Submitted:
01 May 2025
Posted:
07 May 2025
You are already at the latest version
Abstract
The histological evaluation remains the cornerstone of diagnosing highly malignant osteosarcoma, having demonstrated its efficacy and reliability over several decades. However, even in recent times misdiagnoses with severe consequences, including inadequate surgical procedures, have persisted. Consequently, there is a considerable need to enhance diagnostic security further. Adjunct immunohistochemical approaches have proven highly effective in cancer diagnostics generally but have been limited in their utility for differentiating highly malignant osteosarcoma. Molecular genetic findings have significantly improved the diagnosis of Ewing’s sarcoma by identifying specific translocations and chondrosarcoma by detecting specific IDH-gene mutations. However, molecular genetic alterations in highly malignant osteosarcoma exhibit a very high degree of complexity, limiting their diagnostic utility. Given that only 1-2% of the human genome consists of protein-coding sequences, the increasing number of non-coding regulatory RNAs, which are increasingly being described, has garnered significant attention in the field of clinical cancer diagnostics. Over the past several years, patterns of altered non-coding RNA expression have been identified that facilitate the distinction between benign and malignant tumors in various organs. In the field of bone tumors, the experience with this approach has been limited so far. Divergent expression of microRNAs has demonstrated utility for differentiating osteosarcoma from osteoblastoma and discriminating osteosarcoma from giant cell tumor of bone and fibrous dysplasia. However, the application of non-coding(nc)RNA expression patterns for the differential diagnosis of osteosarcoma is still in its nascent stages. This review provides an overview of the current status of ncRNAs in osteosarcoma diagnostics, in conjunction with histological evaluation. The potential of this approach is discussed in detail.
Keywords:
highly malignant osteosarcoma
; non coding RNAs
; differential diagnosis
1. Introduction
High-grade central osteosarcoma is the most common malignant bone tumor and the most common entity of osteosarcomas. It has histologically thoroughly to be distinguished from the other types of osteosarcomas [1]. It is predominantly observed during the second decade of life, though there is a secondary peak in individuals over the age of 40 [2]. In older patients, the efficacy of chemotherapy is reduced [3]. Males are more commonly affected. The preferred sites within the skeleton are the distal femur, proximal tibia, and proximal humerus, although other locations in long bones can also occur. Osteosarcomas of the jaw are rare and have to be assessed differently [4].
The primary symptom is usually pain in the affected region. The interval between the onset of the first clinical symptoms and the diagnosis ranges from weeks to several months, with prolonged courses being uncommon. The prognosis of high-grade osteosarcoma has significantly improved since the 1970s through the use of combined neoadjuvant chemotherapy with methotrexate, doxorubicin, cisplatin, and under certain conditions ifosfamide [5]. With surgical treatment alone, the 5-year survival rate, according to all major statistics, was 10–20%. However, with the introduction of neoadjuvant chemotherapy, this rate has increased to 65–70% [6,7]. But this improvement applies only to patients with localized tumors. The 5-year survival rate remains consistently poor at approximately 30% for patients with metastatic osteosarcoma even with combined chemotherapy [7]. The therapeutic effect of preoperative chemotherapy can be well assessed histologically on the tumor resection specimen (Chapter 9)[8]. However, a correlation between the therapeutic effect and the histological subtype has remained questionable [9]. From an oncological perspective, it is highly unsatisfactory that a plateau phase in the treatment of osteosarcoma patients has been reached with conventional chemotherapy for approximately 40 years. Evidently, no further advancements can be expected from conventional chemotherapy approaches. Similarly, no fundamental developments in the understanding of high-grade osteosarcoma can be anticipated based on histology and immunohistology alone [10]. Recent comprehensive reviews of osteoblastic bone tumors increasingly include molecular genetical and molecular pathological aspects [11,12].
Radiologically, the tumor originates centrally, rapidly destroying the cortex and invading adjacent soft tissues. If the tumor forms abundant mature bone, the radiographic image appears sclerotic. If unmineralized tissue predominates, the tumor presents as an osteolytic type. Macroscopically highly malignant osteosarcoma involves the metaphyseal region, often extending into soft tissues. Epiphyseal involvement is rare, occurring in less than 5% [13]. Some progress has been made over the last several years in primary diagnostics of highly malignant osteosarcoma in the field of radiology and to a lesser extent in the field of histopathology [1]. Molecular genetic studies of osteosarcoma have revealed a tumor of high molecular complexity, yet they lack specificity, rendering them of limited utility for primary diagnostics [14]. In light of this unsatifactory situation, ncRNAs emerged as a promising focus for differential diagnostic challenges in highly malignant osteosarcoma. Consequently, this review focuses on the potential of ncRNAs as an adjunct to the histological primary diagnosis, which has been therapy leading until now [15].
2. Histologic Characteristics
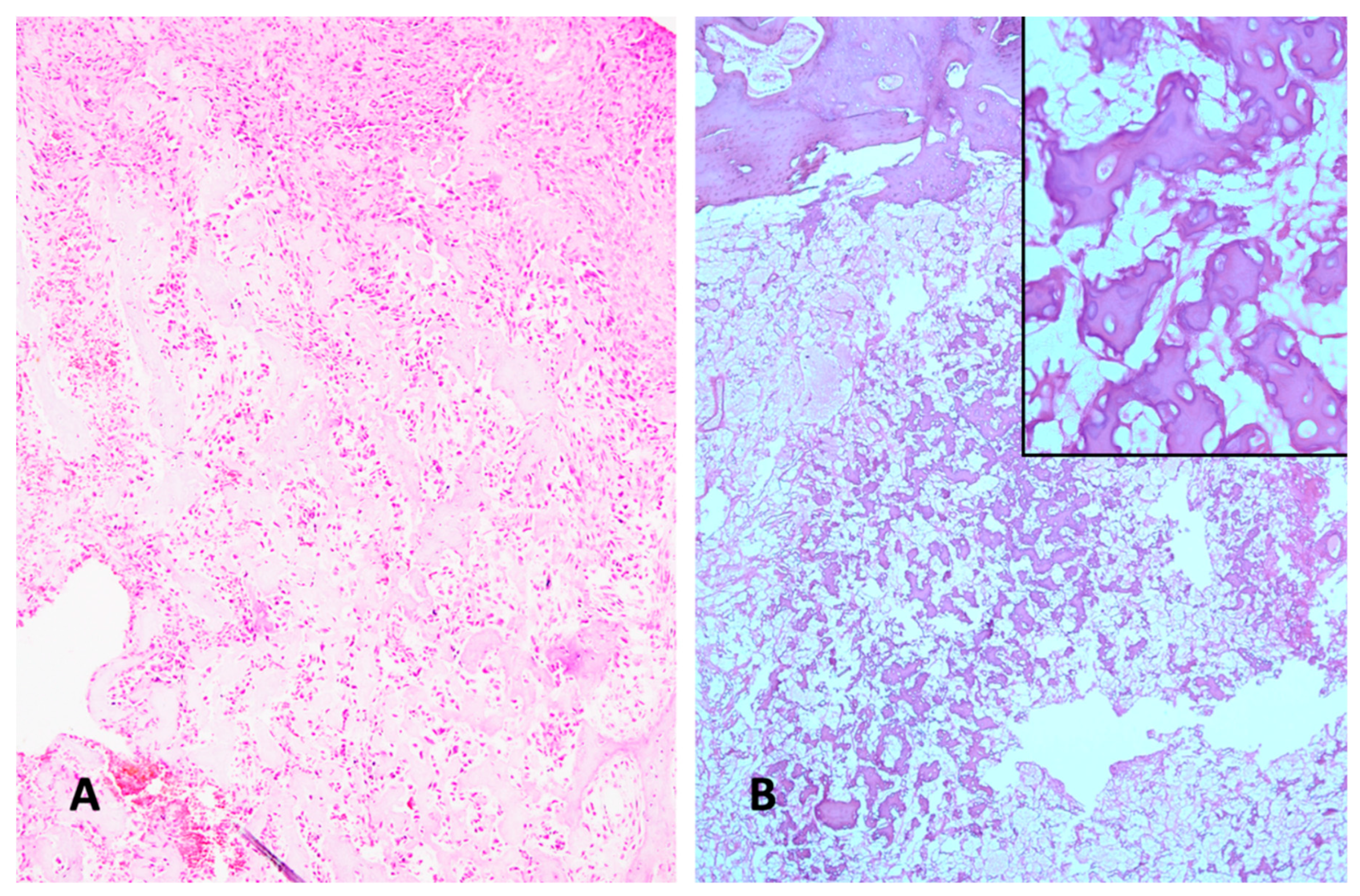
Various subtypes can be distinguished. In osteoblastic osteosarcoma, tumor cells predominantly produce osteoid (Figure 1A). The chondroblastic variant is characterized by neoplastic cartilage (Figure 1B), while the fibroblastic type consists of highly malignant spindle-shaped mesenchymal tumor cells (Figure 1C). Tumor cells consistently exhibit severe nuclear atypia and increased mitotic activity. Rare subtypes include the giant cell-rich variant (Figure 1D). Telangiectatic osteosarcoma can appear similar to aneurysmal bone cysts. However, higher magnification reveals increased mitotic activity and atypical mitoses. The diagnosis of osteosarcoma always requires the detection of at least some osteoid-producing tumor cells. The ability of mesenchymal tumor cells to produce osteoid is considered fundamental to their biological and oncological behavior [16]. The diagnosis of osteosarcoma cannot be made if no tumor osteoid is identified in a malignant bone tumor. Since multifold tissue differentiations can often be found within the same osteosarcoma, the histological appearance of high-grade intramedullary osteosarcoma is extremely heterogeneous. This heterogeneity has raised questions about whether different histological types indicate different prognoses. However, studies so far have not definitively shown that osteoblastic, chondroblastic, fibroblastic, telangiectatic, or giant cell-rich osteosarcomas have distinct prognoses [17]. A more recent study suggests that a histological scoring system may have some prognostic relevance [18]. This scoring system, however, focuses less on histological subtypes and more on characteristics indicative of malignancy, such as the number of mitoses and vascular invasion.
3. Molecular Genetic Characteristics
Alterations in the p53 gene have already been extensively described in osteosarcoma beginning 1987 [19]. Changes in the RB gene were also identified early [20]. The fundamental importance of molecular genetic changes for the pathogenesis of high-grade osteosarcoma has become apparent in its full complexity only after the application of next-generation sequencing (NGS). A first comprehensive study in this area was conducted by Chen et al. [21], followed by additional studies Behjati et al. [22]; Bousquet et al. [23]; Chiappetta et al. [24], Kovac et al. [25], and Perry et al. [26]. In contrast to the majority of malignant tumors in which single nucleotide variations (SNVs) constitute the bulk of genetic alterations, in osteosarcoma structural variations (SVs) and copy number variations (CNVs) are predominant [12]. Comparative molecular genetic studies of other malignant pediatric tumors have shown that juvenile highly malignant osteosarcomas exhibit the highest frequency of structural variations among all pediatric tumors [27]. A specific mechanism of dramatic chromosomal alterations is chromothripsis (from the Greek words chromos for chromosome and thripsis for shattering). This genetic phenomenon was first described by Stephens et al. 2011[28]. In contrast to the gradual model of the adenoma-carcinoma sequence, chromothripsis generates hundreds of genetic alterations in a single cellular crisis involving one or more chromosomes. This phenomenon is observed in only 2-3% of all malignant tumors but in up to 30% of juvenile osteosarcomas [23]. Another genetic alteration phenomenon is kataegis (Greek for "thunderstorm"). It involves hypermutated regions with characteristic features on chromosomes, first described in breast cancer ([29,30]. Kataegis is also found in osteosarcoma [22].
Genomic alterations and allelic imbalances have been suggested as prognostic predictors in highly malignant osteosarcoma [31]. Generally, molecular genetic alterations in this tumor exhibit a high degree of complexity, rendering their diagnostic utility limited thus far [14]. This is in contrast to chondrosarcoma, where IDH mutations have developed as a useful diagnostic tool [32] and specific translocations in Ewing’s sarcoma [33]. Genomic sequencing of osteosarcoma cases has unveiled different genetic alterations that may serve as the foundation for future targeted therapy interventions [34].
4. Challenges in Differential Diagnosis of Highly Malignant Osteosarcoma
The differential diagnosis of other bone tumors and lesions primarily includes osteoblastoma (Figure 2A,B). Additionally, giant cell containing osteosarcoma (Figure 1D) must be differentiated from giant cell tumor of bone and from chondroblastoma. Undifferentiated pleomorphic sarcoma-like osteosarcoma can be barely distinguishable from undifferentiated pleomorphic sarcoma when osteoid is lacking in the former. Another sometimes challenging differential diagnosis is discriminating aneurysmal bone cyst from telangiectatic osteosarcoma. Low grade central osteosarcoma is also included in the differential diagnostic spectrum (Figure 2C). Even the reactive lesion heterotopic ossification can in its proliferative phase cause differential diagnostic problems (Figure 2D). All these lesions require a therapy completely different from osteosarcoma patients. Another notable histodiagnostic challenge is the prediction of chemotherapy response (Figure 3) and, subsequently, the prediction of metastatic risk (Figure 4). Although the histology of highly malignant osteosarcoma has been meticulously described over several decades, histologic indicators for prognosis have never been convincingly validated.
The possibilities of molecular genetics to contribute to the differential diagnostic problems of bone tumors generally has been described in several articles before [35,36,37]. Furthermore, numerous articles on ncRNAs and osteosarcoma have been published in the past decade[15,38,39,40]. The majority of these articles is more focused on prognosis and general diagnostic markers [41] rather than on primary tumor diagnosis in correlation with histological appearance, which remains the essential and legally relevant basis for initiating a specific therapy for osteosarcoma patients. Consequently, this article will concentrate on those ncRNAs that can be beneficial in enhancing the differential diagnostic challenges of highly malignant osteosarcoma. It is crucial to emphasize that a precise diagnosis is paramount for guiding therapy and ensuring patient survival [1].
