
Submitted:
07 May 2025
Posted:
08 May 2025
You are already at the latest version
Abstract
Alcohol Use Disorder (AUD) is a global social burden, with alcohol being the most prevalent psychoactive substance used by older individuals. Alcohol intake is a recognized carcinogen and is regulated by alcohol dehydrogenases (ADHs) and aldehyde dehydrogenases (ALDHs), with activity and expression determined by genetic factors. Alcohol withdrawal challenges include tremors, diaphoresis, anxiety, sleeplessness, hallucinations, and convulsions. Alcohol also stimulates cholinergic interneurons and increases the sensitivity of 5-HT3 receptors within the nucleus accumbens, which play a critical role in reward and addiction. Chronic alcohol consumption alters the mesolimbic dopaminergic system, an important neural pathway involved in reward processing. First-line pharmacotherapies for AUD include oral naltrexone and acamprosate, disulfiram, and nalmefene. Off-label therapies include baclofen, topiramate, gabapentin, ondansetron, and cytisine. Understanding altered neuronal signaling pathways by alcohol helps identify effectors involved in mitigating central actions and offers new therapeutic perspectives for alcohol addiction rehabilitation.
Keywords:
addiction
; alcohol use disorder
; anticraving
; off-label
1. Introduction
Alcohol Use Disorder (AUD) is the most prevalent of all substance use disorders, and it constitutes a worldwide social and economic burden [1]. In the U.S., alcohol consumption is the main psychoactive substance among older individuals, and the excessive and chronic use, including binge drinking, is increasing for recreational purposes, particularly among females [2]. In Europe the pictures are worst, with alcohol responsible for about 6.5% of all deaths (11.0% among men and 0.8% among women) and 11.6% of all disability-adjusted life years DALYs (17.3% for men and 4.4% for women), making it the region with the highest alcohol-attributable burden globally [3]. Alcohol intake is a well-established risk factor for developing injuries, non-communicable diseases, and multiple types of cancer. In 2018, around 23,300 early cancer fatalities in Europe were linked to alcohol consumption, with colorectal, liver, pancreatic, and esophageal cancers representing the highest incidence among males, and breast cancer among females [4].
Alcohol metabolism is governed by alcohol dehydrogenases (ADHs) and aldehyde dehydrogenases (ALDHs), whose activity and expression are determined by genetic factors. The polymorphisms of the ADH1B, ADH1C, and ALDH2 genes affect the regulation of acetaldehyde metabolism and the likelihood of alcohol consumption [5]. CYP2E1 and other cytochrome P450 isozymes play important and complementary roles in the metabolism of alcohol substrates [6]. Acetaldehyde, a product of ethanol metabolism, is not a simple metabolite of alcohol, but a toxic agent with deleterious effects on cellular metabolism and potentially carcinogenic [7]. It can cause significant cellular and tissue damage, particularly through mitochondrial dysfunction and the accumulation of reactive oxygen species (ROS), further damaging cell structures. Acetaldehyde is also recognized as a carcinogen capable of forming adducts with DNA, which are stable covalent bonds that can interfere with the replication and transcription of genetic material, increasing the risk of mutations [8].
Alcohol activates γ-aminobutyric acid type A (GABAa) and glycine receptors, which are the main receptors that inhibit signals in the central nervous system of vertebrates [9]. Chronic use of alcohol decreases the sensitivity and downregulates the expression of these inhibitory receptors while upregulating the Central Nervous System excitatory Kainate receptors (KA-Rs) that include N-methyl-D-aspartate (NMDA) receptors [10,11,12]. Alcohol withdrawal results in insufficient inhibition, triggering activation of the lateral habenula (LHb) and neuronal hyperactivity, which can induce severe clinical manifestations, including tremors, diaphoresis, anxiety, sleeplessness, hallucinations, and convulsions, potentially culminating in delirium tremens [10,13,14]. Furthermore, alcohol stimulates cholinergic interneurons (CIN) and increases the sensitivity of 5-HT3 receptors within the shell region of the nucleus accumbens (NAcSh), which play a critical role in reward and addiction [15]. Chronic alcohol consumption markedly alters the mesolimbic dopaminergic system, an important neural pathway involved in reward processing [16]. This pathway involves the alcohol-induced secretion of β-endorphins, which bind to mu-opioid receptors (MORs) on GABAergic interneurons inside the ventral tegmental area (VTA). Activation of MORs inhibits these interneurons, resulting in a reduction in the GABA-mediated inhibitory action on dopaminergic neurons [17]. This disinhibition increases dopamine release in the nucleus accumbens and enhances dopaminergic activation, hence reinforcing alcohol-related behaviors and facilitating the beginning of dependence [18,19]. In Figure 1 is schematically represented the mechanism of action of the main therapeutic drugs approved for alcohol dependence.
Cessation of alcohol intake causes an increase in craving, which can be categorized, based on the Clinical Theorist’s Questionnaire (CTQ), into three primary subtypes: reward craving, relief craving, and obsessive craving [20]. Reward craving, indicating the desire for the pleasurable effects of alcohol, is linked to the dopaminergic mesolimbic system [21]. Relief craving is motivated by the desire to diminish adverse emotional experiences, involving the GABAergic and endogenous opioid systems [22]. Obsessive craving, linked to habit circuits in the dorsal striatum, is characterized by intrusive thoughts and compulsive urges to consume alcohol [23].
Given the significant health and economic burden of alcohol use and its clinical management, it is essential to provide an evidence-based review of the current pharmacological treatment, to identify their mechanisms of action, efficacy, and pharmacological uses.
This narrative review aims to provide a comprehensive perspective supporting a more informed clinical approach to assessment and treatment in Italy.
2. Pharmacotherapies and Anti-Craving Therapy for AUD
The first-line pharmacotherapies for alcohol use disorder are oral naltrexone and acamprosate [24]; these are the only two therapies approved by the US Food and Drug Administration [25]. In Italy, the treatment of alcoholism is recognized as a social disease (Law 125/2001) and is included among the LEAs (DPCM 12 January 2017): regions must guarantee free access to diagnosis, medication, psychotherapy and rehabilitation. Apart from naltrexone and acamprosate here there are other therapies approved for alcohol dependence: disulfiram, nalmefene and sodium oxybate (https://www.aifa.gov.it).
