
Submitted:
09 May 2025
Posted:
13 May 2025
You are already at the latest version
Abstract
Malignancies of the female upper reproductive tract, especially endometrial and ovarian cancers, consist a significant burden for women worldwide. The possible etiopathogenetic role of chronic human papillomavirus (HPV) infection in the female upper genital tract carcinogenesis is neither clearly established not completely understood. Therefore, we performed a literature review through PubMed and SCOPUS electronic databases about the prevalence of HPV DNA in endometrial, primary fallopian tube, ovarian and primary peritoneal cancers, as well as uterine sarcomas. The present investigation covered 35 studies from different countries of various continents. Overall, HPV prevalence was approximately 15% in all the above cancers. HPV DNA was isolated from 11%, 0%, 0% and 14% of endometrial carcinomas, uterine sarcomas, primary fallopian tube cancers and ovarian malignant neoplasms, respectively. No relevant studies on primary peritoneal cancers were retrieved. The predominant HPV strain from all tumors of the upper female reproductive tract, regardless of the tumor site, was mostly HPV-16, followed by HPV-18. HPV DNA was identified exclusively from subtypes HPV-6, HPV-11, HPV-16, HPV-18, and HPV-33, which are responsible for the development of not only cervical cancer, but also of condylomata acuminata. The findings of the present review indicate that HPV vaccination might prove to be a useful strategy in the prevention HPV-related carcinomas of the upper genital tract in women.
Keywords:
human papillomavirus
; endometrial cancer
; uterine corpus cancer
; uterine sarcoma
; fallopian tube cancer
; ovarian cancer
; primary peritoneal cancer
1. Introduction
The female upper reproductive tract consists of the cervix, uterus, fallopian tubes and ovaries[1]. Malignant transformation in these structures could occur on each of the above sites, leading to the development of cancer, i.e. cancer of the cervix uteri[2], cancer of the corpus uteri[3], uterine sarcoma[4], primary fallopian tube cancer, ovarian cancer, and primary peritoneal cancer[5], respectively. The global burden of these diseases is significantly high. According to the Global Cancer Observatory (GLOBOCAN) of the International Agency for Research on Cancer (IARC) of the World Health Organization (WHO), a total of 662,301 new cervix uteri cancer cases were newly diagnosed in 2022, and a total of 348,874 deaths were attributed to this malignancy, whereas the global incidence and mortality of corpus uteri cancer in 2022 was 420,368 new cases and 97,723 deaths, respectively. Regarding ovarian cancer, 324,603 new cases were diagnosed in 2022 and 206,956 women died of the disease the same year, respectively[6].
The role of chronic human papillomavirus (HPV) infection in the development of cervical cancer has been strongly proven and clearly established since more than two decades ago. A seminal study published in 1999 from The Netherlands by Walboomers et al., demonstrated that high-risk HPV DNA could be detected in nearly all (approximately 99.7%) cervical cancer cases worldwide, thus establishing HPV as a necessary cause of invasive cervical cancer[7]. Moreover, it was also later the same year when German virologist Harald zur Hausen published a comprehensive review of the evidence linking HPV infection to cervical carcinogenesis. zur Hausen's pioneering work in the field laid the groundwork for future research, confirming the causal role of HPV in cervical cancer development[8]. Although HPV DNA has even been isolated from cancerous tissues of human body sites which are neither directly nor obviously linked to sexual intercourse, such as lungs (non-small cell lung cancer, NSCLC)[9] and brain (glioblastoma multiforme, GBM)[10], the possible detrimental contribution of HPV infection to the tumorigenesis in the female upper genital tract at an anatomical level higher than the cervix uteri still remains controversial, as the current published literature is divergent[11,12].
The aim of this comprehensive review is to address the prevalence of HPV DNA isolated from malignant neoplasms of the uterus, fallopian tubes, ovaries and peritoneum and attempt to correlate the presence of the HPV strains identified in these sites with the histopathology of the above malignancies, according to data obtained from individual studies.
2. Materials and Methods
This is a comprehensive review of the literature aiming to summarize the current evidence regarding the prevalence of HPV DNA isolation from malignant tumors of the female upper reproductive tract, excluding cervix uteri, i.e. epithelial and mesenchymal tumors of the corpus uteri, fallopian tube tumors, ovarian tumors and primary peritoneal tumors[13]. The present review was conducted following the preferred reporting items for systematic reviews and meta-analysis (PRISMA) recommendations[14].
2.1. Data Sources and Search Strategy
A search of the literature was conducted on 22 April 2025 through PubMed and SCOPUS electronic databases and designed using the “Systematic Review Accelerator”[15]. The literature search was performed regarding the period from 1 January 1985 to 22 April 2025 for finally published, full-text English journal articles including human adult female individuals of >19 years of age. The searching strategy was formed by combining appropriate MeSH terms and keywords, with the help of the Boolean operators “OR” and “AND”. The reference lists of pertinent articles were further manually searched for potentially eligible results. The “Related Citations” tool in PubMed was also applied whenever a suitable article was included. Table 1 presents the exact search string for each database and each cancer site.
2.2. Eligibility Criteria
The inclusion criteria were: i) prospective and retrospective randomized control trials (RCTs), cohort studies, case–control, case series and case report studies, ii) human female adult patients aged >19 years histologically diagnosed with upper female reproductive tract cancer, irrespective to tumor stage, grade and histologic type; iii) HPV DNA extracted from the tumors and detected by polymerase chain reaction (PCR).
2.3. Exclusion Criteria
The exclusion criteria were: i) books or book chapters, conference abstracts, theses, press articles, expert reviews, narrative reviews, systematic reviews and meta-analyses, medical hypotheses; ii) animal studies, in vitro studies, abstract- or protocol-only publications and video reports; iii) non-English articles and published abstracts without full-text manuscripts; iv) presence of concomitant disease site(s) with precancerous or cancerous lesions; iv) HPV genome extracted from samples other than upper female genital tract malignant tissues, such as blood; v) patients and/or non-patients with prior neoplasia, surgery for malignancy, radiation or cytotoxic therapy; vi) co-presence of other oncogenic viruses; and vii) HPV presence detected by methods other than PCR.
2.4. Study Screening and Selection Process
Two authors, CK and IL, independently selected the articles which fulfilled the inclusion criteria. Once the initial title and abstract screening was completed, the full texts of the included studies from that stage were reviewed by the aforementioned investigators to determine if they should be included. Discrepancies were resolved by consulting a third author, SP. The aforementioned stage was completed with the assistance of the automation tool “Systematic Review Accelerator”[15].
2.5. Data Extraction
Study characteristics and data outcomes from each study were recorded in a data extraction form. Data extraction was independently conducted by two researchers, CK and EAA. A third and a fourth researcher, CMS and GMS, were consulted to resolve disagreements through open discussion. The following data regarding study characteristics and outcomes were extracted from every included study: First author, publication year, type of study, malignant neoplasm(s) histopathologic type(s), HPV DNA positivity and HPV subtypes isolated from the tumors by PCR. The flowcharts of study selection for each malignancy site are presented in Figure 1, Figure 2, Figure 3, Figure 4 and Figure 5.
3. Results
An overview of all selected studies is presented in Table 2. A total of 35 articles, published from 1992 up to 2024, meet the eligibility criteria for the present comprehensive review. These consist of 8 case-control studies[16,17,18,19,20,21,22,23], 25 case series[11,12,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46] and 2 case reports[47,48]. HPV DNA has been isolated from 222 specimens out of 1,666 malignant neoplastic tissues (222/1,666; 13%). All 222 specimens originate exclusively from 101 endometrial and 189 ovarian carcinomas, as no HPV DNA has been isolated from uterine sarcomas, primary fallopian tube carcinomas, or primary peritoneal carcinomas. Although various commercially available kits capable of identifying DNA from several different HPV strains have been deployed for the isolation of viral DNA from the above tumors, HPV DNA was found only from subtypes HPV-6, HPV-11, HPV-16, HPV-18, and HPV-33. In general, the predominant HPV strain from all tumors of the upper female reproductive tract, regardless of the tumor site, was mostly HPV-16 (145/222; 65%), followed by HPV-18 (48/222; 22%).
3.1. Endometrial Cancer (EC)
The presence of HPV DNA in EC was examined in 24 studies, i.e. 5 case-control studies[16,17,18,19,22], 17 case series[24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,40,46] and 2 case reports[47,49], which included a total of 668 patients with EC. Endometrioid endometrial carcinomas were the most frequent histological type. Viral DNA was detected in 15 of 24 studies (62%), including 74 patients (74/668; 11%). HPV DNA positivity ranged from 0 to 100%. DNA from HPV-16 was isolated from 29 patients, which was the most common HPV subtype (29/74; 39%). The rest HPV strains detected were HPV-6, HPV-18, HPV-33, HPV-11 and HPV-31 in 20, 12, 8, 3 and 2 EC specimens, respectively.
3.2. Uterine Sarcomas
Only one leiomyosarcoma was identified from a case series published in 1994 by Koffa et al., from which no HPV DNA was isolated[40].
3.3. Primary Fallopian Tube Cancer (PFTC)
In a case series of 7 PFTCs published in 1996 by Runnebaum et al., no HPV DNA was identified in these relatively rare malignant neoplasms[39].
