
Submitted:
03 December 2024
Posted:
04 December 2024
You are already at the latest version
Abstract
Background/Objectives: Anemia adversely affects children's cognitive and motor devel-25 opment and remains a global public health problem. This study aimed to identify the individual, 26 feeding, household, and community determinants of anemia among children, in Mozambique. 27 Methods: We used pooled datasets of Mozambique representative population-based surveys: the 28 Demographic and Health Surveys (DHS 2022/23 and DHS 2011), the Malaria Indicator Survey 29 (2018), and the Immunization, Malaria and HIV/AIDS Indicator Survey (2015). A total sample of 30 16273 children aged 6-59 months with available hemoglobin testing was included. Multilevel mixed 31 effects analysis was performed using STATA (18.0). Results: The overall prevalence of anemia was 32 71.4%. Children aged 6-11 months were less prone to anemia than children from other age groups 33 (AOR = 0.77, 95% CI = 0.62-0.97). Children who have suffered from illnesses were more likely to 34 have anemia than those who have not (AOR = 1.42, 95% CI = 1.15 -1.74). Children who received 35 Vitamin A supplements are less prone to anemia than those who did not (AOR = 0.76, 95% CI = 0.63- 36 0.93). Children from the highest wealth quintile households were less likely to suffer anemia than 37 their peers (AOR = 0.64, 95% CI = 0.41 -0.93). Overall, 17% of the variability in the prevalence of 38 anemia was attributed to differences between clusters (ICC = 0.17). Conclusions: Childhood anemia 39 remains a critical public health challenge in Mozambique, with prevalence rates exceeding the av-40 erage for Sub-Saharan Africa. The findings underscore the urgent need for multisectoral interven-41 tions targeting individual risk factors and the wider regional disparities contributing to this issue.
Keywords:
Anemia
; childhood
; determinants
; population-based surveys
; Mozambique
; Sub-Saharan Africa
1. Introduction
Anemia is the most common hematologic abnormality identified in infants and children and it adversely affects cognitive and motor development and causes fatigue and low productivity, influencing country development [1,2,3,4]. Anemia is associated with increased morbidity and mortality in children, particularly children of preschool age [2]. Anemic children from disadvantaged communities often fail to achieve their age-related potential, having learning problems and inattentiveness [5]. While iron deficiency is one of the most important factors of anemia, causes for the condition are often multifactorial including other micronutrient deficiencies (such as vitamin B12, and folic acid), infections (e.g. malaria and HIV), and inherited blood diseases. Social and cultural factors may also predispose to anemia [1,6,7,8].
Globally, about 39.8% of children aged 6-59 months are affected by this condition. Low and Middle-income countries bear the highest burden, and anemia risk did not considerably improve over the two decades across most of Africa. In 2019, the prevalence of anemia in children under five was highest in the African Region (with a prevalence rate of 60.2%) [3,7]. Sub-Saharan Africa endures a substantial burden of anemia (overall prevalence rate of 64.1%), showing prevalence variation across the East (56.0%), West (62.2%), Central (75.1%), and Southern (50.7%) regions [9]. Thus, the Sustainable Development Goals (SDGs) targets for anemia reduction might be beyond reach by 2030. The WHO Africa region remains among the most affected, with about 103 million children affected by anemia [3,7]. Anemia serves as a country's growth indicator as it is positively associated with measures of human capital index indicators (such as undernutrition and under-five mortality), with long-term consequences including decreased physical growth, lower educational attainment, cognition, workforce productivity, and wages. Thus, for countries to improve the future economic development of their economies, it is crucial to address the drivers of anemia [10,11,12,13,14,15]. Despite ongoing efforts to address nutritional anemia among children - such as mass deworming, iron supplementation, emergency food assistance, food vouchers, and nutrition counseling - food insecurity persists [16]. As a result, Mozambique continues to be one of the Sub-Saharan African countries with a high burden of childhood anemia, ranking 13th in league tables [16]. This study used a pooled dataset from various national surveys to identify the individual, feeding, household, and community determinants of childhood anemia in Mozambique.
2. Materials and Methods
Study area
The study area of this research was the Republic of Mozambique, located in Southeast Africa. With a long Indian Ocean coastline of 2,700 kilometers, Mozambique is bordered by South Africa, Eswatini, Tanzania, Malawi, Zambia, and Zimbabwe, facing east Madagascar [17]. In 2022, Mozambique´s population was 33 million people, and it’s projected to grow more than double by 2050, to 67.8 million people- which shows the need to address childhood anemia now rather than later [18,19]. The Mozambican population is very young and about two-thirds live and work in rural areas [17,19]. Mozambique has eleven provincial capital cities, including its capital- Maputo City. Mozambique´s Human Development Index is considerably low (185 out of 191 countries in 2021), and the level of education among the Mozambican population is also low, with an average of 4.5 years of schooling for men and 2.7 years for women. The country is often susceptible to natural disasters (cyclones, floods, and droughts) which disrupt the country’s economic development [18,19,20,21]. During natural disasters, poor sanitary conditions and limited access to basic commodities often lead to outbreaks of diseases, particularly, malaria, diarrhea, cholera, and dysentery, and malnutrition resulting from food insecurity is also common [21].
Data source
This study used data from the 2022-2023 Demographic and Health Survey (DHS), the 2018 Malaria Indicator Survey (MIS), the 2015 Immunization, Malaria and HIV/AIDS Indicator Survey (AIS), and the 2011 Demographic and Health Survey (DHS). Data was obtained after administrative approval through The DHS Program website (https://dhsprogram.com/). The DHS 2022-2023, 2018 MIS, 2015 AIS, and DHS 2011 provide information on the health and socio-economic characteristics of the interviewed population, including aspects related to anemia in children under 5 years. More details regarding the methodology used in 2022-2023 DHS, 2018 MIS, 2015 AIS, and DHS 2011 can be found in survey reports publicly available [22,23,24,25].
The 2011 DHS and 2015 AIS comprise a probabilistic, stratified, and multi-stage sample, selected from the 3rd General Population and Housing Census of Mozambique (RPGH 2007), conducted by the Instituto Nacional de Estatística (INE), in 2007. For the 2011 DHS, in the first stage, 611 PSU (Primary Sampling Units) were selected with probability proportional to size, with size being the measure of the number of households in each stratum within each province. In the second sampling stage, 20 households in urban PSUs and 25 households in rural PSUs were selected with equal probabilities. In the third stage, an exhaustive sampling was carried out, and demographic and health data were collected from all women aged 15-49 and children under 5 years old found in the selected households [26]. For the 2015 AIS, the sample design consists of three stages. First, the sample was stratified by province and urban/rural area; subsequently, 307 PSUs were selected through a systematic selection of equal probability. In the second stage, an enumeration area (EA) was selected from each of the 307 PSUs with probability proportional to the size of the enumeration areas (EAs), resulting in a selection of 134 EAs in urban areas and 173 EAs in rural areas. In the third stage, all households were enumerated in each of the 307 EAs [27].
For the MIS 2018, the EAs outlined in the RPGH 2007, updated based on the General Census of Agriculture 2009, were used as the sampling frame. In the first phase, out of the EAs covered in the RPGH 2007, about 224 EAs or conglomerates were selected, with probability proportional to size. Of these EAs, 92 were in urban areas and 132 in rural areas. In urban areas, more samples were collected within the cluster to produce robust estimates for each area or domain. The second sampling phase involved a systematic selection of households within each EA. In each EA, 28 households were selected, totaling a sample size of 6,279 households [28].
As for the 2022-2023 DHS, the sample design consists of two stages. First, a sample of clusters was selected, consisting of EAs defined for the population based on the 4th General Population and Housing Census (RGPH 2017), conducted by the INE, in 2017. A total of 619 EAs were selected with probability proportional to the size, with size being the measure of the number of households in each explicit stratum. Of the 619 EAs, 232 were from urban areas and 387 from rural areas. Due to security concerns, eight districts (Ibo, Macomia, Mocímboa da Praia, Mueda, Muidumbe, Nangade, Palm, and Quissanga) in Cabo Delgado province were excluded from the sample selection. In the second stage, 26 households were systematically selected with equal probabilities from each enumeration area. Based on this procedure, 16,045 households were selected. This number is slightly smaller than the sample size of 16094 because two selected EAs (one in Cabo Delgado and one in Zambézia Province, both rural) could not be completed due to security issues [29]. DHS 20223-2023, DHS 2011, IMASIDA 2015, and MIS 2018 surveys included anemia testing in children aged 6-59 months. For all surveys, testing was performed using the HemoCue® 201+, for measuring the amount of hemoglobin in the blood. Informed consent from the children's guardians was requested before collecting blood samples for anemia testing [22,23,24,25]. This study analyzed a subpopulation of weighted children aged 6-59 months born (and alive) at the time of the survey with available data on hemoglobin testing (n = 16273).
