
Submitted:
08 April 2025
Posted:
09 April 2025
You are already at the latest version
Abstract
Surgical trauma induces a complex inflammatory stress response, associated with postoperative morbidity. Patients’ physiological reserve, comorbidity, underlying disease and type of surgery will interrelate with the response. In addition, different anaesthetic agents are shown to have differential effects on this response. We explored the molecular effects of an intermediate surgical intervention together with the effect of either a propofol or sevoflurane based anaesthesia in a unique cohort of healthy living kidney donors (n=36, propofol 19, sevoflurane 17) undergoing laparoscopic donor nephrectomy by using proteomic profiling of blood plasma samples. Samples were taken before surgery, 2 and 24 hours after surgery. Quantitative analysis resulted in detection of 633 plasma proteins. A subset of 22 proteins showed significant (P<0.05) expression level changes between time points. Proteins with over two-fold change comprised a group of 8 upregulated targets known to be involved in the acute phase response (CRP, SAA1, SAA2, LBP), cellular proliferation (FGL1, A2GL) and anti-inflammation (AACT). These proteins were common in all living donors, except MAN1A1 and SAA2, which were upregulated only in propofol (MAN1A1) or sevoflurane (SAA2) treated individuals. To conclude, proteomic profiling identified upregulated proteins one day after laparoscopic donor nephrectomy involved in the acute phase response, immunogenicity and tissue remodeling.
Keywords:
surgical stress response
; acute phase response
; proteomics
; propofol
; sevoflurane
; anaesthesia
; living kidney donors
; systems biology
; tissue regeneration
; laparoscopic surgery
Introduction
Each year, over 4.2 million patients die within 30 days after a surgical procedure, making postoperative mortality with 7.7% the third leading cause of death after ischemic heart disease and stroke.[1] Next to this, about 20% of patients develop postoperative complications, which are linked to poorer long term outcomes, longer hospital admissions, increased costs and a burden to society.[2] Even after complete recovery, 20-40% of patients experience a decline in functional capacity or quality of life.[3] Consequently, the global disease burden of surgical procedures is substantial.
Poor outcome after surgery is most likely the result of a complex interplay between the underlying disease of the patient, his or her comorbidity and physiological reserve capacity, genetic predisposition and the individual biological stress response to tissue injury. Surgery induces a stress response due to both direct (e.g. tissue dissection, traction and heating) and indirect (e.g. hypoperfusion, acidosis, and ischemia) tissue injury, leading to hormonal, metabolic and immunological changes.[4,5,6] Prolonged elevation of cytokines (e.g. interleukin(IL)-1b, IL-6, IL-8 and tumor necrosis factor alpha (TNF-α), hormones (e.g. cortisol), acute phase proteins (C-reactive protein (CRP)), and activation of the coagulation system after surgery are likely associated with an increased risk of postoperative complications.[7,8,9] Increasing evidence shows that intra-operative interventions like maintenance of normothermia, prevention of acidosis, optimization of fluid therapy and using minimal invasive surgical techniques and choice of anesthetics can modulate the stress response and reduce the incidence of postoperative complications.[10,11,12,13,14,15] Furthermore, it is known that anesthetic agents have immunomodulatory, anti-necrotic as well anti-apoptotic effects.[16,17] Both the intravenous anesthetic propofol and the inhalational anesthetic sevoflurane have protective and anti-inflammatory effects and are routinely used. Reduced levels of IL-1, IL-6 and IL-8, as well as significant reduction in oxidative stress has been found in propofol anaesthesia [18,19,20,21], whilst inhibition of production of IL-1b, IL-6 and apoptosis regulatory proteins such as cytochrome C and caspase 3 have been reported for sevoflurane.[22]
Unravelling the surgical stress response and identifying pre- and intraoperative factors that interfere with this response is important as it may reveal modifiable factors that could improve surgical outcomes. Unfortunately, most patients undergoing a substantial surgical procedure have an indication due to an acute or chronic disease as well as often suffer from comorbidities that will interfere with perioperative stress responses and affect outcomes. This makes it difficult to evaluate the bespoke effect of the proper surgical procedure on the stress on a molecular level. The living donor procedure in kidney transplantation is an unique ‘model’ as this cohort concerns healthy subjects (and not patients) without any or minimal comorbidity who are exposed to an intermediate risk surgical procedure (laparoscopic donor nephrectomy). In this study we assessed the stress response caused by the surgical procedure by analyzing proteomic profiles from sequential plasma samples in the perioperative period. We also compared the effects of either using propofol or sevoflurane based anaesthesia. Gaining a better insight into the effect of surgery and anaesthesia in healthy individuals might enhance our understanding of the surgical stress response and create reference data for future comparison in other patient categories.
2. Results
2.1. Patient Characteristics
Table 1 summarizes donor baseline characteristics and clinically relevant perioperative parameters. Donors had low comorbidity score and were considered by a clinical team fit to donate a kidney. Charlson Comorbidity Index was comparable between the propofol (PROP) group and in the sevoflurane (SEVO) group (1 (0-2) vs. 1 (0-1), P 0.62). Most common comorbidities were hypertension and hypercholesterolemia, combined as cardiovascular comorbidity in table 1. There was a higher incidence of cardiovascular comorbidity in the SEVO group compared to the PROP group (5 (29%) vs. 1 (5%), P 0.080). Medications used preoperatively in both groups were beta blockers (SEVO 2), angiotensin (AT)-II antagonists (SEVO 2), statins (PROP 1, SEVO 3), proton pump inhibitors (PROP 3), platelet aggregation inhibitors (SEVO 2) and antidepressants (PROP 1). Duration of the surgical procedure was comparable between groups. Donors anaesthetized with sevoflurane showed a higher average bispectral index (BIS) value during the procedure (45(6) vs 39(7), P 0.012). Donors anaesthetized with sevoflurane more frequently received a bolus of ephedrine after induction of anaesthesia compared to patients anaesthetized with propofol (17 (100%) vs. 13 (68%), P 0.020). This occurred predominantly after induction of anaesthesia. No extended hypotensive periods were observed and none of the donors received vasoactive medication on a continuous basis. Intraoperative hemodynamic profiles over time of mean arterial pressure and heart rate were comparable between groups (data not shown but available upon request). In all donors, remifentanil was started at 2 ng/ml effect site concentration (Cet) and average Cet of remifentanil during the procedure was significantly higher in the PROP than SEVO group (3.2 (0.86) vs 2.6(0.63); P 0.02). The amount of fluid administered intraoperative was similar and Ringers Lactate was used. No colloids were used. Arterial blood sampling at the time of retrieval of the kidney showed comparable pH, oxygen tension and levels of hemoglobin. Lactate levels at that time point were higher in the SEVO than in the PROP group (1.7 (0.7) vs. 1.3 (0.5); P 0.04). One patient in the prop group developed pneumonia in the postoperative period which was treated with antibiotics. One patient in the PROP group developed hypokalemia which resolved spontaneously. Length of hospital stay was comparable between groups, 5 (5-7) days for the PROP group and 5 (5-7,5) days for the SEVO group (P 0.91).
2.2. Proteomics Profiles Dependent of Anaesthetic Regimen
Quantitative proteomics analysis resulted in the detection of 633 plasma proteins. A subset of 22 proteins showed statistically significant changes in expression levels between time points T2 (24 hours after surgery)-vs-T0 (baseline) (Multiple Testing Correction (MTC) P<0.05, Table 2). When comparing expression changes of these 22 proteins between groups, PROP anaesthesia induced a change in the abundance of 15 proteins (Figure 1); SEVO in 18 proteins (Figure 2). Of the 15 proteins that reached statistical significance in PROP (MTC P<0.05), 7 showed over a 2-fold increase. Similarly, out of 18 significantly increased proteins in SEVO (MTC P<0.05), 7 showed over a 2-fold increase. Changes in plasma protein levels that were independent of the anaesthesia type included 11 proteins that were consistent in the direction and magnitude of change (Table 2). These changes were statistically significant after MTC and a threshold of at least P <0.05 and often lower, reflecting increased stringency. Typically, levels of proteins were increased following surgical intervention, with the exception of plasma serine protease inhibitor (IPSP) which showed a >1.5-fold decrease (P-value<0.01 MTC). There were 6 proteins with greater than 2-fold changes independent of anaesthesia type: CRP (>35-fold), fibrinogen-like protein-1 (FGL-1, >10 fold), serum amyloid A-1 protein (SAA1, >9-fold), LPS binding protein (LBP, >4-fold), leucine-rich alpha-2-glycoprotein (A2GL, >2-fold), alpha 1-antichymotrypsin (AACT, >2-fold). Fold change generally agreed well between the two anaesthesia types, yet showed variability for CRP and SAA1 proteins (35,83 vs. 70.09 and 9,05 vs 110,69 for PROP and SEVO respectively), possibly due to low abundance of the proteins (close to noise signal level) in T0. In addition there were 4 proteins specific to PROP and 7 proteins specific to SEVO, which showed under 2-fold change, with the exception of mannosidase Alpha Class 1A Member 1 (MAN1A1, 2,12 fold change) in PROP and SAA2 in SEVO (48,67 fold change) (Figure 1 and Figure 2).
