
Submitted:
05 April 2025
Posted:
08 April 2025
You are already at the latest version
Abstract
Gliomas diagnosed during pregnancy are rare and there are no established guidelines for their management. Effective treatment requires a multidisciplinary approach to balance maternal health and pregnancy preservation. We here present a case of rapidly progressing glioma in a 33-year-old pregnant woman. The patient initially presented with a generalized tonic-clonic seizure at 21 weeks' gestation. Imaging revealed a tumor in the right cerebral lobe, involving both cortical and subcortical structures, while magnetic resonance spectroscopy suggested a low-grade glioma. The patient remained clinically stable for two months, but then developed severe headaches; MRI showed a worsening mass effect. At 34 weeks' gestation, an emergency and premature caesarean section was performed under general anesthesia. The patient then underwent a craniotomy for maximal tumor resection, which was histologically and molecularly diagnosed as IDH wild-type glioblastoma. Using qPCR, we found that the glioblastoma tissue showed upregulated expression of genes involved in cell structure (GFAP, VIM) and immune response (SSP1, TSPO), as well as increased expression of genes related to potential hormone response (AR, CYP19A1, ESR1, GPER1). After surgery, the patient showed resistance to Stupp protocol therapy and is currently receiving combination therapy with lomustine and bevacizumab. This case illustrates the aggressive nature and rapid progression of glioblastoma during pregnancy.
Keywords:
pregnancy
; brain cancer
; magnetic resonance spectroscopy
; glioblastoma therapy
; maternal-fetal outcome
1. Introduction
The diagnosis of glioma tumors during pregnancy is rare and there are no specific guidelines for its treatment. Instead, clinicians rely on limited case reports or small retrospective studies to guide their clinical approach and determine the optimal timing for tumor surveillance and treatment. Glioblastoma (GB) represents 14% of all primary brain tumors, but it is the most prevalent malignant form of both primary brain tumors and gliomas, comprising 51% and 60% of these categories, respectively [1]. The incidence of GB varies depending on the geographical region and is between 0.59 and 3.69 per 100,000 people, with men being affected more frequently (1.6 times higher incidence) [2]. Since 2005, the Stupp protocol is the standard of care for patients with newly diagnosed GB [3]. This protocol usually involves surgical resection of the tumor as far as possible, followed by tumor-focused radiotherapy and chemotherapy with temozolomide, which is administered daily during radiotherapy and continued over several cycles after radiotherapy has finished. Even under this protocol the median overall survival for GB patients is generally poor, typically around 14 – 16 months [2]. Although attempts have been made to develop new therapeutic approaches such as immunotherapies and vaccines, there have been no significant advances that would substantially improve the life expectancy of GB patients.
The coexistence of pregnancy and glioma requires a multidisciplinary medical team to create an optimal treatment plan for the management of the pregnancy and eradication of the tumor, tailored to the patient's priorities and preferences. This plan may aim to deliver a healthy baby, even if it means delaying glioma treatment until after pregnancy, or it may prioritize aggressive glioma treatment, possibly at the expense of fetal survival [4]. To the best of our knowledge, the last study investigating the incidence of primary brain tumors in pregnant versus non-pregnant women was published in 1987 [5], reporting a similar incidence of gliomas. Several studies have investigated the effects of pregnancy on WHO grade II and III gliomas, as well as GB and vice versa, examining both the cases where the first symptoms of the tumor occurred during pregnancy, as well as those in which the tumor was diagnosed before pregnancy [4,6,7,8,9]. Overall, regardless of the timing of tumor diagnosis these studies came to the conclusion that pregnancy is positively correlated with clinical deterioration. Tumor progression during pregnancy was more likely to be associated with gliomas that had a high grade of malignancy, immunonegative expression of alpha-internexin, or immunopositive expression of p53 [7]. Furthermore, tumor growth progression was quantitatively confirmed by an increased rate of diametric expansion observed in consecutive magnetic resonance images of pregnant patients [9]. In the study of Peters et al. it was noted that 83% of gliomas diagnosed during pregnancy were discovered in the second or third trimesters, with seizures being the presenting symptom in 68% of cases [7].
All of these reports clearly indicate that pregnant patients with a new or prior diagnosis of glioma should be informed that pregnancy may significantly increase the risk of tumor progression. However, with careful management and close monitoring, a favorable outcome of pregnancy is possible and healthy babies were born in the majority of cases [10].
Here we present a newly diagnosed glioma in a pregnant woman at the end of the second trimester whose symptoms worsened in 32nd week of gestation, leading to premature caesarean section and surgical removal of the tumor, which was confirmed as a WHO grade IV IDH wild-type GB.
2. Case Description and Discussion
2.1. Anamnesis
A 33-year-old woman with a predisposition to thrombophilia due to genetic mutations became pregnant after the second attempt at IVF. She was admitted to the clinic after the first neurological symptom: a generalised tonic-clonic seizure at the 21st week of pregnancy. The patient was awake and responsive, without signs of neurological deficits and the electroencephalogram was in the physiological range. The patient had no personal or family history of neurological disease or brain tumors. Of the pre-existing conditions, only mild myopia was reported. Apart from subcutaneous enoxaparin sodium (40 mg/day) and vaginal progesterone (600 mg/day) from IVF onwards, no long-term medication was reported. The further course of her condition is outlined in Figure 1.
2.2. Symptom Development, Imaging and Surgical Intervention
Although antiepileptic drugs carry a risk of congenital malformations, untreated seizures during pregnancy pose a significantly higher risk for mother and fetus [11]. Treatment is therefore essential as the benefits are generally considered to outweigh the potential risks. The patient was started on a monotherapy with levetiracetam, a first-line treatment considered safe for both general and tumor-induced epilepsy during pregnancy [12]. Antiepileptic drugs, including levetiracetam, are associated with an increased risk of neural tube defects in the developing fetus and it is important to note that the patient was already supplementing folic acid [12,13]. The first MRI, performed after the first seizure, showed a hyperintense T2-weighted and FLAIR lesion involving the right frontal cortex, insula, with additional involvement of the temporal cortex, the head of the caudate nucleus, the body of the corpus callosum and the right thalamus. The lesion appeared isointense on T1-weighted imaging. No significant changes were detected on the second and the third MRI examination (T2-weighted MRI shown in Figure 2a) performed at 24 weeks' gestation. Due to two additional seizures that occurred up to the 25th week of pregnancy (manifested by stiffness of the lower jaw, tingling of the tongue and left arm) the initial dose of levetiracetam was gradually increased from 1000 mg to 3000 mg daily. Enoxaparin sodium was continued.
