Submitted:
14 April 2025
Posted:
15 April 2025
You are already at the latest version
Abstract
Aortic stenosis (AS) is a prevalent valvular heart disease, especially among older adults, and is associated with high morbidity and mortality. Left ventricular mass (LVM) in-creases in response to pressure overload in AS. However, excessive LVM is associated with adverse outcomes. The prognostic implications of LVM, particularly potential sex-specific effects on mortality, remain unclear. We conducted a retrospective sin-gle-center cohort study of 531 outpatients with symptomatic but stable severe AS awaiting valve intervention between April 2020 and February 2024. None had prior valve procedures. Baseline clinical and echocardiographic data were collected, and pa-tients were followed for a mean of 2.67 years. The cohort included 283 men and 248 women (mean age 74.7 years). During follow-up, 165 patients (31.1%) died, with 86% of deaths due to cardiovascular causes. Deceased patients had lower left ventricular ejec-tion fraction (LVEF) and higher LVM index (LVMi) than survivors. Multivariate analysis showed that LVMi and atrial fibrillation (AF) were independent predictors of mortality. In women, LVMi, LVEF, and AF were independently associated with death, while no such predictors were identified in men. In conclusion, elevated LVMi was inde-pendently associated with increased mortality in patients with severe AS, particularly among women.
Keywords:
aortic valve stenosis
; left ventricular mass
; prognosis
; women
; men
1. Introduction
Patients with symptomatic severe aortic stenosis (AS) face a substantially poor quality of life and an elevated risk of mortality. While traditional clinical symptoms and echocardiographic parameters have been well-established as predictors of adverse outcomes [1-4], the prognostic significance of left ventricular mass (LVM) remains an area of ongoing investigation and debate. Increased LVM represents a maladaptive response to chronic pressure overload, which induces left ventricular hypertrophy, myocardial fibrosis, and compromised diastolic function [5,6]. These structural and functional alterations contribute to decreased cardiac output, heightened susceptibility to arrhythmias, and an increased risk of heart failure [7-10].
Numerous studies have reported a robust association between elevated LVM and poor clinical outcomes in patients with AS [11-12]. However, inconsistencies in the findings persist, with some studies demonstrating a significant correlation while others report a weaker or negligible association [13-14]. These discrepancies may be due to variations in study design, patient cohorts, and methodological approaches. Furthermore, the intricate relationship between LVM and other clinical or echocardiographic variables, such as age, hypertension, and coronary artery disease, complicates the interpretation of its role in disease progression and prognosis.
Gender also serves as a critical biological factor influencing the development and progression of cardiovascular diseases, including AS. Women with AS often present with distinct clinical profiles compared to men, characterized by older age and a higher prevalence of comorbid conditions such as hypertension and diabetes [15]. Moreover, the impact of LVM on cardiac function and clinical outcomes may vary between sexes due to sex-specific differences in myocardial structure, function, and pathophysiological responses. These gender-based differences underscore the need for tailored approaches in evaluating LVM and managing AS in women and men.
2. Materials and Methods
This single-center retrospective observational study included 531 outpatients diagnosed with symptomatic but stable severe AS between April 2020 and February 2024. The primary objective was to evaluate the impact of LVM on mortality in patients awaiting valve intervention. Inclusion criteria required patients to have symptomatic but stable severe AS while awaiting valve intervention. Exclusion criteria included a history of prior valve procedures and the need for urgent intervention due to clinical instability. The study began as our hospital prioritized COVID-19 patients, which disrupted care for individuals requiring elective procedures, including cardiac surgeries. To reduce risks, the hospital implemented cautious strategies for interventional procedures. Elective cardiac surgeries were deferred, with priority given to patients presenting with clinically unstable AS. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines.
The primary symptoms assessed were dyspnea, angina, and syncope. Dyspnea was classified according to the New York Heart Association (NYHA) functional classification, while angina was evaluated using the Canadian Cardiovascular Society (CCS) functional classification. Syncope was defined as a transient loss of consciousness followed by spontaneous recovery.
In addition to assessing clinical symptoms, the study examined the prevalence of persistent atrial fibrillation (AF) and several traditional cardiovascular risk factors, including hypertension, diabetes, dyslipidemia, smoking status, and anemia. Smokers were categorized as either current or non-smokers. Hypertension was defined as having a systolic blood pressure greater than 140 mmHg, a diastolic blood pressure above 90 mmHg, or using antihypertensive medication. Dyslipidemia was diagnosed in cases where the total cholesterol level was 240 mg/dL or higher, the triglyceride level was 150 mg/dL or more, the low-density lipoprotein (LDL) cholesterol level exceeded 130 mg/dL, or lipid-lowering therapy was in use. Diabetes was diagnosed based on fasting glucose levels of 126 mg/dL or greater, casual plasma glucose levels of 200 mg/dL or higher, or using hypoglycemic agents. Anemia was defined as a hemoglobin plasma concentration below 13.0 g/dL for men and 12.0 g/dL for women, based on the lower cut-off of our laboratory's normal reference values.
The diagnosis of severe AS was confirmed through a transthoracic echocardiogram conducted according to a standardized protocol at the study’s Echocardiography Core Laboratory. Several critical echocardiographic criteria determined the severity of AS: a mean transvalvular gradient of ≥40 mmHg, an aortic valve area (AVA) of ≤1.0 cm², or a peak aortic jet velocity of ≥4.0 meters per second. LVEF was calculated as the ratio of stroke volume to end-diastolic volume. LV volumes were determined using the biplane disc method, a modified version of Simpson’s rule. This method involves summing the volumes of small cylindrical discs to estimate the total LV volume.
The LVMi was calculated by dividing the LVM by the body surface area (BSA). LVM was derived using the following formula [16]:
LVM (grams) = 0.8 ∗ 1.04 ∗ {[(LV diastolic diameter + diastolic interventricular septal thickness + LV posterior wall thickness in diastole)3 – LV diastolic diameter3]} + 0.6
Reference values for LVMi were based on guidelines from the American Society of Echocardiography, which defined left ventricular hypertrophy as an LVMi greater than 95 g/m² for women and 115 g/m² for men [17].
The study assessed various valve interventions, including aortic valve replacement (AVR), valvuloplasty, and transcatheter aortic valve implantation (TAVI). As part of the follow-up protocol, we recorded whether each patient underwent any of these procedures during the study period, categorizing the variable "valve intervention" as either “yes” or “no.” Additionally, we evaluated the prevalence of coronary artery disease (CAD), defined as the presence of at least one major subepicardial coronary artery with a ≥70% stenotic lesion.
