
Submitted:
07 May 2025
Posted:
09 May 2025
You are already at the latest version
Abstract
Background: Endometriosis is a benign and often underdiagnosed condition that affects women of reproductive age. It can cause infertility and pain, including radicular pain and low back pain (LBP). The aim of this case report is to emphasize the importance of making a differential diagnosis when in presence of LBP and radicular symptoms. Case Presentation: A 17-year-old female patient, R.A., presented with a significant LBP (NPRS 8/10) radiating from her lumbar spine to her right buttock and occasionally to both legs, accompanied by weakness. She revealed exacerbation of pain during menstruation, despite being on oral contraceptives. After three physiotherapy sessions that included education, manual therapy, and exercise, the patient’s pain persisted, so her physiotherapist recommended evaluation in the emergency department, where standard radiography did not reveal any significant findings. Physiotherapy continued until the fifth session, when the patient agreed to undergo evaluation at a specialized endometriosis centre. Further investigations revealed endometriotic tissue on the uterosacral ligament, leading to hormonal therapy adjustment, which led to a gradual decrease of pain to a manageable level (NPRS 2/10). Conclusion: This case report highlights the importance of differential diagnosis in patients with LBP, even in younger subjects, and the need for physiotherapists to consider gynaecological factors in some cases of LBP.
Keywords:
endometriosis
; pelvic girdle pain
; low back pain
; radicular pain
; case report
Introduction
Endometriosis is a chronic, non-cancerous inflammatory condition characterized by the presence of endometrial-like tissue outside the uterus. This tissue commonly implants in areas such as the ovaries, uterine ligaments, pelvic peritoneum, cervix, and vagina [1]. During menstruation, the ectopic endometrial tissue also bleeds, but since the blood has no way of being expelled, it causes pain [2]. The exact cause of endometriosis remains unclear, with multiple factors and unknown pathophysiological mechanisms believed to contribute to its development [3]. Several theories, such as retrograde menstruation, coelomic metaplasia, and the theory of embryonic rests, attempt to explain the origins of the disease [1], but none fully account for all aspects. Endometriosis primarily affects women of reproductive age, particularly those between 30 and 40 years old [4] and is observed in 50-80% of women experiencing pelvic pain [5]. However, endometriosis is often misdiagnosed, as its symptoms are frequently dismissed or normalized [2]. It typically takes 7-10 years from the onset of symptoms for a proper diagnosis [3], which can have significant physical, emotional, and socioeconomic impacts on affected women [6].
The symptoms of endometriosis are varied and nonspecific, including pelvic pain (especially during menstruation), dysmenorrhea, dyspareunia, and infertility [1,7]. In addition, it can lead to systemic effects, including diffuse inflammation and peripheral sensitization, which explain why women with endometriosis often experience pain even after the surgical removal of endometrial tissue [8,9]. This alteration in pain perception can lead to central sensitization, causing chronic pain and hyperalgesia [8,10]. The condition is also associated with a reduced quality of life, affecting social, psychological, and physical well-being [11], and can have a significant impact on work productivity, sports participation, and relationships [4,12]. Additionally, approximately 90% of women with endometriosis experience psychological issues, such as anxiety, depression, and catastrophizing, due to the chronic pain that limits daily activities [8,13].
Endometriosis is also prevalent in adolescents, with a significant impact on personal life and academic performance. The signs and symptoms in adolescents may differ from those in adults, leading to delays in diagnosis, which can take up to 23 months [14]. While it was once believed that endometriosis developed after menarche, it is now recognized that it can occur even prior to the first menstrual cycle [15]. Adolescents with endometriosis are at a higher risk for developing anxiety, depression, and concentration problems [16] and are more likely to develop other pain disorders [17]. Symptoms in young women typically include acyclic pelvic pain, low energy, abdominal pain, heavy menstrual bleeding, low back pain (LBP), and other abdominal issues [16].
Diagnosis of endometriosis is based on personal history and symptoms of the patient, both in adolescents and in women, in association with imaging techniques such as ultrasound or MRI, although negative results cannot rule out the disease. If imaging is inconclusive, laparoscopy, considered as the gold standard, is recommended for both diagnosis and treatment. The use of biomarkers, such as blood or uterine fluids, is not currently recommended for diagnosing endometriosis. Treatment options include NSAIDs, other analgesics, combined hormonal therapies, and, when necessary, laparoscopy to remove endometriotic tissue, although it is associated with a high risk of relapse [18]; in fact, symptoms may recur in 0-89% of cases, and new endometriotic tissue may grow. Therefore, postoperative medical treatment is advised to minimize the growth of residual endometriotic cells [19].
