-Year Follow-Up of Community-Dwelling Older Adults (Singapore Longitudinal Ageing Study). Nutrients. 2022;14(6). Epub 2022/03/27. PubMed PubMed Central PMCID: PMCPMC8952785. [CrossRef] [PubMed]
- Ng TP, Feng L, Nyunt MS, Feng L, Gao Q, Lim ML, et al. Metabolic Syndrome and the Risk of Mild Cognitive Impairment and Progression to Dementia: Follow-up of the Singapore Longitudinal Ageing Study Cohort. JAMA neurology. 2016;73(4):456-63. Epub 2016/03/02. [CrossRef] [PubMed]
- Niti M, Yap KB, Kua EH, Tan CH, Ng TP. Physical, social and productive leisure activities, cognitive decline and interaction with APOE-epsilon 4 genotype in Chinese older adults. International psychogeriatrics. 2008;20(2):237-51. Epub 2008/01/15. [CrossRef] [PubMed]
- Ng TP, Niti M, Chiam PC, Kua EH. Ethnic and educational differences in cognitive test performance on mini-mental state examination in Asians. The American journal of geriatric psychiatry : official journal of the American Association for Geriatric Psychiatry. 2007;15(2):130-9. Epub 2007/02/03. [CrossRef] [PubMed]
- Cheung YB, Xu Y, Feng L, Feng L, Nyunt MS, Chong MS, et al. Unconditional and Conditional Standards Using Cognitive Function Curves for the Modified Mini-Mental State Exam: Cross-Sectional and Longitudinal Analyses in Older Chinese Adults in Singapore. The American journal of geriatric psychiatry : official journal of the American Association for Geriatric Psychiatry. 2015;23(9):915-24. Epub 2014/09/28. [CrossRef] [PubMed]
- Jorm AF, Scott R, Cullen JS, MacKinnon AJ. Performance of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) as a screening test for dementia. Psychological medicine. 1991;21(3):785-90. Epub 1991/08/01. [CrossRef] [PubMed]
- Cherbuin N, Anstey KJ, Lipnicki DM. Screening for dementia: a review of self- and informant-assessment instruments. International psychogeriatrics. 2008;20(3):431-58. Epub 2008/02/22. [CrossRef] [PubMed]
- Feng L, Ng TP, Chuah L, Niti M, Kua EH. Homocysteine, folate, and vitamin B-12 and cognitive performance in older Chinese adults: findings from the Singapore Longitudinal Ageing Study. The American journal of clinical nutrition. 2006;84(6):1506-12. Epub 2006/12/13. [CrossRef] [PubMed]
- Lee CK, Collinson SL, Feng L, Ng TP. Preliminary normative neuropsychological data for an elderly chinese population. The Clinical neuropsychologist. 2012;26(2):321-34. Epub 2012/02/01. [CrossRef] [PubMed]
- Segal, DL. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR). The Corsini Encyclopedia of Psychology. p. 1-3.
- Morris, JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. 1993;43(11):2412-4. Epub 1993/11/01. [CrossRef] [PubMed]
- Lee YS, Biddle S, Chan MF, Cheng A, Cheong M, Chong YS, et al. Health Promotion Board-Ministry of Health Clinical Practice Guidelines: Obesity. Singapore medical journal. 2016;57(6):292-300. Epub 2016/06/30. PubMed PubMed Central PMCID: PMCPMC4971447. [CrossRef] [PubMed]
- Tay JC, Sule AA, Chew EK, Tey JS, Lau T, Lee S, et al. Ministry of Health Clinical Practice Guidelines: Hypertension. Singapore medical journal. 2018;59(1):17-27. Epub 2018/01/30. [CrossRef] [PubMed]
- Goh SY, Ang SB, Bee YM, Chen YT, Gardner DS, Ho ET, et al. Ministry of Health Clinical Practice Guidelines: Diabetes Mellitus. Singapore medical journal. 2014;55(6):334-47. Epub 2014/07/16. PubMed PubMed Central PMCID: PMCPMC4294061. [CrossRef] [PubMed]
- Tai ES, Chia BL, Bastian AC, Chua T, Ho SC, Koh TS, et al. Ministry of Health Clinical Practice Guidelines: Lipids. Singapore medical journal. 2017;58(3):155-66. Epub 2017/04/01. [CrossRef] [PubMed]
- Nyunt MS, Fones C, Niti M, Ng TP. Criterion-based validity and reliability of the Geriatric Depression Screening Scale (GDS-15) in a large validation sample of community-living Asian older adults. Aging & mental health. 2009;13(3):376-82. Epub 2009/06/02. [CrossRef] [PubMed]
