
Submitted:
03 April 2025
Posted:
05 April 2025
You are already at the latest version
Abstract
The aim is to present the 'Awake Bruxism Identification Tool (ABIT)' for children and adolescents. This tool was created at the Postgraduate Program of the Faculdade de Odontologia de Piracicaba at the Universidade Estadual de Campinas (FOP/UNICAMP) as part of a preliminary study, which was tested on 10 families from June to August 2023 at the Dental Specialties Center (CEO-Piracicaba-SP). The analysis consisted of Report 1 (R1), Report 2 (R2), Self-report (AR), Clinical Assessment (CA), and Ecological Momentary Assessment (EMA). R1, R2, and SR include questions about the perception of AB on a 5-point Likert scale, along with the recording of perception through analogical and playful EMA. Meanwhile, CA identifies intraoral and extraoral characteristics. Combining these items helps determine whether the child falls within the 'AB spectrum'. The tool was evaluated for comprehensibility, applicability and reliability, showing satisfactory results, with a reported completion time of between 5 and 10 minutes. The frequency of AB was 4 children in the “Possible AB Spectrum” and 3 children in the “Possible AB Spectrum corroborated by EMA”, with “teeth clenching” being the most frequently observed event. Adjustments to the instrument were made based on participant feedback, and the reproducibility of the ABIT seems adequate for the planned expanded study, which aims to contribute to the clinical investigation.
Keywords:
awake bruxism
; bruxism identification
; bruxism in children and adolescents
; momentary ecological assessment
1. Introduction
"Bruxism is a repetitive behavior characterized by the activity of the masticatory muscles, resulting in the action of clenching or grinding the teeth and/or maintaining muscle contraction and jaw protrusion. There are two distinct circadian manifestations: Sleep Bruxism (SB) and Awake Bruxism (AB)" [1]. "SB occurs during sleep and presents either phasic or tonic masticatory action, while AB occurs while awake and is characterized by prolonged or repetitive contact between the teeth and/or bracing (contraction of the facial muscles without teeth contact) and/or thrusting (lateral sliding of the jaw without teeth contact)" [2].
Bruxism is a general term that encompasses a broad spectrum of jaw muscle activities of various etiologies. It can be a sign of underlying disorders, a risk factor for clinical consequences, or possibly just a behavior without any pathological relevance [3,4]. "It has a multifactorial etiology, involving biological and psychosocial factors" [5,6]. The treatment indicated for bruxism depends on an accurate (reliable and valid), applicable (feasible), and accessible (economical and suitable for daily clinical use) assessment [2].
Research aimed at identifying bruxism can categorize it as possible, probable, or definitive [1]. 'Possible' is based on a positive report and self-report; 'probable' is based on a positive clinical examination, while 'definitive' is based on polysomnography (PSG) and electromyography (EMG) [2]. In addition to these categories, there is the Ecological Momentary Assessment (EMA) methodology [7], a recent strategy recommended for categorizing definitive bruxism [8].
Differences in diagnostic strategies may affect the results on the epidemiology of bruxism (SB and AB), which currently has a worldwide range of prevalence for children and adolescents, ranging from 5% to 50% [9], with a recent global finding of 22.22% [10]; Specifically for AB, the observed data are: 37.3% [11]; 4.1% [12]; 38.4% [8]; 16% to 32% [13]; 24.6% [14]; 28.3% to 40% [15] and 23% [10].
In this context, research teams are working hard to develop methods for identifying and diagnosing bruxism, especially those that prioritize family observation, self-perception, low cost, and simplicity to ensure participant adherence. As a result, several studies conducted in the last five years have utilized EMA in smartphone applications developed specifically for this purpose. EMA allows for real-time recording of conditions and is conducted over several days within a natural environment [7,16,17].
The aim of this study is to introduce the tool known as the 'Awake Bruxism Identification Tool' (ABIT) and to describe a pilot study conducted using ABIT. This tool is proposed as an alternative in pediatric and hebiatric clinical practice, utilizing a playful analog EMA for children and adolescents.
2. Materials and Methods
To develop the ABIT tool, a comprehensive literature review was conducted on the concept, classification and method of identifying AB [1,2,18], with a particular focus on studies dedicated on the development of diagnostic tools [1,2,18,19,20,21,22].
2.1. Tool Presentation
The ABIT tool was developed to be applied in two stages, initially in Brazilian Portuguese. The tool comprises the following components: Parents’ Report (R1), Self-Report of children and adolescents (SR), Clinical Assessment (CA), Parents’ Report after Guided Observation (R2), and Ecological Momentary Assessment (EMA). Each of these components will be detailed below:
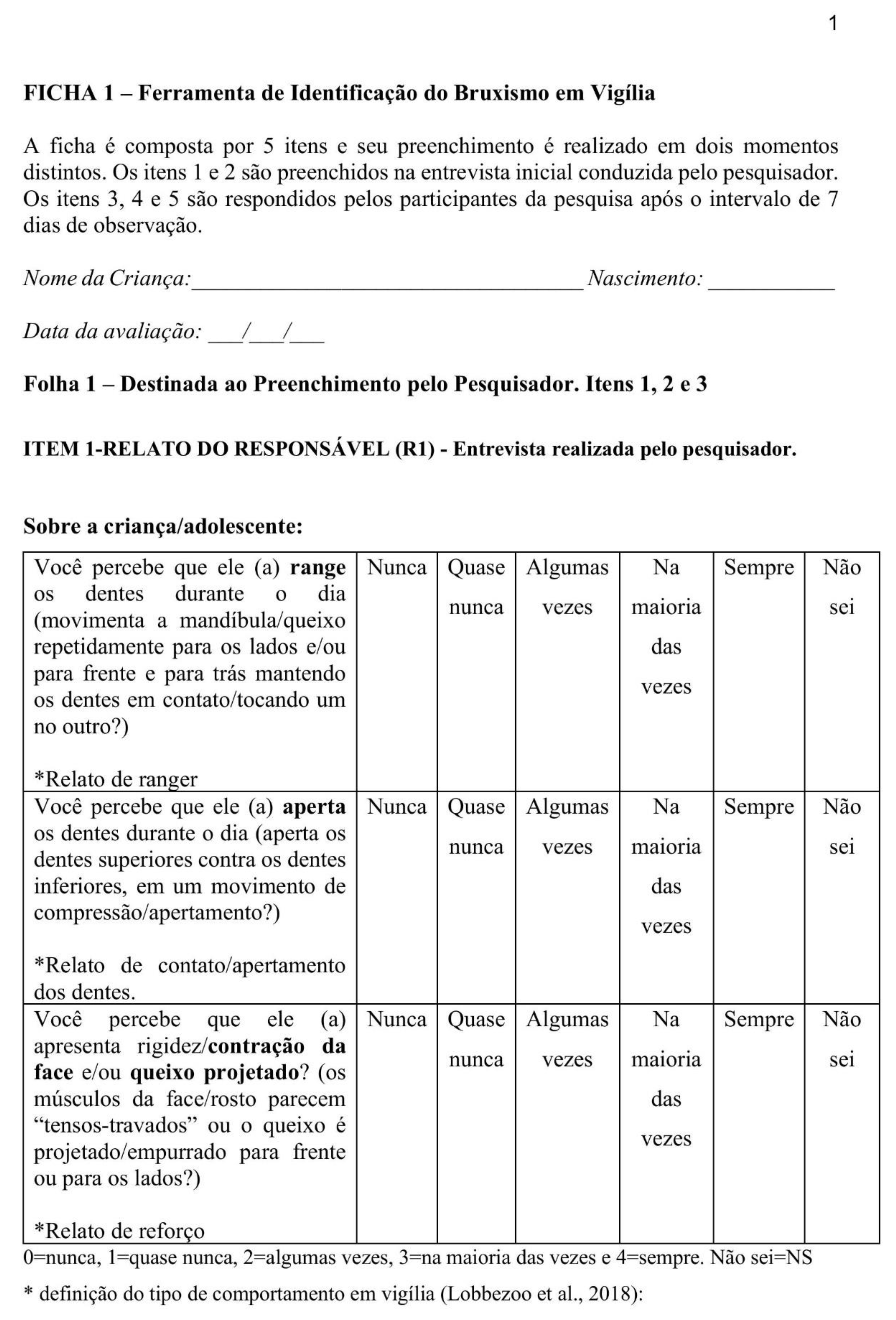
Item 1 (Report 1-R1) consists of three questions that the guardian must answer during the initial interview to assess their perception of the child’s/adolescent’s behavior concerning AB. The first question asks whether the guardian has noticed the child grinding their teeth while awake: (1- Does the child repeatedly move their jaw sideways and/or back and forth, while keeping their teeth in contact?). The second question asks whether they notice that the child is clenching their teeth (2 - Do the upper teeth touch the lower teeth in a clenching movement?). The third question examines whether the child’s facial muscles appear tense or if the jaw protrudes forward: (3 - Do the facial muscles appear “tense-locked,” or does the chin remain protruded forward or to the side?). To facilitate this process, guardians are provided with information on how to identify AB, using illustrative images and real-life examples.
