
Submitted:
13 April 2025
Posted:
14 April 2025
You are already at the latest version
Abstract
Teleoperated robotic systems for robot-assisted minimally invasive surgery (RAMIS) have gained widespread clinical acceptance, making it the first domain in medical robotics to achieve global adoption. Despite its relative success, with limited market penetration, the reliance on human control in this approach ensures that the surgeon remains accountable for the clinical outcomes achieved by the robot. However, there is a growing demand for improved surgical performance, traceability, and safety that surpasses human capabilities, leading to a need for advancements in telesurgical robotics. Challenges such as technical complexity and financial constraints have hindered the full realization of telesurgical robotics' potential. While the da Vinci surgical system dominates the market, there are over 60 emerging RAMIS robot types, with 15 already obtaining regulatory clearance. This review article aims to bridge technological advancements with commercialization principles, particularly focusing on engineering components that can significantly enhance clinical practice. Current RAMIS robots primarily rely on their mechatronics capabilities, lacking data-driven assistance and intelligent human-machine collaboration. However, emerging RAMIS systems are integrating computer assistance, offering enhanced manipulation capabilities, refined sensors, advanced vision, task-level automation, smart safety features, and data integration. This heralds a new era in telesurgical robotics, infused with machine learning (ML) and artificial intelligence (AI) solutions. Robust AI algorithms necessitate high-quality data acquired and shared in real time, enabling ML-based solutions. This review explores historical and future perspectives of emerging RAMIS technologies, considering their potential impact on the field. This article serves as a comprehensive review, examining the latest developments in robot-assisted minimally invasive surgery. It offers an in-depth exploration of key emerging technologies associated with next-generation systems.
Keywords:
machine learning (ml)
; surgeon accountability
; telesurgical robotics
; robot-assisted minimally invasive surgery (Ramis)
; remote-controlled teleoperation
; AI & robotics in healthcare
Introduction And Background
Robotic surgery, commonly known as telerobotic execution of minimally invasive surgery (MIS), involves the surgeon remotely controlling surgical instruments while physically separated from the patient. This approach also referred to as robotically assisted or robotic MIS (RAMIS), has gained popularity due to its compatibility with the modern MIS paradigm. RAMIS offers benefits such as reduced tissue trauma, improved ergonomics for surgeons, and various technological components for use in the operating room (OR). This article aims to highlight the technical capabilities of RAMIS systems with their clinical applicability, taking into account the regulatory environment. The market landscape is dominated by a single product, the "da Vinci surgical system" from Intuitive Surgical Inc., which has performed over 1.5 million procedures annually and remains the most widely used RAMIS system. The success of the da Vinci system can be attributed to factors such as advanced technology features, improved patient outcomes, targeted procedures with quality-of-life improvements, comprehensive training programs, legal responsibility remaining with the surgeon, extensive marketing efforts, and a solution-based business model. The patient's benefit has been a driving force behind the adoption of robotic programs, backed by significant clinical evidence, although some questions regarding long-term benefits compared to open surgery still exist. The adoption of robotic surgery correlates with costs, with higher adoption rates in countries with higher healthcare expenditures. Remote-controlled leader-follower robots are predominantly used in RAMIS, operating in telemanipulation mode where the surgeon controls the surgical tools indirectly [1]. Other classes of surgical or interventional robots with different architectures are also in clinical use. While various technical configurations exist, surgical robot systems generally employ robotic mechanisms to provide accurate guidance, assistance, or direct delivery of instruments or energy. This review focuses on full-scale, teleoperation surgical systems within the RAMIS classification, excluding image-guided interventional robotics, collaborative control, microsurgical systems, and endoluminal robots. The shared feature among these systems is the use of robotic mechanisms to perform precise surgical interventions based on preoperative planning and patient imaging data [2].
