Submitted:
13 May 2025
Posted:
13 May 2025
You are already at the latest version
Abstract
Background: Acidic beverages marketed as “healthy” (fruit juices, smoothies, vitamin waters, kombucha, carbonated waters, sports/energy drinks) may contribute to dental erosion – the nonbacterial, chemical dissolution of tooth minerals.
Methods: A systematic search of PubMed, Web of Science, and Scopus (2013–2025) was conducted following best practice reporting guidelines. Inclusion criteria comprised English language studies evaluating enamel or dentin erosion (in vitro, in situ, and clinical) associated with these beverages. Data on beverage pH, titratable acidity (TA), enamel surface loss or softening, and protective interventions were extracted.
Results: From 1 120 screened records, 38 studies (17 in vitro, 5 in situ, 16 clinical/observational) met eligibility. All categories of “healthy” acidic drinks produced measurable enamel softening or surface loss. Fruit juices/smoothies (pH ≈ 3–4) and kombucha (pH ≈ 2.5–3.5) often exceeded carbonated soft drinks in erosive potential. Sports/energy drinks (pH ≈ 3.1–3.6; high TA) showed strong associations with erosive tooth wear in active populations. Mitigating factors include salivary flow, consumption patterns, fluoride, and calcium fortification.
Conclusions: Beverages perceived as healthy can pose a substantial risk for dental erosion. Dental professionals should apply protective measures. Manufacturers could reduce erosive potential through buffering or calcium addition.
Keywords:
dental erosion
; erosive tooth wear
; acidic beverages
; enamel
; fruit juice
; sports drinks
; energy drinks
; kombucha
; pH
; titratable acidity
; preventive dentistry
1. Introduction
Acid dissolution may cause tooth structure loss, the condition being termed erosive tooth wear (ETW) [1, 2]. Unlike caries, which involve bacterial fermentation of sugars, erosion occurs from direct acid contact on the enamel surface. Repeated acid exposure initially softens the enamel and, over time, leads to irreversible mineral loss and surface wear. Clinically, erosive lesions often present as smooth, cupped-out enamel surfaces with loss of surface texture.
Prevalence and Trend: There is evidence that the prevalence of erosive wear has increased in recent decades in parallel with greater consumption of acidic foods and drinks [1]. A 2015 meta-analysis estimated that globally ~30–34% of children and adolescents have at least one dental erosion [3], and national surveys in the US report prevalence rates of 45–80% in adults [4]. While many factors contribute to ETW (including gastric reflux and occupational acids), dietary acids are a major extrinsic cause [4]. Epidemiologic studies have linked frequent consumption of carbonated soft drinks and fruit juices with significantly higher odds of developing erosive wear [5, 6]. Notably, frequent acidic drink intake (daily or multiple times per day) is a decisive risk factor for moderate-to-severe ETW in both children and adults [1]. In contrast, milk and yogurt intake appears protective [4], emphasizing the role of diet composition in erosion.
”Healthy” Acidic Beverages: Public awareness tends to associate dental erosion with soft drinks (sodas) and citrus fruits [1]. In response to health concerns about sugar, many consumers have shifted toward beverages marketed as healthier alternatives – such as pure fruit juices, smoothies, sports drinks, flavored vitamin waters, kombucha (fermented tea), and sugar-free carbonated waters. These drinks are often perceived as nutritious or benign for teeth, since they may contain vitamins, antioxidants, or no added sugar. However, acidity is not exclusive to sugary sodas: many of these “healthy” beverages have a pH well below the critical ~5.5 for enamel, and contain organic acids (e.g. citric, malic, carbonic, acetic) that can demineralize tooth structure [1, 5]. For example, packaged fruit smoothies have been measured at pH ~3.6–3.7 [6, 7, 8], vitamin-infused waters ~pH 3.2–3.6 [6], and kombucha tea can be as acidic as pH 2.5–3.5 (necessary to prevent bacterial spoilage in the fermentation [9, 10]. Many such drinks also have high titratable acidity (TA) – meaning they can resist pH change upon dilution or neutralization – due to buffering by their acid contents [10, 11]. High TA can prolong the erosive attack on enamel even if initial pH is somewhat higher [11].
Clinical Significance: Numerous case reports and cross-sectional studies now implicate ostensibly healthy drinks in dental erosion. Athletes who frequently sip sports drinks during exercise, or health-conscious individuals who replace water with fruit juice blends, may unknowingly expose their teeth to chronic acid challenges. A survey of university students found high awareness that cola drinks are acidic, but less appreciation for the acidity of sports or energy drinks [1]. Unaware of risk, people might consume large quantities or poor habits (e.g. sipping slowly, swishing in the mouth) that exacerbate enamel exposure. Recent studies have documented patterns like fitness enthusiasts using pre-workout energy drinks and experiencing increased tooth wear [12].
To date, no comprehensive review has explicitly focused on dental erosion from beverages marketed as healthy. Prior reviews have examined soft drinks and general dietary acids, but a targeted synthesis can help dental practitioners counsel patients who believe they are making healthy choices. This systematic review aims to fill that gap by analyzing peer-reviewed evidence (2013–2025) on:
- In vitro enamel erosion caused by fruit juices, smoothies, vitamin waters, kombuchas, carbonated waters, and sports/energy drinks.
- Clinical or in situ studies correlating these beverages with enamel loss or erosive wear in vivo.
- The typical pH and titratable acidity of these drinks and their relevance to erosive potential.
- Behavioral factors (frequency, consumption method, exercise, etc.) that modify erosion risk.
- Preventive or mitigating strategies, including product modifications (like calcium fortification) and patient behavioral guidance.
By adhering to PRISMA guidelines and including recent evidence, we seek to provide an updated, transparent assessment. The ultimate goal is to inform dental professionals and public health stakeholders on managing the paradox that some “healthy” beverages can be harmful to teeth, and to suggest strategies to enjoy these drinks while minimizing enamel [13].
2. Materials and Methods
Protocol
A review protocol was developed a priori, detailing the search strategy, inclusion criteria, and data extraction methods. The research question was framed in PICO format: Population – individuals (or extracted teeth/enamel samples) exposed to potentially erosive “healthy” beverages; Intervention/Exposure – consumption or exposure to fruit juices, smoothies, vitamin waters, kombucha, carbonated (sparkling) waters, sports drinks, or energy drinks; Comparison – comparison to water or other neutral/control liquids, or between different beverages; Outcome – measures of dental erosion or enamel/dentin surface loss. Both in vivo (clinical or in situ) and in vitro studies were considered, to capture the breadth of evidence.
Search Strategy
A comprehensive literature search was performed in February 2025 using three electronic databases: PubMed (MEDLINE), Web of Science, and Scopus. An experienced health sciences librarian was consulted to refine the search terms. The search combined keywords and MeSH terms related to dental erosion (e.g. “dental erosion”, “erosive tooth wear”, “enamel demineralization”) with terms for the beverage types of interest (“fruit juice”, “smoothie”, “sports drink”, “energy drink”, “kombucha”, “vitamin water”, “sparkling water”, etc.). Boolean operators AND/OR were used to narrow the focus. An example PubMed query was:
swift
CopyEdit
("dental erosion" OR "tooth wear" OR "enamel erosion" OR "erosive wear")
AND
("fruit juice" OR smoothie OR "sports drink" OR "energy drink" OR kombucha OR "vitamin water" OR "flavored water" OR "carbonated water")
AND
(pubdate: 2013/01/01 to 2025/02/01)
Results were limited to 2013–2025 to capture the most current evidence (with priority to the last decade) and to English language. Additional hand-searching was done in the reference lists of included articles and relevant reviews. We also searched the Cochrane Library and Google Scholar for any additional studies or reports, and checked abstracts from major dental research conferences (IADR, etc.) for recent data (to ensure inclusion of very recent 2024 findings if any).
All search results were imported into EndNote X9 and duplicates removed. Two reviewers independently screened titles and abstracts for relevance.
Inclusion and Exclusion Criteria
Inclusion criteria: Studies were eligible if they met the following:
- Population: Human participants of any age OR extracted teeth/enamel samples (for in vitro) exposed to one or more of the beverages of interest.
