
Submitted:
07 May 2025
Posted:
07 May 2025
You are already at the latest version
Abstract
Objective: To evaluate the efficacy and safety of Enhanced Recovery After Surgery (ERAS) protocols in adult patients undergoing elective craniotomy.Methods: A systematic review was conducted following PRISMA guidelines. Randomized controlled trials (RCTs) and observational studies with control groups were included. Databases searched included PubMed, Embase, Scopus, Web of Science, and Cochrane Library up to August 2023. Outcomes assessed were length of stay (LOS), postoperative complications, pain, PONV, and functional recovery. Risk of bias was evaluated using RoB 2 and ROBINS-I tools.Results: Ten studies (3 RCTs and 7 observational) were included. ERAS protocols were consistently associated with shorter hospital stays (1–2 days on average), improved postoperative pain control, and reduced PONV. No increase in complication rates was observed. Risk of bias was low in one RCT, moderate in one, and high in another. Observational studies presented moderate to high risk.Conclusions: ERAS protocols in elective craniotomy are effective and safe. Standardization and further high-quality multicenter RCTs are recommended.
Keywords:
Cranial surgery
; Enhanced Recovery After Surgery
; Length of stay
; Neurosurgery
; Patient-reported outcomes
; Patient satisfaction
; Postoperative complications
Introduction
Enhanced Recovery After Surgery (ERAS) is a multimodal, evidence-based perioperative care pathway designed to improve recovery outcomes and reduce complications. Although widely validated in abdominal and pelvic surgeries, its application in neurosurgery remains limited. This systematic review aims to assess the impact of ERAS protocols on postoperative outcomes in patients undergoing elective craniotomy.
Methods
This review followed PRISMA guidelines.The full protocol was prospectively registered in the PROSPERO database (CRD42023480954) X. We searched PubMed, Embase, Scopus, Web of Science, and Cochrane Library for articles published until August 2023. Inclusion criteria were studies involving adult patients (>18 years) undergoing elective craniotomy with implementation of ERAS protocols and a comparison group receiving standard care. We included randomized controlled trials and observational studies with control groups. Risk of bias was assessed using the RoB 2 tool for RCTs and ROBINS-I for observational studies.
Table 1 provides a summary of ERAS (Enhanced Recovery After Surgery) elements implemented in each included study. These elements commonly include components such as postoperative pain control, early mobilization, reduced postoperative nausea and vomiting (PONV), and shorter hospital length of stay (LOS). This table illustrates the variability and core consistency of ERAS strategies across different neurosurgical patient populations.
| Study | ERAS Elements |
| Wang et al. (2022) | Pain control, early mobilization, reduced LOS |
| Lei Wang et al. (2022) | Pain control, reduced PONV, reduced LOS |
| Han et al. (2019) | Pain control, reduced LOS, fewer complications |
| Zaed et al. (2023) | Reduced opioids, early mobilization |
| Elayat et al. (2021) | Pain control, reduced ICU stay |
| McLaughlin et al. (2014) | Reduced LOS and ICU stay |
| Lobatto et al. (2020) | Reduced LOS, fewer complications |
Table 2 presents the demographic characteristics of the included studies, detailing the country of origin, study design, total sample size, and the type of neurosurgical population enrolled. This overview aids in assessing the generalizability and applicability of the findings across different health systems and patient settings.
| Study | Country | Design | Sample Size | Population |
| Wang et al. (2022) | China | RCT | 151 | Glioma |
| Lei Wang et al. (2022) | China | RCT | 151 | Elective craniotomy |
| Han et al. (2019) | China | RCT | 84 | Aneurysm clipping |
| Zaed et al. (2023) | Switzerland | Retrospective | 19 | Elderly with glioblastoma |
| Elayat et al. (2021) | India | Non-randomized | 70 | Supratentorial tumors |
| McLaughlin et al. (2014) | USA | Observational | 121 | Pituitary/skull base tumors |
| Lobatto et al. (2020) | Netherlands | Observational | 150 | Meningioma |
Results
Ten studies met inclusion criteria: 3 RCTs and 7 observational studies.

