
Submitted:
04 June 2025
Posted:
04 June 2025
You are already at the latest version
Abstract
Objectives: To investigate the real-world outcomes of a population-based gastric cancer (GC) screening program in Kawasaki City. Methods: A total of 337,842 citizens underwent population-based GC screening in Kawasaki City between December 2012 and 2021, resulting in the detection of 1,087 GC cases. Esophageal cancer (EC) has been recorded since 2016, with 236 cases detected. To evaluate the short- and long-term clinical outcomes of screening-detected GC and EC, we conducted a retrospective study using electronic medical records of patients treated at our hospital which is a high-volume institution for GC and EC treatment in the city. As a control group, we included 34 GC and EC cases diagnosed based on symptoms at our hospital in 2018. Results: Among the 1,087 GC cases detected through population-based screening, 102 cases treated at our hospital were included in the analysis. Of these, 91 patients (89%) were diagnosed with early-stage GC. All screening-detected GC cases underwent either surgery (27 cases) or endoscopic submucosal dissection (75 cases). The five-year survival rates for GC were 90% in males and 86% in females. Eighteen EC cases were also included in our study. The five-year survival rate for screening-detected advanced GC was 70.0%, and for screening-detected EC was 100%, both significantly higher than those for symptom-diagnosed GC (30.0%) and EC (40.8%). Conclusions: The prognosis of GC and EC detected through population-based endoscopic screening is significantly better than that of cancers diagnosed based on symptoms, underscoring the effectiveness of endoscopic screening as a tool for early detection of upper gastrointestinal tract cancers. Keywords: gastric cancer; esophageal cancer; endoscopy; population-based screening
Keywords:
gastric cancer
; esophageal cancer
; endoscopy
; population-based screening
1. Introduction
Gastric cancer (GC) remains an important cancer worldwide, with more than 1.2 million new cases per year and an estimated 769,000 deaths worldwide; it ranks 5th in incidence and 4th in mortality in 2020 [1]. GC is the most common cancer in Eastern Asia, including Japan [1,2]. Therefore, GC screening has played a significant role in reducing GC mortality in this area [3]. The projected number of GC incidence and deaths in Japan in 2023 were reported to be 129,900 and 41,800, respectively. Population-based GC screening using the upper gastrointestinal (UGI) barium X-ray radiography was introduced in Japan in the 1960s and has been shown to reduce GC mortality [4]. The national government policy recommended population-based GC screening for adults ≥40 years each year using UGI barium X-ray radiography since 1983 [5]. The revised 2016 Japanese guidelines allow for either biennial endoscopic screening for adults ≥50 years or annual UGI barium X-ray radiography screening for adults ≥40 years [6]. Although age-adjusted mortality rates for GC (based on the 1985 population) have been declining, GC screening remains important, with 15.6 (per 100,000) for male (ranked 3rd) and 5.8 (per 100,000) for female (ranked 5th) [2].
Kawasaki City, located next to Metropolitan Tokyo, has a population of approximately 1.54 million and is part of the Keihin Industrial Area. Although annual process indicators for population-based GC screening—such as participation rate, detection rate, recall rate, and positive predictive value—have been reported by the City Bureau [7], detailed patient characteristics, including cancer stage, treatment, and prognosis, remain unclear for screening-detected GC. Population-based endoscopic GC screening can also detect esophageal cancer (EC). Our hospital, a high-volume institution for GC and EC treatment in Kawasaki City, has received many referrals for population-based screening detected GCs and ECs from other registered clinics and hospitals in Kawasaki City. In this study, we evaluated the real-world setting of GCs and ECs detected through population-based screening in a large Japanese city by examining the short- and long-term clinical outcomes of patients treated at our hospital.
2. Results
2.1. Baseline Characteristics of the Patients
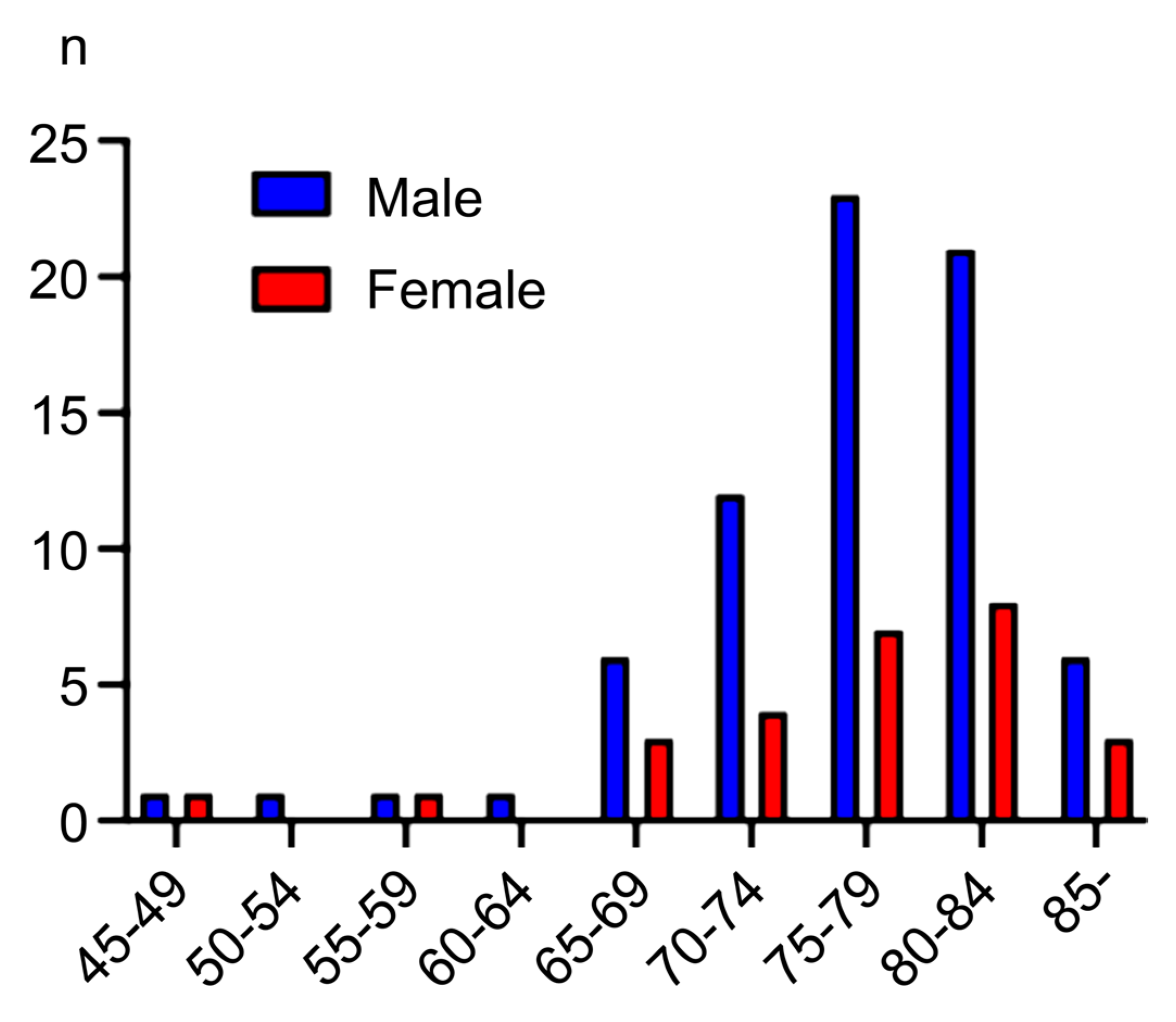
A total of 337,842 Kawasaki City citizens underwent population-based gastric cancer (GC) screening between 2012 and 2021, including 119,009 screened by upper gastrointestinal barium X-ray radiography and 238,833 by endoscopy. Among them, 1,087 GC cases were detected (0.32% overall; 139 by radiography and 948 by endoscopy). Recording of esophageal cancer (EC) cases began in 2016, and 236 cases were detected between 2016 and 2021. In 2021, the participation rate for population-based screening was 13.7%, and the GC detection rate was 0.29% [7]. According to the 2020 nationwide survey on GC screening conducted by the Japanese Society for Gastrointestinal Cancer Screening, the GC detection rates for UGI barium X-ray radiography and endoscopic screening were 0.052% and 0.22%, respectively [8]. Of the 1,087 GC cases detected throughout Kawasaki City during the study period, a total of 102 cases (74 males and 28 females)—97 detected by endoscopic screening and 5 by UGI barium X-ray radiography—were treated at our hospital. The confidence level for this sample of screening-detected GC cases treated at our hospital was 69%. The mean age at diagnosis was 74.8 years (range: 49–88) for males and 74.9 years (range: 47–89) for females (Figure 1).
