Submitted:
04 June 2025
Posted:
05 June 2025
You are already at the latest version
Abstract
Antimicrobial resistance (AMR) represents a critical global health threat, with inappropriate antibiotic self-medication (ASM) being a key contributor. China—as the world's largest antibiotic consumer—faces significant challenges despite regulatory efforts, compounded by limited contemporary data during the COVID-19 pandemic. A nationwide cross-sectional study was conducted using the 2021 China Family Health Index Survey (n=11,031 participants across 120 cities). Trained investigators administered face-to-face questionnaires assessing ASM practices, decision-making factors, and sociodemographic characteristics. Multivariate logistic regression identified determinants of ASM. Overall ASM prevalence was 33.7% (n=3,717), with no urban-rural difference (p>0.05). Physician advice (78.2%), drug safety (67.1%), and efficacy (64.2%) were primary selection criteria; rural residents prioritized drug price and salesperson recommendations more than urban counterparts (p< 0.01). Key predictors included higher ASM odds among females (OR=1.30, 95%CI:1.18-1.43), middle-aged adults (46-59 years; OR=1.20, 95%CI:1.02-1.42), those with health insurance (resident: OR=1.33; commercial: OR=1.62), and individuals with drinking histories (OR=1.20, 95%CI:1.10-1.31). Lower odds were associated with primary education (OR=0.69, 95%CI:0.58-0.81), unemployment (OR=0.88, 95%CI:0.79-0.98), and absence of chronic diseases (OR=0.56, 95%CI:0.47-0.67). One-third of Chinese residents engaged in ASM during the pandemic, driven by intersecting demographic and behavioral factors. Despite converging urban-rural prevalence rates, distinct decision-making drivers necessitate context-specific interventions, including strengthened pharmacy regulation in rural areas, tailored education programs for high-risk groups, and insurance system reforms to disincentivize self-medication.
Keywords:
antibiotic self-medication
; antimicrobial resistance
; determinants
; distribution
; china
1. Introduction
Antimicrobial resistance (AMR) constitutes a critical global health threat, imposing substantial economic and human costs, with projections indicating 10 million annual deaths and 2.5–3% global GDP reduction by 2050 if unaddressed [1,2]. This crisis is acutely pronounced in low- and middle-income countries like China, where antibiotic overuse remains prevalent—exemplified by >80% antibiotic prescription rates for upper respiratory infections and per capita consumption rates fivefold higher than Western nations [3,4]. Inappropriate antibiotic practices, particularly self-medication (ASM)—defined as antibiotic use without professional diagnosis or prescription—accelerate AMR propagation while risking adverse drug reactions, treatment failures, and increased healthcare expenditures [5,6,7].
Global initiatives, including WHO action plans (2011, 2015) and G20 commitments (2016), underscore AMR’s urgency [8,9,10]. China has responded through surveillance systems (e.g., Center for Antibacterial Surveillance, 2005) and policies like the China’s National Action Plan to Contain Antimicrobial Resistance (2016–2020) [11,12]. Despite these efforts, non-prescription antibiotic access persists nationwide, with 63–88% of pharmacies dispensing antibiotics without prescriptions [13,14], fueling widespread ASM. Internationally, ASM prevalence varies significantly—from 50.8% in Asian populations to <20% in France and Australia—reflecting disparities in healthcare access, regulatory enforcement, and cultural norms [15,16,17].
Critical knowledge gaps impede effective antibiotic stewardship interventions in China. First, while existing policies primarily target prescribers, patient-centered strategies remain underdeveloped [18]. Second, disparities in healthcare access between rural and urban areas—such as variations in pharmacy proximity versus hospital wait times—exacerbate ASM in underserved regions [19]. Third, although the COVID-19 pandemic has altered antibiotic usage patterns, population-level data during this period are scarce [20]. Finally, behavioral determinants—including substance use and socioeconomic factors—are not comprehensively assessed despite their documented influence on health decision-making [21].
This study addresses these gaps through a national survey of Chinese residents in 2021, aiming to quantify ASM distribution post-COVID-19 emergence, identify key considerations driving antibiotic procurement, and analyze sociodemographic, behavioral, and regional determinants of ASM, thereby informing targeted antimicrobial stewardship strategies aligned with Healthy China 2030 goals.
2. Results
2.1. Study Participants
The study enrolled 11,031 eligible participants, comprising 8,008 (72.60%) urban and 3,023 (27.40%) rural residents. Over half were female, with nearly half aged ≤30 years. A normal BMI range was observed in 68.40% of participants, while more than half were married, highly educated, and unemployed. Most (70.57%) reported a monthly household income per capita exceeding ¥3,000 (US$420), and 17.63% had ≥1 chronic disease. Non-smokers and non-drinkers constituted 19.82% and 40.37% of the cohort, respectively.
Compared to urban residents, those in rural areas exhibited significantly higher proportions of individuals aged ≥60 years, without spouses, unemployed, with monthly household income per capita <¥3,000, covered by out-of-pocket payment medical insurance, and without alcohol consumption history, but lower proportions of higher education attainment, absence of chronic diseases, and no smoking history (Table 1).
2.2. Distribution of ASM
Among 11,031 participants, 3,717 (33.70%) reported practicing ASM. ASM prevalence varied significantly across sociodemographic strata (Table 2), with higher rates observed among females, middle-aged adults (46–59 years), overweight individuals, married participants, highly educated respondents, white-collar workers, urban residents, and those with chronic diseases, smoking history, or drinking history. Lower ASM rates were associated with out-of-pocket medical insurance and absence of chronic diseases. No significant differences existed for income.