- Kuszewski JC, Wong RHX, Howe PRC. Can Curcumin Counteract Cognitive Decline? Clinical Trial Evidence and Rationale for Combining ω-3 Fatty Acids with Curcumin. Advances in nutrition (Bethesda, Md). 2018;9(2):105-13. Epub 2018/04/17. PubMed PubMed Central PMCID: PMCPMC5916424. [CrossRef] [PubMed]
- Chen Q, Prior M, Dargusch R, Roberts A, Riek R, Eichmann C, et al. A novel neurotrophic drug for cognitive enhancement and Alzheimer’s disease. PloS one. 2011;6(12):e27865. Epub 2011/12/24. PubMed PubMed Central PMCID: PMCPMC3237323. [CrossRef] [PubMed]
- Rainey-Smith SR, Brown BM, Sohrabi HR, Shah T, Goozee KG, Gupta VB, et al. Curcumin and cognition: a randomised, placebo-controlled, double-blind study of community-dwelling older adults. British Journal of Nutrition. 2016;115(12):2106-13. Epub 04/22. [CrossRef]
- Murrow L, Debnath J. Autophagy as a Stress-Response and Quality-Control Mechanism: Implications for Cell Injury and Human Disease. Annual Review of Pathology: Mechanisms of Disease. 2013;8(Volume 8, 2013):105-37. [CrossRef]
- Ravanan P, Srikumar IF, Talwar P. Autophagy: The spotlight for cellular stress responses. Life Sciences. 2017;188:53-67. [CrossRef]
- Wang C, Zhang X, Teng Z, Zhang T, Li Y. Downregulation of PI3K/Akt/mTOR signaling pathway in curcumin-induced autophagy in APP/PS1 double transgenic mice. European Journal of Pharmacology. 2014;740:312-20. [CrossRef]
- Park S-Y, Kim H-S, Cho E-K, Kwon B-Y, Phark S, Hwang K-W, et al. Curcumin protected PC12 cells against beta-amyloid-induced toxicity through the inhibition of oxidative damage and tau hyperphosphorylation. Food and Chemical Toxicology. 2008;46(8):2881-7. [CrossRef]
- Zhang L, Fiala M, Cashman J, Sayre J, Espinosa A, Mahanian M, et al. Curcuminoids enhance amyloid-beta uptake by macrophages of Alzheimer’s disease patients. Journal of Alzheimer’s disease : JAD. 2006;10(1):1-7. Epub 2006/09/22. [CrossRef] [PubMed]
- Kim H, Park BS, Lee KG, Choi CY, Jang SS, Kim YH, et al. Effects of naturally occurring compounds on fibril formation and oxidative stress of beta-amyloid. Journal of agricultural and food chemistry. 2005;53(22):8537-41. Epub 2005/10/27. [CrossRef] [PubMed]
- Ono K, Hasegawa K, Naiki H, Yamada M. Curcumin has potent anti-amyloidogenic effects for Alzheimer’s beta-amyloid fibrils in vitro. Journal of neuroscience research. 2004;75(6):742-50. Epub 2004/03/03. [CrossRef] [PubMed]
- Yang F, Lim GP, Begum AN, Ubeda OJ, Simmons MR, Ambegaokar SS, et al. Curcumin inhibits formation of amyloid beta oligomers and fibrils, binds plaques, and reduces amyloid in vivo. The Journal of biological chemistry. 2005;280(7):5892-901. Epub 2004/12/14. [CrossRef] [PubMed]
- Shimmyo Y, Kihara T, Akaike A, Niidome T, Sugimoto H. Epigallocatechin-3-gallate and curcumin suppress amyloid beta-induced beta-site APP cleaving enzyme-1 upregulation. Neuroreport. 2008;19(13):1329-33. Epub 2008/08/13. [CrossRef] [PubMed]
- Lin R, Chen X, Li W, Han Y, Liu P, Pi R. Exposure to metal ions regulates mRNA levels of APP and BACE1 in PC12 cells: blockage by curcumin. Neuroscience letters. 2008;440(3):344-7. Epub 2008/06/28. [CrossRef] [PubMed]
- Ahmed T, Gilani AH, Hosseinmardi N, Semnanian S, Enam SA, Fathollahi Y. Curcuminoids rescue long-term potentiation impaired by amyloid peptide in rat hippocampal slices. Synapse (New York, NY). 2011;65(7):572-82. Epub 2010/10/22. [CrossRef] [PubMed]
- Moghaddam NSA, Oskouie MN, Butler AE, Petit PX, Barreto GE, Sahebkar A. Hormetic effects of curcumin: What is the evidence? Journal of cellular physiology. 2019;234(7):10060-71. Epub 2018/12/06. [CrossRef] [PubMed]
Figure 1.