3.4. Ovarian Cancer (OC)
The presence of HPV DNA in OC was examined in 16 studies, i.e. 4 case-control studies[20,21,22,23] and 12 case series[11,12,24,32,33,36,40,41,42,43,44,45], which included 996 patients with OC in total, and confirmed in 13 of 16 studies (81%) and 148 patients (148/996; 15%). Ovarian serous adenocarcinomas were the most frequent histological type in both HPV DNA positive and negative ovarian malignant neoplasms, accounting for more than half of all cases (542/996; 54%). HPV DNA positivity ranged from 0 to 62%[45]. DNA from HPV-16 was isolated from 116 patients, which was the most common HPV subtype (116/148; 78%). The rest HPV strains detected were HPV-18 and HPV-33 in 26 and 1 OC specimens, respectively.
3.5. Primary Peritoneal Cancer (PPC)
A study by Gatalica et al. published in 2008 described a case of low-grade peritoneal mucinous carcinomatosis containing high-risk HPV sequences (HPV-16, 18, 31, 33, 35, 39, 51, 52, 56, 58, and 66)[50]. However, it did not pertain to the eligibility criteria and, thus, had to be excluded, because the HPV presence was not confirmed by PCR, but by in situ hybridization, without exact HPV genotyping. Therefore, our search retrieved no relevant results.
4. Discussion
4.1. General Considerations
Evidence from existing literature of the last forty years shows a very wide heterogeneity in the prevalence of HPV DNA isolation from malignant tissues of the upper female genital tract, ranging from 0[11] to 100%[38]. Of note, there are neither narrative nor systematic reviews focused exclusively on examining the potential role of HPVs to the development of uterine sarcomas, primary fallopian tube carcinomas, or primary peritoneal cancers, most probably due to the relative rarity of these malignant neoplasms in comparison to endometrial and ovarian cancer. The most frequently identified HPV subtype for all HPV DNA-positive malignancies studied was HPV-16, regardless of the geographical region from which the samples were collected, which comes in agreement with several meta-analyses published from different researchers in different years[51,52,53,54]. Geographical differences in the prevalence of HPV DNA might be attributed to geographical and biological interactions between HPV subtypes and the host immunogenetic factors, such as HLA (human leukocyte antigen), GST (glutathione-S-transferase), FAS (fatty acid synthase) gene promoter-670, MDM2 (Mouse double minute 2 homolog), and p53 codon 72 polymorphisms[55]. Moreover, HPV DNA prevalence can vary according to the tissue type (for example, frozen tissues versus formalin-fixed paraffin-embedded tissues, FFPE) and the detection method (for example, PCR versus in situ hybridization; PCR is considered as the most sensitive method in HPV detection[51]) used in each study among the included ones. In a meta-analysis from Denmark by Svahn et al. published in 2014, HPV prevalence was slightly higher in frozen tissues than FFPE tissues, but this difference was not statistically significant[51]. Paraffin-embedded tissues amplify DNA products less efficiently than fresh tissues, due to loss of DNA integrity, especially when fixation protocols including non-buffered formalin are implemented[51,54]. A long fixation time with formalin can be responsible for a cross-linking of nucleic acids and proteins, as well as random breaks in nucleotide sequences. Additionally, carryover contamination could occur if FFPE blocks were not strictly processed, thus leading to false positive results[54].
4.2. HPV and Endometrial Cancer
In the present review, endometrial cancer prevalence, regardless of type, was approximately 11%, ranging from 0% to 100%. Endometrioid EC was the most common histological type and HPV-16 was the most frequent HPV subtype. According to a systematic review and meta-analysis from Denmark published by Olesen et al. in 2014, including 1026 cases of EC in 29 studies, the HPV DNA prevalence varied from 0% to 61% and the pooled prevalence of HPV DNA was 10%. The majority (97%, n=761/1026) of endometrial carcinomas were Type 1 (endometrioid, endometrioid with squamous differentiation, villoglandular, secretory, ciliated cell and mucinous)[52].
An important aspect of HPV-related endometrial carcinogenesis involves the route of HPV transmission from the lower female genital tract to the upper female reproductive tract. The former includes the vagina and the ectocervix, is covered with multiple layers of stratified squamous epithelia and is often exposed to pathogens. The latter, which includes the uterus, endometrium and endocervix, consists of a single layer of columnar epithelium that maintains a relatively sterile environment, with intermittent ascending microorganisms from the lower female genital tract. The endocervix functions as an interface between the relatively sterile upper female reproductive tract and the non-sterile lower female genital tract. It is hypothesized that HPVs could ascend to the endometrium from the vagina and the ectocervix, through the endocervix, and infect the squamous epithelium in the endometrium also, in a similar fashion that HPV infects the basal cells of the squamous epithelium in the cervix[52].
4.3. HPV and Ovarian Cancer
The first report on HPV infection in OC was published in 1987 by Kaufmann et al., whose research team had used southern blot hybridization[55], and the first report of HPV-related primary ovarian squamous cell carcinoma was published by Mai et al. in 1996[56]. Thereafter, several reports have examined the HPV DNA prevalence in OC. In a meta-analysis by Svahn et al., HPV prevalence in ovarian carcinomas ranged from 2% to 67% and the pooled prevalence was approximately 16%. HPV-16, which was the most frequently isolated HPV subtype, was found in serous, mucinous and endometrioid ovarian malignant tissues[51]. Moreover, in a meta-analysis from Brazil published by Rosa et al. in 2013, 17.5% of OC cases reported HPV infection. HPV-16 was also the most common strain, followed by HPV-18. Only subtypes 6, 16, 18 and 33 were identified[53]. Furthermore, a more recent meta-analysis by Ibragimova et al., which included 14 studies with a total number of 1163 OC samples, revealed a low risk of OC development with HPV infection. The prevalence of HPV in OC averaged 22%, ranging from 0% to 90%[54]. Similar were the findings of a meta-analysis from Berlin, Germany by Cherif et al., which was published in the same year, and included 2280 cases of OC, in which the prevalence of detection ranged from 0% to 81% and the overall pooled prevalence of HPV was approximately 16%[55].
A variety of possible transmission pathways have been hypothesized for the detection of HPV DNA in ovarian malignant tissues, such as: i) an ascending infection from the lower genital tract-as the endometrium and oviducts are an anatomical continuation of the endocervix[53], ii) semen containing HPV DNA and spermatozoa in contaminated semen absorbing HPV DNA and transmitting it to ovarian tissues, or iii) lymphocytes transporting HPV to the ovaries. In each of the cases above, after the virus reaches the ovaries, the disruption of ovarian epithelium during ovulation, could facilitate ovarian HPV infection[51]. HPV prevalence is significantly higher in the squamous cell cervical tissues rather than the glandular tissues of the ovaries, thus indicating the possibly greater affinity of HPV for the former anatomical site[51]. Moreover, the cervical transformation zone (TZ) might be vulnerable to HPV infection, because the TZ consists of cuboidal epithelial cells, reserve cells, or potentially embryonal stem cells, which are possible targets of HPV, whereas similar target cells have not been described in the ovaries, thus somehow explaining the overall lower HPV DNA prevalence in OC compared to cervical cancer and “protecting” the ovaries from HPV DNA integration into the ovarian cells’ genome [55].
5. Limitations
The present comprehensive review implements a systematic way to retrieve as much evidence as possible published in the last four decades on the issue. However, it has several limitations. First, it does not include older studies published prior to 1992. Second, only two electronic databases (PubMed and SCOPUS) have been searched. Third, three of the included studies[23,40,44] do not clearly state which HPV subtype was isolated from the malignant tumors that were analyzed. Fourth, only 7 out of the 35 included studies were case-control studies. Therefore, it was not feasible to distinguish the possible differences between malignant neoplasms and healthy tissues serving as controls. Fifth, not all studies reported which HPV strains were detected in the malignant tumors by their histological type. Sixth, the samples of some of the included studies were obtained from fresh-frozen paraffin-embedded tissue block, while the samples from other included studies were collected from fresh tissues. Seventh, possible contamination from the cervix of examined malignant tissues could not be totally excluded in every included study, especially in cases where no HPV detection isolated from the cervix has been carried out. Eighth, it was the possible presence of HPV DNA and not of HPV mRNA that was performed in the included studies. HPV mRNA marks transcriptionally-active HPV infection[57], while HPV DNA shows the mere presence of the virus. Ninth, no studies for primary peritoneal cancer have been included in the present review. Last, but not least, there are no information on HPV vaccination status of patients and/or controls, especially in newer included studies.
6. Implications for Practice and Future Research
HPV DNA isolation from the upper female genital tract varies widely among the published studies. Nevertheless, the presence of both high-risk and low-risk HPV subtypes in anatomical sites above the cervix implicates their potential role in the development of cancer at these sites. However, a more sensitive detection method, based on mRNA HPV oncogene expression instead of HPV DNA isolation, could compare viral oncogene expression in malignant tissue samples and adjacent healthy tissues, thus further clarifying the potential role of HPVs in upper female reproductive tract tumorigenesis. Moreover, there is no strong evidence whether HPV vaccines could lower the incidence of these malignant neoplasms. Not only prospective multicenter studies on the incidence of HPV DNA-positive malignant tumors in HPV-vaccinated versus HPV-unvaccinated women, but also retrospective studies with large samples on the prevalence of HPV vaccination in HPV DNA-positive malignancies of the upper female reproductive tract, could shed further light on the potentially protective role of HPV vaccines against carcinogenesis in the corpus uteri, adnexa and peritoneum.
