
Submitted:
22 April 2025
Posted:
22 April 2025
You are already at the latest version
Abstract
Background/Objectives
The rising incidence of papillary thyroid carcinoma (PTC) is largely attributed to increased detection of microcarcinomas. Disease mortality, however, remains unchanged, raising concerns about overdiagnosis and overtreatment. This led to de-escalation in disease management recommendations. Our study compares disease characteristics and outcomes of incidental vs non-incidental cases over ten years.
Methods
This is a single-center retrospective comparative analysis, utilizing a prospectively collected database of patients referred for thyroid surgery.
Results
PTC accounted for 86.7% of thyroid malignancies, with papillary thyroid microcarcinoma (PTMC) comprising 36.2% (137 patients). Incidental PTMC (IPTMC) represented 109 out of 1,012 patients undergoing surgery for benign thyroid disease (10.8%). Nonincidental PTMC (NIPTMC) was found in 28 patients (20.4%( without associated thyroid pathology.
NIPTMCs were more frequently associated with high-risk features (75% vs. 10.1%, P = 0.004), including extrathyroidal extension (21.43% vs. 7.3% P 0.0015), positive central lymph nodes (21.43% vs. 2.8%, P = 0.0291), positive lateral lymph nodes (28.6% vs. 0 % P= 0.012), and lymphovascular invasion (3.6% vs. 0%).
Multifocal PTMC was seen in 37 patients (27%), 27 with bilobar disease. Multifocal tumors were significantly larger compared to unifocal tumors (P = 0.0054) and had a higher likelihood of high-risk features (48.6% vs. 14%, P = 0.007). NIPTMC was a significant predictor of multifocality (P = 0.0098).
All patients underwent surgery, with an increase in total thyroidectomies performed in the latter five years. None opted for active surveillance.
Conclusion
The findings suggest that NIPTMC often necessitates more aggressive surgery, driven by its association with high-risk features.
Keywords:
Papillary thyroid microcarcinoma
; Incidental papillary thyroid microcarcinoma
; Non-incidental papillary thyroid microcarcinoma
; Total thyroidectomy
; Thyroid lobectomy
; Active surveillance
Introduction
Papillary thyroid carcinoma (PTC) stands as the most prevalent endocrine malignancy both nationally and globally, with a rising incidence over the last decade. This increased incidence is largely attributed to the increased detection of papillary thyroid microcarcinoma (PTMC) because of the more prevalent use of head and neck imaging and ultrasound-guided fine needle aspiration cytology (US-FNAC), along with the increased awareness of such lesions [1,2,3,4]. Sosa et al. reported a 16% annual increase in US-FNAC usage in the United States, leading to a higher detection rate of PTC and a 31% rise in thyroid surgeries [5]. Nevertheless, the stable mortality rate from thyroid cancer raises concerns about overdiagnosis and overtreatment. Consequently, this has resulted in a shift to de-escalation in the management of these lesions as reflected in the American Thyroid Association (ATA) guidelines recommending lobectomy as well as active surveillance (AS) as acceptable treatment options in selected patients [6,7] and most recently in the ATA’s consensus statement regarding the clinical use of minimally invasive ablative procedures which included that thermal ablation may be used safely in PTMC with no high-risk features, emphasizing that more data is needed for larger tumors [8]. Notably, active surveillance of low-risk PTMCs has been initiated in Japan based on the high incidence of both latent thyroid carcinoma in autopsy studies, reaching up to 36%, and small PTCs detected in mass screening studies compared to the prevalence of clinical carcinomas [9,10,11].
As per previous WHO classifications, the traditional and widely accepted definition of papillary thyroid microcarcinoma is a papillary carcinoma measuring 1 cm or less, and it was reported as a distinct subtype [12]. However, due to the identification and reporting of biologically diverse types of PTMC, the most recent 2022 World Health Organization (WHO) classification no longer recognizes PTMC as a distinct subtype. Instead, it mandates the classification of these tumors based on their histomorphologic features with an emphasis on the molecular profile [13]. The concept of low-risk neoplasm along with a histologic and molecular-based grading system helps guide personalized therapeutic decisions for patients at different levels of risk [13].
Although most PTMCs exhibit an indolent behavior, a subset of these tumors presents with high-risk aggressive features that are typically identified through final histopathologic examination post-surgery. The absence of reliable clinical criteria for preoperative risk stratification can result in insufficient or delayed treatment for these cases [4,14]. Moreover, current thyroid guidelines [6,7] do not endorse FNAC in sub-centimeter nodules unless certain clinical or ultrasonic features are present. Park et al. [15] concluded that PTMC should not be underestimated as it can act as large PTC, they reported nodal metastasis in 34.9% of their patients. Yan et al. reported that while small PTMCs are diagnosed incidentally, they can lead to regional lymph node involvement which should be considered in the clinical management of these patients [16]. In addition, the frequent multifocality and bilaterality of PTMC dictate a tailored surgical approach involving patients in shared decision-making.
Clinically, PTMC can be incidental (IPTMC), referring to lesions discovered incidentally, often in thyroid resection specimens, or non-incidental or primary (NIPTMC), referring to lesions diagnosed pre-surgically as palpable nodules or in conjunction with clinically apparent lymphadenopathy or distant metastasis. NIPTMCs more often present with aggressive features and can be associated with a worse prognosis [3,17,18,19].
This study aims to present the institution’s experience with incidental and non-incidental PTMC, including a comparative analysis of incidence, updated 2022 WHO histologic classification, clinicopathological characteristics, and therapeutic approach, and assess the impact of evolving management guidelines on surgical practice alongside a review of current literature.
Materials and Methods
This study retrospectively reviews our database of patients referred for thyroid surgery at Jordan Hospital/Ibn Sina University of Medical Sciences, a tertiary care academic medical center, from January 2013 to December 2022. The study includes consecutive patients over the age of 18, excluding patients undergoing combined thyroid and parathyroid surgery, patients with familial MENII syndrome, and patients with medullary thyroid carcinoma. The procedures in the current study were followed and assessed by the institutional review committee in accordance with the Declaration of Helsinki and its later amendments. Informed consent was obtained from all patients before initiation of the study.
Initial data collection encompassed demographic information such as age, sex, and nationality. Clinical evaluations included growth rate, compression symptoms, hoarseness of voice, presence of hypo- or hyperthyroidism, history of radiation exposure, family history of thyroid disease or malignancy, and neck physical examination findings, specifically the presence of palpable thyroid nodules or lymph node enlargement.