The RAMIS Program Simulations and Learning to Operate:
Simulation and training are crucial for surgeons to become proficient in using robot-assisted systems. Various simulators, both physical and virtual, have been developed to support skill development. The insights gained from training sessions have improved system usability and our understanding of human capabilities. Skill assessment is also gaining attention, with classical and machine learning-based methods being used to predict outcomes. Technologies such as eye-tracking systems can provide adaptive functionalities tailored to surgeons' needs. It's also important to assess non-technical skills, like stress management, which can significantly impact patient outcomes [3]. By continuously improving training and assessment, we can ensure better surgical outcomes (Figure 1)
Translational Research: Prototype to Product
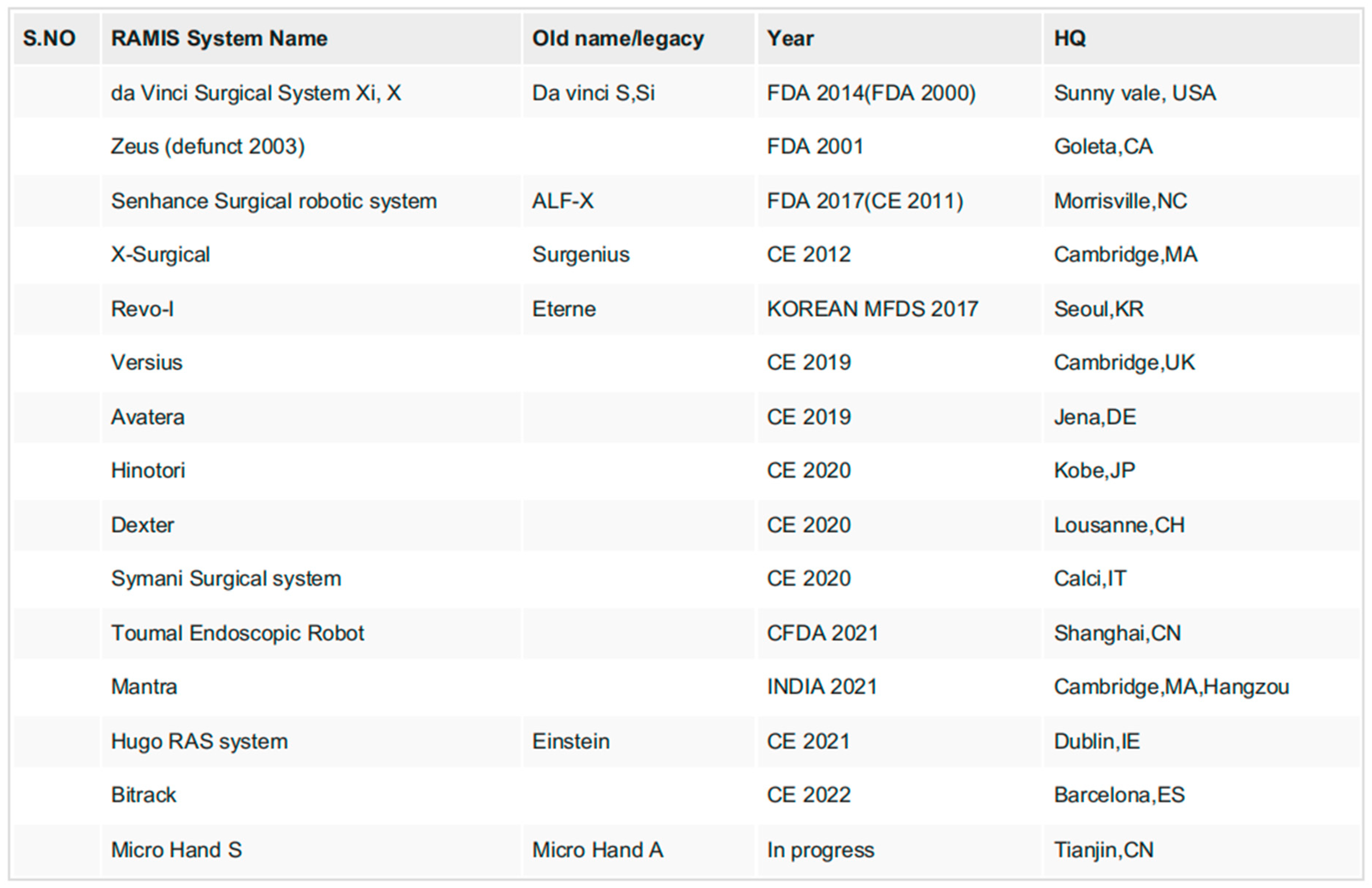
Developing a robot-assisted surgical system for commercial use is a complex process that involves meeting strict regulatory requirements (Table 1). These regulations ensure the safety and reliability of medical devices. Standardization bodies are working on guidelines specific to robot-assisted surgery. However, the path from a functional prototype to a market-ready product is challenging and requires significant time and financial investment. Compliance with regulations is crucial but can be demanding. Despite these challenges, there are ongoing efforts to create sustainable and safe robotics solutions [4]. Funding is essential for research and development, and new entrants in the field should not be underestimated. Collaboration and adherence to ethical standards play a significant role in ensuring the success of robot-assisted surgeries (Figure 2).