5. NcRNAs in Translational Biology
It became increasingly evident that only 1-2% of the human genome’s coding sequence encodes for proteins [42](Figure 3). In addition to the RNAs with coding potential, there are substantial quantities of RNA lacking coding potential [43]. The latest edition of the human genome catalog posits that the human genome comprises approximately 20,000 protein-coding genes. This figure has been steadily declining since the 1980s, when it was estimated to be over 100,000 genes [44]. Consequently, we now understand that coding genes constitute only a minuscule fraction of the human genome [45]. Remarkably, this toolkit of protein-coding genes has remained essentially unchanged since the early stages of metazoan evolution, even in sponges that appeared in evolution more than 600 million years ago [46].
The human genome also contains hundreds of thousands of regulatory elements that do not encode proteins. Previously, these elements were dismissed as “junk DNA” [47,48,49,50]. In contrast to the misconceived hypothesis of “junk DNA” the recognition that ncRNAs perform crucial biological functions has been hailed as a major paradigm shift in contemporary molecular biology [51,52]. The role of messenger RNA (mRNA), transfer RNA (tRNA), and ribosomal RNA (rRNA) in gene expression was established in the 1950s. However, it was not until the end of the 1990s that the discovery of microRNAs (miRNAs) and several other small ncRNAs, along with their pivotal roles in post-transcriptional regulation of gene expression, particularly in eukaryotic organisms, gained widespread recognition [53,54].
Functions of regulatory ncRNAs in metazoan differentiation
It had long been observed that the amount of ncRNAs increases with developmental complexity assessed in the increasing number of differentiated cell types [55,56]. In addition, ncRNAs also play a central role in human development and cognition [57]. In addition to other factors such as distal enhancers and transcription factors regulatory ncRNAs have enabled the regulation of temporal and spatial gene expression in evolutionary processes, which is the precondition for increasingly complex multicellularity in higher metazoan organisms [58]. Alternative splicing was not considered to be a sufficient biological strategy for increasing the biodiversity of the metazoan world [59]. This is also corroborated by the observation that the number of protein-coding genes in the genome has remained relatively constant throughout metazoan evolution, from simple organisms such as C. elegans to homo sapiens [60,61,64](Figure 3). The number of protein coding genes does not directly correlate with the organism’s complexity or the number of differentiated cell types. Conversely, the decreasing ratio of protein-coding sequence in percentage of the entire genomic DNA does [62]. Given the pivotal role of ncRNAs in cellular differentiation, it is plausible to presume that they exhibit a correlation with histological diagnostics, which predominantly concentrate on cellular differentiation. [72,73]. Among the various classes of ncRNAs, the role of microRNAs has been the subject of the most extensive investigation to date [63].
Figure 3.
There is no correlation between the number of protein-coding genes and the developmental complexity of a species. Instead, there is a negative correlation between the percentage of the genome occupied by protein-coding sequences and the developmental complexity [64] (Created with Biorender).
Figure 3.
There is no correlation between the number of protein-coding genes and the developmental complexity of a species. Instead, there is a negative correlation between the percentage of the genome occupied by protein-coding sequences and the developmental complexity [64] (Created with Biorender).

Figure 4.
A Osteoblastic osteosarcoma after preoperative chemotherapy with viable malignant tumor lacking any signs of regression or necrosis (H&E x100). B Completely devitalized necrotic area of former osteoblastic osteosarcoma with no viable tumor cells left after preoperative chemotherapy (H&E x100). Inset: high power view of completely devitalized former osteoblastic tumor tissue and remnants of osteoid (H&E x400).
Figure 4.
A Osteoblastic osteosarcoma after preoperative chemotherapy with viable malignant tumor lacking any signs of regression or necrosis (H&E x100). B Completely devitalized necrotic area of former osteoblastic osteosarcoma with no viable tumor cells left after preoperative chemotherapy (H&E x100). Inset: high power view of completely devitalized former osteoblastic tumor tissue and remnants of osteoid (H&E x400).
Classification of ncRNAs, Basic Facts
Non-coding RNAs (ncRNAs) are primarily categorized into two distinct classes based on the number of nucleotides. Small non-coding RNAs (sncRNAs) are defined as molecules with a length of less than 200 nucleotides, while long non-coding RNAs (lncRNAs) exceed 200 nucleotides in length[43]. In the context of tumor diagnostics, sncRNAs, and lncRNAs including circular RNAs (circRNAs) hold most practical importance. Consequently, this review focuses on these types of ncRNAs [65,66,67]. Within the class of sncRNAs, microRNAs (miRNAs) have garnered the most extensive research attention in the field of cancer. Their primary function is to exert negative regulation of gene expression by targeting specific messenger RNAs, leading to their dysfunction and degradation [68,69]. The details of miRNA biogenesis are discussed elsewhere [70].
6. NcRNAs as Diagnostic Biomarkers in Cancer
An ongoing debate centers on whether the classification of human tumors based on their tissue of origin remains pertinent in the context of cancer genomics and precision oncology [71]. Historically, histologic evaluation of tissue biopsies, augmented by immunohistochemistry, has been the cornerstone of definitive cancer diagnosis [72,73]. In the majority of tumor diagnoses, alternative diagnostic methods that can be utilized have essentially an adjunctive role. This is the case for image radiology and other conventional methods of laboratory medicine. Molecular genetic methods centered on whole genome or whole exome NGS have been demonstrated to significantly enhance histopathologic diagnoses in approximately 15% of all cancer diagnoses [74]. Prior to this background, therapeutic approaches that are agnostic with regard to histology are still subject to ongoing debate [75]. Until now, the basic principle of histopathologic tumor classifications has been the evaluation of tumor tissue in relation to its tissue of origin and the degree of similarity to the tissue of origin [76]. It can be assumed that the future potential of liquid biopsies is not only powered by analysis of circulating-free tumor DNA (cfDNA) but also by analysis of different classes of ncRNAs.
The extensive regulatory RNA machinery is responsible for the evolution of metazoan complexity with increasingly specialized cell types that are contingent upon the evolutionary stage [77]. It can be assumed that the differential expression of non-regulatory RNAs corresponds to histopathological tumor classification and diagnosis [78,79,80]. In the last several years extensive reviews have been published on the central role of ncRNAs in cancer [81,82,83]. A main advantage of ncRNAs as a tool for cancer diagnostics and classification is their detectability in plasma, serum and other body fluids [84,85]. This is all the more important, because the risk of tumor cell seeding through biopsies cannot be entirely ruled out [86]. Particularly the exosomes as carriers of different ncRNAs are considered as an important diagnostic tool [87,88]. Liquid biopsies have also demonstrated remarkable success in detecting gene alterations in cancer patients [89,90].
MiRNA as Tools in Cancer Diagnosis
The biogenesis and mechanism of action of miRNAs have been extensively elucidated in the past several years [91]. The utility of miRNA patterns in the diagnosis of cancer has long been under discussion. Their use as a diagnostic tool is evident, because these small molecules show stability in the different fluids of the human body [79]. In addition to cancer diagnosis miRNAs have also the potential to predict drug efficiency and the clinical prognosis of the cancer patients [92]. They showed a general downregulation in tumors. Poorly differentiated tumors could also successfully be classified using miRNAs [93,94]. To this day, the correct histopathological diagnosis remains the basis for discrimination between benign and malignant tumors. However, uncountable cases of so called “borderline tumors” also in the field of bone and soft tissue tumors [95] point to the limitations of the many decades old histopathologic approach for securing the malignancy of tumors. Recently it could be shown that comprehensive miRNA expression profiles combined with a computational deep cancer classifier were able to differentiate between breast cancer and skin cancer and its benign histologic counterparts. This might be considered as the beginning of computational classifiers for securing the malignant traits of a given tumor [96].
LncRNAs as Diagnostic Biomarkers in Cancer
Over the past several years, it has become increasingly evident that big parts of the human genome are transcribed into a multitude of lncRNAs, whose classification and function have been extensively described in numerous publications [97,98]. LncRNAs have been shown to have functions in many molecular and cellular processes also in development [99]. They have an important role in cancer pathogenesis [100]. Furthermore they show a specificity for different tissues and different cancer entities [101].
CircRNAs as diagnostic Biomarkers in cancer
CircRNAs being shaped in ring structures are characterized by a strong chemical stability and due to lacking free ends show a strong resistance to the activities of ribonucleases. With these features they have good preconditions acting as diagnostic and prognostic markers of cancer [102]. The first endogenous human circRNAs were identified in 1991. A comprehensive time table depicting the discovery and development of knowledge on circRNAs in the field of cancer is dealt with by Pisignano et al. [103]. Their considerable value in molecular cancer diagnosis has increasingly been emphasized by others [104]. For example, it has been convincingly shown that three specific circular RNAs in serum exosomes were successfully applied as diagnostic biomarkers for non-small-cell lung cancer in the Chinese population [105], and a specific exosomal serum circRNA could serve as diagnostic biomarker for colorectal cancer [106]. However, it is recommended that larger and more controlled clinical studies are required before applying circRNAs as secure diagnostic and therapy guiding factors in clinical oncological practice [107].
Utility ncRNAs in Differentiating Benign and Malignant Tumors
Table 1 presents examples of the successful application of ncRNAs for discrimination between benign and malignant tumors in different organs. This approach is also applicable to the skeletal system, where miRNAs are useful in distinguishing enchondroma from low-grade chondrosarcoma [108]. In other organs miRNAs discriminate between benign prostatic hyperplasia and prostatic cancer [109]. MiRNAs, particularly miRNA-122 has been validated for discriminating between thyroid cancer and benign nodules [110]. In breast cancer patients it is possible to discriminate early stages of breast cancer from benign diseases [111]. In another study circulating miRNAs have demonstrated their capacity for detecting breast cancer in comparison to high-risk benign breast tumors [112]. A panel of potential lncRNA biomarkers was detected as useful for distinguishing benign ad malignant liver tumors [113]. In a landmark study Kaczmarek et al. applied a deep cancer classifier for discriminating neoplastic tissue from nonneoplastic tissue on the basis of differential miRNA expression focusing on nonneoplastic tissue and breast cancer and nonneoplastic tissue and skin cancer [96]. Defining different miRNA panels can also be useful discriminating between benign and malignant pleura effusions [114]. Distinguishing malignant borderline tumors from malignant ovarian cancers solely on histological findings presents a diagnostic challenge. MiRNAs have also proven to be valuable in this differential diagnosis [115]. A notable challenge in histopathological diagnosis lies in the distinction between adrenocortical adenoma and carcinoma. In this context, miRNA profiles can serve as a valuable supplementary tool for this distinction [116].
7. NcRNAs as an Adjunct to Histological Differential Diagnosis of Highly Malignant Osteosarcoma
Highly malignant osteosarcoma may even today be misdiagnosed as another tumor entity resulting in inappropriate treatment including wrong surgical procedures [117]. Osteoblastoma is typically radiologically characterized as a well-defined, circumscribed lesion that does not present diagnostic challenges in standard clinical scenarios. But sometimes diagnostic problems can arise discriminating between osteoblastoma and osteosarcoma. This is particularly the case for aggressive osteoblastoma and so called epithelioid osteoblastoma, when atypical nuclei may cause some diagnostic confusion [118]. Furthermore, a tumor entity of osteoblastoma like osteosarcoma has been established, which can generate differential diagnostic problems in both directions [119]. Recently recurrent translocations in FOS and FOSB have been detected in osteoblastoma and also osteoid osteoma and may be of diagnostic value [120,121]. However, osteosarcomas with FOS expression have rarely been described [122]. Furthermore, methylation and copy number profiling might be useful for differentiating osteoblastoma from malignant tumors [123]. In the study by Riester et al. [124] miRNAs from FFPE tumor specimens of 11 osteoblastomas and 11 osteosarcomas were extracted and analyzed by high throughput miRNA sequencing. Elevated expression of hypoxia related miRNA-210 in the osteosarcoma cases in comparison to osteoblastoma cases may be a future diagnostic adjunct in discriminating osteoblastoma and osteosarcoma. Additional to this study investigations of ncRNAs of osteoblastoma are very rare and without mention of differential diagnostic or biomarker aspects [125] . So far there has been only one study published on the differential diagnosis of giant cell tumor of bone and osteosarcoma [41]. The few other available studies on giant cell tumor of bone refer to lncRNA expression in the recurrence of giant cell tumors [126] or general aspects of miRNA expression [125,127]. Araki et al. [41] have found that patients with osteosarcoma have an increased serum level of miR-1261 not only compared to patients with giant cell tumors of bone, but also to patients with fibrous dysplasia, osteoblastoma and chondrosarcoma. No substantial research studies on ncRNAs in chondroblastomas have been published. Similarly, no research studies have been conducted on ncRNAs in aneurysmal bone cysts so far.
Even the reactive lesion of traumatic heterotopic ossification (THO) can pose diagnostic challenges in the differential diagnosis of osteosarcoma [1]. A recent study of miRNAs in THO could contribute to a better understanding of the underlying mechanisms and offer new possibilities for therapeutic targets [128]. However, differential diagnostic aspects are not yet available. Mierzejewskiy et al. [129] could show that miR-99b, miR-146, miR-204, and LINC00320 were up-regulated in THO, when compared with normal bone and muscle tissue. In future these ncRNAs might serve as useful biomarkers for the differential diagnosis of THO to highly malignant osteosarcoma (Figure 2D).
In summary, analyses of various ncRNA categories have thus far yielded only limited reliable data to assist histological diagnosis in distinguishing between highly malignant osteosarcomas, benign tumors, reactive lesions, and low malignant osteosarcomas (Table 2). In contrast, there are numerous results available for discriminating malignant tumors from benign lesions in cancers of other organs (Table 1). Consequently, there is an urgent need to apply advanced molecular data from the field of ncRNAs to enhance these differential diagnoses around osteosarcoma to a more effective level.
8. NcRNAs as General Diagnostic Biomarkers for Highly Malignant Osteosarcoma
NcRNAs in serum or plasma can be useful as diagnostic markers for early detection of osteosarcoma as has been extensively discussed by Araki et al. [130]. This feature can also facilitate the primary diagnosis of osteosarcomas even before taking biopsies. Other studies also focus on the utility of ncRNAs as prognostic markers. Since this review centers on the diagnosis of osteosarcoma, Table 3 depicts the most important markers for early primary diagnosis. Studies with prognostic and therapeutic aspects are not considered here.
