Submitted:
08 May 2025
Posted:
09 May 2025
You are already at the latest version
Abstract
There is a recent growth in evidence around the use, value and impact of photobiomodulation therapy for individuals with fibromyalgia. However, the nature of the evidence, has, to the best of the authors’ knowledge not been presented within a scoping review. The objective of this work is to reveal the nature of the evidence, gaps in the evidence and map of the evidence considering photobiomodulation therapy against established policy guidelines. A scoping review was undertaken considering all academic evidence that has examined the experiences and impact of photobiomodulation therapy on individuals with fibromyalgia. Our results highlight that indeed there is plentiful data available to address a high proportion of concerns portrayed by the National Institute for Healthcare and Excellence. Outcome measures are wide ranging, albeit demonstrating heterogeneity, and results are extremely promising. Based on the current evidence base, the United Kingdom ‘standard of care’ for fibromyalgia needs to be ascertained, and stringent cost-effectiveness data needs to be collected and presented to governing bodies with the aim of integrating recommendations into future healthcare guidelines.
Keywords:
fibromyalgia
; photobiomodulation
; quality of life
; pain
; laser therapy
; guidelines
1. Introduction
In recent years, the potential benefits of photobiomodulation therapy (PBMT) towards the treatment of fibromyalgia (FM) have come to light, demonstrating an improvement in important health outcomes, such as pain severity, fatigue, stiffness, anxiety, depression and overall FM-specific quality of life measures [1], to name a few. However, it is frequently reported that studies can be seen to be heterogeneous and may lack reproducibility [1,2]. Furthermore, studies may stray from the suggested standardised outcome measures; comprising pain, tenderness, fatigue, patient global health, multidimensional function and sleep disturbance as a minimum [3,4]. Despite this initial evidence identifying important findings, no past overview of evidence has been able to map the evidence to more fully understand the gaps and needs. In 2022, the World Health Organization (WHO) for the first time recognised chronic pain as a disease in its own entity in its updated International Classification of Diseases (ICD-11). Chronic widespread pain syndromes, including FM, now fall under the umbrella term ‘chronic primary pain’ [5]. The National Institute for Health and Care Excellence (NICE) recently developed guidance in consensus with the Royal College of Physicians with regards to managing chronic primary pain [6]. Within their evidence review to justify their recommendations, NICE stipulate requirement for six ‘critical outcomes’ along with suggested measures; pain reduction, health-related quality of life, physical function, psychological distress, pain interference and pain self-efficacy. ‘Important’ but not ‘critical’ outcomes are use of healthcare services, sleep, and discontinuation [7]. Despite acknowledgement of promising efficacy data, NICE do not currently recommend PBMT as a treatment for chronic primary pain [6]. Delving into their research summary, the authors felt that significant available data had potentially been overlooked and not incorporated into their decision-making process. The NICE guidelines specifically mention research gaps in terms of pain interference, pain self-efficacy, physical function, sleep and healthcare utilisation [8]. Research is needed which can evaluate this in further detail by considering the breadth of evidence currently available across different methodological approaches. For instance, qualitative data is often under-represented, yet has the ability to address intricacies of real-world scenarios when guiding treatment protocol development [9]. In particular, NHS England holds patient voice in high regard as being integral towards informing healthcare services [10,11], and the WHO acknowledge the requirement for such data to inform guideline development [12].
Given the above, a scoping review is well-placed to address the issues identified, and the aim of this work is to; provide a comprehensive picture or map of current evidence with a view to build a foundation for policy recommendations.
2. Materials and Methods
In order to ensure a high degree of rigor and transparency, the following scoping review is laid out in accordance with best practice guidance and reporting items for development of scoping reviews, as set out by The Joanna Briggs Institute [13], and reported in line with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Extension for Scoping Reviews (PRISMA-ScR) Checklist [14].
2.1. Protocol and Registration
The review protocol can be accessed via Open Science Framework Registries; identifier https://DOI 10.17605/OSF.IO/ZPSA2.
2.2. Eligibility Criteria
Inclusion criteria were defined according to the Joanna Briggs Institute construct [13]; ‘Population’, ‘Concept’, ‘Context’.
2.2.1. Population
This review’s population was defined as any participant with clinician-diagnosed FM based on 1990 ACR criteria document. No age limits were set as PBMT has regulatory approval in all age groups [15,16,17,18]. If a study includes multiple conditions, it will only be included where FM is identifiable by means of separate subgroup analyses.
2.2.2. Concept
The concept of this scoping review examines both whole-body and localised PBMT as the intervention. There was no restriction on data types and ‘grey’ literature was included. A further phenomenon of interest was experience and perspectives of participants, carers, and healthcare professionals involved in delivering this treatment. Due to the broad intent of this review, no restrictions were made with regards to outcome measures – all available participant-reported outcomes measures, experience measures, and performance-based outcomes were sought via quantitative, qualitative and mixed-methods articles. Tools did not need to be validated for FM studies to be included, but any findings in relation to validity will be commented on in the discussion.
2.2.3. Context
No restrictions were set for clinical setting. Therefore, primary and community settings, secondary and tertiary institutes, allied health professionals, research settings were all included. All geographical locations were included to get the broadest overview possible. Locations are represented in Table 5’s TIDieR (Template for Intervention Description and Replication) checklist [19]. After initial ‘pilot’ search and librarian discussions, a decision was made to set no date limits; including all available literature and all languages.
Initial exclusion criteria were animal studies, theses, study protocols only, and trials with combination therapies in which no separate subgroup analyses were available. On discussion with one of the authors (J.C.) it was decided that laser acupuncture would be excluded as it is a combination therapy i.e., not classed as ‘pure’ PMBT. Following article screening, further exclusion criteria were set with regards to meaningful content. It was deemed, in conjunction with all authors, that any descriptions comprising one paragraph or less would be excluded. The most common occurrence of this was review articles that reviewed many types of therapy and would perhaps include one sentence on PBMT. Where this was the case, references were screened and included so that no data would be missed.
2.3. Information Sources
To identify potentially relevant documents, the following bibliographic databases were searched to include all available dates up until April 2024; Ovid MEDLINE (1946-2024), Embase (1974-2024), Emcare (1974-2024), AMED (1985-2024), CINAHL (1985-2024), PubMed (1782-2024), TRIP Database (up to April 2024), Cochrane Library (1993-2024). In order to supplement this review, additional sources were searched to include difficult-to- locate and “grey” literature: NICE Guidelines (1999-2024), Google Scholar (up to April 2024), Google (up to April 2024), The King’s Fund (up to April 2024), The Health Foundation (up to April 2024), www.gov.uk (up to April 2024), and Nuffield Trust (up to April 2024). Sources of information were left open to allow for the inclusion of all sources, i.e., to include primary studies, systematic reviews, meta-analyses, letters to the editor, guidelines, websites, policy documents, and government reports. It was recognised that where there were evidence syntheses there was a potential to duplicate data. However, primary sources would be included, unless the evidence syntheses were to replicate the primary data exactly, compared with for example, data syntheses with other similar studies. For completeness, the references for the articles included were screened to identify further work. We deemed the breadth of this search to be comprehensive, with a view to obtaining all relevant literature to date. The search was not restricted to specific outcome measures as we recognise both widespread symptom involvement in FM, and the multimodal mechanisms underpinning PBMT.
2.4. Search Strategy
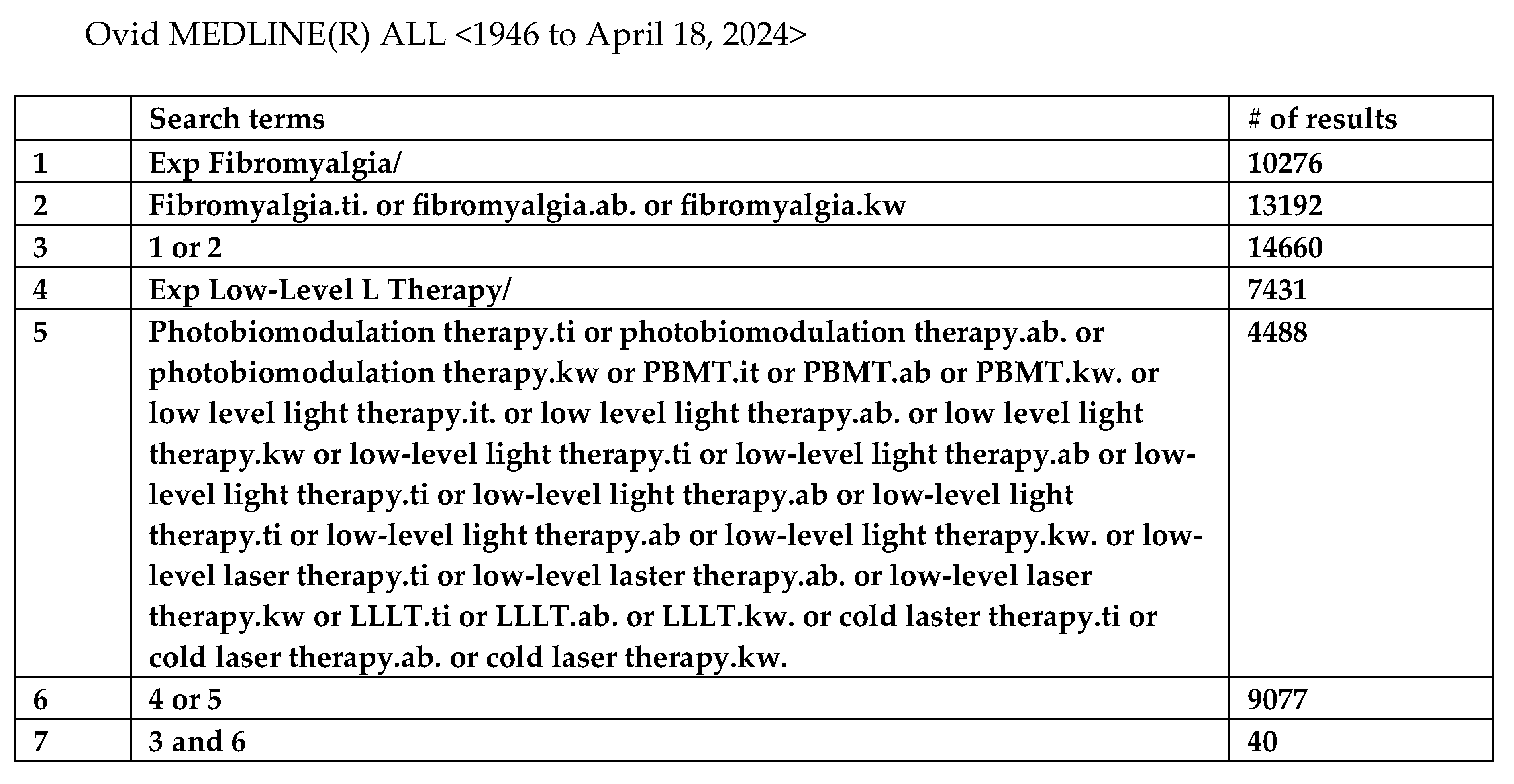
The search strategies used were drafted by an experienced librarian and further refined through team discussion. An initial ‘pilot’ search was undertaken via one database to identify potentially relevant keywords for developing the final search strategy across all databases. No changes were required following the initial search. Results were exported to RefWorks and duplicates were removed. One of the authors (B.F.), scanned reference lists of full texts, searched trial registries, and contacted authors to identify additional relevant material, where applicable. The same librarian, along with an assistant librarian, aided in additional searches and author contact for difficult-to-locate papers. A handful of articles were retrieved by University of Birmingham Library Services. The final search strategy for Ovid MEDLINE is presented in Figure 1, and demonstrates terms and abbreviations previously synonymous with PBMT. The remaining search strategies can be accessed in Supplementary File S1. Synonyms used for the search are represented in Figure 1 and include; “photobiomodulation therapy”, “PBMT”, “low level light therapy”, “low-level light therapy”, “low level laser therapy”, “low-level laser therapy”, “LLLT”, and “cold laser therapy”. “PBMT” is the current and correct terminology, and from here on in all treatment descriptions alluding to this therapy will be described as such. The original source description will be retained in the references.
Figure 1.
Example of final search strategy from Ovid MEDLINE.
2.5. Selection of Sources of Evidence
Identified sources of evidence will be initially screened at the level of title, then abstract, followed by full-text examination of sources that appear to be relevant. A summary of the outcome of this screening process can be found in the Supplementary File – where excluded sources are reported along with reasons for, and stage of, exclusion. The screening and selection of evidence sources was performed by B.F. This process was cross-checked and agreement determined by A.S. Disagreements were managed through discussion between the two data screeners, with a plan for a third party to be consulted to gain consensus, if appropriate. Where technical PBMT questions arose, J.C. was consulted for advice. Due to be broad nature of this scoping review, it was anticipated that searching, screening and selection may reveal new potentially relevant terms, concepts and locations of evidence and as such there was potential for the review process to be modified and expanded. However, we did not find this to be the case.
2.6. Data Charting, Extraction and Selection Process
Data extraction tools were developed by B.F., and cross-checked by A.S., after jointly determining the variables to be extracted. Cross-checking took place at several stages to ensure the required data was appropriately documented. Specific techniques of synthesis were utilized including textual descriptions and tabulation. Data charting was established by developing a standard extraction table for each type of data including experimental studies, qualitative studies and review-based studies. Figure 2 (See Supplementary File) shows the stages of data extraction and provides information around background Tables used to develop tables presented within this thesis. Full and expanded tables can be obtained from the primary author. Table 2 demonstrates adherence to TIDieR checklist [19] for each study included in the synthesis – displaying specifics of how each quantitative study was delivered, aiding in providing a visual representation. The TIDieR checklist is recommended for publication in all research so that interventions can be replicated when building on future research [19]. Further Tables are developed in order to obtain a visual comparison of application and dosage delivery across studies, this was to identify potential factors which contribute to clinical heterogeneity. Qualitative studies using methods like interviews or focus groups to understand experience was limited to a single study. As a result, qualitative findings within studies were tabulated and summarized - as further analysis like content or thematic analysis was not deemed possible due to the different designs used, purposes of the studies and availability of data.
2.7. Quality Assessment of Articles and Level of Evidence Assessment
Assessment of risk of bias was undertaken using the Mixed Methods Appraisal Tool MMAT [20] for empirical studies, which considers 5 questions. This was supplemented by additional methodological comment (see supplementary file). AMSTAR2 [21] was used to assess the quality of included reviews. The Oxford Centre for Evidence based Medicine was used to assess the level of evidence for quantitative and review-based evidence [22]
2.8. Meta Analysis
Meta-analysis was undertaken using fixed effect models looking at the mean difference of continuous data from outcome measures where there were at least three studies with placebo groups. Heterogeneity was tested by considering Chi2 and I2. All meta-analysis was conducted in RevMan 5.0.
3. Results
3.1. Synthesis of RESULTS
Data were grouped together according to article type; namely, quantitative, qualitative, systematic review, meta-analysis, and guidelines. Mixed-method studies were split between quantitative and qualitative data collection tools, and reported as such, respectively. Results are presented according to article type, aims and design, demographics, sample size and participants, outcome measures and findings - specifically pertaining to PBMT in relation to FM. All included studies are then represented according to their adherence to TIDieR checklist [19] (Table 5). The TIDieR checklist provides a partial depiction of methodological quality in terms of data reporting by authors. It additionally serves as a further tool to give a broad picture of study setting, device type and dosage, to name a few.
3.2. Selection of Sources of Evidence
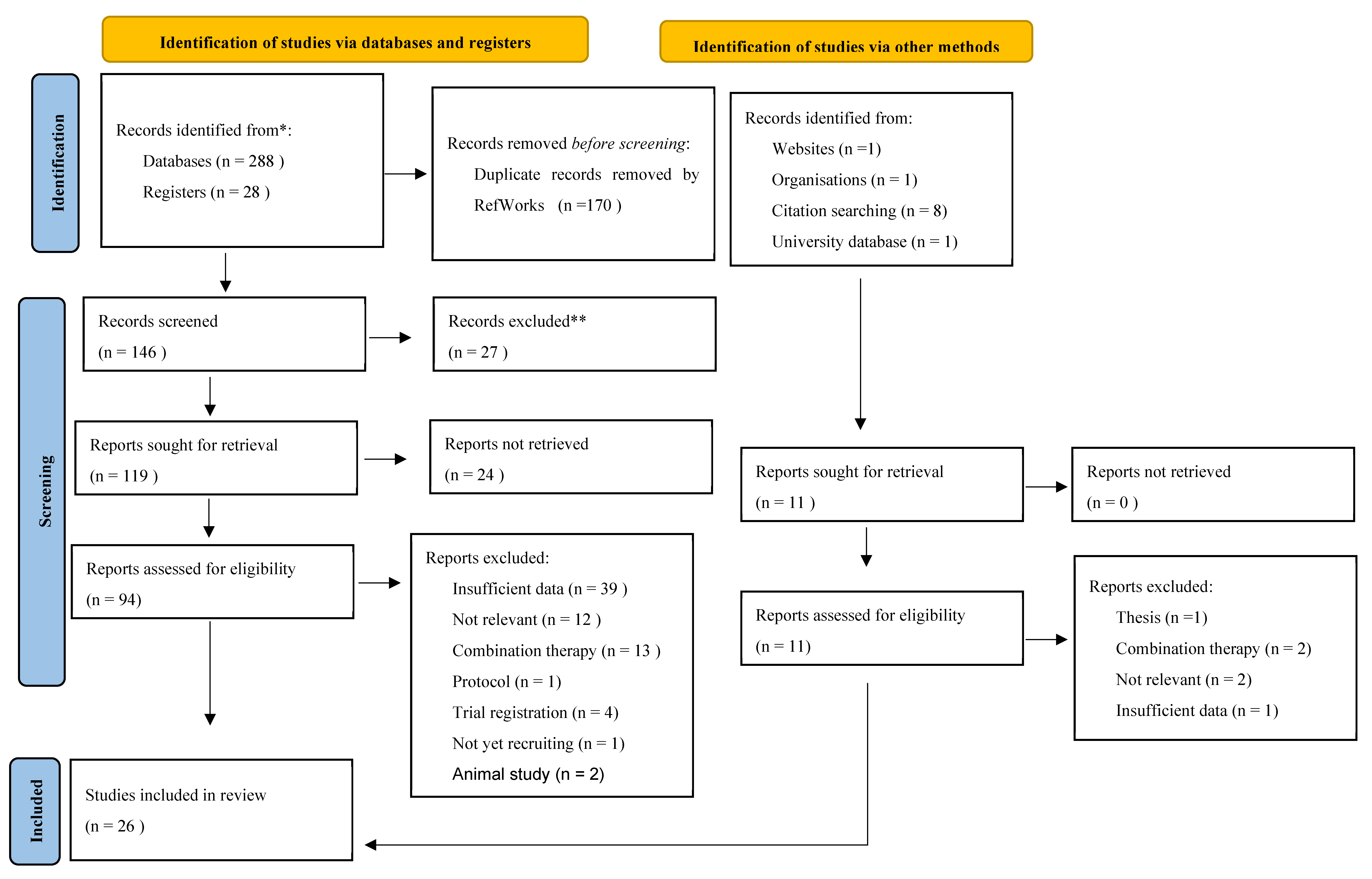
Following screening of eight databases and seven areas of ‘grey literature’ we were left with 355 records in total. An adapted PRISMA-ScR [14] flow diagram is utilised to graphically depict our screening journey in Figure 3. Eighteen articles were excluded by means of our ‘meaningful content’ rule. Where studies were presented as protocols, either published or on trial websites, efforts were made to contact authors to find out study progress and whether any preliminary results were available (n = 16). Six articles underwent ‘Google translation’ by B.F. This was double-checked by another author (A.S.). Four were subsequently excluded. Two translated studies, which included negative results regarding PBMT, were excluded on the basis of not meeting the ‘meaningful content’ rule. This was further assessed by A.S. to reduce risk of bias. Reasons for exclusion at each phase of screening can be accessed for each individual record in the Supplementary File . It should be noted that, despite being included in the final PRISMAScR count, NICE guidelines [6] are not included in the following tables, but instead analysed and compared to existing research in the introduction and discussion.
