
Submitted:
17 May 2025
Posted:
19 May 2025
You are already at the latest version
Abstract
Background/Objectives: Postoperative septic events represent a major parameter of morbidity and mortality following major abdominal surgery. Early identification and prediction can have a major impact in clinical management, reduction of hospitalization costs and restriction of irrational use of antibiotics. For this purpose, two novel biomarkers (C-reactive protein to albumin or transferrin ratios, CAR and CTR respectively) were evaluated. Methods: A combined retrospective and prospective study of 200 patients who underwent elective or emergency abdominal surgery was performed. Patient demographics, emergency status, type of operation, and white blood cells (WBCs) count, serum albumin, serum transferrin (TRF) and CAR-CTR were evaluated. Multiple way ANOVA was utilized. Multiparametric and logistic regression analyses were performed for each confounder. Receiver operating characteristic (ROC) curve analysis and corresponding diagrams of sensitivity vs 1-specificity were applied for CAR and CTR in postoperative days 2 and 3. Results: WBCs number had no predictive significance in septic event identification (p = 0.461) while postoperative CAR, CTR, Alb, TRF, BMI and emergency status were significantly correlated (p<0.001). At postoperative day 2, a CTR of 9.48 and a CAR of 4.14 have 75.9% and 70.4% specificity and 86% and 87.7% sensitivity respectively. At postoperative day 3, a CTR of 8.89 and a CAR of 4.25 have 74.1% and 79.6% specificity and 87.7% and 86% sensitivity respectively. Conclusions: Early identification of postoperative septic events may significantly facilitate in decreasing postoperative morbidity and mortality. Both CAR and CTR have displayed significant predictive ability in identifying patients more prone in developing postoperative septic events, highlighting its significance in every-day clinical practice.
Keywords:
C-reactive protein to albumin ratio
; C-reactive protein to transferrin ratio
; transferrin
; Creactive protein
; surgical site infection
; biomarker
1. Introduction
Postoperative septic events such as surgical site infection (SSI) and anastomotic leak (AL) are major determinants of morbidity and mortality following abdominal surgery regardless if an open or laparoscopic approach has been followed [1,2] even though open operations are more prone to develop SSI [1]. Moreover, emergency status [3], socioeconomic status [4] and the underlying risk factors of each patient (such as obesity, hyperglyceamia, smoking) [5,6] seem to also affect SSI development. Apart from the clinical consequences (morbidity, prolonged length of hospital of stay and development of resistant microbial strains), SSIs result in a significant economic burden for the healthcare systems and patients [7]. It is estimated that patients with a SSI may have higher hospitalization costs than those without it (16.685 € or 19.703 USD and 11.235 € or 13.267 USD respectively) [8]. The same observations apply for ALs. However, their prevalence and consequences seem to vary according to the site of the failed anastomosis [9,10]. For this reason several prognostic and predictive tools that utilize pre and postoperative clinical data and health risk factors have been proposed [11,12,13,14,15]. Despite their overall good performance though, they seem to have poor diagnostic performance. For this reason a number of studies have tried to validate the diagnostic and/or predictive significance of biomarkers in order to early identify post-operative septic events. For instance, high levels of circulating procalcitonin (PCT) and CAR have been proposed as indicators of SSI and AL in colorectal surgery [16,17,18,19,20] while increased levels of peritoneal cytokines tumor necrosis factor (TNF) and interleukin 6 (IL-6) have also been proved to correlate with AL [21] and SSI [22] even though CAR, PCT, TNF and IL-6 seem to outperform CRP for these purposes [16,19,23]. The reason for choosing these biomarkers (or their combination) lies on the fact that surgical operations (especially open ones) are significant drivers of systematic stress responses affecting the metabolism as well as the neuroendocrine and immune systems [24]. If surgical stress is prolonged, its effects may propagate leading the organism to enter hypercatabolism (with substantial decrease of circulating ALB), impairment of wound healing mechanisms, increase of acute phase proteins (such as PCT and CRP) and ultimately systematic inflammatory response syndrome (SIRS) in which unregulated production of pro-inflammatory cytokines (TNF/IL-6) and deregulated immune responses are observed [25,26]. However, routine assessment of PCT, TNF and IL-6 may be impeded by the substantial costs involved and the scarcity of clinical laboratories equipped to perform these tests. This is especially relevant for Secondary Care Hospitals and mid to low income territories where complex or expensive tests cannot be implemented in every-day clinical practice. On the contrary, there is evidence that other more cost-effective acute phase proteins such as transferrin (TRF), may have strong correlation with microbial infection, inflammation and nutritional status [27,28,29,30]. TRF is a key glycoprotein in iron metabolism, crucial for iron transport and homeostasis [31]. It is a monomeric glycoprotein with a molecular weight of approximately 80 kDa consisting of two homologous lobes, the N-lobe and the C-lobe, each capable of binding one ferric ion (Fe3+) allowing TRF to transport iron ions in the bloodstream [32]. It is well identified that TRF plays a crucial role in maintaining iron homeostasis by binding free iron in the blood, thus reducing the availability of free iron for catalyzing harmful free radical formation while also affecting innate immune response. In states of infection and inflammation, TRF levels can decrease, limiting iron availability to pathogens and thereby inhibiting their growth[33]. However, TRF levels may change in the presence of chronic disease anemia or iron deficiency anemia (low vs elevated levels respectively). Interestingly, it has been shown that in states of inflammation and bacterial infection TRF may exhibit earlier changes and higher sensitivity than ALB [34,35]. For this reason, we aimed to evaluate the diagnostic and predictive efficacy of CRP to TRF ratio (CTR) against CRP and CAR for SSIs and ALs.
2. Materials and Methods
Patients
A combined retrospective and prospective study was conducted between 2020 and 2024 including 200 patients (114 males and 86 females). The retrospective arm involved 89 randomly chosen patients using hospital records who underwent emergency or elective major abdominal surgery at the Department of General Surgery of the University Hospital of Heraklion between January 1st 2020 and December 1st 2023. Patients with SSIs were identified using a prospectively maintained database of positive wound cultures and were further cross-referenced with hospital records. For the prospective arm of the study all patients who were submitted to an emergency or elective major abdominal operation between December 1st 2023 and July 1st 2024 were evaluated for their potential to be included. In total, 128 were initially evaluated however only 111 were included since four patients refused to participate, five patients died before completing the study, three were re-operated at 48 hours and another five had incomplete data.
Establishment of Post-Operative Septic Event Diagnosis
For the establishment of a postoperative septic event diagnosis (including SSI), guidelines from the National Healthcare Safety Network that is part of the Centers for Disease Control and Prevention were implemented [36]. Moreover, the infection was confirmed with microbiological evidence of positive wound cultures. Cultures isolating Staphylicoccus epidermidis as the only pathogen were not interpreted except if Methicillin-resistant Staphylococcus epidermidis (MRSE) was identified. Our department does not regularly screen patients for Methicillin-resistant Staphylococcus aureus. Therefore, any isolation of this pathogen is discussed separately with the infections control committee in order to plan a surveillance protocol. Based on this, SSI monitoring was based upon active, patient-based and prospective surveillance. For the diagnosis of intra-abdominal abscess a computed tomography was used. Concurrent and post-discharge surveillance methods were used to detect post-operative septic events following inpatient and outpatient operative procedures for a 30-day period after the operation for all procedure types. For the outpatient surveillance a revised Macefield’s questionnaire for SSIs was translated in Greek and used [37] along with predetermined clinical examination by a surgeon working for the Department of General Surgery at post-operative day 15.
Study Protocol
After an initial identification of the predictive significance of CAR in the retrospective group, cut-off points were established and used as references for the prospective group in order to estimate the diagnostic potential of both CAR and CTR. In a final step, in order to evaluate the diagnostic performance of both CAR and CTR in early detection of wound infection as opposed to clinical evaluation, 40 patients were randomly chosen and evaluated by senior surgeons for signs and symptoms of wound infection at post-operative day 2 and 3. In case that a patient’s CAR and/or CTR values were at or above the cut-off points or if the surgeon suspected a wound infection wound cultures were retrieved. Their estimation of presence of wound infection was recorded and compared against the diagnostic accuracy of CAR/CTR. The protocol for this study has been approved by the Ethics Committee for Patients and Biological Material of the University Hospital of Heraklion, Greece. All participants signed an informed consent agreement. All samples generated by this study were anonymized, and personal data was managed according to the EU General Data Protection Regulation (GDPR).
Inclusion Criteria
All patients who were submitted to a major abdominal operation as defined by Courtney et al [38,39] were considered as potential candidates. In short, major abdominal operation should be defined any intra-peritoneal operation with no primary involvement of the thorax that implements either luminal resection and/or resection of a solid organ associated with the gastrointestinal tract. Consecutive evaluation of CRP and ALB for the first three post-operative days along with a positive wound culture had to be present for a patient to be included in the retrospective arm.
