Submitted:
05 May 2025
Posted:
06 May 2025
You are already at the latest version
Abstract
Endometriosis is a complex gynecological condition affecting 10% of women globally, characterized by the growth of endometrial-like tissue outside the uterus, leading to chronic pelvic pain, infertility, reduced quality of life, and a risk of cancer. This review examines the multifaceted aspects of endometriosis, including its causes, diagnostic approaches, and management strategies. Genetic and environmental factors, hormonal influences, and immunological dysregulation are addressed as potential drivers of disease progression. Treatment options, including pharmacological interventions (hormone therapy, pain management) and surgical interventions, are assessed for their effectiveness in alleviating symptoms and improving outcomes. Emerging therapies, such as small-molecule inhibitors and anti-angiogenic agents, are also explored. Additionally, the psychological impact of endometriosis is addressed, emphasizing the need for holistic care. This review highlights the importance of continued research to unravel the precise mechanisms underlying endometriosis and to develop targeted therapies for improved patient care.
Keywords:
endometriosis
; biomarkers
; treatment of endometriosis
; natural substances
; drug targets
1. Introduction
Endometriosis is a chronic gynecological condition where tissue similar to the lining inside the uterus, known as endometrium, starts to grow outside the uterine cavity. This ectopic endometrial tissue can be found on the ovaries, fallopian tubes, the outer surface of the uterus, and other organs within the pelvis. Rarely, it can spread beyond the pelvic region. However endometriosis is a non-cancerous condition, it exhibits several characteristics commonly associated with malignant tumors. Like cancer, endometriosis is capable of spreading and infiltrating distant areas. It can ad-here to, penetrate, and harm the tissues it affects [1]. Moreover, multiple studies have shown that women with endometriosis face a higher risk of developing epithelial ovarian cancer (EOC) [2,3,4,5,6].
This condition affects approximately 10% of women of reproductive age globally, which translates to around 176 million women worldwide. Women with a first-degree relative (mother, sister) with endometriosis are at higher risk, indicating a genetic predisposition. The exact cause of endometriosis remains uncertain, although several theories have been proposed. One widely accepted theory is retrograde menstruation, where menstrual blood flows backward through the fallopian tubes into the pelvic cavity instead of leaving the body. This allows endometrial cells to implant and grow outside the uterus. Other theories suggest genetic, immunological, and hormonal factors play a role in the development of the disease [7,8].
The normal endometrial tissue, also known as the endometrium, is the inner lining of the uterus. It plays a critical role in the reproductive system, particularly in menstruation and pregnancy. The structure of the endometrium is complex and consists of two main layers, each with distinct cellular compositions and functions. The functional layer is the superficial layer that faces the uterine cavity and undergoes cyclic changes during the menstrual cycle. It is the layer that thickens in response to hormonal changes, supports embryo implantation, and is shed during menstruation if pregnancy does not occur. The second layer (basal layer) is the deeper layer adjacent to the myometrium (muscle layer of the uterus). Unlike the functional layer, the basal layer remains relatively constant and is not shed during menstruation. It serves as the regenerative source for the functional layer after each menstrual cycle [9].
The endometrium comprises various cell types, each playing specific roles in its function and cyclic changes [10]. Epithelial cells form the lining of the endometrial surface and glands. These cells can be ciliated, aiding in fluid movement, or secretory, producing essential secretions for early pregnancy. Stromal cells provide structural support and are involved in the hormonal response, contributing to the cyclic remodeling of the endometrium. They play a crucial role in decidualization during pregnancy. Immune cells include macrophages, natural killer cells, and T cells, which help maintain tissue homeostasis and play roles in the immune response during the menstrual cycle and pregnancy. Vascular cells represented by endothelial cells and pericytes form the extensive network of blood vessels that supply the endometrium, essential for nutrient delivery and tissue remodeling.
The exact mechanisms by which endometriosis spreads are complex and multifactorial, involving several theories and potential pathways. Here, these mechanisms and theories based on current scientific understanding are presented:
- Retrograde menstruation
This theory was first proposed by Dr. John Sampson in the 1920s and is one of the most widely accepted theories for the spread of endometriosis. It involves the backward flow of menstrual blood through the fallopian tubes into the pelvic cavity during menstruation. The menstrual blood contains viable endometrial cells which implant on peritoneal surfaces and other pelvic organs, where they can proliferate and form endometriotic lesions. Because of the fact that retrograde menstruation occurs in most women, only a subset develops endometriosis, suggesting other factors, such as immune system dysfunction, play a role [11].
- Lymphatic and Hematogenous Spread
This theory suggests that endometrial cells can spread through the lymphatic system or blood vessels to distant sites, including the lungs, brain, and skin. First, endometrial cells enter the lymphatic system or bloodstream. Next, they can travel to and implant in distant locations, potentially explaining cases of endometriosis found outside the pelvic region, which supports this theory [12].
- Stem cell theory
The stem cell theory provides a compelling framework for understanding the pathogenesis of endometriosis. This theory posits that stem or progenitor cells, originating from the endometrium, bone marrow, or Müllerian duct derivatives, play a pivotal role in the development and progression of endometriotic lesions. These cells are believed to translocate to ectopic sites through mechanisms such as retrograde menstruation, lymphovascular dissemination, and direct migration or invasion. Upon reaching these sites, they differentiate into the diverse cellular components observed in endometriotic lesions, including glandular, stromal, endothelial, and smooth muscle cells. This process is facilitated by mechanisms such as epithelial-mesenchymal transition (EMT), mesenchymal-epithelial transition (MET), and metaplasia [13,14,15,16,17,18].
In some endometriosis lesions, epithelial cells are monoclonal, indicating a single-cell origin, possibly from an endometrial stem or progenitor cell. In contrast, other lesions are polyclonal, suggesting contamination with polyclonal stromal cells or repeated seeding of the lesion by cells from other sources, such as bone marrow [19].
- Coelomic metaplasia
The coelomic metaplasia theory posits that pelvic endometriosis arises from metaplasia of the peritoneal mesothelium, stimulated by endometrial stroma. Endometrial stroma, a component of retrograde menstrual debris, is rich in growth factors and cytokines, which hypothetically are key drivers of this metaplastic process. The morphological observations support Nakamura et al.'s findings, indicating that endometriosis may develop through a progressive transformation of adjacent mesothelial cells [20].
The metaplastic theory proposes that pelvic endometriosis originates from the metaplastic transformation of peritoneal mesothelium [21]. Morphological observations support this, showing a progressive change from adjacent mesothelial cells. Furthermore, a novel in vitro model using human ovarian surface epithelium (OSE) cells demonstrates that endometriosis-like lesions can develop via metaplasia from OSE. In this model, coculturing OSE and ovarian stromal cells with 17β-estradiol resulted in lumen formation by OSE cells, surrounded by stromal cells in an epithelial-mesenchymal configuration. Glandular cells exhibited immunoreactivity for epithelial membrane antigen and cytokeratin, and electron microscopy revealed cilia, microvilli, and tight junctions.
- Embryonic rest theory
The assumptions of the embryonic rest theory are similar to those of coelomic metaplasia theory, although not limited to the mesothelium. According to this theory, endometriotic lesions originate from cells derived from the Müllerian or Wolffian duct [22]. Signore et al. noted, after conducting analysis of female fetuses, the presence of ectopic endometrium outside the uterine cavity in ten of one hundred fetuses [23]. The locations where ectopic endometrial nests were found matched the locations where endometriosis occurs in women. At the same time, the theory may explain the rare occurrence of endometriosis in men.
- Iatrogenic dissemination
Iatrogenic dissemination refers to the spread of endometrial cells as a result of surgical procedures, such as cesarean sections, laparotomies, or laparoscopies, which can inadvertently transport endometrial cells to new sites. These cells can then implant and grow, leading to endometriotic lesions at surgical scar sites or other locations [24,25,26].
- Genetic and epigenetic factors
Endometriosis is influenced by both genetic and environmental factors, with genetic inheritance accounting for roughly 50% of disease susceptibility [27]. The 5–7% risk among first-degree relatives suggests a polygenic and multifactorial inheritance pattern. Epigenetic factors influencing the development of endometriosis include hypermethylation in the promoter region of tumor suppressor genes and hypomethylation in the promoter region of oncogenes, which have been associated with endometriosis. Moreover, histone modifications are often observed in endometriotic lesions. According to Bedrick et al. histone modification and methylation of genetic sequences occurred simultaneously, suggesting multifactorial epigenetic changes and dysregulation in the pathogenesis of endometriosis [28]. Genetic studies have identified nine loci associated with endometriosis, six of which (rs12700667 at 7p15.2, rs7521902 near WNT4, rs10859871 near VEZT, rs1537377 near CDKN2B-AS1, rs7739264 near ID4, and rs13394619 in GREBI) were confirmed as genome-wide significant. Two additional loci (FNI and 2p14) demonstrated borderline significance in moderate-to-severe cases [27]. A locus near the VEZT gene has been significantly linked to endometriosis in the general population, highlighting the role of specific genetic variants in the disease's progression [29].
2. Psychological Aspects of Pain Management in Endometriosis
Studies indicate that the experience of pain accompanying endometriosis significantly correlates with psychological difficulties, the occurrence of stress and a decrease in the quality of life of women [30]. Thus, the (subjective) psychological aspect of the occurrence of this disease is, on the one hand, a constant experience, while on the other hand - a person-specific element due to the context of their individual, social and cultural development [31]. The psychological manifestations of the experience of pain by women with endometriosis can be defined as a type of suffering of patients presenting for a medical diagnosis, which, however, cannot be entirely explained on the basis of physiological and/or somatic factors (e.g., experiences accompanying intense pain during menstrual bleeding, abdominal pain, sacral pain in the spine, infertility, or dyspareunia) [32].
Psychological suffering of women with endometriosis can be of a diverse nature - it can consist of: a) anxiety and/or depression (e.g., in the form of sadness, lowered self-esteem, guilt, helplessness) [33,34,35,36]; b) trauma (psychological tension associated with the anticipation of pain, nightmares, functioning in traumatic situations) [37,38]; c) chronic stress generated by the perception of multidimensional losses (i.e. due to the high risk of difficulties in falling pregnant, loss of work, difficulties in fulfilling family/professional obligations, problems in social relations, problems in daily activities - e.g. in the form of disturbances with sleeping, eating, movement, sexual intercourse, bowel movements, frequent fatigue, frustration in achieving goals) [39,40]; d) a reduction in the perceived quality of life in various domains (e.g., in the dimensions of physical functioning, mental functioning, sexual functioning, environmental functioning, social functioning, general health, vitality, fulfilled roles, ability to work) [41,42,43,44].
According to literature, it can be concluded that strategies combining medical and psychological interventions are more effective in reducing psychological suffering and physical pain in patients with endometriosis [45,46,47,48,49]. Psychological interventions in the care of women with endometriosis are related to taking the patients' perspective - including areas such as : a) respect for values and specific needs; b) appropriate information, communication and education; c) providing emotional support to alleviate negative emotional states; d) involving loved ones in care; e) increasing the competence of medical personnel (mainly in the areas of building trust, providing support, reinforcing the changes taking place, providing feedback) [50,51].
Improvements in the perceived quality of life by women experiencing pain from endometriosis are often a result of synergistic efforts to : a) receive professional help - such as participation in therapy to improve well-being, understanding and accepting the disease, changing beliefs about pain, constructive coping with the disease and problems experienced (causing both trauma and chronic stress), learning new behaviors; b) experiencing understanding and support from family members - mainly mothers and partners; c) participation in support groups and/or self-help groups in the form of meetings with other women with endometriosis, d) ability to partake in self-care - including having a positive attitude toward life, engaging in relaxation activities, exercising regularly, making sure to eat regularly and get enough sleep [52,53].
3. Diagnosis and Biomarkers
The primary symptoms of endometriosis include chronic pelvic pain, dysmenorrhea (painful periods), and dyspareunia (pain during intercourse). Many women also experience heavy menstrual bleeding and infertility. Additionally, endometriosis can lead to fatigue, diarrhea, constipation, bloating, and nausea, particularly during menstrual periods. The severity of symptoms is not necessarily correlated with the extent of the disease, making diagnosis challenging [54,55]. Other less obvious symptoms of the disease include chronic fatigue, brain fog, depression, dizziness and nausea [56]. The severity of endometriosis symptoms is not necessarily correlated with the severity and extent of the disease; moreover, more than 25% of affected women are asymptomatic, making an appropriate diagnosis much more difficult [37].
Diagnosing endometriosis can be complex and often involves a combination of patient history, physical examinations, imaging tests, and sometimes surgical procedures. Transvaginal ultrasound and magnetic resonance imaging (MRI) can help visualize endometriotic lesions, but the gold standard for diagnosis is laparoscopy. During this minimally invasive surgical procedure, a camera is inserted into the pelvic cavity to directly observe and biopsy suspected endometriotic tissue [57].
Based on physiopathology and location, ectopic endometrial lesions, which are made up of endometrial glands and stroma, can be classified into three distinct types, differing in pathogenesis, location and impact on the body: superficial peritoneal endometriosis (SPE), ovarian endometrioma (OMA), and deep infiltrating endometriosis (DIE) [58]. SPE is the mildest form of the disease, involving small changes on the peritoneal surface, often asymptomatic or causing mild pain. OMAs, also called chocolate cysts, develop in the ovaries as a result of repeated episodes of bleeding into the endometrial cysts, leading to their growth and potential fertility problems. In turn, DIE is the most aggressive form of endometriosis, characterized by infiltration of deep pelvic structures, such as the rectovaginal septum, intestines or urinary bladder, which results in severe pain, organ dysfunction and a significant deterioration in the quality of life of patients. Understanding these differences is crucial to the effective diagnosis and treatment of this complex disease.
3.1. Protein Markers of Endometriosis
Identification of crucial protein markers in endometriosis could have a significant impact on disease treatment in several ways. In early diagnosis they can help detect diseases at an early stage and by understanding the unique protein expression profiles of individual patients, healthcare providers can tailor treatments to be more effective. Moreover, protein markers can provide information about the likely course of a disease. Levels of particular proteins can indicate disease severity or progression, helping clinicians to predict outcomes and plan appropriate treatment strategies. Also, the identification of protein markers is crucial in drug development. They can serve as targets for new therapies or help in the stratification of patients in clinical trials, leading to more efficient and successful drug development processes.
To date several protein markers of endometriosis have been identified and used in diagnosis of this condition.
CA 125
The CA 125 antigen (Mucin-16, Uniprot:Q8WXI7) is believed to form a protective, lubricating barrier against particles and infectious agents at mucosal surfaces [59]. It serves as the basis for a widely used serum assay to monitor ovarian epithelial cancer patients. However, its low sensitivity for stage I disease and lack of specificity limit its usefulness in early cancer detection. Furthermore, similarly elevated levels in some benign conditions render it unsuitable for population screening. The antigen is expressed in corneal and conjunctival epithelia, but is overexpressed in ovarian carcinomas and low-malignant potential (LMP) tumors compared to normal ovarian tissue and adenomas [60].
Cancer antigen 125 (CA 125) is one of the most studied protein markers in endometriosis. Elevated levels of CA 125 are often observed in women with endometriosis, particularly in those with advanced stages of the disease [61]. Despite its widespread use, CA 125 lacks specificity as it can also be elevated in other conditions like ovarian cancer, pelvic inflammatory disease, and pregnancy.
CD 146
CD 146 (MUC18, Uniprot: P43121) protein mediates cell adhesion, maintaining endothelial monolayer integrity in blood vessels. Its expression in melanoma cells may promote interaction with the vascular system, facilitating hematogenous metastasis. It may also function as an adhesion molecule in neural crest cells during embryonic development. Binding to the cell surface triggers FYN and PTK2/FAK1 tyrosine phosphorylation and transient calcium influx. In adults, the protein is primarily found on endothelial cells and vascular smooth muscle; however, in malignant melanoma, its expression is strongly associated with tumor progression and metastasis, being most abundant in metastatic lesions and advanced primary tumors, while rarely present in benign nevi and low-risk melanomas [62,63].
It was found that endometrial stem cells (eSCs) express this cell adhesion molecule (CAM) belonging to the immunoglobulin superfamily. CD146 is recognized as a marker for pericytes and its presence in eSCs confirms their perivascular origin [64,65].
Glycodelin
Glycodelin (Uniprot:P09466) is a major glycoprotein synthesized and secreted by the endometrium during the mid-luteal phase of the menstrual cycle and the first trimester of pregnancy [66,67]. It plays crucial roles in fertilization and exhibits immunomodulatory effects [68,69]. Four glycoforms (Glycodelin-S, -A, -F, and -C) have been identified, differing in glycosylation and biological activity. Glycodelin-A displays contraceptive and immunosuppressive properties. Glycodelin-C promotes sperm binding to the zona pellucida, while Glycodelin-F inhibits this binding and suppresses progesterone-induced acrosome reactions [70]. Glycodelin-S, present in seminal plasma, maintains sperm in an uncapacitated state [71]. While this protein plays a role in reproductive processes, it may contribute to the pathogenesis of endometriosis by affecting immune tolerance and cell proliferation.
Loukovaara, et al. (2007). "Glycodelin: a novel serum anti-inflammatory marker in type 1 diabetic retinopathy during pregnancy." Acta Ophthalmol Scand, 85(1):46-9.