3.3. Demographic Summary
The following tables represent the main results of this synthesis. Table 1 depicts the study type, aims, and clinical characteristics of all 19 included quantitative evidence and case reports (n = 19; 73% of all included articles). The countries with most studies include Spain (n = 6; 31%), Brazil (n = 5; 26%), and Turkey (n = 4; 21%). Only two have taken place in the USA, with one in the UK, and one in Taiwan. Further research is needed from a broader variety of countries. The earliest research identified was by Gür in 2002 [25,26], however most of the work has taken place since 2018 (n = 10; 53%). A total of 697 participants were included across 17 studies (Navarro-Ledesma et al. [27,28,29] collected data from the same participants across three studies). Gender breakdown included 669 (96%) women, 28 (4%) men. This indicates a discrepancy in gender and a need for further research to include men. The aggregated mean age across 14 studies was 39 years, and the average time with an FM diagnosis was 7.64 years across nine studies. The consistency of reporting other demographics including pain intensity, pain duration and other demographics (for instance, ethnicity, marital status, weight, body mass index) were too infrequent to be reported and this identifies a need for future research.
3.4. Descriptive Summary of Interventions (n = 19)
Most of the studies (n = 15; 79%) used portable or hand-held devices and two research groups have produced five outcome studies [27,28,29,30,31] using a whole-body delivery system. Further research is needed to confirm the efficacy of the whole-body device compared with the efficacy of handheld devices. Table 2 provides a visual picture of how each quantitative study and case study (n = 19) report on the intervention elements according to the TIDieR guidelines [19]. Of the professions identified as providing therapy with the device, four studies [27,28,29,31] used the researchers, three studies used physiotherapist(s) [25,26,31], and two studies used independent physicians [32,33]. The location of the interventions when detailed were most often equally distributed at university sites [34,35,36], hospitals [25,26,31,39] or within private clinics [27,28,29,38,40,41]. The most reported outcome was that there was no mention of adverse effects across all studies, there was however a small drop out in five studies (three samples) [27,28,29,30,36]. Little consistent detail was provided on the frequency and duration of treatment. The most consistent number of treatment sessions was identified as 10 sessions in total [25,26,33,34] across three samples, 12 sessions in total [27-29.36.42.43] across four samples, as well as higher numbers of sessions in three studies including 18 sessions [31] and 20 sessions [38,39]. Six studies used a total duration of four weeks for application [27,28,29,37,38,43] across four samples. The most frequent power output of the device reported was 50 mW [33,36,40]. The inconsistency of reporting and heterogeneity of details provided made further grouping of information not possible. Further research is needed to establish the effectiveness of different durations, intensities and frequencies of PBMT use.
3.5. Summary of Quality Assessment and Level of Evidence Across Interventions (n=19)
All studies scored reasonably highly on the MMAT [20]. This included most (73/95, 77%) studies identifying a ‘yes’ response to the criterion question indicating high quality. In addition, several questions were answered as unclear 14 (14/95, 15%) responses to the criteria considered and 8 (8/95, 8%) responses were identified as not meeting the criteria questions. Additional assessment identified two consistent single methodological limitations, these were a lack of a protocol 14/19 (74%) and lack of named sampling approach 18/19 (95%). The split for the levels of evidence assessment [21] was as follows: 10/19 (52.6%) scored level 2 evidence, 7/19 (36.8%) studies scored level 3 evidence and 2/19 (10.5%) scored level 4 evidence.
3.5. Summary of Outcome Measures Across Interventions (n = 19)
The most frequent outcome measurement area was pain, identified by 13 studies (68%). This was followed by sleep (n = 6; 32%) and then fatigue (n = 4; 21%). The most frequently selected outcome measure was the number of tender point examinations in nine studies (n = 9; 47%). This was followed by the FIQ(R) in seven studies (n = 7; 37%). The most frequently used pain outcome measure was the VAS pain scale (n = 6; 32%). Table 3 summarises the results of all quantitative studies (n = 19), depicting sample sizes, outcome measures utilised and corresponding study results. Further use of broader measures is required to capture other potentially significant outcomes. These may be best identified through qualitative-based research.

Table 1.
Summary table reflecting study type, aims and participant characteristics.
| Paper | Study Type & level of evidence (LoE) | Aims | Demographics | |
|---|---|---|---|---|
| Armagan et al. (2006) [33] | Quantitative RCT LoE:3 |
To investigate efficacy of PBMT in FM |
Gender: 32F PBMT/placebo - Age: 38.94±4.85/37.63±5.90 Pain duration: 5.50±3.03/6.12±3.44 Education: elementary 8/7, high school 5/5, university 3/4 Employment: employed 4/3, not working/retired 4/4, homemaker 8/9 Marital status: married 9/8, single/divorced/widowed 7/8 |
|
| da Silva et al. (2018) [40] | Quantitative Randomized, controlled, blinded LoE:2 |
To evaluate the role of phototherapy and exercise training as well as the combined treatment in general symptoms, pain, and quality of life in women suffering from FM |
Gender: 160F Set 1/Set 2 – Age: 35±3/40±2 Average FM duration: 5±9 BMI: 26±5/27±4 Ethnicity: other or biracial 48/41, white 32/39 Education: elementary 14/9, high school 66/71 Employment: employed or self-employed 52/50, unemployed 28/20 Income (Brazilian Real): <10,000 R$ 9/4, 10,000-30,000 R$ 67/75, 30,000-50,000 R$ 4/2 Drug class (Set 1 and 2): analgesics – paracetamol 109, anti-depressant – amitriptyline 62, fluoxetine 30, citalopram 12, paroxetine 8, duloxetine 58, muscle relaxants – cyclobenzaprine 89, tizanidine 23, carisoprodol 5, hypnotics – benzodiazepines 27 |
|
| de Souza et al. (2018) [42] | Mixed methods: Quantitative, parallel, controlled, randomised. See Table 3 for qualitative LoE:2 |
To compare anaesthetic effect of lidocaine 2% and PBMT by GaAlAs into tender points of patients with orofacial pain and FM |
Gender: 62F 4M Age: 46.14±10.91 FM duration: 76% diagnosed in last 5 years (no differentiation between groups, however, to be no significant difference between groups) |
|
| dos Santos et al. (2020) [32] | Quantitative Randomised, cross-over, clinical-controlled, double-blinded LoE:3 |
To investigate acute effects of PBMT on peripheral muscle strength and resistance in FM patients compared to healthy women |
Gender: 37F FM group/Control group - Age: 44±7/50±8 BMI: 27.69±3.95/29.40±6.37 FM duration: 8 years ±4 TPC: 14±4/not assessed in control group Baseline FIQ: 76±16/not assessed in control group Co-morbidities (n): HTN 7/3, DM 4/0, Osteoporosis 3/0, Heart disease 2/1, Respiratory disease 5/2, Depression 10/1, Other 3/6 |
|
| Ergün et al. (2020) [34] | Quantitative Randomised, placebo-controlled LoE:2 |
To investigate efficiency of PBMT in treatment of clinical symptoms and improvement in QoL in primary FMS |
Gender: 60F PBMT/placebo - Age: 39.4+7.1/40.7+7.3 FM duration: 5.7+5.7/4.5+3.4 |
|
| Fernández García et al. (2011) [35] | Quantitative Randomised, placebo-controlled LoE: 2 |
To assess the effect of the Girlase E1.1010 apparatus on fatigue, sleep difficulties, neck pain, vaginal pain during intercourse and general pain in FM |
Gender: 31F PBMT/placebo - Age: 51.6±6.18/52.4±5.88 FM duration: 4.37±1.41/3.80±1.37 |
|
| Fitzmaurice et al. (2023) [31] | Mixed methods Single-armed, feasibility, embedded qualitative component LoE: 3 |
To investigate the feasibility of whole-body PBMT as a treatment option for reducing pain and pain-related co-morbidities in FM |
Gender: 14F, 5M Age: 47.3±10.9 Ethnicity: Asian/Asian British 5, Black British 1, White British 14 FM duration: 15.6±7.7 BMI: 31.5±5.9 Marital status: married 10, single 6, divorced 1, co-habiting 2, civil partnership 1 Employment: employed full-time 4, employed part-time 1, self-employed 2, unemployed (looking for work) 1, unemployed (not looking for work) 7, sick leave 1, retired 4 Education: some secondary school 1, completed secondary school 2, completed further education (sixth form) 1, higher education 16 Drug class (n): paracetamol 6, anti-inflammatories 4, opioids 17, TCAs 11, SSRIs/SNRIs 11, anticonvulsants 11, anxiolytics 3, sleeping tablet 3, beta blockers 2, migraine prophylaxis and treatment 3, antipsychotic 1 |
|
| Gür et al. (2002) [26] | Quantitative Randomised, placebo-controlled LoE: 3 |
To examine the effectiveness of laser therapy in FM |
Gender: 40F No further demographic breakdown |
|
| Gür et al. (2002) [25] | Quantitative Randomised, placebo-controlled LoE: 2 |
To examine the effectiveness of low power laser and low-dose amitriptyline therapy and to investigate effects of clinical symptoms and QoL in FM |
PBMT/placebo/amitriptyline – Age (years): 30.36±6.91/28.52±6.28/30.14±8.65 FM duration (years): 4.86±4.67/4.63±3.28/4.42±3.14 Gender: 60F 15M Marital status: married 16/15/16, single 5/7/6, divorced 3/2/2, other 1/1/1 Education: elementary 13/14/15, secondary 7/6/6, college/university 5/5/4 Employment: unemployed 2/3/3, employed 3/2/2, retired 1/2/1, homemaker 12/11/11, student 5/5/6, other 2/2/2 |
|
| Molina-Torres et al. (2016) [36] | Quantitative Randomised, single-blinded LoE: 2 |
To investigate therapeutic effects of laser therapy and of an occlusal stabilisation splint for reducing pain and dysfunction and improving quality of sleep in patients with TMD and FM |
Laser/occlusal-splint – Age (years): 51.00±8.32/51.79±7.79 FM duration (%): 1-5 years 3.70/10.71, 6-10 years 29.62/35.71, 11-15 years 44.44/28.57, 16-20 years 14.81/17.85, >20 years 7.40/7.14 TMD duration (%): 1-5 years 22.22/17.85, 6-10 years 37.03/25, 11-15 years 14.81/21.42, 16-20 years 14.81/17.85, >20 years 11.11/17.85 Gender: 55F 3M Profession (%): housewife 70.13/60.71, business 11.11/14.28, administrative staff 18.51/25 Education level (%): primary studies 62.96/67.85, higher education 37.03/32.14 |
|
| Moore & Demchak (2012) [44] | Case report LoE: 4 |
Gender: 1F Age: 19 Ethnicity: Hispanic Employment/Education: college student |
||
| Navarro-Ledesma (2022) [27] | Quantitative Randomised, placebo-controlled, triple blinded LoE: 2 |
To analyse changes in BP values, pain pressure threshold (PPT) and elastic properties of tissue in FM after whole-body PBMT |
Gender: 40F Age: 52.8±7.90 BMI: 29.40±6.36 FM duration: 8.90±2.77 SSS: 8.55±1.29 WPI: 8.13±2.55 Menopausal status: pre = 28, post = 12 |
|
| Navarro-Ledesma et al. (2023) [27] | Quantitative Randomised, placebo-controlled, triple blinded LoE: 2 |
To compare the effects of whole-body PBM on pain, functionality and psychological symptoms in FM |
Gender: 44F Age: 52.83±8.04 BMI: 29.32±6.21 Menopausal status: pre = 29 post = 13 |
|
| Navarro-Ledesma et al. (2024) [29] | Quantitative Prospective, randomised, triple-blinded placebo-controlled LoE: 2 |
To conduct a comparative analysis of effects of whole-body PBM and placebo PBM on pain, functionality and psychological symptoms in FM (6m follow up data) |
Gender: 44F (repeat sample) Age: 52.83±8.04 BMI: 29.32±6.21 Menopausal status: pre = 29 post = 13 (same population as above 2 studies) |
|
| Panton et al. (2013) [37] | Quantitative Randomised, placebo-controlled, double- Blinded LoE: 2 |
To examine the effects of Class IV infrared, therapeutic laser therapy on pain, FM impact and physical function in women with FM |
Gender: 38F, 36 Caucasian, 2 African American Laser + heat/Sham + heat – Age: 52±12/54±11 FM duration: 10±8/11±7 BMI: 31.0±10.0/30.2±6.7 |
|
| Ruaro et al. (2014) [45] | Quantitative Randomised, placebo-controlled LoE: 3 |
To evaluate the effects of PBMT in FM |
PBMT/placebo - Gender: 19F, 1M Age: 43.4/39.4 |
|
| Tramontana et al. (2017) [38] | Pilot, single-blinded, placebo-controlled LoE: 3 |
To evaluate integrative approaches for FM in Physical and Rehabilitation Medicine as an alternative or complementary approach to standard care |
Laser/placebo Gender: 8F, 2M |
|
| White et al. (2018) [41] | Case-based review LoE: 4 |
To evaluated low, intermediate and high level HILT in a patient with longstanding FM |
Gender: 1F Age: 67 FM duration: 7 years Employment: retired veterinarian |
|
| Wu et al. (2018) [39] | Quantitative, single arm (design not stipulated in methods) LoE: 3 |
To investigate clinical effects of intravenous laser irradiation of blood on pain, sleep, mood disorders, QoL in FM |
Gender: 15F Age: 53.77 BMI: 24.30 FM duration: 6.33 years |
|
Table 2.
Details of each study listing the Template for Intervention Description and Replication items. Note: For purposes of this particular table, the ‘How’ element of the checklist was omitted as this describes method of delivery of an intervention, for example, in-person versus virtually. All PBMT is delivered in-person. ‘Why’ describes study rationale – this is omitted here due to volume of work being described. Here, we use ‘How well’ to glean any adverse events or side effects, as well as trial retention and reasons for dropouts, where applicable.
Table 2.
Details of each study listing the Template for Intervention Description and Replication items. Note: For purposes of this particular table, the ‘How’ element of the checklist was omitted as this describes method of delivery of an intervention, for example, in-person versus virtually. All PBMT is delivered in-person. ‘Why’ describes study rationale – this is omitted here due to volume of work being described. Here, we use ‘How well’ to glean any adverse events or side effects, as well as trial retention and reasons for dropouts, where applicable.