Figure 1.
Age groups of the Kawasaki City population-based screening detected gastric cancer.
Of the 102 cases, 14 GCs were detected through population-based screening at our hospital, while the remaining 88 cases were detected at other facilities and subsequently referred to our hospital. Early-stage GC, defined as tumor invasion confined to the mucosa or submucosa, was diagnosed in 91 patients (89%), encompassing 94 lesions. The macroscopic classifications of early GC lesions [9] were as follows: 0-I (protruded type) in 1 lesion, 0-IIa (superficial elevated type) in 30 lesions, 0-IIb (superficial flat type) in 4 lesions, 0-IIc (superficial depressed type) in 59 lesions, and none were classified as 0-III (excavated type). Histologically, 86 lesions were of the differentiated type, while 8 were undifferentiated.
We examined the Helicobacter pylori (Hp) infection status in GCs detected through population-based screening. Ninety-five percent of GC cases were associated with Hp infection. Of these, 51 patients (50%) had current infections, 44 (43%) had past infections, and two had previously undergone gastrectomy for peptic ulcers. There were five Hp-negative GC cases (5%), including four early-stage and one advanced-stage GC (T3 with subserosal invasion); all five cases remained recurrence-free five years postoperatively.
Additionally, among the 236 EC cases detected through population-based GC screening across the city, 18 cases (15 males and 3 females) were treated at our hospital. Of these, 15 were squamous cell carcinomas (SCC) and 3 were adenocarcinomas. The confidence level for this sample of screening-detected EC cases treated at our hospital was 33%. The mean age at diagnosis was 70.7 years (range: 47–80). Early-stage EC (intramucosal lesions) was identified in 10 patients (50%).
2.2. Stages, Treatment, and Outcome of Population-Based Screening Detected GCs
All patients with GCs detected through population-based screening underwent either surgery (27 cases, 26.5%) or endoscopic submucosal dissection (ESD; 75 cases, 73.5%) at our hospital (Table 1). Indications for endoscopic treatment were determined according to the endoscopic curability classification (eCura system [10], Appendix A). Six patients subsequently underwent surgery following endoscopic resection, based on the criteria for eCuraC-2 classification, which is considered a standard indication for additional surgical intervention. No treatment-related deaths occurred within 30 days. Figure 2 presents representative endoscopic images and pathological findings of typical early-stage GC detected through population-based screening.
As treatment for the 18 EC cases detected through population-based GC screening, ESD was performed in 10 cases (9 squamous cell carcinomas [SCCs] and 1 adenocarcinoma), thoracic esophagectomy in 3 cases (2 adenocarcinomas and 1 SCC), and chemoradiotherapy in 6 cases (Table 1).
Figure 3.
Overall survival rate of gastric cancer detected through population-based screening. The five-year survival rate was observed to be 86.9%, with a total of 10 confirmed deaths—3 attributable to gastric cancer and 7 resulting from other causes.
Figure 3.
Overall survival rate of gastric cancer detected through population-based screening. The five-year survival rate was observed to be 86.9%, with a total of 10 confirmed deaths—3 attributable to gastric cancer and 7 resulting from other causes.
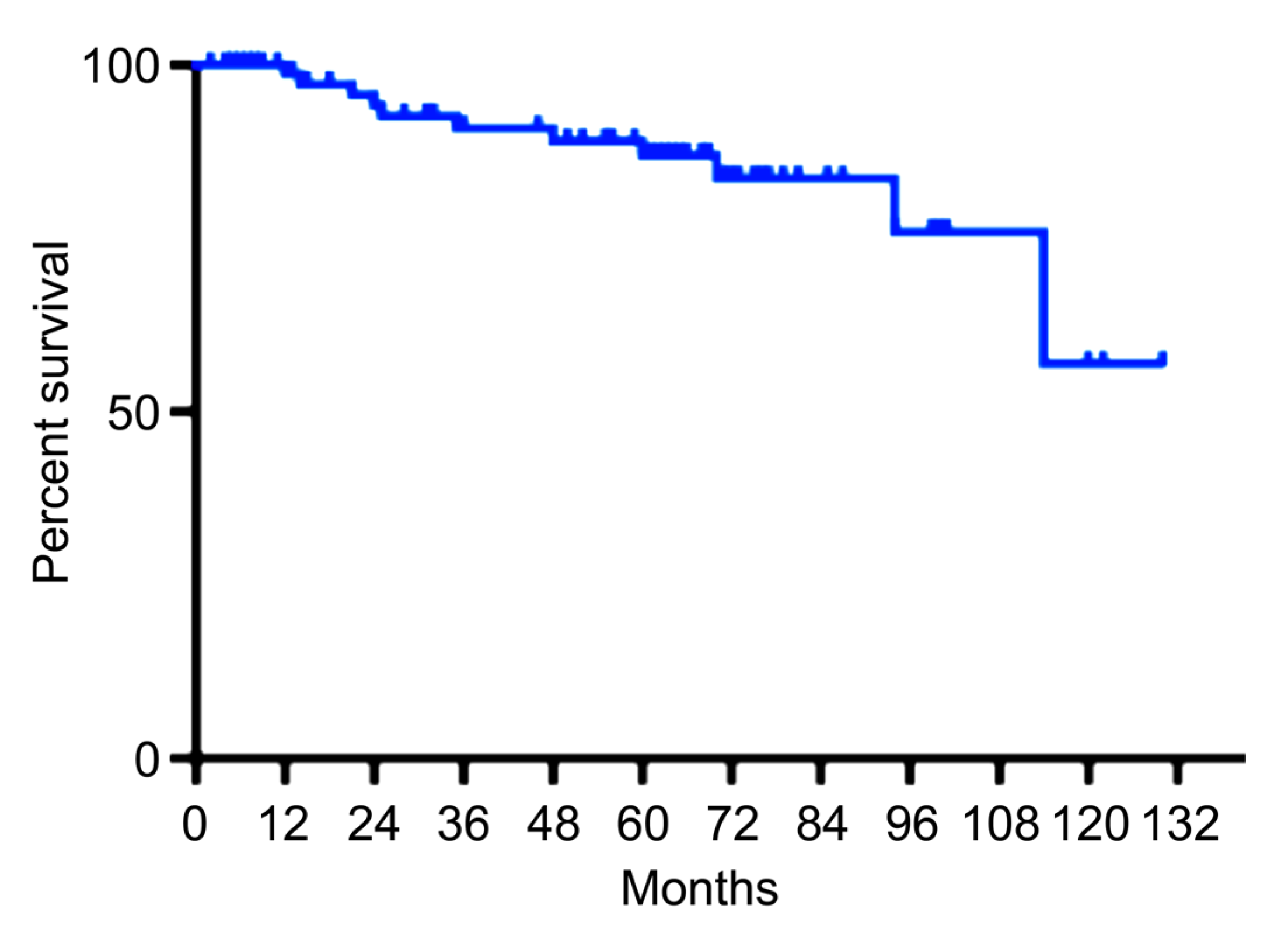
The overall survival rate of GC cases detected through population-based screening was analyzed using the Kaplan–Meier method (Figure 3). The five-year survival rate was 86.9%, with 10 deaths confirmed—3 attributable to GC and 7 due to other causes. The five-year survival rate was 90% in males and 86% in females (Figure 4).