The third MRI examination was accompanied by an analysis of the chemical composition of the tumor with a single and 2D multivoxel MR spectroscopy, which revealed a slight increase in the choline/creatine ratio (Cho/Cr=1.49-1.53 - the highest registered value) together with a decrease in the N-acetylaspartate/creatine (NAA/Cr=0.92-1.27) and choline/N-acetylaspartate ratios (Cho/NAA=1.19-1.62), while myoinositol levels remained within the reference range (mI/Cr=0.61). Although these metabolic changes suggest altered cell metabolism or membrane turnover, some loss of neurons and an unaffected glial cell component, their extent is consistent with a low-grade glioma. Due to concerns regarding pregnancy and fetal safety, MRI was performed without contrast, as this is the technique of choice for monitoring a pregnant patient diagnosed with a brain tumor [10]. Therefore, as gadolinium enhancement was not performed on our patient, there is a possibility that alternative diagnose could be made. In pregnant patients with newly diagnosed glioma, surgery in the second trimester may be recommended if necessary [4]. This is because surgery in the first trimester poses a high risk to fetal survival, while surgery in the third trimester increases the risk of significant intraoperative bleeding [4,11]. Given the patient's condition, the imaging results and the fact that her first neurosurgical consultation was towards the end of the second trimester, emergency neurosurgical intervention was not warranted at the time. However, intensive antenatal and neurological monitoring was recommended along with symptomatic treatment, with definitive treatment delayed until after birth.
Regarding the etiology of the glioma, which remains unknown in most cases, the patient stated that she had not been exposed to high doses of ionizing radiation in the past, the only external risk factor known to be associated with this type of brain tumor [14]. She also denied any previous exposure to cranial diagnostic radiation (computed tomography), which, in childhood or before the age of 22, is a factor that could increase the risk of developing glioma [15].
The first next symptom developed at 32 weeks' gestation, and presented as a tension-type headache during a routine visit to the obstetric clinic. The headache was characterized by generalized pain that did not respond to paracetamol but was not accompanied by other symptoms like nausea or vomiting. The deterioration occurred between the 24th and 32nd weeks of gestation, coinciding with the period when pregnancy-related hemodynamic changes reach their peak [16]. During this period, increased blood volume and cardiac output together with decreased systemic vascular resistance support the metabolic demands of pregnancy and fetal development. However, these changes also lead to an increase in maternal cerebral blood flow, which may promote tumor vascularization, the formation of peritumoral edema and the progression of the tumor itself [16,17]. Moreover, the production of certain growth factors by the placenta, including placental growth factor, vascular endothelial growth factor and insulin-like growth factors, peaks in the second trimester and remains elevated throughout the duration of pregnancy. These factors are known to promote angiogenesis, glioma cell migration and tumor growth in GB. Therefore, they also may play a role in the progression of GB during pregnancy.
The MRI scan followed at the 33rd week of pregnancy (Figure 2b), revealing the progressive mass effect. The lesion has enlarged significantly, resulting in perilesional edema and compressive effects on the ventricular system with a pronounced shift to the left. This was accompanied by subfalcine herniation, dilatation of the left lateral ventricle, initial transependymal cerebrospinal fluid resorption and diffuse cerebral edema. An emergency surgical intervention was scheduled following the caesarean section.
Corticosteroids were administered to promote lung maturity in the fetus and the baby was delivered by caesarean section under general anesthetic at 34 weeks' gestation. The delivery was uneventful, the baby cried spontaneously and achieved an Apgar score of 9 at both one and ten minutes after birth. Five days after delivery and three months after the initial symptom, the patient underwent a craniotomy for maximal surgical resection of the tumor. Total resection was not possible due to the infiltration of deep brain structures. The operation was successful and the postoperative course was uneventful, with stable vital signs and no complications.
2.3. Pathology and Molecular Analysis
Histopathological analysis of the tumor showed poorly differentiated, primitive looking cells, significant microvascular proliferation, abnormal mitotic activity and moderate necrosis (Figure 3a, b). Immunohistochemistry revealed positive staining for GFAP (Figure 3c), Olig2, Vimentin, MAP2, p53 and retained H3K27me3. The tumor cells were negative for IDH-1 R132H, CDKN2A and synaptophysin. In addition, ATRX expression was preserved and the Ki-67 proliferation index was 30% (Figure 3d). PCR analysis indicated the absence of mutations in codon 132 of the IDH1 gene and in codons 140 and 172 of the IDH2 gene. Fluorescence in situ hybridisation with 1p36/1q25 and 19q13/19p13 probes revealed a loss of heterozygosity at 19q13 in the majority of neoplastic cells. Based on these results and according to the WHO 2021 classification for CNS tumors, the diagnosis of IDH wild-type GB, grade IV, was established.
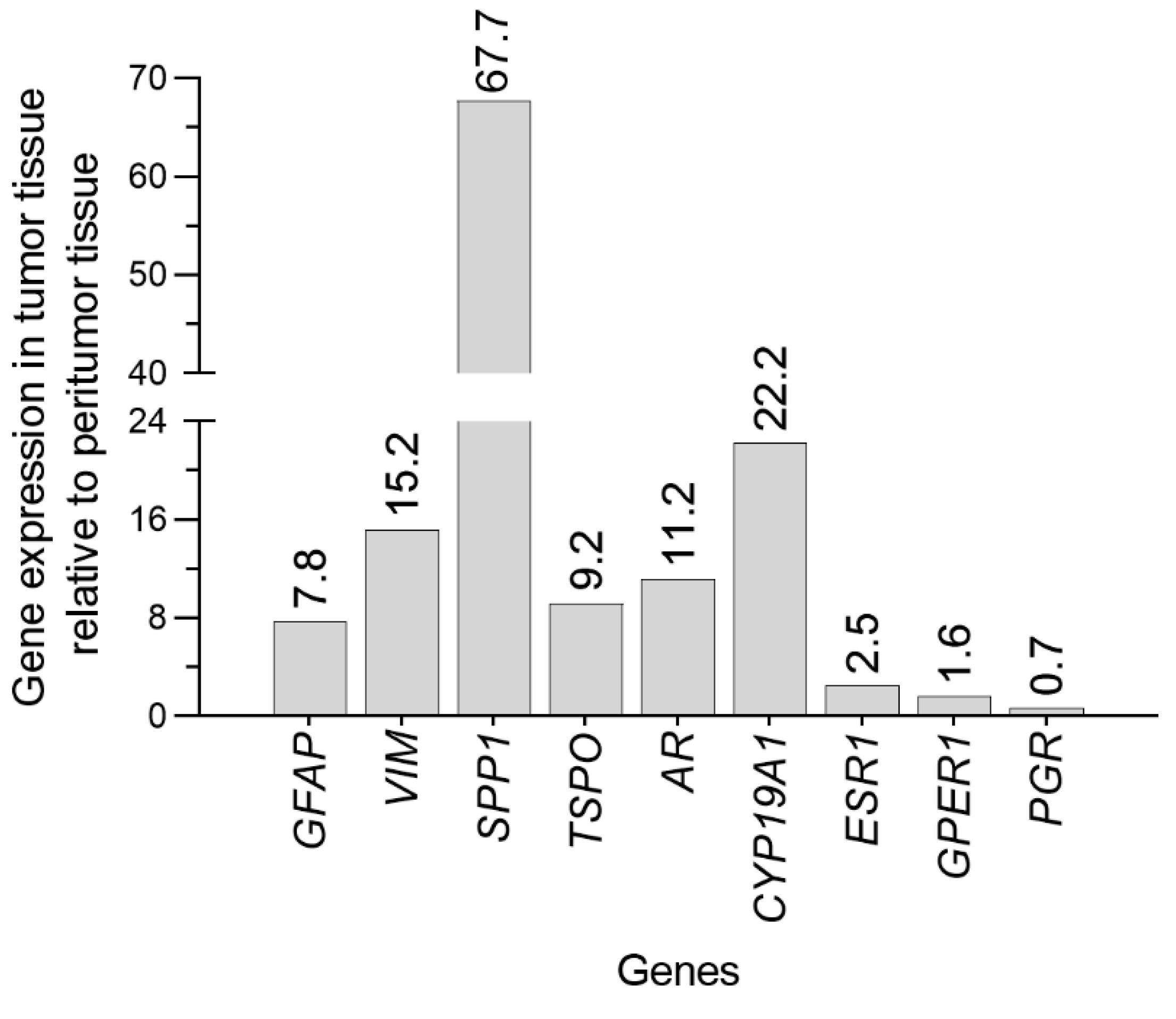
Given pregnancy-related hormonal changes, gene expression in signaling pathways related to hormonal regulation was analyzed using quantitative real-time PCR (qPCR) on both the tumor and surrounding tissue, aiming to explore potential hormonal influences on tumor behavior (Figure 4). The surrounding tissue sample is referred to here as peritumor tissue. To clearly distinguish between tumor and peritumor tissue, the expression of genes coding for proteins involved in cell structure and immune response, expected to be elevated in GB cells, such as GFAP, VIM, SPP1, and TSPO was estimated.