2.1. Naltrexone
Naltrexone is an opioid antagonist of MOR, Delta-Opioid Receptor (DOR), and Kappa-Opioid Receptor (KOR), at first used for substance use disorder, in particular for opioid addiction, currently has been shown to have efficacy in the treatment of alcohol use disorder [26]. Naltrexone is structurally derived from the morphinan family and features a cyclopropylmethyl group linked to a hexahydro-methanobenzofuroisoquinoline core. The molecule contains two hydroxyl groups, optimally located to improve receptor binding affinity [27]. 6-β-naltrexol is the principal metabolite of naltrexone in humans, whereas 2-hydroxy-3-O-methylnaltrexol is a secondary metabolite [28]. The pharmacokinetics of naltrexone indicate that after oral administration, the drug is effectively absorbed by the gastrointestinal tract and is proficiently metabolized by the liver; the mean time to peak plasma concentration (Tmax) is roughly 1 hour. The maximum plasma concentration (Cmax) and area under the curve (AUC) of the principal active metabolite, 6β-naltrexol, exceed those of the parent drug. 6β-Naltrexol exhibits prolonged systemic persistence and considerably enhances overall pharmacological efficacy. The observed elimination half-lives (T1/2) of naltrexone and 6β-naltrexol are comparable and stay consistent across extended administration, despite significant interindividual heterogeneity and among individuals with cirrhosis and other severities of liver disease [28,29,30]. Naltrexone reduces craving by blocking the enhancement of endorphin levels [31]. There are three naltrexone forms: 50 mg/d oral, 100 mg/d oral, and injection. In a risk-benefit analysis, naltrexone, 50 mg/d oral, is the best form of naltrexone therapy. Additional studies have shown the superiority of naltrexone over acamprosate in subjects with severe AUD, particularly among clinical profiles characterized by high reward craving and propensity for relapse into heavy drinking [24,32].
2.2. Acamprosate
Acamprosate is an acetylated form of taurine with a structural analogy to GABA and many other amino acids [33,34]. Acamprosate exhibits low oral bioavailability (~11%) attributed to inadequate gastrointestinal absorption, with food further diminishing systemic exposure. It maintains linear pharmacokinetics within therapeutic ranges, with distribution limited to extracellular fluid, characterized by a low volume of distribution (~0.6 L/kg) and minimal plasma protein binding. Acamprosate is not metabolized by the liver and is excreted unchanged by the kidneys, with renal clearance very similar to the glomerular filtration rate [35]. The mechanism of action of acamprosate is still unclear. The evidence suggests that multimodal effects, mainly the action on the NMDA receptor, play a central role [34]. A preclinical study has shown decreases in postsynaptic potentials in the rat neocortex after it was administered. Acamprosate's daily dose is 1.3 or 2 g in 3 divided administrations [36]. This dosage depends on the complex pharmacokinetics of this drug, and the absorption and elimination of acamprosate are not fully recognized. Recent studies explore possible alternative dosing strategies to improve treatment adherence [24,34,37]. The American Psychiatric Association (APA) practice guideline suggests that acamprosate be offered to patients with moderate to severe AUD who aim to reduce alcohol consumption or reach abstinence [25,37].
2.3. Disulfiram
Disulfiram is the first drug approved for alcohol use disorder, It is a quaternary ammonium compound characterized by strong electrophilic properties, which significantly influence its chemical reactivity and biological interactions [38]. Disulfiram is not an anti-craving drug; it acts as an aversive agent. The main action for maintaining alcohol abstinence is psychological [39]. Disulfiram irreversibly inhibits the enzyme aldehyde dehydrogenase, accumulating acetaldehyde that causes tachycardia, flushing, nausea, and vomiting [40]. Disulfiram dosage is between 250 and 500 mg/day [41]. Disulfiram is an efficacious treatment compared to anticraving pharmacological therapies [39]. The research suggests that disulfiram should be administered continuously under supervision and alongside supportive psychotherapy to increase its effectiveness; in these instances, it is not inferior to conventional oral therapies [42,43].
2.4. Nalmefene
Nalmefene is the most recent treatment of AUD approved by the European Medicines Agency to decrease alcohol use and binge drinking in patients with AUD [44]. Nalmefene is an opiate derivative with a chemical similarity to naltrexone (6-methylene-naltrexone); it acts like a MOR and DOR antagonist and a partial KOR agonist [45]. Preclinical studies indicate that nalmefene is quickly absorbed, reaching its highest level in the blood (Tmax) in about 0.35 hours, with a peak concentration (Cmax) of 12.24 ng/mL. It takes about 10.7 hours for half of the drug to be eliminated from the body, and when taken by mouth, only 41% of it is available in the system. It has an elimination half-life (t1/2) of approximately 10.7 hours and an oral bioavailability of 41%, indicating its modest systemic availability after oral dosing [46]. Nalmefene has a different mechanism of action from that of its extensive competitor. The dosage of nalmefene is 18 mg as needed, although in many trials it is administered once a day [47]. In a paper, the expert opinion underlines that nalmefene has substantial advantages over naltrexone in the treatment of AUD [48].
2.5. Sodium Oxybate
Sodium oxybate or γ-hydroxybutyrate (GHB) is an endogenous short-chain fatty acid synthesized in the nervous system [49]. Sodium oxybate exhibits linear and dose-proportional pharmacokinetics, characterized by fast absorption (Tmax 30–75 minutes), a quick elimination half-life (0.5–1 hour), and no significant accumulation upon repeated dosage, hence endorsing a reliable profile for chronic administration [50]. Sodium Oxybate is approved for the treatment of Alcohol withdrawal syndrome and in the treatment of AUD, has a particular mechanism. Sodium oxybate acts on GABAB receptors and extrasynaptic GABAA receptors, resulting in alcohol-mimetic effects [51]. Most studies on sodium oxybate use a dosage of 50 mg/kg divided into three administrations per day [52]. Sodium oxybate was at least as effective as benzodiazepines in patients with alcohol withdrawal syndrome, rapidly alleviating symptoms, and was at least as effective as other anti-craving drugs in maintaining abstinence in alcohol use disorder, but inexact dosing or illicit sodium oxybate use has an increased risk of overdose [53].
The pharmacological agents currently approved in Italy for the treatment of AUD were summarized in Table 1, highlighting their mechanisms of action and principal clinical effects.
3. The Off-Label Therapy
Despite the availability of approved treatments for AUD, various off-label medications are also used to expand therapeutic options, including some of the most adopted in clinical practice.
