
Submitted:
21 April 2025
Posted:
22 April 2025
You are already at the latest version
Abstract
Accurate adherence to partial weight-bearing instructions is critical for successful rehabilitation after lower limb surgery, yet traditional training methods often fail to ensure consistent patient compliance. This study evaluates the effectiveness of a novel, low-cost tactile biofeedback device ("weight-bearing sensitivity enhancer") designed to enhance patients’ perception of load applications during recovery. A total of 34 patients undergoing rehabilitation after surgeries such as femoral fracture repair, hip arthroplasty, or knee arthroplasty were randomly assigned to either the intervention group (using the biofeedback device) or a control group (standard care). The primary outcome measured was the discrepancy between the recommended and actual partial weight-bearing, assessed digitally at multiple intervals. Patients using the biofeedback device significantly reduced this discrepancy compared to controls, demonstrating statistically significant improvements in accurate weight-bearing (p < 0.05). Conversely, the control group showed no meaningful improvement. These findings suggest that integrating this affordable tactile feedback system into postoperative rehabilitation protocols effectively promotes correct partial weight-bearing. Further research involving larger and more diverse patient populations is necessary to validate these preliminary results and confirm the long-term efficacy and generalizability of the device.
Keywords:
Physical therapy
; rehabilitation
; lower limb surgery
; partial weight bearing
1. Introduction
In orthopaedic rehabilitation following lower limb surgeries, such as fracture repair, total hip replacement, or knee arthroplasty, partial weight-bearing is widely recognised as a cornerstone of effective postoperative care. The clinical rationale for prescribing partial weight-bearing is twofold. On the one hand, applying a controlled mechanical load to the healing bone stimulates osteoblastic activity and bone remodelling, essential for the recovery and strengthening of the skeletal structure[1,2]. On the other hand, limiting the load prevents excessive stress that could lead to complications such as fracture malunion, implant failure, or undesired alterations in gait biomechanics [3,4]. Despite its importance, achieving the recommended weight-bearing remains challenging. Traditional methods of teaching and monitoring partial weight-bearing, such as using home scales, verbal instructions, or tactile cues (e.g., placing a hand under the foot), have been found lacking in several respects. These static modalities fail to capture the dynamic nature of weight distribution during ambulation and daily activities, leading to poor correlation between estimated and actual load application [3]. Research has repeatedly reported that patients, regardless of repeated instruction, struggle to consistently reproduce the given weight-bearing limits over time, with notable deviations noted during dynamic activities such as walking [5,6]. The resulting discrepancies can shift the centre of gravity contrarily, increasing muscular effort, particularly in the abductor muscles, and introduce compensatory movement patterns that further compromise rehabilitation outcomes [7]. In recent years, biofeedback systems have injected a new dimension into postoperative rehabilitation protocols. These systems, which include digital portable insoles and wearable sensor arrays, provide continuous, real-time feedback on the load exerted on the lower limbs. Unlike traditional static assessments, these devices enable patients to adjust their gait dynamically, ensuring that the load remains within prescribed limits during functional activities [5,7]. Despite the demonstrated efficacy of such digital solutions, their widespread adoption is hampered by two critical limitations: high costs and evidence of benefit largely restricted to short-term outcomes. Consequently, an unmet need remains for accessible, economically viable tools to deliver sustained improvements in load perception and weight-bearing accuracy. Addressing this gap, the present study examines a “weight-bearing sensitivity enhancer” constructed from readily available, low-cost materials. This novel biofeedback device is designed to provide continuous tactile input during ambulation, effectively bridging the gap between static instruction and the dynamic realities of everyday movement. By integrating an intuitive feedback mechanism into the rehabilitation process, the device aims to facilitate more accurate reproduction of prescribed partial weight-bearing and mitigate the deleterious effects of imprecise load application [1,3]. Unlike many high-end commercial systems, this prototype promises an economical solution potentially applicable in both clinical settings and community or home-based rehabilitation programs. Furthermore, the multifaceted approach of the study acknowledges the limitations inherent in previous research. Past investigations have often been constrained by small, heterogeneous patient populations and short-term follow-up periods, thereby limiting the generalizability of their findings to diverse clinical contexts [4,6]. Our study seeks to overcome these barriers by providing a more extended evaluation of the weight-bearing sensitivity enhancer’s performance over a longer duration and across a broader spectrum of lower limb pathologies. By doing so, we hope to offer stronger evidence regarding the long-term benefits of continuous biofeedback in enhancing partial weight-bearing accuracy and accelerating postoperative recovery. In summary, integrating an accessible, low-cost biofeedback device into rehabilitation protocols represents a promising evolution in the management of partial weight-bearing. This study is positioned within an emerging body of literature that increasingly recognises the limitations of traditional static methods and advocates for dynamic, real-time solutions that improve load perception and enhance overall functional recovery. The extended evaluation and detailed analysis presented herein aim to lay the groundwork for future research and contribute to the standardisation of innovative, economically feasible rehabilitation strategies for patients recovering from lower limb surgery. (Figure 1.)
