
Submitted:
08 May 2025
Posted:
09 May 2025
You are already at the latest version
Abstract
Background: Eosinophilic esophagitis is a chronic immune-mediated disease with increasing prevalence. In pediatric populations, it often coexists with IgE-mediated food sensitization. This dual diagnosis presents unique therapeutic challenges, including on the one hand both temporary and lifelong dietary restrictions and on the other hand therapeutic interventions with a potential impact on quality of life (QoL). Objectives: This study prospectively evaluated the prevalence of IgE-mediated food sensitization and allergy in children with EoE attending a tertiary center in Flanders, Belgium. Additionally, it prospectively documented dietary habits and restrictions in these children, with or without concomitant IgE-mediated food allergies, and assessed the impact of dietary management on quality of life compared to pharmacological treatment. Methods: We consecutively followed 30 children with biopsy-confirmed pediatric EoE (PedEoE) attending a tertiary referral center, for at least 12 months. Patient demographics, allergy testing, dietary history and treatment modalities were recorded. Symptom score and PedEoE QoL was assessed using validated Pediatric Eosinophilic Esophagitis Symptom Score (PEESS 2.0) and Pediatric Quality of Life Inventory (PedsQL 3.0) questionnaires. Statistical analysis was performed using Mann-Whitney U test and Kruskal-Wallis test with Dunn’s test as a post-hoc test. Results: Among 30 children with EoE (60% male, median age 8 years), 60 PedEoE QoL (PedsQL) and 39 symptom (PEESS) questionnaires were collected at one or more time points over a median follow-up of 14.5 months. IgE sensitization to common dietary triggers was observed in multiple patients, with varying clinical reactivity. Symptom scores tended to be higher in children without histological remission, though differences were not statistically significant (median PEESS 23.75 vs. 17.50, p = 0.1934). Grouped by degree of dietary restriction, QoL scores differed significantly (child p = 0.0102; parent p = 0.0203), with better QoL for children and parents when 1 or 2 food products were excluded from the diet in comparison to more excluded food products or treatment by medication only. Conclusions: IgE sensitization is prevalent among pediatric EoE patients and has significant clinical implications for disease management. Treatment choice can influence not only disease control but also the QoL of both patients and their families.
Keywords:
pediatric eosinophilic esophagitis
; food sensitization
; QoL
1. Introduction
Eosinophilic esophagitis (EoE) is a chronic, food antigen-mediated disease characterized by a local eosinophilic inflammation of the esophagus. It is estimated to affect approximately 1 in 2000 individuals, but its incidence has been increasing. In pediatric EoE (PedEoE), symptoms vary depending on the age of the child, with vomiting, nausea and feeding difficulties resulting in failure to thrive being prominent in young children and nighttime cough, epigastric pain, dysphagia and even food impaction in older children and adolescents [1,2,3]. The diagnosis of EoE requires a combination of symptoms of esophageal dysfunction, macroscopic evidence of esophageal inflammation observed during endoscopy, and histological confirmation of eosinophilic infiltration—defined as at least 15 eosinophils per high-power field—in esophageal biopsy specimens obtained from multiple levels of the esophagus [1,4]. The management of PedEoE necessitates a multidisciplinary approach. According to the PedEoE guidelines published in 2014, high-dose proton pump inhibitors (PPIs) were recommended as the first-line treatment. For patients who did not achieve remission with PPI therapy, the guidelines recommended either topical corticosteroid (tCS) therapy or dietary elimination strategies [5]. The updated PedEoE guidelines now recommend PPIs, tCS and dietary therapy as equally valuable first-line treatments for PedEoE [4]. The choice among these options should be tailored to the individual patient’s clinical situation and preferences. In Europe, the six most common dietary triggers for EoE are cow’s milk (CM), hen’s egg (HE), wheat, soy, (pea)nuts, and (shell)fish. When dietary elimination is selected, it involves the complete avoidance of one or more of these triggers, implemented either through a step-down or step-up approach [6]. Therapeutic efficacy is evaluated using a combination of symptom scoring and follow-up endoscopies. The primary objectives of treatment include achieving symptom relief, improving quality of life (QoL), and preventing long-term complications such as esophageal strictures and fibrosis, which are associated with persistent eosinophilic infiltration [7].
Although EoE is generally considered a non-IgE-mediated disorder in adults, more recent literature indicates that 40–74% of children diagnosed with EoE exhibit concomitant IgE-mediated food sensitization or allergy [1,8]. Additionally, the occurrence of EoE following tolerance induction protocols or during oral immunotherapy for a specific food further suggests a link between EoE and IgE-mediated food allergy [8]. This highlights the necessity of tailoring therapeutic approaches to each individual patient. A standardized dietary strategy may not be universally applicable in patients with EoE, particularly in the context of concomitant IgE-mediated food allergies. For instance, the reintroduction of a specific food in a patient with an IgE-mediated allergy after tolerance acquisition over time may - even if perfectly tolerated - still lead to EoE symptoms if that food is also a trigger of their EoE. This underscores the importance of a personalized approach that considers both the immunological complexity and the potential interplay between EoE and IgE-mediated food allergy.
The aim of this study is to prospectively register during ≥ 12 months dietary habits and restrictions in children diagnosed with EoE with or without concomitant IgE-mediated food allergy in a single center. Secondary, this study seeks to assess the impact of adhering to dietary regimens in these children in comparison to pharmacological treatments (PPI or tCS) on the QoL of both the affected patients and their families and whether changes in the dietary guidance could have an impact on the QoL of these children and their families.
2. Materials and Methods
2.1. Study Population
We consecutively enrolled 30 children (age ≤ 16 years at baseline) with PedEoE, attending the pediatric gastro-enterology or pediatric allergology department at a tertiary center between October 2020 and November 2023 and in whom diagnosis was retained between January 1, 2014 and December 31, 2021. Diagnosis was based on symptoms and histological findings of ≥15 eosinophils per high-power field on esophageal biopsy [4]. Exclusion criteria for the study were children older than 16 years at time of inclusion and other causes of esophageal eosinophilia such as gastro-esophageal reflux disease. Patient characteristics, allergy testing, histological findings and treatment history were extracted from electronic medical records. Parents and children gave informed consent and assent respectively. These 30 children with PedEoE were prospectively followed for at least 12 months at the pediatric gastro-enterology or allergology division at the University Hospitals Leuven, a pediatric tertiary referral center in Belgium. At different standard of care visits, these children and their parents were asked to complete two validated Dutch-translated questionnaires: the Pediatric Quality of Life Inventory (PedsQL, version 3.0) and the Pediatric Eosinophilic Esophagitis Symptom Score (PEESS, version 2.0) [9,10]. PedsQL encompasses 7 Scales: Symptoms I (consisting of 6 items), Symptoms II (4 items), Treatment (5 items), Worry (6 items), Communication (5 items), Food and Eating (4 items) and Food Feelings (3 items). Each of these items recalls the past week. Items are reverse-scored and linearly transformed to a 0–100 scale. Child self-report forms, and parent proxy-report forms in parallel, are specific for ages 5–7 (young child), 8–12 (child), and 13–18 years (adolescent). In addition, there is also a parent proxy-report form for children aged 2-4 years (toddler). PEESS is a self-report patient-reported outcome measure for children 8-18 years designed to assess symptom severity and frequency of the past month in children with EoE. The PEESS questionnaire includes items covering various symptom domains, such as dysphagia, pain, and food-related difficulties, as reported by patients. Items are linearly transformed to a 0-100 scale.
2.2. Data Analysis
Data analysis was performed using GraphPad Prism (version 9.3.0 (463) for Windows, GraphPad Software, San Diego, California USA). Continuous variables were reported as medians with interquartile ranges (IQR). QoL assessments were conducted using the Mann-Whitney U test or the Kruskal-Wallis test with the Dunn’s test as post-hoc test. Statistical significance was established as p < 0.05. Specific IgE was levels were measured using the CAP system (Thermo Fisher Scientific) with sensitization cut-off of > 0.10 kU/L.
2.3. Ethical Approval
Ethical approval was obtained from the institutional review board. Patient confidentiality was maintained throughout the study.