Laboratory investigations included measurements of TSH, T3, T4, thyroglobulin, and thyroid autoantibodies. Preoperative ultrasonography was performed to characterize thyroid nodules, assess lymph node status, and US-FNAC of solitary, dominant, or any suspicious nodules and lymph nodes. FNAC results were categorized according to the Bethesda system [20,21]. Scintigraphy was conducted in selected cases with suspected thyrotoxic nodules. Informed consent and patient counseling covered treatment plans, intraoperative decisions, and patient preferences. All patients underwent surgical resection, with central neck dissection for clinically or ultrasound-positive or suspicious nodes and modified neck dissection for positive lateral nodes. None of the patients opted for AS.
Histopathological examination was performed by two board-certified pathologists experienced in thyroid pathology from Jordan Hospital (Amman, Jordan). The first author, a surgical pathologist from the University of Iowa (Iowa, USA) performed a blinded review of all filed patients’ pathology slides as an external reviewer, and classified all tumors based on the updated 2022 WHO classification of thyroid neoplasms [13]. Benign thyroid specimens were thoroughly examined for incidental microcarcinomas (≤1 cm). Pathologic examination of tumors included assessments of histologic subtype, size, site, margins, bilaterality, multifocality, presence or absence of extrathyroidal extension (ETE), and lymphovascular invasion.
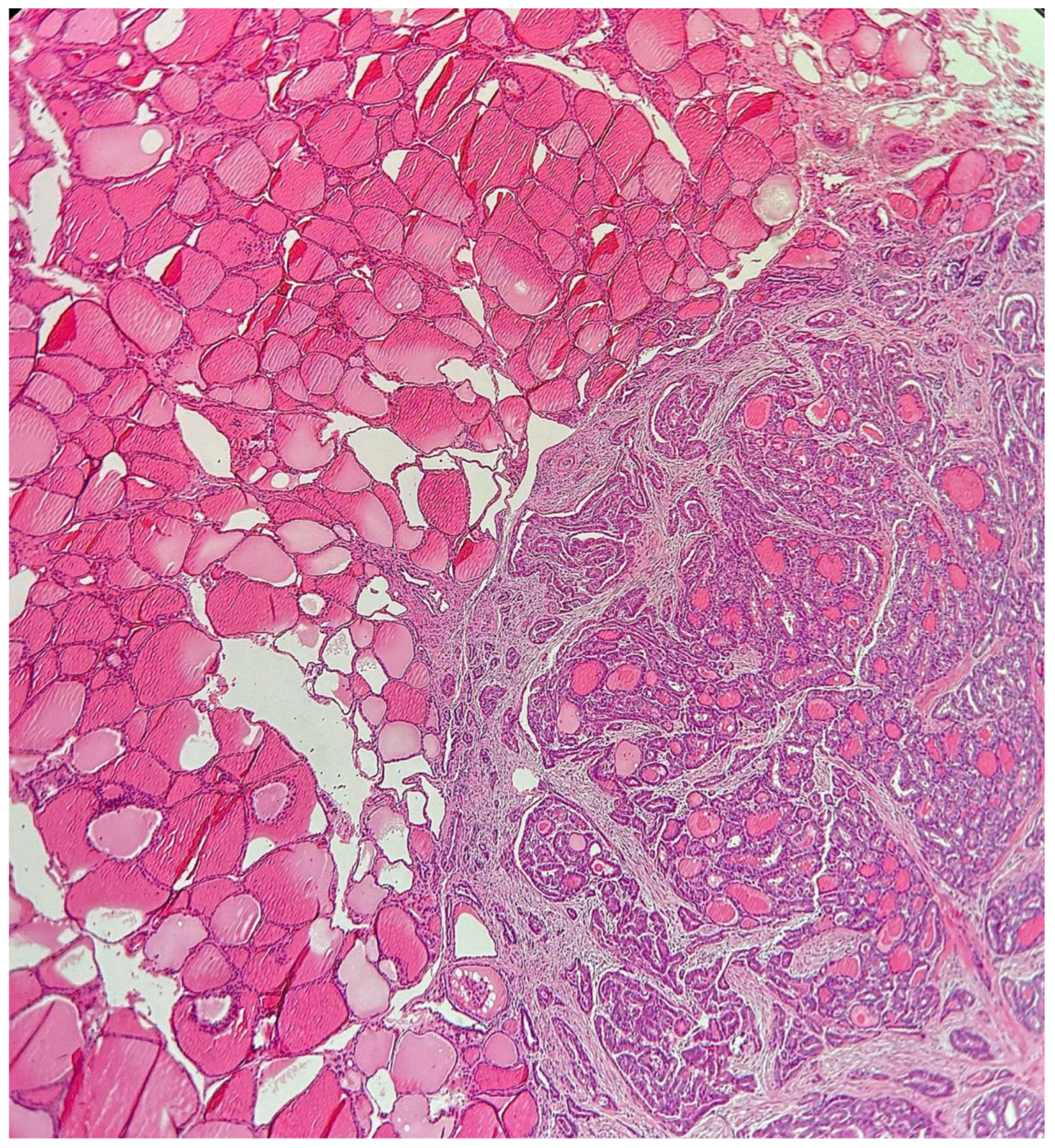
Based on our patient cohort, PTMCs were categorized into two groups: IPTMC, representing tumors identified in surgical specimens performed for benign thyroid disease, and primary or NIPTMC, representing tumors occurring in normal thyroid tissue without associated thyroid pathology (Figure 1), diagnosed preoperatively clinically or via imaging and FNAC. Comparative analysis of incidental versus NIPTMCs was performed, focusing on incidence, demographic data, FNAC results, incidence of associated benign thyroid disease, presence of high-risk aggressive features including local ETE, positive central or lateral cervical lymph nodes, lymphovascular invasion, and aggressive histologic subtypes.
Figure 1.
Non-incidental papillary thyroid microcarcinoma (NIPTMC).
Additionally, multifocality was studied, and a comparative analysis was conducted to assess unifocal versus multifocal disease. The analysis also included an assessment of predictors of multifocality and the incidence of bilaterality. The number of patients with PTMCs and the type of surgery were compared between the study’s first and second five-year periods.
Statistical analysis was conducted using IBM SPSS Statistics for Windows, version 25 (released in 2017, IBM Corp., Armonk, NY). Means were expressed with standard deviation, and a p-value of < 0.05 was considered statistically significant. Appropriate statistical tests, such as the t-test, Chi-Square test, and ANOVA, were utilized to derive p-values and analyze the data.
Results
Over the ten-year duration of the study, there were 378 cases (86.7%) of PTC out of 436 patients diagnosed with thyroid malignancy. PTMC T1a accounted for 137 cases (36.2%), while stages T1b, T2, and T3 PTC comprised 77 (20.4%), 110 (29.1%), and 54 (14.4%) cases, respectively. Within the PTMC (T1a) category, 28 cases were classified as NIPTMC and 109 cases as in IPTMC (Table 1).