Statistical Analysis
Statistical analysis was conducted by expressing continuous variables as means with standard deviations and categorical variables as frequencies with corresponding percentages. The assumption of normality was assessed using tests for equality of variances. Continuous variables were compared between groups using Student’s t-test, while categorical variables were compared using the chi-square test. A p-value of less than 0.05 was considered statistically significant.
The cumulative incidence of all-cause mortality was estimated using the Kaplan–Meier (K-M) method, incorporating Šidák adjustments for multiple comparisons. LVMi was categorized into two strata: Stratum 1, which includes normal (43–95 g/m² for women and 49–115 g/m² for men) to mildly abnormal LVMi (96–108 g/m² for women and 116–131 g/m² for men), and Stratum 2, which includes moderate (109–121 g/m² for women and 132–148 g/m² for men) to severely abnormal LVMi (≥122 g/m² for women and ≥149 g/m² for men) [17].
Cox proportional hazard models were utilized to identify variables independently associated with all-cause mortality. The chi-square score statistic from the Cox model was used to identify the most significant predictors of mortality. The dependent variable in these models was death, with adjustments made for covariates exhibiting a p-value less than 0.1, including LVEF, LVMi, CAD, angina, AF, and valve interventions that included AVR, TAVI, or valvuloplasty. Separate Cox proportional hazard models were constructed for male and female patients, using the same covariates in each model. All statistical analyses were performed using the SAS® Studio software package (SAS Institute, Cary, NC, USA).
3. Results
The analysis included a cohort of 531 patients, with a mean age of 74.7 ± 11.6 years, of which 253 (53.3%) were male. Women exhibited a higher prevalence of dyslipidemia, hypertension, higher LVEF, moderate to severely abnormal LVMi, left ventricular (LV) gradient, and peak aortic jet velocity. Conversely, men had a higher prevalence of AF, larger BSA, higher LVMi, and a higher incidence of CAD (Table 1).
Survivors were more likely to have angina, higher LVEF, and to have undergone AVR or TAVI. In contrast, non-survivors had a higher prevalence of AF, elevated LVMi, and moderate to severely abnormal LVMi and were more likely to have undergone valvuloplasty (Table 2).
Among survivors, women had higher rates of hypertension, LVEF, moderate to severely abnormal LVMi, LV gradient, and peak aortic velocity. In contrast, men had a higher prevalence of syncope, AF, larger BSA, higher LVMi, and CAD. During the study period of 2.7 ± 1.2 years, 165 patients (31.1%) died, with 148 (90%) of these deaths attributed to cardiovascular disease, 79 (53.9%) in men and 69 (46.1%) in women. There were 17 non-cardiovascular deaths (10%), including 8 (47.1%) from COVID-19 (6 men, 2 women), 7 (41.2%) from cancer (2 men, 5 women), and 2 from sepsis (both in men). Among the non-survivors, women had higher rates of dyslipidemia, elevated LVEF, moderate to severely abnormal LVMi, higher LV gradient, peak aortic velocity, and lower valve area, while men demonstrated a higher prevalence of diabetes, larger BSA, larger aortic valve area, and CAD. Notably, women in the non-survivor group exhibited a significantly higher prevalence of moderate to severely abnormal LVMi compared to men. LVEF was nearly significantly higher in both surviving women (p = 0.056) and surviving men (p = 0.052) compared to non-surviving women and men, respectively (Table 3).
Kaplan–Meier survival analysis showed a higher cumulative incidence of death in patients with moderate to severely abnormal LVMi compared to patients with normal to slightly abnormal LVMi (stratum 1 vs. 2; p = 0.031) (Figure 1).
A cumulative incidence of death was also higher in women with moderate to severely abnormal LVMi compared to men with the same classification (stratum 4 vs. 2; p = 0.042). Additionally, women with moderate to severely abnormal LVMi had a significantly higher incidence of death compared to women with normal to slightly abnormal LVMi (stratum 4 vs. 3; p = 0.002) (Figure 2).
Cox multivariate analysis identified LVMi [HR = 1.39 (95% CI: 1.02–1.90); p = 0.032], AF [HR = 1.68 (95% CI: 1.02–2.74); p = 0.038], as independent predictors of mortality, and valve intervention [HR = 0.47 (95% CI: 0.37–0.61); p < 0.001] the only predictor of survival in the overall cohort.
In women, LVMi [HR = 2.52 (95% CI: 1.48–4.28); p = 0.001], AF [HR = 2.77 (95% CI: 1.18–6.50); p = 0.014], as independent predictors of mortality, and valve intervention [HR = 0.43 (95% CI: 0.30–0.63); p < 0.001] the significant predictor of survival. In men, after using the same covariates, less valve intervention [HR = 0.51 (95% CI: 0.37–0.71); p < 0.001] was the only predictor of death. Chi-square test scores revealed LVMi (4.6) as the strongest predictor of death in the overall cohort, followed by AF (4.3). Valve intervention was the only predictor for survivors (40.3). In women, LVMi (11.7) was the most robust predictor of death, followed by AF (6.0) and valve intervention (23.3) for survival. In men, valve intervention (23.3) was the only predictor for survival.
4. Discussion
Our study identified a strong, statistically significant correlation between LVMi and mortality in women with symptomatic severe AS, establishing LVMi as the most robust predictor of death in this group. These findings are consistent with previous research [18,19], including the PARTNER Trials and Registries [20], which showed that elevated LVMi is independently associated with all-cause and cardiovascular mortality, even after adjusting for various covariates. Similar to our results, previous studies also found that LVMi serves as an independent predictor of both all-cause and cardiovascular death in women but not in men [14,21,22].
LVMi is well-established as a prognostic marker, with higher values strongly linked to an increased risk of cardiovascular events in patients with AS. Elevated LVMi has been consistently shown to predict adverse outcomes, emphasizing its role as a critical indicator of prognosis in women with severe AS.
In our study, men exhibited overall higher LVMi values. However, when classified by sex-specific thresholds for moderate and severe LVMi, women showed a higher prevalence of elevated LVMi. This finding is consistent with previous studies [23-25]. Despite these observations, the differences in prognosis and optimal mortality predictors between women and men with symptomatic severe AS awaiting surgical intervention remain insufficiently explored.