Table 1.
List of Most Advanced RAMIS Systems. Only TRL9 Robots Are Shown, Which Have Already Achieved Regulatory Clearance in At Least One Country.
Table 1.
List of Most Advanced RAMIS Systems. Only TRL9 Robots Are Shown, Which Have Already Achieved Regulatory Clearance in At Least One Country.
Data and AI as Facilitating Elements for Democratising RAMIS- SDS:
Data plays a vital role in robot-assisted surgeries, bringing together information from various sources like robot movements, videos, and patient data. Managing and processing this data can be challenging, but with big data techniques, we can develop new applications using machine learning and artificial intelligence. These applications can help automate surgical tasks and provide personalized guidance. However, we still face challenges in obtaining large annotated datasets for training AI models. Researchers are exploring ways to generate synthetic datasets, speed up the annotation process, and develop self-learning methods. It's important to have diverse and representative datasets that capture anatomical variations and patient outcomes. Collaboration and open challenges are crucial to democratize surgical skills and improve the collaboration between surgeons and robots [5].
Human Analytics, Vision, Human Machine Interface:
In robot-assisted surgeries, the interfaces used allow surgeons to manipulate instruments remotely and visualize the surgical site. The vision systems provide high-resolution 3D displays, creating an immersive experience. They can show additional information and augmented reality elements, enhancing the surgeon's understanding. We can also display other imaging modalities like ultrasound or preoperative planning models to assist in decision-making. However, there is room for improvement in providing haptic feedback, which gives a sense of touch. This can help surgeons better feel the surgical environment and adapt their actions accordingly [6]. Developing effective haptic feedback systems is complex but essential for enhancing surgical precision (Figure 3).
The cost of building RAMIS robots is high, especially as new restrictions come into force. New systems' success rely on cutting-edge technology. We want to ensure that AI-powered features enhance patient care without jeopardising security. The use of surgical robots is becoming more and more common, and numerous novel systems are being created. The vast number of RAMIS operations being carried out provides useful information that can aid in our improvement. Although AI has the potential to improve surgery even more, we must be cautious and ensure that patients stand to gain from it [7]. The systems may be more dependable if they have autonomous quality control and safety safeguards. Efforts are being made by standardisation organisations to make surgical robotics safer. Additionally, we're investigating fresh approaches to energy delivery to tissues, which may alter how RAMIS WORKS. The COVID-19 pandemic has shown us the importance of contactless surgery, and RAMIS can play a crucial role in maintaining access to surgeries during such times [8,9,10]. However, there's still work to be done to fully automate the surgical process (Figure 4)
Conclusions
RAMIS is currently the most common type of surgical robotics and it helps many patients. It requires a combination of advanced technology and strict safety measures. The data collected during RAMIS procedures is valuable and can help us improve the systems. We need to continue developing AI and machine learning to assist surgeons and ensure patient safety. The console is an important part of RAMIS, as it allows surgeons to control the robots and receive information. Training and human skills are also crucial for successful outcomes. We should always consider ethics and sustainability as we move forward with RAMIS.