Exclusion criteria
Exclusion criteria were as follows:
- I)
- Lack of microbiological evidence of SSI
- II)
- Refusal of the patient to attend the study
- III)
- Reoperation prior to postoperative day 3
- IV)
- Albumin infusion either preoperatively or within 2 postoperative days
- V)
- Known autoimmune disease under treatment or not
- VI)
- Incomplete laboratory data
- VII)
- Anemia of chronic disease
Blood Sampling
Peripheral blood samples were collected at predetermined time-points pre-operatively, at 24, 48 and 72 hours post-operatively. All blood samples were stored in 5°C until processing within 48 h from sampling.
Data Collection
The data interest included demographic characteristics (age, sex, body mass index -BMI), operative data (emergency or elective operation, type of operation), laboratory data (post-operative white blood cells – WBCs, CRP, ALB, TRF in 24/48/72 hours), comorbidities (namely anemia of chronic disease, diabetes mellitus type 1 or 2, chronic liver disease, chronic renal disease).
Control Group
The control group was constituted by 81 individuals with no clinical or microbial indication of SSI who were submitted to major abdominal operation.
Statistical Analysis
All statistical analyses were conducted using IBM SPSS Statistics 14. Descriptive statistics were utilized to summarize demographic and clinical characteristics. Continuous variables were expressed as means ± standard deviations (SD) or medians with interquartile ranges (IQR), depending on their distribution, while categorical variables were presented as frequencies and percentages. Normality of continuous data was assessed using the Shapiro-Wilk test. Comparative analyses were performed using Mann-Whitney U tests for continuous variables and chi-square or Fisher’s exact tests for categorical variables, as appropriate. A multiple-way ANOVA was conducted to explore differences in key variables across groups, with post-hoc analyses applied where necessary. Logistic regression was employed to identify predictors of postoperative septic events. Due to computational constraints in the logistic regression model, CTR was scaled by multiplying it by 100. This adjustment facilitated the analysis and ensured accurate model functioning. Odds ratios (OR) and 95% confidence intervals (CI) were reported for each variable included in the regression models. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic performance of the C-reactive protein to albumin ratio (CAR) and the adjusted CTR for predicting postoperative septic events. The area under the curve (AUC) was calculated to assess the accuracy of these biomarkers, and optimal cutoff values were determined to maximize sensitivity and specificity. For all analyses, a two-tailed p-value < 0.05 was considered statistically significant.
Theory/Calculation
The predictive power of C-reactive protein to transferrin ratio (CTR) and C-reactive protein to albumin ratio (CAR) hinges on their reflection of two interrelated pathophysiological processes: systemic inflammation and metabolic stress. While CRP is a well-established acute-phase reactant synthesized in response to IL-6 and TNF-α, its ratio to albumin or transferrin amplifies its diagnostic utility by integrating nutritional and iron-homeostasis derangements. Transferrin, a negative acute-phase protein, declines during inflammation due to cytokine-mediated hepatic suppression, while its role in iron sequestration limits microbial growth. This dynamic renders CTR particularly sensitive to early infection, as transferrin’s shorter half-life (∼8 days) compared to albumin (∼21 days) may capture inflammatory shifts more rapidly. Theoretically, CTR’s diagnostic advantage over CAR arises in contexts of hypoalbuminemia (e.g., malnutrition, exogenous albumin administration), where albumin’s fluctuations may obscure true inflammatory burden.
Calculationally, the ratios were derived as:
CAR = and
To address computational constraints in logistic regression, CTR was scaled by 100 (CTR ×100), preserving its predictive validity while ensuring model stability. ROC curve analysis optimized cutoff values by maximizing Youden’s index (sensitivity + specificity −1), with AUC comparisons confirming CTR’s non-inferiority to CAR. This approach bridges theoretical pathophysiology (acute-phase responses) with clinical applicability, offering a quantifiable metric for early septic risk stratification.
3. Results
Patient Characteristics
In total 200 patients were included in the study, 89 in the retrospective arm and 111 in the prospective 86 of whom were females and 114 were males. For the retrospective group the mean age was 63.9 years while for the prospective 66.6. Overall 102 patients were submitted to an elective operation (51%), while the mean length of hospital stay was 11.1 days. Demographic characteristics are presented in Table 1. The type and number of operations for each group are presented in Supplementary Table 1. Chronic diseases that may contribute to SSIs along with cancer rates for each group are presented in Supplementary Table 2. It is shown that apart from hypertension, the rest of the chronic diseases and cancer rates exhibit no statistically significant difference among the two groups. The incidence of post-operative septic complications is presented in Table 1. In detail, it is evidenced that 48.6% and 69.7% of the prospective and retrospective group accordingly had such a complication. The most common complication was wound infection (59.5%) followed by wound dehiscence (18%). Moreover, the majority of patients suffered from one septic complication (30.6% and 35.5% respectively).
Establishment of Post-Operative Septic Event Diagnosis
Out of the 111 patients that were included in the prospective arm, 57 developed a post-operative septic event (51.4%). In detail, 57 developed wound infection (51.4%), 19 developed wound dehiscence (17.1%), 12 developed an intrabdominal abscess (10.8%) and 9 developed an anastomotic/stump or suture line leak (14.1%). Regarding wound cultures, Staphylicoccus epidermidis was isolated from five patients and these cultures were not considered as positive (no MRSE was isolated), Escherichia coli was isolated in 41 specimens (71.9%), Enterococcus spp. in 33 (57.9%), Streptococcus spp in 28 (49.1%) and Candida spp / Klebsiella spp in 19.3% and 24.6% respectively. Out of the 57 patients, 49 were diagnosed while hospitalized and eight as outpatients. For these eight patients, the revised Macefield’s questionnaire had at least two positive answers of the signs and symptoms that are indicative of a wound infection and seven had at least two positive answers of wound care interventions.
Evaluation of the Correlation Between Patient Characteristics, Laboratory Tests and Post-Operative Septic Events
- Laboratory tests
As presented in Table 2, the comparison of WBCs, ALB and TRF values between patients with or without post-operative septic complications did not reach statistical significance. On the contrary, CRP, CAR and CTR measured at post-operative day 1, 2 and 3 proved to have statistically significant difference between patients with or without post-operative septic complications.
- Multiparametric analysis
Following a multi-parametric analysis for binary and continues variables, it was shown that male sex, the prospective nature of the study, emergency operations, BMI, CRP at post-operative day 2 (Post Op CRP D2), Alb at post-operative day 2 (Post Op Alb D2) CAR at post-operative day 2 (CAR DAY 2), CTR at post-operative day 2 (CTR DAY 2) and CTR at post-operative day 2 multiplied by 100 (CTR DAY2 x100) were strongly correlated with the event of post-operative septic complications reaching statistical significance (Table 3).
- Logistic regression analysis
Following logistic regression analysis for binary and continues variables, it was shown that female sex and high postoperative Alb values at D2 had a strong protective significance against post-operative septic complications while postoperative CTR x100 and CAR at postoperative days 2 and 3 had a strong negative impact upon septic post-operative complications (Table 4).