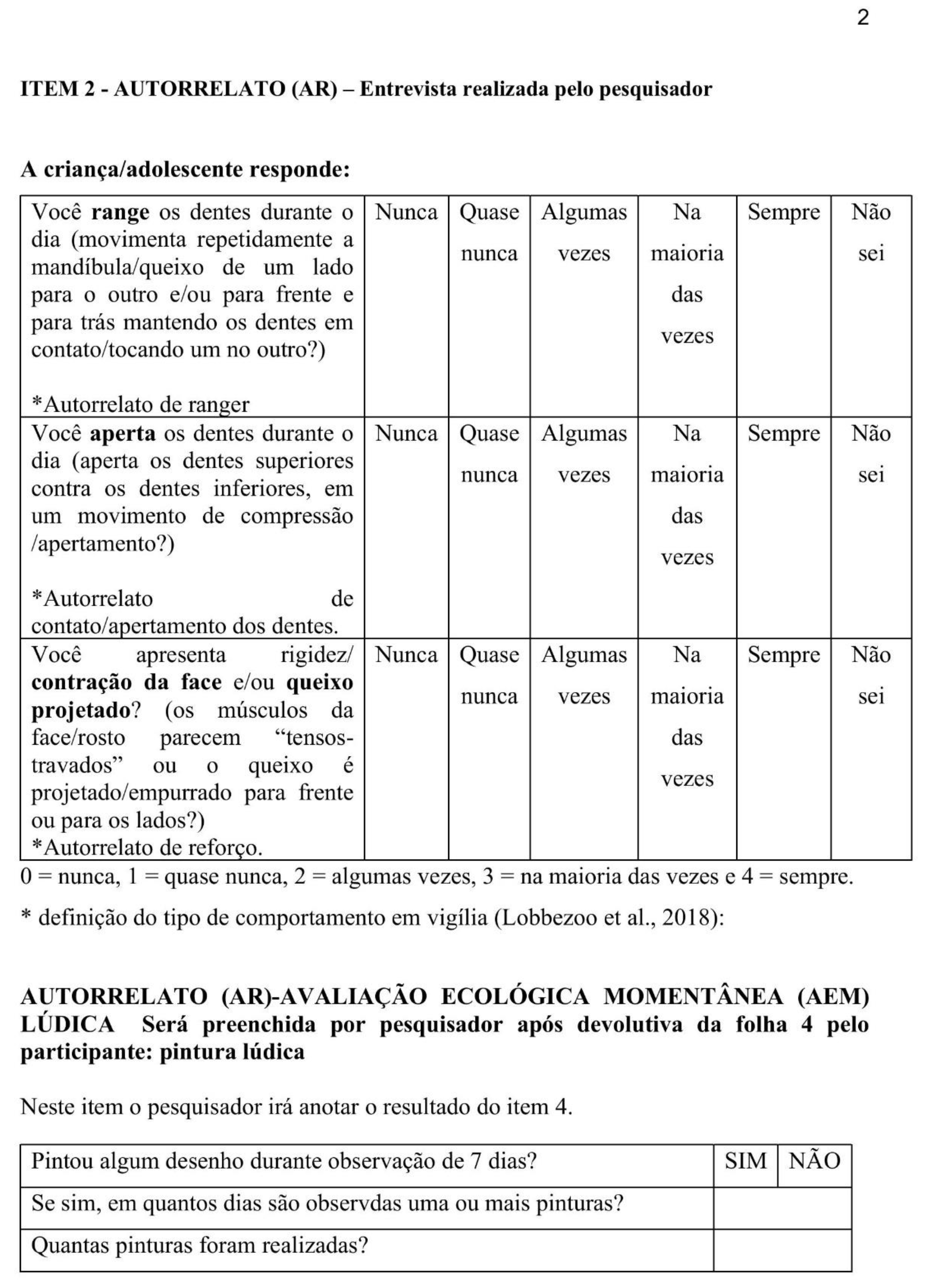
Item 2 (Self-Report-SR) consists of three questions directed to the child/adolescent participants regarding their self-perception of AB, to be answered during the initial interview. The first question asks whether the child grinds their teeth while awake: (1 - Do you repeatedly move your jaw from side to side and/or back and forth while keeping your teeth in contact?). The second question asks whether the child clenches their teeth: (2 - Do you notice that you clench your upper teeth with your lower teeth?). The third question inquires whether the facial muscles are contracted or if the jaw protrudes forward: (3 - Do you notice that your face is tense/locked and/or you protrude your chin forward or to the side?).