GFAP, an intermediate filament and a key component of the cytoskeleton in mature astrocytes, is also highly expressed in tumors of astrocytic origin, including GB, and is frequently used as an immunohistochemical marker for these tumors [18]. Interestingly, GFAP can even be detected in the plasma of GB patients [18]. However, its expression has been reported to correlate both positively and negatively with tumor malignancy [19]. In our report, we observed a clear difference in GFAP mRNA levels between tumor and peritumor sample, with GFAP expression being 8-fold higher in GB tissue (Figure 4). This finding is consistent with some reports of increased GFAP expression in GB, though the correlation with tumor aggressiveness remains debated. In addition, the expression of another intermediate filament VIM was 15- fold higher in the tumor than in the peritumor sample, which is consistent with previous results [20]. It is of note that, the elevate presence of VIM in GB indicates increased cell motility and invasiveness and is associated with tumor progression and poor clinical outcomes [21].
Our results also show SPP1 to be highly induced in GB tissue, with 68-fold higher expression than in peritumor tissue (Figure 4). Osteopontin, a glycophoshoprotein encoded by the SPP1 gene, is also a potent chemokine for macrophages and plays critical role in GB malignancy. Increased gene expression and levels of this protein have been shown to promote glioma cell migration, invasion and radioresistance [22,23]. Moreover, osteopontin drives the recruitment of M2 macrophages into the tumor, which can suppress the anti-tumor immune response and thus create a tumor-friendly environment [24]. Interestingly, hyper-phosphorylation of osteopontin has been shown to be associated with poorer survival only in female GB patients, suggesting potential sex-specific effects [25].
Furthermore, we observed TSPO gene expression to be upregulated in the GB tissue compared to peritumor tissue (Figure 4). TSPO, protein overexpressed in gliomas, especially in GB [26], is located on the outer mitochondrial membrane and plays a role in various cellular processes, including proliferation, apoptosis, migration and mitochondrial functions, many of which could contribute to GB promotion [27]. TSPO is also primarily expressed by microglia in the central nervous system and may be involved in a pro-tumoral immune response similar to osteopontin [26].
Overall, our results, showing a ≥ 9-fold higher expression of VIM, SPP1 and TSPO in tumor tissue compared to peritumor tissue, underline the aggressive nature of GB in our patient.
Although GB are not typically classified as hormone-sensitive cancers, significant gender differences have been observed, with males exhibiting a higher incidence and worse prognosis. These observations suggest that sex hormones, particularly androgens, may influence the development and progression of GB, while estrogens may exert a protective effect [28]. Since hormones mainly exert their effects via nuclear receptors, which act as transcription factors when activated, we have analyzed the level of gene expression of AR, ESR1 and PGR.
Our findings show an 11-fold higher AR mRNA levels in GB tissue versus peritumor tissue (Figure 4), which aligns with previous studies reporting increased AR gene expression (at least 2.5-fold) and elevated protein levels in GB biopsies relative to normal brain tissue [29,30,31]. Higher AR expression is positively correlated with glioma grade, being most pronounced in GB, and is associated with poorer survival across all glioma subtypes [30,32]. Activation of AR in the context of GB enhances the malignant properties of tumor cells, promotes an immunosuppressive tumor environment and contributes to radioresistance [31,33].
The relationship between female hormones and their receptors in GBs is more complex than that of androgens, as they have both protective and tumor-promoting effects, whereas androgens are primarily associated with tumor promotion. Previous studies on the expression of nuclear estrogen receptors (ERα and ERβ) in GB have produced conflicting results regarding their role in tumor progression and clinical outcomes. Some studies report higher mRNA levels of ERα and ERβ in GB compared to low-grade gliomas [34], while others observe an inverse correlation between protein levels and glioma grade [35]. Interestingly, increased expression of these receptors has been associated with both, poor clinical outcomes [34], and significantly longer survival in GB [36,37,38], highlighting the complexity of their role in tumor biology. In addition, studies have shown that estradiol can stimulate astrocytoma tumor growth via ERα [39], whereas ERβ appears to exert the opposite effect in human GB cell lines [40]. With regard to the GB and CYP19A1 gene, which codes for the aromatase that catalyzes the conversion of testosterone to estradiol as a last step in estradiol biosynthesis, the literature data are also divided. One study shows a correlation between high aromatase gene expression and a poor survival rate [37], while another study found a positive correlation between the level of the protein and a longer survival time [36]. In our study, we observed a 22-fold higher CYP19A1 expression in GB tissue compared to peritumor tissue, suggesting that aromatase may play a role in GB pathology (Figure 4). Clinical trials are currently underway on a new combination therapy for GB that contains the aromatase inhibitor letrozole [41]. These studies will clarify whether patients with high aromatase expression are eligible for this therapy. Additionally, we found 2.5-fold higher ESR1 (coding for ERα) expression in GB tissue compared to peritumor tissue, consistent with some reports suggesting increased estrogen receptor expression in GB (Figure 4). However, ESR2 (coding for ERβ) mRNA levels were low in both types of analyzed tissue (data not shown), as indicated by the Ct value beyond cycle 30. These findings may contribute to the ongoing debate about the role of estrogen receptors and aromatase in GB and emphasize the need for further research to clarify their impact on glioma biology and clinical outcomes. Besides nuclear receptors, estradiol can also interact with membrane-bound GPERs, triggering rapid activation of downstream signaling, which could be relevant in oncogenic environments. Hirtz et al. reported that high GPER expression in GB tissue from female patients is associated with a good prognosis, suggesting a potential protective role of GPER in GB [42]. In our study, we observed a modest increase in GPER1 expression in GB tissue compared to peritumor tissue (Figure 4).
