Submitted:
18 May 2025
Posted:
20 May 2025
You are already at the latest version
Abstract
Air pollution, particularly smog, has emerged as a major global health concern, with growing evidence linking its constituents to cardiovascular disease (CVD). This review critically examines the relationship between smog components—including fine particulate matter (PM2.5, PM10), nitrogen dioxide (NO₂), ozone (O₃), sulfur dioxide (SO₂), carbon monoxide (CO), carbon black, and polyaromatic hydrocarbons (PAHs)—and various cardiovascular outcomes such as ischemic heart disease (IHD), stroke, myocardial infarction, and arrhythmia. The pathophysiological mechanisms discussed include systemic inflammation, oxidative stress, endothelial dysfunction, autonomic imbalance, and thrombogenesis, supported by up-to-date epidemiological findings from both high-income and low- and middle-income countries.Special focus is given to Punjab, Pakistan, a region experiencing escalating levels of smog due to rapid urbanization, crop residue burning, and industrial emissions. Case studies and regional data highlight the acute rise in CVD burden correlated with seasonal smog episodes. This review also explores socioeconomic disparities, policy gaps, and mitigation strategies relevant to the region.By synthesizing global literature with local realities, the study underscores the urgent need for targeted environmental and public health interventions. Limitations in existing research and policy frameworks are addressed, and recommendations for interdisciplinary collaboration, early warning systems, and long-term air quality reforms are proposed.
Keywords:
Smog
; Cardiovascular Disease
; Air Pollution
; PM2.5
; Nitrogen Dioxide
; Punjab
; Stroke
; Ischemic Heart Disease
; Inflammation
; Oxidative Stress
Introduction
Air pollution is a critical environmental and public health issue worldwide, contributing substantially to morbidity and mortality. Among air pollution forms, smog is a dense mixture of air pollutants that has emerged as a particularly harmful phenomenon in urban and industrial regions (World Health Organization [WHO], 2021). Smog consists primarily of particulate matter (PM), ozone (O₃), nitrogen dioxide (NO₂), sulfur dioxide (SO₂), carbon monoxide (CO), carbon black, and polycyclic aromatic hydrocarbons (PAHs) (Brook et al., 2010; Cohen et al., 2017). These pollutants mainly originate from anthropogenic activities such as vehicle exhaust, industrial emissions, biomass burning, and fossil fuel combustion (Gupta et al., 2018; Hussain et al., 2020). Over the last few decades, smog episodes have become more frequent and severe, especially in developing countries with rapid urbanization and industrial growth (Kumar et al., 2019; Saeed et al., 2021).
Cardiovascular diseases (CVD) including ischemic heart disease (IHD), myocardial infarction (MI), stroke, and heart failure are the leading causes of death globally, accounting for nearly 31% of all deaths (Roth et al., 2020). Increasing evidence demonstrates that exposure to air pollution and smog significantly contributes to both the incidence and progression of CVD (Brook et al., 2010; Newby et al., 2015). The Global Burden of Disease study in 2019 estimated that ambient air pollution alone was responsible for approximately 4.14 million deaths worldwide, with a substantial fraction attributed to cardiovascular causes (GBD, 2019).
The link between smog components and cardiovascular health is complex, involving multiple biological pathways such as systemic inflammation, oxidative stress, endothelial dysfunction, and autonomic nervous system imbalance (Brook et al., 2010; Rajagopalan & Brook, 2012). While particulate matter, especially PM2.5, is the most extensively studied pollutant related to cardiovascular risk, gaseous pollutants like NO₂, ozone, SO₂, and CO also play important roles (Mustafic et al., 2012; Beelen et al., 2014).
Particulate Matter (PM2.5 and PM10)
Particulate matter, classified by aerodynamic diameter, includes PM2.5 (particles ≤2.5 μm) and PM10 (particles ≤10 μm). PM2.5 is of particular concern due to its ability to penetrate deep into lung tissue and enter the bloodstream (Brook et al., 2010; Miller et al., 2007). Chronic and acute exposures to PM2.5 are linked to systemic inflammation, increased blood coagulation, oxidative stress, atherosclerosis acceleration, and endothelial dysfunction, all contributing to adverse cardiovascular outcomes (Pope et al., 2004; Cesaroni et al., 2013; Rajagopalan & Brook, 2012).