HE4
Human epididymis protein 4 (HE4, Uniprot:Q14508) is a valuable clinical biomarker for detecting epithelial ovarian cancer (EOC) [72]. Although its clinical predictive power is well-established, its molecular role in EOC progression remains poorly understood. Elucidating HE4's mechanistic functions could lead to novel targeted therapies. However, recommending HE4 as a therapeutic target is currently difficult due to limited research on its role in EOC progression. HE4 is expressed in various normal tissues, including the male reproductive system, respiratory tract, and nasopharynx, and is highly expressed in several tumor cell lines (ovarian, colon, breast, lung, and renal). While initially believed to be exclusively expressed in the epididymis, this has since been shown not to be the case.
Human epididymis protein 4 (HE4) has been investigated as a potential marker for endometriosis [73]. Studies have shown that HE4 levels may be elevated in endometriosis patients, though its primary use remains in ovarian cancer detection. Further research is needed to establish its definitive role in endometriosis.
IL-6
Interleukin-6 (IL-6, Uniprot:P05231) is a pleiotropic cytokine with diverse roles in immunity, tissue repair, and metabolism. IL-6 signals through membrane-bound IL-6R and IL6ST (gp130), activating "classic signaling," or via soluble IL-6R and IL6ST, triggering "trans-signaling," or via "cluster signaling" between cells [74]. IL-6 is crucial for acute phase responses, host defense (e.g., stimulating immune cell differentiation and germinal center formation), and bone homeostasis (via angiogenesis). It modulates metabolism (e.g., increasing lipolysis, improving insulin sensitivity), and potentially acts as a myokine. IL-6 also plays protective roles in liver injury and is essential for iron homeostasis by regulating hepcidin expression. While critical for normal physiological processes, excessive IL-6 contributes to various pathologies. Increased concentrations of IL-6 have been detected in the serum and peritoneal fluid of women with endometriosis, suggesting its involvement in the inflammatory milieu of the disease [75]. Its levels were significantly higher in women with endometriosis compared to those with idiopathic infertility or undergoing tubal surgery. Leptin levels also correlated positively with the endometriosis stage. These findings suggest a potential role for leptin in endometriosis pathogenesis, particularly in pain mechanisms. No association was found between peritoneal fluid leptin and idiopathic infertility.
VCAM-1
Vascular cell adhesion protein 1 (VCAM-1; Uniprot:P19320) is single-pass type I transmembrane glycoprotein, predominantly expressed on endothelial cells, with increased expression on inflamed endothelium and immune cells (macrophages and dendritic cells) in both healthy and inflamed tissues [76]. Its expression is upregulated by pro-inflammatory cytokines (e.g., TNFα), reactive oxygen species (ROS), oxidized low-density lipoprotein, high glucose, toll-like receptor agonists, and shear stress . The protein is a key regulator of leukocyte adhesion to endothelium via integrin interactions [77]. During inflammation, it binds ligands on activated endothelial cells, triggering calcium channel activation and RAC1 signaling, which facilitates leukocyte transendothelial migration [78]. Additionally, it acts as a quality-control checkpoint for bone marrow entry, preventing immune cell destruction via MHC class I presentation [79]. Endometriotic tissues showed increased mRNA levels of TGF-β1 and VCAM-1. Reducing TGF-β1 levels in endometriotic cyst stromal cells significantly inhibited cell proliferation, migration, and invasion. Conversely, adding TGF-β1 stimulated these processes and markedly increased VCAM-1 protein expression. This TGF-β1-induced VCAM-1 expression was blocked by silencing Smad3. Finally, silencing VCAM-1 prevented the stimulatory effects of TGF-β1 on stromal cell proliferation, migration, and invasion [80].
VEGF
Vascular endothelial growth factor (VEGF, Uniprot: Q9UNS8) is present in normal endometrial tissue, however its level is increased in response to increasing concentration of estrogen and progesterone. This protein supports angiogenesis of endometriosis tissue by activating Wnt\beta-catenin axis, which helps to establish a new blood source for exfoliated human endometrium [81].
MCP-1
Monocyte chemoattractant protein-1 (MCP-1, Uniprot:Q6UZ82) is a chemokine that recruits monocytes to sites of tissue injury and infection. It is expressed in a variety of cell types, either constitutively or after induction by oxidative stress, cytokines, or growth factors. This chemokine has been shown to be upregulated and implicated in various diseases. The migration of monocytes from the bloodstream through the vascular endothelium is essential for normal immunological surveillance of tissues and for responding to inflammation. Elevated levels of MCP-1 have been found in the peritoneal fluid of women with endometriosis, indicating its role in the recruitment of immune cells and the inflammatory process [82,83].
Urocortin
Urocortin (UCN, Uniprot: P55089) is a neuropeptide present in the endometrium and ovaries, with research indicating similar serum levels in individuals with endometriosis and healthy controls. However, other studies have shown that serum urocortin levels are significantly higher in women with ovarian endometriosis compared to those with other benign ovarian cysts [84]. This diagnostic approach has a sensitivity of 88% and a specificity of 90%. Urocortin could be a potential biomarker for distinguishing ovarian endometriosis from other benign ovarian conditions.
3.2. Other Markers
CA 19-9
The CA 19-9 was initially considered as an oncofetal antigen. This sialylated form of Lewis Antigen is elevated in some types of cancers (e.g. gastrointestinal cancers, pancreatic cancer, the malignant and benign ovarian tumors). Studies show that CA 19-9 can be used as a marker of endometriosis, related to its severity [85,86].
Estrogen level
Endometriosis is closely linked to steroid metabolism, with 17β-estradiol (E2) playing a key role in its growth, persistence, inflammation, and associated pain. While estradiol reaches endometriotic tissue through circulation, it is primarily produced locally within the lesions. This local accumulation of estrogen contributes to the development and progression of endometriotic lesions by activating estrogen receptors (ERs) [87]. The synthesis of E2 is upregulated in endometriotic tissue due to alterations in the activity of enzymes responsible for its biosynthesis and inactivation. Notably, endometriotic tissue can synthesize E2 de novo from cholesterol due to the high expression of two key enzymes: aromatase (CYP19A1) and steroidogenic acute regulatory protein (StAR). These enzymes are absent in normal endometrial cells.
4. Treatment of Endometriosis
There is currently no cure for endometriosis, but several treatment options are available to manage symptoms and improve quality of life [54]. Treatment approaches are tailored to the individual's symptoms, age, and desire for future fertility. Pain management often begins with nonsteroidal anti-inflammatory drugs (NSAIDs). Hormonal therapies, such as oral contraceptives, progestins, and gonadotropin-releasing hormone (GnRH) agonists, aim to reduce or eliminate menstruation, thus minimizing the growth and impact of endometrial tissue. In severe cases, surgical intervention may be necessary to remove endometriotic lesions and adhesions. For women experiencing infertility, assisted reproductive technologies such as in vitro fertilization (IVF) may be considered.
4.1. Classical Treatment Methods
The treatment of endometriosis depends on many factors, including the severity of symptoms, the scope and location of the disease, the desire to become pregnant and the age of the patient. It also includes the type of the variant: superficial peritoneal disease, deep infiltrating endometriosis, or ovarian endometriomas. The patient's condition can be improved through pharmacological treatment and surgery. Pharmacological therapy for endometriosis aims to improve symptoms or prevent recurrence of postsurgical disease. The aim of surgical treatment is to remove pathological tissue including removing large endometriotic lesions [88]. The best results are achieved by using both of these methods. Pharmacology, in addition to reducing adverse symptoms, is also intended to reduce the chance of relapse after surgical treatment. Currently available methods of treating symptoms are collected in the publication of Vercellini et al. [89]. Pharmacological management of endometriosis primarily involves treating the accompanying symptoms. The first-line treatment of endometriosis relies on the use of hormone therapy, namely the contraceptive pill. The problem of excessive exposure to estrogens should be significantly alleviated by the use of contraceptives containing low doses of hormones. Combined estrogen and progestogen preparations in a continuous protocol are recommended, as they reduce endometriosis-associated dyspareunia, dysmenorrhea, and also non-menstrual pain. Mentioned pharmacology controls symptoms and slows the progression of the disease. Vaginal contraceptive rings or transdermal estrogen/progestogen patches are also suggested [90]. Combined contraceptives provide initial pain relief, but long-term efficacy in the treatment of endometriosis has no clinical evidence. Women with suspected endometriosis beyond oral contraceptives, a progestin-only pills can be offered [91]. Progestin-only given orally have been shown to be able to control the extent of endometriotic lesions in long-term use. Its main advantage is low cost. On the other hand, drawbacks of medicines, like medroxyprogesterone acetate include frequent episodes of breakthrough bleeding, decreased bone mineral density, increased risk of venous thromboembolism and unpredictable return of ovarian activity. When deciding on such a procedure, attention should be paid to the choice of progestogen, also in light of the reported increased risk of meningioma.
The use of popular old-fashioned drugs, such as danazol or gestrinone, are possible in the absence of their side effects. Therapy produces a pseudomenopause by inhibiting the release of gonadotropin-releasing hormone, involuntarily increases the androgen and decreases estrogen, which causes atrophy of endometriotic implants. Danazol, although halted the progression of the disease, causes weight gain, virilism, and elevated liver enzyme levels.
Norethisterone acetate (NETA) was considered a good choice of endometriosis treatment due to its strong inhibition effect on the endometrium, satisfactory effectiveness of pain relief associated even with deep lesions, relatively good tolerance and low cost [92]. Side effects such as seborrhea, acne, and weight gain are common. Moreover, oral NETA is associated with a dose dependent risk of venous thromboembolism, and some cases of mild liver toxicity. Therefore, patients using NETA should be prescribed the lowest effective dose and undergo regular liver function monitoring .
Dienogest used orally inhibits ovulation and is as effective as NETA in inhibiting pain symptoms in endometriosis and is also associated with a similar incidence of uterine spotting and breakthrough bleeding during therapy. This drug is well tolerated and can be safely prescribed for several years, but long-term use of dienogest is associated with a mild degree of osteopenia [92].
The approach to managing pelvic pain with endometriosis may also include non-steroidal anti-inflammatory drugs (NSAIDs) to reduce inflammation. NSAIDs and other pain relievers are effective in reducing the pain associated with endometriosis and also have a beneficial effect on primary dysmenorrhea [90].
Gonadotropin-releasing hormone (GnRH) agonists (buserelin, goserelin, leuprorelin, nafarelin, tryptorelin) or antagonists (elagolix, linzagolix, relugolix) are suggested as a next line therapy [93]. Drugs inhibit ovarian function, induce deep, stable hypoestrogenism, and are currently the most effective for alleviating symptoms associated with endometriosis. GnRHant achieves similar metabolic effects to GnRH agonists, i.e. ovarian suppression, hypoestrogenism, and amenorrhea, although through different mechanisms of action. Both types of medications are highly and equally effective in relieving symptoms associated with endometriosis and can provide a real pharmacological lifesaver when oral contraceptives and progestogens fail. GnRH agonists therapy is associated with side effects, including vasomotor symptoms, vaginal dryness, headaches, and osteopenia.
Most hormonal treatments for endometriosis focus on inhibiting estrogen production in the ovaries. Aromatase inhibitors are highly specific and work by inhibiting the aromatase, the final enzyme in the estrogen biosynthesis pathway and stop local estrogen production. An adverse symptom of aromatase inhibitors is vaginal dryness, insomnia, vasomotor symptoms, headaches and increased risk of osteoporosis. Aromatase inhibitors are recommended in therapy for people who experience pain caused by endometriosis located in the rectovaginal region, refractory to other pharmacological or surgical treatments. The main goal of the therapy is to reduce pain, correct infertility and possibly avoid or delay the long-term sequelae associated with endometriosis, such as fibrosis, adhesions and possible malignancy conversion of the lesion.
In addition to safety, efficacy, tolerability, and cost, there are at least two additional aspects to consider when choosing treatment: the main type of symptom reported by the patient and the most severe type of lesion present.
4.2. Surgery
Laparoscopy is the “gold standard” for the diagnosis of endometriosis [94]. Biopsies allow histological confirmation of the disease. Surgery for endometriosis typically is reserved for women who have persistent significant pain despite trials of medical treatments. For deep endometriosis, surgical excision is the method of choice. European Society of Human Reproduction and Embryology (ESHRE), European Society for Gynaecological Endoscopy (ESGE), and the World Endometriosis Society (WES) jointly developed recommendations on how to operate endometrial cysts [95]. Surgery of endometriosis and endometrial cysts is a solution that requires a lot of attention and good training.
Deep infiltrating endometriosis is located deeper in pelvic structures such as the intestines, bladder, and blood vessels. This type of endometriosis should be treated surgically by experienced surgeons, and preferably by interdisciplinary teams. The deep form of ovarian endometriosis is represented by endometrioma – an ovarian cyst surrounded by endometrial tissue. Bilateral endometriomas usually obliterate the Douglas cavity, which makes surgical procedure more difficult.
Pharmacological therapy to reduce the pain caused by deep infiltrating endometriosis is an alternative to surgery, except for some conditions, such as intestinal endometriosis associated with sub-occlusive symptoms, ovarian cysts with a questionable ultrasound appearance, cysts, especially when patient is older than 40 years of age, women trying to conceive a child and those who refuse hormone therapy.
Prolonged suppression of ovulation dramatically reduces the risk of recurrence of lesions, especially in the case of endometrial ovarian cyst. Furthermore, lesions often re-grow over a patient’s reproductive lifespan [96].
Surgical approaches include ovarian cystectomy with cyst wall stripping, cyst drainage, ablation, and sclerotherapy. Ablation or excision of visible endometrial lesions may be done at the time of diagnostic laparoscopy. Endometrial cysts, it is endometrioma aspiration alone, is associated with a high recurrence rate and is not recommended. Cystectomy is associated with a lower recurrence rate, chance of reoperation, dysmenorrhea, dyspareunia. The type of surgery depends on the size of the cyst, the patient's age, the surgical stage and the desire to get pregnant. Endometriomas over 4 cm should be surgically removed. Ovarian cystectomy for either endometriomas or non-endometriotic benign ovarian cysts, both cohorts exhibited a reduction in anti-Müllerian hormone levels following surgery. Surgery should be performed avoiding blind coagulation of bleeding areas, especially during ovarian surgery. Precise spot bipolar coagulation is the key to achieving hemostasis during endometriosis surgery, which is to prevent unnecessary damage of healthy tissue [97]. Postoperative decline in anti-Mullerian hormone is the highest after cystectomy, but cystectomy is associated with lower rates of recurrence compared with ablation and sclerotherapy [98]. In order to spare ovarian tissue and reduce tissue loss, laser is suggested during surgeries. The optimal surgical technique for treating endometriosis has not been established, but the skill of the surgeon plays a role in achieving complete destruction or removal of endometriotic tissue and adhesions. Surgical treatment for endometriosis followed by medical therapy offers longer symptom relief than surgery alone.
4.3. Sclerotherapy of Endometrial Cysts and Other Methods
The subject of research were alternative strategies for the treatment of endometrioma. One of the most popular is the use of sclerotherapy. The rationale for sclerotherapy is to destroy the pseudocapsule of the endometrioma by instilling alcoholic or other substances inside it [99]. The sclerosing agent is left in situ or respirated [100].
The natural history of endometriosis is variable. Although endometriosis often is progressive, some studies have shown spontaneous regression in time [101]. Most women have improvement or resolution of endometrial symptoms with menopause. Postmenopausal hormone therapy appears to promote recurrence in some women.
Semiconservative surgical treatment involves a hysterectomy and reduction of endometrial lesions while conserving the woman's ovaries. This procedure is good for women, who have completed childbearing, and continue to have pain despite medical therapy, but are too young or do not want to undergo surgical menopause.
Alternative therapy for endometriosis is also possible. Resveratrol use, a natural medicine derived from grapes. This compound induces apoptosis in endometrial stromal cells by suppressing survivin expression. Acupuncture, lifestyle changes, transcutaneous high-frequency electrical nerve stimulation, Chinese herbal medicine, vitamins B1 and B6, tropical heat, spinal manipulation, and behavioral interventions are all of interest to physicians treating endometriosis-related.
4.4. Natural Substances Used in the Treatment
Natural compounds are widely used in alternative medicine, including in the treatment of endometriosis, where they can produce satisfactory results [102,103]. Studies indicate that oxidative stress plays an important role in the pathophysiology of the disease and its associated pain. The antioxidant properties of natural compounds, such as polyphenols and secondary metabolites, can help alleviate symptoms and slow the progression of endometriosis. In addition, anti-inflammatory or vegan diets, due to their immunomodulatory properties, can be an effective dietary intervention for patients with the disease. Among the natural compounds present in fruits and vegetables, it is worth noting compounds such as curcumin, resveratrol, rutin, quercetin, kemferol, myricetin, cannabinoids and capsaicin.
Curcumin
Curcumin, a bioactive pigment from the rhizome of Curcuma longa, exhibits anti-inflammatory, antioxidant and antiproliferative properties that may support the treatment of endometriosis [104]. Studies confirm its ability to inhibit inflammation (e.g., by regulating cytokines and chemokines), reduce angiogenesis, and induce apoptosis in ectopic endometrial cells [105]. Curcumin also reduces levels of VEGF and MMPs, key to the development of endometriosis, and promotes folliculogenesis by modulating growth factors [106].