Next, proteomics data were validated by ELISA in both propofol and sevoflurane treated groups (Figure 3A,B). Acute phase response markers CRP and SAA1 were selected for validation. Both treatment groups showed an increase in line with the proteomic findings, with comparisons between T2 vs. T0 and T1 vs. T0 reaching statistical significance for both CRP and SAA1. In case of CRP, ELISA detection showed an approximate 10-fold increase in both PROP and SEVO at T2 (Figure 3C), with SAA1 demonstrating an approximate 100-fold increase (Figure 3D).
2.3. Proteomics Profiles Independent of Anaesthetic Regimen
As most of the changes in protein expression were found to be independent of the type of anaesthetic, we combined both anaesthesia groups (36 samples at three time points) for further analysis (Table 3). 7 proteins showed a change in abundance above 2-fold (MTC P<0.05). Table 3 also illustrates a clear indication of the change of the level of detected proteins over time. When comparing T1 vs. T0, seven proteins showed statistical significance (MTC P<0.05), increasing to 22 proteins in T2 vs. T1 and 28 when comparing T2 vs. T0.
3. Discussion
In this study, we analyzed the surgical stress response on a plasma proteomic level in healthy individuals undergoing a minimally invasive laparoscopic donor nephrectomy receiving either a propofol-based or a sevoflurane-based anaesthesia. Currently, very little is known about the effect of any surgical intervention on the biological pathways involved in injury and repair. Our study provides a first step in this direction since we were able to study the response in healthy individuals with a low comorbidity score whilst being exposed to the stress of a surgical procedure under anaesthesia when donating one kidney for transplantation. The study of this unique ‘healthy’ cohort undergoing surgery may therefore serve as a ‘gold standard’ reference or control group for future research on how surgical and anaesthetic intervention will affect outcomes in patients with acute or chronic diseases and significant comorbidities.
By using an unbiased proteome approach and analyzing individual sequential proteomic profiles, our results show that the highest changes in protein levels were found 24 hours after surgery but appeared to be independent of the anaesthetic agent used. Only some modest changes were detected between sevoflurane and propofol. There is conflicting evidence on which anesthetic agent is most beneficial for postoperative recovery.[26,27] Obviously, the optimal choice of an anesthetic for a particular surgical procedure or patient is the agent that will reduce the inflammatory response and thereby reduce the risk of postoperative morbidity after surgery.[18,28]
A prominent category of proteins that we found upregulated included acute phase proteins (APPs) involved in the acute phase response (ARP). APPs act as first line of defense upon interruption of the homeostasis. APPs may function as pathogen recognition receptors (e.g. CRP, SAA, LPS, FGL-1), proteinase inhibitors (e.g. AACT, A1AT) or involve components of the complement, coagulation and fibrinolytic system. APPs have diverse molecular functions that protect the host against pathogens and tissue injury.[29]
CRP, a non-specific acute phase protein produced in the liver in response to IL-6 and other pro-inflammatory cytokines, plays a critical role in innate immunity by binding to ligands on apoptotic cells. This process activates the complement cascade and stimulates phagocytosis in immune cells.[30] CRP level rises 6-8 h after surgical trauma with half-life of 19 h, and under normal conditions peaks 2-3 days after surgery.[31,32] In our study, the CRP level at baseline was low (3.4mg/L), but reached to 53.9 mg/L one day after surgery, which demonstrates the minimally invasive nature of the procedure, and is similar to increases in levels observed after laparoscopic hysterectomy or surgical repair of ankle fractures.[33,34] Significant changes in upregulation in CRP levels were found in both anaesthetic groups, with less upregulation in the PROP group compared with the SEVO group (35 vs. 70 fold change, respectively). After ELISA validation, no differences in CRP levels between the two anaesthetic groups were found, which suggests that the overall levels of injury and inflammation are similar.
SAA, especially the isoforms SAA1 and SAA2, are early high sensitive acute phase proteins.[35] Plasma levels of SAA1/2 may increase up to 1000-fold or more 24-36 h after injury, and remain elevated for 2-3 days.[36,37] SAA is considered an important protein in the acute phase response during inflammation. The exact physiological role, however, remains unclear. A generally accepted role of SAA in the APR is its role in cholesterol recycling and tissue remodeling trough metalloproteinases.[35] After engulfment of cellular debris macrophages are loaded with cholesterol. SAA-HDL binds to these macrophages and enhances the efflux of un-esterified cholesterol. Un-esterified cholesterol binds with SAA free HDL, upon which HDL-cholesterol can be redistributed and reused in inflammation and repair mechanisms, while cholesterol-depleted macrophages continue phagocytosis.[38] SAA synthesis is induced by cytokines such as IL-1β, IL-6, TNF-α. Linke et al. showed a critical role of SAA in survival: In a cecal ligation and puncture (CLP) model in normal mice, 75% of the wild type mice survived at day 5, while SAA-deficient or antibody treated mice had a 90% mortality rate.[39] Of interest is the fact that based on proteomic data, SAA1 levels in sevoflurane treated individuals increased to a higher extend (110.69 fold change) compared to propofol treated individuals ( 9.05 fold change) and that SAA2 only reached significant upregulation in sevoflurane treated individuals and not in the propofol group. Based on ELISA validation, plasma SAA1 levels increased 677-fold one day after surgery, surpassing CRP levels, indicating SAA1 may serve as a more sensitive marker reflecting severity of tissue injury. Currently it is unknown whether the amount of increase of SAA early in the APR indicates increased injury or enhanced repair capacity. However, persisting high levels of SAA after surgery have been associated with postoperative infections and adverse outcome.[40,41]
LBP plays a dual role in the innate immune response to bacterial infection and inflammation. Baseline concentration (5-15 ug/L) can increase up to 30-50 fold during the acute phase response.[42,43] At low concentration, LPB binds with lipopolysaccharide (LPS), a prominent component of gram-negative bacteria, facilitating its recognition by membrane-bound CD14 (mCD14) on the surface of macrophages. Binding of LPS-LPB complex to mCD14 will lead to upregulation of transcription of pro-inflammatory cytokines like TNF-α and IL-1β.[43] For mCD14-negative cells, LBP transfers LPS to secreted CD14 (sCD14), which is recognized by membrane bound receptors, inducing transcription of pro-inflammatory cytokines like IL-6 and IL-8.[43] In addition to its classic role, LPB can bind bacteria and pathogen associated molecular patterns (PAMPs). At high concentration LPB neutralizes bacterial endotoxins and down regulates the expression of TNF-α, preventing an overwhelming immune reaction.[42,43] LPB increases significantly upon severe infections and has been suggested a biomarker for prediction of severe sepsis, particularly in the first 48 hours.[44]. The exact role of LPB in the perioperative phase, however is unclear, with limited studies showing peak levels 72 h after appendectomy or cardiac surgery.[45,46] In cardiac surgery no correlation was found between levels of LPB and IL-6 or CRP, with surprisingly no differences between on-pump and off-pump procedures whereas higher levels were expected in on-pump patients due to lower perfusion pressure of the splanchnic circulation and higher likelihood of translocation of bacteria.[46] This suggests that LBP production is stimulated by another still unknown danger pattern which is identical in both on-pump and off-pump procedures. In the current study, LBP was significantly upregulated one day after surgery, with no differences between the PROP and SEVO group (both >4 fold change).
Both FGL-1 and A2GL were similarly upregulated under both anaesthesia regimens. FGL-1, member of the fibrinogen family, is produced by the liver upon stimulation by IL6.[47] Its exact role in the APR to date is unknown. Since it is highly upregulated upon liver injury, FGL-1 was primarily linked to liver regeneration, until Liu and colleagues showed that enhanced expression of FGL-1 by IL-6 in the absence of liver injury, suggesting a role of FGL-1 in the APR.[47] Rijken et al. showed that FGL-1 is associated with fibrin matrix formation, indicating a potential function in regulating fibrin polymerization.[48] Additionally, FGL-1 was found upregulated in heart-transplanted rats with induced bacterial pulmonary infection.[49] To the best of our knowledge, this study is the first showing FGL-1 upregulation in healthy subjects undergoing a non-hepatic surgery.
Similar to FGL-1 the exact biological function of A2GL currently is unclear. A2GL is expressed by hepatocytes, neutrophils, macrophages, and epithelial cells in response to cytokines like IL-6, IL-1β, and TNF-α. A2GL is involved in cell adhesion, differentiation of polymorphic nuclear cells, angiogenesis and cell migration.[50] Oncogenic and oncosuppressing properties have been reported, and A2GL is upregulated in many inflammatory diseases, such as rheumatoid arthritis.[51] In a murine epidermal injury model, Gao and colleagues showed that A2GL expression is high during wound repair.[52] In patients undergoing CABG, levels of A2GL are significantly upregulated 24h after surgery.[53] The current study showed significant upregulation one day after surgery in both FGL-1 (>10 fold) and A2GL (>2 fold). The precise role of FGL-1 and A2GL in the APR, whether pro- or anti-inflammatory, or related to injury or repair, remains unclear. Dynamics of these proteins in patients with and without postoperative complications would therefore be an interesting area of study.