3.1. Baclofen
Baclofen is a promising drug approved for muscle spasticity. Baclofen is a lipophilic derivative of GABA with a highly selective agonist action on the γ-aminobutyric acid B (GABAB) receptor [54,55]. Baclofen has fast oral absorption (Tmax 1–2 hours), a short half-life (2–6 hours), and is mainly eliminated by renal excretion, with linear pharmacokinetics facilitating predictable exposure over chronic treatment [56]. Baclofen inhibits the release of excitatory neurotransmitters, particularly in the mesolimbic systems, acting on GABAB receptors, which are numerous in the limbic system [57,58]. Baclofen dosage for AUD treatment is 5 mg three times per day for 3 days, then increasing the dose until 10 mg three times per day for 27 days [59]. Baclofen shows better abstinence rates than placebo, but not in other outcomes like craving or decreasing heavy drinking [57].
3.2. Topiramate
Topiramate is a sulfamate-containing compound approved for epilepsy [60,61]. Topiramate exhibits linear pharmacokinetics over the 100–800 mg dose range, with an oral bioavailability of 81–95%, unaffected by food intake. It has a low oral clearance (22–36 mL/min) and a prolonged elimination half-life of approximately 19–25 hours, primarily eliminated unchanged via renal excretion [62]. Topiramate is a promising drug for AUD, but its mechanism of action is still unclear; it seems to act on GABA receptors and, in animal studies, blocks the effects of kainite-induced excitatory conductance and increases the activation of postsynaptic NMDA receptors [63,64]. Some clinical studies indicate that the dosage of topiramate most efficient for treating AUD is 300 mg/day [65,66]. The topiramate efficacy is questionable; it seems to reduce the abstinence syndrome but does not reach the abstinence [55,67].
3.3. Gabapentin
Gabapentin is a gamma-aminobutyric acid analog, which is an effective antiepileptic and is also finding its use in AUD [68]. Gabapentin displays dose-dependent pharmacokinetics due to saturable absorption, with a half-life of 5–7 hours and renal elimination in unchanged form [69]. The pharmacological actions of gabapentin are not fully understood; it increases the GABA concentration [70]. Gabapentin dosage is between 600 and 1800 mg/day [68,71]. Gabapentin showed good efficacy in reducing cravings and withdrawal symptoms [71,72].
Pregabalin is structurally like gabapentin and the mechanism of action is the same, but it has a higher degree of oral absorption that is linear with the dose. A clinical study reports the efficacy and safety of pregabalin treatment of AUD in doses up to 600 mg per day [72].
3.4. Ondansetron
Ondansetron is a selective 5-HT3 receptor antagonist, it is approved as an antiemetic for cancer treatment-induced and anesthesia-related nausea and vomiting [73]. Ondansetron shows linear pharmacokinetics with a short elimination half-life of approximately 1.6 to 1.9 hours and is primarily excreted unchanged by the kidneys [74].There have been studies since the early 2000s about the use of ondansetron to decrease drinking in patients with AUD [75,76]. The dosage of ondansetron is 4 mcg/kg twice daily for 8 weeks [76]. Ondansetron is an effective drug in AUD patients, presumably for the action on serotoninergic systems, but has no efficacy in treating AUD patients with no comorbid with Major Depressive Disorder (MDD) [75,77].
3.5. Cytisine
Cytisine is a natural alkaloid extracted from plants of the Faboideae subfamily, It was used for the pharmacological treatment of tobacco use disorder [78]. Cytisine is rapidly absorbed, reaching peak plasma concentrations in approximately 1.3 hours. It shows a relatively short elimination half-life of about 4.8 hours, with a maximum concentration around 12.1 nanograms per milliliter and an overall exposure (AUC) of 49.5 nanogram-hours per milliliter. Cytisine is primarily eliminated unchanged in the urine, with no detectable metabolites found in plasma or urine [79]. Cytisine has a high affinity for α4β2 and α7 nAChRs, these receptors acting on the reward system. The anticraving effect of cytisine is attributed to its partial agonist activity at α4β2 nicotinic acetylcholine receptors. cytisine is safe and effective for smoking cessation and shows a potential role in reducing alcohol self-administration in smokers, while various therapeutic regimens have been established for smoking cessation, there is currently no standardized dosing protocol for cytisine in the context of AUD treatment [78,80].
Table 2 summarizes the principal off-label pharmacological agents currently employed in clinical practice in Italy for the management AUD, highlighting their proposed mechanisms of action and reported clinical benefits based on available evidence.
4. Conclusions
This review offers a practical guide for clinicians by illustrating the diverse effects of alcohol on the central nervous system, including widespread psychomotor depression, impaired information storage, disrupted logical reasoning, and motor incoordination. Additionally, alcohol’s stimulation of the brain's reward system may help explain the development of addiction. This comprehensive perspective supports a more informed clinical approach to assessment and treatment.
Understanding the altered neuronal signaling pathways by alcohol seems helpful in identifying effectors involved in the mitigation of central actions, offering new therapeutic perspectives for alcohol addiction rehabilitation.
Naltrexone and acamprosate show successful results in the realm of AUD treatment. A daily oral dose of 50 mg/day of naltrexone is effective in reducing alcohol cravings. At the same time, acamprosate, acting on the NMDA receptor, is recommended for moderate to severe AUD patients. Disulfiram doesn’t act like an anticraving drug, and its effectiveness is related to the psychological mechanism of action.
The European Medicines Agency has approved nalmefene (KOR agonist and MOR antagonist) and sodium oxybate (Agonist GABAAR and GABABR). Promising results demonstrate nalmefene is a potential alternative treatment to naltrexone, due to its dual action, and the potential advantages of sodium oxybate Alcohol Withdrawal Syndrome and AUD treatment.
In patients with a concomitant opioid dependence, it should be noted that naltrexone and nalmefene are contraindicated in patients treated with methadone as it could lead to acute withdrawal syndrome and potential physiological decompensation. In this case, a wash-out and confirmation of suspension of the opioid agonist is required before starting the administration of alcohol dependence treatment. At the same time, the administration of either disulfiram or sodium oxybate in association to methadone treatment may lead to increased CNS toxicity. Acamprosate does not affect the opioid system or depress breathing, so it is generally considered safer in patients on methadone therapy.
Among gabaergic drugs, topiramate and gabapentin, already used to treat alcohol withdrawal symptoms, may also be beneficial to facilitate alcohol cessation, sparing benzodiazepine administration.