7. Conclusions
The present comprehensive review demonstrated that HPV DNA can be found in both endometrial carcinomas and ovarian cancer cases. Highly oncogenic HPV-16 and HPV-18 were the most common HPV strains in the majority of the studies. Therefore, the necessity for HPV vaccination of both women and men remains imperative, so as a significant reduction in the incidence and burden of HPV-related malignancies of the upper female genital tract is achieved worldwide.
Author Contributions
C.K. and I.L. were major contributors in writing the manuscript contributed equally to this work. Conceptualization, C.K. and S.P.; methodology, S.P.; software, S.F.; validation, G.M.-S. and C.M.-S.; formal analysis, S.P.; investigation, C.K.; resources, E. A.-A.; data curation, E. A.-A.; writing—original draft preparation, C.K.; writing—review and editing, I.L.; visualization, E.K.; supervision, K.D.; project administration, K.D.. The submitted manuscript has been read and approved for submission by all named authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
All authors have nothing to acknowledge.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DNA | Deoxyribonucleic Acid |
| EC | Endometrial Cancer |
| FAS | Fatty Acid Synthase |
| FFPE | Formalin-Fixed, Paraffin-Embedded |
| GBM | Glioblastoma Multiforme |
| GLOBOCAN | Global Cancer Observatory |
| GST | Glutathione S-Transferase |
| HLA | Human Leukocyte Antigen |
| HPV | Human Papillomavirus |
| IARC | International Agency for Research on Cancer |
| MDM2 | Mouse Double Minute 2 homolog |
| mRNA | Messenger Ribonucleic Acid |
| NSCLC | Non-Small Cell Lung Cancer |
| OC | Ovarian Cancer |
| PCR | Polymerase Chain Reaction |
| PFTC | Primary Fallopian Tube Carcinoma |
| PPC | Primary Peritoneal Carcinoma |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCT | Randomized Controlled Trial |
| TZ | Transformation Zone |
| WHO | World Health Organization |
References
- Patel, S.K.; Valicherla, G.R.; Micklo, A.C.; Rohan, L.C. Drug Delivery Strategies for Management of Women’s Health Issues in the Upper Genital Tract. Adv Drug Deliv Rev 2021, 177, 113955. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the Cervix Uteri: 2021 Update. International Journal of Gynecology & Obstetrics 2021, 155, 28–44. [Google Scholar] [CrossRef]
- Koskas, M.; Amant, F.; Mirza, M.R.; Creutzberg, C.L. Cancer of the Corpus Uteri: 2021 Update. International Journal of Gynecology & Obstetrics 2021, 155, 45–60. [Google Scholar] [CrossRef]
- Mbatani, N.; Olawaiye, A.B.; Prat, J. Uterine Sarcomas. International Journal of Gynecology & Obstetrics 2018, 143, 51–58. [Google Scholar] [CrossRef]
- Berek, J.S.; Renz, M.; Kehoe, S.; Kumar, L.; Friedlander, M. Cancer of the Ovary, Fallopian Tube, and Peritoneum: 2021 Update. International Journal of Gynecology & Obstetrics 2021, 155, 61–85. [Google Scholar] [CrossRef]
- Filho, A.M.; Laversanne, M.; Ferlay, J.; Colombet, M.; Piñeros, M.; Znaor, A.; Parkin, D.M.; Soerjomataram, I.; Bray, F. The GLOBOCAN 2022 Cancer Estimates: Data Sources, Methods, and a Snapshot of the Cancer Burden Worldwide. Int J Cancer 2025, 156, 1336–1346. [Google Scholar] [CrossRef]
- Walboomers, J.M.; Jacobs, M. V; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K. V; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human Papillomavirus Is a Necessary Cause of Invasive Cervical Cancer Worldwide. J Pathol 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses in Human Cancers. Proc Assoc Am Physicians 1999, 111, 581–587. [Google Scholar] [CrossRef]
- Nachira, D.; Congedo, M.T.; D’Argento, E.; Meacci, E.; Evangelista, J.; Sassorossi, C.; Calabrese, G.; Nocera, A.; Kuzmych, K.; Santangelo, R.; et al. The Role of Human Papilloma Virus (HPV) in Primary Lung Cancer Development: State of the Art and Future Perspectives. Life 2024, 14. [Google Scholar] [CrossRef]
- Oyouni, A.A.A. Human Papillomavirus in Cancer: Infection, Disease Transmission, and Progress in Vaccines. J Infect Public Health 2023, 16, 626–631. [Google Scholar] [CrossRef]
- Ingerslev, K.; Hogdall, E.; Skovrider-Ruminski, W.; Schnack, T.H.; Karlsen, M.A.; Nedergaard, L.; Hogdall, C.; Blaakær, J. High-Risk HPV Is Not Associated with Epithelial Ovarian Cancer in a Caucasian Population. Infect Agent Cancer 2016, 11, 39. [Google Scholar] [CrossRef] [PubMed]
- Kisseljova, N.; Zhordania, K.; Fedorova, M.; Katargin, A.; Valeeva, A.; Pajanidi, J.; Pavlova, L.; Khvan, O.; Vinokurova, S. Detection of Human Papillomavirus Prevalence in Ovarian Cancer by Different Test Systems. Intervirology 2020, 62, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Mayr, D.; Schmoeckel, E.; Höhn, A.K.; Hiller, G.G.R.; Horn, L.-C. Aktuelle WHO-Klassifikation Des Weiblichen Genitale. Pathologe 2021, 42, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Syst Rev 2021, 10, 89. [Google Scholar] [CrossRef]
- Clark, J.; Glasziou, P.; Mar, C. Del; Bannach-Brown, A.; Stehlik, P.; Scott, A.M. A Full Systematic Review Was Completed in 2 Weeks Using Automation Tools: A Case Study. J Clin Epidemiol 2020, 121, 81–90. [Google Scholar] [CrossRef]
- Abu-Lubad, M.A.; Jarajreh, D.A.; Helaly, G.F.; Alzoubi, H.M.; Haddadin, W.J.; Dabobash, M.D.; Albataineh, E.M.; Aqel, A.A.; Alnawaiseh, N.A. Human Papillomavirus as an Independent Risk Factor of Invasive Cervical and Endometrial Carcinomas in Jordan. J Infect Public Health 2020, 13, 613–618. [Google Scholar] [CrossRef]
- Fedrizzi, E.N.; Villa, L.L.; De Souza, I. V; Sebastião, A.P.M.; Urbanetz, A.A.; De Carvalho, N.S. Does Human Papillomavirus Play a Role in Endometrial Carcinogenesis? International Journal of Gynecological Pathology 2009, 28, 322–327. [Google Scholar] [CrossRef]
- Karadayi, N.; Gecer, M.; Kayahan, S.; Yamuc, E.; Onak, N.K.; Korkmaz, T.; Yavuzer, D. Association between Human Papillomavirus and Endometrial Adenocarcinoma. Med Oncol 2013, 30, 597. [Google Scholar] [CrossRef]
- Plunkett, M.; Brestovac, B.; Thompson, J.; Sterrett, G.; Filion, P.; Smith, D.; Frost, F. The Value of HPV DNA Typing in the Distinction between Adenocarcinoma of Endocervical and Endometrial Origin. Pathology 2003, 35, 397–401. [Google Scholar] [CrossRef]
- Alavi, G.; Sharifi, N.; Sadeghian, A.; Rezaei, A.; Shidaee, H. Failure to Demonstrate the Role of High Risk Human Papilloma Virus in Epithelial Ovarian Cancer. 2012.
