
Submitted:
08 May 2025
Posted:
09 May 2025
You are already at the latest version
Abstract
(1) Background: In the absence of locally validated tools, the CHA2DS2-VA score is suggested as a substitute for CHA2DS2-VASc score. This study compared potential discrepancies between these scores; (2) Methods: observational, retrospective, and community-based study included a cohort of 3,370 patients with new diagnosis of atrial fibrillation (AF) between January 01-2015 and December 31-2024; (3) Results: AF prevalence was 8.4%, significantly higher in men. Mean age was 80.1 (SD±6.24) years. Women (42.8%) were older (80.9 SD±6.1 vs. 79.5 SD±6.23; p < 0.001). Men had more diabetes mellitus, peripheral vascular disease, coronary artery disease, and chronic ob-structive pulmonary disease, as well as a higher Charlson Comorbidity Index. Con-versely, women exhibited a higher proportion ≥75 years, cognitive impairment, dyslipidemia, and higher stroke risk as assessed by the CHA2DS2-VASc score (p < 0.001), but not by the CHA2DS2-VA score (p = 0.071). The CHA2DS2-VA reduced the sex-based risk stratification differences, and only 3.2% of women were re-classified as being at very low risk (CHA2DS2-VA < 2); (4) Conclusions: The CHA2DS2-VA exhib-ited comparable predictive accuracy for thromboembolic events, with no sex-based disparities in the selection of ACO treatment modality. The clinical utility of CHA2DS2-VA remains a subject of ongoing debate.
Keywords:
epidemiological studies
; CHA2DS2-VASc score
; stroke-risk
; sex
; anticoagulation.
; atrial fibrillation
1. Introduction
Risk stratification for stroke and systemic embolism is essential in the clinical management of patients with atrial fibrillation (AF). Among patients with AF, there is a wide variability in the risk of thromboembolic events regardless of the temporal pattern of AF. Given this substantial risk, oral anticoagulation is advised for all eligible patients, except those at low risk of incident stroke or thromboembolism. Numerous scores for stroke risk stratification in AF have been proposed [1] over the past 15 years and, in general, these various risk scores showed largely similar discriminative performance. The selection of the CHA2DS2-VASc score as a reference for oral anticoagulant (OAC) prescription guidelines in AF is attributed to its capacity for accurate identification of patients at genuinely low thromboembolic risk. This discriminatory power in defining a truly low-risk cohort has been a key factor in its adoption by clinical practice guidelines [2]. The high prevalence of AF and the severe consequences of stroke require increased efforts to identify patients with AF, even if asymptomatic [3]. There is also a need for user-friendly risk scores to guide appropriate decisions on anticoagulation across a wide range of subjects, including the more frail, multi-morbid and clinically complex patients [4]. A detailed analysis of the components of the CHA2DS2-VASc score identified age and history of prior stroke as the strongest predictors of thromboembolism and stroke in AF patients. However, there has been debate regarding the actual value and significance of female sex in this context. Recent studies [5,6,7] have highlighted that women with atrial fibrillation face a greater risk of stroke compared to men; and the female sex appears to act more as a 'risk modifier' rather than an independent risk factor. This effect is particularly pronounced in older women and when combined with other stroke risk factors. Consequently, these findings hold significant and timely value for supporting the implementation of the CHA₂DS₂-VASc score in everyday clinical practice.
The 2024 ESC/EACTS Guidelines on AF [8] introduced a significant modification to stroke risk assessment for oral anticoagulation initiation. Specifically, in the absence of locally validated risk stratification tools, the CHA2DS2-VA score is indicated as a replacement for the CHA2DS2-VASc score. This substitution is supported by substantial contemporary evidence indicating the appropriate application of oral anticoagulation using identical treatment thresholds irrespective of patient gender. Consequently, the CHA2DS2-VA score excludes gender as a risk factor based on the premise that female sex does not independently contribute to anticoagulation choices but rather acts as a risk modifier, mainly in older individuals who would already meet criteria for anticoagulation [9]. This adaptation to the CHA2DS2-VA score aims to improve the accuracy of stroke risk assessment and encourage broader adoption of appropriate oral anticoagulation in AF patients, employing uniform treatment cut-offs across genders [10]. This study aims to compare and evaluate potential discrepancies or variations in thromboembolic risk stratification by sex when employing the CHA2DS2-VA score versus the CHA2DS2-VASc score in a contemporary and global cohort of patients with prevalent AF.
2. Materials and Methods
2.1. Study Design
The "Gender perspective on cardiovascular diseases in the Terres de l'Ebre" (GECA-TE) project is being conducted as a doctoral thesis within the prestigious Biomedicine PhD Program at the Universitat Rovira i Virgili. This doctoral research project aims to comprehensively explore the existence and nature of sex-related differences in various aspects of cardiovascular health specifically within the Terres de l'Ebre geographical area; and it seeks to contribute to a more nuanced understanding that can inform more effective prevention, diagnosis, and treatment strategies tailored to sex.
This was an observational, retrospective, and community-based study of a cohort of 40,077 general population 65-90 years between January 01-2015 and December 31-2024 without a prior diagnosis of atrial fibrillation or stroke. The protocol received ethics evaluation and approval from the Ethical Committee of Jordi Gol University Institute of Primary Care Research with registration number 24/187-P.