A meta-analysis by Mustafic et al. (2012) quantified that short-term exposure to PM2.5 was associated with a 1.4% increase in risk of myocardial infarction per 10 μg/m³ rise in concentration. Long-term cohort studies have found stronger links, with increased rates of cardiovascular mortality and incident ischemic heart disease (Cesaroni et al., 2013; Wang et al., 2017). Studies also highlight that PM10 contributes to stroke risk, though its effects appear weaker than PM2.5 (Shah et al., 2015).
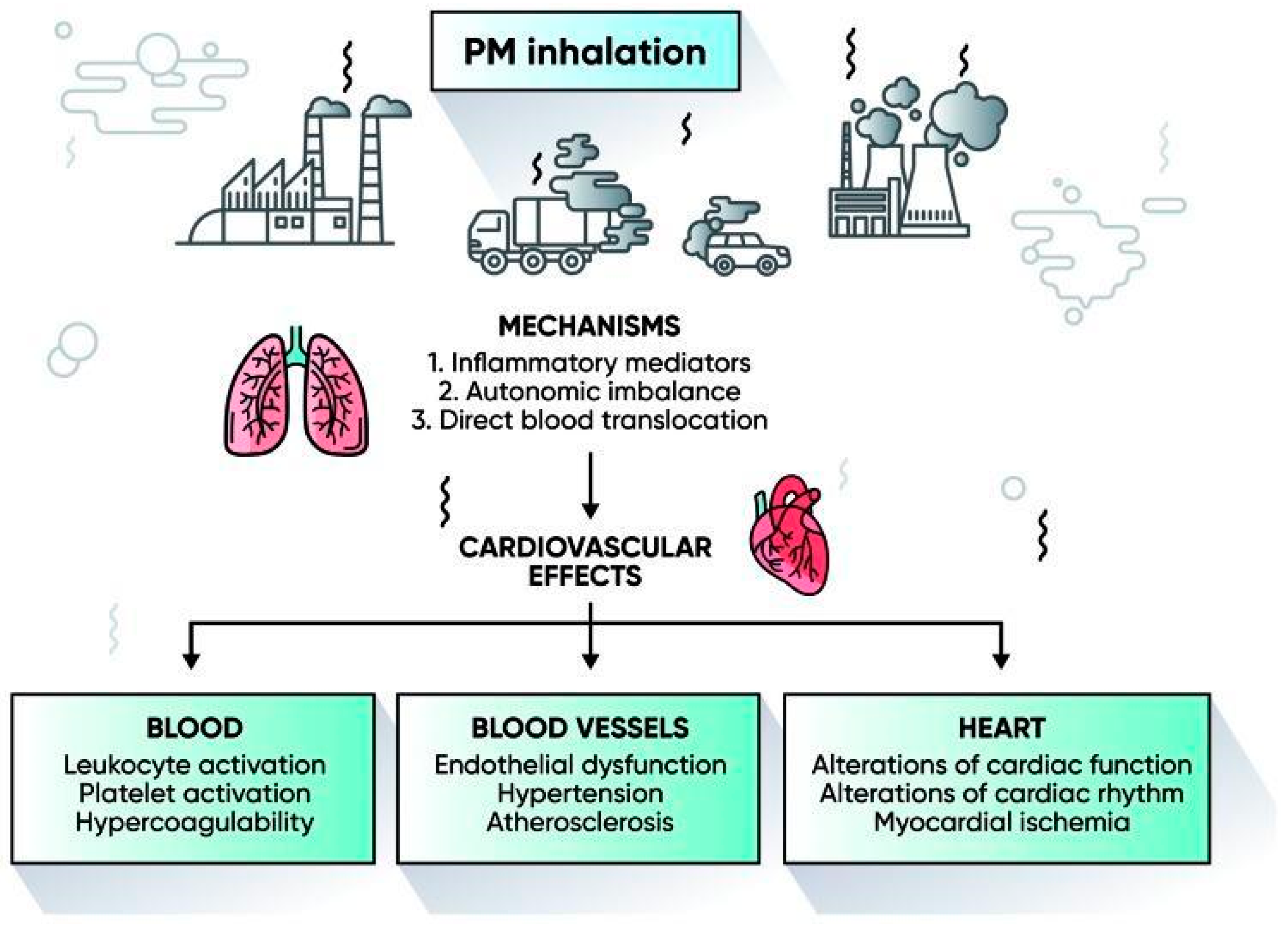
Figure 1.
Cardiovascular Effects of PM Inhalation.
