
Submitted:
29 May 2025
Posted:
30 May 2025
You are already at the latest version
Abstract
Inflammatory Bowel Disease (IBD), encompassing Crohn’s disease and ulcerative colitis, is a chronic condition characterized by immune dysregulation, gut microbiota alterations, and persistent intestinal inflammation. While pharmacological treatments remain the cornerstone of management, growing evidence suggests that diet plays a crucial role in disease modulation. Specific dietary components have been implicated in either exacerbating or alleviating symptoms, potentially influencing disease progression. Understanding the complex interactions between food, gut microbiota, and immune responses is essential for optimizing dietary recommendations in IBD. Recent clinical and mechanistic studies have explored the impact of various dietary patterns, macronutrients, and bioactive compounds on inflammation and gut homeostasis. However, conflicting findings and individual variability highlight the challenges in establishing universal dietary guidelines. Emerging evidence also supports the role of personalized nutrition and elimination diets in improving patient outcomes. Despite progress, gaps remain in translating dietary interventions into clinical practice, necessitating further high-quality research. This review synthesizes current knowledge on the interplay between diet and IBD pathophysiology, focusing on the latest clinical data and mechanistic insights. By bridging research findings with clinical applications, this work aims to provide a comprehensive understanding of the potential role of nutrition in managing IBD.
Keywords:
inflammatory bowel disease nutrition
; Crohn’s disease
; ulcerative colitis
; gut microbiome
; dietary recommendation
Introduction
Inflammatory Bowel Disease (IBD) is a chronic, immune-mediated disorder of the gastrointestinal (GI) tract, encompassing two major conditions: Crohn’s disease (CD) and ulcerative colitis (UC). Both conditions are characterized by periods of exacerbation and remission, significantly impacting patients' quality of life [1]. Despite similarities, CD and UC have distinct pathophysiological features and clinical presentations. CD can affect any part of the digestive tract from the mouth to the anus but most commonly involves the terminal ileum and colon. It is distinguished by transmural inflammation, which can lead to complications such as strictures, fistulas, and abscess formation [2]. In contrast, UC is confined to the colon and rectum, with inflammation limited to the mucosal layer. The disease typically progresses in a continuous manner from the rectum proximally, often presenting with symptoms such as bloody diarrhea and abdominal discomfort [2]. The exact etiology of IBD remains unclear, though it is widely recognized as a multifactorial disease resulting from a complex interplay between genetic predisposition, environmental triggers, gut microbiota alterations, and immune dysregulation [3,4].
Advances in research have highlighted the critical role of diet in modulating gut inflammation, either exacerbating or alleviating symptoms, making dietary management an essential component of IBD treatment strategies [5]. While IBD is primarily an immune-mediated disorder, emerging evidence suggests that dietary components significantly influence gut inflammation, the intestinal microbiota, and disease progression [6]. Patients with IBD often perceive diet as a major factor in their disease and frequently seek dietary modifications to alleviate symptoms [7]. Research indicates that certain dietary patterns, such as the Western diet, which is high in saturated fats, processed foods, and refined sugars, are associated with increased IBD risk and disease flares [8]. Conversely, diets rich in fiber, omega-3 fatty acids, and polyphenols may have protective effects by promoting a healthy gut microbiome and reducing inflammation [9]. Exclusive enteral nutrition (EEN) has also been shown to induce remission in pediatric CD, highlighting the potential of targeted dietary interventions [10]. Despite the increasing recognition of diet as a modifiable factor in IBD management, standardized dietary guidelines remain limited. A multidisciplinary approach, involving dietitians and gastroenterologists, is essential to develop personalized nutrition plans that address individual dietary triggers, nutritional deficiencies, and patient preferences [11].
This review aims to explore the role of diet in IBD by examining its impact on gut microbiota, mucosal integrity, and immune responses. It will synthesize clinical evidence on dietary interventions, highlighting foods that may exacerbate or alleviate symptoms. Additionally, the review will evaluate the efficacy of specific diets, such as the Mediterranean diet and EEN, in disease management. By identifying gaps in current research and emphasizing the need for personalized nutrition strategies, this review seeks to bridge the gap between scientific findings and clinical applications, ultimately improving dietary recommendations for IBD patients.
Pathophysiology of IBD and Dietary Interactions
Role of Gut Microbiota and Dysbiosis
The gut microbiota plays a fundamental role in maintaining intestinal homeostasis and immune regulation (Table 1) [12]. In IBD, dysbiosis—an imbalance in the composition and function of gut microorganisms—has been identified as a key factor contributing to chronic intestinal inflammation [13]. Dysbiosis in IBD is characterized by a reduction in microbial diversity and an imbalance between protective and pathogenic bacteria. Studies have consistently reported a decrease in beneficial bacteria such as Firmicutes and Bacteroidetes and an expansion of pro-inflammatory taxa, particularly Proteobacteria and Enterobacteriaceae [14]. This microbial shift leads to increased production of inflammatory mediators and impairs the gut barrier, allowing microbial antigens to trigger aberrant immune responses [15]. A dysfunctional gut microbiome also affects the production of key microbial metabolites, such as short-chain fatty acids (SCFAs), which play an anti-inflammatory role in gut health. In IBD, there is a notable reduction in SCFA-producing bacteria, leading to compromised intestinal barrier integrity and heightened immune activation [16]. Moreover, alterations in bacterial metabolites disrupt regulatory T-cell functions, further exacerbating inflammation [17]. Given the strong association between dysbiosis and IBD, therapeutic strategies targeting the gut microbiota have gained attention. Approaches such as probiotics, prebiotics, fecal microbiota transplantation (FMT), and dietary modifications have shown promise in restoring microbial balance and improving disease outcomes [18].
Intestinal Barrier Dysfunction and Immune Activation
The intestinal barrier plays a crucial role in maintaining gut homeostasis by regulating the selective absorption of nutrients while preventing the entry of harmful pathogens and antigens. In IBD, this barrier becomes compromised, leading to increased intestinal permeability, which facilitates the translocation of microbial products and triggers immune activation [19]. Intestinal barrier dysfunction in IBD is characterized by alterations in tight junction proteins, increased apoptosis of epithelial cells, and heightened immune responses. Tumor necrosis factor-alpha (TNF-α) and interleukin (IL)-13 have been identified as key cytokines responsible for disrupting epithelial integrity, contributing to increased permeability and inflammation (Figure 1). Studies in experimental colitis models have demonstrated that targeted epithelial dysfunction alone can induce mucosal immune activation, indicating that barrier disruption is a primary contributor to disease pathogenesis rather than a secondary consequence of inflammation [20]. The interaction between a weakened intestinal barrier and the immune system creates a self-perpetuating cycle of inflammation. The increased permeability allows luminal antigens to enter the mucosa, activating innate immune responses, including macrophages and dendritic cells, which in turn promote the production of pro-inflammatory cytokines such as interferon-gamma (IFN-γ) and TNF-α [21]. This immune activation exacerbates epithelial damage, leading to a chronic inflammatory state that drives disease progression. Therapeutic strategies aimed at restoring intestinal barrier integrity are gaining attention as potential treatments for IBD. Experimental studies have shown that activation of the pregnane X receptor (PXR) can attenuate barrier dysfunction by reducing cytokine-induced myosin light-chain kinase (MLCK) expression, thereby stabilizing tight junction proteins [22]. Additionally, interventions such as probiotics, dietary modifications, and prebiotic supplementation have shown promise in modulating gut barrier function and reducing inflammation.
Impact of Diet on Inflammatory Pathways
Diet plays a significant role in modulating inflammation in IBD by influencing immune responses, gut microbiota composition, and epithelial barrier integrity. The Western diet, characterized by high fat, refined sugar, and low fiber, has been linked to increased intestinal inflammation and disease progression. In contrast, fiber-rich and anti-inflammatory diets have demonstrated protective effects by reducing pro-inflammatory cytokine production and maintaining gut homeostasis [23]. High-fat diets, particularly those rich in saturated and trans fats, can promote gut inflammation by altering the microbiome and increasing intestinal permeability. Studies have shown that excessive dietary fat stimulates the release of pro-inflammatory cytokines such as TNF-α and IL-6, which exacerbate mucosal inflammation [24]. Additionally, a high-fat diet promotes dysbiosis by increasing the abundance of Proteobacteria, a bacterial phylum associated with inflammation, while reducing beneficial Firmicutes species that produce anti-inflammatory metabolites like SCFAs [25]. Similarly, diets high in refined sugar have been associated with increased intestinal permeability and endotoxemia, leading to heightened immune activation. Simple carbohydrates can fuel pathogenic gut bacteria and reduce microbial diversity, contributing to a pro-inflammatory gut environment [26]. Moreover, high-sugar intake has been linked to reduced mucin production in the gut lining, which weakens the protective mucus barrier and makes the intestine more susceptible to bacterial invasion and inflammation [27].
In contrast, fiber-rich diets have been shown to have protective effects against IBD by promoting gut barrier integrity and fostering the growth of beneficial bacteria that produce SCFAs, such as Faecalibacterium prausnitzii [28]. SCFAs, including butyrate and propionate, have anti-inflammatory properties, reducing cytokine production and strengthening tight junctions in the intestinal epithelium. Diets emphasizing whole foods, such as the Mediterranean diet and anti-inflammatory diets like the Inflammatory Bowel Disease Anti-Inflammatory Diet (IBD-AID), have demonstrated effectiveness in reducing inflammatory markers and improving clinical symptoms [28,29]. Furthermore, polyphenol-rich foods such as berries, green tea, and turmeric have shown potential in modulating immune responses and reducing oxidative stress in IBD patients. These bioactive compounds inhibit nuclear factor-kappa B (NF-κB) signaling, a key pathway in inflammatory responses, thereby reducing the secretion of pro-inflammatory cytokines [30]. Omega-3 fatty acids, found in fatty fish and flaxseeds, also exhibit anti-inflammatory effects by modulating eicosanoid pathways and reducing the production of pro-inflammatory prostaglandins and leukotrienes [31].
Foods to Avoid in IBD: Mechanistic and Clinical Evidence
Ultra-Processed Foods & Additives
The consumption of ultra-processed foods (UPFs) has been strongly linked to the rising incidence of IBD. UPFs are defined as industrially manufactured foods that contain additives such as emulsifiers, artificial sweeteners, preservatives, and colorants, which enhance texture, flavor, and shelf life. While these additives are considered safe for the general population, accumulating evidence suggests that they may contribute to intestinal inflammation and IBD pathogenesis [32]. Several mechanisms have been proposed to explain the role of UPFs in IBD. One key factor is the disruption of gut microbiota. Studies have shown that food additives such as emulsifiers (e.g., carboxymethylcellulose and polysorbate-80) alter gut microbiota composition, reducing beneficial bacteria such as Faecalibacterium prausnitzii and promoting the growth of pro-inflammatory species like Proteobacteria [33]. This dysbiosis weakens the gut barrier, leading to increased intestinal permeability, a hallmark feature of IBD pathogenesis. Additionally, artificial sweeteners such as aspartame and sucralose have been found to impair gut immune responses and promote oxidative stress. Emulsifiers and preservatives, commonly found in UPFs, enhance bacterial translocation across the intestinal epithelium, triggering immune activation and chronic inflammation [34].
Epidemiological studies have consistently demonstrated a strong association between high UPF consumption and an increased risk of IBD. A large-scale prospective cohort study across 21 countries found that individuals who consumed five or more servings of UPFs per day had an 82% higher risk of developing IBD compared to those consuming fewer than one serving per day [35]. Another cross-sectional study reported that patients with active IBD had significantly higher UPF consumption compared to those in remission [36]. A systematic review and meta-analysis involving over 4 million participants revealed that high UPF intake was particularly associated with an increased risk of CD, rather than UC [37]. This suggests that dietary factors may have a stronger influence on CD pathogenesis, potentially due to differences in immune responses and microbiota composition.
High-Fat Diets
Dietary fat composition significantly influences gut inflammation, and a high-fat diet (HFD) has been implicated in the pathogenesis and exacerbation of IBD. Several studies have demonstrated that diets rich in saturated and trans fats promote intestinal dysbiosis, increase intestinal permeability, and enhance inflammatory responses, contributing to disease progression [38]. A HFD disrupts gut microbiota composition by favoring the growth of pro-inflammatory bacteria while reducing beneficial species. Notably, studies have identified an overgrowth of Bilophila wadsworthia, a sulfide-producing bacterium that exacerbates gut inflammation, in response to high saturated fat intake [39]. Additionally, HFD-induced dysbiosis has been linked to increased intestinal permeability, allowing luminal antigens to penetrate the gut epithelium and activate immune responses [40]. HFDs also trigger oxidative stress and pro-inflammatory cytokine production in the gut. For instance, studies have shown that HFD feeding leads to excessive reactive oxygen species (ROS) production, which damages intestinal epithelial cells and enhances local inflammation [41]. Moreover, an HFD activates MLCK, which regulates tight junction proteins, thereby increasing intestinal permeability and immune system activation [42].
Several epidemiological and experimental studies have provided compelling evidence linking HFDs to IBD progression. A study in genetically susceptible Mdr1a(-/-) mice demonstrated that HFD-induced obesity exacerbates colitis, highlighting the interaction between diet, genetic predisposition, and inflammatory responses [40]. Additionally, an experimental study found that short-term HFD feeding prior to colitis induction resulted in severe inflammation, increased gut permeability, and higher levels of pro-inflammatory cytokines [43]. These findings suggest that even brief exposure to HFD can prime the gut for inflammation, predisposing individuals to IBD flares.
Red and Processed Meats
Red and processed meats have been increasingly implicated in the pathogenesis and progression of IBD. These foods contain high levels of saturated fats, heme iron, and food additives, which can promote gut inflammation and dysbiosis. Several epidemiological and experimental studies suggest that frequent consumption of red and processed meats is associated with an increased risk of IBD onset and worsened disease outcomes [44]. The inflammatory potential of red and processed meats is attributed to multiple factors. One of the primary concerns is the high heme iron content in red meat, which promotes oxidative stress and the formation of cytotoxic compounds such as N-nitroso compounds (NOCs). These compounds have been shown to impair the intestinal barrier and contribute to inflammation in experimental colitis models [45]. Additionally, processed meats often contain preservatives, emulsifiers, and artificial additives, which can disrupt gut microbiota and increase intestinal permeability [35]. Moreover, high-fat content in red meat contributes to pro-inflammatory cytokine production, particularly TNF-α and IL-6, which play central roles in IBD pathogenesis. A study in mice demonstrated that high red meat intake led to intestinal dysbiosis, an increase in pathogenic bacteria such as Bacteroides and Alistipes, and a decline in beneficial bacteria like Faecalibacterium [45]. These changes were accompanied by increased colonic inflammation and disrupted tight junction proteins, further contributing to disease severity.
Epidemiological studies have provided robust evidence linking red and processed meat intake to IBD. A large prospective cohort study from the European Prospective Investigation into Cancer and Nutrition (EPIC) found that high red meat consumption was associated with an increased risk of UC, but not CD [44]. Another cohort study analyzing over 5,763 IBD patients reported that frequent consumption of processed meat (>4 times per week) was linked to a significantly higher risk of mortality in CD patients, suggesting that these foods may worsen disease progression [46]. However, some conflicting findings exist. The Food and Crohn’s Disease Exacerbation Study (FACES), a randomized controlled trial, found no significant association between reduced red meat intake and CD relapse rates [47]. This suggests that while red and processed meats may influence disease risk and progression, other dietary and genetic factors likely play a role in IBD pathophysiology.