Figure 4.
The survival rate of population-based screening detected gastric cancer for males (Left) and females (right). Five-year survival was 90% for males and 86% for females. The solid lines are the life expectancy of a 75-year-old Japanese male and female.
Figure 4.
The survival rate of population-based screening detected gastric cancer for males (Left) and females (right). Five-year survival was 90% for males and 86% for females. The solid lines are the life expectancy of a 75-year-old Japanese male and female.

The average life expectancy in Japan (as of 2022) for a 75-year-old is 12.0 years (151 months) for men and 15.7 years (188 months) for women [11]. When a straight reference line representing the life expectancy of a 75-year-old woman is added to the Kaplan–Meier curve, the survival curve for females appears to lie above this line, suggesting that survival exceeds the national average life expectancy for women of that age.
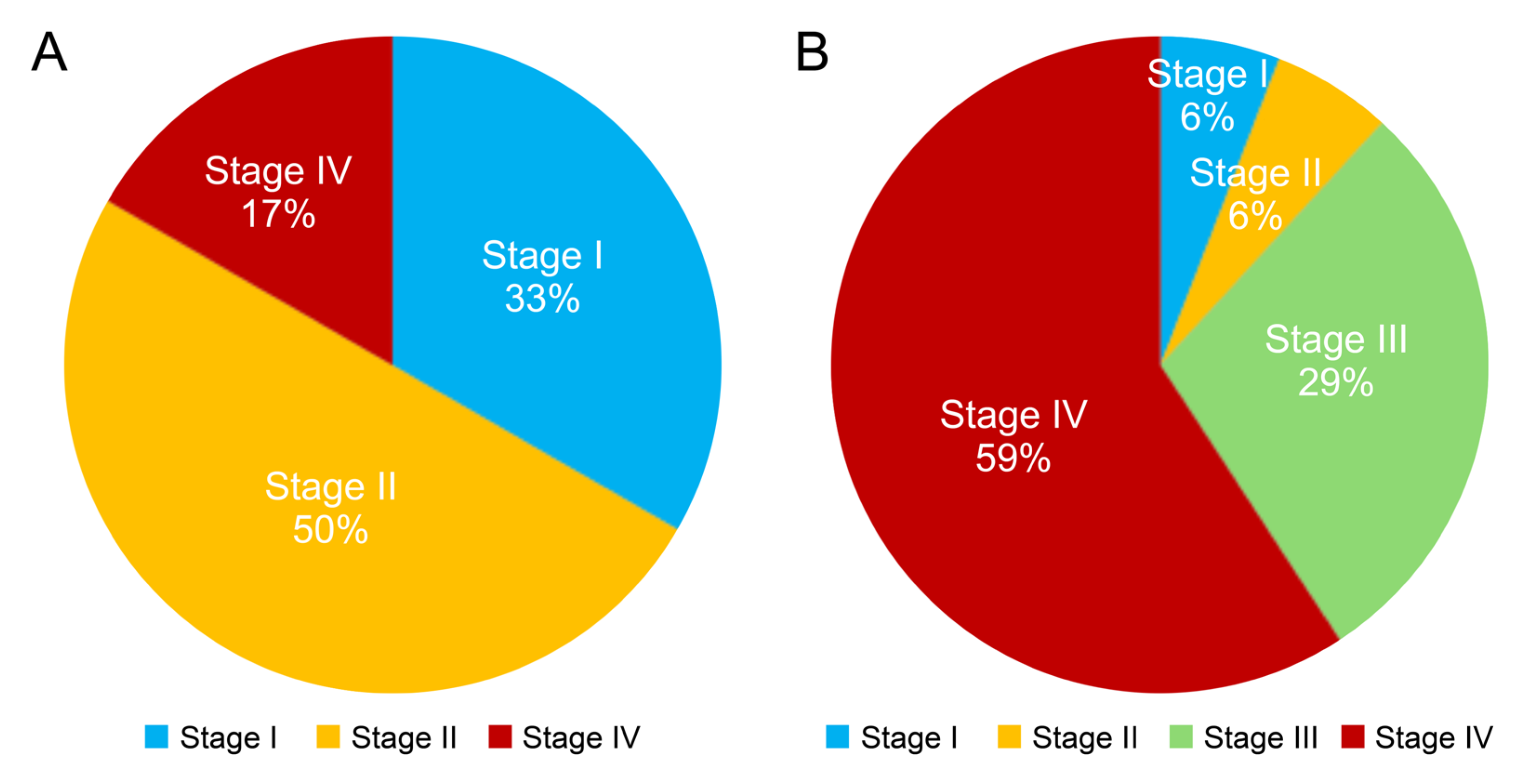
To further compare the prognoses of GC detected through population-based screening and GC diagnosed based on symptoms, we analyzed 11 patients with screening-detected advanced GC and 34 patients with symptom-diagnosed advanced GC who were diagnosed and treated at our hospital in 2018 (24 males and 10 females; mean age at diagnosis, 71.2 years; range: 42–86 years; Supplementary Table A1). The proportion of patients with early-stage disease (stage 1 or 2) among those with advanced GC detected through screening was significantly higher than that among those diagnosed based on symptoms (83% vs. 12%; p < 0.001; Figure 5). Treatments for symptom-diagnosed GC included chemotherapy in 16 cases, surgery in 12 cases, and palliative care in 6 cases.
Figure 5.
The stages of advanced gastric cancers detected by population-based screening (A) and those diagnosed by symptoms (B). The proportion of advanced gastric cancers detected by population-based screening in the early stages (stage 1 or 2) was significantly higher than those diagnosed based on symptoms (83% vs. 12%; p < 0.001).
Figure 5.
The stages of advanced gastric cancers detected by population-based screening (A) and those diagnosed by symptoms (B). The proportion of advanced gastric cancers detected by population-based screening in the early stages (stage 1 or 2) was significantly higher than those diagnosed based on symptoms (83% vs. 12%; p < 0.001).
