
Submitted:
25 May 2025
Posted:
26 May 2025
You are already at the latest version
Abstract
Background Pancreatic neuroendocrine tumors (PanNETs) are relatively rare neoplasms with heterogeneous behavior, ranging from indolent to aggressive disease. The evolution of nuclear medicine has allowed the development of an efficient and advanced toolkit for the diagnosis and treatment of PanNETs. Case A 45-year-old woman was diagnosed with Grade 1 PanNET and multiple liver metastases. She underwent distal pancreatectomy with splenectomy, extended liver resection, and radiofrequency ablation (RFA). Surgical planning was guided by [99mTc]-EDDA/HYNIC-TOC SPECT/CT and preoperative [99mTc]Tc-mebrofenin-based functional liver volumetry. Functional liver volumetry based on dynamic [99mTc]Tc-mebrofenin SPECT/CT facilitated precise surgical planning and reliable assessment of the efficacy of parenchymal modulation, thereby aiding in the prevention of post-hepatectomy liver failure. Liver fibrosis was non-invasively evaluated using two-dimensional shear wave elastography (2D-SWE). Tumor progression was monitored using somatostatin receptor scintigraphy, chromogranin A, and contrast-enhanced CT. Recurrent disease was treated with somatostatin analogues (SSA) and [177Lu]-DOTATATE peptide receptor radionuclide therapy (PRRT). Despite progression to Grade 3 disease (Ki-67 from 1% to 30%), the patient remains alive 53 months post-diagnosis, in complete remission, with an ECOG (Eastern Cooperative Oncology Group) status of 0. Conclusion Functional imaging played a pivotal role in guiding therapeutic decisions throughout the disease course. This case not only underscores the clinical utility of advanced nuclear imaging but also illustrates the dynamic nature of pancreatic neuroendocrine tumors. The transition from low-grade to high-grade disease highlights the need for further studies on tumor progression mechanisms and the potential role of adjuvant therapies in managing PanNETs.
Keywords:
Pancreatic neuroendocrine tumor
; Clinical challenges
; Personalized oncology
; Functional volumetry
; Peptide receptor radionuclide therapy
; Hepatectomy
; Somatostatin receptor scintigraphy
Introduction
Neuroendocrine neoplasms (NENs) originate from the diffuse neuroendocrine cell system and can develop in various locations throughout the body. Gastroenteropancreatic neuroendocrine tumors (GEP-NETs) represent a heterogeneous and rare group of neoplasms. Their incidence has increased in recent decades, largely due to advancements in imaging techniques. In Europe, GEP-NETs are now estimated to occur in 1.33 to 2.33 cases per 100,000 individuals [1,2,3].
Pancreatic neuroendocrine tumors (PanNETs) are relatively rare, accounting for approximately 2% of all pancreatic tumors. [4,5] While histological differentiation of NETs does not always predict their clinical behavior, even small, low-grade (grade 1 or 2) PanNETs can spread to the liver or lymph nodes [6].
According to the European Society of Medical Oncology (ESMO) guidelines, surgical intervention is the preferred treatment for resectable PanNETs [5]. Curative resection (R0 or R1) is associated with a 5-year overall survival (OS) rate of approximately 85% [7]. In some cases, combining surgical resection with radiofrequency ablation (RFA) can enable the complete removal of tumors in areas inaccessible by surgery alone [5]. However, in cases requiring major liver resection, meticulous attention is essential to ensure patient safety. Posthepatectomy liver failure (PHLF) remains a significant cause of severe morbidity, with reported incidence rates ranging from 9% to 30% [8]. Preoperative assessment of liver function is crucial for identifying patients at increased risk of posthepatectomy liver failure (PHLF). The E-AHPBA–ESSO–ESSR Innsbruck consensus guidelines recommend evaluating both global liver function and the volumetric and functional fraction of the future liver remnant (FLR) prior to surgery. Several clinical scoring systems are used to assess global liver function, including the MELD-Na score (Model for End-Stage Liver Disease), APRI score (AST to Platelet Ratio Index), CTP score (Child-Turcotte-Pugh score), and the ICG (indocyanine green) clearance test. CT volumetry is commonly employed to determine the volumetric FLR fraction. Additionally, 2D ultrasound shear wave elastography (SWE) provides a non-invasive method for evaluating liver stiffness and assessing the degree of fibrosis [9]. [99mTc]Tc-mebrofenin SPECT/CT offers the advantage of providing simultaneous volumetric and quantitative functional information. However, its use remains limited to a small number of specialized centers [8].
Currently, no data in the literature supports the use of adjuvant therapy for grade 1 (G1) or grade 2 (G2) NETs, as prospective clinical studies are lacking. Medical therapy is recommended based on established guidelines to manage tumor-associated symptoms and control tumor growth. Somatostatin analogues (SSAs) serve as antiproliferative agents in metastatic PanNETs. In cases of progressive disease, peptide receptor radionuclide therapy (PRRT) with [177Lu]-DOTATATE may be considered, as outlined by the ESMO guidelines, to improve symptoms. PRRT is specifically indicated for progressive somatostatin receptor (SSTR)-positive NETs with homogenous SSTR expression, confirmed through SSTR imaging [5].
In this case report, we present the multidisciplinary management of a PanNET, utilizing some less commonly applied methods in clinical practice.
The Case
Diagnostic Procedures
In autumn 2020, a 45-year-old female patient underwent evaluation for nonspecific abdominal complaints. An abdominal ultrasound revealed multiple hepatic nodules and a lesion in the pancreatic tail. On September 16, 2020, an abdominal CT scan confirmed the presence of a mass in the pancreatic tail along with multiple liver metastases. Endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) was performed on the pancreatic tail lesion, with additional biopsies taken from a peripancreatic lymph node and liver metastases. Histopathological analysis confirmed a neuroendocrine tumor (NET) of pancreatic origin. The patient had no prior personal or family history of tumor-related illnesses.
On November 30, 2020, [99mTc]-EDDA/HYNIC-TOC somatostatin receptor scintigraphy with SPECT/CT was performed using a native, low-dose protocol with oral contrast (1000 mL of polyethylene glycol solution). The imaging revealed increased radiopharmaceutical uptake in CT-identified lesions, consistent with somatostatin receptor expression (Figure 1). Serum chromogranin A (CgA) levels were moderately elevated at 108 ng/mL (reference range: 19.0–98.0).
A multidisciplinary team recommended surgical treatment. In preparation, the patient was started on somatostatin long-acting analogue therapy (lanreotide monotherapy, 120 mg intramuscularly).
The surgical plan included resection of the pancreatic tail with splenectomy, right hemihepatectomy, and additional left hepatic metastasectomy to address metastases in both liver lobes.
As part of preoperative planning, the patient’s global liver function was assessed using clinical scoring systems. The Model for End-Stage Liver Disease (MELD) score was 6, the aspartate aminotransferase (AST) to platelet ratio index (APRI) was 0.3, and the Child-Turcotte-Pugh (CTP) score was 5, all indicating normal liver function. Due to the patient’s iodine allergy, an indocyanine green (ICG) clearance assay was not performed. Instead, ultrasound 2D shear wave elastography was used to assess liver parenchyma in both lobes, revealing no signs of fibrosis (left lobe velocity: 1.3 m/s, right lobe velocity: 1.37 m/s).
To assess segmental liver function, [99mTc]Tc-mebrofenin SPECT/CT (native, low dose) with dynamic acquisition was performed [10]. The analysis showed a future liver remnant (FLR) volume fraction of 38%, a functional fraction of 29%, and an FLR filtration rate of 2.29 %/min/m². Given the borderline FLR rate, a strategy combining metastasectomy and radiofrequency ablation in the left (FLR) lobe was planned (Figure 2). Additionally, parenchymal modulation was deemed necessary to minimize the risk of posthepatectomy liver failure (PHLF).
On January 11, 2021, the patient underwent distal pancreatic resection with splenectomy, along with metastasectomy from segment III of the left liver lobe (Figure 3) and the lower part of segment II. Additionally, radiofrequency ablation (RFA) was performed on an intraparenchymal metastasis in segment II. To prepare for a planned right hemihepatectomy to address multiple metastases in the right liver lobe, a right vena portae ligation was also performed.
After six weeks, a follow-up study was conducted to evaluate global and segmental liver function. Global liver function parameters remained stable despite parenchymal modulation, with a MELD score of 6, APRI score of 0.3, and CTP score of 5. However, ultrasound 2D-shear wave elastography (SWE) revealed the development of mild fibrosis in the right lobe following portal vein ligation (PVL) (velocity: 1.53 m/s). No increase in elasticity indicative of fibrosis was observed in the hypertrophied left lobe (velocity: 1.3 m/s).