3. Results
3.1. Demographics
The cohort of 30 PedEoE patients comprised 18 boys (60%) and 12 girls (40%). The median age at EoE diagnosis was 8 years (IQR 2.9–11.50), while the median age at study inclusion was 11 years (IQR 5.7–15.0). The median duration of follow-up after inclusion was 14.5 months (IQR 10.5–21.0). The medical history of most included patients was unremarkable. However, 2 patients (Patient 26 and Patient 30) were born with esophageal atresia with tracheoesophageal fistula and underwent surgical correction in the first days of life. Participant 21 had duodenal atresia with congenital esophageal stenosis requiring multiple dilations. Additionally, Patient 12 had a history of cystic fibrosis. During study follow-up, the number of gastroscopies per child ranged from 0 to 7: 8 children had none, 13 children had one, 3 children had two, 3 children had three, 1 child had four, 1 child had five, and 1 child underwent seven gastroscopies.
3.2. IgE-Mediated Food Allergy in EoE
The six most common associated dietary triggers for EoE are CM, HE, wheat, soy, (pea)nuts, and (shell)fish. Coincidentally, these six are also the statistically most likely foods to cause an IgE-mediated food allergy in children.
3.2.1. IgE Sensitization to CM
In our PedEoE cohort, seven out of 30 children had detectable sIgE to CM (Figure 1, Table 1). Clear clinical reactions were observed in two of these seven children. Patient 2 developed widespread urticaria along with localized facial swelling and pruritus, whereas Patient 14 experienced diarrhea following CM ingestion. The other children sensitized to CM experienced mostly mild atopic dermatitis for which one or more food products upon sensitization, were dietary excluded, with positive effect on the skin symptoms. During follow up, P11 successfully introduced highly heated CM (sIgE to cow’s milk and components ≤ 0.24 kU/L over time). However, symptoms of dysphagia emerged after four weeks, leading to discontinuation of heated CM ingestion. Recurrence of EoE was confirmed by biopsy four weeks later. Patient 14 first underwent an oral food challenge (OFC) with highly heated (20 minutes cooked) CM based on decreasing sIgE levels to cow’s milk (4.86 kU/L to 0.56 kU/L) and negative IgE to casein. The introduction of highly heated CM was well tolerated without immediate reactions or EoE reactivation. At study completion (3 months after the introduction of highly heated CM), P14 underwent an additional OFC with uncooked CM and again tolerated it without adverse effects nor subsequent EoE reactivation on gastroscopy.
3.2.2. IgE Sensitization to HE
In our cohort of 30 children, seven were sensitized to HE (Figure 1, Table 2), with three of these children exhibiting clinical symptoms upon ingestion of HE. One child (P12) experienced vomiting and periorbital pruritus, P18 developed eczema, and P20 presented with vomiting. During the study period, P11 reintroduced HE based on low sIgE levels to ovomucoid (gal d1 <0.10 kU/L) and decreasing sIgE to egg white (0.30 kU/L to 0.15 kU/L) and to ovalbumin (gal d2 0.31 kU/L to 0.11 kU/L). Highly heated HE (cake) and hard-boiled egg were successfully reintroduced. However, following the introduction of hard-boiled egg, EoE reactivated, necessitating the avoidance of all egg-containing products. Patient 12 tolerated processed products containing HE, such as cookies and pancakes at time of inclusion, though lesser-heated egg products were not introduced during the follow up period. Patient 20 also started the introduction of HE based on low sIgE levels of ovomucoid (decreasing IgE of 0.37 kU/L to 0.27 kU/L) and decreasing sIgE to egg white (0.38 kU/L to 0.32 kU/L). Both highly heated and hard-boiled HE were introduced without immediate reactions, but the patient subsequently experienced EoE recurrence after consuming pancake and omelet, leading to renewed avoidance of all egg forms. Patients 18 and 25 maintained a strict egg-free diet throughout the study, based on their high sIgE to egg white and its components and to egg yolk. In contrast, although Patients 24 and 26 exhibited low sIgE’s to egg white, they preferred not to reintroduce HE and continued an egg-free diet.
3.2.3. IgE Sensitization to Wheat
Among the 30 children in our study, nine were sensitized to wheat (Figure 1, Table 3). Five children (P5, P10, P20, P21 and P24) exhibited concomitant sensitization to grass pollen, suggesting potential cross-reactivity to wheat [11]. Clinical reactivity was only observed in one child: P20 experienced abdominal pain following wheat ingestion, despite low specific IgE levels and concurrent grass pollen allergy. Other patients were on a diet free of wheat based on mildly elevated IgE, although they did not clinically react after wheat consumption. During the study period, P21 underwent a successful OFC to wheat, following a decrease in specific IgE to wheat from 2.16 kU/L to 0.61 kU/L, with no subsequent reactivation of EoE on gastroscopy.
3.2.4. IgE Sensitization to Soy
In our cohort, sensitization to soy was detected in 5 out of 30 children (Figure 1, Table 4). Three of these children (P10, P11, and P21) had a confirmed birch pollen allergy, suggesting potential cross-reactivity with soy (cf. IgE to gly m4 is 100 kU/L in P21) [12]. Clinical reactivity was observed in one child (P20), who experienced vomiting following soy ingestion. Throughout the follow-up period, all children adhered to a strict soy-free diet.
3.2.5. IgE Sensitization to Peanut, Tree Nuts and Legumes
In our study cohort, 14 children were sensitized to peanut and/or tree nuts (Figure 1, Table 5 and Table 6). Clinical reactivity was observed in six cases: Patient 4 developed a skin rash following tree nut ingestion and P18 developed eczema following the ingestion of hazelnut. P12 exhibited dyspnea, angioedema, and urticaria after ingesting chocolate containing hazelnuts. P21 presented with symptoms of oral allergy syndrome (OAS) to hazelnut, and walnut. Similarly, P10 experienced oral pruritus after consuming hazelnuts and P23 experienced symptoms after the ingestion of peanut consistent with OAS. During the observation period, P12 underwent OFCs with peanut, cashew and almond, based on low sIgE levels and minimal skin prick test (SPT) responses. They were initially well tolerated, with no immediate clinical reactions. However, follow-up endoscopy revealed reactivation of EoE, leading to the reimplementation of dietary restrictions on peanut and all tree nuts. The remaining children maintained a peanut- and/or tree nut-free diet throughout the study period.
In literature on EoE, peanuts, lentils, beans, peas, chickpeas, and lupins are frequently categorized under the collective term ‘legumes’. As a result, legumes are often considered in association with peanuts within the context of food elimination therapy [6]. Therefore, in our study, we specifically evaluated sensitization to at least one of these legumes—excluding peanut, which was discussed separately above—in our pediatric EoE cohort. Four children adhered to a legume-free diet. Patients P11 and P28 exhibited both positive sIgE and SPT results to legumes whereas patients P18 and P24 showed elevated sIgE levels to legumes, although SPT results were not available for evaluation (Table 7).
3.2.6. IgE Sensitization to Fish and Shellfish
In our cohort, six children were sensitized to fish and/or shellfish (Figure 1, Table 8). Clinical reactions to (shell)fish ingestion were observed in three children: P01 developed conjunctivitis and vomiting after consuming mussels, P11 experienced a skin rash after the ingestion of tuna (however, no IgE levels or SPT results to tuna were available) and P18 presented with eczema following white fish ingestion. None of the sensitized children introduced fish or shellfish into their diet during the follow-up period.
3.2.7. IgE Sensitization to Other Foods
Six out of 30 children avoided banana in their daily diet. P6 had a sIgE level of 0.12 kU/L to banana and a positive SPT. P10 experienced angioedema following banana ingestion and had an sIgE level of 0.33 kU/L. P11 developed vomiting after consuming bananas and had a positive SPT. P18 exhibited no clinical symptoms but had an sIgE titer of 2.46 kU/L to banana. P23 presented with symptoms consistent with oral allergy syndrome upon banana ingestion and avoided banana for this reason. P24 had a mildly elevated sIgE level to banana (0.14 kU/L).
Five children adhered to a sesame-free diet. P10 and P21 had a positive SPT for sesame, while P12 had an equivocal SPT result. P18 had a highly elevated sIgE level to Ses i1 (20.30 kU/L). Patient 11 followed a sesame-free diet, though no clear documentation was available regarding the reason for dietary avoidance.
Four children (P18, P23, P24, and P25) followed a diet excluding chicken meat. All of these children had elevated sIgE levels to chicken meat, ranging from 0.83 kU/L to 2.62 kU/L. P18, P24 and P25 were known with a concurrent IgE-mediated HE allergy, which may be indicative of “egg-bird syndrome” [13].
Three children adhered to a buckwheat-free diet. P10 had a sIgE level of 1.33 kU/L to buckwheat and a positive SPT. P11 and P24 exhibited elevated sIgE levels to buckwheat, measuring 2.58 kU/L and 7.44 kU/L respectively.