9. Possibilities of ncRNAs for Prediction Chemotherapy Response
Since the advent of neoadjuvant chemotherapy for osteosarcoma patients, histological investigations of post-chemotherapy operation specimens have been of considerable oncological interest. These investigations have been employed to assess the extent of regression alterations and tumor necrosis associated with the chemotherapy effect [140,141]. The ratio of necrosis in correlation to viable tumor tissue with at least 90% necrosis has been considered as a prognostic factor in the majority of studies correlating with patient’s outcome [142]. But this general experience has not been uncontradicted. A multivariate analysis confirmed the prognostic significance of age and stage, while poor necrosis rates did not attain statistical significance [143].
This implies that the ratio of necrosis in post-chemotherapy specimens cannot be reliably utilized as a definitive factor for guiding therapy. Deep learning-based analysis of the tumor resection specimens could enhance the accuracy of the histologic investigation, but did not enhance the prognostic value [144]. Whole exome sequencing genomic analysis revealed only slight variations between histologic responders and non-responders among osteosarcoma patients, indicating that this methodical approach did not attain unequivocal clinical significance so far [145]. Advanced radiological strategies can provide some indications of the chemotherapy response, but they cannot be considered sufficiently reliable for making therapy-related decisions [146,147,148]. A comprehensive evaluation of coding gene expression through the analysis of mRNA expression profiles in conjunction with lncRNAs appears to hold significant value. Nevertheless, the clinical applicability of this approach as a diagnostic tool in oncology remains so far restricted [149].
Given the aforementioned background, the role of ncRNAs has been discussed as a novel and effective tool for predicting chemotherapy response in osteosarcoma patients for several years. The neoadjuvant chemotherapy regimen for osteosarcoma patients has traditionally been based on the combination of high-dose methotrexate (HD-MTX), Adriamycin (ADR), and Cisplatin (DDP) [150] with the possible addition of ifosfamide for poor responders and patients with metastases at presentation [151]. The interplay of different classes of ncRNAs with the pharmacological and cytotoxical effects of these drugs and on multidrug resistance (MDR) is a major topic in current osteosarcoma research [152]. The number of publications exploring the role of ncRNAs in the chemotherapy effects of osteosarcoma has surged significantly over the past few years. While many of these studies are conducted in vitro, utilizing established single-cell lines, their practical clinical relevance may be limited. In contrast, in vivo studies on human tumor tissue or body fluids are considerably rarer. In the following, a concise overview of cell culture studies is provided, with the in vivo studies discussed in greater detail.
Cell culture studies
The miRNA-29 family has a tumor suppressor role in methotrexate resistance and can promote cell apoptosis [153]. Regarding the effects of ncRNAs on cisplatin, it was discovered that a knockdown of lncRNA ANRIL enhances osteosarcoma cells’ sensitivity to cisplatin-induced cytotoxicity. This finding has prompted speculation regarding ANRIL as a potential therapeutic target for osteosarcoma chemotherapy [154]. The lncRNA GAS5 promotes cisplatin chemosensitivity via the GAS5/miR-26b-5p/TP53INP1 axis pointing to lncRNA GAS5 as a possible indicator for cisplatin-based chemotherapy [155]. Furthermore, it has been demonstrated that circRNA CircUBAP2 plays a pivotal role in the cisplatin resistance of osteosarcoma cells by modulating the expression of miR-506-3p [156]. Circ-RNA CHI3L levels were increased in cisplatin-resistant osteosarcoma cells and circRNA-CHI3L1.2 knockdown sensitized cisplatin-resistant osteosarcoma cells to cisplatin through the miR-340-5p-LPAATβ axis [157]. The lncRNA HOTAIR was shown to promote cisplatin resistance of Saos2/DDP, MG-63/DDP, and U2OS/DDP cells by affecting cell proliferation, invasion, and apoptosis via miR-106a-5p/ STAT3 axis [158]. Numerous cell culture studies have underscored the significance of ncRNAs in mediating diverse effects of doxorubicin. For instance, miRNA-150 has the ability to sensitize osteosarcoma cells to chemotherapy treatment with Doxorubicin. [159]. The overexpression of miR-506-3p could inhibit doxorubicin resistance in drug resistant osteosarcoma cells [160]. The circRNA Hsa_circ_0004674 has been shown to increase the doxorubicin resistance of osteosarcoma cells by regulating the miR-342-3p/FBN1 axis [161].
Clinical studies
The number of clinical studies investigating the possibilities of different types of ncRNAs as predictor of chemotherapy response is considerably lower [162,163,164,165]. In a general assessment Chen et al. [166] concluded that drug resistance related miRNAs will probably supplement or may even partly replace existing biomarkers. In addition to this general assessment there have been published studies focusing on specific miRNAs in the last several years. For instance, levels of miRNA-34a were measured in the serum of osteosarcoma patients with favorable and unfavorable responses to chemotherapy. Patients with histologically unfavorable responses exhibited significantly lower levels of that miRNA compared to patients with favorable responses [167]. Results of Diao et al. [168] revealed a significantly lower level of miRNA-22 in a collective of 120 patients with highly malignant osteosarcoma. Low levels of miRNA-22 were significantly correlated with poor tumor response to preoperative chemotherapy. In another study [169] it could be confirmed that low serum levels of miRNA-375 were also significantly correlated with a poor tumor response to preoperative chemotherapy in 95 patients with highly malignant osteosarcoma having graded the chemotherapy response according to the method of Huvos [170]. MiRNA-132 can be induced by angiogenic growth factors [171] and plays a role in the development of osteoarthritis [172]. Jie Yang et al. [173] have analyzed Mi132 expression in the tissue of 166 osteosarcomas and corresponding non-cancerous tissue. MIRNA-132 expression was decreased in the osteosarcoma specimens with poor response to chemotherapy. Yuan et al.[174] have found that high miRNA-21 levels were correlated with an advanced stage after classification according to Enneking and furthermore histological tumor response with increased serum miRNA-21 level in responders compared with poor responders (P<0.001). Another study also showed the usefulness of miRNA-21 for chemosensitivity prediction of osteosarcoma patients with the expression level of patients with osteosarcoma closely related to the therapeutic effects [175]. In an early study comprising 27 osteosarcoma patients 5 miRNAs were identified which can discriminate between good and poor chemotherapy response. MiR-92a, miR-99b, miR-193a-5p and miR-422a were overexpressed in good responders whereas miR-132, was downregulated [176].
In addition to miRNAs circular RNAs have potential for predicting chemotherapy response in osteosarcoma patients as well. Circular RNA LARP4 showed a correlation with histologically assessed response rate in 72 osteosarcoma patients after preoperative treatment with the MAP regimen (high-dose methotrexate, cisplatin, and doxorubicin). Patients with good response were Circ-LARP4 high and with low response CircLARP4 low [177].

Table 4.
ncRNAs from osteosarcoma patient’s serum, plasma or sarcoma tissue, which have been identified as indicators of poor response to chemotherapy.
Table 4.
ncRNAs from osteosarcoma patient’s serum, plasma or sarcoma tissue, which have been identified as indicators of poor response to chemotherapy.
| Non coding RNA | Materials | Results | Source |
|---|---|---|---|
| miRNA-34a | Serum | Negatively associated with chemotherapy resistance of OS patients. | Lian H et al. [167] |
| miRNA-22 | Plasma | Low plasma miR-22 level were corre- lated with poor tumor response to preoperative chemotherapy. |
Diao ZB et al. [168] |
| miRNA-375 | Serum | low serum miR 375 level was significantly associated with poor tumor response to chemotherapy | Liu W et al. [169] |
| miRNA-132 | Sarcoma tissue, fresh frozen |
miR-132 expression was decreased in the osteosarcoma specimens with poor response to chemotherapy. | Yang J et al. [173] |
| miRNA-21 | Serum | High serum miR-21 was significantly correlated with advanced Enneking stage and chemotherapeutic resistance. |
Yuan J et al. [174] |
| miRNA-21 | Serum | The expression level of serum miR-21 in patients with osteosarcoma is closely related to the therapeutic effects of osteosarcoma. |
Hua Y et al. [175] |
| miR-92a, miR-99b, miR-132, miR-193a-5p miR-422a | Sarcoma tissue, FFPE | miRNAs miR-92a, miR-99b, miR-132, miR-193a-5p and miR-422a could discriminate good from bad responders. | Gougelet A et al. [176] |
10. NcRNAs and Prediction of Metastatic Risk
It has been widely held that the conventional histological subtype of highly malignant osteosarcoma does not provide any discernible indicators of the likelihood of hematogenous metastasis development (Figure 5) [178]. But the structure of the extra cellular matrix has been shown to contribute to metastasis and progression of osteosarcoma [179]. MiRNAs are deeply involved in regulating angiogenesis, a central feature of metastasis, and epithelial–mesenchymal transition. Because of these and others features miRNAs have a high potential of being assessed as biomarkers for metastatic risk [180]. In a similar way lncRNAs are also deeply involved in the metastatic cascade. They contribute to epithelial-mesenchymal transition mesenchymal transition, invasion and migration and are affiliated with the nuclear factor κB, and TGFβ pathways. LncRNAs are useful indicators for assessing the metastatic risk in patients with different cancer entities, mostly carcinomas [181]. However, against this biologically promising background clinical oncological studies performed on serum/plasma or tumor tissue of osteosarcoma patients have been rather limited so far (Table 5) in comparison to cell culture studies, which have been performed abundantly [182].
A recent study by Abedi et al.[183] identified early diagnostic biomarkers using miRNA expression profiles associated with osteosarcoma metastasis. Based on network analysis and machine learning algorithms new diagnostic tools have been established, which enable a reliable differentiation between metastatic osteosarcoma and non-metastatic samples based on newly discovered miRNA signatures. The results showed that miR-34c-3p and miR-154-3p act as the most promising parameters in the diagnosis of metastatic osteosarcoma. In osteosarcoma miRNAs and lncRNAs as exosomal biomarkers are predictors for developing hematologic metastases [184]. Another study on exosomal biomarkers has shown that different miRNAs such as miRNA-675, miRNA-1307, and miRNA-25-3p and lncRNAs RAMP2-AS1 and CASC15 may be diagnostically useful for predicting metastatic risk in osteosarcoma and other sarcoma entities [185]. High levels of miRNA-34a in osteosarcoma patients do not only correlate with chemotherapy response but with longer overall survival and a decreased risk of metastasis as well [168]. Another miRNA with predictive potential for metastasis in osteosarcoma patients is miRNA-506, which revealed a significantly higher serum level in patients with non-metastatic osteosarcoma compared to patients with lung metastases [186]. These authors also suggest that a miRNA-mRNA-network of higher complexity might in future serve as predicting factor for hematogenic metastases in osteosarcoma. The level of lncRNA BCAR4 is significantly correlated with the occurrence of distant metastases of osteosarcoma patients [187]. A study by Karras et al. (in preparation) investigating a differential miRNA expression between non-metastasizing primary osteosarcomas, primary osteosarcomas, and their lung and bone metastases, respectively, revealed the most differential expressed miRNAs between the non-metastatic primary OS and the metastatic primary OS, particularly the metastatic primary OS that developed lung metastases. Further analysis is necessary to determine whether this result can be utilized as a predictor of metastatic potential in patients with primary osteosarcomas who do not have hematogenic metastases at the time of initial diagnosis.
11. Concluding Remarks
Histologic evaluation is still the most reliable and most effective method for diagnosing highly malignant osteosarcoma [1]. Despite the well-established histologic diagnostics, highly malignant osteosarcoma can be misdiagnosed as another bone tumor, leading to catastrophic consequences such as incorrect therapy and misguided surgical procedures. [121]. Highly malignant osteosarcoma serves as a paradigmatic example of a tumor characterized by a high degree of molecular genetic complexity. This complexity is likely the primary reason why molecular genetic investigations have not yet yielded clinically significant diagnostic markers [14]. Therefore, additional methods are necessary to enhance the differential diagnosis. Given that over 98% of the human genome is non coding, it is logical to explore diagnostic tools among the various types of ncRNAs [81;82;83]. NcRNAs have demonstrated significant diagnostic potential in tumors of other organs, particularly in distinguishing benign from malignant tumors. However, their application as a diagnostic tool in bone tumor diagnosis has been limited so far, accounting for the focus of this review. To enhance the success of establishing ncRNAs as diagnostic tools in the field of osteosarcoma, more sophisticated deep cancer classifiers may be required [96]. This approach is anticipated to further reduce the incidence of misdiagnoses based solely on histology, thereby ensuring the most effective treatment for bone tumor patients.
Declaration of Interest
The authors declare that there are no competing interests associated with the manuscript.
Author Contributions
Albert Roessner conceived and prepared the manuscript. The other authors contributed to its preparation.