2.2. Study Scope
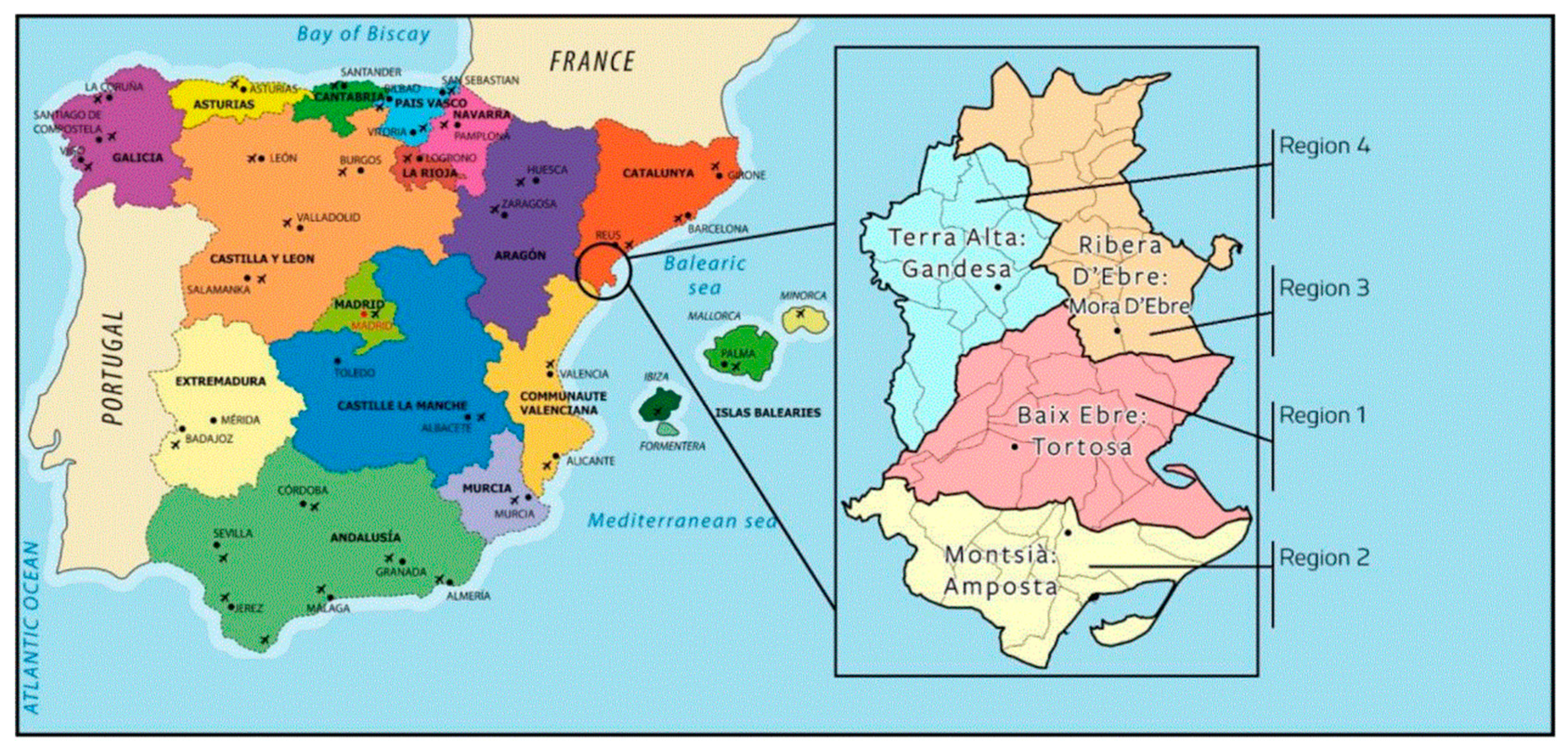
The study was carried out in Terres de l'Ebre (Health Region Terres de l’Ebre, Appendix A1), located in the southern part of Catalonia (Spain). It includes 178,112 inhabitants (49.6% women) across 54 municipalities with an average of 53.8 inhabit-ants/km2 vs 241.8 inhabitants/km2 in Catalonia [11]. It shows the ageing of the population, with an ageing index (159.5) higher than that of Catalonia (131.3) and Spain (118.4) [12]. This index was obtained by the ratio between the population over 65 years of age and the population under 15 years of age per 100 inhabitants. The population aged 65 years or older represents 31.1% of the overall population. The population in the study has a lower average income than the general population in Catalonia (77.4% vs. 100% per capita) [13,14].
The territory is made up of 4 counties with 11 primary care teams (EAPs), managed by the Catalan Health Institute (ICS), Department of Health (CatSalut). Specialized care is received at the reference hospital located in Tortosa, “Hospital Verge de la Cinta”, which is publicly managed by the ICS. The EAPs (Primary care Teams) are organized as independent clinical functional teams. The majority of the census population in the territory (98.2%) has an active Shared Health Record of Catalonia (HCC3) available digitally for continuous care monitoring from any center.
2.3. Data Collection and Information Sources
The clinical background data were obtained retrospectively from a computerized database, provided to the principal investigator by the Information and Communication Technology Department from the minimum basic dataset at hospital discharge (CMBD-HA) register using the specific International Classification of Diseases (10th version; ICD-10) in a fully encrypted format. The particular data sets utilized for this project were as follows:
1. The HCC3 Patient Episode Dataset for Catalonia (CatSalut, Health Department), which includes demographic and clinical data on all daily inpatient and outpatient admissions in Catalonian hospitals.
2. The 11 EAPs shared a clinical information database for all general practice (E-cap, HCC3) and hospital (E-sap) interactions, including clinical data, symptoms, investigations, diagnoses, comorbidities, prescribed medications, referrals to secondary and tertiary care, and status (alive/dead). Pharmacological variables were collected from the SIRE (Catalan acronym for Integrated Electronic Prescription System).
Data on these factors were collected automatically when possible, or manually otherwise.
2.4. Study Population
Initially, the study included people ≥ 65-90 years-old, resulting in 40,077 individuals. The primary endpoint of this study was the new diagnosis of atrial fibrillation between January 1/2015 and December 31/2024. Secondary outcomes included the evaluation of cognitive impairment, cardiovascular comorbidities, and oral anticoagulation treatment. According to the 2024 ESC/EACTS Guidelines on Atrial Fibrillation regarding the periodic reassessment of thrombotic risk, both the CHA2DS2-VASc and CHA2DS2-VA scores were updated. The null hypothesis of this investigation was that there are no statistically significant differences between the two risk scores, nor are there significant differences in these scores when stratified by sex.
2.5. Inclusion and Exclusion Criteria:
2.5.1. Inclusion Criteria:
Patients 65-90 years old, active medical records in any of the health centres with information accessible through the shared history (HCC3), without prior AF or stroke, residence in the territory and assignment to any of the territory’s primary are teams (EAPs). The non-availability or loss of accessibility to the information necessary for the study was considered as a reason for exclusion.
2.5.2. Exclusion Criteria:
Previous diagnosis of AF and/or stroke, pacemaker or defibrillator wearer, absence of or lack of access to individual or their clinical records for any reason, and/or residence outside the Terres de l'Ebre.