2.3. Considerations of ASM Practitioners
The 3,717 ASM practitioners prioritized three key factors when selecting antibiotics: physician’s advice (78.18%), drug safety (67.10%) and drug efficacy (64.22%) (Table 3; Figure 1). Rural residents placed significantly greater emphasis on drug price, salesperson recommendations, and after-sales service, whereas urban residents valued brand reputation and corporate credibility more highly.
2.4. Determinants of ASM
Multivariate logistic regression identified several independent predictors of ASM (Table 4). Males exhibited 23% lower odds of ASM than females (OR = 0.770; 95% CI: 0.700–0.845; p < 0.0001). Middle-aged adults (46–59 years) had 20.3% higher odds than elderly participants (≥60 years) (OR = 1.203; 95% CI: 1.020–1.418; p = 0.0279). Those with primary/below education showed 31.3% lower odds versus higher-educated counterparts (OR = 0.687; 95% CI: 0.580–0.813; p < 0.0001). Unemployed participants had 12.1% lower odds relative to white-collar workers (OR = 0.879; 95% CI: 0.788–0.981; p = 0.0209). Participants with resident/employee health insurance (OR = 1.327; 95% CI: 1.191–1.478; p < 0.0001) or commercial insurance (OR = 1.624; 95% CI: 1.227–2.149; p = 0.0007) demonstrated higher odds than those relying on out-of-pocket payment. Absence of chronic diseases predicted lower odds (none vs. multiple: OR = 0.561; 95% CI: 0.469–0.671; p < 0.0001; one vs. multiple: OR = 0.715; 95% CI: 0.588–0.869; p = 0.0008). Drinking history increased ASM odds by 20.1% (OR = 1.201; 95% CI: 1.097–1.314; p < 0.0001).
3. Discussion
This nationwide study reveals a 33.7% prevalence of ASM among Chinese residents during the COVID-19 pandemic. Notably, despite significant urban-rural socioeconomic disparities, no difference in ASM prevalence was observed, suggesting this practice remains deeply embedded across diverse communities. This finding highlights the urgent need for context-specific interventions to address AMR, a critical global health threat projected to cause 4.73 million in Asia annual deaths by 2050 that imposes substantial economic burdens [2].
China's ASM rate aligns with previous national studies reporting 37.1-45.7% prevalence [23,24], but exceeds rates in high-income nations like the UK (5%) and France (18%) [17,25]. While lower than India (58%) [26], it surpasses WHO's recommended threshold of 30% [27]. This intermediate position reflects China's unique healthcare landscape where rapid economic development coexists with persistent self-medication traditions. The convergence of urban and rural ASM rates underscores how cultural norms and medication accessibility may transcend geographic and socioeconomic boundaries [28,29], particularly during healthcare disruptions like the COVID-19 pandemic which affected medication dispensing patterns [30].
Our analysis identified several demographic predictors of ASM. Females exhibited 30% higher odds than males (OR=1.299), consistent with studies from Sudan and UK [30,31]. This gender disparity may stem from differential care-seeking behaviors, higher antibiotic prescription rates for women, and greater access to leftover medications [32]. Middle-aged adults (46-59 years) showed elevated risk, potentially due to time constraints and healthcare access barriers [34]. Counterintuitively, higher education correlated with increased ASM (OR=1.456 vs. primary education), mirroring patterns observed in Italy [31]. This education paradox suggests knowledge alone is insufficient to modify behavior, potentially reflecting overconfidence in self-diagnosis among educated individuals [35]. Participants with health insurance demonstrated significantly higher ASM odds (Resident/Employee: OR=1.327; Commercial: OR=1.624), aligning with Iranian evidence that insured individuals perceive self-medication as financially lower-risk [36]. Multiple chronic diseases amplified ASM risk (OR=1.782 vs. disease-free), likely due to symptom familiarity and frequent medication exposure [37], while drinking history increased odds by 20.1% (OR=1.201), corroborating European associations between substance use and self-medication [38].
Notable urban-rural divergences emerged in antibiotic selection criteria. Rural residents prioritized drug price, salesperson recommendations, and after-sales service, whereas urban consumers emphasized brand reputation and corporate credibility. These differences likely reflect rural healthcare access barriers, medication literacy gaps, and targeted marketing strategies by community pharmacies [39,40]. The substantial rural reliance on salesperson advice is particularly concerning given frequent deficiencies in formal medical training among pharmacy staff.
These findings suggest four strategic interventions. First, pharmacy regulations require reinforcement through strict enforcement of prescription-only dispensing policies, particularly in rural communities where non-prescription access remains prevalent. Pharmacist certification programs should incorporate AMR stewardship training. Second, contextual public education campaigns should address specific misconceptions such as viewing antibiotics as "panaceas" [41], leveraging frameworks like WHO's World Antibiotic Awareness Week. Such messaging must specifically target educated populations whose knowledge doesn't translate to appropriate use. Third, insurance systems need reform through reevaluation of co-payment structures to reduce financial incentives for self-medication while maintaining healthcare accessibility [42]. Finally, China should capitalize on its advanced telemedicine infrastructure through digital health integration, utilizing platforms like WeChat health portals for AMR education and remote consultations in underserved regions [43].
Several methodological limitations warrant acknowledgment. The cross-sectional design precludes causal inference regarding ASM determinants. Self-reported data introduces potential recall and social desirability biases. Regional specificity limits generalizability beyond China, and exclusion of healthcare provider perspectives omits critical stakeholders in antibiotic dispensing. Future research should employ longitudinal designs to track ASM evolution post-pandemic and incorporate provider insights.