References
- Yoshida, A. Osteosarcoma. Surg. Pathol. Clin. 2021, 14, 567–583. [Google Scholar] [CrossRef] [PubMed]
- Savage, S.A.; Mirabello, L. Using Epidemiology and Genomics to Understand Osteosarcoma Etiology. Sarcoma 2011, 2011, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Nagano, A.; Matsumoto, S.; Kawai, A.; Okuma, T.; Hiraga, H.; Matsumoto, Y.; Nishida, Y.; Yonemoto, T.; Hosaka, M.; Takahashi, M.; et al. Osteosarcoma in patients over 50 years of age: Multi-institutional retrospective analysis of 104 patients. J. Orthop. Sci. 2020, 25, 319–323. [Google Scholar] [CrossRef] [PubMed]
- Baumhoer, D.; Brunner, P.; Eppenberger-Castori, S.; Smida, J.; Nathrath, M.; Jundt, G. Osteosarcomas of the jaws differ from their peripheral counterparts and require a distinct treatment approach. Experiences from the DOESAK Registry. Oral Oncol. 2014, 50, 147–153. [Google Scholar] [CrossRef]
- Robinson, M.J.; Davis, E.J. Neoadjuvant Chemotherapy for Adults with Osteogenic Sarcoma. Curr. Treat. Options Oncol. 2024, 25, 1366–1373. [Google Scholar] [CrossRef]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic Factors in High-Grade Osteosarcoma of the Extremities or Trunk: An Analysis of 1,702 Patients Treated on Neoadjuvant Cooperative Osteosarcoma Study Group Protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef]
- Kager, L.; Zoubek, A.; Pötschger, U.; Kastner, U.; Flege, S.; Kempf-Bielack, B.; Branscheid, D.; Kotz, R.; Salzer-Kuntschik, M.; Winkelmann, W.; et al. Primary Metastatic Osteosarcoma: Presentation and Outcome of Patients Treated on Neoadjuvant Cooperative Osteosarcoma Study Group Protocols. J. Clin. Oncol. 2003, 21, 2011–2018. [Google Scholar] [CrossRef]
- Salzer-Kuntschik, M.; Delling, G.; Beron, G.; Sigmund, R. Morphological grades of regression in osteosarcoma after polychemotherapy ? Study COSS 80. J. Cancer Res. Clin. Oncol. 1983, 106, 21–24. [Google Scholar] [CrossRef]
- Bacci, G.; Bertoni, F.; Longhi, A.; Ferrari, S.; Forni, C.; Biagini, R.; Bacchini, P.; Donati, D.; Manfrini, M.; Bernini, G.; et al. Neoadjuvant chemotherapy for high-grade central osteosarcoma of the extremity. Cancer 2003, 97, 3068–3075. [Google Scholar] [CrossRef]
- Green, J.T.; Mills, A.M. Osteogenic tumors of bone. Semin. Diagn. Pathol. 2014, 31, 21–29. [Google Scholar] [CrossRef]
- Kansara, M.; Teng, M.W.; Smyth, M.J.; Thomas, D.M. Translational biology of osteosarcoma. Nat. Rev. Cancer 2014, 14, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Rickel, K.; Fang, F.; Tao, J. Molecular genetics of osteosarcoma. Bone 2017, 102, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Cè, M.; Cellina, M.; Ueanukul, T.; Carrafiello, G.; Manatrakul, R.; Tangkittithaworn, P.; Jaovisidha, S.; Fuangfa, P.; Resnick, D. Multimodal Imaging of Osteosarcoma: From First Diagnosis to Radiomics. Cancers 2025, 17, 599. [Google Scholar] [CrossRef]
- Franceschini, N.; Lam, S.W.; Cleton-Jansen, A.-M.; Bovée, J.V.M.G. What’s new in bone forming tumours of the skeleton? Virchows Arch. 2019, 476, 147–157. [Google Scholar] [CrossRef]
- Fan, L.; Zhong, Z.; Lin, Y.; Li, J. Non-coding RNAs as potential biomarkers in osteosarcoma. Front. Genet. 2022, 13, 1028477. [Google Scholar] [CrossRef]
- Mutsaers, A.J.; Walkley, C.R. Cells of origin in osteosarcoma: Mesenchymal stem cells or osteoblast committed cells? Bone 2014, 62, 56–63. [Google Scholar] [CrossRef]
- Klein, M.J.; Siegal, G.P. Osteosarcoma. Am. J. Clin. Pathol. 2006, 125, 555–581. [Google Scholar] [CrossRef]
- Chui, M.H.; Kandel, R.A.; Wong, M.; Griffin, A.M.; Bell, R.S.; Blackstein, M.E.; Wunder, J.S.; Dickson, B.C.; Michael Herman Chui, MD; Rita A. Kandel, MD; Marcus Wong, BSc; Anthony M. Griffin, MSc; Robert S. Bell, MD; Martin E. Blackstein, MD, PhD; Jay S. Wunder, MD, MSc; Brendan C. Dickson, MD, MScFrom the Departments of Pathology and Laboratory Medicine; Md; et al. Histopathologic Features of Prognostic Significance in High-Grade Osteosarcoma. Arch. Pathol. Lab. Med. 2016, 140, 1231–1242. [Google Scholar] [CrossRef]
- Masuda, H.; Miller, C.; Koeffler, H.P.; Battifora, H.; Cline, M.J. Rearrangement of the p53 gene in human osteogenic sarcomas. Proc. Natl. Acad. Sci. 1987, 84, 7716–7719. [Google Scholar] [CrossRef]
- Toguchida, J.; Ishizaki, K.; Sasaki, M.S.; Nakamura, Y.; Ikenaga, M.; Kato, M.; Sugimot, M.; Kotoura, Y.; Yamamuro, T. Preferential mutation of paternally derived RB gene as the initial event in sporadic osteosarcoma. Nature 1989, 338, 156–158. [Google Scholar] [CrossRef]
- Chen, X.; Bahrami, A.; Pappo, A.; Easton, J.; Dalton, J.; Hedlund, E.; Ellison, D.; Shurtleff, S.; Wu, G.; Wei, L.; et al. Recurrent Somatic Structural Variations Contribute to Tumorigenesis in Pediatric Osteosarcoma. Cell Rep. 2014, 7, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Behjati, S.; Tarpey, P.S.; Haase, K.; Ye, H.; Young, M.D.; Alexandrov, L.B.; Farndon, S.J.; Collord, G.; Wedge, D.C.; Martincorena, I.; et al. Recurrent mutation of IGF signalling genes and distinct patterns of genomic rearrangement in osteosarcoma. Nat. Commun. 2017, 8, 15936–15936. [Google Scholar] [CrossRef]
- Bousquet, M.; Noirot, C.; Accadbled, F.; de Gauzy, J.S.; Castex, M.; Brousset, P.; Gomez-Brouchet, A. Whole-exome sequencing in osteosarcoma reveals important heterogeneity of genetic alterations. Ann. Oncol. 2016, 27, 738–744. [Google Scholar] [CrossRef]
- Chiappetta, C.; Mancini, M.; Lessi, F.; Aretini, P.; De Gregorio, V.; Puggioni, C.; Carletti, R.; Petrozza, V.; Civita, P.; Franceschi, S.; et al. Whole-exome analysis in osteosarcoma to identify a personalized therapy. Oncotarget 2017, 8, 80416–80428. [Google Scholar] [CrossRef]
- Kovac, M.; Blattmann, C.; Ribi, S.; Smida, J.; Mueller, N.S.; Engert, F.; Castro-Giner, F.; Weischenfeldt, J.; Kovacova, M.; Krieg, A.; et al. Exome sequencing of osteosarcoma reveals mutation signatures reminiscent of BRCA deficiency. Nat. Commun. 2015, 6, 8940–8940. [Google Scholar] [CrossRef]
- Perry, J.A.; Kiezun, A.; Tonzi, P.; Van Allen, E.M.; Carter, S.L.; Baca, S.C.; Cowley, G.S.; Bhatt, A.S.; Rheinbay, E.; Pedamallu, C.S.; et al. Complementary genomic approaches highlight the PI3K/mTOR pathway as a common vulnerability in osteosarcoma. Proc. Natl. Acad. Sci. 2014, 111, E5564–E5573. [Google Scholar] [CrossRef]
- Downing JR, Wilson RK, Zhang J, Mardis ER, Pui C-H, Ley TiJ, et al. The Pediatric Cancer Genome Project. Nat Genet 2013; 44:619–22. [CrossRef]
- Stephens PJ, Greenman CD, Fu B, Yang F, Bignell GR, Mudie LJ et al. Massive genomic rearrangement acquired in a single catastrophic event during cancer development. Cell 2011, 144, 27–40. [Google Scholar] [CrossRef]
- Nik-Zainal, S.; Alexandrov, L.B.; Wedge, D.C.; Van Loo, P.; Greenman, C.D.; Raine, K.; Jones, D.; Hinton, J.; Marshall, J.; Stebbings, L.A.; et al. Mutational Processes Molding the Genomes of 21 Breast Cancers. Cell 2012, 149, 979–993. [Google Scholar] [CrossRef]
- Nik-Zainal, S.; Davies, H.; Staaf, J.; Ramakrishna, M.; Glodzik, D.; Zou, X.; Martincorena, I.; Alexandrov, L.B.; Martin, S.; Wedge, D.C.; et al. Landscape of somatic mutations in 560 breast cancer whole-genome sequences. Nature 2016, 534, 47–54. [Google Scholar] [CrossRef]
- Smida, J.; Baumhoer, D.; Rosemann, M.; Walch, A.; Bielack, S.; Poremba, C.; Remberger, K.; Korsching, E.; Scheurlen, W.; Dierkes, C.; et al. Genomic Alterations and Allelic Imbalances Are Strong Prognostic Predictors in Osteosarcoma. Clin. Cancer Res. 2010, 16, 4256–4267. [Google Scholar] [CrossRef]
- Amary, M.F.; Bacsi, K.; Maggiani, F.; Damato, S.; Halai, D.; Berisha, F.; Pollock, R.; O'Donnell, P.; Grigoriadis, A.; Diss, T.; et al. IDH1 and IDH2 mutations are frequent events in central chondrosarcoma and central and periosteal chondromas but not in other mesenchymal tumours. J. Pathol. 2011, 224, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Zöllner, S.K.; Amatruda, J.F.; Bauer, S.; Collaud, S.; de Álava, E.; DuBois, S.G.; Hardes, J.; Hartmann, W.; Kovar, H.; Metzler, M.; et al. Ewing Sarcoma—Diagnosis, Treatment, Clinical Challenges and Future Perspectives. J. Clin. Med. 2021, 10, 1685. [Google Scholar] [CrossRef] [PubMed]
- Suehara, Y.; Alex, D.; Bowman, A.; Middha, S.; Zehir, A.; Chakravarty, D.; Wang, L.; Jour, G.; Nafa, K.; Hayashi, T.; et al. Clinical Genomic Sequencing of Pediatric and Adult Osteosarcoma Reveals Distinct Molecular Subsets with Potentially Targetable Alterations. Clin. Cancer Res. 2019, 25, 6346–6356. [Google Scholar] [CrossRef]
- Baumhoer, D.; Hench, J.; Amary, F. Recent advances in molecular profiling of bone and soft tissue tumors. Skelet. Radiol. 2024, 53, 1925–1936. [Google Scholar] [CrossRef]
- Lam, S.W.; van Ijzendoorn, D.G.; Cleton-Jansen, A.-M.; Szuhai, K.; Bovée, J.V. Molecular Pathology of Bone Tumors. J. Mol. Diagn. 2019, 21, 171–182. [Google Scholar] [CrossRef]
- Baumhoer, D.; Amary, F.; Flanagan, A.M. An update of molecular pathology of bone tumors. Lessons learned from investigating samples by next generation sequencing. Genes, Chromosom. Cancer 2018, 58, 88–99. [Google Scholar] [CrossRef]
- Moonmuang, S.; Chaiyawat, P.; Jantrapirom, S.; Pruksakorn, D.; Piccolo, L.L. Circulating Long Non-Coding RNAs as Novel Potential Biomarkers for Osteogenic Sarcoma. Cancers 2021, 13, 4214. [Google Scholar] [CrossRef]
- Dey, M.; Skipar, P.; Bartnik, E.; Piątkowski, J.; Sulejczak, D.; Czarnecka, A.M. MicroRNA signatures in osteosarcoma: diagnostic insights and therapeutic prospects. Mol. Cell. Biochem. 2024, 480, 2065–2075. [Google Scholar] [CrossRef]
- Wang, C.; Ren, M.; Zhao, X.; Wang, A.; Wang, J. Emerging Roles of Circular RNAs in Osteosarcoma. Med Sci. Monit. 2018, 24, 7043–7050. [Google Scholar] [CrossRef]
- Araki, Y.; Asano, N.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Miwa, S.; Igarashi, K.; Higuchi, T.; Abe, K.; Taniguchi, Y.; et al. A validation study for the utility of serum microRNA as a diagnostic and prognostic marker in patients with osteosarcoma. Oncol. Lett. 2023, 25, 1–15. [Google Scholar] [CrossRef]
- The ENCODE Project Consortium. An Integrated Encyclopedia of DNA Elements in the Human Genome. Nature 2012, 489, 57–74. [Google Scholar] [CrossRef] [PubMed]
- Beermann, J.; Piccoli, M.-T.; Viereck, J.; Thum, T. Non-coding RNAs in Development and Disease: Background, Mechanisms, and Therapeutic Approaches. Physiol. Rev. 2016, 96, 1297–1325. [Google Scholar] [CrossRef] [PubMed]
- Amaral, P.; Carbonell-Sala, S.; De La Vega, F.M.; Faial, T.; Frankish, A.; Gingeras, T.; Guigo, R.; Harrow, J.L.; Hatzigeorgiou, A.G.; Johnson, R.; et al. The status of the human gene catalogue. Nature 2023, 622, 41–47. [Google Scholar] [CrossRef]
- Mattick, J.S.; Makunin, I.V. Non-coding RNA. Hum. Mol. Genet. 2006, 15, R17–R29. [Google Scholar] [CrossRef]
- Srivastava, M.; Simakov, O.; Chapman, J.; Fahey, B.; Gauthier, M.E.A.; Mitros, T.; Richards, G.S.; Conaco, C.; Dacre, M.; Hellsten, U.; et al. The Amphimedon queenslandica genome and the evolution of animal complexity. Nature 2010, 466, 720–726. [Google Scholar] [CrossRef]
- Slack, F.J. Regulatory RNAs and the demise of 'junk' DNA. Genome Biol. 2006, 7, 328–328. [Google Scholar] [CrossRef]
- Willingham, A.T.; Gingeras, T.R. TUF Love for “Junk” DNA. Cell 2006, 125, 1215–1220. [Google Scholar] [CrossRef]
- Ling, H.; Vincent, K.; Pichler, M.; Fodde, R.; Berindan-Neagoe, I.; Slack, F.J.; Calin, G.A. Junk DNA and the long non-coding RNA twist in cancer genetics. Oncogene 2015, 34, 5003–5011. [Google Scholar] [CrossRef]
- Zuckerkandl, E. Revisiting junk DNA. J. Mol. Evol. 1992, 34, 259–271. [Google Scholar] [CrossRef]
- Mattick, J.S. A Kuhnian revolution in molecular biology: Most genes in complex organisms express regulatory RNAs. BioEssays 2023, 45, e2300080. [Google Scholar] [CrossRef]
- Cech, T.R.; Steitz, J.A. The Noncoding RNA Revolution—Trashing Old Rules to Forge New Ones. Cell 2014, 157, 77–94. [Google Scholar] [CrossRef] [PubMed]
- Mattick, JS. Non-coding RNAs : the architects of eukaryotic complexity 2001; 2:986–91.