Dairy in Lactose-Intolerant Patients
Dairy consumption in IBD is a subject of debate, particularly in lactose-intolerant individuals. While dairy products are rich in calcium, vitamin D, and other essential nutrients, lactose intolerance can exacerbate gastrointestinal symptoms in some IBD patients. Lactose intolerance is more prevalent in patients with CD affecting the small intestine than in those with UC, as small bowel inflammation can lead to secondary lactase deficiency [48]. Lactose intolerance results from a deficiency in lactase, the enzyme responsible for breaking down lactose into glucose and galactose. In lactose-intolerant individuals, undigested lactose reaches the colon, where it is fermented by gut bacteria, producing gas and SCFAs. This process can lead to bloating, diarrhea, and abdominal pain, which overlap with IBD symptoms, making it challenging to differentiate between disease activity and food intolerance [49]. However, research indicates that lactose intolerance is not inherently more common in IBD patients than in the general population [50]. Beyond lactose, milk proteins, such as casein and whey, have been investigated for their potential role in gut inflammation. Some studies suggest that casein may increase intestinal permeability and promote inflammation in genetically susceptible individuals, though definitive evidence linking dairy proteins to IBD flares remains inconclusive [51].
The relationship between dairy consumption and IBD is complex. A large multinational study found that lactose intolerance and dairy sensitivity were more prevalent in IBD patients compared to non-IBD controls, but many patients avoided dairy unnecessarily due to misconceptions about its effects on their disease [52]. Similarly, a meta-analysis revealed that while lactose malabsorption was more common in CD patients with small bowel involvement, dairy foods may actually have protective effects against IBD development [53]. Another study on Arab adults found an inverse association between dairy consumption and IBD, suggesting that frequent dairy intake may reduce the risk of both CD and UC [54]. These findings challenge the notion that all IBD patients should avoid dairy and highlight the need for individualized dietary recommendations.
Gluten in Sensitive Individuals
Gluten, a protein found in wheat, barley, and rye, has been increasingly studied in relation to IBD. While celiac disease (CeD) is a well-defined autoimmune disorder triggered by gluten, non-celiac gluten sensitivity (NCGS) is a less understood condition in which individuals experience gastrointestinal and extraintestinal symptoms following gluten ingestion without the characteristic markers of CeD. Several studies suggest that a subset of IBD patients may have heightened sensitivity to gluten, leading to symptom exacerbation and potential immune activation [55]. The impact of gluten on IBD pathogenesis remains controversial, but several mechanisms have been proposed. Gluten ingestion has been shown to increase intestinal permeability, leading to heightened immune responses. In a mouse model of CD, gluten exposure was found to reduce regulatory T cells and cause ileitis, suggesting a direct pro-inflammatory effect [56]. Additionally, gluten can alter gut microbiota composition, which may contribute to dysbiosis and heightened immune activation in genetically susceptible individuals. Another potential mechanism involves wheat proteins beyond gluten, such as amylase-trypsin inhibitors (ATIs), which have been implicated in activating toll-like receptor 4 (TLR4)-mediated inflammation. This pathway has been suggested as a possible contributor to increased intestinal inflammation in CD [57].
Several studies have explored the prevalence of gluten sensitivity in IBD patients and the effects of a gluten-free diet (GFD). A study assessing 102 IBD patients found that approximately 27% of CD and UC patients reported gluten sensitivity, with symptoms including fatigue, bloating, and diarrhea. Furthermore, gluten sensitivity was associated with recent disease flares and stricturing disease in Crohn’s patients [58]. A large cohort study from the Crohn’s & Colitis Foundation of America (CCFA) Partners found that 19% of IBD patients had tried a GFD, with 65.6% reporting improved gastrointestinal symptoms and 38.3% experiencing fewer IBD flares. However, no definitive evidence supports a GFD as a primary treatment strategy for IBD, and benefits may be limited to those with concurrent NCGS [59]. Conversely, a prospective cohort study analyzing dietary gluten intake and IBD risk in over 200,000 participants found no significant association between gluten consumption and IBD onset [60]. This suggests that while some IBD patients may benefit from a GFD, gluten elimination may not be necessary for all individuals. Prohibited dietary components for IBD patients and their underlying immunomechanisms are listed in Table 2.
Foods Beneficial for IBD: Mechanistic and Clinical Evidence
Fiber & Prebiotics
Dietary fiber and prebiotics play a significant role in gut health, particularly in IBD. While fiber has historically been avoided by IBD patients due to concerns about symptom exacerbation, emerging evidence suggests that specific types of fiber and prebiotics can have anti-inflammatory effects by modulating gut microbiota and enhancing intestinal barrier function [61]. Dietary fiber exerts its beneficial effects primarily through fermentation by gut microbiota, producing SCFAs such as butyrate, acetate, and propionate. These metabolites promote mucosal healing, maintain intestinal barrier integrity, and regulate immune responses [62]. Butyrate, in particular, has been shown to inhibit nuclear factor-kappa B (NF-κB) signaling, a major inflammatory pathway in IBD, while also promoting the production of regulatory T cells that suppress excessive immune activation [63]. Prebiotics, a subset of dietary fiber found in foods such as bananas, onions, garlic, asparagus, and whole grains, selectively stimulate the growth of beneficial bacteria like Bifidobacterium and Lactobacillus, which play a role in reducing gut inflammation [64]. Additionally, resistant starch, a fermentable fiber present in foods like legumes and cooked-and-cooled potatoes, has been shown to increase SCFA production and support colonic health [65].
Despite the known benefits of fiber, IBD patients tend to consume inadequate amounts, often due to misconceptions about fiber exacerbating symptoms. A multicenter cross-sectional study found that only 38% of IBD patients met the recommended fiber intake, with prebiotic fiber consumption being particularly low [65]. Another study highlighted that fiber intake in pediatric IBD patients was significantly lower than in non-IBD controls, underscoring the need for dietary interventions to improve fiber consumption [64]. Experimental models further support the benefits of fiber in IBD. A study using a murine colitis model demonstrated that a high-fiber diet provided protection against acute and chronic colitis when administered as a preventive strategy. However, fiber supplementation after disease onset was less effective, suggesting that fiber may be more beneficial for maintaining remission rather than treating active disease [66].
Probiotics & Fermented Foods
Probiotics and fermented foods have gained increasing attention as potential dietary interventions for managing IBD. Since IBD is characterized by gut dysbiosis and chronic intestinal inflammation, probiotics—live microorganisms that confer health benefits—may help restore microbial balance and modulate immune responses [67]. Fermented foods, such as yogurt, kefir, sauerkraut, and kimchi, naturally contain probiotics and bioactive compounds that may support gut health. Probiotics exert their beneficial effects in IBD through multiple mechanisms. They enhance gut barrier integrity by stimulating mucus production and strengthening tight junction proteins, which reduces intestinal permeability and prevents bacterial translocation [68]. Probiotics also produce SCFAs, particularly butyrate, which has anti-inflammatory properties and supports the health of colonic epithelial cells [69]. Additionally, probiotics modulate the immune system by shifting the balance toward anti-inflammatory responses. Certain strains, such as Lactobacillus plantarum and Bifidobacterium, can reduce levels of pro-inflammatory cytokines like TNF-α and IL-6 while promoting the production of IL-10, an anti-inflammatory cytokine [70]. Meanwhile, fermented foods naturally contain probiotics, organic acids, and bioactive peptides that may help modulate gut microbiota and inflammation. Studies suggest that fermented milk products, such as kefir and yogurt, may improve symptoms in IBD patients by increasing the abundance of beneficial bacteria like Faecalibacterium and Lactobacillus (or Lactiplantibacillus), which produce SCFAs [69]. Additionally, certain fermented plant-based foods, such as kimchi and sauerkraut, contain polyphenols and bioactive peptides that exhibit anti-inflammatory effects [67,71].
Clinical trials suggest that probiotics can be effective in UC, particularly in maintaining remission. A systematic review of randomized human clinical trials found that probiotic formulations containing lactic acid bacteria and Bifidobacterium improved symptoms and prolonged remission in UC patients, though their effects in CD were less clear [72]. Another study found that probiotic supplementation significantly reduced gut inflammation and improved intestinal microbiota composition in patients with IBD-associated pouchitis [73]. However, while probiotics show promise, their efficacy depends on the specific bacterial strains used. The multi-strain probiotic formulation VSL#3 has demonstrated efficacy in inducing and maintaining remission in UC, but its benefits in CD remain inconclusive [74]. Some studies indicate that probiotic therapy alone may not be sufficient for treating active disease but can be beneficial when used as an adjunct to standard therapies [75].
Omega-3 Fatty Acids
Omega-3 polyunsaturated fatty acids (PUFAs), found in fatty fish (e.g., salmon, mackerel, sardines) and plant-based sources such as flaxseeds and walnuts, have been widely studied for their anti-inflammatory properties. These fatty acids include eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), which serve as precursors to specialized lipid mediators that modulate immune responses and promote gut homeostasis [76]. Omega-3 fatty acids reduce inflammation by competing with omega-6 fatty acids, particularly arachidonic acid (AA), for incorporation into cell membranes. This competition leads to a shift from the production of pro-inflammatory eicosanoids, such as prostaglandins and leukotrienes, to anti-inflammatory lipid mediators known as resolvins, protectins, and maresins [77]. These mediators actively resolve inflammation, reducing the recruitment of immune cells and promoting tissue healing. Additionally, omega-3 fatty acids have been shown to lower oxidative stress and reduce intestinal permeability, key factors contributing to IBD pathogenesis. A Mendelian randomization study demonstrated a causal relationship between higher omega-3 levels and a decreased risk of IBD, with a particularly strong protective effect against CD. This study suggested that maintaining a balanced omega-6 to omega-3 ratio is essential for modulating intestinal inflammation [78].
The clinical impact of omega-3 fatty acid supplementation in IBD remains a subject of debate. A systematic review of randomized controlled trials found that omega-3 supplementation was associated with a reduction in pro-inflammatory cytokines and improved quality of life in Crohn’s disease patients [76]. Similarly, a meta-analysis suggested that omega-3 intake might help reduce the risk of IBD relapse and inflammation markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) [79]. However, some studies have reported conflicting results. A large review analyzing omega-3 supplementation in IBD concluded that while these fatty acids have clear anti-inflammatory effects, their clinical benefits in inducing remission or preventing relapse remain inconsistent due to variations in dosage, formulation, and patient characteristics [80]. Recent research has also explored the role of dietary sources of omega-3s, such as fish and flaxseeds, rather than supplements. Observational studies suggest that regular fish consumption is associated with a lower risk of IBD development, likely due to the consistent intake of EPA and DHA from whole foods [81,82].
Curcumin & Polyphenols
Curcumin and polyphenols, bioactive compounds found in turmeric, green tea, berries, and other plant-based foods, have demonstrated significant anti-inflammatory and antioxidant effects in IBD. These natural compounds target multiple inflammatory pathways, helping to modulate immune responses and oxidative stress, which are central to IBD pathogenesis [83]. Curcumin, the active component of turmeric (Curcuma longa), is known for its ability to inhibit key pro-inflammatory pathways, including NF-κB, cyclooxygenase-2 (COX-2), and TNF-α [84]. By downregulating these pathways, curcumin helps reduce intestinal inflammation and oxidative damage, which are hallmarks of IBD. Additionally, curcumin promotes gut barrier integrity by enhancing tight junction protein expression, reducing intestinal permeability [85]. Polyphenols found in green tea (epigallocatechin gallate, EGCG) and berries (anthocyanins, quercetin) exhibit similar anti-inflammatory properties by modulating cytokine expression and suppressing reactive oxygen species (ROS) [86]. These compounds have been shown to shift immune responses from a pro-inflammatory Th1/Th17 profile to a more regulatory Th2 profile, thereby mitigating disease severity.
Several clinical trials have assessed curcumin’s efficacy in IBD management. A meta-analysis of randomized controlled trials found that curcumin supplementation significantly improved clinical remission rates and reduced endoscopic inflammation in UC patients [87]. Another study demonstrated that curcumin treatment effectively suppressed colonic inflammation in a mouse model of IBD, supporting its potential as a therapeutic agent [88]. Green tea polyphenols have also shown promising results. A clinical study found that EGCG supplementation improved intestinal barrier function and reduced inflammatory markers in IBD patients [83]. Additionally, anthocyanins from berries have demonstrated protective effects against colitis by modulating gut microbiota and increasing levels of beneficial bacteria like Lactobacillus and Bifidobacterium [86]. Despite these promising findings, challenges remain in translating curcumin and polyphenol research into clinical practice. Curcumin’s poor bioavailability limits its effectiveness, though novel formulations such as nanoparticles and liposomal curcumin aim to enhance its absorption [89].
Exclusive Enteral Nutrition (EEN) in Crohn’s Disease
EEN is a well-established first-line therapy for inducing remission in pediatric CD and is gaining recognition for its potential role in adult patients. EEN involves the complete replacement of regular food with a nutritionally complete liquid formula for a set duration, usually 6–8 weeks, with the goal of reducing intestinal inflammation and promoting mucosal healing [90]. The precise mechanisms by which EEN induces remission in CD are not fully understood, but several key pathways have been identified. EEN is believed to reduce inflammation by altering gut microbiota composition, decreasing intestinal permeability, and suppressing pro-inflammatory cytokines. Studies have shown that EEN promotes a shift in gut microbiota, reducing levels of Proteobacteria and increasing beneficial Firmicutes, which contribute to gut homeostasis [91]. Additionally, EEN has been shown to modulate the immune system by reducing the levels of circulating effector memory CD8+ T cells, which play a role in the chronic inflammation characteristic of CD [92]. This immune modulation helps dampen the inflammatory response within the gastrointestinal tract, leading to symptom improvement and mucosal healing. Another potential mechanism involves the reduction of dietary antigens that may trigger immune activation. By eliminating whole foods, EEN removes potential dietary triggers of inflammation, leading to a decrease in gut permeability and improved barrier function [93].
EEN is widely used in pediatric CD, with studies showing remission rates of up to 80% in children following an 8-week course [90]. In addition to inducing remission, EEN also supports nutritional status and growth, making it a preferred therapy over corticosteroids in pediatric populations. In adults, the evidence for EEN is more mixed. While some studies suggest that EEN can be effective in inducing remission, adherence remains a significant challenge due to the restrictive nature of the diet [94]. A study exploring patient experiences with EEN in adults found that while initial adherence was difficult, participants reported symptom improvement over time, with social and health system support playing a crucial role in adherence [94]. Another study assessed the impact of EEN on health-related quality of life in adults with active CD. Patients who underwent a 4-week EEN treatment experienced significant improvements in bowel symptoms, systemic symptoms, and emotional well-being, with 84.6% achieving clinical remission [95]. However, adherence to EEN was a key limitation, with some patients struggling with the monotony of a liquid-only diet.
Despite its effectiveness, EEN is underutilized in adult patients due to issues related to compliance and palatability. A review examining EEN use in adults found that non-adherence was a major barrier, with many patients struggling to maintain the diet for extended periods [96]. Strategies to improve adherence, such as partial enteral nutrition (PEN) or combining EEN with dietary guidance, are being explored to make the therapy more acceptable [97]. Additionally, research is needed to optimize EEN formulations to enhance compliance and effectiveness. The development of palatable and nutritionally balanced formulas, as well as better patient education and support systems, could increase the feasibility of EEN in adults [93]. Recommended dietary components for IBD patients and their underlying immunomechanisms are listed in Table 3.
Commonly Asked Questions
Spicy Food and Capsaicin in IBD
Spicy foods, particularly those containing capsaicin, have been a topic of debate in the context of IBD. Capsaicin, the active compound in chili peppers, interacts with transient receptor potential vanilloid 1 (TRPV1) receptors in the gut, which are involved in pain sensation, inflammation, and gut motility [98]. While some evidence suggests that capsaicin may have anti-inflammatory properties, other studies indicate that it may exacerbate symptoms in IBD patients. Capsaicin interacts with TRPV1 receptors located in the gut lining, which can modulate inflammation and gut permeability. Experimental studies suggest that capsaicin may have dual effects—it can reduce inflammation through activation of peroxisome proliferator-activated receptor gamma (PPAR-γ), but it can also stimulate immune cells and increase gut permeability, potentially worsening inflammation [99]. A study on mice with dextran sulfate sodium (DSS)-induced colitis found that oral capsaicin administration worsened colonic inflammation, leading to increased neutrophil infiltration and upregulation of inflammatory cytokines such as TNF-α and IL-6. The inflammatory effects were mediated by TRPV1 activation, as blocking this receptor significantly reduced gut inflammation [100]. These findings suggest that, in individuals with active IBD, capsaicin could contribute to symptom exacerbation by enhancing immune activation and gut permeability.