The symptoms of endometriosis can vary greatly between individuals, but common manifestations include dyspareunia, dysmenorrhea, cyclic pelvic pain, fatigue, cramping during menstruation, pain during intercourse, and LBP [4]. LBP, defined as “pain and discomfort, localised below the costal margin and above the inferior gluteal folds, with or without referred leg pain” [20], is one of the most prevalent conditions globally, with incidence increasing from 1990 to 2019 [21]. LBP is a major reason for seeking medical attention and has significant societal and economic implications due to work absenteeism and the cost of treatment [22]. LBP can be classified as acute (lasting up to 4 weeks) or chronic (lasting more than 3 months). Acute LBP may result from various sources, including muscles, facet joints, intervertebral discs, ligaments, fasciae, nerves, or non-musculoskeletal causes [23]. The literature reports only few cases of patients with LBP accompanied by referred pain in the lower limb [24] or isolated referred pain [25,26] associated to endometriosis, all of which emphasize the challenges in diagnosing these conditions. The association of endometriosis with LBP can be explained by the implant of endometrial tissue on the lumbosacral roots, plexus, or the proximal sciatic nerve [25]. The pain arises from the expression of nerve growth factor in nerves near deep endometriotic lesions, as well as the presence of pro-inflammatory cells, such as interleukins and histamine, which can stimulate sensory nerve endings. Additionally, endometrial lesions may exert pressure and cause inflammation on the nerve, resulting in both localized and radicular pain [26]. Diagnosing endometriosis from LBP can be very challenging, but this pathology must be considered every time there is a cyclical LBP and whose cause is unknown.
Case Presentation
In this case report, we describe the clinical experience of a 17-year-old female patient who, in March 2024, accessed a private physiotherapy clinic through direct access. She was evaluated by an Orthopaedic Manipulative Physical Therapist (OMPT) due to intense and disabling lower back pain. Written informed consent was obtained from the patient for the publication of this case report.
Patient History
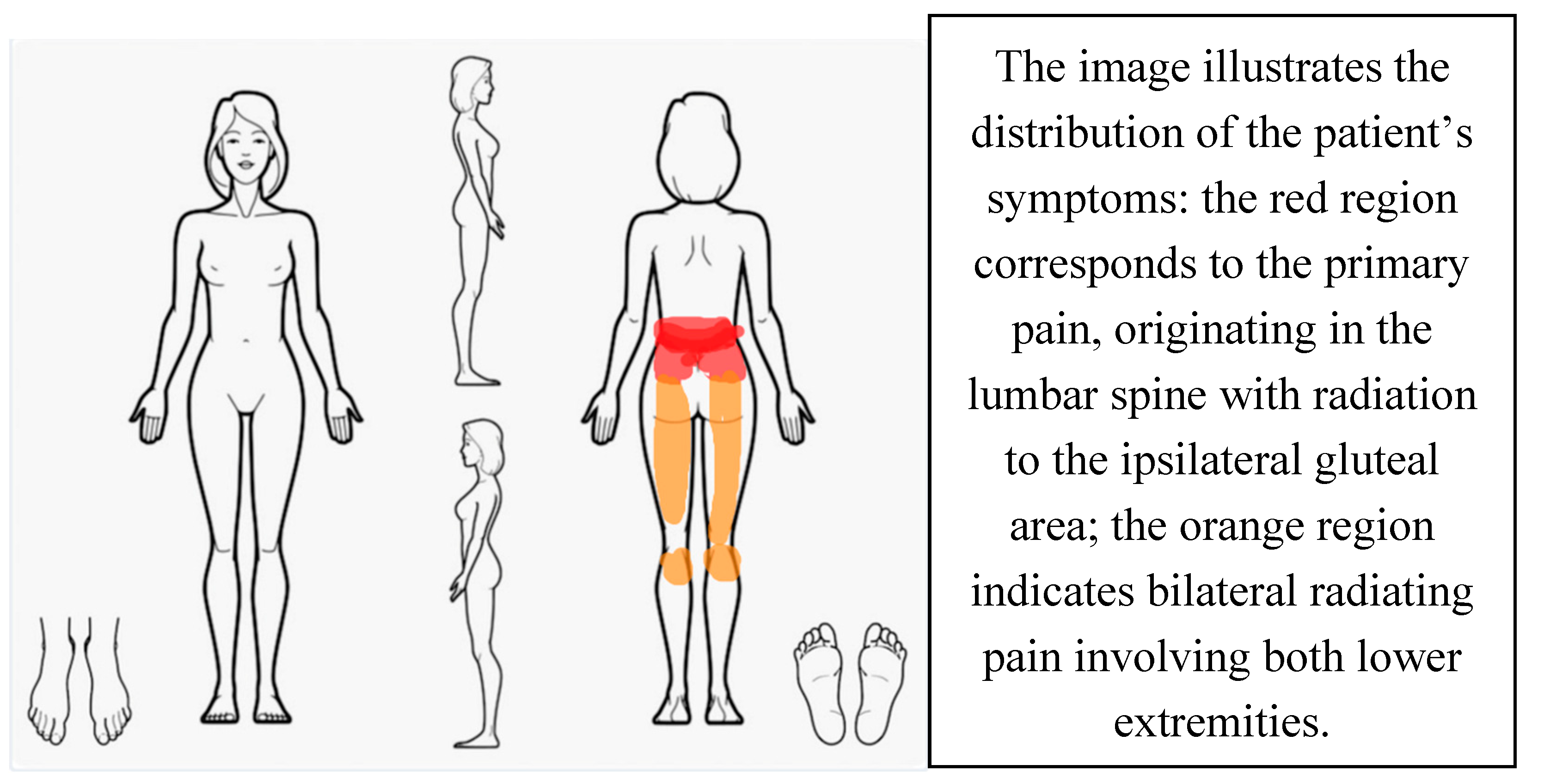
The patient, R.A., presented with severe and disabling low back pain radiating from the lumbar spine to the right buttock and, occasionally, to both legs below the knees. She also reported generalized weakness and claudication. The symptoms had begun approximately one month prior to the physiotherapy evaluation and progressively worsened, with the development of additional knee pain after 20 days [Figure 1]. The patient described her pain as very intense on the lumbar tract, 8/10 on the Numerical Pain Rating Scale (NPRS), in which 0 is equal to no pain while 10 is the worst imaginable pain [27], and leg pain was described with an NPRS of 6-7/10.
