Submitted:
30 May 2025
Posted:
03 June 2025
You are already at the latest version
Abstract
BACKGROUND: The Italian Ministry of Health, following CDC recommendations, advises that all children follow the recommended vaccination schedule. OBJECTIVE: This study aimed to assess Italian families’ knowledge, perceptions, and concerns about vaccinations through surveys. MATERIALS AND METHODS: A national survey was conducted in November 2024 by Euromedia Research among 1,000 families with children aged 2 months to 16 years, stratified by sex, age and area of residence,the statistical error of 3.1%, allows to generate a complete picture also in terms of geography, income, parental age, parents age (18 and 55 years). RESULTS: Most parents (90%) consider pediatric vaccines essential for their child’s health, and 86.5% recognize their importance for public health, 73% of parents believe vaccines are safe. Only 34% correctly identified compulsory vaccines in accordance with the Law 19/2017, and just 17% distinguished between mandatory and recommended ones. Responses regarding compliance with vaccination requirements for school enrolment show a high level of disinformation. The key issues on which respondents are often divided are the safety and effectiveness of vaccines. CONCLUSIONS: Despite the high level of knowledge about vaccines reported by the respondents, their answers do not indicate a very deep knowledge. The findings of the survey highlight parental perspectives within the political and public debate concerning the quality of information regarding vaccination, the aspects of vaccination science that remain uncertain, and the limitations of information provided by institutional sources and media. The necessity for more in-depth and comprehensive information is indisputable and also vaccine information for parents should be focused on safety at its core.
Keywords:
childhood vaccination
; national opinion
; survey
; scientific information
; professional information
INTRODUCTION
The Center for Disease Control recommends a Child and Adolescent Immunization Schedule by Age (1). In compliance with the advice of the CDC, in Italy, the Legislative Decree of 7 June 2017, n. 73, amended by the Conversion Law of 31 July 2017, n. 119 (2), provides for 10 compulsory vaccinations and 4 recommended vaccinations for minors aged between 0 and 16 years (3). It is worth remembering that in 2014, as part of the Global Health Security Agenda, Italy was designated as the world outpost in vaccination strategies and campaigns. The Italian vaccination schedule is included in the National Program (PNPV 2023-2-025) for Vaccination Plan (4) and approved by the State-Regions Conference. Thus, since 2017, 10 vaccines are required by law for children under 16 years of age following a Vaccination Calendar schedule. The compulsory vaccines are anti-polio; - anti-diphtheria; - anti-tetanus; - anti-hepatitis B; - anti-whooping cough; - anti-haemophilus influenzae type B; - anti-measles; - anti-rubella; - anti-mumps; - anti-chickenpox. Four other vaccines (i.e., pneumococcal conjugate vaccine, PCV; rotavirus; B- and A-CYW meningococcal vaccines) are strongly recommended and free of cost (5). Compliance with the vaccination requirements is a condition for admission to kindergartens and nursery schools (for children aged 0 to 6 years), while from primary school onwards children and adolescents can continue to attend school and take exams, but if the requirements are not met, a vaccination recovery process is activated by the local health authority and administrative fines of between 100 and 500 euros can be imposed.
The situation in Europe is somewhat different. Each EU\EEA country is responsible for its own national public health policy, including its national immunization program and schedule. (6). Each country’s immunization program may differ. The differences concern the age of the population to be vaccinated, including population groups, the number and timing of doses, the decision to give one vaccine alone or in combination with others, the extent of obligation. Indeed, there are 17 European countries that have no compulsory vaccinations, sixteen countries have only one obligation or more compulsory vaccinations in their vaccination program.
With the aim of assessing the knowledge, judgements, perceptions, fears and concerns of Italian families with children aged 2 months to 16 years, we commissioned a survey on the level of knowledge of which vaccinations are compulsory and which are recommended in Italy; which vaccinations are necessary to attend nursery school, primary school and secondary school; what the constitutional obligations are; the safety of vaccines and the risks of adverse events and we compared answers with their political orientation. Comparisons with obligations in Europe were also explored.
METODOLOGY
This survey was performed by Euromed Research, one of Italy’s most important market research institutes able to manage any research project, from conception to methodology, from information gathering to statistical analysis and data interpretation, to presentation and definition of marketing strategies (7). The survey was commissioned by the AsSIs (Health Studies and Information Association). A scientific association made up of physician, scientists, health professionals and lawyers who work to promote the disease prevention and care of human beings, maintaining a position of total autonomy towards any organization, school, movement, trend or interest group that could potentially affect health policy decisions or drive medical research.
The survey was conducted using C.A.W.I. (Computer-Assisted Web Interviewing) methodology. The advantages of this questionnaire-based methodology, which involves providing respondents with a link, a panel or a website, are illustrated in the reference (8). The sample of 1,000 interviews was stratified by area of residence, gender and age, with an overall statistical error of ±3.1%. The reference data used to construct the sample were based on households with children, with the youngest child being under 17 years of age, adjusted for sex and age (processed data from ISTAT 2023). The sample was defined as illustrated in Figure 1.
Survey execution
- Completed interviews (fully completed questionnaires) 1,000; - Refusals: 1,982 (representing 66.5% of total contacts). No weight adjustments were made as the sample is representative of the target population. Refusals or incomplete interviews were not included in the final sample.
The 1,000 interviews only include respondents who answered all questions, thus ensuring quota compliance.
Survey administration process
- An email was sent, including an introduction letter about the research (the research sponsor remained anonymous) and an active link to access the questionnaire.
- By clicking the link in the email, respondents were directed to a web platform, where they could complete the survey online.
- Upon completing the questionnaire, a thank-you message appeared on the screen.
RESULTS
The data of the survey clearly shows the extent to which parents consider vaccination to be essential for the health of their child (90.1% of the sample vs 9.01% who consider it to be of little or no importance) and for the health of the community (86.5% vs 12.6%). The overall responses are illustrated in Figure 2 panel A and B for children and community respectively. The detailed information is reported in supplemental excel Table 1 (tables 1 and 1.0 for child health) and 2 (2 and 2.2) for the community health.