Variables of the study
Supplementary file Table 1 displays additional information on study outcome and exposure variables. Supplementary file Figure 1. shows a conceptual framework for child anemia determinants and consequences. The selection of exposure variables was guided by literature evidence which indicates that such determinants are important factors to be considered about anemia [16,30,31,32,33,34,35,36].
Outcome variable
The outcome variable of this study was anemia among children aged 6 to 59 months. This is generated based on the cut-off hemoglobin threshold. The World Health Organization (WHO) defines anemia in children 6 to 59 months of age as hemoglobin (Hb) of < 11.0 g/L [37,38].
Exposure variables
Exposure variables included children's characteristics (age, gender, birth order, received vitamin A, and child illness). For all surveys, the following variables *had diarrhea recently/past 2 weeks, *had fever recently/past 2 weeks, *had cough recently/past 2 weeks were available. Thus, this was the basis for generating the variable "child illness". Children´s feeding characteristics were also considered (intake of different food groups, such as *cereals, roots and tubers, *legumes and nuts, *dairy products, *flesh foods and eggs, *fruits and vegetables, and *oils and fats). Other characteristics included were the mother´s level of education, age of the mother at childbirth, and frequency of antenatal care visits. This study also considered household (wealth index, source of drinking water, type of toilet facility, pollution within the household, sex of household head, age of household head, children under 5 slept under mosquito bed net) and community factors (residence area and province). The basis for generating the variable "pollution within the household" were the variables "type of cooking fuel" and "smoking cigarette". More details on variables can be found in Supplementary file Table 1.
Statistical analysis
Data analysis was performed considering the requirements for the complex survey data. A weighting variable was generated using the sample weight variable in the DHS [39,40]. We designed a complex survey plan that considered the following variables individual sample weight, sample strata for sampling errors/design, and cluster number [6,33,39,40,41].
Multilevel mixed effects analysis
Since child feeding practices were exclusively measured in the 2011 and 2022-2023 surveys and were missing in the 2015 MIS and 2018 AIS, the pooled data analysis was based only on the 2011 and 2022-2023 DHS sample data [22,23,24,25]. We performed a bivariate analysis for all exposure variables that might be able to influence children´s anemia. Crude odds ratios were presented, and the significance threshold was fixed at a p-value < 0.05 (Supplementary file Table 2). Multivariate models were performed for all exposure variables with a p-value <0.20 in the bivariate analysis [33,40,42]. The first model (empty model) was fitted without independent variables to show the childhood anemia variance among different clusters (communities). The second model contained children´s and maternal-level characteristics. The third model contained children´s feeding level factors, and the fourth model contained household and community level factors. Model 5 included children and maternal, feeding, household, and community-level factors. For all models, the threshold of significance was fixed at a p-value < 0.05 [43,44]. The adjusted odds ratio and 95% confidence intervals (CIs) were presented with the results. The random effect of the models' standard errors (and their 95% CIs) and the inter-cluster correlation coefficient (ICC) for each model were also presented. The comparison of the models was performed by applying the Akaike information criterion (AIC). All analyses were performed using STATA version 18.0.120 software (StataCorp, College Station, Texas, United States) [45].
3. Results
3.1. Study Population Characteristics
The main characteristics of study participants are described in Supplementary file Table 3. Out of a total of 16273 children considered for this study, about 50.5% were female, 24.0% were aged between 12-23 months, and 24.7% were from the lowest wealth quintile. Most of the children lived in rural areas (74.1%), in households with unimproved sanitation (73.1%) and unimproved sources of drinking water (52.2%). Most of the children received vitamin A (68.1%). In general, 28.3% of the children experienced an illness. The overall prevalence of anemia among the sample children was 71.4%.
Supplementary file Table 4 shows the prevalence of anemia by selected variables. Most of the children who were aged 6-11 months (84.0%), whose mothers had no schooling (74.0%), lived in households with unimproved sources of drinking water (74.8%), unimproved sanitation (73.3%) and lowest wealth quintile (79.7%) were anemic. Similarly, a relevant share of children living in rural areas (73.9%), and in the provinces of Zambezia (79.2%), Cabo Delgado (78.5%), and Nampula (77.4%) had anemia.
3.2. The Random Effect of Anemia
Model 5 (which includes children and maternal, feeding, household, and community-level factors variables) demonstrates better performance in capturing associations between childhood anemia and selected variables (AIC of 8,824), as supported by improved model fit statistics and random effect estimates (Table 1).
On the other hand, there is a notable clustering of anemia at both regional (ICC of 5.1%, in Model 1) and community levels within regions (ICC of 16.4%, in Model 1), indicating variability in anemia prevalence across different geographic levels.
3.3. Determinants of Anemia Among Children Living in Mozambique
Table 2 shows the association between each factor and anemia in children aged 6 to 59 months. According to Model 5, the child's age, having an illness, and having received Vitamin A supplement play a pivotal role in childhood anemia. Furthermore, the household wealth index and the source of drinking water significantly impact anemia prevalence (p<0.05).
Children aged 6-11 months are less prone to anemia than children from other age groups (AOR = 0.77, 95% CI = 0.62-0.97) and the odds of anemia decrease significantly as the child´s age increases (Figure 1).
Children who have suffered from illnesses are more likely to have anemia than those who have not had illnesses (AOR = 1.42, 95% CI = 1.15 -1.74). Children who received Vitamin A supplements are less prone to anemia than those who did not receive supplements (AOR = 0.76, 95% CI = 0.63- 0.93). Children from the highest wealth quintile households were less likely to suffer anemia than those from the lowest wealth quintiles (AOR = 0.64, 95% CI = 0.41 -0.93) (Figure 2).
Our results also show that children living in households that use unimproved drinking water sources are more prone to anemia than those who live in households that use improved sources (AOR = 1.32, 95% CI = 1.11-1.57) (Table 2).
4. Discussion
This study examined the determinants of anemia among children aged 6-59 months in Mozambique. Throughout the years, the prevalence of anemia in Mozambican children aged 6 to 59 months was found to be 71.4%. The rate reported in our study is above the average of sub-Saharan Africa (64.1%) and East Africa region prevalence (56.0%), being much higher than in countries such as Malawi (63.0%), Burundi (60.9%), Rwanda (53.0 %) and Ethiopia (49.3%) [9,40,46,47]. This rate is also higher than in countries such as Angola (65%), Chad (59.6%), Cape Verde (51.8%), and Egypt (52.0%) [48,49,50,51]. On the other hand, this rate is lower than those reported in some countries from West Africa such as Mali (76-88%), Guinea Bissau (80.2%), and Ghana (78.0%) [52,53,54]. Such disparities in anemia prevalence rates among these countries may be explained by geographical, climate, socioeconomic, and cultural factors [55]. Our results indicate that Mozambique has shown no progress, it´s even worsening and is still far from achieving the global nutrition target by 2030 to reduce anemia rates to less than 15% in children, remaining a severe public health problem [32,38,56,57,58]. The study findings also underscore the relevance of community-level factors in influencing health outcomes. Such persistent high rates of anemia might have an impact on the Mozambique's overall development, as they can harm school performance, productivity in adult life, and overall quality of life in general and may also lead to negative financial impacts for individuals, families, and communities [57,59].
Our study showed that the child´s age, presence of illness, having received Vitamin A supplements, wealth index, and the source of drinking water were determinants for anemia in Mozambican children.