Clinical studies have shown the effectiveness of curcumin supplementation (e.g., 500 mg/day) in relieving pain and inflammation. Curcumin's poor bioavailability can be improved by modern technologies such as nanoformulations. Curcumin supplementation may provide valuable support in the treatment of endometriosis.
Figure 1.
Structural formula of curcumin.
Polyphenols
Polyphenols are one of the most abundant groups of natural compounds found in plants, especially fruits and vegetables. They show numerous health benefits, and their potential in the treatment of endometriosis and chronic pelvic pain (CPP) is promising due to their antioxidant and anti-inflammatory properties. In addition, their ability to affect estrogen receptors may play an important role in alleviating the symptoms of endometriosis. Studies indicate that selected polyphenols are effective in reducing pain and other discomforts associated with the disease.
- Resveratrol
Resveratrol (3,5,4′-trans-trihydroxystilbene) is a polyphenol belonging to the stilbene class, found mainly in the skin and seeds of grapes, as well as in wine, peanuts, berries and tea. The compound is synthesized by more than 70 plant species in response to stress, injury, bacterial or fungal infections or UV radiation, highlighting its protective role in nature [107,108]. Resveratrol in cells is converted to piceatannol, a monohydroxylated derivative of resveratrol, by the cytochrome P450 enzyme CYP1B1. In addition, cytochrome enzymes can convert resveratrol into further polyhydroxylated metabolites. Hexahydroxystilbene, which is an analog of resveratrol, exhibits as much as 6600-fold higher antiradical activity. Hydroxylation at the ortho position, as in the case of 3,4-dihydroxy-trans-stilbene, significantly enhances the ability to counteract lipoprotein peroxidation by forming hydrogen bonds between the methoxyl and phenolic groups. Fig. shows the chemical formulas of resveratrol and piceatannol.
Figure 2.
Sructural formula of resveratrol.
- Epigallocatechin gallate
Epigallocatechin gallate (EGCG), the main flavonoid present in green tea, exhibits antioxidant, antiproliferative and antiangiogenic properties, making it a promising compound for the treatment of endometriosis [109,110,111]. Studies have shown that EGCG reduces endometrial cell proliferation, migration and invasion, inhibits neovascularization and reduces fibrosis in endometriosis. In animal models, EGCG reduced the number and volume of endometriotic lesions, although it was less effective than resveratrol. EGCG's mechanism of action includes modulation of E-cadherin expression, inhibition of the VEGFC/VEGFR2 pathway and enhancement of apoptosis. Chemical modification, such as by esterification, increases the bioavailability and enhances the therapeutic properties of EGCG compared to its natural form.
Figure 3.
Structural formula of epigallocatechin gallate.
- Quercetin
Quercetin, a flavonol found in fruits and vegetables (e.g., apples, berries, onion, chili peppers), exhibits anticancer properties and anti-endometriosis activity. It inhibits cell proliferation through mechanisms such as apoptosis induction, DNA fragmentation, ROS generation, and regulation of ERK1/2, P38 MAPK and AKT kinases [112]. Animal studies have shown that quercetin reduces the size of endometrial implants and affects the levels of FSH, LH and estrogen hormones, which inhibits the growth of ectopic endometrium [113]. Combining quercetin with metformin or danazol further enhances these effects [114]. In a study on women with endometriosis, supplementation with quercetin (200 mg) in combination with curcumin and acetylcysteine for two months reduced pain and reduced the use of anti-inflammatory drugs without significant side effects.
Figure 4.
Structural formula of quercitin.
Flavonoids and derivatives
In vitro and in vivo studies conducted to date have evaluated the effects of flavonoids isolated from various plants on the treatment of endometriosis [115]. Extracts from Melilotus officinalis, traditionally used to treat, among other things, painful menstruation and uterine swelling, containing analogs of quercetin and kemferol, reduced endometrial adhesion and levels of TNF-α, VEGF and IL-6 in rats with experimentally induced endometriosis [116]. Similar properties were shown for flavonoids from Urtica dioica, known for its diuretic effects and relief of menstrual bleeding [117]. Rutin, kemferol and their analogs from the methanolic extract of this plant reduced endometrial tissue adhesion, lesion volume and inflammation. The optimal daily intake was estimated at 1129 mg for a person weighing 70 kg.
Flavonoids from other plants, such as Phaleria macrocarpa, Pinus pinaster (French maritime pine bark), and Pueraria lobata, also showed anti-endometriosis effects [118,119]. Of particular note is pycnogenol (pine bark extract), which in studies on women reduced menstrual pain from 8-9 to 2 on the VAS scale after 3 months of supplementation at a dose of 100 mg per day in combination with contraceptive therapy.
Other compounds, such as myricetin, hexahydroxyflavone, and flavonoids from Kaempferia parviflora, such as 5,7-dimethoxyflavone (DMF), were also effective [120,121]. Myricetin induced apoptosis of endometriosis cells through oxidative stress and mitochondrial dysfunction, while DMF had multiple effects, including cell cycle arrest and inactivation of the PI3K/AKT pathway.
Ginsenoside
Ginsenosides are a group of active chemical compounds responsible for key properties of ginseng. They are natural substances categorized as steroidal glycosides and triterpene saponins, and their amount can vary depending on the species of ginseng. It is worth noting that these compounds are found only in plants of the Panax genus, which is widely distributed in Far Eastern culture such as Panax ginseng C.A. Meyer, Panax quinquefolium L., Panax japonicus C.A. Meyer. Moreover, ginsenosides are anticipated to offer novel therapies for diseases related to the endometrium [122].
Different species of Panax vary in their ginsenoside content, which affects how they can support the body. Ginsenosides exhibit numerous beneficial properties, including anti-inflammatory and antioxidant effects, suggesting their potential use in the treatment of inflammation-related diseases. [123].
Cannabidiol
Cannabinoids are active compounds found in Cannabis sativa, a plant long used in medicine [124,125]. They are divided into three main groups: endocannabinoids produced in the body, phytocannabinoids derived from Cannabis sativa, and synthetic cannabinoids. Their effects are mainly related to CB1 and CB2 receptors. CBD, a natural and non-psychoactive cannabinoid, shows affinity for both of these receptors. In 2018, it became the first cannabinoid approved by the Food and Drug Administration (FDA) in the United States for the treatment of two types of epileptic seizures under the name Epidiolex.
Figure 5.
Structural formula of cannabidiol.
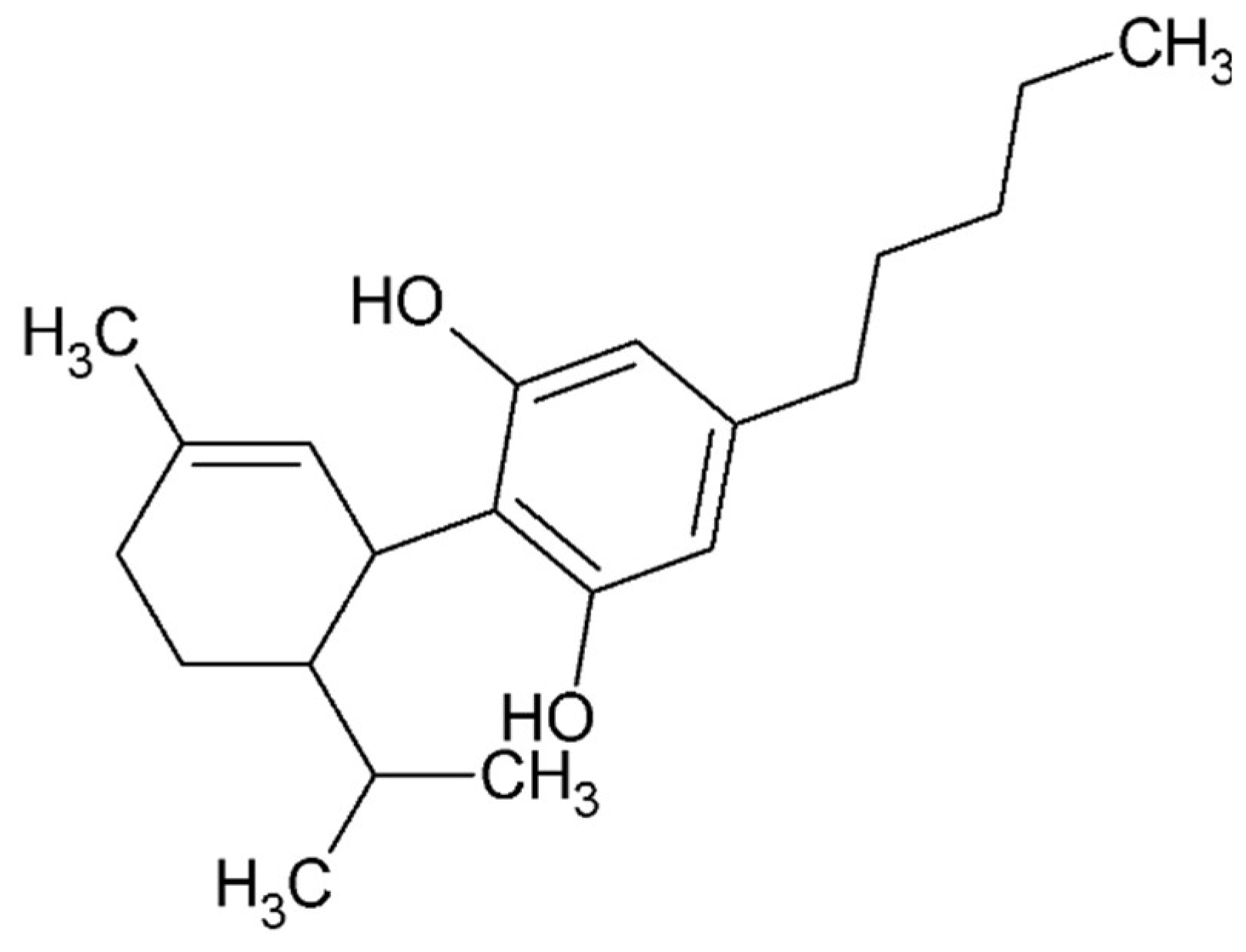
Studies have shown that CBD can inhibit endothelial cell proliferation and migration without inducing toxicity or apoptosis [126]. These processes play a key role in angiogenesis. This effect is related to CBD's action against the formation of tubular structures by endothelial cells, which is important for angiogenesis. Consequently, inhibition of angiogenesis in vivo was observed in the presence of a potent angiogenic cocktail containing VEGF, TNF-α and heparin.
CBD also reduces the expression of various pro-angiogenic factors such as MMP-2, MMP-9, TIMP-1, CXCL16, endothelin-1, IL-8 and PDGF-AA [127]. In addition, cannabidiol hydroxyquinone (HU-331) has shown the ability to inhibit angiogenesis in an ex vivo model of VEGF-induced rat aortic ring. In mouse models of tumor angiogenesis, HU-331 reduced total vessel area, density and size.
In addition, studies on human endothelial cells showed that CBD reduced the expression and levels of ICAM-1 and VCAM-1 induced by high glucose concentrations, and reduced the ability of monocytes to adhere to endothelial cells. It was also found that CBD can reduce NF-κB levels. As shown in Figure 2, both inflammation and angiogenesis play important roles in the pathogenesis of endometriosis, and CBD can inhibit these processes through various molecular pathways [128].
Rosmarinic acid
Rosmarinic acid, present in several plants such as rosemary (Rosmarinus officinalis), sage (Salvia officinalis), thyme (Thymus sp.), lemon balm (Melissa officinalis), basil (Ocimum sp.), oregano (Origanum vulgare) and perilla (Perilla frutescens, also known as Chinese basil, is a phenolic compound with a broad spectrum of health-promoting and therapeutic properties [129]. With its antioxidant, anti-inflammatory, anti-tumor and anti-angiogenic activities, it may play an important role in the treatment of endometriosis [130]. Rosmarinic acid (RA) is an ester of caffeic acid (CA) and 3-(3,4-dihydroxyphenyl) lactic acid (DHPLA). After oral administration, it undergoes extensive pre-systemic metabolism, so that only a small amount of unchanged RA enters the plasma [131,132]. In the body, it is hydrolyzed by colon bacteria into its constituent acids, CA and DHPLA.
Figure 6.
Structural formula of rosmarinic acid.
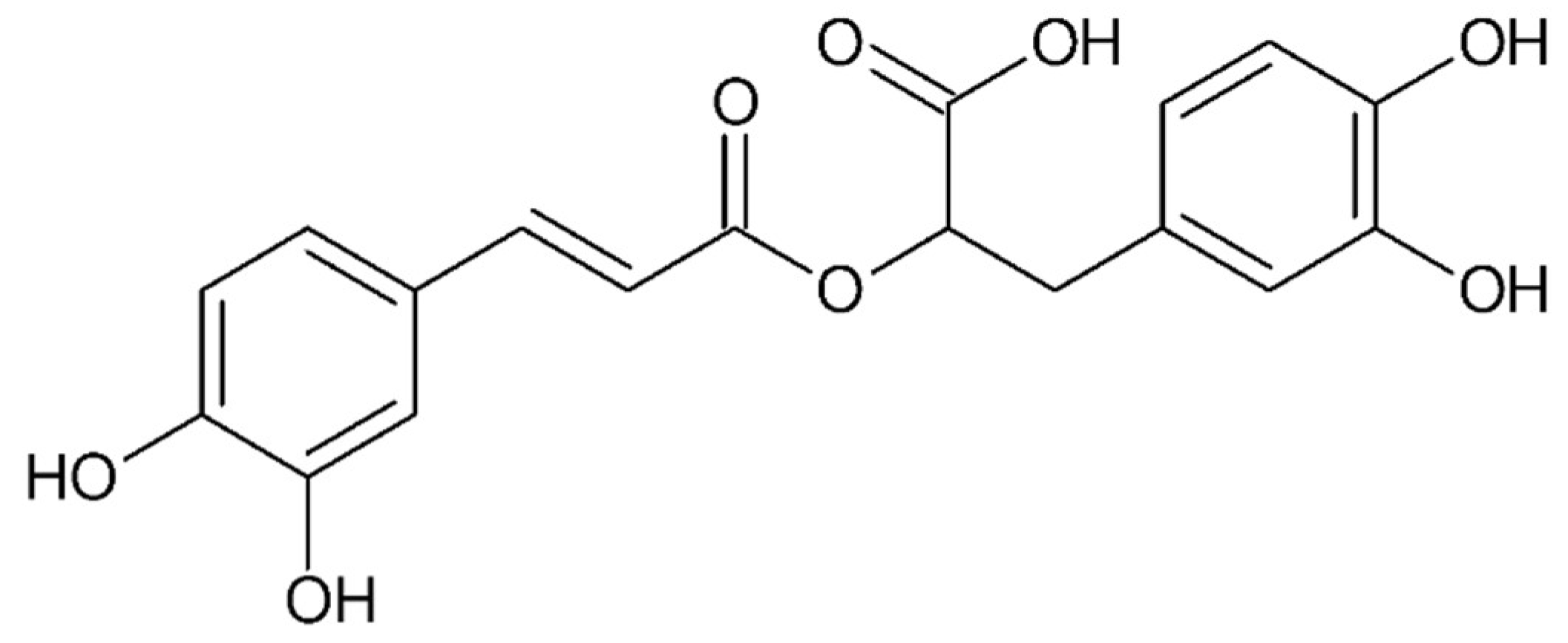
Research by Ferelli's team (2018) evaluated the anti-endometriosis potential of rosemary acid and carnosic acid [133]. The experiment used a culture of human endometrial lining cells and a BALB/c mouse model with induced endometriosis-like lesions. The results showed that both compounds inhibited cell proliferation and reduced the size of endometriotic lesions in mice. In addition, rosmarinic acid induced apoptosis in endometrial tissue and reduced intracellular accumulation of reactive oxygen species (ROS) in human endometrial lining cells.
Capsaicin
Capsaicin (trans-8-methyl-N-vanillyl-6-nonenamide) is the active ingredient in chili peppers and other plants of the bell pepper family. The capsaicin content of these plants ranges from 0.1% to 2.0%, and the peppers themselves are commonly used as food additives. Topical application of capsaicin produces a burning sensation and is used as a tool to induce standardized pain in experimental studies on humans and laboratory animals.
Figure 7.
Structural formula of capsaicin.