Here, we registered a slight decrease in PGR expression in GB tissue compared to the surrounding tissue (Figure 4). This finding is of particular interest as Bello-Alvarez and Camacho-Arroyo reviewed the effects of progesterone on GB cells and concluded that low doses of progesterone (10 nM) have pro-tumorigenic effects, while higher doses (5–300 µM) show anti-tumorigenic effects [43]. The decreased PGR expression observed in GB tissue suggests that lower progesterone receptor activity may favor pro-tumorigenic signaling. Despite the increase in progesterone levels during pregnancy, pregnant glioma patients often experience accelerated disease progression, as in the case we report here [4,6,7,8,9]. This observation may suggest that reduced PGR expression in the tumor may limit the protective potential of progesterone. However, further studies are needed to clarify the exact role of progesterone signaling in glioma progression, especially in the context of hormonal changes during pregnancy.
2.3. Postoperative Course
Six weeks after the tumor resection, the MRI follow-up (Figure 2c) confirmed that the surgical resection was sufficient so that the patient could begin fractionated radiotherapy (60 Gy, 2 Gy/fraction) along with simultaneous chemotherapy with temozolomide (120 mg/day). The radiotherapy lasted six weeks; the chemotherapy was discontinued after five weeks due to grade 1 thrombocytopenia. One month after completion of radiotherapy, the patient developed severe right-sided headaches accompanied with nausea and vomiting. T2-weighted (Figure 2d) and FLAIR MRI showed a hyperintense lesion together with a centrally located FLAIR hypointensity, indicating recurrence of the tumor with significant growth, infiltration of deep brain structures and necrosis. Due to the spread of the tumor into deep brain structures, surgical reoperation was not indicated. Adjuvant temozolomide treatment was discontinued and the patient was started on anti-edema therapy. Secondary chemotherapy was initiated, so far consisting of two cycles of lomustine (80 mg, administered orally every six weeks) in combination with off-label bevacizumab (10 mg/kg, administered intravenously every two weeks). The treatment plan is to continue this regimen as long as the glioblastoma remains under control with manageable side effects. At the time of writing, the patient was stable, functional and without significant neurological deficits.
3. Conclusions
This case illustrates the rapid progression of a GB in a patient diagnosed during pregnancy after IVF treatment. MR spectroscopy initially suggested a low-grade glioma that later transformed into a GB, emphasizing the limitations of imaging and spectroscopy in predicting glioma progression. This transformation is not uncommon, especially when genetic instability or mutations drive rapid tumor development. The gradual changes in MR spectroscopy may have been too subtle to detect the impending transformation to GBM. In addition, early stage GBs may have relatively low metabolic activity, as reflected by Cho/Cr and Cho/NAA ratios, before more pronounced features such as necrosis, vascularity and rapid cell division appear.
Our study highlights the possibility of significant tumor progression over a two-month period during which the patient was treated with antiepileptic drugs and was in a stable clinical state with no obvious symptoms. Notably, this progression coincided with pregnancy period, during which hemodynamic changes and placental production of growth factors might have contributed to tumor growth. In addition, the patient's resistance to therapy after resection suggests that increased gene expression of osteopontin and AR in GB tissue could serve as a potential marker for radioresistance, a hypothesis that requires further investigation.
In terms of hormone sensitivity, AR and aromatase are of particular interest as their altered gene expression is striking and may play a role in GB pathology and could be future therapeutic targets. In conclusion, we emphasize that this case confirms previous findings that patients diagnosed with glioma during pregnancy may experience worsening of the disease but can still successfully give birth to a healthy child, thus contributing to the body of knowledge on the treatment of glioma during pregnancy.
Author Contributions
Conceptualization, I.B, D.S. and V.B.; methodology, A.K., R.I. and M.M.J; data curation, I.B, R.I, A.M. and F.M.; writing - original draft preparation, I.B., I.M.B., D.S. and V.B.; writing - review and editing, I.B., R.I., A.K., A.M., F.M., M.M.J., I.M.B., D.S. and V.B.; supervision V.B.; All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Ministry of Science, Technological Development and Innovation of the Republic of Serbia, Contract No. 451-03-136/2025-03/200007.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. As this is an individual case report, review and approval by the institutional ethics committee was not required, provided informed consent was obtained from the patient.
Informed Consent Statement
Written informed consent has been obtained from the patient for involvement in the study and to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author, but will not be made publicly available to protect the privacy of patient.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| AR | Androgen receptor |
| ATRX | Alpha-thalassemia/mental retardation, X-linked |
| CHT | Chemotherapy |
| CNS | Central nervous system |
| CYP19A1 | Aromatase |
| ESR1 | Estrogen receptor α |
| FLAIR | Fluid-attenuated inversion recovery |
| GB | Glioblastoma |
| GFAP | Glial fibrillary acidic protein |
| GPER | G protein-coupled estrogen receptor |
| IDH | Isocitrate dehydrogenase |
| IVF | In vitro fertilization |
| Ki-67 | Marker of proliferation Kiel 67 |
| MAP2 | Microtubule-associated protein 2 |
| MRI | Magnetic resonance imaging |
| Olig2 | Oligodendrocyte lineage transcription factor 2 |
| p53 | Tumor protein p53 |
| PCR | Polymerase chain reaction |
| PGR | Progesterone receptor |
| RT | Radiotherapy |
| SSP1 | Osteopontin |
| TSPO | Translocator protein |
| VIM | Vimentin |
| H3K27me3 | Histone 3 Lys 27 trimethylation |
| CDKN2A | cyclin-dependent kinase inhibitor 2A |
References
- Ostrom, Q.T.; Price, M.; Neff, C.; Cioffi, G.; Waite, K.A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2016-2020. Neuro-oncology 2023, 25(12) Suppl 2, iv1–iv99. [Google Scholar] [CrossRef]