2.6. Variables
The information on AF and co-morbidities relevant to cardiovascular risk were obtained until loss-to-follow-up, date of death, or 31-December-2024 whichever occurred first. Atrial fibrillation was diagnosed according to the guidelines of the European Society of Cardiology. A cardiologist was consulted when consensus was not reached. Patients were classified according to the presence of AF. In cases of AF, diagnosed during the follow-up period, data were extracted at the time of AF diagnosis or until the end of follow-up. Data for patients who did not present AF during follow-up were obtained according to the mean during follow-up:
1/ Cardiovascular risk factors and diagnostics using specific International Classification of Diseases (ICD–10) code prefixes for cerebrovascular disease (ischemic stroke or transient ischemic attack, I63, G45), heart failure (I50-51), ischemic heart disease (stable or unstable angina, percutaneous coronary intervention, coronary artery bypass grafting or myocardial infarction) (I20-I25), hypertension (I10–I15), hypercholesterolemia (E78), diabetes mellitus (E10–E14), body mass index (BMI), chronic kidney disease (CKD) (N18) and estimated glomerular filtration rate (eGFR ml/min/1.73 m2).
2/ Clinical scores: Charlson Comorbidity Index to assess a patient's comorbidity burden, CHA2DS2-VASc and CHA2DS2-VA, and Pfeiffer Short Mental Status Questionnaire score. The annual stroke risk estimation was calculated according to CHA2DS2-VASc and CHA2DS2-VA scores [15].
3/ Antiplatelet and/ oral anticoagulation treatment.
4/ Vital status (dead/alive) at the end of the study. All participants were followed from 1-January-2015 until 31-December-2024, loss to-follow-up, or date of death, whichever occurred first.
2.7. Statistical Analysis
The characteristics of the population were defined through a descriptive statistical analysis. Baseline characteristics are presented as counts and percentages, mean and standard deviation (SD) for normally distributed continuous variables, or median for non-normally distributed continuous variables, as appropriate. Quantitative variables were examined with Student's t-distribution for independent samples while qualitative variables were analyzed with the chi-square distribution according to bivariate analysis for normal distributions.
The stroke incidence density/1000 people/year and the registered prevalence of cognitive decline were calculated for each group. The incidence rate was calculated in person-years, the denominator was the sum of the length of time for which each person was observed, totalled for all persons. 2-sided p-value <0.05 was considered statistically significant. All statistical analyses were conducted using IBM SPSS Statistics version 21.0.
3. Results
Table 1 presents the baseline characteristics of 40,077 individuals aged 65-90 years enrolled in a study investigating new-onset atrial fibrillation. The mean age of the study population was 77.4 years (SD±6.60). Women constituted 51.3% and were significantly older compared to men (77.6 SD±6.63 vs 77.2 SD±6.56; p < 0.001). Significant sex-based differences were observed in the prevalence of cardiovascular diseases and risk factors. Men presented with a higher prevalence of atrial fibrillation, heart failure, diabetes mellitus, stroke, vascular peripheral disease and coronary artery disease, chronic kidney, and chronic obstructive pulmonary disease (COPD), and a higher risk of stroke as measured by the CHA2DS2-VA score (p < 0.001). Conversely, women had a higher prevalence of cognitive impairment and dyslipidemia; a higher risk of stroke as measured by the CHA2DS2-VASc score (p < 0.001); received less anticoagulant treatment; had fewer average hospital visits; and experienced higher mortality.
Table 2 presents the baseline characteristics of a cohort of 3,370 patients who received a diagnosis of atrial fibrillation during the study's period. The mean follow-up duration for this cohort was 26.16 (SD±20) months. The mean age of the study cohort was 80.1 years (SD±6.24). Women constituted 42.7% and were significantly older compared to men (80.9 SD±6.1 vs 79.5 SD±6.23; p < 0.001). Significant sex-based differences were observed in the prevalence of cardiovascular risk factors. Men presented with a higher prevalence of aged 65 to 74 years, diabetes mellitus, vascular peripheral diasease and coronary artery disease, and chronic obstructive pulmonary disease; and a higher higher predicted mortality rate as measured by Charlson index. Conversely, women had a higher prevalence of aged ≥75 years, cognitive impairment, and dyslipidemia; a higher risk of stroke as measured by the CHA2DS2-VASc score (p < 0.001), but not if measured by CHA2DS2-VA (p = 0.071).
Table 3 shows how suppressing the sex variable leads to a redistribution of women into a lower risk stratification, thereby aligning it with the proportion of the population in each risk stratum as determined by the CHA₂DS₂-VASc for men. This equalizes the population risk distribution by removing an overestimation of risk in women, notably in the low-risk segment, thus classifying the population into a lower risk stratum. As a result, 46 (3.2%) women are excluded from the range where anticoagulation initiation is indicated, and there was no change in the male variable's outcomes. Using the CHA2DS2VASc, the proportion of men with a score <4 is significantly higher, while above a score of 5 the proportion of women is significantly higher. In contrast, through the use of CHA2DS2VA, 46 women (3.2%) are identified with a score <2, with the differences disappearing in the remaining strata except in score 5 where the proportion of men is significantly higher.
Table 4 shows the incidence rate per 100 person-years by CHA2DS2VASc vs CHA2DS2VA according to the registered strokes in the study period. The follow-up time was counted from the date on which atrial fibrillation was diagnosed until the end of the study or withdrawal from it due to the patient's death. The mean follow-up time was 26.16 (SD±20) months. By decreasing the proportion included in the high strata, there is an increase in the incidence density above the score ≥5 with the CHA2DS2VA scale.
4. Discussion
In the cohort of 3,370 patients newly diagnosed with atrial fibrillation, the main findings were: 1) an average age of 80.1 years, notably higher than in many other atrial fibrillation studies [16,17]; 2) an 8.4% prevalence of AF, which was significantly higher in men; and 3) comparable performance of the CHA₂DS₂-VA and CHA₂DS₂-VASc scores in predicting ischemic stroke. The application of the CHA2DS2-VA score substantially mitigated the profile differences in sex-based thromboembolic risk stratification observed with the CHA2DS2-VASc score, and only a small fraction of women (3.2%) were categorized as being at a very low risk (<2) of stroke to warrant withholding oral anticoagulants.