Another protein that was found significantly upregulated in an anaesthesia-independent manner was alpha-1-antichymotrypsin (AACT), a serine protease inhibitor (Serpin). Primarily, serpins neutralize overexpressed serine proteinase activity, thus controlling a variety of biological processes such as coagulation and inflammation.[54] AACT, the most abundant Serpin in human plasma, inhibits a variety of serine proteases of which cathepsin G is thought to be its major target.[53] Cathepsin G is released by neutrophils at the site of inflammation or injury where it activates pro-inflammatory cytokines, enhances coagulation and thrombosis and kills and degrades pathogens.[53] . AACT expression is modulated by, amongst other, IL-6 and IL-1, and forms a feedback loop controlling the APR. Banfi and colleagues showed that levels of AACT peak 24h after coronary artery bypass grafting with an almost 3 fold upregulation.[53] The upregulation of AACT, along with less abundant A1AT and metallopeptidase inhibitor 1 (TIMP1), an inhibitory molecule that regulates matrix metalloproteinases in our living kidney donors one day after surgery suggests an increased anti-inflammatory response.[55,56] The observed downregulation of serine protease inhibitor-IPSP might be explained by enhanced consumption as a result of proteolysis after surgery.
Proteome profiles displayed a number of moderate level anaesthesia-specific changes, with propofol eliciting a larger number of upregulated proteins than sevoflurane. SAA2 was only significantly upregulated in SEVO anaesthesia. MAN1A1 was found upregulated specifically in PROP anaesthesia. MAN1A1 is involved in glycosylation. This is crucial for stability and function of glycoproteins, including cytokines. MAN1A1 overexpression could enhance the expression of pro-inflammatory cytokines, potentially leading to dysregulation of the perioperative stress response.[57]
Although discovering novel molecular insights into post-operative and anaesthetic effects, our post-hoc analysis has limitations. Since this was a pilot discovery study to identify proteomic changes, no power calculation was performed and the sample size was small. Therefore, the results of this study need to be validated in a larger prospective cohort. We observed differences between groups regarding depth of anaesthesia and Cet of remifentanil during the procedure with SEVO showing a higher average BIS and a lower Cet of remifentanil. Although we cannot exclude that this has interfered with our results, we consider these differences small and clinically not relevant. In addition, lactate levels before explanting the kidney in the SEVO group were higher than the PROP group. Both groups, however, were within normal physiological range. Since our living kidney donors were mainly discharged from the hospital on the third day after surgery we were unable to study the proteomic changes over a longer period of time. In addition, only 2 donors developed postoperative complications. Therefore, caution needs to be applied to make correlations between levels of proteins and outcome.
In summary, we have used an unbiased proteomic approach to assess changes in molecular proteomic profiling due to surgical intervention in healthy individuals who are donating a kidney for transplantation. The type and quantification of proteins identified suggests a significant upregulation of the acute phase response, activation of the coagulation cascade and initiation of tissue regeneration within 24 hours after surgical intervention, which is independent of the anaesthetic agent used. The magnitude and timing of the stress response is compatible with the moderate invasive character of the surgical procedure and consistent with the low incidence of postoperative complications and fast recovery in our study. Our proteomic results also suggest that there are delicate balances between pro- and anti-inflammatory acute phase responses, independent of the anaesthetic agent used. It is important that after 24 hours, proteins can be identified that suggest the presence of tissue regeneration and point at a subtle balance between injury and repair in the early postoperative period.
In conclusion, proteomic profiling identified upregulated proteins one day after laparoscopic donor nephrectomy. The proteins identified in this study may serve as a reference when developing a profile of potential markers to better monitor the immune response and effect of postoperative medical treatment attempting to reduce surgery-related complications and improving short-and long-term outcomes.
4. Materials and Methods
4.1. Study Population
Stored plasma samples of donors participating in the Volatile Anaesthetic Protection Of Renal transplants (VAPOR)-1 trial were used. The VAPOR-1 trial is a prospective randomized controlled trial on the effects of two different anaesthetic agents (propofol vs sevoflurane) on renal outcome in living donor kidney transplantation.[23] The Institutional Review Board of the University Medical Centre of Groningen approved the study protocol of VAPOR-1 (METc 2009/334), which was conducted in adherence to the Declaration of Helsinki and registered with ClinicalTrials.gov: NCT01248871. Of the 57 donors, 19 patients received a sevoflurane based anaesthesia and 38 a propofol based anaesthesia. For this post-hoc analysis we selected donors without any or with only minor comorbidities and included 17 donors of the sevoflurane group (SEVO) and 19 matched donors of the propofol group (PROP) with completed set of plasma samples. The two groups were matched for age, gender, body mass index (BMI), concomitant comorbidities, medication, use and smoking.
4.2. Surgery and Anaesthesia
Kidney donation was performed via a hand-assisted laparoscopic procedure under general anaesthesia. Choice of anaesthetic agent (propofol or sevoflurane) was based upon randomization. Intraoperative analgesia was managed with remifentanil with the use of target controlled infusion. Depth of anaesthesia, administration of fluids, hemodynamic management and administration of all medications were strictly protocolized. Postoperative pain management on day 1 encompassed paracetamol 1000 mg 4 times daily and piritramide intravenous with the use of patient-controlled analgesia.[23]
4.3. Samples Acquisition
Blood samples in the VAPOR-1 study were taken at standardized time point.[23] For this project we analyzed samples taken at three different time points (T0-T2): T0: baseline before induction of anaesthesia; T1: end of surgery upon skin closure, and the T2: 24 hours after surgery. Samples were centrifuged (1500g, 20 minutes (min)) and plasma sample collected and stored at -80°C until analysis.
4.4. Sample Preparation
All 108 samples involved in the study were first subjected to depletion of the top 12 most abundant proteins using T12 Depletion (Pierce™ Top 12 Abundant Protein Depletion Spin Columns (Thermo Fisher Scientific, Waltham, MA, U.S.). To this end, 10 L of sample was incubated with gentle mixing for 60 min at room temperature and then centrifuged at 1000g for 2 min. The filtrate containing the depleted sample was suspended in 10 mM phosphate buffer saline (PBS), NaCl, 0.02% azide, pH 7.4. Protein concentration was assessed by Bicinchoninic acid (BCA) protein assay kit (Thermo Fisher Scientific, Waltham, MA, U.S.).
Twenty g of T12 depleted sample was then digested using the SMART method. Briefly, each sample was loaded into a SMART digestion tube (Thermo Fisher Scientific, Waltham, MA, U.S.) containing 150 L of SMART digestion buffer. These were then incubated at 70 C at 1400 revolutions per min (rpm) for 1 hour on a heat shaker (Eppendorf, Hamburg, Germany) and then spun at 2500g for 5 min, collecting the supernatant containing tryptic peptides. The samples were desalted using SOLAu SPE plates (Thermo Fisher Scientific, Waltham, MA, U.S.). Columns were equilibrated using 100% acetonitrile, then 0.1% trifluoroacetic acid (TFA). The samples were then acidified with 1% TFA and pulled through the column using a vacuum pump. They were then washed with 0.1% formic acid (FA) and eluted using 100 L of 65% acetonitrile. Eluted samples were dried using a vacuum concentrator (SpeedVac, Thermo Fisher Scientific, Waltham, MA, U.S.) and resuspended in buffer A (98% MilliQ-H2O, 2% ACN, 0.1% FA) for mass spectrometry analysis.
4.5. Mass Spectrometry
For peptide analysis, nano-liquid chromatography tandem mass spectrometry (LC-MS/MS) was used, consisting of an ultra-high performance liquid chromatography (uHPLC) coupled to a Hybrid Quadrupole-Orbitrap mass spectrometer (Fusion LUMOS, Thermo Fisher Scientific, Waltham, MA, U.S.) as described previously.[24] In brief, 1 µL of 0.5 µg/µL of peptide material was injected for analysis by LC-MS/MS. Peptides were separated by an Easy-Spray LC C18 column (75 µm x 50 cm, Thermo fisher Scientific, Waltham, MA. U.S.) at a flow rate of 250 nL/min. The mobile phases consisted of water with 0.1% FA, 5% DMSO (buffer A) and 95% acetonitrile with 5% DMSO, 0.1% FA (buffer B), respectively. A 60 min linear gradient from 3% buffer A to 40% buffer B was used. The peptides were ionized by electro spray ionization and the 20 most abundant ions per MS scan were fragmented by collision-induced dissociation (CID) as described previously.[25]
4.6. Data Analysis and Statistics
MaxQuant software (v1.5.8.3) was used for processing raw MS data and for peptide and protein identification and quantitation. LC-MS/MS spectra was searched against Uniprot human database (version 2017, 20,205 entries) for peptide homology identification. At least one unique peptide was used for protein quantitation using match between runs. The false discovery rate (FDR) was set to 1% for protein and peptide identification. Label free quantitation (LFQ) intensity data were used for further statistical analysis to compare across the different time points (T2 vs T1 and T0) and groups (propofol vs sevoflurane). Differentially expressed proteins in the analysis were defined as proteins presenting a statistical difference across the group (P<0.05) (proteins detected in at least three individuals/group to allow a Student T-test). Multiple testing correction (MTC) was applied to the comparison between time points in both anaesthetic types. UniProt and Panther (Gene Ontology) databases were utilized for interpretation of molecular function of identified targets. The MS data are available upon request by the authors.