Table 1.
xxx.
| (1) Begin Thyroid Disease (1012) | IPTMC ** Incidence | |
| 1. Nodular Goiter | 770 (76.1%) | 67 (8.7%) |
| 2. Hashimoto Thyroiditis (HT) | 101 (10%) | 21 (20.8%) |
| 3. Grave’s | 62 (6.1%) | 11 (17.74%) |
| 4. Adenoma | 79 (7.8%) | 10 (12.7%) |
| Total | 1012 (100%) | 109 (10.8%) *** |
| (2) Thyroid Malignancies (436) | ||
| (1) Papillary (PTC)* | Number 378 (86.7%) | |
| T1 : T1a : < 1 cm ( PTMC)** | 137 (36.2%) | |
| Incidental *** | 109 | |
| Non-Incidental *** | 28 | |
| T1b : > 1 - < 2 cm | 77 (20.4%) | |
| T 2 : > 2 cm - < 4 cm | 110 (29.1%) | |
| T 3 : > 4 cm | 54 (14.3%) | |
| Total | 378 (100%) | |
| (2) Other Malignancies | Number 58 (13.3%) | |
| Follicular Carcinoma | 23 | |
| Hurthle Cell Carcinoma | 8 | |
| Medullary Carcinoma | 12 | |
| Lymphoma | 4 | |
| Anaplastic Carcinoma | 2 | |
| Well Differentiated Tumour of | 8 | |
| Undetermined Malignant potential | ||
| Renal mets | 1 | |
| Total | 58 | |
| All Malignancies | 436 (100%) | |
* PTC : Papillary Thyroid carcinoma. ** IPTMC : Incidental Papillary Thyroid Microcarcinoma.*** included in T1a PTC.
A total of 1,012 patients underwent surgical resection for benign thyroid disease, of which 109 patients (10.8%) were found to have IPTMC. IPTMC was identified in 67 of 770 patients with multinodular goiter (MNG) (8.7%), 21 of 101 patients with Hashimoto’s thyroiditis (HT) (20.8%), 11 of 62 patients with Graves’ disease (17.74%), and 10 of 79 patients with adenomas (12.7%) (Table 1). In these patients with benign thyroid disease, surgery was performed for non-cancer reasons. In MNG, surgery was done due to compression symptoms, complications, or retrosternal extension. In Graves’ disease, it was done due to ophthalmopathy, failure or complication of medical treatment, or nodular gland. Nodular HT occurred in 9 patients (28.6%). Malignancy was diagnosed in those patients postoperatively in thyroidectomy specimens.
The histologic subtypes of PTMC cases (based on the updated 2022 WHO classification of thyroid neoplasms) are detailed in Table 2. The classic subtype was significantly the most prevalent in NIPTMC cases (89.3%). Similarly, the classic subtype was the most common in IPTMC cases (52.8%), followed by the minimally invasive circumscribed follicular variant of papillary carcinoma (35.8%), which was significantly more prevalent in IPTMC than in NIPTMC (P = 0.001). Aggressive subtypes (tall cell, columnar cell, hobnail, diffuse sclerosing, and solid) were not observed.
Table 2.
Histologic subtypes of Papillary Thyroid Microcarcinoma (PTMC).
| Clinical Presentation | Subtype of PTMC | |||||
| 1. Incidental PTMC (IPTMC) associated with | Classic subtype | Infiltrative follicular subtype | Invasive encapsulated FV PTC (all minimally invasive) | FVPTC non-encapsulated circumscribed (all minimally invasive) | Oncocytic subtype | Total Number |
| _ Multinodular Goiter | 38 (56.7%) | 0 (0%) | 5 (7.5%) | 23(34.3%) | 1(1.5%) | 67 (100%) |
| _ Hashimoto | 8 (38%) | 4 (19%) | 0 (0%) | 9 (43%) | 0 (0%) | 21 (100%) |
| _ Graves’ | 6 (54.5%) | 0 (0%) | 0 (0%) | 4 (36.4%) | 1 (9.1%) | 11 (100%) |
| _ Adenoma | 5 (50%) | 0 (0%) | 1 (10%) | 3 (30%) | 1 (10%) | 10(100%) |
| 1. Total : IPTMC | 57 (52.8%) | 4 (3.7%) | 6 (3.7%) | 39 (35.8%) | 3 (2.8%) | 109 (100%) |
| 2. Non-incidental or Primary (NIPTMC) | 25 (89.3%) | 1 (3.6%) | 0 (0%) | 2 (7.1%) | 0 (0%) | 28 (100%) |
| P Value | 0.002 | 0.4801 | 0.1515 | 0.001 | 0.3751 | 0.0001 |
| < 0.05 | > 0.05 | > 0.05 | < 0.05 | > 0.05 | < 0.5 | |
Classification based on 2022 WHO classification of Thyroid Neoplasms.
A comparative analysis of demographic and clinicopathological features of IPTMC and NIPTMC is presented in Table 3. IPTMC was significantly more prevalent (79.6%) compared to NIPTMC (20.4%) (P < 0.045). There was no significant gender difference between the two types (P = 0.324). The mean age was significantly younger in NIPTMC cases (37.14 ± 14.28 years) compared to IPTMC cases (44.15 ± 13.43 years) (P = 0.0001). Additionally, NIPTMC was significantly more common in patients younger than 55 years (P < 0.05). IPTMC was significantly more associated with MNG (P = 0.0005) and HT (P = 0.0054) than with Graves’ disease (P = 0.1171) and adenomas (P = 0.5513) (Table 3).
Table 3.
Demographic and Clinicopathological Features of Patients with Papillary Thyroid Microcarcinoma (PTMC).
Table 3.
Demographic and Clinicopathological Features of Patients with Papillary Thyroid Microcarcinoma (PTMC).