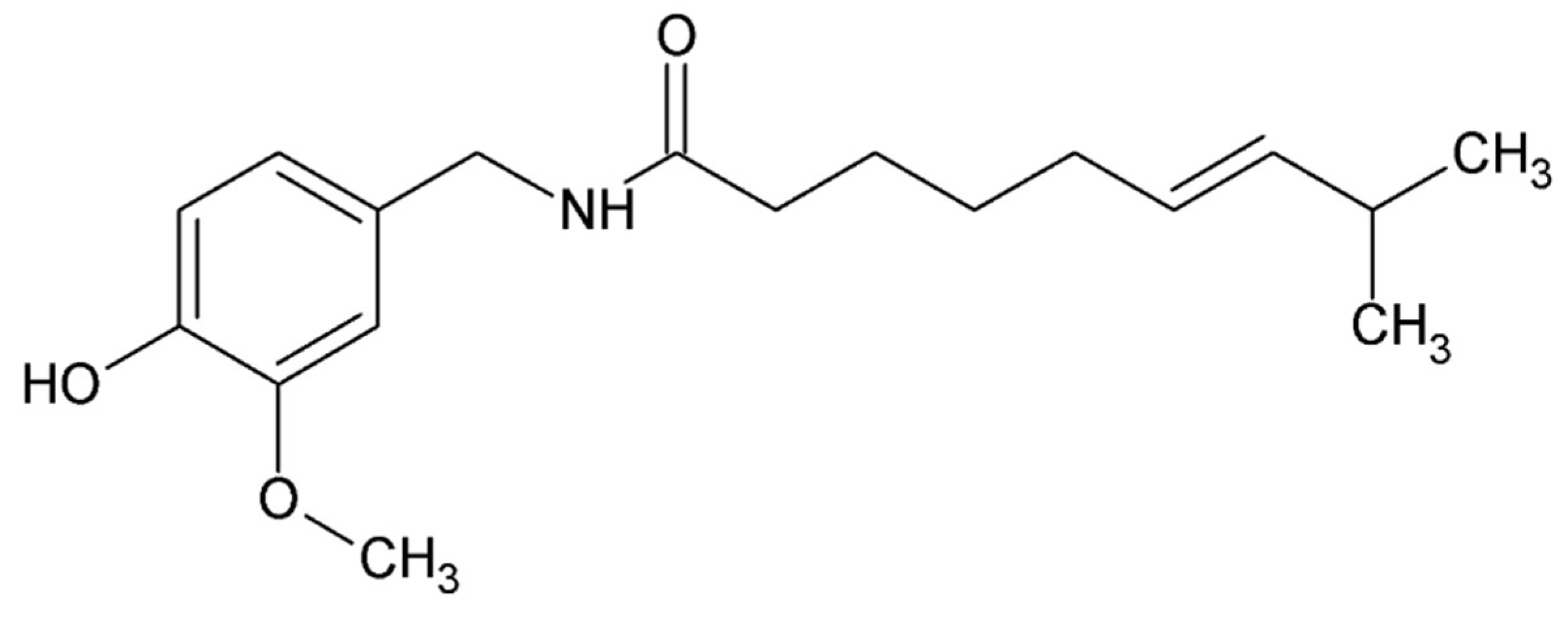
The pharmacological effects of capsaicin, both topically and systemically administered, have been extensively studied in a variety of species [134,135]. Capsaicin has become a reliable model for evaluating the efficacy of new analgesics [136,137].
Despite its potent pain-inducing effects, this substance was used as an analgesic as early as 7000 BC [138,139]. The first formal reports of its analgesic properties date back to 1850, when an alcoholic extract of hot peppers was used to treat toothache [135,140]. Through years of research, capsaicin has been recognized as an effective, non-opioid analgesic with few side effects. In addition to culinary uses, capsaicin has found therapeutic applications in the treatment of various conditions, such as pruritus in psoriasis, obesity, urological diseases, respiratory, cardiovascular, gastrointestinal ailments and cancer [141,142].
Vitamins
Vitamin D plays a key role in regulating blood calcium levels and modulating the immune system. Its main sources are oily fish, fish oils and supplements, but the most effective way to obtain vitamin D is through its dermal synthesis under UVB radiation. Since endometriosis is a chronic inflammatory disease resulting from immune system dysfunction, investigating the effect of vitamin D as an immune modulator on the development of this disease seems a promising direction, especially in the context of its association with autoimmune and inflammatory diseases.
Figure 8.
Structural formula of vitamin D.
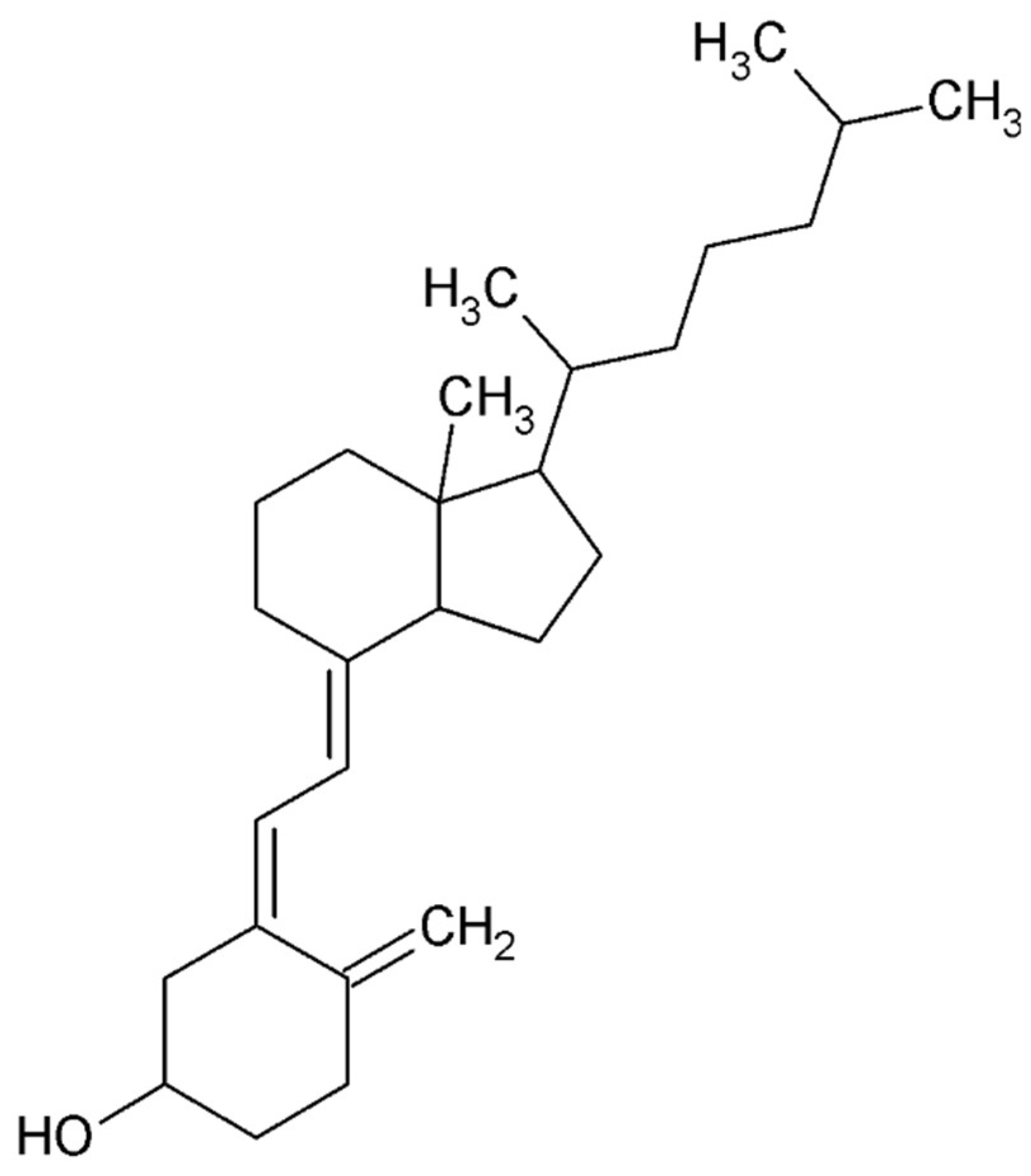
A 2020 meta-analysis found that low levels of vitamin D may be associated with an increased risk of developing endometriosis and exacerbating its symptoms [143]. Similar correlations have been confirmed in other studies, including between vitamin D levels in women of childbearing age and the size of endometrial ovarian lesions [144,145,146,147,148] [2,3,4,5]. However, some studies have found no such correlations [148,149].
Vitamins C and E play an important role in neutralizing free radicals through their antioxidant properties. Vitamin C, being an exogenous component, must be supplied with diet or supplementation. Its rich sources are rosehips, black currants, strawberries, citrus fruits, parsley and peppers. Fat-soluble vitamin E is found in nuts, seeds, vegetable oils, green leafy vegetables and cereals [150].
Figure 9.
Structural formulas of vitamin C and vitamin E.

Hoorsan et al. demonstrated in a mouse study that vitamin C enhances ovarian function and suppresses the induction and growth of endometrial grafts [151]. Similar findings were observed in rats, where intravenous vitamin C inhibited the formation of endometriotic implants and reduced their volume [152]. Additionally, research on the effects of vitamins C and E on VEGF gene expression and production in peritoneal macrophages of women with endometriosis revealed that these vitamins could alter VEGF gene expression at varying incubation times and concentrations, but did not influence VEGF production [153].
It was also confirmed the beneficial effects of vitamins C and E in reducing endometriosis symptoms compared to placebo [154,155]. Furthermore, a prospective cohort study of 1383 cases of laparoscopically confirmed endometriosis indicated an inverse relationship between dietary intake of vitamins C, E, thiamine, and folic acid and the risk of endometriosis. However, the authors suggested that this protective effect may not be directly attributed to the vitamins themselves but rather to other essential nutrients present in the diet[156].
4.5. Small Compounds Used in the Treatment
Endometriosis is a challenging condition to manage, often requiring a combination of medical, surgical, and alternative approaches. Experimental treatments, aiming to improve efficacy and reduce side effects compared to current standard therapies, are continually being explored. Here are some of the promising experimental treatment methods and targets:
Selective Progesterone Receptor Modulators (SPRMs)
Selective Progesterone Receptor Modulators (SPRMs) are a class of drugs that act on progesterone receptors with both agonist and antagonist effects. Ulipristal acetate, a well-known SPRM, has shown potential in reducing endometrial tissue proliferation and associated pain [157].
Mifepristone (DRUGBANK: DB00834) was the first selective progesterone receptor modulator, discovered in the 1980s by the French pharmaceutical company Roussel-Uclaf during research on anti-glucocorticoid drugs. Synthesized by Georges Teutsch, it was originally designated as RU-38486, later shortened to RU-486. Its antiprogestin properties were investigated by endocrinologist Étienne-Émile Baulieu, who played a key role in its development as a medication for pregnancy termination, earning him the title of the "father" of the abortion pill. Mifepristone is a synthetic estrane steroid, chemically named 11β-(4-(dimethylamino) phenyl)-17α-(1-propynyl) estra-4,9-dien-17β-ol-3-one [158].
UPA Ulipristal acetate (DRUGBANK: DB08867) is a steroidal selective progesterone receptor modulator (SPRM) that was initially studied in the 1990s as an antifertility drug, similar to mifepristone. Originally developed by the National Institute of Child Health and Human Development (NICHD), UPA is derived from 19-norprogesterone. Research in animal models has shown that UPA may induce regression of endometriotic lesions, reduce cell proliferation, and decrease inflammation. Clinical reports suggest its potential in alleviating chronic pelvic pain associated with endometriosis, although its effects on different subtypes of the condition remain uncertain. Due to conflicting evidence regarding its efficacy, further research through well-designed randomized controlled trials (RCTs) is necessary [158].
Vilaprisan (DRUGBANK: DB11971) is a potent, orally active selective progesterone receptor modulator (SPRM) developed by Bayer AG. Structurally, it is a 17-hydroxy-17-pentafluoroethyl-estra-4,9(10)-dien-11-aryl derivative, with weak binding to the glucocorticoid and androgen receptors but no effect on the estrogen receptor. Vilaprisan has been investigated in clinical trials for the treatment of heavy menstrual bleeding (HMB) associated with uterine fibroids and for managing symptomatic endometriosis. However, all clinical trials were put on hold due to safety concerns identified in long-term toxicology studies in rodents [158].
Estrogen receptors
Since the endometriosis is a hormone-dependent condition, estrogen receptors play pivotal role in the pathogenesis and progression of endometriosis by mediating the effect of estrogen [87].
Previous studies conducted on mouse models and endometrioma cells from patients have elucidated the molecular mechanisms underlying the specific roles of each estrogen receptor (ER) isoform in the initiation and progression of the disease. Beliard et al. observed a positive correlation between cell proliferation and ER levels in normal and eutopic endometrium obtained from patients aged 26 to 40 years, although they found no correlation with apoptosis and estrogen receptor levels [159]. Notably, the study did not specify the antibody used, which limited the differentiation between ERα and ERβ. Consequently, researchers utilized ERα and ERβ knockout mice to induce endometriosis-like lesions by injecting minced uterine tissue into the peritoneal cavity of syngeneic host mice [160]. These experiments demonstrated that both ER isoforms are essential for the growth of endometriotic-like lesions. However, estradiol significantly enhanced the development of these lesions, predominantly highlighting the necessity of ERα for cell adhesion, proliferation, and neoangiogenesis that support lesion growth. The impact of ERβ knockout on ectopic lesion growth was less significant compared to the effects of ERα knockout.
Bazedoxifene (DRUGBANK: DB06401). The selective estrogen receptor modulator (SERM) bazedoxifene (BZA) effectively inhibits estrogen-induced stimulation of the uterine endometrium while preserving estrogenic effects in bone and the central nervous system [161]. These characteristics make it a promising candidate for treating endometriosis. In an experimental model, endometriosis was induced in reproductive-age CD-1 mice. After treatment, the size of the endometriotic implants was measured, revealing a mean size of 60 mm² in the control group compared to 21 mm² in the BZA treatment group.
SR-16234 (DRUGBANK: DB05966). Treatment with SR significantly decreased both the total number and size of lesions per mouse without promoting endometrial growth [162]. Additionally, SR downregulated the mRNA expression of LPS-enhanced Vegf, Il-6, Ptgs-2, Ccl-2, and ER in endometriosis-like lesions. Immunohistochemical analysis revealed a reduction in the percentage of Ki67-positive cells, as well as a decrease in the intensity and proportion of cells positively expressing ERα, CD3, F4/80, and PECAM following SR treatment. Furthermore, SR treatment led to a reduction in the expression levels of NF-κB p65 and phosphorylated NF-κB p65.
The compound was also tested in a clinical trial. After 12 weeks of oral administration of SR-16234 at a dosage of 40 mg, there were statistically significant reductions in pelvic pain measured by the Visual Analog Scale (VAS), total pelvic pain score, total dysmenorrhea score, stiffness of Douglas’ pouch, and limitations in uterine movement compared to baseline values [163]. This trial indicates that a selective estrogen receptor modulator may be an effective treatment for pain associated with endometriosis.
Steroid sulfatase inhibitors
Steroid sulfatase (STS) is an enzyme that plays a crucial role in the local regulation of estrogen levels by hydrolyzing sulfate conjugates of steroids, such as estrone sulfate, into their active forms, like estrone. This enzymatic activity is particularly relevant in the context of estrogen-dependent conditions, including endometriosis.
The steroid sulfatase pathway provides an alternative source of local estrogens within endometriotic lesions, promoting cell proliferation, inflammation and the associated symptoms of endometriosis such as pain and infertility. By converting estrone sulfate to estrone, which can subsequently be converted to the more potent estrogen, estradiol, STS contributes to the local estrogen pool. This local production of estrogen fuels the growth and persistence of endometriotic tissue [164,165].
Moreover the local estrogen production contributes to a pro-inflammatory environment by inducing the production of cytokines, chemokines, and prostaglandins. These inflammatory mediators not only promote the survival and growth of endometriotic lesions but also contribute to pain and other symptoms associated with the condition [166].
Steroid sulfatase inhibitors as well as combining steroid sulfatase inhibitors with other hormonal therapies, such as aromatase inhibitors or GnRH analogs, may offer synergistic effects in reducing estrogen levels and managing endometriosis symptoms [167]. This multi-targeted approach could enhance treatment efficacy and provide relief for patients who do not respond adequately to conventional therapies.
STS inhibitors include steroidal and non-steroidal compounds. Among the non-steroidal STS inhibitors, the most important role is played by the group of Coumarin Sulfamate derivatives, which includes molecules of which possessing a fused tricyclic structure Irosustat (STX64) is considered the most potent [168,169]. It is the first non-steroidal STS inhibitor which entered the clinical phase in postmenopausal women with breast cancer.
Among steroidal inhibitors estrone-3-O-sulfamate (EMATE, MCE: 148672-09-7 ) and its derivatives are considered one of the most potent. E2MATE (estradiol-3-O-sulfamate, MCE: 172377-52-5 ) efficiently suppresses STS activity in endometrial tissue both in vitro and in vivo [169].
Aromatase Inhibitors
Aromatase inhibitors, typically used in breast cancer treatment, inhibit the enzyme aromatase, which converts androgens to estrogens. This reduction in local estrogen production can potentially decrease endometriotic tissue growth and alleviate symptoms [170]. Here are some III-generation inhibitors of aromatase commonly used.
Letrozole (Femara, Drugbank: DB01006) - A third-generation aromatase inhibitor, is presented as effective in reducing pain associated with endometriosis, often used in combination with other therapies (gestagens, oral contraceptives, or GnRH agonists) [171]. A meta-analysis showed its effectiveness in decreasing pain and improving quality of life.