Control segmental liver function was assessed using [99mTc]Tc-mebrofenin SPECT/CT (Figure 4). The imaging confirmed adequate hypertrophy of the future liver remnant (FLR), with the following values: FLR volume fraction (FLR-V%) at 46%, FLR functional volume fraction (FLR-FV%) at 66%, and FLR filtration rate at 3.16%/min/m².
In March 2021, the patient underwent a successful right hemihepatectomy with metastasectomy from medial hepato-caval junction (Figure 5). No signs of clinically significant posthepatectomy liver failure (PHLF) were observed in the postoperative period.
A follow-up 99mTc-EDDA/HYNIC-TOC somatostatin receptor scintigraphy with SPECT/CT (native, low dose) was performed on April 19, 2021, revealing no somatostatin receptor-expressing lesions (Figure 6).
The multidisciplinary team (MDT) recommended ongoing follow-up to monitor the disease through serum chromogranin A (CgA) measurements and imaging studies.
On July 29, 2021, the patient’s serum CgA level was 52.5 ng/mL (reference range: 19.0–98.0), remaining within the normal range. A follow-up contrast-enhanced CT scan in November 2021 detected a solitary metastasis in the residual left liver lobe and an enlarged retroperitoneal lymph node.
On January 20, 2022, 99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT identified new somatostatin receptor-expressing lesions in the liver, as well as a positive lymph node along the abdominal aorta (Figure 7). These findings represented new disease progression compared to the previous scintigraphy on April 19, 2021. Due to recurrent disease, the patient was started on somatostatin analogue (SSA) therapy with somatuline (120 mg, once a month). The patient tolerated SSA therapy well, without experiencing any significant side effects.
On January 21, 2023, the patient completed four cycles of (177Lu)-DOTATATE therapy due to disease progression despite treatment with somatostatin analogues (SSA). The therapy resulted in a reduction in both the number and activity of somatostatin receptor (SSTR)-positive lesions (Figure 8).
During follow-up, on July 15, 2024, 99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT detected a new SSTR-positive liver metastasis at the site of a previously regressed lesion (Figure 9). However, the remaining SSTR-positive lesions exhibited decreased activity. In September 2024, an R0 resection was performed to remove the newly detected somatostatin receptor-expressing lesion in segment IV of the liver.
Histology
Histopathological examinations revealed the dedifferentiation process of the primary pancreatic neuroendocrine tumor in the various liver metastases. The primary tumor showed co-expression of markers characteristic of the epithelial-mesenchymal transition process (Figure 10).
The patient is currently in good general condition, with 53 months having passed since the initial diagnosis of the disease.
Discussion
Our patient has a pancreatic neuroendocrine tumor characterized by slow growth and low proliferation, yet with metastatic spread. This phenomenon is rarely documented in the literature. Zhou et al. reported that in Grade 1–2 PanNETs, high vimentin expression combined with a loss of E-cadherin expression was associated with lymph node metastasis, distant metastasis, disease progression, and poor prognosis [11]. In our case, we analyzed the expression of E-cadherin and vimentin in the primary tumor as markers of epithelial-mesenchymal transition (EMT). This dual expression could be a contributing factor to the metastatic behavior of PanNETs, despite their typically indolent nature. Interestingly, E-cadherin expression was preserved, while vimentin expression was high, suggesting an early phase of EMT [12]. The examination of E-cadherin and vimentin expression in patients with Grade 1–2 PanNETs holds potential as a prognostic marker for disease behavior and progression. However, further large-scale case-control studies are necessary to validate its clinical use.
Adjuvant therapy for PanNETs is not currently included in the ESMO guidelines [5]. However, in this case, the possibility arises that adjuvant SSA therapy may provide benefits following R0 resection of primary and metastatic lesions, combined with radiofrequency ablation of metastases, provided no SSTR expression is detected on functional imaging. This hypothesis highlights the need for extensive research and large-scale studies to evaluate the potential role of adjuvant SSA therapy in this context.
In our patient, we observed a transition from a low-grade (Grade 1) PanNET to more aggressive biological behavior over time. The primary tumor was Grade 1, but intermediate-grade (Grade 2) lesions appeared among the liver metastases, and a new lesion progressed to Grade 3 following PRRT treatment. This phenomenon underscores the potential for PanNETs to evolve into higher-grade lesions, a pathomechanism that remains poorly understood. Few studies to date have explored the factors driving the progression of lower-grade PanNETs to higher-proliferation phenotypes [13]. Further research is needed to elucidate these mechanisms and inform future therapeutic strategies. A step forward in this regard is the treatment of higher grade, well-differentiated, advanced PanNET patients with first-line [177Lu]Lu-DOTATATE, for which a NETTER-2 trial has been initiated. The study revealed, that the first-line 177Lu-DOTATE with octreotide long-acting repeatable (LAR) significantly prolonged progression-free survival in patients with advanced gastroenteropancreatic neuroendocrine tumors of grade 2 or 3. [14] These new findings open up further possibilities for the use of therapeutic isotopes also in higher grade tumours.
Surgical resection remains the primary treatment for resectable PanNETs. In this case, we demonstrated a multistage liver resection approach with meticulous preoperative planning. We utilized a technique employed in only a few specialized centers, which significantly reduces the risk of postoperative mortality—a critical consideration following major resections, particularly in complex cases like ours. Functional volumetry using [99mTc]Tc-mebrofenin provides not only information on the volumetric fraction of the FLR, but also allows for the calculation of segmental filtration rates, allowing for the identification of high-risk patients prone to post-hepatectomy liver failure (PHLF) [8,15]. In this case, our patient did not develop clinically relevant PHLF [16], demonstrating that preoperative functional volumetry is a valuable tool for guiding objective decisions regarding parenchymal modulation. We recommend the broader use of [99mTc]Tc-mebrofenin SPECT/CT functional volumetry in clinical practice, as it facilitates the identification of patients at risk of PHLF and aids in optimizing surgical outcomes. This approach has the potential to improve safety and decision-making in complex liver resections.
In this case, the fibrotic process following parenchymal modulation was assessed non-invasively using ultrasound 2D shear wave elastography (2D-SWE). Parenchymal modulation induces atrophy in the resectable portion of the liver while stimulating a compensatory hypertrophic response in the contralateral lobe [17]. In our patient, fibrosis was detected in the atrophic lobe, whereas no fibrotic lesions were found in the hypertrophic lobe. 2D-SWE provides valuable insight into liver tissue characteristics, measuring liver elasticity to assess the degree of fibrosis [18]. However, while 2D-SWE ultrasound elastography is effective in detecting liver fibrosis, it does not provide volumetric data, which is essential for comprehensive preoperative planning.
The patient was monitored postoperatively with chromogranin A (CgA) measurements and conventional contrast-enhanced CT (ceCT) scans. CgA levels remained within the normal range after surgery. However, a new hepatic nodule was identified on ceCT, and somatostatin receptor scintigraphy confirmed SSTR expression, suggesting recurrent disease. CgA is a widely used biomarker for NETs, as its levels can correlate with tumor burden, differentiation, and progression. However, CgA levels alone are not always reliable, as small or well-differentiated tumors may not produce elevated levels [19]. Therefore, when interpreting CgA levels, monitoring trends over time is more informative than relying solely on whether values exceed a predefined cutoff threshold [20]. This trend-based approach is essential for assessing disease progression and recurrence with greater accuracy.
Our Grade 1 PanNET patient with multiple liver metastases underwent comprehensive multidisciplinary treatment. The treatment was based on the modern functional imaging techniques, which facilitated the making of the most optimal therapeutic decisions. Initial management included primary surgery combined with radiofrequency ablation (RFA), following ESMO guidelines, and was later complemented by systemic therapy for recurrent disease.
According to the literature, curative resection (R0, R1) in PanNET patients is associated with a 5-year overall survival (OS) rate of approximately 85% [7]. To date, 53 months after her malignant diagnosis, our patient is living in excellent overall health and in complete remission. Her current ECOG (Eastern Cooperative Oncology Group) performance status is zero, indicating that she is fully active and asymptomatic.
Limitation
The patient’s follow-up was disrupted due to the COVID-19 pandemic, resulting in missed medical examinations between April 2021 and November 2021.