Epidemiological studies have reported that a significant number of IBD patients identify spicy foods as a trigger for symptom relapse. A survey conducted among 306 IBD patients found that 54.3% of UC patients and 53.4% of CD patients reported experiencing symptom worsening or disease relapse after consuming spicy food [100]. However, some experimental models suggest potential benefits of capsaicin. Studies indicate that, in controlled doses, capsaicin may help regulate gut microbiota composition and exert anti-inflammatory effects [101]. Capsaicin has also been shown to reduce oxidative stress and modulate macrophage activity in preclinical studies [102]. However, these findings have not yet translated into consistent clinical benefits for IBD patients.
Portion Size and Meal Composition in IBD
Portion size and meal composition are critical factors in managing IBD, as improper dietary habits can contribute to disease flares, malnutrition, and gut dysbiosis. Given that IBD patients often experience altered nutrient absorption, increased metabolic demands, and inflammation-related weight fluctuations, a structured dietary approach is essential for symptom control and overall well-being [103]. A well-balanced diet for IBD patients should include a combination of macronutrients—carbohydrates, proteins, and fats—in proportions that prevent malnutrition while minimizing gastrointestinal distress. A proposed food pyramid (Figure 2) for IBD patients recommends daily intake of complex carbohydrates (3 portions), tolerated fruits and vegetables (5 portions), yogurt (125ml), and extra virgin olive oil, as well as weekly intake of fish (4 portions), white meat (3 portions), eggs (3 portions), pureed legumes (2 portions), and limited red/processed meats (once a week) [104]. Dividing meals into smaller, frequent portions (4-6 meals per day) instead of three large meals is often recommended to improve digestion and nutrient absorption while reducing gut irritation. Large meals may overwhelm the gastrointestinal system, leading to bloating, diarrhea, or pain, whereas smaller meals help regulate bowel movements and prevent excess inflammation [7]. Portion size may need to be adjusted based on disease activity: During active flare-ups, small, easily digestible meals with low fiber (if fiber intolerance is present), moderate protein, and minimal fat are recommended. Liquid nutrition, such as EEN, may be beneficial for severe cases [105]. During remission, a more diverse diet with fiber-rich foods (fruits, vegetables, whole grains) can be introduced gradually, alongside probiotic-rich foods like yogurt and fermented vegetables to support gut microbiota [106]. Importantly, many IBD patients suffer from malnutrition despite consuming adequate calories, as inflammation and intestinal damage impair nutrient absorption. Studies have shown that 41.4% of IBD patients have altered body composition, particularly low fat-free mass, despite appearing well-nourished [107]. This underscores the need for individualized meal planning, focusing on portion control to meet micronutrient requirements, particularly for iron, vitamin D, calcium, and omega-3 fatty acids.
Asian Diet, MSG, and Flavor Enhancers in IBD
The role of diet in IBD has been extensively studied, with dietary patterns differing between Western and Asian populations. The increasing incidence of IBD in Asia has been linked to a shift toward a more Westernized diet, which includes higher consumption of processed foods, food additives, and monosodium glutamate (MSG) [108]. Traditionally, Asian diets have been considered protective against IBD due to their emphasis on fiber-rich foods, fermented products, and anti-inflammatory compounds. However, with increasing urbanization and dietary Westernization, there has been a notable rise in IBD cases in Asian countries [109]. Research suggests that the adoption of higher-fat, lower-fiber diets may contribute to gut dysbiosis and increased intestinal inflammation, similar to patterns observed in Western populations [110]. A study on British South Asians with IBD found that patients frequently modified their traditional diets, avoiding certain foods such as spicy dishes, dairy, and legumes, in an attempt to manage symptoms. Notably, many of these patients had adopted food avoidance behaviors more commonly seen in Western IBD populations, indicating a complex interplay between dietary habits and cultural influences [111].
MSG is a widely used flavor enhancer, particularly in Asian cuisines. While MSG is generally considered safe for human consumption, its potential impact on gut health and IBD remains debated. Some animal studies suggest that high doses of MSG could contribute to increased gut permeability and oxidative stress, which may exacerbate inflammation in IBD [112]. Additionally, the combination of MSG with high-fat diets has been shown to produce contrasting effects on different regions of the intestine. While MSG may have protective effects in some areas, it has been associated with increased pro-inflammatory markers in others. This suggests that the interaction between dietary components may influence gut inflammation differently depending on the individual’s overall diet and IBD status [112]. Given the variability in individual responses to MSG and flavor enhancers, IBD patients should consider tracking their symptoms after consuming foods containing MSG. While current evidence does not definitively link MSG to IBD flares, patients who suspect sensitivity may benefit from reducing processed foods that contain MSG and other additives. Furthermore, the Asian Working Group on Diet and IBD recommends a balanced dietary approach that includes traditional elements of the Asian diet, such as fiber-rich vegetables, fermented foods, and omega-3 fatty acids, while minimizing processed foods and artificial flavor enhancers [108].
Vitamins and Minerals in IBD
Patients with IBD are at a heightened risk of vitamin and mineral deficiencies due to chronic inflammation, malabsorption, altered dietary intake, and the effects of medications such as corticosteroids and immunosuppressants [113]. Deficiencies in essential micronutrients can exacerbate IBD symptoms, impair immune function, and increase the risk of complications such as osteoporosis and anemia. Vitamin D plays a crucial role in modulating immune responses and maintaining gut barrier integrity. Studies indicate that vitamin D deficiency is highly prevalent in IBD patients, with 38.1% of CD and 31.6% of UC patients exhibiting low levels [114]. Vitamin D supplementation has been shown to help regulate inflammatory cytokines and may reduce disease activity [115]. Next, chronic intestinal bleeding, reduced dietary intake, and impaired absorption contribute to iron deficiency anemia (IDA) in IBD. It is estimated that up to 50% of IBD patients suffer from anemia, with iron deficiency being the leading cause [116]. Iron supplementation, either oral or intravenous, is often required, though oral supplementation may be poorly tolerated due to gastrointestinal side effects. Vitamin B12 deficiency is more common in CD patients, particularly those with ileal involvement or resection, as the terminal ileum is the primary site of B12 absorption [117]. Folate deficiency may occur due to malabsorption or long-term use of sulfasalazine and methotrexate. Zinc plays a crucial role in immune function and wound healing. Up to 40% of IBD patients have zinc deficiency, which has been linked to increased disease severity and delayed mucosal healing [117]. Additionally, long-term corticosteroid use and chronic inflammation increase the risk of osteoporosis in IBD patients. Vitamin D and calcium supplementation are recommended to prevent bone loss, while vitamin K deficiency has been linked to increased inflammatory activity in CD [118].
While supplementation is necessary to correct deficiencies, indiscriminate use of multivitamins may not always be beneficial. A randomized controlled trial found that over-the-counter multivitamin and mineral supplements did not significantly reduce infection risk in IBD patients on immunosuppressive therapy [119]. However, targeted supplementation for specific deficiencies, such as vitamin D, iron, and zinc, has shown clear clinical benefits in disease management. A study on pediatric IBD patients found that supplement adherence was relatively poor (32–44%), and those with a better understanding of supplementation's purpose were more likely to follow recommendations [120]. This highlights the need for patient education regarding the importance of vitamins and minerals in IBD management.
Types of Dairy Safe in IBD
Dairy consumption in inflammatory bowel disease (IBD) is a controversial topic, as some patients report dairy-related symptoms, while others tolerate certain types of dairy without issues. The primary concerns include lactose intolerance, dairy protein sensitivity, and potential inflammatory effects. However, research suggests that complete “blanket” dairy elimination may not be necessary for all IBD patients [48]. For IBD patients with lactose intolerance, lactose-free milk and fermented dairy products like yogurt and kefir may be safer options. Fermented dairy contains probiotics that help support gut health by modulating microbiota composition and reducing intestinal inflammation [69]. A systematic review found no strong evidence that dairy significantly worsens IBD symptoms, and fermented dairy was associated with improved gut microbiota diversity [121]. For patients who are sensitive to dairy proteins, plant-based milk alternatives such as almond milk, oat milk, and coconut milk can be good options. However, some of these alternatives contain additives such as emulsifiers and carrageenan, which may disrupt gut microbiota and contribute to inflammation [52]. Choosing minimally processed plant-based milks without artificial additives is recommended. Hard cheeses such as cheddar, Parmesan, and Swiss contain very little lactose and are generally well tolerated by those with lactose intolerance. Butter also contains negligible amounts of lactose and is unlikely to cause symptoms in most IBD patients [122]. Many IBD patients restrict dairy, which may lead to calcium and vitamin D deficiencies, increasing the risk of osteoporosis. A study found that patients who consumed dairy regularly had better bone mineral density compared to those who avoided it [123]. Unless dairy causes significant symptoms, moderate consumption may be beneficial for bone health.
Special Considerations and Emerging Research
Personalized Nutrition Approaches
Personalized nutrition is an emerging concept in IBD management, recognizing that dietary responses vary widely among patients due to differences in genetics, microbiota composition, disease phenotype, and immune responses. Unlike standardized dietary recommendations, personalized nutrition tailors dietary interventions to individual patients, optimizing nutritional intake while reducing inflammation and symptom severity [124]. The effectiveness of dietary interventions in IBD depends on several patient-specific factors: The gut microbiome plays a crucial role in how individuals metabolize nutrients. Studies suggest that patients with dysbiosis (imbalanced gut bacteria) may respond differently to dietary fibers and probiotics compared to those with a more balanced microbiome [125]; Genetic variations, such as mutations in NOD2 or ATG16L1, influence immune responses and intestinal barrier function, which may alter how patients react to specific dietary components [126,127]; Some IBD patients experience heightened immune activation in response to dietary triggers like high-fat or high-sugar foods, while others may not exhibit the same inflammatory responses [128].
Personalized nutrition has shown promise in improving clinical outcomes in IBD patients. A review of dietary interventions found that specific diets, such as the Mediterranean diet, specific carbohydrate diet (SCD), and low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) diet, had varying levels of success depending on the patient’s microbiome and disease activity [124]. A study on the impact of a personalized dietary approach found that patients who followed microbiome-guided dietary recommendations experienced reduced intestinal inflammation and fewer relapses compared to those who followed general dietary guidelines [125]. Another clinical trial investigating the role of precision nutrition in IBD highlighted the need for machine-learning algorithms and biomarkers to optimize dietary interventions based on patient-specific needs. The study concluded that future dietary guidelines should incorporate genetic, microbiome, and metabolic profiling to develop effective dietary strategies [124]. Emerging technologies, such as microbiome sequencing and metabolomics, are expected to revolutionize personalized nutrition for IBD. These advancements will enable healthcare providers to recommend specific foods, probiotics, and supplements tailored to each patient's biological profile, improving disease management and overall quality of life [125].
Role of Elimination Diets
Elimination diets are increasingly used in the management of IBD to identify and remove dietary triggers that may contribute to intestinal inflammation. These diets typically involve the exclusion of specific food groups, followed by a gradual reintroduction process to determine individual tolerance. Two of the most studied elimination diets in IBD are the SCD and the Mediterranean Diet (MD) [129]. The SCD was originally developed to manage celiac disease and has since been explored as a potential dietary therapy for CD and UC. This diet eliminates complex carbohydrates such as disaccharides and polysaccharides while allowing monosaccharides, lean proteins, and unprocessed foods [130]. SCD reduces gut dysbiosis by limiting fermentable carbohydrates that feed pro-inflammatory bacteria, promotes gut microbiota diversity by increasing beneficial bacteria like Lactobacillus and Bifidobacterium, and decreases intestinal permeability and inflammation by minimizing processed foods and additives. Case studies and retrospective analyses suggest that the SCD may improve symptoms and help maintain remission in pediatric IBD patients [131]. However, large randomized controlled trials (RCTs) are lacking, and adherence to the diet can be challenging due to its restrictive nature.
The MD is characterized by high consumption of fruits, vegetables, whole grains, nuts, fish, and olive oil, with moderate dairy intake and limited red meat consumption. Unlike SCD, MD is less restrictive and promotes a balanced, nutrient-dense diet. It increases intake of anti-inflammatory polyphenols and omega-3 fatty acids, which modulate immune responses, enriches gut microbiota with beneficial bacteria, improving gut barrier integrity, as well as reduces oxidative stress and systemic inflammation by promoting high fiber intake [132]. A study on MD adherence in IBD patients found that those who followed MD had lower levels of inflammation and better disease outcomes [133]. However, adherence to MD was low among patients, highlighting the need for dietary education programs. Another study in pediatric IBD patients found that MD adherence was associated with lower fecal calprotectin levels, a marker of intestinal inflammation [134]. While both SCD and MD have shown promise in IBD management, they differ significantly in their approach. The SCD is more restrictive and difficult to maintain but may be effective for symptom relief, particularly in pediatric IBD [135]. The MD, on the other hand, is more sustainable and beneficial for long-term gut health. Future research should focus on large-scale, long-term RCTs comparing different elimination diets to establish clear dietary guidelines for IBD management. Personalized nutrition strategies incorporating elements from both diets may provide optimal benefits.
Ketogenic Diet and IBD
The ketogenic diet (KD), a high-fat, low-carbohydrate dietary regimen, has gained attention for its potential therapeutic effects in various chronic diseases. While KD has been extensively studied for neurological conditions such as epilepsy, its role in IBD remains a subject of debate. Recent studies suggest that KD can modulate gut microbiota, inflammation, and intestinal permeability, with mixed results depending on disease context [136]. KD influences gut health through multiple pathways, including microbiome alterations, immune modulation, and changes in energy metabolism. KD has been shown to alter gut microbiota, increasing beneficial bacteria like Akkermansia while reducing pro-inflammatory Escherichia/Shigella species. This shift may help regulate immune responses and maintain intestinal barrier integrity [137]. In a mouse model, KD was found to reduce group 3 innate lymphoid cells (ILC3s) and related inflammatory cytokines, such as IL-17 and IL-22, thereby alleviating colitis symptoms [137]. However, other studies indicate that KD can increase intestinal permeability, leading to worsened colonic inflammation [136]. A very-low-calorie ketogenic diet (VLCKD) has been investigated for its role in SCFA production, which plays a key role in gut health. SCFAs like butyrate support colonic epithelial function and reduce inflammation, though the impact of KD on SCFA levels in IBD remains unclear [138].
The clinical effects of KD in IBD remain controversial, with conflicting findings from human case reports and animal studies. A study using a dextran sulfate sodium (DSS)-induced colitis mouse model found that KD worsened colitis symptoms, increased pro-inflammatory cytokines (TNF-α, IL-6, IL-17), and disrupted gut barrier function [136]. A case series of 10 IBD patients following a carnivore-ketogenic diet (high in animal fats and proteins) reported significant symptom improvement and medication cessation. However, this study was observational and lacked control groups [139]. Another mouse study found that KD, particularly when rich in polyunsaturated fats, reduced histological signs of colitis, weight loss, and pro-inflammatory cytokine expression [140]. While some evidence suggests that KD could have immunomodulatory effects in IBD, significant concerns remain about its impact on gut barrier function and microbiome stability. First, KD’s high-fat content may negatively influence gut microbiota and promote bile acid metabolism that can increase gut permeability and inflammation [136]. Second, most current data come from small observational studies or animal models. Large-scale, randomized controlled trials are necessary to determine whether KD can be safely implemented in IBD management [139].