- Yang, J.X.; Rastetter, R.H.; Wilhelm, D. Non-coding RNAs: An introduction. Adv. Exp. Med. Biol. 2016; 886, 13–32. [Google Scholar] [CrossRef]
- Taft, R.J.; Pheasant, M.; Mattick, J.S. The relationship between non-protein-coding DNA and eukaryotic complexity. BioEssays 2007, 29, 288–299. [Google Scholar] [CrossRef] [PubMed]
- Morris, K.V.; Mattick, J.S. The rise of regulatory RNA. Nat. Rev. Genet. 2014, 15, 423–437. [Google Scholar] [CrossRef] [PubMed]
- Mattick, J.S. The central role of RNA in human development and cognition. FEBS Lett. 2011, 585, 1600–1616. [Google Scholar] [CrossRef]
- Gaiti, F.; Calcino, A.D.; Tanurdžić, M.; Degnan, B.M. Origin and evolution of the metazoan non-coding regulatory genome. Dev. Biol. 2017, 427, 193–202. [Google Scholar] [CrossRef]
- Graveley, BR. Alternative splicing: increasing diversity in the proteomic world 2001; 17:100–7.
- Nurk, S.; Koren, S.; Rhie, A.; Rautiainen, M.; Bzikadze, A.V.; Mikheenko, A.; Vollger, M.R.; Altemose, N.; Uralsky, L.; Gershman, A.; et al. The complete sequence of a human genome. Science 2022, 376, 44–53. [Google Scholar] [CrossRef]
- Mattick, J.S. RNA out of the mist. Trends Genet. 2022, 39, 187–207. [Google Scholar] [CrossRef]
- Taft, R.J.; Pheasant, M.; Mattick, J.S. The relationship between non-protein-coding DNA and eukaryotic complexity. BioEssays 2007, 29, 288–299. [Google Scholar] [CrossRef]
- Bartel, D.P. Metazoan MicroRNAs. Cell 2018, 173, 20–51. [Google Scholar] [CrossRef]
- Liu, G.; Mattick, J.S.; Taft, R.J. A meta-analysis of the genomic and transcriptomic composition of complex life. Cell Cycle 2013, 12, 2061–2072. [Google Scholar] [CrossRef]
- Kim, T.; Croce, C.M. MicroRNA: trends in clinical trials of cancer diagnosis and therapy strategies. Exp. Mol. Med. 2023, 55, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Di Leva, G.; Croce, C.M. miRNA profiling of cancer. Curr. Opin. Genet. Dev. 2013, 23, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Qi, P.; Du, X. The long non-coding RNAs, a new cancer diagnostic and therapeutic gold mine. Mod. Pathol. 2013, 26, 155–165. [Google Scholar] [CrossRef]
- Ha, M.; Kim, V.N. Regulation of microRNA biogenesis. Nat. Rev. Mol. Cell Biol. 2014, 15, 509–524. [Google Scholar] [CrossRef]
- Castel, S.E.; Martienssen, R.A. RNA interference in the nucleus: roles for small RNAs in transcription, epigenetics and beyond. Nat. Rev. Genet. 2013, 14, 100–112. [Google Scholar] [CrossRef]
- Tétreault, N.; De Guire, V. miRNAs: Their discovery, biogenesis and mechanism of action. Clin. Biochem. 2013, 46, 842–845. [Google Scholar] [CrossRef]
- Chung, C.H.; Bernard, P.S.; Perou, C.M. Molecular portraits and the family tree of cancer. Nat. Genet. 2002, 32, 533–540. [Google Scholar] [CrossRef]
- Cohen, R.L.; Settleman, J. From Cancer Genomics to Precision Oncology—Tissue’s Still an Issue. Cell 2014, 157, 1509–1514. [Google Scholar] [CrossRef]
- Bianchi, J.J.; Zhao, X.; Mays, J.C.; Davoli, T. Not all cancers are created equal: Tissue specificity in cancer genes and pathways. Curr. Opin. Cell Biol. 2020, 63, 135–143. [Google Scholar] [CrossRef]
- Hoadley, K.A.; Yau, C.; Hinoue, T.; Wolf, D.M.; Lazar, A.J.; Drill, E.; Shen, R.; Taylor, A.M.; Cherniack, A.D.; Thorsson, V.; et al. Cell-of-Origin Patterns Dominate the Molecular Classification of 10,000 Tumors from 33 Types of Cancer. Cell 2018, 173, 291–304.e296. [Google Scholar] [CrossRef]
- Mansinho, A.; Fernandes, R.M.; Carneiro, A.V. Histology-Agnostic Drugs: A Paradigm Shift—A Narrative Review. Adv. Ther. 2022, 40, 1379–1392. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.; Wang, Q.; Wang, L.; Zhao, X.; Feng, G. Digitalization and third-party logistics performance: Exploring the roles of customer collaboration and government. International Journal of Physical Distribution & Logistics Management 2023, 53, 467–488. [Google Scholar]
- Gaiti, F.; Fernandez-Valverde, S.L.; Nakanishi, N.; Calcino, A.D.; Yanai, I.; Tanurdzic, M.; Degnan, B.M. Dynamic and Widespread lncRNA Expression in a Sponge and the Origin of Animal Complexity. Mol. Biol. Evol. 2015, 32, 2367–2382. [Google Scholar] [CrossRef]
- Condrat, C.E.; Thompson, D.C.; Barbu, M.G.; Bugnar, O.L.; Boboc, A.; Cretoiu, D.; Suciu, N.; Cretoiu, S.M.; Voinea, S.C. miRNAs as Biomarkers in Disease: Latest Findings Regarding Their Role in Diagnosis and Prognosis. Cells 2020, 9, 276. [Google Scholar] [CrossRef]
- Ludwig, N.; Leidinger, P.; Becker, K.; Backes, C.; Fehlmann, T.; Pallasch, C.; Rheinheimer, S.; Meder, B.; Stähler, C.; Meese, E.; et al. Distribution of miRNA expression across human tissues. Nucleic Acids Res. 2016, 44, 3865–3877. [Google Scholar] [CrossRef]
- Shademan, B.; Karamad, V.; Nourazarian, A.; Masjedi, S.; Isazadeh, A.; Sogutlu, F.; Avcı, C.B. MicroRNAs as Targets for Cancer Diagnosis: Interests and Limitations. Adv. Pharm. Bull. 2022, 13, 435–445. [Google Scholar] [CrossRef]
- Slack, F.J.; Chinnaiyan, A.M. The Role of Non-coding RNAs in Oncology. Cell 2019, 179, 1033–1055. [Google Scholar] [CrossRef]
- Anastasiadou, E.; Jacob, L.S.; Slack, F.J. Non-coding RNA networks in cancer. Nat. Rev. Cancer 2018, 18, 5–18. [Google Scholar] [CrossRef]
- Anastasiadou, E.; Faggioni, A.; Trivedi, P.; Slack, F.J. The Nefarious Nexus of Noncoding RNAs in Cancer. Int. J. Mol. Sci. 2018, 19, 2072. [Google Scholar] [CrossRef]
- Wang, H.; Peng, R.; Wang, J.; Qin, Z.; Xue, L. Circulating microRNAs as potential cancer biomarkers: the advantage and disadvantage. Clin. Epigenetics 2018, 10, 1–10. [Google Scholar] [CrossRef]
- Chen, X.; Liang, H.; Zhang, J.; Zen, K.; Zhang, C.-Y. Horizontal transfer of microRNAs: molecular mechanisms and clinical applications. Protein Cell 2012, 3, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Shyamala, K.; Girish, H.; Murgod, S. Risk of tumor cell seeding through biopsy and aspiration cytology. J. Int. Soc. Prev. Community Dent. 2014, 4, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Kołat, D.; Hammouz, R.; Bednarek, A.K.; Płuciennik, E. Exosomes as carriers transporting long non-coding RNAs: Molecular characteristics and their function in cancer (Review). Mol. Med. Rep. 2019, 20, 851–862. [Google Scholar] [CrossRef]
- Behulová, R.L.; Bugalová, A.; Bugala, J.; Struhárňanská, E.; Šafranek, M.; Juráš, I. Circulating Exosomal miRNAs as a Promising Diagnostic Biomarker in Cancer. Physiol. Res. 2023, 72, S193–S207. [Google Scholar] [CrossRef]
- Chen, M.; Zhao, H. Next-generation sequencing in liquid biopsy: cancer screening and early detection. Hum. Genom. 2019, 13, 34. [Google Scholar] [CrossRef]
- Kwapisz, D. The first liquid biopsy test approved. Is it a new era of mutation testing for non-small cell lung cancer? Ann. Transl. Med. 2017, 5, 46–46. [Google Scholar] [CrossRef]
- Tétreault, N.; De Guire, V. miRNAs: Their discovery, biogenesis and mechanism of action. Clin. Biochem. 2013, 46, 842–845. [Google Scholar] [CrossRef]
- Kim, T.; Croce, C.M. MicroRNA: trends in clinical trials of cancer diagnosis and therapy strategies. Exp. Mol. Med. 2023, 55, 1314–1321. [Google Scholar] [CrossRef]
- Bartels, C.L.; Tsongalis, G.J. MicroRNAs: Novel Biomarkers for Human Cancer. Clin. Chem. 2009, 55, 623–631. [Google Scholar] [CrossRef]
- Lu, J.; Getz, G.; Miska, E.A.; Alvarez-Saavedra, E.; Lamb, J.; Peck, D.; Sweet-Cordero, A.; Ebert, B.L.; Mak, R.H.; Ferrando, A.A.; et al. MicroRNA expression profiles classify human cancers. Nature 2005, 435, 834–838. [Google Scholar] [CrossRef]
- Crim, J.; Layfield, L.J. Bone and soft tissue tumors at the borderlands of malignancy. Skelet. Radiol. 2022, 52, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarek, E.; Pyman, B.; Nanayakkara, J.; Tuschl, T.; Tyryshkin, K.; Renwick, N.; Mousavi, P. Discriminating Neoplastic from Nonneoplastic Tissues Using an miRNA-Based Deep Cancer Classifier. Am. J. Pathol. 2022, 192, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Kopp, F.; Mendell, J.T. Functional Classification and Experimental Dissection of Long Noncoding RNAs. Cell 2018, 172, 393–407. [Google Scholar] [CrossRef] [PubMed]
- Mattick, J.S. The State of Long Non-Coding RNA Biology. Non-Coding RNA 2018, 4, 17. [Google Scholar] [CrossRef]
- Clark, M.B.; Mattick, J.S. Long noncoding RNAs in cell biology. Semin. Cell Dev. Biol. 2011, 22, 366–376. [Google Scholar] [CrossRef]
- Chi, Y.; Wang, D.; Wang, J.; Yu, W.; Yang, J. Long Non-Coding RNA in the Pathogenesis of Cancers. Cells 2019, 8, 1015. [Google Scholar] [CrossRef]
- Iyer, M.K.; Niknafs, Y.S.; Malik, R.; Singhal, U.; Sahu, A.; Hosono, Y.; Barrette, T.R.; Prensner, J.R.; Evans, J.R.; Zhao, S.; et al. The landscape of long noncoding RNAs in the human transcriptome. Nat. Genet. 2015, 47, 199–208. [Google Scholar] [CrossRef]
- Wei, G.; Zhu, J.; Hu, H.-B.; Liu, J.-Q. Circular RNAs: Promising biomarkers for cancer diagnosis and prognosis. Gene 2021, 771, 145365. [Google Scholar] [CrossRef]
- Pisignano, G.; Michael, D.C.; Visal, T.H.; Pirlog, R.; Ladomery, M.; Calin, G.A. Going circular: history, present, and future of circRNAs in cancer. Oncogene 2023, 42, 2783–2800. [Google Scholar] [CrossRef]
- Zhang, H.; Shen, Y.; Li, Z.; Ruan, Y.; Li, T.; Xiao, B.; Sun, W. The biogenesis and biological functions of circular RNAs and their molecular diagnostic values in cancers. J. Clin. Lab. Anal. 2019, 34, e23049. [Google Scholar] [CrossRef]
- Xian, J.; Su, W.; Liu, L.; Rao, B.; Lin, M.; Feng, Y.; Qiu, F.; Chen, J.; Zhou, Q.; Zhao, Z.; et al. Identification of Three Circular RNA Cargoes in Serum Exosomes as Diagnostic Biomarkers of Non–Small-Cell Lung Cancer in the Chinese Population. J. Mol. Diagn. 2020, 22, 1096–1108. [Google Scholar] [CrossRef] [PubMed]
- Pan, B.; Qin, J.; Liu, X.; He, B.; Wang, X.; Pan, Y.; Sun, H.; Xu, T.; Xu, M.; Chen, X.; et al. Identification of Serum Exosomal hsa-circ-0004771 as a Novel Diagnostic Biomarker of Colorectal Cancer. Front. Genet. 2019, 10, 1096. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Xiao, Y.; Ma, J.; Tang, Y.; Tian, B.; Zhang, Y.; Li, X.; Wu, Z.; Yang, D.; Zhou, Y.; et al. Circular RNAs in Cancer: emerging functions in hallmarks, stemness, resistance and roles as potential biomarkers. Mol. Cancer 2019, 18, 1–17. [Google Scholar] [CrossRef]
