
Submitted:
25 April 2025
Posted:
28 April 2025
You are already at the latest version
Abstract
Background/Objectives: This study aimed to develop a nanocarrier (CN) formulation for the efficient administration of Nifedipine (NIF) via pediatric feeding tubes, optimizing its delivery to hospitalized children. Methods: The CN formulation was characterized re-garding particle size, drug release properties, and compared to extemporaneous NIF tab-lets (FE-NIF) in flow-rate tests through pediatric feeding tubes. Recovery efficiency was evaluated across different tube sizes and rinsing volumes. A preliminary toxicity study was conducted using a brine shrimp lethality model. Results: The CN formulation demonstrated favorable physicochemical properties, including controlled release and su-perior flow rates compared to FE-NIF in pediatric tubes. Full recovery of NIF content was achieved with the CN formulation, while FE-NIF recovery depended on tube dimensions and rinsing protocols. Conclusions: The CN formulation represents a promising alterna-tive for administering NIF to hospitalized children via pediatric feeding tubes, offering enhanced delivery efficiency over traditional formulations.
Keywords:
pediatric feeding tube
; nifedipine
; phytantriol nanocarrier
; ultrasonication
; liquid formu-lation
1. Introduction
Nifedipine (NIF) is a potent calcium channel antagonist that falls under the dihydropyridine group. It is extensively used in clinical practice to treat angina pectoris and hypertension [1]. NIF is frequently administered to hospitalized pediatric patients, but it lacks availability in liquid pharmaceutical forms due to its extremely poor water-solubility [2,3].
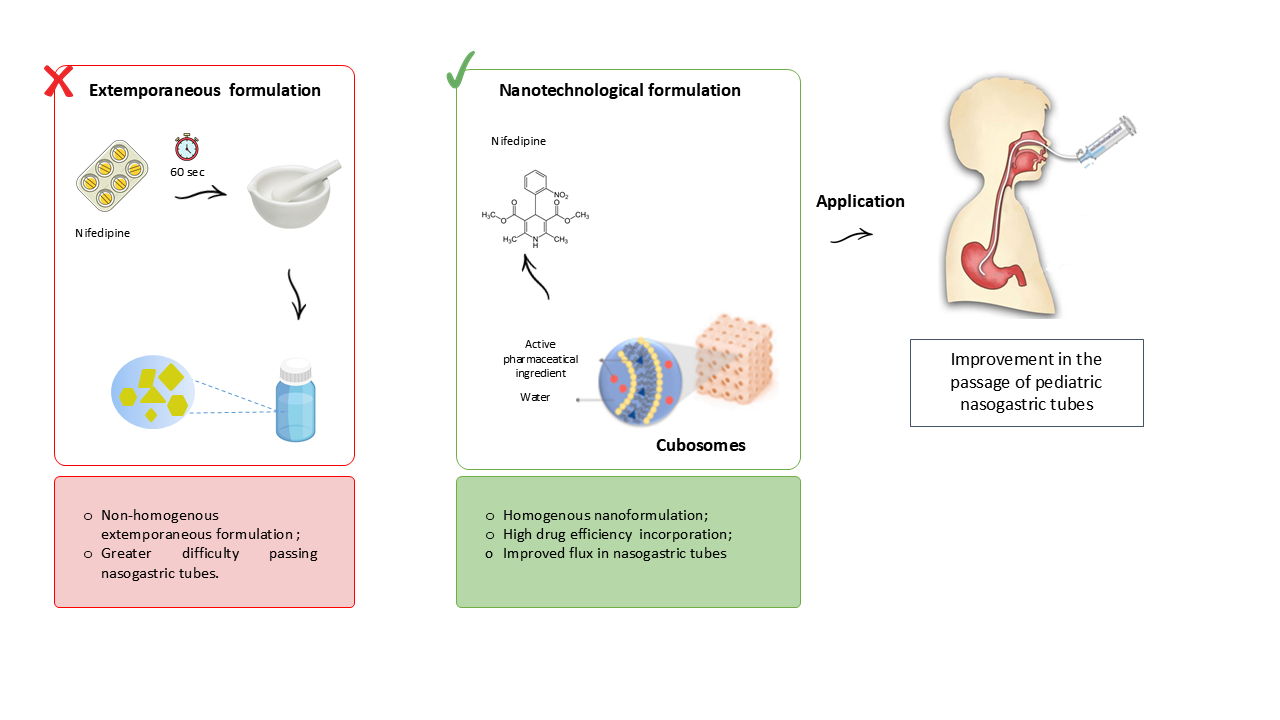
Hospitalized patients often require the use of nasogastric tubes (NGT) for the administration of nutrients and medications. However, the administration of drugs through pediatric NGT can be challenging, especially for drugs that lack liquid pharmaceutical formulations. In such cases, solid dosage forms are used and can be manipulated into suspensions by crushing tablets [4]. This tablet-crushing process can result in drug loss and the prepared suspension may not freely pass through the NGT, leading to potential tube blockage [5].
A promising alternative to develop a liquid pharmaceutical formulation of NIF and enhance the flow through the NGT is incorporating drugs into nanosystems specifically designed for oral administration. Other hydrophobic drugs, such as spironolactone, have been successfully integrated into nanosystems to create liquid formulations, showing neither blockage nor adsorption when administered through NGT [6].
Numerous studies have reported the incorporation of NIF into various types of nanosystems such as nanoemulsions [7], polymeric nanoparticles [8,9], polymeric micelles [10], and proliposomes [11,12]. All nanoparticles presented enhanced stability compared to pure NIF and promising targeted drug delivery systems, protecting the drug from the harsh acid medium in the stomach for later adsorption in the intestines.
In recent years, cubosomes have been explored as nanocarriers due to their potential as an efficient drug delivery system. Cubosomes are nanoparticles of bicontinuous cubic lyotropic liquid crystals composed of curved lipid bilayers containing two internal aqueous channels. Due to their structure, they can carry lipophilic, hydrophilic, and amphiphilic drugs [13]. Cubosomes also have a high surface area, which makes them capable of incorporating high rates of drugs [14]. Among the amphiphilic lipids used in the preparation of cubosomes, phytantriol has shown to be a promising option for oral formulations, as it is less susceptible to degradation by the gastrointestinal tract [15].
Although many authors have described the advantages of incorporating NIF into nanosystems, no literature is currently available on applying nanosystems for nifedipine administration through nasogastric tubes. Furthermore, many of the techniques from previous studies relied on organic solvents to produce their nanosystems, such as chloroform [12] and ethanol [7], raising concerns regarding the presence of toxic residues. Therefore, this study aims to develop and characterize an organic solvent-free formulation containing phytantriol-based cubosomes for the incorporation of nifedipine, to evaluate its flow properties in pediatric nasogastric tubes, and to assess its safety through preliminary toxicity tests.