| Armagan et al. (2006) [33] (Turkey) |
BRIEF NAME: PBMT WHAT: Gal-Al-As diode laser device (Endolaser 476, EnrafNonius,Netherlands) WHO: Assessment by blinded independent physician, all patients treated by same physician WHERE: Physical Therapy and Rehabilitation Dept, Osmangazi University Hospital MODIFICATIONS: None documented HOW WELL: Feasibility/acceptability aspect of this trial/treatment not documented in terms of adherence to a treatment schedule etc “No systemic or local side effects were reported during or after the treatment period.” WHEN: One treatment/day 5d/week, Total = 10 treatments HOW MUCH: Power output = 50 mW; Wavelength = 830 nm; Dose = 2J/tender point; Mode = continuous; 1mm diameter laser beam at each treatment point TAILORING: PBMT - 1 minute at each tender point considered to be one irradiation dose; Placebo - same laser device seemingly working, but with no laser beams transferring to treated area. All painful points irradiated |
| da Silva et al. (2018) [40] (Brazil) |
BRIEF NAME: Photobiomodulation therapy, exercise training WHAT: Multiple light sources (PBMT + LED) Pain Away/PainCure TM 9-diode cluster device (Multi Radiance Medical®, Solon, OH, USA) WHO: Randomisation by independent researcher. Independent research programmed device (on or off). 2nd researcher guided exercise training (blinding to PBM/placebo). Independent assistant controlled PBM for on/off mode. 3rd researcher blinded to all allocations assessed outcomes. 4th research for statistical analysis (blinded) WHERE: 3 Rheumatology centres MODIFICATIONS: None documented HOW WELL: No dropouts following randomisation. No harm or unintended outcomes reported WHEN: Single treatment at baseline; Total = 1 treatment. Treatment time = 300s per tender point HOW MUCH: Aperture of device = 4 cm2; Total energy delivered per tender point = 39.3 J. Device components - 1 super-pulsed infrared laser Laser wavelength = 905 nm; Frequency = 1000 Hz; Average optical output = 0.9 mW; Power density = 2.25 mW/cm2; Peak power = 8.5 W; Dose = 0.3 J; Energy density = 0.75 J/cm2; Laser spot size = 0.4 cm2. 4 red LEDs LED wavelength = 640 nm±10; Frequency = 2 Hz; Average optical output/LED = 15 mW; Power density/LED = 16.66 mW/cm2; Dose/LED = 4.5 J; Energy density/LED = 5 J/cm2; LED spot size = 0.9 cm2. 4 infrared LEDs LED wavelength = 875 nm±10; Frequency = 16 Hz; Average optical output/LED = 17.5 mW; Power density/LED = 19.44 mW/cm2; Dose/LED = 5.25 J; Energy density/LED = 5.83 J/cm2; LED spot size = 0.9 cm2; Magnetic field = 35 mT TAILORING: PBM - 10 tender points which were reported in all patients (occipital, cervical – near C7, trapezius, supraspinatus, 2nd costochondral joint, lateral epicondyle, gluteal/sacrum, greater trochanter, medial knee border) + bilateral TMJ. Exercise - stretching + aerobic training twice/week, 10 weeks. Pain threshold - digital algometer Instrutherm (DD-220). Placed on specific FM tender points and TMJs using rubber tip measuring 1 cm2. Gradual pressure applied until pain felt, displayed values then recorded (once/point). 30s interval between measurements. VAS applied. |
| de Souza et al. (2018) [42] (Brazil) |
BRIEF NAME: PBMT, lidocaine 2% infiltration WHAT: GaALAs diode laser (Twin Flex® MMOptics) WHO: Diagnosis of FM by neurologist with expertise in chronic pain, diagnosis of orofacial pain by an experienced dentist (expert in Oral and Maxillofacial surgery) by manual palpation WHERE: Small capital Northeast of Brazil (recruited from 2 orofacial centres: 1 public, 1 private) MODIFICATIONS: None documented HOW WELL: No dropout. no adverse effects, no complaints of increased pain at study conclusion WHEN: PBMT 2/week, 6 weeks; Total = 12 treatments. Lidocaine 2% 1/week, 4 weeks; Total = 4 treatments HOW MUCH: Power output = 50 mW; Wavelength = 780 nm; Dose = 50 J/cm2; Spot = 0.04 cm2 TAILORING: Prior to treatment, skin disinfected with 70% alcohol, marked with permanent marker. PBMT - applied to selected spots for approx. 40s. Participants exposed to laser application in a spot-skin distance of 1 cm whilst seated in a dental chair, with neck supported. Lidocaine 2% - 30G short needles, 0.5ml infiltrated into each tender point. Stretching after each injection to help distribute solution across muscle. VAS - self-completed 1-day prior to treatment, and 1-day post. Reflecting pain at rest or function in previous 15 days. Tenderness - perpendicular pressure of 2 or 3 fingers on surface of skin, at approx. 4kg/cm2, 5 muscles assessed bilaterally. Participant in supine position. Presence and location of tender points marked on a diagram – used as reference during all treatments. Repeated at end of study. |
| Diniz et al. (2021) [46](Brazil) |
BRIEF NAME: Low intensity red laser therapy and modified/indirect/ transcutaneous ILIB (Intravascular Laser Irradiation of Blood) WHAT: DUO MMP portable laser device (and bracelet for ILIB) WHO: Not documented WHERE: Not documented MODIFICATIONS: None documented HOW WELL: Slept during treatment application, no mention of side effects WHEN: 2 sessions, 5-day interval HOW MUCH: Intensity = 600 mW/cm2; Output area = 3 mm2; Red laser wavelength = 660 nm; Infrared laser wavelength = 808 nm; Dose (fluence) = 200 J/cm2 TAILORING: PBMT - applied at pain trigger points (bilateral TMJ, neck region, between fingers both hands). Modified ILIB - 30 mins each session (right and left wrist) – attached to bracelet over radial artery |
| dos Santos et al. (2020) [32] |
BRIEF NAME: PBMT WHAT: GaAlAs laser device (Laserpulse; Ibramed) WHO: TPC assessment performed by same physiotherapist WHERE: Not documented MODIFICATIONS: None documented HOW WELL: None documented, no mention of side effects WHEN: 1 session (PBMT/placebo) → 7 days → 1 session (PBMT/placebo) HOW MUCH: Laser pen Power output = 30 mW; Wavelength = 840 nm; Dose (intensity) = 4 J; Frequency = 2.5 kHz; Mode = continuous TAILORING: PBMT - applied to 6 different points on the quadriceps. 90s at each point (probe held stationary in skin contact with 90o angle and slight pressure). Placebo - same points with all parameters in zero. All participants were positioned and fixed at the upper body, across the hips and thighs, hip joint aligned 90-100o flexion in seated position, knee positioned 90o flexion |
| Ergün et al. (2020) [34] (Turkey) |
BRIEF NAME: PBMT WHAT: Infrared 27 Gallium-arsenide (GaAs) (Italian made ElettronicaPagani) WHO: Treatment application and assessment by 2 different doctors (assessment doctor blinded) WHERE: Not documented MODIFICATIONS: None documented HOW WELL: None documented, no mention of side effects WHEN: Total = 10 consecutive treatments (days) HOW MUCH: Average power output = 7.2 mW; Wavelength = 904 nm; Dose (energy density/point) = 4.4 J/cm2; Frequency = 3 kHz; Mode = not documented, assumed continuous TAILORING: PBMT - 2 mins per tender point (all tender points). Full contact technique using 90o vertical angle. Placebo - same method, same period and number of sessions with inactive device |
| Fernández García et al. (2011) [35](Spain) |
BRIEF NAME: Laser based program; PBMT WHAT: Portable Laser Girlase E1.1010 WHO: Not documented WHERE: University of Almeria (UAL) MODIFICATIONS: None documented HOW WELL: None documented, no mention of side effects WHEN: Intervention 8 weeks; 1/week on same time and day each week (each treatment approx. 42 mins) HOW MUCH: Wavelength = 905 nm + 10 nm; Mode = pulsed; Peak power of pulse = 1000 mW; Duration of pulses = 70ns; Energy per pulse = 0.70mJ; Frequency of pulses (Hz) = A 292; B 594; C 1168; D 2336; E 4672; F 73; G 146. Individual application of these 6 frequencies (one minute per frequency) TAILORING: PBMT - 7 anatomical areas – (a) anal region; (b) hypogastrium; (c) epigastric region; (d) left chest region; (e) anterior vertical region; (f) crista galli; (g) between bregma and vertex. 2 cycles/second, 1 cm from skin with laser covering 10cm diameter. Placebo - same anatomic sequence as PBMT group. Laser turned off and at a distance of 15 cm from the body All participants in underwear in supine position, head towards ceiling, eyes closed, arms supinated close to body, low limbs spaced at 30 cm |
| Fitzmaurice et al. (2023) [31] (UK) |
BRIEF NAME: Whole-body photobiomodulation therapy WHAT: NovoTHOR® whole-body red and NIR light bed WHO: Treatment provided by all trial investigators, following a short training session WHERE: Clinical Research Facility, Sandwell General Hospital, Sandwell and West Birmingham NHS Trust, West Bromwich, UK MODIFICATIONS: 10 participants received intended treatment schedule of 3x/week over 6 weeks, 10 participants non-adherent (received treatment of 7-9 weeks; total 41 visits re-scheduled): 61% visits due to medical reasons - fibro flare 2, fall 1, poor sleep 2, viral symptoms 5, covid 7, migraine 1, allergic rhinitis 4, elective sinus surgery 3. Practical reasons – lost car keys 1, staffing/investigator availability 3, dissatisfaction with travel expenses 4, DNA 4, unforeseen circumstances 1, work/study 1 HOW WELL: Of 42 who met eligibility criteria, 24 gave consent (18 declined to participate). 21 started treatment (3 no longer met inclusion). 19 completed (1 difficult committing, 1 uncontactable for outcome measure after receiving 17 treatments). Post-treatment physiological parameters did not reveal adverse effects WHEN: 3 treatment/week; 6 weeks; Total = 18 treatments HOW MUCH: Total power output = 694 W; Individual LED power output = 0.289 W (2400 LEDs); Individual LED beam area (LED lens/skin contact area) = 12.0 cm2; Total area of NovoTHOR® emitting surfaces = 26,740 cm2; Red light wavelength = 660 nm; Near-infrared (NIR) wavelength = 850 nm; Ratio red:NIR = 50:50; Mode = continuous wave; Dose (fluence) = 33.6 J/cm2; Irradiance = 0.028 W/cm2 TAILORING: PBM - session 1 = 6 minutes, session 2 = 12 minutes, session 3-18 = 20 minutes. All participants expected to lie horizontally (in underwear or less) in device, with lid as closed as they are comfortable with. Manual Tender Point Survey/Fibromyalgia Intensity Score (MTPS/FIS) - 18 ACR tender points (9 bilateral) assessed with hand-held Wagner FORCE TEN TM FDX digital pressure algometer – incremental increase up to maximum 4kg/cm2. Verbal NRS taken at each point. Anatomical points: low cervical (C5-C7), 2nd costochondral junction, greater trochanter (posterior to trochanteric prominence), knee (medial fat bad proximal to joint line), occiput (suboccipital muscle insertions), trapezius (midpoint upper border), supraspinatus (above scapula spine near medial border), lateral epidocondyle (2 cm distal), gluteal (upper outer buttock quadrants in anterior fold of muscle) |
| Gür et al. (2002) [26] (Turkey) |
BRIEF NAME: Low power laser therapy WHAT: Ga-As infrared laser therapy (class IIIb Laser Product, Frank Line IR 30, Fysiomed, Belgium) WHO: Two physical therapy investigators WHERE: Dept of Physical Therapy and Rehabilitation, University Hospital of Dicle, Diyarbakir, Turkey MODIFICATIONS: None documented HOW WELL: “None of the participants reported any side effects”, no patient reported discomfort related to treatment and no patient complained of an increase in any outcome parameters. WHEN: One treatment/day; 5d/week for 2 weeks; Total = 10 treatments HOW MUCH: Average power output = 11.2 mW; Wavelength = 904 nm; Mode = pulsed; Peak power of pulse = 20 W; Duration of pulse = 200 ns; Frequency of pulse = 2.8 kHz; Dose (energy density/radiant exposure) = 2 J/cm2 TAILORING: PBMT - 3 min at each tender point (1 cm2 surface). Placebo - laser light invisible and emits no heat or other physically detectable indication when active. Same unit used, no laser beam emitted. All participants were treated at same time (in afternoon) and at a temperature of 20oC |
| Gür et al. (2002) [25] (Turkey) |
BRIEF NAME: Low power laser therapy, amitriptyline WHAT: Ga-As infrared laser therapy (class IIIb Laser Product, Frank Line IR 30, Fysiomed, Belgium) WHO: Two physical therapy investigators, depression evaluated by a psychiatrist WHERE: Dept of Physical Therapy and Rehabilitation, University Hospital of Dicle, Diyarbakir, Turkey MODIFICATIONS: None documented HOW WELL: Side effects (or lack of) not directly reported on, but conclusion recommends laser therapy is safe and effective in FM WHEN: One treatment/day; 5d/week for 2 weeks; Total = 10 treatments HOW MUCH: Average power output = 11.2 mW; Wavelength = 904 nm; Mode = pulsed; Peak power of pulse = 20 W; Duration of pulse = 200 ns; Frequency of pulse = 2.8 kHz; Dose (energy density/radiant exposure) = 2 J/cm2 TAILORING: PBMT - 3 min at each tender point. Placebo - same unit used, no laser beam emitted. Amitriptyline - 10mg daily bedtime 8 weeks. All participants were treated at same time (in afternoon) and at a temperature of 20o C |
| Molina-Torres et al. (2016) [36](Spain) |
BRIEF NAME: Laser therapy, occlusal stabilization WHAT: Láser (Enraf-Nonius Ibérica SA, Madrid, Spain) WHO: Assessor blinded to treatment allocation WHERE: Research laboratory, University of Grenada, Grenada, Spain MODIFICATIONS: None documented HOW WELL: Laser group 2 lost to follow up, occlusal-splint group 1 lost to follow-up (unsure why) WHEN: 1 treatment/week; 12 weeks; Total = 12 treatments HOW MUCH: Average power = 50 mW; Peak power = 80 W; Duration of pulse = 1 µs; Frequency of pulse = 1.5 Hz; Dose = 3 J/cm2 TAILORING: Laser - 2 minutes per tender point (selected during 1st examination); Occlusal-splint - fabricated in laboratory of Faculty of Dentistry at University of Grenada. Each participant agreed to wear during sleep every night, average 8 hours per night, for 12 weeks; NTP - palpation of 18 points both sides – (1) 3 points on joint capsules - lateral, posterior, superior; (2) 3 points on masseter – anterior, inferior, deep; (3) 3 points on temporal – anterior, deep middle, origin; (4) 2 points on pterygoid – medial, lateral; (5) 3 points on sternocleidomastoid – upper, middle, lower; (6) 2 points on trapezius – origin and upper; (7) 2 points on splenius capitis muscles; Active mouth opening - asked to open mouth as much as possible for ‘without pain’ and ‘maximal’ measures; Passing mouth opening - measured after application of downward pressure on mandible by participant’s 2nd and 3rd finger; Joint sounds during mouth opening and closing - clicking assessed with examiner’s left index finger on right joint and right finger on preauricular area, fingertip placed anteriorly to tragus. Participant asked to open mouth slowly, as much as possible. After each closing, participant had to place teeth in contact at a maximal intercuspal position (opened + closed 3 times). Total number of sounds recorded for both sides |
| Moore & Demchak (2012) [44] (USA) |
BRIEF NAME: PBMT WHAT: MR4 device (Multi Radiance Medical, Solon, OH), Ga-As laser WHO: Not documented WHERE: Not documented MODIFICATIONS: None documented HOW WELL: None documented, no mention of side effects WHEN: 2d/week for 2 weeks; Total = 4 treatments HOW MUCH: Super-pulsed laser shower transducer. 6 diodes: Power output = 50 W; Wavelength = 905 nm. 4 diodes: Power output = 25 W; Wavelength = 660 nm; Frequency = 5-1000 Hz; Treatment area = 30 cm2 TAILORING: PBMT - 2 mins over each of identified sensitivity points. At beginning of each session, patient identified areas of sensitivity and rated pain level at each point (0-10) before and after PBMT |
| Navarro-Ledesma (2022) [28] (Spain) |
BRIEF NAME: Whole-body photobiomodulation treatment WHAT: NovoTHOR® whole-body red and NIR light bed WHO: Participants, therapists, evaluators, and statistician blinded. Research assistant taught participants BP measurement procedures. Physiotherapist for SEL measurements (10-year experience, expert in MSK imaging) WHERE: Private clinical practice MODIFICATIONS: Further tender point mentioned in methods – Thumbnail. Midfoot – dorsal third metatarsal midpoint HOW WELL: 2 dropouts – omitted due to not completing proposed assessments WHEN: 3 treatment/week; 4 weeks; Total = 12 treatments HOW MUCH: Total power output = 967 W; Individual LED power output = 0.336 W (2880 LEDs); Individual LED beam area (LED lens/skin contact area) = 12.0 cm2; Dimension of emission surface = 35,544 cm2; Red light wavelength = 660 nm; Near-infrared (NIR) wavelength = 850 nm; Ratio red:NIR = 50:50; Mode = continuous wave; Dose (fluence) = 25.2 J/cm2; Irradiance = 0.028 W/cm2 TAILORING: PBM - 20 mins; Placebo - 20 mins. Bed activates heating elements, providing subjects with sensation of active treatment. Goggles worn that emit some red LED light inside. All participants either naked or in underwear lie flat in the device. All treatments between 8am-4pm; BP - daytime BP (0700-0800) and nighttime BP (0000-0100) self-measured over 7 consecutive days; PPT - Up to 4 kg/cm2 to assess 12 ACR tender points (algometer perpendicular, pressure continually increased until pain perceived). Mean of 2 readings at each point; SEL – 15 MHz linear probe, transducer positioned longitudinally to muscle fibres with centre of probe over tender point and control point locations. ~2-5 mm compression applied to tissue. Mean of 3 at each point; PPT and SEL taken at same points - Occiput – suboccipital muscle insertions (1), Low cervical – anterior aspects of C5-C7 intertransverse spaces (2), Trapezius – midpoint of upper border (3), Supraspinatus – origins atop the scapula spine close to the medial border (4), Paraspinous – laterally 3 cm to midline at mid-scapula (5), Lateral pectoral – anterior axillary line at level of 4th rib (6), 2nd rib – just lateral to upper surface of 2nd costochondral junctions (7), Lateral epicondyle – 2 cm distal to epicondyles (8), Medial epicondyle (9) |
| Navarro-Ledesma et al. (2023) [27] (Spain) |
BRIEF NAME: Whole-body photobiomodulation treatment WHAT: NovoTHOR® whole-body red and NIR light bed WHO: Participants, therapists, evaluators, and statistician blinded. Participants screened by physiotherapist to ensure met inclusion criteria. To improve treatment adherence, treating physiotherapist in regular contact with participants to remind them of their time schedule WHERE: Private care practice, Malaga, Spain MODIFICATIONS: None documented HOW WELL: None documented, no mention of side effects WHEN: 3 treatment/week; 4 weeks; Total = 12 treatments HOW MUCH: Total power output = 967 W; Individual LED power output = 0.336 W (2880 LEDs); Individual LED beam area (LED lens/skin contact area) = 12.0 cm2; Dimension of emission surface = 35,544 cm2; Red light wavelength = 660 nm; Near-infrared (NIR) wavelength = 850 nm; Ratio red:NIR = 50:50; Mode = continuous wave; Dose (fluence) = 25.2 J/cm2; Irradiance = 0.028 W/cm2 TAILORING: PBM - 20 mins; Placebo - 20 mins. Bed activates heating elements, providing subjects with sensation of active treatment. Goggles worn that emit some red LED light inside. A switch box selects active or placebo treatment in a way that is undetectable by participant, operator, or observers. All participants lie supine in treatment bed, with no or minimal attire (underwear). LTPAI - 4 components each with 2 levels (light, medium, vigorous). Scores = total hours of activity over preceding 4 weeks |
| Navarro-Ledesma et al. (2024) [29] (Spain) |
BRIEF NAME: Whole-body photobiomodulation treatment WHAT: NovoTHOR® XL whole-body red and NIR light bed WHO: Research assistant evaluated eligibility. To improve treatment adherence, treating physiotherapist in regular contact with participants to remind them of their time schedule WHERE: Private clinic and rehabilitation service, Malaga, Spain MODIFICATIONS: None documented HOW WELL: Two lost to follow up at 6 months WHEN: 3 treatment/week; 4 weeks; Total = 12 treatments HOW MUCH: Total power output = 967 W; Individual LED power output = 0.336 W (2880 LEDs); Individual LED beam area (LED; lens/skin contact area) = 12.0 cm2; Dimension of emission surface = 35,544 cm2; Red light wavelength = 660 nm; Near-infrared (NIR) wavelength = 850 nm; Ratio red:NIR = 50:50; Mode = continuous wave; Dose (fluence) = 25.2 J/cm2;Irradiance = 0.028 W/cm2 TAILORING: PBM - 20 mins; Placebo - 20 mins. Bed activates heating elements, providing subjects with sensation of active treatment. Goggles worn that emit some red LED light inside. A switch box selects active or placebo treatment in a way that is undetectable by participant, operator, or observers. All participants in both groups assumed supine position in treatment bed for 20 min, while adhering to minimal attire requirements. |
| Panton et al. (2013) [37](USA) |
BRIEF NAME: Laser (Class IV) therapy WHAT: LCT-1000 (LiteCure LLC, Newark, DE) solid-state GaAlAs laser WHO: Investigators performing outcome measures and participants blinded to group assignments. Only chiropractor delivering treatment aware of groups. WHERE: Testing at University and Rheumatology office. Tender point assessment by Rheumatologist. Treatment at a chiropractic clinic by a chiropractic physician MODIFICATIONS: None documented HOW WELL: 1 participant did not return after initial assessment. 2 randomised to laser group dropped out due to scheduling conflicts, 1 in laser group could not complete tests due to severe depression. WHEN: 2 treatment/week; 4 weeks; Total = 8 treatments (as per manufacturer’s recommendation) HOW MUCH: Power output = 10 W; Mode = continuous wave; Dual wavelength = 20% 810 nm and 80% 980 nm; Treatment areas = 2.5 inch x 3.5 inch, or ~56.45 cm2; Dose per treatment area = 10.63 J/cm2 (total 600 J); Grid scanning technique utilised to avoid over-heating; Exposure time at each area = 60s TAILORING: Laser - Warm air supply (below) hose bound together with laser’s fibreoptic cable, routed through a hole in the laser handpiece so that warm air could be delivered alone, or in tandem with laser. 7 minutes; application over 7 tender points across neck, shoulders and back; Placebo - Because laser manufacturer mentions “soothing warmth” of laser, sham + heat therapy designed (commercially available air warmer forced through tube, mounted out of view inside vented cart upon which laser mounted to as to appear as single unit); Myalgic score - 0-3 across 18 tender points (total 54). Subjective rating given by the physician to describe sensitivity of tender point when pressure applied; CP-PFP - 10-items to measure functional performance by simulating routine tasks performed at maximal effort within the bounds of safety and comfort. Speed, distance, weight to quantify performance. Weight + speed = (1) pot carrying, (2) carrying groceries. Time = (3) transferring laundry from washer to dryer, dryer to basket, (4) putting jacket on and off, (5) floor sweeping, (6) climbing stairs, (7) getting down and up from floor, (8) picking up 4 scarves from floor. Distance = (9) 6-minute walk, (10) highest reach. Each task scaled 1-100 (higher = higher function). Participants either gowned, or sports bra, to expose skin of cervical, thoracic, lumbar regions. Positioned face down on treatment table or massage chair. Eye protection worn. |
| Ruaro et al. (2014) [45](Brazil) |
BRIEF NAME: PBMT WHAT: Ga-Al-As diode laser (Ibramed, Laserpulse) WHO: Not documented WHERE: Not documented MODIFICATIONS: None documented HOW WELL: None documented, no side effects or complications reported WHEN: 3 treatment/week; 4 weeks; Total = 12 treatments HOW MUCH: Average power output = 20 mW; Wavelength = 670 nm; Dose = 4 J/cm2; Focal spot area = 0.035 cm2; Exposure time at each point = 7s TAILORING: PBMT - 18 tender points, radiation applied at 4 locations around each point, each location separated by a distance of 1 cm (entire area encompassed by PBMT was 1 cm2 per point) = 72 applications/504s, total power density 0.57W/cm2; Placebo - same procedures as PBMT group but received sham laser exposure (0W). Skin cleaned around 18 tender points. Laser pen applied directly to skin at an angle of 90o |
| Tramontana et al. (2017) [38] (Italy and Spain) |
BRIEF NAME: Laser therapy WHAT: Mixed diode (collimated panta-diodic) WHO: Not documented WHERE: Multi-centre private practice and academic institution; Italy (University di Catanzaro and TA SRL outpatients clinic, Reggio) and Spain (Asociación Española Médicos Integrativos, Madrid) MODIFICATIONS: None documented HOW WELL: No side effects or interactions WHEN: 5 sessions/week; 4 weeks; Total = 20 treatments HOW MUCH: Power output = 5 W; Power density = 1.25 W/cm2.; Wavelength = 950 nm; Superpulsed emission mode = 600-1200 Hz; Length of impulses = 125 ns; Energy density = 1125 J/cm2 TAILORING: Laser - 15 minutes per session; Placebo: Laser off, guide-light on |
| White et al. (2018) [41](USA) |
BRIEF NAME: Laser (Class IV) therapy - HILT WHAT: Phoenix Thera-lase device (Phoenix Thera-lase Systems, LLC, Dallas, TX) WHO: Not documented WHERE: McDermott Center for Pain Management, UT Southwestern Medical Center, Dallas, Texas MODIFICATIONS: None documented HOW WELL: None documented, no mention of side effects WHEN: See ‘tailoring’ HOW MUCH: Power output range = 1-75 W; Treatment 1 = 42 W; Treatment 2 = 42 W; Treatment 3 = 1 W; Treatment 4 = 75 W; Wavelength = 1275 nm TAILORING: HILT - Treatment 1 bilateral lower thoracic and lumbar paraspinous region and 10 tender points at shoulder and hip regions. 60s treatments, 4-6inch apart over symptomatic area, laser probe held approx 12 inch from skin surface (total 40 mins); Treatment 2 1 month later, same areas but more abbreviated (total 30 mins); Treatment 3 – 2 weeks later, paraspinous region (total 30 mins); Treatment 4 – 1 week later, same paraspinous region (total 30 mins) |
| Wu et al.(2018) [39] (Taiwan) |
BRIEF NAME: Intravenous (red) Laser Irradiation of Blood (ILIB) WHAT: YJ-ILIB-5, Bio-ILIB (Human Energy Ltd., Taiwan) WHO: Not documented WHERE: Recruited from outpatient clinic in Department of Rehabilitation and Physical Medicine, Taipei Veterans General Hospital, Twaiwan MODIFICATIONS: None documented HOW WELL: No unfavourable events were recorded, no complaints of discomfort WHEN: 10 ILIB sessions; 2 courses; Total = 20 treatments HOW MUCH: Power output = 2.5 mW; Wavelength = 632.8 nm; Mode = continuous wave TAILORING: ILIB - each session was 60 mins; 7-day rest interval between the 2 treatment courses. Participant lying supine on bed, 24G intravenous catheter at antecubital fossa, subsequently replaced with a fibreoptic needle, inserted into inner cannula of IV catheter. Other side of fibreoptic needle connected to laser device. Comparison made with a medication group – details of this not stipulated in methods |
Table 3.