4.7. ELISA
To validate proteomic findings, ELISA was used to detect CRP and serum amyloid A (SAA)1 (R&D Systems, Minneapolis, MN, U.S. CRP DuoSet, SAA1 DuoSet). Plates were coated with capture antibody at room temperature overnight and blocked with Reagent Diluent for 1 hour at room temperature (RT). One hundred L of diluted plasma sample was added for 2 hours at RT followed by antibody detection for 2 hours, then Horseradish peroxidase (HRP) and substrate solution for 20 minutes each at RT. Stop solution was then added and the plate analyzed using a TECAN plate reader at a wavelength of 540 nm.
Author Contributions
Conceptualization, B.B., H.H., S.M., A.M.T., J.H., G.J.N.M.; methodology, B.B., H.H., S.M., A.M.T., J.H., G.H.d.B., G.J.N.M.; software, H.H., S.M., A.M.T. ; validation, H.H., S.M., A.M.T.; formal analysis, B.B., H.H., S.M., A.M.T., J.H., S.K., B.K., G.J.N.M.; investigation, B.B., H.H., S.M., A.M.T., J.H., S.K., B.K., G.J.N.M.; resources, M.M.R.F.S., H.G.D.L., R.J.P., G.J.N.M.; data curation, M.M.R.F.S., H.G.D.L., R.J.P., G.J.N.M.; writing—original draft preparation, B.B., H.H., S.M., A.M.T., J.H., S.K., M.M.R.F.S., H.G.D.L., G.H.d.B., B.K., R.J.P., G.J.N.M.; writing—review and editing, B.B., H.H., S.M., A.M.T., J.H., S.K., M.M.R.F.S., H.G.D.L., G.H.d.B., B.K., R.J.P., G.J.N.M.; visualization, H.H.; supervision, G.J.N.M.; project administration, B.B., G.J.N.M.; funding acquisition not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. This research is a post-hoc analysis of the VAPOR-1 study. The VAPOR-1 study was funded by an internal effectivity grant from the University Medical Center Groningen (grant nr: 684000), Groningen, The Netherlands.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the University Medical Centre of Groningen (VAPOR-1 study: METc 2009/334), and registered with ClinicalTrials.gov: NCT01248871.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the VAPOR-1 study.
Data Availability Statement
All data presented in this study are available upon request from the corresponding author.
Conflicts of Interest
B.B.: has no conflict of interest to declare; H.H.: has no conflict of interest to declare; S.M.: has no conflict of interest to declare; A.T.: has no conflict of interest to declare; J.H.: has no conflict of interest to declare; S.K.: His research group has received consultancy fees from OrganOx Ltd in the past. M.M.R.F.S. His research group/department received (over the last 3 years) research grants and consultancy fees from Masimo (Irvine, CA, USA), Becton Dickinson (Eysins, Switzerland), Fresenius-Kabi (Bad Homburg, Germany), Paion (Aachen, Germany), Medcaptain Europe (Andelst, The Netherlands), Baxter (Chicago, Il, USA), HanaPharm (Seoul, Republic of Korea). He receives royalties on intellectual property from Demed Medical (Sinaai, Belgium) and the Ghent University (Gent, Belgium). H.G.D.L. is Chief Scientific Officer of 34 Lives (West Lafayette, IN, USA) and has received institutional research grants from the Dutch Kidney Foundation and NOVO Nordisk Foundation. G.H.d.B.: has no conflict of interest to declare. R.J.P.: has no conflict of interest to declare. B.K.: has no conflict of interest to declare. G.J.N.M.: Her research group has received research grants from the Dutch Transplant Society, the UMCG Transplant Fund, the European Society of Anaesthesia and Intensive Care, HosmartAI, the De Cock Hadders Foundation and NIAA RCoA/BJA, Sedana Medical and travel grants from the European Society of Anaesthesia and Intensive Care, University Hospital Zurich and the Scandinavia Society of Anaesthesia and Intensive Care; plus, she is an editor of the British Journal of Anaesthesia Education. The funders have no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results
References
- Nepogodiev D, Martin J, Biccard B, et al (2019) Global burden of postoperative death. Lancet 393:401. [CrossRef]
- Kim M, Wall MM, Li G (2018) Risk Stratification for Major Postoperative Complications in Patients Undergoing Intra-abdominal General Surgery Using Latent Class Analysis. Anesth Analg 126.
- Lawrence VA, Hazuda HP, Cornell JE, et al (2004) Functional independence after major abdominal surgery in the elderly. J Am Coll Surg 199:762–772. [CrossRef]
- O’Dwyer MJ, Owen HC, Torrance HDT (2015) The perioperative immune response. Curr Opin Crit Care 21.
- Giannoudis P V, Dinopoulos H, Chalidis B, Hall GM (2006) Surgical stress response. Injury 37:S3–S9. [CrossRef]
- Dobson GP (2015) Addressing the Global Burden of Trauma in Major Surgery. Front Surg 2.
- Bochicchio G V, Napolitano LM, Joshi M, et al (2002) Persistent Systemic Inflammatory Response Syndrome Is Predictive of Nosocomial Infection in Trauma. J Trauma Acute Care Surg 53.
- Mutoh M, Takeyama K, Nishiyama N, et al (2004) Systemic inflammatory response syndrome in open versus laparoscopic adrenalectomy. Urology 64:422–425. [CrossRef]
- Hirai S (2004) Systemic inflammatory response syndrome after cardiac surgery under cardiopulmonary bypass. Ann Thorac Cardiovasc Surg 9:365–370.
- Wigmore TJ, Mohammed K, Jhanji S (2016) Long-term Survival for Patients Undergoing Volatile versus IV Anesthesia for Cancer Surgery: A Retrospective Analysis. Anesthesiology 124.
- Rollins KE, Tewari N, Ackner A, et al (2016) The impact of sarcopenia and myosteatosis on outcomes of unresectable pancreatic cancer or distal cholangiocarcinoma. Clin Nutr 35:1103–1109. [CrossRef]
- Khuri SF, Healey NA, Hossain M, et al (2005) Intraoperative regional myocardial acidosis and reduction in long-term survival after cardiac surgery. J Thorac Cardiovasc Surg 129:372–381. [CrossRef]
- Moola S, Lockwood C (2010) The effectiveness of strategies for the management and/or prevention of hypothermia within the adult perioperative environment: systematic review. JBI Libr Syst Rev 8:752–792. [CrossRef]
- Rampersad C, Patel P, Koulack J, McGregor T (2016) Back-to-back comparison of mini-open vs. laparoscopic technique for living kidney donation. Can Urol Assoc J = J l’Association des Urol du Canada 10:253–257. [CrossRef]
- Agabiti N, Stafoggia M, Davoli M, et al (2013) Thirty-day complications after laparoscopic or open cholecystectomy: a population-based cohort study in Italy. BMJ Open 3:e001943. [CrossRef]
- Vasileiou I, Xanthos T, Koudouna E, et al (2009) Propofol: A review of its non-anaesthetic effects. Eur J Pharmacol 605:1–8. [CrossRef]
- Motayagheni N, Phan S, Eshraghi C, et al (2017) A Review of Anesthetic Effects on Renal Function: Potential Organ Protection. Am J Nephrol 46:380–389. [CrossRef]
- Sugasawa Y, Yamaguchi K, Kumakura S, et al (2012) Effects of sevoflurane and propofol on pulmonary inflammatory responses during lung resection. J Anesth 26:62–69. [CrossRef]
- Luo C, Yuan D, Li X, et al (2015) Propofol Attenuated Acute Kidney Injury after Orthotopic Liver Transplantation via Inhibiting Gap Junction Composed of Connexin 32. Anesthesiology 122.
- Yang S, Chou W-P, Pei L (2013) Effects of propofol on renal ischemia/reperfusion injury in rats. Exp Ther Med 6:1177–1183. [CrossRef]
- Li Y, Zhong D, Lei L, et al (2015) Propofol Prevents Renal Ischemia-Reperfusion Injury via Inhibiting the Oxidative Stress Pathways. Cell Physiol Biochem 37:14–26. [CrossRef]
- Ohsumi A, Marseu K, Slinger P, et al (2017) Sevoflurane Attenuates Ischemia-Reperfusion Injury in a Rat Lung Transplantation Model. Ann Thorac Surg 103:1578–1586. [CrossRef]
- Nieuwenhuijs-Moeke GJ, Nieuwenhuijs VB, Seelen MAJ, et al (2017) Propofol-based anaesthesia versus sevoflurane-based anaesthesia for living donor kidney transplantation: results of the VAPOR-1 randomized controlled trial. Br J Anaesth 118:720–732. [CrossRef]
- Davis S, Charles PD, He L, et al (2017) Expanding Proteome Coverage with CHarge Ordered Parallel Ion aNalysis (CHOPIN) Combined with Broad Specificity Proteolysis. J Proteome Res 16:1288–1299. [CrossRef]
- Huang H, Ideh RC, Gitau E, et al (2014) Discovery and Validation of Biomarkers to Guide Clinical Management of Pneumonia in African Children. Clin Infect Dis 58:1707–1715. [CrossRef]
- Kotani Y, Pruna A, Turi S, et al (2023) Propofol and survival: an updated meta-analysis of randomized clinical trials. Crit Care 27:139. [CrossRef]
- Kampman JM, Hermanides J, Hollmann MW, et al (2024) Mortality and morbidity after total intravenous anaesthesia versus inhalational anaesthesia: a systematic review and meta-analysis. eClinicalMedicine 72:. [CrossRef]
- Bang J-Y, Lee J, Oh J, et al (2016) The Influence of Propofol and Sevoflurane on Acute Kidney Injury After Colorectal Surgery: A Retrospective Cohort Study. Anesth \& Analg 123:363–370.