2. Materials and Methods
2.1. Materials
Nifedipine was obtained by Fagron (Anápolis-GO, Brazil). The PHY (3, 7, 11, 15-tetramethyl-1, 2, 3-hexadecanetriol, 96.9%) and the P407 (PEO98-PPO67-PEO98, MW 12500 g mol-1) were purchased from Alianza (São Paulo, Brazil) and Via Farma (São Paulo, Brazil), respectively. Nifedipine tablets (10 mg) were obtained from Neo química, batch B21H2472. Pediatric nasogastric tubes (size 4, 6, and 8 FR 100 cm long; polyurethane) were purchased from Mark Med ® Santa Apolônia Hospitalar (Florianópolis, Santa Catarina, Brazil) All reagents were used without any purification process.
2.2. Preparation of NIF-Loaded Nanocarrier
The nanocarriers were prepared as described before [16] with some modifications. PHY (600 mg) and NIF (2.5 mg) were melted at 40°C to obtain the oil phase. The aqueous phase (25 ml) containing P407 (300 mg) was heated to the equivalent temperature. The solution was homogenized for 25 min using a 350 W ultrasonic processor (QR350W, Ecosonics, São Paulo, Brazil) at 99% amplitude and with a 13 mm diameter probe. Finally, the final volume was corrected to 25 mL with deionized water. The nanocarrier-drug suspension contained 0.1 mg.mL-1 of NIF and it was coded as CN. A NIF-free nanocarrier suspension was also similarly prepared, omitting the drug, and it was coded as CB.
2.3. Nanocarrier Physicochemical Characterization
2.3.1. Particle Size and Distribution
The diameter and size distribution of the particles were evaluated using the laser diffraction technique (Malvern® 2000 Mastersizer, Malvern Instruments, Malvern, United Kingdom). The sample was inserted into the distilled water container, without previous dilution, until reaching the desired obscurity. Mean particle size (Z-average) and polydispersion index (PDI) were characterized by dynamic light scattering (DLS) using a Zetamaster (ZEN 3600 Zetasizer® Nano Series, Malvern Instruments, UK) at an angle of 173° at 25ºC. The CB and CN formulations were previously diluted in water (1:100, w/w). A refractive index of 1.34 was used in both techniques.
2.3.2. Zeta Potential
The particle surface charge (ZP) was determined by electrophoretic mobility using a ZetaSizer Nano ZS (Malvern Instruments Ltd., UK). The measurements were taken after the samples were diluted in deionized water (1:100 w/w), previously filtered (0.45 µm, Miliipore). The ZP is expressed in millivolts (mV).
2.3.3. Small-Angle X-Ray Scattering Measurements
The Small-angle X-ray scattering (SAXS) measurements were performed to confirm the structure of the nanoparticles, using the Nano-inXider (XENOCS) at CNANO-UFRGS, which operates with Dectris® Pilatus3 detector and CuKα X-ray source (λ = 0.154 nm), being calibrated with silver behenate standard. The CB and CN formulations were placed into thin-walled Boron-Rich capillary tubes with 2.0mm O.D (Charles Supper®, Natick, MA, US). Consecutive 1 min measurements were obtained over 3 h for each sample in the medium resolution mode, at room temperature. The 1D curves were obtained from the 2D SAXS images using Origin® 2019.
2.3.4. NIF Content
The NIF content in the nanocarrier suspension was quantified by high-performance liquid chromatography with UV detection (HPLC-UV; Perkin). The detection wavelength was 236 nm, the Chromatographic column was a C18 (Phenosphere®, 150 mm x 4.6 mm x 5 μm), the mobile phase consisted of methanol: water (70:30, w/w) pH 5 (phosphoric acid), the column temperature was 40°C, the flow rate was 1.0 mL.min-1, and the injection volume was 20 μL. The method was validated for specificity, linearity, precision, and accuracy.
2.3.5. Drug Incorporation Efficiency
The NIF incorporation efficiency was evaluated by the ultrafiltration-centrifugation method. An aliquot of 400 µL of each formulation was added into filter devices (Microcon 10,000 Da, Millipore, USA) and centrifuged at 6,000 RPM for 30 min. The drug content in the ultrafiltrate was directly analyzed, without prior dilution. The drug incorporation efficiency (IE) was expressed as a percentage and it was calculated as described in Eq. (1):
where CT is the total drug content and CI is the drug content in the ultrafiltrate.
2.3.6. Determination of pH and Density
The pH value was determined by measuring the suspension using a calibrated pH meter (Model DM-22, Digimed, Brazil), using the potentiometric method at room temperature. Density was determined using a glass pycnometer
2.4. In Vitro Release Profile in Simulated Gastric Fluid
The in vitro release was performed using an adapted dialysis method (25 mm, MWCO 12 kDa, Sigma–Aldrich, USA). Initially, a dialysis bag containing 2 mL of formulation was immersed into glass flasks containing simulated gastric fluid (40 mL; pH 1.2), maintained at 37 ± 0.5 °C under magnetic stirring. After 60 min, the dialysis bag was immediately placed into another glass flask with a simulated intestinal fluid pH 6.8 (potassium monobasic phosphate mixture and 0.2 M sodium hydroxide; 40 mL) maintained at 37 ± 0.5 °C. At predetermined time intervals, aliquots (1 mL) of release medium were removed, filtered on a 0.45 μm membrane, and analyzed by HPLC-UV method. The removed aliquot volume was replaced by the same volume of fresh-release medium. For the NIF, the diffusion was tested following the same procedure performed for the CN. The concentration of NIF was quantified by HPLC-UV, as previously described in section 2.4. Three replicates of each experiment were carried out and the cumulative percentage of drug release was calculated.