Nitrogen Dioxide (NO₂)
NO₂, mainly from vehicle emissions and industrial sources, is a key marker for traffic-related pollution (Fuks et al., 2014). Exposure to NO₂ induces vascular inflammation and endothelial injury, which promote hypertension and atherosclerosis (Stieb et al., 2016; Hoek et al., 2013). Epidemiological studies show chronic NO₂ exposure increases cardiovascular mortality risk. Beelen et al. (2014) reported a 5% increase in cardiovascular deaths per 10 μg/m³ rise in NO₂ in European cohorts. Similar associations are emerging in Asian populations, highlighting the global health threat (Cai et al., 2019).
Ozone (O₃)
Ozone is a secondary pollutant formed by photochemical reactions between nitrogen oxides and volatile organic compounds under sunlight (Liu et al., 2019). It causes oxidative stress and systemic inflammation, increasing the risk of cardiovascular events (Wang et al., 2016). Though fewer studies focus on ozone compared to PM or NO₂, evidence links ozone peaks to increased hospital admissions for heart failure, arrhythmias, and stroke (Sacks et al., 2011).
Sulfur Dioxide (SO₂) and Carbon Monoxide (CO)
SO₂ is primarily released from coal combustion and industrial processes (Rajagopalan & Brook, 2012). It aggravates hypoxia and induces vascular dysfunction. Similarly, CO, generated by incomplete combustion, binds hemoglobin reducing oxygen transport and can trigger cardiac arrhythmias and ischemia (Ling & Yang, 2019). Both are established contributors to cardiovascular morbidity, particularly in areas with heavy fossil fuel use (Brook et al., 2010).
Polycyclic Aromatic Hydrocarbons (PAHs)
PAHs are a group of organic compounds produced by incomplete combustion, common in smog (Boström et al., 2002). They are genotoxic and pro-inflammatory, worsening vascular health and increasing the risk of atherosclerosis and other CVD (Yin et al., 2019). Though not as extensively studied as PM or gaseous pollutants, PAHs add to the cumulative toxic burden of smog.

Table 1.
Components and Concentration of Smog and their Cardiovascular Health Effects.
| Smog Component | Concentration | Cardiovascular Health Effects | References |
| Ozone (Ground-Level) | Acidic smog: 0.8–1.0 ppmPhotochemical smog: 0.4–0.8 ppm | Ozone promotes systemic inflammation, oxidative stress, arrhythmia and elevate the risk of myocardial infarction | [58–62] |
| Particulate Matter (PM2.5) | In Asian cities: ~10 µg/m³* (varies widely; reported ranges from 4.9 to 32.8ppm in some measurements, though most health studies use µg/m³) | PM2.5 is a risk factor for cardiovascular disease, associated with heart attacks, stroke, and arrhythmias due to deep lung penetration and systemic inflammation | [63–68] |
| Nitrogen Dioxide (NO₂) | Approx. 75 to 175 ppb | Nitrogen dioxide causes vascular inflammation and endothelial dysfunction, increased blood pressure and elevated risk of heart disease | [69–72] |
| Sulphur Dioxide (SO₂) | Approx. 0.75 ppm | Sulphur dioxide causes vasoconstriction and promotes inflammation. It can exacerbate pre-existing cardiovascular conditions and increase the risk of heart failure | [73] |
| Peroxyacetyl Nitrate (PAN) | Approx. 37 ppb | PAN contributes to overall smog toxicity, which may indirectly stress the cardiovascular system via respiratory pathways | [74,75] |
| Benzopyrene | 3.64–61.6 ng/m³ | Benzopyrene acts as a potent oxidant inducing systemic inflammation and it may accelerate atherosclerosis, indirectly affecting cardiovascular health | [76] |
| Phthalate Esters | 10–100 ng/m³ | Phthalate Esters influence cardiovascular risk indirectly through metabolic alterations and hormonal imbalances | [77] |
Smog and Cardiovascular Disease in Punjab, Pakistan: A Case Example
Punjab, the most populous province of Pakistan, experiences some of the most severe smog episodes globally, particularly during the winter months (Hussain et al., 2020). Contributing factors include crop residue burning, high vehicular emissions, industrial discharges, and unfavorable weather conditions such as temperature inversion layers trapping pollutants near ground level (Saeed et al., 2021; Khan et al., 2019).