Anastrozole (Arimidex, Drugbank: DB01217) - This drug is presented as effective in reducing pain associated with endometriosis [172]. A meta-analysis cited in the article demonstrated its effectiveness in decreasing pain, reducing lesion size, and improving quality of life, often used in combination with other treatments. A specific study highlighted its use with goserelin (a GnRH agonist), demonstrating a significant reduction in pain compared to goserelin alone. It was found to reduce pain in postmenopausal patients with endometriosis but it failed to treat a case of ureteral endometriosis due to significant fibrosis. A side effect of bone mineral density decrease in one patient after 9 months of treatment was observed.
Because of the fact that these medications are usually recommended for women who are not seeking to conceive, as they can interfere with fertility, treatment should be guided by a healthcare professional who can consider individual circumstances and other treatment options, such as hormonal therapies or surgical management [167].
GnRH Antagonists
Gonadotropin-releasing hormone (GnRH) antagonists directly inhibit GnRH receptors, reducing the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH), which in turn lowers estrogen levels.
Elagolix (Orilissa, Drugbank: DB11979) - This is a GnRH antagonist specifically approved for the management of moderate to severe endometriosis-related pain [173]. It works by reducing the release of hormones that promote ovarian function and estrogen production.
Degarelix (Firmagon, Drugbank: DB06699) - While primarily used in the treatment of prostate cancer, it is a GnRH antagonist and has been studied for potential use in endometriosis, though it is not commonly used for this indication [174].
Buserelin (Suprefact, Drugbank: DB06719) - Although more often classified as a GnRH agonist, it can have antagonistic effects when used at specific doses [175]. It may be employed off-label in endometriosis treatment settings.
While GnRH antagonists can be effective in treating endometriosis, they can cause side effects related to estrogen deficiency, such as bone density loss. Treatment should be managed by a healthcare professional, taking individual patient needs and potential side effects into account.
Anti-angiogenic Agents
Anti-angiogenic agents are being explored as potential treatments for endometriosis due to their ability to inhibit the formation of new blood vessels, which is a crucial aspect of endometrial tissue growth [176]. Some anti-angiogenic agents that have been studied in the context of endometriosis include:
Bevacizumab - Bevacizumab (Drugbank: DB00112) is a monoclonal antibody that inhibits vascular endothelial growth factor (VEGF). Some studies have suggested that it may be effective in reducing endometriosis-related pain and improving quality of life [177].
Thalidomide - The current findings, along with data from a few published studies, highlight the potential of thalidomide (Drugbank: DB01041) as a treatment for endometriosis [178]. This supports the hypothesis that thalidomide can cause regression in the progression of endometriosis, emphasizing the need for further research to proceed cautiously due to its teratogenic history. Thalidomide effectively reduced the lesion area and the CPI of peritoneal endometriotic implants in rats at both 1 mg/kg/day and 10 mg/kg/day doses, with the lower dose proving as effective as the higher, teratogenic dose. Consequently, thalidomide should be considered a potential treatment option for endometriosis in women.
Sunitinib - Sunitinib (Drugbank: DB01268) was found to inhibit endometriotic lesions by promoting the maturation of myeloid-derived suppressor cells (MDSCs) in peritoneal fluid and inhibiting their immunosuppressive functions [179]. By altering the immune microenvironment, sunitinib hindered the progression of endometriosis. This suggests that sunitinib could have potential therapeutic effects as a novel immunotherapy by promoting the maturation, differentiation, and metabolism of MDSCs for treating endometriosis.
Immune Modulators
Immune modulators target the immune dysregulation associated with endometriosis. Pentoxifylline, which inhibits the production of inflammatory cytokines, has been studied for its potential to reduce endometriosis-related symptoms.
Danazol - Danazol (Drugbank: DB01406) is a treatment option for endometriosis, working by creating a high androgen/low estrogen environment akin to pseudo menopause [180]. This hormonal shift leads to the atrophy of endometriotic implants, resulting in the alleviation of painful symptoms. Studies have shown that danazol, even when used alongside surgical therapy, effectively reduces endometriosis-related pain compared to a placebo. It also improves laparoscopic scores more significantly than placebo or no treatment. However, patients using danazol report side effects more frequently than those on placebo, primarily due to its androgenic effects, which limit its use despite its effectiveness in managing the symptoms and signs of endometriosis.
PD-1/PDL-1 (Programmed cell death protein 1/death ligand 1) inhibitors - Endometriosis stimulates bone marrow mesenchymal stem cell differentiation via paracrine signal transduction and increases PD-1 expression in T cells [181]. Increased PD-1 expression may be a mechanism by which endometrial tissue evades immune monitoring. Targeted PD-1 inhibition may be an effective treatment for endometriosis.
CD47 inhibitors - Overexpression of CD47 molecules on the surface of endometriosis cells is associated with their recognition by macrophages as normal cells [182]. Blocking this signal with the use of siRNA or neutralizing antibodies, may serve to switch macrophages to phagocytosis of endometriosis cells.
Azathioprine - The use of this immunomodulator (Drugbank: DB00993) could be also considered as the findings show that immunosuppression for three months accelerated the progression of spontaneous endometriosis in baboons model but did not influence the development of induced endometriosis, nor did it induce the disease in baboons with a previously confirmed normal pelvis [183].
4.6. Stem Cell Therapy
Stem cell therapy is an emerging field in endometriosis treatment. Mesenchymal stem cells (MSCs) have shown promise in preclinical studies for their potential to modulate immune responses and repair tissue damage associated with endometriosis [184].
Stem cells (SCs) play a significant role in the development and progression of endometriosis by being recruited to ectopic foci from retrograde menstrual fluid and bone marrow. Targeting SC recruitment has been identified as a promising approach to inhibit the progression of this disease. Bazedoxifene, a selective modulator of estrogen receptors, has demonstrated the ability to inhibit ectopic endometrial growth and interfere with SC recruitment in mice. In experimental studies, the combination of bazedoxifene with conjugated estrogens significantly reduced SC recruitment to lesions, leading to a notable reduction in lesion size, while sparing SC recruitment to the uterus in control animals [161]. Additionally, endothelial progenitor cells (EPCs) derived from bone marrow contribute to neo-vasculogenesis in endometriotic lesions, with their recruitment being mediated by the CXCR4/SDF1 signaling axis under hypoxic conditions [185]. Blocking CXCR4 with AMD 3100 effectively reduces EPC recruitment and decreases capillary density within the lesions. Estradiol has also been shown to stimulate the release of CXCL12 and CXCR4, promoting SC migration, a process that can be inhibited by AMD 3100. Conventional progestin treatments may further support this strategy by suppressing CXCL12 production, thereby limiting SC recruitment to ectopic foci. These findings suggest that inhibiting SC recruitment, through safe and effective interventions, represents a relevant therapeutic strategy in endometriosis management [18,186,187].
4.7. Gene Therapy
Gene therapy represents a promising approach for the treatment of endometriosis, utilizing advanced techniques such as nanotechnology, microRNAs, and other molecular strategies. Numerous studies to date have demonstrated the potential of nanotechnology-based gene therapy in managing this condition. One notable example involves the application of nanocarriers in gene delivery systems for endometriosis, including polymeric nanoparticles, cell-penetrating peptides (CPPs), and extracellular vesicles (EVs). These nanocarriers facilitate the targeted delivery of therapeutic genes or siRNA to endometrial lesions [188]. Othman et al. employed an adenoviral vector to deliver the dominant negative estrogen receptor (DN-ER) gene into human endometriotic cells in vitro. This intervention led to the suppression of cell proliferation, reduced cytokine production, and the induction of apoptosis, as a consequence of disrupted estrogen signaling [189]. Another approach includes the use of siRNA carriers. For example Egorova et al. showed inhibition of vascularization in endometrial lesions after the use of CXCR4 receptor-targeted siRNA carrier L1 [190]. Techniques such as CRISPR-Cas9 are also being investigated for their ability to target specific genetic abnormalities in endometriotic cells [191]. They could be used for so-called gene editing. Some genes, for example gene encoding neuropeptide S receptor 1 are promising targets. Tapmeier et al. observed correlation between the deletion at rs142885915 in this gene, and the occurrence of III and IV stage of endometriosis. Moreover, the inhibition of NPSR1 through a selective inhibitor, SHA 68R reduced immune response in mice [192].
5. Impact on Quality of Life
Endometriosis can significantly impact a woman's quality of life, affecting her physical, emotional, and social well-being. Chronic pain and fatigue can limit daily activities and productivity, leading to absenteeism from work or school. The emotional burden of dealing with a chronic, often misunderstood condition can result in anxiety, depression, and strained relationships [55]. Therefore, a multidisciplinary approach involving pain specialists, gynecologists, and mental health professionals is often beneficial in managing the comprehensive effects of the disease.
References
- Vlahos, N. F.; Economopoulos, K. P.; Fotiou, S., Endometriosis, in vitro fertilisation and the risk of gynaecological malignancies, including ovarian and breast cancer. Best Pract Res Clin Obstet Gynaecol 2010, 24, (1), 39-50. [CrossRef]
- Kobayashi, H.; Sumimoto, K.; Kitanaka, T.; Yamada, Y.; Sado, T.; Sakata, M.; Yoshida, S.; Kawaguchi, R.; Kanayama, S.; Shigetomi, H.; Haruta, S.; Tsuji, Y.; Ueda, S.; Terao, T., Ovarian endometrioma--risks factors of ovarian cancer development. Eur J Obstet Gynecol Reprod Biol 2008, 138, (2), 187-93. [CrossRef]
- Melin, A.; Sparén, P.; Persson, I.; Bergqvist, A., Endometriosis and the risk of cancer with special emphasis on ovarian cancer. Hum Reprod 2006, 21, (5), 1237-42. [CrossRef]
- Vercellini, P.; Scarfone, G.; Bolis, G.; Stellato, G.; Carinelli, S.; Crosignani, P. G., Site of origin of epithelial ovarian cancer: the endometriosis connection. BJOG 2000, 107, (9), 1155-7. [CrossRef]
- Ogawa, S.; Kaku, T.; Amada, S.; Kobayashi, H.; Hirakawa, T.; Ariyoshi, K.; Kamura, T.; Nakano, H., Ovarian endometriosis associated with ovarian carcinoma: a clinicopathological and immunohistochemical study. Gynecol Oncol 2000, 77, (2), 298-304. [CrossRef]
- Kumar, S.; Munkarah, A.; Arabi, H.; Bandyopadhyay, S.; Semaan, A.; Hayek, K.; Garg, G.; Morris, R.; Ali-Fehmi, R., Prognostic analysis of ovarian cancer associated with endometriosis. Am J Obstet Gynecol 2011, 204, (1), 63.e1-7. [CrossRef]
- Giudice, L. C., Clinical practice. Endometriosis. N Engl J Med 2010, 362, (25), 2389-98.
- Bulun, S. E., Endometriosis. N Engl J Med 2009, 360, (3), 268-79.
- Jabbour, H. N.; Kelly, R. W.; Fraser, H. M.; Critchley, H. O., Endocrine regulation of menstruation. Endocr Rev 2006, 27, (1), 17-46. [CrossRef]
- Critchley, H. O. D.; Maybin, J. A.; Armstrong, G. M.; Williams, A. R. W., Physiology of the Endometrium and Regulation of Menstruation. Physiol Rev 2020, 100, (3), 1149-1179. [CrossRef]
- Sampson, J. A., Metastatic or Embolic Endometriosis, due to the Menstrual Dissemination of Endometrial Tissue into the Venous Circulation. Am J Pathol 1927, 3, (2), 93-110.43.
- Jubanyik, K. J.; Comite, F., Extrapelvic endometriosis. Obstet Gynecol Clin North Am 1997, 24, (2), 411-40.
- Maruyama, T.; Yoshimura, Y., Stem cell theory for the pathogenesis of endometriosis. Front Biosci (Elite Ed) 2012, 4, (8), 2754-63. [CrossRef]
- Gargett, C. E., Uterine stem cells: what is the evidence? Hum Reprod Update 2007, 13, (1), 87-101.
- Maruyama, T.; Masuda, H.; Ono, M.; Kajitani, T.; Yoshimura, Y., Human uterine stem/progenitor cells: their possible role in uterine physiology and pathology. Reproduction 2010, 140, (1), 11-22. [CrossRef]
- Sasson, I. E.; Taylor, H. S., Stem cells and the pathogenesis of endometriosis. Ann N Y Acad Sci 2008, 1127, 106-15. [CrossRef]
- Du, H.; Taylor, H. S., Contribution of bone marrow-derived stem cells to endometrium and endometriosis. Stem Cells 2007, 25, (8), 2082-6. [CrossRef]
- Hufnagel, D.; Li, F.; Cosar, E.; Krikun, G.; Taylor, H. S., The Role of Stem Cells in the Etiology and Pathophysiology of Endometriosis. Semin Reprod Med 2015, 33, (5), 333-40.
- Duke, C. M.; Taylor, H. S., Stem cells and the reproductive system: historical perspective and future directions. Maturitas 2013, 76, (3), 284-9. [CrossRef]
- Nakamura, M.; Katabuchi, H.; Tohya, T.; Fukumatsu, Y.; Matsuura, K.; Okamura, H., Scanning electron microscopic and immunohistochemical studies of pelvic endometriosis. Hum Reprod 1993, 8, (12), 2218-26. [CrossRef]
- Matsuura, K.; Ohtake, H.; Katabuchi, H.; Okamura, H., Coelomic metaplasia theory of endometriosis: evidence from in vivo studies and an in vitro experimental model. Gynecol Obstet Invest 1999, 47 Suppl 1, 18-20; discussion 20-2. [CrossRef]
- Lamceva, J.; Uljanovs, R.; Strumfa, I., The Main Theories on the Pathogenesis of Endometriosis. Int J Mol Sci 2023, 24, (5). [CrossRef]
- Signorile, P. G.; Viceconte, R.; Baldi, A., New Insights in Pathogenesis of Endometriosis. Front Med (Lausanne) 2022, 9, 879015. [CrossRef]
- Stefanko, D. P.; Eskander, R.; Aisagbonhi, O., Disseminated Endometriosis and Low-Grade Endometrioid Stromal Sarcoma in a Patient with a History of Uterine Morcellation for Adenomyosis. Case Rep Obstet Gynecol 2020, 2020, 7201930. [CrossRef]
- Sepilian, V.; Della Badia, C., Iatrogenic endometriosis caused by uterine morcellation during a supracervical hysterectomy. Obstet Gynecol 2003, 102, (5 Pt 2), 1125-7.