Flow chart of analytical data.
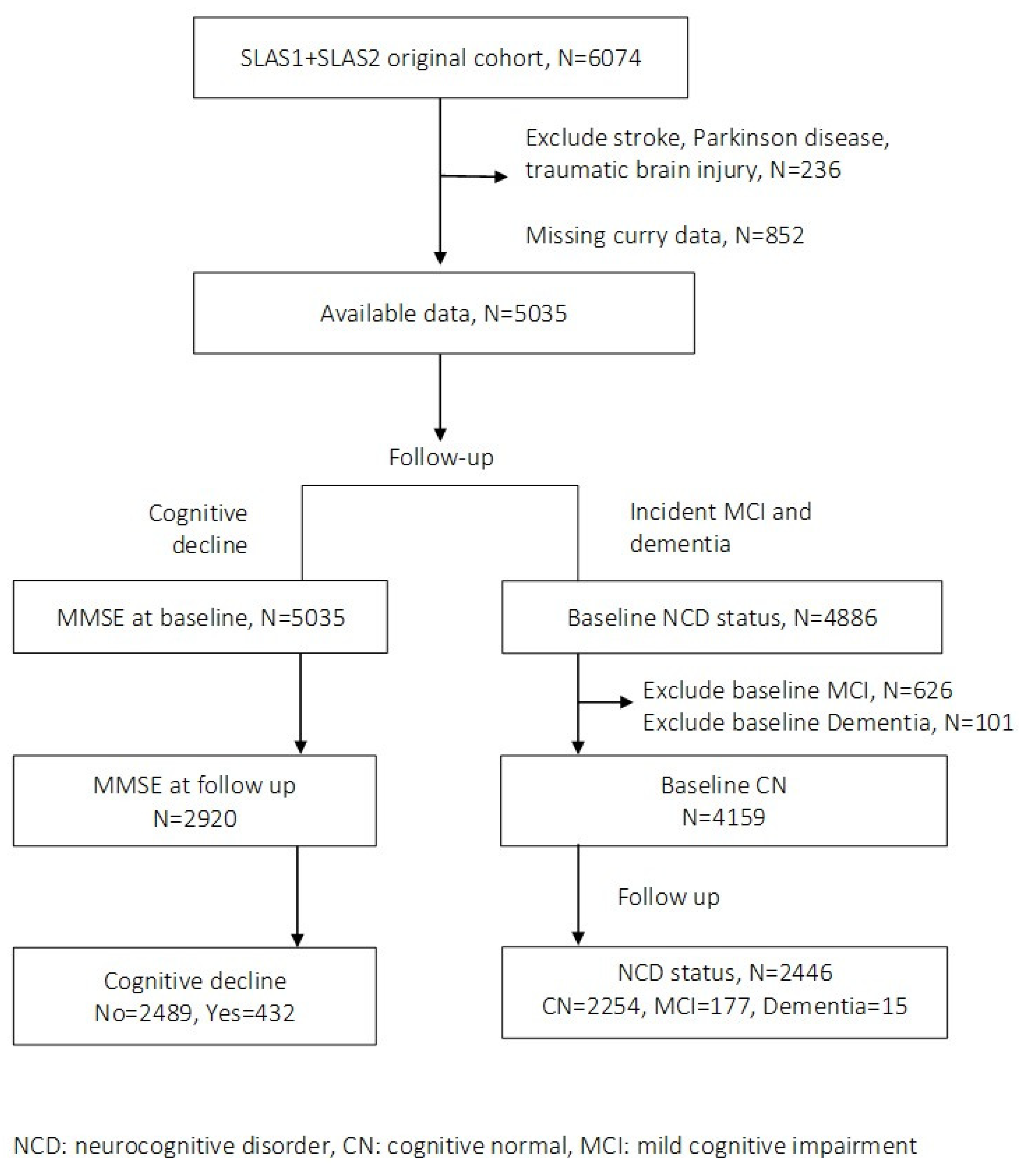
Figure 2.