It is understood that women with moderate to severe LVMi face a worse prognosis compared to men with similar LVMi levels. Several factors help explain this gender disparity. Women often exhibit more pronounced concentric remodeling and hypertrophy than men [26]. They tend to have a more concentric LV remodeling pattern with higher relative wall thickness and smaller LV dimensions. This pattern of concentric hypertrophy has a significantly greater impact on prognosis in women. Additionally, outcomes following AVR indicate that residual left ventricular hypertrophy (LVH) is linked to increased mortality. This link is considerably stronger in women, suggesting that they are more negatively affected by residual LVH than men [27]. Women may also develop a more intense form of concentric remodeling and hypertrophy in response to pressure overload. Compared to men, this condition results in a more significant reduction in LV cavity size, decreased LV compliance, impaired LV filling and pump function, and reduced stroke volume [28]. Women might be more prone to developing diffuse myocardial fibrosis, which can be detected by cardiac magnetic resonance imaging, regardless of the severity of AS [29].
There is ongoing debate regarding whether diffuse myocardial fibrosis is more prevalent in women, and the mechanisms behind sex-related differences in LV remodeling and fibrosis remain unclear [30-32]. A recent study on patients with severe AS undergoing AVR found that women had less replacement fibrosis compared to men. However, while women exhibited lower overall mortality than men, replacement fibrosis in both sexes was associated with LV decompensation and increased post-AVR mortality. These findings suggest that, despite the lower fibrosis in women, the extent of fibrosis remains a significant factor influencing mortality in both genders [33].
The mechanism behind sex differences in myocardial fibrosis remains unclear. Sex hormones, particularly estrogen and testosterone, influence fibrosis, with estrogen offering cardioprotection in women and testosterone promoting hypertrophy and fibrosis in men [34,35]. However, since most patients with AS are over 60, the role of estrogen in postmenopausal women is not fully understood [36]. The loss of estrogen after menopause could increase vulnerability to heightened LV wall stress, myocardial ischemia, LVM, and fibrosis, which tend to escalate with age in women but not in men [37,38].
Studies suggest that estrogen may downregulate the expression of collagen I and III genes in female but not male cardiac fibroblasts [39], thereby inhibiting fibroblast proliferation and reducing overall collagen protein synthesis [40]. Despite these findings, the precise role of estrogen in the fibrotic process for postmenopausal women with AS requires further exploration. The absence of estrogen might contribute to increased susceptibility to LV wall stress and ischemia in aging women, but this hypothesis warrants deeper investigation in future studies.
Moreover, various factors reduce coronary blood flow in patients with concentric LVH, including diminished perfusion pressure, external compressive forces, shortened diastolic perfusion time, and reduced microvascular density [41,42]. Elevated intracavitary pressure worsens these forces, increasing the risk of myocardial ischemia and related complications due to compromised perfusion.
These changes redirect blood flow from the endocardium to the epicardium, resulting in a significant reduction in subendocardial myocardial perfusion [43]. This reversal of the typical endocardial-to-epicardial blood flow gradient at rest is a key factor in AS pathophysiology, leading to subendocardial ischemia, cell death, and fibrosis. Our study also found that AF was an independent predictor of higher mortality, which aligns with established literature [44]. The link between AF and poor outcomes is well-documented. AF is recognized as a significant risk factor for mortality due to its association with complications like stroke and heart failure. The consistency of our findings with existing research underscores the crucial importance of monitoring and managing these factors to enhance patient outcomes.
This study has several limitations. As a single-center retrospective observational analysis, its generalizability is limited to other settings with different patient demographics, clinical practices, and treatment protocols. While the findings offer valuable insights, they require validation through larger, multicenter, randomized studies to ensure broader applicability. Additionally, echocardiography, commonly used to measure LVMi in aortic valve stenosis patients, is less accurate than advanced imaging techniques like magnetic resonance imaging or computed tomography, potentially introducing measurement variability. Furthermore, key clinical data, such as pulmonary artery systolic pressure, were not consistently available, potentially limiting the comprehensive assessment of patients' cardiovascular profiles. Additionally, no invasive or non-invasive evaluations of microvascular dysfunction were performed in the cohort to assess ischemia with or without obstructive coronary disease.
Lastly, as this was an observational study, potential residual confounding factors cannot be entirely ruled out, despite our adjustment for relevant variables.
Despite these limitations, the robustness of the study’s findings is reinforced by the analysis of a large, consecutive series of patients undergoing the same procedure, which reduces variability and highlights consistent patterns in outcomes.
5. Conclusions
Cox multivariate analysis revealed that LVMi and AF are independent predictors of mortality. Notably, in women, LVMi, AF, and less valve intervention were significantly associated with an increased risk of death. In contrast, less valve intervention was an independent predictor of mortality identified in men. These findings indicate that elevated LVMi serves as a critical predictor of mortality, particularly in the female population, highlighting the necessity for targeted interventions to address this demographic's unique risks. Further randomized studies are essential to validate these results and explore potential therapeutic strategies.
Author contributions statement: Conceptualization, S.D.A., A.P.M.; Methodology, S.D.A., F.T., and A.P.M.; Validation, S.D.A., F.T., and A.P.M.; Formal Analysis, S.D.A., F.T., and A.P.M.; Investigation, S.D.A., A.P.M.; Resources, S.D.A., F.T., and A.P.M.; Data Curation, S.D.A., A.P.M.; Writing – Original Draft Preparation, S.D.A., F.T., and A.P.M.; Writing – Review & Editing, S.D.A., A.P.M.; Project Administration, A.P.M.
Funding
The author(s) received no financial support for this article's research, authorship, and/or publication.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki and was approved by the Ethics Committee of Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (CAAE: 54349521.4.0000.0068) on January 21, 2022, with the need for written informed consent waived.
Informed consent: the need for written informed consent was waived.
Data Availability Statement
The raw data in this article will be made available upon reasonable request to the corresponding author.
Acknowledgements
None.
Conflicting interests
The author(s) declared no potential conflicts concerning this article's research, authorship, and/or publication.
