
Submitted:
21 May 2025
Posted:
22 May 2025
You are already at the latest version
Abstract
Background:
To assess the frequency of chronic obstructive pulmonary disease (COPD) exacerbations and their association with lung function in patients treated with ICS/LABA in everyday medical practice in Poland, we conducted a prospective observational study.
Methods:
Patients diagnosed with COPD for at least 12 months before enrolment and ambulatory treatment with ICS/LABA for at least 6 months before study entry were followed up for 2 years after the initial visit. At four subsequent visits, data on pulmonary function, exacerbations, and symptoms were collected. The severity of airflow limitation was assessed using the %pred. (GOLD), and z-scores (ATS/ERS 2022).
Results:
At each visit, approximately 80% of the patients had an mMRC ≥ 2 and CAT score ≥ 10. In 330 patients defined as 'decliners, ’ a decrease in FEV1 greater than 100 ml was observed. At the initial visit, 76.5% of patients reported exacerbation of COPD in the 12-months period preceding study entry. At each subsequent visit, fewer exacerbating patients reported hospitalization (from 27.7% at Visit 2 to 18.4% at Visit 4). Regression analysis revealed that the presence of comorbidities and higher mMRC values (OR=1.556 [CI:1.099–2.203], p=0.013 and OR=2.656 [CI:2.163; 3.262], p< 0.001, respectively) were independent factors associated with COPD exacerbations.
Conclusions:
During the 2-years period, pulmonary function and patient-related outcomes, such as severity of dyspnea measured by mMRC score and CAT, were generally stable throughout the study. Symptoms and comorbidities but not lung function were associated with the risk of exacerbation.
Keywords:
chronic obstructive pulmonary disease
; COPD
; ICS/LABA
; exacerbation
; GOLD
; spirometry
; ATS/ERS
Introduction
Chronic obstructive pulmonary disease (COPD) is a respiratory disorder characterized by irreversible and progressive airflow limitation[1]. COPD is the most common chronic respiratory disease in older adults and the third leading cause of death worldwide[2,3]. Patients with COPD commonly present with dyspnea, chronic cough, and sputum production; their lung function declines, which is routinely assessed by spirometry. Although COPD has different clinical forms and levels of airway obstruction severity, many patients experience exacerbations that lead to hospitalization[4], and the disease significantly decreases the health status of patients[5]. The current recommendations of the American Thoracic Society/European Respiratory Society (ATS/ESR) present a new system for the evaluation of lung function impairment severity that does not use the percentage of predicted FEV1 values but focuses on z-score values[6].
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends maintenance therapy with different types of bronchodilators depending on the disease severity phenotype (short-acting bronchodilators, long-acting beta agonists [LABAs], or long-acting muscarinic antagonists [LAMAs]). For patients with repeated exacerbations, combination treatment with inhaled corticosteroids (ICS) such as ICS/LABA or ICS/LABA/LAMA should be considered[4].
The efficacy of ICS/LABA in COPD treatment has been widely studied since many years. It has been shown that these drugs’ combination reduces the exacerbation rate, improves health status and spirometric characteristics of lung function of COPD patients[7,8,9,10,11]. However, there are a small number of real-life longitudinal (> 12 months) observational studies aimed at evaluating the effectiveness of ICS/LABAs in COPD populations. In particular, there is a lack of studies on Polish COPD patients[12]. Moreover, clinical studies applying new ATS/ERS recommendations for the evaluation of lung function impairment severity have not yet been conducted.
The purpose of this observational, non-interventional study was to assess the frequency of COPD exacerbations and hospitalizations due to these exacerbations and to evaluate changes in lung function for 2 years observation period in patients treated with ICS/LABA in everyday medical practice in Poland. Additionally, the risk of COPD exacerbations was assessed using the new strategy of pulmonary functional test interpretation recommended by the ATS/ERS in 2022.
Materials and Methods
Study Design and Participants
This open, prospective, multicenter, non-interventional observational study enrolled 965 patients who were diagnosed with COPD for at least 12 months before enrolment and were treated with ICS/LABA for at least 6 months prior to enrolment. The study lasted 24 months (2015 – 2017) , during which patients had five visits (visits 0 – 4) to the treating physician.
The study was performed in accordance with the Declaration of Helsinki, the International Conference on Harmonization Harmonized Tripartite Guideline for Good Clinical Practice, and local regulations. This is a prospective observational, non-interventional, real-life study, so according to Polish law, the Local Ethical Committee does not have to approve the study protocol. Additionally, in this type of study, the informed consent of the participants was not required at the time of conducting observation.
Patients were excluded from this study if any of the following criteria were present: (i) had bronchial asthma, (ii) had a contraindication to treatment with an ICS/LABA combination, (iii) were pregnant or lactating, and (iv) were currently participating in another clinical trial. If any of the abovementioned criteria were met, the patient was excluded from the study.
Endpoints and Measurements of the Study
Patients were enrolled in the study at visit 0 (the initial visit). Six months after the initial visit, visit 1 was scheduled. Subsequent visits (Visit 2-4) were performed every 6 months (+/- 14 days). Patient data collected during the initial and subsequent visits are presented in the flow chart (Figure 1).
The primary endpoints of the study were a change of pulmonary function parameter FEV1 and the frequency of COPD exacerbations and hospitalizations due to exacerbations. Secondary endpoints included assessment of GOLD category distribution, type of comorbidities, and degree of stability of COPD treatments. Study variables were following: FEV1 and FVC (expressed in absolute values, % predicted and z-scores) applying Global Lung Function Initiative (GLI) equations[13], number of exacerbation and hospitalization, demographic data of patients and data on: (i) smoking habits (ii) concomitant diseases, (iii) symptoms currently occurring, (iv) level of dyspnea’s severity assessed by modified Medical Research Council (mMRC) scale, (v) COPD Assessment Test (CAT) score, (vi) current treatment, (vii) treatment with antidepressants, (viii) classification to GOLD 2017-2022 groups, (ix) adverse drug reactions.
In this study, it was assumed that the FEV1/FVC ratio in obstructive patients should be ≤ 0.7. Additionally, patients were categorized as ‘decliner’ or ‘non-decliner’ depending on the occurrence of FEV1 loss greater than 100 ml during the study. Based on GOLD and new ATS/ERS recommendations [6], patients were divided into four categories based on spirometry values:
non-severe; ATS/ERS-non-severe (FEV1> 50% pred. and z-score>-4);
GOLD-non-severe: ATS/ERS-severe (FEV1> 50% pred. and z-score<-4);
GOLD-severe - ATS/ERS-non-severe (FEV1< 50% pred. and z-score>-4);
GOLD-severe: ATS/ERS-severe (FEV1<50% pred. and z-score<-4).
Statistical Analysis
Descriptive statistics were provided for all the variables. Multivariate logistic regression was used to assess predictors of COPD exacerbation. results of multivariate regression analysis are presented as odds ratios with respective 95% confidence intervals (CI). Poisson regression analysis was used to assess the predictors of pulmonary function. The results of the Poisson regression are presented as β coefficients and respective p-values. The results were considered statistically significant at p<0.05. All calculations and analyses were performed using R 3.5 statistical software and MedCalc® Statistical Software version 20.218 (MedCalc Software Ltd, Ostend, Belgium; https://www.medcalc.org; 2023).