- Tamimi, A.F.; Juweid, M. Epidemiology and Outcome of Glioblastoma. In Glioblastoma [Internet]; De Vleeschouwer, S., Ed.; Codon Publications: Brisbane, Australia, 2017; pp. 143–153. [Google Scholar]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; Curschmann, J.; Janzer, R.C.; Ludwin, S.K.; Gorlia, T.; Allgeier, A.; Lacombe, D.; Cairncross, J.G.; Eisenhauer, E.; Mirimanoff, R.O. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. The New England journal of medicine 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Mantilla, E.; Sewell, J.; Hatanpaa, K.J.; Pan, E. Occurrence of Glioma in Pregnant Patients: An Institutional Case Series and Review of the Literature. Anticancer research 2020, 40, 3453. [Google Scholar] [CrossRef]
- Roelvink, N.C.A.; Kamphorst, W.; van Alphen, H.A.M.; Rao, B.R. Pregnancy-Related Primary Brain and Spinal Tumors. Archives of Neurology 1987, 44, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Pallud, J.; Duffau, H.; Razak, R.A.; Barbarino-Monnier, P.; Capelle, L.; Fontaine, D.; Frenay, M.; Guillet-May, F.; Mandonnet, E.; Taillandier, L. Influence of pregnancy in the behavior of diffuse gliomas: clinical cases of a French glioma study group. Journal of neurology 2009, 256, 2014–2020. [Google Scholar] [CrossRef] [PubMed]
- Peeters, S.; Pagès, M.; Gauchotte, G.; Miquel, C.; Cartalat-Carel, S.; Guillamo, J.S.; Capelle, L.; Delattre, J.Y.; Beauchesne, P.; Debouverie, M.; Fontaine, D.; Jouanneau, E.; Stecken, J.; Menei, P.; De Witte, O.; Colin, P.; Frappaz, D.; Lesimple, T.; Bauchet, L.; Lopes, M.; Bozec, L.; Moyal, E.; Deroulers, C.; Varlet, P.; Zanello, M.; Chretien, F.; Oppenheim, C.; Duffau, H.; Taillandier, L.; Pallud, J. Interactions between glioma and pregnancy: insight from a 52-case multicenter series. Journal of neurosurgery 2018, 128, 3–13. [Google Scholar] [CrossRef]
- Yust-Katz, S.; de Groot, J.F.; Liu, D.; Wu, J.; Yuan, Y.; Anderson, M.D.; Conrad, C.A.; Milbourne, A.; Gilbert, M.R.; Armstrong, T.S. Pregnancy and glial brain tumors. Neuro-oncology 2014, 16, 1289–1294. [Google Scholar] [CrossRef]
- Pallud, J.; Mandonnet, E.; Deroulers, C.; Fontaine, D.; Badoual, M.; Capelle, L.; Guillet-May, F.; Page, P.; Peruzzi, P.; Jouanneau, E.; Frenay, M.; Cartalat-Carel, S.; Duffau, H.; Taillandier, L. Pregnancy increases the growth rates of World Health Organization grade II gliomas. Annals of neurology 2010, 67, 398–404. [Google Scholar] [CrossRef]
- Blumenthal, D.T.; Parreño, M.G.; Batten, J.; Chamberlain, M.C. Management of malignant gliomas during pregnancy: a case series. Cancer 2008, 113, 3349–3354. [Google Scholar] [CrossRef]
- Molina-Botello, D.; Rodríguez-Sanchez, J.R.; Cuevas-García, J.; Cárdenas-Almaraz, B.V.; Morales-Acevedo, A.; Mejía-Pérez, S.I.; Ochoa-Martinez, E. Pregnancy and brain tumors; a systematic review of the literature. Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia 2021, 86, 211–216. [Google Scholar] [CrossRef]
- Li, Y.; Meador, K.J. Epilepsy and Pregnancy. Continuum (Minneapolis, Minn.) 2022, 28, 34–54. [Google Scholar] [CrossRef] [PubMed]
- Longo, B.; Forinash, A.B.; Murphy, J.A. Levetiracetam use in pregnancy. The Annals of pharmacotherapy 2009, 43, 1692–1695. [Google Scholar] [CrossRef] [PubMed]
- Sadetzki, S.; Chetrit, A.; Freedman, L.; Stovall, M.; Modan, B.; Novikov, I. Long-term follow-up for brain tumor development after childhood exposure to ionizing radiation for tinea capitis. Radiation research 2005, 163, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Hauptmann, M.; Byrnes, G.; Cardis, E.; Bernier, M.O.; Blettner, M.; Dabin, J.; Engels, H.; Istad, T.S.; Johansen, C.; Kaijser, M.; Kjaerheim, K.; Journy, N.; Meulepas, J.M.; Moissonnier, M.; Ronckers, C.; Thierry-Chef, I.; Le Cornet, L.; Jahnen, A.; Pokora, R.; Bosch de Basea, M.; Figuerola, J.; Maccia, C.; Nordenskjold, A.; Harbron, R.W.; Lee, C.; Simon, S.L.; Berrington de Gonzalez, A.; Schüz, J.; Kesminiene, A. Brain cancer after radiation exposure from CT examinations of children and young adults: results from the EPI-CT cohort study. The Lancet. Oncology 2023, 24, 45–53. [Google Scholar] [CrossRef]
- Tewari, K.S.; Cappuccini, F.; Asrat, T.; Flamm, B.L.; Carpenter, S.E.; Disaia, P.J.; Quilligan, E.J. Obstetric emergencies precipitated by malignant brain tumors. American journal of obstetrics and gynecology 2000, 182, 1215–1221. [Google Scholar] [CrossRef]
- Vougioukas, V.I.; Kyroussis, G.; Gläsker, S.; Tatagiba, M.; Scheufler, K.M. Neurosurgical interventions during pregnancy and the puerperium: clinical considerations and management. Acta neurochirurgica 2004, 146, 1287–1291; discussion 1291–1292. [Google Scholar] [CrossRef]
- Zottel, A.; Jovčevska, I.; Šamec, N.; Komel, R. Cytoskeletal proteins as glioblastoma biomarkers and targets for therapy: A systematic review. Critical Reviews in Oncology/Hematology 2021, 160, 103283. [Google Scholar] [CrossRef]
- Skalli, O.; Wilhelmsson, U.; Örndahl, C.; Fekete, B.; Malmgren, K.; Rydenhag, B.; Pekny, M. Astrocytoma grade IV (glioblastoma multiforme) displays 3 subtypes with unique expression profiles of intermediate filament proteins. Human Pathology 2013, 44, 2081–2088. [Google Scholar] [CrossRef]
- Nowicki, M.O.; Hayes, J.L.; Chiocca, E.A.; Lawler, S.E. Proteomic Analysis Implicates Vimentin in Glioblastoma Cell Migration. Cancers 2019, 11, 466. [Google Scholar] [CrossRef]
- Lin, L.; Wang, G.; Ming, J.; Meng, X.; Han, B.; Sun, B.; Cai, J.; Jiang, C. Analysis of expression and prognostic significance of vimentin and the response to temozolomide in glioma patients. Tumor Biology 2016, 37, 15333–15339. [Google Scholar] [CrossRef]
- Lu, D.-Y.; Yeh, W.-L.; Huang, S.-M.; Tang, C.-H.; Lin, H.-Y.; Chou, S.-J. Osteopontin increases heme oxygenase–1 expression and subsequently induces cell migration and invasion in glioma cells. Neuro-oncology 2012, 14, 1367–1378. [Google Scholar] [CrossRef] [PubMed]
- Pietras, A.; Katz, A.M.; Ekström, E.J.; Wee, B.; Halliday, J.J.; Pitter, K. L.; Werbeck, J.L.; Amankulor, N.M.; Huse, J.T.; Holland, E.C. Osteopontin-CD44 Signaling in the Glioma Perivascular Niche Enhances Cancer Stem Cell Phenotypes and Promotes Aggressive Tumor Growth. Cell Stem Cell 2014, 14, 357–369. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Marisetty, A.; Schrand, B.; Gabrusiewicz, K.; Hashimoto, Y.; Ott, M.; Grami, Z.; Kong, L.Y.; Ling, X.; Caruso, H.; Zhou, S.; Wang, Y.A.; Fuller, G.N.; Huse, J.; Gilboa, E.; Kang, N.; Huang, X.; Verhaak, R.; Li, S.; Heimberger, A.B. Osteopontin mediates glioblastoma-associated macrophage infiltration and is a potential therapeutic target. The Journal of clinical investigation 2019, 129, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Jang, B.; Yoon, D.; Lee, J.Y.; Kim, J.; Hong, J.; Koo, H.; Sa, J.K. Integrative multi-omics characterization reveals sex differences in glioblastoma. Biology of Sex Differences 2024, 15, 23. [Google Scholar] [CrossRef]