Conclusion
This case illustrates the multifaceted role of functional imaging in the management of pancreatic neuroendocrine tumors, including preoperative planning, assessment of liver function, and disease monitoring. The integration of advanced nuclear medicine techniques such as [99mTc]Tc-mebrofenin-based SPECT/CT and somatostatin receptor imaging enabled personalized and timely therapeutic decisions across different phases of the disease. The clinical course, marked by a shift from indolent to aggressive behavior, highlights the need for ongoing surveillance and a flexible, multidisciplinary treatment approach. Further studies are warranted to better understand the biological factors driving variable tumor dynamics and to optimize the use of functional imaging and targeted therapies in the management of PanNETs.
Author Contributions
Annamária Bakos: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review & editing; László Libor: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Supervision; Writing – review & editing. : Béla Vasas: Visualization; Writing – review & editing; Kristóf Apró: Visualization; Gábor Sipka: Review & editing; László Pávics: Writing – review & editing; Zsuzsanna Valkusz: Writing – review & editing : Anikó Maráz: Conceptualization; Writing – review & editing; Zsuzsanna Besenyi: Conceptualization; Supervision; Validation; Finalization of the manuscript. All authors contributed to the manuscript revision and approved the submitted version.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics Approval and Consent to Participate
Our institution does not require ethical approval for reporting individual cases or case series. Consent to participate: written informed consent was obtained from the patient.
Consent for Publication
The patient provided consent for publication of this manuscript.
Availability of Data and Material
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Aknowledgments
We thank Anna Mayer for linguistic support.
Competing Interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Fraenkel M, Kim M, Faggiano A, de Herder WW, Valk GD; Knowledge NETwork. Incidence of gastroenteropancreatic neuroendocrine tumours: a systematic review of the literature. Endocr Relat Cancer. 2014;21(3):R153-R163. Published 2014 May 6. [CrossRef]
- Leoncini E, Boffetta P, Shafir M, Aleksovska K, Boccia S, Rindi G. Increased incidence trend of low-grade and high-grade neuroendocrine neoplasms. Endocrine. 2017;58(2):368-379. [CrossRef]
- Huguet I, Grossman AB, O’Toole D. Changes in the Epidemiology of Neuroendocrine Tumours. Neuroendocrinology. 2017;104(2):105-111. [CrossRef]
- Niederle MB, Hackl M, Kaserer K, Niederle B. Gastroenteropancreatic neuroendocrine tumours: the current incidence and staging based on the WHO and European Neuroendocrine Tumour Society classification: an analysis based on prospectively collected parameters. Endocr Relat Cancer. 2010;17(4):909-918. Published 2010 Oct 5. [CrossRef]
- Pavel M, Öberg K, Falconi M, et al. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31(7):844-860. [CrossRef]
- Fischer L, Bergmann F, Schimmack S, et al. Outcome of surgery for pancreatic neuroendocrine neoplasms. Br J Surg. 2014;101(11):1405-1412. [CrossRef]
- Frilling A, Modlin IM, Kidd M, et al. Recommendations for management of patients with neuroendocrine liver metastases. Lancet Oncol. 2014;15(1):e8-e21. [CrossRef]
- Primavesi F, Maglione M, Cipriani F, et al. E-AHPBA-ESSO-ESSR Innsbruck consensus guidelines for preoperative liver function assessment before hepatectomy. Br J Surg. 2023;110(10):1331-1347. [CrossRef]
- Tada T, Kumada T, Toyoda H, et al. Utility of real-time shear wave elastography for assessing liver fibrosis in patients with chronic hepatitis C infection without cirrhosis: Comparison of liver fibrosis indices. Hepatol Res. 2015;45(10):E122-E129. [CrossRef]
- Bakos A, Libor L, Urbán S, et al. Dynamic [99mTc]Tc-mebrofenin SPECT/CT in preoperative planning of liver resection: a prospective study. Sci Rep. 2024;14(1):30305. Published 2024 Dec 5. [CrossRef]
- Zhou B, Xiang J, Jin M, Zheng X, Li G, Yan S. High vimentin expression with E-cadherin expression loss predicts a poor prognosis after resection of grade 1 and 2 pancreatic neuroendocrine tumors. BMC Cancer. 2021;21(1):334. Published 2021 Mar 31. [CrossRef]
- Guo Y, Jiang Y, Rose JB, et al. Protein Kinase D1 Signaling in Cancer Stem Cells with Epithelial-Mesenchymal Plasticity. Cells. 2022;11(23):3885. Published 2022 Dec 1. [CrossRef]
- Alexandraki KI, Spyroglou A, Kykalos S, et al. Changing biological behaviour of NETs during the evolution of the disease: progress on progression. Endocr Relat Cancer. 2021;28(5):R121-R140. Published 2021 Apr 29. [CrossRef]
- Singh S, Halperin D, Myrehaug S, et al. [177Lu]Lu-DOTA-TATE plus long-acting octreotide versus high-dose long-acting octreotide for the treatment of newly diagnosed, advanced grade 2-3, well-differentiated, gastroenteropancreatic neuroendocrine tumours (NETTER-2): an open-label, randomised, phase 3 study. Lancet. 2024;403(10446):2807-2817. [CrossRef]
- Arntz PJW, Deroose CM, Marcus C, et al. Joint EANM/SNMMI/IHPBA procedure guideline for [99mTc]Tc-mebrofenin hepatobiliary scintigraphy SPECT/CT in the quantitative assessment of the future liver remnant function. HPB (Oxford). 2023;25(10):1131-1144. [CrossRef]
- Baumgartner R, Gilg S, Björnsson B, et al. Impact of post-hepatectomy liver failure on morbidity and short- and long-term survival after major hepatectomy. BJS Open. 2022;6(4):zrac097. [CrossRef]
- Kim RD, Kim JS, Watanabe G, Mohuczy D, Behrns KE. Liver regeneration and the atrophy-hypertrophy complex. Semin Intervent Radiol. 2008;25(2):92-103. [CrossRef]
- Garcovich M, Paratore M, Riccardi L, et al. Correlation between a New Point-Shear Wave Elastography Device (X+pSWE) with Liver Histology and 2D-SWE (SSI) for Liver Stiffness Quantification in Chronic Liver Disease. Diagnostics (Basel). 2023;13(10):1743. Published 2023 May 15. [CrossRef]
- Mariën L, Islam O, Van Mileghem L, Lybaert W, Peeters M, Vandamme T. Pathophysiology and Treatment of Pancreatic Neuroendocrine Neoplasms (PNENS): New Developments. In: Feingold KR, Anawalt B, Blackman MR, et al., eds. Endotext. South Dartmouth (MA): MDText.com, Inc.; April 8, 2022.
- Nobels FR, Kwekkeboom DJ, Coopmans W, et al. Chromogranin A as serum marker for neuroendocrine neoplasia: comparison with neuron-sp ecific enolase and the alpha-subunit of glycoprotein hormones. J Clin Endocrinol Metab. 1997;82(8):2622-2628. [CrossRef]
Figure 1.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) Transaxial CT, and (C) Planar images demonstrate the primary lesion in the pancreatic tail (white arrows) and multiple somatostatin receptor (SSTR)-positive hypodense lesions are visible in the liver, indicating metastatic involvement.
Figure 1.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) Transaxial CT, and (C) Planar images demonstrate the primary lesion in the pancreatic tail (white arrows) and multiple somatostatin receptor (SSTR)-positive hypodense lesions are visible in the liver, indicating metastatic involvement.