Results
Patients’ Characteristics and Progress of the Study
In total, 965 patients were enrolled in the study during their initial visit (visit 0). The majority of patients were males (67.7%), and the mean age of participants was 66.9 (9.4) years. Almost all patients (91.6%) were current smokers or ex-smokers. Among concomitant diseases, the most frequent were cardiovascular diseases, such as hypertension (70%), ischemic heart disease (30%), and heart failure (20%). Depression and anxiety disorders were diagnosed in 6.8% of patients.
Regarding medication used during the study, the combinations of ICS/LABA taken by study patients did not differ considerably from visit to visit and was noted in 96% to 100% of visits to visit. Extrafine beclomethasone/formoterol was used in up to 40% of study patients, and fluticasone propionate/salmeterol in about 20%. LAMAs were the most frequently used drugs as concomitant therapy (between 58.9 to 68.9% of patients from visit to visit), then short-acting beta2-adrenergic agonists (between 37.8% and 46.4% of patients), and aminophylline (between 35.5% and 45.7%). More details on the demographic characteristics, smoking status, concomitant diseases, and treatment methods at each visit are given in Table 1 and Table 2.
The number of patients decreased gradually from visit to visit. Eight hundred sixty-seven (89.8%) patients were present at Visit 1, 707 at Visit 2 (73.3%), 536 (55.5%) at Visit 3 and 151 (15.6%) at Visit 4.
Exacerbations During the Study
At the initial visit, 76.5% of patients reported exacerbation of COPD in the 12-month period preceding the study entry. In the 6-month period between Visit 0 and Visit 1, this proportion was 68.3%, and in the 6-month period between all other visits – about 30%). About half of the patients experiencing exacerbations were hospitalized in the 12-month period preceding study entry and in the 6-month period between visits 0 and 1. At each subsequent visit, fewer exacerbating patients reported hospitalizations (from 27.7% at visit 2 to 18.4% at visit 4) (Figure 2).
Patients with exacerbations in the history had more frequently comorbidities (81.4% vs 67.9%, p<0.001) and less frequently were active smokers (32.3% vs 40.0%, p=0.016). Multivariate regression analysis revealed that independent predictors of being classified to C/D GOLD category (factors associated with the occurrence of exacerbations) were the presence of comorbidity and higher mMRC values (OR=1.556 [CI:1.099; 2.203], p=0.013 and OR=2.656 [CI:2.163; 3.262], p<0.001, respectively). Other factors taken into account, such as sex, age, BMI, severity of airway obstruction, the fact of smoking and a significant decrease in FEV1 were found to be not significant in this model. Detailed data for multivariate analysis are provided in Table 3.
Pulmonary Function
At the initial visit, the value of FEV1/FVC ratio was equal or less than 0.7 in 790 patients (81.9%). This group of patients was included in further analyses of pulmonary function. Based on the FEV1 parameters, the proportions of patients with mild, moderate, severe, and very severe airflow limitation were comparable between visits (see Table 4).
In 330 patients a decrease of FEV1 greater than 100 ml was observed, and these patients were defined as 'decliners'. The comparison of 'decliners' with 'non-decliners' is presented in Table 5. ‘Decliners’ had significantly better lung function (FEV1 and FVC) than those with stable lung function, however, there were no differences in terms of exacerbations.
The distribution of patients categorized by two systems of lung function impairment severity (GOLD and ATS/ERS) is presented in Figure 3. There were no patients categorized as GOLD-non-severe/ATS/ERS-severe (FEV1> 50% pred. and z-score <-4). The comparison of patients' GOLD/ATS/ERS categories is presented in Table 6.
COPD Symptoms, Severity of Dyspnea, and GOLD Classification of the Study Patients
In 36.4% of patients the, COPD symptoms occurred between 5 and 10 years before enrolment in the study. In approximately one-quarter cases, the symptoms persisted between 2 and 5 years (25.7%) and between 10 and 20 years (25.6%). The mean time since the diagnosis was 6.42 (5.32) years.
The most common symptom of COPD at each visit was shortness of breath during exercise (approximately 90% of patients). According to GOLD 2017-2022 recommendations, at initial visit, the majority of the patients were categorized into GOLD D group (49.8%), followed by GOLD B (41.2%), GOLD A (7.3%), and GOLD C groups (1.6%) – see Table 7).
The severity of dyspnea was assessed using a mMRC questionnaire and was stable from visit to visit. At each visit about 80% of patients had a mMRC ≧ 2. About half of patients had mMRC grade 2. The second most numerous groups were patients with mMRC grade 3 (about 30%), then with grade 1 (about 20%). Fewest patients had grade 4 (about 3%) or 0 (about 1.5%) dyspnea severity. In the CAT test patients obtained median scores from 15 to 17 points and these results were comparable for each visit (17 [IQR:11-22] for initial visit; 16 [11-21] at 6-month; 16 [11-21] at 12-month; 15 [10-20] at 18-month and 17 [13-21] at 24-month visit]). At each visit at least 80% of patients had CAT score ≧ 10. Figure 4 presents the proportions of patients with mMRC levels (A) and CAT more or less than 10 points (B).
Discussion
This non-interventional observational study aimed to assess the frequency of COPD exacerbations and hospitalizations due to these exacerbations and to evaluate the changes in lung function for 2 years observation period in patients treated with ICS/LABA in everyday medical practice in Poland. Patient-related outcomes, such as symptoms, smoking habits, and type of treatment were also recorded during this study. Moreover, in this publication, the risk of COPD exacerbations was assessed using a new strategy of pulmonary functional test interpretation recommended by the ATS/ERS in 2022[6].
The results of our study demonstrated that the lung function of study patients measured by FEV1 did not change during the study (Table 4). The proportion of patients with mild, moderate, severe, and very severe airflow limitations was generally stable throughout the study. At initial visit patients had mild airflow limitation accounted for 2.5%, with moderate airflow limitation for 25.1%, with severe – for 59.0% and with very severe – and 13.4% (Table 4). Comparable distribution of airflow limitation severity categories can be found in other real-life studies where approximately 10% of patients are categorized with very severe airflow limitation and the patients with mild category are the less numerous (approximately 2-3%)[14,15,16]. An interesting observation is that the decliners were mainly in the group with milder airflow limitation, which agrees with observations from large clinical trials[17].
Above 75% of patients enrolled in the study experienced exacerbation of COPD, and almost half of them were hospitalized due to exacerbation in 12-months period preceding the study entry (Figure 2). This proportion is relatively high and shows that COPD leads to a significant medical and financial burden on the Polish healthcare system. Interestingly, 330 patients were defined as 'decliners' (the decrease of FEV1 greater than 100 ml was observed during the study conduct), but the rate of exacerbation in this group was similar to that in 'non-decliners' (Table 3).