| Type | Incidental | Non- Incidental (Primary) | P value | Status p. v | ||
| Number | 109 (79.6) | 28(20.4%) | 0.045- | <0.05 | ||
| Gender | F | 85 (77.9%) | 20 (71.43%) | 0.324 | >0.05 | |
| M | 24 (22.1%) | 8 (28.57%) | ||||
| Age , Y | 1) Average Y | 44.153 + 11.28y | 37.14 + 13.43y | 0.0001 | <0.05 | |
| 2) < 45 Y | 50 (45.9%) | 20(71.43%) | 6.93- | <0.05 | ||
| > 45 Y | 59 (54.1%) | 8(28.57%) | ||||
| < 55 Y | 86 (78.9%) | 27 (96.43%) | ||||
| > 55 Y | 23 (21.1%) | 1 (3.57%) | ||||
| Associated pathology | ||||||
| Multinodular Goiter | 67 (61.5%) | * | 0.0005 | <0.05 | ||
| Hashimoto Thyroiditis | 21(19.3%) | * | 0.0054 | <0.05 | ||
| Adenoma | 10 (9.2%) | * | 0.5513 | > 0.05 | ||
| Grave’s disease | 11(10%) | * | 0.1174 | > 0.05 | ||
| Nationality | ||||||
| Local | 60 (55%) | 16 (57.1%) | 0.35 | >0.05 | ||
| International | 49 (45%) | 12 (42.9%) | ||||
| *FNAC B VI or / and B V | ||||||
| Yes | 48 (44%) | 24(85.71%) | 0.001 | <0.05 | ||
| No | 61 (56%) | 4(14.29%) | ||||
| Aggressive Features | ||||||
| Extrathyroidal Extension | Yes | 8 (7.3%) | 6(21.43%) | 0.0015 | <0.05 | |
| No | 101 (92.6%) | 22(78.57%) | ||||
| Positive Central nodes | Yes | 3 (2.8%) | 6 (21.41%) | 0.0291 | <0.05 | |
| No | 106 (97.2%) | 22 (75%) | ||||
| Positive Lateral Nodes | Yes | 0 ( 0%) | 8(28.6%) | 0.012 | <0.05 | |
| No | 109 (100%) | 20(71.4%) | ||||
| Lymphovascular invasion | Yes | 0 (0%) | 1 (3.6%) | _ | >0.05 | |
| No | 109 (100%) | 27 (96.4%) | _ | |||
| Aggressive Features : Total | Yes | 11 (10.1%) | 21 (75%) | 0.004 | <0.05 | |
| No | 98 (89.9%) | 7 (25%) | ||||
| Total Thyroidectomy | 97(88.1%) | 28(100%) | 0.0303 | <0.05 | ||
| Total Lobectomy | 12(11.9%) | 0(0%) | ||||
* FNAC B VI or/B V: Fine needle aspiration cytology Bethesda VI or/ Bethesda V.
High-risk aggressive features were observed in 32 out of 137 patients (23.36%) and were significantly more common in NIPTMC than in IPTMC (P = 0.004), including local extrathyroidal extension (ETE) (21.43% vs. 7.3%), positive central nodes (21.4% vs. 2.8%), and positive lateral cervical lymph nodes (28.6% vs. 0%). The diagnosis of malignancy was made preoperatively clinically, by FNAC, or the presence of nodal metastasis (Table 3).
Most patients (100 patients) had unifocal disease (73%); 85 (85%) were IPTMCs and 15 (15%) were NIPTMCs. Multifocal disease (MF) was present in 37 patients (27%), with 24 IPTMC cases (64.8%) and 13 NIPTMC cases (35.2%). Bilateral PTMCs occurred in 27 patients with MF-PTMCs (73%), as shown in (Table 4).
Table 4.
Papillary Thyroid Microcarcinoma (PTMC) Multifocality (MF) and Clinicopathological features.
Table 4.
Papillary Thyroid Microcarcinoma (PTMC) Multifocality (MF) and Clinicopathological features.
| Type | Unifocal | Multifocal (MF) | P - Value |
| 1) Number | 100 (73%) | 37 (27%) | < 0.002 |
| 2) Average maximal tumoral diameter | 0.442 cm | 0.78 cm | 0.0054 |
| 3) Size > 5 mm | 43 (43%) | 29 (78.4%) | < 0.0002 |
| 4) Site Unilobar Right or Left | 97 ( 97%) | Bilobar 27 (73%) | > 0.1367 |
| isthmus | 3 ( 3%) | 0% | |
| 5) Gender | |||
| F | 76 (76%) | 27 (73%) | > 0.7248 |
| M | 24 (24%) | 10 (27%) | |
| 6) Age: | |||
| F | 43.46 + 11.49 | 45.55 + 13.45 | > 0.6323 |
| M | 42.95 + 12.18 | 43.3 + 17.13 | |
| 7) FNA BVI or / BV | 42 ( 42%) | 21 (56.8%) | > 0.1294 |
| 8) Predictors of MF : | |||
| IPTMC | 85 ( 85%) | 24 ( 64.8%) | 0.0915 |
| NIPTMC* | 15 ( 15%) | 13 ( 35.2%) | < 0.0098 |
| Nodular goiter | 52 ( 52%) | 15 ( 40.5%) | > 0.2319 |
| Hashimoto | 14 ( 14%) | 7 ( 18.9%) | > 0.4642 |
| Grave’s | 10 ( 10%) | 1 ( 2.7%) | > 0.1640 |
| Adenoma | 9 ( 9%) | 1 ( 2.7%) | > 0.2048 |
| 8) Aggressive features | |||
| - ETE | ** | ||
| Yes | 8 (8%) | 6 (16.21%) | > 0.2371 |
| NO | 92 (92%) | 31 (83.79%) | |
| Positive Central Nodes | |||
| Yes | 3 (3%) | 5 (13.5%) | > 0.0768 |
| No | 97 (97%) | 32 (86.5%) | |
| Positive Lateral Nodes | |||
| Yes | 3 (3%) | 6 (16.21%) | > 0.0591 |
| No | 97 (97%) | 31 (83.79%) | |
| Lymphovascular invasion | |||
| Yes | 0 (0%) | 1 (2.7%) | > 0.5307 |
| No | 0 (0%) | 36 (97.3%) | |
| Aggressive Criteria : total | |||
| Yes | 14 (14%) | 18 (48.6%) | < 0.007 |
| No | 86 (86%) | 19 (51.4%) | |
| Total Thyroidectomy | |||
| Yes | 88 (88%) | 37 (100%) | < 0.001 |
| No | 12 (12%) | 0 (0%) | |
* Non- IPTMC: Non-Incidental Papillary thyroid microcarcinoma. ** ETE : extrathyroidal extension.
The average maximum tumor diameter was 0.442 cm in unifocal tumors and 0.78 cm in multifocal tumors (P = 0.0054). Multifocality was more common in association with tumors larger than 5 mm; larger tumors (>5 mm) were present in 43 (43%) unifocal cases and 29 (78.4%) multifocal cases (P < 0.0002). There was no significant gender or age difference between unifocal and MF-PTMCs (Table 4).
Predictors of multifocality included NIPTMC (significantly, P = 0.0098) as well as MNG and HT (non-significantly), compared to Graves’ disease and adenomas. Aggressive features were significantly more common in MF-PTMCs, with an incidence of 48.6% compared to 14% in unifocal disease (P < 0.007).
Total thyroidectomy was performed in all cases of NIPTMCs and MF-PTMCs (100%), compared to 88% in IPTMCs and unifocal PTMCs (P < 0.001) (Table 4). This included eight completion thyroidectomies requested by female patients aged 32-36 years due to concerns about malignancy risk.