On the other hand, there are large differences in terms of political orientation. A large majority of Democratic Pary (PD) voters (97.2%) and of Greens and Left Alliance (AVS) voters (96.3%) are more in favor of the benefits of vaccinations for the child and the community. The percentage of undecided and abstainers people is also remarkably high. A graphic representation of the answers is illustrated in Figure 3 panel A and panel B for child and community, respectively.
At the question of “how many are in favor of compulsory vaccination against certain diseases for children under sixteen” 74.0% of the parents surveyed were in favor, especially of the vaccinations currently required by law (49.3%). Noteworthy, around one in four parents (24.7%) also want childhood vaccinations that are currently recommended to be made compulsory. The responses are graphically illustrated in Figure 4 panel A and the raw data are illustrated in supplemental tables 3. As respect of parents age and gender, those most in favor are men, aged between 45 and 64, with children under the age of 2, living in the south and the islands
Regarding political affiliation, PD voters (88.9%) and AVS voters (85.2%) once again stand out among those in favor of compulsory childhood vaccinations; the most skeptical are the supporters of the small parties (60.9%), the League (65.2%) and the undecided (66.1%), as illustrated in Figure 4 panel B and Table 2.2 of supplemental data.
The above data show a high prevalence of positive vaccination responses, but a lack of knowledge about several important aspects, including mandatory or recommended pediatric vaccines is observed in following questions. Indeed, there is a lot of misinformation about which childhood vaccinations are mandatory (M), and which are recommended (R) in Italy. Regarding the M, results are reported in supplemental Table 4 for age, gender, children age, and Table 4.2 for political orientation. As for R, results are reported in Table 5 (for age, gender, children age) and Table 5.2 broken down for political orientation. Less than 50% know the correct answer and 13.5% for M and 18.5% for R, respectively, do not know the answer at all, with a significant proportion of respondents even considering the recommended vaccinations to be compulsory. Conversely, there are compulsory vaccinations, such as against measles and rubella, which are incorrectly recognized as recommended by 21.0% and 20.3% of respondents respectively. About the recommended vaccinations, the highest correct answer was given by 22% only of respondents. A synthetic view of the above data is illustrated in Table “Synthesis 4_5”
Once again, the data show that there are greater differences in political affiliation than in age, gender of parents and age of their children. These misconceptions become even more evident when the issue of vaccination compliance is introduced as a requirement for access to different levels of schooling (Supplemental tables 6, 6.2, 7, 7.2, 8, 8.2, 9, 9.2, 10, 10.2).
Only 35.2% of respondents correctly state that vaccination is required for enrolment in nursery schools and pre-school (supplemental tables 6 and 6.2); in fact, in Italy, enrolment in nursery schools and pre-school (for children aged 0-6) is conditional on compliance with vaccination requirements. Children over 6 and adolescents can continue to attend school and take exams, but if the requirements are not met, a vaccination recovery process will be activated by the local Health Authority and administrative fines between 100 and 500 Euros may be imposed. However, as much as 27.8% believe that vaccination is essential for enrolment in any level of school. Finally, 5.9% of parents believe that it is not necessary to vaccinate their children to enroll them in any school.
With the other school levels, the percentages relating to “Does not know/Does not answer” has significantly increased up to 39.0% for secondary school (children aged 11-16 years). It should be noted, however, that the answer to “No vaccination is compulsory” grows from one school level to the next: for nursery and nursery school it stands at 7.6%, for primary school at 14.6%, for lower secondary school at 19.5% and for upper secondary school at 22.7%. It is worth noting the difference in responses when political orientation is considered. A summary of the above data is illustrated in supplemental Table 7-10.
Knowledge of childhood vaccination requirements in the rest of Europe is also very low. Indeed, when asked about the situation of compulsory childhood vaccinations in the rest of Europe, only 16.1% of the sample correctly said that many European countries have fewer compulsory vaccinations than Italy, or none at all, while as many as 38.6% said that most of other European countries have the same rules as Italy and 21.5% said that about half of the other European countries have compulsory childhood vaccinations as Italy supplemental tables 11 and 11.2.
An overview of obligations and recommendations in Europe and vaccination coverage is given in reference (9). In summary, 17 countries have no obligations (Austria, Greece, the Netherlands, Sweden, Norway, Liechtenstein, Ireland, Finland, Lithuania, Portugal, Estonia, Romania, Iceland, Denmark, Luxembourg, Spain and Cyprus). Germany for measles only and Belgium for polio only. Malta only for diphtheria, tetanus, pertussis and polio. Latvia holds the record with 13 compulsory vaccines.