Child's Age and Childhood Anemia
In line with our findings, previous studies [32,51,60,61,62,63] have also shown that anemia risk lowers as children grow and get older. This might be due to maternal anemia and poor young children's feeding practices during the initiation of complementary feeding [64]. Some studies [65,66,67] showed that maternal iron deficiency plays a substantial role in the iron status of their infants, with mothers’ hemoglobin levels contributing to the variation in their infants’ hemoglobin concentration, in the first six months of life. Children born to anemic mothers often have limited iron reserves, even when born at full term and with normal weight [65]. On the other hand, younger children have higher iron demands linked to early childhood development, and the lack of essential nutrients in their diet may lead to nutritional deficiencies, including iron anemia deficiency. Similarly, the growth spurt coupled with the termination of lactation around 12 months of age also poses a high nutrient demand and often is not reached. As such a good complementary diet, rich in external sources of iron is mandatory to achieve the high iron demands in childhood [60,64,68,69]. The reinforcement of regular monitoring of anemia risk at child healthcare visits, particularly in those aged 12-23 months could help to enable early detection and prompt intervention, contributing to reducing anemia´s prevalence [30]. Mozambique still faces huge challenges linked to the necessity of commodities in health facilities. Previous studies show that only 12.4% of health facilities, at the national level, are ready to deliver nutrition interventions related to anemia testing, and iron and folic acid supplementation through the prevention of mother-to-child transmission services [70]. Thus, more investment and coordinated support from key stakeholders can contribute greatly to overcoming this constraint and tackling children's anemia, improving their health and development [71]. It is crucial to bolster the primary health care network in-country, by ensuring enough skilled staff, essential medicines, and supplies – especially for vulnerable groups like children. Strengthening this network can increase equitable coverage and access to essential health programs such as childcare and nutrition, and contribute to tackling anemia [72,73].
Presence of Illness and Childhood Anemia
This study´s findings concur well with previous studies that showed that children with a history of illnesses (fever, cough, or diarrhea) have a higher risk of being anemic [48, 58). This might be linked to the fact that fever is a symptom of acute febrile illness (such as malaria), resulting in anemia due to the destruction of red blood cells [48,64,74]. Additionally, infectious diseases can decrease the intake and absorption of nutrients, cause intestinal mucosa injury, and induce autoimmune reactions leading to anemia. Children who are sick often lose their appetite, which might also lead to nutritional deficiencies [74,75]. A joint statement by the WHO and the United Nations Children's Fund (UNICEF) was issued in 2006, advising that, in settings where malaria and other infectious disease prevalence is high, iron and folic acid supplementation should be targeted at young children who are anemic and at risk of iron deficiency, in the presence of effective infectious disease control [76]. However as mentioned before, Mozambique needs coordinated action, with the support of partners, to overcome several constraints linked with the limited readiness for delivering iron and acid folic supplementation interventions at health facilities.
Vitamin A Supplementation and Childhood Anemia
Similarly to earlier findings [51] we found out that children who received vitamin A supplements were less prone to suffer anemia than children who did not. The existence of a relationship between vitamin A and anemia is well-reported [77,78]. It is known that vitamin A supplementation contributes to reducing anemia´s prevalence, through several mechanisms, such as the increase in the growth and differentiation of erythrocyte progenitor cells and modulation of bioavailability and mobilization of tissue iron stores [77,78]. Vitamin A supplementation has beneficial effects for preventing the risk of death in children aged 6 to 59 months who are at risk of vitamin A deficiency and play a crucial role in reducing illness (e.g. new occurrences of diarrhea and measles) [79]. As such, vitamin A supplementation indirectly contributes to preventing and reducing important children´s anemia risk factors (e.g. diarrhea and fever) [79,80]. Since 2008, the Ministry of Health (MoH) of Mozambique through the technical and financial support of UNICEF and other partners, started with the implementation of the "National Health Weeks", largely as a response to the low coverage of vitamin A supplementation in routine health services in previous years. This initiative although it achieved high vitamin A supplementation coverage is still not quite sustainable due to the high financial cost. Since 2017, the MoH has been investing efforts to strengthen routine health services, as the main vehicle for administering vitamin A capsules, to all eligible children [81]. In addition to that, the MoH has been conducting efforts by creating mobile brigades with health providers or community health agents (Agentes Polivalentes de Saúde, APSs, in Portuguese) to reach children in the community, where they give lectures with messages encouraging mothers and caregivers to feed their children and babies with foods rich in vitamin A [81]. Nonetheless, the mobile brigade strategy is not always sustainable because most communities are far from health centers, combined with the problem of lack of transport and fuel and cost allowances for health providers [81]. However, while these mobile brigades remain to be carried on, they can still be used to reinforce lectures on proper feeding habits focusing on preventing anemia in children.
Socioeconomic Status and Childhood Anemia
As suggested by previous authors [32,64,74,82,83], the evidence we found points to the fact that the wealth index plays a pivotal role in anemia, with children from the highest wealth quintile households having more risk to suffer anemia than their peers. This could be because caregivers of children from high socioeconomic classes can have better access to and afford good prevention and care health services, as they don´t face major financial constraints [83]. Families from high socioeconomic classes can purchase and provide good nutritious foods, and ensure adequate dietary patterns for their children, decreasing anemia risk [83]. On the other hand, children from low-wealth quintiles often are exposed to community poverty, living in contexts of limited access to health care, lack of social services, lack of proper sanitation, and fewer job opportunities as they grow older [74]. Furthermore, our analysis period coincides with the COVID-19 pandemic that led Mozambique to experience its first severe economic contraction in almost 30 years, affecting enterprises and households, causing income losses, and worsening living conditions [84]. In addition, other studies show there is a high degree of poverty immobility, particularly in the northern and central regions of Mozambique, and education is a crucial factor for moving from the poor to the vulnerable group and from the vulnerable to the nonvulnerable group (across wealth quintiles) [85]. Many years of progress in the fight against poverty in Mozambique suffered a step backward and need a multisectoral approach by the government of Mozambique and its partners, to revert to a downward trend for the poverty rates, aiming at reducing socioeconomic inequalities and thus contribute to tackling children´s anemia [84,86]. Strategies and policies to achieve this goal, include more investments in rural development, increasing the productivity of smallholder farmers, expanding markets to enable subsistence farmers to shift to commercial and sustainable agriculture, and more efforts to improving schooling and health literacy, particularly among women due to their role as child´s caregivers [84,85].
Water and Sanitation and Childhood Anemia
Our results corroborate previous results [48,87], showing that children living in households that use unimproved drinking water sources are more likely to have anemia than their peers, as they are more exposed to acute and chronic infections linked with increased pathogens exposure due to environmental contamination. Policies aimed at improving water sanitation, particularly in low-income settings (within the country) contribute to improving children´s health and preventing anemia [87]. Some authors [82] argue that improved water sanitation can help to prevent infections and reduce enteropathy leading to better iron absorption and reduced loss of nutrients through lower diarrhea prevalence, thus tackling anemia. Shreds of evidence from studies performed in Burkina Faso [88] and India [82], showed an association between access to improved water sanitation and latrines/boreholes to an improved nutritional status in children younger than 5 years, as well, as better protection from enteric exposure. Kothari and collaborators [82] suggest that implementing water, sanitation, and hygiene interventions side-by-side with nutrition-specific interventions (in addition to malaria) is highly relevant, for achieving success in preventing and managing anemia in high-infection burden settings. Nonetheless, further research is required in Mozambique, to explore the interaction between water sanitation (including water off household premises and water quality) and childhood anemia.
5. Conclusions
This study revealed that childhood anemia remains a severe public health problem in Mozambique. The findings underscore the importance of community-level factors in influencing health outcomes, highlighting the urgent need for interventions that address not only individual risk factors but also the wider regional disparities that contribute to this issue. Thus, tackling childhood anemia will require a set of multisectoral approaches involving the government and stakeholders to enhance the provision of anemia essential supplies (such as vitamin A, iron, and acid folic supplements) at primary health care at the national level and reinforce the regular monitoring of anemia risk at child healthcare visits, by health providers and nutritionists, particularly in those aged 12–23 months. Efforts should also be aimed at reducing socioeconomic inequalities through more investments in rural development and sustainable agriculture, improving water sanitation, and, improving schooling and health literacy among children´s caregivers. Continuous and further research on childhood anemia (including feeding habits) in this setting can contribute hugely to leaving no one behind and reaching global nutrition goals.