The disparities in the prevalence of cardiovascular diseases or risk factors between women and men were more noteworthy in the general population (Table 1) compared to those observed within the atrial fibrillation population (Table 2). This suggests that the previously reported sex-based differences in thromboembolic risk may no longer be evident in contemporary cohorts of patients with AF. The finding that women in this study were significantly older (average 80.9 years) compared to men (average 79.5 years) aligns with several studies suggesting that women tend to develop atrial fibrillation around 5 to 10 years later than men on average. In studies on very elderly populations, the trend often shifts towards a higher proportion of women, in contrasts with the male predominance often observed in younger atrial fibrillation populations, underscoring the importance of considering age when analyzing gender differences in this condition.
The age is a significant predictor of various health events and responses to treatment. The high average age of the current cohort suggests that its findings will be particularly relevant to understanding and managing atrial fibrillation in the very elderly, a group that may have different disease characteristics and treatment responses compared to younger elderly individuals. Atrial fibrillation in the very elderly can frequently be asymptomatic or present with non-specific symptoms potentially leading to underdiagnosis and delayed treatment, which could increase the risk of adverse outcomes. In this advanced age group, patients are more likely to have multiple comorbidities such as high blood pressure, coronary artery disease, heart failure, obesity and chronic kidney disease, which can contribute to the development and progression of atrial fibrillation; and have a negative impact on survival [19]. The risk of serious complications, particularly stroke and systemic embolism, is substantially elevated in very elderly individuals with atrial fibrillation, making the decision regarding anticoagulation therapy a critical aspect of management. This decision requires a careful balance between the risk of thromboembolism and the increased risk of bleeding often associated with anticoagulants in older adults, especially considering potential frailty and cognitive impairment. Rhythm control strategies, which aim to restore and maintain a normal heart rhythm, might be less effective in this age group and could carry a higher risk of adverse effects from antiarrhythmic medications. Non-pharmacological interventions like catheter ablation might be considered in carefully selected patients. The presence of frailty and cognitive decline can further complicate management by affecting medication adherence and the ability of patients to participate in treatment decisions. The growing prevalence of multimorbidity and AF significantly burdens global healthcare systems. In addition, three-quarters of atrial fibrillation patients take at least five medications. To develop effective strategies, improve patient outcomes, and address the burden of AF, it is essential to understand the relationship between these conditions.
Our study included the comorbidities of the CHA2DS2-VASc scale and not all those defined by EHRA-PATHS [16] as relevant in patients with AF. Based on the prevalence of specific comorbidities, the modification of the risk calculation from the CHA2DS2-VASc to the CHA2DS2-VA scale resulted in a one-point decrease (sex-woman variable: 1) in the women's group. The CHA2DS2-VA score exhibited comparable predictive accuracy for thromboembolic events to the established CHA2DS2-VASc score. Although the novel scoring system refined the overall assessment of thromboembolic risk, only a small fraction of women (3.2%) were categorized as being at a low risk (<2) of stroke to warrant withholding oral anticoagulants based on this revised stratification. Given their comparable performance, the non-sex-based CHA2DS2-VA score may simplify the initial decision-making process for initiating OAC in patients with AF and would be inclusive of individuals who are "non-binary, transgender, or are undergoing sex hormone therapy[20].
Moreover, it is unclear whether this decrease in thromboembolic risk is associated with a decrease in overall cardiovascular risk related to the comorbidities, since the CHA2DS2-VA scale is characterized by accounting for risk factors in a binary manner and the cumulative number of diseases rather than the overall underlying complexity of multimorbidity [19,21]. Due to significant advantages in big data processing, artificial intelligence is increasingly being integrated into risk stratification and clinical decision support systems for atrial fibrillation (AI) patients. Notably, models employing AI have demonstrated enhanced performance in predicting stroke risk when compared to the conventional CHA2DS2-VASc scoring system [22,23].
Regarding anticoagulant prescription patterns, no statistically significant sex-based disparities were evident in the selection of ACO treatment modality, but a notable prevalence of subtherapeutic dosing, significantly higher in female patients, has been reported [24,25]. If the Sc (sex category) component is removed from the CHA2DS2-VASc score, it could contribute to the established pattern of suboptimal anticoagulation in women with AF [26]. On other hand, while vitamin K antagonists constitute 32% of ACO prescriptions and necessitate regular monitoring via the international normalized ratio, the lack of an equivalent objective adherence monitoring mechanism for NOACs remains a significant clinical challenge [27] in the context of adherence to oral anticoagulants among patients with atrial fibrillation. Ultimately, the interaction between female sex, comorbidities, oral anticoagulant use, and stroke risk may vary across the age spectrum.
As strengths, the study was based on a global, multicenter cohort, and capable of contributing valuable data to the existing body of knowledge on atrial fibrillation in a large patient group. Our findings provide epidemiological data for comparing the predictive performance of CHA2DS2-VA and CHA2DS2-VASc scores in stratifying stroke risk in AF patients. Future research directions include investigating the intricate relationships between specific comorbidities and the pathogenesis of atrial fibrillation, analyzing age-and sex-stratified treatment modalities and their associated outcomes. Furthermore, prospective studies are warranted to ascertain whether the CHA2DS2-VA score will lead to better implementation of oral anticoagulation across the heterogeneous spectrum of at-risk atrial fibrillation patients, excluding only those at “truly very low risk” of thromboembolism, and to confirm that this occurs equitably, aligning with the objective of ensuring universal access to effective and appropriate care.
5. Conclusions
1/ The CHA2DS2-VA score exhibited comparable predictive accuracy for thromboembolic events to the established CHA2DS2-VASc score.
2/ The CHA2DS2-VA scoring system refined the overall assessment of thromboembolic risk, only a small fraction of women (3.2%) were categorized as being at a low risk (<2) of stroke.
3/ No statistically significant sex-based disparities were evident in the selection of ACO treatment modality.