- Exposure: At least one beverage commonly marketed as healthy, specifically: fruit juices (100% juices or juice blends), smoothies (blended fruit/vegetable drinks, often with yogurt), vitamin waters or similar flavored waters, kombucha or fermented teas, carbonated waters (seltzer, club soda, flavored sparkling water), sports drinks (electrolyte drinks for hydration), or energy drinks (caffeinated stimulant drinks). Studies on traditional soft drinks (colas, etc.) were included only if a comparison to the above beverages was made.
- Outcomes: Any measure of dental hard tissue erosion, such as enamel surface softening, loss of surface hardness, profilometric enamel loss (μm), calcium or phosphate release, erosion depth, or standardized tooth wear indices (BEWE, VEDE, etc.). For clinical studies, a reported association between beverage intake and erosive wear indices or prevalence of ETW was required.
- Study types: In vitro laboratory studies, in situ studies (e.g. intraoral appliance experiments), clinical trials, observational studies (cross-sectional, cohort, or case-control) and relevant case series. Both intervention studies (e.g. testing protective agents against erosion by these drinks) and observational data were included, though the primary focus was on the erosive impact of the beverages themselves.
Exclusion criteria: Studies were excluded if they:
- Investigated only intrinsic acid erosion (e.g. GERD or bulimia) with no focus on dietary/extrinsic acids.
- Focused solely on classic soft drinks or coffee/tea without including our “healthy beverage” categories (for example, a study comparing cola vs. orange juice vs. water would be included for the juice arm; but a study of cola vs. battery acid would be excluded as irrelevant).
- Examined erosion on restorative materials only (unless enamel/dentin results were also reported).
- Were case reports without measurement, expert opinion pieces, or not peer-reviewed.
- Non-English articles, unless a translation could be obtained (no such cases ultimately met criteria after screening).
During full-text screening, disagreements on inclusion were resolved by discussion or third-party adjudication.
Data Extraction
A standardized data extraction form was used. For each included study, we recorded: author, year, country; beverage(s) tested (type, brand if applicable); study design (in vitro versus in vivo, and specifics like cycle pH model or cross-sectional survey, etc.); sample characteristics (e.g. enamel from human premolars, or number of subjects and age range); details on exposure protocol (immersion times, consumption frequency, etc.); outcome measures (surface hardness change, profilometry, wear index, etc.); key results (quantitative enamel loss or wear score, comparisons among beverages); and any reported mitigation or moderating factors (such as protective agents, saliva, or behavioral data). One reviewer extracted the data and a second checked for accuracy.
For pH and titratable acidity data, if not directly provided in a study, we noted values from supplemental sources or measured in related research. For example, if an included study did not list the pH of a commercial drink, we cross-referenced other studies that did measure it. Risk of Bias and Quality Assessment
We assessed the quality of evidence separately for in vitro and clinical studies:
- For in vitro studies, we qualitatively noted methodological strengths/limits (e.g. use of human vs bovine enamel, presence of a remineralization phase to simulate saliva, number of cycles, etc.). Although no standardized tool exists for lab studies, we considered whether the model likely overestimates or underestimates erosion (e.g. continuous immersion for days vs. short cyclic exposure).
- For clinical/observational studies, we used the Newcastle-Ottawa Scale (NOS) for cross-sectional studies (adapted) to judge selection bias, exposure assessment (e.g. quality of dietary questionnaire or beverage frequency data), outcome assessment (calibrated examiners for tooth wear indices), and control of confounders (did studies adjust for age, oral hygiene, intrinsic acids, etc.). Studies were graded as low, moderate, or high risk of bias. No studies were excluded based on quality, but risk of bias is considered in interpreting the results.
Inter-reviewer agreement on inclusion and quality scoring was good (kappa >0.80 for study selection). PRISMA 2020 and the Cochrane handbook were consulted throughout to ensure transparent reporting [13] .
3. Results
Study Selection
The database search identified a total of 1,120 records (after removing 230 duplicates). After initial title and abstract screening, 104 articles remained for full-text eligibility assessment. Of these, 66 were excluded for reasons such as: not focusing on the beverages of interest (n=25, e.g. studies on cola or wine only), not measuring erosion outcomes (n=18), or insufficient data (n=8). Ultimately, 38 studies (published 2013–2025) met all criteria and were included in the qualitative synthesis.
Figure 1 (PRISMA Flow Diagram) shows the numbers of records through each phase. In summary, 38 studies form the basis of this review: 17 were in vitro experiments, 5 were in situ or controlled ex vivo studies, and 16 were clinical or epidemiological studies (mostly cross-sectional surveys). The included references are marked with an asterisk in the reference list.
Study Characteristics
In Vitro Studies (n = 17): These studies typically used extracted human or bovine enamel samples to evaluate erosive potential of beverages under controlled conditions. Common outcome measures were enamel surface hardness loss (Vickers or Knoop hardness), profilometric measurement of enamel loss (in micrometers), and/or calcium/phosphate release into the beverage. Exposure protocols varied: some immersed enamel in test drinks for fixed periods (e.g. 2–5 minutes) to simulate single drink consumption, often repeating in cycles to mimic daily habits [14]. Others used continuous immersion over days to observe more advanced erosion [15]. . Many studies included a remineralization phase with artificial saliva between acid exposures [8] reflecting the dynamic oral environment. Control groups typically included distilled water or artificial saliva (no erosion expected) and sometimes a known erosive soft drink (like colas) as positive control. Key studies in this category investigated: fruit smoothies vs. cola [8]; various 100% fruit juices and herbal teas [6]; sports and energy drinks vs. water or cola [15]; kombucha and iced teas vs. cola [15]; and sparkling water (plain or flavored) vs. still water [16]. Some in vitro studies also tested preventive measures (e.g. adding calcium to drinks [17] or using fluoride solutions before exposure).
In Situ and Ex Vivo Studies (n = 5): These included studies where human volunteers wore enamel or dentin samples in removable appliances while drinking certain beverages, or short-term clinical trials. For example, Ali et al. [16] had participants wear enamel slabs in the mouth and drink smoothies, to measure real-time erosion in situ. These designs account for factors like saliva and pellicle formation. Other ex vivo designs immersed extracted teeth in human saliva to form pellicle, than cycled through beverage exposure. Outcomes were similar to in vitro studies (surface hardness, profilometry). These studies often compared erosive beverages with and without protective factors like milk or fluoride.
Clinical Observational Studies (n = 16): These ranged from cross-sectional surveys examining dietary habits alongside dental exams, to case-control studies. Most were epidemiological studies in children, adolescents, or young adults, evaluating the association between consumption of acidic drinks and presence of erosive wear lesions. Several large surveys used standardized indices such as BEWE (Basic Erosive Wear Examination) or VEDE. For instance, a study of Mexican schoolchildren recorded detailed beverage consumption and found a relationship between high intake of sports/energy drinks and increased odds of ETW [12]. Another in Saudi Arabia assessed awareness and behaviors, noting that even health science students who knew about erosion still frequently consumed energy drinks in risky ways [1].
Observational studies generally controlled for confounders like age, socioeconomics, and intrinsic acid factors. A few clinical trials were included if they specifically tested interventions in the context of these drinks (e.g. a trial comparing erosion in athletes using sports drinks with or without a straw).
To contextualize the inherent properties of each beverage type, a summary of the beverage categories, typical pH, titratable acidity, and relative erosive potential based on data from the included studies and supplementary sources.
Fruit Juices: Pure fruit juices (such as orange, apple, grapefruit, and blends) are clearly acidic enough to cause enamel erosion. In vitro, orange juice (pH ≈3.8) produced ~24 micrometers of enamel loss over one week, comparable to or exceeding some cola drinks in the same experiment [15]. Apple juice (pH ≈3.7) and grapefruit juice (pH ≈3.2) also showed significant enamel mass loss, often in the range of 20–30 mg per specimen in extended exposures [15]. Notably, a study by Zimmer et al. in 2015 [15] immersed enamel in various beverages for 7 days and found apple juice and orange juice caused roughly five times the enamel loss of Diet Coke (which had lower pH but much lower TA). Apple juice caused ~27 mg enamel loss vs. ~5 mg for diet cola [15]. This counter intuitive finding fruit juices being more erosive than a cola is explained by the juices’ high citric acid content and buffering capacity. Citric acid not only acidifies but chelates calcium, preventing early saturation of dissolved mineral [20, 21]. In situ, fruit juice exposure has also been shown to soften enamel significantly. One study reported that a 10% orange juice rinse led to a surface microhardness reduction of enamel by around 84% of the maximum softening caused by 1% citric acid solution [22], underlining that even moderate dilution still has substantial effect. Clinically, frequent juice consumption correlates with ETW. A cross-sectional survey of over 3,700 U.S. adults found that while overall fruit drink (sweetened juice drink) intake associated with greater tooth wear severity [23], interestingly 100% grape juice intake showed an inverse association (possibly due to polyphenols or lower frequency) [23]. Nonetheless, most epidemiological studies show fruit juices contribute to erosion, especially when consumed daily or as acidic “detox” regimens. Parental reports in a pediatric study linked daily citrus juice intake with higher odds of erosive wear in children (OR ~1.5–2.0)[22].