4. Materials and Methods
4.1. Study Design and Population
Data were derived from the 2021 China Family Health Index Survey (CFHI-2021) [22], conducted from July 10 to September 15, 2021, across 120 cities in 22 provinces and 5 autonomous regions. Trained investigators in each city administered questionnaires via the online Questionnaire Star platform (https://www.wjx.cn/), using a one-on-one, face-to-face approach. After investigators entered unique questionnaire IDs, respondents independently completed the survey by accessing the provided link. For participants with cognitive capacity but physical limitations, investigators recorded responses based on verbal input. The inclusion criteria were as follows: (1) Age ≥16 years; (2) Response to the ASM question; (3) Provision of written informed consent.
4.2. The Questionnaire and Data Collection
The structured questionnaire comprised two sections: 1. Socio-demographic and clinical characteristics: Gender, age, BMI, marital status, education, occupation, monthly household income per capita, medical insurance, chronic disease count, smoking/drinking history, and residence (urban/rural); 2. Antibiotic self-medication behavior: Question 1 (single-response): "Have you ever purchased and used antibiotics without a prescription?" (Yes/No). Question 2 (multiple-response, for ASM practitioners only): "What factors influenced your antibiotic purchase decisions?" Participants selected from 18 options: (1) Efficacy; (2) Safety; (3) Dosage form; (4) Price; (5) Insurance coverage; (6) Ease of use; (7) Taste; (8) Packaging; (9) Physician advice; (10) Pharmacist advice; (11) Family suggestions; (12) Friend suggestions; (13) Salesperson recommendations; (14) Personal experience; (15) Brand reputation; (16) Manufacturer credibility; (17) Advertising; (18) After-sales service. Respondents selected 1–18 options.
4.3. Statistical Analysis
Descriptive statistics summarized categorical variables as frequencies (%) and normally distributed continuous variables as mean ± standard deviation. Chi-square tests identified potential determinants of ASM and urban-rural differences. Binary logistic regression assessed associations between ASM (dependent variable) and socio-demographic factors (independent variables), reporting adjusted odds ratios (adjusted ORs) with 95% confidence intervals (CIs). Statistical significance was set at p < 0.05. Analyses used SAS 9.4 (SAS Institute, Cary, NC, USA).
5. Conclusions
This study reveals persistent antibiotic ASM practices across both urban and rural China, mediated through factors including gender, education level, insurance status, and health-related behaviors. The convergence of ASM prevalence despite divergent regional socioeconomic profiles necessitates multifaceted interventions. Future research should employ longitudinal designs to track post-pandemic ASM trends and incorporate healthcare provider perspectives. Immediate action is imperative to integrate pharmacist education, public awareness campaigns, and insurance reforms within China's evolving primary healthcare framework to mitigate the escalating AMR crisis.
Author Contributions
Conceptualization, Guo Huang, Pu Ge, He Zhu, Sheng Han and Luwen Shi; Data curation, Guo Huang and He Zhu; Formal analysis, Guo Huang, Pu Ge and Mengyun Sui; Funding acquisition, Luwen Shi; Investigation, Mengyun Sui; Methodology, Guo Huang, Pu Ge and Sheng Han; Project administration, Sheng Han and Luwen Shi; Resources, Pu Ge, Sheng Han and Luwen Shi; Software, Guo Huang, Mengyun Sui, He Zhu and Sheng Han; Supervision, He Zhu, Sheng Han and Luwen Shi; Validation, Pu Ge, Mengyun Sui, He Zhu, Sheng Han and Luwen Shi; Visualization, Guo Huang and Pu Ge; Writing – original draft, Guo Huang and Mengyun Sui; Writing – review & editing, Sheng Han and Luwen Shi.
Funding
This research was funded by the National Natural Science Foundation of China (grant number 82273899).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Committee of Ji’nan University, Guangzhou, China (JNUKY-2021-018).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study can be made available upon request from the corresponding author.
Acknowledgments
We would like to thank all the participants enrolled in this study and local health professionals for contributing to the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. 2014. Available online: https://amr-review.org/ (accessed on 23 April 2022).
- Li, J.; Song, X.; Yang, T.; Chen, Y.; Gong, Y.; Yin, X.; Lu, Z. A systematic review of antibiotic prescription associated with upper respiratory tract infections in China. Medicine (Baltimore) 2016, 95, e3587. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, Q.Q.; Ying, G.G.; Pan, C.G.; Liu, Y.S.; Zhao, J.L. Comprehensive evaluation of antibiotics emission and fate in the river basins of China: source analysis, multimedia modeling, and linkage to bacterial resistance. Environ Sci Technol 2015, 49, 6772–82. [Google Scholar] [CrossRef] [PubMed]
- Ateshim, Y.; Bereket, B.; Major, F.; Emun, Y.; Woldai, B.; Pasha, I.; Habte, E.; Russom, M. Prevalence of self-medication with antibiotics and associated factors in the community of Asmara, Eritrea: a descriptive cross sectional survey. BMC Public Health 2019, 19, 26. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sachdev, C.; Anjankar, A.; Agrawal, J. Self-medication with antibiotics: an element increasing resistance. Cureus 2022, 14, e30844. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zeb, S.; Mushtaq, M.; Ahmad, M.; Saleem, W.; Rabaan, A.A.; Naqvi, B.S.Z.; Garout, M.; Aljeldah, M.; Al-Shammari, B.R.; Al-Faraj, N.J.; Al-Zaki, N.A.; Al-Marshood, M.J.; Al-Saffar, T.Y.; Alsultan, K.A.; Al-Ahmed, S.H.; Alestad, J.H.; Naveed, M.; Ahmed, N. Self-medication as an important risk factor for antibiotic resistance: a multi-institutional survey among students. Antibiotics (Basel) 2022, 11, 842. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Health Organization. Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/193736/9789241509763_eng.pdf?sequence=1&isAllowed=y (accessed on 23 May 2022).