Payment/Services Info
All authors have declared that no financial support was received from any organization for the submitted work.
Financial Relationships
All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
Other relationships
All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Conflicts of Interest
In compliance with the ICMJE uniform disclosure form, all authors declare the following:
References
- C. D’Ettorre .: Accelerating surgical robotics research: A review of 10 years with the da Vinci research kit.
- IEEE Robot. Autom. Mag., vol. 28, no. 4, pp. 56-78, Dec. 2021, 10:2021-3101646. [CrossRef]
- T. Haidegger: Autonomy for surgical robots: Concepts and paradigms, . IEEE Trans. Med. Robot. Bionics, vol.1, no. 2, pp. 65-76, May. 2019. [CrossRef]
- P. E. Dupont , “A decade retrospective of medical robotics research from 2010 to 2020,” . Sci. Robot., vol. 6.
- no.:60-2021. [CrossRef]
- V. R. Patel: “Essential elements to the establishment and design of a successful robotic surgery. Patel.
- programme,” Int. J. Med. Robot. Comput. Assist. Surgery, vol. 2, no. 1, pp. 28-35, Mar. 2006. [CrossRef]
- 5. C. J. Bruns, and H. F: Fuchs, “5G mobile communication applications for surgery: An overview of the latest.
- literature,”. Artif. Intell. Gastrointestinal Endoscopy, vol. 2, no. 1, pp. 1-11, Mar. 2021. [CrossRef]
- 6. T. Haidegger, J. Sandor, and Z: Benyó, “Surgery in space: The future of robotic telesurgery,” . Surgical Endoscopy, vol. 25, no. 3, pp. 681-690, Mar. 2011. [CrossRef]
- . Haidegger T, Speidel, S., Stoyanov, D, & Satava, R. M.: Robot-assisted minimally invasive surgery—Surgical robotics in the data age. Proceedings of robot-assisted minimally invasive surgery—Surgical robotics in the data age. 110:835-846. [CrossRef]
- 8. R. Gupta, A. Shukla, and S. Tanwar, “BATS: A blockchain and AI-empowered drone-assisted telesurgery.
- system towards 6G,”. IEEE Trans. Netw. Sci. Eng., vol. 8, no. 4, pp. 2958-2967, Dec. 2021. [CrossRef]
- 9. M. Giordani, M. Polese, M. Mezzavilla, S. Rangan, and M. Zorzi: Toward 6G networks: Use cases and.
- technologies,. IEEE Commun. Mag., vol. 58, no. 3, pp. 55-61, Mar. 2020. [CrossRef]
- 10. 45] G. Lacava.: Cybsersecurity issues in robotics,. J. Wireless Mobile Netw., Ubiquitous Comput., Dependable Appl., vol. 12, no. 3, pp. 1-28, Sep. 2021.
Figure 1.
Most advanced RAMIS systems, featuring only commercially available, and ready-to-launch platforms, already cleared for at least a limited set of surgical indications (presented in the order of time of appearance). (a) da Vinci Xi. (b) Senhance Surgical Robotic System. (c) Revo-i. (d) Versius. (e) Avatera. (f) Hinotori. (g) Dexter. (h) Symani Surgical System. (i) Toumai Endoscopic Robot. (j) Mantra. (k) Hugo RAS System. (l) Bitrack. Table 1 at the end provides details regarding these robots’ basic engineering and clinical capabilities. (Image credit: the respective manufacturers.).
Figure 1.
Most advanced RAMIS systems, featuring only commercially available, and ready-to-launch platforms, already cleared for at least a limited set of surgical indications (presented in the order of time of appearance). (a) da Vinci Xi. (b) Senhance Surgical Robotic System. (c) Revo-i. (d) Versius. (e) Avatera. (f) Hinotori. (g) Dexter. (h) Symani Surgical System. (i) Toumai Endoscopic Robot. (j) Mantra. (k) Hugo RAS System. (l) Bitrack. Table 1 at the end provides details regarding these robots’ basic engineering and clinical capabilities. (Image credit: the respective manufacturers.).