2.5. Preliminary Toxicity Assay
Brine Shrimp Lethality Assay
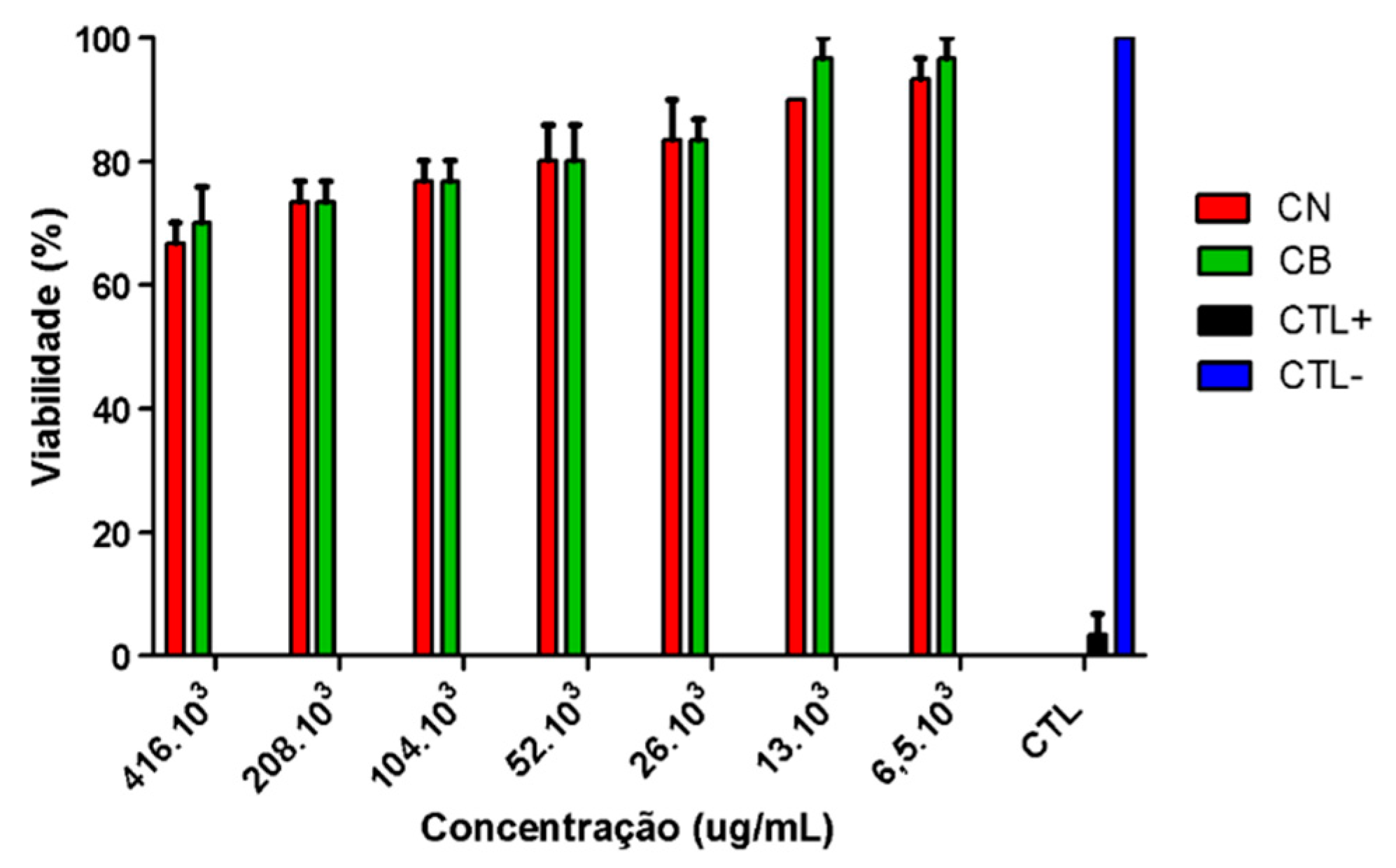
Toxicity was determined using the brine shrimp (Artemia salina) lethality bioassay with CB and CN samples [17]. Initially, Artemia salina cysts were placed in a vial containing artificial seawater (NaCl 77.23%, MgSO4 9.62%, CaCl2 3.32%, KCl 2.11%, and NaHCO3 0.59%) with a salinity of 38 g/L. After an incubation period of 24 hours, the nauplii were separated from the cysts and used for the lethality test [18]. The concentrations for testing the CB and CN samples (w/v) were adjusted based on the concentrations of phytantriol and poloxamer 407 used for the formulation preparation. The following concentrations of the samples were obtained after dilution in artificial seawater: 416. 103, 208. 103, 104. 103, 52. 103, 26. 103, 13. 103, 6.5. 103 µg mL−1. Ten nauplii were added to each test tube and incubated, with the CB tubes exposed to continuous light and the CN tubes protected to prevent degradation of the active ingredient. After 24 hours, the surviving nauplii were counted using a magnifying glass and recorded. Positive control (CTL+) (potassium dichromate) and negative control (CTL-) (artificial seawater) treatments were also performed in parallel to compare the toxicity. The toxicity of the formulations was assessed based on the toxicity scales of McLaughlin and Rogers [19]. According to the scale, concentration lethal (CL)50 values of 1000 µg/mL are considered non-toxic; values between 500 and 1000 µg/mL are considered low toxicity; values between 100 to 500 µg/mL are considered moderate toxicity, and finally, very toxic when the CL50 was below 100 µg/mL.
2.6. Preparation of Extemporaneous Nifedipine Suspensions
Extemporaneous nifedipine suspensions (FE-NIF) were prepared to simulate the procedure commonly performed in hospitals with the solid form NIF [4]. The suspension was prepared by crushing 10 mg nifedipine tablets in a mortar and pestle for 60 seconds. The theoretical concentration of nifedipine for the suspension was 0.1 mg/mL, the same observed for the concentration of nifedipine in the cubosome suspension.
2.7. Evaluation of the Passage of Formulations Through Pediatric Enteral Nutrition Tubes
To simulate the administration of the formulations (CN and FE-NIF) through pediatric enteral nutritional tubes, previous reported methodologies were adapted [5,20].
Various 100 cm long pediatric enteral feeding tubes (calibers 4, 6, and 8 FR) were tested. The tubes were positioned at a 45o angle and kept stationary during administration [21]. All tubes were washed with 20 mL of water before the formulations were administered.
The syringes containing the formulations were attached to the ends of the tubes, and the administration was performed slowly to prevent any loss of content during the process. For each formulation (CN and FE-NIF), the experiment was conducted in batch triplicate and the samples were collected in a beaker placed at the end of the tube. The syringe containing FE-NIF was constantly stirred by small rotations during the administration to avoid accumulation of granules on the inner walls of the syringe barrel.
Due to the limited gastric capacity in infants and newborns [22], the administration volumes for the CN and FE-NIF formulations were defined as 20 mL for the 6 and 8 FR caliber. For the 4 FR probes, the volume was 5 mL, since probes of this caliber are intended for newborns.
Between samples, the 6 and 8 FR caliber tubes were rinsed with 2, 5, or 10 mL of purified water to remove the residue that occasionally adhered to their walls and to determine the best rinse volume after drug administration. As for the 4 FR caliber probe, 1 and 2 mL were used in the rinsing step, considering its smaller administration volume.