3.3. Symptom Score and Quality of Life Questionnaires
To assess the impact of disease remission and dietary restriction on EoE symptom score and/or on QoL, the following three questionnaires were recorded and analyzed. At each standard-of-care visit, two quality of life questionnaires (child PedsQL and parent PedsQL) and a symptom score questionnaire (PEESS) were provided to each study participant and his/her parents for completion. For children who completed more than one questionnaire, the follow-up duration ranged from 12 to 34 months.
3.3.1. Analysis of PEESS Questionnaires
The PEESS questionnaire is intended for children aged 8 years and older. At the first time point, 20 children met this age criterion, of whom 19 completed the questionnaire. During follow-up, these children continued to complete a PEESS questionnaire at each subsequent time point. In total, 39 questionnaires were completed over the course of the study. The distribution of completed questionnaires per child was as follows: 8 children completed 1 questionnaire, 5 children completed 2 questionnaires, 4 children completed 3 questionnaires, 1 child completed 4 questionnaires, and 1 child completed 5 questionnaires.
3.3.1.1. PEESS Symptom Scores in Relation to Remission Status
Among all completed questionnaires (n = 39), symptom scores were compared between children who were in remission at the time of questionnaire completion and those who were not. The median PEESS score was 17.50 in children in remission (n = 31) and 23.75 in those not in remission (n = 8) (p = 0.1934), suggesting a trend toward greater symptom burden in children without EoE remission, although, this difference was not statistically significant.
When restricting the analysis to the first time point only (n = 19), the median PEESS score was 20.00 in the remission group (n = 12) and 27.50 in the non-remission group (n = 7) (p = 0.3293). While not reaching statistical significance, this again indicated a tendency toward higher symptom severity in children without histological remission.
3.3.1.1. PEESS Symptom Scores in Relation to Treatment Type
A similar analysis across all completed questionnaires (n = 39) compared children receiving dietary treatment (with or without pharmacological therapy) to those on pharmacological therapy alone. Median symptom scores were identical in both groups, at 20.00 (diet group: n = 26; non-diet group: n = 13; p = 0.9472). No significant differences were observed based on the number of foods eliminated, whether none, 1-2, 3-4, 5-6, or more than 6 (p = 0.8490).
At the first time point only (n = 19), the median symptom score in the dietary group (n = 16) was 24.38, compared to 20.00 in the non-diet group (n = 3) (p > 0.9999). Again, no significant differences were observed between children on more extensive versus limited food elimination diets (p = 0.9513).
3.3.2. Analysis of QoL Questionnaires
The child self-report version of the PedsQL is intended for children aged 5 years and older. At the first time point, 27 children met this criterion and completed the child PedsQL. These same children continued to complete the questionnaire at each subsequent time point during follow-up. Additionally, one child—who was almost 4 years old at the start of the study—reached the age of 5 by the fourth- (and last) time point and completed the questionnaire for the first time at that visit. In total, 47 child self-report questionnaires were completed throughout the study period. The distribution of completed questionnaires per child was as follows: 13 children completed 1 questionnaire, 6 children completed 2 questionnaires, 6 children completed 3 questionnaires and 1 child completed 4 questionnaires.
The parent proxy-report version of the PedsQL is available for children aged 2 years and older. At the first time point, all participating children met this age requirement. However, one parent failed to correctly complete the proxy-report form—rendering it invalid—while another did not complete the questionnaire. In total, 58 valid parent proxy-report questionnaires were collected during the study. The distribution was as follows: 12 parents completed 1 questionnaire, 6 parents completed 2 questionnaires, 7 parents completed 3 questionnaires, 2 parents completed 4 questionnaires, and 1 parent completed 5 questionnaires.
3.3.2.1. QoL in Relation to Remission Status
Among all completed questionnaires, there were no significant differences in QoL observed between children with EoE in remission and those not in remission. The median Child PedsQL score was 67.86 in the remission group (n = 38) and 65.48 in the non-remission group (n = 9) (p = 0.3134). Parent-reported QoL scores were also similar, with median scores of 69.44 for children in remission (n = 48) and 65.36 for those not in remission (n = 10) (p = 0.4717).
When again limiting the analysis to the first time point only, there were no significant differences in QoL observed between children with EoE in remission and those not in remission. The median Child PedsQL score was almost identical in the remission group in comparison to the non-remission group: 70.58 in the remission group (n = 19) and 70.08 in the non-remission group (n = 8) (p = 0.9285). Parent-reported QoL scores showed median scores of 77.46 for children in remission (n = 20) and 71.75 for those not in remission (n = 8) (p = 0.6718).
Seven children achieved remission during their follow-up period. QoL scores recorded during remission were compared to those obtained from the same child at a different time when they were not in remission (Table 9). No consistent or systematic differences in QoL scores were observed based on remission status, suggesting that QoL did not markedly decline during non-remission periods compared to remission periods. Patient 1 (timepoint a) and Patient 2 lost remission despite no changes in therapy. At the time of non-remission, P01 increased the dose of tCS to 2 mg twice daily (instead of once daily), while P02 initiated tCS in addition to PPI and a diet free of cow’s milk and (pea)nuts. Both patients subsequently regained remission. Patients P11, P21, P22, and P25 were not in remission at their initial evaluation. P11 adhered to a strict 6 food elimination diet (FED), supplemented with potato, buckwheat, sesame, and lupin seed. P25 was receiving high-dose PPI and initiated tCS, whereas P21 and P22 started tCS alongside a 5FED. All patients subsequently achieved remission.
3.3.2.1. QoL in Relation to Treatment Type
In our cohort of 30 children, six received exclusively pharmacological treatment at baseline, comprising one child on tCS and five children treated with PPIs. Two children adhered to a strict dietary regimen, while 22 received a combination of pharmacological therapy and dietary management. Additionally, one child undergoing combined pharmacological therapy and dietary management required enteral nutrition via a nasogastric tube. In total, at 60 different timepoints a child and/or parent PedsQL questionnaire was completed, and the dietary strategy at these visits is summarized in Table 10.
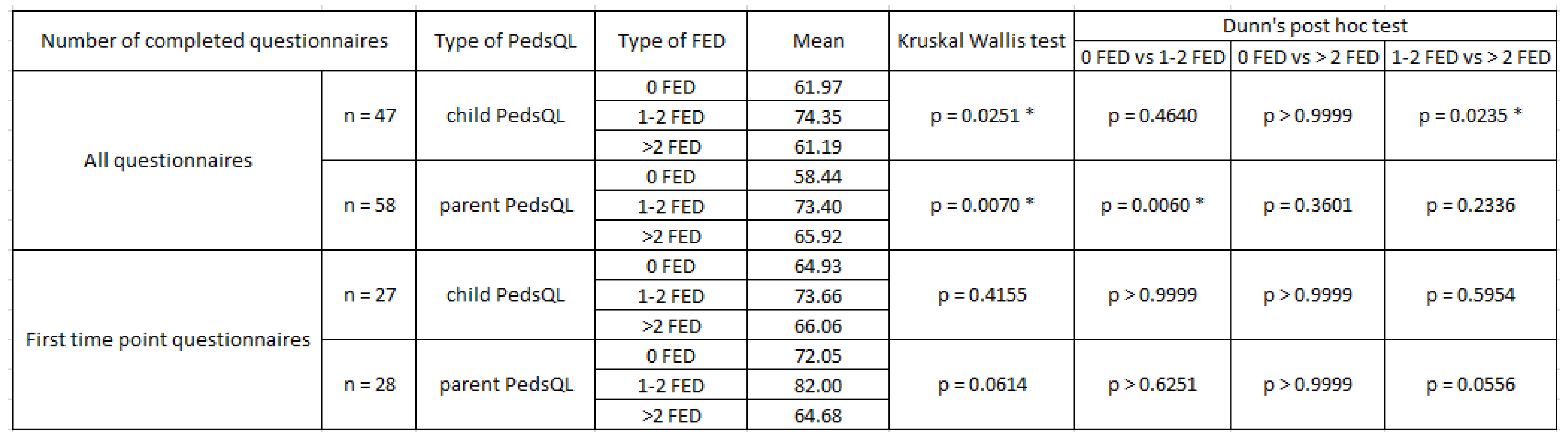
In the total sample of completed questionnaires; QoL assessment showed no significant differences in QoL between children with EoE following a dietary restriction in comparison to those without dietary restrictions. The QoL tended to be slightly better in the non-diet group in comparison to the diet group (the median Child PedsQL score of 65.70 in the diet group (n = 36) and 75.60 in the non-diet group (n = 11) (p = 0.2010)). Parent-reported QoL scores (Parent PedsQL) were slightly inverse; with median scores of 71.13 for the diet group (n = 41) and 64.29 for the no-diet group (n = 17) (p = 0.1463). However; a significant difference in QoL was observed across groups with varying degrees of dietary restriction; categorized by the number of eliminated foods (0; 1-2; 3-4; 5-6; and >6) in both child- and parent-reported assessments: Child PedsQL scores differed significantly between groups (p = 0.0102; n = 47); as did the Parent PedsQL scores (p = 0.0203; n = 58). Additional Dunn’s post hoc analysis showed a higher QoL in children who were on limited food restriction (1 or 2 FED) than in children who were not on a diet or than in children with more than 2 food restrictions (Table 11).