Air quality monitoring in cities like Lahore shows PM2.5 concentrations routinely exceeding WHO guidelines by 5 to 10 times during smog events (Mahmood et al., 2021). NO₂ and SO₂ levels also spike during these episodes. These pollution peaks correspond to increased respiratory and cardiovascular hospital admissions and mortality (Javed et al., 2020). The population in Punjab faces a double burden of traditional cardiovascular risk factors hypertension, diabetes, smoking compounded by high smog exposure, creating a severe public health concern (Ali et al., 2020; Rizwan et al., 2021).
Studies conducted locally suggest that smog-related cardiovascular events contribute significantly to overall mortality, yet public awareness and policy responses remain limited (Hussain et al., 2020; Saeed et al., 2021). There is an urgent need for research, public health interventions, and stricter pollution controls in the region.
This review study was conducted through a systematic literature search to examine the association between smog exposure and cardiovascular disease (CVD). The primary goal was to identify and synthesize relevant research articles published within the last 15 years (2008–2023). The literature search was performed across multiple academic databases including Google Scholar, ScienceDirect, and PubMed, which are freely accessible and widely used sources for environmental health research.
Discussion
The findings synthesized in this review clearly demonstrate a strong association between smog-related air pollutants and the development or exacerbation of cardiovascular disease (CVD). Specifically, pollutants such as particulate matter (PM2.5 and PM10), nitrogen dioxide (NO₂), ozone (O₃), sulphur dioxide (SO₂), carbon monoxide (CO), carbon black, and polycyclic aromatic hydrocarbons (PAHs) were frequently linked with increased incidence of myocardial infarction, stroke, ischemic heart disease (IHD), and overall cardiovascular mortality. Among these, PM2.5 emerged consistently across studies as the most potent cardiovascular risk factor.
Mechanisms of Impact
Air pollutants impact cardiovascular health through several biological mechanisms. PM2.5 and other fine particles penetrate deep into the alveolar regions of the lungs, enter the bloodstream, and contribute to systemic inflammation, oxidative stress, endothelial dysfunction, and atherosclerosis progression (Brook et al., 2010). These effects increase blood pressure, coagulation potential, and insulin resistance each a known risk factor for cardiovascular events (Rajagopalan et al., 2018). Moreover, studies have reported that prolonged NO₂ exposure enhances autonomic imbalance and vascular inflammation, compounding the risk of CVD (Münzel et al., 2017).
Short-term exposure has also been shown to trigger acute cardiovascular events. For instance, several time-series studies across urban centers revealed a rise in emergency admissions and cardiovascular deaths within 24–72 hours of high smog days (Cesaroni et al., 2014; Liu et al., 2019). These results highlight both the chronic and acute hazards posed by air pollution to the cardiovascular system.
Disparities in Exposure and Vulnerability
Another significant insight from the literature is that exposure to smog and its health outcomes are not evenly distributed across populations. Socioeconomically disadvantaged communities and low- to middle-income countries (LMICs) face higher levels of air pollution due to industrial proximity, poor urban planning, limited regulation, and lower access to healthcare (Landrigan et al., 2018). Studies from India, Pakistan, Bangladesh, and sub-Saharan Africa show that CVD mortality attributable to air pollution is disproportionately higher in these regions compared to high-income nations (GBD, 2020; WHO, 2021).
Punjab, Pakistan – A Regional Case Example
Punjab, and particularly the city of Lahore, represents a critical regional hotspot where smog-related CVD risk is both evident and under-researched. The confluence of heavy traffic emissions, industrial discharges, agricultural residue burning, and coal-based energy production leads to extreme levels of particulate matter and gaseous pollutants during winter months. Several monitoring reports show PM2.5 concentrations in Lahore frequently exceed 300 µg/m³ well above WHO’s safe limit of 5 µg/m³ (IQAir, 2023).
A hospital-based study in Lahore reported that emergency visits for cardiovascular events surged during peak smog season, with a notable increase in myocardial infarctions and arrhythmias (Khan et al., 2020). Despite this, there remains a lack of large-scale cohort or case-control studies investigating smog-related cardiovascular morbidity in Punjab. The absence of robust local data continues to hinder policy action and health planning.
Comparison with International Findings
Compared to developed countries where stringent emissions regulations have reduced ambient pollution levels and mitigated cardiovascular impacts (e.g., the USA Clean Air Act), Pakistan and similar LMICs lag in enforcement and public health response. Studies from Europe and North America also highlight the protective effects of clean energy transitions, improved vehicle standards, and urban greening on reducing CVD incidence (EPA, 2020; Lelieveld et al., 2019). These contrasts emphasize the urgent need for environmental and health policy reforms in smog-prone regions like Punjab.