The patient led an active lifestyle; she attended school regularly and practiced volleyball. However, due to her condition, she was forced to suspend all physical and social activities. She became increasingly withdrawn and reported emotional distress and frustration due to the persistent pain, which also interfered with her ability to engage in sexual activity. During the initial evaluation, the patient reported a history of dysmenorrhea and dyspareunia, which preceded the onset of low back pain (LBP), although she noted that the pain had significantly worsened since then. There were no specific positions or activities that aggravated her symptoms. However, prolonged sitting, particularly at school, was associated with increased discomfort, while lying on either side provided some relief. She also experienced nocturnal pain, though she was able to sleep for a few hours. She had been on oral contraceptives for approximately one year, reporting occasional side effects such as spotting and water retention. Non-steroidal anti-inflammatory drugs (NSAIDs) had also been initiated following the onset of symptoms, but provided only limited relief. Her medical history included a tibia and fibula fracture, multiple ankle and wrist sprains, and a cholecystectomy. The persistent pain and reduced functionality had a significant negative impact on her quality of life, and she expressed high levels of frustration and concern.
Physical Examination
At her initial physiotherapy assessment, the patient reported a pain level of 8/10 on the Numerical Pain Rating Scale (NPRS). She presented with mild trunk flexion and generalized stiffness. Neurological and neurodynamic assessments [28] were performed. The Straight Leg Raise (SLR) test reproduced lower limb symptoms without modifying lumbar or sacral pain. Reflexes, sensory testing, and strength assessments were unremarkable, although strength testing was limited due to pain severity. The repeated movements test [29,30] appeared to be negative for the absence of centralization. Muscular palpation did not elicit changes in symptoms. Due to high pain levels, further physical testing was initially deferred. At the second session, repeated movements remained negative. Both seated compression and distraction tests were performed, and both were negative. Springing tests were positive at L3–S1, with maximal tenderness over S1, which referred pain to the sacral region. To investigate the hypothesis of pelvic girdle pain (PGP), the Laslett cluster [31] was administered. The Thigh Thrust, Distraction, Compression, and Sacral Thrust tests were all positive, whereas the Gaenslen test was not performed. Palpation of the long dorsal sacroiliac ligament (LDL) [32] reproduced pain bilaterally. Trigger point palpation of the paravertebral and gluteal muscles did not affect symptoms.