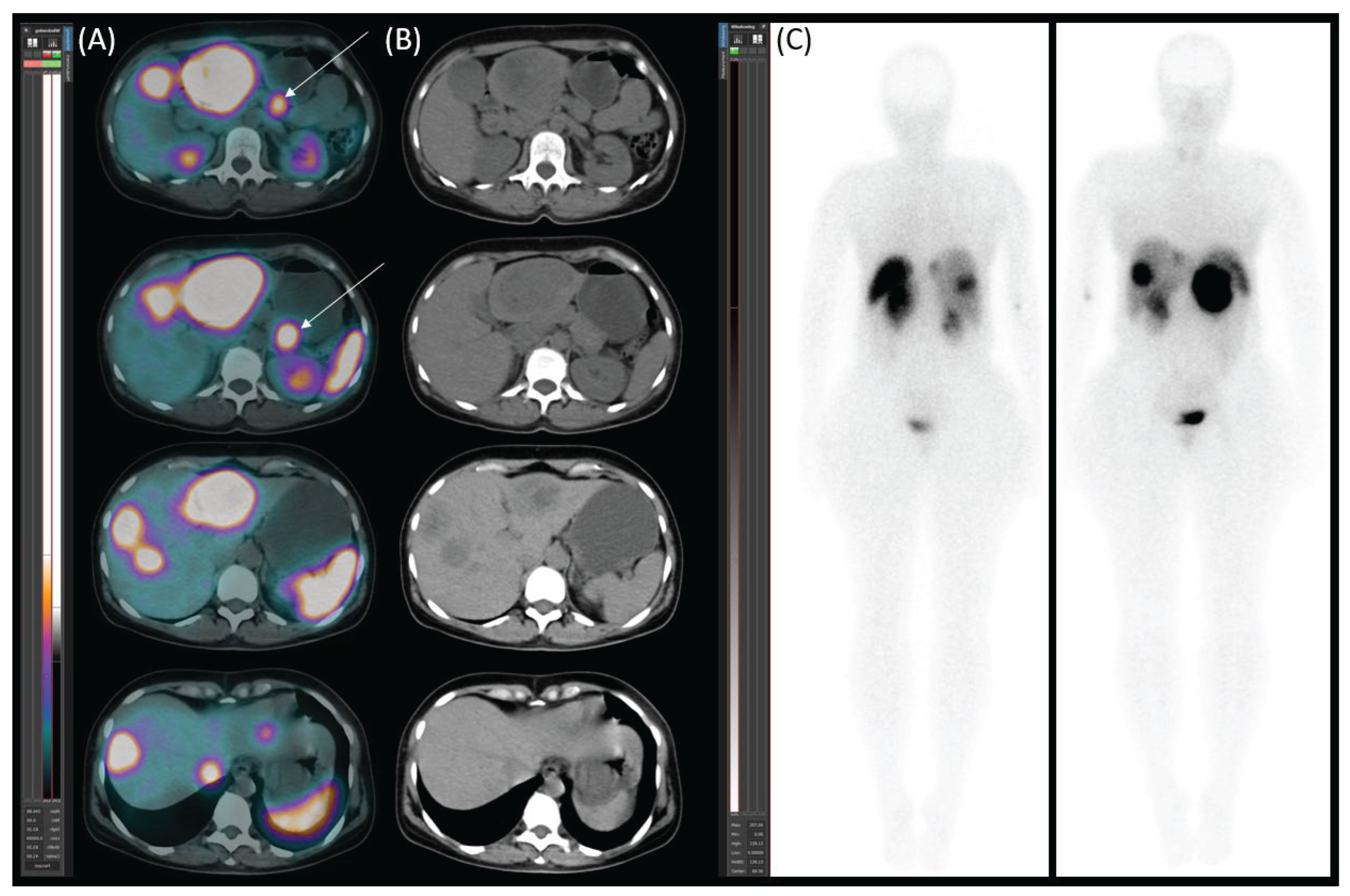
Figure 2.
[99mTc]Tc-mebrofenin SPECT/CT. (A) Transaxial SPECT/CT and (B) native low-dose CT images illustrate the distribution of functional hepatocytes and metastases. The metastases appear as hypodense, photopenic areas (marked with asterisks).
Figure 2.
[99mTc]Tc-mebrofenin SPECT/CT. (A) Transaxial SPECT/CT and (B) native low-dose CT images illustrate the distribution of functional hepatocytes and metastases. The metastases appear as hypodense, photopenic areas (marked with asterisks).
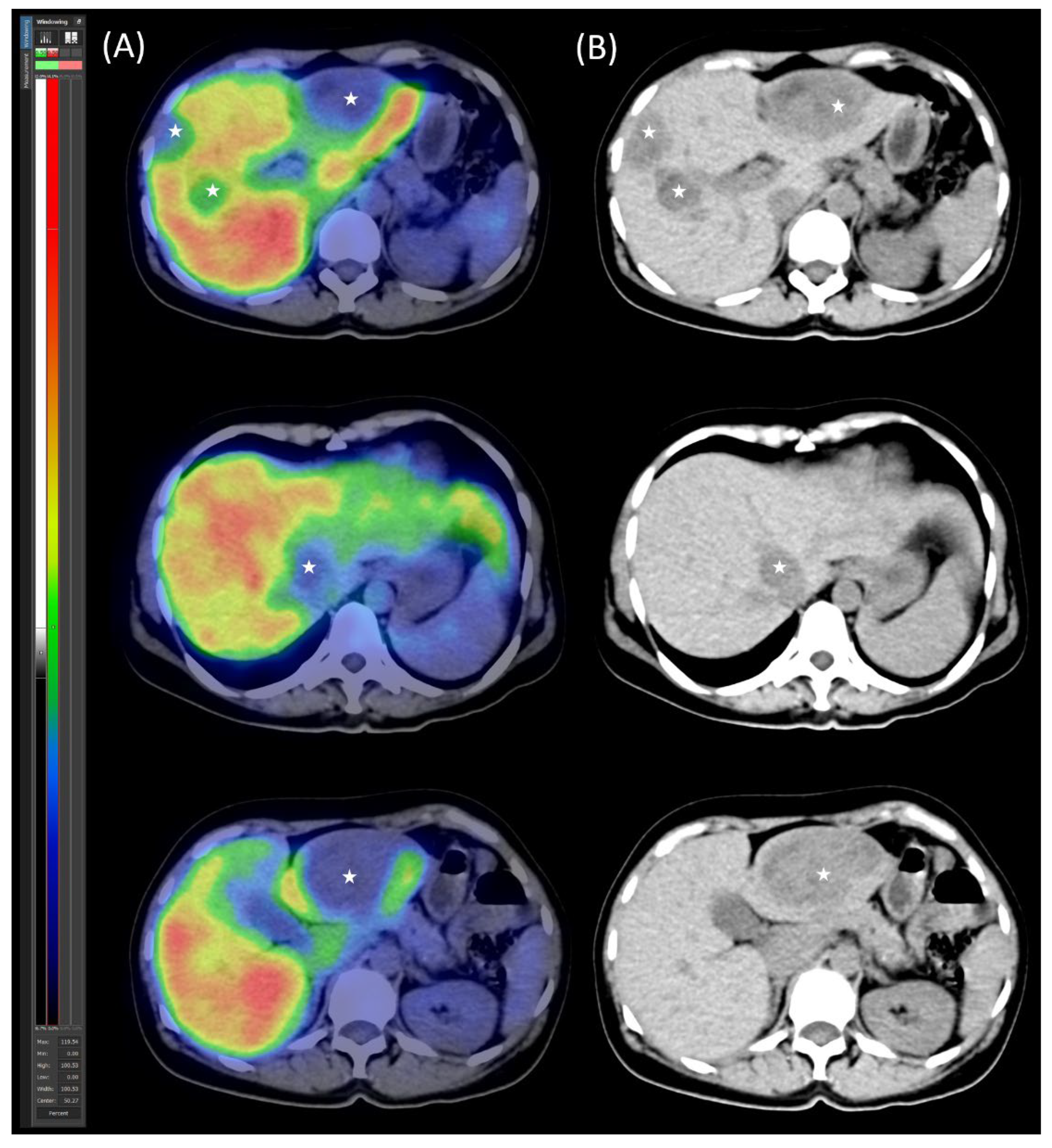
Figure 3.
Surgical specimens. The spleen and pancreatic tail following resection (left), and a metastasis excised from liver segment III (right).
Figure 3.
Surgical specimens. The spleen and pancreatic tail following resection (left), and a metastasis excised from liver segment III (right).