4/ The clinical utility of adopting the CHA2DS2-VA score for stroke risk stratification in patients with atrial fibrillation remains a subject of ongoing debate.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, JL.CE, A.PT, S.RV, J.CQ; and J.LN; methodology, JL.CE, A.PT, S.RV, and J.LN: software, JL.CE, A.PT, S.RV; and J.CQ; validation, JL.CE, J.LN, and S.RV; formal analysis, JL.CE, J.LN, S.RV, A.PT; E.MS; T.FA; JM.CO; J.CQ; and P.MB; investigation, JL.CE; S.RV; A.PT; E.MS, J.CQ, T.FA; JM.CO; and I.FA; resources, A.PT; E.MS; T.FA; J.CQ; and I.FA; data curation, JL.CE, S.RV, and A.PT; writing—original draft preparation, JL.CE, S.RV, A.PT; E.MS; T.FA; J.CQ; JM.CO; and J.LN; writing—review and editing, JL.CE, A.PT; and S.RV; supervision, S.RV, and JL.CE; project administration, JL.CE, S.RV, and A.PT. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding” and “The APC was funded by MDPI.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Independent Ethics Committee of the Foundation University Institute for Primary Health Care Research-IDIAP Jordi Gol, code CEIm 24/187-P. The study was conducted in compliance with the Declaration of Helsinki. All participants received written information and subsequently signed their informed consent before inclusion. The data collection was supervised and conducted in accordance with the most relevant standards regarding data handling, concerning the experimental context with patients, ethics, and data protection and privacy, following Directive 95/46/EC (protection of individuals with regard to the processing of personal data and on the free movement of such data). All of the data were included in an ad hoc repository, which was delivered to the main researcher.
Informed Consent Statement
Patient consent was waived prior to the inclusion of medical data since formal consent is not required for this type of study.
Data Availability Statement
The data supporting the findings of this study are not currently publicly available but can be requested from the authors upon reasonable request. These data will be available through an institutional repository following the public defense of the corresponding PhD thesis.
Acknowledgments
The authors would like to thank the Department of Information and New Technologies of the Management Department of Terres de l’Ebre (Catalan Institute of Health) and Mr. Jesus Carot-Domenech for their technical support in the collection of the data. Equally the authors thank all the collaborators involved in the Ebrictus project for their collaboration and support on the recording, checking, and interpretation of the data and for contributing ideas.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AF | Atrial Fibrillation |
| OAC | Oral Anticoagulants |
| ESC-EACTS Guidelines | Guidelines developed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) |
| GECATE | Acronym for “Gender perspective on cardiovascular diseases in the Terres de l'Ebre” |
| ICS | Acronym for “Catalan Health Institute” |
| EAPs | Acronym for “Primary Care teams” |
| HCC3 | Acronym for “Shared clinical record of Catalonia” |
| SIRE | Acronym for “Integrated Electronic Prescription System” |
| COPD | Chronic Obstructive Pulmonary Disease |
| BMI | Body Mass Index |
| OSAHS | Obstructive Sleep Apnea/Hypopnea Syndrome |
| VKAs | Vitamin K antagonists |
| NOACs | Non-vitamin K oral anticoagulants |
Appendix A
Figure A1.
Regional map of the Terres de l’Ebre study area within Spain.
References
- van der Endt VHW, Milders J, Penning de Vries BBL, Trines SA, Groenwold RHH, Dekkers OM, Trevisan M, Carrero JJ, van Diepen M, Dekker FW, de Jong Y. Comprehensive comparison of stroke risk score performance: a systematic review and meta-analysis among 6 267 728 patients with atrial fibrillation. Europace. 2022 Nov 22;24(11):1739-1753. [CrossRef]
- {2]. Boriani G, Vitolo M, Mei DA. CHA2DS2-VA instead of CHA2DS2-VASc for stroke risk stratification in patients with atrial fibrillation: not just a matter of sex. Europace. 2024 Nov 1;26(11):euae281. [CrossRef]
- Kalarus Z, Mairesse GH, Sokal A, Boriani G, Średniawa B, Casado-Arroyo R, Wachter R, Frommeyer G, Traykov V, Dagres N, Lip GYH, Boersma L, Peichl P, Dobrev D, Bulava A, Blomström-Lundqvist C, de Groot NMS, Schnabel R, Heinzel F, Van Gelder IC, Carbucicchio C, Shah D, Eckardt L. Searching for atrial fibrillation: looking harder, looking longer, and in increasingly sophisticated ways. An EHRA position paper. Europace. 2023 Feb 8;25(1):185-198. Erratum in: Europace. 2024 Jun 3;26(6):euae167. doi: 10.1093/europace/euae167. [CrossRef]
- Wilkinson C, Wu J, Clegg A, Nadarajah R, Rockwood K, Todd O et al. Impact of oral anticoagulation on the association between frailty and clinical outcomes in people with atrial fibrillation: nationwide primary care records on treatment analysis. Europace 2022;24:1065–75.
- Yoshimura H, Providencia R, Finan C, Schmidt AF, Lip GYH. Refining the CHA2DS2VASc risk stratification scheme: shall we drop the sex category criterion? Europace. 2024 Nov 1;26(11):euae280. [CrossRef]
- Lip GYH, Teppo K, Nielsen PB. CHA2DS2-VASc or a non-sex score (CHA2DS2-VA) for stroke risk prediction in atrial fibrillation: contemporary insights and clinical implications. Eur Heart J. 2024 Sep 29;45(36):3718-3720. [CrossRef]
- Teppo K, Lip GYH, Airaksinen KEJ, Halminen O, Haukka J, Putaala J et al. Comparing CHA2DS2-VA and CHA2DS2-VASc scores for stroke risk stratification in patients with atrial fibrillation: a temporal trends analysis from the retrospective Finnish AntiCoagulation in Atrial Fibrillation (FinACAF) cohort. Lancet Reg Health Eur 2024;43:100967.