A wide range of exacerbating COPD patient proportions can be found in other real-life studies. In Bulgarian 1-year prospective observational study, the percentage of patients with exacerbations in 12-months period before the study was similar, accounting for approximately 75%[18]. Two large observational studies conducted in Central and Eastern European countries, Switzerland and Israel, also demonstrated comparable proportions of exacerbating COPD in similar periods [14,15]. The POPE study, another observational study conducted in Central and Eastern European countries, demonstrated much lower percentage of exacerbating patients accounting for 37%)[19]. The German study DACCORD showed that only about 20-25% of COPD patients had exacerbation in 6-months period prior to the study entry[16,20]. Another German non-interventional study on 3653 COPD patients reported a 35% frequency of exacerbations in the 2-years period preceding the study entry[21].
The categorization of patients by two systems of lung function impairment severity evaluation (GOLD and ATS/ERS) showed that there were no patients categorized simultaneously as GOLD-non-severe and ATS/ERS-severe (FEV1> 50% pred. and z-score <-4) (Figure 3). Patients categorized by the two systems as non-severe statistically significantly more frequently were decliners (Table 5). Patients classified into different severity lung function groups (non-severe and severe, independent of the method of classification GOLD or ATS/ERS) had similar exacerbation risk, demonstrating that the new ATS/ERS 2022 strategy for evaluation of lung function impairment severity seems inappropriate for the assessment of exacerbation risk.
The classic risk factors for COPD are male sex and tobacco smoking. According to meta-analysis performed in 2018, the prevalence of COPD among women is 6.16% and among men – 9.23%[22]. In our study men accounted for 67% of enrolled patients and were also more numerous in 'decliners' comparing with non-decliners' (74% vs 64%, p=0.004). Tobacco smoke is the most common cause of COPD, and smoking cessation is recommended for all smoking COPD patients[23]. In the present study smokers accounted for 35.8%, whereas ex-smokers for 55.2% (Table 1), which indicates that the vast majority of patients enrolled in our study were exposed to the tobacco smoke in some period of their lives. These results are generally in line with data from other real-life studies showing that at least 75% of studied COPD patients were current or ex-smokers[14,15,16,18,19,20].
In our study, the number of exacerbations and hospitalizations reported by patients at each visit decreased. Other real-life studies have also shown that during the study course, patients usually improve their state, especially in the first 6 months of the study[15,20]. It was observed that shortly after enrolment in the study, patients adhered to the treatment very well and therefore experienced significant health improvement. Other patient-related outcomes, such as severity of dyspnea measured by mMRC score (grade 2 in half of patients) and CAT (median score from 15 to 17 points) were generally stable throughout the study (Figure 2). According to the GOLD 2017-2022 strategy of classification, we identified the following distribution in the study groups A/B/C/D: 6.7%/41.5%/1.4%,/50.4%, respectively. During this study, data on concomitant diseases and medications were collected. Hypertension was the most frequent concomitant disease reported by the study patients, followed by ischemic heart disease, heart failure, diabetes, and hyperlipidemia (Table 1). The high prevalence of cardiovascular diseases in COPD patients has been reported in other real-life studies[14,15,16,21]. Other important comorbidities in COPD are depression and anxiety, which are associated with poor prognosis and the risk of exacerbations[24,25]. It has been demonstrated that the prevalence of depression in COPD patients is approximately 25% [26]. In our study, depression and anxiety disorders were diagnosed in approximately 7% of patients, which may suggest the underdiagnosis of these disorders in Polish COPD population. The medication taken during the study was stable (Table 2), and there were three combinations of ICS/LABA: extrafine beclomethasone/formoterol, fluticasone propionate/salmeterol, or budesonide/formoterol. Data on the impact of ICS/LABA combination on patient state were not gathered in this study; however, it is known that these three combinations are comparable in terms of their effectiveness and safety, and there is no evidence for the superiority of either ICS/LABA combination in the published literature[27,28,29,30,31,32].
This study has several strengths and limitations. The strong point of this study is its observational, real-world design and long duration, enabling collection of patient-related outcomes and data describing everyday life of ICS/LABA-treated COPD patients in Poland. This study is the first to analyze the use of ICS/LABA fixed-dose combination in the Polish COPD population and utilized the new ATS/ERS 2022 recommendation for the evaluation of lung function impairment severity[6]. The main limitation of the study was the gradual reduction of participants from visit to visit (from 922 at Visit 1 to 151 at Visit 4). The small number of patients at visit 4 impedes proper statistical analysis and weakens the conclusions drawn from the obtained results. However, the reduction in the number of participants is a normal phenomenon in observational studies because, with time, patients lose their interest in participation in the study.
Conclusions
This non-interventional, observational study on COPD patients treated with ICS/LABA in every day medical practice in Poland showed that during 2-year period, pulmonary function, medical treatment, and patient-related outcomes such as severity of dyspnea measured by mMRC score and CAT were generally stable throughout the study;, however in about 30% of patients, a decrease in lung FEV1 loss greater than 100 ml was observed. The new strategy for evaluating lung function impairment severity according to the new ATS/ERS 2022 recommendations utilizing FEV1 z-score value seems to not add benefit in assessing exacerbation risk. Factors that were found to be associated with the occurrence of exacerbations and were classified into the C/D GOLD category included the presence of comorbidities and increased symptoms. The frequency of exacerbations decreased, especially in the first six months of the study, compared to the initial visit, which is a phenomenon already observed in other non-interventional studies.
Author Contributions
PWB: conception and design, data analysis and interpretation, writing draft and final version of the manuscript; TD: conception and design, data collection, writing draft and final version of the manuscript, corresponding author; RP: conception and design, data collection, writing draft and final version of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Chiesi Poland Sp. z o.o.
Conflicts of Interest
PWB reports personal fees from AstraZeneca, personal fees from Boehringer-Ingelheim, personal fees from Berlin-Chemie-Menarini, personal fees from Pfizer, and Chiesi, all outside the submitted work. TD reports being an employee of Chiesi Poland Sp. z o.o. RP reports. All other authors have no conflicts of interest to disclose regarding the present study.
