
Submitted:
03 April 2025
Posted:
07 April 2025
You are already at the latest version
Abstract
Morbidity and mortality rates in intensive care unit (intensive care unit) reflect the severe health challenges faced by critically ill patients. Nutritional and immune status, as measured by the Prognostic Nutritional Index (prognostic nutritional index), are increasingly recognized as important predictors of intensive care unit outcomes. We aimed to compare prognostic nutritional index levels of survived and deceased subjects that treated in intensive care unit. This retrospective study examined the association between prognostic nutritional index and mortality among intensive care unit patients treated from June 2023 to June 2024. Prognostic nutritional index was calculated using serum albumin and lymphocyte levels, and patients were categorized into survived and deceased groups. Statistical analyses, including ROC and logistic regression, were used to evaluate prognostic nutritional index’s predictive capacity. We revealed that deceased patients had significantly lower prognostic nutritional index values, lower platelet counts, and higher C-reactive protein (C-reactive protein) and serum creatinine levels compared to survivors. Prognostic nutritional index was independently associated with mortality, with each unit decrease increasing mortality risk by 94%. These findings highlight prognostic nutritional index’s utility as a prognostic tool in intensive care unit settings, underscoring the need for nutritional assessments and targeted interventions to improve patient outcomes. Further research with larger cohorts is warranted to validate these findings and explore causative mechanisms.
Keywords:
prognostic nutritional index
; inflammation
; mortality
; intensive care unit
1. Introduction
Morbidity and mortality in intensive care units (intensive care units) are key indicators of patient outcomes in critical care settings. Intensive care units are specialized hospital departments where patients with life-threatening conditions receive intensive monitoring and treatment. The complex nature of illnesses and injuries treated in intensive care units often leads to high risks of both morbidity (complications and long-term health impacts) and mortality. Patients who require advanced life support, mechanical ventilation, and continuous care, making them vulnerable to infections, organ failure, and other complications are treated in intensive care units. Prediction of mortality and morbidity in intensive care unit population is crucial and several scoring systems have been developed for this purpose [1]. Moreover, inflammation is a characteristics of intensive care population and inflammation markers have been found to be associated with mortality in patients treated in intensive care units [2,3].
Nutrition indexes have been used in determination of poor nutritional status, which is associated with a higher likelihood of infections, slower wound healing, increased risk of complications, and prolonged hospital stays [4,5,6]. The Prognostic Nutritional Index is one of those nutrition indexes and is a clinical tool used to assess a patient’s nutritional and immunological status, which can help predict outcomes, particularly in surgical or critically ill patients [7]. It is calculated using serum albumin levels and total lymphocyte count, providing a simple yet effective method for evaluating a patient's overall health and recovery potential. Prognostic nutritional index is often used to estimate the risk of complications, morbidity, and mortality in patients undergoing surgery, and those with cancer [8,9,10,11]. By identifying at-risk patients early, the prognostic nutritional index helps guide nutritional interventions and other supportive measures to improve outcomes and reduce postoperative complications [12]. To the best of our knowledge, prognostic role of prognostic nutritional index has not been studied in intensive care unit population in Bolu province in Turkey.
In present retrospective analysis, we hypothesized that prognostic nutritional index could be associated with mortality in patients that treated in intensive care units. Hence the objective of the present study was to evaluate the prognostic role of prognostic nutritional index in intensive care unit population by comparing this value between survived and deceased intensive care unit patients.
2. Materials and Methods
Study Population
After obtaining approval from institutional review board (date: 4th of June 2024, approval no: 2024/142) we retrospectively analyzed the patients that treated in intensive care unit of our institution between June 2023 and June 2024. Patients required treatment in intensive care unit due to infection or acute complication of a chronic condition (i.e. chronic obstructive pulmonary disease, heart failure, diabetes mellitus, chronic kidney disease), were enrolled to the study. Subjects that had acute trauma and those younger than 18 years were excluded. We also excluded subjects that have hematologic disorders or malignant conditions. Figure 1 shows flow chart of the study.
General characteristics such as age, gender and days in treatment in intensive care unit, and laboratory data, including leukocyte count (WBC), neutrophil count (neu), lymphocyte count (lym), monocyte count (mono), hemoglobin (Hb), hematocrit (Htc), red cell distribution width, platelet count (PLT), platelet distribution width, mean platelet volume, plasma glucose, serum creatinine, C-reactive protein, serum albumin levels were obtained from patients’ files and institutional database. Prognostic nutritional index is calculated with the following formula: (10 x serum albumin [g/dL] + (0.005 x blood lymphocyte count [k/mm3]). The patients discharged from intensive care to the ward were grouped as survived and the subjects that died in intensive care were grouped as deceased. Data of the survived and deceased groups were compared.
Statistical Analyses
Statistical analyses were held with statistics software (SPSS 16.0 for Windows, IBM Co. Chicago, IL, USA). Normality analysis of the study variables was done with Kolmogorov Smirnov test. Variables that fit into normal distribution were expressed as means ± standard deviations and compared by independent samples t test. Other variables were expressed as medians and interquartile ranges (IQR) and compared by Mann Whitney U test. Categorical variables were compared with chi-square test and expressed as numbers and percentages. Pearson correlation test was used to analyze correlation between study variables. The sensitivity and specificity of the study variables in determining mortality was analyzed with receiver operative characteristics (ROC) analysis test. Binary logistic regression analysis was used to reveal whether prognostic nutritional index was an independent risk factor for mortality (considering also age, mean platelet volume, PLT, C-reactive protein and serum creatinine). The p values lower than 5% were considered statistically significant.