Intermittent Fasting and IBD
Intermittent fasting (IF), which involves alternating periods of eating and fasting, has been increasingly studied for its potential role in IBD. IF has been proposed to modulate gut inflammation, promote intestinal repair, and alter gut microbiota composition, making it a promising dietary intervention [141]. The beneficial effects of IF in IBD appear to be mediated through several pathways: IF has been associated with decreased levels of pro-inflammatory cytokines such as IL-6 and TNF-α, which are implicated in IBD pathogenesis [142]. IF also promotes beneficial bacterial diversity and reduces pathogenic bacteria that contribute to gut inflammation. Studies in mice have shown that IF alters gut microbiota composition, leading to an increase in SCFA-producing bacteria, which helps maintain intestinal barrier integrity [143]. Furthermore, IF has been shown to upregulate intestinal stem cell markers and promote mucosal healing, potentially improving outcomes in IBD patients [144].
Human studies on IF in IBD remain limited, but emerging evidence suggests potential benefits: A study assessing IF in IBD patients found that those who engaged in periodic fasting experienced reductions in inflammation markers such as CRP and fecal calprotectin, although the study lacked a control group [142]. Mouse models of colitis have demonstrated that fasting-mimicking diets (FMD) reduce inflammation, improve intestinal repair, and decrease immune cell infiltration in the gut [144]. Next, a survey conducted at an IBD nutrition clinic found that 30.8% of patients practiced some form of fasting, with a higher prevalence in those with active disease. However, the effects of fasting on symptom control and disease progression were not clearly established [145]. While preliminary findings suggest that IF may be beneficial in IBD, several challenges remain: First, most existing evidence comes from small observational studies or animal models. Well-designed randomized controlled trials are needed to establish the safety and efficacy of IF in IBD patients [141]. Second, IF may not be suitable for all IBD patients, particularly those who are underweight or at risk of malnutrition, as fasting could exacerbate nutrient deficiencies. Third, given the variability in IBD presentation, a personalized approach to IF, considering disease activity, nutritional status, and microbiome composition, may be necessary.
Ramadan Fasting and IBD
Ramadan fasting is a unique form of intermittent fasting observed by millions of Muslims worldwide, involving daily abstinence from food and drink from sunrise to sunset. Given the increasing interest in the effects of fasting on chronic diseases, research has begun exploring how Ramadan fasting influences IBD. While some studies suggest potential anti-inflammatory effects, others highlight concerns regarding disease exacerbation, particularly in high-risk patients [146]. Studies suggest that Ramadan fasting can improve gut microbiome diversity and alter microbial composition in a way that may reduce gut inflammation [147]. Fasting during Ramadan has also been linked to lower levels of pro-inflammatory cytokines such as TNF-α and IL-6, which are key mediators in IBD pathogenesis [148]. A study found that Ramadan fasting improved anxiety and quality of life in UC patients, suggesting a potential psychosomatic benefit [146].
A cohort study assessing 60 IBD patients during Ramadan found no significant correlation between fasting and disease severity. However, younger UC patients fasted for a greater number of days compared to older individuals, indicating that disease tolerance may vary by age [146]. Another review suggested that while Ramadan fasting generally does not pose a serious risk for IBD patients, older men with UC may be more prone to disease exacerbation [147]. A systematic review found that Ramadan fasting did not significantly impact the quality of life in IBD patients, but it emphasized the need for individualized pre-Ramadan medical consultations [149]. Nonetheless, prolonged fasting hours can increase the risk of dehydration, which may be problematic for IBD patients, particularly those with diarrhea-dominant disease. Moreover, some IBD medications require consistent dosing schedules, which can be challenging to maintain during Ramadan fasting. Physicians should provide clear guidance on modifying medication timing. At last, patients should undergo pre-Ramadan counseling to assess whether fasting is safe for their disease state and nutritional status [147]. Overall, Ramadan fasting appears to be generally safe for IBD patients who are in remission, with potential benefits including reduced systemic inflammation and improved psychological well-being. However, older patients and those with active disease should consult healthcare providers before fasting.
Future Directions in Dietary Intervention Trials
As dietary interventions gain recognition as a potential adjunct therapy for IBD, future clinical trials must address several challenges, including heterogeneity in study design, lack of standardized outcome measures, and individual patient variability. Improving trial methodologies will help establish evidence-based dietary recommendations for IBD management [150]. Several key areas for future research are: (1) one of the major challenges in dietary research for IBD is the lack of standardized protocols. Many studies use different dietary interventions, outcome measures, and control groups, making it difficult to compare results. Future trials should follow rigorous clinical guidelines similar to pharmacological trials, including placebo-controlled designs, objective inflammatory markers, and dietary adherence monitoring [150]. (2) Personalized dietary interventions based on biomarkers such as fecal calprotectin, gut microbiota composition, and genetic profiles are emerging as promising strategies. Studies suggest that individuals with different microbiome profiles may respond differently to specific dietary interventions, highlighting the need for precision nutrition [151]. (3) Adherence to restrictive diets, such as the SCD and low FODMAP diets, remains a challenge for many IBD patients. Future trials should evaluate the long-term feasibility, sustainability, and nutritional adequacy of different dietary interventions to determine their practicality in real-world settings [152]. (4) Many existing dietary trials focus on individual interventions, but comparative studies assessing multiple dietary approaches are needed. Trials should directly compare popular diets such as the Mediterranean diet, ketogenic diet, and anti-inflammatory diet to determine the most effective dietary strategies for different IBD phenotypes [153]. (5) Digital tools such as mobile apps, artificial intelligence-based dietary recommendations, and remote monitoring can improve patient adherence and data collection in dietary trials. Future research should explore how technology can enhance dietary tracking, improve compliance, and facilitate personalized meal planning for IBD patients [154]. (6) The gut microbiome plays a crucial role in mediating dietary effects in IBD. Future studies should investigate how different diets influence microbial diversity, metabolite production (e.g., SCFAs), and intestinal inflammation. This will help refine dietary recommendations based on microbiome responses [155].
Conclusions
Diet plays a significant role in the management of IBD, influencing gut microbiota composition, intestinal barrier function, and immune responses. While certain foods, such as ultra-processed products and high-fat diets, may contribute to disease exacerbation, others, including fiber-rich, anti-inflammatory, and probiotic-containing foods, show potential benefits. Emerging clinical evidence supports the use of personalized nutrition strategies tailored to individual patient responses. However, despite growing research, standardized dietary guidelines for IBD remain limited. Further well-designed clinical trials are essential to establish evidence-based recommendations and integrate dietary interventions into routine care. A multidisciplinary approach involving gastroenterologists, dietitians, and researchers is crucial for optimizing nutritional strategies and improving patient outcomes.
Author Contributions
Henry Sutanto: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Writing - Original Draft, Writing - Review & Editing, Visualization.
Funding
This research receives no external funding.
Conflicts of Interest
The author declares no conflict of interest.
References
- Younge, L. An Overview of Inflammatory Bowel Disease. Nursing Standard 2019, 34, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Baumgart, D.C. The Diagnosis and Treatment of Crohn’s Disease and Ulcerative Colitis. Dtsch Arztebl Int 2009, 106, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.M.; Girardelli, M.; Tommasini, A. Genetics of Inflammatory Bowel Disease from Multifactorial to Monogenic Forms. World J Gastroenterol 2015, 21, 12296–12310. [Google Scholar] [CrossRef]
- M’Koma, A.E. The Multifactorial Etiopathogeneses Interplay of Inflammatory Bowel Disease: An Overview. Gastrointestinal Disorders 2019, 1, 75–105. [Google Scholar] [CrossRef]
- Knight-Sepulveda, K.; Kais, S.; Santaolalla, R.; Abreu, M.T. Diet and Inflammatory Bowel Disease. Gastroenterol Hepatol (N Y) 2015, 11, 511–520. [Google Scholar]
- Issokson, K.; Lee, D.Y.; Yarur, A.J.; Lewis, J.D.; Suskind, D.L. The Role of Diet in Inflammatory Bowel Disease Onset, Disease Management, and Surgical Optimization. Am J Gastroenterol 2025, 120, 98–105. [Google Scholar] [CrossRef]
- Gu, P.; Feagins, L.A. Dining With Inflammatory Bowel Disease: A Review of the Literature on Diet in the Pathogenesis and Management of IBD. Inflammatory Bowel Diseases 2019, izz268. [Google Scholar] [CrossRef]
- Sahu, P.; Kedia, S.; Ahuja, V.; Tandon, R.K. Diet and Nutrition in the Management of Inflammatory Bowel Disease. Indian J Gastroenterol 2021, 40, 253–264. [Google Scholar] [CrossRef]
- De Castro, M.M.; Pascoal, L.B.; Steigleder, K.M.; Siqueira, B.P.; Corona, L.P.; Ayrizono, M.D.L.S.; Milanski, M.; Leal, R.F. Role of Diet and Nutrition in Inflammatory Bowel Disease. WJEM 2021, 11, 1–16. [Google Scholar] [CrossRef]
- Manski, S.; Noverati, N.; Policarpo, T.; Rubin, E.; Shivashankar, R. Diet and Nutrition in Inflammatory Bowel Disease: A Review of the Literature. Crohn’s & Colitis 360 2024, 6, otad077. [Google Scholar] [CrossRef]
- Ghamdi, K.M.A.; Alrahma, H.A.; Alkanhal, F.A.; Alhamazani, F.T.; Aloraini, E.S.; Alqadiri, N.G.; Alhawsawi, M.Z.; Thabet, A.A.; Ajzaji, R.J.; Nasser, J.S.; et al. The Critical Role of Diet and Nutrition in Managing Inflammatory Bowel Disease. Int J Community Med Public Health 2023, 10, 5004–5008. [Google Scholar] [CrossRef]
- Sutanto, H.; Elisa, E.; Rachma, B.; Fetarayani, D. Gut Microbiome Modulation in Allergy Treatment: The Role of Fecal Microbiota Transplantation. The American Journal of Medicine 2025, 0. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Shiva, Km.; Singh, R.; Sherawat, K.S.; Bhardwaj, P. Inflammatory Bowel Disease and Gut Microbiota Dysbiosis: Current Understanding and Future Direction. JBPR 2024, 13. [Google Scholar] [CrossRef]
- Nishida, A.; Inoue, R.; Inatomi, O.; Bamba, S.; Naito, Y.; Andoh, A. Gut Microbiota in the Pathogenesis of Inflammatory Bowel Disease. Clin J Gastroenterol 2018, 11, 1–10. [Google Scholar] [CrossRef]
- Shim, J.O. Gut Microbiota in Inflammatory Bowel Disease. Pediatr Gastroenterol Hepatol Nutr 2013, 16, 17. [Google Scholar] [CrossRef]
- Haneishi, Y.; Furuya, Y.; Hasegawa, M.; Picarelli, A.; Rossi, M.; Miyamoto, J. Inflammatory Bowel Diseases and Gut Microbiota. IJMS 2023, 24, 3817. [Google Scholar] [CrossRef]
- Khalil, H.; Rubab Ahmad; Sawar, M.U.N.; Ahmad, A.; Hareera; Khan, I. The Role of Gut Microbiota in Inflammatory Bowel Disease: Mechanisms, Therapeutic Targets, and Future Directions. IRABCS 2024, 2, 85–90. [CrossRef]
- Lavelle, A.; Sokol, H. The Gut Microbiome in Inflammatory Bowel Disease. In Molecular Genetics of Inflammatory Bowel Disease; Hedin, C., Rioux, J.D., D’Amato, M., Eds.; Springer International Publishing: Cham, 2019; pp. 347–377. ISBN 978-3-030-28702-3. [Google Scholar]
- McGuckin, M.A.; Eri, R.; Simms, L.A.; Florin, T.H.J.; Radford-Smith, G. Intestinal Barrier Dysfunction in Inflammatory Bowel Diseases. Inflammatory Bowel Diseases 2009, 15, 100–113. [Google Scholar] [CrossRef]
- Su, L.; Shen, L.; Clayburgh, D.R.; Nalle, S.C.; Sullivan, E.A.; Meddings, J.B.; Abraham, C.; Turner, J.R. Targeted Epithelial Tight Junction Dysfunction Causes Immune Activation and Contributes to Development of Experimental Colitis. Gastroenterology 2009, 136, 551–563. [Google Scholar] [CrossRef]
- Hering, N.A.; Fromm, M.; Schulzke, J. Determinants of Colonic Barrier Function in Inflammatory Bowel Disease and Potential Therapeutics. The Journal of Physiology 2012, 590, 1035–1044. [Google Scholar] [CrossRef]
