
Submitted:
05 May 2025
Posted:
06 May 2025
You are already at the latest version
Abstract
Childhood anemia is a serious public health issue that adversely affects cognitive and psychomotor development, impacting school performance and adult productivity. In this cross-sectional descriptive study, we characterized the profile of children aged 6 months to 5 years diagnosed with or at risk of anemia while attending consultations at a pediatric hospital in Lisbon, Portugal. We found that 33.3% (74/222) of the children were either anemic or at risk of developing anemia. The overall anemia rates based on hemoglobin levels were 54.5% for mild anemia (36/66), 34.8% for moderate anemia (23/66), and 10.6% for borderline anemia (7/66). More than half (64/70) of the children had microcytic anemia, while 8.6% (6/70) had normocytic anemia. About 40.0% (12/30) of the children had iron deficiency anemia, and 33.3 % (3/9) had sickle cell trait. Our results indicate that anemia rates were higher in male children aged 2-3 years, those whose caregivers had a low level of education, and those whose mothers were from the Community of Portuguese Language Countries. Further research, including analytical cross-sectional or longitudinal studies, is necessary to explore the impact of feeding practices, dietary habits, and socioeconomic and metabolic factors on childhood anemia.
Keywords:
childhood
; anemia
; characteristics
; Portugal
; Southern Europe
; Europe
1. Introduction
Anemia is a condition where the number of erythrocytes or red blood cells (RBCs) is insufficient to meet metabolic demands [1]. It is a serious public health problem that affects both rich and poor countries and is associated with impaired development and reduced quality of life [1,2,3,4,5,6,7]. This condition negatively affects cognitive and psychomotor development, impacting school performance and adult productivity through developmental delays and behavioral disturbances [3,7]. Globally, anemia is one of the most widespread nutritional disorders, affecting nearly 40.0% of children aged 6 months to 5 years [3,8,9,10].
The causes of childhood anemia are multifactorial. For example, lack of iron, folate, vitamin B12, and vitamin A can cause nutritional anemia [6,7,10]. Iron deficiency is the most common nutritional deficiency and the primary cause of iron deficiency anemia (IDA) [11]. It often occurs when dietary iron intake is insufficient to meet iron needs, particularly during periods of life when iron requirements are increased, such as during growth and development in pregnancy and infancy [12]. Deficiencies in several other micronutrients (e.g., vitamin A, B12, folic acid, and riboflavin), which are essential for the normal production of red blood cells, likely contribute to the development of anemia [12]. Nutritional and iron deficiency anemia in children impairs immune function, delays mental, physical, and socioemotional development, and increases the risk of death among infants and young children [7,8,10]. Non-nutritional causes of anemia include parasitic infections (e.g., malaria, hookworm, schistosomiasis), as well as blood loss, blood-inherited diseases (e.g., sickle-cell), and infectious diseases (e.g., HIV/AIDS) [7,10]. The interaction mechanism between anemia and infections is complex. Preexisting anemia influences disease susceptibility, while infections can trigger anemia through inflammation, hemolysis, blood loss, nutrient malabsorption, and impaired red blood cell development [13,14]. Parasitic infections are often transmitted through the ingestion of contaminated water or food. While such infections are rarely fatal, they also impair the intestinal absorption of nutrients, causing malnutrition and anemia [15].
Sociodemographic and economic factors, child feeding practices, accessibility to preventive and curative health services, and maternal anemia also play a role in childhood anemia [16,17]. Anemia represents a key indicator of poor health and nutrition, acting as a marker of socioeconomic disparities, as it is inversely linked to household socioeconomic status, particularly in low- and middle-income settings [18]. Children from lower socioeconomic status are often at a higher risk of anemia and its long-term consequences [18]. Poverty, limited access to healthcare services, urban-rural disparities, and caregivers’ education levels are additional factors that may restrict access to nutritious foods, delay timely medical interventions, and negatively influence feeding habits, further increasing the risk of childhood anemia [19]. Few studies [20,21] have shown an association between maternal and fetal anemia, with infants born to anemic mothers often developing anemia a few months after birth. Still, evidence on whether childhood anemia is due to maternal baseline conditions, particularly during pregnancy, is scarce [20,22].
Anemia is defined quantitatively by hemoglobin (Hb), hematocrit, or red blood cell count levels that fall below the normal age- and sex-specific ranges [1]. Anemia in children aged 6 months to 5 years is characterized by low blood hemoglobin and can be classified into the following categories according to severity: mild (10.0 g/dL ≤ Hb ≤ 10.9 g/dL), moderate (7.0 g/dL ≤ Hb ≤ 9.9 g/dL), and severe (Hb < 7.0 g/dL). Additionally, a borderline or pre-anemic stage is identified when 11.0 g/dL ≤ Hb ≤ 11.4 g/dL [6,12,23,24]. Most children with mild anemia have no signs or symptoms, while some may present irritability, jaundice, shortness of breath, or palpitations [25,26]. Moderate and severe anemia has been associated with poor cognitive, emotional, and physical development [27,28]. Severe anemia carries a high 'silent' morbidity and mortality, often occurring months after initial diagnosis and treatment, contributing to under-five child mortality [17].
Other important anemia classifications are based on mean corpuscular volume (MCV) and are categorized into microcytic (MCV < 80fL), normocytic (MCV = 80- 100fL), and macrocytic (MCV > 100fL) [1,29,30]. Microcytic anemia, commonly caused by iron deficiency due to reduced dietary intake, is a leading cause of childhood anemia and is associated with impaired cognitive performance, motor development, and academic performance [31,32,33]. Many pediatric anemias present as normocytic, while macrocytosis is rarely observed in children [1,34]. Normocytic anemia has many causes (e.g., chronic infections and systemic diseases), making its diagnosis more difficult, whereas macrocytic anemia is usually caused by a deficiency of vitamin B12 or folic acid [1,32,35]. Other possible causes of macrocytic anemia include chronic liver disease, hypothyroidism, and myelodysplastic disorders [31,36]. Often, macrocytosis is considered a significant indicator in the diagnosis of bone marrow diseases and acute leukemia in childhood [34].
In 2021, the global anemia prevalence was 24.3% (95% uncertainty interval [UI] 23.9–24.7), corresponding to 1.92 billion people [37]. In the same year, anemia caused 52·0 million years of healthy life lost due to disability (YLDs) [37]. Evidence in the literature shows that the prevalence of anemia in children remains high, with data from 2019 indicating that 40.0% (95.0% uncertainty interval [UI] 36–44) of children aged 6–59 months were anemic, compared to 48.0% in 2000 [38]. The burden of anemia is particularly high in the African region, affecting 60.2 % (95.0% uncertainty interval [UI] 56.6-63.7) of children under five [37,38]. In contrast, Europe has a lower prevalence, affecting 23.0% of children under five in 2011 [39,40].
In Portugal, national anemia prevalence estimates were 4.3 % (95.0% uncertainty interval [UI] 5.7-32.4) in children under five in 2019 [41]. Previous studies [42,43], have shown that anemia is highly prevalent in Portugal and largely undiagnosed. In 2016, a prevalence of 19.9% (95.0% uncertainty interval [UI] 19.0–20.8%) was observed among adults living in mainland Portugal, accounting for 54.2 % of cases in pregnant women and 20.7 % of cases in non-pregnant fertile women [42,43]. Nutritional deficiency anemia (57.7%), particularly iron deficiency anemia (52.7%), represented most of the cases diagnosed [43]. A recent study [40] showed that the prevalence of anemia remains high in mainland Portugal, accounting for 38.2% (95% uncertainty interval [UI] 35.4–41.1) of pregnant women and 51.8% (95.0% uncertainty interval [UI] 50.1–53.4) in non-pregnant fertile women.
While studies on childhood anemia in Portugal have been conducted, few were inherently reviews [44,45]. A 2005 study [46] examining the long-term developmental effects of anemia among infants in Braga, North Portugal, reported an iron deficiency anemia prevalence of 19,7%. Still, much of the available evidence on childhood anemia in Portugal remains scarce or outdated [47]. Given the implications of anemia on childhood cognitive and motor development, school performance, and adult productivity, there is an urgent need for updated research to better characterize children affected by this condition in Portugal.
This study aims to characterize the profile of children aged 6 months to 5 years who were diagnosed with or at risk of anemia, attending external pediatric consultations at the Dona Estefânia Hospital (HDE) in Lisbon, Portugal. The evidence generated in this research will contribute to a better understanding of childhood anemia in Portugal, providing valuable epidemiological insights that can inform targeted healthcare interventions and improve the management of children affected by this condition.
2. Results
2.1. Sociodemographic Characteristics
A total of 222 children, aged 6 months to 5 years, who were referred from the emergency department, primary health care centers, or evacuated from Portuguese-speaking African countries for various conditions, attended external general pediatric consultations between September 2023 and September 2024. Among them, 74 children had anemia or were at risk of developing anemia, and their caregivers were invited to participate. All caregivers agreed to participate, resulting in a 100% acceptance rate (Figure 1). The reasons for consultation are detailed in Supplementary Table 1. Among the 74 children, anemia was the primary reason for consultation in 51 cases (51/74; 69.3%). Other clinical presentations or reasons for consultation (23/74; 31.9%) included bowel failure, abdominal pain, poor weight gain, and others.
Table 1 summarizes the sociodemographic characteristics of children with or at risk of developing anemia. Most participants were male (42/74; 56.8%), aged 2-3 years (29/74; 39.2%), lived in the Metropolitan Lisbon Area (61/74; 82.4%), and were accompanied by their mothers to the consultations (63/74; 85.1%). Most mothers were originally from the Community of Portuguese Language Countries (CPLP) (32/67; 47.8%) and worked in administrative, managerial, or support occupation roles (36/41; 87.8%). Meanwhile, most children’s fathers were from other countries (including CPLP) (34/52; 65.4%) and worked in non-administrative, non-managerial, or non-support occupation roles (22/40; 55.0%).
2.2. Nutritional and Health Characteristics
Our study results indicate that 33.3% (74/222) of children aged 6 months to 5 years who attended external general pediatric consultations were either anemic or at risk of developing anemia. Their nutritional and health characteristics are presented in Table 2. More than half (55/66; 83.3%) of the children had received exclusive breastfeeding. About 65.3 % (47/72) of the children had five or more meals/day, and 82.4% (61/74) had adequate minimum dietary diversity. Regarding their health status, 31.9% (23/72) had been previously hospitalized, and 16.2% (12/72) had a history of food selectivity behavior/refusal of certain types of food (8/12; 66.6%) or vomiting after consuming certain types of food (4/12; 33.3%). Children whose mothers reported vomiting after eating were attending the consultation primarily due to anemia (2/12; 16.7%), abdominal pain (1/12; 8.3%), and Down syndrome (1/12; 8.3%) (Supplementary Table 2).
The overall prevalence of anemia was 94.3% (66/74) based on hemoglobin levels, with 54.5% having mild anemia (36/66), 34.8% moderate anemia (23/66), and 10.6% borderline anemia (7/66). More than half (64/70) of the children had microcytic anemia, while 8.6% (6/70) had normocytic anemia. About 40.0% (12/30) of the children had iron deficiency anemia, and at least 33.3 % (3/9) had sickle cell trait.