3. Results
Three hundred and fifty four subjects were enrolled to the final analyses (142 in survived, 212 in deceased groups). Median age of the survived and deceased subjects were 68 (27) and 73 (22), respectively (p<0.001).
Eighty two (58%) of the survived group and 130 (61%) of the deceased group were men. Gender of the survived and deceased subjects was not statistically different (p=0.50).
There were no significant difference between survived and deceased patients in terms of Hb (p=0.48), Htc (p=0.56), WBC (p=0.46), neu (p=0.19), mono (p=0.30), red cell distribution width (p=0.40), platelet distribution width (p=0.09), and plasma glucose (p=0.06) levels. Table 1 summarizes the general characteristics and laboratory data of the study population.
Median albumin levels of the survived and deceased subjects were 3.2 (0.8) g/dL and 2.8 (0.7) g/dL, respectively (p<0.001). Median lym levels of survived patients (1.12 [0.8]) were significantly higher than those of the deceased subjects (1[0.9]), (p=0.02). Survived patients had significantly higher PLT levels (217 [115] k/mm3) compared to the deceased subjects (199 [157] k/mm3), (p=0.002). Similarly, mean platelet volume of the survived group (9 [3]fL) was significantly higher than that of the deceased patients (8 [2.9]fL), (p<0.001). On the other hand, serum C-reactive protein of the survived group (49 [82] mg/L) was significantly lower than that of the deceased group (112 [102] mg/L), (p<0.001). Besides, serum creatinine of the survived subjects (0.9 [0.7] mg/dL) was significantly reduced compared to the serum creatinine of the deceased group (1.3 [1.2] mg/dL), (p<0.001).
Mean prognostic nutritional index of the survived group was 39 ± 7.5% while the prognostic nutritional index of deceased subjects was 34 ± 7.3 %. The difference in prognostic nutritional index between survived and deceased groups was statistically significant (p<0.001).
Correlation analysis revealed that prognostic nutritional index was significantly and positively correlated with PLT (r=0.15, p=0.005). Moreover, prognostic nutritional index was inversely correlated with age (r=-0.25, p<0.001), mean platelet volume (r=-0.16, p=0.002), C-reactive protein (r=-0.21, p<0.001) and serum creatinine (r=-0.14, p=0.01) levels.
The sensitivity and specificity of prognostic nutritional index (when lower than 34.2%) in detecting mortality were 73% and 56%, respectively (AUC: 0.69, p<0.001, 95% CI: 0.64-0.74). Figure 2 shows the ROC curve of prognostic nutritional index in detecting mortality in the study population.
According to the binary logistic regression analysis, prognostic nutritional index was an independent risk factor of mortality in intensive care unit patients (considering also age, mean platelet volume, PLT, C-reactive protein and serum creatinine). A unit decrease in prognostic nutritional index increase the risk of mortality by 94% in patients treated in intensive care unit (p<0.001, OR: 0.94, 95%CI: 0.90-0.97).
4. Discussion
The main outcomes of the present work were as follows: (a) prognostic nutritional index was significantly reduced in deceased patients compared to the survived subjects that managed in intensive care unit, (b) prognostic nutritional index was significantly correlated with serum creatinine, C-reactive protein, PLT, mean platelet volume, and age in intensive care population, (c) prognostic nutritional index had moderate sensitivity and considerable sensitivity in detecting mortality in intensive care patients, and (d) prognostic nutritional index was an independent risk factor of mortality in patients treated in intensive care unit.
We also found elevated C-reactive protein levels in deceased patients compared to the survived individuals. This finding is consistent with literature data. C-reactive protein is an acute-phase protein produced by the liver in response to inflammation, infection, or tissue damage, making it a reliable marker for systemic inflammation [13,14]. Elevated C-reactive protein levels in deceased intensive care unit patients suggest that these individuals experienced more severe inflammatory responses, potentially driven by infections (such as sepsis), organ dysfunction, or other life-threatening conditions [3]. In the intensive care unit setting, persistent or excessively high C-reactive protein levels can indicate a poor prognosis. This is because the inflammatory response, when uncontrolled, can lead to complications like multi-organ failure, septic shock, or exacerbation of underlying diseases [15]. Surviving intensive care unit patients typically show a more controlled or resolving inflammatory response, which aligns with lower C-reactive protein levels and better recovery outcomes. Therefore, monitoring C-reactive protein levels can therefore help clinicians assess the severity of illness, guide therapeutic interventions, and predict patient outcomes.
Another finding of the present work was decreased prognostic nutritional index in deceased intensive care unit patients compared to those who survived. This finding underscores the importance of nutritional and immune status in critical care outcomes. Prognostic nutritional index is calculated by using serum albumin levels and total lymphocyte count. It reflects both a patient’s nutritional reserves and immune function. A lower prognostic nutritional index in deceased intensive care unit patients indicates that these individuals were likely in a state of malnutrition and immunosuppression, both of which can contribute to poorer outcomes [16]. Malnutrition in critically ill patients compromises the body’s ability to repair tissues, respond to infections, and manage physiological stress, leading to increased vulnerability to complications like infections, wound healing delays, and organ failure [17]. A low prognostic nutritional index is also associated with a weakened immune system, as reflected by a reduced lymphocyte count, making patients more susceptible to sepsis and other immune-related conditions that can worsen the prognosis [18]. In contrast, patients with higher prognostic nutritional index values typically have better nutritional status and more robust immune function, which supports recovery, reduces complications, and improves survival chances. Accordingly, we reported decreased prognostic nutritional index levels in deceased intensive care patients compared to the survivors. This finding suggests that early identification of nutritional deficits and immune dysfunction through prognostic nutritional index could be key in implementing targeted interventions, such as nutritional support and immunomodulation, to improve outcomes in intensive care unit patients.