- Zhang, L.; Yang, M.; Mayer, T.; Johnstone, B.; Les, C.; Frisch, N.; Parsons, T.; Mi, Q.-S.; Gibson, G. Use of MicroRNA biomarkers to distinguish enchondroma from low-grade chondrosarcoma. Connect. Tissue Res. 2016, 58, 155–161. [Google Scholar] [CrossRef]
- Stella, M.; Russo, G.I.; Leonardi, R.; Carcò, D.; Gattuso, G.; Falzone, L.; Ferrara, C.; Caponnetto, A.; Battaglia, R.; Libra, M.; et al. Extracellular RNAs from Whole Urine to Distinguish Prostate Cancer from Benign Prostatic Hyperplasia. Int. J. Mol. Sci. 2024, 25, 10079. [Google Scholar] [CrossRef]
- Bielak, C.; Arya, A.; Savill, S. Circulating microRNA as potential diagnostic and prognostic biomarkers of well-differentiated thyroid cancer: A review article. Cancer Biomarkers 2023, 36, 193–205. [Google Scholar] [CrossRef]
- Sadeghi, H.; Kamal, A.; Ahmadi, M.; Najafi, H.; Zarchi, A.S.; Haddad, P.; Shayestehpour, B.; Kamkar, L.; Salamati, M.; Geranpayeh, L.; et al. A novel panel of blood-based microRNAs capable of discrimination between benign breast disease and breast cancer at early stages. RNA Biol. 2021, 18, 747–756. [Google Scholar] [CrossRef]
- Khadka, V.S.; Nasu, M.; Deng, Y.; Jijiwa, M. Circulating microRNA Biomarker for Detecting Breast Cancer in High-Risk Benign Breast Tumors. Int. J. Mol. Sci. 2023, 24, 7553. [Google Scholar] [CrossRef]
- Burenina, O.Y.; Lazarevich, N.L.; Kustova, I.F.; Shavochkina, D.A.; Moroz, E.A.; Kudashkin, N.E.; Patyutko, Y.I.; Metelin, A.V.; Kim, E.F.; Skvortsov, D.A.; et al. Panel of potential lncRNA biomarkers can distinguish various types of liver malignant and benign tumors. J. Cancer Res. Clin. Oncol. 2020, 147, 49–59. [Google Scholar] [CrossRef]
- Marqués, M.; Pont, M.; Hidalgo, I.; Sorolla, M.A.; Parisi, E.; Salud, A.; Sorolla, A.; Porcel, J.M. MicroRNAs Present in Malignant Pleural Fluid Increase the Migration of Normal Mesothelial Cells In Vitro and May Help Discriminate between Benign and Malignant Effusions. Int. J. Mol. Sci. 2023, 24, 14022. [Google Scholar] [CrossRef]
- Dolivet, E.; Gaichies, L.; Jeanne, C.; Bazille, C.; Briand, M.; Vernon, M.; Giffard, F.; Leprêtre, F.; Poulain, L.; Denoyelle, C.; et al. Synergy of the microRNA Ratio as a Promising Diagnosis Biomarker for Mucinous Borderline and Malignant Ovarian Tumors. Int. J. Mol. Sci. 2023, 24, 16016. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, K.J.; Helwig, J.; Bertram, S.; Sheu, S.Y.; Suttorp, A.C.; Seggewiß, J.; Willscher, E.; Walz, M.K.; Worm, K.; Schmid, K.W. Differential expression of microRNA-675, microRNA-139-3p and microRNA-335 in benign and malignant adrenocortical tumours. J. Clin. Pathol. 2011, 64, 529–535. [Google Scholar] [CrossRef] [PubMed]
- Hecker-Nolting, S.; Baumhoer, D.; Blattmann, C.; Kager, L.; Kühne, T.; Kevric, M.; Lang, S.; Mettmann, V.; Sorg, B.; Werner, M.; et al. Osteosarcoma pre-diagnosed as another tumor: a report from the Cooperative Osteosarcoma Study Group (COSS). J. Cancer Res. Clin. Oncol. 2022, 149, 1961–1967. [Google Scholar] [CrossRef] [PubMed]
- Suster, D.; Mackinnon, A.C.; Jarzembowski, J.A.; Carrera, G.; Suster, S.; Klein, M.J. Epithelioid osteoblastoma. Clinicopathologic and immunohistochemical study of 17 cases. Hum. Pathol. 2022, 125, 68–78. [Google Scholar] [CrossRef]
- Gambarotti, M.; Tos, A.P.D.; Vanel, D.; Picci, P.; Gibertoni, D.; Klein, M.J.; Righi, A. Osteoblastoma-like osteosarcoma: high-grade or low-grade osteosarcoma? Histopathology 2018, 74, 494–503. [Google Scholar] [CrossRef]
- Fittall, M.W.; Mifsud, W.; Pillay, N.; Ye, H.; Strobl, A.-C.; Verfaillie, A.; Demeulemeester, J.; Zhang, L.; Berisha, F.; Tarabichi, M.; et al. Recurrent rearrangements of FOS and FOSB define osteoblastoma. Nat. Commun. 2018, 9, 1–6. [Google Scholar] [CrossRef]
- Lam, S.W.; Cleven, A.H.G.; Kroon, H.M.; Bruijn, I.H.B.-D.; Szuhai, K.; Bovée, J.V.M.G. Utility of FOS as diagnostic marker for osteoid osteoma and osteoblastoma. Virchows Arch. 2019, 476, 455–463. [Google Scholar] [CrossRef]
- Amary, F.; Markert, E.; Berisha, F.; Ye, H.; Gerrand, C.; Cool, P.; Tirabosco, R.; Lindsay, D.; Pillay, N.; O’donnell, P.; et al. FOS Expression in Osteoid Osteoma and Osteoblastoma. Am. J. Surg. Pathol. 2019, 43, 1661–1667. [Google Scholar] [CrossRef]
- Ameline, B.; Nathrath, M.; Nord, K.H.; de Flon, F.H.; Bovée, J.V.; Krieg, A.H.; Höller, S.; Hench, J.; Baumhoer, D. Methylation and copy number profiling: emerging tools to differentiate osteoblastoma from malignant mimics? Mod. Pathol. 2022, 35, 1204–1211. [Google Scholar] [CrossRef]
- Riester, S.M.; Torres-Mora, J.; Dudakovic, A.; Camilleri, E.T.; Wang, W.; Xu, F.; Thaler, R.R.; Evans, J.M.; Zwartbol, R.; Bruijn, I.H.B.-D.; et al. Hypoxia-related microRNA-210 is a diagnostic marker for discriminating osteoblastoma and osteosarcoma. J. Orthop. Res. 2016, 35, 1137–1146. [Google Scholar] [CrossRef]
- Palmini, G.; Brandi, M.L. microRNAs and bone tumours: Role of tiny molecules in the development and progression of chondrosarcoma, of giant cell tumour of bone and of Ewing's sarcoma. Bone 2021, 149, 115968. [Google Scholar] [CrossRef] [PubMed]
- Jiang, P.; Li, Y.; Yang, X.; Zhou, J.; Wei, P. Clinical Value of Differential lncRNA Expressions in Diagnosis of Giant Cell Tumor of Bone and Tumor Recurrence. Clin. Lab. 2020, 66, 1381–1389. [Google Scholar] [CrossRef] [PubMed]
- Qin, S.; He, N.; Yan, H.; Dong, Y. Characterization of MicroRNA Expression Profiles in Patients with Giant Cell Tumor. Orthop. Surg. 2016, 8, 212–219. [Google Scholar] [CrossRef]
- Lian, K.; Chen, Z.; Chen, L.; Li, Y.; Liu, L. Network study of miRNA regulating traumatic heterotopic ossification. PLOS ONE 2025, 20, e0318779. [Google Scholar] [CrossRef]
- Mierzejewski, B.; Pulik, Ł.; Grabowska, I.; Sibilska, A.; Ciemerych, M.A.; Łęgosz, P.; Brzoska, E. Coding and noncoding RNA profile of human heterotopic ossifications - Risk factors and biomarkers. Bone 2023, 176, 116883. [Google Scholar] [CrossRef]
- Araki, Y.; Asano, N.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Miwa, S.; Igarashi, K.; Higuchi, T.; Abe, K.; Taniguchi, Y.; et al. A validation study for the utility of serum microRNA as a diagnostic and prognostic marker in patients with osteosarcoma. Oncol. Lett. 2023, 25, 1–15. [Google Scholar] [CrossRef]
- Luo, H.; Ye, Z. Identification of Serum miR-337-3p, miR-484, miR-582, and miR-3677 as Promising Biomarkers for Osteosarcoma. Clin. Lab. 2021, 67, 912–921. [Google Scholar] [CrossRef]
- Yang, L.; Li, H.; Huang, A. MiR-429 and MiR-143-3p Function as Diagnostic and Prognostic Markers for Osteosarcoma. Clin. Lab. 2020, 66, 1945–1950. [Google Scholar] [CrossRef]
- Lei, S.; Xiang, L. Up-Regulation of circRNA hsa_circ_0003074 Expression is a Reliable Diagnostic and Prognostic Biomarker in Patients with Osteosarcoma. Cancer Manag. Res. 2020, 12, 9315–9325. [Google Scholar] [CrossRef]
- Yao, Z.-S.; Li, C.; Liang, D.; Jiang, X.-B.; Tang, J.-J.; Ye, L.-Q.; Yuan, K.; Ren, H.; Yang, Z.-D.; Jin, D.-X.; et al. Diagnostic and prognostic implications of serum miR-101 in osteosarcoma. Cancer Biomarkers 2018, 22, 127–133. [Google Scholar] [CrossRef]
- Cong, C.; Wang, W.; Tian, J.; Gao, T.; Zheng, W.; Zhou, C. Identification of serum miR-124 as a biomarker for diagnosis and prognosis in osteosarcoma. Cancer Biomarkers 2018, 21, 449–454. [Google Scholar] [CrossRef] [PubMed]
- Niu, J.; Sun, Y.; Guo, Q.; Niu, D.; Liu, B. Serum miR-95-3p is a diagnostic and prognostic marker for osteosarcoma. SpringerPlus 2016, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Liu, Y.; Liao, W.; Liu, R.; Shi, P.; Wang, L. miRNA-223 is a potential diagnostic and prognostic marker for osteosarcoma. J. Bone Oncol. 2016, 5, 74–79. [Google Scholar] [CrossRef]
- Lian, F.; Cui, Y.; Zhou, C.; Gao, K.; Wu, L. Identification of a Plasma Four-microRNA Panel as Potential Noninvasive Biomarker for Osteosarcoma. PLOS ONE 2015, 10, e0121499–e0121499. [Google Scholar] [CrossRef]
- Yang, Z.; Zhang, Y.; Zhang, X.; Zhang, M.; Liu, H.; Zhang, S.; Qi, B.; Sun, X. Serum microRNA-221 functions as a potential diagnostic and prognostic marker for patients with osteosarcoma. Biomed. Pharmacother. 2015, 75, 153–158. [Google Scholar] [CrossRef]
- Rosen G, Caparros B, Huvos AG, Kosloff C, Nirenberg A, Cacavio A, et al. Preoperative chemotherapy for osteogenic sarcoma: Selection of postoperative adjuvant chemotherapy based on the response of the primary tumor to preoperative chemotherapy. Cancer 1982; 49:1221–30. [CrossRef]
- Glasser DB, Lane JM, Huvos AG, Marcove RC, Rosen G. Survival, prognosis, and therapeutic response in osteogenic sarcoma. The memorial hospital experience. Cancer 1992; 69:698–708. [CrossRef]
- Davis, A.M.; Bell, R.S.; Goodwin, P. Prognostic factors in osteosarcoma: A critical review. J. Clin. Oncol. 1994, 12, 423–431. [Google Scholar] [CrossRef]
- O’kane, G.M.; A Cadoo, K.; Walsh, E.M.; Emerson, R.; Dervan, P.; O’keane, C.; Hurson, B.; O’toole, G.; Dudeney, S.; Kavanagh, E.; et al. Perioperative chemotherapy in the treatment of osteosarcoma: a 26-year single institution review. Clin. Sarcoma Res. 2015, 5, 1–8. [Google Scholar] [CrossRef]
- Ho, D.J.; Agaram, N.P.; Jean, M.-H.; Suser, S.D.; Chu, C.; Vanderbilt, C.M.; Meyers, P.A.; Wexler, L.H.; Healey, J.H.; Fuchs, T.J.; et al. Deep Learning–Based Objective and Reproducible Osteosarcoma Chemotherapy Response Assessment and Outcome Prediction. Am. J. Pathol. 2022, 193, 341–349. [Google Scholar] [CrossRef]
- Chiappetta, C.; Mancini, M.; Lessi, F.; Aretini, P.; De Gregorio, V.; Puggioni, C.; Carletti, R.; Petrozza, V.; Civita, P.; Franceschi, S.; et al. Whole-exome analysis in osteosarcoma to identify a personalized therapy. Oncotarget 2017, 8, 80416–80428. [Google Scholar] [CrossRef]
- Byun, B.H.; Kong, C.-B.; Lim, I.; Kim, B.I.; Choi, C.W.; Song, W.S.; Cho, W.H.; Jeon, D.-G.; Koh, J.-S.; Lee, S.-Y.; et al. Early response monitoring to neoadjuvant chemotherapy in osteosarcoma using sequential 18 F-FDG PET/CT and MRI. Eur. J. Nucl. Med. 2014, 41, 1553–1562. [Google Scholar] [CrossRef]