Abbreviations
The following abbreviations are used in this manuscript:
| AS | Aortic stenosis |
| LVM | Left ventricular mass |
| LVMi | Left ventricular mass index |
| LVEF | Left ventricular ejection fraction |
| AF | Atrial fibrillation |
| AVA | Aortic valve area |
| LVH | Left ventricular hypertrophy |
| AVR | Aortic valve replacement |
| TAVI | Transcatheter aortic valve implantation |
| CAD | Coronary artery disease |
| PASP | Pulmonary artery systolic pressure |
References
- Otto CM, Burwash IG, Legget ME, et al. Prospective study of asymptomatic valvular aortic stenosis. Clinical, echocardiographic, and exercise predictors of outcome. Circulation 1997;95:2262-2270. [CrossRef]
- Rosenhek R, Binder T, Porenta G, et al. Predictors of outcome in severe, asymptomatic aortic stenosis. N Engl J Med 2000;343:611-617.
- Pellikka PA, Sarano ME, Nishimura RA, et al. Outcome of 622 adults with asymptomatic, hemodynamically significant aortic stenosis during prolonged follow-up. Circulation 2005;111:3290-3295. [CrossRef]
- Avakian SD, Grinberg M, Ramires JA, Mansur AP. Outcome of adults with asymptomatic severe aortic stenosis. Int J Cardiol 2008;123:322-327. [CrossRef]
- Bing R, Cavalcante JL, Everett RJ, et al. Imaging and impact of myocardial fibrosis in aortic stenosis. JACC Cardiovasc Imaging 2019;12:283-296. [CrossRef]
- Dweck MR, Boon NA, Newby DE. Calcific aortic stenosis: a disease of the valve and the myocardium. J Am Coll Cardiol 2012;60:1854-1863.
- De Biase N, Mazzola M, Del Punta L, et al. Haemodynamic and metabolic phenotyping of patients with aortic stenosis and preserved ejection fraction: A specific phenotype of heart failure with preserved ejection fraction? Eur J Heart Fail 2023;25:1947-1958.
- Azevedo CF, Nigri M, Higuchi ML, et al. Prognostic significance of myocardial fibrosis quantification by histopathology and magnetic resonance imaging in patients with severe aortic valve disease. J Am Coll Cardiol 2010;56:278-287. [CrossRef]
- Cioffi G, Faggiano P, Vizzardi E, et al. Prognostic effect of inappropriately high left ventricular mass in asymptomatic severe aortic stenosis. Heart 2011;97:301-307. [CrossRef]
- Stassen J, Ewe SH, Hirasawa K, et al. Left ventricular remodelling patterns in patients with moderate aortic stenosis. Eur Heart J Cardiovasc Imaging 2022;23:1326-1335. [CrossRef]
- Lorell BH, Carabello BA. Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation 2000;102:470-479.
- Duncan AI, Lowe BS, Garcia MJ, et al. Influence of concentric left ventricular remodeling on early mortality after aortic valve replacement. Ann Thorac Surg 2008;85:2030-2039. [CrossRef]
- Burchfield JS, Xie M, Hill JA. Pathological ventricular remodeling: mechanisms: part 1 of 2. Circulation 2013;128:388-400.
- Minamino-Muta E, Kato T, Morimoto T, et al. Impact of the left ventricular mass index on the outcomes of severe aortic stenosis. Heart 2017;103:1992-1999. [CrossRef]
- DesJardin JT, Chikwe J, Hahn RT, et al. Sex Differences and Similarities in Valvular Heart Disease. Circ Res 2022;130:455-473. [CrossRef]
- Devereux RB, Alonso DR, Lutas EM, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 1986;57:450-8. [CrossRef]
- Lang RM, Biering M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005;18:1440-1463.
- Fuster RG, Argudo JA, Albarova OG, et al. Left ventricular mass index in aortic valve surgery: a new index for early valve replacement? Eur J Cardiothorac Surg 2003;23:696-702.
- Stassen J, Pio SM, Ewe SH, et al. Sex-Related Differences in Medically Treated Moderate Aortic Stenosis. Struct Heart 2022;6:100042. [CrossRef]
- Gonzales H, Douglas PS, Pibarot P, et al. Left Ventricular Hypertrophy and Clinical Outcomes Over 5 Years After TAVR: An Analysis of the PARTNER Trials and Registries. JACC Cardiovasc Interv 2020;13:1329-1339.
- Rader F, Sachdev E, Arsanjani R, Siegel RJ. Left ventricular hypertrophy in valvular aortic stenosis: mechanisms and clinical implications. Am J Med 2015;128:344-352. [CrossRef]
- Gerdts E, Rossebø AB, Pedersen TR, et al. Relation of Left Ventricular Mass to Prognosis in Initially Asymptomatic Mild to Moderate Aortic Valve Stenosis. Circ Cardiovasc Imaging 2015;8:e003644. [CrossRef]
- Douglas PS, Otto CM, Mickel MC, et al. Gender differences in left ventricle geometry and function in patients undergoing balloon dilatation of the aortic valve for isolated aortic stenosis. NHLBI Balloon Valvuloplasty Registry. Br Heart J 1995;73:548-554. [CrossRef]
- Pighi M, Piazza N, Martucci G, et al. Sex-Specific Determinants of Outcomes After Transcatheter Aortic Valve Replacement. Circ Cardiovasc Qual Outcomes 2019;12:e005363.