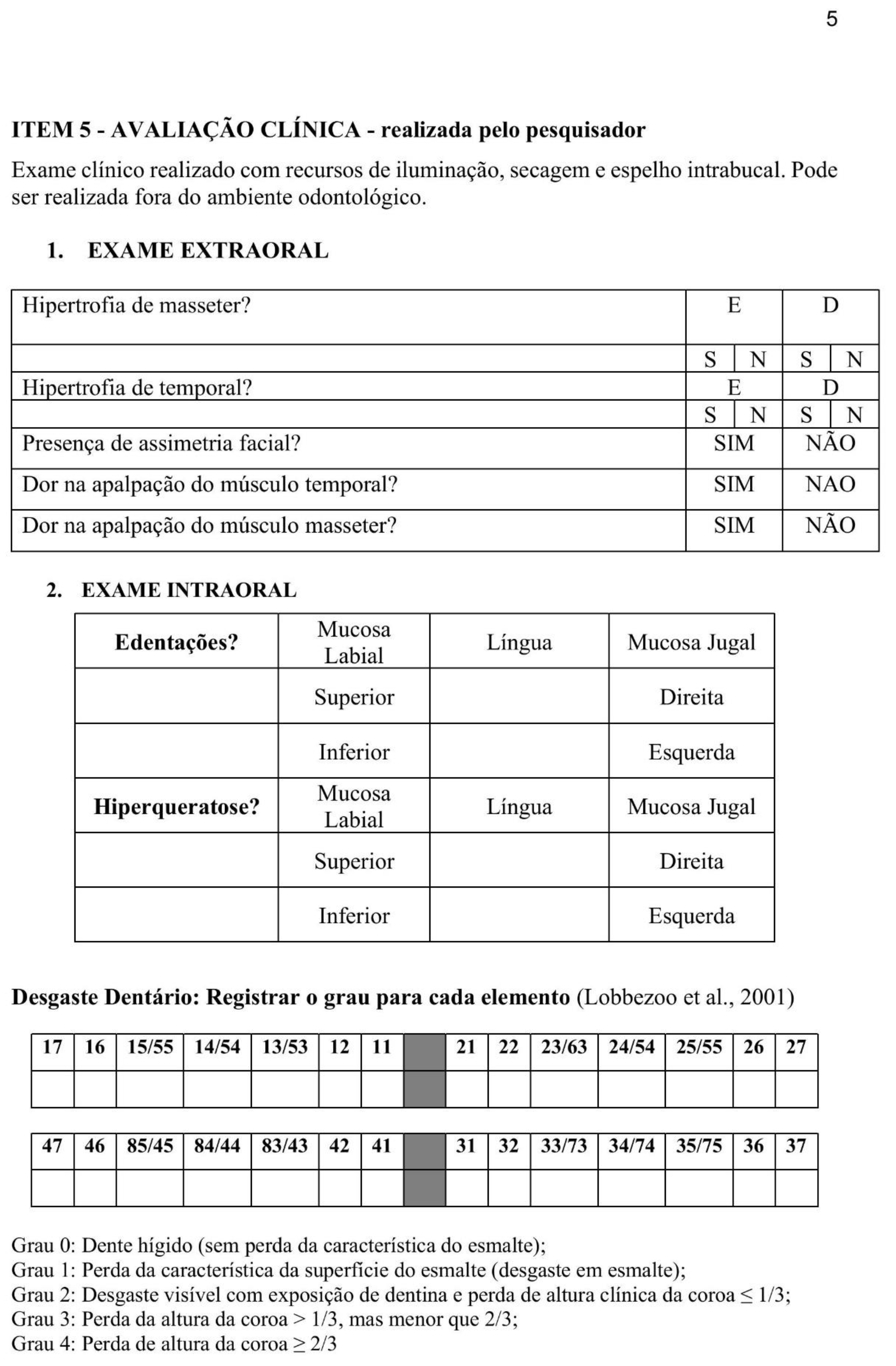
Item 3 (Clinical Assessment-CA) includes information from both the extraoral (ECA) and intraoral (ICA) clinical assessments, which involve the analysis of the masticatory muscles, soft tissues, and teeth. This item must be completed by the research dentist:
i. During the ECA, the right and left masseter muscles are examined for tenderness, swelling, or trigger points. Any noticeable aesthetic asymmetries are also assessed. Pain is evaluated upon palpation of the muscles, and the presence of hypertrophy in the masseter and/or temporal muscles on both sides of the face is recorded as either Yes (Y) or No (N). The interpretation of masseter hypertrophy is based on three conditions that determine a "Yes" answer: palpable and visible hypertrophy during forced occlusion, visible hypertrophy with a prominent mandibular angle, and visible hypertrophy with exostosis at the mandibular angle. The evaluation of the temporal muscle considers whether there is palpable and visible hypertrophy both during forced occlusion and at rest.
ii. In ICA, depressions on the upper and lower labial mucosa, tongue, and buccal mucosa, as well as hyperkeratosis on the tongue and buccal mucosa, are examined, with findings recorded as Yes (Y) or No (N). Tooth wear is evaluated using a five-point ordinal grading scale [5]: Grade 0 = no visible wear; Grade 1 = visible enamel wear; Grade 2 = visible wear with dentin exposure and loss of clinical crown height ≤ 1/3; Grade 3 = loss of clinical crown height >1/3 but < 2/3; Grade 4 = loss of clinical crown height ≥ 2/3 [5], with attention to distinguishing it from chemical wear, based on specific criteria [23,24].
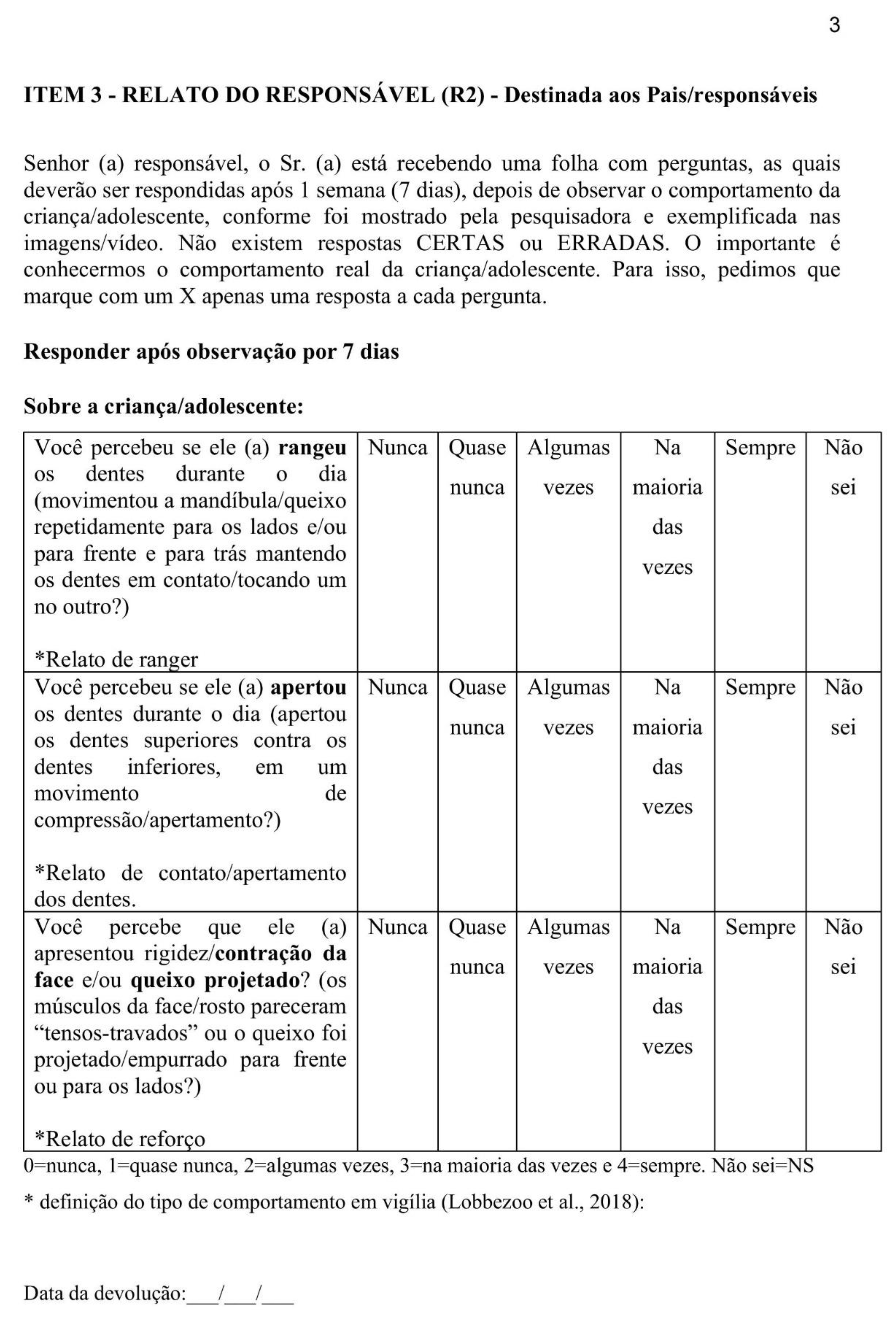
Item 4 (Report 2 - R2) consists of three questions, identical to those in Item 1, using the verb tenses 'creaked,' 'squeezed,' and 'observed’, addressed to the guardian, which must be answered after guidance and observation of the child/adolescents over a period of seven to fifteen days (surveillance interval).