- Garg, A.; Zhao, A.; Erickson, S.L.; Mukherjee, S.; Lau, A.J.; Alston, L.; Chang, T.K.H.; Mani, S.; Hirota, S.A. Pregnane X Receptor Activation Attenuates Inflammation-Associated Intestinal Epithelial Barrier Dysfunction by Inhibiting Cytokine-Induced Myosin Light-Chain Kinase Expression and c-Jun N-Terminal Kinase 1/2 Activation. The Journal of Pharmacology and Experimental Therapeutics 2016, 359, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Albenberg, L.G.; Lewis, J.D.; Wu, G.D. Food and the Gut Microbiota in Inflammatory Bowel Diseases: A Critical Connection. Current Opinion in Gastroenterology 2012, 28, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Ruemmele, F.M. Role of Diet in Inflammatory Bowel Disease. Ann Nutr Metab 2016, 68, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Chapman-Kiddell, C.A.; Davies, P.S.W.; Gillen, L.; Radford-Smith, G.L. Role of Diet in the Development of Inflammatory Bowel Disease. Inflammatory Bowel Diseases 2010, 16, 137–151. [Google Scholar] [CrossRef]
- Sugihara, K.; Morhardt, T.L.; Kamada, N. The Role of Dietary Nutrients in Inflammatory Bowel Disease. Front. Immunol. 2019, 9, 3183. [Google Scholar] [CrossRef]
- Hou, J.K.; Lee, D.; Lewis, J. Diet and Inflammatory Bowel Disease: Review of Patient-Targeted Recommendations. Clinical Gastroenterology and Hepatology 2014, 12, 1592–1600. [Google Scholar] [CrossRef]
- Olednzki, B.; Bucci, V.; Cawley, C.; Maldonado-Contreras, A. A WHOLE FOOD, ANTI-INFLAMMATORY DIET ESTABLISHES A BENEFICIAL GUT MICROBIOME IN INFLAMMATORY BOWEL DISEASE PATIENTS. Gastroenterology 2021, 160, S51. [Google Scholar] [CrossRef]
- Godala, M.; Gaszyńska, E.; Zatorski, H.; Małecka-Wojciesko, E. Dietary Interventions in Inflammatory Bowel Disease. Nutrients 2022, 14, 4261. [Google Scholar] [CrossRef]
- Stein, R.; Baldassano, R.N. Dietary Therapies for Inflammatory Bowel Disease. In Pediatric Inflammatory Bowel Disease; Mamula, P., Grossman, A.B., Baldassano, R.N., Kelsen, J.R., Markowitz, J.E., Eds.; Springer International Publishing: Cham, 2017; pp. 473–483. ISBN 978-3-319-49213-1. [Google Scholar]
- Calder, P.C. Omega-3 Polyunsaturated Fatty Acids and Inflammatory Processes: Nutrition or Pharmacology? Br J Clin Pharmacol 2013, 75, 645–662. [Google Scholar] [CrossRef]
- Marion-Letellier, R.; Amamou, A.; Savoye, G.; Ghosh, S. Inflammatory Bowel Diseases and Food Additives: To Add Fuel on the Flames! Nutrients 2019, 11, 1111. [Google Scholar] [CrossRef]
- Guedelha Sabino, J. OP33 Mechanistic Insights on the Role of Ultra Processed Foods as a Trigger/Fuel for IBD. Journal of Crohn’s and Colitis 2024, 18, i59–i59. [Google Scholar] [CrossRef]
- Raoul, P.; Cintoni, M.; Palombaro, M.; Basso, L.; Rinninella, E.; Gasbarrini, A.; Mele, M.C. Food Additives, a Key Environmental Factor in the Development of IBD through Gut Dysbiosis. Microorganisms 2022, 10, 167. [Google Scholar] [CrossRef] [PubMed]
- Narula, N.; Wong, E.C.L.; Dehghan, M.; Mente, A.; Rangarajan, S.; Lanas, F.; Lopez-Jaramillo, P.; Rohatgi, P.; Lakshmi, P.V.M.; Varma, R.P.; et al. Association of Ultra-Processed Food Intake with Risk of Inflammatory Bowel Disease: Prospective Cohort Study. BMJ 2021, n1554. [Google Scholar] [CrossRef] [PubMed]
- Sarbagili-Shabat, C.; Zelber-Sagi, S.; Isakov, N.F.; Hirsch, A.; Ron, Y.; Grinshpan, L.S.; Anbar, R.; Bromberg, A.; Thurm, T.; Maharshak, N. Ultra-Processed Foods Consumption Is Positively Associated with the Clinical Activity of Inflammatory Bowel Diseases: A Cross-Sectional Single-Center Study. Inflamm Intest Dis 2024, 9, 241–251. [Google Scholar] [CrossRef]
- Babaei, A.; Pourmotabbed, A.; Talebi, S.; Mehrabani, S.; Bagheri, R.; Ghoreishy, S.M.; Amirian, P.; Zarpoosh, M.; Mohammadi, H.; Kermani, M.A.H.; et al. The Association of Ultra-Processed Food Consumption with Adult Inflammatory Bowel Disease Risk: A Systematic Review and Dose-Response Meta-Analysis of 4 035 694 Participants. Nutrition Reviews 2024, 82, 861–871. [Google Scholar] [CrossRef]
- Dang, Y.; Ma, C.; Chen, K.; Chen, Y.; Jiang, M.; Hu, K.; Li, L.; Zeng, Z.; Zhang, H. The Effects of a High-Fat Diet on Inflammatory Bowel Disease. Biomolecules 2023, 13, 905. [Google Scholar] [CrossRef]
- Natividad, J.M.; Lamas, B.; Pham, H.P.; Michel, M.-L.; Rainteau, D.; Bridonneau, C.; da Costa, G.; van Hylckama Vlieg, J.; Sovran, B.; Chamignon, C.; et al. Bilophila Wadsworthia Aggravates High Fat Diet Induced Metabolic Dysfunctions in Mice. Nat Commun 2018, 9, 2802. [Google Scholar] [CrossRef]
- Paik, J.; Fierce, Y.; Treuting, P.M.; Brabb, T.; Maggio-Price, L. High-Fat Diet-Induced Obesity Exacerbates Inflammatory Bowel Disease in Genetically Susceptible Mdr1a Male Mice. The Journal of Nutrition 2013, 143, 1240–1247. [Google Scholar] [CrossRef]
- Li, X.; Wei, X.; Sun, Y.; Du, J.; Li, X.; Xun, Z.; Li, Y.C. High-Fat Diet Promotes Experimental Colitis by Inducing Oxidative Stress in the Colon. American Journal of Physiology-Gastrointestinal and Liver Physiology 2019, 317, G453–G462. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, Z.; Dong, R.; Liu, Y.; Zhang, Y.; Guo, Y.; Yu, M.; Li, X.; Wang, J. Multiomics Analysis Reveals the Potential Mechanism of High-fat Diet in Dextran Sulfate Sodium-induced Colitis Mice Model. Food Science & Nutrition 2024, 12, 8309–8323. [Google Scholar] [CrossRef]
- Wu, Z.-H.; Yang, J.; Chen, L.; Du, C.; Zhang, Q.; Zhao, S.-S.; Wang, X.-Y.; Yang, J.; Liu, Y.; Cai, D.; et al. Short-Term High-Fat Diet Fuels Colitis Progression in Mice Associated With Changes in Blood Metabolome and Intestinal Gene Expression. Front. Nutr. 2022, 9, 899829. [Google Scholar] [CrossRef] [PubMed]
- Dong, C.; Chan, S.S.M.; Jantchou, P.; Racine, A.; Oldenburg, B.; Weiderpass, E.; Heath, A.K.; Tong, T.Y.N.; Tjønneland, A.; Kyrø, C.; et al. Meat Intake Is Associated with a Higher Risk of Ulcerative Colitis in a Large European Prospective Cohort Studyø. Journal of Crohn’s and Colitis 2022, 16, 1187–1196. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Cui, M.; Tan, F.; Liu, X.; Yao, P. High Red Meat Intake Exacerbates Dextran Sulfate-Induced Colitis by Altering Gut Microbiota in Mice. Front. Nutr. 2021, 8, 646819. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Fu, T.; Dan, L.; Chen, X.; Sun, Y.; Chen, J.; Wang, X.; Hesketh, T. P003 Meat Consumption and All-Cause Mortality in 5763 Inflammatory Bowel Disease Patients: A Prospective Cohort Study. Am J Gastroenterol 2021, 116, S1–S1. [Google Scholar] [CrossRef]
- Albenberg, L.; Brensinger, C.M.; Wu, Q.; Gilroy, E.; Kappelman, M.D.; Sandler, R.S.; Lewis, J.D. A Diet Low in Red and Processed Meat Does Not Reduce Rate of Crohn’s Disease Flares. Gastroenterology 2019, 157, 128–136.e5. [Google Scholar] [CrossRef]
- Mishkin, S. Dairy Sensitivity, Lactose Malabsorption, and Elimination Diets in Inflammatory Bowel Disease. The American Journal of Clinical Nutrition 1997, 65, 564–567. [Google Scholar] [CrossRef]
- Asfari, M.M.; Sarmini, M.T.; Kendrick, K.; Hudgi, A.; Uy, P.; Sridhar, S.; Sifuentes, H. Association between Inflammatory Bowel Disease and Lactose Intolerance: Fact or Fiction. Korean J Gastroenterol 2020, 76, 185–190. [Google Scholar] [CrossRef]
- Nardone, O.M.; Manfellotto, F.; D’Onofrio, C.; Rocco, A.; Annona, G.; Sasso, F.; De Luca, P.; Imperatore, N.; Testa, A.; De Sire, R.; et al. Lactose Intolerance Assessed by Analysis of Genetic Polymorphism, Breath Test and Symptoms in Patients with Inflammatory Bowel Disease. Nutrients 2021, 13, 1290. [Google Scholar] [CrossRef]
- Mishkin, S. Controversies Regarding the Role of Dairy Products in Inflammatory Bowel Disease. Canadian Journal of Gastroenterology 1994, 8, 205–212. [Google Scholar] [CrossRef]
- Alavinejad, P.; Nayebi, M.; Parsi, A.; Farsi, F.; Maghool, F.; Alipour, Z.; Alimadadi, M.; Ahmed, M.H.; Cheraghian, B.; Hang, D.V.; et al. IS DAIRY FOODS RESTRICTION MANDATORY FOR INFLAMMATORY BOWEL DISEASE PATIENTS: A MULTINATIONAL CROSS-SECTIONAL STUDY. Arq. Gastroenterol. 2022, 59, 358–364. [Google Scholar] [CrossRef]
- Szilagyi, A.; Galiatsatos, P.; Xue, X. Systematic Review and Meta-Analysis of Lactose Digestion, Its Impact on Intolerance and Nutritional Effects of Dairy Food Restriction in Inflammatory Bowel Diseases. Nutr J 2015, 15, 67. [Google Scholar] [CrossRef] [PubMed]
- Almofarreh, A.M.; Sheerah, H.A.; Arafa, A.; Al Mubarak, A.S.; Ali, A.M.; Al-Otaibi, N.M.; Alzahrani, M.A.; Aljubayl, A.R.; Aleid, M.A.; Alhamed, S.S. Dairy Consumption and Inflammatory Bowel Disease among Arab Adults: A Case–Control Study and Meta-Analysis. Nutrients 2024, 16, 2747. [Google Scholar] [CrossRef] [PubMed]
- Casella, G.; Di Bella, C.; Salemme, M.; Villanacci, V.; Antonelli, E.; Baldini, V.; Bassotti, G. Celiac Disease, Non-Celiac Gluten Sensitivity and Inflammatory Bowel Disease. Minerva Gastroenterol Dietol 2015, 61, 267–271. [Google Scholar] [PubMed]
- Potter, M.D.; Walker, M.M.; Jones, M.P.; Koloski, N.A.; Keely, S.; Talley, N.J. Letter: Gluten Sensitivity in Patients with Inflammatory Bowel Disease. Aliment Pharmacol Ther 2018, 48, 1167–1168. [Google Scholar] [CrossRef]
- Weaver, K.N.; Herfarth, H. Gluten-Free Diet in IBD: Time for a Recommendation? Molecular Nutrition Food Res 2021, 65, 1901274. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Sepulveda, R.; Hing, T.; Shah, N.D.; Choe, M.; Limsui, D.; Shah, S. Prevalence and Factors Associated with Gluten Sensitivity in Inflammatory Bowel Disease. Scandinavian Journal of Gastroenterology 2018, 53, 147–151. [Google Scholar] [CrossRef]
- Herfarth, H.H.; Martin, C.F.; Sandler, R.S.; Kappelman, M.D.; Long, M.D. Prevalence of a Gluten-Free Diet and Improvement of Clinical Symptoms in Patients with Inflammatory Bowel Diseases. Inflammatory Bowel Diseases 2014, 20, 1194–1197. [Google Scholar] [CrossRef]
- Lopes, E.W.; Lebwohl, B.; Burke, K.E.; Ivey, K.L.; Ananthakrishnan, A.N.; Lochhead, P.; Richter, J.M.; Ludvigsson, J.F.; Willett, W.C.; Chan, A.T.; et al. Dietary Gluten Intake Is Not Associated With Risk of Inflammatory Bowel Disease in US Adults Without Celiac Disease. Clinical Gastroenterology and Hepatology 2022, 20, 303–313.e6. [Google Scholar] [CrossRef]
- Wong, C.; Harris, P.; Ferguson, L. Potential Benefits of Dietary Fibre Intervention in Inflammatory Bowel Disease. IJMS 2016, 17, 919. [Google Scholar] [CrossRef]
- Tan, J.K.; Macia, L.; Mackay, C.R. Dietary Fiber and SCFAs in the Regulation of Mucosal Immunity. J Allergy Clin Immunol 2023, 151, 361–370. [Google Scholar] [CrossRef]
- Ferenc, K.; Jarmakiewicz-Czaja, S.; Filip, R. Components of the Fiber Diet in the Prevention and Treatment of IBD—An Update. Nutrients 2022, 15, 162. [Google Scholar] [CrossRef] [PubMed]
- Healey, G.R.; Celiberto, L.S.; Lee, S.M.; Jacobson, K. Fiber and Prebiotic Interventions in Pediatric Inflammatory Bowel Disease: What Role Does the Gut Microbiome Play? Nutrients 2020, 12, 3204. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.; Day, A.; Barrett, J.; Vanlint, A.; Andrews, J.M.; Costello, S.P.; Bryant, R.V. Habitual Dietary Fibre and Prebiotic Intake Is Inadequate in Patients with Inflammatory Bowel Disease: Findings from a Multicentre Cross-sectional Study. J Human Nutrition Diet 2021, 34, 420–428. [Google Scholar] [CrossRef] [PubMed]
- Silveira, A.L.M.; Ferreira, A.V.M.; De Oliveira, M.C.; Rachid, M.A.; Da Cunha Sousa, L.F.; Dos Santos Martins, F.; Gomes-Santos, A.C.; Vieira, A.T.; Teixeira, M.M. Preventive Rather than Therapeutic Treatment with High Fiber Diet Attenuates Clinical and Inflammatory Markers of Acute and Chronic DSS-Induced Colitis in Mice. Eur J Nutr 2017, 56, 179–191. [Google Scholar] [CrossRef]
- Puvvada, S.R.; Luvsannyam, E.; Patel, D.; Hassan, Z.; Hamid, P. Probiotics in Inflammatory Bowel Disease: Are We Back to Square One? Cureus 2020. [Google Scholar] [CrossRef]
- Prisciandaro, L.; Geier, M.; Butler, R.; Cummins, A.; Howarth, G. Probiotics and Their Derivatives as Treatments for Inflammatory Bowel Disease. Inflammatory Bowel Diseases 2009, 15, 1906–1914. [Google Scholar] [CrossRef]
- Gu, Q.; Chen, Z.; Liu, N.; Xia, C.; Zhou, Q.; Li, P. Lactiplantibacillus Plantarum ZJ316–Fermented Milk Ameliorates Dextran Sulfate Sodium–Induced Chronic Colitis by Improving the Inflammatory Response and Regulating Intestinal Microbiota. Journal of Dairy Science 2023, 106, 7352–7366. [Google Scholar] [CrossRef]
- Cristofori, F.; Dargenio, V.N.; Dargenio, C.; Miniello, V.L.; Barone, M.; Francavilla, R. Anti-Inflammatory and Immunomodulatory Effects of Probiotics in Gut Inflammation: A Door to the Body. Front Immunol 2021, 12, 578386. [Google Scholar] [CrossRef]
- Shahbazi, R.; Sharifzad, F.; Bagheri, R.; Alsadi, N.; Yasavoli-Sharahi, H.; Matar, C. Anti-Inflammatory and Immunomodulatory Properties of Fermented Plant Foods. Nutrients 2021, 13, 1516. [Google Scholar] [CrossRef]
- Saez-Lara, M.J.; Gomez-Llorente, C.; Plaza-Diaz, J.; Gil, A. The Role of Probiotic Lactic Acid Bacteria and Bifidobacteria in the Prevention and Treatment of Inflammatory Bowel Disease and Other Related Diseases: A Systematic Review of Randomized Human Clinical Trials. Biomed Res Int 2015, 2015, 505878. [Google Scholar] [CrossRef]
- Nikolova, D. Inflammatory Bowel Disease and Diet: Is There a Place for Probiotics? Galenika Med J 2023, 2, 41–46. [Google Scholar] [CrossRef]
- Akutko, K.; Stawarski, A. Probiotics, Prebiotics and Synbiotics in Inflammatory Bowel Diseases. JCM 2021, 10, 2466. [Google Scholar] [CrossRef] [PubMed]
- Lopes, G.; Sorrentino Dos Santos Campanari, G.; Barbalho, S.M.; Matias, J.N.; Lima, V.M.; Araújo, A.C.; Goulart, R.D.A.; Detregiachi, C.R.P.; Santos Haber, J.F.; Alves De Carvalho, A.C.; et al. Effects of Probiotics on Inflammatory Bowel Disease: A Systematic Review. Japanese J Gastroenterol Res 2021, 1. [Google Scholar] [CrossRef] [PubMed]