When focusing solely on the first time point, QoL assessment showed no significant differences in QoL between children with EoE following a dietary restriction in comparison to those without dietary restrictions with a median Child PedsQL score of 70.58 in the diet group (n = 21) and 67.75 in the non-diet group (n = 6) (p = 0.7628). Parent-reported QoL scores were similar, with median scores of 73.67 for the diet group (n = 21) and 71.42 for the non-diet group (n = 7) (p = 0.8765).
Additionally, no significant difference in QoL was observed across groups with varying degrees of dietary restriction (0, 1-2, 3-4, 5-6, and >6 foods eliminated) in both child- and parent-reported assessments: p = 0.5243 in child PedsQL (n = 27) and p = 0.2306 in parent PedsQL (n = 28). Similarly as in the total group, post hoc pairwise comparison observed a trend towards better QoL scoring in children on a 1 or 2 food elimination diet than children without a diet or than children who are on more than 2 food restrictions. Although this trend was observed, it no longer reached statistical significance (Table 11).
4. Discussion
This study provides novel insights into the difficult overlap between food-specific IgE sensitization/allergy and eosinophilic inflammation in children with EoE. Our findings suggest that IgE sensitization is prevalent among pediatric EoE patients and may have clinical implications for EoE disease management and patient well-being.
A key observation in our study was the high prevalence of IgE sensitization to food allergens in children with EoE. This finding aligns with prior research indicating that EoE is frequently associated with allergic comorbidities in children with EoE, including IgE-mediated food allergies and environmental allergies [1]. The mechanisms underlying this relationship remain incompletely understood, yet it is hypothesized that epithelial barrier dysfunction and immune dysregulation contribute to both EoE and IgE sensitization [14,15]. In contrast, IgE-mediated food allergy appears to be less commonly described in adult patients with EoE [16]. Despite the high prevalence of IgE sensitization to food allergens reported in children with EoE in literature, clinically manifest allergic reactions such as anaphylaxis are rare [17]. In our cohort, most reactions were limited to mild cutaneous or gastrointestinal symptoms, and no cases of severe reactions or anaphylaxis were observed. As a result, the presence of sensitization has to be considered in clinical decision-making to guide dietary management, particularly when supported by a suggestive clinical history or diagnostic work-up.
Given this overlap between EoE and IgE-mediated allergies, distinguishing between IgE-mediated and non IgE-mediated symptoms poses a clinical challenge as overlapping manifestations—such as vomiting and abdominal pain—can mimic one another. This differentiation becomes even more difficult in cases of mild IgE sensitization with subtle symptoms. Nevertheless, IgE-mediated food allergy symptoms typically occur rapidly—within two hours after ingestion of the culprit food—whereas EoE is characterized by a delayed onset of symptoms [18]. The diagnostic complexity highlights the need for a comprehensive evaluation of both IgE-mediated allergic mechanisms and EoE-specific pathophysiology in pediatric patients.
This difficult overlap between food-specific IgE sensitization/allergy and EoE extends to dietary management, which is particularly complex in patients with EoE who also present with IgE-mediated food allergies. Moreover, whereas dietary management for EoE is typically maintained on a continuous basis, dietary avoidance in IgE-mediated food allergy may be temporary and subject to re-evaluation over time [19,20]. Indeed, some children eventually outgrow their IgE-mediated food allergy. The development of tolerance, however, follows a variable natural course that depends on the specific food allergen involved. In IgE-mediated CM allergy, the resolution rates have been reported as 19% by four years of age in the United States and 42% by eight years, 64% by the age of twelve years and 79% by sixteen years of age. In a Korean cohort, 50% of children outgrew their CM allergy at a median age of 8.7 years [20]. Similarly for HE allergy, literature demonstrates that 73-89% of the children with an IgE-mediated HE allergy outgrow their allergy by six years of age [20]. In IgE-mediated wheat allergy, 27% of children in a Thai cohort achieved tolerance by four years of age and 69% by nine years. In a Polish cohort, wheat allergy resolution was observed in 20% of children by four years of age, 52% by eight years, 66% by twelve years, and 76% by eighteen years [20]. Resolution rates for IgE-mediated soy allergy have not been extensively studied. In a U.S. cohort, tolerance development was observed in 25% of children by four years of age, 45% by six years, and 69% by ten years [20]. The natural course of tree nut allergy in children remains poorly studied. A 2005 publication reported that 8.9% of children with prior clinical reactivity and sensitization to tree nuts outgrew their allergy. In contrast, resolution rates for IgE-mediated peanut allergy are well documented, with studies indicating that 22% of children and adolescents outgrow peanut allergy by four years of age and 29% by six years [20]. Natural tolerance development for fish and shellfish is less common compared to other food allergens. A Greek study reported that complete tolerance to fish increased with age, from 3.4% in preschool-aged children to 45% in adolescents. Similarly, a study in Canada estimated resolution rates of 0.6% per person-year for fish and 0.8% per person-year for shellfish [20]. Mostly, reintroduction of a specific allergen in IgE-mediated food allergy can be guided by food specific IgE decline [21]. However, a decline in IgE levels to a specific food over time does not necessarily indicate that the food can be safely reintroduced and/or the presence of specific IgE levels does not necessarily rule out tolerance [22]. While the absence of immediate IgE-mediated symptoms after ingestion may suggest clinical tolerance, the potential for EoE reactivation however remains, necessitating renewed and later on continued dietary restriction. These considerations underscore the importance of individualized dietary strategies that address both IgE-mediated and non-IgE-mediated mechanisms of disease.
Besides the decline in specific IgE, a decline in food-specific IgE components might point to partial tolerance induction. Indeed, as observed in IgE-mediated CM or HE allergy, tolerance can develop gradually over time through exposure to progressively less heated forms of the allergen [23]. The introduction of highly heated proteins can even accelerate the process of tolerance induction [24]. Potentially, heated allergens could also play a role in food tolerance induction in EoE. In a recent case report, we described two children with EoE (also included in this cohort, P11 and P20) in whom the introduction of extensively heated HE was well tolerated, whereas subsequent exposure to less heated forms of HE (hard-boiled egg and pancake respectively) resulted in disease reactivation [25]. These findings suggest that certain heated proteins may be tolerated in some children with EoE. To further investigate whether this approach could safely broaden dietary options, we are currently conducting the PedEoE IgE study (NCT06381219), which explores the feasibility of introducing extensively heated CM or HE in a cohort of children with CM- or HE-induced EoE, while remaining in remission. This might have a positive impact on the children’s QoL.
Indeed, beyond dietary considerations, the impact of multiple food restrictions on QoL in pediatric EoE patients is another critical aspect of EoE management. In our study, we observed that dietary restrictions negatively affected child reported QoL and that there is a significant difference in QoL between groups with varying degrees of dietary restriction. Children avoiding one or two food products seem to have better QoL scores (child PedsQL as well as parent PedsQL scores) than those who have to avoid more than two food products and/or than those who are on pharmacological treatment only. However, the small cohort number might limit the power of this observation, which can be seen as a limitation of this study.
Furthermore, the accuracy and reliability of questionnaire-based QoL assessments in pediatric EoE patients must be carefully considered. Parental influence during questionnaire completion may introduce bias, as parents may inadvertently guide their child's responses when present in the room. Additionally, young children may struggle to recall past events accurately, as their sense of time is still developing. These factors should be considered when interpreting QoL data in a young study population.
5. Conclusions
In conclusion, our findings underscore the importance of considering IgE sensitization when evaluating the clinical profile and QoL in children with EoE. Additionally, the incorporation of multidisciplinary care approaches may enhance disease management and improve overall patient outcomes. Further research is needed to clarify the role of IgE sensitization in EoE pathophysiology and to develop tailored interventions that address both the IgE- and non IgE-mediated aspects of the disease. In this age group, the concurrent development of tolerance to specific food allergens in IgE-mediated food allergy may present an additional challenge for pediatricians managing EoE in children compared to EoE in adolescents or adults.