Items R1, R2 and SR are answered with the following response alternatives (Likert Scale) [25]: never, almost never, sometimes, most of the time, always and I don't know; with scores assigned of 0, 1, 2, 3 and 4, respectively. The “don't know” option is recorded as “DK”.
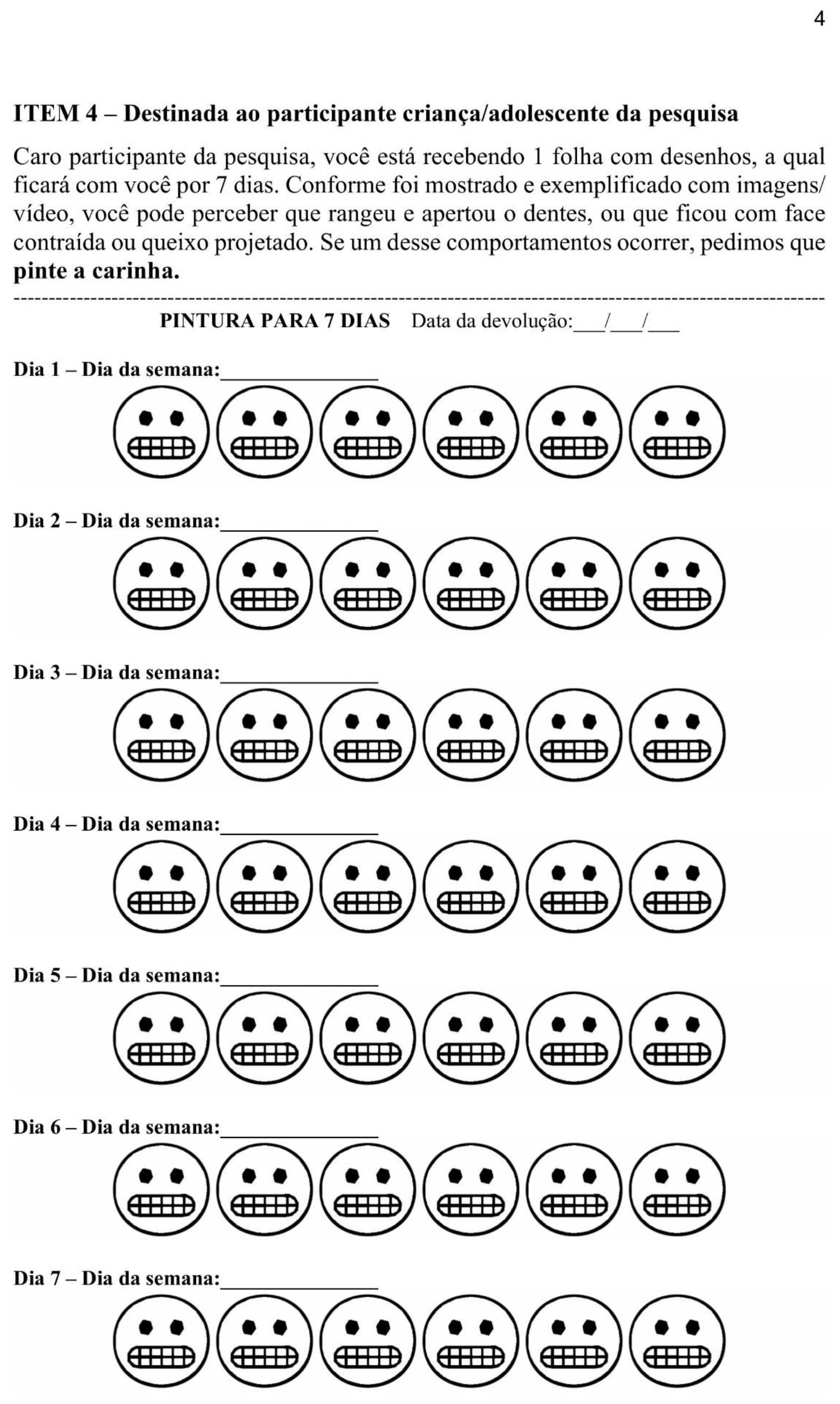
Item 5 (EMA) refers to the child's/adolescent’s self-perception of behavior, which is to be documented within seven days of the initial interview. This is an analog method that employs pencil/pen and paper, where children are instructed to color in the illustration of "emoji" vectors (representing emotional expressions) if any AB events are identified. To facilitate this process, children are provided with guidance on how to recognize AB, based on illustrative images and real-life examples. The guidelines for the home stage are as follows: "The drawing sheet should remain with the child for seven days and must be attached to the wall or furniture with adhesive tape (to help with recall and prevent loss of the paper) in the room where the child spends the most time (usually the living room or bedroom). During school hours, the child should keep the sheet in their notebook or backpack. Parents are advised to communicate with the teachers and request permission for the child to carry the sheet during class. Caregivers should be instructed to collect the sheet after a period of seven days. The sheet includes forty-two vector illustrations of "emoji faces". Six illustrations for each day of the week. One illustration should be colored for each occurrence of AB.
Figure 1.
Example of playful drawings for one day of the week. The children must color the emoji when they notice AB in that day.
Figure 1.
Example of playful drawings for one day of the week. The children must color the emoji when they notice AB in that day.