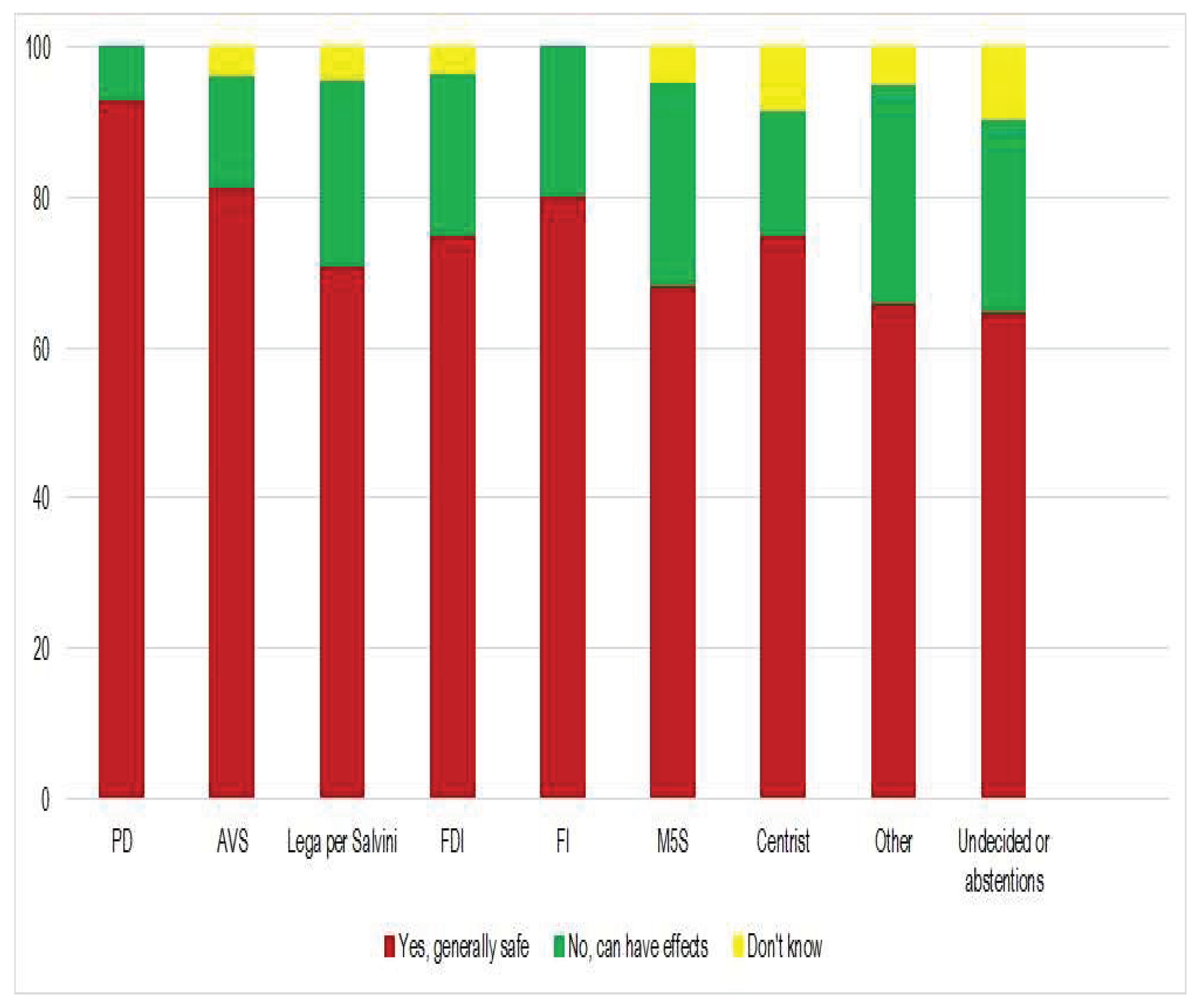
When it comes to trust in vaccines, nearly 3 out of 4 (73.1%) respondents believe that childhood vaccines are a safe health tool. A graphical representation is illustrated in Figure 5. As illustrated in the figure, 93.0% of PD and 81.5%, AVS voters responded that childhood vaccines are a safe health tool versus 71.0% of League for Salvini and 68.2% of M5S. Noteworthy, is the high percentage of undecided at the question “Yes, they are generally safe” the raw data are reported in tables 12 and 12.2.
In Table 12 the answers are reported in terms of demographic variables. The feeling of greater “insecurity” is perceived by mothers (23.8%), those with children aged 2 to 6 (25.3%) and those living in the north-east (27.1%). The perception of the safety of pediatric vaccines is very high among those with children aged up to 2 years (83.2%), i.e., those who have recently come into contact with the world of pediatric vaccination.
Respondents were then asked to agree or disagree with a statement about the danger or otherwise of vaccines: 70.7% of the sample disagree that “childhood vaccines are more dangerous than the diseases they target”, while just over 1 in 4 parents (27.4%) believe the opposite.
Those most in favor are men, those aged between 45 and 64, those with children under the age of 2 and those living in the south and the islands. The data are reported in tables 13 and 13.2. Once again, there are polarized responses when it comes to political orientation. In table excel 13.2 is clear that the PD voters who agree with the question “Pediatric vaccines are more dangerous than the diseases to which they are directed”” are less than a quarter of League voters, the answers being 11.9 and 46.4 respectively.
To minimize response bias caused by distortions due to untruthful responses, we looked at the 2023 (last updating) national vaccination coverage (VC) to see if these were consistent with the survey data (15). Polio coverage (IPV), used as a proxy for hexavalent vaccination (diphtheria, tetanus, whooping cough, hepatitis B, polio, and disease caused by Haemophilus influenzae type b) was 98%. MPR (measles-mumps-rubella) first dose 95%, second dose 85%. Of note, regarding the second dose, MPR has been mandatory in Italy since 2017 and the second dose is given at 5-6 years of age, so not all children will have reached 5-6 years of age in 2023. This table places Italy among the top three countries with the highest rates of childhood vaccination.
All the excel tables are uploaded in the repository at: https://zenodo.org/records/15512208
DISCUSSION
The results of this study are highly relevant in the context of the ongoing political and public debate about children mandatory vaccination, what vaccine knowledge parents have and what aspects are uncertain. Most published survey studies focus on the analysis of vaccine hesitancy. as confirmed by the high number of studies and questionnaires found in the literature on the matter (11). They draw attention to the fact that the concept of VH is a broad one and has been described and applied in somewhat inconsistent ways. (https://www.nature.com/articles/s41562-022-01431-6). Some other studies also focus on the development of practical tools to better estimate vaccine hesitancy (12). Other surveys attempt to monitor the decline in vaccine confidence compared to previous years (13). Instead, the focus of our study is the level of awareness and quality of information that parents receive.
Italian Public Services and Health Authorities run information campaigns to encourage parents to vaccinate their children, in accordance with the schedule of the ten compulsory and 4 recommended vaccines established in the national PNPV (14)
Italy is among the country with the highest children vaccination rate. A recent report (2023) on 21 countries for children under 6 showed that Italy had the highest percentage of fully vaccination (83.6%), United Kingdom had 75.8%, Indonesia the lowest (47.6%) (15).