Author Contributions
Conceptualization, L.N. and D.B.; methodology, L.N. and D.B.; software, L.N.; validation, L.N. and D.B.; formal analysis, L.N.; investigation, L.N.; resources, L.N. and T.D.; data curation, L.N.; writing—original draft preparation, L.N..; writing—review and editing, D.B., T.D, C.K., T.A, S.V., M.D., T.B., I.H. and R.S.; visualization, L.N.; supervision, D.B.; project administration, L.N.; funding acquisition, D.B. and R.S. All authors have read and agreed to the published version of the manuscript.
Funding
The authors declare financial support was received for this project. This project was supported by a Vlaanderen National Fund for Scientific Research (FWO) TBM grant (T000623N). DB is currently supported by a KU Leuven Special Research Fund mandate (BOF-FKO, 3M230694) and R.S. is supported by an FWO senior clinical investigator fellowship (1805523N). The funder(s) had no role in the design and conduct of the study, collection, management, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of KU Leuven (S64441).
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| EoE | Eosinophilic esophagitis |
| PedEoE | Pediatric EoE |
| PPI | Proton pump inhibitor |
| tCS | Topical corticosteroid |
| CM | Cow’s milk |
| HE | Hen’s egg |
| QoL | Quality of life |
| PedsQL | Pediatric Quality of Life Inventory |
| PEESS | Pediatric Eosinophilic Esophagitis Symptom Score |
| OFC | Oral food challenge |
| sIgE | Specific IgE |
| OAS | Oral allergy syndrome |
| SPT | Skin prick test |
| FED | Food elimination diet |
References
- Dominicus, T.; Nuyttens, L.; Hoffman, I.; Bullens, D.M.A. Pediatric eosinophilic esophagitis: a Belgian single-center retrospective analysis reveals real-life difficulties in diagnosis and treatment. Front. Allergy 2024, 5, 1478380. [Google Scholar] [CrossRef] [PubMed]
- Barni, S.; Arasi, S.; Mastrorilli, C.; Pecoraro, L.; Giovannini, M.; Mori, F.; Liotti, L.; Saretta, F.; Castagnoli, R.; Caminiti, L.; et al. Pediatric eosinophilic esophagitis: a review for the clinician. Ital. J. Pediatr. 2021, 47, 1–14. [Google Scholar] [CrossRef]
- Oliva, S.; Dias, J.A.; Rea, F.; Malamisura, M.; Espinheira, M.C.; Papadopoulou, A.; et al. Characterization of Eosinophilic Esophagitis From the European Pediatric Eosinophilic Esophagitis Registry (pEEr) of ESPGHAN. J Pediatr Gastroenterol Nutr. 2022, 75, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Amil-Dias, J.; Oliva, S.; Papadopoulou, A.; Thomson, M.; Gutiérrez-Junquera, C.; Kalach, N.; Orel, R.; Auth, M.K.; Nijenhuis-Hendriks, D.; Strisciuglio, C.; et al. Diagnosis and management of eosinophilic esophagitis in children: An update from the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN). J. Pediatr. Gastroenterol. Nutr. 2024, 79, 394–437. [Google Scholar] [CrossRef]
- Papadopoulou, A.; Koletzko, S.; Heuschkel, R.; Dias, J.; Allen, K.; Murch, S.; Chong, S.; Gottrand, F.; Husby, S.; Lionetti, P.; et al. Management Guidelines of Eosinophilic Esophagitis in Childhood. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 107–118. [Google Scholar] [CrossRef]
- De Vlieger, L.; Smolders, L.; Nuyttens, L.; Verelst, S.; Breynaert, C.; Vanuytsel, T.; Hoffman, I.; Bullens, D.M. A Clinical Perspective on the Dietary Therapies for Pediatric Eosinophilic Esophagitis: The Gap Between Research and Daily Practice. Front. Immunol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Gonsalves, N.P.; Aceves, S.S. Diagnosis and treatment of eosinophilic esophagitis. J. Allergy Clin. Immunol. 2020, 145, 1–7. [Google Scholar] [CrossRef]
- Burk, C.M.; Shreffler, W.G. Triggers for eosinophilic esophagitis (EoE): The intersection of food allergy and EoE. J. Allergy Clin. Immunol. 2024, 153, 1500–1509. [Google Scholar] [CrossRef]
- Franciosi, J.P.; Hommel, K.A.; Bendo, C.B.; King, E.C.; Collins, M.H.; Eby, M.D.; et al. PedsQL eosinophilic esophagitis module: Feasibility, reliability, and validity. J Pediatr Gastroenterol Nutr. 2013, 57, 57–66. [Google Scholar] [CrossRef]
- Martin, L.J.; Franciosi, J.P.; Collins, M.H.; Abonia, J.P.; Lee, J.J.; Hommel, K.A.; Varni, J.W.; Grotjan, J.T.; Eby, M.; He, H.; et al. Pediatric Eosinophilic Esophagitis Symptom Scores (PEESS v2.0) identify histologic and molecular correlates of the key clinical features of disease. J. Allergy Clin. Immunol. 2015, 135, 1519–1528.e8. [Google Scholar] [CrossRef]
- Nilsson, N.; Nilsson, C.; Ekoff, H.; Wieser-Pahr, S.; Borres, M.P.; Valenta, R.; Hedlin, G.; Sjölander, S. Grass-Allergic Children Frequently Show Asymptomatic Low-Level IgE Co-Sensitization and Cross-Reactivity to Wheat. Int. Arch. Allergy Immunol. 2018, 177, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Kato, Y.; Morikawa, T.; Fujieda, S. Comprehensive review of pollen-food allergy syndrome: Pathogenesis, epidemiology, and treatment approaches. Allergol. Int. 2024, 74, 42–50. [Google Scholar] [CrossRef]
- Hemmer, W.; Klug, C.; Swoboda, I. Update on the bird-egg syndrome and genuine poultry meat allergy. Allergo J. Int. 2016, 25, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-López, E.M.; Hill, D.A. Eosinophilic gastrointestinal disorders and the role for the epithelium in pathogenesis and treatment. Curr. Opin. Pediatr. 2024, 36, 668–673. [Google Scholar] [CrossRef]
- Canani, R.B.; Caminati, M.; Carucci, L.; Eguiluz-Gracia, I. Skin, gut, and lung barrier: Physiological interface and target of intervention for preventing and treating allergic diseases. Allergy 2024, 79, 1485–1500. [Google Scholar] [CrossRef]
- Liacouras, C.A.; Furuta, G.T.; Hirano, I.; Atkins, D.; Attwood, S.E.; Bonis, P.A.; Burks, A.W.; Chehade, M.; Collins, M.H.; Dellon, E.S.; et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. J. Allergy Clin. Immunol. 2011, 128, 3–20.e6. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.J.; Arasi, S.; Ballmer-Weber, B.; Conrado, A.B.; Deschildre, A.; Gerdts, J.; Halken, S.; Muraro, A.; Patel, N.; Van Ree, R.; et al. Risk factors for severe reactions in food allergy: Rapid evidence review with meta-analysis. Allergy 2022, 77, 2634–2652. [Google Scholar] [CrossRef]
- Wilson, J.M.; Li, R.-C.; McGowan, E.C. The Role of Food Allergy in Eosinophilic Esophagitis. J. Asthma Allergy 2020, 13, 679–688. [Google Scholar] [CrossRef]
- Urbani, S.; Dinardo, G.; Artesani, M.C.; Fiocchi, A. Outcomes in eosinophilic esophagitis: current understanding and future directions. Curr. Opin. Allergy Clin. Immunol. 2025, 25, 205–211. [Google Scholar] [CrossRef]
- Jeong, K.; Lee, S. Natural course of IgE-mediated food allergy in children. Clin. Exp. Pediatr. 2023, 66, 504–511. [Google Scholar] [CrossRef]
- Shek, L.P.C.; Soderstrom, L.; Ahlstedt, S.; Beyer, K.; Sampson, H.A. Determination of food specific IgE levels over time can predict the development of tolerance in cow’s milk and hen’s egg allergy. Journal of Allergy and Clinical Immunology 2004, 114, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Anvari, S.; Miller, J.; Yeh, C.Y.; Davis, C.M. IgE-Mediated Food Allergy. Clin Rev Allergy Immunol. 2019, 57, 244–260. [Google Scholar] [CrossRef] [PubMed]
- De Vlieger, L.; Nuyttens, L.; Matton, C.; Diels, M.; Verelst, S.; Leus, J.; Coppens, K.; Sauer, K.; Dilissen, E.; Coorevits, L.; et al. Guided Gradual Egg-Tolerance Induction in Hen's Egg Allergic Children Tolerating Baked Egg: A Prospective Randomized Trial. Front. Allergy 2022, 3, 886094. [Google Scholar] [CrossRef] [PubMed]
- Leonard, S.A.; Nowak-Węgrzyn, A.H. Baked Milk and Egg Diets for Milk and Egg Allergy Management. Immunol. Allergy Clin. North Am. 2016, 36, 147–159. [Google Scholar] [CrossRef]
- Nuyttens, L.; De Vlieger, L.; Ieven, T.; Diels, M.; Bosmans, T.; Van Meerbeeck, S.; et al. Case Report: Eosinophilic esophagitis and hen’s egg tolerance—two cases, treated with topical steroids, showing remission with highly heated but not less heated hen’s egg. Frontiers in Allergy 2025, 6, 1475023. [Google Scholar] [CrossRef]
Figure 1.