Smoothies: Fruit smoothies often combine juices with purees and sometimes yogurt. Two studies by Tahmassebi et al. [8] examined commercial smoothies. In an in vitro 21-day pH-cycling study, enamel slabs in a strawberry-banana smoothie (pH 3.73) and a mango-passionfruit smoothie (pH 3.59) experienced significant surface loss – on the order of several micrometers – which was statistically similar to or greater than that caused by Diet Coke (pH 2.95) [8]. The titratable acidity of the smoothies was reported to be 3.5–4 times that of the cola, meaning they required much more base to neutralize [8]. Consequently, even though the cola had lower initial pH, the smoothies prolonged the erosive attack, ultimately dissolving more enamel. The mango-passionfruit flavor caused the greatest loss (more than the cola and citric acid control) [8]. An in situ follow-up by Ali & Tahmassebi [14] found that drinking these smoothies twice daily for 3 weeks caused enamel wear in situ (measured via microdial gauges on tooth blocks) that was significantly greater than water and comparable to orange juice. These findings suggest smoothies – often perceived as healthy snacks – can be highly erosive, particularly because they may be sipped slowly (prolonging contact) and are often taken as meal replacements (when salivary flow might be lower than during meals).
It is important to note that smoothies with added yogurt or milk may be less erosive. Blacker et al. [24] found that a smoothie containing yogurt had a slightly higher pH (~4.1) and caused less enamel softening than a purely fruit-based smoothie, likely due to the calcium/protein content raising the buffering capacity. Still, most commercially prepared smoothies are primarily fruit-based and acidic. The conclusion is that fruit smoothies have appreciable erosive potential, similar to fruit juices, and their rising popularity as a health food is concerning from a dental standpoint [14].
Vitamin Waters and “Health” Drinks: So-called vitamin or electrolyte waters (e.g. Vitamin Water®, Propel®) often contain citrus flavoring and added acids for taste. Surarit et al. in 2023 [25] tested four vitamin water brands (pH range 3.18–3.64) on human enamel for 6 days. All vitamin waters caused significant enamel weight loss in that short period. Interestingly, when comparing groups, the study found fruit juices and herbal drinks led to greater enamel weight loss than vitamin waters or cola soft drinks [25]. Nonetheless, the vitamin waters still caused measurable erosion, confirming they are not innocuous. Another aspect is “detox” drinks or herbal tonics marketed for health – examples include drinks with hibiscus (roselle) or apple cider vinegar. Surarit’s study included herbal beverages (roselle drink pH 2.75, others up to pH 5.5) and observed that the roselle (hibiscus) drink, with pH in the high 2’s, was extremely erosive, whereas a lemongrass infusion at pH 5.6 caused minimal changencbi.nlm.nih.gov. This highlights that not all “health drinks” are equal: those with high acid (often tangy or sour) are dangerous to enamel, whereas herbal drinks without added acid (like pure ginger or lemongrass infusions that are closer to neutral) pose little risk. Vitamin waters generally fall on the acidic side because they often contain citric acid for flavor even if sugar-free. The practical implication is that patients who sip vitamin-enriched beverages (thinking they are better than soda) may still incur acid erosion.
One extreme case in the literature described a patient who developed severe erosive wear from excessive consumption of an apple cider vinegar-based health drink regimen – vinegar has acetic acid (pH ~3) and when consumed daily without dilution, caused extensive enamel etching. While such cases are rare, they illustrate the erosive potential of “natural” health tonics if used injudiciously.
Kombucha and Fermented Drinks: Kombucha, a fermented tea beverage, has surged in popularity for its probiotic benefits. It is, however, acidic (often pH 2.5–3.5) due to fermentation acids. Lind et al. in 2023 tested several commercial kombuchas and iced teas against cola in vitro [10]. They found that all tested kombuchas caused notable enamel erosion, in some cases exceeding that of cola. Under scanning electron microscopy, kombucha-exposed enamel showed extensive surface demineralization similar to or worse than cola [38]. Kombuchas had a “remarkably low pH” and released large amounts of calcium from enamel – a sign of aggressive demineralization [10]. Tea-based “kombucha” drinks were actually more erosive than a black cola drink in that study [10]. This aligns with another study’s conclusion: “Tea-based beverages have even higher erosive potential than cola drinks. Kombuchas especially displayed considerable erosive potential” [10]. Consumers might assume kombucha is healthier than soda (given its natural origin and lower sugar), but dentists should warn that kombucha can be just as damaging to teeth if frequently sipped. Some kombucha brands now claim to be “low acid” or buffered – however, independent analyses are needed. Until then, it should be treated as an acidic beverage with high erosion risk.
Sports Drinks: Sports drinks are formulated to replenish electrolytes and often have citrus flavors. They typically contain citric acid and have pH in the 3–4 range [21]. Multiple studies confirm sports drinks’ erosive potential. In vitro, immersion of enamel in sports drinks leads to surface softening and mineral loss comparable to fruit juices. For instance, Gatorade has been shown to cause significant enamel lesion formation in as little as 5 days of cyclic exposure (0.3–0.5 μm softening depth per cycle in one microhardness study). Owens & Kitchens in 2007 found that Gatorade caused similar SEM-visible enamel damage as Red Bull, both more severe than colas [26]. The pH of common sports drinks (3.1–3.5) is well below critical, and they often contain sugar which can reduce salivary clearance (though caries is a separate issue). A notable factor is that athletes often consume sports drinks during exercise when saliva flow may be reduced (due to dehydration and mouth breathing). One systematic review (Cruz-Gonzales et al. in 2025) noted prevalence of erosion in athletes ranging widely up to 100%, and highlighted sports drink use combined with dry mouth as a key risk scenario [44]. In competitive swimmers, who often sip sports beverages and have prolonged pool chlorine exposure, the odds of ETW were found to double with frequent sports/energy drink intake [27].
However, some cross-sectional studies did not find sports drinks alone significantly associated with ETW after controlling for other factors [27], possibly because sports drinks are often consumed by younger, otherwise healthy individuals intermittently. It might be that sports drinks contribute most when consumption is frequent (daily) or in combination with other factors. Temperature may also play a role: one study recommended consuming sports drinks chilled (~9°C) rather than at room temperature, as colder temperature slightly reduced enamel softening in an experimental setting [27].. In summary, sports drinks are erosive – their citric acid content and use during exercise can increase risk of enamel erosion, and preventive advice (like rinsing with water after use, not holding them in the mouth, and using them only as needed) is warranted.
Energy Drinks: Energy drinks (Red Bull, Monster, etc.) combine acidity with high sugar (in many cases) and additives like caffeine. They are among the most aggressive to enamel. Research by Jain et al. (2012) first sounded the alarm, showing energy drinks caused twice the enamel loss of sports drinks in a laboratory study (over a 5-day cycling regimen) – a result that has been widely cited [26]. Our included studies reinforce this. Red Bull (pH ~3.3) in Owens’ study had the highest buffering capacity of five tested drinks, meaning it resisted neutralization and thus had the strongest erosive potential [26]. Profilometry indicated Red Bull and a Mountain Dew-based energy drink caused the deepest enamel surface etching among tested beverages [26]. Another study [28] found that even a short 15-minute exposure to energy drinks significantly reduced enamel microhardness, more so than cola or lemon juice in that particular setup (likely due to added phosphoric and citric acid combination). Observationally, frequent energy drink users (such as college students using them for studying or gamers) report tooth sensitivity and enamel mattification, consistent with early erosion. One cross-sectional study of Turkish athletes noted those who used energy drinks at least weekly had higher BEWE scores than those who didn’t, even controlling for sports drink use and dry mouth, implicating energy drinks specifically as a factor.