Table 1.
Cochrane Data Extraction for RCTs.
| Study ID | Country | Design | Sample Size | Population | Intervention | Comparator | Outcomes and Results |
| Wang et al. (2022) | China | RCT | 151 | Adults with gliomas | ERAS | Conventional care | Reduced LOS (5 vs 7 days), better pain and mobilization |
| Lei Wang et al. (2022) | China | RCT | 151 | Elective craniotomy | ERAS | Standard care | LOS 3 vs 4 days, reduced cost and PONV |
| Han et al. (2019) | China | RCT | 84 | Aneurysm clipping | ERAS | Standard care | Reduced LOS, fewer complications, higher satisfaction |
Table 2.
Cochrane Data Extraction for Observational Studies.
| Study ID | Country | Design | Sample Size | Population | Intervention | Comparator | Outcomes and Results |
| Zaed et al. (2023) | Switzerland | Retrospective | 19 | Elderly with glioblastoma | ERAS | Historical cohort | Reduced opioid use, increased mobilization |
| Elayat et al. (2021) | India | Non-randomized | 70 | Supratentorial tumor patients | ERAS | Routine care | Reduced ICU stay, better pain control |
| McLaughlin et al. (2014) | USA | Observational | 121 | Pituitary/skull base tumors | ERAS | Historical controls | Reduced LOS and ICU stay |
| Lobatto et al. (2020) | Netherlands | Observational | 150 | Meningioma patients | ERAS | Standard care | LOS reduced from 7.6 to 3 days, fewer complications |
Risk of Bias Assessment
Table 3.
Risk of Bias in RCTs (RoB 2).
| Study | Randomization | Blinding | Overall Risk |
| Wang et al. (2022) | Low | Low | Low |
| Lei Wang et al. (2022) | Low | Some concerns | Moderate |
| Han et al. (2019) | Unclear | High | High |
Table 4.
Risk of Bias in Observational Studies (ROBINS-I).
| Study | Confounding | Selection Bias | Overall Risk |
| Zaed et al. (2023) | Moderate | Moderate | Moderate |
| Elayat et al. (2021) | Moderate | Moderate | Moderate |
| McLaughlin et al. (2014) | High | Moderate | High |
| Lobatto et al. (2020) | Moderate | Low | Moderate |
Conclusions
The use of ERAS protocols in elective craniotomy appears to be safe and beneficial across several outcome domains. While randomized trials offer stronger evidence, observational studies provide valuable real-world insights. There is a need for standardized protocol elements and future high-quality multicenter trials.
Abbreviations and Acronyms
| ERAS | Enhanced Recovery After Surgery |
| LOS | Length of stay |
| PONV | Postoperative nausea and vomiting |
| PRO | Patient-reported outcome |
| RCT | Randomized controlled trial |
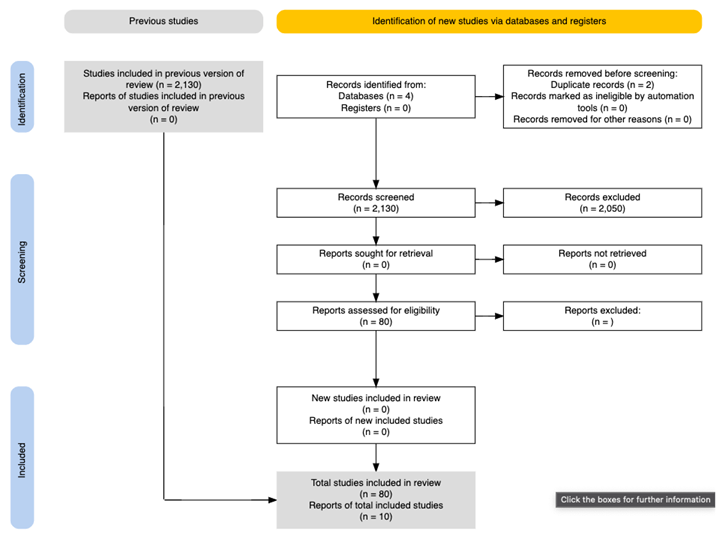
Appendix – PRISMA Flowchart
References
- Wang L, Cai H, Wang Y, et al. Enhanced recovery after elective craniotomy: A randomized controlled trial. J Clin Anesth. 2022;76:110575. [CrossRef]
- Lei Wang et al. Enhanced Recovery After Surgery in Neurosurgical Patients Undergoing Elective Craniotomy: A Randomized Study. J Clin Anesth. 2022.