2. Materials and Methods
The study recruited 34 random patients who had undergone lower limb orthopaedic surgery, meeting the inclusion criteria of being aged between 18 and 85 years and having undergone surgery for femoral fracture, hip arthroplasty, trimalleolar ankle fracture, pelvic fracture, or knee arthroplasty. Randomisation was performed using the Random.org tool (https://www.random.org/). Patients were assigned IDs and participants for each group were randomly selected. Exclusion criteria included pre-existing walking difficulties, neurological conditions, and foot size outside the measurement range of the insole. Before recruitment, all patients were informed about the study and provided signed informed consent. The recruitment was conducted at the Rehabilitation Clinic in Novaggio and the Physiatry Department of San Carlo Hospital in Bordighera. The recruiting physicians and physiotherapists were aware of the study protocol. Patients were randomly assigned to either the treatment group or the control group. The digital insole used for measuring plantar pressure was GeBiom, GP MobilData – Go-tec, and the pressure measurement system was GP MobilData wireless. The software divided the plantar surface into several regions to evaluate the foot's load. The sensory feedback incentivator was designed and created from preformed rubber insoles with protruding automatic buttons, which provided feedback and encouraged sensitivity to the load. Four buttons were placed per insole in a vertical line along the heel, with the first button 2.5 cm from the end of the insole and the other three buttons spaced 1.5 cm apart along the midline. Depending on the load, the starting insole or three materials of variable density (foam rubber, 6 mm neoprene, or 8 mm neoprene) were used to increase the patient's sensitivity to proprioceptive stimuli and impose increased load on the limb (Figure 2).
The insoles were calibrated to apply a specific load on the heel before the material reached zero height, and the buttons were felt for proprioceptive feedback. The complete insole was placed inside the patient's shoe to provide sensory feedback on the correct load. The sensory feedback incentivator was utilised in the treatment group's evaluation and treatment phases. The evaluation protocol included collecting demographic data, medical history, and conducting physical examinations such as the Numeric Rating Scale (NRS) and the 6 Minutes Walking Test (6MWT). The study design was quasi-experimental, where the treated group received treatment with an incentivator while the control group did not receive any treatment. The primary outcome measure of the study was the change in loaded weight (Δ loaded weight), defined as the difference between the theoretical weight and the actual weight measured at two time points: T0 (before the start of treatment) and T1 (at the end of hospitalisation). Statistical analysis compared the treatment and control groups regarding their Δ loaded weight at T0 and T1. Specifically, the values at T0 and T1 were compared using a parametric intra-group test, assuming a normal distribution: the T-test (or Student's t-test). A non-parametric test, the Wilcoxon-Mann-Whitney test for paired data, was also performed for confirmation. The significance level for both tests was set at p<0.05, meaning that results at the 95th percentile were considered valid, resulting in 95% confidence that the differences between the groups were significant. SPSS® v19.0 and Excel 2019 were used for data analysis.
This study was conducted by the ethical standards outlined by the Declaration of Helsinki and approved by the University of Insubria Ethics Committee (protocol number 0026262).