- Singh A, Musa TA, Treibel TA, et al. Sex differences in left ventricular remodelling, myocardial fibrosis and mortality after aortic valve replacement. Heart 2019;105:1818-1824. [CrossRef]
- Capoulade R, Clavel MA, Le Ven F, et al. Impact of left ventricular remodelling patterns on outcomes in patients with aortic stenosis. Eur Heart J Cardiovasc Imaging 2017;18:1378-1387. [CrossRef]
- Gavina C, Falcao-Pires I, Pinho P, et al. Relevance of residual left ventricular hypertrophy after surgery for isolated aortic stenosis. Eur J Cardiothorac Surg 2016;49:952–959. [CrossRef]
- Hachicha Z, Dumesnil JG, Bogaty P, Pibarot P. Paradoxical low-flow, low-gradient severe aortic stenosis despite preserved ejection fraction is associated with higher afterload and reduced survival. Circulation 2007;115:2856–2864. [CrossRef]
- Tastet L, Kwiecinski J, Pibarot P, et al. Sex-Related Differences in the Extent of Myocardial Fibrosis in Patients With Aortic Valve Stenosis. JACC Cardiovasc Imaging 2020;13:699-711. [CrossRef]
- Kararigas G, Dworatzek E, Petrov G, et al. Sex dependent regulation of fibrosis and inflammation in human left ventricular remodelling under pressure overload. Eur J Heart Fail 2014;16:1160–1167. [CrossRef]
- Naoum C, Blanke P, Dvir D, et al. Clinical Outcomes and Imaging Findings in Women Undergoing TAVR. JACC Cardiovasc Imaging 2016;9:483-493. [CrossRef]
- Treibel TA, Kozor R, Fontana M, et al. Sex Dimorphism in the Myocardial Response to Aortic Stenosis. JACC Cardiovasc Imaging 2018;11:962-973. [CrossRef]
- Kwak S, Singh A, Everett RJ, et al. Sex-Specific Association of Myocardial Fibrosis With Mortality in Patients With Aortic Stenosis. JAMA Cardiol 2025;19:e245593. [CrossRef]
- Zwadlo C, Schmidtmann E, Szaroszyk M, et al. Antiandrogenic therapy with finasteride attenuates cardiac hypertrophy and left ventricular dysfunction. Circulation 2015;131:1071-1081. [CrossRef]
- Chehab O, Shabani M, Varadarajan V, et al. Endogenous sex hormone levels and myocardial fibrosis in men and postmenopausal women. JACC Adv 2023;2:100320. [CrossRef]
- Greiten LE, Holditch SJ, Arunachalam SP, Miller VM. Should there be sex-specific criteria for the diagnosis and treatment of heart failure? J Cardiovasc Transl Res 2014;7:139-155.
- Shub C, Klein AL, Zachariah PK, et al. Determination of left ventricular mass by echocardiography in a normal population: effect of age and sex in addition to body size. Mayo Clin Proc 1994;69:205-211. [CrossRef]
- Sickinghe AA, Korporaal SJA, den Ruijter HM, Kessler EL. Estrogen contributions to microvascular dysfunction evolving to heart failure with preserved ejection fraction. Front Endocrinol (Lausanne) 2019;10:442. [CrossRef]
- Petrov G, Regitz-Zagrosek V, Lehmkuhl E, et al. Regression of myocardial hypertrophy after aortic valve replacement: faster in women? Circulation 2010;122(11 Suppl):S23-S28.
- Zhou L, Shao Y, Huang Y, Yao T, Lu LM. 17-Estradiol inhibits angiotensin II-induced collagen synthesis of cultured rat cardiac fibroblasts via modulating angiotensin II receptors. Eur J Pharmacol 2007;567:186 –192. [CrossRef]
- Michail M, Davies JE, Cameron JD, et al. Pathophysiological coronary and microcirculatory flow alterations in aortic stenosis. Nat Rev Cardiol 2018;15:420-431. [CrossRef]
- McConkey HZR, Marber M, Chiribiri A, et al. Coronary Microcirculation in Aortic Stenosis. Circ Cardiovasc Interv 2019;12:e007547. [CrossRef]
- Reynolds HR, Bairey Merz CN, Berry C, et al. Coronary Arterial Function and Disease in Women With No Obstructive Coronary Arteries. Circ Res 2022;130:529-551. [CrossRef]
- Oguz D, Huntley GD, El-Am EA, et al. Impact of atrial fibrillation on outcomes in asymptomatic severe aortic stenosis: a propensity-matched analysis. Front Cardiovasc Med 2023;10:1195123. [CrossRef]
Figure 1.
Kaplan-Meier curves showing the risk of death by left ventricular mass index (LVMi) in symptomatic severe aortic stenosis.
Figure 1.
Kaplan-Meier curves showing the risk of death by left ventricular mass index (LVMi) in symptomatic severe aortic stenosis.
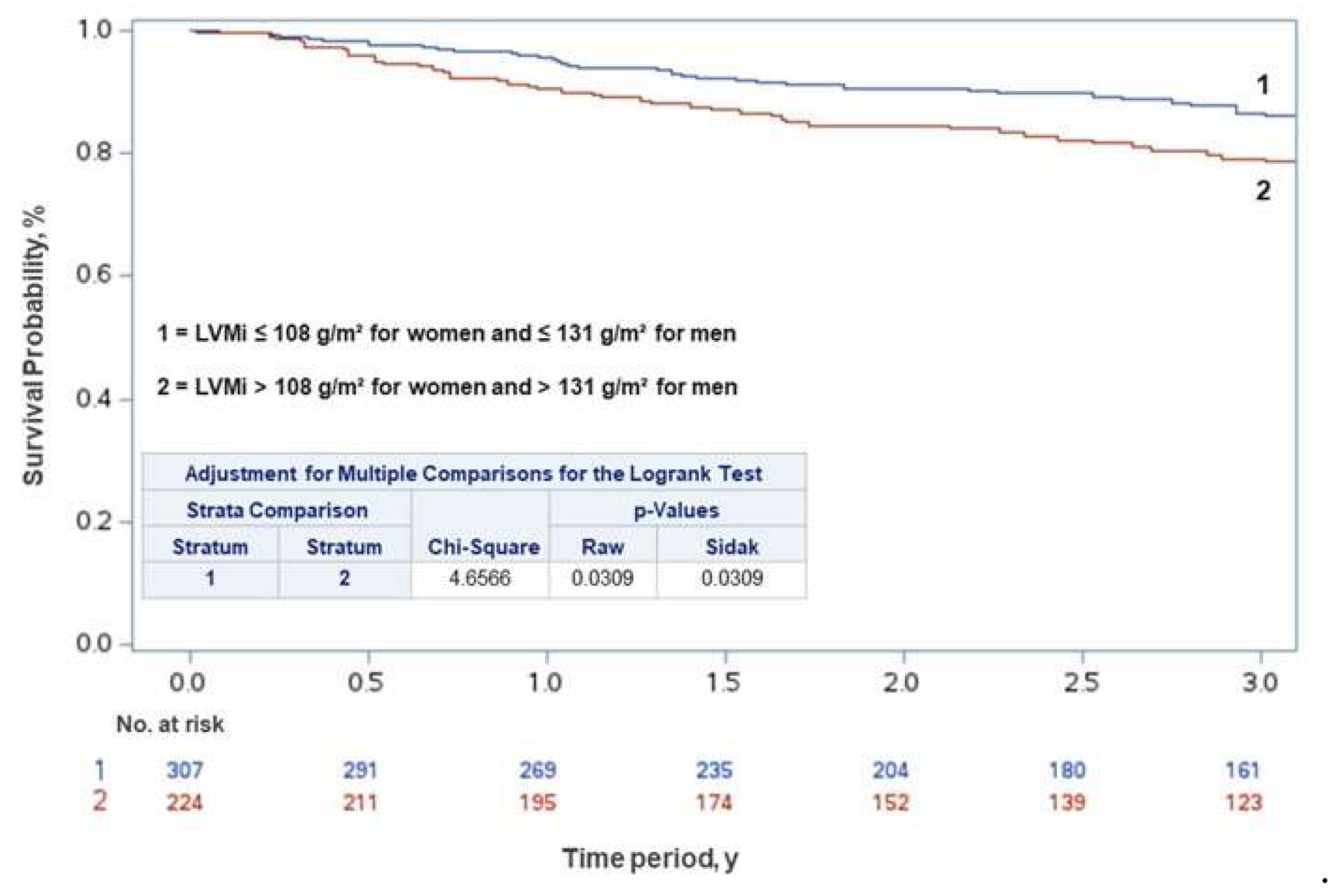
Figure 2.