- World Health Organization. Antimicrobial Resistance: No Action Today, No Cure Tomorrow. 2011. Available online: https://www.who.int/dg/speeches/detail/antimicrobial-resistance-no-action-today-no-cure-tomorrow (accessed on 23 April 2022).
- G20 Summits. Communiqué of the G20 Leaders, Hangzhou, China. 2016. Available online: http://www.g20chn.org/hywj/dncgwj/201609/t20160906_3392.html (accessed on 23 April 2022).
- Li, H.; Yan, S.; Li, D.; Gong, Y.; Lu, Z.; Yin, X. Trends and patterns of outpatient and inpatient antibiotic use in China's hospitals: data from the Center for Antibacterial Surveillance, 2012-16. J Antimicrob Chemother 2019, 74, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission of the People’s Republic of China. China’s National Action Plan to Contain Antimicrobial Resistance. 2016. Available online: http://www.nhc.gov.cn/yzygj/s3593/201608/f1ed26a0c8774e1c8fc89dd481ec84d7.shtml (accessed on 23 April 2022).
- Y, F. China should curb non-prescription use of antibiotics in the community[J]. BMJ 2014, 348, g4233. [Google Scholar] [CrossRef]
- Shi, L.; Chang, J.; Liu, X.; Zhai, P.; Hu, S.; Li, P.; Hayat, K.; Kabba, J.A.; Feng, Z.; Yang, C.; Jiang, M.; Zhao, M.; Hu, H.; Fang, Y. Dispensing antibiotics without a prescription for acute cough associated with common cold at community pharmacies in shenyang, northeastern china: a cross-sectional study. Antibiotics (Basel) 2020, 9, 163. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Widowati, I.G.A.R.; Budayanti, N.N.S.; Januraga, P.P.; Duarsa, D.P. Self-medication and self-treatment with short-term antibiotics in Asian countries: a literature review[J]. Pharm Educ 2021, 21, 152–62. [Google Scholar] [CrossRef]
- Huh, K.; Chung, D.R.; Kim, S.H.; Cho, S.Y.; Ha, Y.E.; Kang, C.I.; Peck, K.R.; Song, J.H. Factors affecting the public awareness and behavior on antibiotic use. Eur J Clin Microbiol Infect Dis 2018, 37, 1547–1552. [Google Scholar] [CrossRef] [PubMed]
- Demoré, B.; Mangin, L.; Tebano, G.; Pulcini, C.; Thilly, N. Public knowledge and behaviours concerning antibiotic use and resistance in France: a cross-sectional survey. Infection 2017, 45, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Zhang, J.; Zheng, B.; Zhao, L.; Li, S.; Li, L. Changes in Chinese policies to promote the rational use of antibiotics. PLoS Med 2013, 10, e1001556. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Do, N.T.T.; Vu, H.T.L.; Nguyen, C.T.K.; Punpuing, S.; Khan, W.A.; Gyapong, M.; Asante, K.P.; Munguambe, K.; Gómez-Olivé, F.X.; John-Langba, J.; et al. Community-based antibiotic access and use in six low-income and middle-income countries: a mixed-method approach. Lancet Glob Health 2021, 9, e610–e619. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Euro Surveill 2020, 25, 2001886. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, Y.; Fan, S.; Chen, W.; Wu, Y. Broader open data needed in psychiatry: practice from the psychology and behavior investigation of chinese residents. Alpha Psychiatry 2024, 25, 564–565. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- China Family News. CFHI-2021 China Family Health Index Survey General Report[EB/OL]. (Chinese). Available from: https://www.cfnews.org.cn/newsinf o/2685237.html.
- Ye, D.; Chang, J.; Yang, C.; Yan, K.; Ji, W.; Aziz, M.M.; Gillani, A.H.; Fang, Y. How does the general public view antibiotic use in China? Result from a cross-sectional survey. Int J Clin Pharm 2017, 39, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Deng, P.; Yu, J.; Zhou, N.; Hu, M. Access to medicines for acute illness and antibiotic use in residents: A medicines household survey in Sichuan Province, western China. PLoS One 2018, 13, e0201349. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McNulty, C.A.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. Don't wear me out--the public's knowledge of and attitudes to antibiotic use. J Antimicrob Chemother 2007, 59, 727–38. [Google Scholar] [CrossRef] [PubMed]
- Virmani, S.; Nandigam, M.; Kapoor, B.; Makhija, P.; Nair, S. Antibiotic use among health science students in an Indian University: a cross sectional study[J]. Clin Epidemiol Global Health 2017, 5, 176–9. [Google Scholar] [CrossRef]
- World Health Organization. Using Indicators to Measure Country Pharmaceutical Situations: Fact Book on WHO Level I and Level II Monitoring Indicators. 2006. Available online: http://apps.who.int/medicinedocs/index/assoc/s14101e/s14101e.pdf (accessed on 23 April 2022).