Strengths and Limitations
There are several strengths linked to our study. Although there are studies on anemia in children in Mozambique, to our knowledge, this is the first study that, in addition to social, maternal, and community factors, also includes the analysis of dietary factors and anemia in children aged 6-59 months. Our study was based on 04 nationally representative surveys (2022-2023 DHS, 2018 MIS, 2015 AIS, and 2011 DHS). The data was weighted, and genuine and reliable estimations and standard errors were provided through multivariate logistic regression. The results obtained in this study, corroborate with current literature, and can greatly contribute to improving multisectoral strategies, designing interventions tailored to the needs of specific groups, and implementing a more holistic approach to reducing anemia in Mozambican children.
Some limitations of this study are linked to the fact that we used secondary data and issues related to data collection of some variables that may be affected by memory participants leading to recall bias and misclassification. For common morbidities (such as malaria and HIV) and other possibly relevant factors (such as worm infestation and food insecurity), direct measures were not available in the datasets. Thus, and similarly, to previous studies [32,89] we used proxies for suspected malaria (e.g children under 5 that slept under a bed net, and have had a fever recently), for worm infestation (e.g. household sanitation), and food insecurity (e.g. household wealth index).
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary file. Table 1. Study outcome and exposure variables. Supplementary file. Figure 1. Conceptual framework for child anemia determinants and consequences. Supplementary file. Table 2. Bivariate analysis. Supplementary file. Table 3. Unweighted distribution of study variables. Supplementary file. Table 4. Prevalence of anemia by the selected categorical variables.
Author Contributions
Conceptualization: RMC, RM, RW, MPG, IC, and LV; Methodology: RMC, RM, RW, and MPG; Dataset extraction: RMC, RM, and RW; Formal Analysis: RMC, RM, RW, and MPG ; Investigation: RMC, RM, RW, and MPG; Resources: RMC, RM, RW, and MPG; Data Curation: RMC, RM, RW and MPG; Writing-Original Draft Preparation: RMC; Writing—Review and Editing: RMC, RM, RW, MPG, IC, and LV; Visualization: RMC, RW and MPG; Supervision: IC and LV. All authors have read and agreed to the published version of the manuscript.
Funding
RMC., LV., and IC. were supported by Fundação para a Ciência e a Tecnologia for funds to GHTM - UID/04413/2020 and LA-REAL – LA/P/0117/2020. RMC was supported by Fundação para a Ciência e a Tecnologia for funds for her Doctoral Program (UI/BD/151065/2021; https://doi.org/10.54499/UI/BD/151065/2021). The views expressed in this paper are from the authors and not the official position of the institutions or funder.
Institutional Review Board Statement
The data used in this study is publicly available online at The DHS Program website (https://www.dhsprogram.com/data/available-datasets.cfm). The DHS Program granted administrative access upon request. This research is also a sub-study – that integrates the study protocol on the same topic (PAMC, Ref. Of 0110/CC/2020) that was approved by the Institutional Committee of Bioethics in Health of the Faculty of Medicine/Maputo Central Hospital (CIBS FM&HCM/004/2020).
Informed Consent Statement
Data Availability Statement
Data generated during this study is available in this article and its supplementary information files.
Acknowledgments
The authors would like to thank the ICF-DHS Program, the National Statistics Institute, and the National Institute of Health of Mozambique. The first author would like to thank Maria João Mbebe, António Carlos Langa, Dalila Maulide Ibraimo, Laura Neto, Fernando Pina and Victor Manuel Guedes Pereira. Special thanks to Michel Jareski Andrade for his valuable support in formatting the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Leung AK, C.; Lam, J.M.; Wong AH, C.; Hon, K.L.; Li, X. Iron Deficiency Anemia: An Updated Review. Current Pediatric Reviews 2024, 20, 339–356. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, P.G. Anemia in the pediatric patient. Blood 2022, 140, 571–593. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Anaemia in women and children. WHO Global Anaemia estimates, 2021 Edition. Retrieved May 21, 2024. 2021. Available online: https://www.who.int/data/gho/data/themes/topics/anaemia_in_women_and_children.
- Lozoff, B.; Beard, J.; Connor, J.; Barbara, F.; Georgieff, M.; Schallert, T. Long-lasting neural and behavioral effects of iron deficiency in infancy. Nutrition reviews 2006, 64(5 Pt 2), S34–S91. [Google Scholar] [CrossRef]
- Gwetu, T.P.; Taylor, M.; Chhagan, M.; Kauchali, S.; Craib, M. Health and educational achievement of school-aged children: The impact of anaemia and iron status on learning. Health SA = SA Gesondheid 2019, 24, 1101. [Google Scholar] [CrossRef] [PubMed]
- Nuwabaine, L.; Kawuki, J.; Kamoga, L.; Sserwanja, Q.; Gatasi, G.; Donkor, E.; Mutisya, L.M.; Asiimwe, J.B. Factors associated with anaemia among pregnant women in Rwanda: an analysis of the Rwanda demographic and health survey of 2020. BMC pregnancy and childbirth 2024, 24, 328. [Google Scholar] [CrossRef]
- Daru, J. Sustainable Development Goals for anaemia: 20 years later, where are we now? The Lancet. Global health 2022, 10, e586–e587. [Google Scholar] [CrossRef]
- Weze, K.; Abioye, A.I.; Obiajunwa, C.; Omotayo, M. Spatio-temporal trends in anaemia among pregnant women, adolescents and preschool children in sub-Saharan Africa. Public health nutrition 2021, 24, 3648–3661. [Google Scholar] [CrossRef]
- Tesema, G.A.; Worku, M.G.; Tessema, Z.T.; Teshale, A.B.; Alem, A.Z.; Yeshaw, Y.; Alamneh, T.S.; Liyew, A.M. Prevalence and determinants of severity levels of anemia among children aged 6-59 months in sub-Saharan Africa: A multilevel ordinal logistic regression analysis. PloS one 2021, 16, e0249978. [Google Scholar] [CrossRef]
- Asmare, A.A.; Agmas, Y.A. Determinants of coexistence of undernutrition and anemia among under-five children in Rwanda; evidence from 2019/20 demographic health survey: Application of bivariate binary logistic regression model. PloS one 2024, 19, e0290111. [Google Scholar] [CrossRef]
- Akseer, N.; Al-Gashm, S.; Mehta, S.; Mokdad, A.; Bhutta, Z.A. Global and regional trends in the nutritional status of young people: a critical and neglected age group. Annals of the New York Academy of Sciences 2017, 1393, 3–20. [Google Scholar] [CrossRef]
- Murthi, M.; Shekar, M. Breastfeeding: A Key Investment in Human Capital. Pediatrics 2021, 147, e2020040824. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.P.; Chen-Edinboro, L.P.; Caulfield, L.E.; Murray-Kolb, L.E. The impact of anemia on child mortality: an updated review. Nutrients 2014, 6, 5915–5932. [Google Scholar] [CrossRef] [PubMed]
- Victora, C. G., Adair, L., Fall, C., Hallal, P. C., Martorell, R., Richter, L., Sachdev, H. S.,; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [PubMed]
- Brabin, B.J.; Premji, Z.; Verhoeff, F. An analysis of anemia and child mortality. The Journal of Nutrition 2001, 131(2S-2), 636S–648S. [Google Scholar] [CrossRef] [PubMed]
- Muhajarine, N., Adeyinka, D. A., Matandalasse, M.,; Chicumbe, S. Inequities in childhood anaemia at provincial borders in Mozambique: Cross-sectional study results from multilevel Bayesian analysis of 2018 National Malaria Indicator Survey. BMJ Open 2021, 11, e051395. [Google Scholar] [CrossRef]
- The World Bank. The World Bank in Mozambique: Overview. Retrieved May 2, 2024. 2024. Available online: https://www.worldbank.org/en/country/mozambique/overview.
- United States Census Bureau. Mozambique: Population Vulnerability and Resilience Profile. Retrieved May 2, 2024. 2024. Available online: https://www.census.gov/programs-surveys/international-programs/data/population-vulnerability/mozambique.html.