Figure 2.
ISO/IEC standard concept of RAMIS components and interfaces linking the robotic parts to the other medical devices (MEE/MES) in the OR.
Figure 2.
ISO/IEC standard concept of RAMIS components and interfaces linking the robotic parts to the other medical devices (MEE/MES) in the OR.
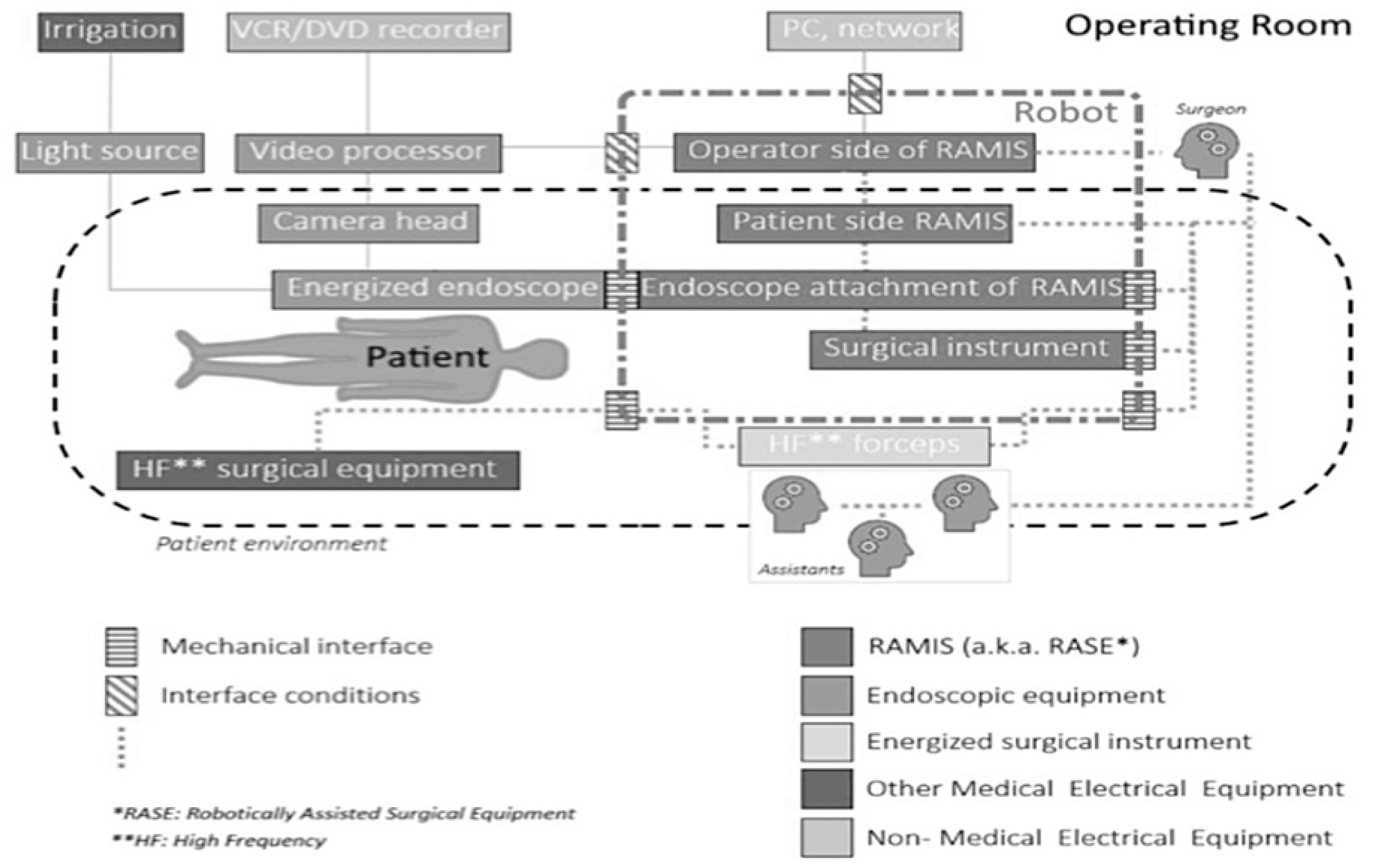
Figure 3.