The Oswestry Disability Index (ODI) [33] was administered to assess functional impairment. The ODI is a self-administered questionnaire made of 10 items that investigate disability associated to LBP in different daily activities; every item has a score that ranges from 0 to 5, the sum of the scores is then expressed with a percentage, the higher the percentage, the greater the disability. The baseline ODI score was 64%, indicating severe disability.
Treatment
since the first session of physiotherapy, education of the patient was performed [34]; it focused on pain management strategies, including antalgic postures and frequent position changes. Manual therapy (MT) techniques [34] were introduced, including rotational Maitland mobilizations, sacral mobilizations (counter-nutation of the sacrum on the ilium and anterior rotation of the ilium), soft tissue massage of the gluteal and paravertebral muscles, and neurodynamic mobilizations. A home exercise program was prescribed, incorporating neurodynamic techniques and active mobilizations of the sacrum on the ilium. After initial sessions, the patient reported temporary pain relief, with NPRS scores decreasing to NPRS 6/10 for the lumbar region and NPRS 5/10 for the lower limbs. However, by the third session, pain intensity increased to NPRS 9-10/10, prompting a referral to the emergency department.
Patient underwent a radiograph that didn’t show anything relevant, with exclusion of fractures and a mild disc height reduction at L1–L2 and L2–L3. NSAIDs were prescribed, providing only minimal relief. Physiotherapy treatments continued, but due to persistent high pain levels, the patient underwent MRI imaging on the recommendation of her mother. The MRI revealed annular fissuring at L4–L5 with a protrusion slightly contacting the dural sac.
Symptoms remained unchanged, with short-lasting relief from therapy. At the fifth session, the physiotherapist referred the patient to a specialized endometriosis center. The patient, after 3 months from the first evaluation, underwent a specialist consultation in a specialized centre for endometriosis in Padova (Italy). Further investigations revealed endometriotic tissue on the uterosacral ligament that led to an adjustment in her hormonal therapy. At this point, a repeat ODI showed a score of 62%.
With the new pharmacological therapy, the patient referred a progressive and constant reduction of pain in a very short period. After a month since the therapy change, a new physiotherapy evaluation was made, in which the irradiated pain was completely resolved, while the lumbar pain was still present but with an NPRS 3. She continued active mobilization exercises and initiated lumbar strengthening [34] with the physiotherapist. Pain progressively diminished and became manageable. Four months after diagnosis and hormonal therapy adjustment, the patient reported NPRS 2 and ODI 44%, with reduced pain intensity, fewer LBP episodes, and no menstrual exacerbations. At a final follow-up two months later, her NPRS was 1/10 and ODI 14%. During this session it was agreed with the patient to have follow-up calls to monitor symptoms.
| BASELINE | AFTER DIAGNOSIS | 4 MONTHS SINCE DIAGNOSIS | 6 MONTHS SINCE DIAGNOSIS | |
| NPRS | 8 | 9 | 2 | 1 |
| ODI | 64% | 62% | 44% | 14% |
Discussion
This case report emphasizes the critical role of differential diagnosis in the cases where musculoskeletal symptoms do not respond to standard treatment, and it highlights the value of clinical reasoning performed by the physiotherapist in identifying a pathology outside his area of competence.
The patient initially presented with progressive low back pain (LBP) radiating to the lower limb, which significantly impaired her daily activities. During the initial assessment, the condition appeared to be of musculoskeletal origin, with findings such as high levels of pain (8/10), nocturnal symptoms, positive springing tests, and a positive Laslett cluster, leading to the consideration of PGP as a possible diagnosis. At first, symptoms of visceral origin, including dyspareunia and dysmenorrhea, were overlooked, partly due to the patient’s young age. Consequently, the physiotherapy treatment plan focused on musculoskeletal dysfunction and pain control through manual therapy and therapeutic exercise [31,35] However, after five sessions, the patient showed an increase in pain intensity. For this reason, using clinical reasoning and a commitment to ongoing reassessment, the physiotherapist reconsidered the initial diagnosis and referred the patient to a specialized endometriosis centre. Further evaluation confirmed a diagnosis of endometriosis. With an appropriate hormonal therapy, the patient's condition significantly improved, and her pain became sporadic and manageable.