- Marton, L.T.; Goulart, R.D.A.; Carvalho, A.C.A.D.; Barbalho, S.M. Omega Fatty Acids and Inflammatory Bowel Diseases: An Overview. IJMS 2019, 20, 4851. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Goulart, R. de A.; Quesada, K.; Bechara, M.D.; de Carvalho, A. de C.A. Inflammatory Bowel Disease: Can Omega-3 Fatty Acids Really Help? Ann Gastroenterol 2016, 29, 37–43. [Google Scholar]
- Astore, C.; Nagpal, S.; Gibson, G. Mendelian Randomization Indicates a Causal Role for Omega-3 Fatty Acids in Inflammatory Bowel Disease. IJMS 2022, 23, 14380. [Google Scholar] [CrossRef]
- Ajabnoor, S.M.; Thorpe, G.; Abdelhamid, A.; Hooper, L. Long-Term Effects of Increasing Omega-3, Omega-6 and Total Polyunsaturated Fats on Inflammatory Bowel Disease and Markers of Inflammation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Eur J Nutr 2021, 60, 2293–2316. [Google Scholar] [CrossRef]
- Farrukh, A. Is There a Role for Fish Oil in Inflammatory Bowel Disease? WJC 2014, 2, 250. [Google Scholar] [CrossRef]
- He, J.; Luo, X.; Xin, H.; Lai, Q.; Zhou, Y.; Bai, Y. The Effects of Fatty Acids on Inflammatory Bowel Disease: A Two-Sample Mendelian Randomization Study. Nutrients 2022, 14, 2883. [Google Scholar] [CrossRef]
- Fu, J.; Chai, C.; Chen, L.; Cai, M.; Ai, B.; Li, H.; Yuan, J.; Lin, H.; Zhang, Z. Associations of Fish and Fish Oil Consumption With Incident Inflammatory Bowel Disease: A Population-Based Prospective Cohort Study. Inflamm Bowel Dis 2024, 30, 1812–1819. [Google Scholar] [CrossRef]
- Farzaei, M.; Rahimi, R.; Abdollahi, M. The Role of Dietary Polyphenols in the Management of Inflammatory Bowel Disease. CPB 2015, 16, 196–210. [Google Scholar] [CrossRef] [PubMed]
- Hanai, H.; Sugimoto, K. Curcumin Has Bright Prospects for the Treatment of Inflammatory Bowel Disease. CPD 2009, 15, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Ye, X.; Huang, Z.; Jiang, S.; Lin, D. Curcumin@Fe/Tannic Acid Complex Nanoparticles for Inflammatory Bowel Disease Treatment. ACS Omega 2024, 9, 14316–14322. [Google Scholar] [CrossRef] [PubMed]
- Vaghari-Tabari, M.; Alemi, F.; Zokaei, M.; Moein, S.; Qujeq, D.; Yousefi, B.; Farzami, P.; Hosseininasab, S.S. Polyphenols and Inflammatory Bowel Disease: Natural Products with Therapeutic Effects? Critical Reviews in Food Science and Nutrition 2024, 64, 4155–4178. [Google Scholar] [CrossRef]
- Liu, F.; Li, D.; Wang, X.; Cui, Y.; Li, X. Polyphenols Intervention Is an Effective Strategy to Ameliorate Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. International Journal of Food Sciences and Nutrition 2021, 72, 14–25. [Google Scholar] [CrossRef]
- Nones, K.; Dommels, Y.E.M.; Martell, S.; Butts, C.; McNabb, W.C.; Park, Z.A.; Zhu, S.; Hedderley, D.; Barnett, M.P.G.; Roy, N.C. The Effects of Dietary Curcumin and Rutin on Colonic Inflammation and Gene Expression in Multidrug Resistance Gene-Deficient ( Mdr1a−/− ) Mice, a Model of Inflammatory Bowel Diseases. Br J Nutr 2008, 101, 169–181. [Google Scholar] [CrossRef]
- Karthikeyan, A.; Young, K.N.; Moniruzzaman, M.; Beyene, A.M.; Do, K.; Kalaiselvi, S.; Min, T. Curcumin and Its Modified Formulations on Inflammatory Bowel Disease (IBD): The Story So Far and Future Outlook. Pharmaceutics 2021, 13, 484. [Google Scholar] [CrossRef]
- Ashton, J.J.; Gavin, J.; Beattie, R.M. Exclusive Enteral Nutrition in Crohn’s Disease: Evidence and Practicalities. Clinical Nutrition 2019, 38, 80–89. [Google Scholar] [CrossRef]
- White, B.; Curle, J.; Gervais, L.; Wands, D.; Nichols, B.; Hansen, R.; Russell, R.K.; Gerasimidis, K.; Milling, S. Exclusive Enteral Nutrition Impacts Peripheral Blood Mononuclear Cell Profile of Children with Crohn’s Disease. J. pediatr. gastroenterol. nutr. 2024, 79, 148–153. [Google Scholar] [CrossRef]
- White, B.; Curle, J.; Gervais, L.; Wands, D.; Nichols, B.; Hansen, R.; Russell, R.; Gerasmidis, K.; Milling, S. P976 Treatment with Exclusive Enteral Nutrition (EEN) Impacts the Peripheral Blood Mononuclear Cell Profile of Paediatric Patients with Crohn’s Disease. Journal of Crohn’s and Colitis 2024, 18, i1769–i1771. [Google Scholar] [CrossRef]
- Day, A.; Wood, J.; Melton, S.; Bryant, R.V. Exclusive Enteral Nutrition: An Optimal Care Pathway for Use in Adult Patients with Active Crohn’s Disease. JGH Open 2020, 4, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Mutsekwa, R.N.; Edwards, J.T.; Angus, R.L. Exclusive Enteral Nutrition in the Management of Crohn’s Disease: A Qualitative Exploration of Experiences, Challenges and Enablers in Adult Patients. J Human Nutrition Diet 2021, 34, 440–449. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Wu, R.; Zhu, W.; Gong, J.; Zhang, W.; Li, Y.; Gu, L.; Li, N.; Li, J. Effect of Exclusive Enteral Nutrition on Health-Related Quality of Life for Adults With Active Crohn’s Disease. Nut in Clin Prac 2013, 28, 499–505. [Google Scholar] [CrossRef] [PubMed]
- Wall, C.L.; McCombie, A.; Mulder, R.; Day, A.S.; Gearry, R.B. Adherence to Exclusive Enteral Nutrition by Adults with Active Crohn’s Disease Is Associated with Conscientiousness Personality Trait: A Sub-Study. Journal of Human Nutrition and Dietetics 2020, 33, 752–757. [Google Scholar] [CrossRef]
- González-Torres, L.; Moreno-Álvarez, A.; Fernández-Lorenzo, A.E.; Leis, R.; Solar-Boga, A. The Role of Partial Enteral Nutrition for Induction of Remission in Crohn’s Disease: A Systematic Review of Controlled Trials. Nutrients 2022, 14, 5263. [Google Scholar] [CrossRef]
- Luo, C.; Wang, Z.; Mu, J.; Zhu, M.; Zhen, Y.; Zhang, H. Upregulation of the Transient Receptor Potential Vanilloid 1 in Colonic Epithelium of Patients with Active Inflammatory Bowel Disease. Int J Clin Exp Pathol 2017, 10, 11335–11344. [Google Scholar]
- Xiang, Y.; Xu, X.; Zhang, T.; Wu, X.; Fan, D.; Hu, Y.; Ding, J.; Yang, X.; Lou, J.; Du, Q.; et al. Beneficial Effects of Dietary Capsaicin in Gastrointestinal Health and Disease. Experimental Cell Research 2022, 417, 113227. [Google Scholar] [CrossRef]
- Chen, Y.; Ma, C.; Dang, Y.; Chen, K.; Shen, S.; Jiang, M.; Zeng, Z.; Zhang, H. P082 Spicy Food Is a Vital Trigger for Relapse in Patient with Inflammatory Bowel Disease. Journal of Crohn’s and Colitis 2020, 14, S176–S176. [Google Scholar] [CrossRef]
- Rosca, A.E.; Iesanu, M.I.; Zahiu, C.D.M.; Voiculescu, S.E.; Paslaru, A.C.; Zagrean, A.-M. Capsaicin and Gut Microbiota in Health and Disease. Molecules 2020, 25, 5681. [Google Scholar] [CrossRef]
- Li, J.; Wang, H.; Zhang, L.; An, N.; Ni, W.; Gao, Q.; Yu, Y. Capsaicin Affects Macrophage Anti-Inflammatory Activity via the MAPK and NF-κB Signaling Pathways. International Journal for Vitamin and Nutrition Research 2023, 93, 289–297. [Google Scholar] [CrossRef]
- Vasudevan, J.; DiVincenzo, C.; Feagins, L.A. Optimizing Nutrition to Enhance the Treatment of Patients With Inflammatory Bowel Disease. Gastroenterol Hepatol (N Y) 2022, 18, 95–103. [Google Scholar] [PubMed]
- Rondanelli, M.; Lamburghini, S.; Faliva, M.A.; Peroni, G.; Riva, A.; Allegrini, P.; Spadaccini, D.; Gasparri, C.; Iannello, G.; Infantino, V.; et al. A Food Pyramid, Based on a Review of the Emerging Literature, for Subjects with Inflammatory Bowel Disease. Endocrinología, Diabetes y Nutrición 2021, 68, 17–46. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, U.; Romano, C.; Dipasquale, V. Diet and Nutrition in Pediatric Inflammatory Bowel Diseases. Nutrients 2021, 13, 655. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, K.; Kamada, N. Diet–Microbiota Interactions in Inflammatory Bowel Disease. Nutrients 2021, 13, 1533. [Google Scholar] [CrossRef]
- Bian, D.; Shi, Y.; Jiang, Y.; Zhong, J.; Sun, J.; Gu, Y. Combined Patient-Generated Subjective Global Assessment and Body Composition Facilitates Nutritional Support in Inflammatory Bowel Disease: An Ambulatory Study in Shanghai. Asia Pacific Journal of Clinical Nutrition 2018, 27. [Google Scholar] [CrossRef]
- Sood, A.; Ahuja, V.; Kedia, S.; Midha, V.; Mahajan, R.; Mehta, V.; Sudhakar, R.; Singh, A.; Kumar, A.; Puri, A.S.; et al. Diet and Inflammatory Bowel Disease: The Asian Working Group Guidelines. Indian J Gastroenterol 2019, 38, 220–246. [Google Scholar] [CrossRef]
- Park, J.; Cheon, J.H. Incidence and Prevalence of Inflammatory Bowel Disease across Asia. Yonsei Med J 2021, 62, 99. [Google Scholar] [CrossRef]
- Mijan, M.A.; Lim, B.O. Diets, Functional Foods, and Nutraceuticals as Alternative Therapies for Inflammatory Bowel Disease: Present Status and Future Trends. WJG 2018, 24, 2673–2685. [Google Scholar] [CrossRef]
- Crooks, B.; Misra, R.; Arebi, N.; Kok, K.; Brookes, M.J.; McLaughlin, J.; Limdi, J.K. The Dietary Practices and Beliefs of British South Asian People Living with Inflammatory Bowel Disease: A Multicenter Study from the United Kingdom. Intest Res 2022, 20, 53–63. [Google Scholar] [CrossRef]
- Feng, Z.; Li, T.; Wu, C.; Tao, L.; Blachier, F.; Yin, Y. Monosodium L-Glutamate and Dietary Fat Exert Opposite Effects on the Proximal and Distal Intestinal Health in Growing Pigs. Appl. Physiol. Nutr. Metab. 2015, 40, 353–363. [Google Scholar] [CrossRef]
- Ghishan, F.K.; Kiela, P.R. Vitamins and Minerals in IBD. Gastroenterol Clin North Am 2017, 46, 797–808. [Google Scholar] [CrossRef] [PubMed]
- Parizadeh, S.M.; Jafarzadeh-Esfehani, R.; Hassanian, S.M.; Mottaghi-Moghaddam, A.; Ghazaghi, A.; Ghandehari, M.; Alizade-Noghani, M.; Khazaei, M.; Ghayour-Mobarhan, M.; Ferns, G.A.; et al. Vitamin D in Inflammatory Bowel Disease: From Biology to Clinical Implications. Complementary Therapies in Medicine 2019, 47, 102189. [Google Scholar] [CrossRef]
- Alhassan Mohammed, H.; Mirshafiey, A.; Vahedi, H.; Hemmasi, G.; Moussavi Nasl Khameneh, A.; Parastouei, K.; Saboor-Yaraghi, A.A. Immunoregulation of Inflammatory and Inhibitory Cytokines by Vitamin D3 in Patients with Inflammatory Bowel Diseases. Scandinavian Journal of Immunology 2017, 85, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Gold, S.L.; Manning, L.; Kohler, D.; Ungaro, R.; Sands, B.; Raman, M. Micronutrients and Their Role in Inflammatory Bowel Disease: Function, Assessment, Supplementation, and Impact on Clinical Outcomes Including Muscle Health. Inflammatory Bowel Diseases 2023, 29, 487–501. [Google Scholar] [CrossRef] [PubMed]
- Alkhouri, R.H.; Hashmi, H.; Baker, R.D.; Gelfond, D.; Baker, S.S. Vitamin and Mineral Status in Patients With Inflammatory Bowel Disease. J. pediatr. gastroenterol. nutr. 2013, 56, 89–92. [Google Scholar] [CrossRef]
- Nakajima, S.; Iijima, H.; Egawa, S.; Shinzaki, S.; Kondo, J.; Inoue, T.; Hayashi, Y.; Ying, J.; Mukai, A.; Akasaka, T.; et al. Association of Vitamin K Deficiency with Bone Metabolism and Clinical Disease Activity in Inflammatory Bowel Disease. Nutrition 2011, 27, 1023–1028. [Google Scholar] [CrossRef]
- Laheij, R.L.H.; Van Knippenberg, Y.M.W.; Heil, A.L.J.; Mannaerts, B.J.W.; Bruin, K.F.; Lutgens, M.W.M.D.; Sikkema, M.; De Wit, U.; Laheij, R.J.F. The Efficacy of an Over-the-Counter Multivitamin and Mineral Supplement to Prevent Infections in Patients With Inflammatory Bowel Disease in Remission With Immunomodulators and/or Biological Agents: A Randomized, Double-Blind, Placebo-Controlled Clinical Trial. Inflammatory Bowel Diseases 2024, 30, 1510–1516. [Google Scholar] [CrossRef]
- Greenley, R.N.; Stephens, K.A.; Nguyen, E.U.; Kunz, J.H.; Janas, L.; Goday, P.; Schurman, J.V. Vitamin and Mineral Supplement Adherence in Pediatric Inflammatory Bowel Disease. Journal of Pediatric Psychology 2013, 38, 883–892. [Google Scholar] [CrossRef]
- Kempinski, R.; Arabasz, D.; Neubauer, K. Effects of Milk and Dairy on the Risk and Course of Inflammatory Bowel Disease versus Patients’ Dietary Beliefs and Practices: A Systematic Review. Nutrients 2024, 16, 2555. [Google Scholar] [CrossRef]
- Opstelten, J.L.; Leenders, M.; Dik, V.K.; Chan, S.S.M.; Van Schaik, F.D.M.; Khaw, K.-T.; Luben, R.; Hallmans, G.; Karling, P.; Lindgren, S.; et al. Dairy Products, Dietary Calcium, and Risk of Inflammatory Bowel Disease: Results From a European Prospective Cohort Investigation. Inflammatory Bowel Diseases 2016, 22, 1403–1411. [Google Scholar] [CrossRef]
- Ratajczak, A.E.; Zawada, A.; Rychter, A.M.; Dobrowolska, A.; Krela-Kaźmierczak, I. Milk and Dairy Products: Good or Bad for Human Bone? Practical Dietary Recommendations for the Prevention and Management of Osteoporosis. Nutrients 2021, 13, 1329. [Google Scholar] [CrossRef] [PubMed]
- Wellens, J.; Vissers, E.; Matthys, C.; Vermeire, S.; Sabino, J. Personalized Dietary Regimens for Inflammatory Bowel Disease: Current Knowledge and Future Perspectives. PGPM 2023, Volume 16, 15–27. [Google Scholar] [CrossRef]
- Collins, C.B.; Roche, H.M. Personalized Nutrition for Inflammatory Bowel Disease. Crohn’s & Colitis 360 2020, 2, otaa042. [Google Scholar] [CrossRef]
- Yamamoto, T.; Shimoyama, T. Nutrition and Diet in Inflammatory Bowel Disease. Current Opinion in Gastroenterology 2023, 39, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Jarmakiewicz-Czaja, S.; Zielińska, M.; Sokal, A.; Filip, R. Genetic and Epigenetic Etiology of Inflammatory Bowel Disease: An Update. Genes (Basel) 2022, 13, 2388. [Google Scholar] [CrossRef]
- Mokhtari, Z.; Hekmatdoost, A. Dietary Interventions and Inflammatory Bowel Disease. In Dietary Interventions in Gastrointestinal Diseases; Elsevier, 2019; pp. 33–42 ISBN 978-0-12-814468-8.