An analysis of the data of the survey discussed in this article reveals a scenario characterized by a lack of clarity and a certain degree of confusion, which would not be expected among the families of children and adolescents who are the protagonists of pediatric vaccination. In an earlier survey, published in 2014 (unpublished data). and commissioned by a pharmaceutical company (Sanofi), it was found that the positions of parents differed significantly in terms of information channels they consulted, although, it seems to us that the percentages are not so different. In fact, about 51% of parents belonging to the group of supporters prefer to consult institutional sites and specialized or scientific sites (see discussion below). Critics, defined as “holistic”, rely in 50.0% of cases on the information available in forums and blogs. However, no raw data is available to support our observation. Furthermore, the political position of the parents was not explored in the former 2014 survey. Indeed, our survey shows a strong ideological connotation as respect to vaccine culture. Italy has 10 compulsory vaccinations which is the highest level in comparison with other European countries, and is among the three countries with the highest obligation rate (13 for Lithuania, 11 for France, 10 for Italy). Seventeen European countries do not have any mandatory vaccinations, Germany and Belgium have only one mandatory vaccination. Thus suggesting, as pointed out from Institutional information itself, that the governmental choice is a political choice.
The analysis of the results of the survey commissioned by AsSIS shows that the vaccination obligation is highly supported by the respondents, in fact more than 90% believe that it is beneficial for their children, and these data are in line with the national vaccination coverage updated in 2023. Noteworthy, the survey highlighted some critical issues in the three objectives it set itself: Knowledge, Perceptions and Concerns; these critical issues point to a lack of knowledge that undermines informed and responsible choice among a significant proportion of the population. From the critical reading of official information (vaccinal calendar, ministry of health dedicated portal (5) it seems that do little to spark deliberation but to increase blind trust. As pointed out by Tom Beauchamp’s A History and Theory of Informed Consent, the deliberative consent should include “understanding (of all important information), no control (freedom from coercion) and intentionality” (16).
Despite the high value of respondents in favor of obligations, a certain misinformation was observed among them regarding several issues. One of this issue concerns the answer to the benefit of vaccines for the community. The health of the community assumes that vaccines are highly immunizing and that the absolute risk-benefit ratio (ARR) is in favor of vaccinations (for discussion about absolute and relative risk see below). However at least 8 of the current compulsory pediatric vaccines do not lead to herd immunity i.e., the condition to allow an infectious disease eradication. A dedicated references are reported in “supplemental references”. In this survey a concept of herd immunity is perceived by respondents as homogeneous between the different vaccines, with the consequent belief that compulsory vaccination is a value for the society for all these products. Indeed, 86.5% of parents believe that vaccination is essential for the health of the community; 24.7% also want the currently recommended childhood vaccinations to be made compulsory. One of the origins of these beliefs is the fact that products with different pharmacological and clinical profiles are grouped together in the same category. Some generic statements in institutional documents also contribute to this general and imprecise perception, such as PNPV 2023-2025 statement: “All countries recognize vaccination as a priority” or “Vaccines have great value from a human, ethical and social point of view” (PNPV 2023-2025 - 20 March 2023 - Update of the National Vaccination Prevention Plan - Integration of the National Prevention Plan 2020-2025).
A fragmented perception of the risk-benefit ratio of different vaccines is also observed in this survey, 70.7% of the sample disagree that “childhood vaccines are more dangerous than the diseases they target”, while over 1 in 4 parents (27.4%) believe the opposite. Moreover, 24.7% would also like to see currently recommended childhood vaccinations made compulsory. Contributing to this lack of uniformity of judgement is the absence of information on the absolute risk reduction (ARR) for each product in most scientific publications and communications to the public where, conversely, the relative risk is provided. This contrasts with the requirement of FDA which states “Provide absolute risks, not just relative risks. Patients are unduly influenced when risk information is presented using a relative risk approach; this can lead to sub-optimal decisions. Therefore, an absolute risk format should be used” (FDA Communicating Risks and Benefits: An Evidence-Based User’s Guide - August 2011).
This survey also evidences a partial knowledge of the topics covered by the investigation. For example, to the question “From what you know, what are the MANDATORY pediatric vaccinations in Italy? MULTIPLE ANSWERS ALLOWED” less than 50% know how to answer correctly. There are mandatory vaccinations such as anti-measles and anti-rubella which are incorrectly recognized as recommended by 21.0% and 20.3% respectively with a maximum of 29,4 %. The inability to access monovalent vaccines nationwide, probably contributes to this inaccuracy; the use of polyvalent formulations (hexavalent and tetravalent or trivalent) leads to an unclear perception of the number of vaccines and doses to be administered for each subject. Even more disinformation is evident when the question regarded recommended vaccination as for example the case of the Anti-meningococcal B and C where more than 25% of respondents believed them compulsory, while they are recommended.
Responses based on political orientation revealed even more fragmentation, for example the response to the question Do you consider childhood vaccines to be a safe health tool 93% of the Italian Democratic Party (PD) versus 74.9% of the Fratelli d’ Italia (FdI) a national conservative political party consider pediatric vaccines a safe health tool. This fragmentation is an expression of how information is somehow conditioned by ideological-electoral issues rather than a serious biomedical and pharmacological approach. This observation has also been reported in other national surveys whose results suggest that most parents, including the vaccinating majority, are susceptible to vaccine messages from political and medical leaders (17).
A great deal of unawareness of the provisions of other European States on vaccination obligations is also shown from respondents, more than 60% with a peak 81.1 % % of PD voters think that obligations are the same in most European countries. Only 16.1% correctly responded that almost all European states have fewer or no obligations at all.