This case brings attention to the fact that endometriosis can also show in very young women, challenging the previously held belief that it predominantly affects older women, a misconception often due to delayed diagnosis [15]. It demonstrates that adolescents may present with atypical symptoms, making diagnosis more complex and prone to delay [14]
Endometriosis can mimic musculoskeletal disorders such as LBP and radicular pain, contributing to misdiagnosis. The disease is also associated with systemic inflammation and central sensitization, which promote chronic pain mechanisms such as allodynia and hyperalgesia [3,8,36].
The research on this topic reveals a central aspect, specifically that endometriosis can easily imitate musculoskeletal symptoms, such as LBP and referred pain, that makes the diagnosis more difficult and often delayed.
Moreover, endometriosis has a documented psychosocial impact: patients frequently experience depression, anxiety, and pain catastrophizing, all of which reduce quality of life and negatively affect social relationships, work performance, and daily functioning [2,8]
This case reinforces the need to consider endometriosis as a differential diagnosis in females, particularly adolescents, presenting with LBP and associated symptoms, especially when conventional treatments prove ineffective. Further studies are needed to identify criteria that can help physiotherapists recognizing the pathology.
A multidisciplinary approach is crucial, combining medical management, physiotherapy, and psychological support to improve outcomes and long-term well-being. Additional research is needed to develop diagnostic criteria that aid physiotherapists in identifying potential gynecological origins of LBP [37].
Conclusion
This case report highlights the importance of adopting a comprehensive and multidisciplinary approach to patient assessment, emphasizing the need for a thorough review of the patient’s medical history and the application of accurate clinical reasoning. It is imperative not to limit the diagnostic process to musculoskeletal pathologies alone, but to actively perform a comprehensive differential diagnosis. In patients with LBP, the potential involvement of gynaecological factors should be considered, even in younger individuals. Continuous reassessment of therapeutic progress is essential to ensure that both diagnostic process and treatment strategies remain appropriate and effective. In cases involving endometriosis, a multidisciplinary approach, that integrates the expertise of various healthcare professionals, is crucial to delivering optimal, patient-centred care that addresses all dimensions of the disease.
Informed Consent
The patient gave her consent to create this work.
Disclosure
The authors report no conflict of interest concerning the financial aspect or personal relationships that could have influenced this work.
Abbreviations
| OMPT | Orthopaedic Manipulative Physical Therapist |
| NPRS | Numerical Pain Rating Scale |
| LBP | low back pain |
| SLR | Straight Leg Raise |
| PGP | Pelvic Girdle Pain |
| LDL | Long Dorsal Sacroiliac Ligament |
| TrPs | Trigger Points |
| ODI | Oswestry Disability Index |
| MT | Manual Therapy |
| NSAIDs | Non-steroidal Anti-inflammatory Drugs |
| MRI | Magnetic Resonance Imaging |
References
- Agarwal, N. , Subramanian, A., 2010. Endometriosis – Morphology, Clinical Presentations and Molecular Pathology. J. Lab. Physicians 2, 1–9. [CrossRef]