- Grigoryan, L.; Burgerhof, J.G.; Degener, J.E.; Deschepper, R.; Lundborg, C.S.; Monnet, D.L.; Scicluna, E.A.; Birkin, J.; Haaijer-Ruskamp, F.M.; SAR consortium. Attitudes, beliefs and knowledge concerning antibiotic use and self-medication: a comparative European study. Pharmacoepidemiol Drug Saf 2007, 16, 1234–43. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Bjerrum, L. Background for different use of antibiotics in different countries. Clin Infect Dis. 2005, 40, 333. [Google Scholar] [CrossRef] [PubMed]
- Frazer, J.S.; Frazer, G.R. Analysis of primary care prescription trends in England during the COVID-19 pandemic compared against a predictive model. Fam Med Community Health 2021, 9, e001143. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mitsi, G.; Jelastopulu, E.; Basiaris, H.; Skoutelis, A.; Gogos, C. Patterns of antibiotic use among adults and parents in the community: a questionnaire-based survey in a Greek urban population. Int J Antimicrob Agents 2005, 25, 439–43. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.R.M.; Dolk, F.C.K.; Smieszek, T.; Robotham, J.V.; Pouwels, K.B. Understanding the gender gap in antibiotic prescribing: a cross-sectional analysis of English primary care. BMJ Open 2018, 8, e020203. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McNulty, C.A.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. The public's attitudes to and compliance with antibiotics. J Antimicrob Chemother 2007, 60, 63–8. [Google Scholar] [CrossRef] [PubMed]
- Bogale, A.A.; Amhare, A.F.; Chang, J.; Bogale, H.A.; Betaw, S.T.; Gebrehiwot, N.T.; Fang, Y. Knowledge, attitude, and practice of self-medication with antibiotics among community residents in Addis Ababa, Ethiopia. Expert Rev Anti Infect Ther 2019, 17, 459–466. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Antibiotic Resistance: Multi-Country Public.
- Vahedi, S.; Jalali, F.S.; Bayati, M.; Delavari, S. Predictors of self-medication in Iran: a notional survey study. Iran J Pharm Res 2021, 20, 348–358. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grigoryan, L.; Haaijer-Ruskamp, F.M.; Burgerhof, J.G.; Mechtler, R.; Deschepper, R.; Tambic-Andrasevic, A.; Andrajati, R.; Monnet, D.L.; Cunney, R.; Di-Matteo, A.; et al. Self-medication with antimicrobial drugs in Europe. Emerg Infect Dis 2006, 12, 452–9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lukovic, J.A.; Miletic, V.; Pekmezovic, T.; Trajkovic, G.; Ratkovic, N.; Aleksic, D.; Grgurevic, A. Self-medication practices and risk factors for self-medication among medical students in Belgrade, Serbia. PLoS One 2014, 9, e114644. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liang, Y.; Zhou, M.; Yu, W.; Wang, H. Changes in social support among patients with hematological malignancy undergoing hematopoietic stem cell transplantation in Souzhou, China. Indian J Cancer 2020, 57, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Awuah, R.B.; Asante, P.Y.; Sakyi, L.; Biney, A.A.E.; Kushitor, M.K.; Agyei, F.; de-Graft Aikins, A. Factors associated with treatment-seeking for malaria in urban poor communities in Accra, Ghana. Malar J 2018, 17, 168. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xiao, Y.; Li, L. Legislation of clinical antibiotic use in China. Lancet Infect Dis 2013, 13, 189–91. [Google Scholar] [CrossRef] [PubMed]