2.3. Childhood Anemia by Sociodemographic Characteristics
Our results indicate that anemia cases in children aged 6 months to 5 years, measured by hemoglobin levels, were slightly higher in males (54.5%; 36/66) (Table 3). Similarly, this pattern was observed for cases of microcytic anemia, with 54.7% (35/70) in males. Regarding anemia and its risk by age, the highest proportion of cases was found among children aged 2–3 years (39.4%; 26/66) compared to their peers. Microcytic anemia was also most common in the 2–3 years group (45.3%; 29/70) compared to their peers. Concerning anemia by regional and socioeconomic factors, most cases were in children residing in the Metropolitan Lisbon Area (81.8%; 54/66). Such a pattern was also observed across all anemia classifications. Regarding caregiver characteristics, most anemia cases were observed among children whose caregivers had a basic or secondary level of education (59.1%; 39/66), whose mothers were from CPLP countries (48.3%; 29/60), and whose mothers worked in administrative, managerial, or support roles (91.2%; 31/38). Similarly, children of fathers from non-Portuguese origins accounted for a higher proportion of cases of anemia (66.7%; 30/49) compared to their peers.
2.4. Childhood Anemia by Nutritional and Health Characteristics
Our findings indicate that more than half of the children with or at risk of anemia, as determined by hemoglobin levels, engaged in exclusive breastfeeding (81.4%; 48/59), had received or were receiving complementary feeding (84.8%; 56/66), and consumed cereal porridge (61.5%; 40/65) (Table 4). A similar pattern was observed among children with microcytic anemia, with 87.9% (51/58) receiving exclusive breastfeeding, 89.1% (57/64) having received or currently receiving complementary feeding, and 55.6% (35/63) consuming cereal porridge. Children with low minimum dietary diversity (consumption of 1-3 food groups) had lower rates of anemia, as measured by hemoglobin levels (19.7%; 13/66), than those with adequate dietary diversity (80.3%;53/66). Likewise, more cases of microcytic anemia were also reported among children with low minimum dietary diversity (12.5; 8/64). Supplement intake, after confirmation of anemia diagnosis, during the period of study, was reported in 51.5% (34/66) of anemic children, with iron supplements being the most commonly consumed (61.8%; 21/34). Among children with anemia or at risk, 86.7% (26/30) had an adequate weight-for-age percentile, while 13.3% (4/30) had an inadequate weight-for-age percentile. About 87.1% (27/31) of children with microcytic anemia also had an adequate weight-for-age percentile. A history of food selectivity behavior/refusal to eat certain types of food or vomiting after consuming certain types of food was reported in 16.7% (11/66) of children with anemia (measured by hemoglobin levels). The presence of infection or inflammation was reported in 34.9% (15/43) of anemic cases. About 14.3% (5/35) of children with anemia or at risk had uremia. At least 35.4% (23/66) of anemic children had a history of previous hospitalization, with longer hospital stays (>5 days) being slightly more frequent (53.8%; 7/13) than shorter stays.
3. Discussion
This study characterized the profile of children aged 6 months to 5 years who attended the Dona Estefânia Hospital (HDE) in Lisbon, Portugal, and were diagnosed with or at risk of anemia. Our research focused on a specific subgroup of the pediatric population presenting a particular condition within a specialized sector of the hospital unit. We also observed that a significant portion of the anemic children had a background from the Community of Portuguese Language Countries (CPLP), reflecting the multicultural composition of the hospital's catchment area. Our findings are especially relevant in providing recent evidence on childhood anemia within this specific context in Portugal. Consequently, they cannot be fully generalized to the general pediatric Portuguese population, and some comparisons presented with population-based studies should be interpreted with caution.
Our results showed that the overall prevalence of anemia among children in this age group was 33.3%, indicating that anemia poses a moderate public health issue [48,49]. This prevalence is higher than the national estimates for under-five anemia in Portuguese children (14.3%), the European region (20.3%), and Central and Eastern Europe (22.0%) [38,41]. This prevalence was also slightly higher than those reported by other authors in various regions of Brazil (23.1%) [50] and in Timor-Leste (31.3%) [51]. However, anemia rates were lower than those found in the Community of Portuguese Language Countries (CPLP), namely, in Brazil (38.1% - 56.6%) [52,53,54], in Angola (44.4%) [55], in Cape Verde (51.8%) [56], in São Tomé and Príncipe (83.0%) [57], in Equatorial Guinea (85.0%) [58], and in Mozambique (62.2% - 83.0%) [59,60,61]. Our findings are also slightly higher than those reported for the Portuguese adult population residing in mainland Portugal (19.9%) [42].
We observed that rates of moderate (MO) and mild (MI) anemia were 54.5% and 34.8%, respectively, higher than the national estimates for Central and Eastern Europe (6.0% for moderate and 16.0% for mild anemia) [38]. These rates were also higher than those reported in studies conducted in Northwest Ethiopia (MO: 42.3% and MI: 23.7%) [62], in Western Peru (MO: 32.7% and MI: 10.9%) [63], in Southwest Ethiopia (MO: 15.8% and MI: 25.0%) [64], in Tanzania (MO: 44.8% and MI: 9.1%) [65]. Microcytic anemia rates were high (91.4%), with 74.0% of children having an iron deficiency (ID), 40.0% having iron deficiency anemia (IDA), and 33.3% having the sickle cell trait (SCT). The rates of iron deficiency and iron deficiency anemia observed in our study are higher than those reported in a previous study [47] conducted in the Cascais Municipality of the Metropolitan Lisbon Area among children aged 6 to 24 months (15.8% and 5.0%, respectively). We found higher rates of ID and IDA than those reported in Brazil (ID: 35.8%) [66], in Thessaloniki-Northern Greece (ID: 14.0% and IDA: 2.9%) [67], in Almería-Spain (ID: 8.7% and IDA: 2.0%) [68], in Thessalia- Central Greece (IDA: 7.9%) [69] and in Western Europe (ID:11.8%) [70].
The high rates of anemia reported in our study should be interpreted in the light of its unique sociodemographic characteristics. As such, these rates might be partly explained by the considerable portion of children who have a background from the Community of Portuguese Language Countries (CPLP) and African regions, where anemia and hemoglobinopathies are more prevalent [71]. Additionally, as stated in previous studies, these variations in anemia prevalence might also be attributed to a combination of geographical disparities (e.g. differences in climate), cultural factors (e.g. food practices), nutritional factors (e.g. dietary habits and food intake), genetic factors (e.g. inherited blood disorders), and socioeconomic context (e.g. caregivers' education level and access to health facilities) [17,44,70,72,73].
Sociodemographic patterns in childhood anemia
Our results indicate that anemia rates were higher in male children, aged 2-3 years, and among those with caregivers who had a basic or secondary level of education. Consistent with our findings, several studies [17,74,75,76] have demonstrated that boys are generally more susceptible to anemia than their peers. This may be attributed to increased prenatal and post-natal growth in males, which elevates their micronutrient needs, often not fulfilled through diet alone [74,76].
Our results align with previous studies in Brazil [66] and India (Raju et al., 2024). Nevertheless, our findings differ from studies conducted in northern Tanzania [77], Ethiopia [78] and Eastern Burkina Faso [2], which reported higher anemia rates among children aged 6-23 months compared to their peers. This discrepancy may be explained by differences in disease burden, cultural and dietary practices, and maternal nutrition between Portugal and these countries [17,37,42,70,72,73].
Similar to previous studies [77,79,80], higher anemia rates were observed among children whose caregivers had a lower level of education. Our study also showed higher rates of anemia among children whose mothers are from the Community of Portuguese Language Countries (CPLP) and fathers of non-Portuguese origins. Few studies [44] were conducted to analyze anemia in Portugal and other CPLP countries, showing that anemia plays a relevant role in disability and life imbalances in pregnant women and children under five years of age in Mozambique compared with Portugal. In addition, some authors [81] argue that, in past years, sickle cell trait disease in Portugal has been aggravated by immigrants from Angola and São Tomé and Príncipe. Other authors [82] state that immigrant mothers often may carry pre-existing conditions common in their countries of origin (e.g., anemia and hemoglobinopathies) that are less frequent in host countries like Portugal, and these women often request and receive less health care during and after pregnancy. A recent study [71] conducted in the municipalities of Amadora and Sintra, in the Lisbon Metropolitan Area, also reported high rates of anemia (30.1%; 65/216) and iron deficiency anemia (27.7%; 18/65) among migrant children and adolescents (aged between 1 and 16 years). The same study [71] emphasized the need to include systematic screening for sickle cell disease among the migrant population from African countries, where haemoglobinopathies are common, due to the importance of the disease in the Portuguese population. Broader socioeconomic strategies [83], nutrition education for caregivers [78], and strengthening the training and education of healthcare providers in the area of multiculturalism [82] could be crucial for mitigating childhood anemia in this setting. Nationwide strategies for the prevention and management of anemia in Portugal, which integrate nutrition education, particularly for pregnant women and caregivers of young children [42,43] may play a vital role in the prevention of childhood anemia. More research on socioeconomic disparities and childhood anemia is needed to better guide future strategies for mitigating this condition in this setting.
Nutritional patterns and health-related characteristics in childhood anemia
In this study, we observed that exclusive breastfeeding and complementary feeding rates were high among children with anemia. Meal frequency (consumption of five or more food groups per day) and adequate dietary diversity (consumption of four or more food groups) were also higher in children with anemia. These results contrast with several studies [80,84,85]. An explanation for this discrepancy may be linked to the nutritional quality of children's diets, particularly a low intake of key micronutrients such as iron, folate, and vitamin A, or the limited bioavailability of iron due to poor absorption [84].
Our findings show that some children with anemia also exhibit uremia. As noted by several authors [80,86], comorbidities (such as metabolic dysfunctions and infections) may play a crucial role in childhood anemia. On the other hand, anemia-related impairment may worsen the management of children with coexisting comorbidities, negatively impacting their quality of life [87]. Thus, more research (e.g., analytical cross-sectional or longitudinal studies) is needed to assess not only feeding practices and dietary habits in this age group but also the cultural, socioeconomic, and metabolic factors that might influence childhood anemia in this setting.