Rates of cognitive decline and incident MCI-dementia by frequency of curry consumption.
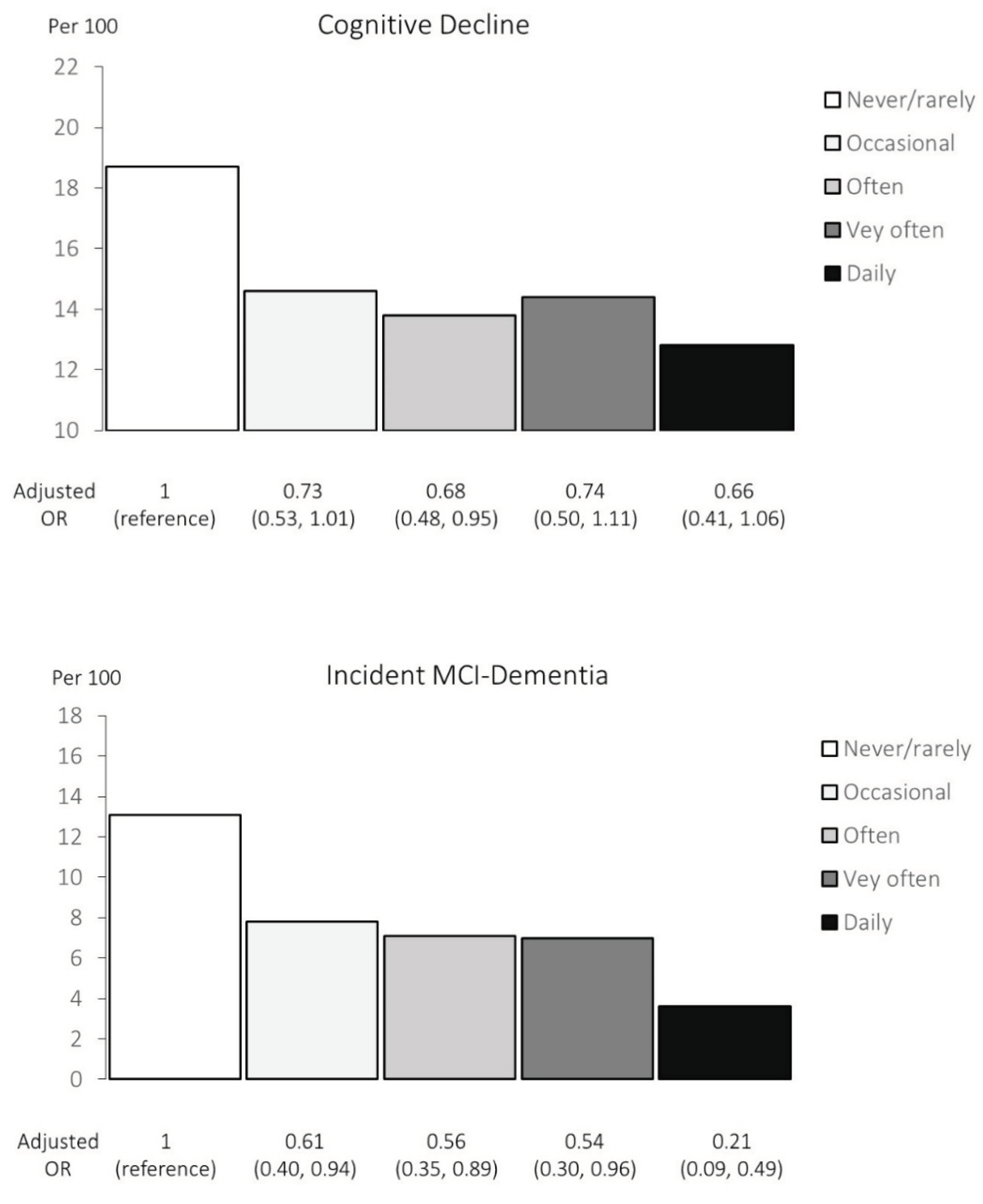

Table 1.