- USAID. Mozambique: Nutrition Profile. Retrieved May 2, 2024. 2021. Available online: https://www.usaid.gov/document/mozambique-nutrition-profile.
- United Nations, Department of Economic and Social Affairs, Population Division. (2020). World fertility and family planning 2020. Retrieved July 3, 2024, from https://www.un.org/en/development/desa/population/publications/pdf/family/Ten_key_messages%20for%20WFFP2020_highlights.pdf.
- WHO Africa. (2024). Health Topics (Mozambique). Retrieved May 3, 2024, from https://www.afro.who.int/countries/mozambique/topic/health-topics-mozambique.
- Instituto Nacional de Estatística (INE) & ICF. (2024). Inquérito Demográfico e de Saúde em Moçambique 2022–23. Maputo, Moçambique e Rockville, Maryland, EUA: INE e ICF. Retrieved May 20, 2024, from https://dhsprogram.com/pubs/pdf/FR389/FR389.pdf.
- Instituto Nacional de Saúde (INS) & ICF. (2019). Inquérito Nacional sobre Indicadores de Malária em Moçambique 2018. Maputo, Moçambique. Rockville, Maryland, EUA: INS e ICF. Retrieved May 3, 2024, from https://dhsprogram.com/pubs/pdf/MIS33/MIS33.pdf.
- Ministério da Saúde (MISAU), Instituto Nacional de Estatística (INE), & ICF Internacional. (2016). Inquérito de Indicadores de Imunização, Malária e HIV/SIDA em Moçambique 2015. Retrieved May 3, 2024, from https://dhsprogram.com/pubs/pdf/ais12/ais12.pdf.
- Instituto Nacional de Estatística (INE). (2011). Moçambique—Inquérito Demográfico e de Saúde 2011. Retrieved May 3, 2024, from https://dhsprogram.com/pubs/pdf/fr266/fr266.pdf.
- The World Bank. (2013). Demográfico e de Saúde 2011. Study description. Microdata Library. Retrieved May 3, 2024, from https://microdata.worldbank.org/index.php/catalog/1563/study-description.
- The World Bank. (2018). Inquérito de Indicadores de Imunização, Malária e HIV/SIDA 2015 Study description. Microdata Library. Retrieved May 3, 2024, from https://microdata.worldbank.org/index.php/catalog/2977#study_desc1674579234511.
- The World Bank. (2019). Inquérito Nacional sobre Indicadores de Malária 2018. Study description. Microdata Library. Retrieved May 3, 2024, from https://microdata.worldbank.org/index.php/catalog/3488/study-description.
- The World Bank. (2024a). Inquérito Demográfico e de Saúde 2022-2023. Study description. Microdata Library. Retrieved May 3, 2024, from https://microdata.worldbank.org/index.php/catalog/6247.
- Usanzineza, H.; Nsereko, E.; Niyitegeka, J.P.; Uwase, A.; Tuyishime, D.H.; Sunday, F.X.; Mazimpaka, C.; Ahishakiye, J. Prevalence and risk factors for childhood anemia in Rwanda: Using Rwandan demographic and health survey 2019–2020. Public Health Challenges 2024, 3, e159. [Google Scholar] [CrossRef]
- Christian, A.K.; Afful-Dadzie, E.; Marquis, G.S. Infant and young child feeding practices are associated with childhood anaemia and stunting in sub-Saharan Africa. BMC Nutrition 2023, 9. [Google Scholar] [CrossRef]
- Heinrichs, H.; Endris, B.S.; Dejene, T.; Dinant, G.J.; Spigt, M. Anaemia and its determinants among young children aged 6-23 months in Ethiopia (2005-2016). Maternal & child nutrition 2021, 17, e13082. [Google Scholar] [CrossRef]
- Mohammed, S.; Larijani, B.; Esmaillzadeh, A. Concurrent anemia and stunting in young children: Prevalence, dietary and non-dietary associated factors. Nutrition Journal 2019, 18. [Google Scholar] [CrossRef]
- Prieto-Patron, A.; Van der Horst, K.; Hutton, Z.V.; Detzel, P. Association between Anaemia in Children 6 to 23 Months Old and Child, Mother, Household and Feeding Indicators. Nutrients 2018, 10, 1269. [Google Scholar] [CrossRef]
- USAID. (2013). Conceptual frameworks for anemia. Retrieved May 27, 2024, from https://spring-nutrition.org/sites/default/files/events/multisectoral_anemia_meeting_diagrams.pdf.
- MOST, USAID Micronutrient Program. (2004). A strategic approach to anemia control programs. Arlington, VA: MOST, USAID Micronutrient Program.
- Owais, A.; Merritt, C.; Lee, C.; Bhutta, Z.A. Anemia among Women of Reproductive Age: An Overview of Global Burden, Trends, Determinants, and Drivers of Progress in Low- and Middle-Income Countries. Nutrients 2021, 13, 2745. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. (2011). Vmnis: Vitamin and mineral nutrition information system. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Geneva, Switzerland: WHO. Retrieved May 20, 2024, from https://www.who.int/publications/i/item/WHO-NMH-NHD-MNM-11.1.
- Croft, T. N., Allen, C. K., Zachary, B. W., et al. (2023). Guide to DHS Statistics. Rockville, Maryland, USA: ICF. Retrieved from https://www.dhsprogram.com/pubs/pdf/DHSG1/Guide_to_DHS_Statistics_DHS-8.pdf.
- Wasswa, R.; Kananura, R.M.; Muhanguzi, H.; Waiswa, P. Spatial variation and attributable risk factors of anaemia among young children in Uganda: Evidence from a nationally representative survey. PLOS Global Public Health 2023, 3, e0001899. [Google Scholar] [CrossRef] [PubMed]
- Armah-Ansah, E.K. Determinants of anemia among women of childbearing age: analysis of the 2018 Mali demographic and health survey. Archives of Public Health = Archives Belges de Sante Publique 2023, 81, 10. [Google Scholar] [CrossRef] [PubMed]
- El Sanharawi, M.; Naudet, F. Comprendre la régression logistique [Understanding logistic regression]. Journal Francais d'Ophtalmologie 2013, 36, 710–715. [Google Scholar] [CrossRef]
- Yakum, M.N.; Atanga, F.D.; Ajong, A.B.; Eba Ze, L.E.; Shah, Z. Factors associated with full vaccination and zero vaccine dose in children aged 12-59 months in 6 health districts of Cameroon. BMC Public Health 2023, 23, 1693. [Google Scholar] [CrossRef]
- Danaei, G.; Andrews, K.G.; Sudfeld, C.R.; Fink, G.; McCoy, D.C.; Peet, E.; Sania, A.; Smith Fawzi, M.C.; Ezzati, M.; Fawzi, W.W. Risk Factors for Childhood Stunting in 137 Developing Countries: A Comparative Risk Assessment Analysis at Global, Regional, and Country Levels. PLoS medicine 2016, 13, e1002164. [Google Scholar] [CrossRef]
- StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC.