- Cubuk, A.; Ozkaptan, O.; Neymeyer, J., Iatrogenic endometriosis following apical pelvic organ prolapse surgery: a case report. J Med Case Rep 2020, 14, (1), 3. [CrossRef]
- Rahmioglu, N.; Mortlock, S.; Ghiasi, M.; Møller, P. L.; Stefansdottir, L.; Galarneau, G.; Turman, C.; Danning, R.; Law, M. H.; Sapkota, Y.; Christofidou, P.; Skarp, S.; Giri, A.; Banasik, K.; Krassowski, M.; Lepamets, M.; Marciniak, B.; Nõukas, M.; Perro, D.; Sliz, E.; Sobalska-Kwapis, M.; Thorleifsson, G.; Topbas-Selcuki, N. F.; Vitonis, A.; Westergaard, D.; Arnadottir, R.; Burgdorf, K. S.; Campbell, A.; Cheuk, C. S. K.; Clementi, C.; Cook, J.; De Vivo, I.; DiVasta, A.; Dorien, O.; Donoghue, J. F.; Edwards, T.; Fontanillas, P.; Fung, J. N.; Geirsson, R. T.; Girling, J. E.; Harkki, P.; Harris, H. R.; Healey, M.; Heikinheimo, O.; Holdsworth-Carson, S.; Hostettler, I. C.; Houlden, H.; Houshdaran, S.; Irwin, J. C.; Jarvelin, M. R.; Kamatani, Y.; Kennedy, S. H.; Kepka, E.; Kettunen, J.; Kubo, M.; Kulig, B.; Kurra, V.; Laivuori, H.; Laufer, M. R.; Lindgren, C. M.; MacGregor, S.; Mangino, M.; Martin, N. G.; Matalliotaki, C.; Matalliotakis, M.; Murray, A. D.; Ndungu, A.; Nezhat, C.; Olsen, C. M.; Opoku-Anane, J.; Padmanabhan, S.; Paranjpe, M.; Peters, M.; Polak, G.; Porteous, D. J.; Rabban, J.; Rexrode, K. M.; Romanowicz, H.; Saare, M.; Saavalainen, L.; Schork, A. J.; Sen, S.; Shafrir, A. L.; Siewierska-Górska, A.; Słomka, M.; Smith, B. H.; Smolarz, B.; Szaflik, T.; Szyłło, K.; Takahashi, A.; Terry, K. L.; Tomassetti, C.; Treloar, S. A.; Vanhie, A.; Vincent, K.; Vo, K. C.; Werring, D. J.; Zeggini, E.; Zervou, M. I.; Adachi, S.; Buring, J. E.; Ridker, P. M.; D'Hooghe, T.; Goulielmos, G. N.; Hapangama, D. K.; Hayward, C.; Horne, A. W.; Low, S. K.; Martikainen, H.; Chasman, D. I.; Rogers, P. A. W.; Saunders, P. T.; Sirota, M.; Spector, T.; Strapagiel, D.; Tung, J. Y.; Whiteman, D. C.; Giudice, L. C.; Velez-Edwards, D. R.; Uimari, O.; Kraft, P.; Salumets, A.; Nyholt, D. R.; Mägi, R.; Stefansson, K.; Becker, C. M.; Yurttas-Beim, P.; Steinthorsdottir, V.; Nyegaard, M.; Missmer, S. A.; Montgomery, G. W.; Morris, A. P.; Zondervan, K. T.; Consortium, D. G.; Study, F.; Taskforce, F. E.; Team, C. R.; Team, a. R., The genetic basis of endometriosis and comorbidity with other pain and inflammatory conditions. Nat Genet 2023, 55, (3), 423-436. [CrossRef]
- Bedrick, B. S.; Courtright, L.; Zhang, J.; Snow, M.; Amendola, I. L. S.; Nylander, E.; Cayton-Vaught, K.; Segars, J.; Singh, B., A Systematic Review of Epigenetics of Endometriosis. F S Rev 2024, 5, (1). [CrossRef]
- Pagliardini, L.; Gentilini, D.; Sanchez, A. M.; Candiani, M.; Viganò, P.; Di Blasio, A. M., Replication and meta-analysis of previous genome-wide association studies confirm vezatin as the locus with the strongest evidence for association with endometriosis. Hum Reprod 2015, 30, (4), 987-93. [CrossRef]
- Edwards, M. J., Functional neurological disorder: lighting the way to a new paradigm for medicine. Brain 2021, 144, (11), 3279-3282. [CrossRef]
- Laganà, A. S.; Condemi, I.; Retto, G.; Muscatello, M. R.; Bruno, A.; Zoccali, R. A.; Triolo, O.; Cedro, C., Analysis of psychopathological comorbidity behind the common symptoms and signs of endometriosis. Eur J Obstet Gynecol Reprod Biol 2015, 194, 30-3. [CrossRef]
- Kroenke, K., Patients presenting with somatic complaints: epidemiology, psychiatric comorbidity and management. Int J Methods Psychiatr Res 2003, 12, (1), 34-43. [CrossRef]
- Delanerolle, G.; Ramakrishnan, R.; Hapangama, D.; Zeng, Y.; Shetty, A.; Elneil, S.; Chong, S.; Hirsch, M.; Oyewole, M.; Phiri, P.; Elliot, K.; Kothari, T.; Rogers, B.; Sandle, N.; Haque, N.; Pluchino, N.; Silem, M.; O'Hara, R.; Hull, M. L.; Majumder, K.; Shi, J. Q.; Raymont, V., A systematic review and meta-analysis of the Endometriosis and Mental-Health Sequelae; The ELEMI Project. Womens Health (Lond) 2021, 17, 17455065211019717. [CrossRef]
- Laganà, A. S.; La Rosa, V. L.; Rapisarda, A. M. C.; Valenti, G.; Sapia, F.; Chiofalo, B.; Rossetti, D.; Ban Frangež, H.; Vrtačnik Bokal, E.; Vitale, S. G., Anxiety and depression in patients with endometriosis: impact and management challenges. Int J Womens Health 2017, 9, 323-330. [CrossRef]
- Agarwal, S. K.; Foster, W. G.; Groessl, E. J., Rethinking endometriosis care: applying the chronic care model via a multidisciplinary program for the care of women with endometriosis. Int J Womens Health 2019, 11, 405-410. [CrossRef]
- Mundo-López, A.; Ocón-Hernández, O.; Lozano-Lozano, M.; San-Sebastián, A.; Fernández-Lao, C.; Galiano-Castillo, N.; Cantarero-Villanueva, I.; Arroyo-Morales, M.; Artacho-Cordón, F., Impact of symptom burden on work performance status in Spanish women diagnosed with endometriosis. Eur J Obstet Gynecol Reprod Biol 2021, 261, 92-97. [CrossRef]
- Taylor, H. S.; Kotlyar, A. M.; Flores, V. A., Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet 2021, 397, (10276), 839-852. [CrossRef]
- McPeak, A. E.; Allaire, C.; Williams, C.; Albert, A.; Lisonkova, S.; Yong, P. J., Pain Catastrophizing and Pain Health-Related Quality-of-Life in Endometriosis. Clin J Pain 2018, 34, (4), 349-356. [CrossRef]
- Maulenkul, T.; Kuandyk, A.; Makhadiyeva, D.; Dautova, A.; Terzic, M.; Oshibayeva, A.; Moldaliyev, I.; Ayazbekov, A.; Maimakov, T.; Saruarov, Y.; Foster, F.; Sarria-Santamera, A., Understanding the impact of endometriosis on women's life: an integrative review of systematic reviews. BMC Womens Health 2024, 24, (1), 524. [CrossRef]
- Della Corte, L.; Di Filippo, C.; Gabrielli, O.; Reppuccia, S.; La Rosa, V. L.; Ragusa, R.; Fichera, M.; Commodari, E.; Bifulco, G.; Giampaolino, P., The Burden of Endometriosis on Women's Lifespan: A Narrative Overview on Quality of Life and Psychosocial Wellbeing. Int J Environ Res Public Health 2020, 17, (13). [CrossRef]
- Pontoppidan, K.; Olovsson, M.; Grundström, H., Clinical factors associated with quality of life among women with endometriosis: a cross-sectional study. BMC Womens Health 2023, 23, (1), 551. [CrossRef]
- Gete, D. G.; Doust, J.; Mortlock, S.; Montgomery, G.; Mishra, G. D., Impact of endometriosis on women's health-related quality of life: A national prospective cohort study. Maturitas 2023, 174, 1-7. [CrossRef]
- Warzecha, D.; Szymusik, I.; Wielgos, M.; Pietrzak, B., The Impact of Endometriosis on the Quality of Life and the Incidence of Depression-A Cohort Study. Int J Environ Res Public Health 2020, 17, (10). [CrossRef]
- Leuenberger, J.; Kohl Schwartz, A. S.; Geraedts, K.; Haeberlin, F.; Eberhard, M.; von Orellie, S.; Imesch, P.; Leeners, B., Living with endometriosis: Comorbid pain disorders, characteristics of pain and relevance for daily life. Eur J Pain 2022, 26, (5), 1021-1038. [CrossRef]
- Linton, S. J.; Shaw, W. S., Impact of psychological factors in the experience of pain. Phys Ther 2011, 91, (5), 700-11. [CrossRef]
- Gerdle, B.; Åkerblom, S.; Brodda Jansen, G.; Enthoven, P.; Ernberg, M.; Dong, H. J.; Stålnacke, B. M.; Äng, B. O.; Boersma, K., Who benefits from multimodal rehabilitation - an exploration of pain, psychological distress, and life impacts in over 35,000 chronic pain patients identified in the Swedish Quality Registry for Pain Rehabilitation. J Pain Res 2019, 12, 891-908. [CrossRef]
- Evans, S.; Fernandez, S.; Olive, L.; Payne, L. A.; Mikocka-Walus, A., Psychological and mind-body interventions for endometriosis: A systematic review. J Psychosom Res 2019, 124, 109756. [CrossRef]
- Buggio, L.; Barbara, G.; Facchin, F.; Frattaruolo, M. P.; Aimi, G.; Berlanda, N., Self-management and psychological-sexological interventions in patients with endometriosis: strategies, outcomes, and integration into clinical care. Int J Womens Health 2017, 9, 281-293. [CrossRef]
- van Aken, M. A. W.; Oosterman, J. M.; van Rijn, C. M.; Ferdek, M. A.; Ruigt, G. S. F.; Peeters, B. W. M. M.; Braat, D. D. M.; Nap, A. W., Pain cognition versus pain intensity in patients with endometriosis: toward personalized treatment. Fertil Steril 2017, 108, (4), 679-686. [CrossRef]
- Dancet, E. A.; Apers, S.; Kremer, J. A.; Nelen, W. L.; Sermeus, W.; D'Hooghe, T. M., The patient-centeredness of endometriosis care and targets for improvement: a systematic review. Gynecol Obstet Invest 2014, 78, (2), 69-80. [CrossRef]
- Grundström, H.; Kilander, H.; Wikman, P.; Olovsson, M., Demographic and clinical characteristics determining patient-centeredness in endometriosis care. Arch Gynecol Obstet 2023, 307, (4), 1047-1055. [CrossRef]
- Boersen, Z.; de Kok, L.; van der Zanden, M.; Braat, D.; Oosterman, J.; Nap, A., Patients' perspective on cognitive behavioural therapy after surgical treatment of endometriosis: a qualitative study. Reprod Biomed Online 2021, 42, (4), 819-825. [CrossRef]
- Aerts, L.; Grangier, L.; Streuli, I.; Dällenbach, P.; Marci, R.; Wenger, J. M.; Pluchino, N., Psychosocial impact of endometriosis: From co-morbidity to intervention. Best Pract Res Clin Obstet Gynaecol 2018, 50, 2-10. [CrossRef]
- Kennedy, S.; Bergqvist, A.; Chapron, C.; D'Hooghe, T.; Dunselman, G.; Greb, R.; Hummelshoj, L.; Prentice, A.; Saridogan, E.; Group, E. S. I. G. f. E. a. E. G. D., ESHRE guideline for the diagnosis and treatment of endometriosis. Hum Reprod 2005, 20, (10), 2698-704. [CrossRef]
- Soliman, A. M.; Coyne, K. S.; Zaiser, E.; Castelli-Haley, J.; Fuldeore, M. J., The burden of endometriosis symptoms on health-related quality of life in women in the United States: a cross-sectional study. J Psychosom Obstet Gynaecol 2017, 38, (4), 238-248. [CrossRef]
- Vannuccini, S.; Clemenza, S.; Rossi, M.; Petraglia, F., Hormonal treatments for endometriosis: The endocrine background. Rev Endocr Metab Disord 2022, 23, (3), 333-355. [CrossRef]
- Exacoustos, C.; Malzoni, M.; Di Giovanni, A.; Lazzeri, L.; Tosti, C.; Petraglia, F.; Zupi, E., Ultrasound mapping system for the surgical management of deep infiltrating endometriosis. Fertil Steril 2014, 102, (1), 143-150.e2. [CrossRef]
- Nisolle, M.; Donnez, J., Peritoneal endometriosis, ovarian endometriosis, and adenomyotic nodules of the rectovaginal septum are three different entities. Fertil Steril 1997, 68, (4), 585-96.
- O'Brien, T. J.; Beard, J. B.; Underwood, L. J.; Shigemasa, K., The CA 125 gene: a newly discovered extension of the glycosylated N-terminal domain doubles the size of this extracellular superstructure. Tumour Biol 2002, 23, (3), 154-69.
- Yin, B. W.; Lloyd, K. O., Molecular cloning of the CA125 ovarian cancer antigen: identification as a new mucin, MUC16. J Biol Chem 2001, 276, (29), 27371-5.
- Barbieri, R. L.; Niloff, J. M.; Bast, R. C.; Scaetzl, E.; Kistner, R. W.; Knapp, R. C., Elevated serum concentrations of CA-125 in patients with advanced endometriosis. Fertil Steril 1986, 45, (5), 630-4. [CrossRef]
- Anfosso, F.; Bardin, N.; Vivier, E.; Sabatier, F.; Sampol, J.; Dignat-George, F., Outside-in signaling pathway linked to CD146 engagement in human endothelial cells. J Biol Chem 2001, 276, (2), 1564-9. [CrossRef]
- Johnson, J. P.; Rothbächer, U.; Sers, C., The progression associated antigen MUC18: a unique member of the immunoglobulin supergene family. Melanoma Res 1993, 3, (5), 337-40.
- Leñero, C.; Kaplan, L. D.; Best, T. M.; Kouroupis, D., CD146+ Endometrial-Derived Mesenchymal Stem/Stromal Cell Subpopulation Possesses Exosomal Secretomes with Strong Immunomodulatory miRNA Attributes. Cells 2022, 11, (24). [CrossRef]
- Hilage, P.; Birajdar, A.; Marsale, T.; Patil, D.; Patil, A. M.; Telang, G.; Somasundaram, I.; Sharma, R. K.; Joshi, M. G., Characterization and angiogenic potential of CD146. Stem Cell Res Ther 2024, 15, (1), 330. [CrossRef]
- Chiu, P. C.; Koistinen, R.; Koistinen, H.; Seppala, M.; Lee, K. F.; Yeung, W. S., Zona-binding inhibitory factor-1 from human follicular fluid is an isoform of glycodelin. Biol Reprod 2003, 69, (1), 365-72. [CrossRef]
- Loukovaara, S.; Immonen, I. R.; Loukovaara, M. J.; Koistinen, R.; Kaaja, R. J., Glycodelin: a novel serum anti-inflammatory marker in type 1 diabetic retinopathy during pregnancy. Acta Ophthalmol Scand 2007, 85, (1), 46-9. [CrossRef]
- Oehninger, S.; Coddington, C. C.; Hodgen, G. D.; Seppala, M., Factors affecting fertilization: endometrial placental protein 14 reduces the capacity of human spermatozoa to bind to the human zona pellucida. Fertil Steril 1995, 63, (2), 377-83. [CrossRef]
- Rachmilewitz, J.; Riely, G. J.; Tykocinski, M. L., Placental protein 14 functions as a direct T-cell inhibitor. Cell Immunol 1999, 191, (1), 26-33. [CrossRef]
- Chiu, P. C.; Chung, M. K.; Koistinen, R.; Koistinen, H.; Seppala, M.; Ho, P. C.; Ng, E. H.; Lee, K. F.; Yeung, W. S., Cumulus oophorus-associated glycodelin-C displaces sperm-bound glycodelin-A and -F and stimulates spermatozoa-zona pellucida binding. J Biol Chem 2007, 282, (8), 5378-88. [CrossRef]
- Chiu, P. C.; Chung, M. K.; Tsang, H. Y.; Koistinen, R.; Koistinen, H.; Seppala, M.; Lee, K. F.; Yeung, W. S., Glycodelin-S in human seminal plasma reduces cholesterol efflux and inhibits capacitation of spermatozoa. J Biol Chem 2005, 280, (27), 25580-9. [CrossRef]
- Moore, R. G.; McMeekin, D. S.; Brown, A. K.; DiSilvestro, P.; Miller, M. C.; Allard, W. J.; Gajewski, W.; Kurman, R.; Bast, R. C.; Skates, S. J., A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol 2009, 112, (1), 40-6. [CrossRef]
- Drapkin, R.; von Horsten, H. H.; Lin, Y.; Mok, S. C.; Crum, C. P.; Welch, W. R.; Hecht, J. L., Human epididymis protein 4 (HE4) is a secreted glycoprotein that is overexpressed by serous and endometrioid ovarian carcinomas. Cancer Res 2005, 65, (6), 2162-9.
- Kang, S.; Tanaka, T.; Narazaki, M.; Kishimoto, T., Targeting Interleukin-6 Signaling in Clinic. Immunity 2019, 50, (4), 1007-1023. [CrossRef]
- Bedaiwy, M. A.; Falcone, T.; Goldberg, J. M.; Sharma, R. K.; Nelson, D. R.; Agarwal, A., Peritoneal fluid leptin is associated with chronic pelvic pain but not infertility in endometriosis patients. Hum Reprod 2006, 21, (3), 788-91. [CrossRef]
- Li, Y.; Huang, X.; Guo, F.; Lei, T.; Li, S.; Monaghan-Nichols, P.; Jiang, Z.; Xin, H. B.; Fu, M., TRIM65 E3 ligase targets VCAM-1 degradation to limit LPS-induced lung inflammation. J Mol Cell Biol 2020, 12, (3), 190-201. [CrossRef]
- Taooka, Y.; Chen, J.; Yednock, T.; Sheppard, D., The integrin alpha9beta1 mediates adhesion to activated endothelial cells and transendothelial neutrophil migration through interaction with vascular cell adhesion molecule-1. J Cell Biol 1999, 145, (2), 413-20. [CrossRef]
- Marchese, M. E.; Berdnikovs, S.; Cook-Mills, J. M., Distinct sites within the vascular cell adhesion molecule-1 (VCAM-1) cytoplasmic domain regulate VCAM-1 activation of calcium fluxes versus Rac1 during leukocyte transendothelial migration. Biochemistry 2012, 51, (41), 8235-46. [CrossRef]
- Chu, X.; Qin, X.; Xu, H.; Li, L.; Wang, Z.; Li, F.; Xie, X.; Zhou, H.; Shen, Y.; Long, J., Structural insights into Paf1 complex assembly and histone binding. Nucleic Acids Res 2013, 41, (22), 10619-29. [CrossRef]
- Zhang, J.; Li, H.; Yi, D.; Lai, C.; Wang, H.; Zou, W.; Cao, B., Knockdown of vascular cell adhesion molecule 1 impedes transforming growth factor beta 1-mediated proliferation, migration, and invasion of endometriotic cyst stromal cells. Reprod Biol Endocrinol 2019, 17, (1), 69. [CrossRef]
- Chung, M. S.; Han, S. J., Endometriosis-Associated Angiogenesis and Anti-angiogenic Therapy for Endometriosis. Front Glob Womens Health 2022, 3, 856316. [CrossRef]
- Arici, A.; Oral, E.; Attar, E.; Tazuke, S. I.; Olive, D. L., Monocyte chemotactic protein-1 concentration in peritoneal fluid of women with endometriosis and its modulation of expression in mesothelial cells. Fertil Steril 1997, 67, (6), 1065-72. [CrossRef]
- Jolicoeur, C.; Boutouil, M.; Drouin, R.; Paradis, I.; Lemay, A.; Akoum, A., Increased expression of monocyte chemotactic protein-1 in the endometrium of women with endometriosis. Am J Pathol 1998, 152, (1), 125-33.