Gaps in Literature and Research Limitations
While this review consolidates significant evidence, some gaps remain. First, most studies are observational, making it difficult to fully isolate causal effects of specific pollutants due to confounding variables. Second, personal exposure data is often lacking, as studies rely on city-wide averages that may not reflect individual risk. Third, relatively few studies have explored long-term cardiovascular outcomes in younger populations or integrated gender-specific analyses.
Moreover, the interaction between air pollution and other non-communicable disease risk factors such as smoking, poor diet, and sedentary lifestyle needs further investigation. Climate change is likely to exacerbate air quality issues, yet few studies consider its synergistic impact on cardiovascular health (Shaddick et al., 2020).
Conclusion
This review provides compelling evidence that smog and its constituent air pollutants pose a significant threat to cardiovascular health globally and more acutely in low- and middle-income countries like Pakistan. Pollutants such as PM2.5, PM10, NO₂, O₃, CO, SO₂, carbon black, and PAHs are consistently associated with elevated risks of myocardial infarction, stroke, ischemic heart disease, and cardiovascular mortality. Among these, PM2.5 has emerged as the most consistent and potent driver of CVD-related outcomes across multiple studies.
Mechanistic insights reveal that the inflammatory, oxidative, and thrombotic pathways triggered by these pollutants are central to cardiovascular pathophysiology. This burden is disproportionately high in densely populated, poorly regulated regions such as Punjab, where environmental degradation, inadequate policy frameworks, and seasonal smog episodes contribute to hazardous air quality levels. Lahore, in particular, has become a recurrent smog epicenter with critical public health implications.
Despite extensive international literature, there remains a dearth of high-quality, localized research in Pakistan that quantifies long-term cardiovascular impacts of smog. This limits both public awareness and evidence-based policymaking. Moving forward, it is essential to prioritize local epidemiological studies, integrate cardiovascular outcomes in air quality assessments, and strengthen environmental health governance. Public health messaging, regulatory interventions, and cross-sector collaboration will be crucial in reducing exposure and preventing pollution-induced cardiovascular harm.
In conclusion, addressing the cardiovascular burden of smog must be recognized as a public health priority requiring urgent and coordinated action across health, environmental, industrial, and policy domains.
Table 2.
Major Air Pollutants in Smog and Their Cardiovascular Health Effects.
| Pollutant | Source | Cardiovascular Effects |
| PM2.5 | Combustion, vehicles, biomass | Stroke, IHD, systemic inflammation |
| PM10 | Dust, construction, traffic | Atherosclerosis, heart failure |
| Nitrogen Dioxide (NO₂) | Traffic, power plants | Autonomic dysfunction, vascular damage |
| Ozone (O₃) | Photochemical reactions | Arrhythmias, oxidative stress |
| Carbon Monoxide (CO) | Incomplete combustion | Reduced oxygen delivery, ischemia |
| Sulphur Dioxide (SO₂) | Fossil fuel burning | Vasoconstriction, increased CVD admissions |
| Polycyclic Aromatic Hydrocarbons (PAHs) | Biomass, traffic | Atherosclerosis, inflammation |
| Carbon Black | Diesel exhaust | Endothelial dysfunction |
Table 3.
Summary of Epidemiological Studies Linking Smog to Cardiovascular Disease.
| Location | Study Type | Key Finding |
| USA | Review | PM2.5 strongly linked to myocardial infarction |
| Italy | Time-series | PM10 exposure increased daily CVD hospital visits |
| Global | Meta-analysis | Smog exposure increases stroke risk |
| China | Cohort | Long-term NO₂ exposure increases CVD mortality |
| Lahore, Pakistan | Observational | Increased cardiac admissions during smog season |
| Global | Global burden study | LMICs bear 90% of CVD deaths linked to air pollution |
List of Abbreviations
| Abbreviation | Full Form |
| EPA | Environmental Protection Agency |
| CVD | Cardiovascular Disease |
| IHD | Ischemic Heart Disease |
| PM | Particulate Matter |
| PM₂.₅ | Particulate Matter ≤ 2.5 micrometers in diameter |
| PM₁₀ | Particulate Matter ≤ 10 micrometers in diameter |
| NO₂ | Nitrogen Dioxide |
| SO₂ | Sulphur Dioxide |
| CO | Carbon Monoxide |
| PAHs | Polycyclic Aromatic Hydrocarbons |
| O₃ | Ozone |
References
- Anderson, J.O., Thundiyil, J.G. and Stolbach, A., 2012. Clearing the air: a review of the effects of particulate matter air pollution on human health. Journal of Medical Toxicology, 8(2), pp.166–175. [CrossRef] [PubMed]
- Bourdrel, T., Bind, M.A., Béjot, Y., Morel, O. and Argacha, J.F., 2017. Cardiovascular effects of air pollution. Archives of Cardiovascular Diseases, 110(11), pp.634–642.