Baseline characteristics of SLAS study participants (N=2920) by curry consumption levels at baseline.
Table 1.
Baseline characteristics of SLAS study participants (N=2920) by curry consumption levels at baseline.
| Never or rarely | Occasional | Often | Very Often | Daily | ||||
|---|---|---|---|---|---|---|---|---|
| (Never or <once/year) | (>once/year, <once/month) | (>once/month, <once/week) | (>once/week, not daily) | (≥ once daily) | P | |||
| N of participants | 417 | 1030 | 805 | 395 | 273 | |||
| Sex: Women | 71.5 (298) | 70.6 (727) | 63.2 (509) | 58.0 (229) | 52.0 (142) | <0.001 | ||
| Age, years | 66.4 ± 7.3 | 65.7 ± 7.0 | 65.6 ± 7.2 | 64.9 ± 7.1 | 64.4 ± 6.7 | 0.003 | ||
| Ethnicity: Chinese | 98.6 (411) | 97.4 (1003) | 93.4 (752) | 89.9 (355) | 75.5 (206) | |||
| Malay, Indian and Other | 1.4 (6) | 2.6 (27) | 6.6 (53) | 10.1 (40) | 24.5 (67) | <0.001 | ||
| Education: 0-6 years | 63.3 (264) | 53.2 (548) | 48.9 (394) | 44.6 (176) | 42.5 (116) | <0.001 | ||
| Smoking: Past smoker | 8.4 (35) | 6.7 (69) | 9.7 (78) | 11.4 (45) | 8.4 (23) | |||
| Current smoker | 5.0 (21) | 6.3 (65) | 7.8 (63) | 6.3 (25) | 9.5 (26) | 0.005 | ||
| Alcohol >=once /week | 5.3 (22) | 4.1 (42) | 2.2 (18) | 5.3 (21) | 8.1 (22) | 0.143 | ||
| Physical activity score | 2.45 ± 1.91 | 2.42 ± 1.82 | 2.30 ±1.70 | 2.39 ± 1.84 | 2.43 ± 1.88 | 0.594 | ||
| Social activity score | 2.87 ± 2.30 | 3.32 ± 2.48 | 3.28 ± 2.54 | 3.30 ± 2.44 | 3.35 ±2.60 | 0.023 | ||
| Productive activity score | 3.96 ± 1.76 | 4.02 ± 1.73 | 4.05 ± 1.85 | 4.18 ± 1.82 | 4.15 ±1.92 | 0.375 | ||
| APOE-e4 ≥1 allele | 16.3 (68) | 17.6 (181) | 15.7 (126) | 15.0 (65) | 18.3 (50) | 0.901 | ||
| Central obesity | 43.2 (180) | 48.7 (502) | 52.7 (424) | 50.1 (198) | 52.7 (144) | 0.009 | ||
| Hypertension | 59.2 (247) | 59.2 (610) | 62.2 (501) | 56.7 (224) | 54.6 (149) | 0.256 | ||
| Diabetes or FBG>5.6mmol/L | 17.3 (72) | 17.8 (183) | 22.5 (181) | 19.0 (75) | 22.7 (62) | 0.032 | ||
| High triglyceride >2.2 mmol/L | 18.0 (75) | 27.6 (284) | 33.4 (269) | 21.0 (83) | 26.0 (71) | 0.167 | ||
| Low HDL-Cholesterol (<1.0mmol/L) | 18.7 (78) | 27.2 (280) | 34.7 (279) | 19.2 (76) | 29.3 (80) | 0.068 | ||
| Cardiac diseases | 8.2 (34) | 6.3 (65) | 8.2 (66) | 5.6 (22) | 8.8 (24) | 0.819 | ||
| GDS depression score | 1.58 ± 2.30 | 1.01 ± 1.94 | 0.91 ± 1.74 | 1.27 ± 2.30 | 1.33 ± 2.42 | <0.001 | ||
| GDS ≥5 | 9.8 (41) | 5.8 (60) | 3.6 (29) | 7.6 (30) | 7.7 (21) | <0.001 | ||
| MMSE | 27.3 ± 3.0 | 27.9 ± 2.5 | 28.2 ± 2.2 | 28.1 ± 2.3 | 27.8 ± 2.8 | <0.001 |
Table 2.