- Salvioli S, Monti D, Lanzarini C, et al (2013) Immune system, cell senescence, aging and longevity--inflamm-aging reappraised. Curr Pharm Des 19:1675–1679.
- Akhmedov A, Sawamura T, Chen C-H, et al (2021) Lectin-like oxidized low-density lipoprotein receptor-1 (LOX-1): a crucial driver of atherosclerotic cardiovascular disease. Eur Heart J 42:1797–1807. [CrossRef]
- Colley CM, Fleck A, Goode AW, et al (1983) Early time course of the acute phase protein response in man. J Clin Pathol 36:203 LP – 207. [CrossRef]
- Rosa Neto NS, de Carvalho JF, Shoenfeld Y (2009) Screening tests for inflammatory activity: applications in rheumatology. Mod Rheumatol 19:469–477. [CrossRef]
- Labib M, Palfrey S, Paniagua E, Callender R (1997) The Postoperative Inflammatory Response to Injury following Laparoscopic Assisted Vaginal Hysterectomy versus Abdominal Hysterectomy. Ann Clin Biochem 34:543–545. [CrossRef]
- Neumaier M, Scherer MA (2008) C-reactive protein levels for early detection of postoperative infection after fracture surgery in 787 patients. Acta Orthop 79:428–432. [CrossRef]
- Sack GH (2020) Serum Amyloid A (SAA) Proteins BT - Vertebrate and Invertebrate Respiratory Proteins, Lipoproteins and other Body Fluid Proteins. In: Hoeger U, Harris JR (eds). Springer International Publishing, Cham, pp 421–436.
- Baranova IN, Souza ACP, Bocharov A V, et al (2017) Human SR-BII mediates SAA uptake and contributes to SAA pro-inflammatory signaling in vitro and in vivo. PLoS One 12:e0175824.
- Yamada T, Okuda Y, Takasugi K, et al (2001) Relative serum amyloid A (SAA) values: the influence of SAA1 genotypes and corticosteroid treatment in Japanese patients with rheumatoid arthritis. Ann Rheum Dis 60:124 LP – 127. [CrossRef]
- Eklund KK, Niemi K, Kovanen PT (2012) Immune functions of serum amyloid A. Crit Rev Immunol 32:335–348. [CrossRef]
- Linke RP, Meinel A, Chalcroft JP, Urieli-Shoval S (2017) Serum amyloid A (SAA) treatment enhances the recovery of aggravated polymicrobial sepsis in mice, whereas blocking SAA’s invariant peptide results in early death. Amyloid 24:149–150. [CrossRef]
- Wierdak M, Pisarska M, Kuśnierz-Cabala B, et al (2018) Serum Amyloid A as an Early Marker of Infectious Complications after Laparoscopic Surgery for Colorectal Cancer. Surg Infect (Larchmt) 19:622–628. [CrossRef]
- He Y, Ma C, Xing J, et al (2019) Serum amyloid a protein as a potential biomarker in predicting acute onset and association with in-hospital death in acute aortic dissection. BMC Cardiovasc Disord 19:282. [CrossRef]
- Schumann RR (1992) Function of lipopolysaccharide (LPS)-binding protein (LBP) and CD14, the receptor for LPS/LBP complexes: a short review. Res Immunol 143:11–15. [CrossRef]
- Ding P-H, Jin LJ (2014) The role of lipopolysaccharide-binding protein in innate immunity: a revisit and its relevance to oral/periodontal health. J Periodontal Res 49:1–9. [CrossRef]
- Prucha M, Herold I, Zazula R, et al (2003) Significance of lipopolysaccharide-binding protein (an acute phase protein) in monitoring critically ill patients. Crit Care 7:R154. [CrossRef]
- Brănescu C, Şerban D, Şavlovschi C, et al (2012) Lipopolysaccharide binding protein (L.B.P.)--an inflammatory marker of prognosis in the acute appendicitis. J Med Life 5:342–347.
- Kudlova M, Kunes P, Kolackova M, et al (2007) Lipopolysaccharide Binding Protein and sCD14 are Not Produced as Acute Phase Proteins in Cardiac Surgery. Mediators Inflamm 2007:72356. [CrossRef]
- Liu Z, Ukomadu C (2008) Fibrinogen-like protein 1, a hepatocyte derived protein is an acute phase reactant. Biochem Biophys Res Commun 365:729–734. [CrossRef]
- Rijken DC, Dirkx SPG, Luider TM, Leebeek FWG (2006) Hepatocyte-derived fibrinogen-related protein-1 is associated with the fibrin matrix of a plasma clot. Biochem Biophys Res Commun 350:191–194. [CrossRef]
- Chen H, Yang J, Zhang S, et al (2019) Serological cytokine profiles of cardiac rejection and lung infection after heart transplantation in rats. J Cardiothorac Surg 14:26. [CrossRef]
- Zhang Q, Huang R, Tang Q, et al (2018) Leucine-rich alpha-2-glycoprotein-1 is up-regulated in colorectal cancer and is a tumor promoter. Onco Targets Ther 11:2745–2752. [CrossRef]
- Shirai R, Hirano F, Ohkura N, et al (2009) Up-regulation of the expression of leucine-rich α2-glycoprotein in hepatocytes by the mediators of acute-phase response. Biochem Biophys Res Commun 382:776–779. [CrossRef]
- Gao Y, Zhou J, Xie Z, et al (2019) Mechanical strain promotes skin fibrosis through LRG-1 induction mediated by ELK1 and ERK signalling. Commun Biol 2:359. [CrossRef]
- Banfi C, Parolari A, Brioschi M, et al (2010) Proteomic Analysis of Plasma from Patients Undergoing Coronary Artery Bypass Grafting Reveals a Protease/Antiprotease Imbalance in Favor of the Serpin α1-Antichymotrypsin. J Proteome Res 9:2347–2357. [CrossRef]
- Hack CE, Abbink JJ, Nuijens JH (1990) [Serine protease inhibitors (serpins); regulators of coagulation and inflammation reactions with therapeutic potential]. Ned Tijdschr Geneeskd 134:1035–1039.
- Dai E, Guan H, Liu L, et al (2003) Serp-1, a Viral Anti-inflammatory Serpin, Regulates Cellular Serine Proteinase and Serpin Responses to Vascular Injury *. J Biol Chem 278:18563–18572. [CrossRef]
- Bergin DA, Hurley K, McElvaney NG, Reeves EP (2012) Alpha-1 Antitrypsin: A Potent Anti-Inflammatory and Potential Novel Therapeutic Agent. Arch Immunol Ther Exp (Warsz) 60:81–97. [CrossRef]
- Radovani B, Gudelj I (2022) N-Glycosylation and Inflammation; the Not-So-Sweet Relation.
Figure 1.
Propofol exposure affects the plasma proteome pre- versus post operation. Volcano plot showing changes in protein abundance levels between PROP-T2 vs. PROP-T0. Abundance thresholds are set to 1 and -1 (log2), respectively. A multiple test correction (MTC) was applied to highlight plasma proteins with significantly altered levels (marked as red dots).
Figure 1.
Propofol exposure affects the plasma proteome pre- versus post operation. Volcano plot showing changes in protein abundance levels between PROP-T2 vs. PROP-T0. Abundance thresholds are set to 1 and -1 (log2), respectively. A multiple test correction (MTC) was applied to highlight plasma proteins with significantly altered levels (marked as red dots).