4. Materials and Methods
Study setting
Portugal, officially the Portuguese Republic, is the westernmost country of mainland Europe, located in the Iberian Peninsula and occupying a total area of 92,211.9 km2 [88,89]. It is bordered to the north and east by Spain, and its western and southern coastline is surrounded by the Atlantic Ocean. Portugal’s territory also includes two autonomous regions, the archipelagos of the Azores and Madeira, located in the Atlantic Ocean [88,89,90]. Portugal has the 12th-largest population in the European Union, with 10.6 million inhabitants [88,90]. Lisbon is the capital of Portugal, the largest Portuguese municipality (with over 550,000 inhabitants), and, along with 17 other municipalities, forms the Lisbon Metropolitan Area (which has around 3 million inhabitants) [90]. This study was conducted at the External Consultations of the Pediatrics Medical Service of Dona Estefânia Hospital (HDE)—Unidade Local de Saúde de São José (ULS São José) in Lisbon. Dona Estefânia Hospital is a reference unit in pediatrics for Southern Portugal and the archipelagos of the Azores and Madeira. It specializes in maternal and child health care [91]. The external consultations are conducted in a building with two sections: one dedicated to medical specialties and the other to surgical specialties. Within the medical specialties, consultations are offered in nine areas: general pediatrics, pulmonology, cystic fibrosis, sleep pathology, infectious diseases, travel medicine, rheumatology, nephrology, and chronic renal failure [92]. In addition, other specialized consultations are included, such as the Acute Patient Reassessment Consultation (CORDA), adolescent pediatrics, cooperation, palliative care, the Pre-Immunosuppressive Treatment Infectious Screening Consultation (CRIIPTO), and the Pediatric Risk Support Consultation (CARPE), as well as the Acute Diseases Consultation. In 2024, Dona Estefânia Hospital recorded a total of 59,870 pediatric medical consultations across all medical specialties. Of these, 4,169 were general pediatrics consultations, with 1,046 corresponding to first consultations and 2,420 to subsequent consultations (follow-up appointments), covering a total of 2,301 patients [92].
Study design, population, and sample universe
This hospital-based, cross-sectional descriptive study was conducted from September 2023 to September 2024. The sample universe was the External General Pediatrics Consultation section (area) of the Dona Estefânia Hospital. All children aged 6 months to 5 years old who attended the external general pediatric consultations during the study period were included (census-based approach).
Inclusion and Exclusion Criteria
The inclusion criteria were children aged between 6 months and 5 years, diagnosed with or at risk of anemia, who attended the External General Pediatrics Consultation section (area) at Dona Estefânia Hospital. This included: children referred from the emergency department for evaluation or follow-up by a pediatrician; children referred by family doctors from Health Centers; and children evacuated from Portuguese-speaking African countries due to various pathologies.
The exclusion criteria were children younger than 6 months, children aged 6 years or older, and children without available hemoglobin or hematocrit measurements. Also excluded were children followed in hematology or other specialized consultations.
Data collection and quality control
The total number of children aged 6 months to 5 years, both with and without anemia, who attended external pediatric consultations during the study period was obtained from daily consultation records. Children diagnosed with anemia or those identified as at risk were selected during each consultation. The study was then explained to the children’s caregivers, and their written informed consent was obtained. A pretested questionnaire, consisting of three sections on sociodemographic characteristics, feeding habits, and health status, was used to collect information. Clinical data were obtained from electronic medical records and children’s health cards. Investigators carefully monitored data collection. To ensure data quality, double data entry verification was conducted, and the information from paper-based forms and electronic questionnaires was compared. Data cleaning was performed to verify frequencies, consistency, and missing values, and any errors identified were corrected.
Outcome variable
The outcome variable for this study was the presence of anemia or the risk of developing anemia in children aged 6 months to 5 years. In the context of this study, anemia and the risk of developing anemia were defined as 11.0 g/dL ≤ Hb ≤ 11.4 g/dL. We used the following hemoglobin (Hb) cut-off values to classify anemia in children aged 6 months to 5 years: not anemic (Hb > 11.4 g/dL), borderline or pre-anemic stage (11.0 g/dL ≤ Hb ≤ 11.4 g/dL), mild (10.0 g/dL ≤ Hb ≤ 10.9 g/dL), moderate (7.0 g/dL ≤ Hb ≤ 9.9 g/dL), and severe (Hb < 7.0 g/dL) anemia [6,12,23,24]. Other anemia definitions used in this study were: anemia based on hematocrit levels [not anemic (hematocrit = 34.0%-40.0%) and anemic (hematocrit<33.0%)] and red blood cell size, measured by the mean corpuscular volume (MCV) [microcytic (<80 fL), normocytic (80-100 fL) and macrocytic (>100fL)] [29,93]. More details on definitions of anemia and the outcome variable can be found in the Supplementary file Table 3.
Exposure variables
In this study, exposure variables included sociodemographic characteristics (sex, age, residence area, caregiver’s degree of kinship, caregiver’s education level, country of origin, and parental occupation) and nutritional characteristics (history of breastfeeding, complementary feeding, cereal porridge intake, number of meals/day, intake of various food groups: cereals and derivatives, tubers, meat, fish and eggs, dairy products, fruits, legumes, vegetables, fats, and oils). Minimum dietary diversity was classified as "adequate" if children consumed four or more food groups, and "inadequate" if children consumed less than four food groups. Other exposure variables included anthropometric characteristics (weight percentiles) and health characteristics (vomiting or refusal to eat, presence of infections or inflammatory conditions, glucose and bilirubin levels, uremia, hospitalization, and duration of hospitalization). More details on exposure variables can be found in Supplementary file Table 3.
Data analysis
Data were analyzed using SPSS 28.0 software (International Business Machine Corporation [IBM Corp]) [95]. Descriptive statistics, including frequency distributions and cross-tabulations, were performed to summarize the characteristics of study participants and key variables.
5. Conclusions
This study describes anemia among children aged 6 months to 5 years attending external general pediatric consultations in Portugal. Our findings indicate that childhood anemia poses a moderate public health issue in this setting. Anemia rates were higher among male children, those aged 2-3 years, those whose caregivers had a low level of education, and those whose mothers were from the Community of Portuguese Language Countries (CPLP). Further research, including analytical cross-sectional or longitudinal studies, is necessary to better understand the role of feeding practices, dietary habits, nutritional adequacy, and other potential influencing determinants, such as cultural, socioeconomic, and metabolic factors, in childhood anemia in this setting.
6. Strengths and Limitations
To our knowledge, this is the first hospital-based study in Lisbon to characterize children aged 6 months to 5 years who are diagnosed with or at risk of anemia. Given the limited existing research on this issue in Portugal, our study can serve as a baseline for future research (whether analytical cross-sectional or longitudinal) focused on the role of feeding practices, dietary habits, nutritional adequacy, and other potential influencing determinants, such as cultural, socioeconomic, and metabolic aspects, on childhood anemia in Portugal. In addition, by providing valuable evidence, our study establishes a foundation for improving the prevention, management, and care of anemia in children living in Portugal.
However, there are some limitations to our study. First, due to constraints from the COVID-19 pandemic, which placed significant pressure on the National Health Service (SNS) and pediatric care in Portugal, the data collection process was impacted. Consequently, this study adopted a purely descriptive design. Our one-year study focused on characterizing the profiles of children diagnosed with or at risk of anemia and did not include children without anemia, limiting the analysis of relationships or associations between various determinants and childhood anemia. Second, our sample universe was not randomly selected, as it consisted of all children aged 6 months to 5 years old who attended the external general pediatric consultations section of Dona Estefânia Hospital and were chosen based on availability during the study period. As such, our findings should not be generalized to all pediatric consultations or patient profiles at the hospital. Third, the sociodemographic composition of our sample, which includes a substantial proportion of anemic children with backgrounds from the Community of Portuguese Language Countries (CPLP), may contribute to the high rates of anemia observed in this study and further limit the generalizability of our findings to the broader Portuguese pediatric population. Therefore, more comprehensive studies are needed to explore anemia associations with various determinants, provide more generalizable results, and enhance our understanding of the factors influencing anemia in children in Portugal.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary Table 1. Reasons for consultations, Supplementary Table 2. Reasons for Consultation Among Children With a History of Food Selectivity, Refusal to Eat, or Vomiting After Eating, Supplementary Table 3. Study variables.
Author Contributions
Conceptualization: R.M.C., L.V., and I.C.; methodology: R.M.C., L.V., and I.C.; data collection: R.M.C., A.C., B.M.S., J.V., B.L.V., A.S., M.C., and F.B.C.; coordination of data collection on site: R.M.C.; software: R.M.C.; formal analysis: R.M.C., S.C. and Y.K.; investigation: R.M.C.; resources: R.M.C., L.V., and I.C.; data curation: R.M.C., and S.C.; writing—original draft preparation: R.M.C; writing—review and editing: R.M.C., A.C., Y.K., S.C., B.M.S., J.V., B.L.V., A.S., M.C., F.B.C., L.V. and I.C.; visualization: R.M.C.; supervision: L.V and I.C. All authors have read and agreed to the published version of the manuscript.
Funding
R.M.C., L.V., and I.C. were supported by Fundação para a Ciência e a Tecnologia for funds to GHTM - UID/04413/2020 and LA-REAL – LA/P/0117/2020. R.M.C was supported by Fundação para a Ciência e a Tecnologia for funds for her Doctoral Program (Reference UI/BD/151065/2021; DOI: https://doi.org/10.54499/UI/BD/151065/2021). The views expressed in this paper are from the authors and not the official position of the institutions or funder.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee for Health of the Central Lisbon University Hospital Center (CES-CHULC) (CES 947/2020, first approval on 19th November 2020; with the second approval extension on 3rd April 2024). This research is also described as a sub-study - that integrates the study protocol on the same topic (PAMC, Ref. Of 0110/CC/2020) approved by the Institutional Committee of Bioethics in Health of the Faculty of Medicine/Maputo Central Hospital (CIBS FM&HCM; HCM/004/2020, first approval on 30th March 2020, with the fourth approval extension granted on 29th February 2024).
Informed Consent Statement
Informed consent was obtained from all parents or legal guardians of the subjects involved in this study.
Data Availability Statement
Data from this study are not publicly available due to patients’ privacy and ethical restrictions. However, the data presented in this study are available in this article and its supplementary information files.
Acknowledgments
We sincerely thank the children’s caregivers for agreeing to participate in this study. We also thank the doctors and pediatric residents of Dona Estefânia Hospital for their support in data collection: Ana Isabel Carvalho, António Campos, Caroline Lopes, Conceição Neves, Diana Amaral, João Simões, Margarida Almendra, Mafalda Borges, Rita Machado, and Sara Ferreira. We further thank the operational assistants and "Ludoteca” personnel of Dona Estefânia Hospital: Andreia Filipa, Cátia Dias, Fernanda Pires Paulo, Claudia, Rute Gomes, Maria dos Anjos Santos, Sara Fernanda Paiva, Susana Mendes, Isabel Fernandes, and Tomé André. The first author would like to express gratitude to Francisco Merca, Ana Varão, Alexandre Azeredo, Duarte Santos, Eduardo Pedro, Diogo Gonçalves, Rui Ribeiro, Salima Rehemtula and André Gonçalves. Special thanks to Michel Jareski Andrade for his valuable support in formatting the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AIDS | Acquired immunodeficiency syndrome |
| CPLP | Community of Portuguese Language Countries |
| ID | Iron deficiency |
| IDA | Iron deficiency anemia |
| Hb | Hemoglobin |
| HIV | Human immunodeficiency virus |
| HDE | Dona Estefânia Hospital |
| MI | Mild anemia |
| MCV | Mean corpuscular volume |
| MO | Moderate anemia |
| RCBs | Red blood cells |
| UI | Uncertainty interval |
| ULS | Unidade Local de Saúde |
References
- Gallagher, P.G. Anemia in the pediatric patient. Blood 2022, 140, 571–593. [Google Scholar] [CrossRef] [PubMed]
- Ouédraogo, O.; Compaoré, E.W.R.; Kiburente, M.; Dicko, M.H. Prevalence and Associated Factors of Anemia in Children Aged 6 to 59 Months in the Eastern Region of Burkina Faso. Glob. Pediatr. Heal. 2024, 11, 2333794X241263163. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. (2023). Anaemia. World Health Organization. Retrieved January 30, 2025. Available online: https://www.who.int/news-room/fact-sheets/detail/anaemia.