- Anastasiu, C. V.; Moga, M. A.; Elena Neculau, A.; Bălan, A.; Scârneciu, I.; Dragomir, R. M.; Dull, A. M.; Chicea, L. M., Biomarkers for the Noninvasive Diagnosis of Endometriosis: State of the Art and Future Perspectives. Int J Mol Sci 2020, 21, (5). [CrossRef]
- Harada, T.; Kubota, T.; Aso, T., Usefulness of CA19-9 versus CA125 for the diagnosis of endometriosis. Fertil Steril 2002, 78, (4), 733-9. [CrossRef]
- Shen, A.; Xu, S.; Ma, Y.; Guo, H.; Li, C.; Yang, C.; Zou, S., Diagnostic value of serum CA125, CA19-9 and CA15-3 in endometriosis: A meta-analysis. J Int Med Res 2015, 43, (5), 599-609. [CrossRef]
- Chantalat, E.; Valera, M. C.; Vaysse, C.; Noirrit, E.; Rusidze, M.; Weyl, A.; Vergriete, K.; Buscail, E.; Lluel, P.; Fontaine, C.; Arnal, J. F.; Lenfant, F., Estrogen Receptors and Endometriosis. Int J Mol Sci 2020, 21, (8).
- Chen, S.; Liu, Y.; Zhong, Z.; Wei, C.; Zhu, X., Peritoneal immune microenvironment of endometriosis: Role and therapeutic perspectives. Front Immunol 2023, 14, 1134663. [CrossRef]
- Vercellini, P.; Buggio, L.; Frattaruolo, M. P.; Borghi, A.; Dridi, D.; Somigliana, E., Medical treatment of endometriosis-related pain. Best Pract Res Clin Obstet Gynaecol 2018, 51, 68-91. [CrossRef]
- Becker, C. M.; Bokor, A.; Heikinheimo, O.; Horne, A.; Jansen, F.; Kiesel, L.; King, K.; Kvaskoff, M.; Nap, A.; Petersen, K.; Saridogan, E.; Tomassetti, C.; van Hanegem, N.; Vulliemoz, N.; Vermeulen, N.; Group, E. E. G., ESHRE guideline: endometriosis. Hum Reprod Open 2022, 2022, (2), hoac009. [CrossRef]
- Casper, R. F., Progestin-only pills may be a better first-line treatment for endometriosis than combined estrogen-progestin contraceptive pills. Fertil Steril 2017, 107, (3), 533-536. [CrossRef]
- Vercellini, P.; Bracco, B.; Mosconi, P.; Roberto, A.; Alberico, D.; Dhouha, D.; Somigliana, E., Norethindrone acetate or dienogest for the treatment of symptomatic endometriosis: a before and after study. Fertil Steril 2016, 105, (3), 734-743.e3. [CrossRef]
- Surrey, E. S., GnRH agonists in the treatment of symptomatic endometriosis: a review. F S Rep 2023, 4, (2 Suppl), 40-45. [CrossRef]
- Wang, P. H.; Yang, S. T.; Chang, W. H.; Liu, C. H.; Lee, F. K.; Lee, W. L., Endometriosis: Part I. Basic concept. Taiwan J Obstet Gynecol 2022, 61, (6), 927-934.
- Saridogan, E.; Becker, C. M.; Feki, A.; Grimbizis, G. F.; Hummelshoj, L.; Keckstein, J.; Nisolle, M.; Tanos, V.; Ulrich, U. A.; Vermeulen, N.; De Wilde, R. L.; Working group of ESGE, E. S. H. R., and WES, Recommendations for the surgical treatment of endometriosis-part 1: ovarian endometrioma. Gynecol Surg 2017, 14, (1), 27. [CrossRef]
- Imperiale, L.; Nisolle, M.; Noël, J. C.; Fastrez, M., Three Types of Endometriosis: Pathogenesis, Diagnosis and Treatment. State of the Art. J Clin Med 2023, 12, (3). [CrossRef]
- Sanchez, A. M.; Viganò, P.; Somigliana, E.; Panina-Bordignon, P.; Vercellini, P.; Candiani, M., The distinguishing cellular and molecular features of the endometriotic ovarian cyst: from pathophysiology to the potential endometrioma-mediated damage to the ovary. Hum Reprod Update 2014, 20, (2), 217-30. [CrossRef]
- Falik, R. C.; Li, A.; Farrimond, F.; Meshkat Razavi, G.; Nezhat, C.; Nezhat, F., Endometrios: classification and surgical management. OBG Manag 2017, 29, 38–43.
- Castellarnau Visus, M.; Ponce Sebastia, J.; Carreras Collado, R.; Cayuela Font, E.; Garcia Tejedor, A., Preliminary results: ethanol sclerotherapy after ultrasound-guided fine needle aspiration without anesthesia in the management of simple ovarian cysts. J Minim Invasive Gynecol 2015, 22, (3), 475-82. [CrossRef]
- Hsieh, C. L.; Shiau, C. S.; Lo, L. M.; Hsieh, T. T.; Chang, M. Y., Effectiveness of ultrasound-guided aspiration and sclerotherapy with 95% ethanol for treatment of recurrent ovarian endometriomas. Fertil Steril 2009, 91, (6), 2709-13. [CrossRef]
- Zondervan, K. T.; Becker, C. M.; Missmer, S. A., Endometriosis. N Engl J Med 2020, 382, (13), 1244-1256.
- Clower, L.; Fleshman, T.; Geldenhuys, W. J.; Santanam, N., Targeting Oxidative Stress Involved in Endometriosis and Its Pain. Biomolecules 2022, 12, (8). [CrossRef]
- Salehi, B.; Butnariu, M.; Corneanu, M.; Sarac, I.; Vlaisavljevic, S.; Kitic, D.; Rahavian, A.; Abedi, A.; Karkan, M. F.; Bhatt, I. D.; Jantwal, A.; Sharifi-Rad, J.; Rodrigues, C. F.; Martorell, M.; Martins, N., Chronic pelvic pain syndrome: Highlighting medicinal plants toward biomolecules discovery for upcoming drugs formulation. Phytother Res 2020, 34, (4), 769-787. [CrossRef]
- Chowdhury, I.; Banerjee, S.; Driss, A.; Xu, W.; Mehrabi, S.; Nezhat, C.; Sidell, N.; Taylor, R. N.; Thompson, W. E., Curcumin attenuates proangiogenic and proinflammatory factors in human eutopic endometrial stromal cells through the NF-κB signaling pathway. J Cell Physiol 2019, 234, (5), 6298-6312. [CrossRef]
- Cao, W. G.; Morin, M.; Metz, C.; Maheux, R.; Akoum, A., Stimulation of macrophage migration inhibitory factor expression in endometrial stromal cells by interleukin 1, beta involving the nuclear transcription factor NFkappaB. Biol Reprod 2005, 73, (3), 565-70. [CrossRef]
- Cao, H.; Wei, Y. X.; Zhou, Q.; Zhang, Y.; Guo, X. P.; Zhang, J., Inhibitory effect of curcumin in human endometriosis endometrial cells via downregulation of vascular endothelial growth factor. Mol Med Rep 2017, 16, (4), 5611-5617. [CrossRef]
- Markowska, A.; Antoszczak, M.; Markowska, J.; Huczyński, A., The Role of Selected Dietary Factors in the Development and Course of Endometriosis. Nutrients 2023, 15, (12). [CrossRef]
- Hipólito-Reis, M.; Neto, A. C.; Neves, D., Impact of curcumin, quercetin, or resveratrol on the pathophysiology of endometriosis: A systematic review. Phytother Res 2022, 36, (6), 2416-2433. [CrossRef]
- Farzaei, M. H.; Bahramsoltani, R.; Rahimi, R., Phytochemicals as Adjunctive with Conventional Anticancer Therapies. Curr Pharm Des 2016, 22, (27), 4201-18. [CrossRef]
- Ricci, A. G.; Olivares, C. N.; Bilotas, M. A.; Bastón, J. I.; Singla, J. J.; Meresman, G. F.; Barañao, R. I., Natural therapies assessment for the treatment of endometriosis. Hum Reprod 2013, 28, (1), 178-88. [CrossRef]
- Wang, C. C.; Xu, H.; Man, G. C.; Zhang, T.; Chu, K. O.; Chu, C. Y.; Cheng, J. T.; Li, G.; He, Y. X.; Qin, L.; Lau, T. S.; Kwong, J.; Chan, T. H., Prodrug of green tea epigallocatechin-3-gallate (Pro-EGCG) as a potent anti-angiogenesis agent for endometriosis in mice. Angiogenesis 2013, 16, (1), 59-69. [CrossRef]
- Delenko, J.; Xue, X.; Chatterjee, P. K.; Hyman, N.; Shih, A. J.; Adelson, R. P.; Safaric Tepes, P.; Gregersen, P. K.; Metz, C. N., Quercetin enhances decidualization through AKT-ERK-p53 signaling and supports a role for senescence in endometriosis. Reprod Biol Endocrinol 2024, 22, (1), 100. [CrossRef]
- Cao, Y.; Zhuang, M. F.; Yang, Y.; Xie, S. W.; Cui, J. G.; Cao, L.; Zhang, T. T.; Zhu, Y., Preliminary study of quercetin affecting the hypothalamic-pituitary-gonadal axis on rat endometriosis model. Evid Based Complement Alternat Med 2014, 2014, 781684. [CrossRef]
- Jamali, N.; Zal, F.; Mostafavi-Pour, Z.; Samare-Najaf, M.; Poordast, T.; Dehghanian, A., Ameliorative Effects of Quercetin and Metformin and Their Combination Against Experimental Endometriosis in Rats. Reprod Sci 2021, 28, (3), 683-692. [CrossRef]
- Zaurito, A.; Mehmeti, I.; Limongelli, F.; Zupo, R.; Annunziato, A.; Fontana, S.; Tardugno, R., Natural compounds for endometriosis and related chronic pelvic pain: A review. Fitoterapia 2024, 179, 106277. [CrossRef]
- Ilhan, M.; Ali, Z.; Khan, I. A.; Taştan, H.; Küpeli Akkol, E., The regression of endometriosis with glycosylated flavonoids isolated from Melilotus officinalis (L.) Pall. in an endometriosis rat model. Taiwan J Obstet Gynecol 2020, 59, (2), 211-219. [CrossRef]
- Ilhan, M.; Ali, Z.; Khan, I. A.; Taştan, H.; Küpeli Akkol, E., Bioactivity-guided isolation of flavonoids from Urtica dioica L. and their effect on endometriosis rat model. J Ethnopharmacol 2019, 243, 112100. [CrossRef]
- Kohama, T.; Herai, K.; Inoue, M., Effect of French maritime pine bark extract on endometriosis as compared with leuprorelin acetate. J Reprod Med 2007, 52, (8), 703-8.
- Kim, J. H.; Woo, J. H.; Kim, H. M.; Oh, M. S.; Jang, D. S.; Choi, J. H., Anti-Endometriotic Effects of Pueraria Flower Extract in Human Endometriotic Cells and Mice. Nutrients 2017, 9, (3).
- Park, W.; Park, M. Y.; Song, G.; Lim, W., 5,7-Dimethoxyflavone induces apoptotic cell death in human endometriosis cell lines by activating the endoplasmic reticulum stress pathway. Phytother Res 2020, 34, (9), 2275-2286. [CrossRef]
- Park, S.; Song, G.; Lim, W., Myricetin inhibits endometriosis growth through cyclin E1 down-regulation in vitro and in vivo. J Nutr Biochem 2020, 78, 108328. [CrossRef]
- Zhang, Y. Y.; Li, M. Z.; Shen, H. H.; Abudukeyoumu, A.; Xie, F.; Ye, J. F.; Xu, F. Y.; Sun, J. S.; Li, M. Q., Ginsenosides in endometrium-related diseases: Emerging roles and mechanisms. Biomed Pharmacother 2023, 166, 115340. [CrossRef]
- Uchendu, E.; Shukla, M.; Reed, B.; Brown, D.; Saxena, P.; MooYoung, M., Improvement of Ginseng by <i>In Vitro</i> Culture: Challenges and Opportunities. Comprehensive Biotechnology, Vol 4: Agricultural and Related Biotechnologies, 2nd Edition 2011, 317-329.
- Norooznezhad, A. H.; Norooznezhad, F., Cannabinoids: Possible agents for treatment of psoriasis via suppression of angiogenesis and inflammation. Med Hypotheses 2017, 99, 15-18. [CrossRef]
- Brunetti, P.; Lo Faro, A. F.; Pirani, F.; Berretta, P.; Pacifici, R.; Pichini, S.; Busardò, F. P., Pharmacology and legal status of cannabidiol. Ann Ist Super Sanita 2020, 56, (3), 285-291. [CrossRef]
- Kogan, N. M.; Blázquez, C.; Alvarez, L.; Gallily, R.; Schlesinger, M.; Guzmán, M.; Mechoulam, R., A cannabinoid quinone inhibits angiogenesis by targeting vascular endothelial cells. Mol Pharmacol 2006, 70, (1), 51-9. [CrossRef]
- Solinas, M.; Massi, P.; Cantelmo, A. R.; Cattaneo, M. G.; Cammarota, R.; Bartolini, D.; Cinquina, V.; Valenti, M.; Vicentini, L. M.; Noonan, D. M.; Albini, A.; Parolaro, D., Cannabidiol inhibits angiogenesis by multiple mechanisms. Br J Pharmacol 2012, 167, (6), 1218-31. [CrossRef]
- Anvari Aliabad, R.; Hassanpour, K.; Norooznezhad, A. H., Cannabidiol as a possible treatment for endometriosis through suppression of inflammation and angiogenesis. Immun Inflamm Dis 2024, 12, (8), e1370. [CrossRef]
- Alagawany, M.; Abd El-Hack, M. E.; Farag, M. R.; Gopi, M.; Karthik, K.; Malik, Y. S.; Dhama, K., Rosmarinic acid: modes of action, medicinal values and health benefits. Anim Health Res Rev 2017, 18, (2), 167-176. [CrossRef]
- Adomako-Bonsu, A. G.; Chan, S. L.; Pratten, M.; Fry, J. R., Antioxidant activity of rosmarinic acid and its principal metabolites in chemical and cellular systems: Importance of physico-chemical characteristics. Toxicol In Vitro 2017, 40, 248-255. [CrossRef]
- Baba, S.; Osakabe, N.; Natsume, M.; Terao, J., Orally administered rosmarinic acid is present as the conjugated and/or methylated forms in plasma, and is degraded and metabolized to conjugated forms of caffeic acid, ferulic acid and m-coumaric acid. Life Sci 2004, 75, (2), 165-78. [CrossRef]
- Baba, S.; Osakabe, N.; Natsume, M.; Yasuda, A.; Muto, Y.; Hiyoshi, K.; Takano, H.; Yoshikawa, T.; Terao, J., Absorption, metabolism, degradation and urinary excretion of rosmarinic acid after intake of Perilla frutescens extract in humans. Eur J Nutr 2005, 44, (1), 1-9.
- Ferella, L.; Bastón, J. I.; Bilotas, M. A.; Singla, J. J.; González, A. M.; Olivares, C. N.; Meresman, G. F., Active compounds present inRosmarinus officinalis leaves andScutellaria baicalensis root evaluated as new therapeutic agents for endometriosis. Reprod Biomed Online 2018, 37, (6), 769-782. [CrossRef]
- Holzer, P., Capsaicin: cellular targets, mechanisms of action, and selectivity for thin sensory neurons. Pharmacol Rev 1991, 43, (2), 143-201. [CrossRef]
- Szallasi, A.; Blumberg, P. M., Vanilloid (Capsaicin) receptors and mechanisms. Pharmacol Rev 1999, 51, (2), 159-212. [CrossRef]
- Wang, H.; Bolognese, J.; Calder, N.; Baxendale, J.; Kehler, A.; Cummings, C.; Connell, J.; Herman, G., Effect of morphine and pregabalin compared with diphenhydramine hydrochloride and placebo on hyperalgesia and allodynia induced by intradermal capsaicin in healthy male subjects. J Pain 2008, 9, (12), 1088-95. [CrossRef]
- Wallace, M.; Duan, R.; Liu, W.; Locke, C.; Nothaft, W., A Randomized, Double-Blind, Placebo-Controlled, Crossover Study of the T-Type Calcium Channel Blocker ABT-639 in an Intradermal Capsaicin Experimental Pain Model in Healthy Adults. Pain Med 2016, 17, (3), 551-560. [CrossRef]
- Lembeck, F., Columbus, Capsicum and capsaicin: past, present and future. Acta Physiol Hung 1987, 69, (3-4), 265-73.