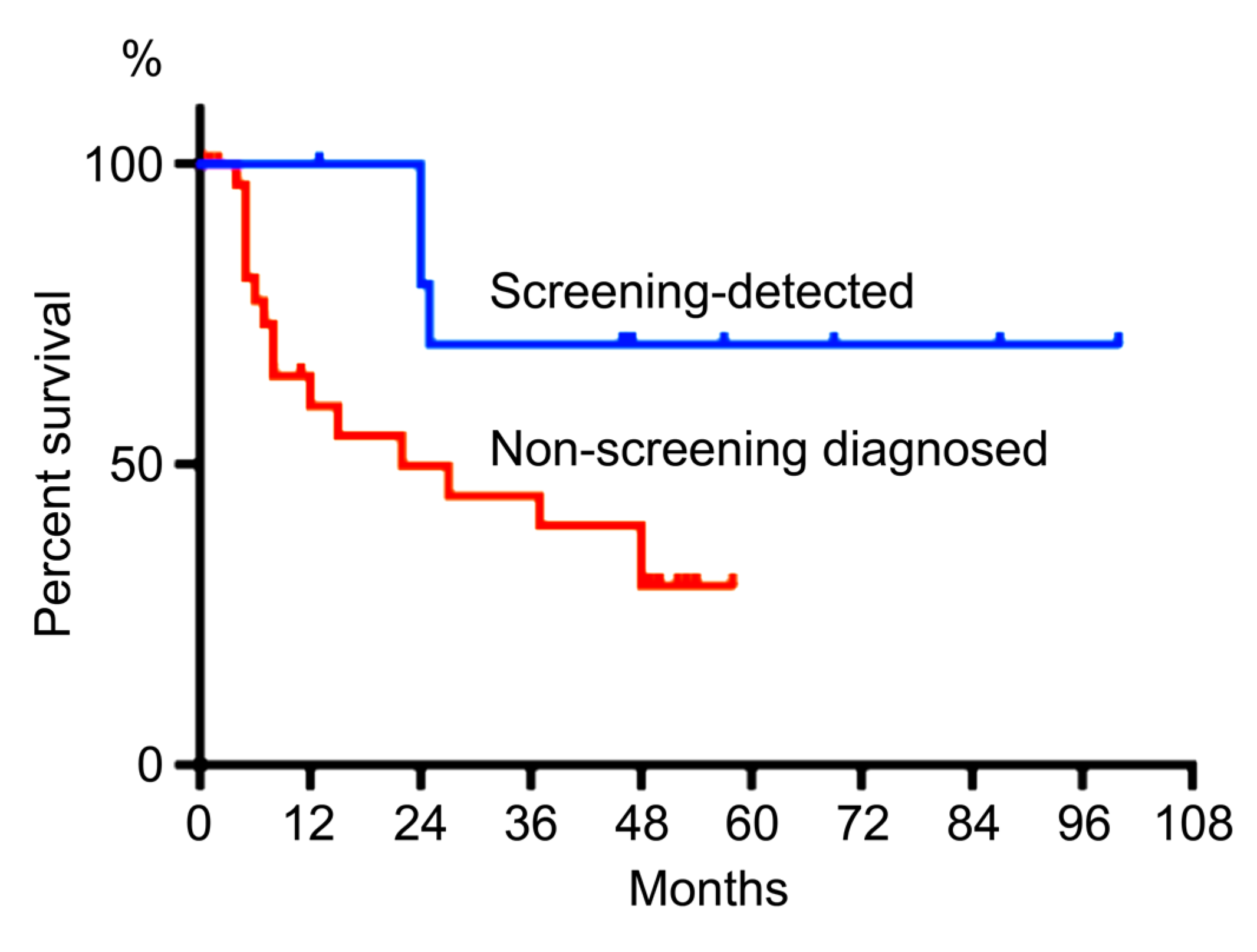
Accordingly, the 5-year survival rate for advanced GC detected through population-based screening was 70.0%, which was significantly higher than the 30.0% survival rate observed in the 34 cases of symptom-diagnosed advanced GC (p < 0.05; Figure 6).
Figure 6.
The survival rate of population-based screening detected advanced gastric cancer or non-screening diagnosed advanced gastric cancer. The 5-year survival rate of population-based screening detected advanced gastric cancer was 70.0%, which was significantly better than that of non-screening-diagnosed gastric cancer (30.0 %).
Figure 6.
The survival rate of population-based screening detected advanced gastric cancer or non-screening diagnosed advanced gastric cancer. The 5-year survival rate of population-based screening detected advanced gastric cancer was 70.0%, which was significantly better than that of non-screening-diagnosed gastric cancer (30.0 %).
Finally, we compared the prognosis of EC cases detected through population-based GC screening with those diagnosed based on symptoms at our hospital in 2018 (24 males and 10 females; mean age at diagnosis: 69.4 years; range: 55–86 years). The clinical stages of symptom-detected EC were as follows: Stage I in 3 cases, Stage II in 7 cases, Stage III in 8 cases, and Stage IV in 16 cases. Treatments included surgery in 13 cases, chemoradiotherapy in 12 cases, chemotherapy in 5 cases, radiotherapy in 2 cases, and other treatments in 1 case. The proportion of patients with early-stage EC (Stage 0 or I) detected through population-based GC screening was significantly higher than that among symptom-diagnosed cases (83% vs. 8.8%; p < 0.05). The 5-year survival rate for screening-detected EC was 100%, which was significantly higher than the 40.8% survival rate for the 34 cases of symptom-diagnosed EC (p < 0.001; Figure 7).
3. Discussion
In this study, we evaluated the real-world setting of GCs detected through population-based screening in a large Japanese city by examining the short- and long-term clinical outcomes of screening-detected cases treated at a high-volume institution. Among these, 89% were diagnosed at an early stage, and the five-year survival rate reached 86%.
Because GC is often asymptomatic in its early stages, the prognosis for advanced GC diagnosed based on symptoms is generally poor [12]. Compared with advanced GCs detected through population-based screening, the present study showed that the prognosis of symptom-diagnosed advanced GC remained significantly worse. Most patients with stage I–II GC do not die from the disease, whereas the majority of those with stage IV cancer do [13]. These findings highlight the importance of early detection in improving long-term survival outcomes for GC.
In the present study, 95% of GC cases detected through population-based screening were identified by endoscopic screening. Endoscopy detected nearly seven times more GC cases than population-based UGI barium X-ray radiography. Endoscopy is known to have higher sensitivity than UGI barium X-ray radiography in both clinical and screening settings. In Japan, the use of UGI barium X-ray radiography for GC screening has been declining. Contributing factors include a decreasing number of physicians skilled in interpreting barium studies, and the requirement for upper endoscopy prior to Hp system. As shown in the present study, the mean age at GC detection was 75 years. Patients of this age often have trouble changing positions during barium imaging and may suffer from constipation after ingesting barium. A population-based case-control study conducted in Tottori and Niigata Prefectures, Japan, demonstrated a 30% reduction in GC mortality with endoscopic screening compared to no screening within a 36-month period [14]. Similarly, a population-based cohort study in the cities of Tottori and Yonago showed that endoscopic screening reduced GC mortality by 67% compared to UGI barium X-ray radiography screening [15]. Based on these findings, the Japanese guidelines were revised in 2016 to recommend either endoscopic or UGI barium X-ray screening for adults aged ≥50 years [6]. In South Korea, a biennial national screening program offering either endoscopic or radiographic screening for adults aged ≥40 years was launched in 2002 [16]. A nested case-control study using data from the Korean National Database reported a 47% reduction in GC mortality associated with endoscopic screening [17]. During this time, the proportion of early GC diagnoses increased from 39% in 2001 to 73% in 2016 [12]. Furthermore, a systematic review and meta-analysis indicated that endoscopic screening in Asian countries may result in a 40% relative risk reduction in GC mortality. However, no significant association has been reported between endoscopic screening and the incidence of GC [18].