- Matysiak, M. Anemia in children: a pediatrician’s view. Acta Haematol. Pol. 2021, 52, 402–405. [Google Scholar] [CrossRef]
- Lopes, A.I.; Azevedo, S.; Cabral, J.; Ferreira, M.G.; Sande-Lemos, P.; Ferreira, R.; Trindade, E.; Lima, R.; Antunes, H. Portuguese Consensus on Diagnosis, Treatment, and Management of Anemia in Pediatric Inflammatory Bowel Disease. GE Port. J. Gastroenterol. 2020, 27, 244–254. [Google Scholar] [CrossRef]
- Gelaw, Y.; Getaneh, Z.; Melku, M. Anemia as a risk factor for tuberculosis: a systematic review and meta-analysis. Environ. Heal. Prev. Med. 2021, 26, 1–15. [Google Scholar] [CrossRef]
- Ohene-Agyei, P.; Ndoadoumgue, A.L.; Bana-Ewai, E.; Yaya, I.; Nambiema, A. Population attributable fractions for risk factors for childhood anaemia: Findings from the 2017 Togo Malaria Indicator Survey. Br. J. Nutr. 2025, 1–27. [Google Scholar] [CrossRef]
- Thompson, L.; Arnold, C.; Peerson, J.; Long, J.M.; Westcott, J.L.E.; Islam, M.M.; Black, R.E.; Krebs, N.F.; McDonald, C.M. Predictors of Anaemia Among Young Children Receiving Daily Micronutrient Powders (MNPs) for 24 Weeks in Bangladesh: A Secondary Analysis of the Zinc in Powders Trial. Matern. Child Nutr. 2025, e13806. [Google Scholar] [CrossRef]
- Braat, S.; Fielding, K.L.; Han, J.; E Jackson, V.; Zaloumis, S.; Xu, J.X.H.; Moir-Meyer, G.; Blaauwendraad, S.M.; Jaddoe, V.W.V.; Gaillard, R.; et al. Haemoglobin thresholds to define anaemia from age 6 months to 65 years: estimates from international data sources. Lancet Haematol. 2024, 11, e253–e264. [Google Scholar] [CrossRef]
- King, F. S. , Burgess, A., Quinn, V. J., & Osei, A. J. (2015). Nutrition for developing countries (3rd ed.). Oxford University Press.
- Qiu, Y.; Long, Z.; Long, Z. Epidemiology of dietary iron deficiency in China from 1990 to 2021: findings from the global burden of disease study 2021. BMC Public Heal. 2025, 25, 1–6. [Google Scholar] [CrossRef]
- Chaparro, C.M.; Suchdev, P.S. Anemia epidemiology, pathophysiology, and etiology in low- and middle-income countries. Ann. New York Acad. Sci. 2019, 1450, 15–31. [Google Scholar] [CrossRef]
- Brittenham, G.M.; Moir-Meyer, G.; Abuga, K.M.; Datta-Mitra, A.; Cerami, C.; Green, R.; Pasricha, S.-R.; Atkinson, S.H. Biology of Anemia: A Public Health Perspective. J. Nutr. 2023, 153, S7–S28. [Google Scholar] [CrossRef] [PubMed]
- USAID Advancing Nutrition. (2022). Understanding anemia and its coexisting factors: A brief. USAID. Retrieved April 2, 2025. Available online: https://www.advancingnutrition.org/sites/default/files/2022-10/usaid-an-anemia-coexisting-brief-2022.pdf.
- Martins, R.R.; Paixão, F.; Mendes, I.; Schäfer, S.; Monge, I.; Costa, F.; Correia, P. Intestinal Parasitic Infections in Children: A 10-Year Retrospective Study. Cureus 2024, 16, e75862. [Google Scholar] [CrossRef] [PubMed]
- Shimanda, P.P.; Amukugo, H.J.; Norström, F. Socioeconomic factors associated with anemia among children aged 6-59 months in Namibia. J. Public Heal. Afr. 2020, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Melku, M.; Alene, K.A.; Terefe, B.; Enawgaw, B.; Biadgo, B.; Abebe, M.; Muchie, K.F.; Kebede, A.; Melak, T.; Melku, T. Anemia severity among children aged 6–59 months in Gondar town, Ethiopia: a community-based cross-sectional study. Ital. J. Pediatr. 2018, 44, 107. [Google Scholar] [CrossRef]
- Yang, F.; Liu, X.; Zha, P. Trends in Socioeconomic Inequalities and Prevalence of Anemia Among Children and Nonpregnant Women in Low- and Middle-Income Countries. JAMA Netw. Open 2018, 1, e182899. [Google Scholar] [CrossRef]
- Osborne, A.; Adeleye, K.; Bangura, C.; Wongnaah, F.G. Trends and inequalities in anaemia prevalence among children aged 6–59 months in Ghana, 2003–2022. Int. J. Equity Heal. 2024, 23, 1–12. [Google Scholar] [CrossRef]
- Zhao, B.; Sun, M.; Wu, T.; Li, J.; Shi, H.; Wei, Y. The association between maternal anemia and neonatal anemia: a systematic review and meta-analysis. BMC Pregnancy Childbirth 2024, 24, 677. [Google Scholar] [CrossRef]
- Chandran, V.; Kirby, R.S. An Analysis of Maternal, Social and Household Factors Associated with Childhood Anemia. Int. J. Environ. Res. Public Heal. 2021, 18, 3105. [Google Scholar] [CrossRef]
- Sowe, A.; Wood, E.; Gautam, S.K. Maternal Anemia as a Predictor of Childhood Anemia: Evidence from Gambian Health Data. Nutrients 2025, 17, 879. [Google Scholar] [CrossRef]
- World Health Organization. (2011). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. World Health Organization. Retrieved April 2, 2025. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-MNM-11.1.
- Williams, A. M. Williams, A. M., Ansai, N., Ahluwalia, N., & Nguyen, D. T. (2024). Anemia prevalence: United States, August 2021–August 2023 (NCHS Data Brief No. 519). National Center for Health Statistics. Retrieved April 2, 2025. Available online: https://www.cdc.gov/nchs/products/databriefs/db519.htm.
- Leung, A.K.; Lam, J.M.; Wong, A.H.; Hon, K.L.; Li, X. Iron Deficiency Anemia: An Updated Review. Curr. Pediatr. Rev. 2024, 20, 339–356. [Google Scholar] [CrossRef]
- Janus, J., & Moerschel, S. K. (2010). Evaluation of anemia in children. American family physician, 81(12), 1462–1471.
- Ngnie-Teta, I.; Receveur, O.; Kuate-Defo, B. Risk Factors for Moderate to Severe Anemia among Children in Benin and Mali: Insights from a Multilevel Analysis. Food Nutr. Bull. 2007, 28, 76–89. [Google Scholar] [CrossRef] [PubMed]
- Benedict, R.K.; Pullum, T.W.; Riese, S.; Milner, E. Is child anemia associated with early childhood development? A cross-sectional analysis of nine Demographic and Health Surveys. PLOS ONE 2024, 19, e0298967. [Google Scholar] [CrossRef] [PubMed]
- Maner, B. S., Killeen, R. B., & Moosavi, L. (2024). Mean corpuscular volume. In StatPearls [Internet]. StatPearls Publishing. Retrieved April 5, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK545275/.
- Turner, J., Parsi, M., & Badireddy, M. (2023). Anemia. In StatPearls [Internet]. StatPearls Publishing. Retrieved April 5, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK499994/.
- Yeboah, F.A.; Bioh, J.; Amoani, B.; Effah, A.; Senu, E.; Mensah, O.S.O.; Agyei, A.; Kwarteng, S.; Agomuo, S.K.S.; Opoku, S.; et al. Iron deficiency anemia and its association with cognitive function among adolescents in the Ashanti Region - Ghana. BMC Public Heal. 2024, 24, 1–12. [Google Scholar] [CrossRef]
- Irwin, J. J., & Kirchner, J. T. (2001). Anemia in children. American family physician, 64(8), 1379–1386.
- Chaudhry, H. S., & Kasarla, M. R. (2025). Microcytic hypochromic anemia. In StatPearls. StatPearls Publishing. Retrieved April 29, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470252/.
- Sarbay, H.; Ay, Y. Evaluation of children with macrocytosis: clinical study. Pan Afr. Med J. 2018, 31, 54. [Google Scholar] [CrossRef]
- Yilmaz, G., & Shaikh, H. (2023). Normochromic normocytic anemia. In StatPearls. StatPearls Publishing. Retrieved April 29, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK565880/.
- Moore, C. A., Killeen, R. B., & Adil, A. (2025). Macrocytic anemia. In StatPearls. StatPearls Publishing. Retrieved April 29, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459295/.
- Gardner, W.M.; Razo, C.; A McHugh, T.; Hagins, H.; Vilchis-Tella, V.M.; Hennessy, C.; Taylor, H.J.; Perumal, N.; Fuller, K.; Cercy, K.M.; et al. Prevalence, years lived with disability, and trends in anaemia burden by severity and cause, 1990–2021: findings from the Global Burden of Disease Study 2021. Lancet Haematol. 2023, 10, e713–e734. [Google Scholar] [CrossRef]
- A Stevens, G.; Paciorek, C.J.; Flores-Urrutia, M.C.; Borghi, E.; Namaste, S.; Wirth, J.P.; Suchdev, P.S.; Ezzati, M.; Rohner, F.; Flaxman, S.R.; et al. National, regional, and global estimates of anaemia by severity in women and children for 2000–19: a pooled analysis of population-representative data. Lancet Glob. Heal. 2022, 10, e627–e639. [Google Scholar] [CrossRef]
- World Health Organization. (2015). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. WHO/NMH/NHD/MNM/11.1. Retrieved March 12, 2025. Available online: https://iris.who.int/bitstream/handle/10665/177094/9789241564960_eng.pdf.
- Nunes, A.R.; Mairos, J.; Brilhante, D.; Marques, F.; Belo, A.; Cortez, J.; Fonseca, C. Screening for Anemia and Iron Deficiency in the Adult Portuguese Population. Anemia 2020, 2020, 1048283. [Google Scholar] [CrossRef]
- World Health Organization. (2022). Global Health Observatory Data Repository: By Category, Child Malnutrition, Anaemia in children.