Applied research directions on RAMIS systems already established, based on the first ten years of DVRK-related projects. Initial focus was mostly on hardware capabilities and component analysis, while more recently, much attention is paid to software enhancements, decision support, and autonomous function development.
Figure 3.
Applied research directions on RAMIS systems already established, based on the first ten years of DVRK-related projects. Initial focus was mostly on hardware capabilities and component analysis, while more recently, much attention is paid to software enhancements, decision support, and autonomous function development.
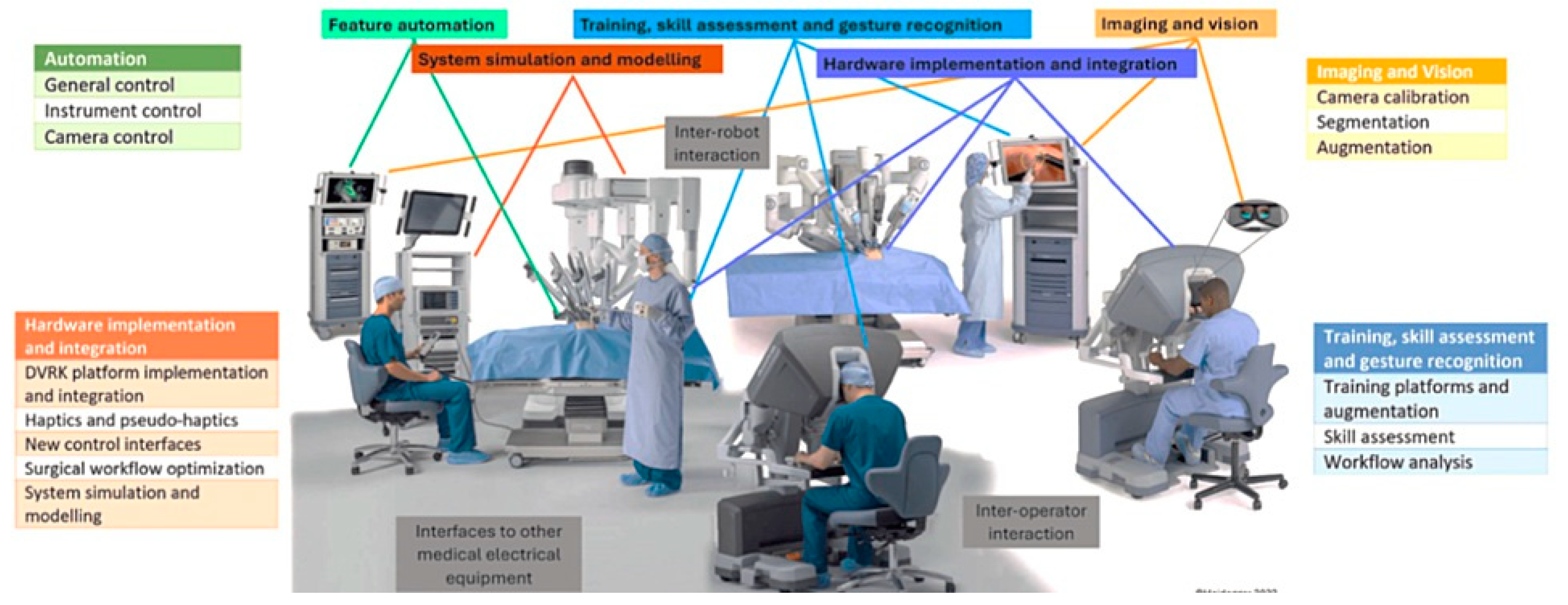
Figure 4.