During the first five years of the study (2013-2017), 67 PTMC cases (48.9%) were identified, compared to 70 cases (51.1%) in the second five years (2018-2023) (P = 0.071). Total thyroidectomy (TT) and thyroid lobectomy (TL) were performed in 57 (85.1%) and 10 (14.9%) patients, respectively, during the first period, compared to 68 (97.1%) and 2 (2.9%) patients during the second period (P = 0.0022). This suggests that the new ATA guideline recommendations for performing TL for unifocal small low-risk tumors had no impact on institutional surgical practice during the study period. Upon follow-up, all patients with PTMC were alive with no disease recurrence. Recurrence occurred in 12 patients with higher-stage PTC (T1b and above), including ten female and two male patients. One patient succumbed to dedifferentiated recurrent PTC.
Table 5 presents comparative demographics and clinicopathological features of PTMC (T1a) and T1b PTC. There were no significant differences in gender, age, multifocality, or surgical treatment. T1b PTCs were more frequently associated with high-risk aggressive features (56.65%) compared to PTMC (T1a) (23.35%), P = 0.001), indicating advancing disease.
Table 5.
Patient Cohort in the Two Five-Year Periods and Type of Surgery.
| Pathology | 2013-2017 | 2018-2023 |
| NIPTMC | 17 (60.7%) | 11 (30.3%) |
| IPTMC | 50 (45.9%) | 59 (54.6%) |
|
Multinodular Goiter TT TL |
23 7 |
36 1 |
|
Hashimoto’s TT TL |
6 2 |
12 1 |
|
Adenoma TT TL |
5 1 |
4 0 |
|
Thyrotoxicosis TT TL |
6 0 |
5 0 |
*NIPTMC: Non-incidental papillary thyroid microcarcinoma. † IPTMC: Incidental papillary thyroid microcarcinoma. †† TT & TL: Total thyroidectomy & total lobectomy.
Discussion
PTC is the most common thyroid malignancy. Kaliszewski et al. [22] reported a fourfold increase in PTMC incidence. In this study, PTC accounted for 86.7% of thyroid malignancies, PTMC comprising 36.2% of cases. The literature describes two clinically distinct types of PTMC: IPTMC and NIPTMC, which differ in clinical presentation, characteristics, and behavior [19,22].
Lombardi et al. and Durante et al. reported that IPTMC constituted the majority of PTMC cases, at 75.5% and 77%, respectively [23,24]. Elliot et al. [17] found an equal distribution of IPTMC and NIPTMC, whereas Kaliszewski et al. [22] reported that NIPTMC comprised 66.67% of PTMCs. In our study, 79.6% of PTMCs were IPTMCs found in post-surgical specimens (Table 1), while NIPTMCs represented 20.4% of cases occurring in normal thyroid tissue without associated pathology (Figure 1). The variation in the reported incidence of PTMC is likely related to different geographic populations, with some cohorts arising from endemic goiter areas [17].
The incidence of IPTMC in patients operated on for benign thyroid disease was 10.8%, compared to 9.3%, 10.41%, 16.5%, and 15.6% reported by Miccoli et al., de Carlos et al., Slijepcevic et al., and Smith et al. [25,26,27,28], respectively. IPTMC was significantly associated with MNG (P = 0.0005) and HT (P = 0.005) compared to Graves’ disease (P = 0.1171) and follicular adenoma (P = 0.5513) (Table 3). Similar findings were reported by other authors [27,28]. Smith et al. [28] found a significant association of IPTMC with MNG and toxic nodular goiter compared to Graves’ disease (P = 0.01), while Slijepcevic et al. [27] reported a higher incidence in HT patients and a lower incidence in toxic nodular goiter and Graves’ disease.
The association between HT and PTC has been extensively investigated. Bircan et al. [29] reported a 39% overall incidence of HT in PTMC cases, with concomitant occurrence ranging from 0.5% to 58% [29]. Graceffa et al. [30] reported a 40.2% association with the nodular variant of HT and 8.1% with the diffuse variant (P < 0.001), hypothesizing that the link may be due to an autoimmune response that develops alongside an antitumoral immune response. Nodular HT occurred in (42.9%) in the present study. Anderson et al. [31] reported nodular HT and PTMC in 42.7% and 16% respectively. Miccoli et al. [25] and Paparodes et al. [32] found that incidental thyroid carcinoma was significantly more frequent in euthyroid patients than in thyrotoxic or fully hypothyroid HT patients (P < 0.03).
Our study showed no significant gender difference between incidental and non-incidental PTMC (P = 0.324). NIPTMC patients were significantly younger, with a mean age of 37.14 + 14.28years compared to 44.15 +13.43 years in IPTMC cases (P = 0.0001), consistent with Elliott et al. [17]. Miccoli et al. and de Carlos et al. [25,26] reported no significant age or sex differences, while Smith et al. [28] and Lee et al. [16] found significant associations of young age and male sex with IPTMC.
PTMC generally has an indolent course with an excellent prognosis. However, an increasing number of studies have identified an aggressive subset of PTMC with high-risk pathologic features that negatively impact clinical outcomes and overall survival. In our study, high-risk features were present in 23.36% of cases, significantly more common in NIPTMC than IPTMC (75% vs. 10.1%, P = 0.004) (Table 3). Retrospective analyses by Lee et al. [14] and Al-Qurayshi et al. [33] using the National Cancer Database found that 20% and 19% of PTMCs, respectively, presented with high-risk aggressive features including ETE, central or lateral node involvement, lymphovascular invasion, and distant metastasis.
Aggressive histologic subtypes of PTMC have been associated with increased ETE and nodal involvement, as reported by Lee et al., indicating that these variants should be considered important factors when determining the extent of surgical intervention. In a study of 148 PTMC cases, Ghossein et al. found that larger nodal metastases (>1 cm) and aggressive histologic subtypes were associated with worse recurrence-free survival [34]. Our cohort did not include aggressive histologic subtypes such as tall cells, columnar cells, hobnail, diffuse sclerosing, and solid subtypes. The classic subtype was the most common in both NIPTMC (89.3%) and IPTMC (52.8%) cases, consistent with previous reports [25,35]. The minimally invasive follicular variant of papillary thyroid carcinoma (FVPTC) was significantly more common in IPTMC (35.8%) (Table 2).