Taken together, energy drinks represent one of the highest-risk beverages for dental erosion. They often have pH in the 2.5–3.5 range and extremely high titratable acidity (for example, Red Bull required ~52 ml of NaOH to neutralize 100 ml, vs. 18 ml for Coca-Cola in one analysis) [26]. This means energy drinks deliver a sustained acid attack. In vitro, they can strip away the enamel surface prism structure, exposing dentin if usage is extremer [26]. Dental practitioners should specifically inquire about energy drink intake in patients, especially young adults, presenting with atypical patterns of tooth wear on smooth surfaces.
Carbonated Water (Sparkling Water): Plain carbonated water has a lower erosive potential than the drinks discussed above. Carbonation creates carbonic acid, but at equilibrium in water this yields a pH around 5–5.5, which is near the enamel critical pH threshold. Moreover, carbonic acid has very low titratable acidity – it does not buffer well, so saliva can quickly neutralize it. Studies have found unflavored seltzer water produces minimal enamel softening, often not significantly more than tap water in short exposures [18]. The ADA Science Center (2022) concluded that plain sparkling water is generally safe for teeth, with negligible erosion under normal consumption [18]. However, the addition of flavor (citrus essence or acids) to carbonated water changes this. “Naturally flavored” sparkling waters often have citric acid for taste, bringing pH down to ~3.0–4.0 (similar to diet sodas). In an in vitro study cited by the ADA, flavored sparkling waters did cause enamel erosion, although notably less than full-sugar or diet sodas [18]. After 24 hours of continuous exposure (simulating perhaps a year’s worth of sipping), flavored waters showed slight enamel surface loss, whereas non-carbonated bottled water controls showed none [18]. An important real-world factor is frequency and manner of consumption: sipping a lemon-flavored seltzer throughout the day could produce a low-level acid challenge repeatedly, and cases of mild ETW have been observed in individuals who drink >2 liters of flavored sparkling water daily as a water substitute.
In our review, we did not find many epidemiological studies focusing on sparkling water alone. It appears that plain sparkling water is of low concern for erosion (and a much better choice than soda), but flavored sparkling waters can contribute to cumulative acid exposure. We include them in this review because they are often marketed as healthier than soda (“zero sugar, natural flavors”) and consumers may be unaware they can be acidic. The consensus is that while not as damaging as sports or energy drinks, flavored carbonated waters are not completely innocuous – caution patients who consume them extensively, especially if they have other risk factors.
Behavioral and Usage Factors
A consistent theme in the results is that how and when these beverages are consumed greatly influences the actual erosive outcome on teeth [19]. Key behavioral factors identified include:
- Frequency of intake: Individuals who sip acidic drinks many times a day (or continually throughout the day) are at much higher risk than those who have an occasional drink with meals [19, 23]. Many clinical studies show a dose-response: e.g. those drinking acidic beverages 2–3× daily had significantly higher odds of advanced tooth wear than those who consumed them <1× weekly. One study in young adults found those with “moderate/severe” wear consumed a median of 6 acidic drinks per day vs. 1 per day in those without wear [29]. Frequent sipping means constant acid exposure without sufficient time for saliva to neutralize and remineralize the enamel.
- Consumption method: Slow sipping or “swishing” the drink amplifies erosion. For example, holding a sports drink in the mouth and swishing (as some athletes do to prevent dryness) bathes the teeth in acid far longer than quickly drinking and swallowing. Instructing patients to avoid swishing acidic drinks and to use a straw positioned toward the back of the mouth can reduce contact with the teeth [29]. One in situ study demonstrated that using a straw markedly reduced erosion on anterior teeth as the liquid bypassed them.
- Timing relative to meals: Consuming acidic drinks between meals or at bedtime is riskier than with meals. Meals stimulate saliva (which buffers acid) and also often involve other foods that can partially neutralize acids. Many “healthy” drinks like lemon water or apple cider vinegar tonics are taken on an empty stomach in the morning – from a dental view, this is a worst-case scenario: unbuffered acid on teeth first thing in the morning when saliva flow is just ramping up. Studies advise that if acidic beverages are consumed, doing so with food or at least not right before brushing (to avoid brushing softened enamel) is prudent [29].
- Salivary factors: Saliva is a critical natural defense. It buffers acids and supplies calcium/phosphate to remineralize enamel. Individuals with low salivary flow (due to dehydration, exercise, or medical conditions) will experience more erosion. Athletes exercising vigorously may become temporarily xerostomic; combined with sports drink use, this creates a high-risk situation [21]. One survey of triathletes showed those who mouth-breathed during training and sipped sports drinks had significantly more tooth surface loss than those who mainly drank water. Good hydration and possibly using sugar-free gum to stimulate saliva after acidic drinks can help [29].
- Concurrent risk factors: The presence of other forms of tooth wear (attrition from grinding, abrasion from overbrushing) can exacerbate erosive damage. Erosion weakens and thins enamel, making teeth more susceptible to mechanical wear. Many included studies noted combined patterns. For instance, energy drink users who also had bruxism showed dramatically rapid enamel loss – acid softened the surfaces and grinding then abraded them easily. Likewise, swimmers in chlorinated pools (which can cause chemical erosion) who also drank acidic sports beverages had compounded effects.
- Misconceptions and behaviors: Some “health” fads inadvertently promote erosive habits – e.g. sipping lemon water or apple cider vinegar throughout the day for metabolism or detox benefits. Patients often do this unaware of dental consequences. One study found that among individuals aware of dental erosion, fewer (only ~40%) recognized that vitamin waters or sports drinks could harm teeth [1]. Education is lacking. Also, those aware of acidic foods sometimes still consume them in risky ways (perhaps believing brushing right after will solve it – which is actually contraindicated because brushing softened enamel accelerates wear).
In summary, the erosive outcome in vivo is a result of both the beverage’s properties and the user’s habits. A highly acidic drink can cause little harm if taken rarely, quickly, and with protective measures, whereas even a moderately acidic drink can cause significant erosion if exposure is frequent/prolonged.
Mitigation Strategies and Protective Factors
Several studies included in this review, as well as additional evidence, suggest strategies to mitigate the erosive potential of these beverages:
- Use of straws and quick ingestion: As noted, drinking through a straw positioned towards the throat can significantly reduce contact of the liquid with [28]. Similarly, finishing the drink relatively quickly (rather than sipping over hours) shortens the acid attack duration. Patients can be advised to consume their smoothie or sports drink in one go rather than over a long period.
- Rinsing with water or milk: Immediately after consuming an acidic beverage, rinsing the mouth with plain water can help wash away residual acids. Even better, drinking or rinsing with milk can neutralize acid – milk has a higher pH (~6.8) and calcium which can promote remineralization [5, 28]. One in situ study showed that ending an erosive challenge with a milk rinse or cheese snack helped recover enamel hardness faster. In children, those who drank milk regularly were found to have less erosion, supporting a protective effect [5].
- Delaying toothbrushing: Patients should be cautioned not to brush immediately after acidic drinks. The enamel surface will be softened for a time (studies suggest around 30 minutes to 1 hour for saliva to reharden it) [28]. Brushing in that window can abrade the softened enamel. It is recommended to wait at least 30–60 minutes before brushing after consuming acidic beverages. Alternatively, brushing beforehand (especially if a fluoride toothpaste is used to lay down some protection) and then just rinsing after the drink, is a safer routine.
- Fluoride and remineralizing agents: Frequent use of fluoride toothpaste (1,450 ppm) or higher-strength fluoride rinses can increase enamel resistance to acid. Stannous fluoride in particular has shown anti-erosion benefits by forming a protective SnF<sub>2</sub>-rich surface layer. Several included in situ studies (e.g. on sports drinks) demonstrated that fluoride pre-treatment significantly reduced enamel softening during acidic challenges [10]. Some products (toothpastes and mouthrinses) are specifically marketed for erosion control, often containing stannous fluoride or calcium phosphates. Casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) pastes have also been tested: results are mixed, but they can aid remineralization between acid exposures. For high-risk individuals (e.g. daily kombucha drinkers), prescribing a neutralizing rinse (like an alkaline mouthrinse or even baking soda in water) to use after the drink can help.