After all, a detailed look at the information in the PNPV (18) reveals that the recommendations issued by institutions and scientific societies are more reassuring than informative. They explicitly report the benefits of a certain treatment while minimizing the risks; the various citations appearing in these documents refer only to research that proves a priori thesis by excluding what does not conform to it. Instead, one of the main keys to be effective, compulsory programs must have a reliable supply of safe and effective vaccines (19). Furthermore, because children’s vaccines are compulsory and because state law requisite for children is to be vaccinated before being admitted to daycare and school, it is essential that safety concerns be fully and carefully studied.
Despite the current assumption that social media is becoming the main source of health news and information, most parents still rely on traditional media, official government websites and health professionals for information about vaccines (20).
However, we noticed that the official channels sometimes underestimated the risk of the occurrence of adverse events. For example, the official channels of the Italian Ministry of Health and even the FAC portal lack information, on reliable scientific literature, which raises serious concerns in several respects. Moreover, based on an Italian survey on the beliefs of public health professionals as respect of mandatory vaccines, there is no mention of the risks of adverse events concerns, risk-benefit ratio or side effects (21).
CONCLUSIONS
In conclusion, the survey highlights an oscillation between two antithetical positions, a mistrust of vaccine (hesitancy) contrasted with a blind trust of vaccine (promptness). The data shows a great deal of misinformation revealing that the information provided to the population is not commensurate with the importance of the issue; to use a scientific term, we could speak of a lack of “herd knowledge”, which, similarly to some vaccines, should reach at least 90% correct answers to be functional.
The public’s opinion is based on two key entities, health professionals and the media. As both are subject to the attention of the industry, which benefits from their decisions and behavior, the authors believe that until conflicts of interest between these subjects are excluded, it will not be possible to achieve an adequate level of objectivity, i.e., the “herd knowledge” that supports a conscious and responsible choice, as the law would require when it imposes “informed consent”. Another concern is “regulatory capture”, where the industries or interests dominate regulators, they are supposed to regulate, rather than by the public interest. With this survey, we would like to encourage the provision of accurate information based on serious and thorough scientific work and valid clinical trials, result of a rediscovered honest scientific dialectic, an essential prerequisite for something that wants to be defined as “Science”. To address the current situation, we propose a structured approach that includes a transparent, independent information portal reporting on clinical trials. This portal would explain the use of each vaccine in a clear and professional way, share personal experiences and work with associations to widen reach. We also call for active pharmacovigilance. Italy urgently needs this online platform to consolidate these efforts and serve as a hub for independent research, free from the influence of the pharmaceutical industry.
Funding
The work was financially supported by the AsSIS association. AsSIS is a not-for-profit association financed exclusively by the subscriptions of its members and by voluntary contributions of “5 per thousand” (part of the IRPEF tax that the Italian State distributes to non-profit organizations registered with the Revenue Agency) as indicated by citizen-taxpayer.
Acknowledgements
The authors thank Dr Rossitza Toneva for critical reading of the manuscript. The author also thank Ing Matteo Manganelli, Dr Alessia Zurlini for the artwork and Dr Valeria Bianchi, Sergio Segantini for technical assistance.
Conflict of Interest
The authors declare no conflict of interest of any kind.
References
- CDC Recommended Schedules. Available online: https://www.immunize.org/official-guidance/cdc/rec-schedules/ (accessed on 27, April, 2025).
- https://www.gazzettaufficiale.it/eli/gu/2017/08/05/182/sg/pdf.
- https://www.aslroma2.it/attachments/article/311/Legge%20n.119%20del%2031%20luglio%202017.
- Piano Nazionale Prevenzione Vaccinale 2023 – 2025. Available online: https://www.cirinet.it/index.php/news/piano-nazionale-prevenzione-vaccinale-2023-2025/#:~:text=Il%20Piano%20Nazionale%20Prevenzione%20vaccinale,sicuri%20e%20accessibili%20nel%20tempo. (accessed on 27, April, 2025).
- https://www.salute.gov.it/new/it/tema/vaccinazioni/.
- European Vaccination Information Portal. Available online: https://vaccination-info.europa.eu/en/about-vaccines/when-vaccinate/vaccination-schedules-eueea.. (accessed on 27, April, 2025).
- EUROMEDIA research. Available on line: https://www.euromediaresearch.it/ (accessed on 27, April, 2025).
- CAWI Methodology – Computer Assisted Web Interview. Available online https://www.idsurvey.com/en/cawi-methodology/ (accessed on 27, April, 2025).
- https://ednh.news/it/vaccini-ecco-la-mappa-di-quelli-obbligatori-nellue/ (accessed on 27, April, 2025).
- https://en.wikipedia.org/wiki/List_of_political_parties_in_Italy (accessed on 27, April, 2025).
- https://pmc.ncbi.nlm.nih.gov/articles/PMC7595070/.
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11834527/.
- https://pubmed.ncbi.nlm.nih.gov/38216441/.
- Carta italiana per la promozione delle vaccinazioni. Available on line:.
- https://www.epicentro.iss.it/vaccini/pdf/Carta_ita_promo_vaccinazioni_highres.pdf (accessed on 27, April, 2025).
- Italy_insight_report.pdf.
- https://pmc.ncbi.nlm.nih.gov/articles/PMC11834450/#cit0001.
- Influence of political and medical leaders on parental perception of vaccination: a cross-sectional survey in Australia - PMC.
- https://www.epicentro.iss.it/vaccini/piano-nazionale-vaccini-2023-2025.
- https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(06)68144-0/abstract).
- PLoS Curr. 2017 Mar 3;9: ecurrents.outbreaks.0561a011117a1d1f9596e24949e8690b. [CrossRef]
- https://sfera.unife.it/retrieve/36fcc6ce-18f2-4759-883a-0d109a43adff/Pitini_Italian_2020.pdf. https://riviste.unimi.it/index.php/ebph/article/view/20862.
Figure 1.
Definition of the interviewed sample based on years and gender (panel A), and the geographical area of the respondents (panel B).
Figure 1.
Definition of the interviewed sample based on years and gender (panel A), and the geographical area of the respondents (panel B).