- Dadashi, M.; Eslami, G.; Faghihloo, E.; Pourmohammad, A.; Hosseini, J.; Taheripanah, R.; Arab-Mazar, Z. Detection of Human Papilloma Virus Type 16 in Epithelial Ovarian Tumors Samples. Arch Clin Infect Dis 2017, 12, 1–5. [Google Scholar] [CrossRef]
- Lai, C.H.; Hsueh, S.; Lin, C.Y.; Huang, M.Y.; You, G.B.; Chang, H.C.; Pao, C.C. Human Papillomavirus in Benign and Malignant Ovarian and Endometrial Tissues. Int J Gynecol Pathol 1992, 11, 210–215. [Google Scholar] [CrossRef]
- Mohamed, N.E.; Abdel Fattah, N.F.; Seadawy, M.G.; Lymona, A.M.; Nasr, S.S.; El Leithy, A.A.; Abdelwahed, F.M.; Nassar, A. The Clinical Importance of IFN-γ and Human Epididymis Protein 4 in Egyptian Patients with Epithelial Ovarian Cancer Combined with HPV Infection. Hum Immunol 2024, 85. [Google Scholar] [CrossRef]
- Anwar, K.; Nakakuki, K.; Imai, H.; Shiraishi, T.; Inuzuka, M. Infection of Human Papillomavirus (HPV) and P53 over-Expression in Human Female Genital Tract Carcinoma. JOURNAL-PAKISTAN MEDICAL ASSOCIATION 1996, 46, 220–224. [Google Scholar]
- O’Leary, J.J.; Landers, R.J.; Crowley, M.; Healy, I.; O’Donovan, M.; Healy, V.; Kealy, W.F.; Hogan, J.; Doyle, C.T. Human Papillomavirus and Mixed Epithelial Tumors of the Endometrium. Hum Pathol 1998, 29, 383–389. [Google Scholar] [CrossRef]
- Jiang, L.; Malpica, A.; Deavers, M.T.; Guo, M.; Villa, L.L.; Nuovo, G.; Merino, M.J.; Silva, E.G. Endometrial Endometrioid Adenocarcinoma of the Uterine Corpus Involving the Cervix: Some Cases Probably Represent Independent Primaries. International Journal of Gynecological Pathology 2010, 29, 146–156. [Google Scholar] [CrossRef]
- Bures, N.; Nelson, G.; Duan, Q.; Magliocco, A.; Demetrick, D.; Duggan, M.A. Primary Squamous Cell Carcinoma of the Endometrium: Clinicopathologic and Molecular Characteristics. Int J Gynecol Pathol 2013, 32, 566–575. [Google Scholar] [CrossRef]
- Fujita, M.; Shroyer, K.R.; Markham, N.E.; Inoue, M.; Iwamoto, S.; Kyo, S.; Enomoto, T. Association of Human Papillomavirus with Malignant and Premalignant Lesions of the Uterine Endometrium. Hum Pathol 1995, 26, 650–658. [Google Scholar] [CrossRef]
- Hachisuga, T.; Matsuo, N.; Iwasaka, T.; Sugimori, H.; Tsuneyoshi, M. Human Papilloma Virus and P53 Overexpression in Carcinomas of the Uterine Cervix, Lower Uterine Segment and Endometrium. Pathology 1996, 28, 28–31. [Google Scholar] [CrossRef]
- Giordano, G.; D’Adda, T.; Gnetti, L.; Froio, E.; Merisio, C.; Melpignano, M. Detection of Human Papillomavirus in Organs of Upper Genital Tract in Women with Cervical Cancer. International Journal of Gynecological Cancer 2006, 16, 1601–1607. [Google Scholar] [CrossRef]
- Hording, U.; Daugaard, S.; Visfeldt, J. Adenocarcinoma of the Cervix and Adenocarcinoma of the Endometrium: Distinction with PCR-Mediated Detection of HPV DNA. APMIS 1997, 105, 313–316. [Google Scholar] [CrossRef]
- Ip, S.M.; Wong, L.C.; Xu, C.M.; Cheung, A.N.Y.; Tsang, P.C.K.; Ngan, H.Y.S. Detection of Human Papillomavirus DNA in Malignant Lesions from Chinese Women with Carcinomas of the Upper Genital Tract. Gynecol Oncol 2002, 87, 104–111. [Google Scholar] [CrossRef]
- Lai, C.H.; Wang, C.Y.; Lin, C.Y.; Pao, C.C. Detection of Human Papillomavirus RNA in Ovarian and Endometrial Carcinomas by Reverse Transcription/Polymerase Chain Reaction. Gynecol Obstet Invest 1994, 38, 276–280. [Google Scholar] [CrossRef]
- Mariño-Enríquez, A.; González-Rocha, T.; Burgos, E.; Stolnicu, S.; Mendiola, M.; Nogales, F.F.; Hardisson, D. Transitional Cell Carcinoma of the Endometrium and Endometrial Carcinoma with Transitional Cell Differentiation: A Clinicopathologic Study of 5 Cases and Review of the Literature. Hum Pathol 2008, 39, 1606–1613. [Google Scholar] [CrossRef]
- Park, T.-W.; Zivanovic, O.; Theuerkauf, I.; Dürkop, B.; Hernando, J.J.; Simon, M.; Büttner, R.; Kuhn, W. The Diagnostic Utility of Human Papillomavirus-Testing in Combination with Immunohistochemistry in Advanced Gynaecologic Pelvic Tumours: A New Diagnostic Approach. Int J Oncol 2004, 24, 829–836. [Google Scholar] [CrossRef]
- Yang, H.-J.; Liu, V.W.S.; Tsang, P.C.K.; Yip, A.M.W.; Ng, T.-Y.; Cheung, A.N.Y.; Ngan, H.Y.S. Comparison of Human Papillomavirus DNA Levels in Gynecological Cancers: Implication for Cancer Development. Tumour Biol 2003, 24, 310–316. [Google Scholar] [CrossRef]
- Zielinski, G.D.; Snijders, P.J.F.; Rozendaal, L.; Daalmeijer, N.F.; Risse, E.K.J.; Voorhorst, F.J.; Jiwa, N.M.; van der Linden, H.C.; de Schipper, F.A.; Runsink, A.P.; et al. The Presence of High-Risk HPV Combined with Specific P53 and P16INK4a Expression Patterns Points to High-Risk HPV as the Main Causative Agent for Adenocarcinoma in Situ and Adenocarcinoma of the Cervix. J Pathol 2003, 201, 535–543. [Google Scholar] [CrossRef]
- Brewster, W.R.; Monk, B.J.; Burger, R.A.; Bergen, S.; Wilczynski, S.P. Does Human Papillomavirus Have a Role in Cancers of the Uterine Corpus? Gynecol Oncol 1999, 75, 51–54. [Google Scholar] [CrossRef]
- Runnebaum, I.B.; Köhler, T.; Stickeler, E.; Rosenthal, H.E.; Kieback, D.G.; Kreienberg, R. P53 Mutation Is Associated with High S-Phase Fraction in Primary Fallopian Tube Adenocarcinoma. Br J Cancer 1996, 74, 1157–1160. [Google Scholar] [CrossRef]
- Koffa, M.; Koumantakis, E.; Ergazaki, M.; Malamou-Mitsi, V.; Spandidos, D.A. Detection of Ras Gene Mutations and HPV in Lesions of the Human Female Reproductive Tract. Int J Oncol 1994, 5, 189–195. [Google Scholar] [CrossRef]
- Runnebaum, I.B.; Maier, S.; Tong, X.W.; Rosenthal, H.E.; Mobus, V.J.; Kieback, D.G.; Kreienberg, R. Human Papillomavirus Integration Is Not Associated with Advanced Epithelial Ovarian Cancer in German Patients. Cancer Epidemiology-Biomarkers and Prevention 1995, 4, 573–576. [Google Scholar]
- Chen, T.R.; Chan, P.J.; Seraj, I.M.; King, A. Absence of Human Papillomavirus E6-E7 Transforming Genes from HPV 16 and 18 in Malignant Ovarian Carcinoma. Gynecol Oncol 1999, 72, 180–182. [Google Scholar] [CrossRef]
- Hassan, Z.K.; Hafez, M.M.; Kamel, M.M.; Zekri, A.R.N. Human Papillomavirus Genotypes and Methylation of CADM1, PAX1, MAL and ADCYAP1 Genes in Epithelial Ovarian Cancer Patients. Asian Pacific Journal of Cancer Prevention 2017, 18, 169–176. [Google Scholar] [CrossRef]
- Yang, X.; You, Q.; Yao, G.; Geng, J.; Ma, R.; Meng, H. Evaluation of P16 in Epithelial Ovarian Cancer for a 10-Year Study in Northeast China: Significance of Hpv in Correlation with Pd-L1 Expression. Cancer Manag Res 2020, 12, 6747–6753. [Google Scholar] [CrossRef]
- Jarych, D.; Mikulski, D.; Wilczyński, M.; Wilczyński, J.R.; Kania, K.D.; Haręża, D.; Malinowski, A.; Perdas, E.; Nowak, M.; Paradowska, E. Differential MicroRNA Expression Analysis in Patients with HPV-Infected Ovarian Neoplasms. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Wong, W.S.; Wong, Y.F.; Tam, O.S.; Tam, J.S. Detection of Human Papilloma Virus (HPV) Infection in Paraffin-Embedded Tissues of Endometrial Carcinoma. Aust N Z J Obstet Gynaecol 1993, 33, 180–182. [Google Scholar] [CrossRef]
- Giordano, G.; D’Adda, T.; Merisio, C.; Gnetti, L. Primary Squamous Cell Carcinoma of the Endometrium: A Case Report with Immunohistochemical and Molecular Study. Gynecol Oncol 2005, 96, 876–879. [Google Scholar] [CrossRef]
- Kataoka, A.; Nishida, T.; Okina, H.; Tomioka, Y.; Hirai, N.; Sugiyama, T.; Yakushiji, M. Squamous Cell Carcinoma of the Endometrium with Human Papillomavirus Type 31. Kurume Med J 1997, 44, 67–69. [Google Scholar] [CrossRef]
- Kataoka, A.; Nishida, T.; Sugiyama, T.; Hori, K.; Honda, S.; Yakushiji, M. Squamous Cell Carcinoma of the Endometrium with Human Papillomavirus Type 31 and without Tumor Suppressor Gene P53 Mutation. Gynecol Oncol 1997, 65, 180–184. [Google Scholar] [CrossRef]
- Gatalica, Z.; Foster, J.M.; Loggie, B.W. Low Grade Peritoneal Mucinous Carcinomatosis Associated with Human Papilloma Virus Infection: Case Report. Croat Med J 2008, 49, 669–673. [Google Scholar] [CrossRef]
- Svahn, M.F.; Faber, M.T.; Christensen, J.; Norrild, B.; Kjaer, S.K. Prevalence of Human Papillomavirus in Epithelial Ovarian Cancer Tissue. A Meta-Analysis of Observational Studies. Acta Obstet Gynecol Scand 2014, 93, 6–19. [Google Scholar] [CrossRef]
- Olesen, T.B.; Svahn, M.F.; Faber, M.T.; Duun-Henriksen, A.K.; Junge, J.; Norrild, B.; Kjaer, S.K. Prevalence of Human Papillomavirus in Endometrial Cancer: A Systematic Review and Meta-Analysis. Gynecol Oncol 2014, 134, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Rosa, M.I.; Silva, G.D.; De Azedo Simões, P.W.T.; Souza, M. V; Panatto, A.P.R.; Simon, C.S.; Madeira, K.; Medeiros, L.R. The Prevalence of Human Papillomavirus in Ovarian Cancer : A Systematic Review. International Journal of Gynecological Cancer 2013, 23, 437–441. [Google Scholar] [CrossRef]
- Ibragimova, M.K.; Kokorina, E. V; Tsyganov, M.M.; Churuksaeva, O.N.; Litviakov, N. V Human Papillomavirus and Ovarian Cancer (Review of Literature and Meta-Analysis). Infection, Genetics and Evolution 2021, 95. [Google Scholar] [CrossRef]
- Cherif, S.; Amine, A.; Thies, S.; Taube, E.T.; Braicu, E.I.; Sehouli, J.; Kaufmann, A.M. Prevalence of Human Papillomavirus Detection in Ovarian Cancer: A Meta-Analysis. European Journal of Clinical Microbiology and Infectious Diseases 2021, 40, 1791–1802. [Google Scholar] [CrossRef]
- Verguts, J.; Amant, F.; Moerman, P.; Vergote, I. HPV Induced Ovarian Squamous Cell Carcinoma: Case Report and Review of the Literature. Arch Gynecol Obstet 2007, 276, 285–289. [Google Scholar] [CrossRef]
- Forslund, O.; Miriam Elfström, K.; Lamin, H.; Dillner, J. HPV-MRNA and HPV-DNA Detection in Samples Taken up to Seven Years before Severe Dysplasia of Cervix Uteri. Int J Cancer 2019, 144, 1073–1081. [Google Scholar] [CrossRef]
Figure 1.