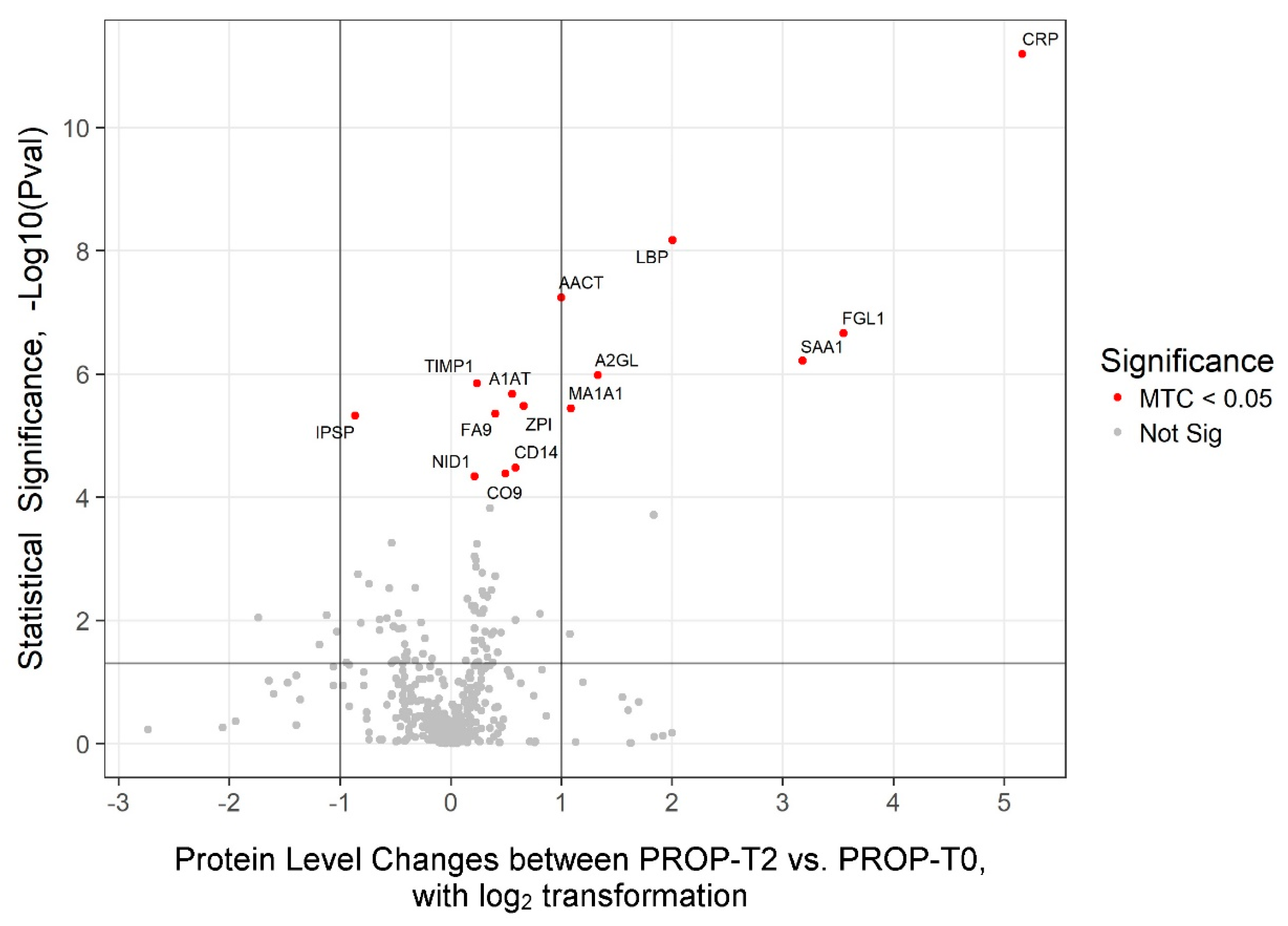
Figure 2.
Sevoflurane exposure affects the plasma protein pre- versus post-operation. Volcano plot showing changes in protein abundance levels between SEVO-T2 vs. SEVO-T0. Abundance thresholds are set to 1 and -1 (log2), respectively. A multiple test correction (MTC) was applied to highlight plasma proteins with significantly altered levels (marked as red dots).
Figure 2.
Sevoflurane exposure affects the plasma protein pre- versus post-operation. Volcano plot showing changes in protein abundance levels between SEVO-T2 vs. SEVO-T0. Abundance thresholds are set to 1 and -1 (log2), respectively. A multiple test correction (MTC) was applied to highlight plasma proteins with significantly altered levels (marked as red dots).
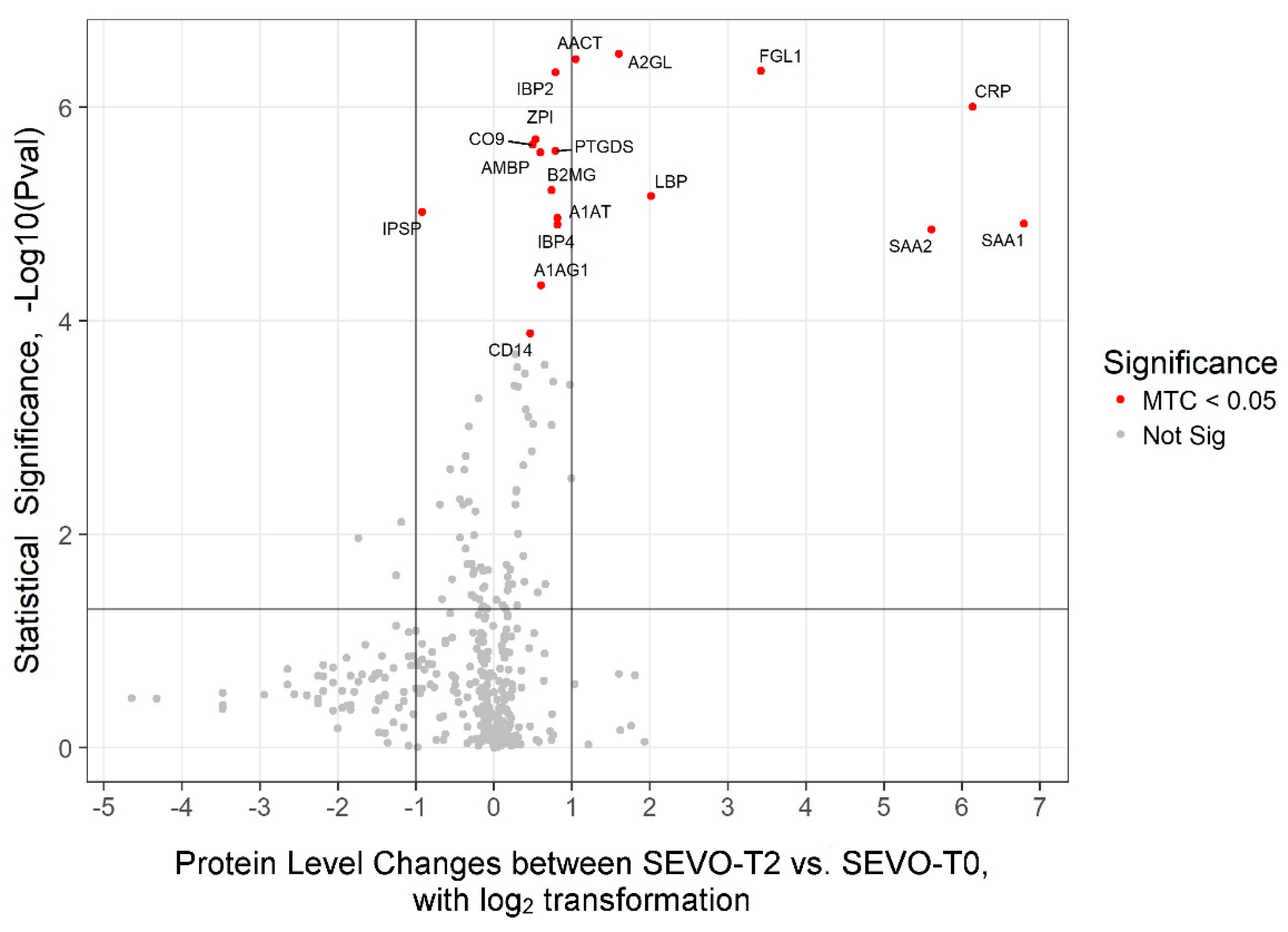
Figure 3.
Global changes in plasma proteome levels induce by exposure to both anaesthetics. Proteome levels of C-reactive proteins (CRP) (A) and serum amyloid-A1 (SAA1) (B) in both propofol and sevoflurane at three time points. ELISA validation of CRP (C) and SAA-1 (D) proteome levels in both propofol and sevoflurane at three time points.
Figure 3.
Global changes in plasma proteome levels induce by exposure to both anaesthetics. Proteome levels of C-reactive proteins (CRP) (A) and serum amyloid-A1 (SAA1) (B) in both propofol and sevoflurane at three time points. ELISA validation of CRP (C) and SAA-1 (D) proteome levels in both propofol and sevoflurane at three time points.