After passing through the probes, the suspensions (CN and FE-NIF) and the rinsing water were collected and analyzed in UV-vis. In short, 800 uL of the suspensions and the rinsing water were diluted in methanol to obtain a theoretical concentration of 8 ug/mL and subsequently analyzed in UV-vis to quantify the content. The amount of NIF that successfully reached the end of the tube (the amount that would be ingested by the patient) was calculated for all formulations and the rinsing water.
The administration time for all formulations was registered and expressed in mL.seconds-1.
2.8. Statistical Analysis
One-way analysis of variance (ANOVA) followed by Tukey's test was used to compare experimental data with a significance level of 0.05 using GraphPad Prism version 5.0.
3. Results
3.1. Physical-Chemical Characterization
The cubosomes formulation was prepared and characterized (Table 1) using the top-down technique with ultrasound equipment. The nanocarrier exhibited a particle size of 152 ± 5.5 nm (measured by laser diffraction) and 159 ± 2.8 nm (measured by dynamic light scattering). The sample showed a homogenous pattern with a Span value of 1.22 ± 0.02 and PDI of 0.099 ± 0.001. The zeta potential of -18.9 ± 0.78 mV indicated colloidal stability primarily due to steric effects [23]. The negative charge was attributed to the ionization of the carboxylic acid group in phytantriol [24].
The CN sample exhibited a content of 99 ± 0.69% and a high incorporation efficiency (EI) of 94.73 ± 4.9 %. The pH of the CN sample was close to neutral (6.64 ± 0.12), and its density was similar to water (1.050 ± 0.0014 g/mL). The average values of particle size, PDI, zeta potential, pH, and density for the CN sample were almost identical to those of the CB sample (Table 1). These data demonstrate that the incorporation of drug molecules into the nanosystem had no significant impact on the analyzed physicochemical parameters compared to the drug-free nanosystem (CB).
The SAXS measurements are shown in Figure 1. The diffraction patterns for both CB and CN showed at least four Braggs peaks with relative positions at spacing ratios of √2 : √3 : √4 : √6.
3.2. In Vitro Release
NIF release in both the free drug dispersion and the CN formulation varied over time and was influenced by the simulated fluid medium (Figure 2). In the simulated gastric medium (pH 1.2), the dispersion of free NIF released 60.53 ± 2.58% in 60 minutes, while the CN formulation promoted a delay in the release of NIF, releasing 24.05 ± 1.1% in 60 min. These results demonstrate that the CN formulation showed the ability to trap NIF in the system at simulated gastric pH.
The nanocarrier exhibited a lower release rate of nifedipine compared to free nifedipine in simulated intestinal fluid, indicating a controlled release effect (24.05 ± 1.1% and 60.53 ± 2.5% respectively). After 6 hours, the formulation with free NIF released 100% of the drug, while the CN formulation released 61.23 ± 3.05%. The complete release of NIF from the nanocarriers was observed only after 72 hours.
3.3. Passage of Formulations Through Pediatric Enteral Nutrition Tubes
The flow rate of the formulations through the tubes varied depending on the formulation type and tube caliber. No obstructions were observed during the study; however, greater resistance was observed in the passage of the extemporaneous formulation (FE-NIF) for the 4 FR caliber probes. The improved flow rate of the CN sample compared to the FE-NIF formulation can be infuenced by the lower viscosity of colloidal systems compared to extemporaneous formulation. Therefore, it can be assumed that less force is required for the administration of nanoparticle suspensions through the probe, which facilitates continuous flow [29].
The recovery percentages of NIF for CN and FE-NIF after rinsing with different volumes for the 4, 6, and 8 FR caliber tubes are presented in Table 2. The rinsing water volumes used for 4 FR caliber probes did not have a statistically significant effect on the total recovery of NIF for the extemporaneous formulations (FE-NIF). The drug recovery values were significantly lower, almost 30% less than the content of the administered sample, indicating the poor reliability of the tablet-crushing method to administer the desired dosage to the patient. Although the rinsing volume increased the FE-NIF drug recovery for the 6 and 8 FR caliber probes, they were still not equivalent to the original dosage of the NIF tablets. The CN formulation, however, presented a complete drug recovery independently from the rinsing volumes used, indicating its delivery efficiency for all probe calibers.
3.4. Brine Shrimp Lethality Assay
The results of Artemia salina lethality for the CB and CN formulations indicated that lethality was influenced by the concentration of the tested formulations, with higher concentrations resulting in increased lethality. The positive control using potassium dichromate showed lethality close to 100% after 24 hours, while the negative control using saline seawater had no lethal effect. The LC50 (lethal concentration for 50% of the samples) was determined for the CB and CN formulations, demonstrating low toxicity for both formulations. Previous studies with different types of nanoparticles have also shown toxic effects at different stages of Artemia salina development, depending on the type of nanoparticle used.
Figure 3.
Artemia salina lethality for CN and CB formulations, positive control group (potassium dichromate), and negative control group (saline seawater).
Figure 3.
Artemia salina lethality for CN and CB formulations, positive control group (potassium dichromate), and negative control group (saline seawater).
4. Discussion
The results of the physicochemical characterization demonstrate that the nifedipine-containing cubosomes formulation (CN) exhibited appropriate physicochemical properties, with nanometric particle size, low polydispersity, and negative zeta potential, suggesting good colloidal stability. Furthermore, it showed high drug incorporation efficiency without significant changes in the physical parameters compared to the control formulation (CB), implying that the presence of nifedipine did not compromise the system structure.
Similar high IE values (93%) were reported with the incorporation of NIF into monoolein cubosomes [12]. In contrast, lower incorporation efficiencies were observed for NIF in polymeric micelles (34.1 ± 1.1%) [10] and poly(D,L-lactide-co-glycolide) (61.81 ± 3.41%) [25]. The high NIF incorporation efficiency into the cubosomes could be explained by the high lipophilicity of the drug, promoting the complete NIF solubilization by the oil phase.
The incorporation of the drug NIF into monolein-based cubosomes was investigated previously, aiming to improve its oral bioavailability [12]. The particle size obtained was 91.3 nm, the PDI was 0.168, and the ZP was −12.8 mV. However, this cubosomes production process involved the use of organic solvent chloroform, raising concerns regarding the presence of toxic residues. Additionally, the processing time required for sample production was long, exceeding 24 hours.
In contrast, in the present study, the cubosomes were developed using a solvent-free production approach, with a significantly reduced processing time of only 25 minutes. This approach mitigates the risks associated with organic solvent residues presence in the samples and enhances the safety of the final product.