Summary table for all studies with quantitative element, highlighting sample size and type, outcome measures utilised and results summary. At each initial mention of outcome measure, score range is exhibited in brackets. Standard deviations are denoted by a preceding ‘±’ symbol. P values and Cohen’s d values are explicitly mentioned at point of reference, where applicable.
Table 3.
Summary table for all studies with quantitative element, highlighting sample size and type, outcome measures utilised and results summary. At each initial mention of outcome measure, score range is exhibited in brackets. Standard deviations are denoted by a preceding ‘±’ symbol. P values and Cohen’s d values are explicitly mentioned at point of reference, where applicable.
| Paper | Sample size and participants | Outcome measures and findings | |
|---|---|---|---|
| Armagan et al. (2006) [33] |
FM patients = 32 PBMT = 16 Placebo = 16 |
Number of tender points (NTP). Digital palpation across 18 ACR point (+ve = pain reported on palpation) |
Pre/post/6m PBMT 13.68±2.12/11.81±1.80/12.5±1.71 (p<0.01 baseline vs. post, p<0.05 baseline vs. 6m) Pre/post/6m Placebo 13.94±2.11/12.88±2.09/13.95±1.88 (p<0.05 baseline vs. post) |
| Fibromyalgia Impact Questionnaire (FIQ) |
0-100 Pre/post/6m PBMT 65.50±9.01/58.50±10.3/62.02±8.99 (p<0.01 baseline vs. post, p<0.05 baseline vs. 6m) Pre/post/6m Placebo 65.38±9.44/63.63±9.59/66.94±8.44 |
||
| Morning stiffness |
Likert scale 0-4 (none→extreme) Pre/post/6m PBMT 3.00±0.63/2.38±0.62/2.56±0.89 (p<0.01 baseline vs. post, p<0.05 baseline vs. 6m) Pre/post/6m Placebo 3.06±0.77/2.50±0.89/3.25±0.58 (p<0.05 baseline vs. post) |
||
| Global improvement on a verbal scale (VSGI) |
1-5 (great improvement→worsening) Pre/post/6m PBMT 3.44±1.03/2.56±0.63/3.00±0.73 (p<0.01 baseline vs. post, p<0.05 baseline vs. 6m) Pre/post/6m Placebo 3.38±0.96/3.19±0.75/3.69±0.70 |
||
| Total myalgia score |
18 tender points with 4kg digital force 0-3 (no discomfort→pain with grimace/flinch/withdraw). Total 0-54 Pre/post/6m PBMT 25.00±8.66/19.50±6.95/22.44±6.79 Pre/post/6m Placebo 27.56±9.67/26.00±8.95/28.75±9.86 |
||
| da Silva et al. (2018) [40] |
FM patients = 160 Set 1 (acute effect) = 80 Control = 20 PBM = 20 EXT = 20 PBM + EXT = 20 |
Control group/PBM group/exercise group/PBM+exercise group (average of right and left sides). PBM data in bold where there is significant difference to control group. Underlined where there is significant difference to exercise group. Set 1 → Set 2 NB all below scores are with reference to % improvement from baseline |
|
|
Set 2 (long-term effect/10 weeks) = 80 Control = 20 PBM = 20 EXT = 20 PBM + EXT = 20 |
PPT |
TMJ: 7.06/39.87/27.96/38.76 → 8.21/38.51/25.08/46.27 Occipital: 3.29/26.02/19.02/41.66 → 10.45/24.93/25.38/43.14 C7: 2.38/20.81/7.88/28.62 → 13.14/28.36/30.15/42.09 Trapezius: 0.00/20.81/1.79/30.95 → 11.20/28.66/25.52/35.82 Supraspinatus: 1.50/20.74/6.70/12.28 → 8.66/24.63/33.14/36.27 2nd costochondral joint: 0.00/20.82/4.61/10.06 → 5.98/34.03/38.21/45.44 Lateral epicondyle: 1.19/21.14/6.33/9.83 → 5.97/16.72/23.59/42.84 Gluteal/sacrum: 1.78/24.69/5.95/13.6 → 1.50/30.30/10.75/25.33 Greater trochanter: 5.95/28.71/5.06/14.50 → 5.67/27.76/5.67/22.02 Medial knee border: 1.79/32.64/8.45/17.84 à 6.12/33.44/18.06/25.97 |
|
|
VAS TPC FIQ anxiety FIQ depression FIQ stiffness FIQ fatigue FIQ total |
Set 2 13.13/61.41/43.43/66.67 4.04/53.33/24.24/84.85 0.00/8.35/10.26/15.65 8.35/15.65/15.65/20.87 2.78/10.61/5.65/10.09 1.74/10.09/8.00/19.13 0.87/5.74/22.78/24.78 |
||
| Research Diagnostic Criteria (RDC) score Sleep disturbance Night awakenings Trouble sleeping |
0.00/23.65/19.13/33.04 0.00/10.78/23.65/24.34 2.61/6.96/23.48/74.78 |
||
| Quality of life (SF-36) (0-100) Physical functioning Role-emotional Role-physical Social functioning Mental health Vitality General health |
2.65/28.67/14.16/30.97 1.77/15.93/14.34/24.78 5.49/16.81/13.81/28.32 3.10/12.21/14.60/23.01 1.77/7.08/7.08/21.24 5.31/19.12/9.73/40.71 5.66/12.57/16.81/38.94 |
||
| de Souza et al. (2018) [42] |
FM patients = 66 PBMT = 33 Lidocaine = 33 |
Pain intensity (VAS) |
Pre/post PBMT: 7.85±2.22/2.85±1.77 (p=0.0001) Pre/post LA infiltration: 8.08±2.03/3.18±1.87 (p=0.0001) |
| Overall muscle tenderness to palpation |
Pre/post PBMT: 7.85±2.22/2.85±1.77 (p=0.0001) Pre/post LA infiltration: 8.08±2.03/3.18±1.87 (p=0.0001) |
||
|
Posterior masseter Anterior masseter Anterior temporal Medium temporal Posterior temporal |
No. of participants tender to palpation (right pre/post treatment + left pre-post treatment) PBMT: 21/8 (p=0.00) + 17/8 (p=0.01); LA: 19/5 (p=0.00) + 15/4 (p=0.00) PBMT: 14/6 (p=0.00) + 12/6 (p=0.07); LA: 16/2 (p=0.00) + 13/3 (p=0.01) PBMT: 22/11 (p=0.01) + 24/11 (p=0.00); LA: 25/14 (p=0.00) + 25/14 (p=0.00) PBMT: 22/11 (p=0.00) + 25/13 (p=0.00); LA: 23/13 (p=0.01) + 21/13 (p=0.06) PBMT: 28/25 (p=0.45) + 28/24 (p=0.28); LA: 29/24 (p=0.26) + 30/25 (p=0.12) |
||
| dos Santos et al. (2020) [32] |
N = 37 FM group = 20 Healthy (sedentary) with no MSK/CVS/Resp disease = 17 Each group randomised to PBMT/placebo à 7d washout à PBMT/placebo |
Isokinetic dynamometer muscle strength and endurance Dominant quadriceps muscle (3 series of 5 contractions with 60o/s) |
PBMT group (FM/control) Max torque (Nm): 77.75±21.07/101.12±30.43 Torque peak (%): 90.50±53.13/129.06±60.03 Total work (J): 268.00±94.75/383.06±127.58 Power (W): 44.40±16.16/63.59±22.72 Placebo group (FM/control) Max torque (Nm): 84.05±25.64/100.94±33.28 Torque peak (%): 96.80±55.76/127.35±31.28 Total work (J): 282.30±103.80/361.12±144.24 Power (W):49.90±17.58/62.94±26.92 |
| Isokinetic dynamometer muscle resistance Dominant quadriceps muscle (3 series of 5 contractions with 240o/s) |
PBMT group (FM/control) Max torque (Nm): 42.90±14.73/62.47±15.22 Torque peak (%): 48.95±30.71/81.06±34.64 Total work (J): 409.10±166.40/641.82±171.21 Power (W): 57.10±25.22/94.71±26.29 Placebo group (FM/control) Max torque (Nm): 43.90±13.92/60.12±18.47 Torque peak (%): 50.45±31.34/76.41±35.83 Total work (J): 411.80±159.20/621.82±219.70 Power (W): 57.90±24.02/91.82±36.31 |
||
| Ergün et al. (2020) [34] |
FM patients = 60 PBMT = 30 Placebo = 30 |
NTP |
Pre/post PBMT: 13.4+2.4/7.1+4. Pre/post placebo: 13.1+1.9/7.6+3.8 |
| LIKERT TYPE SCALE (0-4; none à intolerable), all p<0.001 | |||
| Pain intensity | Pre/post PBMT: 2.6+0.8/1.4+0.6. Pre/post placebo: 2.7+0.7/1.6+0.7 | ||
| Stiffness | Pre/post PBMT: 2+1.1/1+1. Pre/post placebo: 1.9+0.8/1.1+0.8 | ||
| Sleep disorders | Pre/post PBMT: 1.6+1.1/0.8+1. Pre/post placebo: 1.3+1.3/0.9+0.9 | ||
| Fatigue | Pre/post PBMT: 2.5+0.8/1.4+0.7. Pre/post placebo: 2.6+1/1.3+0.9 | ||
| Muscle spasms | Pre/post PBMT: 1.9+1/0.9+0.9. Pre/post placebo: 2.3+1.1/1.2+1.1 | ||
| Subjective swelling | Pre/post PBMT: 1.3+0.9/0.6+0.7. Pre/post placebo: 1.3+1.1/0.5+0.6 | ||
| Paraesthesia | Pre/post PBMT: 1.7+0.9/0.7+0.5. Pre/post placebo: 1.3+0.9/0.7+0.8 | ||
| Total Likert | Pre/post PBMT: 13.5+3.9/6.8+3.4. Pre/post placebo: 13.3+3.9/6.9+4.2 | ||
| FIQ | Pre/post PBMT: 54.6+11.7/2.3+12.3. Pre/post placebo: 55.6+12.5/33.9+14.8 | ||
| Fitzmaurice et al. (2023) [31] |
FM patients=19 PBMT = 19 |
Pre/post PBM/mean improvement (Cohen’s d)à 6-month follow up: mean improvement (Cohen’s d) | |
| FIQR (0-100) |
79.7±13.26/55.3±19.72 (p≤0.001)/24.44±20.38 (1.49) à 65.68±16.53/Week 6: Week 24 -10.41, p=0.23 (0.57); Baseline: Week 24 14.02, p=0.001 (0.94) | ||
| Patient Global Impression of Change (PGIC) (1-7; 1=no changer or worse, 7 = great deal better) | 6 weeks: 5.47±1.43; 6 months: 3.79±2.1 (0.94) |
||
| Pre/post PBM (Cohen’s d) | |||
| Brief Pain Index-Short Form (BPI-SF): BPI Pain Intensity BPI Pain Interference (0-10) Perceived analgesic efficacy (%) |
7.08±1.28/3.93±1.38 (2.37) 6.59±1.32/4.17±1.99 (1.43) 43.5±17.55/53.89±20.0 |
||
| Fibromyalgia Severity Score (WPI+SSS) (0-31) | 25.1±2.86 (15±2.45 + 10.1±1.45)/16.21±5.78 (9.89±4.21 + 6.32±2.54) (1.95) |
||
| Fatigue severity score (FSS) (1-7) | 6.30±0.86/5.61±1.16 (0.68) |
||
| Jenkins Sleep Questionnaire (JSQ) (0-20) | 17.35±1.90/11.53±6.17 (1.27) |
||
| Hospital Anxiety and Depression Scale (HADS) HADS-A (0-21) HADS-D (0-21) |
14± 3.71/10.53± 4.57 (0.83) 12.5± 3.26/8.21± 3.68 (1.23) |
||
| Stiffness (subsection FIQR) (0-10) | 9.05± 1.02/5.95± 2.56 (1.59) |
||
| Dyscognition (subsection FIQR) (0-10) | 8.35± 1.31/5.58± 2.56 (1.38) |
||
| Fibromyalgia Intensity Score (0-10) Average pressure tolerated (kg/cm2) |
6.35±1.84/5.17± 1.91 (0.52) 1.21± 1.05/1.71± 1.16 (0.49) |
||
| Stroop Test: Total score (in 60s) Accuracy (%) |
27.4±16.0/31.21± 15.11 (0.24) 85.23±24.06/85.45±24.04 (0.01) |
||
| Medications reduced or stopped (n) | Paracetamol 3, anti-inflammatories 2, opioids 9, TCAs 2, SSRIs/SNRIs 2, anticonvulsants 1 | ||
|
Fernández García et al. (2011) ]35] |
FM patients = 31 Ratio not clear |
Impact on FM (FIQ) 0-100 | Pre/post PBMT: 71.45±11.80/52.30±15.22. Pre/post placebo: 60.89±15.28/50.37±24.18 |
| VAS 1-10 (minimal à severe) | |||
| Fatigue |
Pre/post PBMT: 8.25±1.48/3.93±1.76; p<0.049 Pre/post placebo: 7.93±1.79/5.92±3.38 |
||
| Sleeping difficulties (fatigue on waking) |
Pre/post PBMT: 7.53±2.09/5.23±2.56; p<0.044 Pre/post placebo: 5.72±3.13/7.14±2.44 |
||
| General pain |
Pre/post PBMT: 8.43±1.75/6.12±2.91 Pre/post placebo: 7.46±2.44/6.73±2.25 |
||
| Neck pain |
Pre/post PBMT: 8.29±1.64/6.33±2.82 Pre/post placebo: 7.36±2.29/6.81±3.02 |
||
| Vaginal pain during intercourse |
Pre/post PBMT: 6.87±4.34/4.75±2.35 Pre/post placebo: 5.20±2.65/5.73±3.21 |
||
| All other than fatigue and sleep non-significant | |||
| Gür et al. (2002) [26] |
FM patients = 40 PBMT = 20 Placebo = 20 |
NTP |
Pre/post PBMT: 13.18±2.3/6.63±3.86. Pre/post placebo: 12.7±0.71/8.55±4.11 |
| Likert scale 0-4 (none à extreme) | |||
| Pain | Pre/post PBMT: 3.09±0.52/1.270.76. Pre/post placebo: 3.48±0.8/2.44±0.98 | ||
| Skinfold tenderness | Pre/post PBMT: 2.18±0.95/0.90±0.5. Pre/post placebo: 2.10±0.71/1.33±1.37 | ||
| Morning stiffness | Pre/post PBMT: 2.54±0.8/1.09±0.92. Pre/post placebo: 2.7±0.86/2.01±0.8 | ||
| Sleep disturbance | Pre/post PBMT: 2.36±1.25/1.27±1.07. Pre/post placebo: 1.7±1.12/1.66±1.60 | ||
| Fatigue | Pre/post PBMT: 3.09±0.81/1.36±1.17. Pre/post placebo: 2.10±0.71/2.04±1.09 | ||
| Muscle spasm | Pre/post PBMT: 2.27±0.45/0.81±0.73. Pre/post placebo: 2.3±0.47/1.33±0.68 | ||
| P<0.05 improvement in pain, muscle spasm, morning stiffness, and NTP in PBMT group compared with placebo | |||
| Gür et al. (2002) [25] |
FM patients = 75 PBMT = 25 Placebo PBMT = 25 Amitriptyline = 25 |
NTP |
Pre/post PBMT: 13.92±2.30/6.40±3.90. Pre/post placebo: 11.90±2.30/8.00±3.84 Pre/post amitriptyline: 12.72±1.16/7.27±3.20 |
| Likert scale 0-4 (none à extreme) | |||
| Pain intensity |
Pre/post PBMT: 3.04±0.53/1.24±0.72. Pre/post placebo: 3.19±0.87/2.19±0.74 Pre/post amitriptyline: 2.90±0.68/2.09±0.92 |
||
| Skin fold tenderness |
Pre/post PBMT: 2.12±0.92/0.80±0.57. Pre/post placebo: 2.08±0.60/1.64±1.20 Pre/post amitriptyline: 2.27±0.76/1.45±1.18 |
||
| Morning stiffness |
Pre/post PBMT: 2.56±1.01/0.96±0.93. Pre/post placebo: 2.66±0.91/1.90±0.83 Pre/post amitriptyline: 2.45±0.80/1.15±0.67 |
||
| Sleep disturbance |
Pre/post PBMT: 2.40±1.22/1.12±1.09. Pre/post placebo: 2.11±0.80/1.79±1.36 Pre/post amitriptyline: 2.09±1.26/0.81±0.73 |
||
| Muscle spasm |
Pre/post PBMT: 2.28±0.54/0.84±0.68. Pre/post placebo: 2.19±0.40/1.13±0.62 Pre/post amitriptyline: 1.81±0.73/1.00±0.61 |
||
| Fatigue |
Pre/post PBMT: 3.12±0.83/1.32±1.10. Pre/post placebo: 3.04±0.74/2.28±0.90 Pre/post amitriptyline: 2.86±0.90/2.49±1.26 |
||
| Depression | Hamilton Depression Rating Scale 0 - ≥23 (normal → very severe) Pre/post PBMT: 19.24±5.88/11.48±3.96/Pre/post placebo: 18.08±4.13/15.79±4.07 Pre/post amitriptyline: 17.57±4.19/7.16±3.24 |
||
| QoL (FIQ) |
Pre/post PBMT: 56.27±7.57/33.02±11.96Pre/post placebo: 59.94±8.18/50.30±8.87 Pre/post amitriptyline: 57.73±9.11/39.78±8.62 |
||
| Significant improvements in all parameters of PBMT group (p=0.001), and all in amitriptyline group, except fatigue. Significant difference in pain intensity and fatigue in favour of laser group over other groups. |
|||
| Molina-Torres et al. (2016) [36] |
FM + TMD patients = 58 Laser = 29 Occlusal-splint = 29 |
Widespread pain (WPI) (0-19) + Severity of symptoms (SSS) (0-12) |
Between group differences in score changes: -4.138 Pre/post laser/within group score change (Cohen’s d): 15.59±3.50 + 9.72±2.99/14.62±3.75 + 8.69±3.04/0.966 + 1.034 (0.267 + 0.341) Pre/post occlusal-splints/within group score change (Cohen’s d): 15.62±2.89 + 9.72±1.93/13.45±4.16 + 8.07±2.82/2.172 + 1.655 (0.614 + 0.696) Between group differences in score changes: -1.172 + -0.621 |
| Pain intensity (VAS) (0-100) |
Pre/post laser/within group score change (Cohen’s d): 78.62±20.13/70.69±19.07/7.931 (0.404) Pre/post occlusal-splints/within group score change (Cohen’s d): 76.55±14.71/66.55±21.92/10.00 (0.546) |
||
| NTP (0-36) |
Pre/post laser/within group score change (Cohen’s d): 11.69±2.24/7.24±1.81/4.448 (0.200) Pre/post occlusal-splints/within group score change (Cohen’s d): 11.86±2.31/6.76±1.53/5.103 (0.659) Between group differences in score changes: -0.483 |
||
| Quality of sleep (Pittsburgh Quality of Sleep Questionnaire Index – PSQI) (0-21) |