- Watson, C. P., Topical capsaicin as an adjuvant analgesic. J Pain Symptom Manage 1994, 9, (7), 425-33. [CrossRef]
- Arora, V.; Campbell, J. N.; Chung, M. K., Fight fire with fire: Neurobiology of capsaicin-induced analgesia for chronic pain. Pharmacol Ther 2021, 220, 107743. [CrossRef]
- Basith, S.; Cui, M.; Hong, S.; Choi, S., Harnessing the Therapeutic Potential of Capsaicin and Its Analogues in Pain and Other Diseases. Molecules 2016, 21, (8). [CrossRef]
- Fattori, V.; Hohmann, M. S.; Rossaneis, A. C.; Pinho-Ribeiro, F. A.; Verri, W. A., Capsaicin: Current Understanding of Its Mechanisms and Therapy of Pain and Other Pre-Clinical and Clinical Uses. Molecules 2016, 21, (7). [CrossRef]
- Qiu, Y.; Yuan, S.; Wang, H., Vitamin D status in endometriosis: a systematic review and meta-analysis. Arch Gynecol Obstet 2020, 302, (1), 141-152. [CrossRef]
- Delbandi, A. A.; Torab, M.; Abdollahi, E.; Khodaverdi, S.; Rokhgireh, S.; Moradi, Z.; Heidari, S.; Mohammadi, T., Vitamin D deficiency as a risk factor for endometriosis in Iranian women. J Reprod Immunol 2021, 143, 103266. [CrossRef]
- Yarmolinskaya, M.; Denisova, A.; Tkachenko, N.; Ivashenko, T.; Bespalova, O.; Tolibova, G.; Tral, T., Vitamin D significance in pathogenesis of endometriosis. Gynecol Endocrinol 2021, 37, (sup1), 40-43. [CrossRef]
- Harris, H. R.; Chavarro, J. E.; Malspeis, S.; Willett, W. C.; Missmer, S. A., Dairy-food, calcium, magnesium, and vitamin D intake and endometriosis: a prospective cohort study. Am J Epidemiol 2013, 177, (5), 420-30. [CrossRef]
- Miyashita, M.; Koga, K.; Izumi, G.; Sue, F.; Makabe, T.; Taguchi, A.; Nagai, M.; Urata, Y.; Takamura, M.; Harada, M.; Hirata, T.; Hirota, Y.; Wada-Hiraike, O.; Fujii, T.; Osuga, Y., Effects of 1,25-Dihydroxy Vitamin D3 on Endometriosis. J Clin Endocrinol Metab 2016, 101, (6), 2371-9. [CrossRef]
- Baek, J. C.; Jo, J. Y.; Lee, S. M.; Cho, I. A.; Shin, J. K.; Lee, S. A.; Lee, J. H.; Cho, M. C.; Choi, W. J., Differences in 25-hydroxy vitamin D and vitamin D-binding protein concentrations according to the severity of endometriosis. Clin Exp Reprod Med 2019, 46, (3), 125-131. [CrossRef]
- Somigliana, E.; Panina-Bordignon, P.; Murone, S.; Di Lucia, P.; Vercellini, P.; Vigano, P., Vitamin D reserve is higher in women with endometriosis. Hum Reprod 2007, 22, (8), 2273-8. [CrossRef]
- Mier-Cabrera, J.; Aburto-Soto, T.; Burrola-Méndez, S.; Jiménez-Zamudio, L.; Tolentino, M. C.; Casanueva, E.; Hernández-Guerrero, C., Women with endometriosis improved their peripheral antioxidant markers after the application of a high antioxidant diet. Reprod Biol Endocrinol 2009, 7, 54. [CrossRef]
- Hoorsan, H.; Simbar, M.; Tehrani, F. R.; Fathi, F.; Mosaffa, N.; Riazi, H.; Akradi, L.; Nasseri, S.; Bazrafkan, S., The effectiveness of antioxidant therapy (vitamin C) in an experimentally induced mouse model of ovarian endometriosis. Womens Health (Lond) 2022, 18, 17455057221096218. [CrossRef]
- Erten, O. U.; Ensari, T. A.; Dilbaz, B.; Cakiroglu, H.; Altinbas, S. K.; Çaydere, M.; Goktolga, U., Vitamin C is effective for the prevention and regression of endometriotic implants in an experimentally induced rat model of endometriosis. Taiwan J Obstet Gynecol 2016, 55, (2), 251-7. [CrossRef]
- Ansariniya, H.; Hadinedoushan, H.; Javaheri, A.; Zare, F., Vitamin C and E supplementation effects on secretory and molecular aspects of vascular endothelial growth factor derived from peritoneal fluids of patients with endometriosis. J Obstet Gynaecol 2019, 39, (8), 1137-1142. [CrossRef]
- Amini, L.; Chekini, R.; Nateghi, M. R.; Haghani, H.; Jamialahmadi, T.; Sathyapalan, T.; Sahebkar, A., The Effect of Combined Vitamin C and Vitamin E Supplementation on Oxidative Stress Markers in Women with Endometriosis: A Randomized, Triple-Blind Placebo-Controlled Clinical Trial. Pain Res Manag 2021, 2021, 5529741. [CrossRef]
- Mier-Cabrera, J.; Genera-García, M.; De la Jara-Díaz, J.; Perichart-Perera, O.; Vadillo-Ortega, F.; Hernández-Guerrero, C., Effect of vitamins C and E supplementation on peripheral oxidative stress markers and pregnancy rate in women with endometriosis. Int J Gynaecol Obstet 2008, 100, (3), 252-6. [CrossRef]
- Santanam, N.; Kavtaradze, N.; Murphy, A.; Dominguez, C.; Parthasarathy, S., Antioxidant supplementation reduces endometriosis-related pelvic pain in humans. Transl Res 2013, 161, (3), 189-95.
- Tang, H. C.; Lin, T. C.; Wu, M. H.; Tsai, S. J., Progesterone resistance in endometriosis: A pathophysiological perspective and potential treatment alternatives. Reprod Med Biol 2024, 23, (1), e12588. [CrossRef]
- Critchley, H. O. D.; Chodankar, R. R., 90 YEARS OF PROGESTERONE: Selective progesterone receptor modulators in gynaecological therapies. J Mol Endocrinol 2020, 65, (1), T15-T33. [CrossRef]
- Béliard, A.; Noël, A.; Foidart, J. M., Reduction of apoptosis and proliferation in endometriosis. Fertil Steril 2004, 82, (1), 80-5. [CrossRef]
- Burns, K. A.; Rodriguez, K. F.; Hewitt, S. C.; Janardhan, K. S.; Young, S. L.; Korach, K. S., Role of estrogen receptor signaling required for endometriosis-like lesion establishment in a mouse model. Endocrinology 2012, 153, (8), 3960-71.
- Kulak, J.; Fischer, C.; Komm, B.; Taylor, H. S., Treatment with bazedoxifene, a selective estrogen receptor modulator, causes regression of endometriosis in a mouse model. Endocrinology 2011, 152, (8), 3226-32. [CrossRef]
- Khine, Y. M.; Taniguchi, F.; Nagira, K.; Nakamura, K.; Ohbayashi, T.; Osaki, M.; Harada, T., New insights into the efficacy of SR-16234, a selective estrogen receptor modulator, on the growth of murine endometriosis-like lesions. Am J Reprod Immunol 2018, 80, (5), e13023.
- Harada, T.; Ohta, I.; Endo, Y.; Sunada, H.; Noma, H.; Taniguchi, F., SR-16234, a Novel Selective Estrogen Receptor Modulator for Pain Symptoms with Endometriosis: An Open-label Clinical Trial. Yonago Acta Med 2017, 60, (4), 227-233.
- Clemenza, S.; Vannuccini, S.; Ruotolo, A.; Capezzuoli, T.; Petraglia, F., Advances in targeting estrogen synthesis and receptors in patients with endometriosis. Expert Opin Investig Drugs 2022, 31, (11), 1227-1238. [CrossRef]
- Bulun, S. E.; Zeitoun, K. M.; Takayama, K.; Sasano, H., Estrogen biosynthesis in endometriosis: molecular basis and clinical relevance. J Mol Endocrinol 2000, 25, (1), 35-42. [CrossRef]
- Attar, E.; Tokunaga, H.; Imir, G.; Yilmaz, M. B.; Redwine, D.; Putman, M.; Gurates, B.; Attar, R.; Yaegashi, N.; Hales, D. B.; Bulun, S. E., Prostaglandin E2 via steroidogenic factor-1 coordinately regulates transcription of steroidogenic genes necessary for estrogen synthesis in endometriosis. J Clin Endocrinol Metab 2009, 94, (2), 623-31.
- Słopień, R.; Męczekalski, B., Aromatase inhibitors in the treatment of endometriosis. Prz Menopauzalny 2016, 15, (1), 43-7. [CrossRef]
- Stanway, S. J.; Purohit, A.; Woo, L. W.; Sufi, S.; Vigushin, D.; Ward, R.; Wilson, R. H.; Stanczyk, F. Z.; Dobbs, N.; Kulinskaya, E.; Elliott, M.; Potter, B. V.; Reed, M. J.; Coombes, R. C., Phase I study of STX 64 (667 Coumate) in breast cancer patients: the first study of a steroid sulfatase inhibitor. Clin Cancer Res 2006, 12, (5), 1585-92. [CrossRef]
- Rižner, T. L.; Romano, A., Targeting the formation of estrogens for treatment of hormone dependent diseases-current status. Front Pharmacol 2023, 14, 1155558. [CrossRef]
- Pavone, M. E.; Bulun, S. E., Aromatase inhibitors for the treatment of endometriosis. Fertil Steril 2012, 98, (6), 1370-9. [CrossRef]
- Ailawadi, R. K.; Jobanputra, S.; Kataria, M.; Gurates, B.; Bulun, S. E., Treatment of endometriosis and chronic pelvic pain with letrozole and norethindrone acetate: a pilot study. Fertil Steril 2004, 81, (2), 290-6. [CrossRef]
- Ferrero, S.; Gillott, D. J.; Venturini, P. L.; Remorgida, V., Use of aromatase inhibitors to treat endometriosis-related pain symptoms: a systematic review. Reprod Biol Endocrinol 2011, 9, 89. [CrossRef]
- Taylor, H. S.; Giudice, L. C.; Lessey, B. A.; Abrao, M. S.; Kotarski, J.; Archer, D. F.; Diamond, M. P.; Surrey, E.; Johnson, N. P.; Watts, N. B.; Gallagher, J. C.; Simon, J. A.; Carr, B. R.; Dmowski, W. P.; Leyland, N.; Rowan, J. P.; Duan, W. R.; Ng, J.; Schwefel, B.; Thomas, J. W.; Jain, R. I.; Chwalisz, K., Treatment of Endometriosis-Associated Pain with Elagolix, an Oral GnRH Antagonist. N Engl J Med 2017, 377, (1), 28-40. [CrossRef]
- Sbracia, M.; Scarpellini, F., Use of depot GNRH antagonist (Degarelix) in the treatment of endometriomas (ovarian endometriosis) before IVF: a controlled trial. Fertility and sterility 2015, 104, (3). [CrossRef]
- Franssen, A. M.; Kauer, F. M.; Chadha, D. R.; Zijlstra, J. A.; Rolland, R., Endometriosis: treatment with gonadotropin-releasing hormone agonist Buserelin. Fertil Steril 1989, 51, (3), 401-8. [CrossRef]
- Rocha, A. L.; Reis, F. M.; Taylor, R. N., Angiogenesis and endometriosis. Obstet Gynecol Int 2013, 2013, 859619. [CrossRef]
- Bouquet de Joliniere, J.; Fruscalzo, A.; Khomsi, F.; Stochino Loi, E.; Cherbanyk, F.; Ayoubi, J. M.; Feki, A., Antiangiogenic Therapy as a New Strategy in the Treatment of Endometriosis? The First Case Report. Front Surg 2021, 8, 791686. [CrossRef]
- Antônio, L. G. L.; Rosa-E-Silva, J. C.; Machado, D. J.; Westin, A. T.; Garcia, S. B.; Candido-Dos-Reis, F. J.; Poli-Neto, O. B.; Nogueira, A. A., Thalidomide Reduces Cell Proliferation in Endometriosis Experimentally Induced in Rats. Rev Bras Ginecol Obstet 2019, 41, (11), 668-672. [CrossRef]
- He, Y.; Hung, S. W.; Liang, B.; Zhang, R.; Gao, Y.; Chu, C. Y.; Zhang, T.; Xu, H.; Chung, J. P. W.; Wang, C. C., Receptor Tyrosine Kinase Inhibitor Sunitinib as Novel Immunotherapy to Inhibit Myeloid-Derived Suppressor Cells for Treatment of Endometriosis. Front Immunol 2021, 12, 641206. [CrossRef]
- Selak, V.; Farquhar, C.; Prentice, A.; Singla, A., Danazol for pelvic pain associated with endometriosis. Cochrane Database Syst Rev 2000, (2), CD000068. [CrossRef]
- Chen, P.; Mamillapalli, R.; Habata, S.; Taylor, H. S., Endometriosis stromal cells induce bone marrow mesenchymal stem cell differentiation and PD-1 expression through paracrine signaling. Mol Cell Biochem 2021, 476, (4), 1717-1727.
- Li, J.; Yan, S.; Li, Q.; Huang, Y.; Ji, M.; Jiao, X.; Yuan, M.; Wang, G., Macrophage-associated immune checkpoint CD47 blocking ameliorates endometriosis. Mol Hum Reprod 2022, 28, (5). [CrossRef]
- D'Hooghe, T. M.; Bambra, C. S.; Raeymaekers, B. M.; De Jonge, I.; Hill, J. A.; Koninckx, P. R., The effects of immunosuppression on development and progression of endometriosis in baboons (Papio anubis). Fertil Steril 1995, 64, (1), 172-8. [CrossRef]
- Chatzianagnosti, S.; Dermitzakis, I.; Theotokis, P.; Kousta, E.; Mastorakos, G.; Manthou, M. E., Application of Mesenchymal Stem Cells in Female Infertility Treatment: Protocols and Preliminary Results. Life (Basel) 2024, 14, (9). [CrossRef]
- Laschke, M. W.; Giebels, C.; Nickels, R. M.; Scheuer, C.; Menger, M. D., Endothelial progenitor cells contribute to the vascularization of endometriotic lesions. Am J Pathol 2011, 178, (1), 442-50. [CrossRef]
- Wang, X.; Mamillapalli, R.; Mutlu, L.; Du, H.; Taylor, H. S., Chemoattraction of bone marrow-derived stem cells towards human endometrial stromal cells is mediated by estradiol regulated CXCL12 and CXCR4 expression. Stem Cell Res 2015, 15, (1), 14-22. [CrossRef]
- Artemova, D.; Vishnyakova, P.; Gantsova, E.; Elchaninov, A.; Fatkhudinov, T.; Sukhikh, G., The prospects of cell therapy for endometriosis. J Assist Reprod Genet 2023, 40, (5), 955-967. [CrossRef]
- Yuxue, J.; Ran, S.; Minghui, F.; Minjia, S., Applications of nanomaterials in endometriosis treatment. Front Bioeng Biotechnol 2023, 11, 1184155. [CrossRef]
- Othman, E. E.; Salama, S.; Ismail, N.; Al-Hendy, A., Toward gene therapy of endometriosis: adenovirus-mediated delivery of dominant negative estrogen receptor genes inhibits cell proliferation, reduces cytokine production, and induces apoptosis of endometriotic cells. Fertil Steril 2007, 88, (2), 462-71. [CrossRef]
- Egorova, A.; Shubina, A.; Sokolov, D.; Selkov, S.; Baranov, V.; Kiselev, A., CXCR4-targeted modular peptide carriers for efficient anti-VEGF siRNA delivery. Int J Pharm 2016, 515, (1-2), 431-440. [CrossRef]
- Mazzone, M.; Dettori, D.; de Oliveira, R. L.; Loges, S.; Schmidt, T.; Jonckx, B.; Tian, Y. M.; Lanahan, A. A.; Pollard, P.; de Almodovar, C. R.; De Smet, F.; Vinckier, S.; Aragonés, J.; Debackere, K.; Luttun, A.; Wyns, S.; Jordan, B.; Pisacane, A.; Gallez, B.; Lampugnani, M. G.; Dejana, E.; Simons, M.; Ratcliffe, P.; Maxwell, P.; Carmeliet, P., Heterozygous deficiency of PHD2 restores tumor oxygenation and inhibits metastasis via endothelial normalization. Cell 2009, 136, (5), 839-851. [CrossRef]
- Tapmeier, T. T.; Rahmioglu, N.; Lin, J.; De Leo, B.; Obendorf, M.; Raveendran, M.; Fischer, O. M.; Bafligil, C.; Guo, M.; Harris, R. A.; Hess-Stumpp, H.; Laux-Biehlmann, A.; Lowy, E.; Lunter, G.; Malzahn, J.; Martin, N. G.; Martinez, F. O.; Manek, S.; Mesch, S.; Montgomery, G. W.; Morris, A. P.; Nagel, J.; Simmons, H. A.; Brocklebank, D.; Shang, C.; Treloar, S.; Wells, G.; Becker, C. M.; Oppermann, U.; Zollner, T. M.; Kennedy, S. H.; Kemnitz, J. W.; Rogers, J.; Zondervan, K. T., Neuropeptide S receptor 1 is a nonhormonal treatment target in endometriosis. Sci Transl Med 2021, 13, (608). [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