3. Results
Results from the study were objectively quantified by digitally recording the load expressed in Kg maintained by patients during ambulation, using measurements at the beginning, middle, and end of treatment. The experimental treatment's effectiveness was calculated by considering the difference between the load granted during the orthopaedic visit and the load used by the patients (Δ weight loaded), comparing the average values and standard deviations between the experimental and control groups. In the experimental group, a Δ load was observed at the beginning of treatment without using the load incentivizer, equal to 12.9 kg ± 10.9. At the beginning of therapy utilising the incentivizer, the Δ weight loaded decreased to 5.6 kg ± 8.5. In the middle of treatment, following the integration of the load incentivizer in the treatment plan, the Δ weight loaded was 4.4 kg ± 6.3, and at the end of treatment, it was 2.0 kg ± 3.0. The change in load perception was confirmed by the T-test between T0 and T1, with a P-value = 0.021251 and therefore < 0.05, confirming the alternative hypothesis of a difference between the beginning and end of treatment at 95% (Table 1).
Other parameters were also analysed, such as the standard deviations of individual subjects at different measurement times (columns), indicating the intra-step variability of the subject (how much the patient varies the load in different steps within the same measurement). Between T0 and T1, the mean value of the standard deviations goes from 2.5 kg ± 1.0 at T0, to 3.4 kg ± 1.6 at T0 with incentivator, to 2.0 kg ± 1.2 at T1. In the control group, the Δ weight loaded at the beginning of treatment was 16.3 kg ± 14.7, while at the end of treatment, where the incentivizer was never used, the Δ weight loaded decreased to 12.8 kg ± 8.4. In this case, the statistical test with a P-value = 0.218672 and therefore > 0.05 confirms the null hypothesis of equality and the absence of improvement between the beginning and end of treatment (Table 2).
Intra-step variability was also analysed in this group, with 3.1 kg ± 1.9 at T0 and 3.5 kg ± 3.1 at T1. Non-parametric statistics were also performed in this study. In the T0 and T1 comparison, the test group showed a greater improvement in weight load than the control group. The difference between T0 and T1 is confirmed at 99% in the test group, with a P-value < 0.01. The comparison between the test T0 and control T0 and the absence of a P-value < 0.01 allows me to confirm that the two groups start from homogeneous baseline conditions and can be compared. The comparison between control T0 and control T1 and the absence of a P-value < 0.01 confirms the equality between the beginning and end of treatment and the lack of improvement in the control group. The intergroup analysis at T1 between the test and control groups, with a P-value < 0.01, shows that the two groups behave differently at discharge. The statistical significance is confirmed. As for the NRS and 6MWT, significant improvements were observed in both the experimental and control groups (Figure 3).
4. Discussion
The current study addressed the longstanding controversy regarding the standardised implementation of partial weight-bearing protocols—a topic that has generated both patient and therapist apprehension. Our findings demonstrate that using a load incentivizer, as a biofeedback device, significantly improves patients’ perception and application of partial load during rehabilitation. Specifically, the study shows an immediate enhancement in load perception, as revealed by statistically significant differences between baseline (T0) and post-stimulation (T0 stimulus) assessments. This immediate improvement appears to be linked to an enhanced anticipatory system that better prepares the neuromuscular system to regulate weight distribution during gait.
The immediate impact observed in the experimental group is particularly notable when contrasted with the control group, which received conventional partial weight-bearing training without biofeedback support. The control group showed no significant improvements in the application of partial load, suggesting that traditional techniques may lack the dynamic feedback necessary to achieve precise weight-bearing. This observation aligns with previous research indicating that biofeedback-based interventions play a pivotal role in maintaining long-term compliance with weight-bearing prescriptions, as the real-time cueing allows patients to adjust their performance continuously throughout rehabilitation [8,9].
Furthermore, the data indicate that the beneficial effects of the load incentivizer persist over time. Such long-term retention of proper weight-bearing may be attributed to the repetitive, self-correcting nature of the biofeedback mechanism, which reinforces correct loading behaviours. In contrast, other rehabilitation modalities, which rely primarily on verbal instructions or static measures, have not demonstrated comparable sustained improvements. This sustained effect is especially relevant given research emphasising the importance of integrating wearable and real-time biofeedback devices in rehabilitation protocols [7,10].