Kaplan-Meier curves showing risk of death based on left ventricular mass index (LVMi) in women and men with symptomatic severe aortic stenosis.
Figure 2.
Kaplan-Meier curves showing risk of death based on left ventricular mass index (LVMi) in women and men with symptomatic severe aortic stenosis.
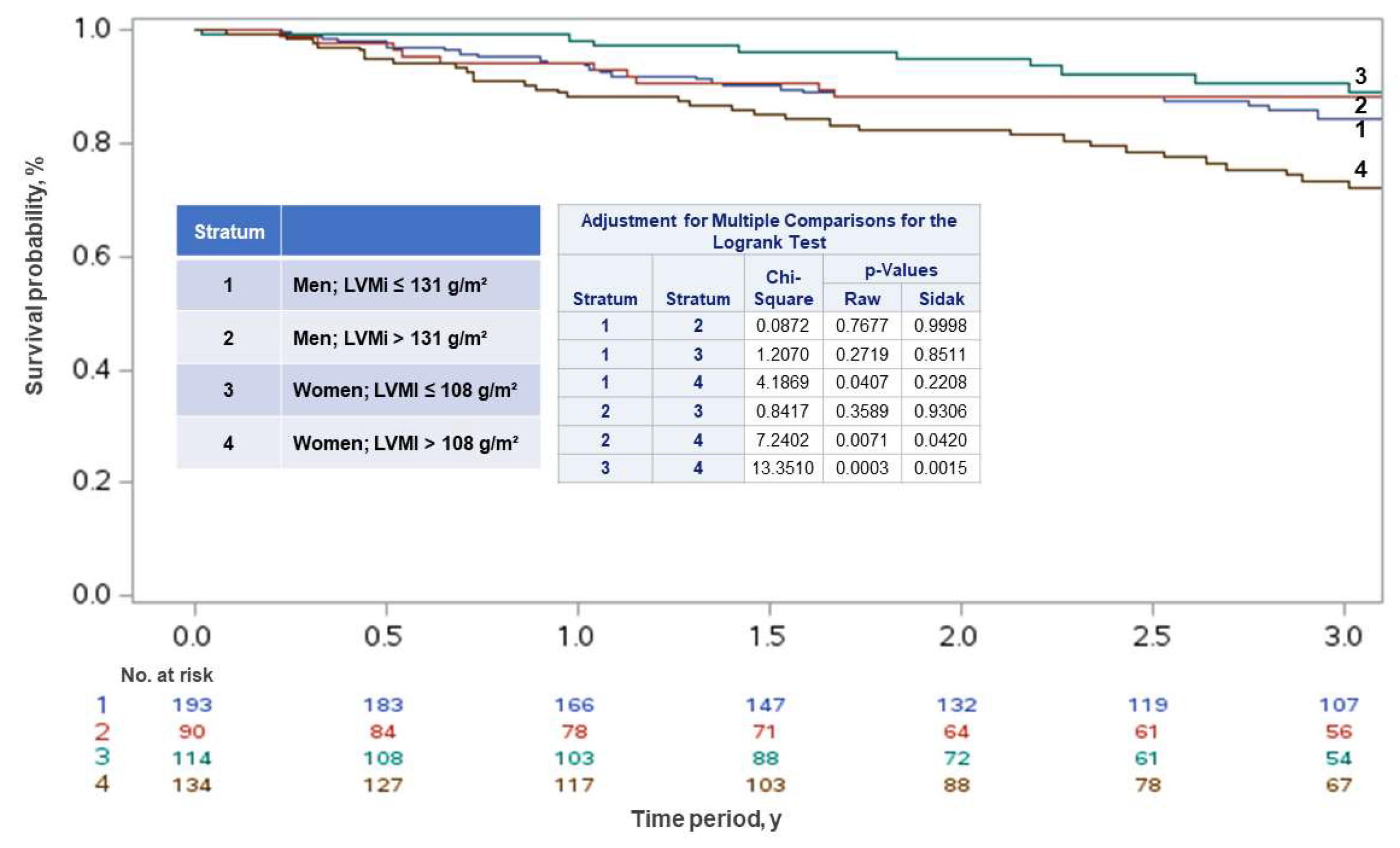

Table 1.
Clinical characteristics, echocardiographic data, and surgical interventions of all patients, women, and men with symptomatic severe aortic valve stenosis.
Table 1.
Clinical characteristics, echocardiographic data, and surgical interventions of all patients, women, and men with symptomatic severe aortic valve stenosis.