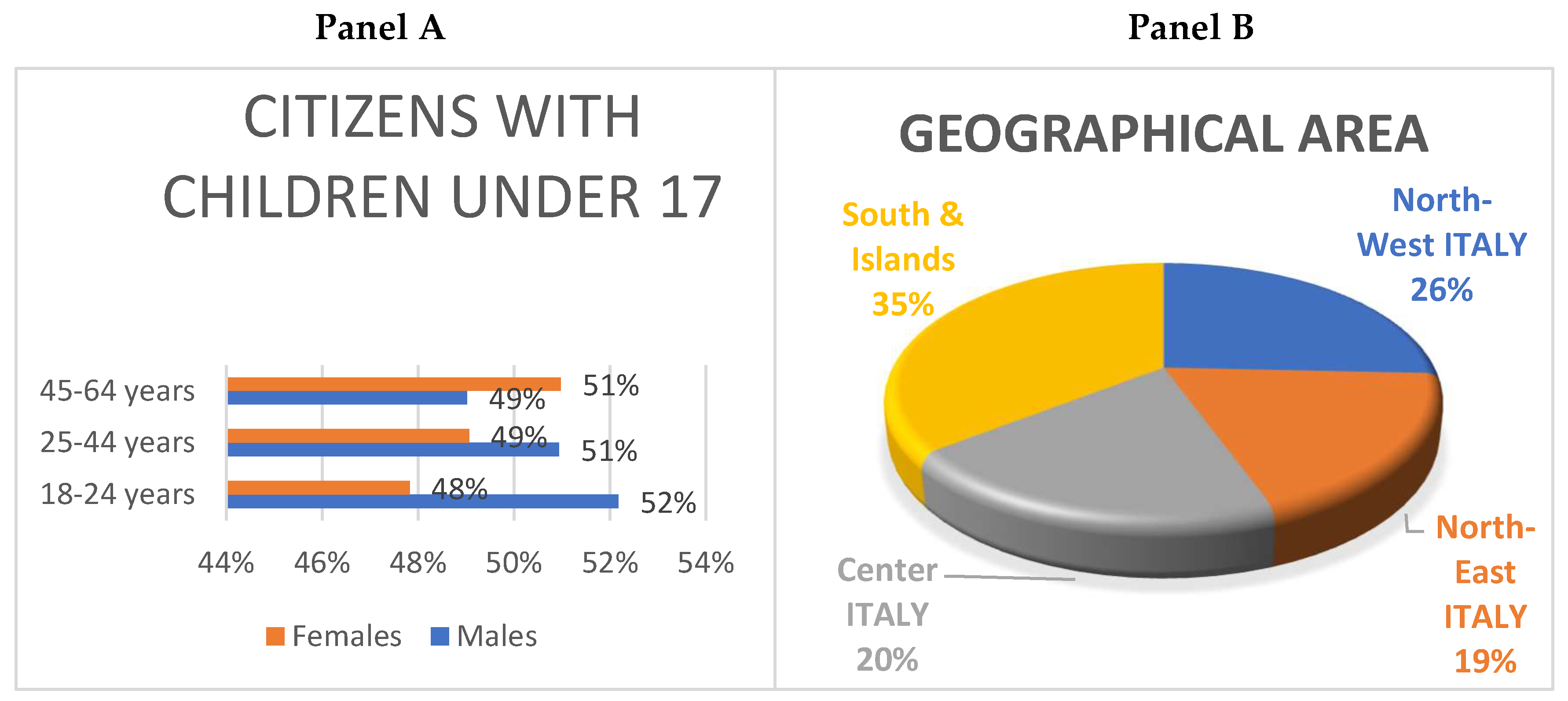
Figure 2.
This graph shows the percentage of respondents who expressed a high (dark green) or moderate (light green) level of consensus, compared to those who expressed a low (yellow) level of consensus or indicated that they did not know (red). There is not much difference in the answers according to the sex and age of the parents, or the age of their child (see Tables 1 and 2). Panel A is for children’s health and Panel B is for community health.
Figure 2.
This graph shows the percentage of respondents who expressed a high (dark green) or moderate (light green) level of consensus, compared to those who expressed a low (yellow) level of consensus or indicated that they did not know (red). There is not much difference in the answers according to the sex and age of the parents, or the age of their child (see Tables 1 and 2). Panel A is for children’s health and Panel B is for community health.