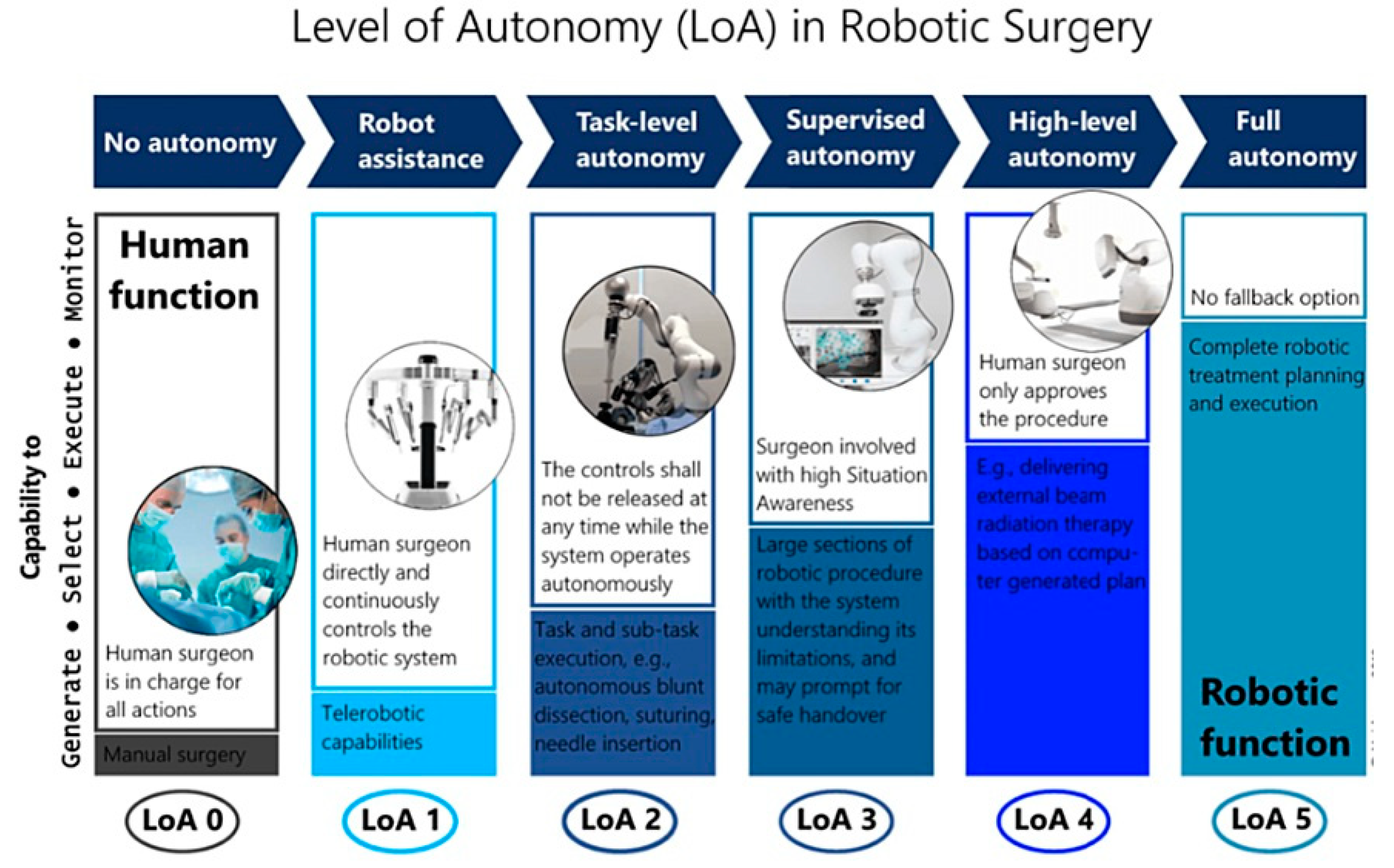
Concept of LoA classification in RAMIS, where currentteleoperational systems reach only LoA 1 typically, providing assistance with basic safety support under remote control.
Figure 4.
Concept of LoA classification in RAMIS, where currentteleoperational systems reach only LoA 1 typically, providing assistance with basic safety support under remote control.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