- Weidner, L.; Lorenz, J.; Quach, S.; Braun, F.K.; Rothhammer-Hampl, T.; Ammer, L.M.; Vollmann-Zwerenz, A.; Bartos, L.M.; Dekorsy, F.J.; Holzgreve, A.; Kirchleitner, S.V.; Thon, N.; Greve, T.; Ruf, V.; Herms, J.; Bader, S.; Milenkovic, V.M.; von Baumgarten, L.; Menevse, A.N.; Hussein, A.; Sax, J.; Wetzel, C.H.; Rupprecht, R.; Proescholdt, M.; Schmidt, N.O.; Beckhove, P.; Hau, P.; Tonn, J.C.; Bartenstein, P.; Brendel, M.; Albert, N.L.; Riemenschneider, M.J. Translocator protein (18kDA) (TSPO) marks mesenchymal glioblastoma cell populations characterized by elevated numbers of tumor-associated macrophages. Acta neuropathologica communications 2023, 11, 147. [Google Scholar] [CrossRef]
- Ammer, L.-M.; Vollmann-Zwerenz, A.; Ruf, V.; Wetzel, C.H.; Riemenschneider, M.J.; Albert, N.L.; Beckhove, P.; Hau, P. The Role of Translocator Protein TSPO in Hallmarks of Glioblastoma. Cancers 2020, 12, 2973. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Rubin, J.B.; Lathia, J.D.; Berens, M.E.; Barnholtz-Sloan, J.S. Females have the survival advantage in glioblastoma. Neuro-oncology 2018, 20, 576–577. [Google Scholar] [CrossRef]
- Zalcman, N.; Canello, T.; Ovadia, H.; Charbit, H.; Zelikovitch, B.; Mordechai, A.; Fellig, Y.; Rabani, S.; Shahar, T.; Lossos, A.; Lavon, I. Androgen receptor: a potential therapeutic target for glioblastoma. Oncotarget 2018, 9, 19980–19993. [Google Scholar] [CrossRef]
- Zhang, C.; Zhao, N.; Khan, R.; Hung, M.-y.; Zhang, C.; Wang, S.; Wang, T.J.C.; Lin, C. The prognostic significance of androgen receptor expression in gliomas. Scientific Reports 2024, 14, 22122. [Google Scholar] [CrossRef]
- Werner, C.K.; Nna, U.J.; Sun, H.; Wilder-Romans, K.; Dresser, J.; Kothari, A.U.; Zhou, W.; Yao, Y.; Rao, A.; Stallard, S.; Koschmann, C.; Bor, T.; Debinski, W.; Hegedus, A.M.; Morgan, M.A.; Venneti, S.; Baskin-Bey, E.; Spratt, D.E.; Colman, H.; Sarkaria, J.N.; Chinnaiyan, A.M.; Eisner, J.R.; Speers, C.; Lawrence, T.S.; Strowd, R.E.; Wahl, D.R. Expression of the Androgen Receptor Governs Radiation Resistance in a Subset of Glioblastomas Vulnerable to Antiandrogen Therapy. Molecular cancer therapeutics 2020, 19, 2163–2174. [Google Scholar] [CrossRef]
- Fariña-Jerónimo, H.; de Vera, A.; Medina, L.; Plata-Bello, J. Androgen Receptor Activity Is Associated with Worse Survival in Glioblastoma. Journal of integrative neuroscience 2022, 21, 86. [Google Scholar] [CrossRef]
- Sharpe, M.A.; Baskin, D.S.; Jenson, A.V.; Baskin, A.M. Hijacking Sexual Immuno-Privilege in GBM-An Immuno-Evasion Strategy. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef]
- Hernández-Vega, A.M.; Del Moral-Morales, A.; Zamora-Sánchez, C.J.; Piña-Medina, A.G.; González-Arenas, A.; Camacho-Arroyo, I. Estradiol Induces Epithelial to Mesenchymal Transition of Human Glioblastoma Cells. Cells 2020, 9, 1930. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Zhang, Y.; Zhang, K.; Bian, C.; Zhao, Y.; Zhang, J. Expression of estrogen receptors, androgen receptor and steroid receptor coactivator-3 is negatively correlated to the differentiation of astrocytic tumors. Cancer epidemiology 2014, 38, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Hönikl, L.S.; Lämmer, F.; Gempt, J.; Meyer, B.; Schlegel, J.; Delbridge, C. High expression of estrogen receptor alpha and aromatase in glial tumor cells is associated with gender-independent survival benefits in glioblastoma patients. J Neurooncol 2020, 147, 567–575. [Google Scholar] [CrossRef] [PubMed]
- Dueñas Jiménez, J.M.; Candanedo Arellano, A.; Santerre, A.; Orozco Suárez, S.; Sandoval Sánchez, H.; Feria Romero, I.; López-Elizalde, R.; Alonso Venegas, M.; Netel, B.; de la Torre Valdovinos, B.; Dueñas Jiménez, S.H. Aromatase and estrogen receptor alpha mRNA expression as prognostic biomarkers in patients with astrocytomas. Journal of Neuro-Oncology 2014, 119, 275–284. [Google Scholar] [CrossRef]
- Batistatou, A.; Kyzas, P.A.; Goussia, A.; Arkoumani, E.; Voulgaris, S.; Polyzoidis, K.; Agnantis, N.J.; Stefanou, D. Estrogen receptor beta (ERβ) protein expression correlates with BAG-1 and prognosis in brain glial tumours. Journal of Neuro-Oncology 2006, 77, 17–23. [Google Scholar] [CrossRef]
- González-Arenas, A.; Hansberg-Pastor, V.; Hernández-Hernández, O.T.; González-García, T.K.; Henderson-Villalpando, J.; Lemus-Hernández, D.; Cruz-Barrios, A.; Rivas-Suárez, M.; Camacho-Arroyo, I. Estradiol increases cell growth in human astrocytoma cell lines through ERα activation and its interaction with SRC-1 and SRC-3 coactivators. Biochimica et Biophysica Acta (BBA) - Molecular Cell Research 2012, 1823, 379–386. [Google Scholar] [CrossRef]
- Sareddy, G.R.; Nair, B.C.; Gonugunta, V.K.; Zhang, Q.-g.; Brenner, A.; Brann, D.W.; Tekmal, R.R.; Vadlamudi, R.K. Therapeutic Significance of Estrogen Receptor β Agonists in Gliomas. Molecular cancer therapeutics 2012, 11, 1174–1182. [Google Scholar] [CrossRef]
- Desai, P.B.; Karve, A.S.; Zawit, M.; Arora, P.; Dave, N.; Awosika, J.; Li, N.; Fuhrman, B.; Medvedovic, M.; Sallans, L.; Kendler, A.; DasGupta, B.; Plas, D.; Curry, R.; Zuccarello, M.; Chaudhary, R.; Sengupta, S.; Wise-Draper, T.M. A Phase 0/I Pharmacokinetic and Pharmacodynamics and Safety and Tolerability Study of Letrozole in Combination with Standard Therapy in Recurrent High-Grade Gliomas. Clinical Cancer Research 2024, 30, 2068–2077. [Google Scholar] [CrossRef]
- Hirtz, A.; Lebourdais, N.; Rech, F.; Bailly, Y.; Vaginay, A.; Smaïl-Tabbone, M.; Dubois-Pot-Schneider, H.; Dumond, H. GPER Agonist G-1 Disrupts Tubulin Dynamics and Potentiates Temozolomide to Impair Glioblastoma Cell Proliferation. Cells 2021, 10, 3438. [Google Scholar] [CrossRef] [PubMed]
- Bello-Alvarez, C.; Camacho-Arroyo, I. Impact of sex in the prevalence and progression of glioblastomas: the role of gonadal steroid hormones. Biology of Sex Differences 2021, 12, 28. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Major events during disease course. RT – radiotherapy, CHT – chemotherapy.