- Hailu, B.A. Mapping, trends, and factors associated with anemia among children aged under 5 y in East Africa. Nutrition 2023, 116, 112202. [Google Scholar] [CrossRef]
- Sahiledengle, B.; Mwanri, L.; Agho, K.E. Household environment associated with anaemia among children aged 6–59 months in Ethiopia: A multilevel analysis of Ethiopia demographic and health survey (2005–2016). BMC Public Health 2024, 24. [Google Scholar] [CrossRef]
- Austin, A.M.; Fawzi, W.; Hill, A.G. Anaemia among Egyptian Children between 2000 and 2005: trends and predictors. Maternal & Child Nutrition 2012, 8, 522–532. [Google Scholar] [CrossRef]
- Semedo, R.M.; Santos, M.M.; Baião, M.R.; Luiz, R.R.; da Veiga, G.V. Prevalence of anaemia and associated factors among children below five years of age in Cape Verde, West Africa. Journal of Health, Population, and Nutrition 2014, 32, 646–657. [Google Scholar]
- Fançony, C.; Lavinha, J.; Brito, M.; Barros, H. Anemia in preschool children from Angola: a review of the evidence. Porto Biomedical Journal 2020, 5, e60. [Google Scholar] [CrossRef] [PubMed]
- Zavala, E.; Adler, S.; Wabyona, E.; Ahimbisibwe, M.; Doocy, S. Trends and determinants of anemia in children 6-59 months and women of reproductive age in Chad from 2016 to 2021. BMC Nutrition 2023, 9, 117. [Google Scholar] [CrossRef] [PubMed]
- Thorne, C.J.; Roberts, L.M.; Edwards, D.R.; Haque, M.S.; Cumbassa, A.; Last, A.R. Anaemia and malnutrition in children aged 0-59 months on the Bijagós Archipelago, Guinea-Bissau, West Africa: a cross-sectional, population-based study. Paediatrics and International Child Health 2013, 33, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Shenton, L.M.; Jones, A.D.; Wilson, M.L. Factors associated with anemia status among children aged 6–59 months in Ghana 2020, 2003–2014. Maternal and Child Health Journal 24, 483–502. [CrossRef]
- Gebreegziabher, T.; Sidibe, S. Prevalence and contributing factors of anaemia among children aged 6-24 months and 25-59 months in Mali. Journal of Nutritional Science 2023, 12, e112. [Google Scholar] [CrossRef]
- Obeagu, E.I.; Obeagu, G.U. Tackling childhood anemia in malaria zones: Comprehensive strategies, challenges, and future directions. Academia Medicine 2024, 1. [Google Scholar] [CrossRef]
- Global Nutrition Report (GNR). (2024). Mozambique: The burden of malnutrition at a glance. Retrieved May 20, 2024, from https://globalnutritionreport.org/resources/nutrition-profiles/africa/eastern-africa/mozambique/.
- World Health Organization. (2019). Nutrition landscape information system (Nlis): Anaemia. Nutrition and nutrition-related health and development data. Geneva, Switzerland: WHO. Retrieved May 20, 2024, from https://iris.who.int/bitstream/handle/10665/332223/9789241516952-eng.pdf?sequence=1.
- Maulide Cane, R.; Keita, Y.; Lambo, L.; Pambo, E.; Gonçalves, M.P.; Varandas, L.; Craveiro, I. Prevalence and factors related to anaemia in children aged 6–59 months attending a quaternary health facility in Maputo, Mozambique. Global Public Health 2023, 18. [Google Scholar] [CrossRef]
- Zavaleta, N.; Astete-Robilliard, L. Efecto de la anemia en el desarrollo infantil: consecuencias a largo plazo [Effect of anemia on child development: long-term consequences]. Revista Peruana de Medicina Experimental y Salud Publica 2017, 34, 716–722. [Google Scholar] [CrossRef]
- Engidaye, G., Melku, M., Yalew, A.,; et al. Under nutrition, maternal anemia and household food insecurity are risk factors of anemia among preschool aged children in Menz Gera Midir district, Eastern Amhara, Ethiopia: A community based cross-sectional study. BMC Public Health 2019, 19, 968. [Google Scholar] [CrossRef]
- Patel, K.K.; Vijay, J.; Mangal, A.; Mangal, D.K.; Gupta, S.D. Burden of anaemia among children aged 6–59 months and its associated risk factors in India – Are there gender differences? Children and Youth Services Review 2021, 122, 10591. [Google Scholar] [CrossRef]
- Sun, J., Wu, H., Zhao, M., Magnussen, C. G.,; Xi, B. Prevalence and changes of anemia among young children and women in 47 low- and middle-income countries, 2000-2018. EClinicalMedicine 2021, 41, 101136. [Google Scholar] [CrossRef] [PubMed]
- Agho, K.E.; Chitekwe, S.; Rijal, S.; Paudyal, N.; Sahani, S.K.; Akombi-Inyang, B.J. Association between child nutritional anthropometric indices and iron deficiencies among children aged 6–59 months in Nepal. Nutrients 2024, 16, 698. [Google Scholar] [CrossRef] [PubMed]
- Alamneh, T.S.; Melesse, A.W.; Gelaye, K.A. Determinants of anemia severity levels among children aged 6-59 months in Ethiopia: Multilevel Bayesian statistical approach. Scientific Reports 2023, 13, 4147. [Google Scholar] [CrossRef] [PubMed]
- Teixeira M de LP, D.; Lira PI, C.; Coutinho, S.B.; Eickmann, S.H.; Lima M de, C. Influence of breastfeeding type and maternal anemia on hemoglobin concentration in 6-month-old infants. J Pediatr (Rio J) 2010, 86, 65–72. [Google Scholar] [CrossRef]
- Zeeshan, F.; Bari, A.; Farhan, S.; Jabeen, U.; Rathore, A.W. Correlation between maternal and childhood VitB12, folic acid and ferritin levels. Pakistan Journal of Medical Sciences 2017, 33, 162–166. [Google Scholar] [CrossRef]
- Marques, R.d.e.F.; Taddei, J.A.; Konstantyner, T.; Marques, A.C.; Braga, J.A. Correlation between hemoglobin levels of mothers and children on exclusive breastfeeding in the first six months of life. Jornal de Pediatria 2016, 92, 479–485. [Google Scholar] [CrossRef]
- Miniello, V.L.; Verga, M.C.; Miniello, A.; Di Mauro, C.; Diaferio, L.; Francavilla, R. Complementary feeding and iron status: "The unbearable lightness of being" infants. Nutrients 2021, 13, 4201. [Google Scholar] [CrossRef]
- Mutonhodza, B.; Dembedza, M.P.; Lark, M.R.; Joy EJ, M.; Manzeke-Kangara, M.G.; Njovo, H.; Nyadzayo, T.K.; Kalimbira, A.A.; Bailey, E.H.; Broadley, M.R.; Matsungo, T.M.; Chopera, P. Anemia in children aged 6-59 months was significantly associated with maternal anemia status in rural Zimbabwe. Food Science & Nutrition 2022, 11, 1232–1246. [Google Scholar] [CrossRef]
- Maulide Cane, R., Sheffel, A., Salomão, C.,; et al. Structural readiness of health facilities in Mozambique: How is Mozambique positioned to deliver nutrition-specific interventions to women and children? Journal of Global Health Reports 2023, 7, e2023074. [Google Scholar] [CrossRef]
- Amaro, M. Accelerating progress in micronutrient deficiencies in Mozambique: A Ministry of Health perspective. Maternal & Child Nutrition 2019, 15 Suppl 1, e12707. [Google Scholar] [CrossRef]
- World Health Organization. (2024). Strengthening primary health care with a community health strategy in Mozambique. World Health Organization. Retrieved September 13, 2024, from https://www.who.int/news-room/feature-stories/detail/strengthening-primary-health-care-with-a-community-health-strategy-in-mozambique.
- Van Weel, C.; Kidd, M.R. Why strengthening primary health care is essential to achieving universal health coverage. Canadian Medical Association Journal = Journal de l'Association Medicale Canadienne 2018, 190, E463–E466. [Google Scholar] [CrossRef] [PubMed]
- Gebrehaweria Gebremeskel, M.; Lemma Tirore, L. Factors Associated with Anemia Among Children 6-23 Months of Age in Ethiopia: A Multilevel Analysis of Data from the 2016 Ethiopia Demographic and Health Survey. Pediatric Health, Medicine and Therapeutics 2020, 11, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Tegegne, M.; Abate, K.H.; Belachew, T. Anaemia and associated factors among children aged 6-23 months in agrarian community of Bale zone: a cross-sectional study. Journal of Nutritional Science 2022, 11, e96. [Google Scholar] [CrossRef] [PubMed]
- Harding, K.B.; Neufeld, L.M. Iron deficiency and anemia control for infants and young children in malaria-endemic areas: a call to action and consensus among the research community. Advances in Nutrition 2012, 3, 551–554. [Google Scholar] [CrossRef]
- Jimenez, C.; Leets, I.; Puche, R.; Anzola, E.; Montilla, R.; Parra, C.; Aguilera, A.; García-Casal, M.N. A single dose of vitamin A improves haemoglobin concentration, retinol status and phagocytic function of neutrophils in preschool children. The British Journal of Nutrition 2010, 103, 798–802. [Google Scholar] [CrossRef]
- Silva AD, P.; Pereira AD, S.; Simões BF, T.; Omena, J.; Cople-Rodrigues CD, S.; De Castro IR, R.; Citelli, M. Association of vitamin A with anemia and serum hepcidin levels in children aged 6 to 59 mo. Nutrition 2021, 91-92, 111463. [Google Scholar] [CrossRef]
- Imdad, A.; Mayo-Wilson, E.; Haykal, M.R.; Regan, A.; Sidhu, J.; Smith, A.; Bhutta, Z.A. Vitamin A supplementation for preventing morbidity and mortality in children from six months to five years of age. The Cochrane Database of Systematic Reviews 2022, 3, CD008524. [Google Scholar] [CrossRef]
- Semba, R.D.; de Pee, S.; Ricks, M.O.; Sari, M.; Bloem, M.W. Diarrhea and fever as risk factors for anemia among children under age five living in urban slum areas of Indonesia. International Journal of Infectious Diseases : IJID : official publication of the International Society for Infectious Diseases 2008, 12, 62–70. [Google Scholar] [CrossRef]
- INS, MISAU, & UNICEF. (2022). Relatório sobre avaliação da suplementação com vitamina A nos cuidados de saúde primários nas províncias de Sofala, Manica, Tete, Zambézia e Nampula (ASUVA) - Uma avaliação da implementação, Retrieved May 28, 2024, from https://drive.google.com/file/d/16LDjk_u4TWx9nX3MonjU8rjpK-omlKhy/view.