2.2. Cut-Off Points and Data Interpretation
For data analysis, the aggregation of items determines whether the child/adolescent is classified within the 'AB Spectrum,' with the following clinical categories adopted: 'Not AB,' 'Possible AB,' 'Possible AB corroborated by EMA,' 'Probable AB,' and 'Probable AB corroborated by EMA.' The 'Definitive AB' classification is not determined by ABIT.
The 'Not AB' classification corresponds to zero or null scores. R1, R2, and SR receive a zero score when the answers are 'Never,' and a null score if only a single item is marked as 'Almost Never' (score 1). The EMA record receives a zero score if no painting is recorded and a null score if the painting is below the cut-off point (less than four days with painting records). Null values are indicated in the tables as 'Null' (R1/R2/AR) and '<4' (EMA).
'Possible AB' refers to scores higher than zero on the Likert scale of R1, R2, and SR. 'Possible AB corroborated by EMA' corresponds to the correlation between 'Possible AB' and a positive EMA.
'Probable AB' is characterized by the combination of positive ICA and ECA scores. A score higher than 0 on the ICA is recorded in the presence of indentations and/or hyperkeratosis (on the lips, buccal mucosa, and tongue), with each occurrence corresponding to an increase of one score point. A score greater than 0 on the ECA is recorded in the presence of masseter or temporal hypertrophy, with each occurrence resulting in an increase of 1 point. Tooth wear is recorded as complementary data and does not serve a diagnostic purpose.
Thus, ABIT defines parameters based on cut-off points: each item has a score, clinical interpretation, and maximum spectrum. The sum of the spectra results in the Awake Bruxism Spectrum (AB Spectrum), which ranges from 0 to 96 (Table 1).
2.3. Pilot Study
The study represented the initial phase of a broader investigation, which was submitted to and approved by the Research Ethics Committee of FOP-UNICAMP, Piracicaba, SP, Brazil (protocol code: 67100922.1.0000.5418, dated May 18, 2023). The study was conducted in accordance with the guidelines of the Declaration of Helsinki and Informed consent was obtained from all subjects involved in the study.
The ABIT tool (Appendix A1) was used for the first time with a group of 10 families who attended the Dental Specialties Center (CEO II, Piracicaba, SP, Brazil) of the municipal public health between June and August 2023. This group was selected based on the pediatric dentistry waiting list for that period, which included thirty-one children. Of these, sixteen were invited through invitations addressed to parents/guardians; ten accepted, three later dropped out, and five new invitations were extended until a convenience sample of ten participants was reached.
The inclusion criteria for the children were: eight to twelve years old (based on the profile and age limit for care at the CEO II) of either sex, The exclusion criteria included users of centrally acting drugs and/or patients with conditions that impaired their ability to understand and answer the questions. The inclusion criteria for parents were being the responsible companion during the initial interview and return visit. The exclusion criteria included illiteracy and/or conditions that impaired their ability to understand and answer the questions.
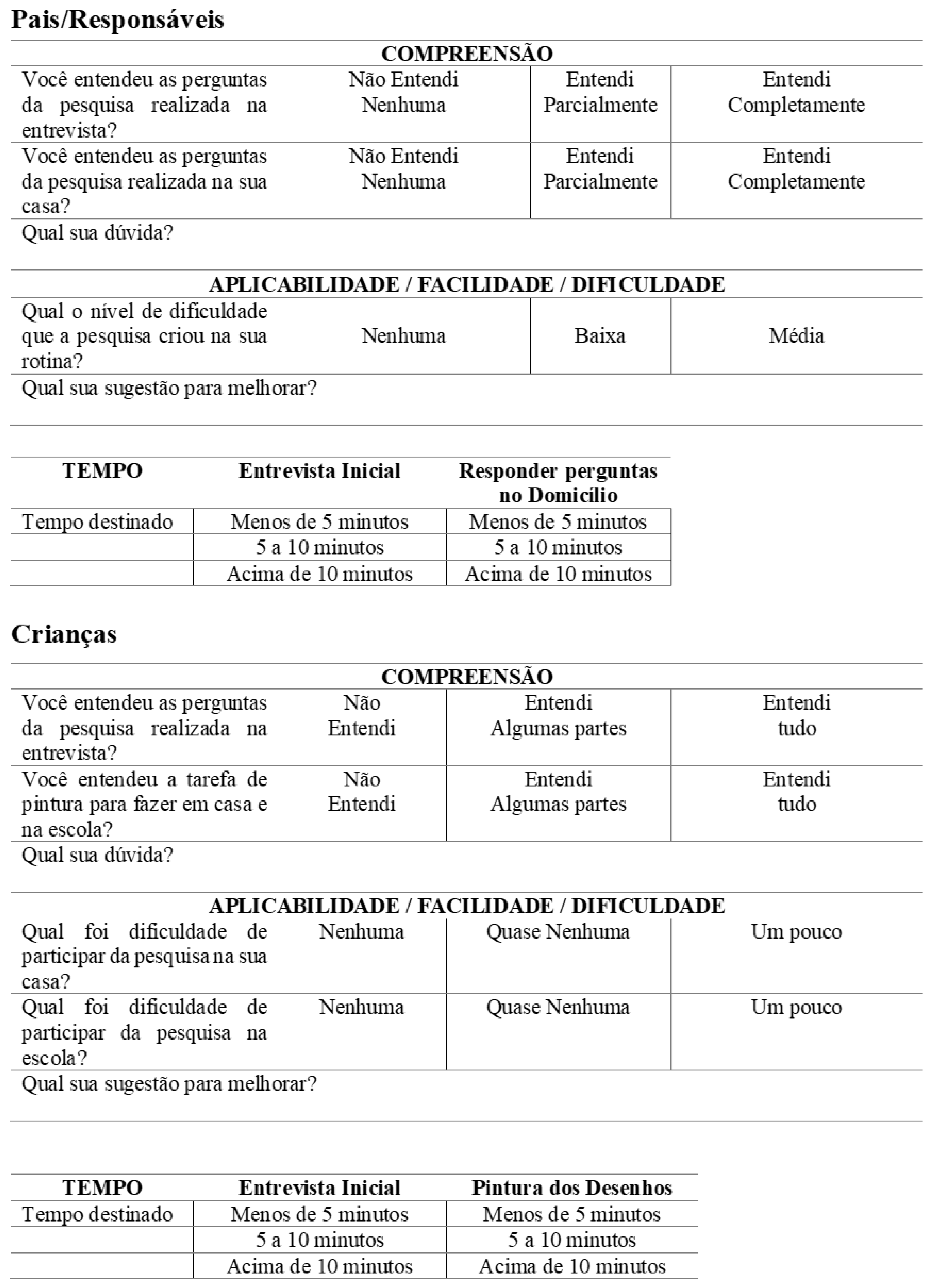
After acceptance, an anamnesis form was filled out (including the question about BS), and then the ABIT tool was applied by a single examiner (N. R. R. A) who had been properly trained (M. B. D. G.). Following this, a qualitative assessment of the ABIT items was conducted, focusing on comprehensibility, applicability, and temporal stability (Appendix A2), using a questionnaire with three-point Likert Scale [25] response options.