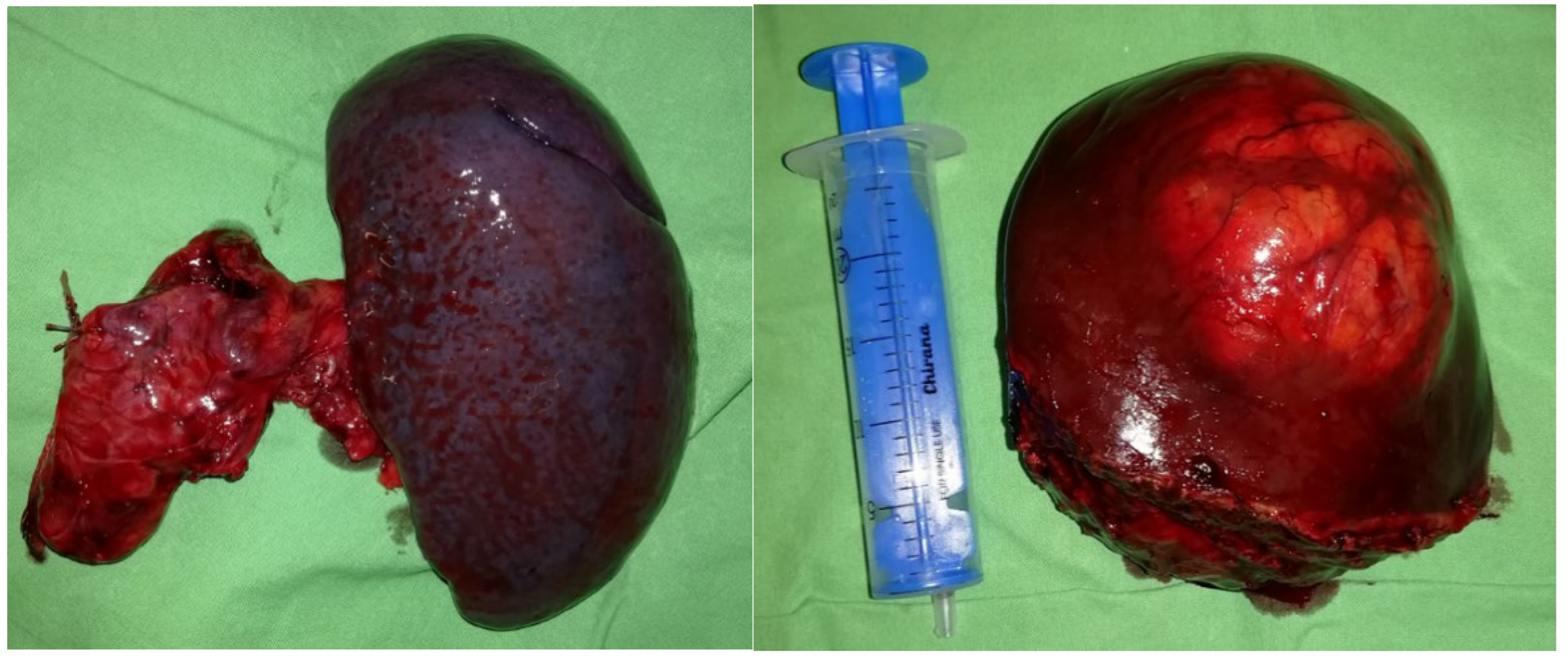
Figure 4.
[99mTc]Tc-mebrofenin SPECT/CT after parenchymal modulation. (A) Transaxial SPECT/CT and (B) native low-dose CT images show the distribution of functional hepatocytes, highlighting the dominance of the hypertrophied left lobe. The right lobe metastases appear as photopenic hypodense areas (marked with asterisks), with the arrow indicating the right portal vein ligation.
Figure 4.
[99mTc]Tc-mebrofenin SPECT/CT after parenchymal modulation. (A) Transaxial SPECT/CT and (B) native low-dose CT images show the distribution of functional hepatocytes, highlighting the dominance of the hypertrophied left lobe. The right lobe metastases appear as photopenic hypodense areas (marked with asterisks), with the arrow indicating the right portal vein ligation.
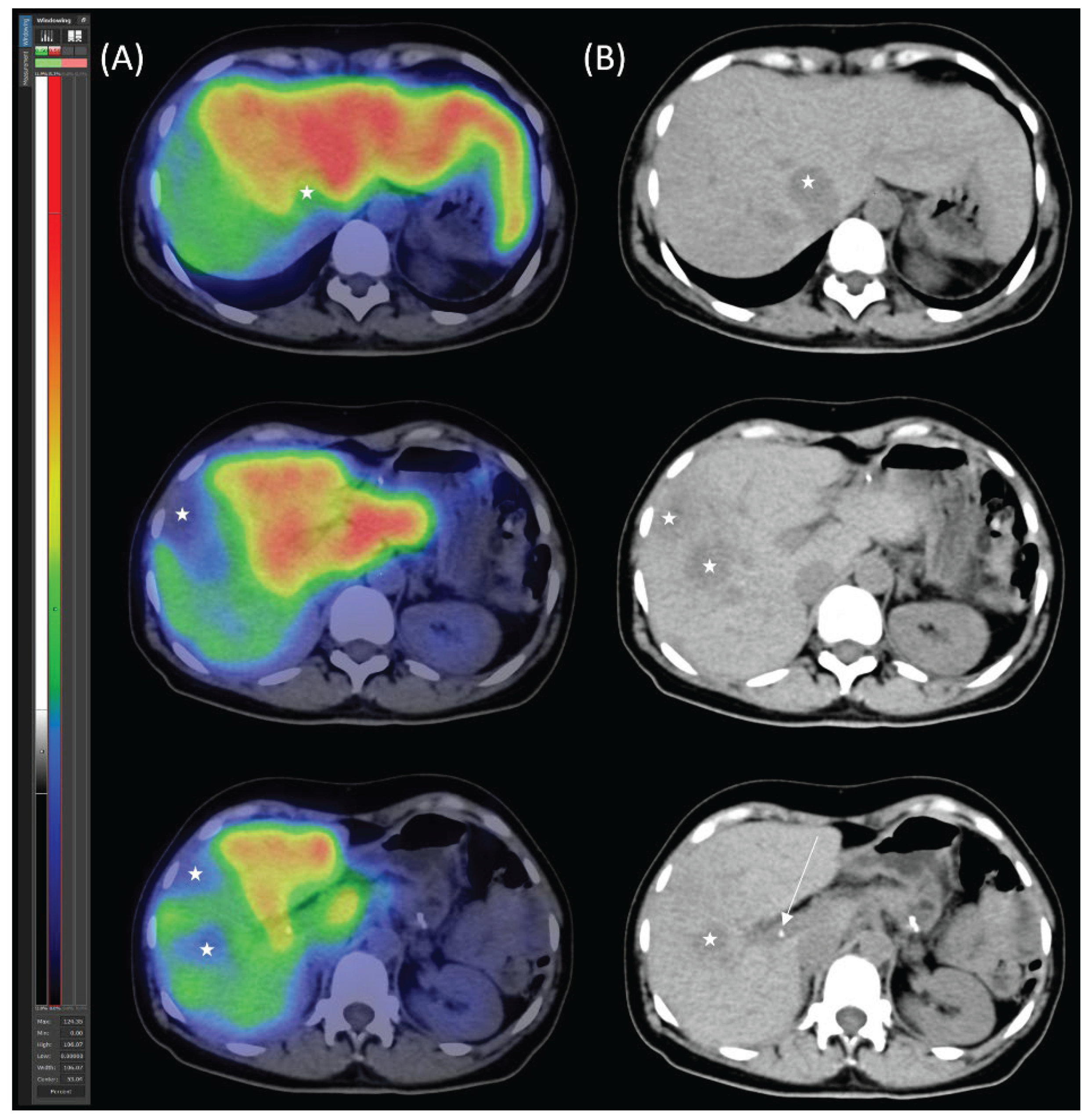
Figure 5.
Surgical specimen: Resected right liver lobe with multiple metastatic lesions (left), metastasis from medial hepato-caval junction (right), consistent with PanNET metastases.
Figure 5.
Surgical specimen: Resected right liver lobe with multiple metastatic lesions (left), metastasis from medial hepato-caval junction (right), consistent with PanNET metastases.