An additional strength of the load incentivizer lies in its universal applicability across different age groups. Our study indicates that improvements in load perception were independent of patient age, demonstrating that both younger and older patients can benefit from such biofeedback technologies. This finding is significant since many patients requiring partial weight-bearing protocols are elderly, and previous studies have identified age-related challenges in complying with weight-bearing instructions [9,11]. The demonstrated efficacy of our device across age groups supports the potential of biofeedback to serve as an essential adjunct in rehabilitation for a heterogeneous patient population.
Beyond the objective measures of load application, the subjective benefits reported by patients further underscore the value of the load incentivizer. Participants consistently reported a heightened awareness of their weight-bearing patterns and an improved ability to transfer these learned strategies from the clinical setting to daily activities. This enhanced self-efficacy will likely contribute to overall patient confidence and adherence to the rehabilitation plan. In practical terms, using a load incentivizer facilitates safer limb loading, which is crucial for preventing complications in the post-surgical phase. It contributes to a more positive overall rehabilitation experience.
It is important to note that while secondary outcomes such as pain reduction and overall walking quantity did not significantly differ between groups, these results indicate that the primary benefits of biofeedback are specific to the modulation of weight distribution rather than general functional activity. In other words, the device appears to be optimised for fine-tuning partial weight-bearing's perceptual and motor control aspects without necessarily altering broader clinical parameters such as pain or activity level. This specificity aligns with the understanding that biofeedback devices primarily act at the neuromuscular and perceptual levels, reinforcing correct load application rather than inducing direct symptomatic relief [12].
5. Conclusions
This study has shown the effectiveness of an incentivator for load perception and correct partial weight therapy in a population of patients undergoing rehabilitation post-lower limb surgery. The traditional methods, such as using a home scale, were ineffective in load perception. At the same time, a tactile exteroceptive input showed a positive effect on load perception with statistically and clinically significant results in the long term. The implementation of correct partial load is essential for effective and rapid recovery, as well as safe patient work. The study also reflects on the control group and the lack of improvement in load perception without using the incentivator. The limitations of this study include the small sample size and the large variability of analysed pathologies. Therefore, further studies are needed to evaluate the effectiveness of the load perception incentivator on a larger sample size and the effect on specific pathologies. Improving the incentivator's accuracy and standardisation for even more accurate use would also be useful. On the other hand, this prototype of incentivator has been built using widely available and cheap materials. Authors would like to highlight that this incentivator could be an inexpensive solution for accurate physical therapy in a house or community-based setting. This is a pilot study, and further research is necessary to consolidate the evidence regarding the effectiveness of the load perception incentivator, the rehabilitation protocol, and further investigation in non-hospital environments.
Author Contributions
AM: Methodology; IC: Data curation; MF: Formal analysis; SN: Project administration; RD: Resources; MP: Writing - review & editing; AB: Writing - review & editing; PAZ: Writing - original draft.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request from the authors.