- Airaksinen, O. , Brox, J.I., Cedraschi, C., Hildebrandt, J., Klaber-Moffett, J., Kovacs, F., Mannion, A.F., Reis, S., Staal, J.B., Ursin, H., Zanoli, G., COST B13 Working Group on Guidelines for Chronic Low Back Pain, 2006. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 15 Suppl 2, S192-300. [CrossRef]
- Aredo, J.V. , Heyrana, K.J., Karp, B.I., Shah, J.P., Stratton, P., 2017. Relating Chronic Pelvic Pain and Endometriosis to Signs of Sensitization and Myofascial Pain and Dysfunction. Semin. Reprod. Med. 35, 88–97. [CrossRef]
- Bajaj, P. , 2003. Endometriosis is associated with central sensitization: a psychophysical controlled study. J. Pain 4, 372–380. [CrossRef]
- Carbone, M.G. , Campo, G., Papaleo, E., Marazziti, D., Maremmani, I., 2021. The Importance of a Multi-Disciplinary Approach to the Endometriotic Patients: The Relationship between Endometriosis and Psychic Vulnerability. J. Clin. Med. 10, 1616. [CrossRef]
- Ceccaroni, M. , Bounous, V.E., Clarizia, R., Mautone, D., Mabrouk, M., 2019. Recurrent endometriosis: a battle against an unknown enemy. Eur. J. Contracept. Reprod. Health Care Off. J. Eur. Soc. Contracept. 24, 464–474. [CrossRef]
- Chen, S. , Xie, W., Strong, J.A., Jiang, J., Zhang, J.-M., 2016. Sciatic endometriosis induces mechanical hypersensitivity, segmental nerve damage, and robust local inflammation in rats. Eur. J. Pain Lond. Engl. 20, 1044–1057. [CrossRef]
- Crump, J. , Suker, A., White, L., 2024. Endometriosis: A review of recent evidence and guidelines. Aust. J. Gen. Pract. 53, 11–18. [CrossRef]
- Denny, E. , 2004. Women’s experience of endometriosis. J. Adv. Nurs. 46, 641–648. [CrossRef]
- Dessole, M. , Melis, G. Endometriosis in Adolescence. Obstet. Gynecol. Int. 2012, 869191. [Google Scholar] [CrossRef]
- Dun, E.C. , Kho, K.A., Morozov, V.V., Kearney, S., Zurawin, J.L., Nezhat, C.H., 2015. Endometriosis in Adolescents. JSLS 19, e2015.00019. [CrossRef]
- Endometriosis guideline [WWW Document], n.d. URL https://www.eshre.eu/guideline/endometriosis (accessed 4.21.25).
- Facchin, F. , Barbara, Giussy, Saita, Emanuela, Mosconi, Paola, Roberto, Anna, Fedele, Luigi, and Vercellini, P., 2015. Impact of endometriosis on quality of life and mental health: pelvic pain makes the difference. J. Psychosom. Obstet. Gynecol. 36, 135–141. [CrossRef]
- Fang, Q.Y. , Campbell, N., Mooney, S.S., Holdsworth-Carson, S.J., Tyson, K., 2024. Evidence for the role of multidisciplinary team care in people with pelvic pain and endometriosis: A systematic review. Aust. N. Z. J. Obstet. Gynaecol. 64, 181–192. [CrossRef]
- Floyd, J.R. , Keeler, E.R., Euscher, E.D., McCutcheon, I.E., 2011. Cyclic sciatica from extrapelvic endometriosis affecting the sciatic nerve. [CrossRef]
- Fourquet, J. , Báez, L., Figueroa, M., Iriarte, R.I., Flores, I., 2011. Quantification of the Impact of Endometriosis Symptoms on Health Related Quality of Life and Work Productivity. Fertil. Steril. 96, 107–112. [CrossRef]
- George, S.Z. , Fritz, J.M., Silfies, S.P., Schneider, M.J., Beneciuk, J.M., Lentz, T.A., Gilliam, J.R., Hendren, S., Norman, K.S., 2021. Interventions for the Management of Acute and Chronic Low Back Pain: Revision 2021. J. Orthop. Sports Phys. Ther. 51, CPG1–CPG60. [CrossRef]
- Hudelist, G. , Fritzer, N., Thomas, A., Niehues, C., Oppelt, P., Haas, D., Tammaa, A., Salzer, H., 2012. Diagnostic delay for endometriosis in Austria and Germany: causes and possible consequences. Hum. Reprod. 27, 3412–3416. [CrossRef]
- Laslett, M. , Williams, M., 1994. The reliability of selected pain provocation tests for sacroiliac joint pathology. Spine 19, 1243–1249. [CrossRef]