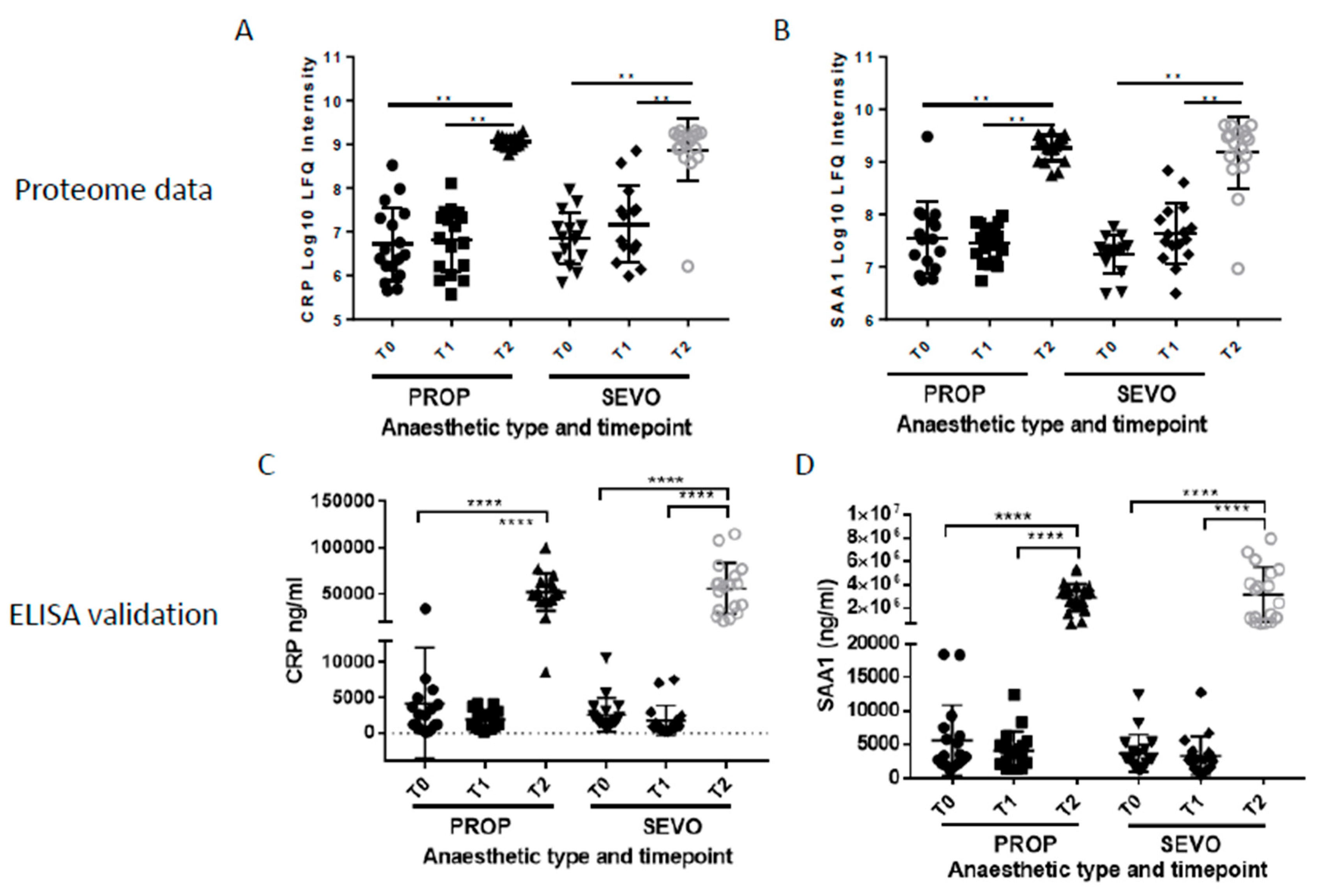

Table 1.
Patients’ demographics and peri-operative data in PROP and SEVO anaesthesia groups. Data are given as n (%), mean (SD) or median (IQR).
Table 1.
Patients’ demographics and peri-operative data in PROP and SEVO anaesthesia groups. Data are given as n (%), mean (SD) or median (IQR).
| PROP n=19 |
SEVO n=17 |
P |
|
|---|---|---|---|
| Baseline characteristics | |||
| Age y | 49.6 (13.2) | 33.8 (10.6) | 0.297 |
| Male n (%) | 10 (53%) | 9 (53%) | >0.999 |
| BMI kg/m2 | 25.9 (3.6) | 27.4 (3.5) | 0.233 |
| ASA I/II | 15/4 | 11/6 | 0.463 |
| mGFR ml/kg | 125 (98-140) | 107 (97-132) | 0.364 |
| Smoking n (%) | 7 (37%) | 5 (30%) | 0.728 |
| CCI Cardiovascular comorbidity n (%) |
1 (0-2) 1 (5%) |
1 (0-1) 5 (29%) |
0.620 0.080 |
| MAP baseline mmHg | 93 (90-96) | 94 (85-104) | 0.863 |
| Perioperative data | |||
| Duration procedure min | 230 (28.4) | 245 (42.5) | 0.196 |
| Amount of fluid ml/kg BW | 61.5 (10.0) | 60.2 (11.7) | 0.730 |
| BIS | 39 (7) | 45 (6) | 0.012 |
| Blood sample clip renal artery | |||
| pH | 7.41 (0.04) | 7.39 (0.04) | 0.146 |
| PaO2 kPa | 20.3 (4.9) | 20.4 (4.7) | 0.955 |
| Hemoglobin mmol/l | 7.2 (0.9) | 7.3 (1.0) | 0.725 |
| Lactate mmol/l | 1.3 (0.5) | 1.7 (0.7) | 0.044 |
| Anaesthetics/analgesics | |||
| Propofol Cet (ug/ml) | 3.3 (0.5) | - | - |
| Sevoflurane EtC | - | 1.53 (0.14) | - |
| Remifentanil Cet (ng/ml) | 3.2 (0.86) | 2.6 (0.63) | 0.020 |
| Vasoactive medication | |||
| Ephedrine n (%) | 13 (68%) | 17 (100%) | 0.020 |
| Dose mg | 15 (10-20) | 15 (10-30) | 0.207 |
| Phenylephrine n (%) | 2 (11%) | 1 (6%) | >0.999 |
| Dose ug | 150 (100-200) | 100 | n too small |
| Other medication | |||
| Piritramide intraoperative mg | 8 (7.0-9.0) | 7.5 (7.0-8.5) | 0.901 |
| Piritramide postoperative mg | 12 (10.0-16.0) | 11 (8.5-19.0) | 0.688 |
| Ondansetron intraoperative n(%) | 2 (11%) | 8 (47%) | 0.025 |
| Ondansetron PACU n (%) | 8 (42%) | 3 (18%) | 0.156 |
| Dexamethasone n (%) | 2 (11%) | 3 (18%) | 0.650 |
| Droperidol n (%) | 1 (5%) | 1 (6%) | >0.999 |
| Postoperative complications | 2 (10%) | 0 (0%) | 0.487 |
| LOH d | 5 (5-7) | 5 (5-7,5) | 0.912 |
n: number in group; BMI: body mass Index; ASA: classification American Society for Anaesthesiology; mGFR: Glomerular Filtration Rate measured by isotope 125I-iothalamate; CCI; Charlson comorbidity index; MAP: Mean Arterial Pressure; BW: Body weight BIS: bispectral index; Cet: effect side concentration; EtC: end tidal concentration; PACU: post anaesthetic care unit; LOH: length of hospital stay; d:days.
Table 2.
Proteins displaying plasma level changes in patients stratified by the type of anaesthesia (PROP and SEVO) between time points T2-vs-T0.
Table 2.
Proteins displaying plasma level changes in patients stratified by the type of anaesthesia (PROP and SEVO) between time points T2-vs-T0.
| UniProt ID | Gene | Protein | PROP (T2-vs-T0) | SEVO (T2-vs-T0) | ||||
|---|---|---|---|---|---|---|---|---|
| MTC level | P-value | Fold change | MTC level | P-value | Fold change | |||
| P02763 | A1AG1 | Alpha-1-acid glycoprotein 1 | - | - | - | P<0.05 | 4,60E-05 | 1,52 |
| P01009 | A1AT | Alpha-1-antitrypsin | P<0.01 | 2,10E-06 | 1,47 | P<0.01 | 1,10E-05 | 1,76 |
| P02750 | A2GL | Leucine-rich alpha-2-glycoprotein | P<0.01 | 1,00E-06 | 2,51 | P<0.01 | 3,20E-07 | 3,04 |
| P01011 | AACT | Alpha-1-antichymotrypsin | P<0.01 | 5,70E-08 | 2 | P<0.01 | 3,50E-07 | 2,07 |
| P02760 | AMBP | Protein AMBP | - | - | - | P<0.01 | 2,60E-06 | 1,51 |
| P61769 | B2MG | Beta-2-microglobulin | - | - | - | P<0.01 | 6,00E-06 | 1,67 |
| P08571 | CD14 | Monocyte differentiation antigen CD14 | P<0.05 | 3,30E-05 | 1,5 | P<0.05 | 1,30E-04 | 1,38 |
| P02748 | CO9 | Complement component C9 | P<0.05 | 4,10E-05 | 1,41 | P<0.01 | 2,20E-06 | 1,41 |
| P02741 | CRP | C-reactive protein | P<0.01 | 6,40E-12 | 35,83 | P<0.01 | 9,90E-07 | 70,09 |
| P00740 | FA9 | Coagulation factor IX | P<0.01 | 4,40E-06 | 1,32 | - | - | - |
| Q08830 | FGL1 | Fibrinogen-like protein 1 | P<0.01 | 2,20E-07 | 11,69 | P<0.01 | 4,50E-07 | 10,69 |
| P18065 | IBP2 | Insulin-like growth factor-binding protein 2 | - | - | - | P<0.01 | 4,70E-07 | 1,73 |
| P22692 | IBP4 | Insulin-like growth factor-binding protein 4 | - | - | - | P<0.01 | 1,30E-05 | 1,76 |
| P05154 | IPSP | Plasma serine protease inhibitor | P<0.01 | 4,80E-06 | -1,82 | P<0.01 | 9,50E-06 | -1,89 |
| P18428 | LBP | Lipopolysaccharide-binding protein | P<0.01 | 6,60E-09 | 4,01 | P<0.01 | 6,80E-06 | 4,04 |
| P33908 | MAN1A1 | Mannosyl-oligosaccharide 1,2-alpha-mannosidase IA |
P<0.01 | 3,60E-06 | 2,12 | - | - | - |
| P14543 | NID1 | Nidogen-1 | P<0.05 | 4,60E-05 | 1,16 | - | - | - |
| P41222 | PTGDS | Prostaglandin-H2 D-isomerase | - | - | - | P<0.01 | 2,60E-06 | 1,73 |
| P0DJI8 | SAA1 | Serum amyloid A-1 protein | P<0.01 | 6,10E-07 | 9,05 | P<0.01 | 1,20E-05 | 110,69 |
| P0DJI9 | SAA2 | Serum amyloid A-2 protein | - | - | - | P<0.01 | 1,40E-05 | 48,67 |
| P01033 | TIMP1 | Metalloproteinase inhibitor 1 | P<0.01 | 1,40E-06 | 1,18 | - | - | - |
| Q9UK55 | ZPI | Protein Z-dependent protease inhibitor | P<0.01 | 3,30E-06 | 1,58 | P<0.01 | 2,00E-06 | 1,45 |
Table 3.