- Van Gelder IC, Rienstra M, Bunting KV, Casado-Arroyo R, Caso V, Crijns HJGM, De Potter TJR, Dwight J, Guasti L, Hanke T, Jaarsma T, Lettino M, Løchen ML, Lumbers RT, Maesen B, Mølgaard I, Rosano GMC, Sanders P, Schnabel RB, Suwalski P, Svennberg E, Tamargo J, Tica O, Traykov V, Tzeis S, Kotecha D; ESC Scientific Document Group. 2024 ESC Guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024 Sep 29;45(36):3314-3414. [CrossRef]
- Wu VC, Wu M, Aboyans V, Chang SH, Chen SW, Chen MC, Wang CL, Hsieh IC, Chu PH, Lin YS. Female sex as a risk factor for ischaemic stroke varies with age in patients with atrial fibrillation. Heart. 2020 Apr;106(7):534-540. [CrossRef]
- Rienstra M, Tzeis S, Bunting KV, Caso V, Crijns HJGM, De Potter TJR, Sanders P, Svennberg E, Casado-Arroyo R, Dwight J, Guasti L, Hanke T, Jaarsma T, Lettino M, Løchen ML, Lumbers RT, Maesen B, Mølgaard I, Rosano GMC, Schnabel RB, Suwalski P, Tamargo J, Tica O, Traykov V, Kotecha D, Van Gelder IC. Spotlight on the 2024 ESC/EACTS management of atrial fibrillation guidelines: 10 novel key aspects. Europace. 2024 Dec 3;26(12):euae298. [CrossRef]
- Ictus: Plan de Actuación en Europa (2018-2030). Ed Stroke Alliance for Europe (SAFE). 2018. www.safestroke.eu (accessed on 25 April 2025).
- Pla de salut de la Regió Sanitària Terres de l’Ebre 2021-2025. Tortosa: Direcció General de Planificació i Recerca en Salut;2022. https://scientiasalut.gencat.cat/handle/11351/7964 (accessed on 5 May 2025).
- Idescat. Indicadors Demogràfics i de Territori. Estructura per Edats, Envelliment i Dependència. Comarques i Aran. Available online: http://www.idescat.cat/pub/?id=inddt&n=915&by=com (accessed on 5 May 2025).
- Generalitat de Catalunya. Projeccions de Població Principals Resultats 2013–2051. 2008. Available online: https://www.idescat.cat/serveis/biblioteca/docs/cat/pp2021-2041pr.pdf (accessed on 25 April 2025).
- Alshehri AM. Stroke in atrial fibrillation: Review of risk stratification and preventive therapy. J Family Community Med. 2019 May-Aug;26(2):92-97. [CrossRef]
- Heidbuchel H, Van Gelder IC, Desteghe L; EHRA-PATHS Investigators. ESC and EHRA lead a path towards integrated care for multimorbid atrial fibrillation patients: the Horizon 2020 EHRA-PATHS project. Eur Heart J. 2022 Apr 14;43(15):1450-1452. [CrossRef]
- Steven Ho Man Lam, Giulio Francesco Romiti, Bernadette Corica, Tommaso Bucci, Brian Olshansky, Tze-Fan Chao, Menno V Huisman, Gregory Y H Lip, on behalf of the GLORIA-AF Investigators, Stroke risk stratifications according to CHA2DS2-VASc vs. CHA2DS2-VA in patients with Atrial Fibrillation: insights from the GLORIA-AF registry, European Heart Journal - Cardiovascular Pharmacotherapy, 2025;, pvaf031. [CrossRef]
- Clua-Espuny JL, Hernández-Pinilla A, Gentille-Lorente D, Muria-Subirats E, Forcadell-Arenas T, de Diego-Cabanes C, Ribas-Seguí D, Diaz-Vilarasau A, Molins-Rojas C, Palleja-Millan M, Satué-Gracia EM, Martín-Luján F; PREFATE Project-Group. Evidence Gaps and Lessons in the Early Detection of Atrial Fibrillation: A Prospective Study in a Primary Care Setting (PREFATE Study). Biomedicines. 2025 Jan 7;13(1):119. [CrossRef]
- Romiti, G.F., Corica, B., Mei, D.A. et al. Patterns of comorbidities in patients with atrial fibrillation and impact on management and long-term prognosis: an analysis from the Prospective Global GLORIA-AF Registry. BMC Med 22, 151 (2024). [CrossRef]
- Lip GYH, Teppo K, Nielsen PB. CHA2DS2-VASc or a non-sex score (CHA2DS2-VA) for stroke risk prediction in atrial fibrillation: contemporary insights and clinical implications. Eur Heart J. 2024 Sep 29;45(36):3718-3720. [CrossRef]
- Champsi A, Mobley AR, Subramanian A, Nirantharakumar K, Wang X, Shukla D, Bunting KV, Molgaard I, Dwight J, Arroyo RC, Crijns HJGM, Guasti L, Lettino M, Lumbers RT, Maesen B, Rienstra M, Svennberg E, Țica O, Traykov V, Tzeis S, van Gelder I, Kotecha D. Gender and contemporary risk of adverse events in atrial fibrillation. Eur Heart J. 2024 Sep 29;45(36):3707-3717. [CrossRef]
- Lu J, Hutchens R, Hung J, Bennamoun M, McQuillan B, Briffa T, Sohel F, Murray K, Stewart J, Chow B, Sanfilippo F, Dwivedi G. Performance of multilabel machine learning models and risk stratification schemas for predicting stroke and bleeding risk in patients with non-valvular atrial fibrillation. Comput Biol Med. 2022 Nov;150:106126. [CrossRef]
- Moltó-Balado, P.; Reverté-Villarroya, S.; Alonso-Barberán, V.; Monclús-Arasa, C.; Balado-Albiol, M.T.; Clua-Queralt, J.; Clua-Espuny, J.-L. Machine Learning Approaches to Predict Major Adverse Cardiovascular Events in Atrial Fibrillation. Technologies 2024, 12, 13. [Google Scholar] [CrossRef]
- Giner-Soriano M, Prat-Vallverdú O, Ouchi D, Vilaplana-Carnerero C, Morros R. Sex and gender differences in the use of oral anticoagulants for non-valvular atrial fibrillation: A population-based cohort study in primary health care in catalonia. Front Pharmacol. 2023 Feb 7;14:1110036. [CrossRef]
- Teppo K, Airaksinen KEJ, Jaakkola J, Halminen O, Salmela B, Kalatsova K, Kouki E, Haukka J, Putaala J, Linna M, Aro AL, Mustonen P, Hartikainen J, Lehto M. Temporal trends of gender disparities in oral anticoagulant use in patients with atrial fibrillation. Eur J Clin Invest. 2024 Jan;54(1):e14107. [CrossRef]
- Nielsen PB, Overvad TF. Female Sex as a Risk Modifier for Stroke Risk in Atrial Fibrillation: Using CHA2DS2-VASc versus CHA2DS2-VA for Stroke Risk Stratification in Atrial Fibrillation: A Note of Caution. Thromb Haemost. 2020 Jun;120(6):894-898. [CrossRef]
- Salmasi S, Loewen PS, Tandun R, Andrade JG, De Vera MA. Adherence to oral anticoagulants among patients with atrial fibrillation: a systematic review and meta-analysis of observational studies. BMJ Open. 2020 Apr 8;10(4):e034778. [CrossRef]

Table 1.