- Bartoloni, A.; Cutts, F.; Leoni, S.; Austin, C.C.; Mantella, A.; Guglielmetti, P.; Roselli, M.; Salazar, E.; Paradisi, F. Patterns of antimicrobial use and antimicrobial resistance among healthy children in Bolivia. Trop Med Int Health 1998, 3, 116–23. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Xu, S.; Zhu, S.; Li, Z.; Yu, J.; Zhang, Y.; Zu, J.; Fang, Y.; Ross-Degnan, D. Assessment of non-prescription antibiotic dispensing at community pharmacies in China with simulated clients: a mixed cross-sectional and longitudinal study. Lancet Infect Dis 2019, 19, 1345–1354. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Considerations distribution of ASM Practitioners.
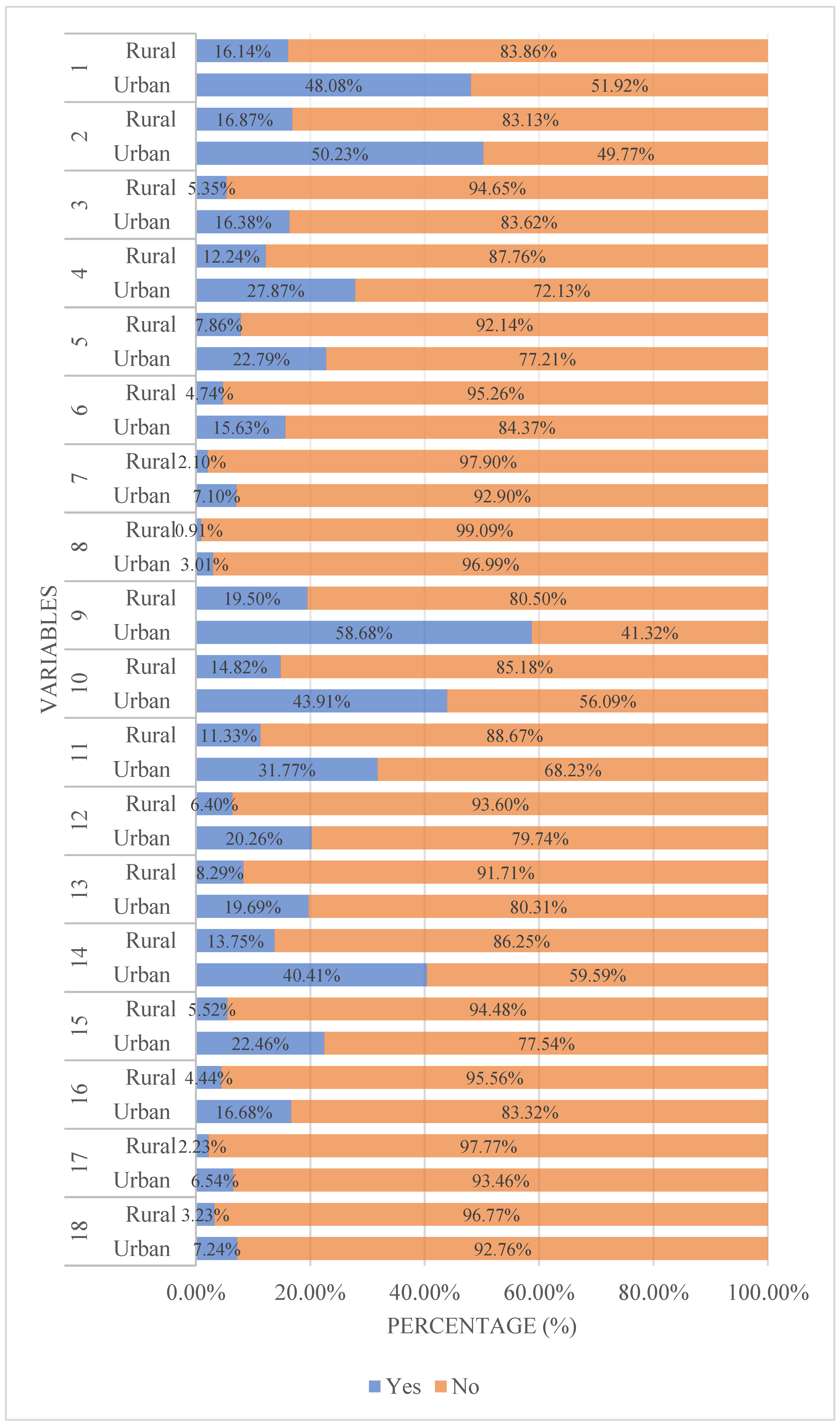

Table 1.
General characteristics of Chinese residents.
| Variables | n (%) | χ2 | p-Value | |||
|---|---|---|---|---|---|---|
| Urban | Rural | Total | ||||
| Total | 8008 (72.60) | 3023 (27.40) | 11031 (100.00) | |||
| Gender | 0.0831 | 0.7731 | ||||
| Male | 3647 (45.54) | 1386 (45.86) | 5033 (45.63) | |||
| Female | 4361 (54.56) | 1637 (54.15) | 5998 (54.37) | |||
| Age (years) | 179.8654 | <0.0001 | ||||
| 0–30 | 3377 (42.17) | 1288 (42.61) | 4665 (42.29) | |||
| 31–45 | 2325 (29.03) | 676 (22.36) | 3001 (27.21) | |||
| 46–59 | 1652 (20.63) | 566 (18.72) | 2218 (20.11) | |||
| 60– | 654 (8.17) | 493 (16.31) | 1147 (10.40) | |||
| BMI (kg/m2) | 3.7998 | 0.1496 | ||||
| <18.5 | 1103 (13.77) | 459 (15.18) | 1562 (14.16) | |||
| 18.5–24.9 | 5510 (68.81) | 2035 (67.32) | 7545 (68.40) | |||
| 25– | 1395 (17.42) | 529 (17.50) | 1924 (17.44) | |||
| Spouse | 34.7433 | <0.0001 | ||||
| Yes | 2243 (60.34) | 3983 (54.56) | 6226 (56.44) | |||
| No | 1474 (39.66) | 3331 (45.54) | 4805 (43.56) | |||
| Education level | 832.9165 | <0.0001 | ||||
| Primary or below | 473 (5.91) | 654 (21.63) | 1127 (10.22) | |||
| Secondary | 2272 (28.37) | 1145 (37.88) | 3417 (30.98) | |||
| Higher | 5263 (65.72) | 1224 (40.49) | 6487 (58.81) | |||
| Occupation | 527.0434 | <0.0001 | ||||
| Unemployed | 4496 (56.14) | 2379 (78.70) | 6875 (62.32) | |||
| Blue-collar | 992 (12.39) | 295 (9.76) | 1287 (11.67) | |||
| White-collar | 2520 (31.47) | 349 (11.54) | 2869 (26.01) | |||
| Monthly household income per capita | 1020.805 | <0.0001 | ||||
| 0–3000 | 1714 (21.40) | 1532 (50.68) | 3246 (29.43) | |||
| 3001–6000 | 3229 (40.32) | 1025 (33.91) | 4254 (38.56) | |||
| 6001– | 3065 (38.27) | 466 (15.42) | 3531 (32.01) | |||
| Medical insurance | 60.1299 | <0.0001 | ||||
| Resident/employee | 6083 (75.96) | 2206 (72.97) | 8289 (75.14) | |||
| Commercial | 203 (2.53) | 34 (1.12) | 237 (2.15) | |||
| Government-funded | 168 (2.10) | 38 (1.26) | 206 (1.87) | |||
| Out-of-pocket payment | 1554 (19.41) | 745 (24.64) | 2299 (20.84) | |||
| Number of chronic diseases | 11.7185 | 0.0029 | ||||
| none | 6644 (82.97) | 2442 (80.78) | 9086 (82.37) | |||
| Single | 932 (11.64) | 369 (12.21) | 1301 (11.79) | |||
| Multiple | 432 (5.39) | 212 (7.01) | 644 (5.84) | |||
| Smoking history | 15.2551 | <0.0001 | ||||
| Yes | 1514 (18.91) | 672 (22.23) | 2186 (19.82) | |||
| No | 6494 (81.09) | 2351 (77.77) | 8845 (80.18) | |||
| Drinking history | 42.7765 | <0.0001 | ||||
| Yes | 3383 (42.25) | 1070 (35.40) | 4453 (40.37) | |||
| No | 4652 (57.75) | 1953 (64.60) | 6578 (59.63) | |||
Table 2.