Predictive Value of CAR and CTR for Post-Operative Septic Complications
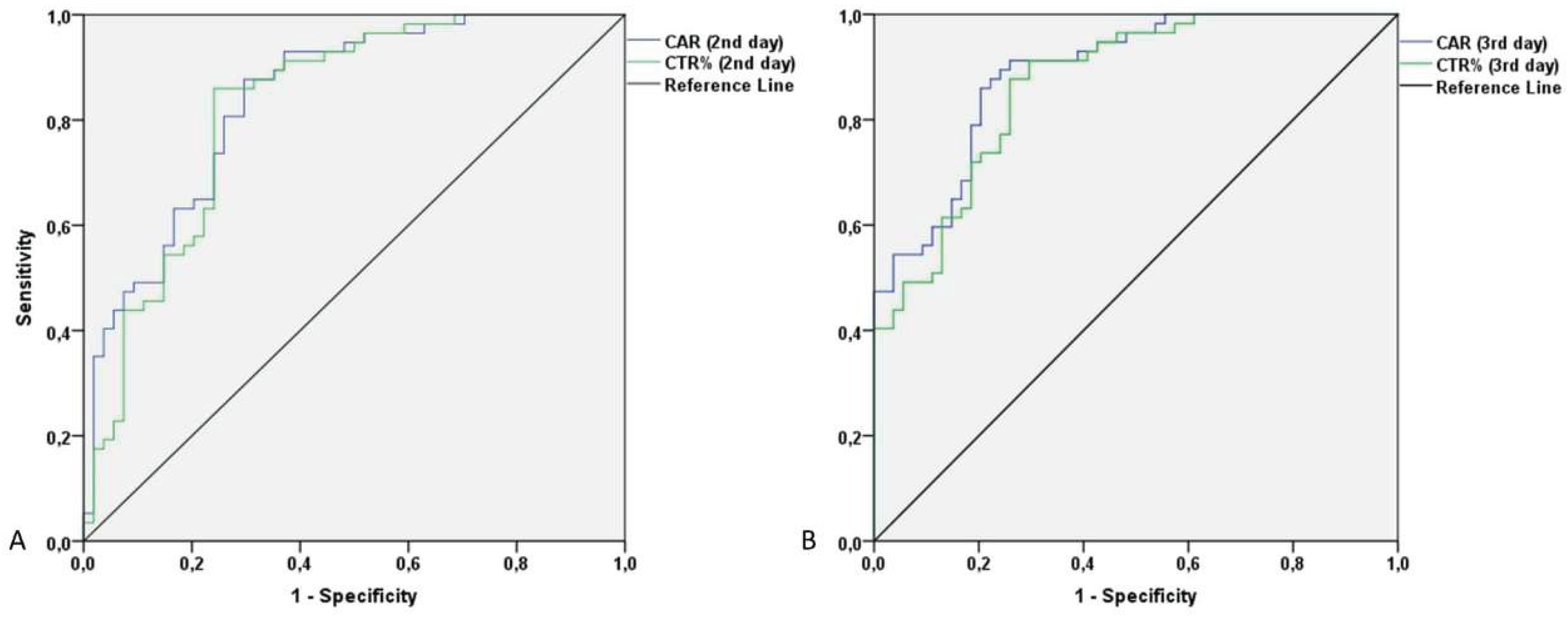
In order to evaluate the predictive value of CAR and CTR for the identification of post-operative septic complications, a ROC curve analysis was performed and the best sets of sensitivity/specificity were identified. As shown in Figure 1. CTR DAY2 x100 had an AUC of 0,825 (95% CI 0.745 – 0.904) while CAR DAY 2 had an AUC of 0.848 (95% CI 0.794 – 0.902). CTR DAY3 x100 had an AUC of 0,868 (95% CI 0.803 – 0.932) while CAR DAY 2 had an AUC of 0.890 (95% CI 0.832 – 0.948). For CAR at post-operative days 2 and 3 the best set of sensitivity and specificity was found at 4.14 (sensitivity 0.877, specificity 0.704) and 4.26 (sensitivity 0.86, specificity 0.796) respectively while for CTR (multiplied by 100) at post-operative days 2 and 3 was found at 9.48 (sensitivity 0.860, specificity 0.759) and 8.89 (sensitivity 0.877, specificity 0.741) respectively.
Figure 1.
ROC curve analysis for CAR and CTR at the second and third post-operative day.
Correlation Between Examiner’s and CAR/CTR Diagnostic/Predictive Performance
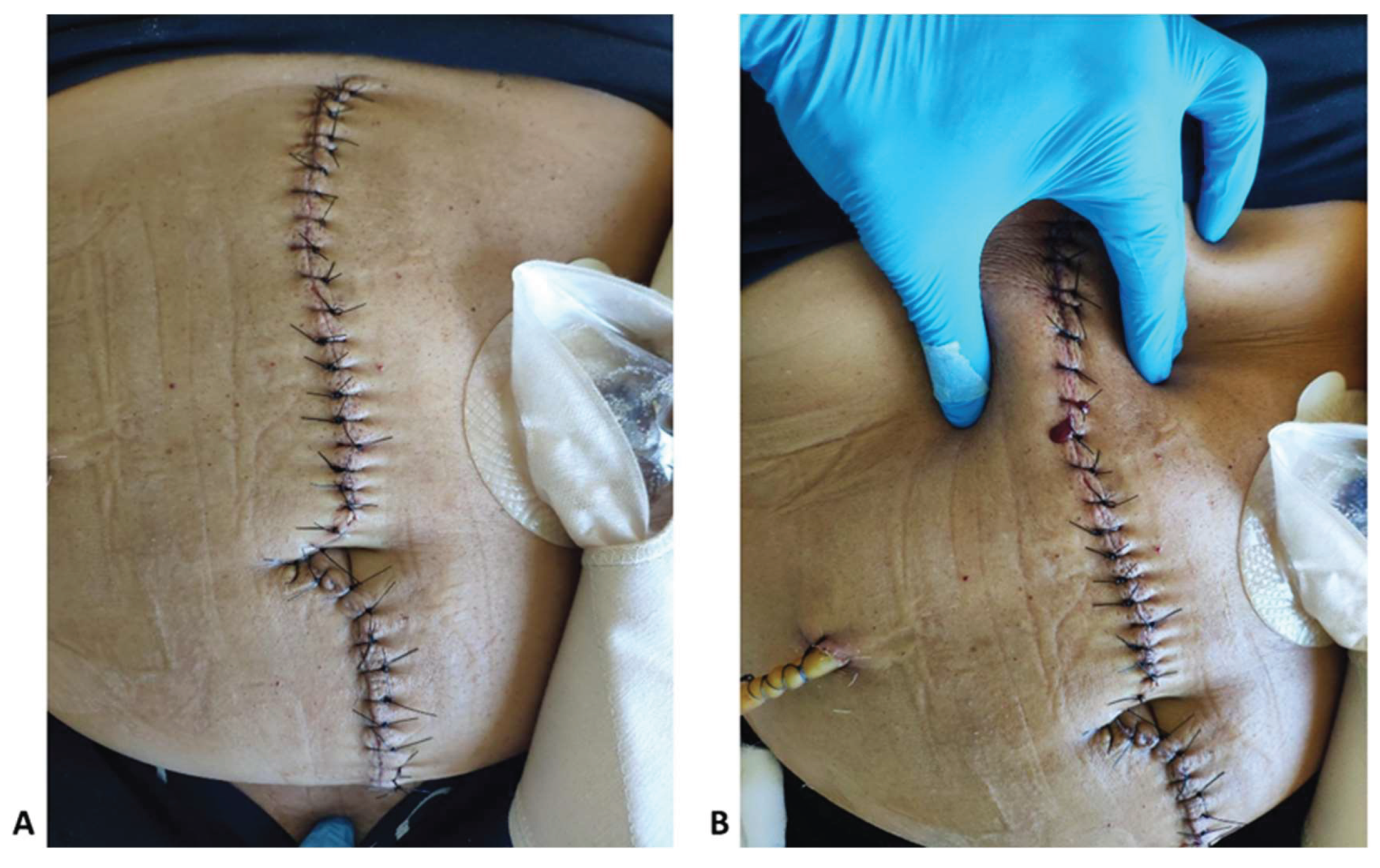
Out 40 patients that were included 26 (65%) were found to have a wound infection proved by wound culture. Regarding CAR/CTR performance, both ratios were able to correctly identify 25 out of 26 wound infections (96.2%) starting at post-operative day 2 while 2 times CAR was falsely positive resulting in Staphylicoccus epidermidis isolation. On the contrary, clinical examination resulted in three true positive identifications of wound infection (11.5%). However, these three cases that were correctly identified by clinical examination were also identified by CAR or CTR. An example of a falsely negative wound infection is depicted in Figure 2.
Figure 1.
A Photographic documentation of a clinically considered clean wound at post-operative day 3 (Hartmann's Sigmoidectomy). B Photographic documentation of the same wound. Due to the positive CAR/CTR, thorough clinical evaluation of the wound revealed a heamoserous exudate from which the wound culture isolated E.coli, Enterococcus spp and Candida spp.
Figure 1.
A Photographic documentation of a clinically considered clean wound at post-operative day 3 (Hartmann's Sigmoidectomy). B Photographic documentation of the same wound. Due to the positive CAR/CTR, thorough clinical evaluation of the wound revealed a heamoserous exudate from which the wound culture isolated E.coli, Enterococcus spp and Candida spp.