Baseline characteristics of cases by sex. General population.
| Variables | Men | (%) | Women | (%) | p | ALL (%) |
|---|---|---|---|---|---|---|
| All (n %) | 19,531 | 48.7% | 20,548 | 51.3% | - | 40,077 |
| FA | 1,928 | 9.9% | 1,442 | 7.0% | < 0.001 | 3,370 (8.4%) |
| Age average | 77.28±6.56 | 77.6±6.63 | < 0.001 | 77.4±6.60 | ||
| CHA2DS2-VASc | 2.7±1.1 | 3.6±1.1 | < 0.001 | 3.2±1.2 | ||
| CHA2DS2-VA | 2.8±1.1 | 2.6±1.1 | < 0.001 | 2.68±1.1 | ||
| Heart failure | 1,790 | 9.2% | 1,558 | 7.6.·% | < 0.001 | 3,348 (8.4%) |
| Hypertension arterial | 11,526 | 59.0% | 12,218 | 59.5% | 0.360 | 23,744 (59.2%) |
| Age 65 to 74 years | 7,748 | 39.6% | 7,765 | 37.8% | < 0.001 | 15,513 (38.7%) |
| Age ≥75 years | 11,783 | 60.3% | 12,783 | 62.6% | < 0.001 | 24,566 (61.3%) |
| Diabetes mellitus | 5,763 | 29.5% | 4,498 | 21.9% | < 0.001 | 10,261 (25.6%) |
| Stroke/TIA/Systemic embolism | 843 | 4.7% | 724 | 3.5% | < 0.001 | 1567 (3.9%) |
| Vascular peripheral disease | 1,983 | 10.2% | 798 | 3.9% | < 0.001 | 2,781 (6.9%) |
| Ischemic cardiomyopathy | 2,073 | 10.6% | 917 | 4.5% | < 0.001 | 2,990 (7.5%) |
| BMI1 (kg/m2) | 28.1±4.5 | 28.4±5.7 | < 0.001 | 28.3±5.2 | ||
| Charlson index | 1.5±1.4 | 1.2±1.2 | < 0.001 | 1.38±1.9 | ||
| Dementia/cognitive impairment | 1,452 | 7.4% | 2,225 | 10.8% | < 0.001 | 3,677 (9.2%) |
| Pfeiffer score | 2.72±3.20 | 3.63±3.35 | < 0.001 | 3.23±3.3 | ||
| Chronic Kidney Disease | 3,181 | 16.3% | 3,080 | 15.0% | < 0.001 | 6,261 (15.6%) |
| Glomerular filtration rate (ml/min/1.73 m2) |
72.2±18.0 | 73.4±17.6 | < 0.001 | 72.9±17.7 | ||
| COPD2/asthma/bronchitis | 2,895 | 14,8% | 2,224 | 10.8% | < 0.001 | 5,119 (12.8%) |
| OSAHS3 | 966 | 4.9% | 473 | 2.3% | < 0.001 | 1,439 (3.6%) |
| Dyslipidemia | 8,394 | 43.0% | 10,623 | 51.7% | < 0.001 | 19,017 (47.5%) |
| Statins | 6,006 | 30.8% | 6,326 | 30.8% | 0.940 | 12,332 (30.8%) |
| Antiaggregants | 3,411 | 17.5% | 2,335 | 11.4% | < 0,001 | 5,746 (14.3%) |
| Anticoagulation | 1,977 | 10.1% | 1,468 | 7.1% | < 0.001 | 3,445 (8.6%) |
| Hospital visits | 0.36±1.3 | 0.27±0.95 | < 0.001 | 0.31±1,15 | ||
| Active medications | 5.17±4.3 | 5.76±4.40 | < 0.001 | 5.48±4.36 | ||
| Exitus | 14,492 | 74.2% | 17,173 | 83.6% | < 0.001 | 31,665 (79.0%) |
1BMI: Body Mass Index; 2COPD: Chronic Obstructive Pulmonary Disease; 3OSAHS: Obstructive Sleep Apnea/Hypopnea Syndrome.
Table 2.
Baseline characteristics of cases by sex. Population with new AF.