Platelets are essential for blood clotting and play a role in preventing excessive bleeding. Additionally, they contribute to the body's immune defense and tissue repair. A decrease in platelet count is a common complication in intensive care unit patients and is often associated with poorer outcomes [19]. In deceased intensive care unit patients, low platelet counts can be a marker of severe illness, such as disseminated intravascular coagulation (DIC), sepsis, or multi-organ failure, conditions that are common in critically ill patients and often precede death. Thrombocytopenia can result from various causes, including systemic infections, which can trigger the immune system to overreact, leading to platelet destruction or consumption [20]. Moreover, liver dysfunction, which often occurs in critically ill patients, impairs platelet production as the liver is crucial for producing thrombopoietin, a hormone involved in platelet synthesis [21]. In contrast, survivors generally maintain higher platelet counts, which suggests a better ability to manage bleeding risk and immune responses, as well as a less severe overall disease course. Monitoring platelet counts in intensive care unit patients can serve as an important prognostic marker, helping clinicians identify those at higher risk of complications and death. Numerous works in literature reported that low platelet count predicted mortality in intensive care unit population [22,23]. In accordance with the literature data, we found reduced platelet counts in deceased patients compared to the survived subjects.
Present study showed that mean platelet volume is decreased in deceased intensive care unit patients compared to survivors. mean platelet volume is a measure of the average size of platelets in the blood, with larger platelets generally being more active and having greater hemostatic potential [24]. Interestingly, mean platelet volume has been proposed as a marker of inflammation in various conditions including type 2 DM [25], diabetic nephropathy [26], hypothyroidism [27], infections [28], vertebral disc disease [29], irritable bowel disease [30], gastrointestinal conditions [31], rheumatoid arthritis [32], and obesity [33]. All of these conditions are characterized with inflammation as the deceased subjects in intensive care. Additionally, mean platelet volume is often used as an indirect marker of platelet production and activity, and changes in mean platelet volume can indicate alterations in platelet function or bone marrow response. Decreased mean platelet volume in deceased intensive care unit patients in present study may suggest that these patients had impaired bone marrow production of platelets or a diminished ability to release larger, more active platelets into circulation. This could be a consequence of severe systemic conditions such as sepsis, multi-organ failure, or other critical illnesses that suppress bone marrow activity or lead to increased platelet destruction. Another possible explanation could be that mean platelet volume may decrease due to consumption of larger platelets because of inflammation and remaining smaller platelets in the circulation [34]. On the other hand, intensive care unit survivors with higher mean platelet volume levels may have a better capacity for platelet production and function, reflecting more robust bone marrow activity or a more controlled inflammatory response. Larger platelets are typically more reactive, which could offer better protection against bleeding and aid in tissue repair and immune defense. Increased mean platelet volume in survived patients and decreased mean platelet volume in deceased subjects in present study highlights the importance of monitoring mean platelet volume as part of a broader assessment of platelet function and overall health status in intensive care unit patients.
The prognostic nutritional index was correlated with various study variables in the present report. These correlations may be a consequence of interaction between nutritional status, inflammation, age, and organ function in critically ill patients. We showed that prognostic nutritional index was correlated with PLT in the study cohort. This finding suggests that better nutritional and immune status is associated with higher platelet levels in intensive care unit patients. Platelets play a crucial role not only in coagulation but also in immune responses and tissue repair [35]. Higher prognostic nutritional index values reflect better nutritional reserves and immune function, which may promote more intact bone marrow activity and platelet production. This association implies that malnourished patients (with lower prognostic nutritional index) might also have lower platelet counts, which could contribute to an increased risk of poor outcome in the intensive care unit setting.
Present study revealed an inverse correlation between prognostic nutritional index and age of the patients. That means older intensive care unit patients tend to have lower prognostic nutritional index values. This is likely due to the fact that aging is often accompanied by sarcopenia, decreased nutrient intake, and a general decline in immune function [36,37,38]. Older individuals also have a higher likelihood of chronic diseases that can affect both nutritional and immune status. The inverse correlation between age and prognostic nutritional index in the present study warrants necessity for particular attention to the nutritional needs of older intensive care unit patients, as they may be at higher risk for malnutrition and related complications.
We also reported an inverse correlation between prognostic nutritional index and C-reactive protein. The negative correlation between prognostic nutritional index and C-reactive protein suggests that patients with higher levels of systemic inflammation tend to have lower prognostic nutritional index values. Inflammation often leads to a catabolic state, where protein breakdown exceeds synthesis, resulting in malnutrition and a reduction in immune competence [39]. Elevated C-reactive protein levels reflect a more severe inflammatory response, which can deplete nutritional reserves and worsen patient outcomes. Inverse correlation between C-reactive protein and prognostic nutritional index in present work emphasizes the interaction between inflammation and nutrition in critically ill patients and the importance of managing both aspects to improve patient outcome.
Present study also revealed an inverse correlation between prognostic nutritional index and serum creatinine levels, which suggests that patients with poorer nutritional status may have impaired renal function. Elevated serum creatinine is a marker of kidney dysfunction, which can contribute to malnutrition through fluid imbalances, reduced nutrient absorption, and metabolic disturbances [40]. For instance, acute kidney injury is common in critically ill patients and can exacerbate malnutrition by increasing catabolism and reducing dietary intake [41]. The negative correlation between prognostic nutritional index and serum creatinine, which reported in the present study, suggests that nutritional support might be required for intensive care unit patients with kidney dysfunction to improve their prognosis.