The three possible structures of the cubic phase are Pn3m, Im3m, Ia3d [15]. The peaks in the SAXS pattern for CB and CN can be respectively indexed according to the Miller indices hkl= 110, 111, 200, 211, which is an indicative of the cubic phase Pn3m [26,27].
In previous studies, the release profile of NIF when incorporated into proliposomes exhibited a lower release rate compared to free NIF, similar to cubosomes. However, the cumulative release of NIF from proliposomes reached 88.7% in artificial intestinal fluid [11], whereas in the present study, after 10 hours, the cumulative release of NIF from cubosomes was 73.47 ± 2.17%, indicating that incorporating NIF into cubosomes resulted in a slower release rate compared to its incorporation into proliposomes. When incorporated into monoolein cubosomes, the release rate of NIF was approximately 5% for both simulated gastric fluid and simulated intestinal fluid over a period of 24 hours [12].
Another advantage of the present system is the use of phytantriol as the structural component of the cubosomes, instead of monoolein. While monoolein exhibits gastric instability, phytantriol has demonstrated resistance to the gastric environment, making it more suitable for oral administration of the drug. This characteristic is of great importance in ensuring the efficacy of NIF when it is orally administered [15,28].
In summary, the present study overcomes previous limitations by offering a more efficient and safe approach to cubosomes production, free from organic solvents, and using phytantriol as a gastric-resistant structural component. These improvements contribute to the potential clinical application of these nanosystems as promising vehicles for oral drug delivery.
The impact of rinse volume on the total recovery of proton pump inhibitors in pediatric tubes was studied before [5]. Similarly to the presented results, the authors found that higher rinse volumes led to greater recovery percentages. In the present study, the CN sample showed a 100% recovery rate on all probes, with no losses during administration. This can be attributed to the high incorporation efficiency of nifedipine into the cubosomes. Administering medications through feeding tubes poses challenges in the hospital setting, emphasizing the importance of considering formulation characteristics. Significant losses were observed during the administration of extemporaneous formulations, and tube rinsing protocols are commonly used to minimize losses. Grinding methods, such as mortar and pestle, have shown losses during the crushing process of paracetamol.
Other report in the literature showed thar the process of crushing a sotalol tablet in a mortar and transferring it to another container was found to result in a loss of 5.5 - 13% of the tablet weight [30]. This finding, along with our results, suggests that the losses during the preparation process of the extemporaneous formulation can vary and have a significant impact on the total percentage of NIF recovered at the end of the administration through the FE-NIF formulation.
One consequence of losses in the total percentage of FE-NIF is the administration of inconsistent doses. Additionally, drug residues in nasogastric tubes can interact with food, leading to the formation of bezoars that can cause tube blockage [31]. To date, there have been no studies reporting the oral bioavailability of crushed NIF tablets administered via nasogastric tubes. The lack of information combined with the high percentage of NIF lost during the administration process further increases the uncertainty surrounding this practice.
In contrast, the CN nanotechnology formulation shows promise in overcoming these limitations. The total recovery rate for the CN sample was 100%, regardless of the probe size and rinse volume. The total percentage of NIF recovery for the FE-NIF formulation was influenced by the probe caliber and rinse volume.
Different from what was observed for other nanoparticles, the CN sample showed a safe profile in the Artemia salina assay. Studies using gold nanoparticles (AuNPs), silver nanoparticles (AgNPs) and titanium dioxide nanoparticles (TiO₂NPs) demonstrated the broad sensitivity of Artemia salina at different developmental stages, depending on the type of nanoparticle used [32]. Exposure to concentrations of 10⁻¹, 10⁻² and 10⁻³ μg/mL of the different nanoparticles revealed that TiO₂NPs were non-toxic, AuNPs exerted toxic effects on cyst hatching but not on nauplii development, and AgNPs were toxic to both hatching nauplii and adults.
5. Conclusions
A new phytantriol-based cubosomes formulation containing nifedipine has been developed without the use of organic solvents, making it suitable for pediatric use. The formulation exhibited physicochemical parameters compatible with cubossomes.
The CN formulation proved to be highly applicable for use in enteral nutrition, with a total recovery rate of 100% for all tested probe sizes (4, 6, and 8 FR). Furthermore, it was observed that the rinsing volume did not affect the recovery rate of NIF for the CN sample, indicating that a minimal rinsing volume could be used during probe flushing.
These results indicate that the CN formulation has the potential to overcome common issues encountered in hospitals during the administration of crushed nifedipine tablets via enteral feeding tubes, such as tube blockage. The implementation of the CN formulation could lead to significant benefits, including increased safety in dose administration and prevention of active ingredient losses during the preparation and administration of extemporaneous formulations, particularly in pediatric cases.
Acknowledgments
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior–Brazil (CAPES) Finance Code 001. This research was also funded by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (grant number 88887.614058/2021-00 for L.A.L. and 314680/2021-7 for I.C.K.G.) and Fundação de Amparo à Pesquisa do Rio Grande do Sul (FAPERGS).
Abbreviations
The following abbreviations are used in this manuscript:
| CN | Cubosomes with Nifedipine |
| CB | Control Blank |
| NIF | Nifedipine |
| FE-NIF | Extemporaneous Formulation of Nifedipine |
| PHY | Phytantriol (3,7,11,15-tetrametil-1,2,3-hexadecanotriol) |
| P407 | Poloxamer 407 (PEO98-PPO67-PEO98) |
| NGT | Nasogastric Tube |
| IE (%) | Incorporation Efficiency |
| DLS | Dynamic Light Scattering |
| PDI | Polydispersity Index |
| ZP | Zeta Potential |
| SAXS | Small-Angle X-ray Scattering |
| HPLC-UV | High-Performance Liquid Chromatography with UV Detection |
| MWCO | Molecular Weight Cut-Off |
| mL.min⁻¹ | Milliliters per minute |
| µg.mL⁻¹ | Micrograms per milliliter |
| CL50 / LC50 | Lethal Concentration for 50% |
| CTL+ | Positive Control |
| CTL− | Negative Control |
| FR | French |
| ANOVA | Analysis of Variance |
| UV-vis | Ultraviolet-visible spectroscopy |
References
- M. Sakurai, I. Naruto, and K. Matsuyama, “Evaluation for zero-order controlled release preparations of nifedipine tablet on dissolution test, together with cost benefit point of views,” Yakugaku Zasshi-J. Pharm. Soc. Jpn., vol. 128, no. 5, pp. 819–826, May 2008.