PTMC shares similar molecular and immunophenotypic characteristics with larger PTCs. Park et al. reported comparable frequencies of the BRAFV600E mutation in PTMC and larger PTCs (65.6% vs. 67.2%) [15]. Recent studies suggest that telomerase reverse transcriptase (TERT) promoter mutations, which correlate with aggressive behavior and poor outcomes, are more common in aggressive histologic subtypes. However, their occurrence in PTMC is extremely low. Yang et al. reported a TERT promoter mutation frequency of 0.5% in PTMC compared to 5.8% in PTC >1 cm [36]. Currently, molecular testing is primarily used for larger PTC and its applicability to PTMC remains unclear. Further studies are needed to explore its prognostic role in PTMC [37,38,39]. However, if thyroidectomy is needed or preferred, molecular testing is unnecessary [40].
In our series, multifocal disease (MF) was present in 29.6% of PTMC patients who underwent total thyroidectomy (37 out of 125) in our study, 73% were bilateral with an average of 2.9 tumor foci. This aligns with published reports indicating multifocality ranging from 18-87% and bilaterality from 13-56% (41, 42, 14, 19, 26). So et al. [41] noted that the likelihood of contralateral lobe involvement increases with the increase in number of foci in one lobe, at 30.2% with two foci and 46.2% with three or more foci.
Like previously published reports [42], our analysis concluded that multifocal PTMCs were more frequently associated with high-risk aggressive features compared to unifocal tumors (48.6% vs. 14%, P = 0.007) and had a larger average maximum tumor diameter (P = 0.0054) (Table 4). Varshney et al. found that only ETE had a significant association with lymph node metastases (P > 0.05) [43]. In contrast, Dirikoc et al. identified MF and ETE as significant factors for lymph node metastasis [44].
Age and sex were not significant predictors of multifocality in our study, consistent with other reports [41]. Elbasan et al. [42] also reported no differences in age, sex, and BRAF mutation positivity between unifocal and bilateral tumors. Park et al. [45] identified age as a determinant of overall survival (OS) and disease-specific survival (DSS), while sex and multifocality were also prognosticators of OS. Our analysis showed that NIPTMC had a significantly higher association with multifocality, which was more common in MNG and HT (non-significantly) compared to Grave’s disease and adenomas (Table 4).
The number of PTMC cases remained stable over the two five-year periods of our study (2013-2017 vs. 2018-2022, P = 0.071), contrary to literature reporting an increased incidence over time [22,26]. This stability may reflect the impact of new ATA guidelines limiting FNAC in sub-centimeter nodules and possibly the effect of the 2020 pandemic on patient numbers.
The optimal management of PTMC continues to be a subject of significant debate due to variability in tumor presentation and behavior, challenging preoperative diagnosis, and variable incidence of multifocality, bilaterality, and aggressive features. Aggressive PTMCs often lack clinical signs and reliable diagnostic criteria for preoperative identification. Distinguishing between aggressive and indolent PTMC remains difficult [3,4].
Current ATA guidelines recommend TL or active surveillance for selected PTMC patients [6]. Despite this, TT remains the most common surgical approach, performed in 82.63%, 83%, and 73.9% of PTMCs reported by Al-Qurayshi et al. [33], Lee et al. [14], and Park et al. [45], respectively. The incidence of TT increased by 12% per year in the U.S., while lobectomies increased by 1% per year [5]. Advocates of TT cite frequent multifocality, bilaterality, and easier follow-up, while proponents of TL highlight lower surgical complication rates, especially for low-volume surgeons [46], and avoidance of lifetime thyroxine replacement therapy [47] and hypoparathyroidism risk [48]. In our study, fewer TLs (2.9%) and more TTs (97.1%) were performed in the second period compared to the first (14.9% TLs and 85.1% TTs) (P = 0.0007), indicating no impact of the 2017 ATA guidelines on our surgical practice [6].
The management strategy at Jordan Hospital Medical Center includes:
- High-Risk PTMCs: PTMCs with high-risk features such as ETE, lymph node metastasis, aggressive histologic subtype, and proximity to the trachea or recurrent laryngeal nerve require aggressive surgical management [49], including total thyroidectomy, lymph node dissection for clinical or US-positive nodes, and radioactive iodine ablation.
- Benign Thyroid Disease: Patients with presumed benign thyroid disease are referred for surgery based on specific indications related to the thyroid pathology. Total thyroidectomy is often required for associated conditions like MNG, toxic nodular goiter, Graves’ disease, and Hashimoto thyroiditis (HT). PTMC diagnosis in these cases is typically made postoperatively through pathological examination of thyroidectomy specimens.
- Low-Risk PTMCs: For preoperatively diagnosed low-risk PTMCs, including unifocal intrathyroidal tumors with clinically negative nodes, management remains controversial. Decisions are made through a physician-patient shared decision-making process, considering patient preferences, beliefs, comorbidities, and available resources [45,50,51]. A5 or TL are viable options.
Ultimately, physicians should base decisions on the best available evidence, considering patient comorbidities, age, and treatment preferences [45,50,51]. Enhancing patient education on the disease process and current management guidelines is essential for better-shared decision-making [51]. However, Bashir et al. [50] found that patient preference-based decisions for TT vs. TL were less guideline-concordant (21% vs. 79%), with more TTs performed (74.4% vs. 41%, P = 0.001). Our experience shows patients favor TT due to fear of cancer recurrence or potential future surgeries, to avoid waiting lists, and for ease of follow-up, especially for international patients seeking treatment [50]. The ATA risk stratification for PTMCs aids clinical decision-making [4].
This study has several limitations. It is a retrospective analysis from a single institution with a relatively small sample size. Most patients were young and underwent surgical treatment, which may overestimate the prevalence of PTMC. None of the patients underwent AS; therefore, disease progression data is unavailable. Multi-center clinical trials are needed to help with presurgical disease progression risk stratification and determine the best treatment strategies, prognosis, and outcomes.
Conclusions
PTMC is the most common thyroid malignancy. While classically it is considered indolent, some cases are associated with aggressive behavior and high-risk features, requiring more aggressive surgical intervention, especially in NIPTMC as demonstrated in our study. The challenge lies in identifying and applying prognostic features in the preoperative setting, such as identifying aggressive histologic features or molecular high-risk mutations in FNA specimens, similar to larger PTCs. The outcomes for patients in the current study were favorable, with no mortality or recurrence during the follow-up period. However, most patients underwent total thyroidectomy. Further investigation is needed to evaluate the prognosis, outcomes, and cost of new less aggressive treatment methods. Shared decision-making between physicians and patients is crucial for optimal outcomes, especially in low-risk PTMC where active surveillance (AS) or lobectomy are viable options.
Disclosure
The authors have no disclosures or conflicts that could jeopardize the current study. No funding was received for this study.