- Gleave, A.; Shah, A.; Tahir, U.; Blom, J.-J.; Dong, E.; Patel, A.; Marshall, J.K.; Narula, N. Using Diet to Treat Inflammatory Bowel Disease: A Systematic Review. Am J Gastroenterol 2025, 120, 83–97. [Google Scholar] [CrossRef]
- Kakodkar, S.; Mutlu, E.A. Diet as a Therapeutic Option for Adult Inflammatory Bowel Disease. Gastroenterol Clin North Am 2017, 46, 745–767. [Google Scholar] [CrossRef]
- Kakodkar, S.; Farooqui, A.J.; Mikolaitis, S.L.; Mutlu, E.A. The Specific Carbohydrate Diet for Inflammatory Bowel Disease: A Case Series. Journal of the Academy of Nutrition and Dietetics 2015, 115, 1226–1232. [Google Scholar] [CrossRef]
- Ratajczak, A.E.; Festa, S.; Aratari, A.; Papi, C.; Dobrowolska, A.; Krela-Kaźmierczak, I. Should the Mediterranean Diet Be Recommended for Inflammatory Bowel Diseases Patients? A Narrative Review. Front. Nutr. 2023, 9, 1088693. [Google Scholar] [CrossRef]
- Migdanis, A.; Migdanis, I.; Gkogkou, N.D.; Papadopoulou, S.K.; Giaginis, C.; Manouras, A.; Polyzou Konsta, M.A.; Kosti, R.I.; Oikonomou, K.A.; Argyriou, K.; et al. The Relationship of Adherence to the Mediterranean Diet with Disease Activity and Quality of Life in Crohn’s Disease Patients. Medicina (Kaunas) 2024, 60, 1106. [Google Scholar] [CrossRef]
- Sigall Boneh, R.; Assa, A.; Lev-Tzion, R.; Matar, M.; Shouval, D.; Shubeli, C.; Tsadok Perets, T.; Chodick, G.; Shamir, R. Adherence to the Mediterranean Diet Is Associated with Decreased Fecal Calprotectin Levels in Children with Crohn’s Disease in Clinical Remission under Biological Therapy. Dig Dis 2024, 42, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, N.R.M.; McNichol, S.R.; Devine, B.; Phipps, A.I.; Roth, J.A.; Suskind, D.L. Assessing Barriers to Use of the Specific Carbohydrate Diet in Pediatric Inflammatory Bowel Disease: A Qualitative Study. JPGN Rep 2022, 3, e239. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Zhuge, A.; Wang, K.; Lv, L.; Bian, X.; Yang, L.; Xia, J.; Jiang, X.; Wu, W.; Wang, S.; et al. Ketogenic Diet Aggravates Colitis, Impairs Intestinal Barrier and Alters Gut Microbiota and Metabolism in DSS-Induced Mice. Food Funct. 2021, 12, 10210–10225. [Google Scholar] [CrossRef] [PubMed]
- Kong, C.; Yan, X.; Liu, Y.; Huang, L.; Zhu, Y.; He, J.; Gao, R.; Kalady, M.F.; Goel, A.; Qin, H.; et al. Ketogenic Diet Alleviates Colitis by Reduction of Colonic Group 3 Innate Lymphoid Cells through Altering Gut Microbiome. Sig Transduct Target Ther 2021, 6, 154. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The Therapeutic Role of Short-Chain Fatty Acids Mediated Very Low-Calorie Ketogenic Diet–Gut Microbiota Relationships in Paediatric Inflammatory Bowel Diseases. Nutrients 2022, 14, 4113. [Google Scholar] [CrossRef]
- Norwitz, N.G.; Soto-Mota, A. Case Report: Carnivore–Ketogenic Diet for the Treatment of Inflammatory Bowel Disease: A Case Series of 10 Patients. Front Nutr 2024, 11, 1467475. [Google Scholar] [CrossRef]
- Luiskari, L.; Lindén, J.; Lehto, M.; Salmenkari, H.; Korpela, R. Ketogenic Diet Protects from Experimental Colitis in a Mouse Model Regardless of Dietary Fat Source. Nutrients 2024, 16, 1348. [Google Scholar] [CrossRef]
- Lavallee, C.M.; Bruno, A.; Ma, C.; Raman, M. A Review of the Role of Intermittent Fasting in the Management of Inflammatory Bowel Disease. Therap Adv Gastroenterol 2023, 16, 17562848231171756. [Google Scholar] [CrossRef]
- Roco-Videla, Á.; Villota-Arcos, C.; Pino-Astorga, C.; Mendoza-Puga, D.; Bittner-Ortega, M.; Corbeaux-Ascui, T. Intermittent Fasting and Reduction of Inflammatory Response in a Patient with Ulcerative Colitis. Medicina 2023, 59, 1453. [Google Scholar] [CrossRef]
- Rangan, P.; Choi, I.; Wei, M.; Navarrete, G.; Guen, E.; Brandhorst, S.; Enyati, N.; Pasia, G.; Maesincee, D.; Ocon, V.; et al. Fasting-Mimicking Diet Modulates Microbiota and Promotes Intestinal Regeneration to Reduce Inflammatory Bowel Disease Pathology. Cell Reports 2019, 26, 2704–2719.e6. [Google Scholar] [CrossRef]
- Song, S.; Bai, M.; Ling, Z.; Lin, Y.; Wang, S.; Chen, Y. Intermittent Administration of a Fasting-Mimicking Diet Reduces Intestinal Inflammation and Promotes Repair to Ameliorate Inflammatory Bowel Disease in Mice. The Journal of Nutritional Biochemistry 2021, 96, 108785. [Google Scholar] [CrossRef] [PubMed]
- Bonsack, O.; Caron, B.; Baumann, C.; Heba, A.C.; Vieujean, S.; Arnone, D.; Netter, P.; Danese, S.; Quilliot, D.; Peyrin-Biroulet, L. Food Avoidance and Fasting in Patients with Inflammatory Bowel Disease: Experience from the Nancy IBD Nutrition Clinic. UEG Journal 2023, 11, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Tavakkoli, H.; Haghdani, S.; Emami, M.H.; Adilipour, H.; Tavakkoli, M.; Tavakkoli, M. Ramadan Fasting and Inflammatory Bowel Disease. Indian J Gastroenterol 2008, 27, 239–241. [Google Scholar] [PubMed]
- Tibi, S.; Ahmed, S.; Nizam, Y.; Aldoghmi, M.; Moosa, A.; Bourenane, K.; Yakub, M.; Mohsin, H. Implications of Ramadan Fasting in the Setting of Gastrointestinal Disorders. Cureus 2023. [Google Scholar] [CrossRef]
- Ebrahimi, S.; Rahmani, F.; Avan, A.; Nematy, M.; Parizadeh, S.M.; Hasanian Mehr, S.M.; Parizadeh, S.M.R. Effects of Ramadan Fasting on the Regulation of Inflammation. JFH 2016, 4. [Google Scholar] [CrossRef]
- Sadeghpour, S.; Hassanzadeh Keshteli, A.; Daneshpajouhnejad, P.; Jahangiri, P.; Adibi, P. Ramadan Fasting and Digestive Disorders: SEPAHAN Systematic Review No. 7. Journal of Research in Medical Sciences 2012, 17, S150–S158. [Google Scholar]
- Day, A.S.; Ballard, T.M.; Yao, C.K.; Gibson, P.R.; Bryant, R.V. Food-Based Interventions as Therapy for Inflammatory Bowel Disease: Important Steps in Diet Trial Design and Reporting of Outcomes. Inflammatory Bowel Diseases 2024, izae185. [Google Scholar] [CrossRef]
- Saeed, S.; Ekhator, C.; Abdelaziz, A.M.; Naveed, H.; Karski, A.; Cook, D.E.; Reddy, S.M.; Affaf, M.; Khan, S.J.; Bellegarde, S.B.; et al. Revolutionizing Inflammatory Bowel Disease Management: A Comprehensive Narrative Review of Innovative Dietary Strategies and Future Directions. Cureus 2023. [Google Scholar] [CrossRef]
- Green, N.; Miller, T.; Suskind, D.; Lee, D. A Review of Dietary Therapy for IBD and a Vision for the Future. Nutrients 2019, 11, 947. [Google Scholar] [CrossRef]
- Barros, V.J.D.S.; Severo, J.S.; Mendes, P.H.M.; Da Silva, A.C.A.; De Oliveira, K.B.V.; Parente, J.M.L.; Lima, M.M.; Neto, E.M.M.; Aguiar Dos Santos, A.; Tolentino Bento Da Silva, M. Effect of Dietary Interventions on Inflammatory Biomarkers of Inflammatory Bowel Diseases: A Systematic Review of Clinical Trials. Nutrition 2021, 91–92, 111457. [Google Scholar] [CrossRef]
- Reznikov, E.A.; Suskind, D.L. Current Nutritional Therapies in Inflammatory Bowel Disease: Improving Clinical Remission Rates and Sustainability of Long-Term Dietary Therapies. Nutrients 2023, 15, 668. [Google Scholar] [CrossRef]
- Olendzki, B.; Bucci, V.; Cawley, C.; Maserati, R.; McManus, M.; Olednzki, E.; Madziar, C.; Chiang, D.; Ward, D.V.; Pellish, R.; et al. Dietary Manipulation of the Gut Microbiome in Inflammatory Bowel Disease Patients: Pilot Study. Gut Microbes 2022, 14, 2046244. [Google Scholar] [CrossRef]
Figure 1.
Immune dysregulation and increased intestinal permeability in inflammatory bowel disease. On the left, the normal intestinal environment maintains homeostasis through a balanced interaction between immune cells, regulatory T cells, and anti-inflammatory cytokines (TGF-β, IL-10). The intestinal epithelial barrier remains intact, preventing bacterial invasion and inflammation. On the right, in IBD, there is a loss of the protective mucus layer, leading to increased epithelial permeability and bacterial entry. This triggers an immune dysregulation, where elevated pro-inflammatory cytokines (TNF-α, IL-12, IL-23) drive an overactive immune response. The recruitment of immune cells, including activated macrophages and neutrophils, sustains a chronic inflammatory cycle. This results in an expanded lamina propria, excessive chemokine and cytokine production, and ongoing intestinal damage. This dysregulated immune response underlies the chronic inflammation characteristic of IBD, contributing to disease progression and symptoms.
Figure 1.
Immune dysregulation and increased intestinal permeability in inflammatory bowel disease. On the left, the normal intestinal environment maintains homeostasis through a balanced interaction between immune cells, regulatory T cells, and anti-inflammatory cytokines (TGF-β, IL-10). The intestinal epithelial barrier remains intact, preventing bacterial invasion and inflammation. On the right, in IBD, there is a loss of the protective mucus layer, leading to increased epithelial permeability and bacterial entry. This triggers an immune dysregulation, where elevated pro-inflammatory cytokines (TNF-α, IL-12, IL-23) drive an overactive immune response. The recruitment of immune cells, including activated macrophages and neutrophils, sustains a chronic inflammatory cycle. This results in an expanded lamina propria, excessive chemokine and cytokine production, and ongoing intestinal damage. This dysregulated immune response underlies the chronic inflammation characteristic of IBD, contributing to disease progression and symptoms.
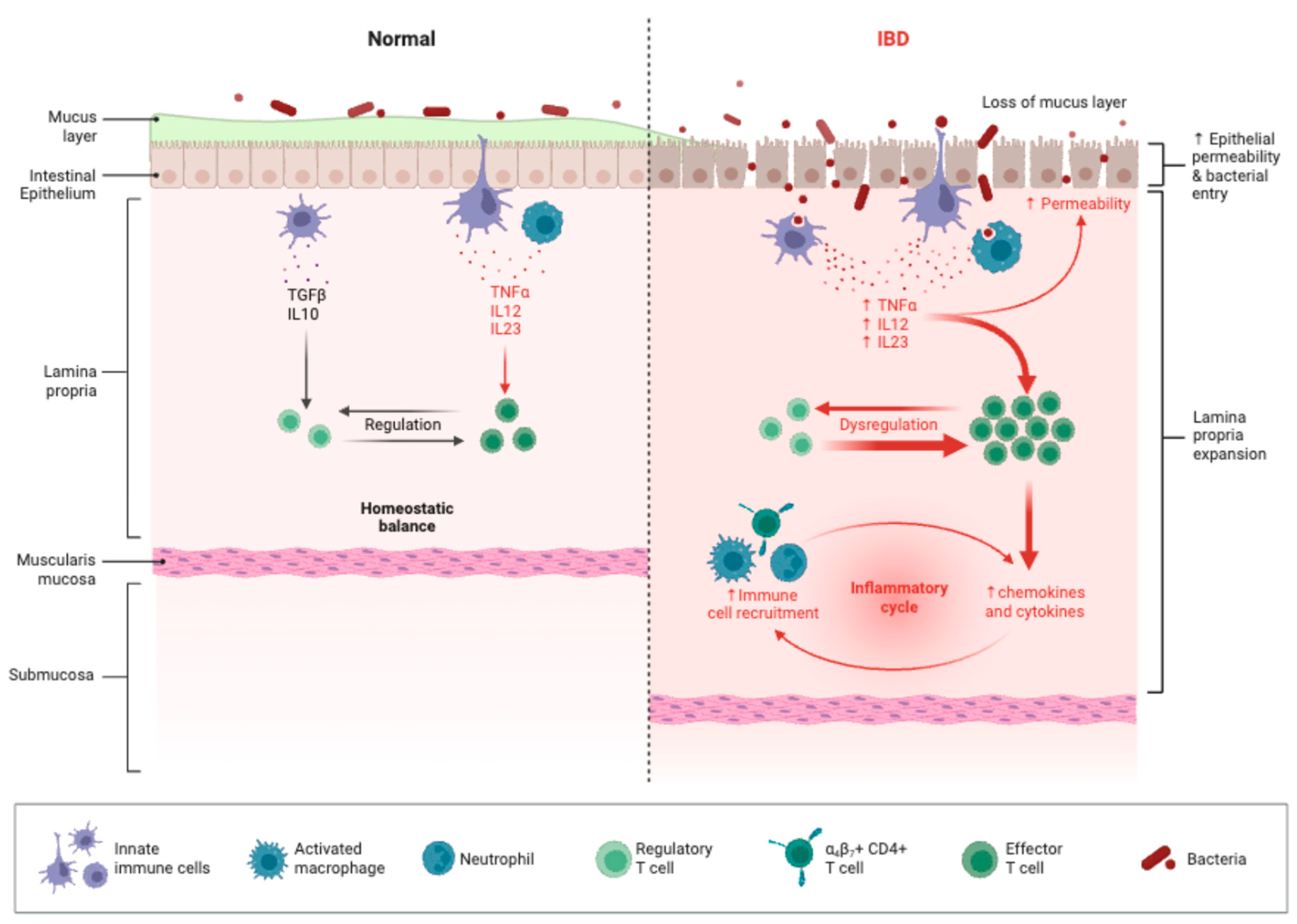
Figure 2.
The IBD food pyramid. The IBD food pyramid provides guidance on a balanced diet tailored for individuals managing inflammatory bowel disease. The foundation of this pyramid consists of vegetables, salad, and fruits, recommending at least five portions per day to ensure a high intake of essential vitamins, minerals, and fiber. These foods support overall gut health while reducing inflammation. This pyramid serves as a general guideline, and dietary needs may vary depending on individual tolerance and specific IBD conditions. It is always recommended to consult a healthcare provider or a registered dietitian for personalized advice.
Figure 2.
The IBD food pyramid. The IBD food pyramid provides guidance on a balanced diet tailored for individuals managing inflammatory bowel disease. The foundation of this pyramid consists of vegetables, salad, and fruits, recommending at least five portions per day to ensure a high intake of essential vitamins, minerals, and fiber. These foods support overall gut health while reducing inflammation. This pyramid serves as a general guideline, and dietary needs may vary depending on individual tolerance and specific IBD conditions. It is always recommended to consult a healthcare provider or a registered dietitian for personalized advice.