The sensitivity and specificity of prognostic nutritional index in detecting mortality in intensive care unit patients were not low in the present work. A 73% sensitivity and 56% specificity of prognostic nutritional index was demonstrated in mortality detection. Prognostic nutritional index can correctly select 73% of patients who died in intensive care unit when it is lower than 34.2%. This is a moderately high sensitivity, meaning the prognostic nutritional index is relatively effective in identifying critically ill patients who are likely to have poor outcomes. Similar reports have been published in the literature. Wang et al found that prognostic nutritional index had 73% sensitivity and 53% specificity in detecting survival of the patients with hepatocellular carcinoma [42]. Usefulness of prognostic nutritional index has been shown in another study which reported 60% sensitivity and 83% specificity of prognostic nutritional index in detecting survival of rectal cancer patients [43]. In addition, a meta-analysis revealed that prognostic nutritional index had 61% sensitivity and 60% specificity in detecting mortality of the patients with esophageal cancer [44]. These data suggest that prognostic nutritional index could be useful in detecting mortality of the conditions characterized with chronic inflammation. The sensitivity and specificity of the prognostic nutritional index in detecting mortality in present study was comparable to the literature data.
We also demonstrated that prognostic nutritional index was an independent risk factor for mortality in intensive care unit patients. This finding emphasizes the critical role of nutritional status in determining patient outcomes in intensive care. The effects of prognostic nutritional index on survival of the patients in intensive care unit did not rely on the influence of age, mean platelet volume, PLT, C-reactive protein or serum creatinine. Thus, the argument that prognostic nutritional index serves as a vital indicator of a patient’s overall health and prognosis in the intensive care unit, specifically reflecting the nutritional and immune status that can significantly impact recovery and survival is strengthened. Similar findings has been reported in the literature. Jiang et al reported that prognostic nutritional index was a risk factor of survival in patients with esophagus cancer with a 1.51 odds ratio [44]. Moreover, hazard ratio of low prognostic nutritional index was 1.3 in survival of colorectal cancer patients [45]. These data suggest the findings of the present work.
Several limitations may limit he accuracy of our findings in the present study. First, the study was retrospective, meaning we just found a simple association rather than causal relationship between prognostic nutritional index and mortality of intensive care unit patients. Second, the study cohort was relatively small. Third, single center nature of the work may limit globalization of the study findings. However, present study was important by reporting prognostic nutritional index as an independent risk factor of mortality in the intensive care unit setting.
5. Conclusions
In conclusion, these findings highlight the critical importance of nutritional assessment in the intensive care unit and establishes prognostic nutritional index as a valuable prognostic tool. Given its independent association with mortality risk, physicians should integrate regular prognostic nutritional index evaluations into their clinical practice to identify at-risk patients early. Thus, timely nutritional interventions and improvement of the management of critically ill patients ultimately enhanced patient outcomes and survival rates in the intensive care unit setting could be implemented.
Author Contributions
Conceptualization: BO and IK; Methodology: IK and GA; Formal analysis: SPO and BO; Data curation; SPO and IK; Visualization: GA; Project administration: IK and GA; Writing-original draft: IK and SPO; Writing-review & editing: BO and GA. All authors are reviewed and agree to the final form of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Abant Izzet Baysal University Ethics committee (approval date: 4th of June 2024, approval no: 2024/142).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data related to this work is available by corresponding author on reasonable requests.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| WBC | White blood cell count |
| neu | Neutrophil count |
| lym | Lymphocyte count |
| mono | Monocyte count |
| RDW | Red cell distribution width |
| PLT | Platelet count |
| Hb | Hemoglobin |
| Htc | Hematocrit |
| PDW | Platelet distribution width |
| MPV | Mean platelet volume |
| PG | Plasma glucose |
| CRP | c-reactive protein |
| PNI | Prognostic nutritional index |
References
- Pellathy, T. P., M. R. Pinsky, and M. Hravnak. "Intensive Care Unit Scoring Systems.". Crit Care Nurse 2021, 41, 54–64. [CrossRef] [PubMed]
- Karagoz, I., G. Aktas, H. Yoldas, I. Yildiz, M. N. Ogun, M. Bilgi, and A. Demirhan. "Association between Hemogram Parameters and Survival of Critically Ill Patients.". J Intensive Care Med 2019, 34, 511–13. [CrossRef] [PubMed]
- Karagoz, I., B. Ozer, I. Ital, M. Turkoglu, A. Disikirik, and S. Ozer. "C-Reactive Protein-to-Serum Albumin Ratio as a Marker of Prognosis in Adult Intensive Care Population.". Bratisl Lek Listy 2023, 124, 277–79.
- Demirkol, M. E., G. Aktas, M. Alisik, O. M. Yis, M. Kaya, and D. Kocadag. "Is the Prognostic Nutritional Index a Predictor of Covid-19 Related Hospitalizations and Mortality?". Malawi Med J 2023, 35, 15–21. [CrossRef]
- Aktas, G. "Association between the Prognostic Nutritional Index and Chronic Microvascular Complications in Patients with Type 2 Diabetes Mellitus." J Clin Med 12, no. 18 (2023).