Flowchart of study selection for endometrial cancer.
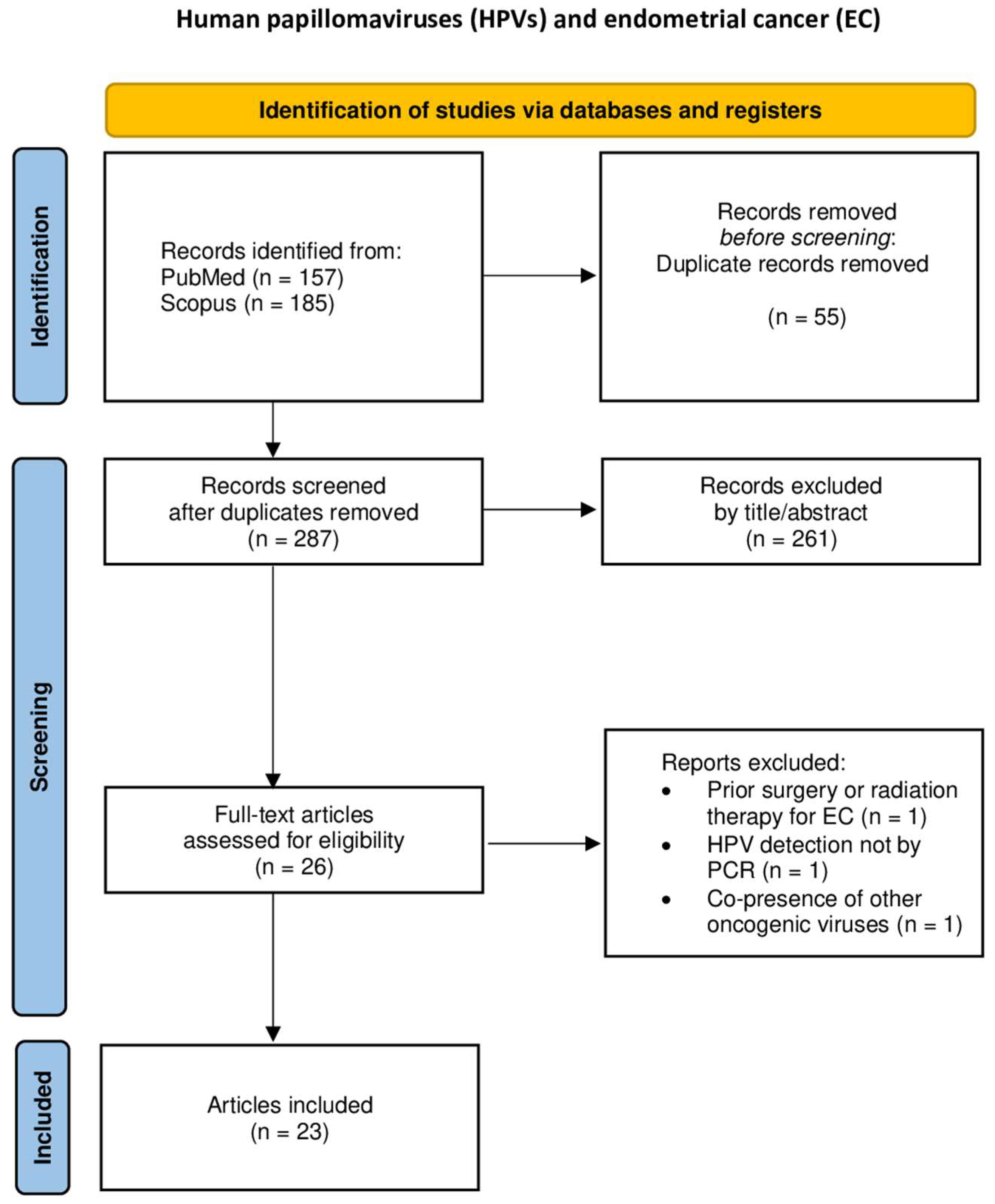
Figure 2.
Flowchart of study selection for uterine sarcoma
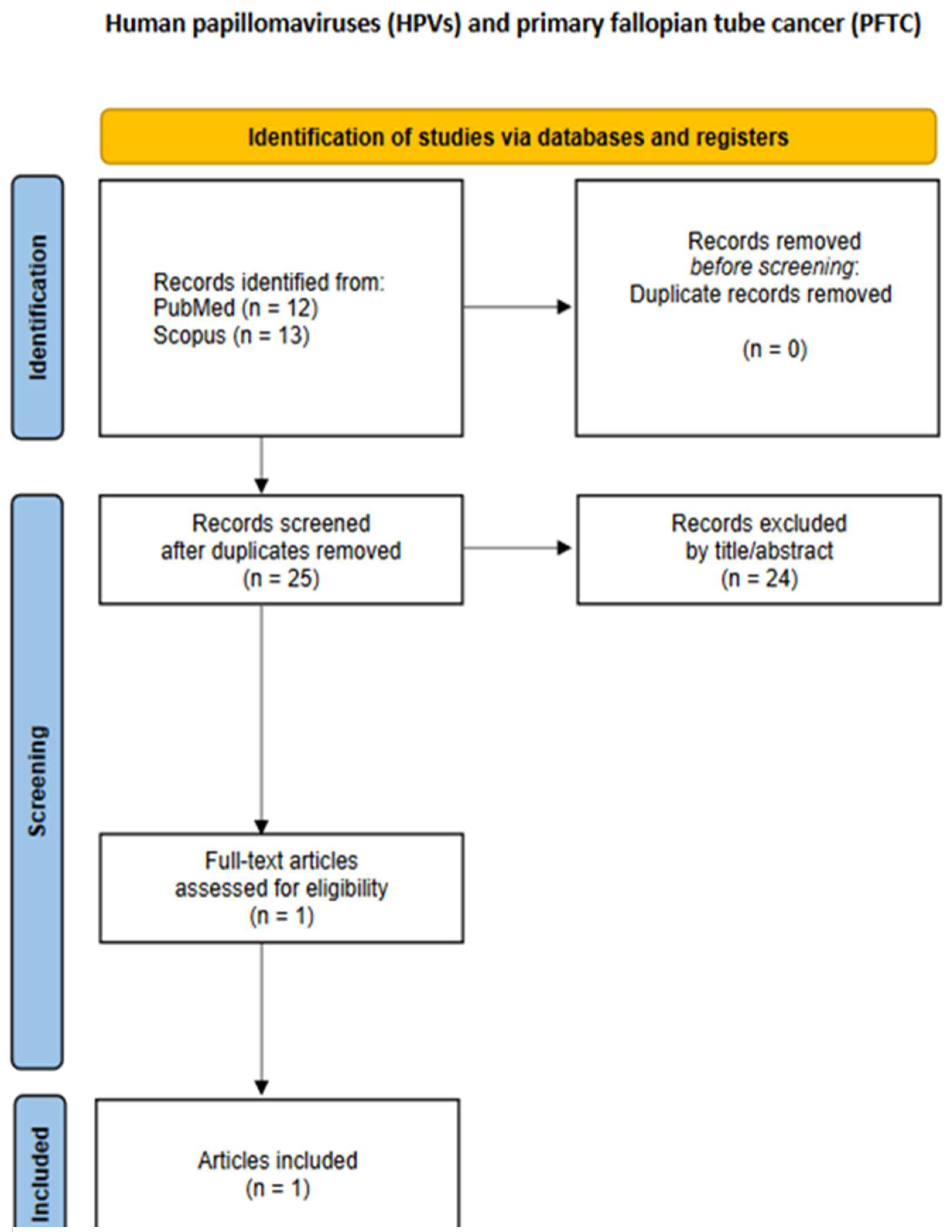
Figure 3.