- Miwa, S.; Takeuchi, A.; Shirai, T.; Taki, J.; Yamamoto, N.; Nishida, H.; Hayashi, K.; Tanzawa, Y.; Kimura, H.; Igarashi, K.; et al. Prognostic Value of Radiological Response to Chemotherapy in Patients with Osteosarcoma. PLOS ONE 2013, 8, e70015. [Google Scholar] [CrossRef] [PubMed]
- Laux, C.J.; Berzaczy, G.; Weber, M.; Lang, S.; Dominkus, M.; Windhager, R.; Nöbauer-Huhmann, I.-M.; Funovics, P.T. Tumour response of osteosarcoma to neoadjuvant chemotherapy evaluated by magnetic resonance imaging as prognostic factor for outcome. Int. Orthop. 2014, 39, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Cheng, W.-T.; Li, H.; Zhang, Z.; Lu, X.-L.; Deng, S.-S.; Li, J.; Yang, C.-H. Comprehensive Analysis of Key mRNAs and lncRNAs in Osteosarcoma Response to Preoperative Chemotherapy with Prognostic Values. Curr. Med Sci. 2021, 41, 916–929. [Google Scholar] [CrossRef]
- Carrle, D.; Bielack, S.S. Current strategies of chemotherapy in osteosarcoma. Int. Orthop. 2006, 30, 445–451. [Google Scholar] [CrossRef]
- Tsukamoto, S.; Errani, C.; Angelini, A.; Mavrogenis, A.F. Current Treatment Considerations for Osteosarcoma Metastatic at Presentation. Orthopedics 2020, 43, E345–E358. [Google Scholar] [CrossRef]
- Lin, Z.; Xie, X.; Lu, S.; Liu, T. Noncoding RNAs in osteosarcoma: Implications for drug resistance. Cancer Lett. 2021, 504, 91–103. [Google Scholar] [CrossRef]
- Xu, W.; Li, Z.; Zhu, X.; Xu, R.; Xu, Y. miR-29 Family Inhibits Resistance to Methotrexate and Promotes Cell Apoptosis by Targeting COL3A1 and MCL1 in Osteosarcoma. Med Sci. Monit. 2018, 24, 8812–8821. [Google Scholar] [CrossRef]
- Li, G.; Zhu, Y. Effect of lncRNA ANRIL knockdown on proliferation and cisplatin chemoresistance of osteosarcoma cells in vitro. Pathol. - Res. Pr. 2019, 215, 931–938. [Google Scholar] [CrossRef]
- Li, G.; Yan, X. Long non-coding RNA GAS5 promotes cisplatin-chemosensitivity of osteosarcoma cells via microRNA-26b-5p/TP53INP1 axis. J. Orthop. Surg. Res. 2023, 18, 1–12. [Google Scholar] [CrossRef]
- Dong, L.; Qu, F. CircUBAP2 promotes SEMA6D expression to enhance the cisplatin resistance in osteosarcoma through sponging miR-506-3p by activating Wnt/β-catenin signaling pathway. Histochem. J. 2020, 51, 329–340. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhou, Q.; Luo, F.; Zhou, R.; Xu, J.; Xiao, J.; Dai, F.; Song, L. Circular RNA circ-CHI3L1.2 modulates cisplatin resistance of osteosarcoma cells via the miR-340-5p/LPAATβ axis. Hum. Cell 2021, 34, 1558–1568. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Dou, D.; Zhang, T.; Wang, B. HOTAIR Promotes Cisplatin Resistance of Osteosarcoma Cells by Regulating Cell Proliferation, Invasion, and Apoptosis via miR-106a-5p/STAT3 Axis. Cell Transplant. 2020, 29. [Google Scholar] [CrossRef] [PubMed]
- Ling, Z.; Fan, G.; Yao, D.; Zhao, J.; Zhou, Y.; Feng, J.; Zhou, G.; Chen, Y. MicroRNA-150 functions as a tumor suppressor and sensitizes osteosarcoma to doxorubicin-induced apoptosis by targeting RUNX2. Exp. Ther. Med. 2019, 19, 481–488. [Google Scholar] [CrossRef]
- Wang, X.; Ding, R.; Fu, Z.; Yang, M.; Li, D.; Zhou, Y.; Qin, C.; Zhang, W.; Si, L.; Zhang, J.; et al. Overexpression of miR-506-3p reversed doxorubicin resistance in drug-resistant osteosarcoma cells. Front. Pharmacol. 2024, 15, 1303732. [Google Scholar] [CrossRef]
- Bai, Y.; Li, Y.; Bai, J.; Zhang, Y. Hsa_circ_0004674 promotes osteosarcoma doxorubicin resistance by regulating the miR-342-3p/FBN1 axis. J. Orthop. Surg. Res. 2021, 16, 1–12. [Google Scholar] [CrossRef]
- Pei, Y.; Li, S. Unraveling the impact of noncoding RNAs in osteosarcoma drug resistance: a review of mechanisms and therapeutic implications. Int. J. Surg. 2024, 111, 2112–2130. [Google Scholar] [CrossRef]
- He, H.; Ni, J.; Huang, J. Molecular mechanisms of chemoresistance in osteosarcoma (Review). Oncol. Lett. 2014, 7, 1352–1362. [Google Scholar] [CrossRef]
- Hu, S.; Han, X.; Liu, G.; Wang, S. LncRNAs as potential prognosis/diagnosis markers and factors driving drug resistance of osteosarcoma, a review. Front. Endocrinol. 2024, 15, 1415722. [Google Scholar] [CrossRef]
- Chen, H.; Gong, Z.; Zhou, H.; Han, Y. Deciphering chemoresistance in osteosarcoma: Unveiling regulatory mechanisms and function through the lens of noncoding RNA. Drug Dev. Res. 2024, 85, e22167. [Google Scholar] [CrossRef]
- Chen, R.; Wang, G.; Zheng, Y.; Hua, Y.; Cai, Z. Drug resistance-related microRNAs in osteosarcoma: Translating basic evidence into therapeutic strategies. J. Cell. Mol. Med. 2019, 23, 2280–2292. [Google Scholar] [CrossRef]
- Lian, H.B.; Zhou, Y.B.; Sun, Z.B.; Liu, K.B. MicroRNA34a is associated with chemotherapy resistance, metastasis, recurrence, survival, and prognosis in patient with osteosarcoma. Medicine 2022, 101, e30722. [Google Scholar] [CrossRef]
- Diao, Z.-B.; Sun, T.-X.; Zong, Y.; Lin, B.-C.; Xia, Y.-S. Identification of plasma microRNA-22 as a marker for the diagnosis, prognosis, and chemosensitivity prediction of osteosarcoma. J. Int. Med Res. 2020, 48. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Zhao, X.; Zhang, Y.-J.; Fang, G.-W.; Xue, Y. MicroRNA-375 as a potential serum biomarker for the diagnosis, prognosis, and chemosensitivity prediction of osteosarcoma. J. Int. Med Res. 2017, 46, 975–983. [Google Scholar] [CrossRef] [PubMed]
- Rosen, G.; Murphy, M.L.; Huvos, A.G.; Gutierrez, M.; Marcove, R.C. Chemotherapy,en bloc resection, and prosthetic bone replacement in the treatment of osteogenic sarcoma. Cancer 1976, 37, 1–11. [Google Scholar] [CrossRef]
- Anand, S.; Majeti, B.K.; Acevedo, L.M.; A Murphy, E.; Mukthavaram, R.; Scheppke, L.; Huang, M.; Shields, D.J.; Lindquist, J.N.; E Lapinski, P.; et al. MicroRNA-132–mediated loss of p120RasGAP activates the endothelium to facilitate pathological angiogenesis. Nat. Med. 2010, 16, 909–914. [Google Scholar] [CrossRef]
- Zhang, W.; Hu, C.; Zhang, C.; Luo, C.; Zhong, B.; Yu, X. MiRNA-132 regulates the development of osteoarthritis in correlation with the modulation of PTEN/PI3K/AKT signaling. BMC Geriatr. 2021, 21, 1–10. [Google Scholar] [CrossRef]
- Yang, J.; Gao, T.; Tang, J.; Cai, H.; Lin, L.; Fu, S. Loss of microRNA-132 predicts poor prognosis in patients with primary osteosarcoma. Mol. Cell. Biochem. 2013, 381, 9–15. [Google Scholar] [CrossRef]
- Yuan, J.; Chen, L.; Chen, X.; Sun, W.; Zhou, X. Identification of Serum MicroRNA-21 as a Biomarker for Chemosensitivity and Prognosis in Human Osteosarcoma. J. Int. Med Res. 2012, 40, 2090–2097. [Google Scholar] [CrossRef]
- Zhou, H.; Wang, Q.; Wang, L.; Zhao, X.; Feng, G. Digitalization and third-party logistics performance: Exploring the roles of customer collaboration and government. International Journal of Physical Distribution & Logistics Management 2023, 53, 467–488. [Google Scholar]
- Gougelet, A.; Pissaloux, D.; Besse, A.; Perez, J.; Duc, A.; Dutour, A.; Blay, J.; Alberti, L. Micro-RNA profiles in osteosarcoma as a predictive tool for ifosfamide response. Int. J. Cancer 2010, 129, 680–690. [Google Scholar] [CrossRef]
- Hu, Y.; Gu, J.; Shen, H.; Shao, T.; Li, S.; Wang, W.; Yu, Z. Circular RNA LARP4 correlates with decreased Enneking stage, better histological response, and prolonged survival profiles, and it elevates chemosensitivity to cisplatin and doxorubicin via sponging microRNA-424 in osteosarcoma. J. Clin. Lab. Anal. 2019, 34, e23045. [Google Scholar] [CrossRef] [PubMed]
- Roessner, A.; Lohmann, C.; Jechorek, D. Translational cell biology of highly malignant osteosarcoma. Pathol. Int. 2021, 71, 291–303. [Google Scholar] [CrossRef]
- Cui, J.; Dean, D.; Hornicek, F.J.; Chen, Z.; Duan, Z. The role of extracelluar matrix in osteosarcoma progression and metastasis. J. Exp. Clin. Cancer Res. 2020, 39, 1–11. [Google Scholar] [CrossRef]
- Grzywa, T.M.; Klicka, K.; Włodarski, P.K. Regulators at Every Step—How microRNAs Drive Tumor Cell Invasiveness and Metastasis. Cancers 2020, 12, 3709. [Google Scholar] [CrossRef]
- Liu, S.J.; Dang, H.X.; Lim, D.A.; Feng, F.Y.; Maher, C.A. Long noncoding RNAs in cancer metastasis. Nat. Rev. Cancer 2021, 21, 446–460. [Google Scholar] [CrossRef]
- Mosca, N.; Alessio, N.; Di Paola, A.; Marrapodi, M.M.; Galderisi, U.; Russo, A.; Rossi, F.; Potenza, N. Osteosarcoma in a ceRNET perspective. J. Biomed. Sci. 2024, 31, 1–30. [Google Scholar] [CrossRef]
- Abedi, S.; Behmanesh, A.; Mazhar, F.N.; Bagherifard, A.; Sami, S.H.; Heidari, N.; Hossein-Khannazer, N.; Namazifard, S.; Arki, M.K.; Shams, R.; et al. Machine learning and experimental analyses identified miRNA expression models associated with metastatic osteosarcoma. Biochim. et Biophys. Acta (BBA) - Mol. Basis Dis. 2024, 1870, 167357. [Google Scholar] [CrossRef]
- Behulová, R.L.; Bugalová, A.; Bugala, J.; Struhárňanská, E.; Šafranek, M.; Juráš, I. Circulating Exosomal miRNAs as a Promising Diagnostic Biomarker in Cancer. Physiol. Res. 2023, 72, S193–S207. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Y.; Hu, X.; Min, L. The Roles of Exosomes in Metastasis of Sarcoma: From Biomarkers to Therapeutic Targets. Biomolecules 2023, 13, 456. [Google Scholar] [CrossRef]
- Meng, F.; Wang, L.; Gao, G.; Chen, J.; Wang, X.; Wu, G.; Miu, Y. Identification and verification of microRNA signature and key genes in the development of osteosarcoma with lung metastasis. Medicine 2022, 101, e32258. [Google Scholar] [CrossRef]
- Karras, F.S.; Schmidt, C.; Franke, F.; Jechorek, D. Roessner A Integrated Genomic and Epigenetic Analysis of Matched Primary and Metastatic Highly Malignant Osteosarcoma. 2025, in preparation. [Google Scholar] [CrossRef]
Figure 1.
A. Typical osteoblastic osteosarcoma with ample osteoid formation (H&E x200). B. Chondroblastic osteosarcoma (H&E x200) C. Fibroblastic osteosarcoma with typical fibroblast-like spindle cells (H&E x200). D. Giant cell rich osteosarcoma containing abundant osteoclast like giant cells (H&E x200).
Figure 1.
A. Typical osteoblastic osteosarcoma with ample osteoid formation (H&E x200). B. Chondroblastic osteosarcoma (H&E x200) C. Fibroblastic osteosarcoma with typical fibroblast-like spindle cells (H&E x200). D. Giant cell rich osteosarcoma containing abundant osteoclast like giant cells (H&E x200).
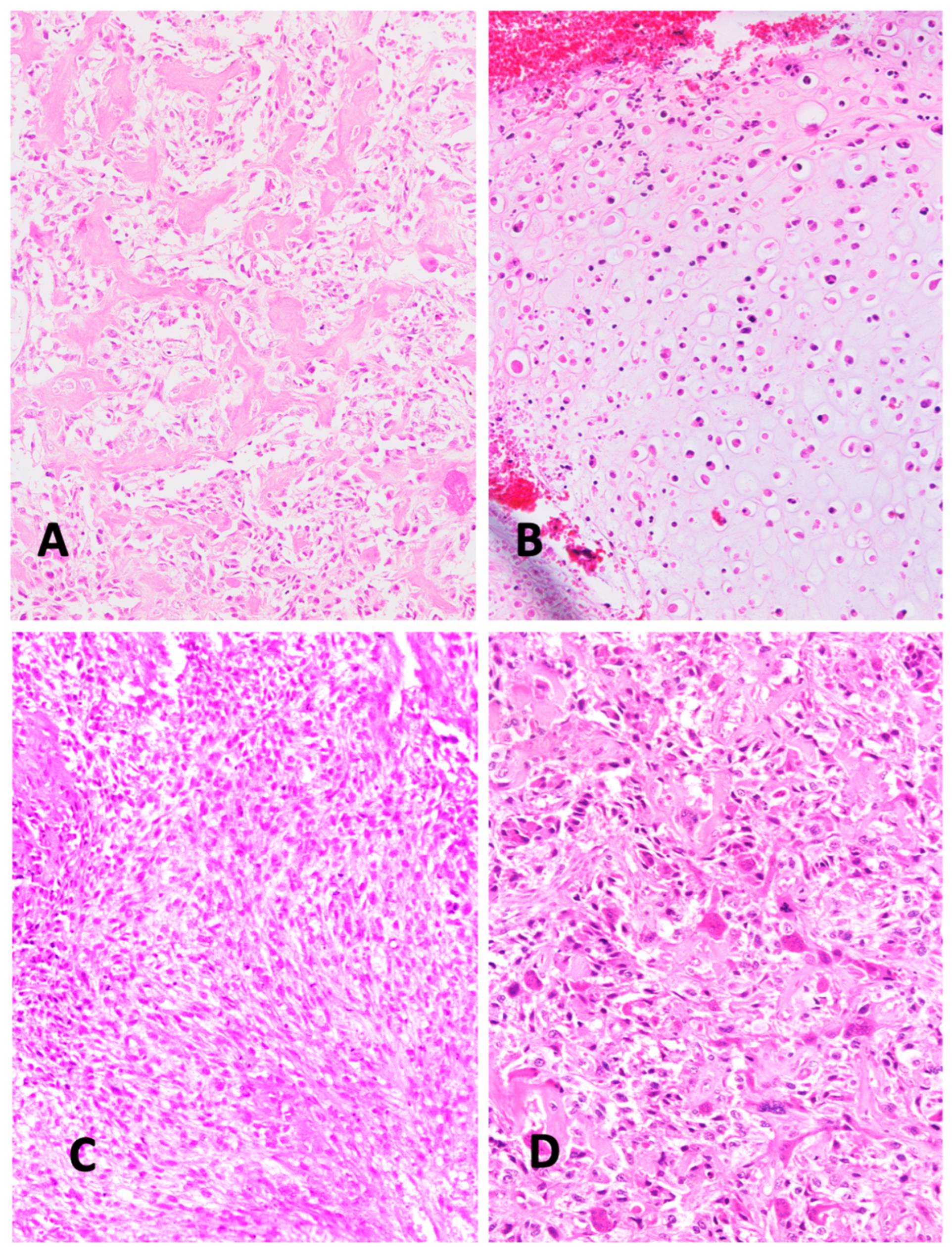
Figure 2.