Distributions of ASM among Chinese residents.
| Variables | ASM [n (%)] | χ2 | p-Value | |||
|---|---|---|---|---|---|---|
| Yes | No | Total | ||||
| Total | 3717 (33.70) | 7314 (66.30) | 11031 (100.00) | |||
| Gender | 6.6819 | 0.0097 | ||||
| Male | 1632 (43.91) | 3401 (46.50) | 5033 (45.63) | |||
| Female | 2085 (56.09) | 3913 (53.50) | 5998 (54.37) | |||
| Age (years) | 55.2949 | <0.0001 | ||||
| 0–30 | 1423 (38.28) | 3242 (44.33) | 4665 (42.29) | |||
| 31–45 | 1020 (27.44) | 1981 (27.09) | 3001 (27.21) | |||
| 46–59 | 876 (23.57) | 1342 (18.35) | 2218 (20.11) | |||
| 60– | 398 (10.71) | 749 (10.24) | 1147 (10.40) | |||
| BMI (kg/m2) | 14.5356 | 0.0007 | ||||
| <18.5 | 471 (12.67) | 1091 (14.92) | 1562 (14.16) | |||
| 18.5–24.9 | 2548 (68.55) | 4997 (68.32) | 7545 (68.40) | |||
| 25– | 698 (18.78) | 1226 (16.72) | 1924 (17.44) | |||
| Spouse | 34.7433 | <0.0001 | ||||
| Yes | 2243 (60.34) | 3983 (54.46) | 6226 (56.44) | |||
| No | 1474 (39.66) | 3331 (45.54) | 4805 (43.56) | |||
| Education level | ||||||
| Primary or below | 324 (8.72) | 803 (10.98) | 1127 (10.22) | 14.7739 | 0.0006 | |
| Secondary | 1148 (30.89) | 2269 (31.02) | 3417 (30.98) | |||
| Higher | 2245 (60.40) | 4242 (58.00) | 6487 (58.81) | |||
| Occupation | 48.6309 | <0.0001 | ||||
| Unemployed | 2156 (58.00) | 4719 (64.52) | 6875 (62.32) | |||
| Blue-collar | 455 (12.24) | 832 (11.38) | 1287 (11.67) | |||
| White-collar | 1106 (29.76) | 1763 (24.10) | 2869 (26.01) | |||
| Monthly household income per capita | 4.7330 | 0.0938 | ||||
| 0–3000 | 1045 (28.11) | 2201 (30.09) | 3246 (29.43) | |||
| 3001–6000 | 1454 (39.12) | 2800 (38.28) | 4254 (38.56) | |||
| 6001– | 1218 (32.77) | 2313 (31.62) | 3531 (32.01) | |||
| Medical insurance | 60.5866 | <0.0001 | ||||
| Resident/employee | 2931 (78.85) | 5358 (72.98) | 8289 (75.14) | |||
| Commercial | 95 (2.56) | 142 (1.94) | 237 (2.15) | |||
| Government-funded | 70 (1.88) | 136 (1.86) | 206 (1.87) | |||
| Out-of-pocket payment | 621 (16.71) | 1678 (22.94) | 2299 (20.84) | |||
| Number of chronic diseases | 65.5118 | <0.0001 | ||||
| none | 2921 (78.58) | 6165 (84.29) | 9086 (82.37) | |||
| Single | 501 (13.48) | 800 (10.94) | 1301 (11.79) | |||
| Multiple | 295 (7.94) | 349 (4.77) | 644 (5.84) | |||
| Smoking history | 6.7482 | 0.0094 | ||||
| Yes | 788 (21.20) | 1398 (18.99) | 2186 (19.82) | |||
| No | 2929 (78.80) | 5916 (80.89) | 8845 (80.18) | |||
| Drinking history | 19.8502 | <0.0001 | ||||
| Yes | 1609 (43.29) | 2844 (38.88) | 4453 (40.37) | |||
| No | 2108 (56.71) | 4470 (61.12) | 6578 (59.63) | |||
| Residence | 11.0567 | 0.0009 | ||||
| Urban | 2772 (74.58) | 5236 (71.59) | 8008 (72.60) | |||
| Rural | 945 (25.42) | 2078 (28.41) | 3023 (27.40) | |||
Table 3.
Considerations of ASM Practitioners by residence.