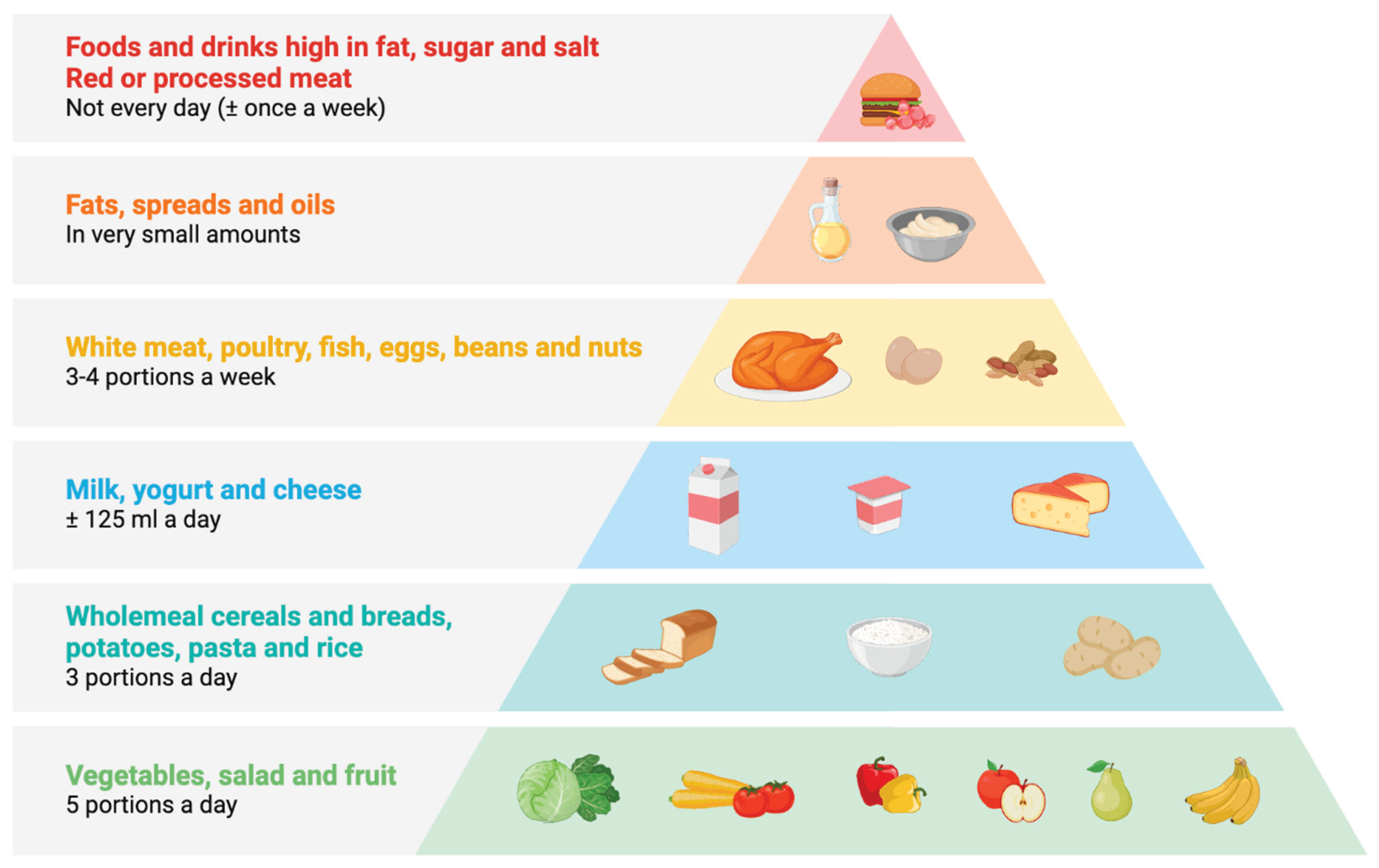

Table 1.
Gut microbiota in IBD and associated immune mechanisms.
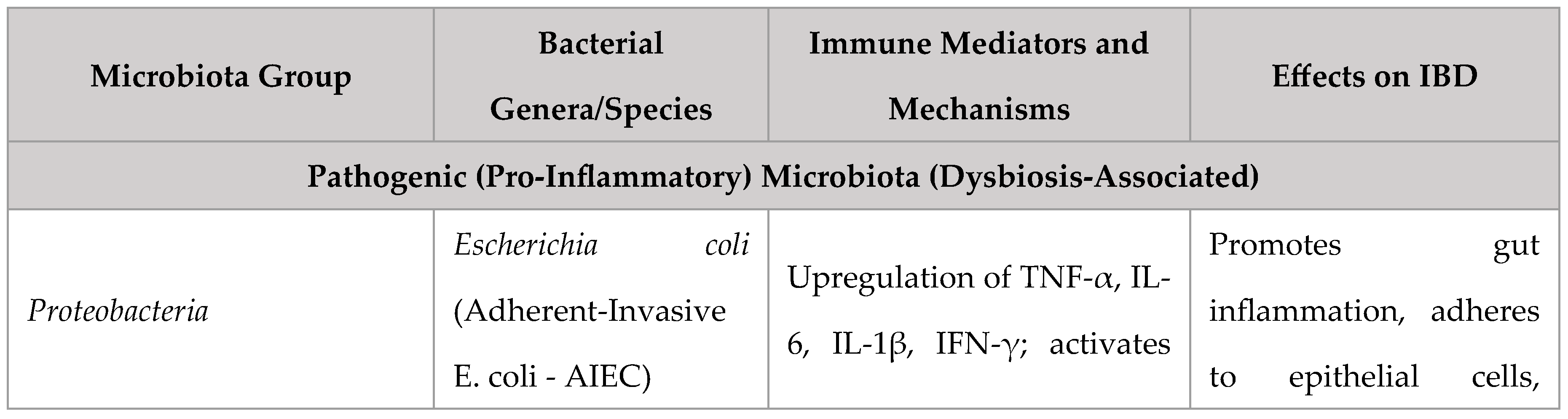
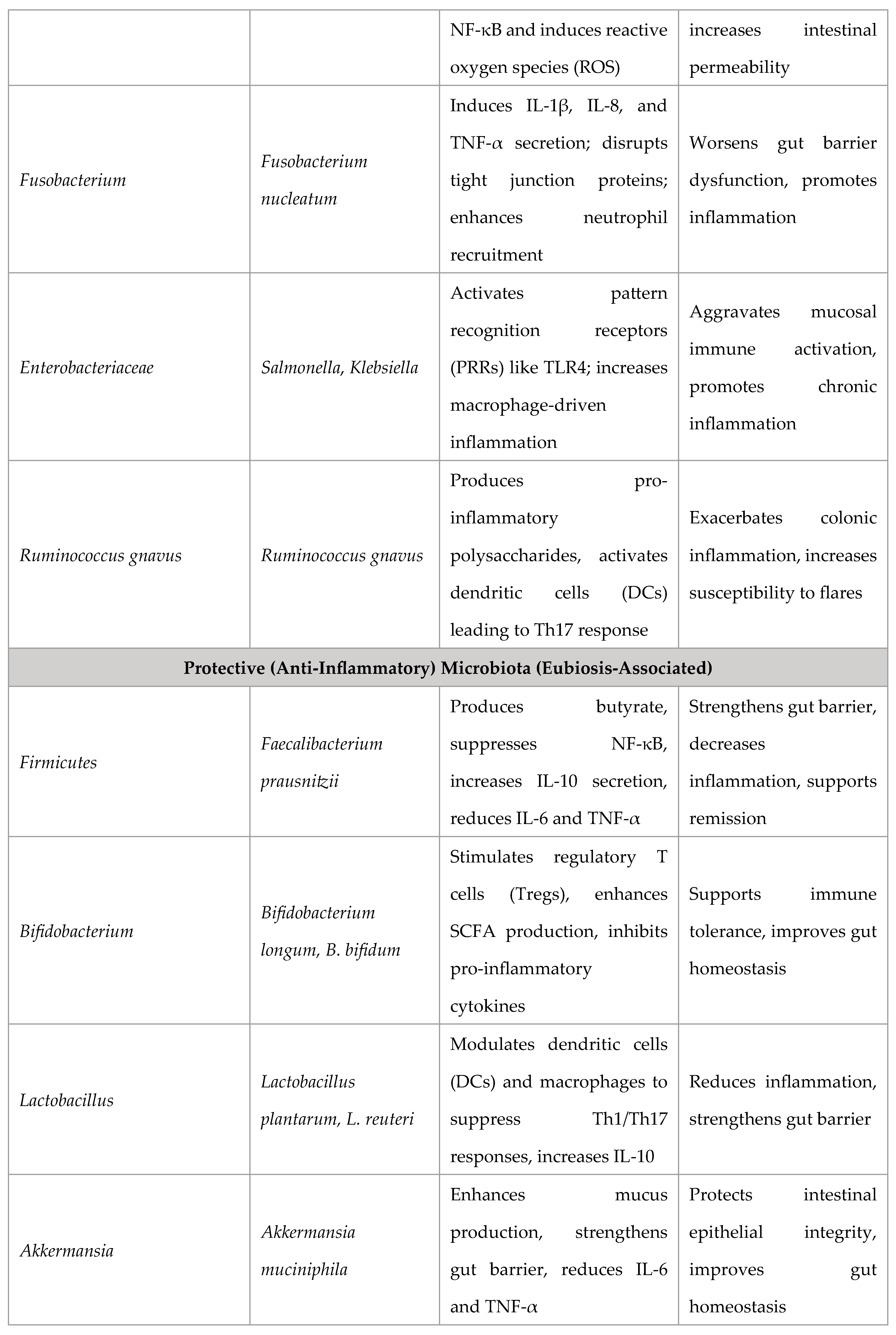
Table 2.
Prohibited dietary components for IBD patients.
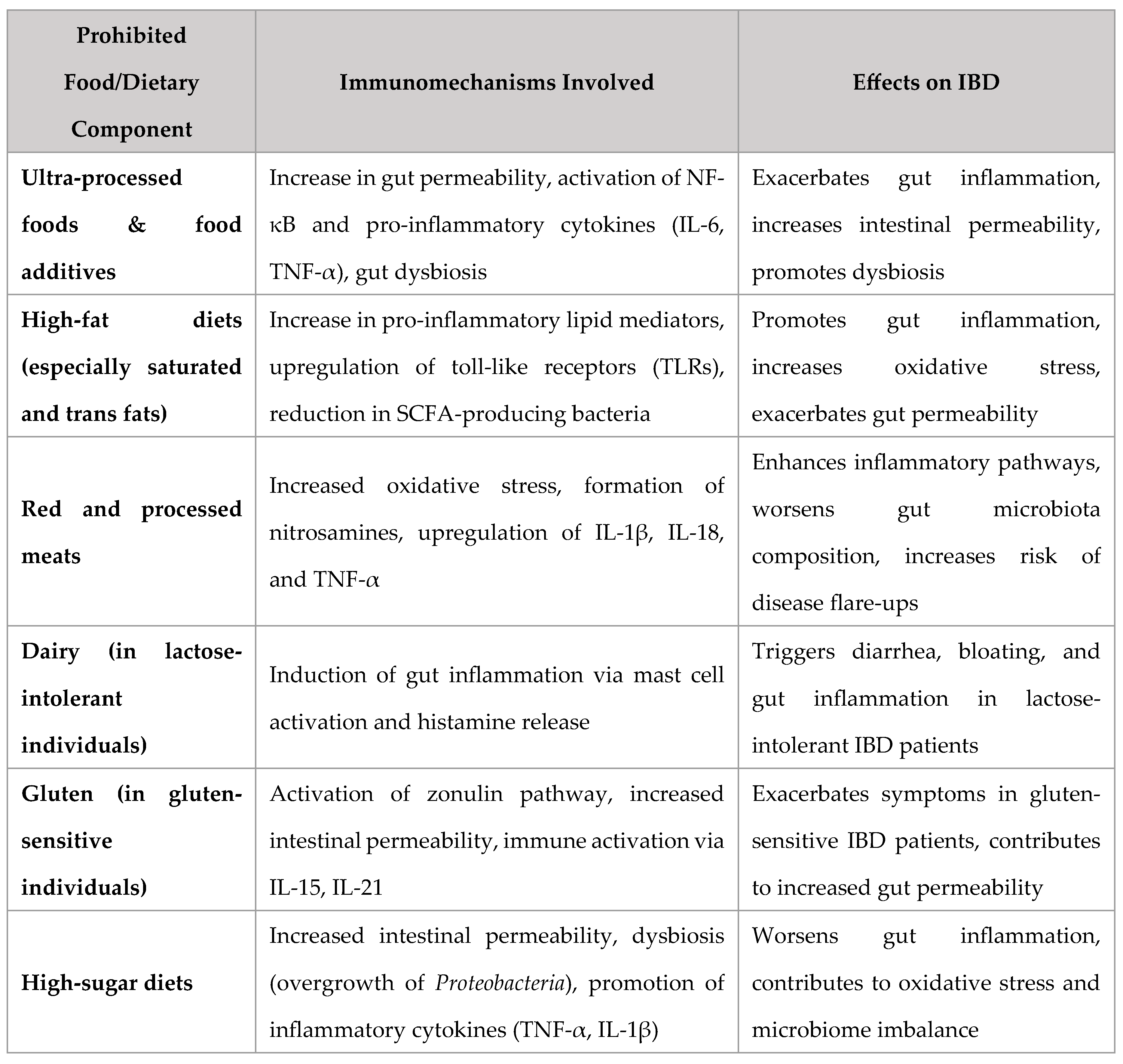
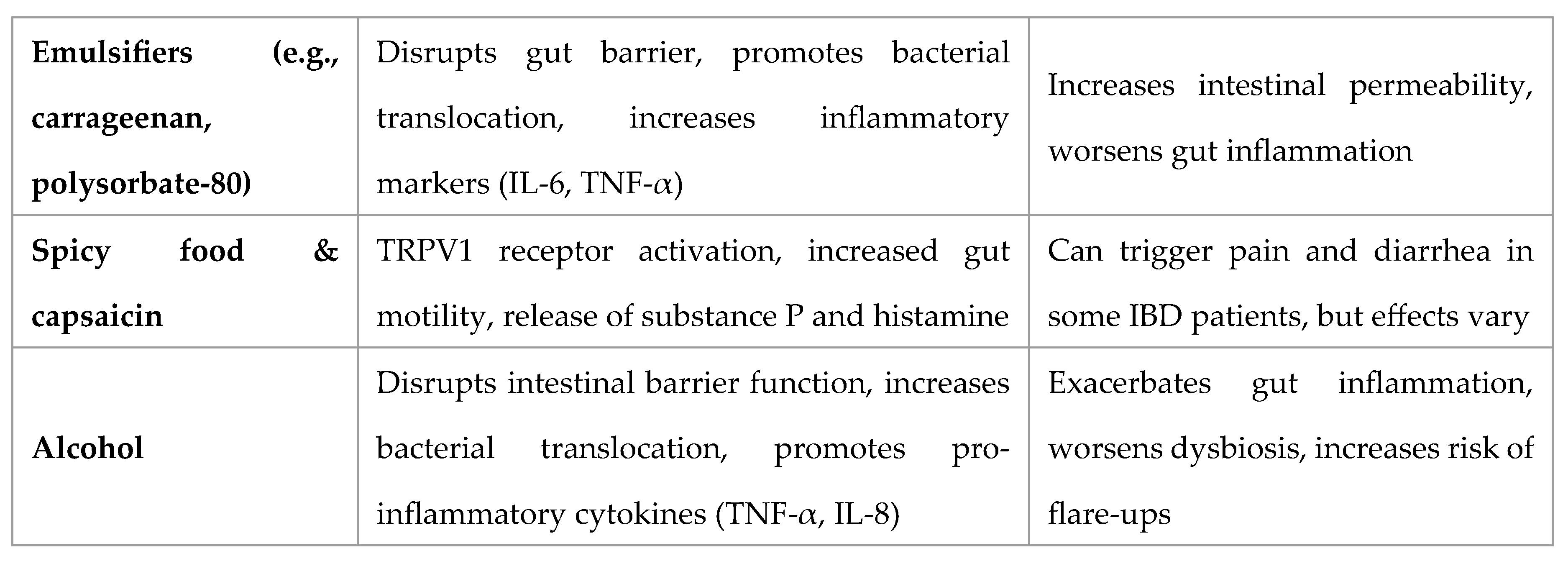
Table 3.
Recommended dietary components for IBD patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