References
- Yu, S.; McDonald, T.; Jesudason, C.; Stiller, K.; Sullivan, T. Orthopedic inpatients' ability to accurately reproduce partial weight bearing orders. Orthopedics 2014, 37, e10–e18. [Google Scholar] [CrossRef] [PubMed]
- Aesch, A.V.v.; Häckel, S.; Kämpf, T.; Baur, H.; Bastian, J.D. Audio-Biofeedback Versus the Scale Method for Improving Partial Weight-Bearing Adherence in Healthy Older Adults: A Randomised Trial. European Journal of Trauma and Emergency Surgery 2024, 50, 2915–2924. [Google Scholar] [CrossRef] [PubMed]
- Ebert, J.R.; Ackland, T.; Lloyd, D.G.; Wood, D. Accuracy of Partial Weight Bearing After Autologous Chondrocyte Implantation. Archives of Physical Medicine and Rehabilitation 2008, 89, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- Vusse, M.v.d.; Kalmet, P.H.S.; Bastiaenen, C.H.G.; Horn, Y.; Brink, P.R.; Seelen, H.A. Is the AO Guideline for Postoperative Treatment of Tibial Plateau Fractures Still Decisive? A Survey Among Orthopaedic Surgeons and Trauma Surgeons in the Netherlands. Archives of Orthopaedic and Trauma Surgery 2017, 137, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, Ø.; Gulliksen, W.; Kwiatkowski, A.D.; Skavø, M.; Isern, H.; Shayestehpour, M.; Steinert, M.; Bye, R.T.; Hellevik, A.I. Implementation and Evaluation of a Vibrotactile Assisted Monitoring and Correction System for Partial Weight-Bearing in Lower Extremities. 2023. [CrossRef]
- Abdalbary, S.A. Partial Weight Bearing in Hip Fracture Rehabilitation. Future Science Oa 2017, 4. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Xu, X.; Chai, Z.; Wang, T.; Shen, X.; Sun, T. A Wearable Biofeedback Device for Monitoring Tibial Load During Partial Weight-Bearing Walking. Ieee Transactions on Neural Systems and Rehabilitation Engineering 2023, 31, 3428–3436. [Google Scholar] [CrossRef] [PubMed]
- Lieshout, R.v.; Stukstette, M.J.; Bie, R.A.d.; Vanwanseele, B.; Pisters, M.F. Biofeedback in Partial Weight Bearing: Validity of 3 Different Devices. Journal of Orthopaedic and Sports Physical Therapy 2016, 46, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Hustedt, J.W.; Blizzard, D.J.; Baumgaertner, M.R.; Leslie, M.; Grauer, J.N. Lower-Extremity Weight-Bearing Compliance Is Maintained Over Time After Biofeedback Training. Orthopedics 2012, 35. [Google Scholar] [CrossRef] [PubMed]
- Bowman, T.; Gervasoni, E.; Arienti, C.; Lazzarini, S.G.; Négrini, S.; Crea, S.; Cattaneo, D.; Carrozza, M.C. Wearable Devices for Biofeedback Rehabilitation: A Systematic Review and Meta-Analysis to Design Application Rules and Estimate the Effectiveness on Balance and Gait Outcomes in Neurological Diseases. Sensors 2021, 21, 3444. [Google Scholar] [CrossRef] [PubMed]
- Hustedt, J.W.; Blizzard, D.J.; Baumgaertner, M.R.; Leslie, M.; Grauer, J.N. Effect of Age on Partial Weight-Bearing Training. Orthopedics 2012, 35. [Google Scholar] [CrossRef] [PubMed]
- Raaben, M.; Redzwan, S.; Augustine, R.; Blokhuis, T.J. COMplex Fracture Orthopedic Rehabilitation (COMFORT) - Real-Time Visual Biofeedback on Weight Bearing Versus Standard Training Methods in the Treatment of Proximal Femur Fractures in the Elderly: Study Protocol for a Multicenter Randomized Controlled Trial. Trials 2018, 19. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic of partial weight-bearing functionality: A graphical representation of the relationship between the load applied on the operated foot and the feedback provided by the load perception incentivator.
Figure 1.
Schematic of partial weight-bearing functionality: A graphical representation of the relationship between the load applied on the operated foot and the feedback provided by the load perception incentivator.