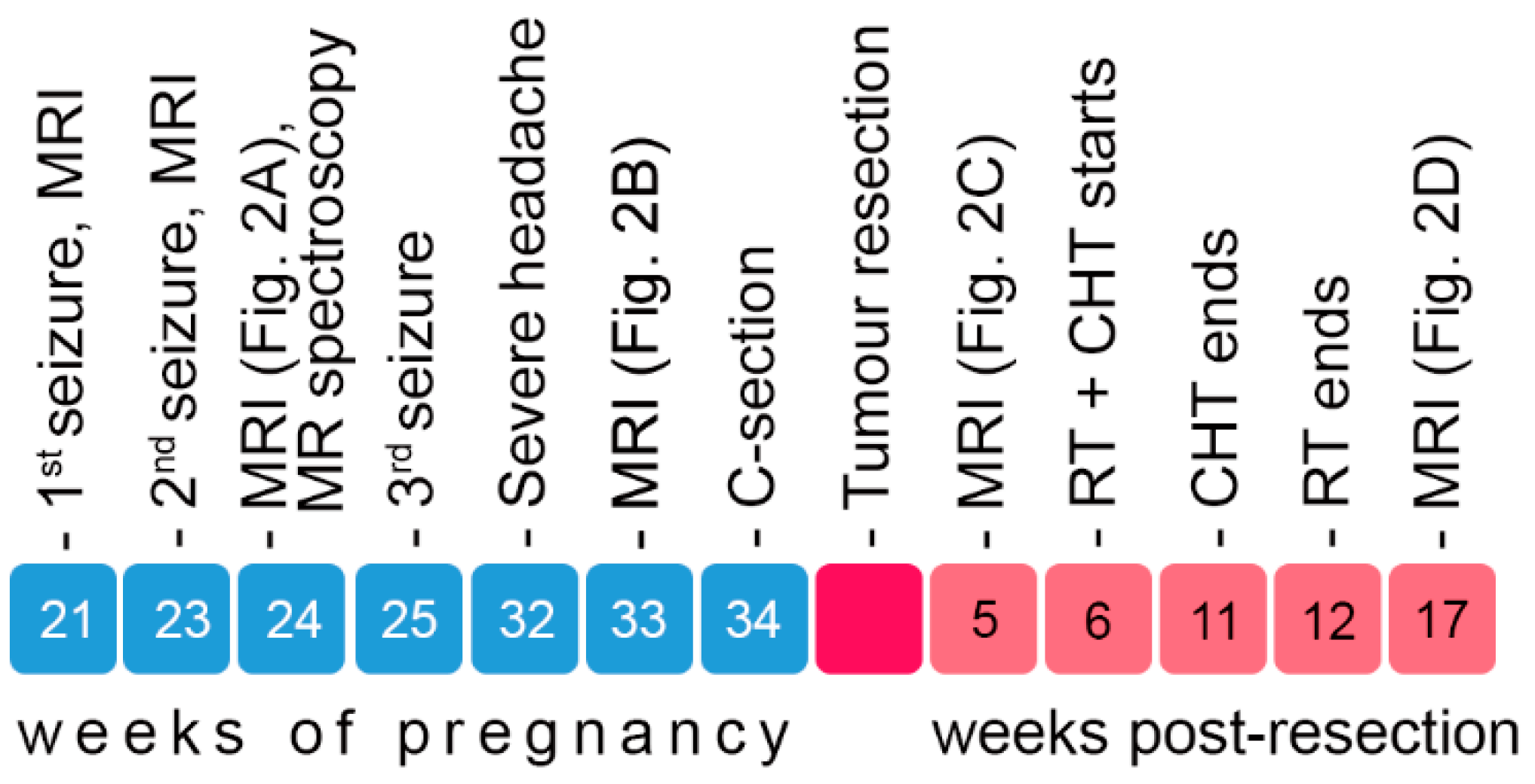
Figure 2.
Changes in the patient's MRI during seven months from discovery of the tumor to terminal deterioration. (a – c) T2-weighted MRI images in the axial plane, without contrast agent (a, b) and with gadolinium enhancement (c, d). (a) MRI at 24 weeks of pregnancy showing a hyperintense lesion in the right lobe. (b) Tumor progression in the 33rd week of pregnancy with significant enlargement of the lesion. (c) Follow-up MRI five weeks after tumor resection. (d) Gadolinium-enhanced MRI image four months after tumor resection and seven months after the onset of symptoms, showing tumor recurrence and progression after therapy (surgical and RT+CHT).
Figure 2.
Changes in the patient's MRI during seven months from discovery of the tumor to terminal deterioration. (a – c) T2-weighted MRI images in the axial plane, without contrast agent (a, b) and with gadolinium enhancement (c, d). (a) MRI at 24 weeks of pregnancy showing a hyperintense lesion in the right lobe. (b) Tumor progression in the 33rd week of pregnancy with significant enlargement of the lesion. (c) Follow-up MRI five weeks after tumor resection. (d) Gadolinium-enhanced MRI image four months after tumor resection and seven months after the onset of symptoms, showing tumor recurrence and progression after therapy (surgical and RT+CHT).
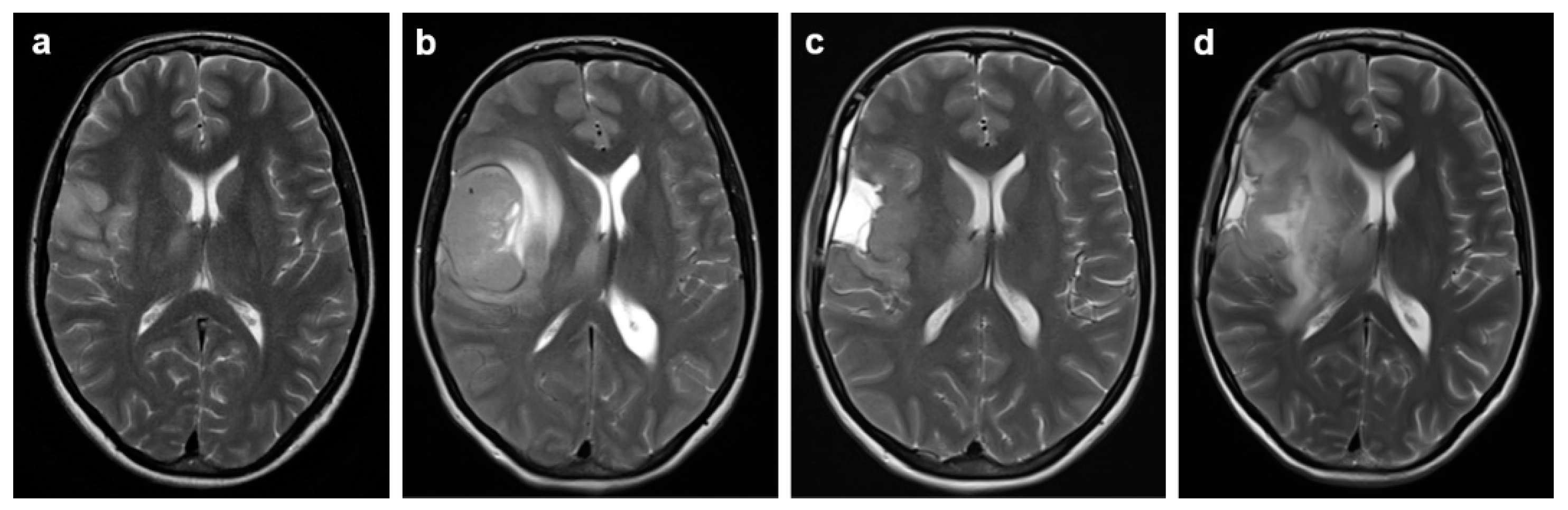
Figure 3.