Despite the existence of approved (on-label) pharmacological therapies for AUD, and the increasing use of off-label strategies, there is still a significant gap in robust evidence on their safety and tolerability in real patients. The latter often present complex clinical pictures, with psychiatric and organic comorbidities and multiple addictions (from opiates, benzodiazepines, stimulants or cannabis), which alter the risk-benefit profile of treatments. In addition, the poor therapeutic adherence and frequent psychosocial instability make the "ideal patient" of traditional clinical trials unrepresentative.
Therefore, it is urgent to design pragmatic and realistic studies that evaluate the efficacy, safety and tolerability of anti-alcohol drugs in highly complex populations, including those on methadone substitution treatment or other concomitant addiction therapies.
To address the complexities of AUD, the strategies of these pharmacotherapies consider the mechanisms of action, dosages, and potential advantages in different patient populations. Ongoing research endeavors aim to refine existing treatments in other countries and introduce novel medications.
Further studies should be conducted to map emerging trends and future approaches in pharmacological management and develop effective and safe therapeutic algorithms with an integrated and personalized approach in a comprehensive framework.
Author Contributions
All authors contributed substantially to the conception, design, analysis, and/or interpretation of data and the writing and critical revision of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
Not Applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AUD | Alcohol Use Disorder |
| ADHs | Alcohol Dehydrogenases |
| ALDHs | Aldehyde Dehydrogenases |
| DALYs | Disability-adjusted life years |
| ROS | Reactive Oxygen Species |
| GABA | γ-Aminobutyric Acid |
| KA-Rs | Kainate Receptors |
| NMDA | N-methyl-D-aspartate |
| LHBs | Lateral Habenula |
| CIN | Cholinergic Interneurons |
| NAcSh | Nucleus Accumbens |
| MOR | Mu-Opioid Receptor |
| VTA | Ventral Tegmental Area |
| CTQ | Clinical Theorist’s Questionnaire |
| KOR | Kappa-Opioid Receptor |
| DOR | Delta-Opioid Receptor |
| GHB | γ-Hydroxybutyrate |
| MDD | Major Depressive Disorder |
References
- The Global Burden of Disease Attributable to Alcohol and Drug Use in 195 Countries and Territories, 1990-2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry 2018, 5. [CrossRef]
- Han, B.H.; Moore, A.A.; Sherman, S.; Keyes, K.M.; Palamar, J.J. Demographic Trends of Binge Alcohol Use and Alcohol Use Disorders among Older Adults in the United States, 2005-2014. Drug Alcohol Depend. 2017, 170, 198–207. [Google Scholar] [CrossRef]
- Rehm, J.; Zatonksi, W.; Taylor, B.; Anderson, P. Epidemiology and Alcohol Policy in Europe. Addict. Abingdon Engl. 2011, 106 Suppl 1, 11–19. [Google Scholar] [CrossRef]
- Rumgay, H.; Ortega-Ortega, M.; Sharp, L.; Lunet, N.; Soerjomataram, I. The Cost of Premature Death from Cancer Attributable to Alcohol: Productivity Losses in Europe in 2018. Cancer Epidemiol. 2023, 84, 102365. [Google Scholar] [CrossRef] [PubMed]
- Matejcic, M.; Gunter, M.J.; Ferrari, P. Alcohol Metabolism and Oesophageal Cancer: A Systematic Review of the Evidence. Carcinogenesis 2017, 38, 859–872. [Google Scholar] [CrossRef] [PubMed]
- Song, B.-J.; Abdelmegeed, M.A.; Cho, Y.-E.; Akbar, M.; Rhim, J.S.; Song, M.-K.; Hardwick, J.P. Contributing Roles of CYP2E1 and Other Cytochrome P450 Isoforms in Alcohol-Related Tissue Injury and Carcinogenesis. Adv. Exp. Med. Biol. 2019, 1164, 73–87. [Google Scholar] [CrossRef] [PubMed]
- Terracina, S.; Caronti, B.; Lucarelli, M.; Francati, S.; Piccioni, M.G.; Tarani, L.; Ceccanti, M.; Caserta, M.; Verdone, L.; Venditti, S.; et al. Alcohol Consumption and Autoimmune Diseases. Int. J. Mol. Sci. 2025, 26, 845. [Google Scholar] [CrossRef]
- Ferraguti, G.; Terracina, S.; Petrella, C.; Greco, A.; Minni, A.; Lucarelli, M.; Agostinelli, E.; Ralli, M.; de Vincentiis, M.; Raponi, G.; et al. Alcohol and Head and Neck Cancer: Updates on the Role of Oxidative Stress, Genetic, Epigenetics, Oral Microbiota, Antioxidants, and Alkylating Agents. Antioxid. Basel Switz. 2022, 11, 145. [Google Scholar] [CrossRef]
- Krasowski, M.D.; Harrison, N.L. The Actions of Ether, Alcohol and Alkane General Anaesthetics on GABAA and Glycine Receptors and the Effects of TM2 and TM3 Mutations. Br. J. Pharmacol. 2000, 129, 731–743. [Google Scholar] [CrossRef]
- Carta, M.; Ariwodola, O.J.; Weiner, J.L.; Valenzuela, C.F. Alcohol Potently Inhibits the Kainate Receptor-Dependent Excitatory Drive of Hippocampal Interneurons. Proc. Natl. Acad. Sci. U. S. A. 2003, 100, 6813–6818. [Google Scholar] [CrossRef]
- Long, D.; Long, B.; Koyfman, A. The Emergency Medicine Management of Severe Alcohol Withdrawal. Am. J. Emerg. Med. 2017, 35, 1005–1011. [Google Scholar] [CrossRef]
- Meloy, P.; Rutz, D.; Bhambri, A. Alcohol Withdrawal. J. Educ. Teach. Emerg. Med. 2025, 10, O1–O30. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Zuo, W.; Wu, W.; Zuo, Q.K.; Fu, R.; Wu, L.; Zhang, H.; Ndukwe, M.; Ye, J.-H. Activation of Glycine Receptors in the Lateral Habenula Rescues Anxiety- and Depression-like Behaviors Associated with Alcohol Withdrawal and Reduces Alcohol Intake in Rats. Neuropharmacology 2019, 157, 107688. [Google Scholar] [CrossRef] [PubMed]