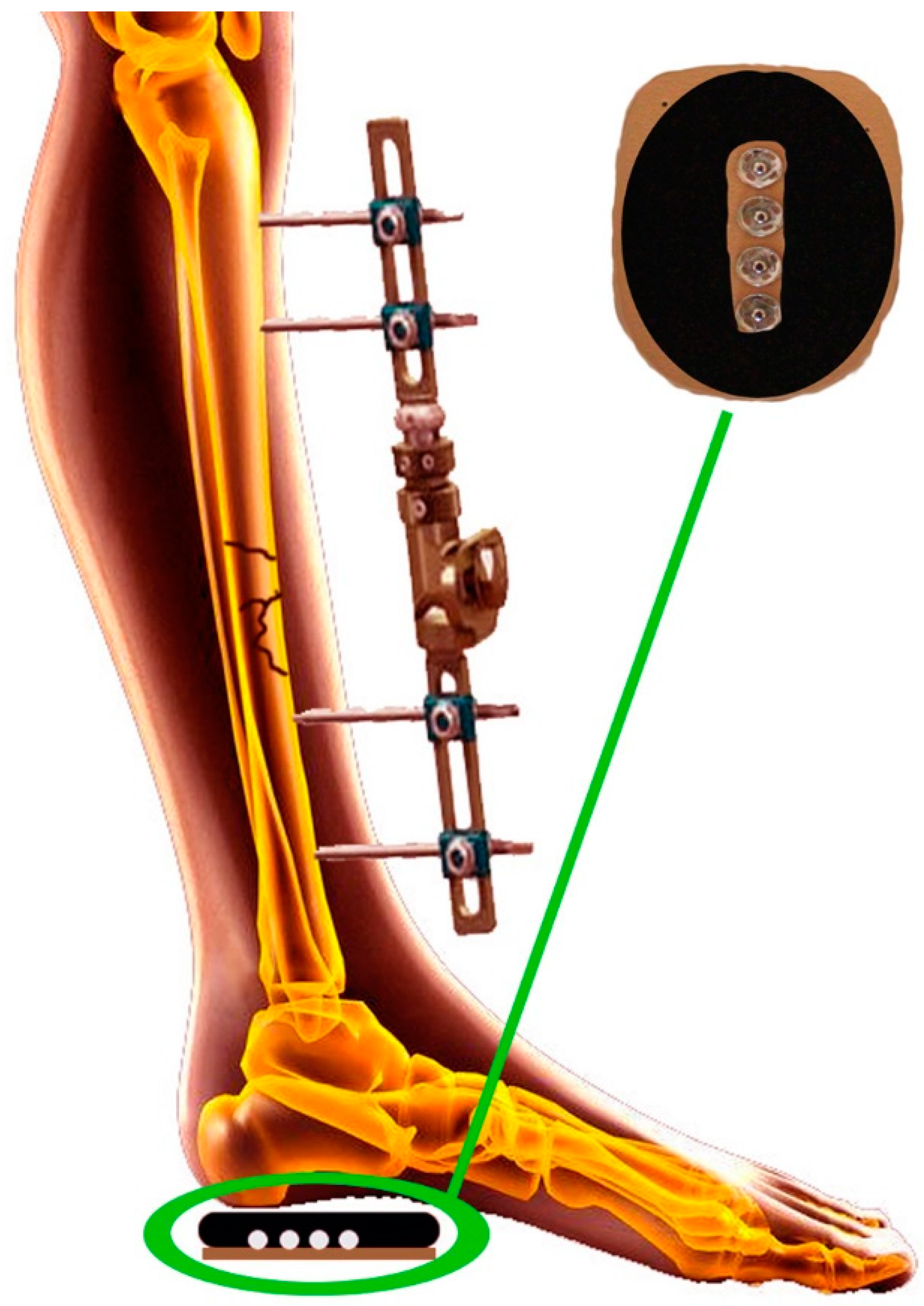
Figure 2.
Design and Construction of the Load Perception Incentivator.