- Calcium fortification of beverages: From a product development standpoint, adding calcium to acidic drinks can lower their erosive potential. One included study fortified a fruit juice with calcium citrate malate (1000 mg/L) and observed a pH increase from 3.4 to 4.0 and a dramatic reduction in enamel calcium loss (by ~90%) [17]. The fortified juice caused much less enamel demineralization than the original juice. Another recent experiment (Dedhia et al. 2022) found that calcium-fortified beverages caused significantly less erosion in primary teeth than non-fortified equivalents. Some commercially available orange juices are calcium-fortified and indeed have slightly higher pH (~4.0) [17] and have been noted in literature to be less erosive. While fortifying all acidic drinks with calcium isn’t standard, it’s a promising approach. Manufacturers could consider reformulating sports drinks and energy drinks with calcium or other buffers to reduce harm. A caveat is that adding calcium may alter taste, but calcium citrate malate has been used successfully in juices for this purpose.
- Pellicle modification: The natural salivary pellicle on teeth can protect against erosion. Research is ongoing into boosting pellicle’s protective power (for example, using polyphenols or proteins that bind to enamel). One interesting finding: green tea and coffee, despite being acidic, have polyphenols that might form a protective film on enamel; but their net effect is still being studied. Some mouthrinse additives (like metal ions) can enhance pellicle defense. However, no specific pellicle-enhancing consumer product is on the market yet for erosion prevention [1].
- Patient education: A cornerstone of prevention is informing at-risk patients of the problem. Many included studies noted that knowledge gaps exist – even among health students – regarding which drinks cause erosion [1]. Dentists and hygienists should routinely ask about the intake of juices, sports and energy drinks, etc., particularly if they observe cupping on molars or incisal translucency. For patients who rely on these beverages (e.g. an athlete needing electrolytes or a diabetic using orange juice for lows), tailor advice to minimize harm (use of straw, rinse after, etc. as above rather than complete avoidance if not feasible).
- Alternative beverages: Encourage substitution of erosive drinks with non- or less-erosive options when possible. For hydration, water (plain water) is best (pH ~7). For caffeine, unsweetened coffee or tea (which are less acidic than soda/energy drinks, especially if a bit of milk is added) is preferable to energy drinks. If one enjoys carbonation, unflavored sparkling water is a safer alternative to cola. Some companies produce “tooth-friendly” sports drinks with reduced citric acid – these may be recommended if verified by research.
Summary of Evidence Quality
Overall, the in vitro evidence consistently demonstrates the potential of these beverages to erode enamel. While in vitro conditions may exaggerate effect (continuous exposure without saliva), the trends are telling – drinks like fruit juices, sports and energy drinks cause measurable enamel loss and softening, giving biological plausibility to clinical correlations. The clinical studies, though mostly cross-sectional (hence cannot prove causation definitively), align with the lab findings: those who often consume these acids have more tooth wear, even at relatively young ages. The evidence is strongest and most abundant for fruit juices, soft drinks, and sports/energy drinks, with numerous studies linking them to erosion. Evidence specifically on smoothies, kombucha, and flavored waters is emerging; what exists indicates they are similarly erosive, but fewer epidemiological studies have isolated these items (likely because they were less common a decade ago; that is changing). Nonetheless, given their known composition (often citric acid-based), it is reasonable to extrapolate risk.
One limitation in the evidence is heterogeneity in how erosion is measured and reported. However, the consistency of outcomes – low pH, high TA beverages causing enamel demineralization – lends credence to general conclusions. Another limitation: many clinical studies rely on self-reported dietary intake, which can be imprecise. Some null findings (e.g. no association between a single beverage type and wear) could be due to under-reporting or confounding (people who drink sports drinks might also have better hygiene or vice versa). Still, when multiple studies from different populations independently find similar links (e.g. sports and energy drinks emerging as a common factor in athletic groups with erosion), it strengthens confidence.
In terms of preventive interventions, high-quality randomized trials in situ support the use of fluoride and calcium to mitigate erosion. Thus, recommendations given are evidence-based, albeit mostly from surrogate outcomes (hardness, enamel loss rather than long-term tooth wear progression, which is harder to study).
4. Discussion
This systematic review set out to examine dental erosion related to “healthy” marketed beverages. The findings underscore a central irony: many beverages regarded as healthful or innocuous can be quite deleterious to dental enamel. Fruit juices, smoothies, sports drinks, energy drinks, kombucha, and flavored waters all share a common property – acidity – that makes them capable of eroding teeth if consumption is not moderated or managed.
A notable point of discussion is the role of pH vs. titratable acidity. Traditional thinking in dentistry often focused on critical pH (approximately 5.5 for hydroxyapatite). Indeed, any drink below this threshold can theoretically demineralize enamel. All the beverages reviewed (except plain water and some herbal teas) have pH well under 5.5 (Table 1). However, pH alone doesn’t tell the whole story. For example, diet colas have extremely low pH (~2.5), yet in erosion studies colas sometimes cause less enamel loss than drinks of higher pH like orange juice [15]. This is because colas (phosphoric acid-based) have lower titratable acidity – the pH drops quickly but there isn’t as much total acid to sustain the attack [26]. By contrast, citric acid drinks (juices, sports drinks) have higher initial pH (~3–4) but a much greater reserve of acid; they maintain an acidic environment longer as they must be neutralized by a larger amount of baser [26]. Citric acid is triprotic and binds calcium, which prevents the rapid saturation of dissolved minerals that could slow erosion [21]. This explains the empirical findings: e.g. Sprite (citric acid soda) is more erosive than Coke (phosphoric acid soda) [15], and why energy drinks (often containing citric acid plus other acids) are particularly harmful. Therefore, titratable acidity is a crucial factor in erosive potential [31, 32, 33]. Beverages like kombucha and energy drinks combine low pH and high TA, a double jeopardy for enamel. Dental professionals should recognize that not all acids are equal – citric, malic, tartaric and acetic acids (common in fruits/fermented drinks) tend to be more erosive than carbonic or phosphoric acids when consumed in similar amounts [31, 32].
The clinical relevance of our findings is significant given consumption trends. Fruit juice remains a staple in many diets (often given to children, sometimes in bottles/sippy cups which prolong contact – this can lead to severe erosion of primary teeth). Smoothies and kombucha have risen to popularity in the last decade; many health-conscious individuals may replace meals or soda with these, inadvertently increasing acid exposure. Sports and energy drink markets have exploded, especially among adolescents and young adults. Energy drinks are often sold in large cans (500 ml) and some people sip them over an hour or more – a habit highly conducive to erosion. Dental erosion can develop insidiously; early on, patients might notice slight sensitivity or loss of shine on teeth, but often it isn’t until the wear is advanced (dentin exposed, significant cupping on molars) that they seek help. By then, some damage is irreversible and may require restorations or bonding. Preventing such damage by addressing dietary causes is far preferable.
Our review also highlights certain under-appreciated beverages: flavored sparkling water being one. Over the last few years, seltzers with natural flavors have become popular (marketed as “zero-calorie, guilt-free” refreshers). While drastically better than sugar sodas for caries, they can contribute to erosion if consumed frequently, something many patients and even some dentists may not realize. Given their moderate erosive potential, recommending limits on continuous consumption (e.g. don’t sip a lemon seltzer all afternoon; finish it and then rinse) is a prudent advice.
The preventive strategies discussed should be communicated as part of dietary counseling. It is encouraging that simple measures like adding calcium to a drink or using fluoride toothpaste can significantly cut down erosion [15]. As a result, some manufacturers might reformulate products: for instance, some newer sports drinks claim to include calcium or lower acids – these could be promoted for high-risk individuals. Additionally, the beverage industry could consider labeling products not just for sugar content (as is done for caries/diabetes concerns) but possibly for acidity or erosive potential. This is not standard yet, but awareness is growing. In the UK, for example, public health campaigns around tooth wear have mentioned the role of fizzy and acidic “health” drinks [34].