Pre/post laser/within group score change (Cohen’s d): 14.07±4.38/13.45±4.68/0.620 (0.137) Pre/post occlusal-splints/within group score change (Cohen’s d): 16.00±3.17/13.69±4.05/2.310 (0.639) Between group differences in score changes: 0.240 |
||
| Active mouth opening without pain |
Pre/post laser/within group score change (Cohen’s d): 26.10±5.22/27.45±5.27/-1.344 (0.256) Pre/post occlusal-splints/within group score change (Cohen’s d): 27.34±5.15/30.03±5.08/-2.689 (0.525) Between group differences in score changes: 2.586 |
||
| Maximal active + passive mouth opening |
Pre/post laser/within group score change (Cohen’s d): 34.72±5.04 + 38.34±5.32/35.34±5.29 + 39.24±5.74/-0.620 + -0.896 (0.119 + 0.162) Pre/post occlusal-splints/within group score change (Cohen’s d): 37.17±6.23 + 40.79±6.13/38.41±6.29 + 42.47±6.16 (-1.241 + -1.655) Between group differences in score changes: 3.068 + 3.206 |
||
| Clicking sound during palpation when opening (right + left) |
Pre/post laser/within group score change (Cohen’s d): 0.31±0.47/0.17±0.38 + 0.45±0.51/0.24±0.44/0.138 + 0.207 (0.327 + 0.445) Pre/post occlusal-splints/within group score change (Cohen’s d): 0.28±0.46/0.10±0.31 + 0.21±0.41/0.17±0.38/0.172 + 0.034 (0.471 + 0.100) Between group differences in score changes: -0.069 + -0.069 |
||
| Click sound during palpation when closing (right + left) |
Pre/post laser/within group score change (Cohen’s d): 0.34±0.48/0.17±0.38 + 0.41±0.50/0.21±0.41/0.172 + 0.207 (0.391 + 0.438) Pre/post occlusal-splints/within group score change (Cohen’s d): 0.24±0.44/0.03±0.19 + 0.21±0.41/0.03±0.19/0.207 + 0.172 (0.677 + 0.602) Between group differences in score changes: -0.138 + -0.172 |
||
| PGIC (5-point version; much improved à much worse) |
Pre/post laser/within group score change (Cohen’s d): 4.45±0.78/3.83±0.54/0.621 (0.937) Pre/post occlusal-splints/within group score change (Cohen’s d): 4.41±0.87/3.48±1.18/0.931 (0.907) Between group differences in score changes: -0.345 All pre and post intervention values statistically significant, excepting left clicking sound when opening in occlusal-splint group |
||
| Moore & Demchak (2012) [44] | FM patient = 1 |
NTP VAS FIQ Subjective Activity of Daily Living (SADL) – subsection of FIQ |
Pre/post PBMT/2 weeks post PBMT 14/6/14 6/2 82/23/34 20/5/0 |
| Navarro-Ledesma (2022) [28] |
FM patients = 40 |
Circadian BP Index |
Between group difference after intervention: -3.01, p=0.036, SE -0.06 |
| PPT |
PPT in tender points with significant differences (between group differences after intervention) Occiput: -0.273, p=0.039, SE 0.127 Low cervical: -0.254, p=0.035, SE 0.134 Trapezius: -0.235, p=0.037, SE 0.109 2nd rib: -0.632, p=<0.0001, SE 0.109 Medial epicondyle: -0.505, p=0.006, SE 0.173 |
||
| Strain elastography (SEL) (objective alternative for PPT) | SEL in tender points with significant differences (between group differences after intervention), and/or non-significant difference but medium effect size of ~0.5 Trapezius: 0.0522, p=0.028, SE 0.53 Forearm: 0.730, p=<0.001, SE 0.14 Low cervical: dominant -0.004, p=0.808, SE 0.74. non-dominant 0.174, p=0.469, SE 0.62 Supraspinatus: -0.146, p=0.480, SE 0.49 Lateral epicondyle: 0.072, p=0.697, SE 0.60 Anterior tibial: -0.291, p=0.342, SE 0.62 |
||
| Navarro-Ledesma et al. (2023) [27] |
FM patients = 44 |
Baseline = T0, after session 6 (2 weeks) = T1, after session 12 (4 weeks) = T2, 2 weeks after treatment = T3 Significant between group at T1/T2/T3 or non-significant difference but medium effect size of ~0.5 |
|
| Pain intensity (NPRS) – average over preceding 7 days (0-10) | T2; 3.00, p=<0.001, Cohen’s d = 2.06 T3; p=<0.001, Cohen’s d = 2.87 T0 → T1 → T2 → T3: PBMT 8.22 à 7.18 à 5.22 à 4.32; Placebo 8.0 à 7.69 à 7.74 à 8.11 |
||
| Health-related quality of life (HRQL) – average over preceding 7 days (0-10) |
T1; -2.00, p=<0.001, Cohen’s d = -0.129 T2; -3.00, p=<0.001, Cohen’s d = -2.49 T3; -4.00, p=<0.001, Cohen’s d = -3.26 T0 → T1 → T2 → T3: PBMT 3.33 à 4.9 à 6.16 à 7.0; Placebo 2.83 à 3.2 à 2.91 à 3.05 |
||
| Leisure Time Physical Activity Instrument (LTPAI) |
T2; -28.00, p=<0.001, Cohen’s d = -1.90 T3; -43.00, p=<0.001, Cohen’s d = -2.70 T0 → T1 → T2 → T3: PBMT 28 à 25.6 à 47.56 à 72.5; Placebo 30 à 28.4 à 24.4 à 29.17 |
||
| Tampa Scale of Kinesiophobia (11-44; higher score = greater fear movement/injury) |
T1: 6.00, p=<0.008, Cohen’s d = 0.87 T2; 10.00, p=<0.001, Cohen’s d = 1.25 T3; 12.00, p=<0.001, Cohen’s d = 1.49 T0 → T1 → T2 → T3: PBMT 25 à 23.11 à 19.2 à 17.63; Placebo 30.67 à 29.19 à 28.8 à 28.5 |
||
| Self-efficacy questionnaire (0-44; higher score = greater perception confidence to handle situation) | T2; -7.00, p=0.034, Cohen’s d = -0.73 T3; -8.00, p=<0.001, Cohen’s d = -1.33 T0 → T1 → T2 → T3: PBMT 27.93 à 26.93 à 31.03 à 33.80; Placebo 26.55 à 26.13 à 25.71 à 25.86 |
||
| Pain Catastrophising Scale (0-52; higher score = higher catastrophism) |
T0 → T1 → T2 → T3: PBMT 28.21 → 26.21 → 23.18 → 21.43; Placebo 27.14 → 27.38 → 27.14 → 28.5 None statistically significant, all small effect sizes |
||
| Navarro-Ledesma et al. (2024) [29] |
FM patients = 42 |
3 months = T4, 6 months = T5 (see above study for T0, T1, T2, T3 data) Significant between group at T4/T5 and/or non-significant difference but medium effect size of ~0.5 |
|
| Pain intensity (NPRS) – average over preceding 7 days (0-10) |
T4; -1.00, p=0.17, Cohen’s d = -0.53 T5; 2.00, p=0.001, Cohen’s d = 1.16 T4 → T5 PBMT 6.36 à 4.91; Placebo 5.23 à 6.73 |
||
| Health-related quality of life (HRQL) – average over preceding 7 days (0-10) |
T4; -3.03, p=<0.001, Cohen’s d = -3.2 T5; -2.00, p=<0.001, Cohen’s d = -2.35 T4 → T5 PBMT 6.24 à 5.94; Placebo 3.23 à 3.56 |
||
| Leisure Time Physical Activity Instrument (LTPAI) (AKA Godin test) |
T4; -41.23, p=<0.001, Cohen’s d = -2.55 T5; -43.00, p=<0.001, Cohen’s d = -2.86 T4 → T5 PBMT 72.84 à 74.63; Placebo 31.34 à 32.84 |
||
| Tampa Scale of Kinesiophobia (11-44; higher score = greater fear movement/injury) |
T4; 9.52, p=<0.001, Cohen’s d = 1.24 T5; 13.00, p=<0.001, Cohen’s d = 2.16 T4 → T5 PBMT 16.47 à 14.35; Placebo 28.24 à 25.88 |
||
| Self-efficacy questionnaire (0-44; higher score = greater perception confidence to handle situation) | T4; -11.19, p=<0.001, Cohen’s d = -2.31 T5; -12.00, p=<0.001, Cohen’s d = -2.04 T4 → T5 PBMT 36.98 à 38.46; Placebo 18.34 à 17.75 |
||
| Pain Catastrophising Scale (0-52; higher score = higher catastrophism) | T4; 7.00, p=0.05, Cohen’s d = 0.64 T5; 10.00, p=0.006, Cohen’s d = 0.83 T4 → T5 PBMT 19.03 à 19.70; Placebo 25.75 à 29.48 |
||
| Panton et al. (2013) [37] |
FM patients = 38 Laser + heat therapy = 20 Sham + heat therapy = 18 |
Myalgic score 8 tender points (back) Myalgic score (back) |
Pre/post laser + heat: 15±5/12±6 (p≤0.05). Pre/post placebo + heat: 14±4/11±5 (p≤0.05) Pre/post laser: 6±2/5±2. Pre/post placebo: 6±1/5±2 (p≤0.05) Pre/post laser: 16±6/13±7 (p≤0.05). Pre/post placebo: 14±5/11±5 (p≤0.05) |
| NTP |
Pre/post laser + heat: 14±3/11±5 (p≤0.05). Pre/post placebo + heat: 13±3/10±4 (p≤0.05) | ||
| FIQ FIQ Pain subsection |
Pre/post laser: 62±21/55±16 (p≤0.05). Pre/post placebo: 57±11/55±12 Pre/post laser: 7.1±2.3/6.2±2.1 (p≤0.05; ES 12). Pre/post placebo: 5.8±1.3/6.1±1.4 |
||
| Continuous scale physical functional performance (CS-PFP): Upper body strength Upper body flexibility Lower body strength Balance and coordination Endurance CS-PFP total Overall rating of perceived exertion (RPE) post CS-PFP |
Pre/post laser: 33±17/39±16 (p≤0.05). Pre/post placebo: 38±14/42±15 Pre/post laser: 71±17/78±12 (p≤0.05; ES 21). Pre/post placebo: 77±12/77±11 Pre/post laser: 33±15/39±15 (p≤0.05). Pre/post placebo: 39±16/44±16 (p≤0.05) Pre/post laser: 43±16/52±14 (p≤0.05). Pre/post placebo: 51±16/56±16 (p≤0.05) Pre/post laser: 44±15/52±13 (p≤0.05). Pre/post placebo: 52±15/57±16 (p≤0.05) Pre/post laser: 42±15/49±13 (p≤0.05). Pre/post placebo: 49±14/53±15 (p≤0.05) Pre/post laser: 13±2/13±2. Pre/post placebo: 13±1/13±2 FIQ Pain and Upper body flexibility improvements were statistically significant compared with placebo therapy |
||
| Ruaro et al. (2014) [45] |
FM patients = 20 PBMT = 10 Placebo = 10 |
NTP |
Pre/post PBMT: 11.6±2.4/7.3±2. Pre/post placebo: 11.8±1.5/10.4±1.5, p<0.0001 |
| FIQ physical impairment FIQ feel good FIQ work missed FIQ difficult to work FIQ pain FIQ fatigue FIQ rested FIQ stiffness FIQ anxiety FIQ depression FIQ total |
Pre/post PBMT: 4.9±1.8/3.4±1.4. Pre/post placebo: 3.6±2.4/3.0±2.1 1.5 PBMT improvement versus 0.5 placebo, p=0.04 Pre/post PBMT: 7.7±1.8/5.6±1.6. Pre/post placebo: 5.9±4.3/3.6±3.5 2.1 PBMT improvement versus 2.3 placebo, p=0.9 Pre/post PBMT: 2.2±1.9/0.6±1.0. Pre/post placebo: 1.4±1.4/1.3±1.3 1.6 PBMT improvement versus 0.1 placebo, p=0.015 Pre/post PBMT: 7.0±1.9/5.8±1.0. Pre/post placebo: 7.7±2.0/7.3±2.0 1.2 PBMT improvement versus 0.4 placebo, p=0.16 Pre/post PBMT: 8.1±1.6/5.4±1.1. Pre/post placebo: 8.8±1.6/7.7±1.3 2.7 PBMT improvement versus 1.1 placebo, p=0.0075 Pre/post PBMT: 7.6±2.1/5.5±1.2. Pre/post placebo: 8.3±1.6/7.5±1.7 2.1 PBMT improvement versus 0.8 placebo, p=0.0043 Pre/post PBMT: 8.1±1.4/6.4±0.8. Pre/post placebo: 7.9±1.1/7.9±1.4 1.7 PBMT improvement versus 0.0 placebo, p=0.06 Pre/post PBMT: 7.7±1.8/6.0±0.9. Pre/post placebo: 7.8±1.5/8.0±1.6 1.7 PBMT improvement versus 0.2 placebo, p=0.0034 Pre/post PBMT: 7.6±1.6/5.4±1.4. Pre/post placebo: 7.9±1.3/7.4±1.4 2.2 PBMT improvement versus 0.5 placebo, p=0.0012 Pre/post PBMT: 6.7±1.6/4.9±1.3. Pre/post placebo: 7.8±1.6/7.8±1.3 1.8 PBMT improvement versus 0.0 placebo, p<0.0001 Pre/post PBMT: 67.5±13.2/48.9±7.2. Pre/post placebo: 66.7±11.9/61.5±10.0 18.6 PBMT improvement versus 5.2 placebo, p=0.0003 All significant reductions in PBMT group, versus only physical impairment in placebo group |
||
| McGill Pain Questionnaire |
0-78 (no pain → severe pain) Pre/post PBMT: 45/32.1. Pre/post placebo: 47.5/42.6 p=0.0078 Pre/post PBMT: 6.58/4.06. Pre/post placebo: 5.81/5.34 p=0.002 |
||
| VAS |
Pre/post PBMT: 6.58/4.06. Pre/post placebo: 5.81/5.34 p=0.002 |
||
| Tramontana et al. (2017) [38] |
FM patients = 10 Laser = 5 Placebo = 5 |
Reduction of conventional treatment doses (50% average) cortisone, duloxetine, pregabalin |
Laser/placebo First evaluation: 34.85%/42.43% After 15 days: 9.7%/31.06% (p=0.001) |
| White et al. (2018) [41] | FM patient = 1 | VAS |
6-7/1-2 after treatment 1 for 1 week/returned to 3-3.5 after 1 week 0-1 after treatment 4, lasting >10d |
| Baseline scores |
WPI = 10, SSS = 7, FIQ/SIQ = 38.3, SF-36: Physical functioning = 45, role-emotional = 0, role-physical = 0, social functioning = 25, general health = 25, pain = 10, emotional well-being = 56, energy/fatigue = 30 | ||
| NRS pain relief (0 = none, 10 = complete pain relief) |
Post treatment 1 = 7 Post treatment 2 = 6, lasted 4 days Post treatment 3 = 2-3, lasting 2-3 hours. Pain returned to baseline after 1 week Post treatment 4 = 8-9, lasting >10d. After 2w pain symptoms returned to >50% baseline |
||
| Wu et al. (2018) [39] |
FM patients = 15 |
VAS NTP FIQR Beck Depression Inventory (BDI) (0-63, >30 = severe) Pittsburgh Sleep Quality Index (PSQI) |
Pre IV laser irradiation/24 hours after last treatment 7.86/5 (p=0.001) 15/13.27 (p=0.002) 74.08/51.43 (p=0.001) 18.29/8.34 (p=0.003) 15.99/10.72 (p=0.01) |
3.6. Meta-Analysis
Only VAS pain scale and FIQ total score had enough data points to undertaken meta-analysis. The use of Likert scales prevented further meta-analysis [22,23,32]. Meta-analysis was possible for VAS pain scale [26,33,43] and the FIQ total score [22,31,32,35,43] was undertaken. For VAS pain at 4-6 weeks (post treatment) a signficant overall effect and clinically meaninful change was found and the pooled mean difference was -3.13 [-3.45, -2.82 95% CI], although the I2 test identified signficant heterogenity (94%). For FIQ total at 2 weeks [n=3] and 4 weeks [n=2] post treatment the Chi2 identified heterogenity but I2 (0%) did not. A signficant overall effect was found and the pooled mean difference was -13.46[-3.45 - -0.94 95%CI]. This change was close to the clinically meaningful change (14%).
Figure 4.
A forest plot of the pain VAS scale at the point of post treatment (at 4 to 6 weeks).

Figure 5.
A forest plot of the FIQ total score at the points of post treatment (2 to 4 weeks).

6.3.1. Clinical Heterogenity Considering Application of the Device
Table 4 and Table 5 provide a summary of the parameters and application of the different PBM devices used across studies against the outcome measures and changes in VAS pain (Table 4) and FIQ total score (Table 5). The clinical parameters are most consistent within VAS pain where 8 measure meants can be attribute to one whole body device. The results illustrate the importance of understanding variability in application when designing future studies and using teams that understand this knowledge base.
Table 4.
The dosage and clinical parameters consider photobiomodulation devices used across studies when considering changes in pain VAS scale scores.
Table 4.
The dosage and clinical parameters consider photobiomodulation devices used across studies when considering changes in pain VAS scale scores.
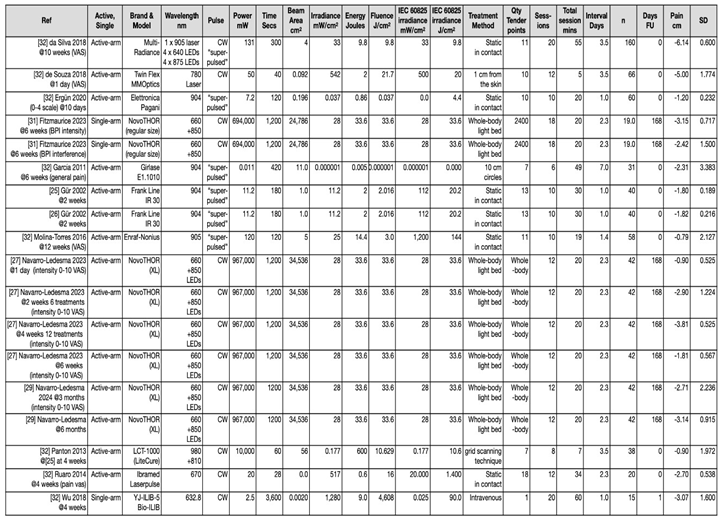
Table 5.
Table 4. The dosage and clinical parameters consider photobiomodulation devices used across studies when considering changes in FIQ total scores .