- Fonseca, C.; Marques, F.; Nunes, A.R.; Belo, A.; Brilhante, D.; Cortez, J. Prevalence of anaemia and iron deficiency in Portugal: the EMPIRE study. Intern. Med. J. 2016, 46, 470–478. [Google Scholar] [CrossRef]
- Marques, F. , Fonseca, C., Robalo Nunes, A., Belo, A., Brilhante, D., & Cortez, J. (2016). Contextualising the High Prevalence of Anaemia in the Portuguese Population: Perception, Characterisation and Predictors: an EMPIRE Sub-Study. Internal Medicine, 23(4), 26–38. [CrossRef]
- Cane, R.M.; Chidassicua, J.B.; Varandas, L.; Craveiro, I. Anemia in Pregnant Women and Children Aged 6 to 59 Months Living in Mozambique and Portugal: An Overview of Systematic Reviews. Int. J. Environ. Res. Public Heal. 2022, 19, 4685. [Google Scholar] [CrossRef]
- Palaré, M.J. , Ferrão, A., Carreira, M., & Morais, A. (2004). Défice de ferro na criança. Acta Pediátrica Portuguesa, 3 (35), 243-247.
- Antunes, H., Gonçalves, S., Teixeira-Pinto, A., Costa-Pereira, A., Tojo-Sierra, R., & Aguiar, Á. (2005). Anemia por deficiência de ferro no lactente: Resultados preliminares do desenvolvimento aos cinco anos. Acta Médica Portuguesa, 18(4), 261–266. Retrieved March 10, 2025. Available online: https://www.actamedicaportuguesa.com/revista/index.php/amp/article/view/1034/702.
- Virella, D.; Pina, M.J. [Prevalence of iron deficiency in early infancy]. . 1998, 11, 607–13. [Google Scholar] [PubMed]
- World Health Organization. (2024). Haemoglobin cutoffs to define anaemia in individuals and populations. Guideline Central. Retrieved March 20, 2025. Available online: https://www.guidelinecentral.com/guideline/3534081/#section-3534102.
- World Health Organization. (2023). Nutrition landscape information system (Nlis). Anaemia. Nutrition and nutrition-related health and development data. Geneva, Switzerland: WHO. Retrieved March 20, 2025. Available online: https:// www.who.int/data/nutrition/nlis/info/anaemia.
- da Silva, L.L.S.; Fawzi, W.W.; Cardoso, M.A. ; ENFAC Working Group Factors associated with anemia in young children in Brazil. PLOS ONE 2018, 13, e0204504. [Google Scholar] [CrossRef] [PubMed]
- E Agho, K.; Dibley, M.J.; D'Este, C.; Gibberd, R. Factors Associated with Haemoglobin Concentration among Timor-Leste Children Aged 6–59 Months. 2008, 26, 200–209.
- Ferreira, H.S.; Vieira, R.C.S.; Livramento, A.R.S.; Dourado, B.L.L.; Silva, G.F.; Calheiros, M.S.C. Prevalence of anaemia in Brazilian children in different epidemiological scenarios: an updated meta-analysis. Public Health Nutr 2021, 24, 1–14. [Google Scholar] [CrossRef]
- dos Santos, R.F.; Gonzalez, E.S.C.; de Albuquerque, E.C.; de Arruda, I.K.G.; Diniz, A.d.S.; Figueroa, J.N.; Pereira, A.P.C. Prevalence of anemia in under five-year-old children in a children's hospital in Recife, Brazil. Rev. Bras. de Hematol. e Hemoter. 2011, 33, 100–104. [Google Scholar] [CrossRef]
- Oliveira, C. S. M., Cardoso, M. A., Araújo, T. S., & Muniz, P. T. (2011). Anemia em crianças de 6 a 59 meses e fatores associados no Município de Jordão, Estado do Acre, Brasil. Cadernos de Saúde Pública, 27(5), 1008–1020. Retrieved March 25, 2025. Available online: https://repositorio.usp.br/item/002344964.
- Fançony, C.; Lavinha, J.; Brito, M.; Barros, H. Anemia in preschool children from Angola: a review of the evidence. Porto Biomed. J. 2020, 5, e60. [Google Scholar] [CrossRef]
- Semedo, R.M.; Santos, M.M.; Baião, M.R.; Luiz, R.R.; Da Veiga, G.V. Prevalence of Anaemia and Associated Factors among Children below Five Years of Age in Cape Verde, West Africa. 2014, 32, 646–657.
- Silva, C.C.; Catarino, E. Malnutrition and anemia in children aged 6 to 59 months in the Autonomous Region of Príncipe and its relation to maternal health. Popul. Med. 2023, 5. [Google Scholar] [CrossRef]
- Ncogo, P.; Romay-Barja, M.; Benito, A.; Aparicio, P.; Nseng, G.; Berzosa, P.; Santana-Morales, M.A.; Riloha, M.; Valladares, B.; Herrador, Z. Prevalence of anemia and associated factors in children living in urban and rural settings from Bata District, Equatorial Guinea, 2013. PLOS ONE 2017, 12, e0176613. [Google Scholar] [CrossRef]
- Aly, M.M.; Berti, C.; Chemane, F.; Macuelo, C.; Marroda, K.R.; La Vecchia, A.; Agostoni, C.; Baglioni, M. Prevalence of anemia among children aged 6–59 months in the Ntele camp for internally displaced persons (Cabo Delgado, Mozambique): a preliminary study. Eur. J. Clin. Nutr. 2025, 79, 79–82. [Google Scholar] [CrossRef]
- Cane, R.M.; Keita, Y.; Lambo, L.; Pambo, E.; Gonçalves, M.P.; Varandas, L.; Craveiro, I. Prevalence and factors related to anaemia in children aged 6–59 months attending a quaternary health facility in Maputo, Mozambique. Glob. Public Heal. 2023, 18, 2278876. [Google Scholar] [CrossRef]
- Muhajarine, N.; A Adeyinka, D.; Matandalasse, M.; Chicumbe, S. Inequities in childhood anaemia at provincial borders in Mozambique: cross-sectional study results from multilevel Bayesian analysis of 2018 National Malaria Indicator Survey. BMJ Open 2021, 11, e051395. [Google Scholar] [CrossRef]
- Hailu, B.A. Mapping, trends, and factors associated with anemia among children aged under 5 y in East Africa. Nutrition 2023, 116, 112202. [Google Scholar] [CrossRef] [PubMed]
- Huamani, M.A.A.; Aliaga-Gastelumendi, R.A. Calidad de atención y satisfacción del usuario en un Servicio de Emergencia de un Hospital del Seguro Social. Acta MEDICA Peru. 2023, 40. [Google Scholar] [CrossRef]
- Kebede, D.; Getaneh, F.; Endalamaw, K.; Belay, T.; Fenta, A. Prevalence of anemia and its associated factors among under-five age children in Shanan gibe hospital, Southwest Ethiopia. BMC Pediatr. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Mghanga, F.P.; Genge, C.M.; Yeyeye, L.; Twalib, Z.; Kibopile, W.; Rutalemba, F.J.; Shengena, T.M. Magnitude, Severity, and Morphological Types of Anemia in Hospitalized Children Under the Age of Five in Southern Tanzania. Cureus 2017, 9, e1499. [Google Scholar] [CrossRef]
- Ferraz, I. S. , Daneluzzi, J. C., Vannucchi, H., Jordão, A. A., Jr, Ricco, R. G., Del Ciampo, L. A., Martinelli, C. E., Jr, Engelberg, A. A., Bonilha, L. R., & Custódio, V. I. (2005). Prevalência da carência de ferro e sua associação com a deficiência de vitamina A em pré-escolares [Prevalence of iron deficiency and its association with vitamin A deficiency in preschool children]. Jornal de Pediatria, 81(2), 169–174.
- Gompakis, N.; Economou, M.; Tsantali, C.; Kouloulias, V.; Keramida, M.; Athanasiou-Metaxa, M. The Effect of Dietary Habits and Socioeconomic Status on the Prevalence of Iron Deficiency in Children of Northern Greece. Acta Haematol. 2007, 117, 200–204. [Google Scholar] [CrossRef]
- López-Ruzafa, E.; Vázquez-López, M.A.; Galera-Martínez, R.; Lendínez-Molinos, F.; Gómez-Bueno, S.; Martín-González, M. Prevalence and associated factors of iron deficiency in Spanish children aged 1 to 11 years. Eur. J. Pediatr. 2021, 180, 2773–2780. [Google Scholar] [CrossRef]
- Tympa-Psirropoulou, E.; Vagenas, C.; Dafni, O.; Matala, A.; Skopouli, F. Environmental risk factors for iron deficiency anemia in children 12-24 months old in the area of Thessalia in Greece. . 2008, 12, 240–50. [Google Scholar]
- Akkermans, M.D.; van der Horst-Graat, J.M.; Eussen, S.R.; van Goudoever, J.B.; Brus, F. Iron and Vitamin D Deficiency in Healthy Young Children in Western Europe Despite Current Nutritional Recommendations. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 635–642. [Google Scholar] [CrossRef]
- Ribeiro, L.C.-B.; Paixão, F.; Costa, F.; Correia, P. Migrant Pathology Screening in the Pediatric Population: A Five-Year Retrospective Study From a Level II Hospital. Cureus 2024, 16, e53770. [Google Scholar] [CrossRef]
- van der Merwe, L.F.; Eussen, S.R. Iron status of young children in Europe. Am. J. Clin. Nutr. 2017, 106, 1663S–1671S. [Google Scholar] [CrossRef] [PubMed]
- Leal, L.P.; Filho, M.B.; de Lira, P.I.C.; Figueiroa, J.N.; Osório, M.M. Prevalência da anemia e fatores associados em crianças de seis a 59 meses de Pernambuco. Rev. de Saude publica 2011, 45, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Aheto, J.M.K.; Alhassan, Y.; Puplampu, A.E.; Boglo, J.K.; Sedzro, K.M. Anemia prevalence and its predictors among children under-five years in Ghana. A multilevel analysis of the cross-sectional 2019 Ghana Malaria Indicator Survey. Heal. Sci. Rep. 2023, 6, e1643. [Google Scholar] [CrossRef] [PubMed]
- Belachew, A.; Tewabe, T. Under-five anemia and its associated factors with dietary diversity, food security, stunted, and deworming in Ethiopia: systematic review and meta-analysis. Syst. Rev. 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Tadesse, S.E.; Zerga, A.A.; Mekonnen, T.C.; Tadesse, A.W.; Hussien, F.M.; Feleke, Y.W.; Anagaw, M.Y.; Ayele, F.Y. Burden and Determinants of Anemia among Under-Five Children in Africa: Systematic Review and Meta-Analysis. Anemia 2022, 2022, 1–9. [Google Scholar] [CrossRef]
- Mboya, I.B.; Mamseri, R.; Leyaro, B.J.; George, J.; Msuya, S.E.; Mgongo, M. Prevalence and factors associated with anemia among children under five years of age in Rombo district, Kilimanjaro region, Northern Tanzania. F1000Research 2020, 9, 1102. [Google Scholar] [CrossRef]
- Omer, A.; Hailu, D.; Nigusse, G.; Mulugeta, A. Magnitude and morphological types of anemia differ by age among under five children: A facility-based study. Heliyon 2022, 8, e10494. [Google Scholar] [CrossRef]
- Martinez-Torres, V.; Torres, N.; A Davis, J.; Corrales-Medina, F.F. Anemia and Associated Risk Factors in Pediatric Patients. Pediatr. Heal. Med. Ther. 2023, ume 14, 267–280. [Google Scholar] [CrossRef]
- Sunardi, D.; Bardosono, S.; Basrowi, R.W.; Wasito, E.; Vandenplas, Y. Dietary Determinants of Anemia in Children Aged 6–36 Months: A Cross-Sectional Study in Indonesia. Nutrients 2021, 13, 2397. [Google Scholar] [CrossRef]
- Costa, S. N., Madeira, S., Sobral, M. A., & Delgadinho, G. (2016). Hemoglobinopatias em Portugal e a intervenção do médico de família. Revista Portuguesa de Medicina Geral e Familiar, 32, 416–424. Available online: https://rpmgf.pt/ojs/index.php/rpmgf/article/view/11963.