GC has been strongly associated with prior or current infection with Hp [19,20]. In the present study, nearly 95% of the population-based screening detected GCs were related to Hp infection. In the present study, 50% of the patients had a current infection, and 43% had a past infection, indicating that GC screening is important even after Hp eradication. GC is detected during endoscopic surveillance at an annual rate of 0.35% for more than 20 years after Hp eradication in patients with mild-to-moderate gastric atrophy [20]. Most countries have observed a decline in the prevalence of Hp infections [21,22]. In Japan, a decreasing trend in the prevalence of Hp infection over the last few decades, coupled with a decrease in the extent and severity of gastric atrophy [23,24]. Currently, Hp antibody and serum pepsinogen tests are not recommended for population-based screening in Japan because of insufficient evidence [25,26,27]. Risk stratification using Hp status and degree of gastric atrophy could identify high-risk groups and provide more effective screening.
GC has been strongly associated with prior or current Hp infection [19,20]. In the present study, nearly 95% of GC cases detected through population-based screening were related to Hp infection. Specifically, 50% of patients had a current infection and 43% had a past infection, indicating that GC screening remains important even after Hp eradication. GC continues to be detected at an annual rate of 0.35% during endoscopic surveillance for over 20 years after Hp eradication in patients with mild-to-moderate gastric atrophy [20]. Most countries have observed a decline in the prevalence of Hp infection [21,22]. In Japan, this downward trend has been accompanied by a reduction in both the extent and severity of gastric atrophy over recent decades [23,24]. Currently, Hp antibody and serum pepsinogen tests are not recommended for population-based screening in Japan due to insufficient supporting evidence [25,26,27]. However, risk stratification using Hp infection status and the degree of gastric atrophy may help identify high-risk individuals and enable more targeted and effective screening strategies.
In addition to its impact on GC mortality, nationwide screening in South Korea may also reduce mortality from other upper gastrointestinal diseases, including EC and peptic ulcers. EC is the seventh most common cancer and the sixth leading cause of cancer-related deaths worldwide [1]. Early detection is particularly important in patients with EC. In the present study, 18 cases of EC detected through population-based GC screening were included, of which 50% were diagnosed at an early stage. The prognosis for EC detected through screening was significantly better than that for EC diagnosed based on symptoms. According to the aforementioned nationwide GC screening survey in Japan, EC was identified in 0.05% of individuals undergoing GC endoscopic screening, with 62% of those cases being early-stage cancer [8]. However, there are currently no global screening recommendations for EC, particularly for squamous cell carcinoma [28]. Korean studies have reported that national GC screening may also reduce EC mortality, with upper endoscopy proving superior to UGI barium X-ray screening [29]. Taken together, these findings suggest that endoscopic screening for GC has the potential to serve as an effective screening method for upper gastrointestinal tract cancers, including EC. In the present study, ESD was performed in 73.5% of GC cases and 56% of EC cases, indicating that population-based GC screening facilitates early detection of cancers that are amenable to endoscopic treatment.
This study had several limitations. First, symptomatic individuals were not excluded. The free-of-charge population-based GC screening program for individuals aged ≥70 years may have encouraged the participation of symptomatic individuals. Second, although the study was conducted at a high-volume institution that treated approximately 10% of the GCs detected through population-based screening, it was a single-center study, and the sample size was limited. Third, lead-time bias may have influenced the results. GCs detected through population-based screening are typically asymptomatic and associated with better prognoses, whereas symptom-detected GCs often present at more advanced biological stages and have poorer outcomes. Fourth, this study included many older individuals with GC. In Japan, GC screening is commonly conducted as part of routine workplace health checkups for individuals in their 40s to 60s [30], which may limit the generalizability of these findings to younger populations.
4. Patients and Methods
4.1. Population-Based GC Screening of Kawasaki City
In Kawasaki City, population-based endoscopic GC screening was introduced in December 2012, supplementing the existing annual population-based GC screening using UGI barium X-ray radiography, which had been conducted for decades. Participants could choose to undergo either upper endoscopy or UGI barium X-ray radiography. Initially, endoscopic screening was offered annually to individuals aged ≥40 years. In accordance with national guidelines [6], the screening protocol was revised in 2020 to recommend biennial endoscopic screening for individuals aged ≥50 years or annual UGI barium X-ray radiography for those aged ≥40 years.
4.2. Patients
This retrospective study was conducted at a single institution. St. Marianna University Hospital (Kawasaki, Japan) has participated in the Kawasaki City population-based GC screening program since the introduction of endoscopic screening. As controls, we included 34 patients with advanced GC and 34 patients with EC who were diagnosed based on symptoms at our hospital between January and December 2018. The main presenting symptoms for GC were epigastric pain, anemia, and weight loss; for EC, they included dysphagia, pharyngeal discomfort, and epigastric pain. Diagnosis and staging of GC were performed according to the Japanese Classification of Gastric Carcinoma issued by the Japanese Gastric Cancer Association [9]. Treatment of GC followed the Japanese Gastric Cancer Treatment Guidelines [10]. Indications for endoscopic treatment were determined based on the endoscopic curability (eCura) system [Appendix], which recommends subsequent surgery following eCuraC-2 classification as standard treatment. Staging and treatment of EC were performed according to the Esophageal Cancer Practice Guidelines established by the Japan Esophageal Society [31].
4.3. Helicobacter pylori (Hp) Infection Status
Serum Hp antibodies, urea breath test, fecal antigen test, patient history of Hp eradication, and endoscopic findings—including assessment of gastric atrophy using the Kimura–Takemoto classification—were combined to determine Hp infection status.
4.4. Statistical Analysis
The χ² test or Fisher’s exact test was used to compare categorical variables. Kaplan–Meier analysis and log-rank tests were employed for survival analysis. All statistical analyses were performed using GraphPad Prism, version 9 (GraphPad Software, San Diego, CA, USA). P-values < 0.05 were considered statistically significant. The confidence level for the sample size was calculated assuming a population proportion of 0.5.
5. Conclusions
The prognosis for GC and EC detected through population-based endoscopic screening was significantly better than that of cancers diagnosed based on symptoms, indicating the utility of endoscopy as a screening tool for upper gastrointestinal tract cancers. Population-based endoscopic screening for GC may offer an additional survival benefit for patients with both GC and EC.
Author Contributions
Conceptualization, H.Y. and K.T..; Investigation, H.Y., Y.S.; M.K., T.K., Y.N..; methodology, T.M..; validation, H.Y., Y.S. and H.K.; formal analysis, T.M.; resources, H.Y.; data curation, H.Y.; writing—original draft preparation, H.Y.; writing—review and editing, H.Y.; visualization, H.Y.; supervision, K.T; funding acquisition, H.Y.