Table 5.
Table 4. The dosage and clinical parameters consider photobiomodulation devices used across studies when considering changes in FIQ total scores .
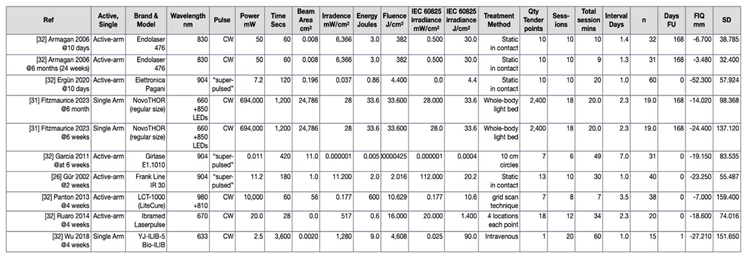
3.6. Systematic Review-Based Evidence and Summary of Meta-Analyses (n=3)
Table 6 summaries the three identified systematic reviews and meta-analyses. Two systematic reviews [1,50] were rated by AMSTAR2 [22] as low quality and one systematic review [47] was rated as high quality. All systematic reviews contained Level 1 evidence according to the Oxford Centre for Evidence Based Medicine [21]. It should be noted that no extra studies are analysed within these latter reviews, but results are presented in an alternative fashion; pooling and comparing mean differences between studies and therefore the authors deemed relevant for inclusion. All meta-analyses utilised FIQ or FIQR in assessing function. Pain was assessed via a variety of scales, for instance, VAS, Brief Pain Inventory, and Tender Point Count. Mood was assessed in two of the three meta-analyses via a variety of outcome measures including Beck Depression Inventory, Hospital Anxiety and Depression Scale, as well as FIQ “subitems”. Only one meta-analysis assessed fatigue and stiffness in their own right. Out of the 3045 subjects included in Gikaro et al. [47], 374 (12.3%) were specific to PBMT; taken from eight [25,26,33,36,42,43,48] out of the total of 54 studies analysed for electrophysical agents. Seven of these studies are included in summary Table 1, Table 2 and Table 3 - the latter [48] being excluded due to examining combination therapies. Similarly, Honda et al. [49] examined effects of electrophysical therapies in FM. As such, 39.8% (187 participants) data pertains specifically to PBMT. From the 11 RCTs analysed, 5 [25,26,33,43,48] are in relation to PBMT. Of note, these overlap with the studies from Gikaro et al. [47]. When contrasting electrophysical agents, these meta-analyses summise that PBMT has the highest probability of being among the best modality for pain relief [47,49] and mood [47]. Yeh et al. [1] pools data from nine (n = 325) of the quantitative studies we have analysed [25,26,33,35,40,43,48,50,51]to summate that focussed PBMT when compared to placebo, provides statistically significant improvement in pain severity, fatigue, stiffness, anxiety, depression and overall FM-specific quality of life; all with large effect sizes. It should be noted, we excluded three [48,50,51] of the nine RCTs due to being combination therapy and not pure PBMT.
3.7. Qualitative Data (n = 6)
The six studies with qualitative elements are summarised in Table 5, representing 88 participants, 87 of which are included quantitatively in Table 1, Table 2 and Table 3. Participants in Fitzmaurice et al. studies [27,28] represent a crossover i.e., 16 of the 19 participants undergoing PBMT underwent semi-structured qualitative interviews. As such, of the total 702 participants represented in this review, 12.6% of these participants contributed to qualitative data. The results in this table speak for themselves – participants consistently and compellingly describe reduction in pain, pain medications, stiffness, fatigue, and memory impairment. They have experienced increased energy, motivation, confidence and overall engagement in life. Importantly, the “icing on the cake” so to speak, is that they also had a very positive experience of using this therapy.
Table 5.
Summary table for all studies with qualitative element, reflecting feasibility and experiences of treatment.
Table 5.
Summary table for all studies with qualitative element, reflecting feasibility and experiences of treatment.
| Paper | Feasibility outcomes pertaining to treatment and schedule | Qualitative outcomes |
|---|---|---|
| de Souza et al. (2018) [42] Mixed methods (n = 66) |
Qualitative component on perceptions of efficacy and well-being: Effectiveness: PBMT Yes: n = 33, No: n = 0; LA Yes: 32 No: 1 Improvement of well-being: PBMT Yes: 32 No: 1; LA Yes: 27 No: 6 |
|
| Diniz et al. (2021) [46] Case report (n = 1) |
During 1st ILIB application for 30 minutes, patient slept sitting in the dental chair. Got up from the chair much better than when she arrived. “She felt a sense of improvement as soon as we completed the laser therapy applications at the trigger points and ILIB” |
Baseline: all teeth aching, pain and burning in face, neck, hips, knees and hands – presented to ED with tooth ache (X rays normal). Poor sleep, waking up with burning hands, patient reported already attempted suicide with husband’s gun to try and end the pain she felt every day. No longer working due to FM: due to severe pain for consecutive days felt too insecure to dedicate herself to activity outside the home. Previously consulted with physiotherapy and psychologist. Medications: escitalopram, pregabalin, topiramate, cyclobenzaprine, bupropion Post treatment: patient reported her pains are completely gone for 2 months, felt much better, feels she seems to have changed, more patient with life events and the people around her, had the courage to travel with her husband. Did not take analgesics, anti-inflammatories, or muscle relaxants during this period. After 2 months, pains were coming back |
| Fitzmaurice et al. (2023) [31] Mixed methods (n = 19) |
Barriers to uptake: 7 could not commit time to treatment schedule, 3 felt would be too fatigued by travel, 1 could not afford petrol (lived >20miles away), 1 worried about personal unreliability due to flare unpredictability, 2 uncontactable, 1 move area, 1 trying for pregnancy, 1 claustrophobic Acceptability of treatment schedule: 12 satisfied with number and frequency of sessions, 5 would have preferred higher frequency (daily), 1 would prefer less due to travel money Acceptability of trial device: 13 felt device easy to access. Suggestions for support rail to make entry and exit easier. 2 were required to remove fentanyl patch for each treatment. Claustrophobic? 79.3% strongly disagree. Comfortable in underwear? 84.1% strongly agree Easy to operate? 100% strongly agree Comfortable to use? 79.3% agree or strongly agree Willingness towards future trial: all participants willing to be involved in future research relating to this device |
Treatment satisfaction Positive experiences: helpful (n = 4), pleasant (n = 3), positive (n = 3), enjoyable (n = 2), comfortable (n = 1), efficient (n = 1), great (n = 1), useful (n = 1), interesting (n = 1), painless (n = 1), quick (n = 1), beneficial (n = 1), easy (n =1), worthwhile (n = 1), necessary (n = 1) Low-energy positive emotions: relaxing (n = 11), calming (n = 3), soothing (n = 2) High-energy positive emotions: pain relief (n = 4), warm (n = 3), better memory (n = 2), good mood (n = 2), better sleep (n = 1), more energy (n = 1), less confused (n = 1), reduced headaches (n = 1), clearer minded (n = 1), addictive (n = 1), fun (n = 1) Future-related: hope (n = 1) Negative experience: pain made it ‘difficult’ to adhere to treatment schedule (n =1) |
| Fitzmaurice et al. (2024) [30] Qualitative (n = 16) |
Subthemes (n = 5) highlighting intervention experience Positive PBMT experience Attributable changes to PBMT Recommendation to others Fear of treatment ending Unanticipated effects |
Themes (n = 3) and subthemes (n = 18) highlighting treatment response Body structure and function Improvement in pain; Reduced lethargy and fatigue; Improved sleep; Mood lifted; Reduction in analgesics and interventional therapy; Reduction in stiffness and improved mobility; Anxiety and agitation decreased; Improved memory and concentration; Reduction in time needed to mobilise; Brain fog cleared; Enjoyment of body warmth; Reduced number and intensity of flares Activities and participation Starting/re-commencing hobbies/enjoyable activities; More able to cope with everyday chores/tasks/work; More willing to engage in activities with others Environment Noticeable physical and emotional improvements; Improved relationships; Insight and reduced reliance on poor habits 4 subsequent processes identified: increased motivation, feeling proud, improved confidence, feeling like ‘old self’ Ultimately identifying a ‘recomposition phase’ in the FM condition, further described by 5 final sub-themes: Ability to cope with and push aside other symptoms; Self-awareness and insight into symptom interlinkage; Improved pain and sleep having substantial effect on mood, energy, confidence, motivation and ability to cope; Improved sleep and more importantly improved sleep hygiene; New-found enjoyment in hobbies secondary to improved memory and concentration |
| Moore et al. (2012) [44] Case report (n = 1) |
Despite an increase in symptoms 2 weeks post PBMT patient felt ADLs were not adversely affected | |
| White et al. (2018) [41] Case report (n = 1) |
Baseline: Difficulty primarily expressed for household chores, lifting and carrying groceries, climbing stairs, prolonged sitting – taken from FIQ. Medical problems stopped her from accomplishing weekly goals. Reported symptoms of depression, difficulty sleeping, memory and balance problems, sensitivity to: touch, loud noises, bright lights, odours, cold. Previously tried a number of treatments including limited series of PBMT (810-980 nm). Hydrocodone 5mg 4-5 times per month for acute FM flares. Post treatment 1: Improved range of motion, mood, level of physical activity, quality of sleep lasting for 1 week. Required no opioid analgesics during this time. Stated she would be willing to pay $90USD out-of-pocket per treatment session to continue receiving 42W and 75W HILT 2-3 times per month Post treatment 4: No longer using opioid analgesics |
3.8. Use of Validated Outcome Measures
When checking the above quantitative data and its compliance against suggested outcome measures by the Outcome Measures in Rheumatological Clinical Trials (OMERACT) FM Working Group 2012 [3], 15 out of 19 (78.9%) papers are seen to be at least partially in keeping with these recommendations. No paper completely satisfied the required core symptom domain outcome measures, with a study on whole-body PBMT [31] being the closest at 88.9% compliance. However, 5 out of these 19 papers were published on or before OMERACT’s 2012 recommendations. Similarly, all quantitative studies and meta-analyses satisfied one or more NICE-recommended outcomes [8], with no study covering every outcome. Only two studies (10.5%) utilised the 2009-updated Revised Fibromyalgia Impact Questionnaire (FIQR) [52]. Six studies (31.6%) did incorporate FIQ outcomes, however, five of which did so in an out-dated fashion (which could be correlated and/or extrapolated to give an up-to-date FIQR if necessary [52]). Furthermore, it was the FIQR (not FIQ) recommended by OMERACT in 2012 [3]. Of more concern is that only seven studies (36.8%), utilised this widely accepted and recommended FM-specific quality of life measure [3,52].
3.9. Results to Address NICE Concerns
Below, we report on compliance with our primary objective. That is, how many of the assessed trials cover recommended NICE ‘critical’ and ‘important’ outcomes, respectively. It is worth pointing out that a recent FM review of outcome measures found that only 8.6% (n = 9 out of a total of 105) studies since 2015 covered all OMERACT recommended symptom domains [4].
3.3.1. NICE Critical Outcomes
3.3.1.1. Pain Reduction
NICE evidence review stipulates that any validated pain reduction scale is an acceptable outcome measure [6]. Our own meta-analysis identified a significant reduction versus placebo at 4- and 6-weeks post treatment. Further to this, eighteen quantitative studies (94.7%) incorporate a participant-reported pain measure, one being indirectly via FIQ and number of tender points. All three published meta-analyses directly address pain reduction. Taking the quantitative studies alone, pain reduction is apparent across all studies, in many cases this is compared with placebo. The improvement is statistically significant across 15 of these, totalling 297 participants (that is 42.3% of total participants analysed). Of note, significant reduction is seen in favour of PBMT versus pharmacological agents and injection therapy: amitriptyline in one study [25], and local anaesthetic infiltration in another [42]. Three studies address NICE concerns, exhibiting an ongoing and significant relief at 6 months compared with baseline [29,31,33].
3.3.1.2. Health-Related Quality of Life
No specific measures are suggested for health-related quality of life, other than stipulating to ‘include meaningful activity’ [6]. Twelve (63.2%) of our included quantitative papers incorporated numerical quality of life measures, as well as all meta-analyses. All qualitative data alludes to an improved quality of life in the participant’s own words. One paper in particular goes on to develop a number of themes and processes to exhibit the magnitude in which 16 FM patients’ lives changed for the better after a course of whole-body PBMT [29]. The 12 quantitative studies that assessed quality of life did so in the form of FIQ(R), SF-36 – showing improved physical, emotional, social functioning and vitality, PGIC and HRQL. This amounts to 238 participants. The meta-analysis focused on the FIQ scale and demonstrated a significant improvement in the overall score when considering a short time scale of between 2- to 4- weeks post intervention. Ten studies demonstrated statistically significant improvements, two of which continued to exhibit this at six months’ follow-up.
3.3.1.3. Physical Function
Despite not being some of the NICE recommended objective measures of physical function [7], several studies do go on to measure physical function objectively by means of: isokinetic dynamometer to determine muscle strength, endurance and resistance [32]; active and passing mouth opening and palpation in those with co-existing temporomandibular dysfunction [36]; strain elastography [28]; upper and lower body strength, upper body flexibility, balance, coordination and endurance via Continuous Scale Physical Functional Performance (CS-PFP) [37]. For this outcome, OMERACT recommend only a self-report in the form of the FIQR subscale, ‘physical function’. As such, all studies encompassing FIQ or FIQR therefore fulfil this requirement, contrary to NICE’s evidence review. Further data reporting on subjective physical functioning exists: Leisure Time Physical Activity Instrument (LTPAI) and Tampa Scale of Kinesiophobia [27]; and overall rating of perceived exertion (RPE) post CS-PFP [37]. The former instrument is not only validated in FM patients but has shown significant associations with the 6-minute walk test [53], therefore could deemed as a surrogate marker of physical function, fulfilling one of the six symptom domains listed in NICE’s list of ‘critical’ outcomes [2]. Four studies (other than those utilising FIQ) specifically assessed physical function, surmounting to 91 participants. All demonstrated statistically significant improvements; one study exhibiting continued improvement in physical functioning at 6 months.
3.3.1.4. Psychological Distress
Ten quantitative studies (52.6%) assessed anxiety and depression; three directly via specific validated questionnaires: Hospital Anxiety and Depression Scale, Hamilton Depression Rating Scale, and Beck Depression Inventory. The remaining seven were via FIQ or FIQR anxiety and depression subscales. It should be noted anxiety and depression are not listed in the recommended ‘core’ domains for research set out by OMERACT [3]. Two of three meta-analyses pool data give a verdict regarding anxiety and depression – revealing significant improvements in anxiety and depression secondary to a course of PBMT [1,47]. Again, all studies incorporating FIQ or FIQR will have assessed psychological distress. Five studies (n = 89) have specifically reported on it, all demonstrating significantly improved levels of psychological distress and emotional functioning. Although Navarro et al. [28,29] has not directly assessed, the Pain Catastrophising Scale was utilised and demonstrated post-treatment improvement, which could be seen as a surrogate marker of emotional dysfunction and negative thought patterns [54].
3.3.1.5. Pain Interference
Only one quantitative study (5.3%) incorporates the NICE recommended Brief Pain Inventory (BPI) for the pain interference outcome – demonstrating significant improvement [30]. A further nine quantitative studies utilise the FIQ or FIQR which represents ‘fibromyalgia interference’. One of the meta-analyses specifically reports on BPI [47].
3.3.1.6. Pain Self-Efficacy
Two quantitative studies (10.5%), and no meta-analysis, report specifically on self-efficacy. Qualitative data does, however, indirectly represent many of the aspects covered in the Pain Self-Efficacy Questionnaire. Navarro et al. [27,29] demonstrate a significant and ongoing improvement in pain self-efficacy at 6 months.
3.3.2. NICE Important Outcomes
3.3.2.1. Use of Healthcare Services
Here, NICE do not recommend one specific questionnaire. However, no quantitative study has directly reported on this important outcome. Two quantitative studies do mention medication reductions, which could be seen as a potential reduction in healthcare service usage. Furthermore, three qualitative studies report on medication reductions, as well as injection therapy being postponed until a later date. No study reports on health economics, however, one participant states they would be willing to pay a significant sum in order to continue receiving PBMT.
3.3.2.2. Sleep
Again, NICE do not stipulate a specific tool. OMERACT recommend the Jenkins Sleep Questionnaire [3]. Twelve quantitative studies (63.2%) report on sleep, eight of which utilise a Likert Scale or FIQ/FIQR subscale. Four studies use a specific sleep questionnaire: Jenkins Sleep Questionnaire (n = 1); Research Diagnostic Criteria score (n = 1); Pittsburgh Quality of Sleep Index (n = 2). No meta-analysis specifically reports on sleep. Two qualitative studies report on sleep. Of the assessed quantitative studies, an improvement in sleep is demonstrated across 199 participants, significantly so in 179 participants.
3.3.2.3. Discontinuation
Only very few trials identified very low dropout (n = 11; 1.6%). Four participants could not commit to treatment schedules, six were lost to follow-up, and one could not complete initial outcome measures due to severe depression. To the best of the authors’ knowledge, from this review no discontinuation was identified because of negative experiences or side effects secondary to the intervention.
4. Discussion
4.1. NICE Guidance
This scoping review provides a summary of all available evidence to date, of all data types, regarding the use of PBMT in the treatment of FM. Whilst we acknowledge the valuable points made by NICE in their latest guidance [6], this review demonstrates that some data may have been missed. In their evidence summary [7], studies for PBMT (or rather their outdated use of “LLLT”) in chronic primary pain were grouped together with all electrophysical modalities. Thus, only three relevant studies were identified [26,33,37], one of which was almost 20 years old [26]. From our searches, prior to NICE’s 2021 guidance, twelve additional papers were identified for ‘pure’ PBM alone – surmounting to 564 FM patients. Additionally, two recent systematic reviews and meta-analyses [1,49] were overlooked. Furthermore, a wide variety of conditions were included in their searches; myofascial pain (1 study, n = 26), burning mouth syndrome (5 studies, n = 122), FM (3 studies, n = 64), chronic neck pain (2 studies, n = 55), TMD (4 studies, n = 85) [7]. Furthermore, only literature surrounding ‘focused’ PBMT was available at the time of NICE guidance, with whole-body PBMT data emerging from 2022 onwards.
The current review can support an update to the NICE recommendations by highlighting the high level of evidence currently supporting PBMT findings. This includes the use of 3 systematic reviews representing level 1 evidence [21] as well as a significant number of studies with level 2 evidence [21]. Importantly, the most recent systematic review [47] rated high through AMSTAR assessment and approaching a 10-fold increase in patient numbers compared to the other two reviewers (rated as low by AMSTAR2) illustrates positive results around pain, general FM symptoms, sleep and fatigue, a finding that is consistent with the 19 experimental studies identified in the current scoping review. Our current meta-analysis has identified that PBMT produces a clinically important change beyond the minimally important change of 13mm on the VAS scale [55]. Clinically important changes in FIQ for patients with FM are identified as 14% or an absolute change of 8.1 points [56]. This evidence should be considered appropriate in supporting the use of PBMT within a short intervention (between 2-6 weeks or 10-12 sessions) and when considering the most consistently reported demographics i.e., women of an aggregated mean age around 40. Heterogeneity in studies makes recommendations beyond this currently difficult. Further research is needed to identify the different elements of TIDiER guidelines [19]. Further clinical trials with longer term follow-up and systematic review-based evidence is required to move recommendations beyond the current evidence.
Further concerns with NICE guidance are their hypothesis that the therapeutic mechanism underpinning PBMT is via local heating is fundamentally inaccurate. Local heating can be a byproduct of the actual mechanism which is primarily photon absorption at the level of the mitochondria, which brings about a cascade of chemical and biological events [57]. Only singe wavelength analysis was included, and we know dual wavelengths are both common and effective, utilised in order to treat a range and depth of tissue [58]. Finally, PBMT analysis was grouped together with all other electrophysical therapies: TENS, PENS, interferential therapy, therapeutic US, TMS, and transcranial direct current stimulation. Therefore, there is considerable potential that PBMT’s positive effects have been diluted by unrelated therapies, especially so as NICE state that “laser” therapy was the intervention with the largest benefit [6].