Author Contributions
Amani A. Bashir: Conceptualization, Investigation, Writing-Original draft preparation, Mohamed M. El-Zaheri: Writing- Reviewing and Editing, Ahmad A. Bashir: Surgeon contributor, Visualization, Writing- Reviewing and Editing, Luma Fayyad: Investigating pathologist, Aiman H. Obed: Surgeon contributor, Writing- Reviewing & Editing, Dima Alkam: Investigating pathologist, Writing- Reviewing and Editing, Abdalla Y. Bashir: Conceptualization, Surgeon contributor, Data Curation, Investigation, Resources, Supervision, Writing- Reviewing and Editing.
Funding
No funding was received for this study.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board (Ethics Committee) of Jordan Hospital (JH/IRB/2022/08-9 on August 10th, 2022).” .
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
Special thanks to Mrs. Shyma Taha for her editorial services and to Mr. Ghaleb Alhelli for performing the statistical analysis.
Abbreviations
| PTC: Papillary thyroid carcinoma | FNA: Fine needle aspiration |
| PTMC: Papillary thyroid microcarcinoma | US: Ultrasonography |
| IPTMC: Incidental PTMC | ETE: Extra-thyroidal extension |
| NIPTMC: Non-incidental PTMC | US-FNAC: ultrasound-guided FNAC |
| AS: Active surveillance | ATA: American Thyroid Association |
| TL: Total lobectomy | WHO: World Health Organization |
| TT: Total thyroidectomy | HT: Hashimoto’s thyroiditis |
| FNAC: Fine needle aspiration cytology | MNG: Multinodular goiter |
References
- Nimri O, Arqoub K, Jemal A. Jordan Cancer Registry. Amman, Jordan : Ministry of Health (MOH), 2015.
- Siegel RL, Miller KD, Jemal A. Cancer Statistics 2020 CA cancer. J Elin 2020, 70, 7–50. [Google Scholar]
- Rovira, A Nition IJ, Simo R. Papillary microcarcinoma of the thyroid gland: current controversies and management. Curr Opin Otolaryngol Head Neck Surg 2019, 27, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Stefanova DI, Bose A, Ullmann TM, et al. Does the ATA Risk Stratification Apply to Patients with Papillary Thyroid Microcarcinoma? World J Surg 2020, 44, 452–460.
- Sosa JA, Hanna JW, Robinson KA, Lanman RB. Does the ATA Risk Stratification Apply to Patients with Papillary Thyroid Microcarcinoma? Surgery 2013, 154, 1420–1426, discussion 1426-7. [Google Scholar]
- Haugen, BR. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: What is new and what has changed? Cancer 2017, 123, 372–381. [Google Scholar] [CrossRef]
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Sinclair CF, Baek JH, Hands KE, et al. General Principles for the Safe Performance, Training, and Adoption of Ablation Techniques for Benign Thyroid Nodules: An American Thyroid Association Statement. Thyroid 2023, 33, 1150–1170. [Google Scholar] [CrossRef]
- Miyauchi A, Ito Y, Oda H. Insights into the Management of Papillary Microcarcinoma of the Thyroid. Thyroid 2018, 28, 23–31. [Google Scholar] [CrossRef]
- Takebe K, Date M, Yamamoto Y. Mass screening for thyroid cancer with ultrasonography [in Japanese]. Karkinos 1994, 7, 309–317. [Google Scholar]
- Bondeson L, Ljungberg O. Occult thyroid carcinoma at autopsy in Malmö, Sweden. Cancer. 1981, 47, 319–323. [Google Scholar] [CrossRef]
- Lloyd RV, Osamura RY, Klöppel G, Rosai J. WHO Classification of Tumours of Endocrine Organs WHO Classification of Tumours, 4th Edition, Volume 10. IARC Publications, 2017. ISBN-13: 978-92-832-4493-6.
- Jung CK, Bychkov A, Kakudo K. Update from the 2022 World Health Organization Classification of Thyroid Tumors: A Standardized Diagnostic Approach. Endocrinol Metab (Seoul) 2022, 37, 703–718. [Google Scholar] [CrossRef] [PubMed]
- Lee CI, Kutlu O, Khan ZF, Picado O, Lew JI. Margin Positivity and Survival in Papillary Thyroid Microcarcinoma: A National Cancer Database Analysis. J Am Coll Surg 2021, 233, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Park YJ, Kim YA, Lee YJ, et al. Papillary microcarcinoma in comparison with larger papillary thyroid carcinoma in BRAF(V600E) mutation, clinicopathological features, and immunohistochemical findings. Head Neck 2010, 32, 38–45. [Google Scholar] [CrossRef]
- Yan L, Blanco J, Reddy V, Al-Khudari S, Tajudeen B, Gattuso P. Clinicopathological features of papillary thyroid microcarcinoma with a diameter less than or equal to 5 mm. Am J Otolaryngol. 2019, 40, 560–563. [Google Scholar] [CrossRef]
- Elliott MS, Gao K, Gupta R, Chua EL, Gargya A, Clark J. Management of incidental and non-incidental papillary thyroid microcarcinoma. J Laryngol Otol, 2013; 127, Suppl. 2, S17–S23.
- Kaliszewski K, Wojtczak B, Strutyńska-Karpińska M, Łukieńczuk T, Forkasiewicz Z, Domosławski P. Incidental and non-incidental thyroid microcarcinoma. Oncol Lett 2016, 12, 734–740. [Google Scholar] [CrossRef]
- Mehanna H, Al-Maqbili T, Carter B, et al. Differences in the recurrence and mortality outcomes rates of incidental and nonincidental papillary thyroid microcarcinoma: a systematic review and meta-analysis of 21 329 person-years of follow-up. J Clin Endocrinol Metab 2013, 99, 2834–2843. [Google Scholar]
- Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2009, 19, 1159–1165. [Google Scholar] [CrossRef]
- Cibas ES, Ali SZ. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346.