- Estrela, P. (2009). A saúde dos imigrantes em Portugal. Revista Portuguesa de Clínica Geral, 25, 45–55. Available online: https://rpmgf.pt/ojs/index.php/rpmgf/article/view/10590.
- Raju, A. A. Raju, A. A., Boddu, A. B., Raju, D. S. S. K., & Surabhi, U. S. (2023). The prevalence and predictors of iron deficiency anemia in toddlers: A population-based study. Journal of Advances in Medicine and Pharmacy, 6(2), 648–651. Retrieved March 25, 2025. Available online: https://academicmed.org/Uploads/Volume6Issue2/137.%20[3019.%20JAMP_PH]%20648-651.pdf.
- Shibeshi, A.H.; Mare, K.U.; Kase, B.F.; Wubshet, B.Z.; Tebeje, T.M.; Asgedom, Y.S.; Asmare, Z.A.; Asebe, H.A.; Lombebo, A.A.; Sabo, K.G.; et al. The effect of dietary diversity on anemia levels among children 6–23 months in sub-Saharan Africa: A multilevel ordinal logistic regression model. PLOS ONE 2024, 19, e0298647. [Google Scholar] [CrossRef]
- Kathuria, N.; Bandyopadhyay, P.; Srivastava, S.; Garg, P.R.; Devi, K.S.; Kurian, K.; Rathi, S.K.; Mehra, S. Association of minimum dietary diversity with anaemia among 6–59 months’ children from rural India: An evidence from a cross-sectional study. J. Fam. Med. Prim. Care 2023, 12, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.T.; De Sanctis, V.; Yassin, M.; Wagdy, M.; Soliman, N. Chronic anemia and thyroid function. Acta Bio-Medica Atenei Parmensis 2017, 88, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Chand, D.H.; Valentini, R.P. Chronic Kidney Disease: Treatment of Comorbidities II (Hypertension, Anemia, and Electrolyte Management). Curr. Treat. Options Pediatr. 2019, 5, 93–101. [Google Scholar] [CrossRef]
- Ministério dos Negócios Estrangeiros. (2025). Sobre Portugal. Portal Diplomático. Retrieved February 19, 2025. Available online: https://portaldiplomatico.mne.gov.pt/sobre-portugal.
- European Union. (2024). Portugal. Retrieved February 6, 2025. Available online: https://european-union.europa.eu/principles-countries-history/eu-countries/portugal_en.
- European Parliament. (2019). Economic, social and territorial situation of Portugal: Briefing requested by the REGI committee. Retrieved February 6, 2025, Available online:. Available online: https://www.europarl.europa.eu/RegData/etudes/BRIE/2019/629190/IPOL_BRI (accessed on day month year).
- Serviço Nacional de Saúde. (2025). Unidade Local de Saúde de São José. Retrieved February 20, 2025. Available online: https://www.sns.gov.pt/entidades-de-saude/unidade-local-de-saude-de-sao-jose/.
- Hospital Dona Estefânia. (2025). ULS São José: Contexto regional e nacional da instituição.
- Staples, A.O.; Wong, C.S.; Smith, J.M.; Gipson, D.S.; Filler, G.; Warady, B.A.; Martz, K.; Greenbaum, L.A. Anemia and Risk of Hospitalization in Pediatric Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 48–56. [Google Scholar] [CrossRef]
- World Health Organization. (2025). Child growth standards. World Health Organization. Retrieved March 15, 2025. Available online: https://www.who.int/tools/child-growth-standards/standards.
- IBM Corp. (2021). IBM SPSS Statistics for Windows, Version 28.0. Armonk, NY: IBM Corp.
Figure 1.
Flowchart of the study population.
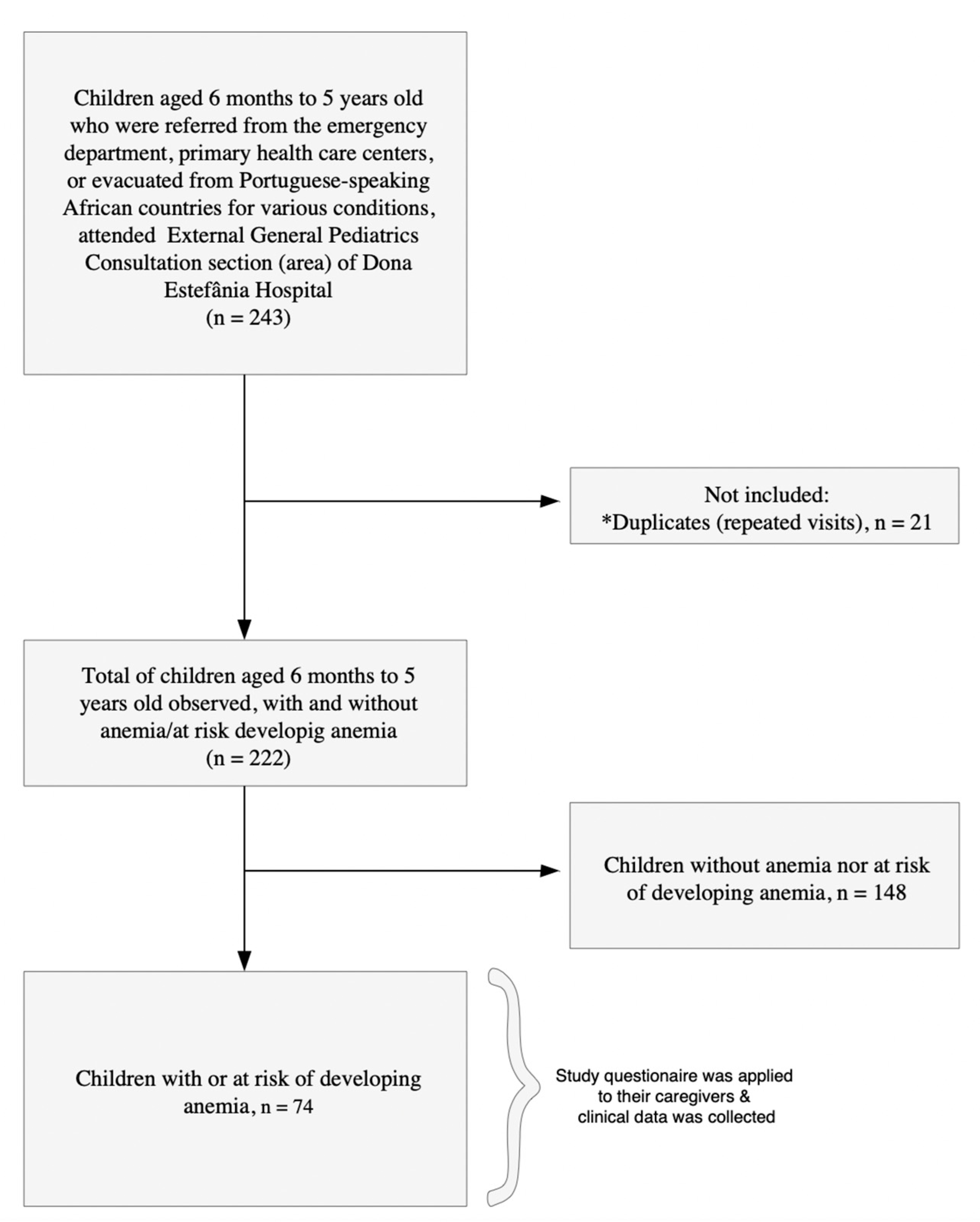

Table 1.
Sociodemographic characteristics of children aged 6 months - 5 years at Dona Estefânia Hospital, PAMC, September 2023 – September 2024.
Table 1.
Sociodemographic characteristics of children aged 6 months - 5 years at Dona Estefânia Hospital, PAMC, September 2023 – September 2024.
| Variables (n = 74) | Categories | N | % |
| Sex | Male | 42 | 56.8 |
| Female | 32 | 43.2 | |
| Child´s age | 6 months - 1 year | 28 | 37.8 |
| 2 -3 years | 29 | 39.2 | |
| 4-5 years | 17 | 23.0 | |
| Country of residence | Portugal | 73 | 98.6 |
| Cape Verde | 1 | 1.4 | |
| Region of residence | Metropolitan Lisbon Area (Greater Lisbon) | 61 | 82.4 |
| Other regions (Setúbal peninsula, Alentejo, Madeira, West and Tagus Valley, etc) | 13 | 17.6 | |
| Caregiver's Degree of Kinship | Mother | 63 | 85.1 |
| Father | 11 | 14.9 | |
| Caregiver´s Level of Education | Basic/Primary or Secondary Level | 41 | 55.4 |
| Technical or Higher education (bachelor's, master's, doctorate) | 22 | 29.7 | |
| Other | 11 | 14.9 | |
| Country of origin of the child´s mother | Portugal | 20 | 29.9 |
| CPLP | 32 | 47.8 | |
| Other countries | 15 | 22.4 | |
| Mother's occupation (by role) | Specialized Intellectual and scientific roles | 5 | 12.2 |
| Administrative, Managerial, or Support roles | 36 | 87.8 | |
| Country of origin of the child's father | Portugal | 18 | 34.6 |
| Other countries | 34 | 65.4 | |
| Father´s occupation (by role) | Administrative, Managerial, or Support roles | 18 | 45.0 |
| Other roles | 22 | 55.0 | |
| Notes: | • CPLP: Community of Portuguese Language Countries. • Mother’s other origin countries included: Nepal, Bangladesh, Ukraine, Lithuania, Spain, India, Venezuela, Ivory Coast, and the Republic of Guinea (Conakry). Father’s other countries of origin included CPLP countries, Nepal, Bangladesh, India, and Ukraine. | ||
| • Mother’s occupation, by roles, includes two large groups, namely: Specialized Intellectual and Scientific roles (experts in intellectual and scientific professions) and Administrative, Managerial or Support roles (administrative staff and similar, managers, self-employed individuals, entrepreneurs, service and sales staff, and unemployed or domestic workers). | |||
| • Father’s occupation, by roles, includes two large groups, namely: Administrative, Managerial, or Support roles (administrative staff and similar, managers, self-employed individuals, entrepreneurs, service and sales staff, and unemployed or domestic workers) and other roles (experts in intellectual and scientific professions, technicians and professionals at the intermediate level, and industrial, agricultural, and fishing workers). | |||
Table 2.
Nutritional and health characteristics of children aged 6 months - 5 years at Dona Estefânia Hospital, PAMC, September 2023 – September 2024.
Table 2.