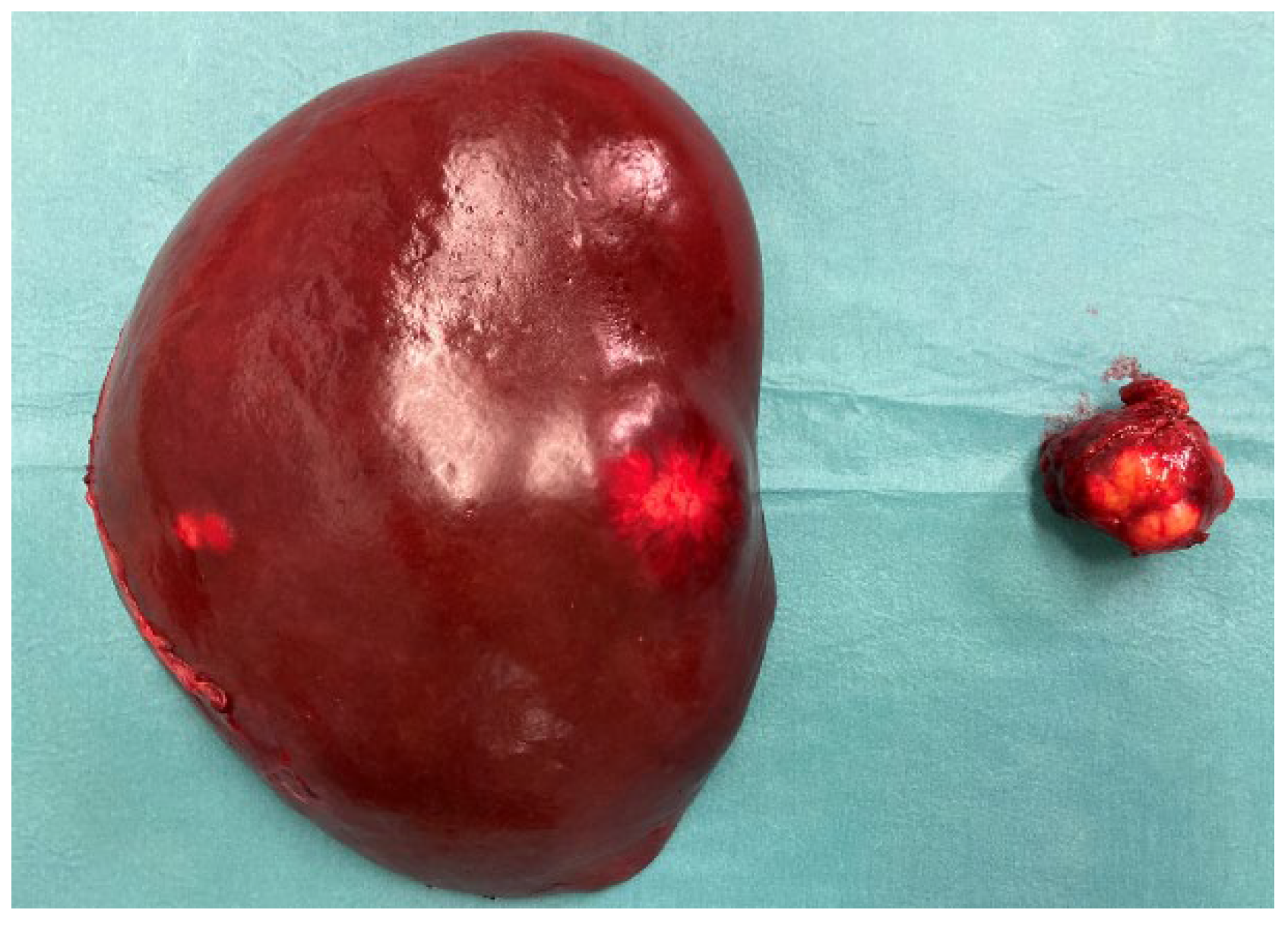
Figure 6.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) transaxial CT, and (C) planar images reveal no abnormal lesions.
Figure 6.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) transaxial CT, and (C) planar images reveal no abnormal lesions.
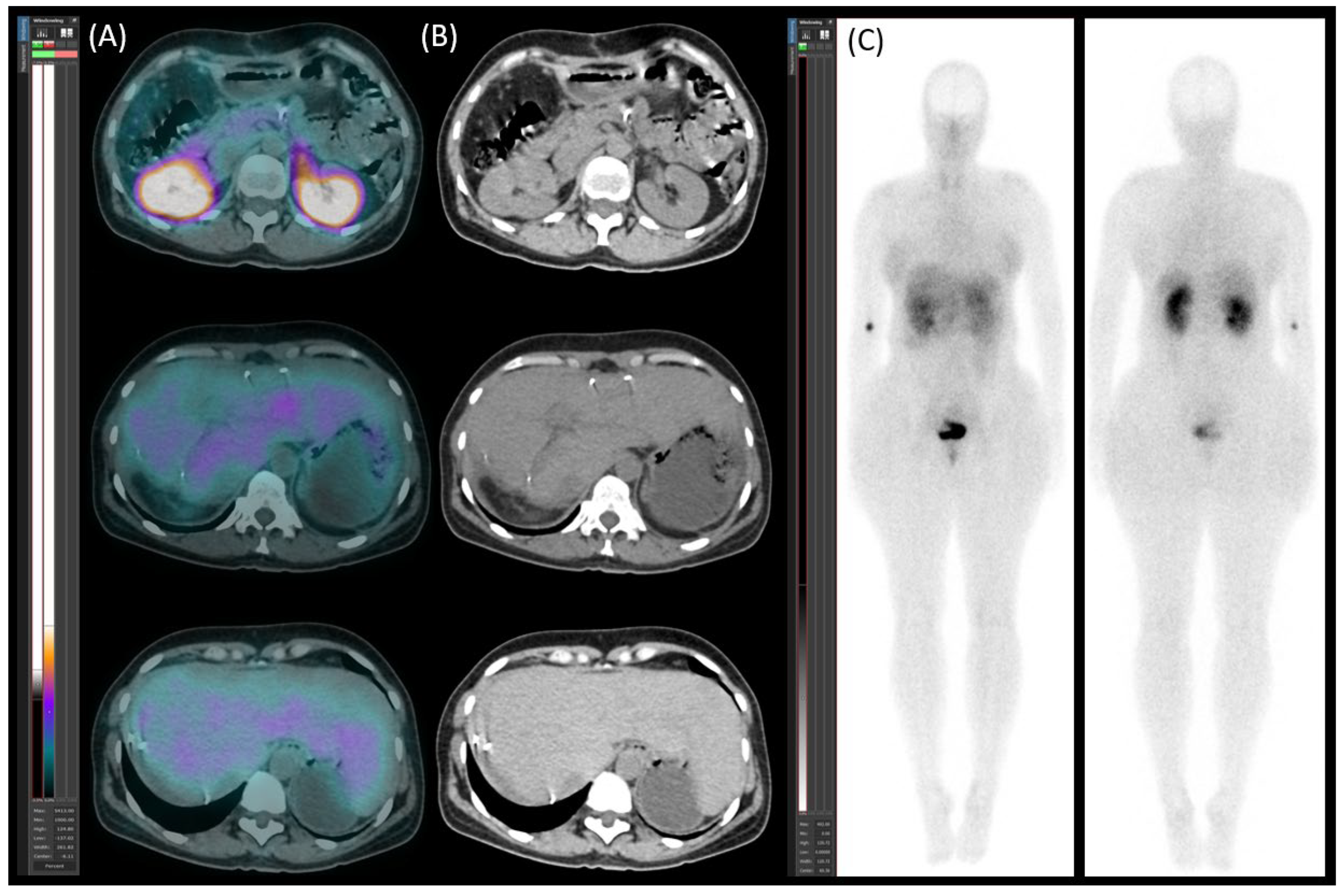
Figure 7.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) transaxial CT, and (C) planar images reveal new somatostatin receptor (SSTR)-positive lesions (red arrows) in the residual liver and paraaortic lymph node metastases (white arrows).
Figure 7.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) transaxial CT, and (C) planar images reveal new somatostatin receptor (SSTR)-positive lesions (red arrows) in the residual liver and paraaortic lymph node metastases (white arrows).