- Kothari, M.T.; Coile, A.; Huestis, A.; Pullum, T.; Garrett, D.; Engmann, C. Exploring associations between water, sanitation, and anemia through 47 nationally representative demographic and health surveys. Annals of the New York Academy of Sciences 2019, 1450, 249–267. [Google Scholar] [CrossRef]
- Li, H.; Xiao, J.; Liao, M.; Huang, G.; Zheng, J.; Wang, H.; Huang, Q.; Wang, A. Anemia prevalence, severity and associated factors among children aged 6-71 months in rural Hunan Province, China: a community-based cross-sectional study. BMC Public Health 2020, 20, 989. [Google Scholar] [CrossRef]
- Barletta, G.; Castigo, F.; Egger, E.M.; Keller, M.; Salvucci, V.; Tarp, F. The impact of COVID-19 on consumption poverty in Mozambique. Journal of International Development 2022, 34, 771–802. [Google Scholar] [CrossRef] [PubMed]
- Salvucci, V.; Tarp, F. Poverty and vulnerability in Mozambique: An analysis of dynamics and correlates in light of the Covid-19 crisis using synthetic panels. Review of Development Economics 2021, 25, 1895–1918. [Google Scholar] [CrossRef] [PubMed]
- Pierce, H.; Foster, K. Health and well-being outcomes of women and children in Sub-Saharan Africa: Examining the role of formal schooling, literacy, and health knowledge. International Journal of Educational Development 2020, 79. [Google Scholar] [CrossRef]
- Baldi, A.J.; Clucas, D.; Pasricha, S.R. Anemia and water, sanitation, and hygiene (WASH)—is there really a link? American Journal of Clinical Nutrition 2020, 112, 1145–1146. [Google Scholar] [CrossRef]
- Bountogo, M., Ouattara, M., Sié, A., Compaoré, G., Dah, C., Boudo, V., Zakane, A., Lebas, E., Brogdon, J. M., Godwin, W. W., Lin, Y., Arnold, B. F., Oldenburg, C. E.,; Étude CHAT Group. Access to Improved Sanitation and Nutritional Status among Preschool Children in Nouna District, Burkina Faso. The American Journal of Tropical Medicine and Hygiene 2021, 104, 1540–1545. [Google Scholar] [CrossRef]
- Arntson, L.; McLaughlin, K.R.; Smit, E. Factors influencing fever care-seeking for children under five years of age in The Gambia: a secondary analysis of 2019-20 DHS data. Malaria Journal 2024, 23, 124. [Google Scholar] [CrossRef]
Figure 1.
Predictive margins of child illness interacting with age.
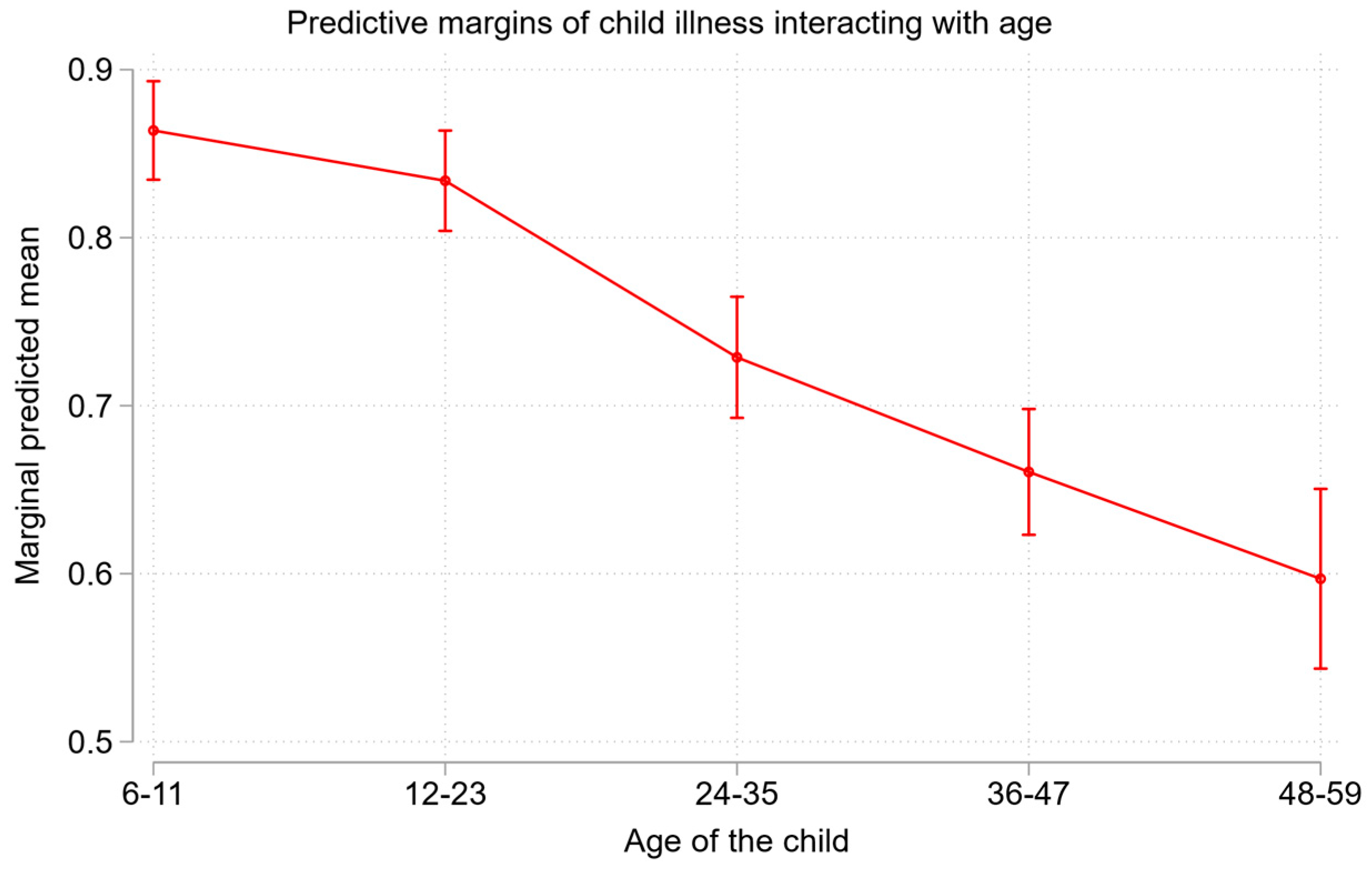
Figure 2.
Predicted probabilities of anemia by wealth index quintiles.