Total IgE level (kU/L) and specific IgE levels (kU/L) to different food allergens in individual study patients.
Figure 1.
Total IgE level (kU/L) and specific IgE levels (kU/L) to different food allergens in individual study patients.
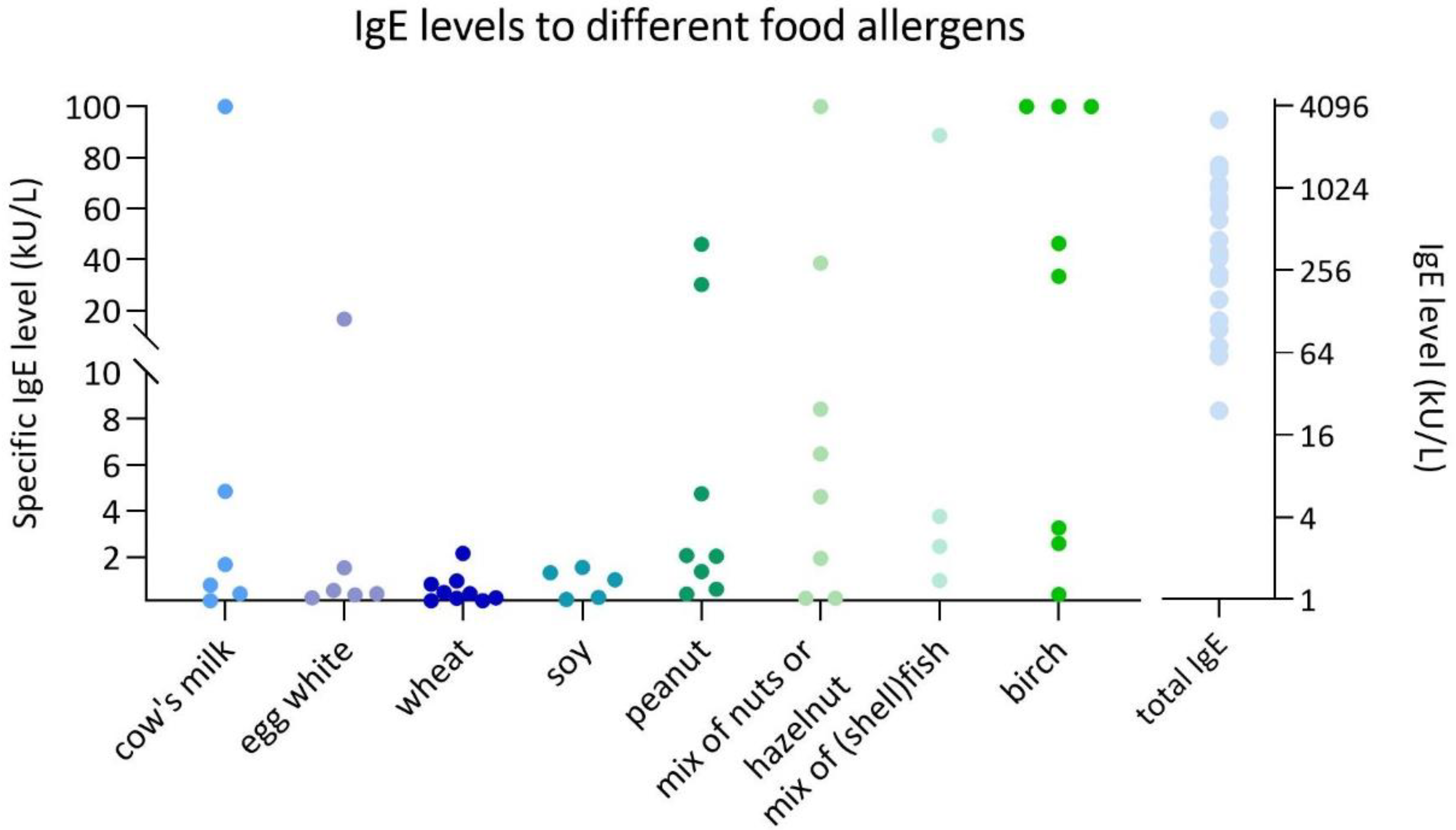

Table 1.
IgE levels (kU/L) of CM and its components in individual study patients at inclusion ± 5 months.
Table 1.
IgE levels (kU/L) of CM and its components in individual study patients at inclusion ± 5 months.
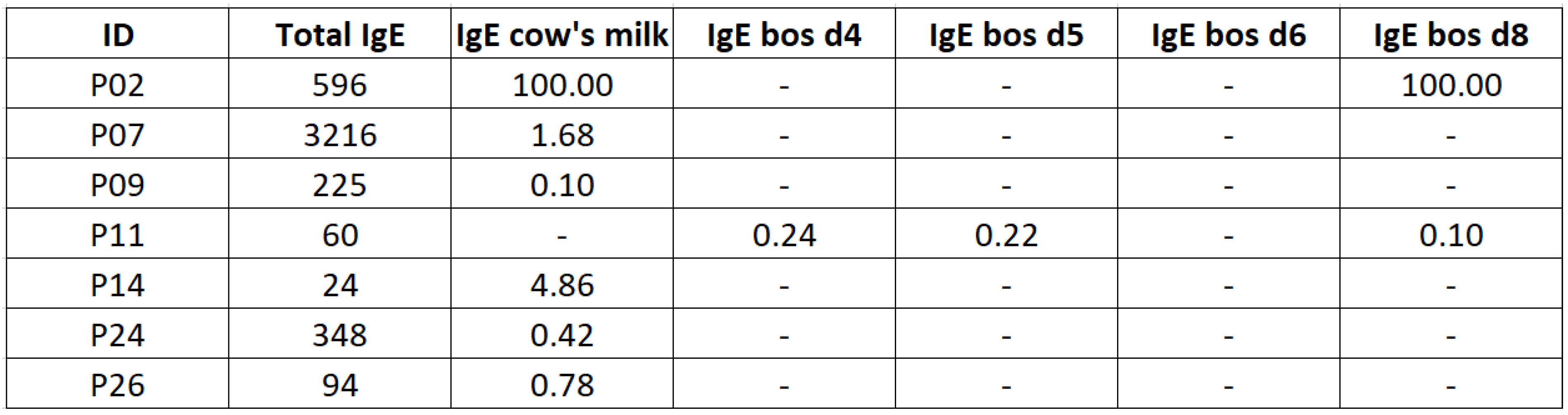 |
Table 2.
IgE levels (kU/L) of HE and its components in individual study patients at inclusion ± 5 months.
Table 2.
IgE levels (kU/L) of HE and its components in individual study patients at inclusion ± 5 months.