- Leuenberger, J. , Kohl Schwartz, A.S., Geraedts, K., Haeberlin, F., Eberhard, M., von Orellie, S., Imesch, P., Leeners, B., 2022. Living with endometriosis: Comorbid pain disorders, characteristics of pain and relevance for daily life. Eur. J. Pain Lond. Engl. 26, 1021–1038. [CrossRef]
- May, S. , Aina, A., 2012. Centralization and directional preference: A systematic review. Man. Ther. 17, 497–506. [CrossRef]
- Monticone, M. , Baiardi, P., Ferrari, S., Foti, C., Mugnai, R., Pillastrini, P., Vanti, C., Zanoli, G., 2009. Development of the Italian version of the Oswestry Disability Index (ODI-I): A cross-cultural adaptation, reliability, and validity study. Spine 34, 2090–2095. [CrossRef]
- Oertel, J. , Sharif, S., Zygourakis, C., Sippl, C., 2024. Acute low back pain: Epidemiology, etiology, and prevention: WFNS spine committee recommendations. World Neurosurg. X 22, 100313. [CrossRef]
- Sachedin, A. , Todd, N., 2020. Dysmenorrhea, Endometriosis and Chronic Pelvic Pain in Adolescents. J. Clin. Res. Pediatr. Endocrinol. 12, 7–17. [CrossRef]
- Shim, J.Y. , Laufer, M.R., 2020. Adolescent Endometriosis: An Update. J. Pediatr. Adolesc. Gynecol. 33, 112–119. [CrossRef]
- Skytte, L. , May, S., Petersen, P., 2005. Centralization: its prognostic value in patients with referred symptoms and sciatica. Spine 30, E293-299. [CrossRef]
- Soliman, A.M. , Coyne,Karin S., Zaiser,Erica, Castelli-Haley,Jane, and Fuldeore, M.J., 2017. The burden of endometriosis symptoms on health-related quality of life in women in the United States: a cross-sectional study. J. Psychosom. Obstet. Gynecol. 38, 238–248. [CrossRef]
- Song, S.Y. , Jung, Y.W., Shin, W., Park, M., Lee, G.W., Jeong, S., An, S., Kim, K., Ko, Y.B., Lee, K.H., Kang, B.H., Lee, M., Yoo, H.J., 2023. Endometriosis-Related Chronic Pelvic Pain. Biomedicines 11, 2868. [CrossRef]
- Tawa, N. , Rhoda, A., Diener, I., 2017. Accuracy of clinical neurological examination in diagnosing lumbo-sacral radiculopathy: a systematic literature review. BMC Musculoskelet. Disord. 18, 93. [CrossRef]
- Taylor, H.S. , Kotlyar, A.M., Flores, V.A., 2021. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. The Lancet 397, 839–852. [CrossRef]
- Uppal, J. , Sobotka, S., Jenkins III, A.L., 2017. Cyclic sciatica and back pain responds to treatment of underlying endometriosis: case illustration. World Neurosurg. 97, 760-e1.
- Vleeming, A. , Albert, H.B., Ostgaard, H.C., Sturesson, B., Stuge, B., 2008. European guidelines for the diagnosis and treatment of pelvic girdle pain. Eur. Spine J. Off. Publ. Eur. Spine Soc. Eur. Spinal Deform. Soc. Eur. Sect. Cerv. Spine Res. Soc. 17, 794–819. [CrossRef]
- Williamson, A. , Hoggart, B., 2005. Pain: a review of three commonly used pain rating scales. J. Clin. Nurs. 14, 798–804. [CrossRef]
- Woolf, A.D. , Pfleger, B., 2003. Burden of major musculoskeletal conditions. Bull. World Health Organ. 81, 646–656.
- Wu, Z. , Huang, G., Ai, J., Liu, Y., Pei, B., 2024. The burden of low back pain in adolescents and young adults. J. Back Musculoskelet. Rehabil. 37, 955–966. [CrossRef]
- Zaina, F. , Côté, P., Cancelliere, C., Di Felice, F., Donzelli, S., Rauch, A., Verville, L., Negrini, S., Nordin, M., 2023. A Systematic Review of Clinical Practice Guidelines for Persons With Non-specific Low Back Pain With and Without Radiculopathy: Identification of Best Evidence for Rehabilitation to Develop the WHO’s Package of Interventions for Rehabilitation. Arch. Phys. Med. Rehabil. 104, 1913–1927. [CrossRef]
- Zanette, G. , Magrinelli, F., Tamburin, S., 2014. Periodic thigh pain from radicular endometriosis. Pract. Neurol. 14, 351–353. [CrossRef]
Figure 1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