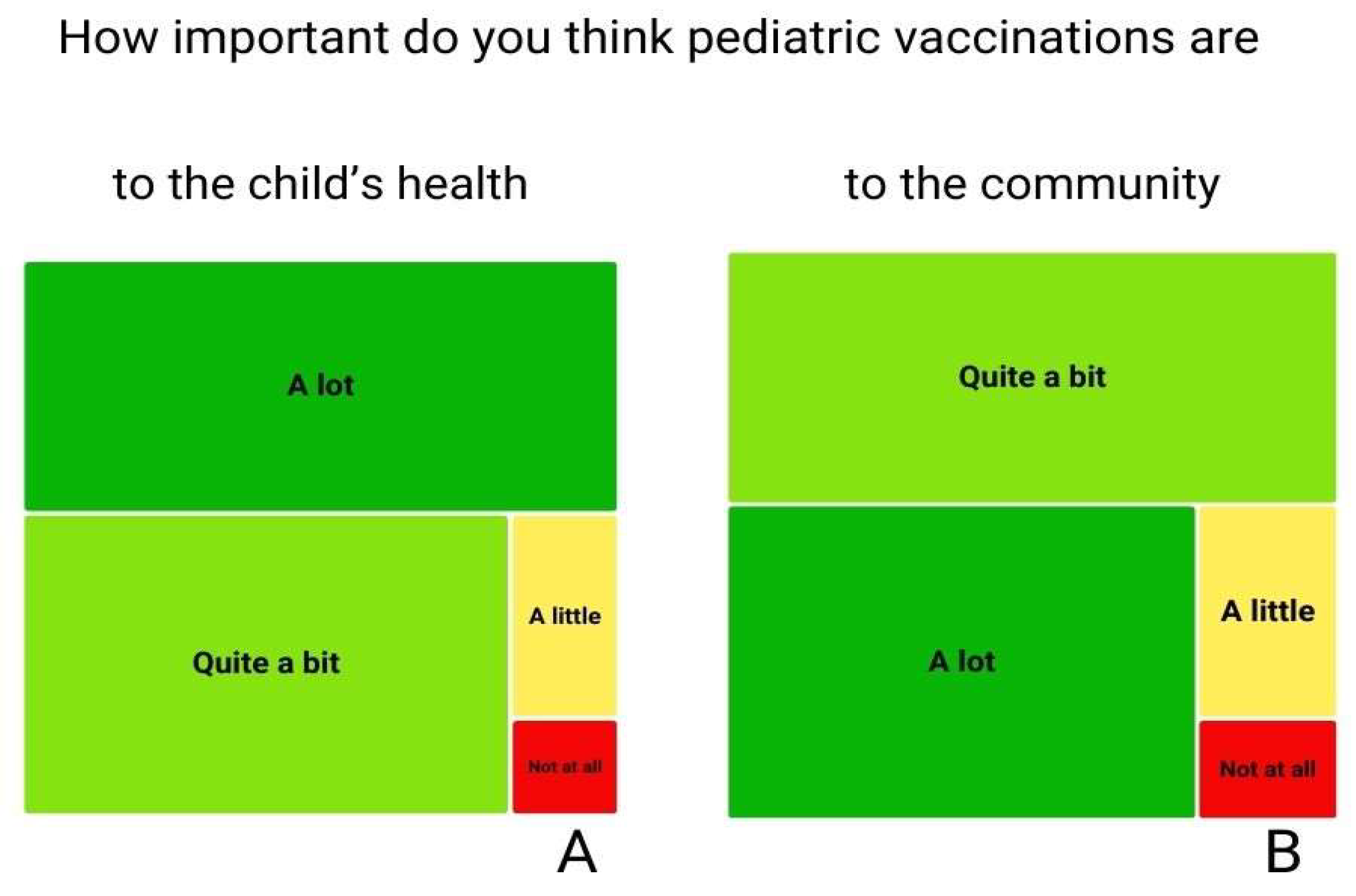
Figure 3.
This figure shows the differences in consensus according to political orientation. Those expressing consensus are shown in red and orange, those expressing little or no consensus in green, and those unsure of their answer in yellow. Panel A is for children’s health and Panel B is for community health. For comprehensive information on Italian parties, see reference (10). The detailed answers are reported in supplemental data in tables 1.2 and 2.2.
Figure 3.
This figure shows the differences in consensus according to political orientation. Those expressing consensus are shown in red and orange, those expressing little or no consensus in green, and those unsure of their answer in yellow. Panel A is for children’s health and Panel B is for community health. For comprehensive information on Italian parties, see reference (10). The detailed answers are reported in supplemental data in tables 1.2 and 2.2.
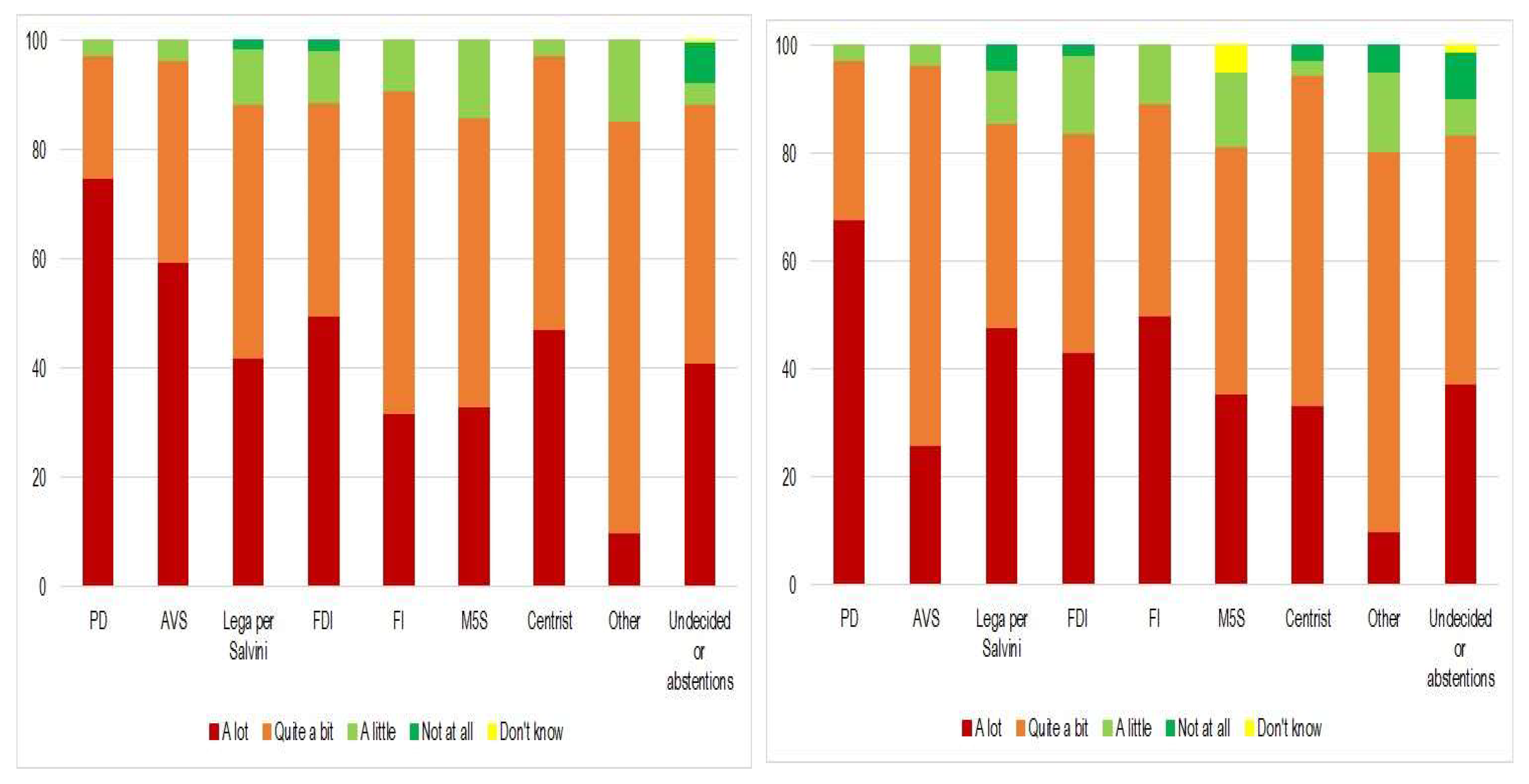
Figure 4.