4. Discussion
Postoperative septic events such as SSI and AL are two major drivers of morbidity and mortality following major abdominal operations leading to prolonged hospital stay and a net increase of hospitalization cost [40,41]. It is estimated that 0.5-11% of all surgical patients will develop a SSI [40] and 3-19% of the patients with an anastomosis will develop a clinically relevant AL[42]. In order to address this problem several organizations have proposed a number of bundles of pre and intra-operative measures [43]. According to our data 51.4% of the prospective and 30.3% of the retrospective arms developed a post-operative septic event. No significant difference between the AL and intrabdominal abscess formation rate was detected. The higher percentage of wound infections than that described in the literature may be partially explained by the fact that, to a certain extent, daily wound handling was not performed using strict sterile conditions (such as sterile gloves, sterile drapes and two examiners per patient). Ιn coordination with the infection control committee of our hospital, our department has adopted certain perioperative measures in order to address the high incidence of wound infections. However, improvements in outpatient care over the past five years have facilitated earlier hospital discharge, even in cases of moderate wound infections. Interestingly as indicated by the multi-parametric analysis none of well-known risk factors for SSI/AL was found to be statistically important. The only parameters that were found to be strongly related with SSI/AL were male sex, emergency operations, BMI, CRP, ALB, CAR and CTR. Male sex is controversially discussed as a risk factor for SSI after abdominal surgery with ample evidence supporting both standpoints [44,45,46]. Emergency status of an operation is a well-accepted risk factor for post-operative SSI/AL [2] for which numerous perioperative protective measures have been proposed such as intraoperative wound protection, wound irrigation with saline, anti-bacterial solution, or a diluted povidone-iodine solution, perioperative normothermia, euglycemia, prophylactic negative pressure wound therapy and others [47,48,49,50]. Obesity (expressed as high BMI) and malnutrition (expressed as low albumin) are also well-identified risk factors [51,52,53]. It is proved that in obesity, chronic low-grade inflammation is present since adipose tissue produces pro-inflammatory cytokines (e.g., TNF-α, IL-6), chemokines (monocyte chemoattractant protein (MCP1/CCL2) [54], and pro-inflammatory fatty acids [55] leading to systemic chronic inflammation that alters leukocyte’s number and phenotype, thereby expanding the inflammatory environment within adipose tissue beds. In addition, due to chronic systemic inflammation, insulin signaling pathways are impaired via mechanisms such as serine phosphorylation of the insulin receptor and insulin receptor substrate-1 through the activation of IkB kinase, c-Jun N-terminal kinase and protein kinase C[56]. This results to macrophage dysfunction, while hyperglycemia due to insulin resistance can further impair normal function of neutrophils and T-cells [57]. Excess adipose tissue has poor vascularization, leading to hypoxia in wound areas which impairs fibroblast activity, collagen deposition and angiogenesis that are critical for wound healing. On the other hand, malnourished patients have protein-energy malnutrition which reduces the production of immunoglobulins, cytokines and complement proteins [58]. Malnutrition exhibits delayed wound healing through protein deficiency impairing fibroblast proliferation, collagen synthesis and angiogenesis. Finally, both obesity and malnutrition alter skin and gut microbiomes increasing colonization with pathogenic bacteria while malnutrition can lead to gut barrier dysfunction leading to bacterial translocation and systemic infections[59]. Regarding CRP, CAR and CTR, all three components (CRP, ALB and TRF) are identified as acute phase proteins[60,61]. CRP is a highly conserved acute-phase protein primarily produced by hepatocytes and to a lesser extent by other tissues in response to interleukin-6 (IL-6), interleukin-1β (IL-1β) and tumor necrosis factor-α (TNF-α) stimulation during inflammation [62,63]. IL-6 binds to its receptor (IL-6R), triggering activation of the JAK/STAT pathway in hepatocytes [64]. It has been proved that CRP levels begin to rise 6–8 hours after the onset of an inflammatory stimulus, reaching a peak at 48 hours. Once the inflammatory stimulus resolves, its levels decline rapidly given the relative short half-life (approximately 19 hours)[65]. TRF is a glycoprotein predominantly synthesized by hepatocytes in the liver that plays an important role in iron metabolism, since it is crucial for iron transport and homeostasis [31]. The expression of the TRF gene is regulated by transcription factors such as hepatocyte nuclear factor-4α (HNF-4α) that plays a key role in maintaining baseline transferrin expression in hepatocytes and the hypoxia-inducible factor-1α (HIF-1α) which under hypoxic conditions, upregulates TRF synthesis in order to facilitate iron transport for erythropoiesis [66]. Owing to its role in maintaining iron homeostasis, TRF regulates the availability of free iron and therefore free radical formation while also affecting innate immune response. In states of infection and inflammation, TRF levels decrease, limiting iron availability to pathogens and thereby inhibiting their growth [33]. Pro-inflammatory cytokines (IL-6 and TNF-α) are known downregulators of TRF production[67]. In normal state, its plasma half-life is approximately 8 days. However, TRF levels may change in the presence of chronic disease anemia or iron deficiency anemia (low vs elevated levels respectively). Albumin is the most abundant protein in human plasma, constituting approximately 50-60% of the total plasma protein content. It is synthesized exclusively by hepatocytes, and its production is tightly regulated by various factors, including nutritional status, hormonal signals, and inflammatory responses[68]. Infection triggers a complex immune response that can significantly affect albumin synthesis and function. During an acute-phase response acute-phase proteins such as CRP, fibrinogen and serum amyloid A (SAA) are produced while ALB synthesis is suppressed[69]. This downregulation serves as a protective mechanism aiming at prioritizing the production of proteins that are essential for immune defense and tissue repair. This occurs via the activation of signaling pathways such as the JAK/STAT pathway, which leads to changes in gene expression that favor the synthesis of acute-phase proteins while inhibiting albumin gene expression. TNF-α and IL-1 contribute to the suppression of albumin production by direct action on hepatocytes. TNF-α, in particular, can activate nuclear factor-kappa B (NF-κB) signaling, which is involved in the inflammatory response and can directly suppress albumin synthesis by interfering with the transcriptional machinery in hepatocytes[70]. What is more, pro-inflammatory cytokines seem to be able to stimulate ALB breakdown by the liver and other tissues, further reducing circulating ALB levels[69]. Interestingly, it has been shown that in states of inflammation and bacterial infection TRF may exhibit earlier changes and higher sensitivity than ALB [34,35]. For this reason and in conjunction with the nutritional status of a patient, our study showcased their significant role in predicting SSIs and ALs. Even though the predictive significance of CAR in certain abdominal operations has been exhibited, our study was the first to our knowledge, to have used and proved the clinical significance of CTR in SSIs/ALs after major abdominal surgery [71,72]. The addition of CTR in the clinical armamentarium is critically important because as our data indicate a CTR value of 9.48 measured at post-operative day 2 achieved greater specificity (75.9%) than a 4.14 value of CAR (70.4%) while having almost the same sensitivity 86% and 87.7% respectively. On the other hand a CTR value of 8.89 measured at post-operative day 3 has 74.1% specificity and 87.7% sensitivity as opposed to a CAR value of 4.25 that demonstrates a 79.6% specificity and 86% sensitivity. Moreover, in critically ill and malnourished patients, clinicians may choose to administer human albumin solutions as intravascular volume expanders, especially in sepsis where fluid resuscitation with crystalloids alone may be insufficient or even harmful (for example in case of heart failure), or in combination with diuretics in order to address fluid overload and improve oxygenation by reducing pulmonary edema. In such cases serum ALB will be falsely increased leading to an inaccurate low CAR and therefore prohibiting its predictive capacity. However, serum TRF will not be affected by the exogenous administration of human albumin allowing its use for predicting major septic events. Interestingly, both biomarkers significantly outperformed clinical evaluation in detecting septic events, even by senior surgeons. Their routine use could enhance early detection, enabling timely interventions such as thorough wound care, early wound cultures, proper upscaling of antibiotics (in accordance to the local infection control committee guidance), early imaging (ultrasonography or computed tomography) or even early use of negative pressure wound therapy. This approach would reduce complications, improve rational use of antibiotics, prevent the emergence of resistant microbial strains, and lower healthcare costs. However, our study faces certain restrictions to draw safe conclusions. To begin with, our sample size is relatively small. Therefore, even though that we were able to discriminate between different septic complications (wound infections, SSIs and AL), the relative numbers of each complication were small and for this reason no further analysis regarding possible predictive cut-off values was made for each complication. Second, even though our department does not have a special surgical focus that would restrict the range of operations, being a single center trial we don’t cover the full range of general surgery (for example advanced hepatobilliary, pancreatic or oesophageal surgery). A third factor is the lack of long-term surveillance given that our protocol followed up our patients for 30 days. However, no data beyond this time point were retrieved. For these reasons, a larger study with a wider range of emergency and elective operations with longer follow up is needed.