- Aktas, G. "Importance of the Geriatric Nutritional Risk Index in Survival among the Geriatric Population. " Geriatr Gerontol Int 2024, 24, 444–45. [Google Scholar] [CrossRef]
- Wullur, Yulia, and Nurpudji Astuti Taslim. "Neutrophil-Lymphocyte Ratio, Prognostic Nutritional Index and Crp-Albumin Ratio Significantly Predict Mortality in Icu Patients with Low Nutrition Risk.". Nutr Clín Diet Hosp 2024, 44, 253–60.
- Sun, K., S. Chen, J. Xu, G. Li, and Y. He. "The Prognostic Significance of the Prognostic Nutritional Index in Cancer: A Systematic Review and Meta-Analysis.". J Cancer Res Clin Oncol 2014, 140, 1537–49. [CrossRef]
- Yan, L., T. Nakamura, A. Casadei-Gardini, G. Bruixola, Y. L. Huang, and Z. D. Hu. "Long-Term and Short-Term Prognostic Value of the Prognostic Nutritional Index in Cancer: A Narrative Review.". Ann Transl Med 2021, 9, 1630. [CrossRef]
- Cheng, Y. L., S. H. Sung, H. M. Cheng, P. F. Hsu, C. Y. Guo, W. C. Yu, and C. H. Chen. "Prognostic Nutritional Index and the Risk of Mortality in Patients with Acute Heart Failure." J Am Heart Assoc 6, no. 6 (2017).
- Zhang, J., X. Xiao, Y. Wu, J. Yang, Y. Zou, Y. Zhao, Q. Yang, and F. Liu. "Prognostic Nutritional Index as a Predictor of Diabetic Nephropathy Progression." Nutrients 14, no. 17 (2022).
- He, M., Q. Fan, Y. Zhu, D. Liu, X. Liu, S. Xu, J. Peng, and Z. Zhu. "The Need for Nutritional Assessment and Interventions Based on the Prognostic Nutritional Index for Patients with Femoral Fractures: A Retrospective Study.". Perioper Med (Lond) 2021, 10, 61. [CrossRef]
- Demirkol, M. E., G. Aktas, S. Bilgin, G. Kahveci, O. Kurtkulagi, B. M. Atak, and T. T. Duman. "C-Reactive Protein to Lymphocyte Count Ratio Is a Promising Novel Marker in Hepatitis C Infection: The Clear Hep-C Study." Rev Assoc Med Bras (1992) 68, no. 6 (2022): 838-41.
- Demirkol, Muhammed Emin, and Gulali Aktas. "C-Reactive Protein to Lymphocyte Count Ratio Could Be a Reliable Marker of Thyroiditis; the Clear-T Study.". Precision Medical Sciences 2022, 11, 31–34. [CrossRef]
- Faix, J. D. "Biomarkers of Sepsis. " Crit Rev Clin Lab Sci 2013, 50, 23–36. [Google Scholar] [CrossRef]
- Al-Shami, I., H. M. A. Hourani, and B. Alkhatib. "The Use of Prognostic Nutritional Index (Pni) and Selected Inflammatory Indicators for Predicting Malnutrition in Covid-19 Patients: A Retrospective Study.". J Infect Public Health 2023, 16, 280–85. [CrossRef]
- Nomellini, V., L. J. Kaplan, C. A. Sims, and C. C. Caldwell. "Chronic Critical Illness and Persistent Inflammation: What Can We Learn from the Elderly, Injured, Septic, and Malnourished?". Shock 2018, 49, 4–14. [CrossRef] [PubMed]
- Ni, L., J. Huang, J. Ding, J. Kou, T. Shao, J. Li, L. Gao, W. Zheng, and Z. Wu. "Prognostic Nutritional Index Predicts Response and Prognosis in Cancer Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis.". Front Nutr 2022, 9, 823087. [CrossRef] [PubMed]
- Strauss, R., M. Wehler, K. Mehler, D. Kreutzer, C. Koebnick, and E. G. Hahn. "Thrombocytopenia in Patients in the Medical Intensive Care Unit: Bleeding Prevalence, Transfusion Requirements, and Outcome.". Crit Care Med 2002, 30, 1765–71. [CrossRef]
- Wu, X., Y. Li, and X. Yang. "Platelet Phagocytosis by Leukocytes in a Patient with Cerebral Hemorrhage and Thrombocytopenia Caused by Gram-Negative Bacterial Infection.". J Int Med Res 2022, 50, 3000605221079102. [CrossRef] [PubMed]
- Mitchell, O., D. M. Feldman, M. Diakow, and S. H. Sigal. "The Pathophysiology of Thrombocytopenia in Chronic Liver Disease.". Hepat Med 2016, 8, 39–50.
- Moreau, D., J. F. Timsit, A. Vesin, M. Garrouste-Orgeas, A. de Lassence, J. R. Zahar, C. Adrie, F. Vincent, Y. Cohen, B. Schlemmer, and E. Azoulay. "Platelet Count Decline: An Early Prognostic Marker in Critically Ill Patients with Prolonged Icu Stays.". Chest 2007, 131, 1735–41.
- uertas, M., J. L. Zayas-Castro, and P. J. Fabri. "Statistical and Prognostic Analysis of Dynamic Changes of Platelet Count in Icu Patients.". Physiol Meas 2015, 36, 939–53. [CrossRef]
- Korniluk, A., O. M. Koper-Lenkiewicz, J. Kamińska, H. Kemona, and V. Dymicka-Piekarska. "Mean Platelet Volume (Mpv): New Perspectives for an Old Marker in the Course and Prognosis of Inflammatory Conditions.". Mediators Inflamm 2019, 2019, 9213074.