- K. A. Mfoafo, M. Omidian, C. D. Bertol, Y. Omidi, and H. Omidian, “Neonatal and pediatric oral drug delivery: Hopes and hurdles,” Int. J. Pharm., vol. 597, p. 120296, Mar. 2021. [CrossRef]
- WHO, “Nifedipine (Nifedipinum),” The International Pharmacopoeia. 2022. [Online]. Available: https://digicollections.net/phint/2022/index.html#d/b.6.1.252.
- D. Salmon et al., “Pharmaceutical and safety considerations of tablet crushing in patients undergoing enteral intubation,” Int. J. Pharm., vol. 443, no. 1–2, pp. 146–153, Feb. 2013. [CrossRef]
- M. Ponrouch, V. Sautou-Miranda, A. Boyer, D. Bourdeaux, A. Montagner, and J. Chopineau, “Proton pump inhibitor administration via nasogastric tube in pediatric practice: Comparative analysis with protocol optimization,” Int. J. Pharm., vol. 390, no. 2, pp. 160–164, May 2010. [CrossRef]
- F. Hallouard, G. Dollo, N. Brandhonneur, F. Grasset, and P. Le Corre, “Preparation and characterization of spironolactone-loaded nano-emulsions for extemporaneous applications,” Int. J. Pharm., vol. 478, no. 1, pp. 193–201, Jan. 2015. [CrossRef]
- R. Jog, K. Unachukwu, and D. Burgess, “Formulation design space for stable, pH sensitive crystalline nifedipine nanoparticles,” Int. J. Pharm., vol. 514, no. 1, pp. 81–92, Nov. 2016. [CrossRef]
- I. Javed, N. Ranjha, K. Mahmood, S. Kashif, M. Rehman, and F. Usman, “Drug release optimization from microparticles of poly(ε-caprolactone) and hydroxypropyl methylcellulose polymeric blends: formulation and characterization,” J. Drug Deliv. Sci. Technol., vol. 24, no. 6, pp. 607–612, Jan. 2014.
- M. Tagliari et al., “Development of oral nifedipine-loaded polymeric nanocapsules: physicochemical characterisation, photostability studies, in vitro and in vivo evaluation,” Quimica Nova, vol. 38, no. 6, pp. 781–786, Jul. 2015. [CrossRef]
- E. Bordallo, M. Torneiro, and M. Lazzari, “Dissolution of amorphous nifedipine from micelle-forming carboxymethylcellulose derivatives,” Carbohydr. Polym., vol. 247, Nov. 2020. [CrossRef]
- Y. Bi et al., “A Liposomal Formulation for Improving Solubility and Oral Bioavailability of Nifedipine,” Molecules, vol. 25, no. 2, Jan. 2020. [CrossRef]
- M. Ali et al., “Enhancing the Solubility and Oral Bioavailability of Poorly Water-Soluble Drugs Using Monoolein Cubosomes,” Chem. Pharm. Bull. (Tokyo), vol. 65, no. 1, pp. 42–48, Jan. 2017.
- H. Barriga, M. Holme, and M. Stevens, “Cubosomes: The Next Generation of Smart Lipid Nanoparticles?,” Angew. Chem.-Int. Ed., vol. 58, no. 10, pp. 2958–2978, Mar. 2019. [CrossRef]
- I. D. M. Azmi, S. M. Moghimi, and A. Yaghmur, “Cubosomes and Hexosomes As Versatile Platforms for Drug Delivery,” Ther. Deliv., vol. 6, no. 12, pp. 1347–1364, Dec. 2015. [CrossRef]
- Z. Karami and M. Hamidi, “Cubosomes: remarkable drug delivery potential,” Drug Discov. Today, vol. 21, no. 5, pp. 789–801, May 2016. [CrossRef]
- S. Akhlaghi, I. Ribeiro, B. Boyd, and W. Loh, “Impact of preparation method and variables on the internal structure, morphology, and presence of liposomes in phytantriol-Pluronic® F127 cubosomes,” Colloids Surf. B-Biointerfaces, vol. 145, pp. 845–853, Sep. 2016. [CrossRef]
- B. Meyer, N. Ferrigni, J. Putnam, L. Jacobsen, D. Nichols, and J. Mclaughlin, “Brine shrimp - a convenient general bioassay for active-plant constituents,” Planta Med., vol. 45, no. 1, pp. 31–34, Jan. 1982.
- K. Leng, S. Vijayarathna, S. Jothy, S. Sasidharan, and J. Kanwar, “In vitro and in vivo toxicity assessment of alginate/eudragit S 100-enclosed chitosan-calcium phosphate-loaded iron saturated bovine lactoferrin nanocapsules (Fe-bLf NCs),” Biomed. Pharmacother., vol. 97, pp. 26–37, Jan. 2018. [CrossRef]
- J. McLaughlin and L. Rogers, “The use of biological assays to evaluate botanicals,” Drug Inf. J., vol. 32, no. 2, pp. 513–524, Apr. 1998.
- D. Messaouik, V. Sautou-Miranda, S. Bagel-Boithias, and J. Chopineau, “Comparative study and optimisation of the administration mode of three proton pump inhibitors by nasogastric tube,” Int. J. Pharm., vol. 299, no. 1–2, pp. 65–72, Aug. 2005. [CrossRef]
- M. do R. D. L. de Unamuno and J. S. Marchini, “Sonda nasogástrica/nasoentérica: cuidados na instalação, na administração da dieta e prevenção de complicações,” Med. Ribeirão Preto, vol. 35, no. 1, pp. 95–101, 3AD. [CrossRef]
- J. N. van den Anker, M. Schwab, and G. L. Kearns, “Developmental Pharmacokinetics,” in Pediatric Clinical Pharmacology, H. W. Seyberth, A. Rane, and M. Schwab, Eds., Berlin, Heidelberg: Springer Berlin Heidelberg, 2011, pp. 51–75. [CrossRef]
- T. Barradas et al., “Development and characterization of promising o/w nanoemulsions containing sweet fennel essential oil and non-ionic sufactants,” Colloids Surf. -Physicochem. Eng. Asp., vol. 480, pp. 214–221, Sep. 2015. [CrossRef]
- A. Avachat and S. Parpani, “Formulation and development of bicontinuous nanostructured liquid crystalline particles of efavirenz,” Colloids Surf. B-Biointerfaces, vol. 126, pp. 87–97, Feb. 2015. [CrossRef]
- M. Elkomy et al., “Intratracheally Inhalable Nifedipine-Loaded Chitosan-PLGA Nanocomposites as a Promising Nanoplatform for Lung Targeting: Snowballed Protection via Regulation of TGF-β/β-Catenin Pathway in Bleomycin-Induced Pulmonary Fibrosis,” Pharmaceuticals, vol. 14, no. 12, Dec. 2021. [CrossRef]
- S. T. Hyde, “Identification of Lyotropic Liquid Crystalline Mesophases,” Chap. 16 of Handbook of Applied Surface and Colloid Chemistry. John Willey & Sons, New York. 2001:299.