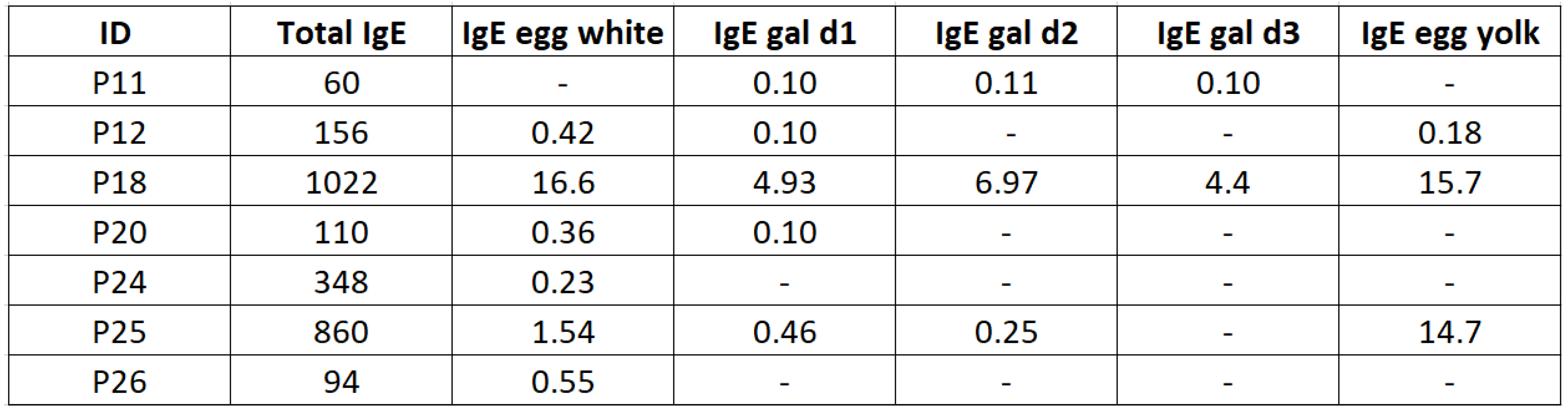 |
Table 3.
IgE levels (kU/L) of wheat and its components in individual study patients at inclusion ± 5 months.
Table 3.
IgE levels (kU/L) of wheat and its components in individual study patients at inclusion ± 5 months.
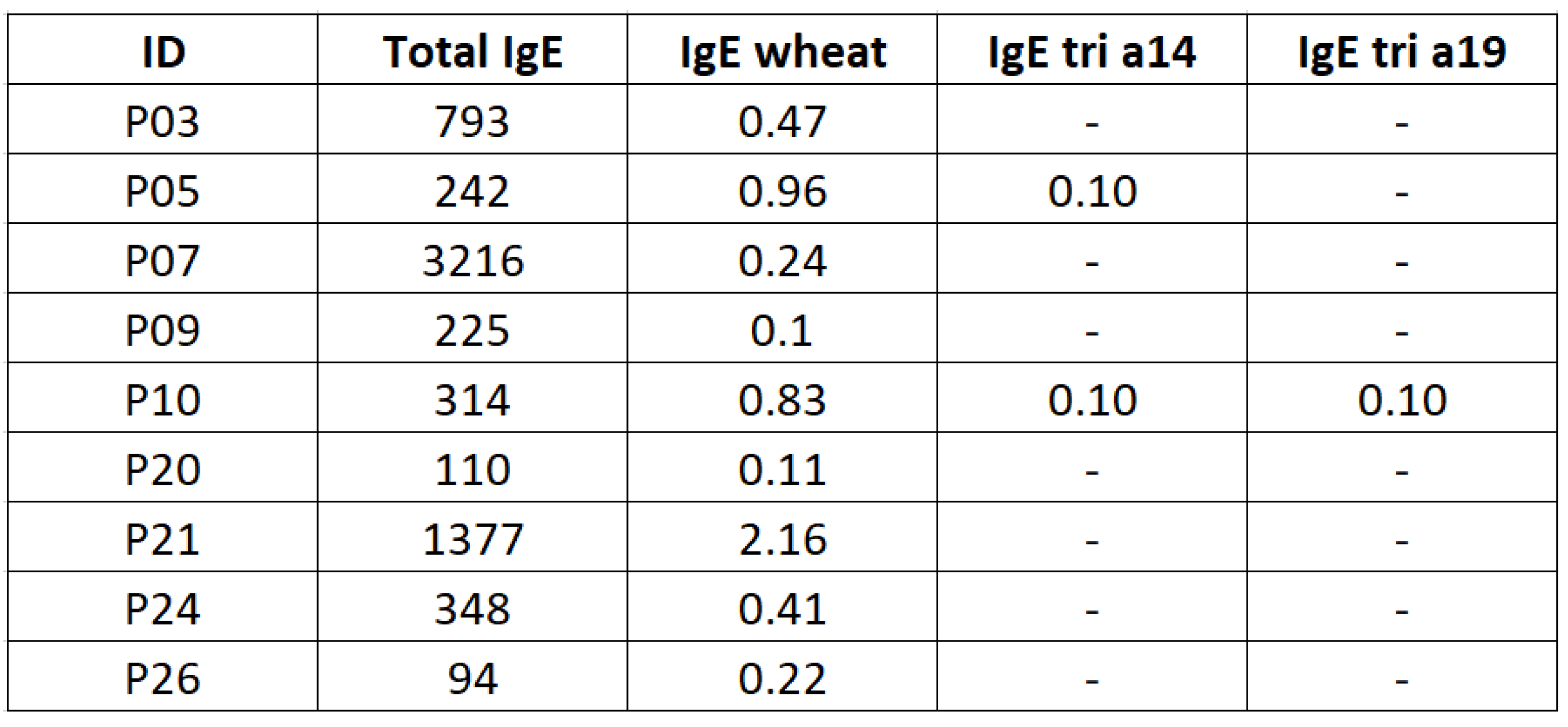 |
Table 4.
IgE levels (kU/L) of soy and its components in individual study patients at inclusion ± 5 months.
Table 4.
IgE levels (kU/L) of soy and its components in individual study patients at inclusion ± 5 months.
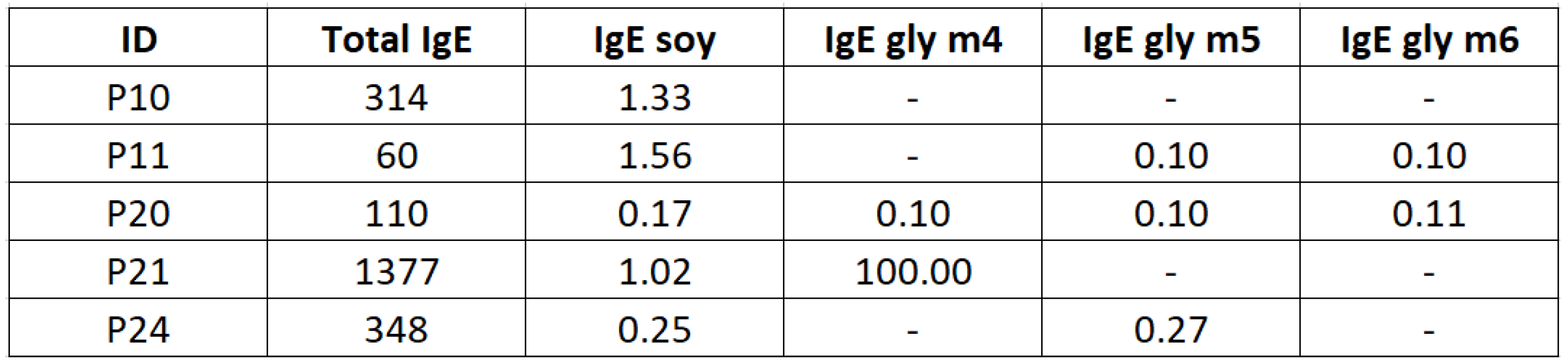 |
Table 5.
IgE levels (kU/L) of peanut and its components in individual study patients at inclusion ± 5 months.
Table 5.
IgE levels (kU/L) of peanut and its components in individual study patients at inclusion ± 5 months.