References
- Decramer M, Janssens W, Miravitlles M. Chronic obstructive pulmonary disease. Lancet Lond Engl 2012;379:1341–51. [CrossRef]
- Bousquet J, Kiley J, Bateman ED, Viegi G, Cruz AA, Khaltaev N, et al. Prioritised research agenda for prevention and control of chronic respiratory diseases. Eur Respir J 2010;36:995–1001. [CrossRef]
- Celli BR, Wedzicha JA. Update on Clinical Aspects of Chronic Obstructive Pulmonary Disease. N Engl J Med 2019;381:1257–66. [CrossRef]
- Yawn BP, Mintz ML, Doherty DE. GOLD in Practice: Chronic Obstructive Pulmonary Disease Treatment and Management in the Primary Care Setting. Int J Chron Obstruct Pulmon Dis 2021;16:289–99. [CrossRef]
- Janson C, Marks G, Buist S, Gnatiuc L, Gislason T, McBurnie MA, et al. The impact of COPD on health status: findings from the BOLD study. Eur Respir J 2013;42:1472–83. [CrossRef]
- Stanojevic S, Kaminsky DA, Miller MR, Thompson B, Aliverti A, Barjaktarevic I, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J 2022;60. [CrossRef]
- Ferguson GT, Tashkin DP, Skärby T, Jorup C, Sandin K, Greenwood M, et al. Effect of budesonide/formoterol pressurized metered-dose inhaler on exacerbations versus formoterol in chronic obstructive pulmonary disease: The 6-month, randomized RISE (Revealing the Impact of Symbicort in reducing Exacerbations in COPD) study. Respir Med 2017;132:31–41. [CrossRef]
- Calverley PM, Anderson JA, Celli B, Ferguson GT, Jenkins C, Jones PW, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007;356:775–89. [CrossRef]
- Zheng J-P, Yang L, Wu YM, Chen P, Wen ZG, Huang W-J, et al. The Efficacy and Safety of Combination Salmeterol (50 μg)/Fluticasone Propionate (500 μg) Inhalation Twice Daily Via Accuhaler in Chinese Patients With COPD. Chest 2007;132:1756–63. [CrossRef]
- Jenkins CR, Jones PW, Calverley PMA, Celli B, Anderson JA, Ferguson GT, et al. Efficacy of salmeterol/fluticasone propionate by GOLD stage of chronic obstructive pulmonary disease: analysis from the randomised, placebo-controlled TORCH study. Respir Res 2009;10:59–59. [CrossRef]
- Wedzicha JA, Singh D, Vestbo J, Paggiaro PL, Jones PW, Bonnet-Gonod F, et al. Extrafine beclomethasone/formoterol in severe COPD patients with history of exacerbations. Respir Med 2014;108:1153–62. [CrossRef]
- Ming SWY, Haughney J, Ryan D, Small I, Lavorini F, Papi A, et al. A Comparison of the Real-Life Clinical Effectiveness of the Leading Licensed ICS/LABA Combination Inhalers in the Treatment for COPD. Int J Chron Obstruct Pulmon Dis 2020;15:3093–103. [CrossRef]
- Quanjer PH, Stanojevic S, Cole TJ, Baur X, Hall GL, Culver BH, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J 2012;40:1324–43. [CrossRef]
- Valipour A, Avdeev S, Barczyk A, Bayer V, Fridlender Z, Georgieva M, et al. Therapeutic Success of Tiotropium/Olodaterol, Measured Using the Clinical COPD Questionnaire (CCQ), in Routine Clinical Practice: A Multinational Non-Interventional Study. Int J Chron Obstruct Pulmon Dis 2021;16:615–28. [CrossRef]
- Valipour A, Tamm M, Kociánová J, Bayer V, Sanzharovskaya M, Medvedchikov A, et al. Improvement In Self-Reported Physical Functioning With Tiotropium/Olodaterol In Central And Eastern European COPD Patients. Int J Chron Obstruct Pulmon Dis 2019;14:2343–54. [CrossRef]
- Buhl R, Criée C-P, Kardos P, Vogelmeier CF, Kostikas K, Lossi NS, et al. Dual bronchodilation vs triple therapy in the “real-life” COPD DACCORD study. Int J Chron Obstruct Pulmon Dis 2018;13:2557–68. [CrossRef]
- Tantucci C, Modina D. Lung function decline in COPD. Int J Chron Obstruct Pulmon Dis 2012;7:95–9. [CrossRef]
- Ivanov Y, Nikolaev I, Nemeth I. Real-life evaluation of COPD treatment in a Bulgarian population: a 1-year prospective, observational, noninterventional study. Int J Chron Obstruct Pulmon Dis 2018;13:653–63. [CrossRef]
- Koblizek V, Milenkovic B, Barczyk A, Tkacova R, Somfay A, Zykov K, et al. Phenotypes of COPD patients with a smoking history in Central and Eastern Europe: the POPE Study. Eur Respir J 2017;49:1601446. [CrossRef]
- Worth H, Buhl R, Criée C-P, Kardos P, Mailänder C, Vogelmeier C. The ‘real-life’ COPD patient in Germany: The DACCORD study. Respir Med 2016;111:64–71. [CrossRef]
- Plate T, Friedrich FW, Beier J. Effectiveness and Tolerability of LABA/LAMA Fixed-Dose Combinations Aclidinium/Formoterol, Glycopyrronium/Indacaterol and Umeclidinium/Vilanterol in the Treatment of COPD in Daily Practice - Results of the Non-Interventional DETECT Study. Int J Chron Obstruct Pulmon Dis 2020;15:1335–47. [CrossRef]
- Ntritsos G, Franek J, Belbasis L, Christou MA, Markozannes G, Altman P, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis 2018;Volume 13:1507–14. [CrossRef]
- Lopez, AD. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J 2006;27:397–412. [CrossRef]
- Blakemore A, Dickens C, Chew-Graham CA, Afzal CW, Tomenson B, Coventry PA, et al. Depression predicts emergency care use in people with chronic obstructive pulmonary disease: a large cohort study in primary care. Int J Chron Obstruct Pulmon Dis 2019;14:1343–53. [CrossRef]
- Vikjord SAA, Brumpton BM, Mai X-M, Romundstad S, Langhammer A, Vanfleteren L. The HUNT study: Association of comorbidity clusters with long-term survival and incidence of exacerbation in a population-based Norwegian COPD cohort. Respirology 2022;27:277–85. [CrossRef]
- Zhang MWB, Ho RCM, Cheung MWL, Fu E, Mak A. Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: a systematic review, meta-analysis and meta-regression. Gen Hosp Psychiatry 2011;33:217–23. [CrossRef]
- Solidoro P, Patrucco F, Bagnasco D. Comparing a fixed combination of budesonide/formoterol with other inhaled corticosteroid plus long-acting beta-agonist combinations in patients with chronic obstructive pulmonary disease: a review. Expert Rev Respir Med 2019;13:1087–94. [CrossRef]
- Larsson K, Janson C, Lisspers K, Jørgensen L, Stratelis G, Telg G, et al. Combination of budesonide/formoterol more effective than fluticasone/salmeterol in preventing exacerbations in chronic obstructive pulmonary disease: the PATHOS study. J Intern Med 2013;273:584–94. [CrossRef]
- Partridge MR, Schuermann W, Beckman O, Persson T, Polanowski T. Effect on lung function and morning activities of budesonide/formoterol versus salmeterol/fluticasone in patients with COPD. Ther Adv Respir Dis 2009;3:147–57. [CrossRef]
- Roberts M, Mapel D, Petersen H, Blanchette C, Ramachandran S. Comparative effectiveness of budesonide/formoterol and fluticasone/salmeterol for COPD management. J Med Econ 2011;14:769–76. [CrossRef]
- Kern DM, Davis J, Williams SA, Tunceli O, Wu B, Hollis S, et al. Comparative effectiveness of budesonide/formoterol combination and fluticasone/salmeterol combination among chronic obstructive pulmonary disease patients new to controller treatment: a US administrative claims database study. Respir Res 2015;16:52–52. [CrossRef]
- Perrone V, Sangiorgi D, Buda S, Degli Esposti L. Comparative analysis of budesonide/formoterol and fluticasone/salmeterol combinations in COPD patients: findings from a real-world analysis in an Italian setting. Int J Chron Obstruct Pulmon Dis 2016;11:2749–55. [CrossRef]
Figure 1.
Data collected during initial visit and next visits.