Declaration of Generative AI and AI-assisted technologies in the writing process: None of the authors used artificial intelligence during the writing of this manuscript
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, TKN. and EC.; methodology, TKN and AA.; software, TKN and AA; validation, AA and MN., formal analysis, TKN, AA, MK.; investigation, TKN, MK, EC.; data curation, TKN and AA.; writing—original draft preparation, TKN.; writing—review and editing, TKN, AA, MN,MK, EC.; supervision, EC.; project administration, EC.; All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
The studies involving human participants were reviewed and approved by the Human Ethics Committee at the University Hospital of Heraklion (No.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available from the corresponding author without undue reservation.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
References
- Caroff, D.A.; Chan, C.; Kleinman, K.; Calderwood, M.S.; Wolf, R.; Wick, E.C.; Platt, R.; Huang, S. Association of Open Approach vs Laparoscopic Approach With Risk of Surgical Site Infection After Colon Surgery. JAMA Netw. Open 2019, 2, E1913570. [Google Scholar] [CrossRef] [PubMed]
- Jatoliya, H.; Pipal, R.K.; Pipal, D.K.; Biswas, P.; Pipal, V.R.; Yadav, S.; Verma, B.; Vardhan, V. Surgical Site Infections in Elective and Emergency Abdominal Surgeries: A Prospective Observational Study About Incidence, Risk Factors, Pathogens, and Antibiotic Sensitivity at a Government Tertiary Care Teaching Hospital in India. Cureus 2023, 15, e48071. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Li, H.; Lv, P.; Peng, X.; Wu, C.; Ren, J.; Wang, P. Prospective multicenter study on the incidence of surgical site infection after emergency abdominal surgery in China. Sci. Rep. 2021, 11, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bhangu, A.; Ademuyiwa, A.O.; Aguilera, M.L.; Alexander, P.; Al-Saqqa, S.W.; Borda-Luque, G.; Costas-Chavarri, A.; Drake, T.M.; Ntirenganya, F.; Fitzgerald, J.E.; et al. Surgical site infection after gastrointestinal surgery in high-income, middle-income, and low-income countries: a prospective, international, multicentre cohort study. Lancet Infect Dis 2018, 18, 516–525. [Google Scholar] [CrossRef]
- Allegranzi, B.; Bischoff, P.; de Jonge, S.; Kubilay, N.Z.; Zayed, B.; Gomes, S.M.; Abbas, M.; Atema, J.J.; Gans, S.; van Rijen, M.; et al. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis 2016, 16, e276–e287. [Google Scholar] [CrossRef] [PubMed]
- de Vries, F.E.E.; Gans, S.L.; Solomkin, J.S.; Allegranzi, B.; Egger, M.; Dellinger, E.P.; Boermeester, M.A. Meta-analysis of lower perioperative blood glucose target levels for reduction of surgical-site infection. Br. J. Surg. 2017, 104, e95–e105. [Google Scholar] [CrossRef]
- Jenks, P.J.; Laurent, M.; McQuarry, S.; Watkins, R. Clinical and economic burden of surgical site infection (SSI) and predicted financial consequences of elimination of SSI from an English hospital. J. Hosp. Infect. 2014, 86, 24–33. [Google Scholar] [CrossRef]
- Strobel, R.M.; Leonhardt, M.; Förster, F.; Neumann, K.; Lobbes, L.A.; Seifarth, C.; Lee, L.D.; Schineis, C.H.W.; Kamphues, C.; Weixler, B.; et al. The impact of surgical site infection—a cost analysis. Langenbeck’s Arch. Surg. 2022, 407, 819–828. [Google Scholar] [CrossRef]
- Hummel, R.; Bausch, Di. Anastomotic Leakage after Upper Gastrointestinal Surgery: Surgical Treatment. Visc. Med. 2017, 33, 207–211. [Google Scholar] [CrossRef]
- Telem, D.A.; Chin, E.H.; Nguyen, S.Q.; Divino, C.M. Risk factors for anastomotic leak following colorectal surgery: A case-control study. Arch. Surg. 2010, 145, 371–376. [Google Scholar] [CrossRef]
- Litchinko, A.; Buchs, N.; Balaphas, A.; Toso, C.; Liot, E.; Meurette, G.; Ris, F.; Meyer, J. Score prediction of anastomotic leak in colorectal surgery: a systematic review. Surg. Endosc. 2024, 38, 1723–1730. [Google Scholar] [CrossRef] [PubMed]
- Karliczek, A.; Harlaar, N.J.; Zeebregts, C.J.; Wiggers, T.; Baas, P.C.; van Dam, G.M. Surgeons lack predictive accuracy for anastomotic leakage in gastrointestinal surgery. Int. J. Colorectal Dis. 2009, 24, 569–576. [Google Scholar] [CrossRef]
- Klose, J.; Tarantino, I.; von Fournier, A.; Stowitzki, M.J.; Kulu, Y.; Bruckner, T.; Volz, C.; Schmidt, T.; Schneider, M.; Büchler, M.W.; et al. A Nomogram to Predict Anastomotic Leakage in Open Rectal Surgery—Hope or Hype? J. Gastrointest. Surg. 2018, 22, 1619–1630. [Google Scholar] [CrossRef] [PubMed]
- McKenna, N.P.; Bews, K.A.; Cima, R.R.; Crowson, C.S.; Habermann, E.B. Development of a Risk Score to Predict Anastomotic Leak After Left-Sided Colectomy: Which Patients Warrant Diversion? J. Gastrointest. Surg. 2020, 24, 132–143. [Google Scholar] [CrossRef]
- Kornmann, V.; van Ramshorst, B.; van Dieren, S.; van Geloven, N.; Boermeester, M.; Boerma, D. Early complication detection after colorectal surgery (CONDOR): study protocol for a prospective clinical diagnostic study. Int. J. Colorectal Dis. 2016, 31, 459–464. [Google Scholar] [CrossRef]
- El Zaher, H.A.; Ghareeb, W.M.; Fouad, A.M.; Madbouly, K.; Fathy, H.; Vedin, T.; Edelhamre, M.; Emile, S.H.; Faisal, M. Role of the triad of procalcitonin, C-reactive protein, and white blood cell count in the prediction of anastomotic leak following colorectal resections. World J. Surg. Oncol. 2022, 20, 1–10. [Google Scholar] [CrossRef]
- Choi, J.D.W.; Kwik, C.; Shanmugalingam, A.; Allan, L.; Khoury, T. El; Pathmanathan, N.; Toh, J.W.T. C-Reactive Protein as a Predictive Marker for Anastomotic Leak Following Restorative Colorectal Surgery in an Enhanced Recovery After Surgery Program. J. Gastrointest. Surg. 2023, 27, 2604–2607. [Google Scholar] [CrossRef]
- Yeung, D.E.; Peterknecht, E.; Hajibandeh, S.; Hajibandeh, S.; Torrance, A.W. C-reactive protein can predict anastomotic leak in colorectal surgery: a systematic review and meta-analysis. Int. J. Colorectal Dis. 2021, 36, 1147–1162. [Google Scholar] [CrossRef] [PubMed]
- Paliogiannis, P.; Deidda, S.; Maslyankov, S.; Paycheva, T.; Farag, A.; Mashhour, A.; Misiakos, E.; Papakonstantinou, D.; Mik, M.; Losinska, J.; et al. C reactive protein to albumin ratio (CAR) as predictor of anastomotic leakage in colorectal surgery. Surg. Oncol. 2021, 38, 101621. [Google Scholar] [CrossRef]
- Ge, X.; Cao, Y.; Wang, H.; Ding, C.; Tian, H.; Zhang, X.; Gong, J.; Zhu, W.; Li, N. Diagnostic accuracy of the postoperative ratio of C-reactive protein to albumin for complications after colorectal surgery. World J. Surg. Oncol. 2017, 15, 1–7. [Google Scholar] [CrossRef]
- Sparreboom, C.L.; Wu, Z.; Dereci, A.; Boersema, G.S.A.; Menon, A.G.; Ji, J.; Kleinrensink, G.J.; Lange, J.F. Cytokines as early markers of colorectal anastomotic leakage: A systematic review and meta-analysis. Gastroenterol. Res. Pract. 2016, 2016. [Google Scholar] [CrossRef] [PubMed]
- Hajong, R.; Newme, K.; Nath, C.; Moirangthem, T.; Dhal, M.; Pala, S. Role of serum C-reactive protein and interleukin-6 as a predictor of intra-abdominal and surgical site infections after elective abdominal surgery. J. Fam. Med. Prim. Care 2021, 10, 403. [Google Scholar] [CrossRef]
- Azzini, A.M.; Dorizzi, R.M.; Sette, P.; Vecchi, M.; Coledan, I.; Righi, E.; Tacconelli, E. A 2020 review on the role of procalcitonin in different clinical settings: an update conducted with the tools of the Evidence Based Laboratory Medicine. Ann. Transl. Med. 2020, 8, 610–610. [Google Scholar] [CrossRef] [PubMed]
- Desborough, J.P. The stress response to trauma and surgery. Br. J. Anaesth. 2000, 85, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, K.; Ogawa, E.; Wada, H.; Hirata, T. Systemic inflammatory response syndrome and surgical stress in thoracic surgery. J. Crit. Care 2006, 21, 48–53. [Google Scholar] [CrossRef]
- Talmor, M.; Hydo, L.; Barie, P.S. Relationship of Systemic Inflammatory Response Syndrome to Organ Dysfunction, Length of Stay, and Mortality in Critical Surgical Illness: Effect of Intensive Care Unit Resuscitation. Arch. Surg. 1999, 134, 81–87. [Google Scholar] [CrossRef]
- Lin, L.; Pantapalangkoor, P.; Tan, B.; Bruhn, K.W.; Ho, T.; Nielsen, T.; Skaar, E.P.; Zhang, Y.; Bai, R.; Wang, A.; et al. Transferrin Iron Starvation Therapy for Lethal Bacterial and Fungal Infections. J. Infect. Dis. 2014, 210, 254–264. [Google Scholar] [CrossRef]
- Claise, C.; Saleh, J.; Rezek, M.; Vaulont, S.; Peyssonnaux, C.; Edeas, M. Low transferrin levels predict heightened inflammation in patients with COVID-19: New insights. Int. J. Infect. Dis. 2022, 116, 74–79. [Google Scholar] [CrossRef]
- Bharadwaj, S.; Ginoya, S.; Tandon, P.; Gohel, T.D.; Guirguis, J.; Vallabh, H.; Jevenn, A.; Hanouneh, I. Malnutrition: laboratory markers vs nutritional assessment. Gastroenterol. Rep. 2016, 4, 272–280. [Google Scholar] [CrossRef]
- Sharma, A.; Giraddi, G.; Krishnan, G.; Shahi, A.K. Efficacy of Serum Prealbumin and CRP Levels as Monitoring Tools for Patients with Fascial Space Infections of Odontogenic Origin: A Clinicobiochemical Study. J. Maxillofac. Oral Surg. 2014, 13, 1. [Google Scholar] [CrossRef]
- Ogun, A.S.; Adeyinka, A. Biochemistry, Transferrin; StatPearls Publishing, 2018.