- M. Ali, S. Noguchi, Y. Iwao, T. Oka, and S. Itai, “Preparation and Characterization of SN-38-Encapsulated Phytantriol Cubosomes Containing α-Monoglyceride Additives,” Chem. Pharm. Bull. (Tokyo), vol. 64, no. 6, pp. 577–584, Jun. 2016.
- T. Nguyen, T. Hanley, C. Porter, and B. Boyd, “Nanostructured liquid crystalline particles provide long duration sustained-release effect for a poorly water soluble drug after oral administration,” J. Controlled Release, vol. 153, no. 2, pp. 180–186, Jul. 2011. [CrossRef]
- I. Kazemi, M. Sefid, and M. Afrand, “A novel comparative experimental study on rheological behavior of mono & hybrid nanofluids concerned graphene and silica nano-powders: Characterization, stability and viscosity measurements,” Powder Technol., vol. 366, pp. 216–229, Apr. 2020. [CrossRef]
- A. Ruzsíková, L. Soucková, P. Suk, R. Opatrilová, M. Kejdusová, and V. Srámek, “Quantitative analysis of drug losses administered via nasogastric tube - In vitro study,” Int. J. Pharm., vol. 478, no. 1, pp. 368–371, Jan. 2015. [CrossRef]
- Q. A. Tawfic, P. Bhakta, R. R. Date, and P. K. Sharma, “Esophageal bezoar formation due to solidification of enteral feed administered through a malpositioned nasogastric tube: Case report and review of the literature,” Acta Anaesthesiol. Taiwan., vol. 50, no. 4, pp. 188–190, Dec. 2012. [CrossRef]
- R. Pecoraro et al., “Artemia salina: A microcrustacean to assess engineered nanoparticles toxicity,” Microsc. Res. Tech., vol. 84, no. 3, pp. 531–536, Sep. 2020. [CrossRef]
Figure 1.
Intensity vs. the Norm of the Scattering Vector Obtained by SAXS Measurements for the NIF-Loaded (CN) and Blank Cubosomes (CB). q=2 sinθ/λ, where θ is the Bragg angle and λ is the wavelength of x-ray.
Figure 1.
Intensity vs. the Norm of the Scattering Vector Obtained by SAXS Measurements for the NIF-Loaded (CN) and Blank Cubosomes (CB). q=2 sinθ/λ, where θ is the Bragg angle and λ is the wavelength of x-ray.
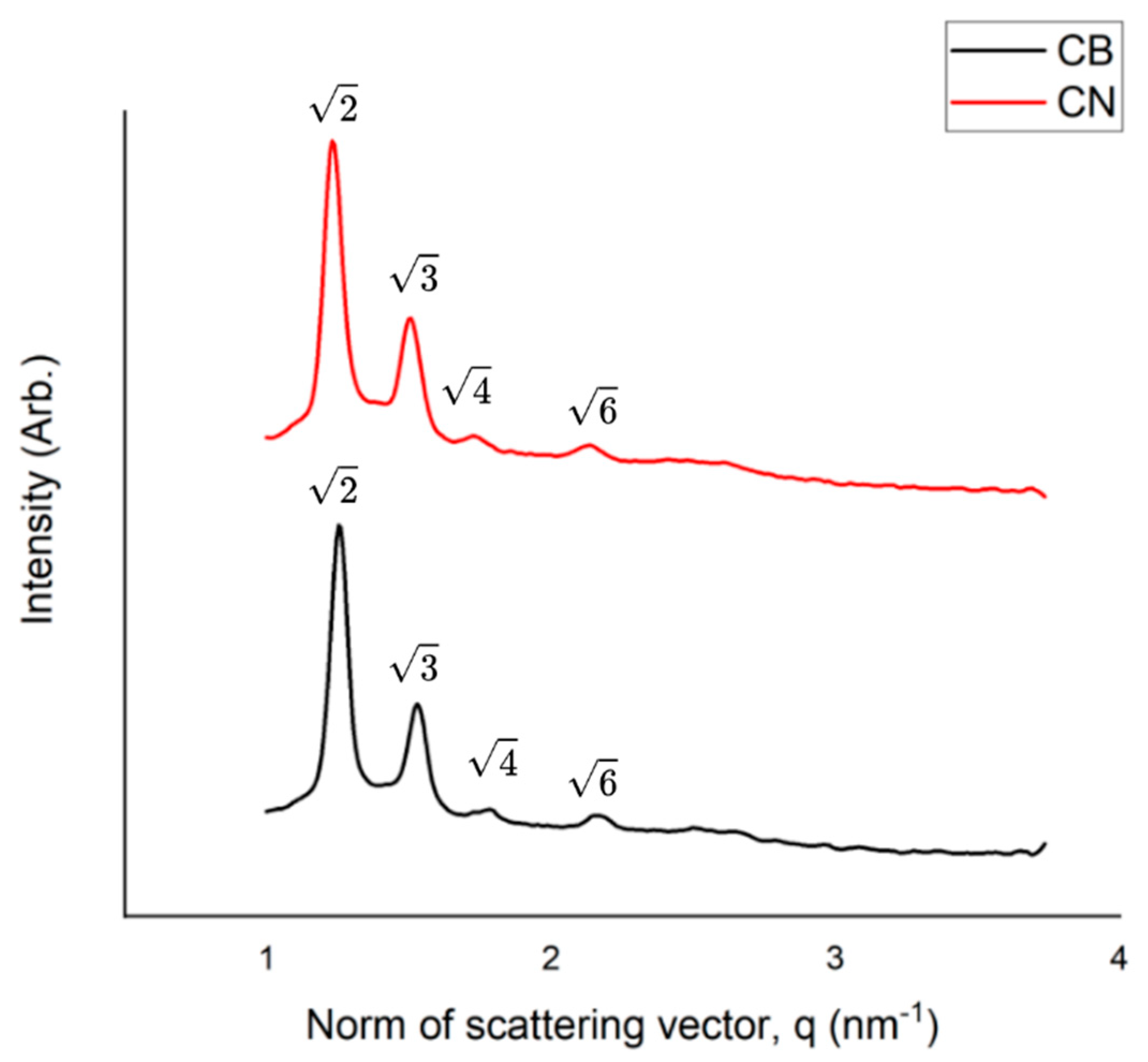
Figure 2.