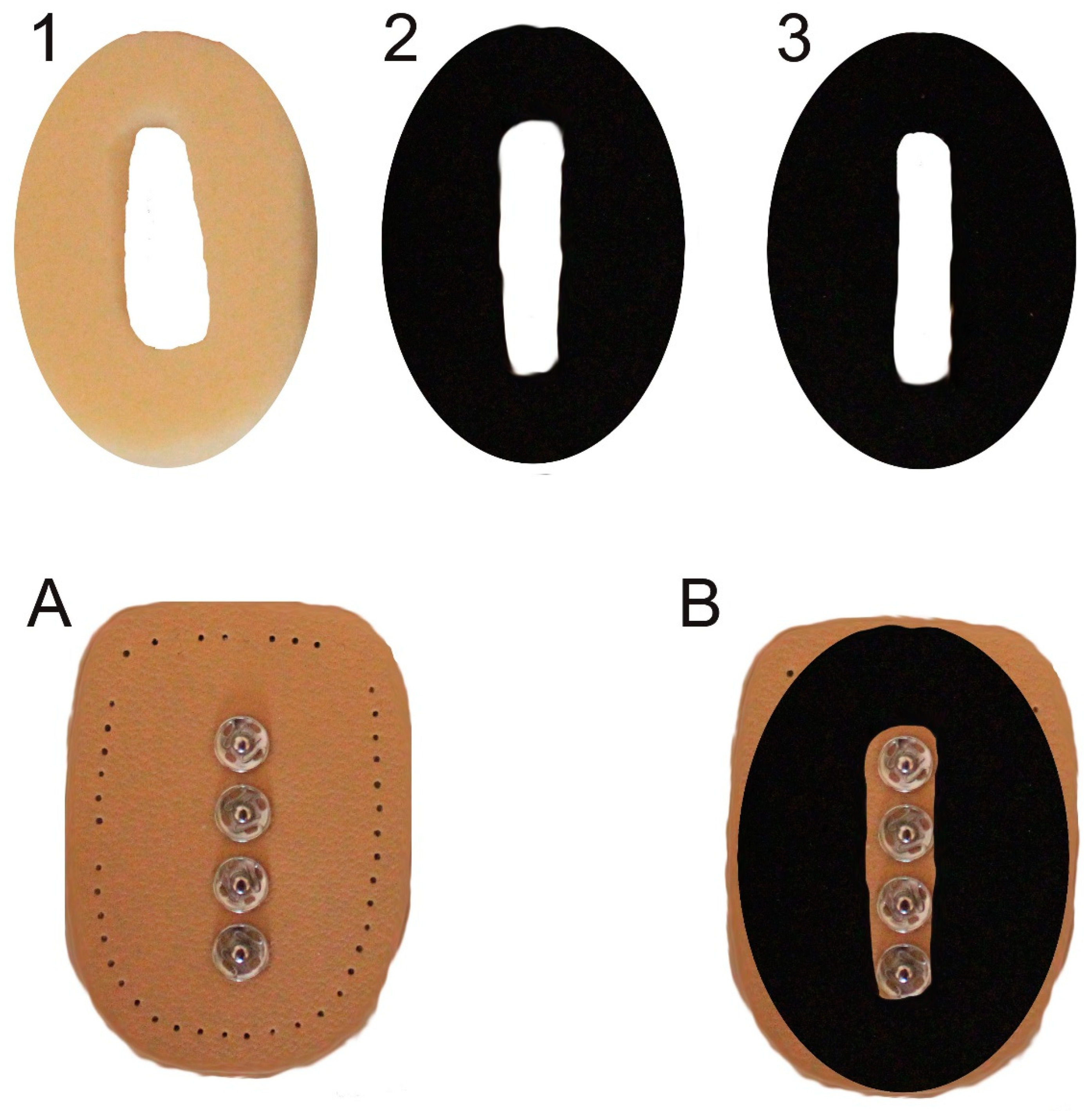
Figure 3.
This is a figure. Schemes follow the same formatting.