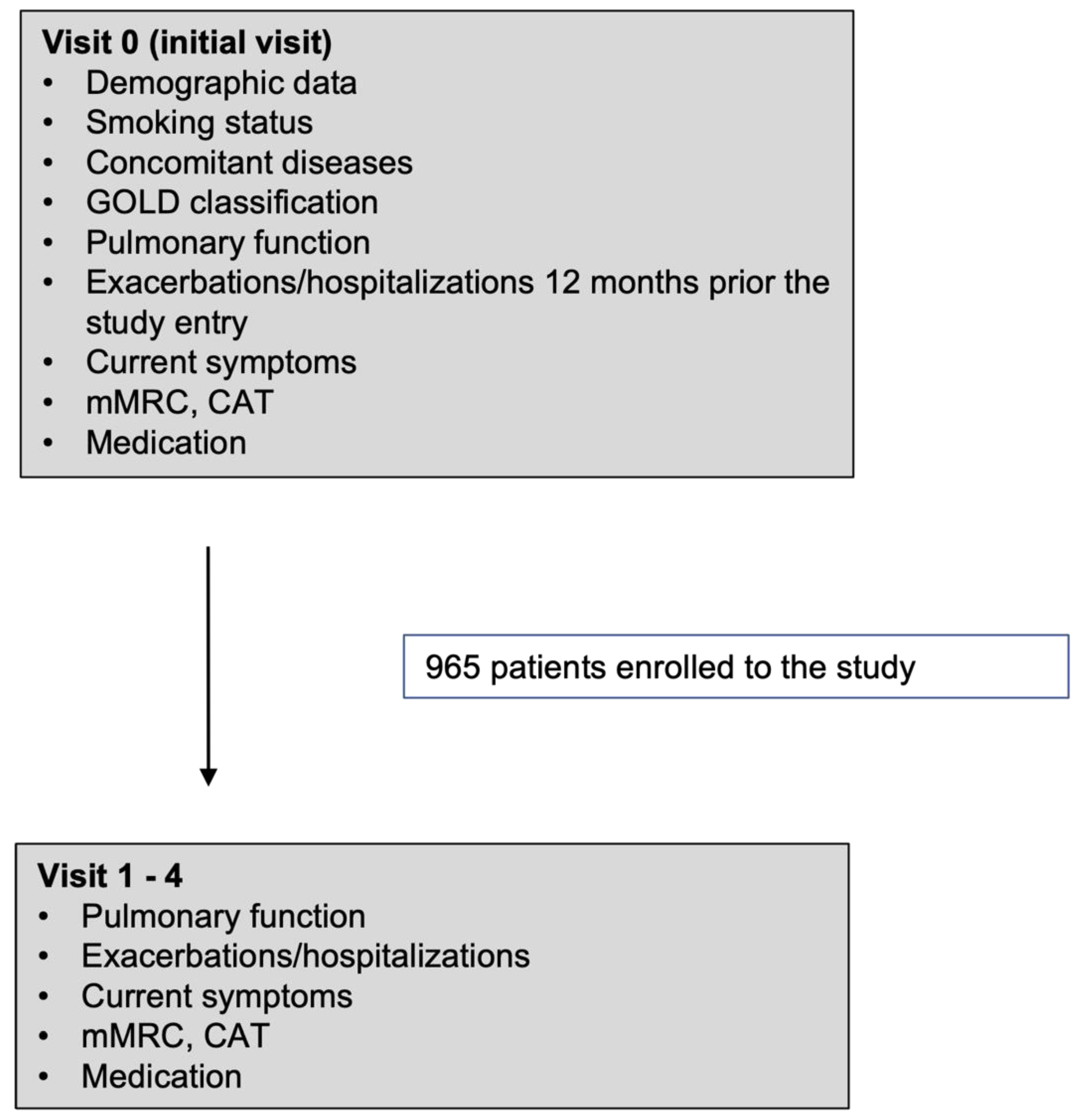
Figure 2.
Proportions of COPD patients reporting no exacerbations (blue bar), exacerbations without hospitalization (orange bars) and severe exacerbations requiring hospitalization (grey bars). Proportions are demonstrated for each visit and are derived from the total number of 932 patients for Visit 0, 703 for 6-month, 578 for 12-month, 531 for 18-month and 149 for 24-month visit.
Figure 2.
Proportions of COPD patients reporting no exacerbations (blue bar), exacerbations without hospitalization (orange bars) and severe exacerbations requiring hospitalization (grey bars). Proportions are demonstrated for each visit and are derived from the total number of 932 patients for Visit 0, 703 for 6-month, 578 for 12-month, 531 for 18-month and 149 for 24-month visit.
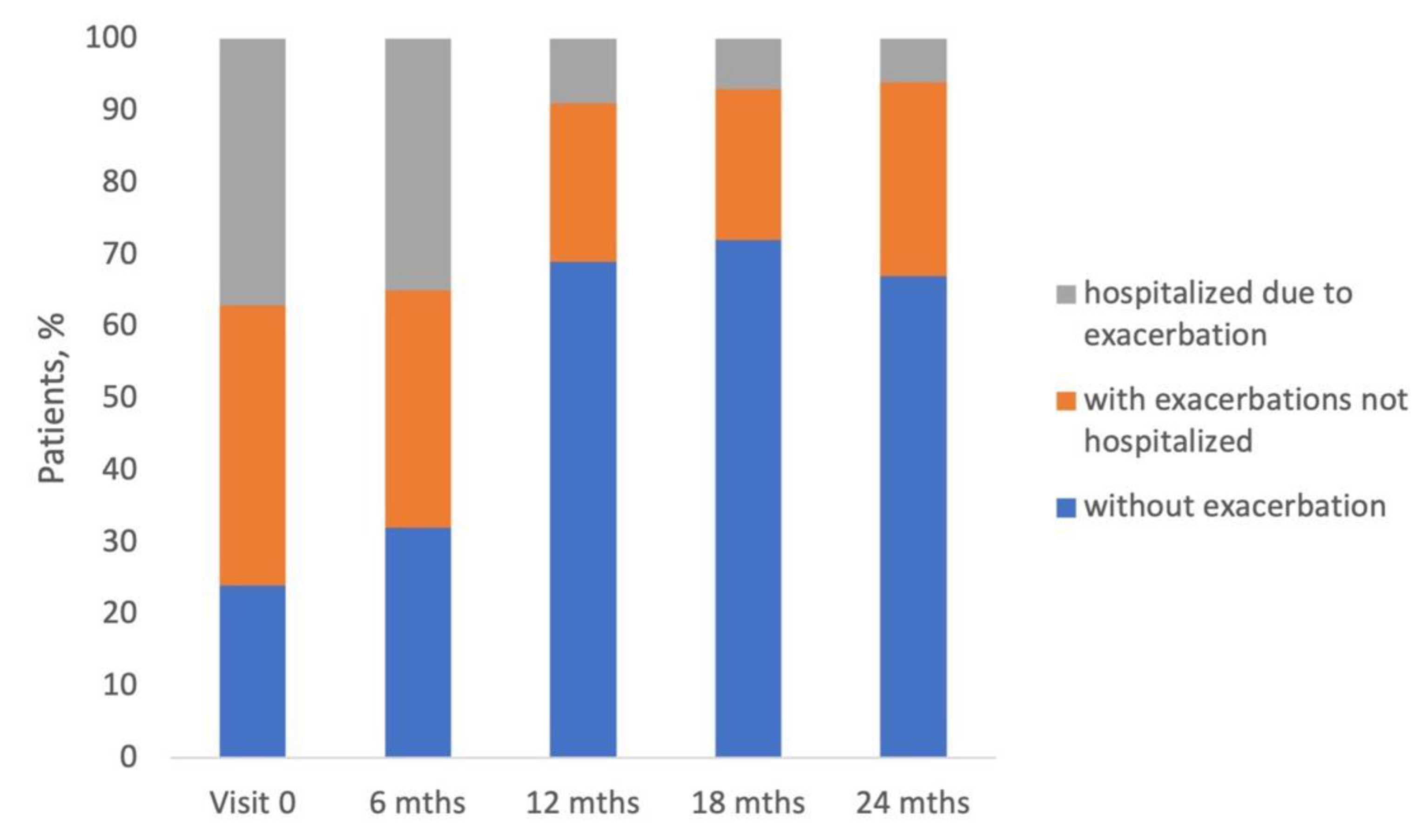
Figure 3.