- Schuckit, M.A. Recognition and Management of Withdrawal Delirium (Delirium Tremens). N. Engl. J. Med. 2014, 371, 2109–2113. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Chischolm, A.; Parikh, M.; Thakkar, M. Cholinergic Interneurons in the Shell Region of the Nucleus Accumbens Regulate Binge Alcohol Consumption: A Chemogenetic and Genetic Lesion Study. Alcohol Clin. Exp. Res. 2024, 48, 827–842. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurobiology of Addiction: A Neurocircuitry Analysis. Lancet Psychiatry 2016, 3, 760–773. [Google Scholar] [CrossRef]
- Gianoulakis, C. Endogenous Opioids and Addiction to Alcohol and Other Drugs of Abuse. Curr. Top. Med. Chem. 2009, 9, 999–1015. [Google Scholar] [CrossRef]
- Spanagel, R. Alcoholism: A Systems Approach from Molecular Physiology to Addictive Behavior. Physiol. Rev. 2009, 89, 649–705. [Google Scholar] [CrossRef]
- Morales, A.M.; Jones, S.A.; Carlson, B.; Kliamovich, D.; Dehoney, J.; Simpson, B.L.; Dominguez-Savage, K.A.; Hernandez, K.O.; Lopez, D.A.; Baker, F.C.; et al. Associations between Mesolimbic Connectivity, and Alcohol Use from Adolescence to Adulthood. Dev. Cogn. Neurosci. 2024, 70, 101478. [Google Scholar] [CrossRef]
- Martinotti, G.; Di Nicola, M.; Tedeschi, D.; Callea, A.; Di Giannantonio, M.; Janiri, L. ; Craving Study Group Craving Typology Questionnaire (CTQ): A Scale for Alcohol Craving in Normal Controls and Alcoholics. Compr. Psychiatry 2013, 54, 925–932. [Google Scholar] [CrossRef]
- Verheul, R.; van den Brink, W.; Geerlings, P. A Three-Pathway Psychobiological Model of Craving for Alcohol. Alcohol Alcohol. Oxf. Oxfs. 1999, 34, 197–222. [Google Scholar] [CrossRef] [PubMed]
- Heilig, M.; Egli, M.; Crabbe, J.C.; Becker, H.C. Acute Withdrawal, Protracted Abstinence and Negative Affect in Alcoholism: Are They Linked? Addict. Biol. 2010, 15, 169–184. [Google Scholar] [CrossRef]
- Everitt, B.J.; Robbins, T.W. Neural Systems of Reinforcement for Drug Addiction: From Actions to Habits to Compulsion. Nat. Neurosci. 2005, 8, 1481–1489. [Google Scholar] [CrossRef] [PubMed]
- McPheeters, M.; O’Connor, E.A.; Riley, S.; Kennedy, S.M.; Voisin, C.; Kuznacic, K.; Coffey, C.P.; Edlund, M.D.; Bobashev, G.; Jonas, D.E. Pharmacotherapy for Alcohol Use Disorder: A Systematic Review and Meta-Analysis. JAMA 2023, 330, 1653–1665. [Google Scholar] [CrossRef]
- Shen, W.W. Anticraving Therapy for Alcohol Use Disorder: A Clinical Review. Neuropsychopharmacol. Rep. 2018, 38, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Sawicka, M.; Tracy, D.K. Naltrexone Efficacy in Treating Alcohol-Use Disorder in Individuals with Comorbid Psychosis: A Systematic Review. Ther. Adv. Psychopharmacol. 2017, 7, 211–224. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, K. de O.; Ribeiro, L.; Oliveira, C.M.A. de; Carvalho, J.F.; Martins, F.T. New Solvates of the Drug Naltrexone: Protonation, Conformation and Interplay of Synthons. Acta Crystallogr. Sect. C Struct. Chem. 2018, 74, 274–282. [Google Scholar] [CrossRef]
- Bello, M. Molecular Basis of Inhibitory Mechanism of Naltrexone and Its Metabolites through Structural and Energetic Analyses. Mol. Basel Switz. 2022, 27, 4919. [Google Scholar] [CrossRef]
- Bertolotti, M.; Ferrari, A.; Vitale, G.; Stefani, M.; Trenti, T.; Loria, P.; Carubbi, F.; Carulli, N.; Sternieri, E. Effect of Liver Cirrhosis on the Systemic Availability of Naltrexone in Humans. J. Hepatol. 1997, 27, 505–511. [Google Scholar] [CrossRef]
- Ferrari, A.; Bertolotti, M.; Dell’Utri, A.; Avico, U.; Sternieri, E. Serum Time Course of Naltrexone and 6 Beta-Naltrexol Levels during Long-Term Treatment in Drug Addicts. Drug Alcohol Depend. 1998, 52, 211–220. [Google Scholar] [CrossRef]
- Anton, R.F.; Drobes, D.J.; Voronin, K.; Durazo-Avizu, R.; Moak, D. Naltrexone Effects on Alcohol Consumption in a Clinical Laboratory Paradigm: Temporal Effects of Drinking. Psychopharmacology (Berl.) 2004, 173, 32–40. [Google Scholar] [CrossRef] [PubMed]
- Morley, K.C.; Teesson, M.; Reid, S.C.; Sannibale, C.; Thomson, C.; Phung, N.; Weltman, M.; Bell, J.R.; Richardson, K.; Haber, P.S. Naltrexone versus Acamprosate in the Treatment of Alcohol Dependence: A Multi-Centre, Randomized, Double-Blind, Placebo-Controlled Trial. Addict. Abingdon Engl. 2006, 101, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Zornoza, T.; Cano, M.J.; Polache, A.; Granero, L. Pharmacology of Acamprosate: An Overview. CNS Drug Rev. 2003, 9, 359–374. [Google Scholar] [CrossRef]
- Rösner, S.; Hackl-Herrwerth, A.; Leucht, S.; Lehert, P.; Vecchi, S.; Soyka, M. Acamprosate for Alcohol Dependence. Cochrane Database Syst. Rev. 2010, CD004332. [Google Scholar] [CrossRef]
- Saivin, S.; Hulot, T.; Chabac, S.; Potgieter, A.; Durbin, P.; Houin, G. Clinical Pharmacokinetics of Acamprosate. Clin. Pharmacokinet. 1998, 35, 331–345. [Google Scholar] [CrossRef]
- Wilde, M.I.; Wagstaff, A.J. Acamprosate. A Review of Its Pharmacology and Clinical Potential in the Management of Alcohol Dependence after Detoxification. Drugs 1997, 53, 1038–1053. [Google Scholar] [CrossRef]