Flowchart of study selection for primary fallopian tube cancer.
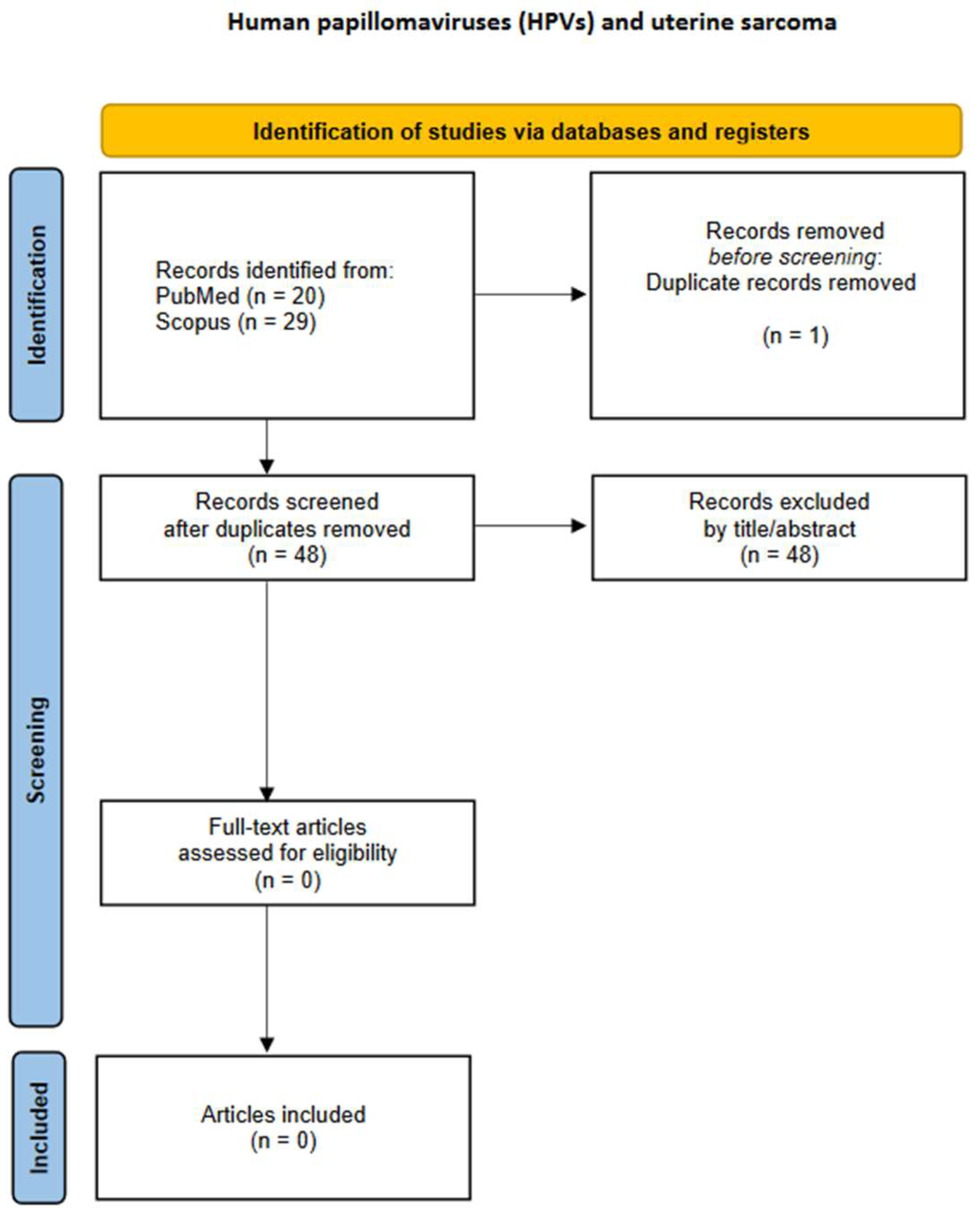
Figure 4.
Flowchart of study selection for ovarian cancer.

Figure 5.
Flowchart of study selection for primary peritoneal cancer.
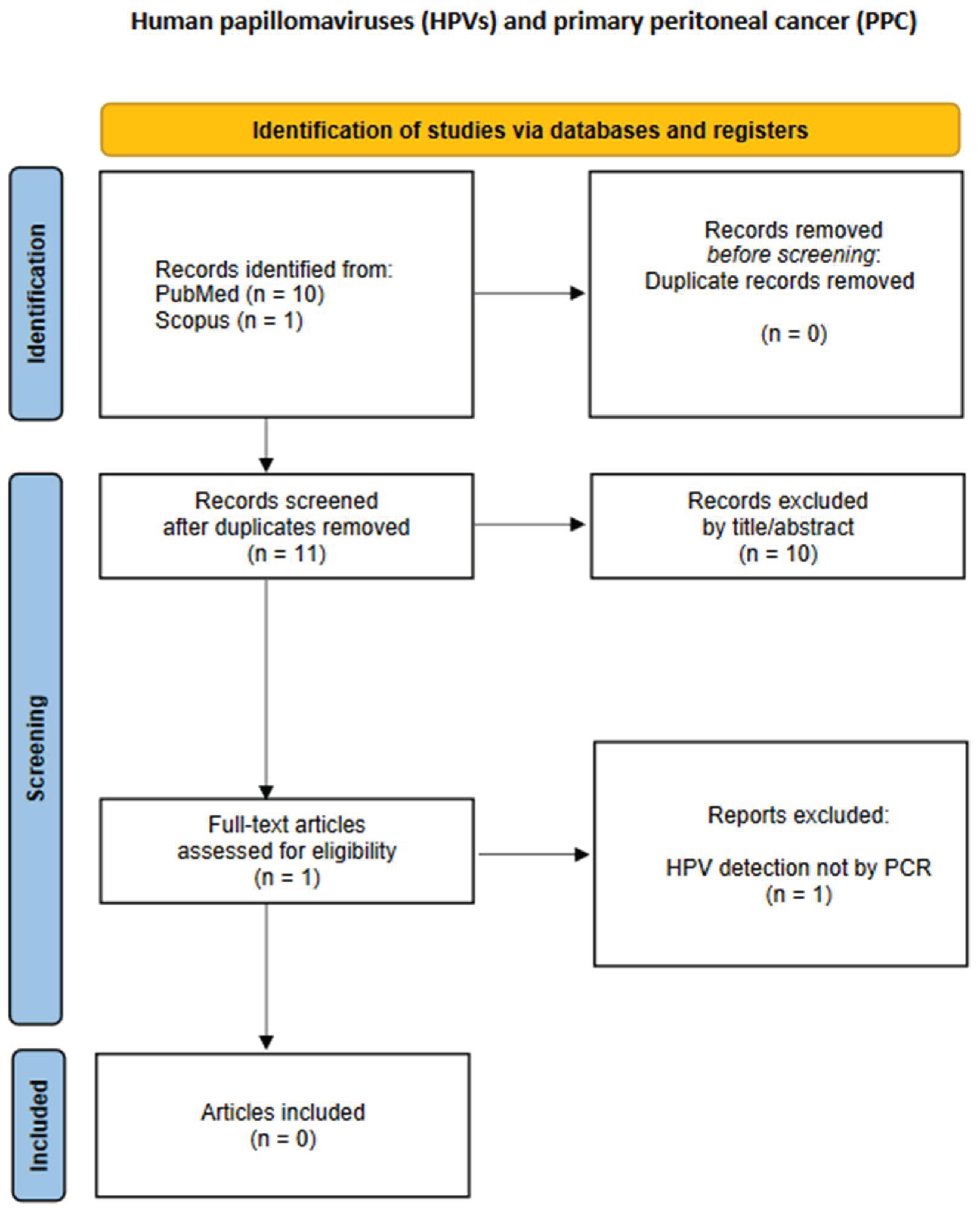

Table 1.