Funding
This work was supported in part by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology of Japan (23K06917; H. Y.).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Institutional Review Board of St. Marianna University School of Medicine on March 29, 2024 (No. 6371).
Informed Consent Statement
Written informed consent for the secondary use of screening data for research purposes was obtained from all participants in the endoscopic GC screening. Informed consent was obtained via an opt-out manner on the intuitional website for this study.
Data Availability Statement
Details of the research data presented in this paper will be provided within three months upon request to the corresponding author.
Acknowledgements
We would like to thank all members of the Kawasaki City Medical Association, including the chairperson, Dr. Toshiaki Okano. We would like to thank Editage (www.editage.com) for the English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| GC | gastric cancer |
| EC | esophageal cancer |
| Hp | Helicobacter pylori |
| SCC | squamous cell carcinomas |
| ESD | endoscopic submucosal dissection |
| eCura | endoscopic curability |
| DG | distal gastrectomy |
| TG | total gastrectomy |
| CRT | chemoradiotherapy |
| UGI | upper gastrointestinal |
Appendix A
Japanese Gastric Cancer Association’s Japanese Gastric Cancer Treatment Guidelines [10] defines endoscopic curability (eCura system) of gastric cancer as follows:
Endoscopic curability A (eCuraA):
The resection is classified as endoscopic curability A (eCuraA) when all of the following conditions are fulfilled, provided the cancer has no ulcerative findings (UL0): en bloc resection, any tumor size in case of histologically differentiated type-dominant, tumor size ≤ 2 cm in case of histologically undifferentiated type-dominant, pT1a, negative horizontal margin (HM0), negative vertical margin (VM0), and no lymphovascular infiltration (Ly0, V0). However, if the undifferentiated component of the lesion exceeds 2 cm in length, the endoscopic curability is classified as C-2 (eCuraC-2).
When the cancer has ulcerative findings (UL1), the resection is still classified as eCuraA when all of the following conditions are fulfilled: en bloc resection, tumor size ≤ 3 cm, histologically differentiated type-dominant, pT1a, HM0, VM0, Ly0, V0.
Endoscopic curability B (eCuraB):
The resection is classified as endoscopic curability B (eCuraB) for pT1b cancer when all of the following conditions are fulfilled: en bloc resection, histologically of differentiated type-dominant, pT1b1 (SM1) (< 500 μm from the muscularis mucosae), HM0, VM0, Ly0, V0, tumor size ≤ 3 cm. However, if the undifferentiated component is included in the portion of submucosal invasion, the endoscopic curability is classified as C-2 (eCuraC-2).
Endoscopic curability C (eCuraC):
The resection is classified as endoscopic curability C (eCuraC) when it does not fulfill the conditions described above to be classified as either eCuraA or eCuraB. The resection is classified as endoscopic curability C-1 (eCuraC-1) when it is histologically differentiated type either not resected en bloc or had a positive horizontal margin even though fulfilling other criteria to be classified into either eCuraA or eCuraB. All other eCuraC resections are subclassified as endoscopic curability C-2 (eCuraC-2).
Appendix B

Table A1.
Patients characteristics of screening-detected and non-screening diagnosed advanced gastric cancer (GC). BSC; best supportive care.
Table A1.
Patients characteristics of screening-detected and non-screening diagnosed advanced gastric cancer (GC). BSC; best supportive care.
| Screening detected advanced GC | Non-screening diagnosed advanced GC | ||
| (n=11) | (n=34) | ||
| Age mean(range) | 71.0 (47-86) | 71.2 (42-86) | |
| Sex (male/female) | 8 / 3 | 24 / 10 | |
| Stage | I | 3 | 2 |
| II | 6 | 2 | |
| III | 10 | ||
| IV | 2 | 20 | |
| Treatment | surgery | 11 | 12 |
| chemotherapy | 16 | ||
| BSC | 6 |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021, 71, 209–249. [CrossRef]
- National Cancer Center. Cancer statistics in Japan 2023. Available online: https://ganjoho.jp/public/qa_links/report/statistics/2023_en.html (accessed on 26 May 2025).
- Sun, D.; Mülder, D.T.; Li, Y.; Nieboer, D.; Park, J.Y.; Suh, M.; Hamashima, C.; Han, W.; O’Mahony, J.F.; Lansdorp-Vogelaar, I. The effect of nationwide organized cancer screening programs on gastric cancer mortality: A synthetic control study. Gastroenterology 2024, 166, 503–514. [CrossRef]
- Fukao, A.; Tsubono, Y.; Tsuji, I.; Hisamichi, S.; Sugahara, N.; Takano, A. The evaluation of screening for gastric cancer in Miyagi Prefecture, Japan: a population-based case-control study. Int J Cancer 1995, 60, 45–48. [CrossRef]
- Oshima, A. A critical review of cancer screening programs in Japan. Int J Technol Assess Health Care 1994, 10, 346–358. [CrossRef]
- Hamashima, C. Cancer screening guidelines and policy making: 15 years of experience in cancer screening guideline development in Japan. Jpn J Clin Oncol 2018, 48, 278–286. [CrossRef]
- Kawasaki City Health and Welfare Bureau. Annual Reports of Results of Kawasaki City Gastric and Colon Cancer Screening. (in Japanese).
- Japanese Society for Gastrointestinal Cancer Screening. Nationwide survey of gastric cancer screening status. Available online: https://www.jsgcs.or.jp/files/uploads/2020zenkoku_naisikyo.pdf (in Japanese, last accessed Oct. 19, 2024).
- Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 2011, 14, 101.
- 10. Japanese Gastric Cancer Association. Japanese Gastric Cancer Treatment Guidelines 2021: 6th edition. Gastric Cancer 2023, 26, 1.
- Ministry of Heal, Labor and Welfare. Japanese life expectancy at major ages groups. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/life/life23/dl/life23-02.pdf (in Japanese, last accessed May 26. 2025).
- Huang, R.J.; Epplein, M. An Approach to the primary and secondary prevention of gastric cancer in the United States. Clin Gast Hepatol 2021, 20, 2218–2228.e2.
- Chang, E.T.; Clarke, C.A.; Colditz, G.A.; Kurian, A.W.; Hubbell, E. Avoiding lead-time bias by estimating stage-specific proportions of cancer and non-cancer deaths. Cancer Causes Control 2024, 35, 849–864. [CrossRef]
- Hamashima, C.; Ogoshi, K.; Okamoto, M.; Shabana, M.; Kishimoto, T.; Fukao, A. A community-based, case-control study evaluating mortality reduction from gastric cancer by endoscopic screening in Japan. PLOS ONE 2013, 8, e79088. [CrossRef]
- Hamashima, C.; Shabana, M.; Okada, K.; Okamoto, M.; Osaki, Y. Mortality reduction from gastric cancer by endoscopic and radiographic screening. Cancer Sci 2015, 106, 1744–1749. [CrossRef]
- Kim, Y.; Jun, J.K.; Choi, K.S.; Lee, H.Y.; Park, E.C. Overview of the National Cancer screening programme and the cancer screening status in Korea. Asian Pac J Cancer Prev 2011, 12, 725–730.