| All patients N=531 (%) |
Men N=283 (53.3) |
Women N=248 (46.7) |
p | |
| Age, mean (SD), y | 74.7 (11.6) | 74.1 (12.6) | 75.5 (10.2) | 0.149 |
| Time since baseline, mean (SD), y | 2.7 (1.2) | 2.8 (1.3) | 2.6 (1.2) | 0.138 |
| Dyslipidemia, No. (%) | 177 (33.3) | 81 (28.6) | 96 (38.7) | 0.014 |
| Hypertension, No. (%) | 390 (73.6) | 192 (68.1) | 198 (79.8) | 0.002 |
| Diabetes, No. (%) | 153 (28.8) | 85 (30.0) | 68 (27.4) | 0.507 |
| Smoking, No. (%) | 43 (8.1) | 23 (8.1) | 20 (8.1) | 0.979 |
| Anemia, No. (%) | 145 (27.3) | 81 (28.6) | 64 (25.8) | 0.468 |
| Syncope, No. (%) | 46 (8.7) | 32 (11.3) | 14 (5.7) | 0.021 |
| Angina, No. (%) | 197 (37.1) | 112 (39.6) | 85 (34.3) | 0.207 |
| Dyspnea, No. (%) | 475 (89.5) | 247 (87.3) | 228 (91.9) | 0.081 |
| AF, No. (%) | 33 (6.2) | 24 (8.5) | 9 (3.6) | 0.021 |
| Weight, mean (SD), Kg | 74.3 (14.3) | 79.1 (13.0) | 68.6 (13.6) | <0.001 |
| BSA, mean (SD), m2 | 1.8 (0.2) | 1.9 (0.2) | 1.7 (0.2) | <0.001 |
| LVEF, mean (SD), % | 60.6 (9.6) | 58.7 (10.7) | 62.8 (7.6) | <0.001 |
| LVMi, mean (SD), g/m2 | 118.6 (30.6) | 122.1 (29.9) | 114.5 (30.9) | 0.004 |
| LVMi moderate+severe | 224 (42.2) | 90 (31.8) | 134 (54.0) | <0.001 |
| LA Volume, mean (SD), ml | 44.9 (15.2) | 45.3 (14.5) | 44.5 (16.0) | 0.666 |
| Peak Gradient, mean (SD), mmHg | 79.8 (22.9) | 76.9 (21.4) | 83.1 (24.2) | 0.002 |
| Mean Gradient, mean (SD), mmHg | 50.5 (15.6) | 48.6 (14.7) | 52.6 (16.3) | 0.003 |
| Valve area, mean (SD), cm2 | 0.87 (2.42) | 1.0 (3.3) | 0.72 (0.19) | 0.155 |
| Peak Jet velocity, mean (SD), m/s | 4.4 (0.6) | 4.3 (0.6) | 4.5 (0.6) | 0.002 |
| Bicuspid / Tricuspid, No. (%) | 54 (10.2) / 477 (89.8) | 30 (10.6) / 253 (89.4) | 24 (9.68) / 224 (90.3) | 0.725 |
| CAD, No. (%) | 279 (52.5) | 172 (60.78) | 107 (43.2) | <0.001 |
| AVR, No. (%) | 162 (30.5) | 91 (32.2) | 71 (28.6) | 0.378 |
| Valvuloplasty, No. (%) | 13 (2.45) | 10 (3.5) | 3 (1.21) | 0.084 |
| TAVI, No. (%) | 98 (18.5) | 46 (16.3) | 52 (20.97) | 0.163 |
| Death, No. (%) | 165 (31.1) | 89 (31.5) | 76 (30.7) | 0.842 |
| Cardiovascular death, No. (%) | 148 (27.9) | 79 (27.9) | 69 (27.8) | 0.921 |
Abbreviations: AF, atrial fibrillation; AVR, aortic valve replacement; BSA, body surface area; CAD, coronary artery disease; LA, left atrial; LVEF, left ventricular ejection fraction; LVMi, left ventricular mass index; PASP, pulmonary artery systolic pressure; TAVI, transcatheter aortic valve implantation.
Table 2.
Clinical characteristics, echocardiographic data, and surgical interventions in patients with symptomatic severe aortic valve stenosis: a comparative analysis of survivors and non-survivors.
Table 2.
Clinical characteristics, echocardiographic data, and surgical interventions in patients with symptomatic severe aortic valve stenosis: a comparative analysis of survivors and non-survivors.
| All patients N=531 (%) |
Survivors N=366 (68.9) |
Non-Survivors N=165 (31.1) |
p | |
| Age, mean (SD), y | 74.7 (11.6) | 74.4 (11.3) | 75.5 (12.1) | 0.133 |
| Female, No. (%) | 366 (68.9) | 172 (47.0) | 76 (46.1) | 0.841 |
| Time since baseline, mean (SD), y | 2.7 (1.2) | 2.73 (1.2) | 2.55 (1.3) | 0.146 |
| Dyslipidemia, No. (%) | 177 (33.3) | 124 (33.4) | 53 (32.1) | 0.691 |
| Hypertension, No. (%) | 390 (73.6) | 270 (73.8) | 120 (73.2) | 0.885 |
| Diabetes, No. (%) | 153 (28.8) | 101 (27.6) | 52 (31.5) | 0.356 |
| Smoking, No. (%) | 43 (8.1) | 26 (7.1) | 17 (10.3) | 0.211 |
| Anemia, No. (%) | 145 (27.3) | 96 (26.2) | 49 (29.7) | 0.410 |
| Syncope, No. (%) | 46 (8.7) | 35 (9.6) | 11 (6.7) | 0.272 |
| Angina, No. (%) | 197 (37.1) | 146 (39.9) | 51 (30.9) | 0.047 |
| Dyspnea, No. (%) | 475 (89.5) | 325 (88.8) | 150 (90.9) | 0.463 |
| AF, No. (%) | 33 (6.2) | 15 (4.1) | 18 (10.9) | 0.003 |
| Weight, mean (SD), Kg | 74.3 (14.3) | 74.7 (14.2) | 73.4 (14.6) | 0.334 |
| BSA, mean (SD), m2 | 1.8 (0.21) | 1.8 (0.2) | 1.7 (0.2) | 0.205 |
| LVEF, mean (SD), % | 60.6 (9.6) | 61.4 (8.9) | 58.8 (10.8) | 0.008 |
| LVMi, mean (SD), g/m2 | 118.6 (30.6) | 115.5 (29.3) | 125.3 (32.5) | <0.001 |
| LVMi moderate+severe | 224 (42.2) | 136 (37.2) | 88 (53.3) | <0.001 |
| LA Volume, mean (SD), ml | 44.9 (15.2) | 44.4 (16.1) | 46.3 (12.8) | 0.246 |
| Peak Gradient, mean (SD), mmHg | 79.8 (22.9) | 80.4 (23.3) | 78.4 (22.0) | 0.365 |
| Mean Gradient, mean (SD), mmHg | 50.5 (15.6) | 50.6 (15.7) | 50.4 (15.3) | 0.894 |
| Valve area, mean (SD), cm2 | 0.87 (2.42) | 0.9 (2.9) | 0.7 (0.2) | 0.258 |
| Peak Jet velocity, mean (SD), m/s | 4.4 (0.6) | 4.4 (0.6) | 4.4 (0.6) | 0.359 |
| Bicuspid / Tricuspid, No. (%) | 54 (10.2) / 477 (89.8) | 42 (11.5) / 324 (88.5) | 12 (7.2) / 153 (92.7) | 0.138 |
| CAD, No. (%) | 279 (52.5) | 183 (50.0) | 96 (58.1) | 0.081 |
| AVR, No. (%) | 162 (30.5) | 142 (38.8) | 20 (12.1) | <0.001 |
| Valvuloplasty, No. (%) | 13 (2.45) | 5 (1.37) | 8 (4.9) | 0.016 |
| TAVI, No. (%) | 98 (18.5) | 85 (23.2) | 13 (7.9) | <0.001 |
Abbreviations: AF, atrial fibrillation; AVR, aortic valve replacement; BSA, body surface area; CAD, coronary artery disease; LA, left atrial; LVEF, left ventricular ejection fraction; LVMi, left ventricular mass index; PASP, pulmonary artery systolic pressure; TAVI, transcatheter aortic valve implantation.