Hematoxylin and eosin staining (a, b) and immunohistochemistry (C, D) of GB, IDH-wild type, CNS WHO grade 4. a) Hypercellular sheets of anaplastic glial cells. b) Palisading necrosis and microvascular proliferation with endothelial hyperplasia. c) GFAP immunoexpression by tumor cells. d) High Ki-67 proliferation index.
Figure 3.
Hematoxylin and eosin staining (a, b) and immunohistochemistry (C, D) of GB, IDH-wild type, CNS WHO grade 4. a) Hypercellular sheets of anaplastic glial cells. b) Palisading necrosis and microvascular proliferation with endothelial hyperplasia. c) GFAP immunoexpression by tumor cells. d) High Ki-67 proliferation index.
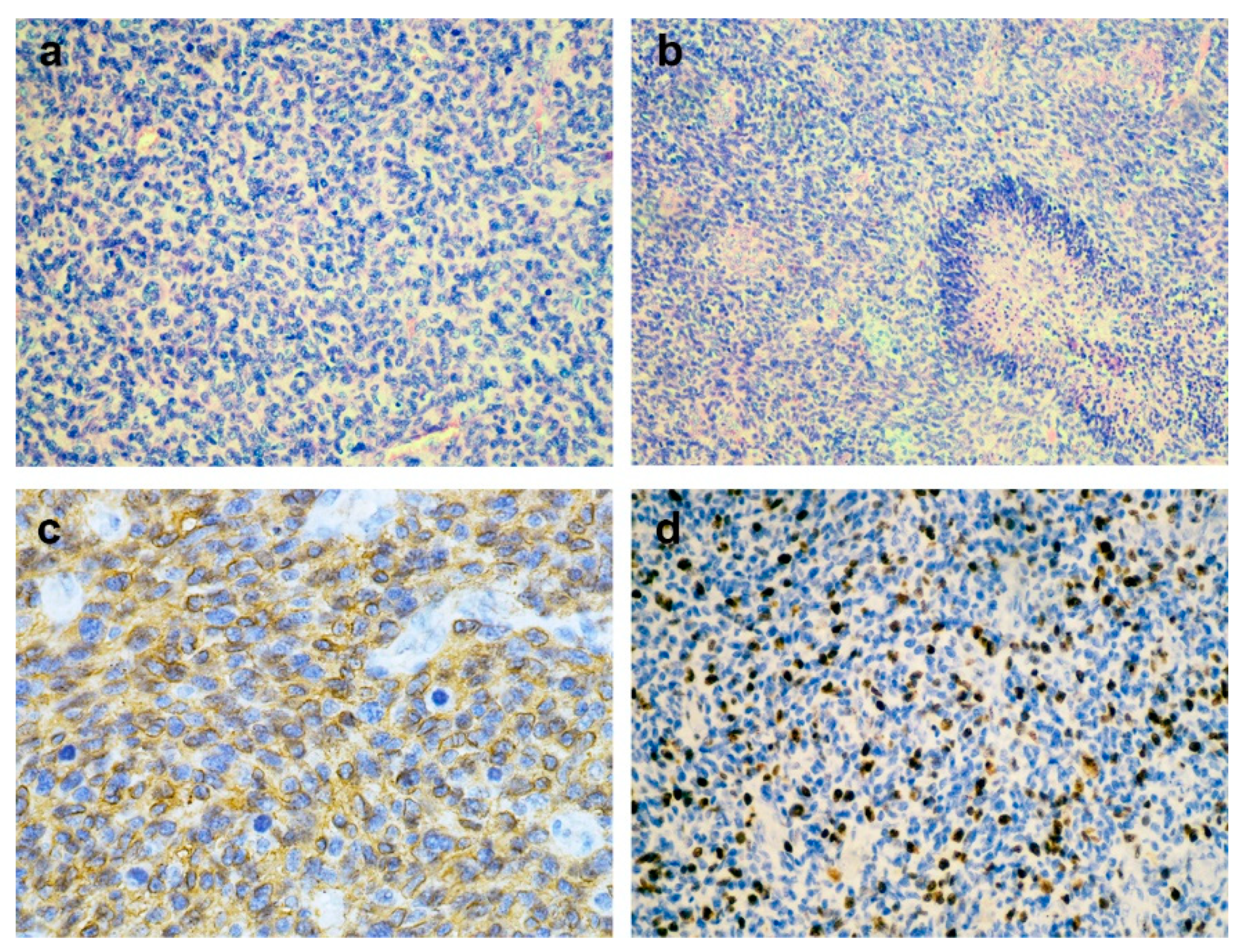
Figure 4.
Expression of genes associated with cell structure, immune response and hormone signalling in GB. Levels of target genes (GFAP, VIM, SPP1, TSPO, AR, CYP19A1, ESR1, GPER1 and PGR) in tumor tissue are expressed relative to the expression of corresponding gene in peritumor tissue. Tumor and peritumor tissue acquired during operation were stored in RNAlater® RNA Stabilization Solution. Total RNA was extracted with TRIzol reagent. After determining RNA concentrations reverse transcription was done with High Capacity cDNA Reverse Transcription Kit; qRT-PCR analysis was done using the QuantStudio™ 3 Real-Time PCR System with SYBR™ Green reagent. The expression levels of target genes were quantified by comparative 2−ΔCt method, using hypoxanthine phosphoribosyltransferase gene (HPRT1) as a housekeeping gene.
Figure 4.
Expression of genes associated with cell structure, immune response and hormone signalling in GB. Levels of target genes (GFAP, VIM, SPP1, TSPO, AR, CYP19A1, ESR1, GPER1 and PGR) in tumor tissue are expressed relative to the expression of corresponding gene in peritumor tissue. Tumor and peritumor tissue acquired during operation were stored in RNAlater® RNA Stabilization Solution. Total RNA was extracted with TRIzol reagent. After determining RNA concentrations reverse transcription was done with High Capacity cDNA Reverse Transcription Kit; qRT-PCR analysis was done using the QuantStudio™ 3 Real-Time PCR System with SYBR™ Green reagent. The expression levels of target genes were quantified by comparative 2−ΔCt method, using hypoxanthine phosphoribosyltransferase gene (HPRT1) as a housekeeping gene.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