Electronic databases search string per cancer site.
| Malignancy site | PubMed | SCOPUS |
|---|---|---|
| Endometrial cancer | (("human papillomavirus viruses"[MeSH Terms] OR "human papillomavirus"[Title/Abstract] OR "HPV"[Title/Abstract]) AND ("endometrial neoplasms"[MeSH Terms] OR "endometrial neoplasms"[MeSH Terms] OR ("endometrial"[All Fields] AND "neoplasms"[MeSH Terms]) OR "endometrial cancer*"[Title/Abstract] OR "endometrial carcinoma*"[Title/Abstract] OR ("endometrial"[All Fields] AND "malignant neoplasm*"[Title/Abstract]) OR "endometrial ca"[Title/Abstract])) AND ((excludepreprints[Filter]) AND (fft[Filter]) AND (humans[Filter]) AND (female[Filter]) AND (1985/1/1:2025/1/1[pdat]) AND (english[Filter]) AND (alladult[Filter])) | (INDEXTERMS("human papillomavirus viruses") OR TITLE-ABS("human papillomavirus") OR TITLE-ABS(HPV)) AND (INDEXTERMS("endometrial neoplasms") OR INDEXTERMS("endometrial neoplasms") OR (ALL(endometrial) AND INDEXTERMS(neoplasms)) OR TITLE-ABS("endometrial cancer*") OR TITLE-ABS("endometrial carcinoma*") OR (ALL(endometrial) AND TITLE-ABS("malignant neoplasm*")) OR TITLE-ABS("endometrial ca")) AND PUBYEAR > 1985 AND PUBYEAR < 2026 AND ( LIMIT-TO ( DOCTYPE,"ar" ) ) AND ( LIMIT-TO ( PUBSTAGE,"final" ) ) AND ( LIMIT-TO ( SRCTYPE,"j" ) ) AND ( LIMIT-TO ( LANGUAGE,"English" ) ) |
| Uterine sarcoma | (("human papillomavirus viruses"[MeSH Terms] OR "human papillomavirus"[Title/Abstract] OR "HPV"[Title/Abstract]) AND ((("uterin"[All Fields] OR "uterines"[All Fields] OR "uterus"[MeSH Terms] OR "uterus"[All Fields] OR "uterine"[All Fields]) AND "sarcoma"[MeSH Terms]) OR "uterine sarcoma*"[Title/Abstract])) AND ((excludepreprints[Filter]) AND (fft[Filter]) AND (humans[Filter]) AND (female[Filter]) AND (1985/1/1:2025/1/1[pdat]) AND (english[Filter]) AND (alladult[Filter])) | (INDEXTERMS("human papillomavirus viruses") OR TITLE-ABS("human papillomavirus") OR TITLE-ABS(HPV)) AND (((ALL(uterin) OR ALL(uterines) OR INDEXTERMS(uterus) OR ALL(uterus) OR ALL(uterine)) AND INDEXTERMS(sarcoma)) OR TITLE-ABS("uterine sarcoma*")) AND PUBYEAR > 1984 AND PUBYEAR < 2026 AND ( LIMIT-TO ( DOCTYPE,"ar" ) ) AND ( LIMIT-TO ( PUBSTAGE,"final" ) ) AND ( LIMIT-TO ( SRCTYPE,"j" ) ) AND ( LIMIT-TO ( LANGUAGE,"English" ) ) |
| Fallopian tube cancer | (("human papillomavirus viruses"[MeSH Terms] OR "human papillomavirus"[Title/Abstract] OR "HPV"[Title/Abstract]) AND ("ovarian neoplasms"[MeSH Terms] OR "ovarian neoplasms"[MeSH Terms] OR (("ovarian"[All Fields] OR "ovarians"[All Fields]) AND "neoplasms"[MeSH Terms]) OR "ovarian cancer*"[Title/Abstract] OR "ovarian carcinoma*"[Title/Abstract] OR "ovarian malignant neoplasm*"[Title/Abstract] OR "ovarian ca"[Title/Abstract])) AND ((excludepreprints[Filter]) AND (fft[Filter]) AND (humans[Filter]) AND (female[Filter]) AND (1985/1/1:2025/1/1[pdat]) AND (english[Filter]) AND (alladult[Filter])) | (INDEXTERMS("human papillomavirus viruses") OR TITLE-ABS("human papillomavirus") OR TITLE-ABS(HPV)) AND (INDEXTERMS("fallopian tube neoplasms") OR TITLE-ABS("fallopian tube cancer*") OR TITLE-ABS("fallopian tube carcinoma*") OR ((INDEXTERMS("fallopian tubes") OR (ALL(fallopian) AND ALL(tubes)) OR ALL("fallopian tubes") OR (ALL(fallopian) AND ALL(tube)) OR ALL("fallopian tube")) AND TITLE-ABS("malignant neoplasm*"))) AND PUBYEAR > 1995 AND PUBYEAR < 2022 AND ( LIMIT-TO ( DOCTYPE,"ar" ) ) AND ( LIMIT-TO ( PUBSTAGE,"final" ) ) AND ( LIMIT-TO ( SRCTYPE,"j" ) ) AND ( LIMIT-TO ( LANGUAGE,"English" ) ) |
| Ovarian cancer | (("human papillomavirus viruses"[MeSH Terms] OR "human papillomavirus"[Title/Abstract] OR "HPV"[Title/Abstract]) AND ("ovarian neoplasms"[MeSH Terms] OR "ovarian neoplasms"[MeSH Terms] OR (("ovarian"[All Fields] OR "ovarians"[All Fields]) AND "neoplasms"[MeSH Terms]) OR "ovarian cancer*"[Title/Abstract] OR "ovarian carcinoma*"[Title/Abstract] OR "ovarian malignant neoplasm*"[Title/Abstract] OR "ovarian ca"[Title/Abstract])) AND ((excludepreprints[Filter]) AND (fft[Filter]) AND (humans[Filter]) AND (female[Filter]) AND (1985/1/1:2025/1/1[pdat]) AND (english[Filter]) AND (alladult[Filter])) | (INDEXTERMS("human papillomavirus viruses") OR TITLE-ABS("human papillomavirus") OR TITLE-ABS(HPV)) AND (INDEXTERMS("ovarian neoplasms") OR INDEXTERMS("ovarian neoplasms") OR ((ALL(ovarian) OR ALL(ovarians)) AND INDEXTERMS(neoplasms)) OR TITLE-ABS("ovarian cancer*") OR TITLE-ABS("ovarian carcinoma*") OR TITLE-ABS("ovarian malignant neoplasm*") OR TITLE-ABS("ovarian ca")) AND PUBYEAR > 1986 AND PUBYEAR < 2026 AND ( LIMIT-TO ( DOCTYPE,"ar" ) ) AND ( LIMIT-TO ( PUBSTAGE,"final" ) ) AND ( LIMIT-TO ( SRCTYPE,"j" ) ) AND ( LIMIT-TO ( LANGUAGE,"English" ) ) |
| Primary peritoneal cancer | (("human papillomavirus viruses"[MeSH Terms] OR "human papillomavirus"[Title/Abstract] OR "HPV"[Title/Abstract]) AND ((("primaries"[All Fields] OR "primary"[All Fields]) AND ("peritoneally"[All Fields] OR "peritoneum"[MeSH Terms] OR "peritoneum"[All Fields] OR "peritoneal"[All Fields] OR "peritonism"[All Fields] OR "peritonitis"[MeSH Terms] OR "peritonitis"[All Fields]) AND "neoplasms"[MeSH Terms]) OR (("primaries"[All Fields] OR "primary"[All Fields]) AND ("peritoneally"[All Fields] OR "peritoneum"[MeSH Terms] OR "peritoneum"[All Fields] OR "peritoneal"[All Fields] OR "peritonism"[All Fields] OR "peritonitis"[MeSH Terms] OR "peritonitis"[All Fields]) AND "carcinoma"[MeSH Terms]) OR "primary peritoneal cancer*"[Title/Abstract] OR "primary peritoneal carcinoma*"[Title/Abstract] OR (("primaries"[All Fields] OR "primary"[All Fields]) AND ("peritoneally"[All Fields] OR "peritoneum"[MeSH Terms] OR "peritoneum"[All Fields] OR "peritoneal"[All Fields] OR "peritonism"[All Fields] OR "peritonitis"[MeSH Terms] OR "peritonitis"[All Fields]) AND "malignant neoplasm*"[Title/Abstract]))) AND ((excludepreprints[Filter]) AND (fft[Filter]) AND (humans[Filter]) AND (female[Filter]) AND (1985/1/1:2025/1/1[pdat]) AND (english[Filter]) AND (alladult[Filter])) | (INDEXTERMS("human papillomavirus viruses") OR TITLE-ABS("human papillomavirus") OR TITLE-ABS(HPV)) AND (((ALL(primaries) OR ALL(primary)) AND (ALL(peritoneally) OR INDEXTERMS(peritoneum) OR ALL(peritoneum) OR ALL(peritoneal) OR ALL(peritonism) OR INDEXTERMS(peritonitis) OR ALL(peritonitis)) AND INDEXTERMS(neoplasms)) OR ((ALL(primaries) OR ALL(primary)) AND (ALL(peritoneally) OR INDEXTERMS(peritoneum) OR ALL(peritoneum) OR ALL(peritoneal) OR ALL(peritonism) OR INDEXTERMS(peritonitis) OR ALL(peritonitis)) AND INDEXTERMS(carcinoma)) OR TITLE-ABS("primary peritoneal cancer*") OR TITLE-ABS("primary peritoneal carcinoma*") OR ((ALL(primaries) OR ALL(primary)) AND (ALL(peritoneally) OR INDEXTERMS(peritoneum) OR ALL(peritoneum) OR ALL(peritoneal) OR ALL(peritonism) OR INDEXTERMS(peritonitis) OR ALL(peritonitis)) AND TITLE-ABS("malignant neoplasm*"))) AND PUBYEAR > 1986 AND PUBYEAR < 2026 AND ( LIMIT-TO ( DOCTYPE,"ar" ) ) AND ( LIMIT-TO ( PUBSTAGE,"final" ) ) AND ( LIMIT-TO ( SRCTYPE,"j" ) ) AND ( LIMIT-TO ( LANGUAGE,"English" ) ) |
Table 2.