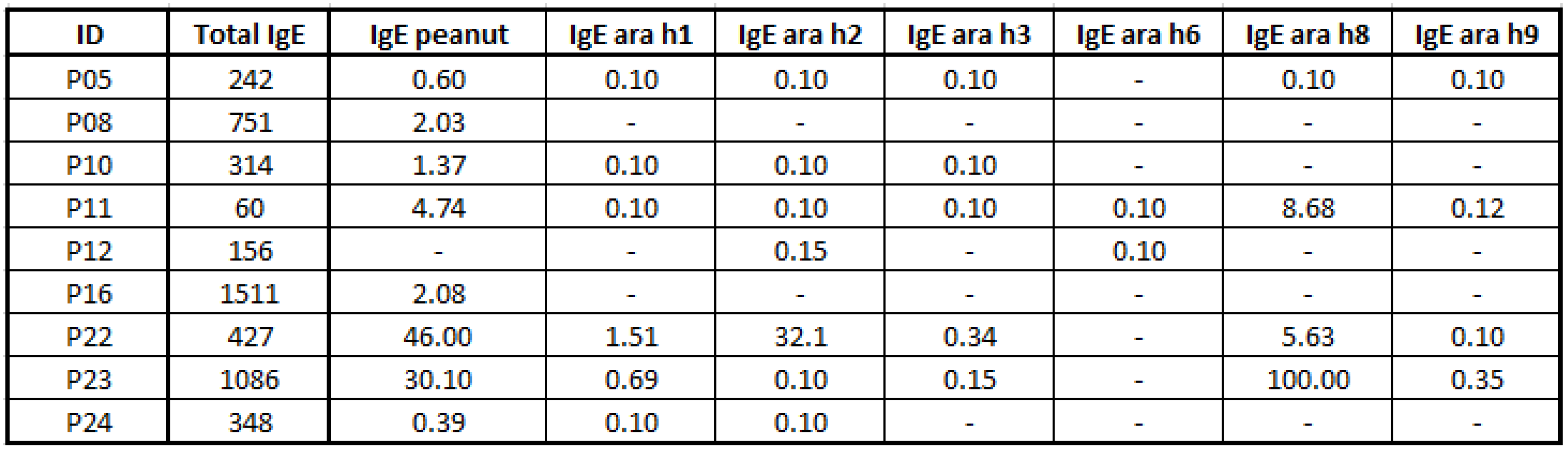 |
Table 6.
IgE levels (kU/L) of the different tree nuts and its components in individual study patients at inclusion ± 5 months.
Table 6.
IgE levels (kU/L) of the different tree nuts and its components in individual study patients at inclusion ± 5 months.
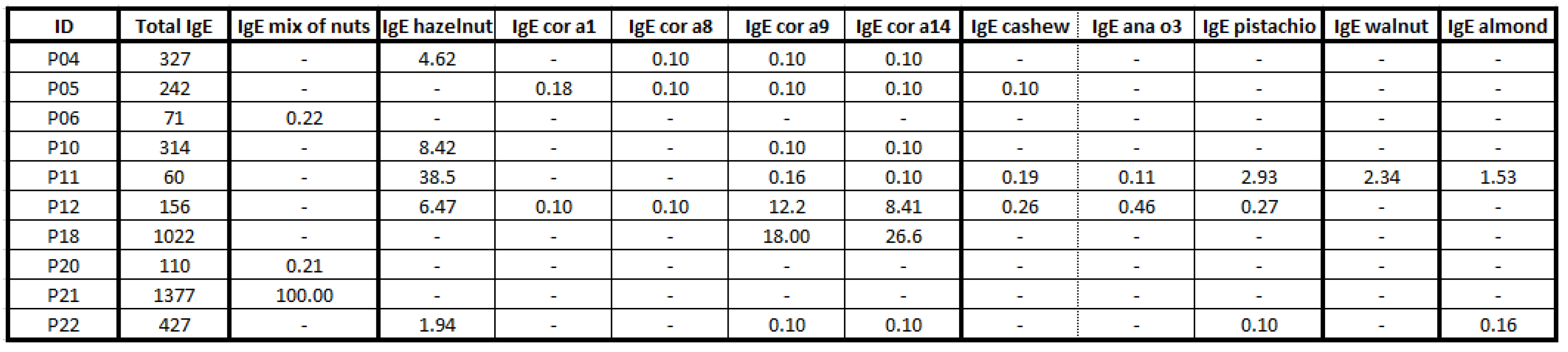 |
Table 7.
IgE levels (kU/L) of the different legumes in individual study patients at inclusion +- 5 months.
Table 7.
IgE levels (kU/L) of the different legumes in individual study patients at inclusion +- 5 months.
 |
Table 8.
IgE levels (kU/L) of fish and shellfish in individual study patients at inclusion ± 5 months.
Table 8.
IgE levels (kU/L) of fish and shellfish in individual study patients at inclusion ± 5 months.
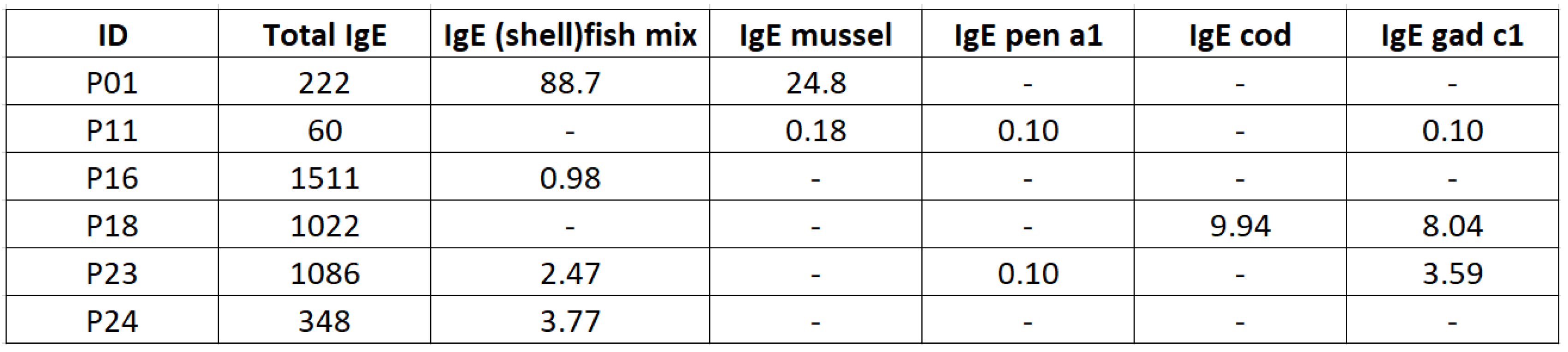 |
Table 9.
PEESS and PedsQL scores of children who changed remission status during the follow-up period.
Table 9.
PEESS and PedsQL scores of children who changed remission status during the follow-up period.
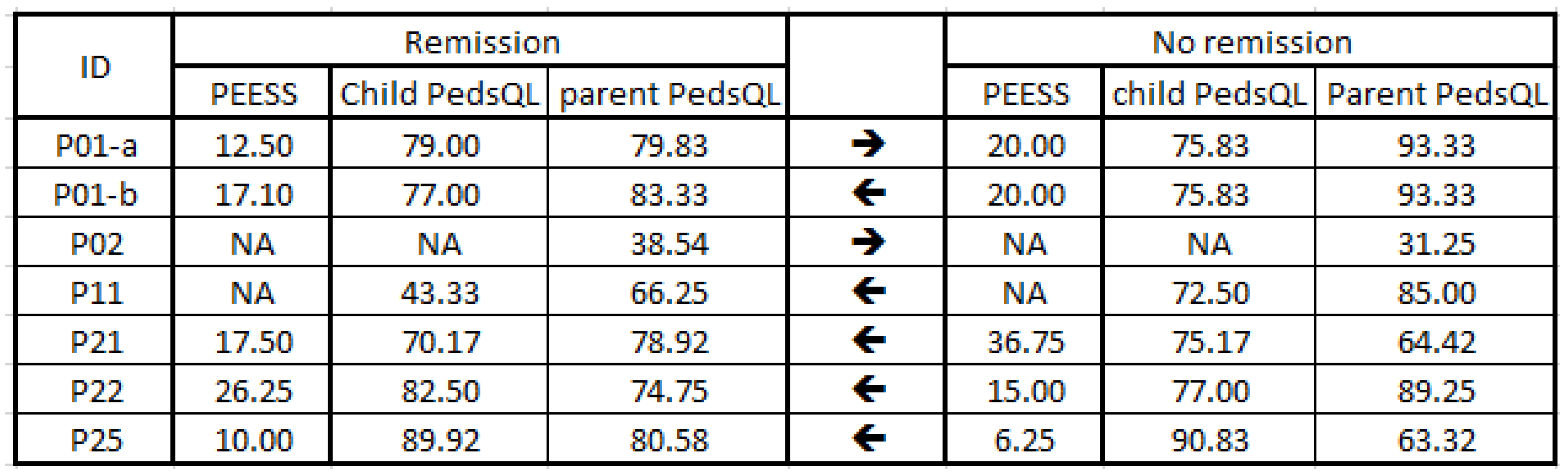 |
Table 10.
Type of food elimination diet (FED) at time of questionnaire.
 |
Table 11.
QoL assessment in relation to treatment type, using the Kruskal-Wallis test followed by post-hoc Dunn’s test; significant values are indicated with *.
Table 11.
QoL assessment in relation to treatment type, using the Kruskal-Wallis test followed by post-hoc Dunn’s test; significant values are indicated with *.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