Nutritional and health characteristics of children aged 6 months - 5 years at Dona Estefânia Hospital, PAMC, September 2023 – September 2024.
| Variables (n = 74) | Categories | N | % | |
|---|---|---|---|---|
| Nutritional characteristics | History of exclusive breastfeeding | Yes (Past/Present) | 55 | 83.3 |
| No | 11 | 16.7 | ||
| Duration of breastfeeding | 1-5 months | 21 | 42.0 | |
| 6-12 months | 29 | 58.0 | ||
| Complementary feeding* | Yes | 64 | 86.5 | |
| No | 10 | 13.5 | ||
| Cereal porridge intake | Yes | 43 | 58.9 | |
| No | 30 | 41.1 | ||
| Number of meals/days | 3-4 meals/day | 25 | 34.7 | |
| 5 or more meals/day | 47 | 65.3 | ||
| Cereals and derivatives, tubes | Yes | 57 | 77.0 | |
| No | 17 | 23.0 | ||
| Meat, fish, and eggs | Yes | 65 | 87.8 | |
| No | 9 | 12.2 | ||
| Dairy products | Yes | 70 | 94.6 | |
| No | 4 | 5.4 | ||
| Fruits | Yes | 63 | 85.1 | |
| No | 11 | 14.9 | ||
| Legumes | Yes | 67 | 90.5 | |
| No | 7 | 9.5 | ||
| Vegetables | Yes | 53 | 71.6 | |
| No | 21 | 28.4 | ||
| Fats and oils | Yes | 14 | 18.9 | |
| No | 60 | 81.1 | ||
| Minimum dietary diversity | Adequate (4 or more food groups) | 61 | 82.4 | |
| Inadequate (1-3 food groups) | 13 | 17.6 | ||
| Excessive milk consumption | Yes (> 500mL/day) | 8 | 10.8 | |
| No | 66 | 89.2 | ||
| Supplements intake | Yes | 39 | 52.7 | |
| No | 35 | 47.3 | ||
| Type of supplements | Iron | 25 | 64.1 | |
| Iron, folic acid, and vitamin B12, and/or multivitamins | 14 | 35.9 | ||
| Anthropometric characteristics | Weight percentile | Adequate weight for age (Percentile 3-97) | 30 | 88.2 |
| Not adequate for age [Percentile <3 (low weight for age) or Percentile >97 (high weight for age] | 4 | 11.8 | ||
| Child anemia | Anemia based on hemoglobin (Hb) level | Has anemia/At risk of developing anemia (11.0g/dL≤Hb≤11.4g/dL) | 66 | 94.3 |
| Without anemia (Hb>11.4g/dL) | 4 | 5.7 | ||
| Anemia severity, based on hemoglobin (Hb) level | Borderline or pre-anemic stage (11.0 g/dL ≤ Hb ≤ 11.4 g/dL | 7 | 10.6 | |
| Mild (10.0 g/dL ≤ Hb ≤ 10.9 g/dL) | 36 | 54.5 | ||
| Moderate (7.0 g/dL ≤ Hb ≤ 9.9 g/dL) | 23 | 34.8 | ||
| Anemia based on hematocrit (%) level | Has anemia (Hematocrit<34.0%) | 59 | 85.5 | |
| Normal (34.0%≤Hematocrit≤40.0%) | 10 | 14.5 | ||
| Anemia based on the size of red blood cells (RCBs) measured by the mean corpuscular volume (MCV) | Microcytic (<80 fL) | 64 | 91,4 | |
| Normocytic (80-100 fL) | 6 | 8.6 | ||
| Iron deficiency by serum iron level | Iron deficiency (Serum iron < 30.0 mcg/dL) | 10 | 37.0 | |
| Mild iron deficiency /Pre-anemic stage (30.0 mcg/dL ≤ Serum iron ≤ 50.0 mcg/dL) | 10 | 37.0 | ||
| Normal (> 50.0 mcg/dL-120.0 mcg/dL) | 7 | 25.9 | ||
| Iron deficiency anemia (IDA) by ferritin level | Iron deficiency anemia (Ferritin< 12 ng/mL) | 12 | 40.0 | |
| Adequate iron storage in children with infection or inflammation/ IDA in children with no inflammation (12-30 ng/mL) | 4 | 13.3 | ||
| Normal (> 30.0 ng/mL) | 12 | 40.0 | ||
| Risk of iron overload (> 500.0 ng/mL) | 2 | 6.7 | ||
| Sickle cell trait | Yes (Sickle trait cell) | 3 | 33.3 | |
| No/pendent | 6 | 66.7 | ||
| Health characteristics | Vomit or refusal to eat** | Yes (had vomited or refused to eat) | 12 | 16.2 |
| No | 62 | 83.8 | ||
| Presence of infection or inflammation by C-reactive protein (CRP) level | Yes (CRP > 5.0 mg/mL) | 15 | 31.9 | |
| No (CRP <5.0 mg/mL) | 32 | 68.1 | ||
| Blood glucose level | Normal (60.0–180.0 mg/dL) | 18 | 100.0 | |
| Bilirubin | Hyperbilirubinemia (Bilirubin>1.20 mg/dL) | 10 | 90.9 | |
| Normal (0.30-1.20 mg/dL) | 1 | 9.1 | ||
| Urea | Uremia (Blood urea >36.0mg/dL) | 5 | 13.9 | |
| Normal (5.0-36.0mg/dL) | 31 | 86.1 | ||
| Had any hospitalization (in the past) | Yes | 23 | 31.9 | |
| No | 49 | 68.1 | ||
| Duration of hospitalization (in days) | Up to 5 days | 7 | 53.8 | |
| More than 5 days | 6 | 46.2 | ||
| Notes: | (*) Children whose mothers reported that they had either previously received or were currently receiving complementary feeding.(**) Children whose mothers reported a history of food selectivity behavior (e.g., children who eat "normally" at kindergarten or school but refuse to eat the same foods at home), refusal to eat certain types of food (such as meat), or vomiting after consuming certain types of food (e.g., due to irritability or irritated behavior, abdominal pain, or an unspecified reason). | |||
Table 3.
Distribution of anemia cases among children aged 6 months to 5 years by sociodemographic characteristics, hemoglobin, hematocrit, and mean corpuscular volume.
Table 3.
Distribution of anemia cases among children aged 6 months to 5 years by sociodemographic characteristics, hemoglobin, hematocrit, and mean corpuscular volume.
| Characteristics | Categories | Cases of anemia based on hemoglobin (Hb) | Cases of anemia based on hematocrit (%) | Cases of anemia based on mean corpuscular value (MCV) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Has anemia/At risk of developing anemia (11.0g/dL≤Hb≤11.4g/dL) | Without anemia (Hb>11.4g/dL) | Has anemia (<33.0%) | Normal (34.0%-40.0%) | Microcytic anemia(<80 fL) | Normocytic anemia (80-100 fL) | ||||||||
| n | % | n | % | N | % | N | % | N | % | n | % | ||
| Gender | Male | 36 | 54.5 | 3 | 75.0 | 34 | 57.6 | 4 | 40.0 | 35 | 54.7 | 4 | 66.7 |
| Female | 30 | 45.5 | 1 | 25.0 | 25 | 42.4 | 6 | 60.0 | 29 | 45.3 | 2 | 33.3 | |
| Child´s age | 6 months - 1 year | 23 | 34.8 | 1 | 25.0 | 22 | 37.3 | 2 | 20.0 | 21 | 32.8 | 4 | 66.7 |
| 2 -3 years | 26 | 39.4 | 3 | 75.0 | 23 | 39.0 | 6 | 60.0 | 29 | 45.3 | 0 | 0.0 | |
| 4-5 years | 17 | 25.8 | 0 | 0.0 | 14 | 23.7 | 2 | 20.0 | 14 | 21.9 | 2 | 33.3 | |
| Region of residence | Metropolitan Lisbon Area (Greater Lisbon) | 54 | 81.8 | 3 | 75.0 | 48 | 81.4 | 9 | 90.0 | 53 | 82.8 | 4 | 66.7 |
| Other regions (Setúbal peninsula, Alentejo, Madeira, West and Tagus Valley, etc) | 12 | 18.2 | 1 | 25.0 | 11 | 18.6 | 1 | 10.0 | 11 | 17.2 | 2 | 33.3 | |
| Caregiver's Degree of Kinship | Mother | 56 | 84.8 | 4 | 100.0 | 50 | 84.7 | 9 | 90.0 | 54 | 84.4 | 6 | 100.0 |
| Father | 10 | 15.2 | 0 | 0.0 | 9 | 15.3 | 1 | 10.0 | 10 | 15.6 | 0 | 0.0 | |
| Caregiver´s Level of Education | Basic/Primary or Secondary Level | 39 | 59.1 | 1 | 25.0 | 34 | 57.6 | 5 | 50.0 | 36 | 56.3 | 3 | 50.0 |
| Technical or Higher education (bachelor's, master's, doctorate) | 17 | 25.8 | 2 | 50.0 | 17 | 28.8 | 2 | 20.0 | 17 | 26.6 | 3 | 50.0 | |
| Other | 10 | 15.2 | 1 | 25.0 | 8 | 13.6 | 3 | 30.0 | 11 | 17.2 | 0 | 0.0 | |
| Country of origin of the child's mother | Portugal | 18 | 30.0 | 2 | 50.0 | 17 | 31.5 | 3 | 33.3 | 19 | 32.8 | 1 | 16.7 |
| CPLP | 29 | 48.3 | 1 | 25.0 | 24 | 44.4 | 5 | 55.6 | 26 | 44.8 | 4 | 66.7 | |
| Other countries | 13 | 21.7 | 1 | 25.0 | 13 | 24.1 | 1 | 11.1 | 13 | 22.4 | 1 | 16.7 | |
| Mother's occupation (by role) | Specialized Intellectual and scientific roles | 3 | 8.8 | 1 | 2.0 | 3 | 9.1 | 2 | 50.0 | 5 | 13.2 | - | - |
| Administrative, Managerial or Support roles | 31 | 91.2 | 3 | 75.0 | 30 | 90.9 | 2 | 50.0 | 33 | 86.8 | - | - | |
| Country of origin of the child's father | Portugal | 15 | 33.3 | 3 | 75.0 | 14 | 32.6 | 4 | 80.0 | 18 | 39.1 | 0 | 0.0 |
| Other countries | 30 | 66.7 | 1 | 25.0 | 29 | 67.4 | 1 | 20.0 | 28 | 60.9 | 3 | 100.0 | |
| Father´s occupation (by role) | Administrative, Managerial or Support roles | 15 | 45.5 | 1 | 25.0 | 15 | 46.9 | 2 | 50.0 | 17 | 45.9 | - | - |
| Other roles | 18 | 54.5 | 3 | 75.0 | 17 | 53.1 | 2 | 50.0 | 20 | 54.1 | - | - | |
| Notes: | •Metropolitan Lisbon area: Amadora, Barreiro, Cascais, Lisbon, Loures, Moita, Montijo, Odivelas, Seixal, Sintra, Sesimbra, Vila Franca de Xira. •CPLP: Community of Portuguese Language Countries. •Mother’s other origin countries included: Nepal, Bangladesh, Ukraine, Lithuania, Spain, India, Venezuela, Ivory Coast, and the Republic of Guinea (Conakry). Father’s other countries of origin included CPLP countries, Nepal, Bangladesh, India, and Ukraine. | ||||||||||||
| •Mother’s occupation, by roles, includes two large groups, namely: Specialized Intellectual and Scientific roles (experts in intellectual and scientific professions) and Administrative, Managerial or Support roles (administrative staff and similar, managers, self-employed individuals, entrepreneurs, service and sales staff, and unemployed or domestic workers). | |||||||||||||
| •Father’s occupation, by roles, includes two large groups, namely: Administrative, Managerial, or Support roles (administrative staff and similar, managers, self-employed individuals, entrepreneurs, service and sales staff, and unemployed or domestic workers) and Other roles (experts in intellectual and scientific professions, technicians and professionals of intermediate level, industrial, agricultural and fishing workers). | |||||||||||||
Table 4.