- Cakir, Lutfullah, Gulali Aktas, OZGUR Enginyurt, and Sahika Altas Cakir. "Mean Platelet Volume Increases in Type 2 Diabetes Mellitus Independent of Hba1c Level.". Acta Medica Mediterranea 2014, 30, 425–28.
- Kocak, M. Z., G. Aktas, E. Erkus, T. T. Duman, B. M. Atak, and H. Savli. "Mean Platelet Volume to Lymphocyte Ratio as a Novel Marker for Diabetic Nephropathy.". J Coll Physicians Surg Pak 2018, 28, 844–47. [CrossRef]
- Bilgin, Satilmis, Burcin Meryem Atak Tel, Gizem Kahveci, Tuba Taslamacioglu Duman, Ozge Kurtkulagi, Semanur Yurum, Asli Erturk, Buse Balci, and Gulali Aktas. "Hypothyroidism Is Strongly Correlated with Mean Platelet Volume and Red Cell Distribution Width.". National Journal of Health Sciences 2021, 6, 7–10.
- Aktas, Gulali, Basri Cakiroglu, MUSTAFA Sit, UGUR Uyeturk, Aytekin Alçelik, Haluk Savli, and Eray Kemahli. "Mean Platelet Volume: A Simple Indicator of Chronic Prostatitis.". Acta Medica Mediterranea 2013, 29, 551–54.
- Dagistan, Y., E. Dagistan, A. R. Gezici, S. Halicioglu, S. Akar, N. Özkan, and A. Gulali. "Could Red Cell Distribution Width and Mean Platelet Volume Be a Predictor for Lumbar Disc Hernias?" Ideggyogy Sz 69, no. 11-12 (2016): 411-14.
- Aktas, G., A. Alcelik, B. K. Tekce, V. Tekelioglu, M. Sit, and H. Savli. "Red Cell Distribution Width and Mean Platelet Volume in Patients with Irritable Bowel Syndrome." Prz Gastroenterol 9, no. 3 (2014): 160-3.
- Balci, Sumeyye Buse , and Gulali Aktas. "A Comprehensive Review of the Role of Hemogram Derived Inflammatory Markers in Gastrointestinal Conditions.". Iranian Journal of Colorectal Research 2022, 10, 75–86.
- Cakır, Lutfullah, Gulali Aktas, Oznur Berke Mercimek, Ozgur Enginyurt, Yasemin Kaya, and Kutsal Mercimek. "Are Red Cell Distribution Width and Mean Platelet Volume Associated with Rheumatoid Arthritis.". Biomed Res 2016, 27, 292–94.
- Aktas, Gulali, Mehmet Zahid Kocak, Tuba Taslamacioglu Duman, Edip Erkus, Burcin Meryem Atak, Mustafa Sit, and Haluk Savli. "Mean Platelet Volume (Mpv) as an Inflammatory Marker in Type 2 Diabetes Mellitus and Obesity.". Bali Medical Journal 2018, 7, 650–53.
- Aktas, G., M. Sit, H. Tekce, A. Alcelik, H. Savli, T. Simsek, E. Ozmen, A. Z. Isci, and T. Apuhan. "Mean Platelet Volume in Nasal Polyps.". West Indian Med J 2013, 62, 515–8.
- Mandel, J., M. Casari, M. Stepanyan, A. Martyanov, and C. Deppermann. "Beyond Hemostasis: Platelet Innate Immune Interactions and Thromboinflammation." Int J Mol Sci 23, no. 7 (2022).
- Akan, S. , and G. Aktas. "Relationship between Frailty, According to Three Frail Scores, and Clinical and Laboratory Parameters of the Geriatric Patients with Type 2 Diabetes Mellitus." Rev Assoc Med Bras (1992) 68, no. 8 (2022): 1073-77.
- Chen, Y., L. Liu, X. Yang, W. Wan, Y. Liu, and X. Zhang. "Correlation between Malnutrition and Mortality in Older Patients Aged ≥90 Years with Multimorbidity." Geriatr Nurs 59 (2024): 321-29.
- Suzuki, E., N. Kawata, A. Shimada, H. Sato, R. Anazawa, M. Suzuki, Y. Shiko, M. Yamamoto, J. Ikari, K. Tatsumi, and T. Suzuki. "Prognostic Nutritional Index (Pni) as a Potential Prognostic Tool for Exacerbation of Copd in Elderly Patients.". Int J Chron Obstruct Pulmon Dis 2023, 18, 1077–90. [CrossRef]
- Rosenthal, M. D., T. Bala, Z. Wang, T. Loftus, and F. Moore. "Chronic Critical Illness Patients Fail to Respond to Current Evidence-Based Intensive Care Nutrition Secondarily to Persistent Inflammation, Immunosuppression, and Catabolic Syndrome." JPEN J Parenter Enteral Nutr 44, no. 7 (2020): 1237-49.
- Molina, Pablo, Belén Vizcaíno, Emma Huarte, Luis M Pallardó, and Juan J Carrero. "Pathophysiology, Detection, and Treatment." In Nutritional Disorders in Chronic Kidney Disease, edited by Jonathan Craig, Donald Molony and Giovanni Strippoli, 617-57: Wiley, 2022.
- Khor, B. H., H. C. Tiong, S. C. Tan, R. Abdul Rahman, and A. H. Abdul Gafor. "Protein-Energy Wasting Assessment and Clinical Outcomes in Patients with Acute Kidney Injury: A Systematic Review with Meta-Analysis." Nutrients 12, no. 9 (2020).