Studies on HPV DNA presence in malignancies of the upper female reproductive tract.
| First author, year, reference | Study type | Malignant neoplasm histopathologic type | HPV positivity |
|---|---|---|---|
| Anwar et al., 1996[24] | Case series | 15 endometrial carcinomas |
|
| 3 ovarian carcinomas | None | ||
| O'Leary et al., 1998[25] | Case series | 20 endometrial adenocarcinomas | 2/20 (10%) HPV-11 |
| 41 endometrial adenocarcinomas with squamous metaplasia |
|
||
| 2 adenosquamous endometrial carcinomas | 1/2 (50%) HPV-6 & HPV-33 (same patient) |
||
| Jiang et al., 2010[26] | Case series | 4 endometrioid endometrial adenocarcinomas |
|
| Abu-Lubad et al., 2020[16] | Case-control study | 36 endometrial carcinomas | 3/20 (15%) HPV-18 |
| Bures et al., 2013[27] | Case series | 5 primary squamous cell carcinomas of the endometrium8 endometrioid endometrial carcinomas | None |
| Fedrizzi et al., 2009[17] | Case-control study | 50 endometrial carcinomas |
|
| Fujita et al., 1995[28] | Case series | 85 endometrial adenocarcinomas | 8/85 (9%) HPV-16 |
| Giordano et al., 2006[30] | Case series | 2 mucinous microglandular endometrial adenocarcinomas | None |
| Giordano et al., 2005[47] | Case report | 1 primary squamous cell endometrial carcinoma | None |
| Hachisuga et al., 1996[29] | Case series | 30 endometrial carcinomas | None |
| Hording et al., 1997[31] | Case series | 23 endometrial carcinomas | None |
| Ip et al., 2002[32] | Case series | 55 endometrial adenocarcinomas | 5/55 (9%) HPV-16 |
| 60 primary epithelial ovarian carcinomas | 6/60 (10%) HPV-16/18 | ||
| 4 mucinous borderline ovarian tumors | 3/60 (5%) HPV-16 1/60 (2%) HPV-18 |
||
| 1 clear cell ovarian adenocarcinoma | 1/60 (2%) HPV-16 | ||
| 1 mucinous ovarian adenocarcinoma | 1/60 (2%) HPV-16 | ||
| Karadayi et al., 2013[18] | Case-control study | 30 endometrial adenocarcinomas | None |
| Kataoka et al., 1997[49] | Case report | 1 primary squamous cell carcinoma of the endometrium | 1 (100%) HPV-31 |
| Lai et al., 1994[33] | Case series | 18 epithelial ovarian adenocarcinomas, of which: 9 serous 7 mucinous 2 undifferentiated adenocarcinomas |
9/18 (50%) HPV-16 3/18 (17%) HPV-18 |
| 18 endometrial adenocarcinomas, of which: 10 adenocarcinomas 6 adenosquamous carcinomas 1 clear cell carcinoma 1 undifferentiated carcinoma |
8/18 (44%) HPV-16 3/18 (17%) HPV-18 |
||
| Mariño-Enríquez et al., 2008[34] | Case series | 5 primary transitional cell carcinomas of the endometrium and endometrial carcinomas with transitional cell differentiation | None |
| Park et al., 2004[35] | Case series | 10 endometrial adenocarcinomas | None |
| Plunkett et al., 2003[19] | Case-control study | 50 endometrial carcinomas, of which: 38 endometrioid villoglandular 1 serous papillary 7 mixed adenocarcinomas 1 adenosquamous |
1/50 (2%) HPV-16 |
| Yang et al., 2003[36] | Case series | 46 endometrioid endometrial carcinomas | Endometrial carcinomas: 7/46 (15%) HPV-16 |
| 14 endometrioid ovarian carcinomas | |||
| 21 serous ovarian carcinomas | |||
| 11 mucinous ovarian carcinomas | Ovarian carcinomas: 18/56 (32%) HPV-16 1/56 (2%) HPV-18 |
||
| 6 clear cell ovarian carcinomas | |||
| 4 undifferentiated ovarian carcinomas | |||
| Zielinski et al., 2003[37] | Case series | 20 endometrial adenocarcinomas | None |
| Brewster et al., 1999[38] | Case series | 58 endometrioid endometrial carcinomas | None |
| 4 adenosquamous endometrial carcinomas | 1/4 (25%) HPV-16 | ||
| 3 malignant mixed mesodermal tumors of the endometrial cavity | None | ||
| 1 squamous cell carcinoma of the endometrial cavity | 1 (100%) HPV-18 | ||
| Wong et al., 1993[46] | Case series | 22 endometrial adenocarcinomas | 1/22 (5%) HPV-16 |
| Runnebaum et al., 1996[39] | Case series | 7 primary fallopian tube adenocarcinomas | None |
| Koffa et al., 1994[40] | Case series | 14 endometrial adenocarcinomas | 5/14 (36%) HPV-? (11/16/18/33) |
| 1 clear cell endometrial carcinoma | None | ||
| 1 uterine leiomyosarcoma | None | ||
| 5 ovarian adenocarcinomas | None | ||
| 1 ovarian serous cystadenocarcinoma | None | ||
| 1 borderline mucinous ovarian tumor | None | ||
| 1 Krukenberg tumor | None | ||
| Runnebaum et al., 1995[41] | Case series | 20 ovarian serous cystadenocarcinomas | None |
| 2 ovarian endometrioid adenocarcinomas | None | ||
| 2 ovarian mucinous cystadenocarcinomas | None | ||
| 1 ovarian mixed (endometrioid and serous) cystadenocarcinoma | None | ||
| 1 heterologous malignant mixed Müllerian ovarian tumor | None | ||
| 1 undifferentiated ovarian carcinoma | None | ||
| 1 granulosa cell ovarian tumor | None | ||
| Chen et al., 1999[42] | Case series | 20 ovarian carcinomas | None |
| Alavi et al., 2012[20] | Case-control study | 43 ovarian serous cystadenocarcinomas | 2/43 (5%) HPV-? (16/18) |
| 7 ovarian mucinous adenocarcinomas | 1/7 (14%) HPV-? (16/18) | ||
| Ingerslev et al., 2016[11] | Case series | 146 ovarian serous adenocarcinomas | 1/146 (1%) HPV-18 |
| 10 ovarian mucinous adenocarcinomas | None | ||
| 12 ovarian endometrioid adenocarcinomas | None | ||
| 6 ovarian clear cell carcinomas | None | ||
| Dadashi et al., 2017[21] | Case-control study | 25 ovarian carcinomas | 25/70 (36%) HPV-16 |
| Hassan et al., 2017[43] | Case series | 100 ovarian carcinomas | 5/100 (5%) HPV-16 4/100 (4%) HPV-18 1/100 (1%) HPV-33 |
| Kisseljova et al., 2020[12] | Case series | 29 ovarian serous adenocarcinomas | 18/34 (53%) HPV-16 |
| 2 ovarian mucinous adenocarcinomas | |||
| 3 ovarian endometrioid adenocarcinomas | |||
| Yang et al., 2020[44] | Case series | 310 ovarian carcinomas, of which: 208 serous ovarian adenocarcinomas 48 mucinous ovarian adenocarcinomas |
78/310 (25%) HPV-? |
| Jarych et al., 2024[45] | Case series | 33 serous ovarian adenocarcinomas | 14/46 (30%) HPV-16 9/46 (20%) HPV-18 7/46 (15%) HPV-16+18 |
| 5 borderline ovarian tumors | |||
| 3 clear-cell ovarian adenocarcinomas | |||
| 3 mucinous ovarian adenocarcinomas | |||
| 2 other types of epithelial ovarian adenocarcinomas | |||
| Lai et al., 1992[22] | Case-control study | 11 epithelial ovarian carcinomas, of which: 7 serous ovarian carcinomas 3 mucinous ovarian carcinomas 1 mixed ovarian carcinoma |
2/11 (18%) HPV-16 3/11 (27%) HPV-18 |
| 8 endometrial adenocarcinomas | 2/8 (25%) HPV-16 | ||
| Mohamed et al., 2024[23] | Case-control study | 47 epithelial ovarian carcinomas, of which: 15 high grade serous carcinomas 11 papillary serous adenocarcinomas 10 endometrioid adenocarcinomas 4 undifferentiated carcinomas 2 squamous cell carcinomas 2 mucinous borderline tumors (atypical proliferative mucinous tumors) 2 adult type granulosa cell tumors 1 mixed malignant mullerian tumor |
6/47 (13%) HPV-16 1/47 (2%) HPV-18 5/47 (11%) HPV-? |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