The distribution of patients categorized by two systems of lung function impairment severity: GOLD, based on FEV 1 % of predicted value, and ATS/ERS based on FEV1 z-score.
Figure 3.
The distribution of patients categorized by two systems of lung function impairment severity: GOLD, based on FEV 1 % of predicted value, and ATS/ERS based on FEV1 z-score.
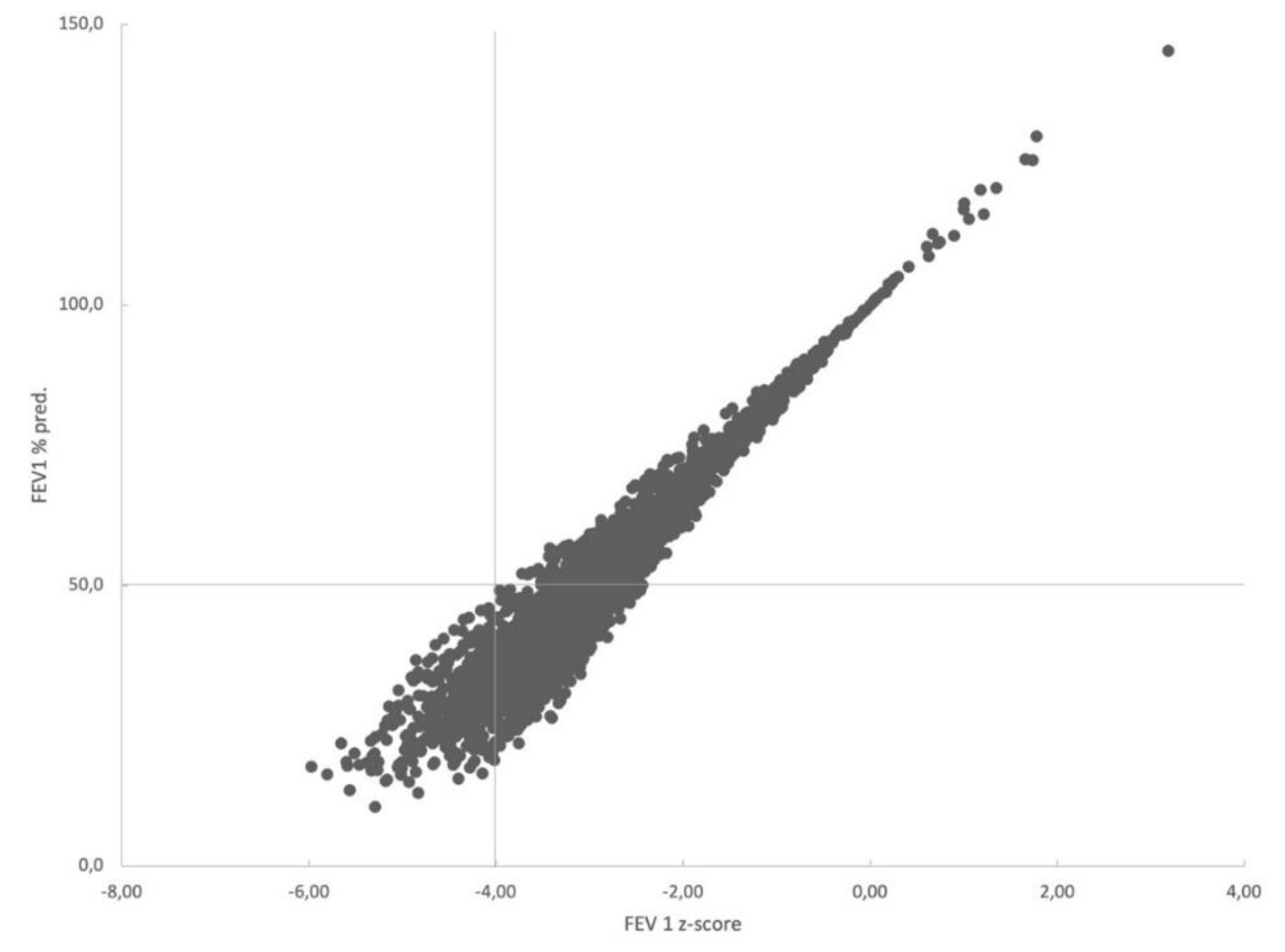
Figure 4.
Percentages of patients declaring mMRC and CAT scores at subsequent visits.