- Wang, D., X. Hu, L. Xiao, G. Long, L. Yao, Z. Wang, and L. Zhou. "Prognostic Nutritional Index and Systemic Immune-Inflammation Index Predict the Prognosis of Patients with Hcc.". J Gastrointest Surg 2021, 25, 421–27. [CrossRef]
- Xia, L. J., W. Li, J. C. Zhai, C. W. Yan, J. B. Chen, and H. Yang. "Significance of Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio and Prognostic Nutritional Index for Predicting Clinical Outcomes in T1-2 Rectal Cancer." BMC Cancer 20, no. 1 (2020): 208.
- Jiang, Y., D. Xu, H. Song, B. Qiu, D. Tian, Z. Li, Y. Ji, and J. Wang. "Inflammation and Nutrition-Based Biomarkers in the Prognosis of Oesophageal Cancer: A Systematic Review and Meta-Analysis." BMJ Open 11, no. 9 (2021): e048324.
- Xie, H., L. Wei, G. Yuan, M. Liu, S. Tang, and J. Gan. "Prognostic Value of Prognostic Nutritional Index in Patients with Colorectal Cancer Undergoing Surgical Treatment.". Front Nutr 2022, 9, 794489. [CrossRef] [PubMed]
Figure 1.
Study flow chart.
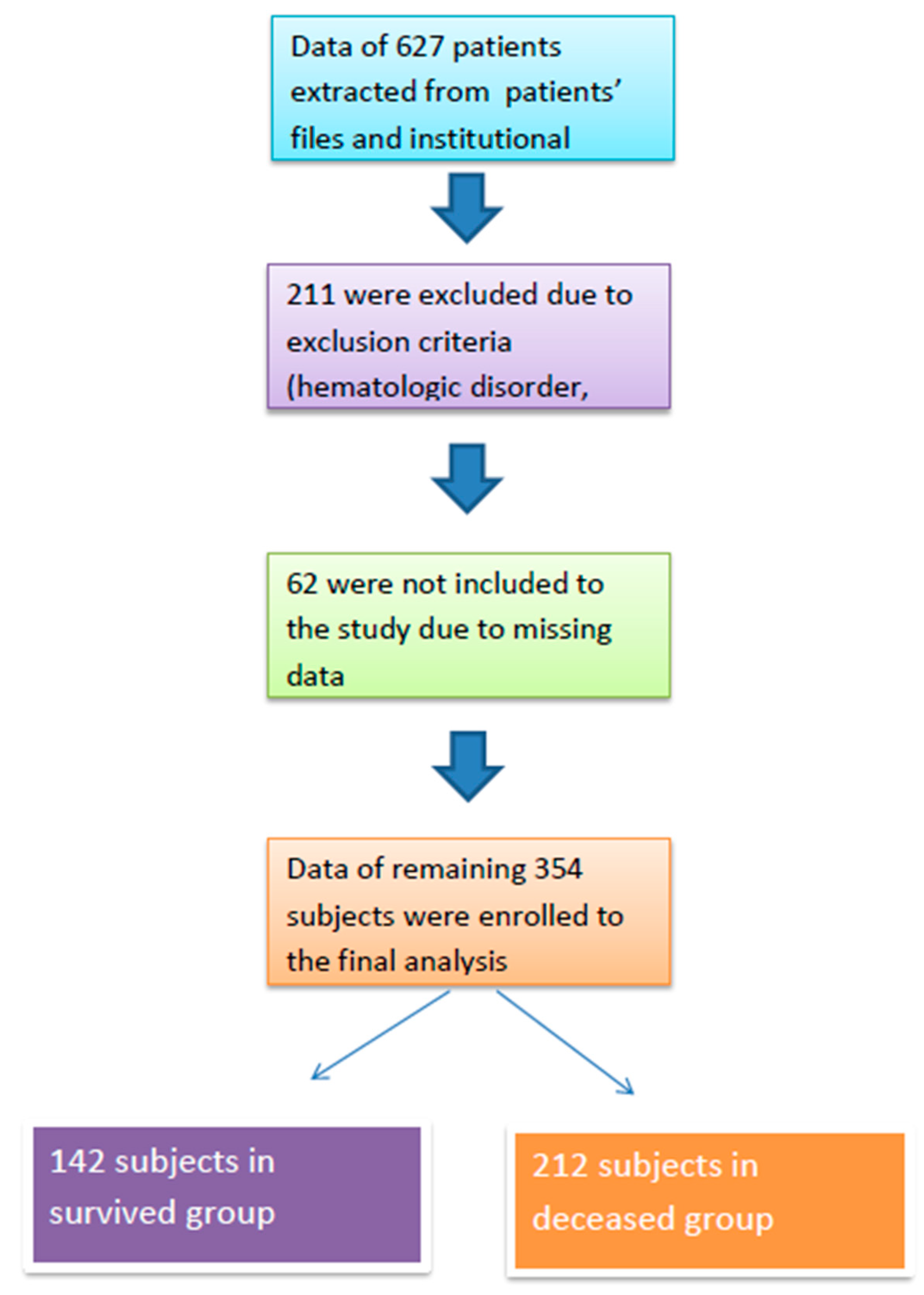
Figure 2.
ROC curve of prognostic nutritional index in detecting survival of intensive care unit population.
Figure 2.
ROC curve of prognostic nutritional index in detecting survival of intensive care unit population.