- Brook, R.D., Rajagopalan, S., Pope III, C.A., Brook, J.R., Bhatnagar, A., Diez-Roux, A.V., Holguin, F., Hong, Y., Luepker, R.V., Mittleman, M.A. and Peters, A., 2010. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation, 121(21), pp.2331–2378.
- Cesaroni, G., Badaloni, C., Gariazzo, C., Stafoggia, M., Sozzi, R., Davoli, M. and Forastiere, F., 2014. Long-term exposure to urban air pollution and mortality in a cohort of more than a million adults in Rome. Environmental Health Perspectives, 121(3), pp.324–331. [CrossRef] [PubMed]
- Chen, H., Burnett, R.T., Kwong, J.C., Villeneuve, P.J., Goldberg, M.S., Brook, R.D., van Donkelaar, A., Jerrett, M., Martin, R.V., Brook, J.R. and Kopp, A., 2013. Risk of incident diabetes in relation to long-term exposure to fine particulate matter in Ontario, Canada. Environmental Health Perspectives, 121(7), pp.804–810. [CrossRef]
- Cohen, A.J., Brauer, M., Burnett, R., Anderson, H.R., Frostad, J., Estep, K., Balakrishnan, K., Brunekreef, B., Dandona, L., Dandona, R. and Feigin, V., 2017. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet, 389(10082), pp.1907–1918. [CrossRef] [PubMed]
- EPA (United States Environmental Protection Agency), 2020. Integrated Science Assessment for Particulate Matter. EPA/600/R-19/188.
- Feng, S., Gao, D., Liao, F., Zhou, F. and Wang, X., 2016. The health effects of ambient PM2.5 and potential mechanisms. Ecotoxicology and Environmental Safety, 128, pp.67–74.
- Forouzanfar, M.H., Afshin, A., Alexander, L.T., Anderson, H.R., Bhutta, Z.A., Biryukov, S., Brauer, M., Burnett, R., Cercy, K. and Charlson, F.J., 2016. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks. The Lancet, 388(10053), pp.1659–1724. [CrossRef]
- GBD 2020 Risk Factors Collaborators, 2021. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis. The Lancet, 396(10258), pp.1223–1249.
- Gharibvand, L., Shavlik, D., Ghamsary, M., Beeson, W.L., Soret, S., Knutsen, R. and Knutsen, S.F., 2017. The association between ambient fine particulate air pollution and lung cancer incidence: Results from the AHSMOG-2 study. Environmental Health Perspectives, 125(3), p.378–384. [CrossRef]
- Hoek, G., Krishnan, R.M., Beelen, R., Peters, A., Ostro, B., Brunekreef, B. and Kaufman, J.D., 2013. Long-term air pollution exposure and cardio-respiratory mortality: a review. Environmental Health, 12(1), p.43. [CrossRef]
- Khan, S., Mahmood, A., Raza, A., Rehman, A. and Butt, Z.A., 2020. Acute health impacts of smog episodes on cardiovascular and respiratory admissions in Lahore, Pakistan. Pakistan Journal of Medical Sciences, 36(6), pp.1290–1295.
- Lelieveld, J., Klingmüller, K., Pozzer, A., Burnett, R.T., Haines, A. and Ramanathan, V., 2019. Effects of fossil fuel and total anthropogenic emission removal on public health and climate. Proceedings of the National Academy of Sciences, 116(15), pp.7192–7197. [CrossRef]
- Liu, C., Chen, R., Sera, F., Vicedo-Cabrera, A.M., Guo, Y., Tong, S., Coelho, M.S.Z.S., Saldiva, P.H.N., Lavigne, E., Matus, P. and Valdes Ortega, N., 2019. Ambient particulate air pollution and daily mortality in 652 cities. New England Journal of Medicine, 381(8), pp.705–715. [CrossRef]
- Mills, N.L., Donaldson, K., Hadoke, P.W., Boon, N.A., MacNee, W., Cassee, F.R., Sandström, T., Blomberg, A. and Newby, D.E., 2009. Adverse cardiovascular effects of air pollution. Nature Clinical Practice Cardiovascular Medicine, 6(1), pp.36–44.