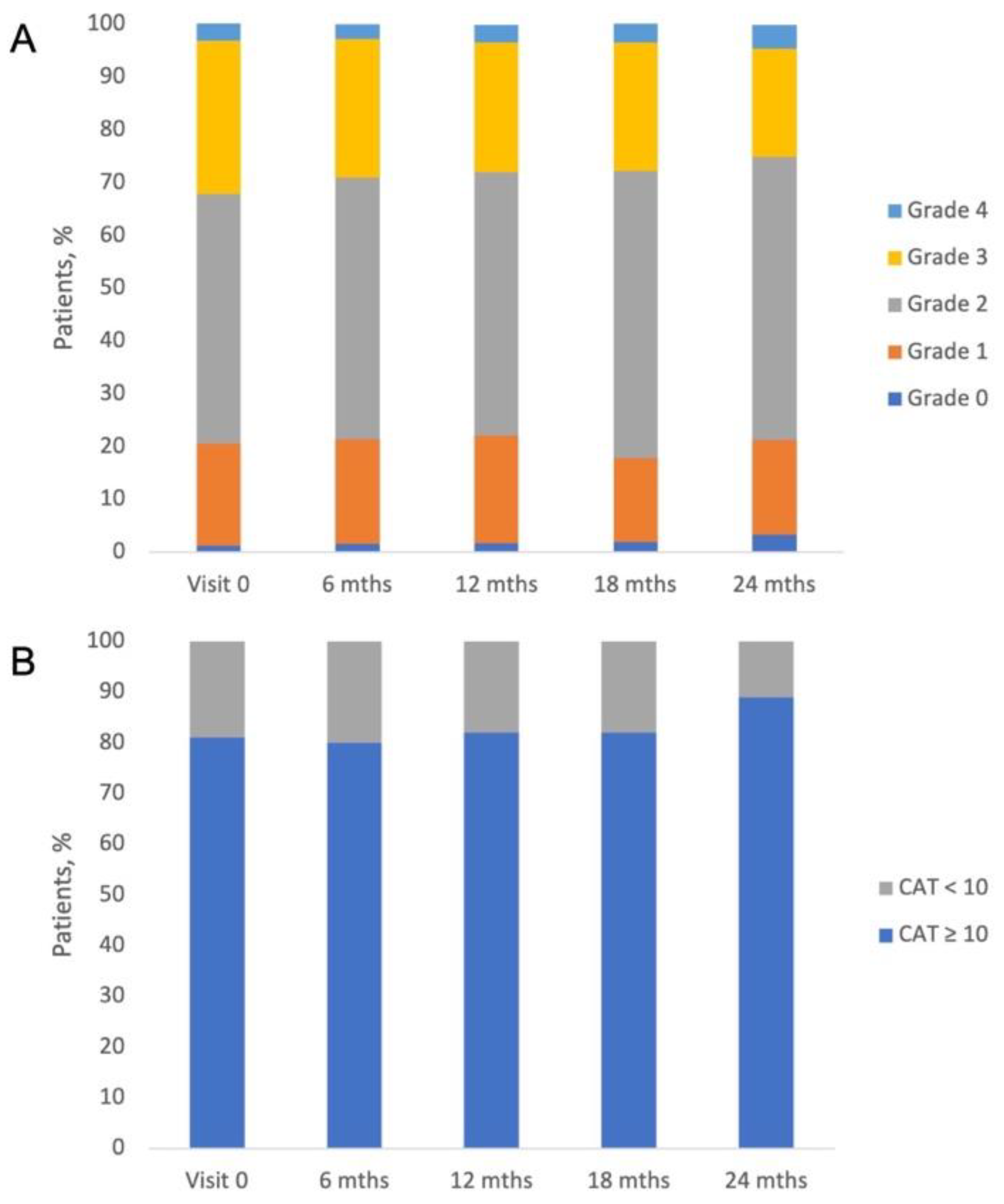

Table 1.
Characteristics of the study patients: demographic data, smoking status, concomitant diseases.
Table 1.
Characteristics of the study patients: demographic data, smoking status, concomitant diseases.
| Characteristic | N = 965 |
|---|---|
| Age [years] | |
| Mean (SD) | 66.9 (9.4) |
| Missing | 4 |
| Gender, n (%) | |
| Female | 311 (32.2) |
| Male | 651 (67.5) |
| Missing | 3 (0.3) |
| BMI [kg/m2] | |
| Mean (SD) | 27.1 (5.4) |
| Missing | 6 |
| Smoker, n (%) | |
| Smoker | 345 (35.8) |
| Ex-Smoker | 533 (55.2) |
| Non-smoker | 80 (8.3) |
| Missing | 7 (0.7) |
| Concomitant diseases; n (%) | |
| Hypertension | 568 (70.7) |
| Ischemic heart disease | 249 (31) |
| Heart failure | 165 (20.5) |
| Diabetes | 154 (19.2) |
| Hyperlipidemia | 153 (19.1) |
| Osteoporosis | 60 (7.5) |
| Depression and anxiety disorder | 55 (6.8) |
| Myopathy (muscle weakness) | 45 (5.6) |
| Persistent atrial fibrillation | 36 (4.5) |
| Paroxysmal atrial fibrillation | 33 (4.1) |
| Lung cancer | 7 (0.9) |
| Other cancers | 29 (3.6) |
| Sleep apneas | 15 (1.9) |
| Other disorders | 310 (32.1) |
Table 2.
Pharmacotherapy of patients during the study.
| Parameter | Visit 0 | Visit 1 | Visit 2 | Visit 3 | Visit 4 |
|---|---|---|---|---|---|
| Short-acting beta2-adrenergic agonists | 416 (43.1%) | 328 (37.8%) | 275 (38.9%) | 214 (39.9%) | 70 (46.4%) |
| LABAs | 69 (7.2%) | 54 (6.2%) | 47 (6.6%) | 40 (7.5%) | 8 (5.3%) |
| Short-acting anticholinergics | 256 (26.5%) | 199 (23%) | 161 (22.8%) | 122 (22.8%) | 45 (29.8%) |
| LAMAs | 600 (62.2%) | 511 (58.9%) | 481 (68%) | 373 (69.6%) | 104 (68.9%) |
| ICS | 26 (2.7%) | 23 (2.7%) | 26 (3.7%) | 24 (4.5%) | 3 (2%) |
| ICS/LABA | 926 (96%) | 813 (93.8%) | 704 (99.6%) | 525 (97.9%) | 147 (97.4%) |
| Beclomethasone/ formoterol | 364 (37.7%) | 320 (36.9%) | 276 (39%) | 198 (36.9%) | 53 (35.1%) |
| Budesonide/ formoterol | 208 (21.6%) | 179 (20.6%) | 154 (21.8%) | 119 (22.2%) | 24 (15.9%) |
| Fluticasone/salmeterol | 354 (36.7%) | 314 (36.2%) | 274 (38.8%) | 208 (38.8%) | 70 (46.4%) |
| PD4 inhibitors | 2 (0.2%) | 2 (0.2%) | 2 (0.3%) | 1 (0.2%) | 0 (0.0%) |
| Aminophylline | 369 (38.2%) | 308 (35.5%) | 274 (38.8%) | 217 (40.5%) | 69 (45.7%) |
| Other drugs | 25 (2.6%) | 29 (3.0%) | 36 (3.7%) | 38 (3.9%) | 11 (1.1%) |
Table 3.
Odds ratios and 95% confidence intervals for factors associated with exacerbations (univariate analysis and multivariate model).
Table 3.
Odds ratios and 95% confidence intervals for factors associated with exacerbations (univariate analysis and multivariate model).
| Variable | Coefficient | Odds ratio | 95% CI | p-value |
|---|---|---|---|---|
| Male sex | -0.2682 | 0.7648 | 0.5631 to 1.0387 | 0.086 |
| Age (years)_ | -0.00057465 | 0.9994 | 0.9820 to 1.0172 | 0.9491 |
| BMI kg/m2 | -0.017148 | 0.9830 | 0.9571 to 1.0096 | 0.2083 |
| Comorbidities | 0.44212 | 1.5560 | 1.0989 to 2.2033 | 0.0127 |
| GOLD-severe – ATS/ERS non-severe* | -0.014633 | 0.9855 | 0.7152 to 1.3580 | 0.9287 |
| GOLD-severe – ATS/ERS-severe* | -0.020001 | 0.9802 | 0.6148 to 1.5627 | 0.933 |
| ‘Decliner’ | -0.069795 | 0.9326 | 0.6924 to 1.2561 | 0.646 |
| mMRC | 0.97698 | 2.6564 | 2.1632 to 3.2621 | <0.0001 |
| Smoking | -0.27197 | 0.7619 | 0.5575 to 1.0411 | 0.0878 |
* vs. GOLD non-severe ATS/ERS non-severe.