- Aisen, P.; Enns, C.; Wessling-Resnick, M. Chemistry and biology of eukaryotic iron metabolism. Int. J. Biochem. Cell Biol. 2001, 33, 940–959. [Google Scholar] [CrossRef]
- Weinberg, E.D. Iron availability and infection. Biochim. Biophys. Acta - Gen. Subj. 2009, 1790, 600–605. [Google Scholar] [CrossRef]
- Siddiqui, K.; Uqaili, A.A.; Memon, S.; Shah, T.; Shaikh, S.N.; Memon, A.R. Association of Serum Albumin, Globulin, and Transferrin Levels in Children of Poorly Managed Celiac Disease. Biomed Res. Int. 2023, 2023, 5081303. [Google Scholar] [CrossRef]
- Ogle, C.K.; Wesley Alexander, J.; Macmillan, B.G. The relationship of bacteremia to levels of transferrin, albumin and total serum protein in burn patients. Burns 1981, 8, 32–38. [Google Scholar] [CrossRef]
- CDC Surgical Site Infection Event (SSI) Introduction. Natl. Healthc. Saf. Netw. 2022, 1–39.
- Macefield, R.; Blazeby, J.; Reeves, B.; Brookes, S.; Avery, K.; Rogers, C.; Woodward, M.; Welton, N.; Rooshenas, L.; Mathers, J.; et al. Validation of the Bluebelle Wound Healing Questionnaire for assessment of surgical-site infection in closed primary wounds after hospital discharge. Br. J. Surg. 2019, 106, 226–235. [Google Scholar] [CrossRef]
- Courtney, A.; Clymo, J.; Dorudi, Y.; Moonesinghe, S.R.; Dorudi, S. Scoping review: The terminology used to describe major abdominal surgical procedures. World J. Surg. 2024, 48, 574–584. [Google Scholar] [CrossRef]
- Courtney, A.; Dorudi, Y.; Clymo, J.; Cosentino, D.; Cross, T.; Moonesinghe, S.R.; Dorudi, S. Novel approach to defining major abdominal surgery. Br. J. Surg. 2024, 111. [Google Scholar] [CrossRef]
- Guest, J.F.; Fuller, G.W.; Griffiths, B. Cohort study to characterise surgical site infections after open surgery in the UK’s National Health Service. BMJ Open 2023, 13, e076735. [Google Scholar] [CrossRef]
- Hou, Y.; Collinsworth, A.; Hasa, F.; Griffin, L. Incidence and impact of surgical site infections on length of stay and cost of care for patients undergoing open procedures. Surg. Open Sci. 2023, 11, 1–18. [Google Scholar] [CrossRef]
- Eriksen, M.T.; Wibe, A.; Norstein, J.; Haffner, J.; Wiig, J.N. Anastomotic leakage following routine mesorectal excision for rectal cancer in a national cohort of patients. Color. Dis. 2005, 7, 51–57. [Google Scholar] [CrossRef]
- Seidelman, J.L.; Mantyh, C.R.; Anderson, D.J. Surgical Site Infection Prevention: A Review. JAMA 2023, 329, 244–252. [Google Scholar] [CrossRef]
- Zwicky, S.N.; Gloor, S.; Tschan, F.; Candinas, D.; Demartines, N.; Weber, M.; Beldi, G. Impact of gender on surgical site infections in abdominal surgery: A multi-center study. Br. J. Surg. 2022, 109, 17–21. [Google Scholar] [CrossRef]
- Aghdassi, S.J.S.; Schröder, C.; Gastmeier, P. Gender-related risk factors for surgical site infections. Results from 10 years of surveillance in Germany. Antimicrob. Resist. Infect. Control 2019, 8, 1–8. [Google Scholar] [CrossRef]
- Offner, P.J.; Moore, E.E.; Biffl, W.L. Male gender is a risk factor for major infections after surgery. Arch. Surg. 1999, 134, 935–940. [Google Scholar] [CrossRef]
- Gagen, B.; Hall, C. Preventing Surgical Site Infections in Emergency General Surgery: Current Strategies and Recommendations. Curr. Surg. Reports 2024, 12, 227–237. [Google Scholar] [CrossRef]
- Pellino, G.; Sciaudone, G.; Selvaggi, F.; Canonico, S. Prophylactic negative pressure wound therapy in colorectal surgery. Effects on surgical site events: current status and call to action. Updates Surg. 2015, 67, 235–245. [Google Scholar] [CrossRef]
- Wells, C.I.; Ratnayake, C.B.B.; Perrin, J.; Pandanaboyana, S. Prophylactic Negative Pressure Wound Therapy in Closed Abdominal Incisions: A Meta-analysis of Randomised Controlled Trials. World J. Surg. 2019, 43, 2779–2788. [Google Scholar] [CrossRef]
- Ban, K.A.; Minei, J.P.; Laronga, C.; Harbrecht, B.G.; Jensen, E.H.; Fry, D.E.; Itani, K.M.F.; Dellinger, E.P.; Ko, C.Y.; Duane, T.M. American College of Surgeons and Surgical Infection Society: Surgical Site Infection Guidelines, 2016 Update. J. Am. Coll. Surg. 2017, 224, 59–74. [Google Scholar] [CrossRef]
- De Simone, B.; Sartelli, M.; Coccolini, F.; Ball, C.G.; Brambillasca, P.; Chiarugi, M.; Campanile, F.C.; Nita, G.; Corbella, D.; Leppaniemi, A.; et al. Intraoperative surgical site infection control and prevention: A position paper and future addendum to WSES intra-abdominal infections guidelines. World J. Emerg. Surg. 2020, 15. [Google Scholar] [CrossRef]
- Xie, J.; Du, Y.; Tan, Z.; Tang, H. Association between malnutrition and surgical site wound infection among spinal surgery patients: A meta-analysis. Int. Wound J. 2023, 20, 4061. [Google Scholar] [CrossRef]
- Winfield, R.D.; Reese, S.; Bochicchio, K.; Mazuski, J.E.; Bochicchio, G. V. Obesity and the risk for surgical site infection in abdominal surgery. In Proceedings of the American Surgeon; Vol. 82; SAGE PublicationsSage CA: Los Angeles, CA, 2016; pp. 331–336. [Google Scholar]
- Kanda, H.; Tateya, S.; Tamori, Y.; Kotani, K.; Hiasa, K.I.; Kitazawa, R.; Kitazawa, S.; Miyachi, H.; Maeda, S.; Egashira, K.; et al. MCP-1 contributes to macrophage infiltration into adipose tissue, insulin resistance, and hepatic steatosis in obesity. J. Clin. Invest. 2006, 116, 1494–1505. [Google Scholar] [CrossRef]
- Nguyen, M.T.A.; Favelyukis, S.; Nguyen, A.K.; Reichart, D.; Scott, P.A.; Jenn, A.; Liu-Bryan, R.; Glass, C.K.; Neels, J.G.; Olefsky, J.M. A subpopulation of macrophages infiltrates hypertrophic adipose tissue and is activated by free fatty acids via toll-like receptors 2 and 4 and JNK-dependent pathways. J. Biol. Chem. 2007, 282, 35279–35292. [Google Scholar] [CrossRef]
- Lauterbach, M.A.R.; Wunderlich, F.T. Macrophage function in obesity-induced inflammation and insulin resistance. Pflugers Arch. Eur. J. Physiol. 2017, 469, 385–396. [Google Scholar] [CrossRef]