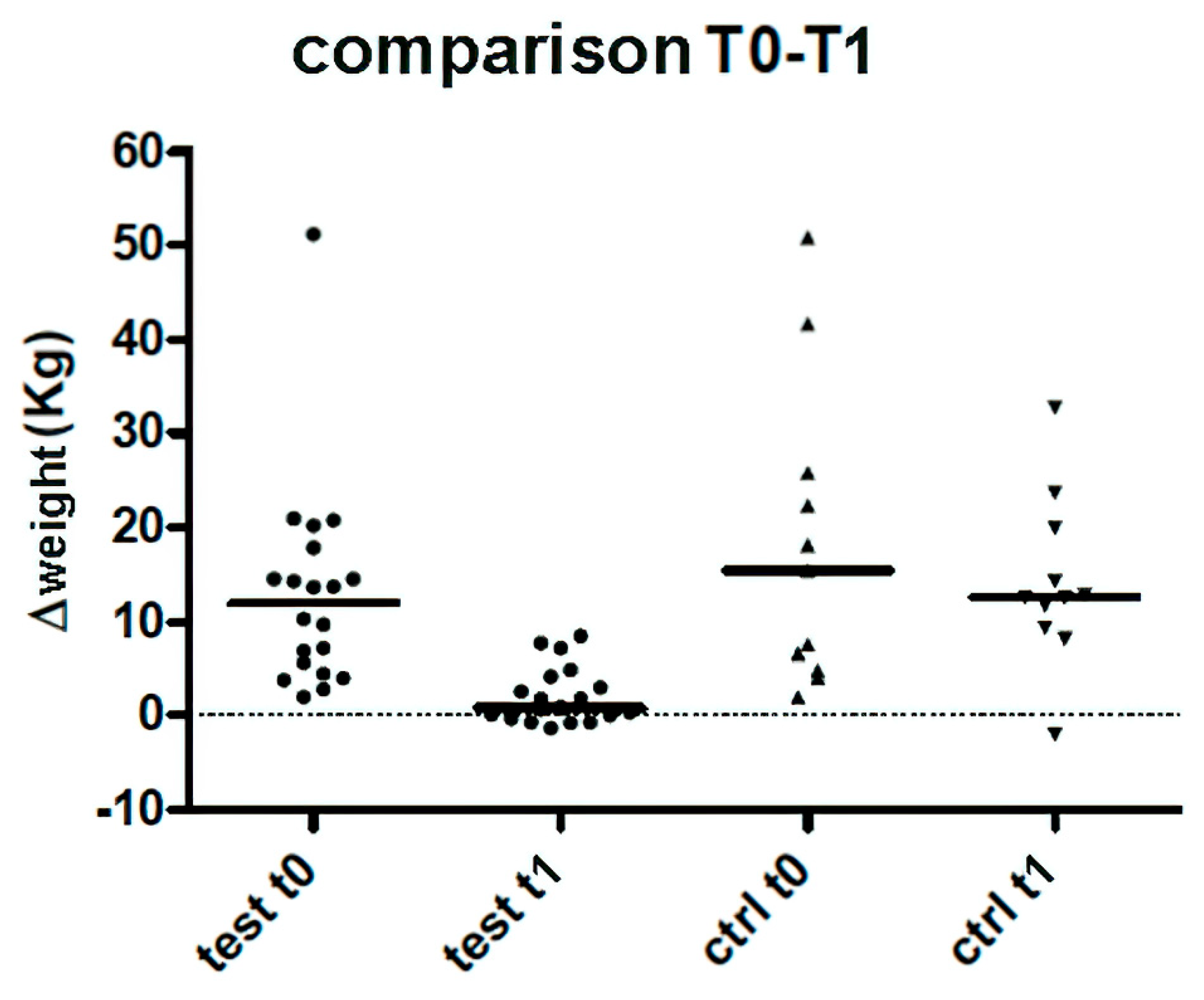

Table 1.
Summary tables of data obtained, cases treated, and control cases.
| TEST GROUP | Weight (Kg) | Δ loaded weight T0 | Δloaded weight T0 | Δ loaded weight T1 | NRS T0 | NRS T1 | 6MWT T0 | 6MWT T1 |
|---|---|---|---|---|---|---|---|---|
| Mean | 78 | 12,9 | 5,6 | 2 | 4,2 | 1,6 | 35,4 | 206,2 |
| Median | 78,5 | 12 | 5 | 0,8 | 4 | 1 | 0 | 220,8 |
| St. Dev. | 16,8 | 10,9 | 8,5 | 3 | 2,5 | 1,4 | 66,1 | 90,2 |
Table 2.
Summary tables of data obtained, cases treated, and control cases.
| CONTROL GROUP | Weight (Kg) | Δ loaded weight | Δ loaded weight T1 | NRS T0 | NRS T1 | 6MWT T0 | 6MWT T1 |
|---|---|---|---|---|---|---|---|
| Mean | 69,9 | 16,3 | 12,8 | 4,2 | 2 | 45,9 | 181,1 |
| Median | 61 | 15,4 | 12,6 | 4 | 1 | 0 | 219 |
| St. Dev. | 14,2 | 14,7 | 8,4 | 1,7 | 1,9 | 74,4 | 92,3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