- Kim SH, Choi SH, Moon J, et al. Enhanced Recovery After Surgery for Craniotomies: A Systematic Review and Meta-analysis. J Neurosurg Anesthesiol. 2025;37(1):11–19. [CrossRef]
- Li M, Liu M, Cui Q, et al. Effect of Dexmedetomidine on Postoperative Delirium in Patients Undergoing Awake Craniotomies: Study Protocol of a Randomized Controlled Trial. Trials. 2023;24:607. [CrossRef]
- Elayat A, Jena SS, Nayak S, et al. Enhanced recovery after surgery – ERAS in elective craniotomies: a non-randomized controlled trial. BMC Neurol. 2021;21(1):127. [CrossRef]
- Zaed I, Marchi F, Milani D, et al. Role of Enhanced Recovery after Surgery (ERAS) Protocol in the Management of Elderly Patients with Glioblastoma. J Clin Med. 2023;12(18):6032. [CrossRef]
- McLaughlin N, et al. The Enhanced Recovery After Surgery Pathway for Pituitary Surgery: Early Results. World Neurosurg. 2014;82(5):e661–e669. [CrossRef]
- Lobatto DJ, et al. Enhanced Recovery After Surgery in Meningioma Patients: Results From a Pilot Study. World Neurosurg. 2020;134:e756–e764.
- Han X, et al. Enhanced Recovery After Surgery Protocol for Aneurysmal Clipping: A Randomized Controlled Trial. Chin J Prac Nerv Dis. 2019.
- Wang C, et al. Effect of an Enhanced Recovery After Surgery (ERAS) Program on Perioperative Outcomes in Neurosurgery. J Neurosurg Sci. 2019.
- X-Peters E, Robinson M, Serletis D. Registration for “Enhanced recovery after surgery for patients un dergoing cranial surgery: a systematic review.” PROSPERO international prospective register of systematic reviews. Available at: https://www.crd. york.ac.uk/prospero/display_record.php?RecordID¼ 197187. Accessed February 25, 2021.
- Kim et al. (2025): Uma meta-análise de cinco ensaios clínicos randomizados demonstrou que protocolos ERAS reduziram significativamente o tempo de internação, a dor pós-operatória e a incidência de náuseas e vômitos em pacientes submetidos a craniotomia, sem aumento nas complicações. ResearchGate+1ResearchGate+1.
- Choudhary et al. (2025): Esta revisão sistemática e meta-análise abrangendo 15 estudos concluiu que protocolos ERAS em craniotomias eletivas resultaram em menor tempo de internação, redução de custos hospitalares e melhora no desempenho funcional dos pacientes. ScienceDirect+3Brieflands+3PubMed+3.
- ERAS® Society Guidelines: Embora ainda não existam diretrizes específicas para neurocirurgia, a ERAS® Society fornece recomendações para diversas especialidades, enfatizando a importância de abordagens multimodais e centradas no paciente. SpringerLink+2erassociety.org+2PMC+2Supbumrung et al. (2023): Este estudo destacou que a adesão aos protocolos ERAS em craniotomias neuro-oncológicas está associada a melhores desfechos pós-operatórios, incluindo menor tempo de internação e redução de complicações. thejns.org.
- Jolly et al. (2024): Uma revisão narrativa discutiu os desafios e estratégias para a implementação de protocolos ERAS em neurocirurgia, enfatizando a necessidade de colaboração multidisciplinar e abordagens centradas no paciente. PubMed.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