NIF release profile for CN and free NIF in simulated gastric and intestinal fluid medium. Data expressed as percentage of NIF versus time (hours).
Figure 2.
NIF release profile for CN and free NIF in simulated gastric and intestinal fluid medium. Data expressed as percentage of NIF versus time (hours).
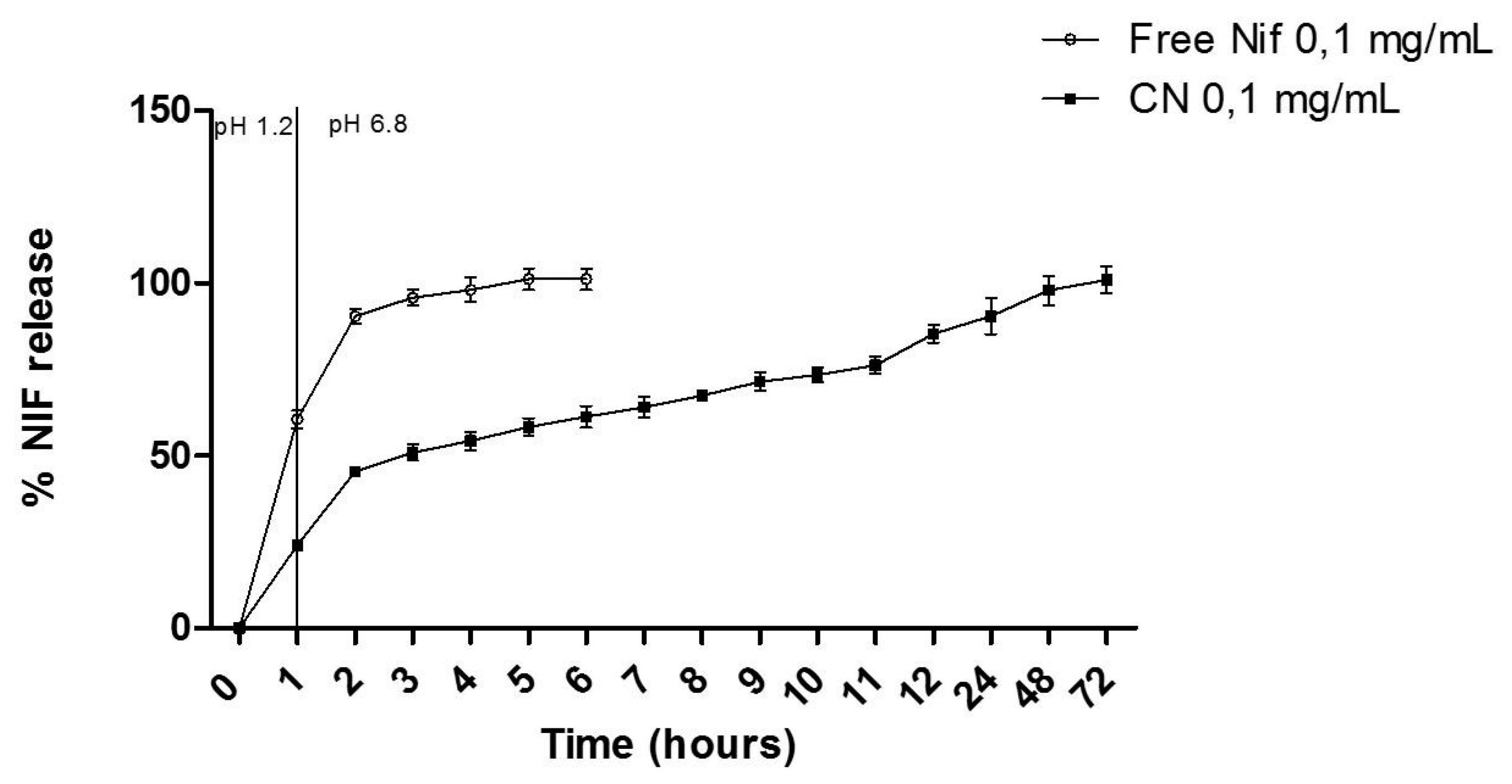

Table 1.
Physical-chemical characterization of the CB and CN (0.1 mg/mL) formulations.
| Sample | ||
|---|---|---|
| CB | CN | |
| D[4,3] (v) (nm) | 145 ± 6.1a | 152 ± 5.5 a |
| Span (v) | 1.22 ± 0.02a | 1.22 ± 0.02a |
| Size (nm) | 156 ± 0.17 a | 159 ± 2.8 a |
| PDI | 0.099 ± 0.001 a | 0.094 ± 0.018 a |
| ZP (mV) | -17.3 ± 0.55 a | -18.9 ± 0.78 a |
| pH | 6.79 ± 0.07a | 6.64 ± 0.12 a |
| Density (g/mL) | 1.050 ± 0.0014a | 1.020 ± 0.001a |
| Drug content (%) | - | 99 ± 0.69 |
| IE (%) | - | 94.73 ± 4.9 |
Results expressed by mean ± standard deviation Matching letters within the same row indicate no statistical difference (p≤0.05).;.
Table 2.
NIF recovery after passage through 4, 6 and 8 FR caliber pediatric tubes with different rinse volumes.
Table 2.
NIF recovery after passage through 4, 6 and 8 FR caliber pediatric tubes with different rinse volumes.
| Total drug recovered (%) after passing through the probe | ||||||
|---|---|---|---|---|---|---|
| Probe caliber | Sample | Original drug content (%) | Probe 1 (1 mL rinse) | Probe 2 (2 mL rinse) |
Probe 3 (5 mL rinse) |
Probe 4 (10 mL rinse) |
| 4 FR | FE-NIF | 101.1 ± 1.8a | 62.5 ± 4.2b | 67.6 ± 5.6b | — | — |
| CN | 102.5 ± 4a | 103.9 ± 4a | 100.3 ± 4a | — | — | |
| 6 FR | FE-NIF | 101.1 ± 1.8a | — | 65.0 ± 12b | 72.6 ± 6b | 82.9 ± 9b |
| CN | 102.5 ± 4a | — | 103.9 ± 4a | 100.3 ± 4a | 100.8 ± 5a | |
| 8 FR | FE-NIF | 101.1 ± 1.8a | — | 70.2 ± 9.3b | 78.1 ± 8.9b | 91.1 ± 10a, b |
| CN | 102.5 ± 4a | — | 103.9 ± 4a | 100.3 ± 4a | 100.8 ± 5a | |
Results expressed by mean ± standard deviation; Matching letters within the column indicate no statistical difference (p≤0.05)..
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