- Jun, J.K.; Choi, K.S.; Lee, H.Y.; Suh, M.; Park, B.; Song, S.H.; Jung, K.W.; Lee, C.W.; Choi, I.J.; Park, E.C.; et al. Effectiveness of the Korean National Cancer Screening Program in reducing gastric cancer mortality. Gastroenterology 2017, 152, 1319–1328.e7. [CrossRef]
- Zhang, X.; Li, M.; Chen, S.; Hu, J.; Guo, Q.; Liu, R.; Zheng, H.; Jin, Z.; Yuan, Y.; Xi, Y.; et al. Endoscopic screening in Asian countries Is associated with reduced gastric cancer mortality: a meta-analysis and systematic review. Gastroenterology 2018, 155, 347–354.e9. [CrossRef]
- Uemura, N.; Okamoto, S.; Yamamoto, S.; Matsumura, N.; Yamaguchi, S.; Yamakido, M.; Taniyama, K.; Sasaki, N.; Schlemper, R.J. Helicobacter pylori infection and the development of gastric cancer. N Engl J Med 2001, 345, 784–789. [CrossRef]
- Take, S.; Mizuno, M.; Ishiki, K.; Kusumoto, C.; Imada, T.; Hamada, F.; Yoshida, T.; Yokota, K.; Mitsuhashi, T.; Okada, H. Risk of gastric cancer in the second decade of follow-up after Helicobacter pylori eradication. J Gastroenterol 2020, 55, 281–288. [CrossRef]
- Graham, D.Y. History of Helicobacter pylori, duodenal ulcer, gastric ulcer and gastric cancer. World J Gastroenterol 2014, 20, 5191–5204. [CrossRef]
- Nagy, P.; Johansson, S.; Molloy-Bland, M. Systematic review of time trends in the prevalence of Helicobacter pylori infection in China and the USA. Gut Pathog 2016, 8, 8. [CrossRef]
- Hirayama, Y.; Kawai, T.; Otaki, J.; Kawakami, K.; Harada, Y. Prevalence of Helicobacter pylori infection with healthy subjects in Japan. J Gastroenterol Hepatol 2014, 29(Suppl 4), 16–19. [CrossRef]
- Kamada, T.; Haruma, K.; Ito, M.; Inoue, K.; Manabe, N.; Matsumoto, H.; Kusunoki, H.; Hata, J.; Yoshihara, M.; Sumii, K.; et al. Time trends in Helicobacter pylori infection and atrophic gastritis over 40 years in Japan. Helicobacter 2015, 20, 192–198. [CrossRef]
- Yanaoka, K.; Oka, M.; Mukoubayashi, C.; Yoshimura, N.; Enomoto, S.; Iguchi, M.; Magari, H.; Utsunomiya, H.; Tamai, H.; Arii, K.; et al. Cancer high-risk subjects identified by serum pepsinogen tests: outcomes after 10-year follow-up in asymptomatic middle-aged males. Cancer Epidemiol Biomarkers Prev 2008, 17, 838–845. [CrossRef]
- Terasawa, T.; Nishida, H.; Kato, K.; Miyashiro, I.; Yoshikawa, T.; Takaku, R.; Hamashima, C. Prediction of gastric cancer development by serum pepsinogen test and Helicobacter pylori seropositivity in Eastern Asians: a systematic review and meta-analysis. PLOS ONE 2014, 9, e109783. [CrossRef]
- Hamashima, C.; Systematic Review Group and Guideline Development Group for Gastric Cancer Screening Guidelines. Update version of the Japanese Guidelines for Gastric Cancer Screening. Jpn J Clin Oncol 2018, 48, 673–683. [CrossRef]
- Domper Arnal, M.J.; Ferrández Arenas, Á.; Lanas Arbeloa, Á. Esophageal cancer: risk factors, screening and endoscopic treatment in Western and Eastern countries. World J Gastroenterol 2015, 21, 7933–7943. [CrossRef]
- Kim, J.H.; Han, K.D.; Lee, J.K.; Kim, H.S.; Cha, J.M.; Park, S.; Kim, J.S.; Kim, W.H.; Big Data Research Group (BDRG) of the Korean Society of Gastroenterology (KSG). Association between the National Cancer Screening Programme (NSCP) for gastric cancer and oesophageal cancer mortality. Br J Cancer 2020, 123, 480–486. [CrossRef]
- Goto, E.; Ishikawa, H.; Okuhara, T.; Kiuchi, T. Relationship of health literacy with utilization of health-care services in a general Japanese population. Prev Med Rep 2019, 14, 100811. [CrossRef]
- Japan Esophageal Society. Esophageal cancer practice guidelines 2022. Esophagus 2023, 20, 343-389. [CrossRef]
Figure 2.
Early gastric cancer detected through population-based endoscopic screening. A 74-year-old male with a history of Helicobacter pylori eradication. A. Transnasal endoscopic image (white light). B. The lesion margin is clearly visualized using linked color imaging. C. Endoscopic submucosal dissection specimen (40×) showing an intramucosal lesion (T1a). D. Magnified view of the blue-framed area (200×).
Figure 2.
Early gastric cancer detected through population-based endoscopic screening. A 74-year-old male with a history of Helicobacter pylori eradication. A. Transnasal endoscopic image (white light). B. The lesion margin is clearly visualized using linked color imaging. C. Endoscopic submucosal dissection specimen (40×) showing an intramucosal lesion (T1a). D. Magnified view of the blue-framed area (200×).
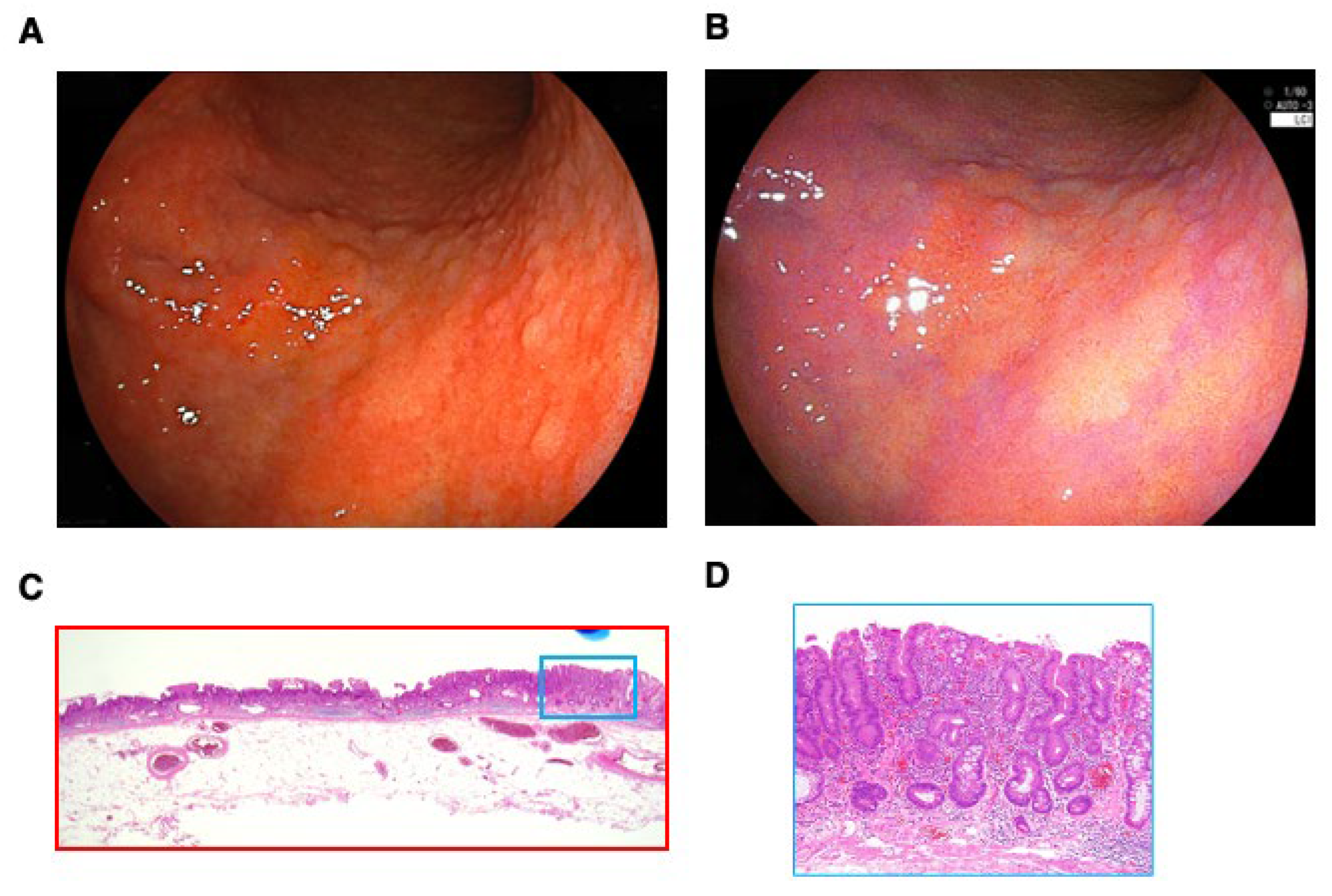
Figure 7.