Comprehensibility was assessed based on responses regarding how well the questions were understood (Table 1/Appendix A2), and applicability (feasibility) was evaluated through questions about routine, ease/difficulty of participation, and the time taken to complete the form (Table 2/Appendix A2). Temporal stability (reliability) was assessed using a 'Test-Retest' method in a group of five participants, with a retest conducted after fifteen days.
Participants were also asked for suggestions, and adjustments were made based on their feedback. The results of the qualitative ABIT test, AB frequency, and the comparison of test and retest data will be presented descriptively.
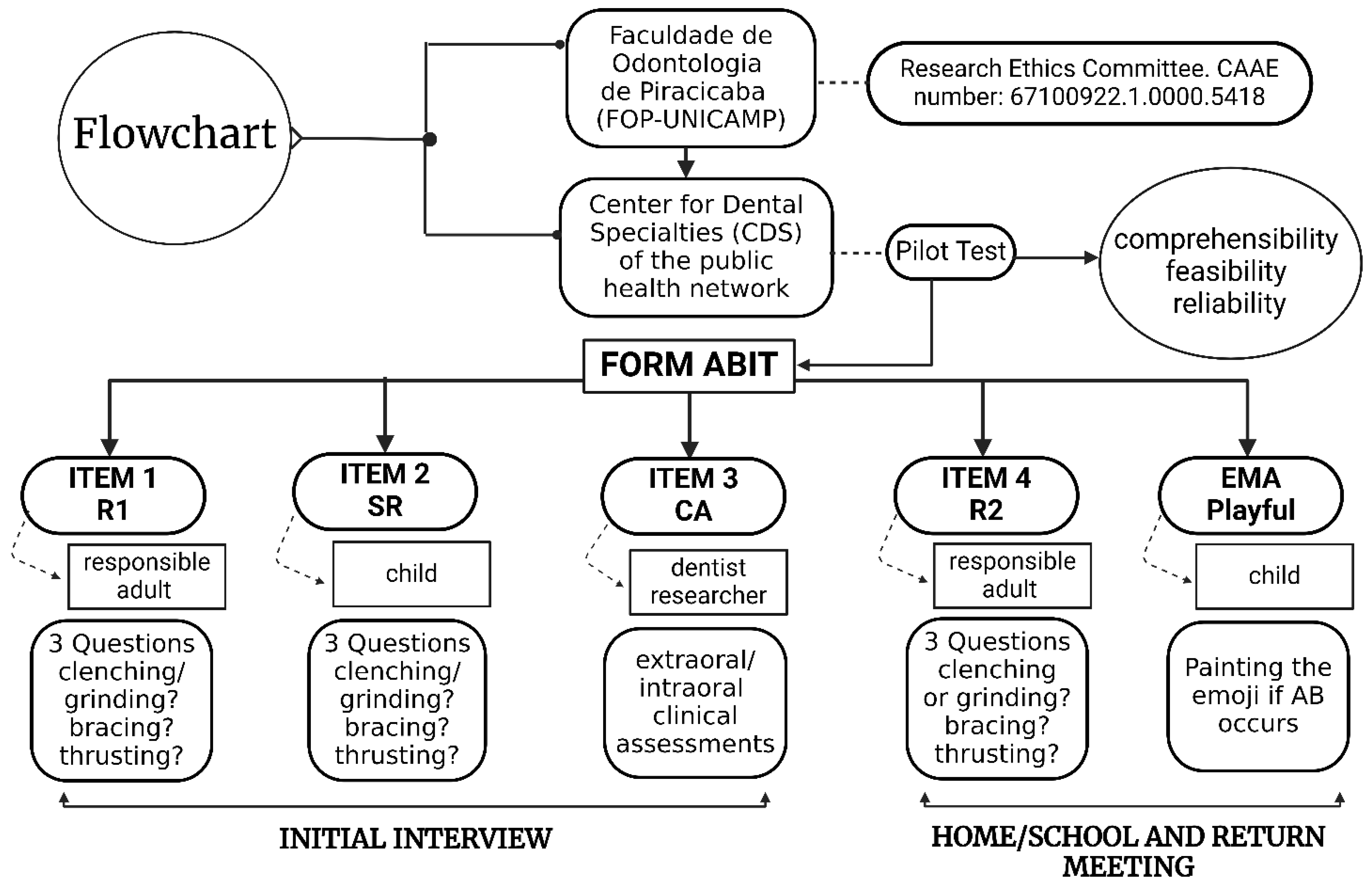
Figure 2.
Study methodology flowchart.
3. Results
3.1. Testing ABIT Items
In the evaluation of comprehensibility, six guardians said they fully understood the questions in the initial interview, while four said they partially understood. The recurring doubt referred to: “whether the answers should take SB into account”. Regarding the household questions, all guardians reported fully understanding them.
The ten children selected the item 'I understood everything' in relation to both the interview questions and the painting sheet task for home/school. One child expressed doubts about whether they could color the drawing later if the sheet was not available at the time. Despite this uncertainty, reported not having colored the drawing.
When assessing applicability, six guardians reported a 'low level of difficulty' in their routines, while four stated there was 'no difficulty at all. All the children reported that it was easy to participate in the survey, both at home and at school. Five children selected the item 'none' regarding the difficulty of participating at home, while the other five chose the item 'almost none’. Regarding the difficulty of participating at school, seven children selected 'none,' and three chose 'almost none.' In terms of the time taken to complete the survey, all participants, both adults and children, selected the option 'five to ten minutes.' As for suggestions for improvement, two mothers recommended that the home sheets be printed on a single page.
The results of the retests conducted with five children/guardians, aimed at assessing the temporal stability of the tool, are presented along with the test data (Table 2, Table 3 and Table 4) in the following section.