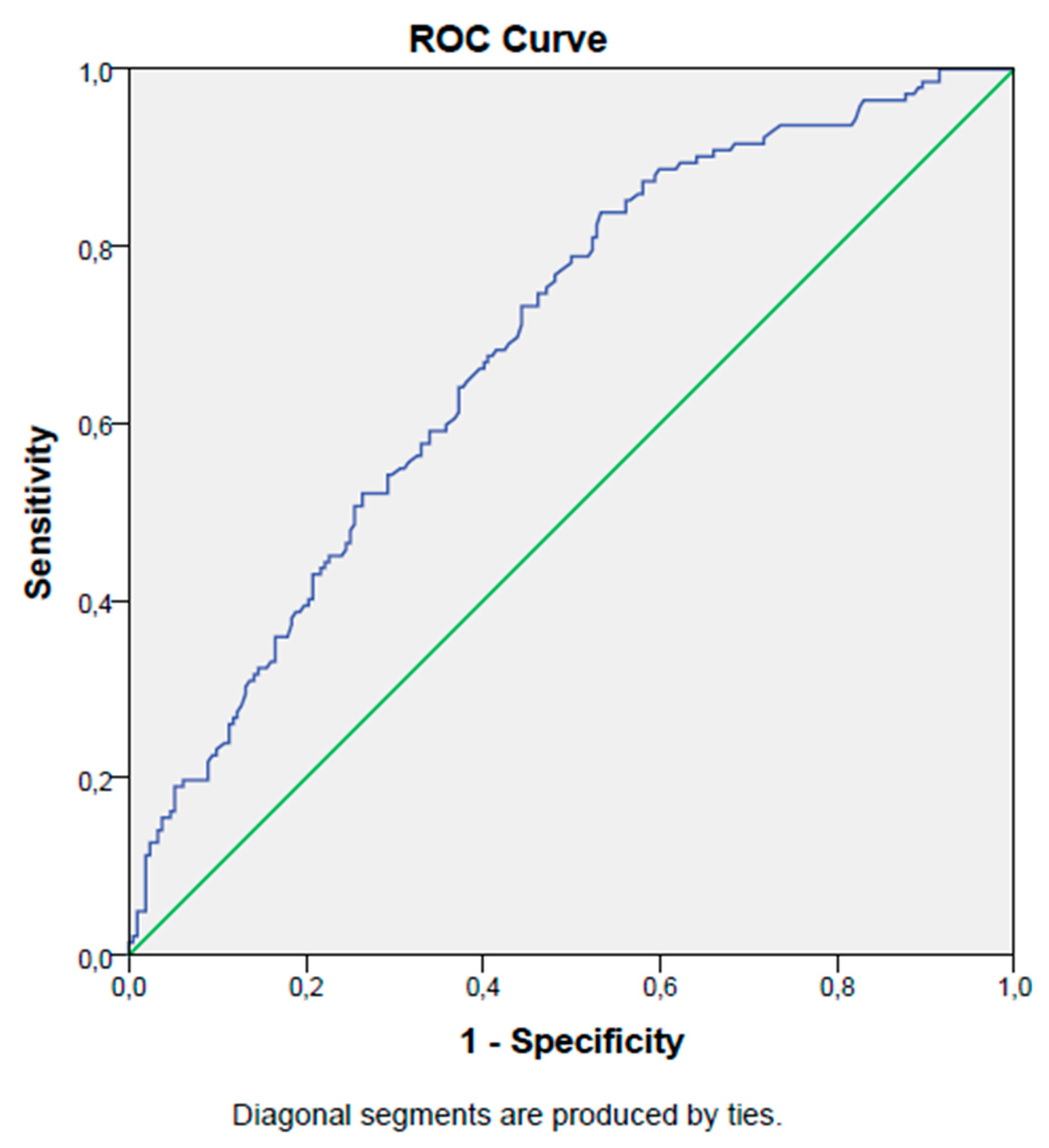

Table 1.
Summary of the general characteristics and laboratory data of the study population.
| Survived Group | Deceased Group | p | ||
| Gender | Men (n,(%)) | 82 (58) | 130 (61) | 0.50 |
| Women (n,(%)) | 60 (42) | 82 (39) | ||
| Median (IQR) | ||||
| Age (years) | 68 (27) | 73 (22) | <0.001 | |
| Serum albumin (g/dL) | 3.2 (0.8) | 2.8 (0.7) | <0.001 | |
| WBC (k/mm3) | 11.5 (8.8) | 12.6 (10) | 0.46 | |
| neu (k/mm3) | 9.5 (8.2) | 10.5 (9) | 0.19 | |
| lym (k/mm3) | 1.12 (0.8) | 1(0.9) | 0.02 | |
| mono (k/mm3) | 0.6 (0.4) | 0.6 (0.5) | 0.30 | |
| RDW (%) | 17 (4) | 16 (4) | 0.40 | |
| PLT (k/mm3) | 217 (115) | 199 (157) | 0.002 | |
| PDW (%) | 17 (4) | 17 (6) | 0.09 | |
| MPV (fL) | 9 (3) | 8 (2.9) | <0.001 | |
| PG (mg/dL) | 133 (75) | 143 (85) | 0.06 | |
| CRP (mg/L) | 49 (82) | 112 (102) | <0.001 | |
| Serum creatinine (mg/dL) | 0.9 (0.7) | 1.3 (1.2) | <0.001 | |
| Mean ± SD | ||||
| Hb (g/dL) | 12 ± 2.5 | 13 ± 2.4 | 0.48 | |
| Htc (%) | 36 ± 8 | 39 ± 7 | 0.56 | |
| PNI (%) | 39 ± 7.5 | 34 ± 7.3 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