Table 3.
Clinical characteristics, echocardiographic data, and surgical interventions in women and men with symptomatic severe aortic valve stenosis: a comparative analysis of survivors and non-survivors.
Table 3.
Clinical characteristics, echocardiographic data, and surgical interventions in women and men with symptomatic severe aortic valve stenosis: a comparative analysis of survivors and non-survivors.
| Survivors | p | Non-Survivors | p | |||
| Men N=194 (53) |
Women N=172 (47) |
Men N=89 (53.9) |
Women N=76 (46.1) |
|||
| Age, mean (SD), y | 75.1 (10.5) | 75.1 (10.8) | 0.792 | 73.9 (15.0) | 73.0 (11.2) | 0.650 |
| Time since baseline, mean (SD), y | 2.8 (1.2) | 2.7 (1.1) | 0.284 | 2.7 (1.4) | 2.4 (1.3) | 0.289 |
| Dyslipidemia, No. (%) | 59 (30.4) | 65 (37.8) | 0.137 | 22 (24.7) | 31 (40.8) | 0.028 |
| Hypertension, No. (%) | 127 (65.5) | 143 (83.1) | <0.001 | 65 (73.9) | 55 (72.4) | 0.829 |
| Diabetes, No. (%) | 50 (25.8) | 51 (29.7) | 0.408 | 35 (39.3) | 17 (22.4) | 0.019 |
| Smoking, No. (%) | 16 (8.3) | 10 (5.8) | 0.366 | 7 (7.9) | 10 (13.2) | 0.265 |
| Anemia, No. (%) | 52 (26.8) | 44 (25.6) | 0.791 | 29 (32.6) | 20 (26.3) | 0.380 |
| Syncope, No. (%) | 25 (12.9) | 10 (5.8) | 0.022 | 7 (7.9) | 4 (5.3) | 0.506 |
| Angina, No. (%) | 86 (44.3) | 60 (34.8) | 0.066 | 26 (29.2) | 25 (32.9) | 0.610 |
| Dyspnea, No. (%) | 169 (87.1) | 156 (90.7) | 0.279 | 78 (87.6) | 72 (94.7) | 0.114 |
| AF, No. (%) | 12 (6.19) | 3 (1.74) | 0.032 | 12 (13.5) | 6 (7.9) | 0.251 |
| Weight, mean (SD), Kg | 79.7 (12.6) | 69.0 (13.7) | <0.001 | 27.9 (13.9) | 67.6 (13.5) | <0.001 |
| BSA, mean (SD), m2 | 1.9 (0.2) | 1.7 (0.2) | <0.001 | 1.9 (0.2) | 1.7 (0.2) | <0.001 |
| LVEF, mean (SD), % | 59.6 (9.7) | 63.4 (6.9) | <0.001 | 56.7 (12.0) | 61.3 (8.7) | 0.006 |
| LVMi, mean (SD), g/m2 | 120.3 (29.1) | 110.1 (28.5) | <0.001 | 125.9 (31.5) | 124.5 (33.8)a | 0.784 |
| LVMi moderate+severe | 60 (30.9) | 76 (44.2) | 0.009 | 30 (33.7) | 58 (76.3)a | <0.001 |
| LA Volume, mean (SD), ml | 44.8 (15.4) | 43.8 (16.9) | 0.619 | 46.6 (12.2) | 46.3 (13.7) | 0.995 |
| Peak Gradient, mean (SD), mmHg | 77.6 (20.5) | 83.6 (25.8) | 0.015 | 75.4 (23.1) | 82.0 (20.2) | 0.057 |
| Mean Gradient, mean (SD), mmHg | 48.9 (14.0) | 52.5 (17.3) | 0.030 | 48.1 (16.1) | 53.1 (13.9) | 0.038 |
| Valve area, mean (SD), cm2 | 1.1 (4.0) | 0.7 (0.2) | 0.200 | 0.8 (1.2) | 0.7 (0.2) | <0.001 |
| Peak Jet velocity, mean (SD), m/s | 4.4 (0.6) | 4.5 (0.7) | 0.023 | 4.3 (0.7) | 4.5 (0.6) | 0.039 |
| Bicuspid / Tricuspid, No. (%) | 23 (11.9)/171 (88.1) | 19 (11.1)/153 (88.9) | 0.809 | 7 (7.9)/82 (92.1) | 5 (6.6)/71 (93.4) | 0.751 |
| CAD, No. (%) | 114 (58.8) | 69 (40.1) | <0.001 | 58 (65.2) | 38 (50) | 0.049 |
| AVR, No. (%) | 82 (42.3) | 60 (34.9) | 0.148 | 9 (10.1) | 11 (14.5) | 0.392 |
| Valvuloplasty, No. (%) | 4 (2.1) | 1 (0.6) | 0.223 | 6 (6.7) | 2 (2.6) | 0.220 |
| TAVI, No. (%) | 38 (19.6) | 47 (27.3) | 0.081 | 8 (9.0) | 5 (6.6) | 0.567 |
ap<0.001, Survivors (women) vs. Non-Survivors (women). Abbreviations: AF, atrial fibrillation; AVR, aortic valve replacement; BSA, body surface area; CAD, coronary artery disease; LA, left atrial; LVEF, left ventricular ejection fraction; LVMi, left ventricular mass index; PASP, pulmonary artery systolic pressure; TAVI, transcatheter aortic valve implantation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