From an FM viewpoint, the NICE ‘critical’ outcome recommendations do not encompass the whole spectrum of FM symptoms, as seen by OMERACT [59]. The two major domains that have been omitted are fatigue and cognitive function, both of which are known to be extremely intrusive to FM patients [11,60,61], and indeed with PBMT demonstrating efficacy in these same domains [25,26,30,31,35,40,43]. That being said, 13 years on, it could be argued OMERACT’s research standards guidelines are due an update, with the preceding workshop taking place eight years prior [62]. Perhaps at this point in time, the most pragmatic approach, at least in the UK, would be to address any remaining questions that pose an obstacle to being NICE approved in the future. Whilst we acknowledge the complexity of addressing chronic primary pain as a whole, the authors feel that some significant domains have perhaps been overlooked and call for updated guidelines to discuss FM in its own right as it affects a significant proportion of our population alone, with a recent UK epidemiological study estimated 5.4% (more than 1 in 20) UK population being burdened with the condition [63].
Economic data, both then and now, remains scant. NICE had to extrapolate their data from NHS supply chain information in a 2014 low back pain guideline [64]. This cost is potentially over-estimated as they incorporate a Band 5/6/7 Allied Healthcare Professional into their estimate. Bandings may not need to be this senior, for example, with whole-body PBMT a Band 2 Healthcare Assistant would suffice, thus, costing significantly less.
This data corroborates with our proposed hypothesis, that is, that evidence suggests PBMT can drastically and significantly reduce a multitude of FM related symptoms. Our data is compellingly in favour of PBMT as an efficacious and safe treatment in FM. Those aspects that may have not been covered as well amongst the quantitative data have certainly been addressed in the qualitative work assessed. NICE recognise quality data to be vital in guideline development [65], yet in this instance have not proceeded to utilise it towards their latest recommendations.
4.2. Limitations
There were limited consistent details of other demographics outside of age, gender and time with symptoms. There was clinical heterogeneity around the intervention device used and associated protocols i.e., details of frequency, intensity and duration of device use. Further clinical heterogeneity exists in the form and correct application of outcome measures across studies and the correct application of PBM. For instance, whilst PBM has benefits for patients with fibromyalgia, the dosimetry is less clear. Study personnel applying PBM (e.g., medical students) were often not trained in basic photobiology or optical physics; as such, they are not equipped to critique or verify the performance of the products they use and the calculation of doses; they reasonably expect medical devices to perform in accordance with the label. Within the current studies there were identification of dose calculation errors, sometimes caused by believing the marketing material, such as products marketed with a 50 W peak but not the average power (see supplementary file for details), which is used to calculate the dose and the beam area is incorrectly measured by the manufacturer Further to this, authors of manuscripts seem not to verify the dose calculations. Despite this, laboratory and clinical benefits are widely reported, suggesting that the therapeutic window may be large. Many of these papers are more than a decade old. With the introduction of the new Medical Device Regulations (MDR) from the EU, modern and future devices should be closer to the truth. What is missing is official guidance on what to report and how to characterise light sources for PBM, not just individual laser beams but also arrays of lasers or Light-emitting diodes (LEDs). For a full break down and assessment of application of PBM see the supplementary file. Such findings are identified in the wider literature [66].
Statistical heterogeneity was identified as part of the meta-analyses performed. It should also be noted that whilst some the standard deviation of differences were obtained in actual values for some studies, however they estimated using an equation from the Cochrane Reviewer’s handbook. Factors that influence heterogeneity as identified above should be critically considered for past review evidence and past meta-analysis. As both clinical and statistical heterogeneity if not accounted for may distort the true effects of PBMT. Going forwards, inclusion of experiential data can only be an asset to future research and its set up.
A further limitation is the varied use of nomenclature. The term “photobiomodulation” was first used in 1992 [67]. Since this time, there have been hundreds of wide-ranging synonyms for what is essentially the same therapy. In 2014, a consensus meeting between the American Association for Light Therapy and the World Association for Laser Therapy it was decided that all other synonyms including “LLLT” superseded by “PBM” [68]. Subsequently, in the same year, the National Library of Medicine adopted this and re-indexed all preceding work in their database. In spite of this, our searches returned ongoing uses of multiple synonyms even since 2014. NICE were among these. Anecdotally, the issue seems to arise when journals do not utilise PBM expert reviewers – this is a recurrent problem throughout the literature, repeatedly reporting incomplete, inaccurate and unverified irradiation parameters, miscalculation of ‘dose’, and misuse of appropriate light terminology [69]. For instance, the World Association for Laser Therapy (WALT) recommend researchers report dosing in Joules and not Joules per centimetre squared [70] – studies rarely adhere to this. Going forward it is recommended that studies utilise an optical engineer and/or physicist.
4.3. Recommendations for Future Research and Clinical Implications
No studies in the NICE guidance [6], nor in this scoping review, utilised ‘usual care’ as a control group. This would be the recommended control group in future FM research, as this is what NHS leaders will pragmatically want to know. One of the drawbacks here is that the question itself – ‘what is usual care for FM in the UK’ – remains to be answered, and has shown to be considerable disparities across regions [71]. Interestingly, acupuncture is one of the therapies that ‘passed the bar’ for NICE recommendation and the included studies compared this therapy to usual care [6]. Furthermore, we recognise the impact of other non-pharmacological approaches, for instance, the recent benefit of exercise on sleep outcomes [72]. But also, other non-pharmacological approaches can produce variables results, for instance physiotherapy [73]. Therefore, utilising multi-modal therapies is important [74] and considering effect sizes for PMBT compare well to other non-pharmacological treatments [75], identifying PMBT as a part of future trials or complex interventions as important.
There is limited data provided at 6 months follow up and more is needed. Provisional data from current research [24] demonstrates a clinically meaningful pain decrease [55] at this follow up point. However, data using FIQR [31] was not clinically meaningful [76] at this time point. Further research needs to consider longer term assessment with a greater number of measures to establish this.
There is little available literature to suggest that FM patients feel more validated secondary to filling out FM-specific questionnaires. However, it was certainly one of the author’s experiences that these patients appreciated being given specifically the FIQR questionnaire, as it came to light during baseline semi-structured interviews [11] that some had not previously felt validated by neither personal relations nor healthcare professionals. This is certainly something that is mirrored in the results of a recent nationwide questionnaire [71]. One suggestion going forward is incorporating routine FIQR assessments at each clinical contact, not only to improve patient’s feeling of validation, but for both clinician and patient to compare results with previous encounters in order to guide management strategies. FIQR is by far the most frequently administered disease-specific instrument in FM research populations, demonstrating good psychometric properties and available in several languages [4], but again there is little evidence to see that it is being used routinely in clinical practice. The PACFiND study [71] also suggested that referral and care pathways possess significant disparities. The FIQR could potential be used to streamline referral pathways, depending on FIQR severity at the time of assessment, and thus get the patient into the right care pathway in a timely manner.
Throughout this article we have highlighted areas that require further work. This includes whole-body photobiomodulation, as its investigation into chronic primary pain has only relatively recently emerged. There are several reasons why whole-body therapy may prove to be more efficacious than focussed therapy in widespread conditions such as FM, having the propensity to target the postulated widespread mitochondrial dysfunction, reduced capillary supply to muscles, and widespread small-fibre neuropathies [30]. A phenomenon has been recently highlighted as to why the addition of transcranial PBMT via whole-body therapy may be more beneficial in conditions such as FM. Neuroimaging studies have demonstrated that patients with FM exhibit altered thalamic structure and function, and that high-frequency oscillatory activities in specific brain areas are responsible for modulating cognitive and emotional pain modulation, and as such were associated with higher affective pain scores in FM. This may contribute to the persistent perception of pain in FM. Is it thus recommended that therapeutic high quality fully powered interventions be based on manipulating these neural oscillations in order to restore normal thalamocortical activity towards relieving pain in FM [77]. A further paper supports this and describes FM as a neurogenic condition preceding by central dysrhythmic gamma oscillations – the photophysical mechanisms of PBMT have been shown to disrupt these brain patterns, potentially via local resonant interactions [57]. We know, however, from this review that PBMT targets so much more than pain pathways.
In terms of pragmatic assessment towards instituting PBMT into a UK healthcare service, further research is required that considers cost-effectiveness. A recent publication [4] recommends the widely utilised SF-6D and EQ-5D to perform these analyses. However, over and above these, the PROMIS Preference Score (PROPr) is recommended as an alternative in FM as it covers FM-relevant domains such as fatigue and cognition, echoing our concerns about these lacking in the latest NICE guidelines. Qualitative data on the experiences of devices is severely limited and is required to explore mechanistic factors further.
5. Conclusions
It should be noted that although NICE mentions PBMT not ‘making the cut’ this time round, one of the reasons stipulated is lack of cost-effectiveness data. Yet, NICE view this as an ‘important’ factor, not ‘critical’. Going forwards, pragmatically, the authors deem this to be ‘critical’. It is well-known both anecdotally, and other [77], that this will be the question on every NHS manager’s lips, rightly so, in the current climate of our under-funded and under-resourced healthcare environment [78]. As identified in the discussion, our current studies support recommendations for PBMT to be recommended for women around the age of 40 years for sessions that last between 2-6 weeks (or 10-12 sessions) based on the current evidence. Further research is needed to address considerations beyond this recommendation. The aim of future high-quality research will be to make further recommendations to NICE of the efficacy of PBMT in FM specifically. Researchers and clinicians, and those with specialist PBMT expertise, need to work with teams at NICE to simultaneously create cost codes so there are no further delays in making this treatment accessible to those who need it the most.
Author Contributions
Conceptualisation, B.F. and A.S.; methodology, B.F. and A.S.; validation, B.F. and A.S.; formal analysis, B.F. and A.S.; writing-original draft preparation, B.F. and A.S.; writing-review and editing, B.F., A.S., J.C., and A.R.; supervision, A.S. and N.H.
Funding
The author(s) received no financial support for the research and authorship specifically relevant to this manuscript. Publication was supported by University of Birmingham.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgements
The authors thank librarian Holly Austin-Davies and librarian assistant Gareth Sunley (Royal Orthopaedic Hospital, Birmingham, UK) for their comprehensive searches and seeking out difficult-to-locate articles. The authors would like to thank the reviewers for extensive and well-considered comments which allowed significant improvement to this review.
Conflicts of Interest
One of the authors, J.C., is the founder and CEO of THOR Photomedicine. Within the current project he provided a role as a reviewer of the text and contributed after the results were organised, thus limiting the conflict. He is also well versed with academic procedures and requirements. For instance, he has previously published extensive research, supported policy development and advised governments on photomedicine.
References
- Yeh, S.W., et al., Low-level laser therapy for fibromyalgia: A systematic review and meta-analysis. Pain Physician, 2019. 22(3): p. 241-254.
- National Institute for Health and Care Excellence: Guidelines, in Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain. 2021, National Institute for Health and Care Excellence (NICE). Copyright © NICE 2021.: London.
- Boomershine, C.S., A comprehensive evaluation of standardized assessment tools in the diagnosis of fibromyalgia and in the assessment of fibromyalgia severity. Pain Res Treat, 2012. 2012: p. 653714.
- Döhmen, A., et al., Are OMERACT recommendations followed in clinical trials on fibromyalgia? A systematic review of patient-reported outcomes and their measures. Qual Life Res, 2023. 32(6): p. 1521-1536.
- Organization, W.H. ICD-11 for Mortality and Morbidity Statistics. 2023 [cited 2023 11th September]; Available from: https://icd.who.int/browse11/l-m/en#!
- Excellence, N.I.f.H.a.C. Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain. 2021 [cited 2024 3rd March]; Available from: https://www.nice.org.uk/guidance/ng193/chapter/Recommendations.
- Excellence, N.I.f.H.a.C. Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain [H] Evidence review for electrical physical modalities for chronic primary pain. 2021 [cited 2024 8th October ]; Available from: https://www.nice.org.uk/guidance/ng193/evidence/h-electrical-physical-modalities-for-chronic-primary-pain-pdf-9071987013.
- Health, N.N.I.f. and E. Care, Chronic pain (primary and secondary) in over 16s: assessment of all chronic pain and management of chronic primary pain 2021, NICE - National Institute for Health and Care Excellence.
- Kate, F., et al., Qualitative evidence synthesis for complex interventions and guideline development: clarification of the purpose, designs and relevant methods. BMJ Global Health, 2019. 4(Suppl 1): p. e000882.
- England, P.P.T.N. Patient and Public Voice Partners Policy. 2017 [cited 2023 7th October]; Available from: https://www.england.nhs.uk/wp-content/uploads/2017/08/patient-and-public-voice-partners-policy-july-2017.pdf.
- Fitzmaurice, B.C., et al., The Fibromyalgia Decomposition Phenomenon: A Reflexive Thematic Analysis. Behav Sci (Basel), 2024. 14(1).
- Unni, G. and J.H. Steven, Institutionalising an evidence-informed approach to guideline development: progress and challenges at the World Health Organization. BMJ Global Health, 2018. 3(5): p. e000716.
- Peters, M.D.J., et al., Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid Synth, 2022. 20(4): p. 953-968.
- Tricco, A.C., et al., PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med, 2018. 169(7): p. 467-473.
- Excellence, N.I.f.H.a.C. Low-level laser therapy for preventing or treating oral mucositis caused by radiotherapy or chemotherapy (Interventional procedures guidance [IPG615]). 2018 [cited 2020 18th July]; Available from: https://www.nice.org.uk/guidance/ipg615.
- Ltd., T.P. NovoTHOR. 2019-2023 [cited 2021 8th December]; Available from: https://www.novothor.com/?utm_source=google&utm_medium=cpc&keyword=novothor&utm_campaign=602860951&gad=1&gclid=CjwKCAjww7KmBhAyEiwA5-PUSgUI0Ry2inGx2zfW936PictCTP41gfbKRfJXWx3lQ7m5qovrNDs8VBoCnlUQAvD_BwE.
- Magee, K., et al., Implementation of a light therapy team to administer photobiomodulation therapy: A standardized protocol to prevent and treat oral mucositis in the pediatric hematopoietic stem cell transplant population. Pediatr Blood Cancer, 2024. 71(6): p. e30966.
- Pritchard, M., et al., Utilization of Photobiomodulation for the Prevention and Treatment of Oral Mucositis. J Pediatr Hematol Oncol Nurs, 2024. 41(2): p. 107-113.
- Hoffmann, T.C., et al., Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. Bmj, 2014. 348: p. g1687.
- Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, Dagenais P, Gagnon M-P, Griffiths F, Nicolau B, O’Cathain A, Rousseau M-C, Vedel I. Mixed Methods Appraisal Tool (MMAT), version 2018. Registration of Copyright (#1148552), Canadian Intellectual Property Office, Industry Canada.
- Howick, J., Chalmers, I., Glasziou, P., Greenhalgh, T., Heneghan, C., Liberati, A. Moschetti, I., Phillips, B., Thornton, H. (2011). Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) Levels of Evidence (Background Document). Oxford Centre for Evidence-Based Medicine. https://www.cebm.ox.ac.uk/resources/levels-of-evidence/ocebm-levels-of-evidence.
- Shea, B. J., Reeves, B. C., Wells, G., Thuku, M., Hamel, C., Moran, J., Moher, D., Tugwell, P., Welch, V., Kristjannsson, E., Henry, D. A. (2017). AMSTAR 2: A critical appraisal tool for systematic reviews that include rnadomised or non-randomised studies of healthcare interventions, or both. British Medical Journal, 358. [CrossRef]
- PRISMA. PRISMA Flow Diagram 2020; Available from: https://www.prisma-statement.org/prisma-2020-flow-diagram.
- Page, M.J., et al., The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 2021. 372: p. n71.
- Gür, A., et al., Effects of low power laser and low dose amitriptyline therapy on clinical symptoms and quality of life in fibromyalgia: a single-blind, placebo-controlled trial. Rheumatol Int, 2002. 22(5): p. 188-93.
- Gür, A., et al., Efficacy of low power laser therapy in fibromyalgia: a single-blind, placebo-controlled trial. Lasers in medical science, 2002. 17(1): p. 57-61.
- Navarro-Ledesma, S., et al., Short-Term Effects of Whole-Body Photobiomodulation on Pain, Quality of Life and Psychological Factors in a Population Suffering from Fibromyalgia: A Triple-Blinded Randomised Clinical Trial. Pain Ther, 2023. 12(1): p. 225-239.
- Navarro-Ledesma S, C.J.G.-M.A.P.L.B.P., Changes in Circadian Variations in Blood Pressure, Pain Pressure Threshold and the Elasticity of Tissue after a Whole-Body Photobiomodulation Treatment in Patients with Fibromyalgia: A Tripled-Blinded Randomized Clinical Trial. Biomedicines, 2022.
- Navarro-Ledesma, S., et al., Outcomes of whole-body photobiomodulation on pain, quality of life, leisure physical activity, pain catastrophizing, kinesiophobia, and self-efficacy: a prospective randomized triple-blinded clinical trial with 6 months of follow-up. Frontiers in Neuroscience, 2024. 18(pagination): p. Article Number: 1264821. Date of Publication: 2024.
- Fitzmaurice, B.C., et al., Whole-Body Photobiomodulation Therapy Propels the Fibromyalgia Patient into the Recomposition Phase: A Reflexive Thematic Analysis. Biomedicines, 2024. 12(5): p. 1116.
- Fitzmaurice, B.C., et al., Whole-Body Photobiomodulation Therapy for Fibromyalgia: A Feasibility Trial. Behavioral sciences (Basel, Switzerland), 2023. 13(9): p. 717. [CrossRef]
- Dos Santos, R.C., et al., Acute low-level laser therapy effects on peripheral muscle strength and resistance in patients with fibromyalgia. Lasers in medical science, 2020. 35(2): p. 505-510.
- Armagan, O., et al., Long-term efficacy of low level laser therapy in women with fibromyalgia: A placebo-controlled study. Journal of Back and Musculoskeletal Rehabilitation, 2006. 19(4): p. 135-140.
- Ergün, G., E. Atalar, and G. Aydın, Assessment of the efficiency of low level laser therapy in women with primary fibromyalgia syndrome: a randomized, placebo-controlled, double-blind study. Acta Oncologica Turcica. 53(2): p. 288-293.
- Fernández García, R., et al., Using a laser based program in patients diagnosed with fibromyalgia. Reumatologia clinica, 2011. 7(2): p. 94-97.
- MolinaTorres, G., et al., Laser Therapy and Occlusal Stabilization Splint for Temporomandibular Disorders in Patients With Fibromyalgia Syndrome: A Randomized, Clinical Trial. Alternative Therapies in Health and Medicine, 2016. 22(5): p. 23-31.
- Panton, L., et al., Effects of class IV laser therapy on fibromyalgia impact and function in women with fibromyalgia. Journal of Alternative and Complementary Medicine, 2013. 19(5): p. 445-452.
- Tramontana, A., et al., Evaluating integrative approaches for fibromyalgia in physical and rehabilitation medicine (PM&R). Archives of Physical Medicine and Rehabilitation, 2017. 98(10): p. e65-e66.
- Yi Wu, P., et al., Effects of Intravenous Laser Irradiation of Blood on Pain, Function and Depression of Fibromyalgia Patients. Genetics in Medicine, 2018. 6: p. 1-8.
- da Silva, M.M., et al., Randomized, blinded, controlled trial on effectiveness of photobiomodulation therapy and exercise training in the fibromyalgia treatment. Lasers Med Sci, 2018. 33(2): p. 343-351.
- White, P.F., et al., Treatment of drug-resistant fibromyalgia symptoms using high-intensity laser therapy: a case-based review. Rheumatology international, 2018. 38(3): p. 517-523.