Baseline levels of curry consumption and covariates by cognitive decline status (N=2920) and Incident NCD status (N=2446).
Table 2.
Baseline levels of curry consumption and covariates by cognitive decline status (N=2920) and Incident NCD status (N=2446).
| Cognitive decline | Incident NCD | ||||||
|---|---|---|---|---|---|---|---|
| No | Yes | P | No | Yes | |||
| No. of participants | N=2489 | N=432 | N=2254 | N=192 | |||
| Never or rarely | Never or <once/year | 13.6 (339) | 18.1 (78) | 0.037 | 12.9 (291) | 22.9 (44) | <0.001 |
| Occasionally | >once/year,<once/month | 35.4 (880) | 34.8 (78) | 35.5 (801) | 35.4 (68) | ||
| Often | >once/month,<once/week | 27.9 (694) | 25.8 (150) | 28.4 (641) | 25.5 (49) | ||
| Very often | >once/week, not daily | 13.6 (338) | 13.2 (57) | 13.6 (307) | 12.0 (23) | ||
| Daily | ≥ once daily | 9.6 (238) | 8.1 (35) | 9.5 (214) | 4.2 (8) | ||
| Sex | Female | 64.3 (1601) | 70.5 (304) | 0.012 | 63.8 (1439) | 73.4 (141) | 0.008 |
| Age, years | Mean ± SD | 65.2 ± 6.9 | 67.4 ± 7.8 | <0.001 | 64.6 ±6.6 | 68.8 ± 7.9 | <0.001 |
| Non-Chinese ethnicity | Malay, Indian and Other | 6.3 (156) | 8.6 (37) | <0.001 | 5.2 (118) | 10.9 (21) | <0.001 |
| Education | 0-6 years | 49.4 (1229) | 62.4 (269) | <0.001 | 43.5 (981) | 72.4 (139) | <0.001 |
| Smoking | Past smoker | 9.0 (224) | 6.0 (26) | 0.056 | 8.6 (193) | 6.8 (13) | 0.657 |
| Current smoker | 7.0 (175) | 5.8 (25) | 7.1 (159) | 7.8 (15) | |||
| Alcohol | >=once /week | 4.3 (106) | 4.4 (19) | 0.887 | 4.5 (101) | 4.2 (8) | 0.839 |
| Physical activity score | Mean ± SD | 2.41 ± 1.81 | 2.30 ± 1.83 | 0.258 | 2.49 ± 1.82 | 2.10 ± 1.75 | 0.004 |
| Social activity score | Mean ± SD | 3.25 ± 2.47 | 3.19 ± 2.51 | 0.653 | 3.36 ±2.55 | 3.10 ± 2.06 | 0.174 |
| Productive activity score | Mean ± SD | 4.09 ± 1.80 | 3.87 ±1.80 | 0.020 | 4.16 ±1.80 | 3.94 ± 1.78 | 0.097 |
| APOE-e4 ≥1 allele | 16.6 (413) | 17.9 (77) | 0.514 | 16.1 (362) | 19.3 (37) | 0.248 | |
| Central obesity | 49.0 (1219) | 53.1 (229) | 0.111 | 48.8 (1101) | 56.8 (109) | 0.035 | |
| Hypertension | 58.3 (1452) | 64.7 (279) | 0.013 | 58.4 (1317) | 62.5 (120) | 0.271 | |
| Diabetes or FBG | >5.6mmol/L | 19.7 (490) | 19.3 (83) | 0.836 | 17.7 (400) | 25.5 (49) | 0.010 |
| High triglyceride | >2.2 mmol/L | 27.5 (685) | 22.5 (97) | 0.029 | 27.9 (628) | 21.4 (41) | 0.052 |
| Low HDL-Cholesterol | (<1.0mmol/L) | 27.6 (686) | 24.8 (107) | 0.239 | 28.0 (631) | 22.9 (44) | 0.131 |
| Cardiac diseases | 6.7 (168) | 10.0 (43) | 0.020 | 6.7 (151) | 6.3 (12) | 0.811 | |
| GDS depression score | Mean ± SD | 1.14 ± 2.05 | 1.24 ± 2.07 | 0.326 | 0.91 ± 1.67 | 1.47 ± 2.36 | <0.001 |
| GDS ≥5 | 6.1 (153) | 6.5 (28) | 0.781 | 4.2 (95) | 9.9 (19) | <0.001 | |
| MMSE | Mean ± SD | 27.8 ± 2.55 | 28.2 ± 2.35 | 0.009 | 28.7 ±1.62 | 27.2 ± 2.43 | <0.001 |
NCD: neurocognitive disorder (mild cognitive impairment or dementia).