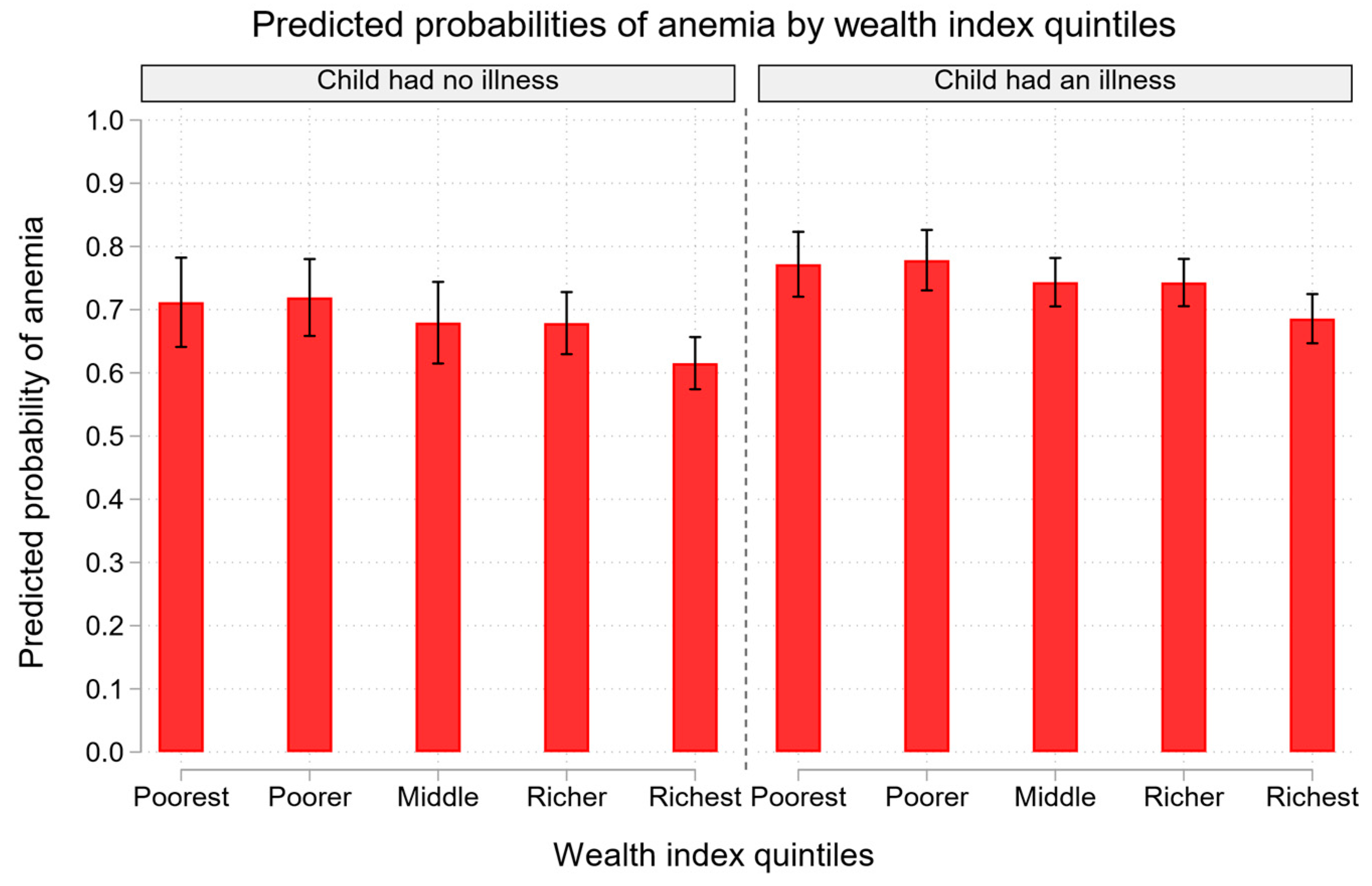

Table 1.
Random effect of anemia among children aged 6-59 months.
| Random effect | Model 1 (Empty) | Model 2 | Model 3 | Model 4 | Model 5 |
| Regional level variance (SE) | 0.20(0.08) | 0.16(0.05) | 0.20(0.08) | 0.08(0.03) | 0.09(0.03) |
| Region > Community level variance (SE) | 0.44(0.15) | 0.50(0.17) | 0.46(0.16) | 0.41(0.14) | 0.47(0.16) |
| Regional ICC(%) | 5.1 | 4.1 | 5.0 | 2.1 | 2.4 |
| Community | Region ICC(%) | 16.4 | 16.7 | 16.6 | 12.9 | 14.7 |
| Model fit statistics | |||||
| Log likelihood | -4,675 | -4,436 | -4,659 | -4,591 | -4,402 |
| AIC | 9,355 | 8,891 | 9,332 | 9,203 | 8,824 |
| Notes: | SE: standard error. ICC: intra-cluster correlation coefficient. AIC: Akaike Information Criterion | ||||
Table 2.
Association between anemia and the selected variables.
| Variable | Model 1 (Empty) |
Model 2 aOR[95%CI] |
Model 3 aOR[95%CI] |
Model 4 aOR[95%CI] |
Model 5 aOR[95%CI] |
| Age of the woman | 0.99[0.98,1.01] | 0.99[0.98,1.01] | |||
| Education level | |||||
| No education† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Primary | 0.96[0.82,1.12] | 1.03[0.87,1.21] | |||
| Secondary/Higher | 0.64[0.50,0.82]** | 0.83[0.58,1.18] | |||
| At least 4 ANC visits | |||||
| less than 4 visits† | 1.00[1.00,1.00] | ||||
| 4+ visits | 0.97[0.78,1.22] | 0.99[0.79,1.26] | |||
| Child´s age (in months) | |||||
| 6-11† | 1.00[1.00,1.00] | 1.00 | |||
| 12-23 | 0.75[0.59,0.96]* | 0.77[0.62,0.97]* | |||
| 24-35 | 0.40[0.32,0.50]** | 0.38[0.29,0.50]** | |||
| 36-47 | 0.28[0.25,0.33]** | 0.27[0.22,0.32]** | |||
| 48-59 | 0.20[0.17,0.24]** | 0.19[0.16,0.24]** | |||
| Child illness | |||||
| No† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Yes | 1.41[1.14,1.73]** | 1.42[1.15,1.74]** | |||
| Children aged 6-59 months given Vit. A supplement | |||||
| No† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Yes | 0.74[0.61,0.91]** | 0.76[0.63,0.93]** | |||
| Feeding characteristics | |||||
| Group 1 (cereals, roots, and tubers) | 1.24[1.01,1.54]* | 0.78[0.58,1.04] | |||
| Group 2 (Legumes and nuts) | 1.16[1.02,1.31]* | 1.10[0.94,1.28] | |||
| Group 4 (Flesh foods (meat, fish, fowl, liver, or other organs and eggs) | 1.05[0.85,1.30] | 1.08[0.83,1.40] | |||
| Group5 (Fruits and vegetables) | 1.01[0.87,1.17] | 0.99[0.87,1.13] | |||
| Wealth index | |||||
| Poorest† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Poorer | 1.03[0.88,1.20] | 1.04[0.87,1.25] | |||
| Middle | 0.81[0.65,1.01] | 0.84[0.68,1.05] | |||
| Richer | 0.78[0.63,0.97]* | 0.84[0.68,1.04] | |||
| Richest | 0.56[0.40,0.79]** | 0.62[0.41,0.93]* | |||
| Sex of household head | |||||
| Male† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Female | 1.10[0.96,1.26] | 1.13[0.99,1.29] | |||
| Source of drinking water | |||||
| Improved† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Unimproved | 1.30[1.13,1.49]** | 1.32[1.11,1.57]** | |||
| Type of toilet facility | |||||
| Improved† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Not improved | 0.98[0.74,1.30] | 0.98[0.74,1.29] | |||
| Residence area | |||||
| Urban† | 1.00[1.00,1.00] | 1.00[1.00,1.00] | |||
| Rural | 1.10[0.93,1.31] | 1.10[0.91,1.32] | |||
| Notes: | † is a Reference category; aOR is the adjusted odds ratio; SE is the standard error; ICC is the inter-cluster correlation coefficient; AIC is the Akaike Information Criterion; 95% CI is the Confidence Interval; * p < 0.05, ** p < 0.01; the assessment was based on multivariate three-level logistic regression model. | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