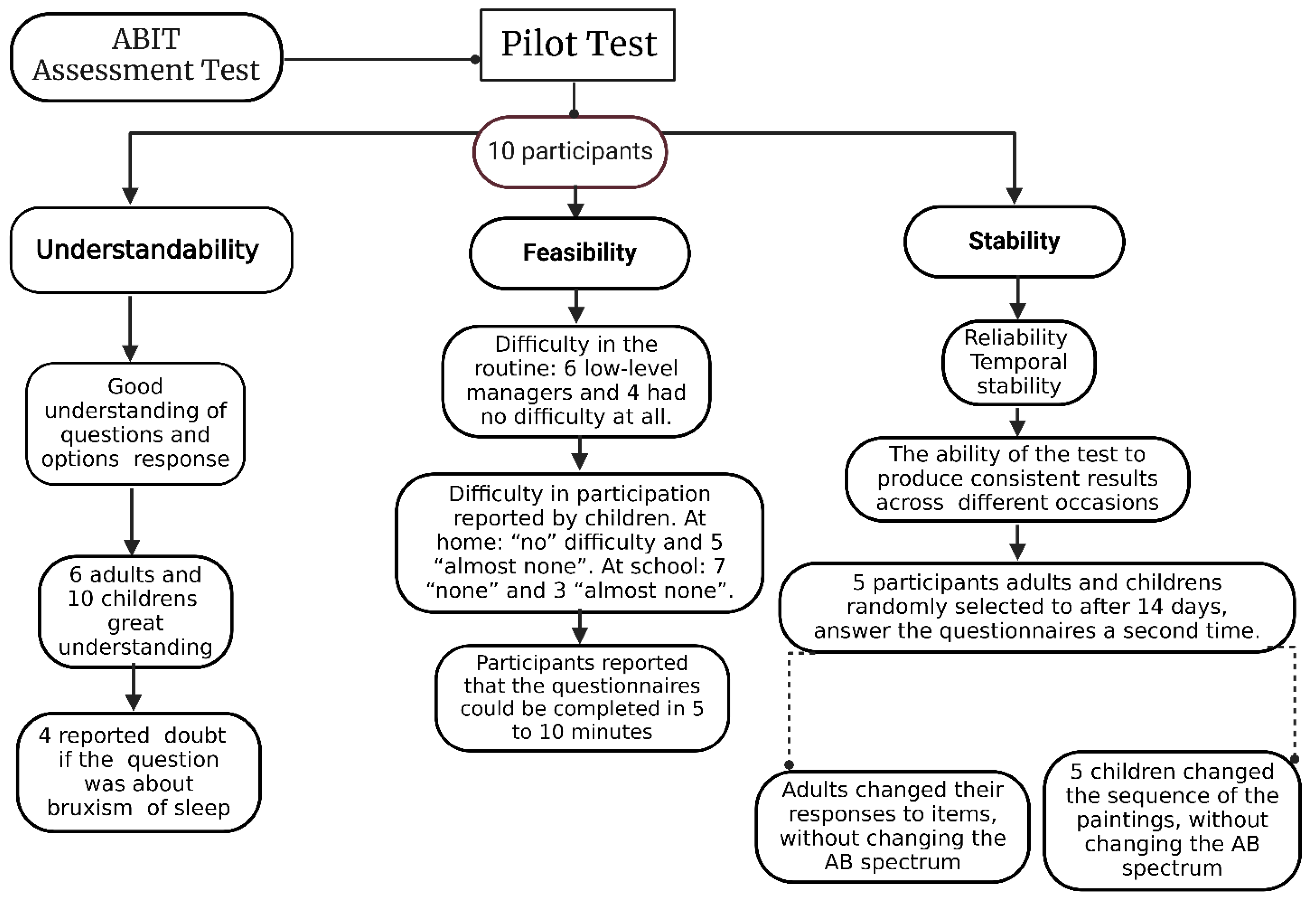
Figure 3.
Pilot test results on ABIT items.
3.2. AB frequency in the Test Group
The results on the frequency of AB (Table 2) pertain to the individualization of the AB spectrum within the sample of children/adolescents. In addition to the ABIT data of the Test (T) and Retest (R), we also present BS data based on parental perception, collected during the anamnesis.
The EMA report (Table 3) presents the records from D1 (Day 1) to D7 (Day 7) and the average number of paintings per day per child of the Test (T) and Retest (R), with a maximum of six paintings allowed per day.
The perceptions recorded (Table 4) display the type of AB event perceived (squeaking, squeezing, or bracing/thrusting) in both the parents' reports and the children's self-reports of the Test (T) and Retest (R)
The findings related to dental wear (Appendix B) revealed that grade 1 wear was identified in sixteen dental elements, grade 2 in six elements, while grades 3 and 4 were not detected in any tooth.
4. Discussion
4.1. About the Tool Development
The design of evaluation tools aims to contribute to prevalence studies and conditions that require further understanding [26], such as AB, which involves several aspects that need clarification, especially considering the larger number of studies related to SB [27]. Thus, the ABIT was designed to identify AB in children and adolescents from a 'Spectrum' perspective, moving away from the dichotomous 'Present versus Absent' approach. This aligns with suggestions [6] regarding the diagnosis of bruxism [2,6].
Instrumental methods, such as EMG, are considered the gold standard for identifying AB. However, due to limitations in assessment dynamics and cost, an alternative is to incorporate EMA [7] into the methodologies, with the potential to suggest 'Definitive AB' [8].
Therefore, ABIT, by integrating reports, self-reports, and clinical assessments into a scoring system for non-self-explanatory questions, requires the researcher's commitment to training the participant to recognize AB, particularly thrusting (muscle contraction) and bracing (mandibular projection) [1], as a lack of awareness among participants can affect the results [28], and parental education in recognizing AB is a significant variable [29]. Additionally, the employed of questionnaires with report and self-report, in most studies, aims to reduce reporting bias with parental collaboration (perceiving and recording daily behavior) [6,30].
Thus, EMA can enhance measurement accuracy [31], real-time self-perception [32], and awareness, in contrast to one-time reporting [20,33,34]. This is particularly important as AB is a behavior subject to variation, and its identification through retrospective self-report alone may fail to capture these variations [6]. Moreover, the frequency of AB measured with EMA may remain consistent over months [35]. EMA is typically recorded in apps, and their logs generate a report.
However, the cut-off point has been established [36] as 'four affirmative results' (when monitored concurrently with electromyography, based on the identification of four concordant entries between the two). Based on this, the ABIT EMA uses the parameter of ≥ 4, as it is the only alternative reference cut-off point, despite reflecting virtual EMA results. Analog-ludic EMA appears to be feasible and appropriate [37] when utilizing paper and pencil/pen [38], as it avoids the use of screens with children [39].
Documenting the behavior for seven consecutive days aligns with response rates that have shown no significant differences between weekdays and weekends [19]. Although tested without comparative references, a study combining analog EMA with reminders/stickers and digital EMA has already been documented [40].
Another item is CA, which is based on clinical markers [2] that define 'Probable AB' under strict criteria (ICA and ECA ≥ 1 concomitantly), due to the higher predictive value that the term 'probable' represents. ICA involves clinical inspection in accordance with previous recommendations [22,41]; while ECA examines visible and palpable muscle asymmetries [41,42,43,44], due to the correlation between AB, hypertrophy, and muscle myalgia [45]. Although some studies use imaging tests and photographs, ABIT offers a low-cost assessment. On the other hand, tooth wear is considered complementary data [44], as it may result from physiological wear or past behavior [46].
The ABIT aims to identify AB using simple clinical resources, In line with practical assessment tools [22,31]. Additionally, it aligns with the recommendations of the 'Standardized Tool for the Assessment of Bruxism' (STAB-Axis A) [18,47], despite not incorporating EMG, which is rarely included in research [48] due to the cost and software limitations for interpreting EMG in line with the current definition of bruxism [49].
The identification of AB in children and adolescents is complex [50]. The proposed scoring system serves as a strategy for the clinical interpretation of the items [51], based on Classical Test Theory (CTT), which asserts that 'the sum of the items provides information about the individual [52], although no studies have compared this data [53]. Nonetheless, initial impressions of the tool suggest that it effectively reflects the construct (AB) it aims to measure.
4.2. Pilot Test of the Tool
The pilot experiment aimed to evaluate the ABIT items by gathering feedback from participants and reflecting on their clinical interpretability [54], utilizing the 'probing' method [22]. The tool was well accepted, possibly due to the research team's management in handling interactions with parents and children, which is a crucial factor for the reproducibility of the method, considering that parental reports are the most commonly used data collection method in this type of study [29,18]. One challenge is maintaining objectivity in this type of data collection; however, efforts were made to design questions based on verifiable data, rather than on personal opinions or assumptions.