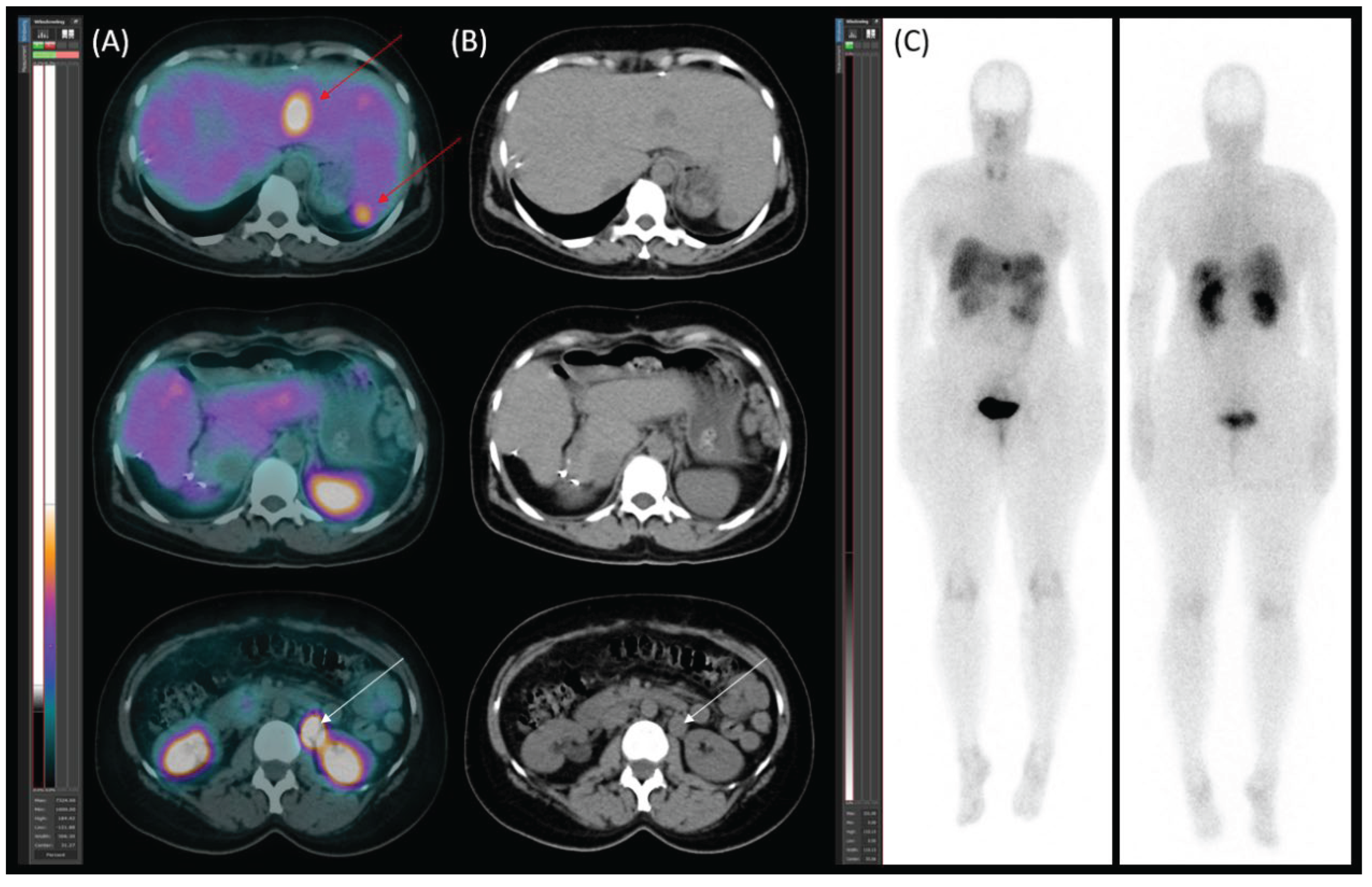
Figure 8.
[177Lu]Lu-DOTA-TATE therapy response. Transaxial (A and B) SPECT/CT images and planar images (C and D) were obtained after the first (A, C) and fourth (B, D) therapy cycles with [177Lu]Lu-DOTA-TATE demonstrate a reduction in both the number and activity of somatostatin receptor (SSTR)-positive lesions in the liver and paraaortic lymph node metastases (white arrow) following therapy.
Figure 8.
[177Lu]Lu-DOTA-TATE therapy response. Transaxial (A and B) SPECT/CT images and planar images (C and D) were obtained after the first (A, C) and fourth (B, D) therapy cycles with [177Lu]Lu-DOTA-TATE demonstrate a reduction in both the number and activity of somatostatin receptor (SSTR)-positive lesions in the liver and paraaortic lymph node metastases (white arrow) following therapy.
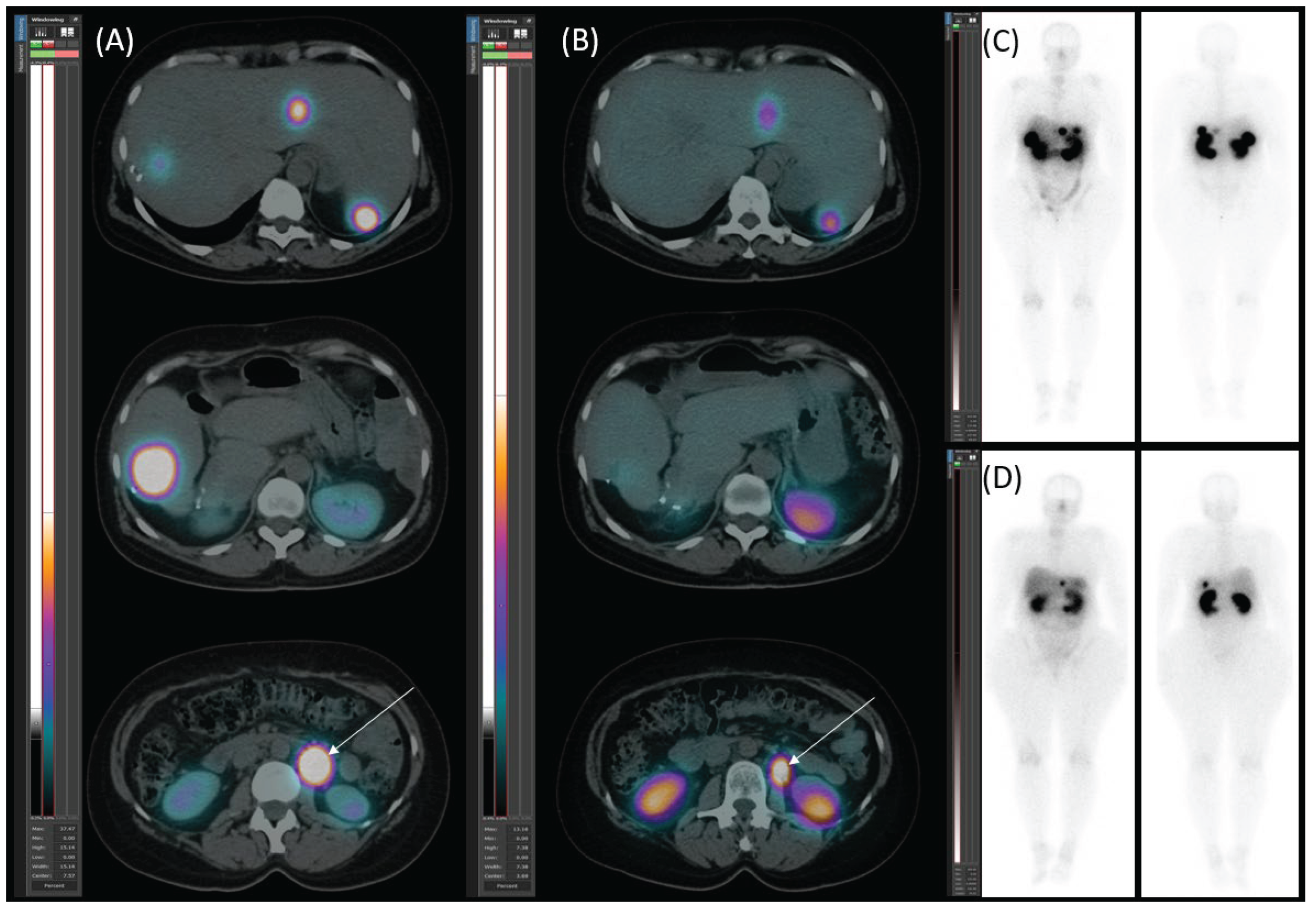
Figure 9.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) transaxial CT, and (C) planar images reveal new hypodense somatostatin receptor (SSTR)-positive lesion (white arrow).
Figure 9.
99mTc-EDDA/HYNIC-TOC scintigraphy with SPECT/CT. (A) Transaxial SPECT/CT, (B) transaxial CT, and (C) planar images reveal new hypodense somatostatin receptor (SSTR)-positive lesion (white arrow).