Changes in plasma proteomic profile independent of the anaesthesia type (PROP or SEVO). Listed in the table are proteins displaying statistically significant (MTC P-value<0.05) plasma level changes in at least one of the comparisons T2-vs-T0, T2-vs-T1, or T1-vs-T0 in the combined patient cohort of this study (36 patients including 19 PROP and 17 SEVO anaesthesia cases).
Table 3.
Changes in plasma proteomic profile independent of the anaesthesia type (PROP or SEVO). Listed in the table are proteins displaying statistically significant (MTC P-value<0.05) plasma level changes in at least one of the comparisons T2-vs-T0, T2-vs-T1, or T1-vs-T0 in the combined patient cohort of this study (36 patients including 19 PROP and 17 SEVO anaesthesia cases).
| ALL T2-T0 | ALL T2-T1 | ALL T1-T0 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UniPro ID |
Gene | Protein | MTC | P-value | Fold change |
Direction | MTC | P-value | Fold change |
Direction | MTC | P-value | Fold change |
Direction |
| P02741 | CRP | C-reactive protein | P<0.01 | 2,7E-16 | 46,42 | UP | P<0.01 | 2,4E-14 | 22,61 | UP | - | - | - | - |
| P01011 | AACT | Alpha-1-antichymotrypsin | P<0.01 | 3,4E-14 | 2,03 | UP | P<0.01 | 2,9E-13 | 1,93 | UP | - | - | - | - |
| P18428 | LBP | Lipopolysaccharide-binding protein | P<0.01 | 1,5E-13 | 4,04 | UP | P<0.01 | 1,8E-09 | 3,73 | UP | - | - | - | - |
| Q08830 | FGL1 | Fibrinogen-like protein 1 | P<0.01 | 1,6E-13 | 11,76 | UP | P<0.01 | 6,8E-11 | 8,48 | UP | - | - | - | - |
| P02750 | A2GL | Leucine-rich alpha-2-glycoprotein | P<0.01 | 7,2E-13 | 2,74 | UP | P<0.01 | 7,9E-12 | 2,63 | UP | - | - | - | - |
| Q9UK55 | ZPI | Protein Z-dependent protease inhibitor | P<0.01 | 3,1E-11 | 1,52 | UP | P<0.01 | 3,5E-08 | 1,41 | UP | - | 4,3E-02 | 1,08 | UP |
| P0DJI8 | SAA1 | Serum amyloid A-1 protein | P<0.01 | 5,7E-11 | 17,69 | UP | P<0.01 | 2,2E-11 | 32,42 | UP | - | - | - | - |
| P05154 | IPSP | Plasma serine protease inhibitor | P<0.01 | 1,0E-10 | 1,85 | DOWN | P<0.01 | 8,1E-09 | 1,69 | DOWN | - | - | - | - |
| P01009 | A1AT | Alpha-1-antitrypsin | P<0.01 | 3,2E-10 | 1,61 | UP | P<0.01 | 1,2E-11 | 2,09 | UP | P<0.05 | 8,8E-05 | 1,3 | DOWN |
| P02748 | CO9 | Complement component C9 | P<0.01 | 4,2E-10 | 1,41 | UP | P<0.01 | 3,1E-07 | 1,25 | UP | - | 9,3E-03 | 1,13 | UP |
| P00740 | FA9 | Coagulation factor XI | P<0.01 | 6,7E-09 | 1,32 | UP | - | 1,5E-02 | 1,1 | UP | P<0.05 | 2,8E-05 | 1,2 | UP |
| P0DJI9 | SAA2 | Serum amyloid A-2 protein | P<0.01 | 9,1E-09 | 4,58 | UP | P<0.01 | 2,7E-09 | 16,47 | UP | - | - | - | - |
| P33908 | MAN1A1 | Mannosyl-oligosaccharide 1,2-alhpa-mannosidase IA | P<0.01 | 1,0E-08 | 1,93 | UP | P<0.05 | 6,2E-05 | 1,63 | UP | - | - | - | - |
| P08571 | CD14 | Monocyte differentiation antigen CD14 | P<0.01 | 1,1E-08 | 1,44 | UP | P<0.01 | 1,2E-06 | 1,38 | UP | - | - | - | - |
| P18065 | IBP2 | Insulin-like growth factor-binding protein 2 | P<0.01 | 1,2E-08 | 1,38 | UP | P<0.01 | 2,9E-07 | 1,47 | UP | - | 2,6E-02 | 1,06 | DOWN |
| P15169 | CBPN | Carboxy peptidase N catalytic chain | P<0.01 | 1,9E-06 | 1,25 | UP | - | 8,0E-04 | 1,22 | UP | - | - | - | - |
| P02760 | AMBP | Protein AMBP | P<0.01 | 2,9E-06 | 1,4 | UP | P<0.05 | 2,6E-05 | 1,22 | UP | - | - | - | - |
| P01033 | TIMP1 | Metalloproteinase inhibitor 1 | P<0.01 | 3,2E-06 | 1,23 | UP | P<0.01 | 1,4E-05 | 1,24 | UP | - | - | - | - |
| P36955 | PEDF | Pigment epithelium-derived factor | P<0.01 | 3,3E-06 | 1,27 | UP | P<0.01 | 1,1E-06 | 1,21 | UP | - | - | - | - |
| P05019 | IGF1 | Insulin-like growth factor I | P<0.01 | 8,5E-06 | 1,25 | UP | - | - | - | - | - | 1,3E-02 | 1,14 | UP |
| P04004 | VTNC | Vitronectin | P<0.01 | 1,4E-05 | 1,22 | UP | - | - | - | - | - | 2,0E-02 | 1,13 | UP |
| P49747 | COMP | Cartilage oligomeric matrix protein | P<0.01 | 1,5E-05 | 1,47 | DOWN | - | 1,6E-02 | 1,2 | DOWN | - | 7,1E-04 | 1,2 | DOWN |
| P00748 | FA12 | Coagulation factor XII | P<0.05 | 2,6E-05 | 1,32 | DOWN | - | 1,5E-03 | 1,27 | DOWN | - | - | - | - |
| P02787 | TRFE | Serotransferrin | P<0.05 | 3,2E-05 | 1,54 | DOWN | - | - | - | - | - | 7,0E-03 | 1,3 | DOWN |
| P02763 | A1AG1 | Alpha-1-acid glycoprotein 1 | P<0.05 | 3,4E-05 | 1,38 | UP | P<0.01 | 3,3E-10 | 1,7 | UP | - | 2,6E-02 | 1,23 | DOWN |
| Q86UD1 | OAF | Out at first protein homolog | P<0.05 | 4,1E-05 | 1,87 | UP | P<0.01 | 8,1E-06 | 1,67 | UP | - | - | - | - |
| P02649 | APOE | Apolipoprotein E | P<0.05 | 8.0E-05 | 1,25 | UP | - | - | - | - | P<0.01 | 6,5E-06 | 1,31 | UP |
| P22792 | CPN2 | Carboxy peptidase N subunit 2 | P<0.05 | 8,3E-05 | 1,16 | UP | - | - | - | - | - | - | - | - |
| Q92820 | GGH | Gamma-glutamyl hydrolase | - | 1,5E-04 | 1,15 | UP | - | - | - | - | P<0.05 | 9,0E-05 | 1,15 | UP |
| P14543 | NID1 | Nidogen-1 | - | 2,5E-04 | 1,05 | UP | P<0.01 | 3,2E-10 | 1,08 | UP | - | - | - | - |
| P05160 | F13B | Coagulation factor XIII B chain | - | 1,9E-03 | 1,39 | DOWN | P<0.05 | 7,9E-06 | 1,59 | DOWN | - | - | - | - |
| P22352 | GPX3 | Glutathione peroxidase 3 | - | 2,8E-03 | 1,2 | UP | - | - | - | - | P<0.01 | 6,5E-06 | 1,3 | UP |
| Q06033 | ITIH3 | Inter-alpha-trypsin inhibitor heavy chain H3 | - | 1,2E-02 | 1,17 | UP | P<0.01 | 1,9E-07 | 1,19 | UP | - | - | - | - |
| P22105 | TENX | Tenascin-X | - | 4,0E-02 | 1,14 | UP | - | - | - | - | P<0.05 | 2,7E-05 | 1,35 | UP |
| O75636 | FCN3 | Ficolin-3 | - | - | - | - | - | 4,2E-03 | 1,19 | DOWN | P<0.05 | 5,0E-05 | 1,26 | UP |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