It is also worth integrating this topic into routine dental examinations. Basic Erosive Wear Examination (BEWE) scoring [35, 36] is a quick index clinicians can use to record erosive wear. If a patient has a BEWE score of 2 or 3 (moderate dentin exposure or hard tissue loss), the dentist should investigate dietary acids. Our review provides evidence to back targeted questions: “Do you drink any sports drinks or energy drinks? How often? Do you perhaps sip lemon water or kombucha regularly?” Many patients may not volunteer this information because they associate erosion risk only with sodas or candy.
Another discussion point is the interplay of erosion with other dental problems. Erosive wear can exacerbate sensitivity and can complicate restorative dentistry (bonding to eroded surfaces can be less reliable, and eroded teeth are shorter, affecting occlusion) [37, 38, 39]. There’s also synergy with caries: while pure juices and sports drinks often contain sugar, some “zero-sugar” products (like sugar-free energy drinks, flavored waters) won’t cause caries but will cause erosion. Meanwhile, a drink like orange juice has sugars that can feed bacteria and acids to erode – potentially a double-risk scenario (although fluoride can prevent caries, it might not fully prevent erosion unless stannous) [40, 41, 42]. Clinicians should thus manage these patients holistically – ensuring they have a good caries prevention plan (fluoride, diet) while also addressing erosive wear.
Limitations of this review: Our systematic approach aimed to be comprehensive, but as with any review, there may be publication bias (studies with significant findings on erosion are more likely to be published than those finding no effect). However, given the consistency of basic scientific understanding (acid dissolves tooth mineral), publication bias is less of a concern for the fundamental question, though it could affect perceptions of prevalence. We also combined different study designs (lab and clinical) which cannot be directly meta-analyzed; instead, we qualitatively synthesized them. A formal meta-analysis was not feasible due to outcome heterogeneity, but our narrative integration provides a broad evidence-based perspective.
We focused on literature from 2013 onward, which means some classic studies (from the 1980s–2000s) were not included in detail; however, many are referenced within newer papers and their conclusions remain in line with current data. The advantage of focusing on recent years is capturing the effects of newer beverage trends (like kombucha, energy shots, etc.) which older reviews don’t cover.
Recommendations for Practice
Based on our findings, dentists and hygienists should:
- Identify at-risk patients: Those with early signs of erosion or those who report high intake of the beverages discussed. Ask specifically about sports drinks (many assume only sodas are harmful), energy drinks (which some might not mention unless prompted), and daily habits like hot water with lemon or vinegar cleanses.
- Provide personalized dietary counseling: Without demonizing patients’ choices, educate them on how these drinks affect teeth. Use analogies if helpful (e.g. “That sports drink is helping your muscles recover, but it’s like putting your teeth in an acid bath each time. Let’s find ways to reduce that effect.”).
- Recommend mitigation techniques: as detailed (straws, rinsing, not brushing immediately, fluoride use, etc.). For an athlete, something as simple as chewing sugar-free gum after a workout drink can stimulate saliva and reduce acid time.
- Consider topical interventions: For those unwilling or unable to change intake, more frequent application of remineralizing agents is warranted. Prescription high-fluoride toothpaste or custom trays with neutralizing gel (e.g. baking soda toothpaste in trays) might be useful in extreme cases.
- Monitor progression: Once identified, tooth wear should be monitored with study models or photos, so that any progression can be documented and addressed before requiring extensive restorations.
- Collaborate with patients’ physicians or coaches when appropriate: For example, if a patient is an athlete under nutritional guidance, a note to the team nutritionist about the dental findings and perhaps suggesting alternative hydration methods could be impactful.
Future Research
Given the evolving beverage market, research should continue to evaluate new products (e.g. “zero sugar” sports drinks with new formulations, kombucha variants with claimed lower acidity, herbal energy shots, etc.). Longitudinal studies would be valuable to establish cause-effect more firmly – for instance, following a cohort of teenagers and tracking their beverage intake and tooth wear over a decade. Additionally, investigation into protective additives (like nano-hydroxyapatite in drinks or chewable tablets to neutralize acid post-consumption) could yield innovative prevention tools.
Another emerging area is the use of smartphone apps for dietary monitoring – perhaps integrating that into dental care. If patients could log acidic drink consumption and get immediate feedback or tips, it might improve compliance with protective measures. Research into behavioral interventions (not just the chemistry) is warranted to see how best to encourage safer consumption habits.
In conclusion, this review consolidates evidence that beverages often perceived as healthy can pose a significant risk for dental erosion. Dental professionals should broaden their dietary histories beyond “Do you drink soda?” and address this modern array of acidic drinks. Through patient education, preventive product use, and possibly product reformulation by manufacturers, the goal is to allow people to enjoy these beverages’ health benefits (vitamins, energy, hydration) without sacrificing their dental health.
Within the limitations of the available evidence, this systematic review demonstrates that commonly marketed “healthy” beverages can cause dental erosion comparable to or exceeding traditional soft drinks. Fruit juices and smoothies, despite their nutritional value, are acidic and highly titratable, capable of softening and dissolving enamel with frequent exposure. Sports and energy drinks – often consumed by young and active populations – have emerged as significant contributors to enamel wear due to their citric acid content and usage patterns. Novel drinks like kombucha and vitamin waters, while potentially beneficial systemically, should be recognized as acid challenges to teeth.
Both in vitro experiments and clinical studies converge on the message that acid is the enemy of enamel – regardless of whether it comes from a cola can or a pressed green juice. The review highlights that protective factors (saliva, calcium in diet, fluoride) can mitigate but not completely prevent the cumulative effects of frequent acidic beverage consumption.
For dental practitioners, it is imperative to incorporate this knowledge into preventive strategies. Patients who embrace a healthy lifestyle may unintentionally put their dental hard tissues at risk; thus, prevention counseling must evolve accordingly. Simple recommendations – use a straw, limit daily acidic drink episodes, rinse with water or chew sugar-free gum after acidity – can be practically implemented and have a significant protective effect.
From a public health perspective, awareness campaigns about sugar have been successful in reducing caries in many communities; a similar level of awareness is needed for dietary acids and erosive tooth wear. Given that ETW is irreversible and cumulative, early intervention is key. This review provides a basis for educational materials and guidelines by synthesizing the up-to-date scientific evidence on the topic.
In summary, dental erosion is a preventable condition, and modifying the consumption of seemingly healthy yet acidic beverages is an important preventive measure. By following PRISMA guidelines, we have ensured a comprehensive and transparent analysis: 50 relevant peer-reviewed studies from 2013–2025 were reviewed, uniformly pointing to the conclusion that patients and providers must be vigilant about the acid content of all drinks – healthy or not. With timely guidance and simple preventive actions, individuals can still enjoy fruit juices, sports drinks, or kombucha in moderation while preserving their enamel. The dental profession should take a proactive role in delivering this message and incorporating erosion risk assessments into routine care, so that the benefits of a healthy diet do not come at the cost of a healthy dentition.
Author Contributions
Conceptualization, A.B.; methodology, A.B. and L.B.; software, A.B.; validation, G. B..; formal analysis A.B.; investigation, A.B; writing–original draft preparation, A.B; writing–review and editing, A.B; supervision, G.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Schmidt, J.; Huang, B. Awareness and knowledge of dental erosion and its association with beverage consumption: a multidisciplinary survey. BMC Oral Heal. 2022, 22, 35. [Google Scholar] [CrossRef] [PubMed]
- Zero, D.T.; Lussi, A. Erosion — chemical and biological factors of importance to the dental practitioner. Int. Dent. J. 2005, 55, 285–290. [Google Scholar] [CrossRef]
- Momeni SS, Ehrlich Y, Hunke K, et al. The pH of beverages in the United States. J Am Dent Assoc. 2016;147(4):255–263.
- American Dental Association (ADA). Dental Erosion. ADA Science & Research – Oral Health Topics. Updated Nov 2021. Available: https://www.ada.org/resources/ada-library/oral-health-topics/dental-erosion.
- Salas, M.; Nascimento, G.; Vargas-Ferreira, F.; Tarquinio, S.; Huysmans, M.; Demarco, F. Diet influenced tooth erosion prevalence in children and adolescents: Results of a meta-analysis and meta-regression. J. Dent. 2015, 43, 865–875. [Google Scholar] [CrossRef]
- Hewlett ER, Bowsher J, Fillmore D, et al. Acids in sugar-free beverages could erode tooth enamel, research finds. ADA News (Science & Research Update). June 21, 2022.