- Münzel, T., Sørensen, M., Gori, T. and Schmidt, F.P., 2017. Effects of gaseous and solid constituents of air pollution on endothelial function. European Heart Journal, 38(20), pp.1590–1591.
- Nawaz, M., Ahmad, S., Saeed, M.A., Saleem, T. and Rana, I.A., 2021. Investigating the impact of smog on human health in Punjab: A spatio-temporal analysis. Environmental Monitoring and Assessment, 193(4), p.238.
- Pope III, C.A., Dockery, D.W., 2006. Health effects of fine particulate air pollution: lines that connect. Journal of the Air & Waste Management Association, 56(6), pp.709–742. [CrossRef]
- Pope III, C.A., Turner, M.C., Burnett, R.T., Jerrett, M., Gapstur, S.M., Diver, W.R. and Krewski, D., 2015. Relationships between fine particulate air pollution, cardiometabolic disorders, and cardiovascular mortality. Circulation Research, 116(1), pp.108–115. [CrossRef] [PubMed]
- Rajagopalan, S. and Brook, R.D., 2012. Air pollution and type 2 diabetes: mechanistic insights. Diabetes, 61(12), pp.3037–3045.
- Rajagopalan, S., Al-Kindi, S.G. and Brook, R.D., 2018. Air pollution and cardiovascular disease. Journal of the American College of Cardiology, 72(17), pp.2054–2070.
- Requia, W.J., Adams, M.D., Koutrakis, P., 2017. Association of PM2.5 with diabetes incidence in the elderly. Environment International, 104, pp.284–290.
- Shah, A.S.V., Langrish, J.P., Nair, H., McAllister, D.A., Hunter, A.L., Donaldson, K., Newby, D.E. and Mills, N.L., 2013. Global association of air pollution and heart failure: a systematic review and meta-analysis. The Lancet, 382(9897), pp.1039–1048. [CrossRef]
- Shaddick, G., Thomas, M.L., Mudu, P., Ruggeri, G. and Gumy, S., 2020. Half the world’s population are exposed to increasing air pollution. NPJ Climate and Atmospheric Science, 3(1), pp.1–5. [CrossRef]
- Simoni, M., Baldacci, S., Maio, S., Cerrai, S., Sarno, G. and Viegi, G., 2015. Adverse effects of outdoor pollution in the elderly. Journal of Thoracic Disease, 7(1), pp.34–45. [CrossRef]
- Sorensen, M., Andersen, Z.J., Nordsborg, R.B., Becker, T., Tjonneland, A., Overvad, K. and Raaschou-Nielsen, O., 2012. Road traffic noise and incident myocardial infarction: a prospective cohort study. PLoS One, 7(6), p.e39283. [CrossRef] [PubMed]
- Tonne, C., Elbaz, A., Beevers, S., Singh-Manoux, A. and Dugravot, A., 2014. Traffic-related air pollution in relation to cognitive function in older adults. Epidemiology, 25(5), pp.674–681. [CrossRef]
- Turner, M.C., Jerrett, M., Pope III, C.A., Krewski, D., Gapstur, S.M., Diver, W.R., Beckerman, B.S., Marshall, J.D. and Burnett, R.T., 2016. Long-term ozone exposure and mortality in a large prospective study. American Journal of Respiratory and Critical Care Medicine, 193(10), pp.1134–1142.
- Vohra, K., Vodonos, A., Schwartz, J., Marais, E.A., Sulprizio, M.P. and Mickley, L.J., 2021. Global mortality from outdoor fine particle pollution generated by fossil fuel combustion: Results from GEOS-Chem. Environmental Research, 195, p.110754. [CrossRef]
- Wang, M., Aaron, C.P., Madrigano, J., Hoffman, E.A., Angelini, E., Yang, J., Laine, A., Shea, S. and Vedal, S., 2019. Association between long-term exposure to ambient air pollution and change in quantitatively assessed emphysema and lung function. JAMA, 322(6), pp.546–556. [CrossRef] [PubMed]
- WHO (World Health Organization), 2021. Air pollution. [online] Available at: https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health [Accessed 17 May 2025].