A. Aggressive osteoblastoma with atypical cellular nuclei (H&E x200). B. Highly malignant osteoblastic osteosarcoma with high nuclear pleomorphism (H&E x200). C. Low grade intramedullary osteosarcoma (H&E x200). D. Heterotopic ossification mimicking osteosarcoma (H&E x200).
Figure 2.
A. Aggressive osteoblastoma with atypical cellular nuclei (H&E x200). B. Highly malignant osteoblastic osteosarcoma with high nuclear pleomorphism (H&E x200). C. Low grade intramedullary osteosarcoma (H&E x200). D. Heterotopic ossification mimicking osteosarcoma (H&E x200).
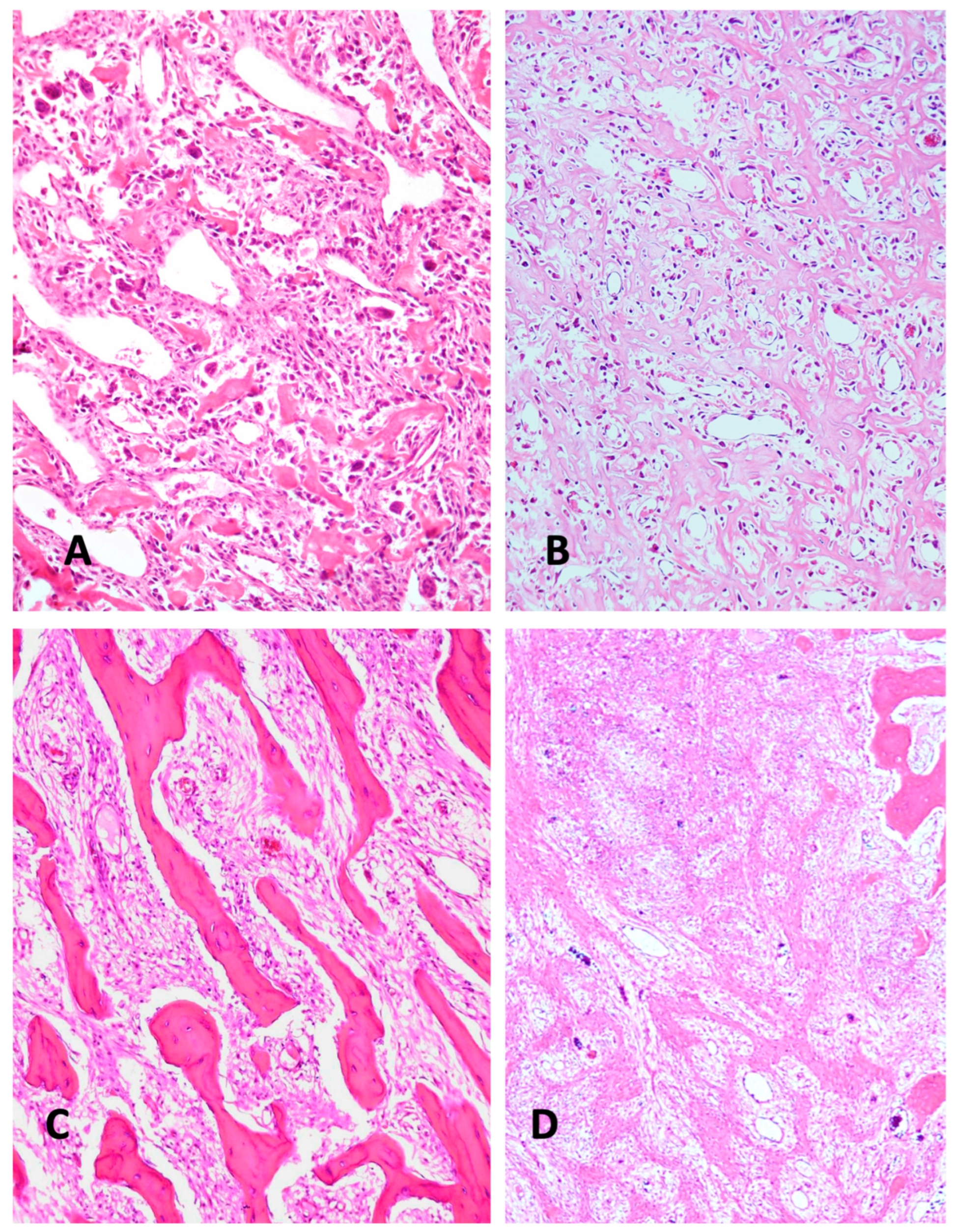
Figure 5.
A. Typical histological appearance of primary of osteoblastic osteosarcoma, no metastases (H&Ex200). B. Primary osteoblastic osteosarcoma with lung metastasis at time of diagnosis (H&E x200). The non-metastasizing and metastasizing malignant tumors appear histologically indistinguishable.
Figure 5.
A. Typical histological appearance of primary of osteoblastic osteosarcoma, no metastases (H&Ex200). B. Primary osteoblastic osteosarcoma with lung metastasis at time of diagnosis (H&E x200). The non-metastasizing and metastasizing malignant tumors appear histologically indistinguishable.

Table 1.
Examples of differentially expressed ncRNAs as diagnostic adjuncts for discriminating benign and malignant lesions in several cancer entities.
Table 1.
Examples of differentially expressed ncRNAs as diagnostic adjuncts for discriminating benign and malignant lesions in several cancer entities.
| Tumor Benign/ Malignant |
ncRNA | Material | Results | Source |
|---|---|---|---|---|
| Enchondroma/Chondrosarcoma | miR-181a and -138 | Tumor tissue FFPE |
Increased expression of miR-181a and -138 in low grade chondrosarcoma compared with enchondroma | Zhang, L. et al. 2017 [108] |
| Benign Hyperplasia (BPH)/ Prostatic Cancer |
miR-27b-3p, miR-574-3p, miR-30a-5p, and miR-125b-5p | Urine | These miRNAs can discriminate between BPH and Prostatic Cancer | Stella et al. [109] |
| Benign Nodules/Thyroid Cancer | miRNA-222 | Serum | Discriminating between thyroid cancer and benign nodules. |
Bielak et al. [110] |
| High risk benign Breast Tumors/ Breast Cancer | miRNAs, hsa-mir-128-3p, hsa-mir-421, hsa-mir-130b-5p, and hsa-mir-28-5p, | Plasma | four miRNAs, hsa-mir-128-3p, hsa-mir-421,has-mir-130b-5p, and hsa-mir-28-5p, were differentially expressed in CA vs. HB and had diagnostic power to discriminate CA from HB | Khadka et al. [112] |
| Benign Breast Disease/ Breast Cancer | miR-106b-5p, −126-3p, −140-3p, −193a-5p, and −10b-5p | Plasma | multi-marker panel consisting of hsa- miR-106b-5p, −126-3p, −140-3p, −193a-5p, and −10b-5p could detect early-stages of BC with 0.79 sensitivity, 0.86 specificity and 0.82 accuracy. |
Sadeghi et al. [111] |
| Benign liver tumors/liver cancer | LincRNA- 01093 lncRNA HELIS |
Serum | LINC01093 and lncRNA HELIS are down-regulated in all malignant liver cancers; in benign tumors LINC01093 expression is just twice decreased in comparison to adjacent tissue samples. |
Burenina et al. [113] |
| Nonneoplastic skin diseases/different skin cancers | miRNA-Based Deep Cancer Classifier miR-375 and miR-451 |
Serum | miR-375 and miR-451 are candidate biomarkers of neoplastic and non neoplastic skin lesions | Kaczmarek et al. [96] |
| Benign and Malignant Effusions | miR-141-3p, miR-203a-3 | Pleural fluid | abundance of three miRNAs miR-141-3p, miR-203a-3, and miR-200c-3p correctly classi- fies malignant pleura effusions |
Marques et al. [114] |
| Malignant borderline tumors/ovarian cancer | miR-30a-3p, miR-30c, miR-30d and miR-30e-3p | Tumor tissue FFPE | Four miRNAs could discriminate mucinous borderline tumors and ovarian cancers |
Dolivet et al. [115] |
| Benign versus malignant adrenocortical tumors | miR-139-3p, miR-335, miR-675 | miRNA profiling of miR-675, and miR-335, and miRNA-139-3p helps in discriminating ACCs from ACAs Adreno-cortical adenomas and carcinomas | Schmitz et al. [116] |
Table 2.
Examples of differentially expressed ncRNAs as diagnostic adjuncts in the differential diagnosis of highly malignant osteosarcoma.
Table 2.
Examples of differentially expressed ncRNAs as diagnostic adjuncts in the differential diagnosis of highly malignant osteosarcoma.
| Tumor Benign/ Malignant |
ncRNA | Material | Results | Source |
|---|---|---|---|---|
| Osteoblastoma/ Osteosarcoma |
miRNA-210 | Tumor tissue FFPE |
miRNA-210 displays low levels of expression across all of the osteoblastoma specimens and high expression in the majority of the osteosarcoma specimens. |
Riester et al. [124] |
| Fibrous dysplasia; giant cell tumor of the bone; osteoblastoma; chondrosarcoma; versus osteosarcoma |
miR-1261 | Serum | patients with osteosarcoma had higher serum miR-1261 levels than those with benign or intermediate-grade bone tumors |
Araki Y et al. 2023 [130] |
Table 3.
ncRNAs for early clinical diagnosis of osteosarcoma.
| Non coding RNA | Materials | Results | Source |
|---|---|---|---|
| miR-1261 | Serum | Higher miRNA serum levels point to a bone tumor of high-grade malignancy. | Araki A et al. [130] |
| miR-337-3p, miR-484, miR-582, miR-3677 | Serum | These miRNAs were decreased in serum of osteosarcoma patients | Luo, H et al. [131] |
| MiR-429 and MiR-143-3p | Serum | MiR-429 and miR-143-3p expression were significantly down-regulated in the serum from OS patients. | Yang, L et al. [132] |
| circRNA hsa_circ_0003074 | Serum | hsa_circ_0003074 is highly expressed and peripheral blood of osteosarcoma patients. . |
Lei, S et al. [133] |
| miR-101 | Serum | miR-101 expression levels were under-expressed in serum samples from osteo-sarcoma patients compared to controls. | Yao, ZS et al. [134] |
| miR-124 | Serum | The level of serum miR-124 was decreased in osteosarcoma patients when compared to healthy controls. | Cong, C et al. [135] |
| miR-95-3p | Serum | Compared to healthy controls, the expression levels of miR-95-3p in serum of osteosarcoma patients was signifi-cantly decreased. |
Niu, J et al. [136] |
| miRNA-223 | Serum | The expression of miR-223 was significantly decreased in the serum of osteosarcoma patients compared to healthy controls. | Dong, J et al. [137] |
| miR-195-5p, miR-199a-3p, miR-320a and miR-374a-5p | Plasma | Were significantly increased in the osteosarcoma patients and markedly decreased in the plasma after operation. | Lian F et al. [138] |
| microRNA-221 | Serum; Fresh frozen tissue |
The expression levels of miR-221 in osteosar-coma tissues and sera were both upregulated. | Yang, Z et al. [139] |
Table 5.
Non coding RNAs with potential as predictors of hematogenic metastasis development of osteosarcoma patients.
Table 5.
Non coding RNAs with potential as predictors of hematogenic metastasis development of osteosarcoma patients.
| Non coding RNA | Materials | Results | Source |
|---|---|---|---|
| miR-34c-3p and miR-154-3p | Sarcoma tissue, FFPE | The combined values of miR-34c-3p and miR-154-3p showed 90 % diagnostic power for osteosarcoma samples and 85 % for metastatic osteosarcoma. | Abedi, S. et al. [183] |
| miR-675 miR-1307 miR-25-3p |
Serum and plasma | Osteosarcoma-derived exosomal biomarkers, including miRNAs, and lnc-RNAs, reveal diagnostic value and the potential of predicting prognosis for osteosarcoma metastasis. |
Tan, L. et al. [185] |
| miR-34a | Serum | Elevated serum levels of miR-34a were associated with a reduced incidence of metastasis in OS patients. |
Lian, H. et al. [167] |
| miR-506 | Sarcoma tissue, FFPE | microRNA-506 was differentially expressed between osteosarcoma tissues with lung metastasis and non-metastatic tumor tissue. | Meng, F. et al. [186] |
| miR-98-3p; miR-134-3p; miR-378C; miR-516A-5p; miR-548A-3p; miR-606; miR-650; miR-802; miR-1233-3p; miR-1271-3p; miR-3158-3p |
Sarcoma tissue, FFPE | The most differential expressed miRNAs (highly significantly) were observed between the non-metastasizing OS and the metastasizing primary OS | Karras, F. in preparation [187] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