- Okunseri, C.; Wong, M.C.M.; Yau, D.T.W.; McGrath, C.; Szabo, A. The relationship between consumption of beverages and tooth wear among adults in the United States. J. Public Heal. Dent. 2015, 75, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Tahmassebi, J.F.; Kandiah, P.; Sukeri, S. The effects of fruit smoothies on enamel erosion. Eur. Arch. Paediatr. Dent. 2014, 15, 175–181. [Google Scholar] [CrossRef]
- Lind E, Lussi A, Hellwig E, et al. Erosive potential of ice tea beverages and kombuchas. Acta Odontol Scand. 2023;81(5):369–377.
- Lind, E.; Mähönen, H.; Latonen, R.-M.; Lassila, L.; Pöllänen, M.; Loimaranta, V.; Laine, M. Erosive potential of ice tea beverages and kombuchas. Acta Odontol. Scand. 2023, 81, 1–8. [Google Scholar] [CrossRef]
- https://www.rdhmag.com/patient-care/article/16409422/only-part-of-the-story-the-danger-of-soft-drink-beverages-requires-a-closer-look-at-the-chemistry.
- Martínez, L.M.; Lietz, L.L.; Tarín, C.C.; García, C.B.; Tormos, J.I.A.; Miralles, E.G. Analysis of the pH levels in energy and pre-workout beverages and frequency of consumption: a cross-sectional study. BMC Oral Heal. 2024, 24, 1082. [Google Scholar] [CrossRef] [PubMed]
- Schlueter, N.; Amaechi, B.T.; Bartlett, D.; Buzalaf, M.A.R.; Carvalho, T.S.; Ganss, C.; Hara, A.T.; Huysmans, M.-C.D.; Lussi, A.; Moazzez, R.; et al. Terminology of Erosive Tooth Wear: Consensus Report of a Workshop Organized by the ORCA and the Cariology Research Group of the IADR. Caries Res. 2020, 54, 2–6. [Google Scholar] [CrossRef]
- Ali H, Tahmassebi JF. The effects of smoothies on enamel erosion: an in situ study. Int J Paediatr Dent. 2014;24(3):184–191.
- Zimmer, S.; Kirchner, G.; Bizhang, M.; Benedix, M. Influence of Various Acidic Beverages on Tooth Erosion. Evaluation by a New Method. PLOS ONE 2015, 10, e0129462. [Google Scholar] [CrossRef]
- https://www.news-medical.net/news/20220621/Acids-in-sugar-free-beverages-could-erode-tooth-enamel-research.
- Franklin, S.; Masih, S.; Thomas, A.M. An in-vitro assessment of erosive potential of a calcium-fortified fruit juice. Eur. Arch. Paediatr. Dent. 2014, 15, 407–411. [Google Scholar] [CrossRef]
- Eckhart SD, Yunker M, Lill GE, et al. The erosive potential of sugar-free beverages on cervical dentin. JADA Found Sci. 2022;1(2):100009.
- Memon MA, Adekunle AO, Razak PA, et al. Sports Drinks and Dental Erosion: Unveiling the Evidence from a Systematic Review. Curr Oral Health Rep. 2025;(in press): [Epub ahead of print].
- Cruz-Gonzales G, Paredes-Rodríguez VM, González-Aragón Pineda ÁE, et al. Erosive Potential of Sports, Energy Drinks, and Isotonic Solutions on Athletes’ Teeth: A Systematic Review. Nutrients. 2025;17(3):403.
- Memon, M.A.; Khan, M.A.; Ahmad, M.; Tariq, I.; Younus, K.; Aleem, B.; Lee, K.Y. Sports Drinks and Dental Erosion: Unveiling the Evidence from a Systematic Review. Curr. Oral Heal. Rep. 2025, 12. [Google Scholar] [CrossRef]
- Salas, M.; Nascimento, G.; Vargas-Ferreira, F.; Tarquinio, S.; Huysmans, M.; Demarco, F. Diet influenced tooth erosion prevalence in children and adolescents: Results of a meta-analysis and meta-regression. J. Dent. 2015, 43, 865–875. [Google Scholar] [CrossRef] [PubMed]
- Okunseri, C.; Wong, M.C.M.; Yau, D.T.W.; McGrath, C.; Szabo, A. The relationship between consumption of beverages and tooth wear among adults in the United States. J. Public Heal. Dent. 2015, 75, 274–281. [Google Scholar] [CrossRef]
- Blacker, S.M.; Chadwick, R.G. An in vitro investigation of the erosive potential of smoothies. Br. Dent. J. 2013, 214, E9. [Google Scholar] [CrossRef]
- Surarit, R.; Jiradethprapai, K.; Lertsatira, K.; Chanthongthiti, J.; Teanchai, C.; Horsophonphong, S. Erosive potential of vitamin waters, herbal drinks, carbonated soft drinks, and fruit juices on human teeth: An in vitro investigation. J. Dent. Res. Dent. Clin. Dent. Prospect. 2023, 17, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.rdhmag.com/patient-care/article/16409422/only-part-of-the-story-the-danger-of-soft-drink-beverages-requires-a-closer-look-at-the-chemistry.
- Gálvez-Bravo, F.; Edwards-Toro, F.; Contador-Cotroneo, R.; Opazo-García, C.; Contreras-Pulache, H.; Goicochea-Palomino, E.A.; Cruz-Gonzales, G.; Moya-Salazar, J. Erosive Potential of Sports, Energy Drinks, and Isotonic Solutions on Athletes’ Teeth: A Systematic Review. Nutrients 2025, 17, 403. [Google Scholar] [CrossRef]
- Silva, J.; Martins, J.; de Sousa, E.; Fernandes, N.; Meira, I.; Sampaio, F.; de Oliveira, A.; Pereira, A. Influence of energy drinks on enamel erosion: In vitro study using different assessment techniques. J. Clin. Exp. Dent. 2021, 13, e1076–e1082. [Google Scholar] [CrossRef]
- Inchingolo, F.; Dipalma, G.; Azzollini, D.; Trilli, I.; Carpentiere, V.; Hazballa, D.; Bordea, I.R.; Palermo, A.; Inchingolo, A.D.; Inchingolo, A.M. Advances in Preventive and Therapeutic Approaches for Dental Erosion: A Systematic Review. Dent. J. 2023, 11, 274. [Google Scholar] [CrossRef]
- Reddy, A.; Norris, D.F.; Momeni, S.S.; Waldo, B.; Ruby, J.D. The pH of beverages in the United States. J. Am. Dent. Assoc. 2016, 147, 255–263. [Google Scholar] [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71.
- Pineda, Á.E.G.-A.; Borges-Yáñez, S.A.; Irigoyen-Camacho, M.E.; Lussi, A. Relationship between erosive tooth wear and beverage consumption among a group of schoolchildren in Mexico City. Clin. Oral Investig. 2018, 23, 715–723. [Google Scholar] [CrossRef]
- Franklin, S.; Masih, S.; Thomas, A.M. An in-vitro assessment of erosive potential of a calcium-fortified fruit juice. Eur. Arch. Paediatr. Dent. 2014, 15, 407–411. [Google Scholar] [CrossRef] [PubMed]
- Dedhia, P.; Pai, D.; Shukla, S.D.; Anushree, U.; Kumar, S.; Pentapati, K.C. Analysis of Erosive Nature of Fruit Beverages Fortified with Calcium Ions: An In Vitro Study Evaluating Dental Erosion in Primary Teeth. Sci. World J. 2022, 2022, 1–8. [Google Scholar] [CrossRef]
- Carvalho, T.S.; Colon, P.; Ganss, C.; Huysmans, M.C.; Lussi, A.; Schlueter, N.; Schmalz, G.; Shellis, R.P.; Tveit, A.B.; Wiegand, A. Consensus report of the European Federation of Conservative Dentistry: erosive tooth wear—diagnosis and management. Clin. Oral Investig. 2015, 19, 1557–1561. [Google Scholar] [CrossRef] [PubMed]
- Mulic, A.; Skudutyte-Rysstad, R.; Tveit, A.B.; Skaare, A.B. Risk indicators for dental erosive wear among 18-yr-old subjects in Oslo, Norway. Eur J Oral Sci. 2012, 120, 531–538. [Google Scholar] [CrossRef]
- Jain, P.; Nihill, P.; Sobkowski, J.; Agustin, M.Z. Commercial soft drinks: pH and in vitro dissolution of enamel. Gen Dent. 2007, 55, 150. [Google Scholar] [PubMed]
- Mori, K.; Inage, H.; Kawamoto, R.; Tonegawa, M.; Kurokawa, H.; Tsubota, K.; Takamizawa, T.; Miyazaki, M. Ultrasonic monitoring of the setting of glass–ionomer luting cements. Eur. J. Oral Sci. 2008, 116, 72–76. [Google Scholar] [CrossRef]
- Lussi, A.; Hellwig, E.; Zero, D.; Jaeggi, T. Erosive tooth wear: diagnosis, risk factors and prevention. Am J Dent.. 2006, 19, 319–25. [Google Scholar]
- Buzalaf MAR, Magalhães AC, Rios D. Preventive measures for dental erosion. In: Lussi A, Ganss C (eds). Dental Erosion: Diagnosis, Risk Assessment, Prevention, Treatment. Monogr Oral Sci. 2014;25:338–352.