- WHO, 2018. Ambient air pollution: Health impacts. Geneva: World Health Organization. Available at: https://www.who.int/airpollution/ambient/health-impacts/en/ [Accessed 17 May 2025].
- World Bank, 2020. Air Quality Management in Pakistan. [online] Available at: https://openknowledge.worldbank.org [Accessed 17 May 2025].
- Xie, Y., Bowe, B., Yan, Y., Al-Aly, Z., 2019. Burden of cause-specific mortality associated with PM2.5 air pollution in the United States. JAMA Internal Medicine, 179(11), pp.1521–1529.
- Yang, W.S., Zhao, H., Wang, X., Deng, Q., Fan, W.Y. and Wang, Y., 2014. An evidence-based review of the relationship between long-term exposure to air pollution and cardiovascular disease. International Journal of Environmental Research and Public Health, 11(7), pp.6840–6860.
- Yin, P., Brauer, M., Cohen, A., Burnett, R.T., Liu, J., Liu, Y., Liang, R., Wang, W., Qi, J., Wang, L. and Zhou, M., 2017. The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces. Proceedings of the National Academy of Sciences, 114(39), pp.10384–10389.
- Zhang, Z., Laden, F., Forman, J.P., Hart, J.E., 2016. Long-term exposure to particulate matter and self-reported hypertension: a prospective analysis in the Nurses’ Health Study. Environmental Health Perspectives, 124(9), pp.1414–1420. [CrossRef]
- Zhang, Z., Wang, J., Shen, L., Yang, Y. and Wu, J., 2020. Assessing the impact of air pollutants on hospital admissions for cardiovascular disease in Wuhan, China. International Journal of Environmental Research and Public Health, 17(7), p.2452.
- Zhou, M., Wang, H., Zhu, J., Chen, W., Wang, L., Liu, S., Li, Y., Wang, L., Yang, G., Wang, Y. and Liang, X., 2016. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the Global Burden of Disease Study 2013. The Lancet, 387(10015), pp.251–272. [CrossRef]
- Brook, R.D., Newby, D.E., Rajagopalan, S., 2017. The global threat of outdoor ambient air pollution to cardiovascular health: time for intervention. JAMA Cardiology, 2(4), pp.353–354.
- Nawaz, M., Rana, I.A., Sadiq, M.A. and Mahmood, A., 2019. Public perception and response to smog in Lahore: A case of environmental hazard in Pakistan. Sustainability, 11(7), p.1939.
- Manisalidis, I., Stavropoulou, E., Stavropoulos, A. and Bezirtzoglou, E., 2020. Environmental and health impacts of air pollution: a review. Frontiers in Public Health, 8, p.14. [CrossRef]
- Dominici, F., Peng, R.D., Bell, M.L., Pham, L., McDermott, A., Zeger, S.L. and Samet, J.M., 2006. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA, 295(10), pp.1127–1134. [CrossRef] [PubMed]
- Ghauri, B., Lodhi, A. and Mansha, M., 2007. Development of baseline (air quality) data in Pakistan. Environmental Monitoring and Assessment, 127(1–3), pp.237–252. [CrossRef] [PubMed]
- Knol, A.B., de Hartog, J.J., Boogaard, H., Slottje, P., van der Sluijs, J.P., Lebret, E., Cassee, F.R., Wardekker, J.A. and Kruize, H., 2009. Expert elicitation on ultrafine particles: likelihood of health effects and causal pathways. Particle and Fibre Toxicology, 6(1), p.19. [CrossRef] [PubMed]
- Pakistan Bureau of Statistics, 2021. Punjab Environmental Profile 2020–21. Government of Pakistan. Available at: https://www.pbs.gov.pk [Accessed 17 May 2025].
- Rasheed, A., Khoso, A.R., Butt, Q. and Sheikh, S.A., 2023. Urban smog in Pakistan: sources, health risks and mitigation strategies. Environmental Science and Pollution Research, 30, pp.54521–54535.
- Salim, W., Sheikh, R. and Kazmi, S.J.H., 2022. Association of ambient air quality with cardiovascular disease: a case study from Lahore, Pakistan. Pakistan Journal of Public Health, 12(3), pp.99–104.
- Ali, M., Ahmed, M. and Yousaf, A., 2020. Evaluation of air quality in urban areas of Pakistan during winter months: A case study of Lahore. International Journal of Environmental Studies, 77(6), pp.997–1010.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