- de Souza, R.C.V., et al., Low-level laser therapy and anesthetic infiltration for orofacial pain in patients with fibromyalgia: a randomized clinical trial. Medicina oral, patologia oral y cirugia bucal, 2018. 23(1): p. e65-e71.
- Ruaro, J.A., et al., Low-level laser therapy to treat fibromyalgia. Lasers in medical science, 2014. 29(6): p. 1815-1819.
- Moore, J. and T. Demchak, Treatment of fibromyalgia syndrome with low-level laser therapy. International Journal of Athletic Therapy and Training, 2012. 17(4): p. 28-31.
- Ruaro, J.A., et al., Low-level laser therapy to treat fibromyalgia. Lasers Med Sci, 2014. 29(6): p. 1815-9.
- Diniz, V.H.P., A.D. Vial, and R.T.D. Alves. Effectiveness of blood irradiation by modified intravenous laser (ILIB) on the clinical parameters of fibromyalgia. 2021.
- Gikaro, J.M., et al., Efficacy of electrophysical agents in fibromyalgia: A systematic review and network meta-analysis. Clinical rehabilitation, 2023. 37(10): p. 1295-1310.
- Vayvay, E.S., et al., The effect of Laser and taping on pain, functional status and quality of life in patients with fibromyalgia syndrome: A placebo- randomized controlled clinical trial. Journal of back and musculoskeletal rehabilitation, 2016. 29(1): p. 77-83.
- Honda, Y., et al., Effects of Physical-Agent Pain Relief Modalities for Fibromyalgia Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Pain Res Manag, 2018. 2018: p. 2930632.
- Germano Maciel, D., et al., Low-level laser therapy combined to functional exercise on treatment of fibromyalgia: a double-blind randomized clinical trial. Lasers in medical science, 2018. 33(9): p. 1949-1959.
- Matsutani, L.A., et al., Effectiveness of muscle stretching exercises with and without laser therapy at tender points for patients with fibromyalgia. Clinical & Experimental Rheumatology, 2007. 25(3): p. 410-415.
- Bennett, R.M., et al., The Revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther, 2009. 11(4): p. R120.
- Mannerkorpi, K. and C. Hernelid, Leisure Time Physical Activity Instrument and Physical Activity at Home and Work Instrument. Development, face validity, construct validity and test-retest reliability for subjects with fibromyalgia. Disabil Rehabil, 2005. 27(12): p. 695-701.
- Petrini, L. and L. Arendt-Nielsen, Understanding Pain Catastrophizing: Putting Pieces Together. Frontiers in Psychology, 2020. 11.
- Sadovsky, R. (2002). Clinically importance changes in pain severity on VAS. American Family Physician, 65; 1915-1921.
- Williams, D. A., Arnold, L. M. (2011). Measures applied to the Assessment of Fibromyalgia. Arthritis Care Research, 63 (0 11): S86-S97. [CrossRef]
- Liebert, A., et al., Photophysical Mechanisms of Photobiomodulation Therapy as Precision Medicine. Biomedicines, 2023. 11(2): p. 237.
- González-Muñoz, A., et al., Efficacy of Photobiomodulation Therapy in the Treatment of Pain and Inflammation: A Literature Review. Healthcare, 2023. 11(7): p. 938.
- Mease, P., et al., Fibromyalgia syndrome module at OMERACT 9: domain construct. J Rheumatol, 2009. 36(10): p. 2318-29.
- Bell, T., et al., Meta-analysis of cognitive performance in fibromyalgia. J Clin Exp Neuropsychol, 2018. 40(7): p. 698-714.
- Vincent, A., et al., Beyond pain in fibromyalgia: insights into the symptom of fatigue. Arthritis Research & Therapy, 2013. 15(6): p. 221.
- Mease, P.J., et al. OMERACT 7 Workshop Fibromyalgia Syndrome. 2005.
- Fayaz, A., et al., Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ open, 2016. 6(6): p. e010364.
- Excellence, N.I.f.H.a.C. Low back pain and sciatica in over 16s: assessment and management. NG59 2014 [cited 2024 19th December]; Available from: https://www.nice.org.uk/guidance/ng59.
- NICE. Methods for the development of NICE public health guidance (third edition) [PMG4]. 2012 [cited 2025 8th January ]; Available from: https://www.nice.org.uk/process/pmg4/chapter/reviewing-the-scientific-evidence.
- Hadis, M. A., Zainal, S. A., Holder, M. J., Carroll, J. D., Cooper, P. R., Milward, M. R. Palin, W. M. (2016). The dark art of light measurement: accurate radiometry for low-level light therapy. Lasers Medical Science, 10; 789-809.
- Van Breugel, H.H. and P.R. Bär, Power density and exposure time of He-Ne laser irradiation are more important than total energy dose in photo-biomodulation of human fibroblasts in vitro. Lasers Surg Med, 1992. 12(5): p. 528-37.
- 2014 NAALT/WALT Meeting Nomenclature Breakout. 2015 [cited 2024 19th December]; Available from: https://www.naalt.org/whitepapers/2014-naalt-walt-meeting-nomenclature-breakout/.
- Hadis, M.A., et al., The dark art of light measurement: accurate radiometry for low-level light therapy. Lasers Med Sci, 2016. 31(4): p. 789-809.
- Bjordal, J.M., et al., A systematic review with meta-analysis of the effect of low-level laser therapy (LLLT) in cancer therapy-induced oral mucositis. Support Care Cancer, 2011. 19(8): p. 1069-77.
- Wilson, N., et al., UK healthcare services for people with fibromyalgia: results from two web-based national surveys (the PACFiND study). BMC Health Serv Res, 2022. 22(1): p. 989.
- Hudson, Jemma, Imamura, Mari, Robertson, Clare, Whibley, Daniel, Aucott, Lorna, Gillies, Katie, Manson, Paul, Dulake, Debra, Abhishek, Abhishek, Tang, Nicole K. Y., Macfarlane, Gary and Brazzelli, Miriam (2025) Effects of pharmacological and non-pharmacological interventions for the management of sleep problems in people with fibromyalgia: systematic review and network meta-analysis of randomised controlled trials. Arthritis Care & Research. (In Press) ISSN 2151-464X. [CrossRef]
- Hong-Baik, I., Úbeda-D’Ocasar, E., Cimadevilla-Fernández-Pola, E., Jiménez-Díaz-Benito, V., & Hervás-Pérez, J. P. (2023). The Effects of Non-Pharmacological Interventions in Fibromyalgia: A Systematic Review and Metanalysis of Predominants Outcomes. Biomedicines, 11(9), 2367. [CrossRef]
- Hernando-Garijo I, Jiménez-del-Barrio S, Mingo-Gómez T, Medrano-de-la-Fuente R, Ceballos-Laita L. Effectiveness of non-pharmacological conservative therapies in adults with fibromyalgia: A systematic review of high-quality clinical trials. Journal of Back and Musculoskeletal Rehabilitation. 2022;35(1):3-20. [CrossRef]
- Kundakci, Buraka,b,c,*; Kaur, Jaspreeta,b,d; Goh, Siew Lie; Hall, Michellea,b,f,g; Doherty, Michaela,b,f; Zhang, Weiyaa,b,f; Abhishek, Abhisheka,b,f. Efficacy of nonpharmacological interventions for individual features of fibromyalgia: a systematic review and meta-analysis of randomised controlled trials. PAIN 163(8):p 1432-1445, August 2022. |. [CrossRef]
- Surendran, S., Mithun, C. B. (2018). FRIO647 estimattion of minimum clinically important difference in fibromyalgia for fiqr using bpi as anchor measure. Annals of the Rheumatic Diseases, 77, 845. [CrossRef]
- Lim, M., et al., Increased Low- and High-Frequency Oscillatory Activity in the Prefrontal Cortex of Fibromyalgia Patients. Front Hum Neurosci, 2016. 10: p. 111.
- McCabe, C., K. Claxton, and A.J. Culyer, The NICE Cost-Effectiveness Threshold. PharmacoEconomics, 2008. 26(9): p. 733-744.
- Al-Janabi, H., I. Williams, and M. Powell, Is the NHS underfunded? Three approaches to answering the question. Journal of the Royal Society of Medicine, 2023. 116(12): p. 409-412.
Table 6.
Summary of systematic reviews and meta-analyses; depicting aims, methods, outcome measures, results pertaining to FM and PBMT, author comments and conclusions.
Table 6.
Summary of systematic reviews and meta-analyses; depicting aims, methods, outcome measures, results pertaining to FM and PBMT, author comments and conclusions.
| Paper | Aims, design, outcomes and AMSTAR2 rating | Results synthesis pertaining to FM and PBMT | Author comments/conclusions |
|---|---|---|---|
| Gikaro et al. (2023) [47] Systematic review and network meta-analysis (n = 3045) |
To examine effectiveness of electrophysical agents in FM (looked at 25 treatments) 54 studies, RCTs comparing therapy to control/placebo/no treatment Primary outcomes: pain, functional status, mood Pain assessment: VAS, NPRS, BPI, Likert scale Functional assessment: Original or revised FIQ Mood assessment: Beck’s Depression Inventory, Depression Anxiety Stress Scale-21, Hamilton Depression Rate Scale, Hamilton Depression and Anxiety Scale, HADS – depression domain, Montgomery Asberg Rating Scale AMSTAR2 rating: High |
Node-splitting method showed significant local inconsistency for comparisons between placebo and PBMT (p=0.001), PBMT and no treatment (p=0.000) PBMT comparison to placebo Pain (47 studies): pooled SMD (95% CI) = -1.18 (-4.20 to 1.85), p=0.446, likelihood of being best agent 0.1%, worst agent 0%, surface under the cumulative ranking (SUCRA) 80% Function (31 studies) and mood (26 studies): pooled SMD (95% CI) -0.57 (-1.66 to 0.52), p=0.304, likelihood of being best agent 0.3%, worst agent 0.1%, SUCRA 60%. Consistency model did not show significant improvement after intervention for PBMT alone, but combination of PBMT and exercise therapy had highest SUCRA (80%) Mood: SUCRA revealed PBMT amongst agents most likely to be suitable for managing mood – 70% Side-split analysis from network meta-analysis examining effects expressed as beta coefficients (standard error) PAIN Placebo c/w PBMT: direct -0.86 (0.98), indirect -7.37 (1.72), difference 6.50 (1.98), p=0.001 Amitriptyline c/w PBMT: direct -1.05 (1.94), indirect -4.51 (4.05), difference 3.47 (4.49), p=0.442 Exercise c/w PBMT: direct -3.71 (1.91), indirect -0.14 (2.07), difference -3.57 (2.82), p=0.206 Lidocaine c/w PBMT: direct -0.18 (1.92), indirect -4.93 (632.37), difference 4.75 (632.39), p=0.994 PBMT c/w no treatment: direct 9.54 (1.60), indirect 0.96 (1.05), difference 8.57 (1.92), p=0.000 PBMT c/w occlusal splint: direct -0.20 (1.92), indirect 4.93 (633.02), difference -5.13 (633.02), p=0.994 PBMT c/w taping: direct -0.17 (1.91), indirect 6.13 (3.97), difference -6.30 (4.40), p=0.153 FUNCTION Placebo c/w PBMT: direct -0.89 (0.61), indirect 0.88 (1.29), difference -1.77 (1.42), p=0.213 Amitriptyline c/w PBMT: direct -0.67 (1.20), indirect 2.24 (2.43), difference -2.92 (2.71), p=0.282 Exercise c/w PBMT: direct 1.83 (1.10), indirect -1.27 (1.10), difference 3.09 (1.55), p=0.047 PBMT c/w no treatment: direct 0.57 (1.23), indirect 1.01 (0.99), difference 1.47 (2.54), p=0.562 |
PBMT (and microcurrent) had the highest probability of being among the best modalities for pain relief PBMT (and microcurrent, and transcranial magnetic stimulation) had highest probability of being the best electrophysical agents for managing mood disorders Low-moderate quality evidence that PBMT (and microcurrent, and transcranial magnetic stimulation) are the most effective electrophysical agents for improving at least one outcome in FM |
| Honda et al. (2018) [49] Systematic review and meta-analysis of RCTs (n = 470) |
To investigate the effects of physical-agent modalities (PBMT, thermal therapy, electromagnetic field therapy, TENS) for pain relief in FM. 5 PBMT RCTs out of 11 RCTs analysed Primary outcome: pain relief (VAS) Secondary outcomes: NTP (subjective), FIQ, QoL scores (SF-36) AMSTAR2 rating: Low |
PBMT comparison to control group PAIN No reduction (mean difference: -4.00; 95% CI -23.4 to 15.4, p=0.69) NTP Significant reduction (-2.21; 95% CI -3.51 to -0.92, I2=42%, p=0.0008) FIQ Significant reduction (-4.35; 95% CI -6.69 to -2.01, I2=62%, p=0.03) QoL SF-36 No significant difference (5.80; 95% CI -4.72 to 16.32, p=0.28) |
PBMT had a partial effect on pain relief in FM patients, and this beneficial effect may have a positive influence on FM patients’ health status |
| Yeh et al. (2019) [1] Systematic review and quantitative meta-analysis (n = 325) |
To determine the efficacy of PBMT on patients with FM Analysed all published RCTs (n = 9), evaluating effect of PBMT on FM (with or without exercise programme) Primary outcomes: FIQ, pain severity, NTP Secondary outcomes: fatigue, stiffness, anxiety, depression Pain assessment methods: i. extraction of “pain” subitem from FIQ (0-10), ii. 5-point Likert scale (0 = none → 4 = extreme), iii. VAS NTP: i. points that were reported by patients as being painful, ii. more rigorous definition = patients felt pain at a pressure ≤2.6kgf/cm2 Fatigue: i. extraction of “fatigue” subitem from FIQ (0-10), ii. Likert score Stiffness: i. extraction of “stiffness” subitem from FIQ (0-10), ii. Likert score for ‘morning stiffness’ Anxiety: extraction of “anxiety” subitem from FIQ (0-10) Depression: extraction of “depression” subitem from FIQ (0-10) AMSTAR2 rating: Low |
Note: of the 9 RCTs, only included here the relevant ones to this scoping review. Table 1 and Table 2 describe individual study results. Included here also as extra results and/or presented differently, derived from pooled meta-analysis PBMT comparison to placebo FIQ (p<0.00001) Monowavelength PBMT: overall significant improvement compared with placebo (pooled SMD: 1.16; 95% CI 0.64-1.69, I2 = 47%) Amargan 2006: mean change 7±7.59; placebo 1.75±7.37 (SMD 0.68; 95% CI -0.03-1.40) Garcia 2011: mean change 10.56±10.97; placebo 1.93±8.96 (SMD 0.84; 95% CI 0.10-1.58) Gur 2002: mean change 23.25±8.58; placebo 9.64±6.63 (SMD 1.75; 95% CI 1.09-2.41) Ruaro 2014: mean change 18.6±9.64; placebo 5.2±8.66 (SMD 1.40; 95% CI 0.40-2.40) Combined PBMT/LED phototherapy: 1 RCT, significant improvement da Silva 2018: mean change 0.06±0.06; placebo 0.01±0.02 (SMD 1.10; 95% CI 0.43-1.77) PAIN SEVERITY (p=0.0009) Monowavelength PBMT: overall significant improvement compared with placebo (pooled SMD: 1.18; 95% CI 0.82-1.54, I2 = 0%) Garcia 2011: mean change 2.31±2.1; placebo 0.73±1.82 (SMD 0.78; 95% CI 0.05-1.52) Gur 2002: mean change 1.8±0.51; placebo 1±0.63 (SMD 1.37; 95% CI 0.75-2.00) Gur 2002: mean change 1.82±0.54; placebo 1.04±0.71 (SMD 1.21; 95% CI 0.53-1.89) Ruaro 2014: mean change 2.7±1.14; placebo 1.1±1.16 (SMD 1.33; 95% CI 0.34-2.32) Combined PBMT/LED phototherapy: 1 RCT, significant improvement (larger effect than monowavelength) da Silva 2018: mean change 0.62±0.08; placebo 0.14±0.03 (SMD 7.79; 95% CI 5.89-9.69) NTP (p=0.002) Monowavelength PBMT: overall significant improvement compared with placebo (pooled SMD: 1.01; 95% CI, 0.49-1.52, I2 = 49%) Amargan 2006: mean change 1.87±1.55; placebo 1.06±1.63 (SMD 0.50; 95% CI -0.21-1.20) Gur 2002: mean change 7.52±2.82; placebo 3.9±2.77 (SMD 1.27; 95% CI 0.66-1.99) Gur 2002: mean change 6.55±2.79; placebo 4.15±3.65 (SMD 0.72; 95% CI 0.08-1.37) Ruaro 2014: mean change 4.3±1.74; placebo 1.4±1.16 (SMD 1.88; 95% CI 0.79-2.97) Combined PBMT/LED phototherapy: 1 RCT, significant improvement (larger effect than monowavelength) da Silva 2018: mean change 0.54±0.08; placebo 0.05±0.09 (SMD 5.64; 95% CI 4.20-7.08) FATIGUE (p<0.00001) Monowavelength PBMT: overall significant improvement compared with placebo (pooled SMD: 1.4; 95% CI, 0.96-1.8) Garcia 2011: mean change 4.32±1.28; placebo 2.01±2.48 (SMD 1.15; 95% CI 0.38-1.92) Gur 2002: mean change 1.8±0.79; placebo 0.76±0.65 (SMD 1.42; 95% CI 0.79-2.04) Gur 2002: mean change 1.73±0.84; placebo 0.06±0.78 (SMD 2.02; 95% CI 1.24-2.79) Ruaro 2014: mean change 2.1±1.52; placebo 0.8±1.28 (SMD 0.89; 95% CI -0.04-1.81) Combined PBMT/LED phototherapy: 1 RCT, significant improvement da Silva 2018: mean change 0.08±0.1; placebo 0.02±0.04 (SMD 0.77; 95% CI 0.13-1.42) STIFFNESS (p<0.0001) Monowavelength PBMT: overall significant improvement compared with placebo (pooled SMD: 0.92; 95% CI, 0.36-1.48) Amargan 2006: mean change 0.62±0.48; placebo 0.56±0.65 (SMD 0.10; 95% CI -0.59-0.80) Gur 2002: mean change 1.6±0.75; placebo 0.76±0.68 (SMD 1.15; 95% CI 0.55-1.76) Gur 2002: mean change 1.45±0.68; placebo 0.69±0.65 (SMD 1.12; 95% CI 0.45-1.79) Ruaro 2014: mean change 1.7±1.33; placebo -0.2±1.2 (SMD 1.44; 95% CI 0.43-2.44) Combined PBMT/LED phototherapy: 1 RCT, significant improvement da Silva 2018: mean change 0.11±0.07; placebo 0.03±0.02 (SMD 1.52; 95% CI 0.81-2.44) ANXIETY (p<0.00001) Monowavelength PBMT: overall significant improvement compared with placebo (pooled SMD: 1.46; 95% CI, 0.45-2.47) Ruaro 2014: mean change 2.2±1.18; placebo 0.5±1.05 (SMD 1.46; 95% CI 0.45-2.47) Combined PBMT/LED phototherapy: 1 RCT, significant improvement da Silva 2018: mean change 0.08±0.06; placebo 0.0±0.02 (SMD 1.75; 95% CI 1.01-2.49) DEPRESSION (p=0.001) Monowavelength PBMT: overall significant improvement compared with placebo (pooled SMD: 1.46; 95% CI, 0.93-2.00) Gur 2002: mean change 7.76±4.2; placebo 2.27±3.18 (SMD 1.45; 95% CI 0.82-2.08) Ruaro 2014: mean change 1.8±1.16; placebo 0±1.16 (SMD 1.49; 95% CI 0.47-2.50) Combined PBMT/LED phototherapy: 1 RCT, no significant improvement da Silva 2018: mean change 0.16±0.12; placebo 0.08±0.17 (SMD 0.53; 95% CI -0.10-1.16) |
PBMT is an effective, safe, and well-tolerated treatment for FM. Low-to-middle methodological quality of studies, heterogeneity between groups and PBMT delivery. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