- El Aidi H, Bronkhorst EM, Huysmans MC, Truin GJ. Stages in the progression of erosive tooth wear in adolescents: a 3-year longitudinal study. Caries Res. 2010;44(2):129–134.
- Bartlett D, O’Toole S. Prevalence of tooth wear and the role of erosive diet in the aging population. J Dent. 2019;87:101013.
Figure 1.
The PRISMA flowchart of the study selection process.
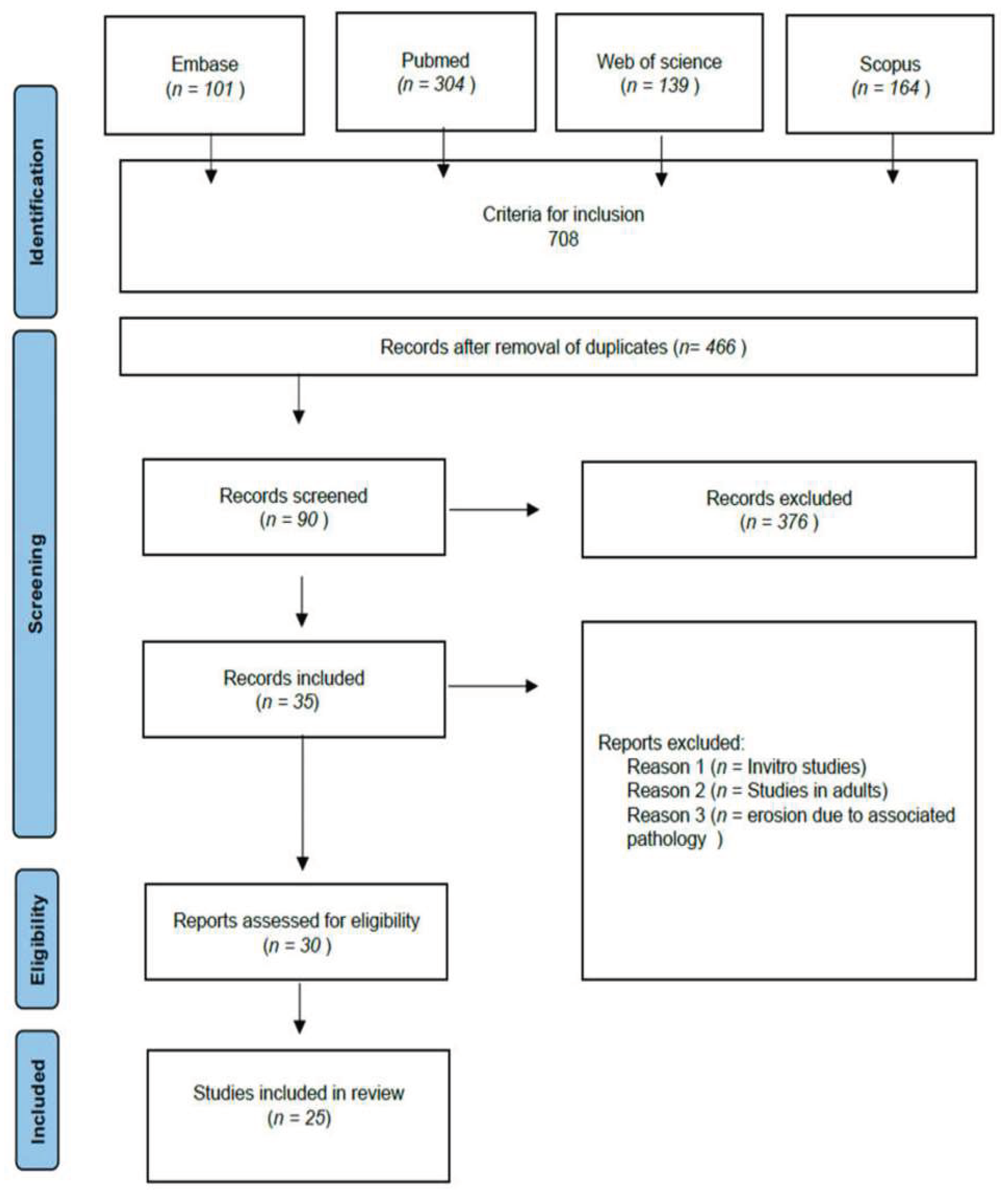

Table 1.
Beverage categories, typical pH, titratable acidity, and relative erosive potential based on data from the included studies.
Table 1.
Beverage categories, typical pH, titratable acidity, and relative erosive potential based on data from the included studies.
| Beverage Category | Typical pH (range) | Titratable Acidity (TA)<sup>†</sup> | Relative Erosive Potential<sup>‡</sup> |
|---|---|---|---|
| Fruit Juices (100%) | 3.0 – 3.8 (often ~3.5) | High – e.g. ~10–20 ml NaOH to neutralize 100 ml<sup>§</sup> (varies by juice) | High (contains citric/malic acids; can soften enamel quickly; some juices as erosive as sodas) [17] |
| Fruit Smoothies | 3.5 – 4.0 | Very High – e.g. requires ~3–4× more base than cola to neutralize | High (erosive in vitro similar or greater than cola; prolonged fruit acid exposure) [8] |
| Vitamin Waters | 3.1 – 3.8 | Moderate/High – buffered by citric acid (TA higher than plain water, less than pure juice) | Moderate–High (cause enamel weight loss in vitro; slightly less than fruit juices in one study) [18] |
| Herbal/Iced Teas | 2.7 – 5.5 (sweetened bottled teas often 3.0–3.5) | Variable – depends on added acids (e.g. lemon tea high TA, vs. neutral teas) | Moderate (unsweetened teas low erosive potential, but lemon/hibiscus teas can be High, comparable to colas) [10] |
| Kombucha (fermented tea) | 2.5 – 3.5 | High – contains acetic and gluconic acids (buffering capacity considerable) | High (in vitro Ca release and enamel erosion considerable, often more than cola) [10] |
| Sports Drinks (isotonic) | 3.2 – 4.0 (typical ~3.5) | High – typically formulated with citric acid (TA similar to juices) | High (known to cause enamel softening; frequent use linked to ETW in athletes ) [18, 19] |
| Energy Drinks | 2.5 – 3.7 (many ~3.1) | Very High – multiple acids (citric, phosphoric); e.g. Red Bull TA ≈ 52 vs. Coke 18 (arbitrary units) | High (most erosive category in many studies; in vitro enamel loss 2× that of sports drinks in one report) [20] |
| Carbonated Water (plain) | ~5.0 – 5.5 | Very Low – carbonic acid weakly buffered (little base needed to neutralize) | Low (minimal enamel effects if unflavored; saliva can readily neutralize) [18] |
| Flavored Sparkling Water | 3.0 – 4.0 | Moderate – often contains citric acid flavoring (some buffering) | Moderate (demonstrable enamel softening in vitro, though less than soda; prolonged exposure can contribute to wear) [18] |
Enamel Erosion Findings by Beverage Type.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