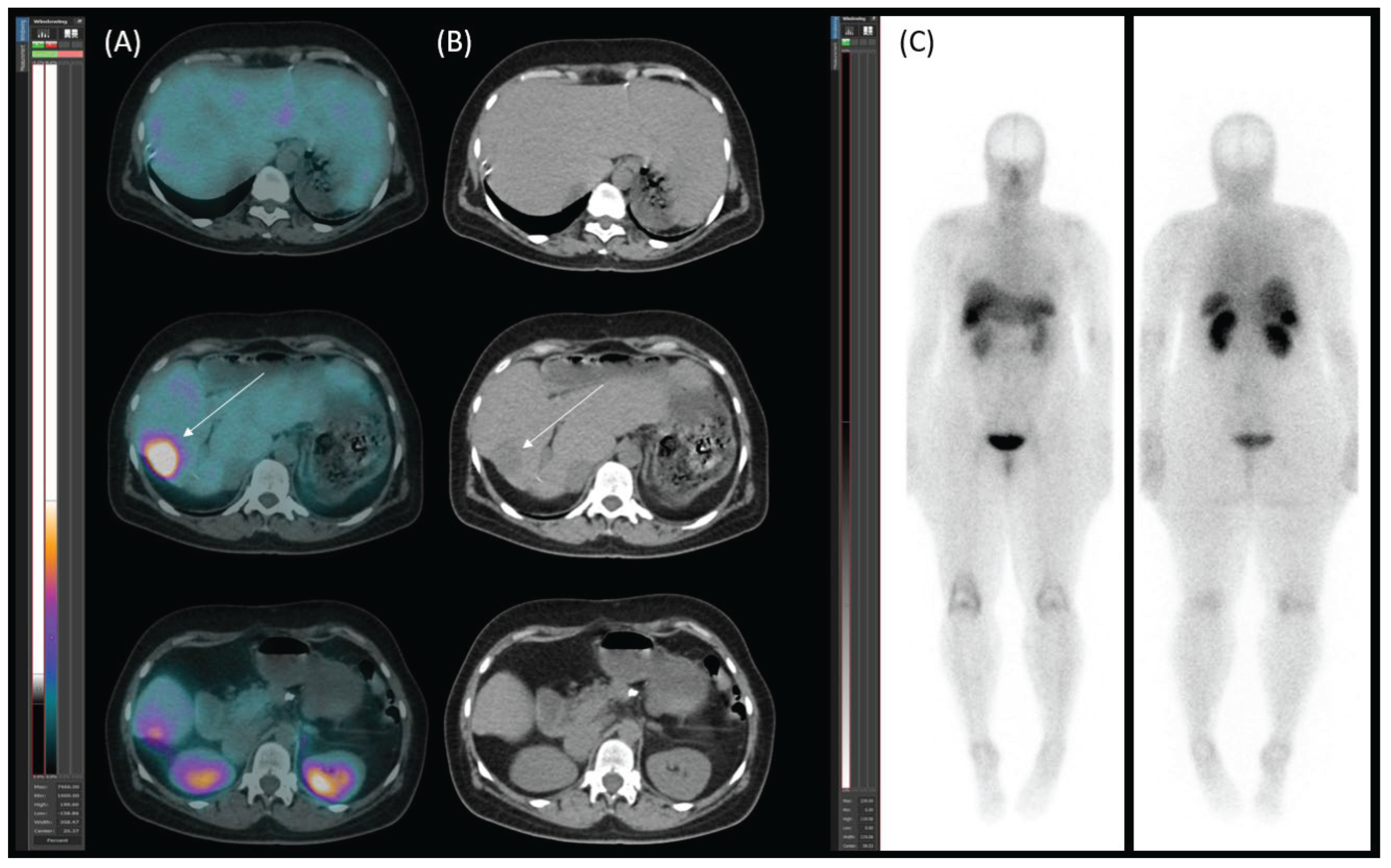
Figure 10.
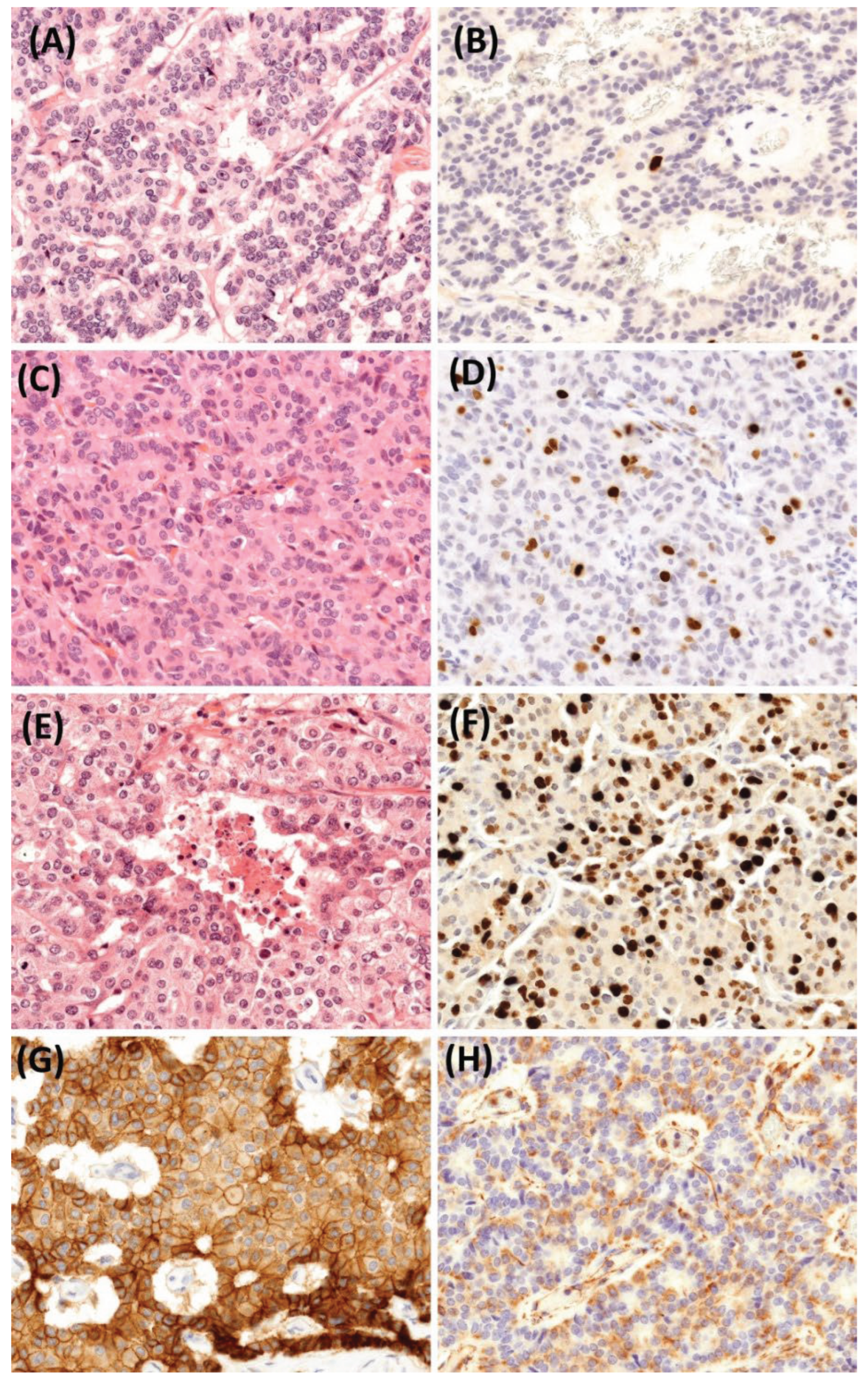
Representative images illustrate the dedifferentiation of the pancreatic neuroendocrine tumor (PanNET) from its primary site to metastatic lesions, highlighting the changes in tumor grade and Ki-67 index. (A) shows the primary pancreatic NET, classified as grade 1 (H&E, 400x), and (B) displays the corresponding Ki-67 index of 1% (400x). (C) depicts the liver metastasis from hepato-caval junction, showing dedifferentiation to a grade 2 NET (H&E, 400x), and (D) shows the corresponding elevated Ki-67 index of 6% (400x). (E) depicts the last operated liver metastasis, which has already dedifferentiated into a grade 3 NET, with small areas of necrosis, increased mitotic rate, and (F) a Ki-67 index of 30%. The tumor exhibited robust E-cadherin expression, with more than 90% of cells displaying strong (2-3+) and complete circular membrane staining (G). Concurrently, vimentin expression was notably elevated, with moderate (2+) intensity observed in half of the tumor cells (H).
Figure 10.
Representative images illustrate the dedifferentiation of the pancreatic neuroendocrine tumor (PanNET) from its primary site to metastatic lesions, highlighting the changes in tumor grade and Ki-67 index. (A) shows the primary pancreatic NET, classified as grade 1 (H&E, 400x), and (B) displays the corresponding Ki-67 index of 1% (400x). (C) depicts the liver metastasis from hepato-caval junction, showing dedifferentiation to a grade 2 NET (H&E, 400x), and (D) shows the corresponding elevated Ki-67 index of 6% (400x). (E) depicts the last operated liver metastasis, which has already dedifferentiated into a grade 3 NET, with small areas of necrosis, increased mitotic rate, and (F) a Ki-67 index of 30%. The tumor exhibited robust E-cadherin expression, with more than 90% of cells displaying strong (2-3+) and complete circular membrane staining (G). Concurrently, vimentin expression was notably elevated, with moderate (2+) intensity observed in half of the tumor cells (H).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