Distribution of anemia cases among children aged 6 months to 5 years by nutritional and health characteristics, hemoglobin, hematocrit, and mean corpuscular volume.
Table 4.
Distribution of anemia cases among children aged 6 months to 5 years by nutritional and health characteristics, hemoglobin, hematocrit, and mean corpuscular volume.
| Characteristics | Categories | Cases of anemia based on hemoglobin (Hb) | Cases of anemia based on hematocrit (%) | Cases of anemia based on mean corpuscular value (MCV) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Has anemia/At risk of developing anemia (11.0g/dL≤Hb≤11.4g/dL) | Without anemia (Hb>11.4g/dL) | Has anemia (<33.0%) | Normal (34.0%-40.0%) | Microcytic anemia (<80 fL) | Normocytic anemia (80-100 fL) | |||||||||
| n | % | N | % | N | % | n | % | N | % | n | % | |||
| Nutritional characteristics | History of exclusive breastfeeding | Yes (Past/Present) | 48 | 81.4 | 4 | 100.0 | 43 | 81.1 | 9 | 90.0 | 51 | 87.9 | 2 | 33.3 |
| No | 11 | 18.6 | 0 | 0.0 | 10 | 18.9 | 1 | 10.0 | 7 | 12.1 | 4 | 66.7 | ||
| Duration of breastfeeding | 1-5 months | 18 | 40.9 | 1 | 33.3 | 17 | 42.5 | 3 | 42.9 | 19 | 41.3 | 1 | 50.0 | |
| 6-12 months | 26 | 59.1 | 2 | 66.7 | 23 | 57.5 | 4 | 57.1 | 27 | 58.7 | 1 | 50.0 | ||
| History of complementary feeding | Yes (Past/Present) | 56 | 84.8 | 4 | 100.0 | 49 | 83.1 | 10 | 100.0 | 57 | 89.1 | 3 | 50.0 | |
| No | 10 | 15.2 | 0 | 0.0 | 10 | 16.9 | 0 | 0.0 | 7 | 10.9 | 3 | 50.0 | ||
| Cereal porridge intake | Yes | 40 | 61.5 | 1 | 25.0 | 34 | 58.6 | 6 | 60.0 | 35 | 55.6 | 5 | 83.3 | |
| No | 25 | 38.5 | 3 | 75.0 | 24 | 41.4 | 4 | 40.0 | 28 | 44.4 | 1 | 16.7 | ||
| Number of meals/days | 3-4 meals/day | 23 | 35.9 | 3 | 75.0 | 18 | 31.6 | 6 | 60.0 | 22 | 34.9 | 2 | 40.0 | |
| 5 or more meals/day | 41 | 64.1 | 1 | 25.0 | 39 | 68.4 | 4 | 40.0 | 41 | 65.1 | 3 | 60.0 | ||
| Cereals and derivatives, tubes | Yes | 52 | 78.8 | 2 | 50.0 | 48 | 81.4 | 4 | 40.0 | 49 | 76.6 | 4 | 66.7 | |
| No | 14 | 21.2 | 2 | 50.0 | 11 | 18.6 | 6 | 60.0 | 15 | 23.4 | 2 | 33.3 | ||
| Meat, fish, and eggs | Yes | 57 | 86.4 | 4 | 100.0 | 50 | 84.7 | 10 | 100.0 | 57 | 89.1 | 4 | 66.7 | |
| No | 9 | 13.6 | 0 | 0.0 | 9 | 15.3 | 0 | 0.0 | 7 | 10.9 | 2 | 33.3 | ||
| Dairy products | Yes | 62 | 93.9 | 4 | 100.0 | 55 | 93.2 | 10 | 100.0 | 62 | 96.9 | 4 | 66.7 | |
| No | 4 | 6.1 | 0 | 0.0 | 4 | 6.8 | 0 | 0.0 | 2 | 3.1 | 3 | 33.3 | ||
| Fruits | Yes | 56 | 84.8 | 4 | 100.0 | 50 | 84.7 | 9 | 90.0 | 56 | 87.5 | 4 | 66.7 | |
| No | 10 | 15.2 | 0 | 0.0 | 9 | 15.3 | 1 | 10.0 | 8 | 12.5 | 2 | 33.3 | ||
| Legumes | Yes | 59 | 89.4 | 4 | 100.0 | 53 | 89.8 | 9 | 90.0 | 59 | 92.2 | 4 | 66.7 | |
| No | 7 | 10.6 | 0 | 0.0 | 6 | 10.2 | 1 | 10.0 | 5 | 7.8 | 2 | 33.3 | ||
| Vegetables | Yes | 49 | 74.2 | 1 | 25.0 | 45 | 76.3 | 5 | 50.0 | 45 | 70.3 | 5 | 83.3 | |
| No | 17 | 25.8 | 3 | 75.0 | 14 | 23.7 | 5 | 50.0 | 19 | 29.7 | 1 | 16.7 | ||
| Fats and oils | Yes | 14 | 21.2 | 0 | 0.0 | 13 | 22.0 | 1 | 10.0 | 14 | 21.9 | 0 | 0.0 | |
| No | 52 | 78.8 | 4 | 100.0 | 46 | 78.0 | 9 | 90.0 | 50 | 78.1 | 6 | 100.0 | ||
| Minimum dietary diversity | Adequate (4 or more food groups) | 53 | 80.3 | 4 | 100.0 | 47 | 79.7 | 9 | 90.0 | 56 | 87.5 | 1 | 16.7 | |
| Inadequate (1-3 food groups) | 13 | 19.7 | 0 | 0.0 | 12 | 20.3 | 1 | 10.0 | 8 | 12.5 | 5 | 83.3 | ||
| Excessive milk consumption | Yes (> 500mL/day) | 6 | 9.1 | 2 | 50.0 | 6 | 10.2 | 1 | 10.0 | 8 | 12.5 | 0 | 0.0 | |
| No | 60 | 90.9 | 2 | 50.0 | 53 | 89.3 | 9 | 90.0 | 56 | 87.5 | 6 | 100.0 | ||
| Supplements intake | Yes | 34 | 51.5 | 3 | 75.0 | 29 | 49.2 | 7 | 70.0 | 32 | 50.0 | 5 | 83.3 | |
| No | 32 | 48.5 | 1 | 25.0 | 30 | 50.8 | 3 | 30.0 | 32 | 50.0 | 1 | 16.7 | ||
| Type of supplements | Iron | 21 | 61.8 | 3 | 100.0 | 18 | 62.1 | 4 | 57.1 | 22 | 68.8 | 1 | 20.0 | |
| Iron, folic acid, and vitamin B12, and/or multivitamins | 13 | 38.2 | 0 | 0.0 | 11 | 37.9 | 3 | 42.9 | 10 | 31.3 | 4 | 80.0 | ||
| Anthropometric characteristics | Weight percentile | Adequate weight for age (Percentile 3-97) | 26 | 86.7 | 3 | 100.0 | 24 | 85.7 | 4 | 100.0 | 27 | 87.1 | 2 | 100.0 |
| Not adequate for age [Percentile <3 (low weight for age) or Percentile >97 (high weight for age] | 4 | 13.3 | 0 | 0.0 | 4 | 14.3 | 0 | 0.0 | 4 | 12.9 | 0 | 0.0 | ||
| Health characteristics | Vomit or refusal to eat* | Yes (had vomited or refused to eat) | 11 | 16.7 | 1 | 25.0 | 10 | 16.9 | 1 | 10.0 | 11 | 17.2 | 1 | 16.7 |
| No | 55 | 83.3 | 3 | 75.0 | 49 | 83.1 | 9 | 90.0 | 53 | 82.8 | 5 | 83.3 | ||
| Presence of infection or inflammation by C reactive protein (CRP) level | Yes (CRP>5.0mg/mL) | 15 | 34.9 | 0 | 0.0 | 15 | 36.6 | 0 | 0.0 | 14 | 33.3 | 1 | 20.0 | |
| No (CRP<5.0mg/mL) | 28 | 65.1 | 3 | 100.0 | 26 | 63.4 | 6 | 100.0 | 28 | 66.7 | 4 | 80.0 | ||
| Glucose | Normal (60.0-180.0mg/dL) | 18 | 100.0 | - | - | 16 | 100.0 | 2 | 100.0 | 15 | 100.0 | 3 | 100.0 | |
| Bilirubin | Hyperbilirubinemia (Bilirubin>1.20mg/dL) | 1 | 9.1 | - | - | 1 | 11.1 | 0 | 0.0 | 0 | 0.0 | 1 | 25.0 | |
| Normal (0.30-1.20mg/dL) | 10 | 90.9 | - | - | 8 | 88.9 | 2 | 100.0 | 7 | 100.0 | 3 | 75.0 | ||
| Urea | Uremia (Blood urea >36.0mg/dL) | 5 | 14.3 | 0 | 0.0 | 3 | 9.4 | 2 | 50.0 | 5 | 15.6 | 0 | 0.0 | |
| Normal (5.0-36.0mg/dL) | 30 | 85.7 | 1 | 100.0 | 29 | 90.6 | 2 | 50.0 | 27 | 84.4 | 4 | 100.0 | ||
| Had any hospitalization (in the past) | Yes | 23 | 35.4 | 0 | 0.0 | 20 | 34.5 | 3 | 30.0 | 18 | 28.6 | 5 | 83.3 | |
| No | 42 | 64.6 | 4 | 100.0 | 38 | 65.5 | 7 | 70.0 | 45 | 71.4 | 1 | 16.7 | ||
| Duration of hospitalization (in days) | Up to 5 days | 6 | 46.2 | - | - | 7 | 58.3 | 0 | 0.0 | 6 | 60.0 | 1 | 33.3 | |
| More than 5 days | 7 | 53.8 | - | - | 5 | 41.7 | 1 | 100.0 | 4 | 40.0 | 2 | 66.7 | ||
| Notes: | (*) Children whose mothers reported a history of food selectivity behavior (e.g., children who eat "normally" at kindergarten or school but refuse to eat the same foods at home), refusal to eat certain types of food (such as meat), or vomiting after consuming certain types of food (e.g., due to irritability or irritated behavior, abdominal pain, or an unspecified reason). | |||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