- Kaliszewski K, Zubkiewicz-Kucharska A, Kiełb P, Maksymowicz J, Krawczyk A, Krawiec O. Comparison of the prevalence of incidental and non-incidental papillary thyroid microcarcinoma during 2008-2016: a single-center experience. World J Surg Oncol 2018, 16, 202. [Google Scholar] [CrossRef]
- Lombardi CP, Bellantone R, De Crea C, et al. Papillary thyroid microcarcinoma: extrathyroidal extension, lymph node metastases, and risk factors for recurrence in a high prevalence of goiter area. World J Surg 2010, 34, 1214–1221. [Google Scholar] [CrossRef]
- Durante C, Attard M, Torlontano M, et al. Identification and optimal postsurgical follow-up of patients with very low-risk papillary thyroid microcarcinomas. J Clin Endocrinol Metab 2010, 95, 4882–4888. [Google Scholar] [CrossRef] [PubMed]
- Miccoli P, Minuto MN, Galleri D, et al. Incidental thyroid carcinoma in a large series of consecutive patients operated on for benign thyroid disease. ANZ J Surg 2006, 76, 123–126. [Google Scholar] [CrossRef] [PubMed]
- de Carlos J, Ernaga A, Irigaray A. Incidentally discovered papillary thyroid microcarcinoma in patients undergoing thyroid surgery for benign disease. Endocrine 2022, 77, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Slijepcevic N, Zivaljevic V, Marinkovic J, Sipetic S, Diklic A, Paunovic I. Retrospective evaluation of the incidental finding of 403 papillary thyroid microcarcinomas in 2466 patients undergoing thyroid surgery for presumed benign thyroid disease. BMC Cancer 2015, 15, 330. [Google Scholar]
- Smith JJ, Chen X, Schneider DF, et al. Cancer after thyroidectomy: a multi-institutional experience with 1,523 patients. J Am Coll Surg 2013, 216, 571–577, discussion 577-9. [Google Scholar] [CrossRef]
- Bircan HY, Koc B, Akarsu C, et al. Is Hashimoto’s thyroiditis a prognostic factor for thyroid papillary microcarcinoma? Eur Rev Med Pharmacol Sci 2014, 18, 1910–1915.
- Graceffa G, Patrone R, Vieni S, et al. Association between Hashimoto’s thyroiditis and papillary thyroid carcinoma: a retrospective analysis of 305 patients. BMC Endocr Disord, 2019 May. 29;19(Suppl 1):26.
- Anderson L, Middleton WD, Teefey SA, et al. Hashimoto thyroiditis: Part 2, sonographic analysis of benign and malignant nodules in patients with diffuse Hashimoto thyroiditis. AJR Am J Roentgenol. 2010, 195, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Paparodis R, Imam S, Todorova-Koteva K, Staii A, Jaume JC. Hashimoto’s thyroiditis pathology and risk for thyroid cancer. Thyroid 2014, 24, 1107–1114. [Google Scholar] [CrossRef]
- Al-Qurayshi Z, Nilubol N, Tufano RP, Kandil E. Wolf in Sheep’s Clothing: Papillary Thyroid Microcarcinoma in the US. J Am Coll Surg 2020, 230, 484–491. [Google Scholar] [CrossRef]
- Ghossein R, Ganly I, Biagini A, Robenshtok E, Rivera M, Tuttle RM. Prognostic factors in papillary microcarcinoma with emphasis on histologic subtyping: a clinicopathologic study of 148 cases. Thyroid. Thyroid 2104, 24, 245–253. [Google Scholar]
- Domínguez JM, Nilo F, Martínez MT, et al. Papillary thyroid microcarcinoma: characteristics at presentation, and evaluation of clinical and histological features associated with a worse prognosis in a Latin American cohort. Arch Endocrinol Metab 2018, 62, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Yang J, Gong Y, Yan S, Chen H, Qin S, Gong R. Association between TERT promoter mutations and clinical behaviors in differentiated thyroid carcinoma: a systematic review and meta-analysis. Endocrine 2020, 67, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Xing M, Liu R, Liu X, et al. BRAF V600E and TERT promoter mutations cooperatively identify the most aggressive papillary thyroid cancer with highest recurrence. J Clin Oncol 2014, 32, 2718–2726. [Google Scholar] [CrossRef]
- Liu R, Bishop J, Zhu G, Zhang T, Ladenson PW, Xing M. Mortality Risk Stratification by Combining BRAF V600E and TERT Promoter Mutations in Papillary Thyroid Cancer: Genetic Duet of BRAF and TERT Promoter Mutations in Thyroid Cancer Mortality. JAMA Oncol 2017, 3, 202–208. [Google Scholar] [CrossRef]
- Melo M, da Rocha AG, Vinagre J, et al. TERT promoter mutations are a major indicator of poor outcome in differentiated thyroid carcinomas. J Clin Endocrinol Metab 2014, 99, E754–E765. [Google Scholar] [CrossRef]
- Patel KN, Yip L, Lubitz CC, et al. The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults. Ann Surg 2020, 271, e21–e93. [Google Scholar] [CrossRef]
- So YK, Kim MW, Son YI. Multifocality and bilaterality of papillary thyroid microcarcinoma. Clin Exp Otorhinolaryngol 2015, 8, 174–178. [Google Scholar] [CrossRef]
- Elbasan O, Ilgın C, Gogas Yavuz D. Does total tumour diameter, multifocality, number of tumour foci, or laterality predict lymph node metastasis or recurrence in differentiated thyroid cancer? Endokrynol Pol 2023, 74, 153–167.
- Varshney R, Pakdaman MN, Sands N, et al. Lymph node metastasis in thyroid papillary microcarcinoma: a study of 170 patients. J Laryngol Otol 2014, 128, 922–925. [Google Scholar] [CrossRef]
- Dirikoc A, Tam AA, Ince N, et al. Papillary thyroid microcarcinomas that metastasize to lymph nodes. Am J Otolaryngol 2021, 42, 103023. [Google Scholar] [CrossRef]
- Park KW, Han AY, Kim CM, Wang MB, Nguyen CT. Is lobectomy sufficient for multifocal papillary thyroid microcarcinoma? Am J Otolaryngol 2023, 44, 103881. [Google Scholar] [CrossRef] [PubMed]
- Duclos A, Peix JL, Colin C, et al. Influence of experience on performance of individual surgeons in thyroid surgery: prospective cross sectional multicentre study. BMJ 2012, 344, d8041. [Google Scholar] [CrossRef] [PubMed]
- Brito JP, Hay ID. Management of Papillary Thyroid Microcarcinoma. Endocrinol Metab Clin North Am 2019, 48, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Bashir AY, Alzubaidi AN, Bashir MA, et al. he Optimal Parathyroid Hormone Cut-Off Threshold for Early and Safe Management of Hypocalcemia After Total Thyroidectomy. Endocr Pract 2021, 27, 925–933. [Google Scholar] [CrossRef]
- Yu XM, Wan Y, Sippel RS, Chen H. Should all papillary thyroid microcarcinomas be aggressively treated? An analysis of 18,445 cases. Ann Surg 2011, 254, 653–660. [Google Scholar] [CrossRef]
- Bashir AY, Zaheri MM, Obed A, et al. Patients’ preferences impact on decision-making for clinical solitary thyroid nodule in a global healthcare setting: a clinical study. Series Endo Diab Met 2021, 3, 48–58. [Google Scholar] [CrossRef]
- Koot A, Soares P, Robenshtok E, et al. Position paper from the Endocrine Task Force of the European Organisation for Research and Treatment of Cancer (EORTC) on the management and shared decision making in patients with low-risk micro papillary thyroid carcinoma. Eur J Cancer 2023, 179, 98–112. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