| Variables | n (%) | χ2 | p-Value | |||
|---|---|---|---|---|---|---|
| Urban | Rural | Total | ||||
| Total | 2772 (74.58) | 945 (25.42) | 3717 (100.00) | |||
| Clinical factors | ||||||
| 1 Drug efficacy | 1787 (64.47) | 600 (63.49) | 2387 (64.22) | 0.2910 | 0.5896 | |
| 2 Drug safety | 1867 (67.35) | 627 (66.35) | 2494 (67.10) | 0.3211 | 0.5710 | |
| 3 Dosage form (e.g., capsules, patches) | 609 (21.97) | 199 (21.06) | 808 (21.74) | 0.3442 | 0.5574 | |
| Economic & accessibility | ||||||
| 4 Drug price | 1036 (37.37) | 455 (48.15) | 1491 (40.11) | 34.0566 | <0.0001 | |
| 5 Insurance reimbursement eligibility | 847 (30.56) | 292 (30.90) | 1139 (30.64) | 0.0392 | 0.8430 | |
| Convenience & experience | ||||||
| 6 Ease of administration | 581 (20.96) | 176 (18.62) | 757 (20.37) | 2.3697 | 0.1237 | |
| 7 Taste of medication | 264 (9.52) | 78 (8.25) | 342 (9.20) | 1.3602 | 0.2435 | |
| 8 Packaging aesthetics | 112 (4.04) | 34 (3.60) | 146 (3.93) | 0.3657 | 0.5453 | |
| Social & personal advice | ||||||
| 9 Physician’s advice | 2181 (78.68) | 725 (76.72) | 2906 (78.18) | 1.5873 | 0.2077 | |
| 10 Pharmacist’s advice | 1632 (58.87) | 551 (58.31) | 2183 (58.73) | 0.0937 | 0.7596 | |
| 11 Family member’s suggestions | 1181 (42.60) | 421 (44.55) | 1602 (43.10) | 1.0879 | 0.2969 | |
| 12 Friend’s suggestions | 753 (27.16) | 238 (25.19) | 991 (26.66) | 1.4120 | 0.2347 | |
| 13 Recommendations from sales personnel | 732 (26.41) | 308 (32.59) | 1040 (27.98) | 13.3816 | 0.0003 | |
| 14 Personal experience | 1502 (54.18) | 511 (54.07) | 2013 (54.16) | 0.0035 | 0.9530 | |
| Brand & corporate | ||||||
| 15 Brand reputation | 835 (30.12) | 205 (21.69) | 1040 (27.98) | 24.8509 | <0.0001 | |
| 16 Corporate credibility | 620 (22.37) | 165 (17.46) | 785 (21.12) | 10.1830 | 0.0014 | |
| 17 Advertising influence | 243 (8.77) | 83 (8.78) | 326 (8.77) | 0.0002 | 0.9874 | |
| 18 After-sales service | 269 (9.70) | 120 (12.70) | 389 (10.47) | 6.7430 | 0.0094 | |
Table 4.
Multivariate logistic regression on ASM among Chinese residents.
| Variables | β | SE | Wald χ2 | p-Value | OR (95%CI) | |
|---|---|---|---|---|---|---|
| Intercept | -0.2714 | 0.1474 | 3.3924 | 0.0655 | ||
| Gender (Ref: Female) | ||||||
| Male | -0.2619 | 0.0480 | 29.7837 | <0.0001 | 0.770 (0.700, 0.845) | |
| Age (Ref: 60–) | ||||||
| 0–30 | -0.0321 | 0.0953 | 0.1133 | 0.7364 | 0.968 (0.803, 1.167) | |
| 31–45 | -0.0108 | 0.0857 | 0.0159 | 0.8997 | 0.989 (0.836, 1.170) | |
| 46–59 | 0.1848 | 0.0841 | 4.8313 | 0.0279 | 1.203 (1.020, 1.418) | |
| BMI (Ref: 25–) | ||||||
| <18.5 | -0.1350 | 0.0771 | 3.0688 | 0.0798 | 0.874 (0.751, 1.016) | |
| 18.5–24.9 | -0.0362 | 0.0553 | 0.4279 | 0.5130 | 0.964 (0.865, 1.075) | |
| Spouse (Ref: No) | ||||||
| Yes | 0.0408 | 0.0610 | 0.4482 | 0.5032 | 1.042 (0.924, 1.174) | |
| Education level (Ref: Higher) | ||||||
| Primary or below | -0.3759 | 0.0863 | 18.9833 | <0.0001 | 0.687 (0.580, 0.813) | |
| Secondary | -0.0769 | 0.0509 | 2.2792 | 0.1311 | 0.926 (0.838, 1.023) | |
| Occupation (Ref: White-collar) | ||||||
| Unemployed | -0.1291 | 0.0559 | 5.3329 | 0.0209 | 0.879 (0.788, 0.981) | |
| Blue-collar | -0.0905 | 0.0729 | 1.5406 | 0.2145 | 0.913 (0.792, 1.054) | |
| Monthly household income per capita (Ref: 6001–) | ||||||
| 0-3000 | 0.0330 | 0.0570 | 0.3365 | 0.5618 | 1.034 (0.924, 1.156) | |
| 3001-6000 | 0.0203 | 0.0492 | 0.1707 | 0.6795 | 1.021 (0.927, 1.124) | |
| Medical insurance (Ref: Out-of-pocket payment) | ||||||
| Resident/employee | 0.2826 | 0.0552 | 26.2324 | <0.0001 | 1.327 (1.191, 1.478) | |
| Commercial | 0.4848 | 0.1430 | 11.4930 | 0.0007 | 1.624 (1.227, 2.149) | |
| Government-funded | 0.2163 | 0.1572 | 1.8926 | 0.1689 | 1.241 (0.912, 1.690) | |
| Number of chronic diseases (Ref: Multiple) | ||||||
| None | -0.5776 | 0.0913 | 39.9822 | <0.0001 | 0.561 (0.469, 0.671) | |
| Single | -0.3353 | 0.0997 | 11.3167 | 0.0008 | 0.715 (0.588, 0.869) | |
| Smoking history (Ref: No) | ||||||
| Yes | 0.0849 | 0.0608 | 1.9542 | 0.1621 | 1.089 (0.966, 1.226) | |
| Drinking history (Ref: No) | ||||||
| Yes | 0.1830 | 0.0461 | 15.7526 | <0.0001 | 1.201 (1.097, 1.314) | |
| Residence (Ref: Rural) | ||||||
| Urban | 0.0454 | 0.0501 | 0.8211 | 0.3648 | 1.046 (0.949, 1.154) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