- Reus, V.I.; Fochtmann, L.J.; Bukstein, O.; Eyler, A.E.; Hilty, D.M.; Horvitz-Lennon, M.; Mahoney, J.; Pasic, J.; Weaver, M.; Wills, C.D.; et al. The American Psychiatric Association Practice Guideline for the Pharmacological Treatment of Patients With Alcohol Use Disorder. Am. J. Psychiatry 2018, 175, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Lanz, J.; Biniaz-Harris, N.; Kuvaldina, M.; Jain, S.; Lewis, K.; Fallon, B.A. Disulfiram: Mechanisms, Applications, and Challenges. Antibiot. Basel Switz. 2023, 12, 524. [Google Scholar] [CrossRef]
- Skinner, M.D.; Lahmek, P.; Pham, H.; Aubin, H.-J. Disulfiram Efficacy in the Treatment of Alcohol Dependence: A Meta-Analysis. PloS One 2014, 9, e87366. [Google Scholar] [CrossRef]
- Swift, R.M. Drug Therapy for Alcohol Dependence. N. Engl. J. Med. 1999, 340, 1482–1490. [Google Scholar] [CrossRef]
- Wright, C.; Moore, R.D. Disulfiram Treatment of Alcoholism. Am. J. Med. 1990, 88, 647–655. [Google Scholar] [CrossRef] [PubMed]
- Schallenberg, M.; Vogel-Blaschka, D.; Spreer, M.; Göstl, J.; Petzold, J.; Pilhatsch, M. Effectiveness of Disulfiram as Adjunct to Addiction-Focused Treatment for Persons With Severe Alcohol Use Disorder. Addict. Biol. 2025, 30, e70035. [Google Scholar] [CrossRef]
- Holt, S.R. Supervised Disulfiram Should Be Considered First-Line Treatment for Alcohol Use Disorder. J. Addict. Med. 2024, 18, 614–616. [Google Scholar] [CrossRef]
- Burnette, E.M.; Nieto, S.J.; Grodin, E.N.; Meredith, L.R.; Hurley, B.; Miotto, K.; Gillis, A.J.; Ray, L.A. Novel Agents for the Pharmacological Treatment of Alcohol Use Disorder. Drugs 2022, 82, 251–274. [Google Scholar] [CrossRef] [PubMed]
- Soyka, M.; Lieb, M. Recent Developments in Pharmacotherapy of Alcoholism. Pharmacopsychiatry 2015, 48, 123–135. [Google Scholar] [CrossRef]
- Papich, M.G.; Narayan, R.J. Naloxone and Nalmefene Absorption Delivered by Hollow Microneedles Compared to Intramuscular Injection. Drug Deliv. Transl. Res. 2022, 12, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Quelch, D.R.; Mick, I.; McGonigle, J.; Ramos, A.C.; Flechais, R.S.A.; Bolstridge, M.; Rabiner, E.; Wall, M.B.; Newbould, R.D.; Steiniger-Brach, B.; et al. Nalmefene Reduces Reward Anticipation in Alcohol Dependence: An Experimental Functional Magnetic Resonance Imaging Study. Biol. Psychiatry 2017, 81, 941–948. [Google Scholar] [CrossRef]
- Soyka, M.; Rösner, S. Nalmefene for Treatment of Alcohol Dependence. Expert Opin. Investig. Drugs 2010, 19, 1451–1459. [Google Scholar] [CrossRef]
- Pardi, D.; Black, J. Gamma-Hydroxybutyrate/Sodium Oxybate: Neurobiology, and Impact on Sleep and Wakefulness. CNS Drugs 2006, 20, 993–1018. [Google Scholar] [CrossRef]
- Borgen, L.A.; Okerholm, R.A.; Lai, A.; Scharf, M.B. The Pharmacokinetics of Sodium Oxybate Oral Solution Following Acute and Chronic Administration to Narcoleptic Patients. J. Clin. Pharmacol. 2004, 44, 253–257. [Google Scholar] [CrossRef]
- van den Brink, W.; Addolorato, G.; Aubin, H.-J.; Benyamina, A.; Caputo, F.; Dematteis, M.; Gual, A.; Lesch, O.-M.; Mann, K.; Maremmani, I.; et al. Efficacy and Safety of Sodium Oxybate in Alcohol-Dependent Patients with a Very High Drinking Risk Level. Addict. Biol. 2018, 23, 969–986. [Google Scholar] [CrossRef] [PubMed]
- Busardò, F.P.; Kyriakou, C.; Napoletano, S.; Marinelli, E.; Zaami, S. Clinical Applications of Sodium Oxybate (GHB): From Narcolepsy to Alcohol Withdrawal Syndrome. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4654–4663. [Google Scholar] [PubMed]
- Keating, G.M. Sodium Oxybate: A Review of Its Use in Alcohol Withdrawal Syndrome and in the Maintenance of Abstinence in Alcohol Dependence. Clin. Drug Investig. 2014, 34, 63–80. [Google Scholar] [CrossRef]
- Brown, J.W.; Moeller, A.; Schmidt, M.; Turner, S.C.; Nimmrich, V.; Ma, J.; Rueter, L.E.; van der Kam, E.; Zhang, M. Anticonvulsant Effects of Structurally Diverse GABA(B) Positive Allosteric Modulators in the DBA/2J Audiogenic Seizure Test: Comparison to Baclofen and Utility as a Pharmacodynamic Screening Model. Neuropharmacology 2016, 101, 358–369. [Google Scholar] [CrossRef]
- Lyon, J. More Treatments on Deck for Alcohol Use Disorder. JAMA 2017, 317, 2267–2269. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Kriel, R.L.; Cloyd, J.C.; Coles, L.D.; Scherkenbach, L.A.; Tobin, M.H.; Krach, L.E. A Pilot Study Assessing Pharmacokinetics and Tolerability of Oral and Intravenous Baclofen in Healthy Adult Volunteers. J. Child Neurol. 2015, 30, 37–41. [Google Scholar] [CrossRef]
- Rose, A.K.; Jones, A. Baclofen: Its Effectiveness in Reducing Harmful Drinking, Craving, and Negative Mood. A Meta-Analysis. Addict. Abingdon Engl. 2018, 113, 1396–1406. [Google Scholar] [CrossRef] [PubMed]
- Brennan, J.L.; Leung, J.G.; Gagliardi, J.P.; Rivelli, S.K.; Muzyk, A.J. Clinical Effectiveness of Baclofen for the Treatment of Alcohol Dependence: A Review. Clin. Pharmacol. Adv. Appl. 2013, 5, 99–107. [Google Scholar] [CrossRef]
- Addolorato, G.; Caputo, F.; Capristo, E.; Colombo, G.; Gessa, G.L.; Gasbarrini, G. Ability of Baclofen in Reducing Alcohol Craving and Intake: II--Preliminary Clinical Evidence. Alcohol. Clin. Exp. Res. 2000, 24, 67–71. [Google Scholar]