- Pugliese, G.; Liccardi, A.; Graziadio, C.; Barrea, L.; Muscogiuri, G.; Colao, A. Obesity and infectious diseases: pathophysiology and epidemiology of a double pandemic condition. Int. J. Obes. 2021 463 2022, 46, 449–465. [Google Scholar] [CrossRef]
- Ralph, N.; Brown, L.; McKillop, K.L.; Duff, J.; Osborne, S.; Terry, V.R.; Edward, K.L.; King, R.; Barui, E. Oral nutritional supplements for preventing surgical site infections: Protocol for a systematic review and meta-analysis. Syst. Rev. 2020, 9, 1–10. [Google Scholar] [CrossRef]
- Bucataru, A.; Balasoiu, M.; Ghenea, A.E.; Zlatian, O.M.; Vulcanescu, D.D.; Horhat, F.G.; Bagiu, I.C.; Sorop, V.B.; Sorop, M.I.; Oprisoni, A.; et al. Factors Contributing to Surgical Site Infections: A Comprehensive Systematic Review of Etiology and Risk Factors. Clin. Pract. 2024, Vol. 14, Pages 52-68 2023, 14, 52–68. [Google Scholar] [CrossRef]
- Khalil, R.H.; Al-Humadi, N. Types of acute phase reactants and their importance in vaccination (Review). Biomed. Reports 2020, 12, 143–152. [Google Scholar] [CrossRef]
- Gruys, E.; Toussaint, M.J.M.; Niewold, T.A.; Koopmans, S.J. Acute phase reaction and acute phase proteins. J. Zhejiang Univ. Sci. 2005, 6 B, 1045–1056. [Google Scholar] [CrossRef]
- Black, S.; Kushner, I.; Samols, D. C-reactive Protein. J. Biol. Chem. 2004, 279, 48487–48490. [Google Scholar] [CrossRef] [PubMed]
- Calabro, P.; Chang, D.W.; Willerson, J.T.; Yeh, E.T.H. Release of C-reactive protein in response to inflammatory cytokines by human adipocytes: linking obesity to vascular inflammation. J. Am. Coll. Cardiol. 2005, 46, 1112–1113. [Google Scholar] [CrossRef]
- Jain, S.; Gautam, V.; Naseem, S. Acute-phase proteins: As diagnostic tool. J. Pharm. Bioallied Sci. 2011, 3, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: a critical update. J. Clin. Invest. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.L.; Jiang, B.H.; Rue, E.A.; Semenza, G.L. Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS heterodimer regulated by cellular O2 tension. Proc. Natl. Acad. Sci. U. S. A. 1995, 92, 5510–5514. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T.; Nemeth, E. Iron Sequestration and Anemia of Inflammation. Semin. Hematol. 2009, 46, 387–393. [Google Scholar] [CrossRef]
- Van Der Poll, T.; Van De Veerdonk, F.L.; Scicluna, B.P.; Netea, M.G. The immunopathology of sepsis and potential therapeutic targets. Nat. Rev. Immunol. 2017, 17, 407–420. [Google Scholar] [CrossRef]
- Rollier, A.; DiPersio, C.M.; Cereghini, S.; Stevens, K.; Tronche, F.; Zaret, K.; Weiss, M.C. Regulation of albumin gene expression in hepatoma cells of fetal phenotype: dominant inhibition of HNF1 function and role of ubiquitous transcription factors. Mol. Biol. Cell 1993, 4, 59–69. [Google Scholar] [CrossRef]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Donlon, N.E.; Mohan, H.; Free, R.; Elbaghir, B.; Soric, I.; Fleming, C.; Balasubramanian, I.; Ivanovski, I.; Schmidt, K.; Mealy, K. Predictive value of CRP/albumin ratio in major abdominal surgery. Ir. J. Med. Sci. 2020, 189, 1465–1470. [Google Scholar] [CrossRef]
- Goulart, A.; Ferreira, C.; Estrada, A.; Nogueira, F.; Martins, S.; Mesquita-Rodrigues, A.; Sousa, N.; Leão, P. Early Inflammatory Biomarkers as Predictive Factors for Freedom from Infection after Colorectal Cancer Surgery: A Prospective Cohort Study. Surg. Infect. (Larchmt). 2018, 19, 446–450. [Google Scholar] [CrossRef]

Table 1.
Demographic characteristics and Mean length of hospital stay (in days) and presence of post-operative complications and the incidence of each complication (SD standard deviation, n number, R rate).
Table 1.
Demographic characteristics and Mean length of hospital stay (in days) and presence of post-operative complications and the incidence of each complication (SD standard deviation, n number, R rate).
| Type of Study | ||||||||
| Prospective | Retrospective | Total | p | |||||
| N (%) | N (%) | N (%) | ||||||
| Sex | Female | 48 (55.8%) | 38 (44.2%) | 86 (43%) | 0.938 | |||
| Male | 63 (55.3%) | 51 (44.7%) | 114 (57%) | |||||
| Age groups | <= 40 | 8 (66.7%) | 4 (33.3%) | 12 (6%) | 0.685 | |||
| 41 - 50 | 8 (53.3%) | 7 (46.7%) | 15 (7.5%) | |||||
| 51 - 60 | 17 (58.6%) | 12 (41.4%) | 29 (14.5%) | |||||
| 61 - 70 | 38 (61.3%) | 24 (38.7%) | 62 (31%) | |||||
| 71 - 80 | 27 (49.1%) | 28 (50.9%) | 55 (27.5%) | |||||
| 81+ | 13 (48.1%) | 14 (51.9%) | 27 (13.5%) | |||||
| Elective Operation | Yes | 62 (60%) | 40 (39.2%) | 102 (51%) | 0.125 | |||
| No | 49 (40%) | 49 (60.8%) | 98 (49%) | |||||
| Post-Operative complications | No | 54 (48.6%) | 27 (30.3%) | 81 (40.5%) | 0,002 | |||
| 1 | 34 (30.6%) | 37 (41.6%) | 71 (35.5%) | |||||
| 2 | 10 (9%) | 21 (23.6%) | 31 (15.5%) | |||||
| 3 | 9 (8.1%) | 4 (4.5%) | 13 (6.5%) | |||||
| 4 | 4 (3.6%) | 0 (0%) | 4 (2%) | |||||
| Wound Infection | No | 54 (48.6%) | 27 (30.3%) | 81 (40.5%) | 0,009 | |||
| Yes | 57 (51.4%) | 62 (69.7%) | 119 (59.5%) | |||||
| Wound dehiscence | No | 92 (82.9%) | 72 (80.9%) | 164 (82%) | 0,717 | |||
| Yes | 19 (17.1%) | 17 (19.1%) | 36 (18%) | |||||
| Intrabdominal Abscess | No | 99 (89.2%) | 77 (86.5%) | 176 (88%) | 0,563 | |||
| Yes | 12 (10.8%) | 12 (13.5%) | 24 (12%) | |||||
| Anastomotic /stump Leak | No | 64 (85.9%) | 61 (100%) | 125 (95.4%) | 0,006 | |||
| Yes | 9 (14.1%) | 0 (0%) | 9 (4.6%) | |||||
| Re-operation | No | 109 (98.2%) | 83 (93.3%) | 192 (96%) | 0,076 | |||
| Yes | 2 (1.8%) | 6 (6.7%) | 8 (4%) | |||||
| Mean | SD | Mean | SD | Mean | SD | |||
| Age | 63.9 | 15 | 66.6 | 14.6 | 65.1 | 14.8 | 0.204 | |
| BMI | 27 | 3.8 | 27.5 | 3.6 | 27.2 | 3.7 | 0.399 | |
| Length of Stay (Days) | 8.9 | 4.7 | 13.9 | 8.0 | 11.1 | 6.8 | <0.001 | |
Table 2.