| Variables | Men | (%) | Women | (%) | p | ALL (%) |
|---|---|---|---|---|---|---|
| All (n %) | 1,928 | 57.2% | 1,442 | 42.8% | < 0.001 | 3,370 |
| Age average | 79.5±6.23 | 80.9±6.1 | < 0.001 | 80.1±6.24 | ||
| CHA2DS2-VASc | 3.58±1.18 | 4.51±1.12 | < 0.001 | 3.98±1.24 | ||
| CHA2DS2-VA | 3.58±1.18 | 3,51±1.12 | 0.071 | 3.55±1.16 | ||
| Heart failure | 690 | 35.8% | 543 | 37.7% | 0.278 | 1,233 (36.6%) |
| Hypertension arterial | 1,439 | 74.6% | 1,091 | 75.7% | 0.520 | 2,530 (75.1%) |
| Age 65 to 74 years | 460 | 23.8% | 246 | 17.1% | < 0.001 | 706 (20.94%) |
| Age ≥75 years | 1,468 | 76.1% | 1,196 | 82.9% | < 0.001 | 2,664 (79.1%) |
| Diabetes mellitus | 727 | 37.7% | 461 | 32.0% | 0.001 | 1,188 (35.3%) |
| Stroke/TIA/Systemic embolism | 194 | 10.1% | 137 | 9.5% | 0.599 | 331 (9.8%) |
| Vascular peripheral disease | 351 | 18.2% | 119 | 8.3% | < 0.001 | 470 (13.8%) |
| Ischemic cardiomyopathy | 375 | 19.5% | 162 | 11.2% | < 0.001 | 537 (15.8%) |
| BMI1 (kg/m2) | 29.07±5.1 | 28.53±6.2 | 0.022 | 29.2±5.5 | ||
| Charlson index | 2.27±1.5 | 1.91±1.38 | < 0.001 | 2.10±1.45 | ||
| Dementia/cognitive impairment | 196 | 10.2% | 212 | 14.7% | < 0.001 | 408 (12.1%) |
| Pfeiffer score | 2.14±2.7 | 3.31±3.0 | < 0.001 | 2.71±2.9 | ||
| Chronic Kidney Disease | 58155 | 30.1% | 417 | 28.9% | 0.446 | 998 (29.6%) |
| Glomerular filtration rate (ml/min/1.73 m2) |
65.5±20.0 | 64.7±19.8 | 0.356 | 65.16±19.9 | ||
| COPD3/asthma/bronchitis | 454 | 23.5% | 223 | 15.5% | < 0.001 | 677 (20.1%) |
| OSAHS2 | 170 | 8.8% | 54 | 3.7% | < 0.001 | 224 (6.6%) |
| Dyslipidemia | 933 | 48.4% | 774 | 53.7% | 0.002 | 1707 (50.7%) |
| Statins | 721 | 37.4% | 505 | 35.0% | 0.158 | 1,226 (36.4%) |
| Antiaggregants | 122 | 6.3% | 48 | 3.3% | < 0,001 | 170 (5.0%) |
| Anticoagulation VKAs4 NOACs5 |
1,522 492 1,030 |
78.9% 32.3% 67.6% |
1,140 378 762 |
79.0% 33.1% 66.8% |
0.9694 0.6810 0-6810 |
2,662 (78.9%) 870 (32.6%) 1,792 (67.3%) |
| Hospital visits | 0.68±1.7 | 0.58±1.51 | 0.070 | 0.64±1.64 | ||
| Active medications | 8.03±4.6 | 8.57±4.7 | 0.001 | 8.26±4.68 | ||
| Exitus | 1,445 | 74.9% | 1,125 | 78.0% | 0.095 | 2,570 (76.3%) |
1 BMI: Body Mass Index; 2 COPD: Chronic Obstructive Pulmonary Disease; 3 OSAHS: Obstructive Sleep Apnea/Hypopnea Syndrome; 4 VKAs: vitamin K antagonists; 5 NOACs: Non-vitamin K oral anticoagulants.
Table 3.
Thrombotic Risk Stratification by CHA₂DS₂-VASc and CHA₂DS₂-VA in Men and Women with New AF.
Table 3.
Thrombotic Risk Stratification by CHA₂DS₂-VASc and CHA₂DS₂-VA in Men and Women with New AF.
| Tab | CHA2DS2VASc | CHA2DS2VA | |||||
| score | WOMEN N1 (%) |
MEN n1 (%) |
p | WOMEN N2 (%) |
MEN n2 (%) |
P | Total registered stroke |
| 1 | - | 61 (3.1%) | < 0.001 | 46 (3.2%) | 61 (3.1%) | 0.9549 | - |
| 2 | 46 (3.2%) | 276 (14.3%) | < 0.001 | 210 (14.5%) | 276 (14.3%) | 0.8784 | 10 (3.02%) |
| 3 | 210 (14.6%) | 593 (30.7%) | <0.001 | 459 (31.8%) | 593 (30.8%) | 0.5301 | 48 (14.50%) |
| 4 | 459 (31.8%) | 589 (30.5%) | 0.4489 | 481 (33.3%) | 589 (30.5%) | 0.0902 | 112 (33.83%) |
| 5 | 481 (33.5%) | 307 (15.9%) | < 0.001 | 183 (12.7%) | 307 (15.9%) | 0.0098 | 84 (25.37%) |
| 6 | 183 (12.6%) | 88 (4.5%) | < 0.001 | 58 (4.0%) | 88 (4.5%) | 0.4969 | 58 (17.52%) |
| 7 | 58 (4.0%) | 14 (0.7%) | < 0.001 | 5 (0.3%) | 14 (0.7%) | 0.2214 | 19 (5.74%) |
| 8 | 5 (0.3%) | - | 0.0327 | - | - | - | |
| 9 | - | - | - | - | - | ||
| Total | 1,442 (7.0%) | 1,928 (9.9%) | < 0.001 | 1,442 (7.0%) | 1,928 (9.9%) | < 0.001 | 331 |
Table 4.
Stroke Incidence Rates per 100 Person-Years: Comparison of CHA₂DS₂-VASc and CHA₂DS₂-VA Scores.
Table 4.
Stroke Incidence Rates per 100 Person-Years: Comparison of CHA₂DS₂-VASc and CHA₂DS₂-VA Scores.
| CHA2DS2VASc | CHA2DS2VA | |||||
| score | FA (N) |
Stroke (n) |
Incidence rate per 100 person-years CI95% | FA (N) |
Incidence rate per 100 person-years CI95% | Razon de tasas CI95% |
| 1 | 61 | - | 107 | - | ||
| 2 | 322 | 10 | 1.41 [0.68-2.59] | 486 | 0.93 [0.45-1.71] | 1.51 [0.63-3.64] |
| 3 | 803 | 48 | 2.80 [2.06-3.71] | 1052 | 2.16 [1.59-2.86] | 1.29 [0.86-1.93] |
| 4 | 1048 | 112 | 4.85 [3.99-5.83] | 1070 | 4.67 [3.85-5.62] | 1.03 [0.79-1.34] |
| 5 | 788 | 84 | 4.82 [3.84-5.96] | 490 | 7.58 [6.05-9.39] | 0.63 [0.46-0.85] |
| 6 | 271 | 58 | 9.49 [7.21-12.27] | 146 | 19.3 [14.68-24.99] | 0.49 [0.34-0.70] |
| 7 | 72 | 19 | 13.10 [7.89-20.46] | 19 | 50.0 [30.1-78.0] | 0.26 [0.13-0.49] |
| 8 | 5 | - | - | - | ||
| 9 | - | - | - | - | ||
| Total | 3370 | 331 | 4,51 [4.03-5.02] | 3370 | 4,51 [4.03-5.02] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