Table 3.
Association of curry consumption with cognitive decline (N=2920).
| Exposed | Cognitive decline | Unadjusted | Adjusted † | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Yes | Per 100 | OR | 95% | CI | P | OR | 95% | CI | P | ||
| Never or rarely | Never or <once/year | 417 | 78 | 18.7 | 1 | 1 | ||||||
| Occasionally | >once/year, <once/month | 1030 | 150 | 14.6 | 0.74 | 0.55, | 1.00 | 0.73 | 0.53, | 1.01 | ||
| Often | >once/month, <once/week) | 805 | 111 | 13.8 | 0.69 | 0.51, | 0.96 | * | 0.68 | 0.48, | 0.95 | * |
| Very often | >once/week, not daily) | 395 | 57 | 14.4 | 0.73 | 0.50, | 1.06 | 0.74 | 0.50, | 1.11 | ||
| Daily | ≥ once daily | 273 | 35 | 12.8 | 0.64 | 0.41, | 0.98 | * | 0.66 | 0.41, | 1.06 | |
| Linear trend, p | 0.037 | 0.150 | ||||||||||
†Adjusted for age, sex, ethnicity, education (≤ 6 years of schooling), smoking, physical activity score, social activity score, productive activity score, apolipoprotein E-e4 allele, central obesity, high fasting blood glucose or diabetes, hypertension, low high-density lipoprotein cholesterol level, high triglycerides, cardiac disease, GDS score, and baseline MMSE. *p<0.05; **p<0.01; ***p<0.001. NCD: neurocognitive disorder (mild cognitive impairment or dementia)
Table 4.
Associations of curry consumption with incident NCD among cognitive normal participants (N=2446).
Table 4.
Associations of curry consumption with incident NCD among cognitive normal participants (N=2446).
| Exposed | NCD | Unadjusted | Adjusted † | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | MCI+dementia | Per 100 | OR | 95% | CI | P | OR | 95% | CI | P | ||
| Never or rarely | Never or <once/year | 335 | 42+2 | 13.1 | 1 | 1 | ||||||
| Occasionally | >once/year, <once/month | 869 | 61+7 | 7.8 | 0.56 | 0.38, | 0.84 | ** | 0.61 | 0.40, | 0.94 | * |
| Often | >once/month, <once/week) | 690 | 46+3 | 7.1 | 0.51 | 0.33, | 0.78 | ** | 0.56 | 0.35, | 0.89 | * |
| Very often | >once/week, not daily) | 330 | 20+3 | 7.0 | 0.49 | 0.29, | 0.84 | ** | 0.54 | 0.30, | 0.96 | * |
| Daily | ≥ once daily | 222 | 8 | 3.6 | 0.25 | 0.11, | 0.54 | *** | 0.21 | 0.09, | 0.49 | *** |
| Linear trend, p | <0.001 | 0.021 | ||||||||||
†Adjusted for age, sex, ethnicity, education (≤ 6 years of schooling), smoking, physical activity score, social activity score, productive activity score, apolipoprotein E-ε4 allele, central obesity, high fasting blood glucose or diabetes, hypertension, low high-density lipoprotein cholesterol level, high triglycerides, cardiac disease, and GDS score. *p<0.05; **p<0.01; ***p<0.001 NCD: neurocognitive disorder (mild cognitive impairment or dementia).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