Anova (N/I =No infection, Inf =Infection).
| Laboratory Test | Day 1 | Day 2 | Day 3 | df1. df2 | F | p | ||||
| Mean | SD | Mean | SD | Mean | SD | |||||
| WBCs (10^3) | Total | 11.8 | 4.5 | 10.9 | 3.9 | 9.7 | 3.3 | 2. 588 | 24.28 | <0.001 |
| N/I | 11.9 | 4.4 | 10.7 | 3.9 | 9.5 | 3. | 3. 585 | 0.86 | 0.461 | |
| Inf | 11.7 | 4.5 | 11 | 4 | 9.9 | 3.4 | ||||
| CRP (mg/dl) | Total | 11.55 | 8.33 | 17.53 | 8.92 | 16.47 | 8.42 | 2. 398 | 66.73 | <0.001 |
| N/I | 7.99 | 6.06 | 11.76 | 7.24 | 10.76 | 6.01 | 2. 396 | 7.24 | 0.001 | |
| Inf | 13.98 | 8.79 | 21.46 | 7.75 | 20.35 | 7.59 | ||||
| Alb (g/dl) | Total | 3.3 | 0.5 | 3.2 | 0.4 | 3.1 | 0.4 | 2. 398 | 99.66 | <0.001 |
| N/I | 3.5 | 0.4 | 3.4 | 0.4 | 3.3 | 0.3 | 2. 396 | 3.13 | 0.052 | |
| Inf | 3.2 | 0.5 | 3.0 | 0.4 | 2.9 | 0.4 | ||||
| Transferrin (mg/dl) | Total | 171.5 | 44.8 | 158.6 | 41.2 | 150.9 | 37.7 | 2. 220 | 76.11 | <0.001 |
| N/I | 182.8 | 43.7 | 172.7 | 41.9 | 163.0 | 37.2 | 2. 218 | 76.05 | 0.272 | |
| Inf | 160.7 | 43.5 | 145.3 | 36.2 | 139.4 | 34.7 | ||||
| CRP/ Alb | Total | 3.7 | 3.0 | 5.8 | 3.2 | 5.6 | 3.1 | 2. 398 | 72.19 | <0.001 |
| N/I | 2.4 | 2.0 | 3.6 | 2.3 | 3.3 | 1.9 | 2. 396 | 10.97 | <0.001 | |
| Inf | 4.6 | 3.2 | 7.3 | 2.9 | 7.1 | 2.9 | ||||
| CRP/ Trans | Total | 0.07 | 0.06 | 0.11 | 0.07 | 0.11 | 0.07 | 2. 220 | 39.36 | <0.001 |
| N/I | 0.05 | 0.07 | 0.08 | 0.06 | 0.07 | 0.04 | 2. 218 | 15.12 | <0.001 | |
| Inf | 0.08 | 0.06 | 0.15 | 0.07 | 0.15 | 0.07 | ||||
Table 3.
Multi-parametric analysis for binary and continues variables (COPD chronic obstructive pulmonary disease, BMI body mass index, CAR C-reactive protein to albumin ratio, CTR C-reactive protein to transferrin ratio).
Table 3.
Multi-parametric analysis for binary and continues variables (COPD chronic obstructive pulmonary disease, BMI body mass index, CAR C-reactive protein to albumin ratio, CTR C-reactive protein to transferrin ratio).
| Post-Operative complications | ||||
| Parameter | No | Yes | p | |
| N (%) | N (%) | |||
| Sex | Female | 44 (54.3%) | 42 (35.3%) | 0.008 |
| Male | 37 (45.7%) | 77 (64.7%) | ||
| Type of Study | Prospective | 54 (66.7%) | 57 (47.9%) | 0.009 |
| Retrospective | 27 (33.3%) | 62 (52.1%) | ||
| Elective Operation | No | 52 (64.2%) | 46 (38.7%) | <0.001 |
| Yes | 29 (35.8%) | 73 (61.3%) | ||
| Age (years) | <= 40 | 5 (6.2%) | 7 (5.9%) | 0.343 |
| 41 - 50 | 3 (3.7%) | 12 (10.1%) | ||
| 51 - 60 | 10 (12.3%) | 19 (16.0%) | ||
| 61 - 70 | 25 (30.9%) | 37 (31.1%) | ||
| 71 - 80 | 23 (28.4%) | 32 (26.9%) | ||
| 81+ | 15 (18.5%) | 12 (10.1%) | ||
| Hypertension | No | 35 (43.2%) | 50 (42.0%) | 0.867 |
| Yes | 46 (56.8%) | 69 (58.0%) | ||
| Diabetes Type II | No | 61 (75.3%) | 86 (72.3%) | 0.633 |
| Yes | 20 (24.7%) | 33 (27.7%) | ||
| COPD | No | 67 (82.7%) | 97 (81.5%) | 0.828 |
| Yes | 14 (17.3%) | 22 (18.5%) | ||
| Chronic Renal Disease | No | 75 (92.6%) | 106 (89.1%) | 0.405 |
| Yes | 6 (7.4%) | 13 (10.9%) | ||
| Cancer | No | 40 (49.4%) | 58 (48.7%) | 0.929 |
| Yes | 41 (50.6%) | 61 (51.3%) | ||
| Metastatic Cancer | No | 75 (92.6%) | 111 (93.3%) | 0.952 |
| Yes | 6 (7.4%) | 8 (6.7%) | ||
| Mean (SD) | Mean (SD) | |||
| Age (years) | 67.16 (14.61) | 63.76 (14.86) | 0.092 | |
| BMI (Kg/m2) | 26.98 (3.4) | 27.37 (3.89) | <0.001 | |
| Post Op CRP D2 | 11.76 (7.24) | 21.46 (7.75) | <0.001 | |
| Post Op Alb D2 | 3.37 (0.36) | 3 (0.41) | <0.001 | |
| Post Op WBCs D2 | 10.54 (3.86) | 10.99 (3.97) | 0.351 | |
| CAR DAY 2 | 3.59 (2.32) | 7.31 (2.89) | <0.001 | |
| CTR DAY 2 | 0.08 (0.06) | 0.15 (0.07) | <0.001 | |
| CTR DAY2 x100 | 7.56 (6.01) | 14.92 (6.96) | <0.001 | |
Table 4.
Logistic regression analysis (OR odds ratio, LL lower limit, UL upper limit, COPD chronic obstructive pulmonary disease, BMI body mass index, CAR C-reactive protein to albumin ratio, CTR C-reactive protein to transferrin ratio).
Table 4.
Logistic regression analysis (OR odds ratio, LL lower limit, UL upper limit, COPD chronic obstructive pulmonary disease, BMI body mass index, CAR C-reactive protein to albumin ratio, CTR C-reactive protein to transferrin ratio).
| Parameter | OR | 95%LL | 95%UL | p |
| Age (years) | 0.98 | 0.94 | 1.01 | 0.166 |
| BMI (Kg/m2) | 0.90 | 0.79 | 1.02 | 0.101 |
| Female Sex | 0.23 | 0.08 | 0.68 | 0.008 |
| Elective Operation | 0.86 | 0.29 | 2.54 | 0.781 |
| Hypertension | 1,07 | 0,45 | 2,54 | 0,870 |
| Diabetes Type II | 1,52 | 0,61 | 3,78 | 0,372 |
| COPD | 1,20 | 0,37 | 3,91 | 0,764 |
| Chronic Renal Disease | 0,99 | 0,19 | 5,25 | 0,992 |
| Presence of Cancer | 1,70 | 0,69 | 4,21 | 0,251 |
| Post Op TRF D2 | 1.01 | 1.00 | 1.03 | 0.137 |
| Post Op Alb D2 | 0.05 | 0.01 | 0.33 | 0.002 |
| CTR DAY 2 x 100 | 1.23 | 1.10 | 1.39 | 0.000 |
| CTR DAY 3 x 100 | 1,40 | 1,21 | 1,61 | <0,001 |
| CAR DAY 2 | 1.73 | 1.32 | 2.29 | <0.001 |
| CAR DAY 3 | 2,02 | 1,63 | 2,51 | 0,000 |
| FORWARD | OR | 95%LL | 95%UL | p |
| Female Sex | 0.26 | 0.09 | 0.71 | 0.009 |
| Post Op Alb D2 | 0.12 | 0.03 | 0.52 | 0.005 |
| CTR DAY 2 x 100 | 1.18 | 1.07 | 1.29 | <0.001 |
| CTR DAY 3 x 100 | 1,42 | 1,24 | 1,63 | <0,001 |
| CAR DAY 2 | 1.68 | 1.31 | 2.17 | <0.001 |
| CAR DAY 3 | 2,02 | 1,65 | 2,48 | <0,001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