- Zaraei, S.-O.; Abduelkarem, A.R.; Anbar, H.S.; Kobeissi, S.; Mohammad, M.; Ossama, A.; El-Gamal, M.I. Sulfamates in Drug Design and Discovery: Pre-Clinical and Clinical Investigations. Eur. J. Med. Chem. 2019, 179, 257–271. [Google Scholar] [CrossRef]
- Raffa, R.B.; Finno, K.E.; Tallarida, C.S.; Rawls, S.M. Topiramate-Antagonism of L-Glutamate-Induced Paroxysms in Planarians. Eur. J. Pharmacol. 2010, 649, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Bialer, M.; Doose, D.R.; Murthy, B.; Curtin, C.; Wang, S.-S.; Twyman, R.E.; Schwabe, S. Pharmacokinetic Interactions of Topiramate. Clin. Pharmacokinet. 2004, 43, 763–780. [Google Scholar] [CrossRef]
- Yehuda, R.; Yang, R.-K.; Golier, J.A.; Tischler, L.; Liong, B.; Decker, K. Effect of Topiramate on Glucocorticoid Receptor Mediated Action. Neuropsychopharmacol. Off. Publ. Am. Coll. Neuropsychopharmacol. 2004, 29, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, J.W.; Sombati, S.; DeLorenzo, R.J.; Coulter, D.A. Cellular Actions of Topiramate: Blockade of Kainate-Evoked Inward Currents in Cultured Hippocampal Neurons. Epilepsia 2000, 41, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.A.; Ait-Daoud, N.; Akhtar, F.Z.; Ma, J.Z. Oral Topiramate Reduces the Consequences of Drinking and Improves the Quality of Life of Alcohol-Dependent Individuals: A Randomized Controlled Trial. Arch. Gen. Psychiatry 2004, 61, 905–912. [Google Scholar] [CrossRef]
- Johnson, B.A.; Rosenthal, N.; Capece, J.A.; Wiegand, F.; Mao, L.; Beyers, K.; McKay, A.; Ait-Daoud, N.; Anton, R.F.; Ciraulo, D.A.; et al. Topiramate for Treating Alcohol Dependence: A Randomized Controlled Trial. JAMA 2007, 298, 1641–1651. [Google Scholar] [CrossRef]
- Kampman, K.M.; Pettinati, H.M.; Lynch, K.G.; Spratt, K.; Wierzbicki, M.R.; O’Brien, C.P. A Double-Blind, Placebo-Controlled Trial of Topiramate for the Treatment of Comorbid Cocaine and Alcohol Dependence. Drug Alcohol Depend. 2013, 133, 94–99. [Google Scholar] [CrossRef]
- Zour, E.; Lodhi, S.A.; Nesbitt, R.U.; Silbering, S.B.; Chaturvedi, P.R. Stability Studies of Gabapentin in Aqueous Solutions. Pharm. Res. 1992, 9, 595–600. [Google Scholar] [CrossRef]
- Swearingen, D.; Aronoff, G.M.; Ciric, S.; Lal, R. Pharmacokinetics of Immediate Release, Extended Release, and Gastric Retentive Gabapentin Formulations in Healthy Adults. Int. J. Clin. Pharmacol. Ther. 2018, 56, 231–238. [Google Scholar] [CrossRef]
- Taylor, C.P.; Gee, N.S.; Su, T.Z.; Kocsis, J.D.; Welty, D.F.; Brown, J.P.; Dooley, D.J.; Boden, P.; Singh, L. A Summary of Mechanistic Hypotheses of Gabapentin Pharmacology. Epilepsy Res. 1998, 29, 233–249. [Google Scholar] [CrossRef]
- Furieri, F.A.; Nakamura-Palacios, E.M. Gabapentin Reduces Alcohol Consumption and Craving: A Randomized, Double-Blind, Placebo-Controlled Trial. J. Clin. Psychiatry 2007, 68, 1691–1700. [Google Scholar] [CrossRef] [PubMed]
- Mariani, J.J.; Pavlicova, M.; Choi, C.J.; Brooks, D.J.; Mahony, A.L.; Kosoff, Z.; Naqvi, N.; Brezing, C.; Luo, S.X.; Levin, F.R. An Open-Label Pilot Study of Pregabalin Pharmacotherapy for Alcohol Use Disorder. Am. J. Drug Alcohol Abuse 2021, 47, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Ye, J.H.; Ponnudurai, R.; Schaefer, R. Ondansetron: A Selective 5-HT(3) Receptor Antagonist and Its Applications in CNS-Related Disorders. CNS Drug Rev. 2001, 7, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Sotelo, C.K.; Shropshire, S.B.; Quimby, J.; Simpson, S.; Gustafson, D.L.; Zersen, K.M. Pharmacokinetics and Anti-Nausea Effects of Intravenous Ondansetron in Hospitalized Dogs Exhibiting Clinical Signs of Nausea. J. Vet. Pharmacol. Ther. 2022, 45, 508–515. [Google Scholar] [CrossRef]
- Johnson, B.A.; Roache, J.D.; Javors, M.A.; DiClemente, C.C.; Cloninger, C.R.; Prihoda, T.J.; Bordnick, P.S.; Ait-Daoud, N.; Hensler, J. Ondansetron for Reduction of Drinking among Biologically Predisposed Alcoholic Patients: A Randomized Controlled Trial. JAMA 2000, 284, 963–971. [Google Scholar] [CrossRef]
- Kranzler, H.R.; Pierucci-Lagha, A.; Feinn, R.; Hernandez-Avila, C. Effects of Ondansetron in Early- versus Late-Onset Alcoholics: A Prospective, Open-Label Study. Alcohol. Clin. Exp. Res. 2003, 27, 1150–1155. [Google Scholar] [CrossRef]
- Torrens, M.; Fonseca, F.; Mateu, G.; Farré, M. Efficacy of Antidepressants in Substance Use Disorders with and without Comorbid Depression. A Systematic Review and Meta-Analysis. Drug Alcohol Depend. 2005, 78, 1–22. [Google Scholar] [CrossRef]
- Gotti, C.; Clementi, F. Cytisine and Cytisine Derivatives. More than Smoking Cessation Aids. Pharmacol. Res. 2021, 170, 105700. [Google Scholar] [CrossRef]
- Jeong, S.H.; Newcombe, D.; Sheridan, J.; Tingle, M. Pharmacokinetics of Cytisine, an A4 Β2 Nicotinic Receptor Partial Agonist, in Healthy Smokers Following a Single Dose. Drug Test. Anal. 2015, 7, 475–482. [Google Scholar] [CrossRef]
- Etter, J.-F.; Lukas, R.J.; Benowitz, N.L.; West, R.; Dresler, C.M. Cytisine for Smoking Cessation: A Research Agenda. Drug Alcohol Depend. 2008, 92, 3–8. [Google Scholar] [CrossRef]
Figure 1.