The figure shows that 74.0% of responses were in favor of compulsory vaccination against certain diseases for children under sixteen, 49.3% were in favor only of vaccinations currently required by law, 24.7 want childhood vaccinations currently recommended to be made compulsory (Panel A).
Figure 4.
The figure shows that 74.0% of responses were in favor of compulsory vaccination against certain diseases for children under sixteen, 49.3% were in favor only of vaccinations currently required by law, 24.7 want childhood vaccinations currently recommended to be made compulsory (Panel A).
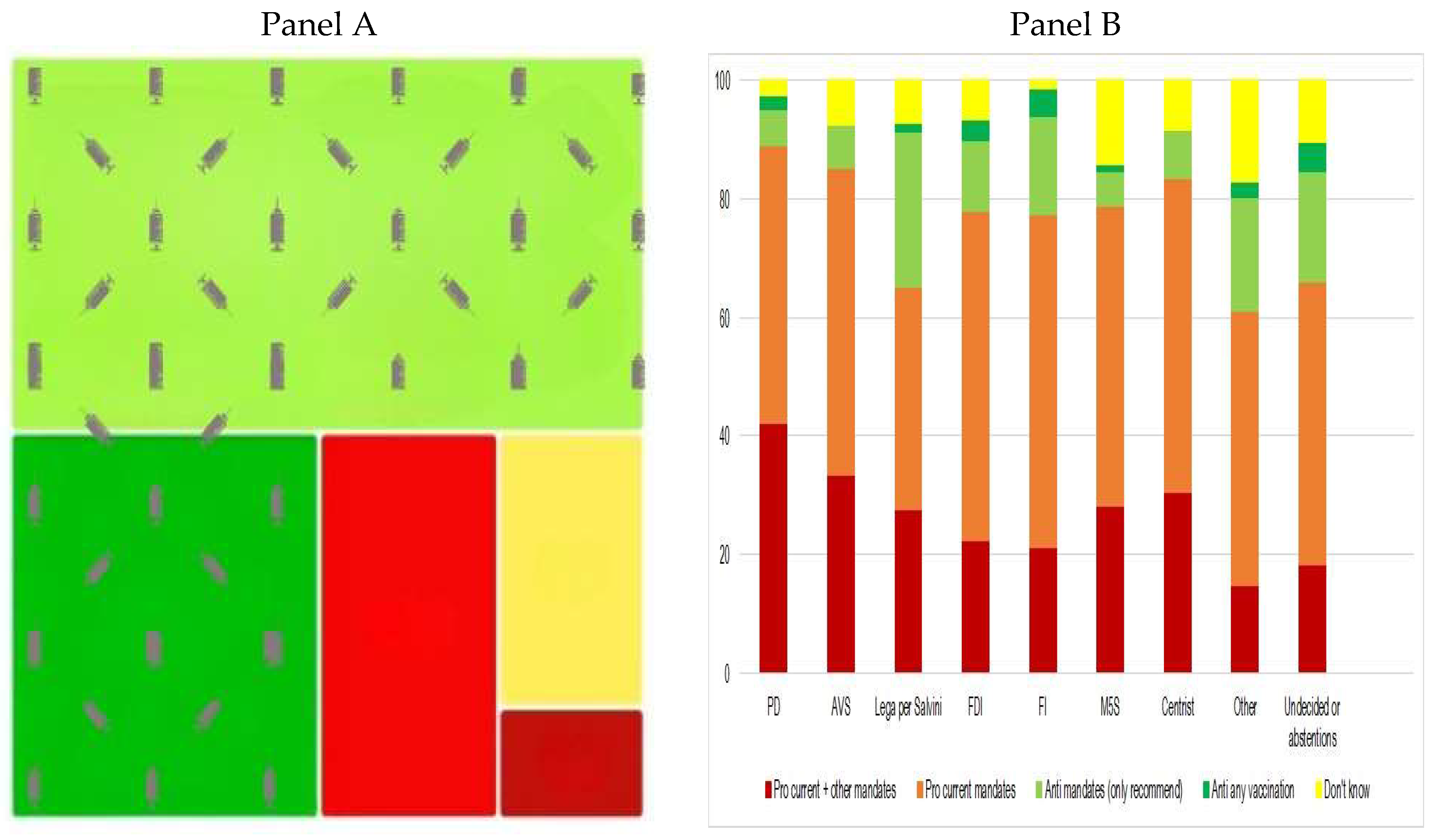
Figure 5.
Graphical representation of the parents truth on safety of the childhood vaccines based on the political orientation, Namely, 93.0% of PD and 81.5%, AVS voters, 71.0% of League for Salvini and 68.2% of M5S and 65 % of other parties voters state that are a safe health tool.
Figure 5.
Graphical representation of the parents truth on safety of the childhood vaccines based on the political orientation, Namely, 93.0% of PD and 81.5%, AVS voters, 71.0% of League for Salvini and 68.2% of M5S and 65 % of other parties voters state that are a safe health tool.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