The survival rate of population-based gastric cancer screening detected esophageal cancer or non-screening diagnosed esophageal cancer. The 5-year survival rate of screening-detected esophageal cancer was 100%, which was significantly better than that of non-screening-diagnosed esophageal cancer (40.8 %).
Figure 7.
The survival rate of population-based gastric cancer screening detected esophageal cancer or non-screening diagnosed esophageal cancer. The 5-year survival rate of screening-detected esophageal cancer was 100%, which was significantly better than that of non-screening-diagnosed esophageal cancer (40.8 %).
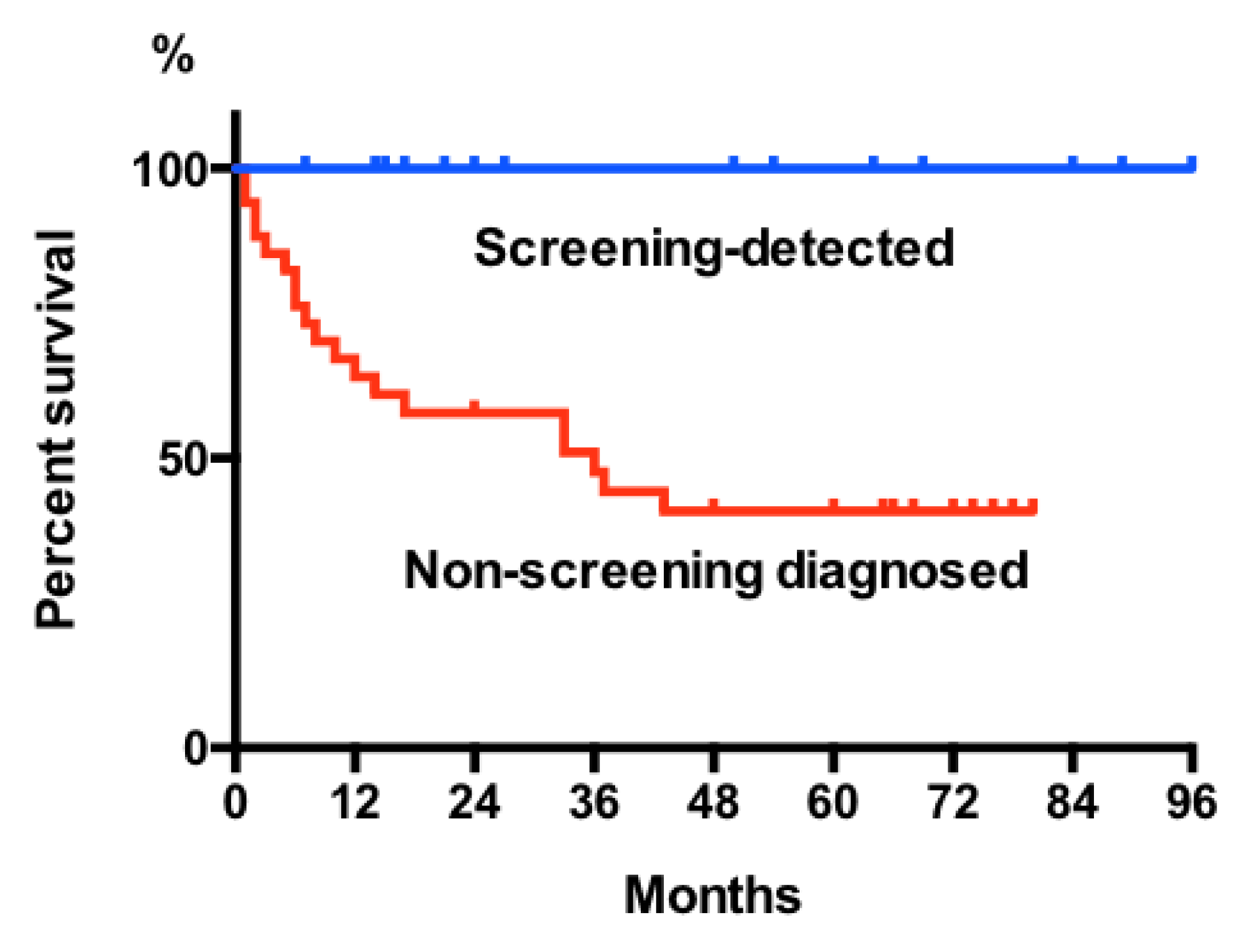
Table 1.
Stages and treatment for population-based screening detected gastric cancer and esophageal cancer treated at our hospital. DG; distal gastrectomy, TG; total gastrectomy, CRT; chemoradiotherapy.
Table 1.
Stages and treatment for population-based screening detected gastric cancer and esophageal cancer treated at our hospital. DG; distal gastrectomy, TG; total gastrectomy, CRT; chemoradiotherapy.
| Stage grouping | n | Treatment | n | |
| Gastric cancer | Stage IA | 69 | ESD | 63 |
| DG | 6 | |||
| StageIB | 25 | DG/TG | 13 | |
| ESD | 6 | |||
| ESD→DG | 6 | |||
| StageⅡA | 6 | DG/TG | 6 | |
| StageⅣB | 2 | DG/TG | 2 | |
| Esophageal cancer | Stage 0 (T1a) | 11 | ESD | 9 |
| thoracic esophagectomy | 1 | |||
| CRT | 1 | |||
| Stage I (T1b) | 4 | ESD | 1 | |
| CRT | 3 | |||
| Stage II | 2 | thoracic esophagectomy | 2 | |
| Stage III | 1 | CRT | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