Table 4.
Airflow limitation grades based on FEV1 expressed as % of predicted value according to GOLD 2017-2022.
Table 4.
Airflow limitation grades based on FEV1 expressed as % of predicted value according to GOLD 2017-2022.
| Airflow limitation, n (%) | Visit 0 | 6 months | 12 months | 18 months | 24 months |
|---|---|---|---|---|---|
| Mild (>80%) | 20 (2.5) | 28 (4.6) | 20 (3.7) | 15 (4.0) | 3 (2.6) |
| Moderate (50%-80%) | 198 (25.1) | 173 (28.5) | 155 (28.9) | 117 (31.0) | 30 (25.9) |
| Severe (30%-50%) | 466 (59.0) | 321 (52.9) | 293 (54.7) | 194 (51.5) | 66 (56.9) |
| Very severe (<30%) | 106 (13.4) | 85 (14.0) | 68 (12.7) | 51 (13.5) | 17 (14.7) |
Table 5.
Comparison of 'decliners' and 'non-decliners' populations.
| Characteristic | Decliners, N=330 | Non-decliners, N=592 | p-value | |
|---|---|---|---|---|
| Males, n (%) | 244 (73.9) | 382 (64.5) | 0.004 a | |
| Age, years (median, IQR) | 66 (60 - 72) | 67 (61 - 75) | 0.026 b | |
| FEV1 % pred. median (IQR) | 46.62 (38.66 - 59.22) | 42.06 (33.76 - 53.6) | <0.001 b | |
| FEV1 (z-score) (mean, SD) | -2.96 (1.04) | -3.21 (1) | <0.001 c | |
| FVC % pred.median (IQR) | 68.66 (57.41 - 80.66) | 62.92 (52.07 - 75.3) | <0.001 b | |
| FVC (z-score) mean (SD) | -1.99 (1.17) | -2.29 (1.23) | <0.001 c | |
| GOLD-non-severe/ATS/ERS-non-severe, n (%) | 139 (42.1) | 176 (29.7) | 0.004 a | |
| GOLD-severe/ATS/ERS-non-severe, n (%) | 155 (47.0) | 300 (50.7) | ||
| GOLD-severe/ATS/ERS-severe, n (%) | 36 (10.9) | 116 (19.6) | ||
| CAT, median (IQR) | 17 (12 - 22) | 17 (11 - 23) | 0.549 b | |
| mMRC grade, n (%) | 0 | 1 (0.3) | 9 (1.5) | 0.004 a |
| 1 | 72 (21.8) | 105 (17.9) | ||
| 2 | 176 (53.3) | 256 (43.6) | ||
| 3 | 74 (22.4) | 194 (33.0) | ||
| 4 | 7 (2.1) | 23 (3.9) | ||
| Exacerbations, n (%) | yes | 285 (88.2) | 507 (88.6) | 0.943 a |
| no | 38 (11.8) | 65 (11.4) | ||
| Ever-smokers, n (%) | yes | 308 (93.9) | 534 (90.5) | 0.096 a |
| no | 20 (6.1) | 56 (9.5) | ||
| Cardiovascular disease, n (%) | yes | 125 (37.9) | 234 (39.5) | 0.673 a |
| no | 205 (62.1) | 358 (60.5) |
Statistical significance of differences assessed by: a - Chi2 test; b - Mann-Whitney U test; c - T test.
Table 6.
Comparison of patients categorized by two systems of lung function impairment severity (GOLD and ATS/ERS).
Table 6.
Comparison of patients categorized by two systems of lung function impairment severity (GOLD and ATS/ERS).
| Characteristic | GOLD-non-severe/ATS/ERS-non-severe | GOLD-severe/ATS/ERS-non-severe | GOLD-severe/ATS/ERS-severe | p-value | |
|---|---|---|---|---|---|
| Males, n (%) | 190 (60.3) | 325 (71.4) | 111 (73.0) | 0.002 a | |
| Age [years], median (IQR) | 67 (60 - 75) | 69 (64 - 75) | 60 (55 - 64) | <0.001 b | |
| FEV1 % pred., median (IQR) | 62.68 (55.69 - 73.6) | 40.78 (36.51 - 45.06) | 28.73 (25.26 - 33.98) | <0.001 b | |
| FEV1 (z-score), mean (SD) | -2.06 (0.88) | -3.43 (0.34) | -4.41 (0.38) | <0.001 c | |
| FVC % pred., median (IQR) | 78.16 (67.88 - 90.72) | 60.82 (52.44 - 71.44) | 50.94 (42.93 - 60.41) | <0.001 b | |
| FVC (z-score), mean (SD) | -1.32 (1.03) | -2.39 (0.99) | -3.36 (0.87) | <0.001 c | |
| Decliners, n (%) | 139 (44.1) | 155 (34.1) | 36 (23.7) | <0.001 a | |
| Non-decliners, n (%) | 176 (55.9) | 300 (65.9) | 116 (76.3) | ||
| mMRC grade, n (%) | 0 | 8 (2.6) | 2 (0.4) | 0 (0) | <0.001 a |
| 1 | 85 (27.2) | 68 (15.0) | 24 (15.8) | ||
| 2 | 156 (50.0) | 214 (47.2) | 62 (40.8) | ||
| 3 | 60 (19.2) | 154 (34.0) | 54 (35.5) | ||
| 4 | 3 (1.0) | 15 (3.3) | 12 (7.9) | ||
| CAT, median (IQR) | 16 (10.25 - 22) | 16 (11 - 22) | 19 (12 - 24.5) | 0.006 b | |
| Exacerbations, n (%) | yes | 267 (88.4) | 394 (88.9) | 131 (87.3) | 0.866 a |
| no | 35 (11.6) | 49 (11.1) | 19 (12.7) | ||
| Ever-smokers, n (%) | yes | 280 (89.5) | 417 (91.9) | 145 (96.0) | 0.055 a |
| no | 33 (10.5) | 37 (8.1) | 6 (4.0) | ||
| Cardiovascular disease, n (%) | yes | 114 (36.2) | 201 (44.2) | 44 (28.9) | 0.002 a |
| no | 201 (63.8) | 254 (55.8) | 108 (71.1) |
Statistical significance of differences assessed by: a - Chi2 test; b Kruskal-Wallis test; c ANOVA.
Table 7.
RT - % of raw total, CT - % of column total, GT - % of grand total.
| GOLD 2017-2022 category | |||||
| mMRC | A | B | C | D | |
| 0 | 9 | 1 | 0 | 0 | 10 (1.1%) |
| 1 | 58 | 75 | 15 | 29 | 177 (19.3%) |
| 2 | 0 | 219 | 0 | 213 | 432 (47.1%) |
| 3 | 0 | 80 | 0 | 188 | 268 (29.2%) |
| 4 | 0 | 3 | 0 | 27 | 30 (3.3%) |
| 67 (7.3%) | 378 (41.2%) | 15 (1.6%) | 457 (49.8%) | 917 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