Mechanism of action of the main therapeutic drugs for alcohol dependence.
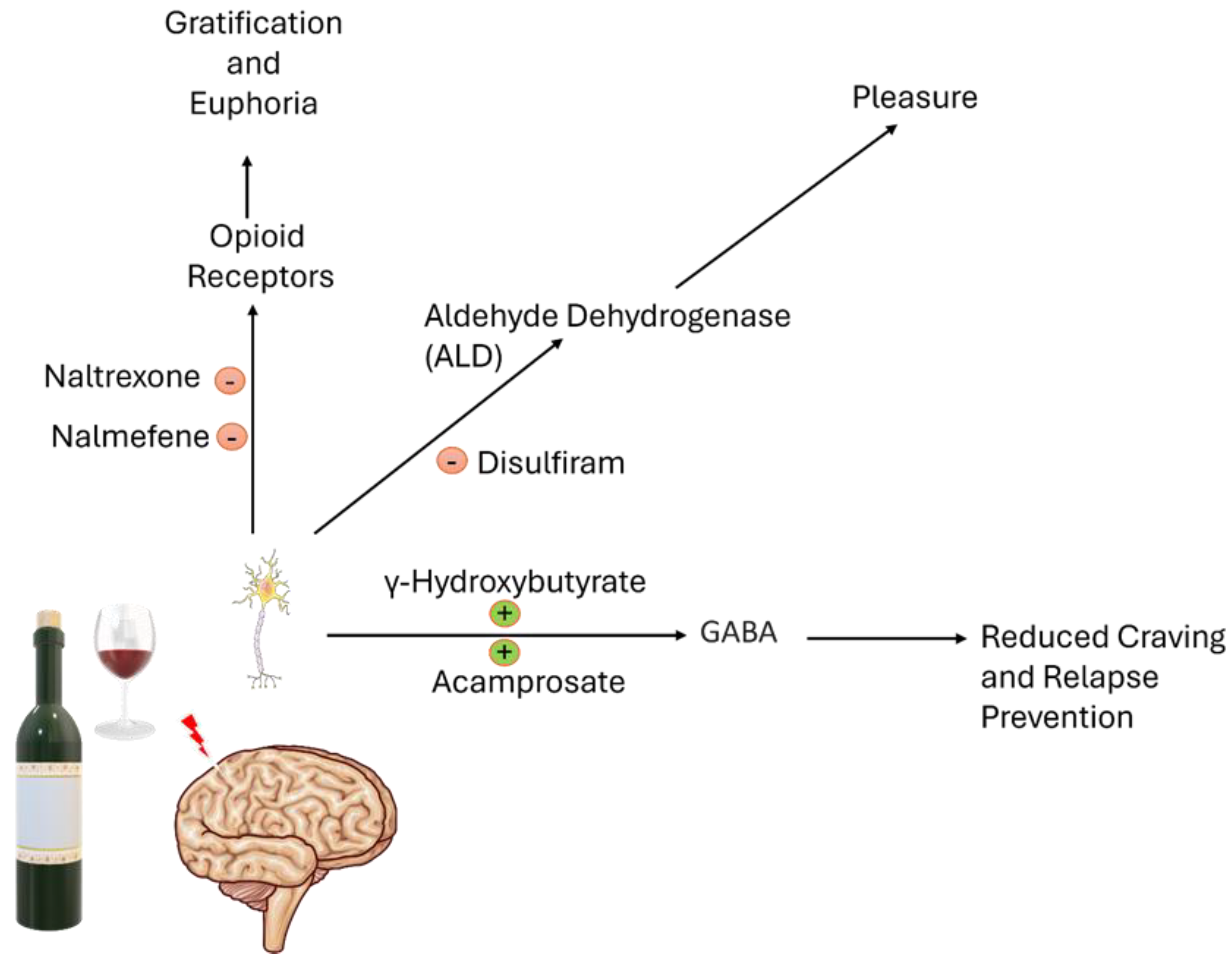

Table 1.
Approved drugs for AUD: targets and main clinical effects.
| Drug | Signaling | Clinical Effect |
|---|---|---|
| Naltrexone | Antagonist of MOR, DOR, KOR opioid receptors | Reduces craving and heavy drinking, superior in high-relapse profiles |
| Acamprosate | Unclear; likely modulates NMDA receptors and GABA analog | Supports abstinence, especially in moderate to severe AUD |
| Disulfiram | Aldehyde dehydrogenase inhibitor; aversive agent | Maintains abstinence via psychological deterrent |
| Nalmefene | MOR/DOR antagonist, KOR partial agonist | Reduces alcohol use and binge drinking, effective |
| Sodium Oxybate | GABAB agonist, acts also on extrasynaptic GABAA | Effective in withdrawal and abstinence maintenance, mimics alcohol effects |
Table 2.
Principal off-label medications employed in Italy for AUD: mechanisms of action and clinical effect.
Table 2.
Principal off-label medications employed in Italy for AUD: mechanisms of action and clinical effect.
| Drug | Signaling | Clinical Effect |
|---|---|---|
| Baclofen | Selective GABAB receptor agonist | Improves abstinence, not effective for craving or heavy drinking |
| Topiramate | Modulates GABA and glutamate (NMDA/kainate) receptors | Reduces withdrawal symptoms, limited effect on abstinence |
| Gabapentin | Increases GABA levels | Reduces craving and withdrawal symptoms |
| Pregabalin | Binds α2δ subunit of Ca²⁺ channels | Reduces craving, effective and better absorption than gabapentin |
| Ondansetron | 5-HT3 receptor antagonist | Reduces drinking in AUD with comorbid MDD |
| Cytisine | Partial agonist of α4β2 nAChRs, modulates dopamine reward system | Reduces alcohol self-administration in smokers |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