The comprehensibility assessment evaluated vocabulary, sentence complexity, linguistic clarity, and the understanding of the context in the formulation of the questions. It also tested the ease of comprehension by the participants, with results indicating no difficulties in answering the questions and no instances of non-response [55].
Regarding applicability, the ABIT proved to be a viable tool for use in the family routine, taking between 5 and 10 minutes to complete. These findings corroborate the results of the Bruxscreen [22]. In addition, it demonstrated reliability, as evidenced by the consistency of results [56] (p. 651). Despite variations in responses, the "Spectrum AB" remained unchanged after the retest.
The adjustments made to the tool involved adding a single reporting question on SB in items R1 and R2 to eliminate bias, as SB is better understood [9]. Simultaneously, secondary data were collected, considering that AB appears to be positively associated with indicators of poorer sleep quality [46], and that BS and AB may serve as predictors of each other [57,58].
"Based on the discussion, the ABIT was developed, tested, and appears to have fulfilled its purpose as a simplified tool for clinical investigation, in accordance with Bracci et al. [37], who state that new instruments with effective, clinically oriented research pathways are desirable. This facilitates the implementation of knowledge regarding AB metrics and contributes to a comprehensive understanding of the full awake bruxism spectrum."
4.3. Frequency of AB in the Pilot Group
The frequencies observed included 3 children with "Possible AB corroborated by EMA" and 4 with "Possible AB" among the ten children in the pilot group. While these data were useful for the initial application of the tool, they do not represent data that can be directly compared to larger studies. Nevertheless, it is anticipated that the ABIT may contribute to the collection of data on AB in children and adolescents, given that the global prevalence rate (AB and SB) in this group ranges from 5% to 50% [9], with a recent global finding of 22.22% (SB and AB) and 23% (AB) [10].
Another aspect concerns the nature of the perceived AB event. In the present study, the highest mean was recorded for teeth clenching, followed by muscle contraction with bracing or thrusting and teeth grinding. In contrast, a study conducted in 2018 identified teeth grinding as the most frequent event, followed by muscle contraction [59]. Although a direct comparison between these studies is not possible, these findings reinforce the current approaches to address the events (traits) of AB in the natural environment [59].
The term “corroborated by EMA” highlights the effort to enhance the accuracy of AB recognition, as self-report alone can be prone to questionable accuracy [36] and may provide insufficient certainty regarding AB frequency [60]. Additionally, the findings of positive EMA were consistent with positive parental reports, which may indicate the potential for future validation of analog EMA. On the other hand, a discrepancy was observed in one child who had a positive self-report but a null EMA. Null EMA scores were also common among five children, indicating that they perceived some “trace of AB” on one or more occasions, but below the cut-off point (<4). This suggests the possibility of sporadic, low-level AB, which could only be more accurately analyzed through continuous follow-ups, without relying on specific cut-off points [54].
Another aspect observed was that, although there was no change in the AB spectrum with the retest, there was a decrease in the rates for parental reports, self-reports, and EMA. It is difficult to determine which of the assessment moments more accurately reflects reality, although there is a greater tendency to trust the retest due to its association with a longer training period for observation. This may be linked to the hypothesis of raising awareness and behavioral re-education, as proposed in the Ecological Momentary Intervention (EMI) framework [61]. Other hypotheses include the reduction of the confounding factor between AB and SB, which may have influenced responses about SB in the initial assessment, as well as the possibility that participants may have based their responses in the first moment on past behaviors.
As for the clinical markers (particularly hyperkeratosis, indentations, presence of the linea alba, and masseter hypertrophy), which did not influence the "AB Spectrum" in the present study, they cannot be excluded from future analyses, as they are associated with AB in the young adult population. Furthermore, the data collected represent the results of an initial test on a small convenience sample, and it is essential that the CA is maintained for the larger study planned to assess the reproducibility of the ABIT.
This study has several limitations: the potential occurrence of AB behavior at times when the tool is not accessible to the child (e.g., during bathroom use, outings, birthdays, physical activities, school courses, or tests); complete dependence on the collaboration and commitment of the participants, which introduces the potential bias of behavioral differences in adherence; and the possibility of forgetfulness or distraction during the observation and recording process (spontaneous analog EMA).
knowing that the establishment of non-instrumental methods for AB is problematic [62], the research team is considering the development of a strategy, such as a children's watch or wristband with a programmed random alarm, or an auditory device worn as a wristband. This suggestion, however, requires further refinement and consideration after the tool has been tested on more representative samples.
5. Conclusions
The present study described a proposed tool for defining AB in spectra, which, when tested on a pilot group, demonstrated satisfactory comprehensibility, applicability, and reliability. The results indicated the presence of children in the categories of "Possible AB" and "Possible AB corroborated by EMA."
The analog and playful EMA shows promising potential for validation and clinical application. The reproducibility of ABIT appears adequate for the planned expanded study, with expectations for its translation and cross-cultural adaptation, which may significantly contribute to clinical research involving children and adolescents.
Appendix A1: Appendix A2 e Appendix B: This Appendix contains the ABIT, ABIT Test Items and Dental wear results. The respective language is in Brazilian Portuguese. English versions, not cross-culturally translated, can be requested from the authors.
Author Contributions
“Conceptualization, N.R.R.A., M.B.D.G. and C.R.V.M; methodology, N.R.R.A. and M.B.D.G; formal analysis, N.R.R.A. and M.B.D.G; investigation, N.R.R.A.; data curation, N.R.R.A. and M.B.D.G; writing, N.R.R.A., M.B.D.G, A.C.F.d.S and C.R.V.M; supervision, M.B.D.G; project administration, N.R.R.A., M.B.D.G, A.C.F.d.S and C.R.V.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Research Ethics Committee of FOP-UNICAMP, Piracicaba, SP, Brazil (protocol code: 67100922.1.0000.5418, dated 18 May 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
This study thanks the institutions that made it possible to carry out this study: Faculdade de Odontologia de Piracicaba - Universidade Estadual de Campinas and Oral health coordination - Prefeitura Municipal de Piracicaba.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Appendix A.1 - Awake Bruxism Identification Tool (ABIT) in Brazilian Portuguese
Appendix A.2
Pilot Test of items the Tool: Questions of pilot test in Brazilian Portuguese
A2 Pilot Test of items the Tool. Questions de understandability, feasibility and stability in language Portuguese. Source: developed by research
Appendix B - Dental Wear Results
| Participant | Degree 0 | Degree 1 | Degree 2 | Degree 3 | Degree 4 |
| 1 | 24 | 0 | 0 | 0 | 0 |
| 2 | 22 | 2 | 0 | 0 | 0 |
| 3 | 24 | 0 | 0 | 0 | 0 |
| 4 | 19 | 4 | 1 | 0 | 0 |
| 5 | 20 | 4 | 0 | 0 | 0 |
| 6 | 22 | 0 | 2 | 0 | 0 |
| 7 | 19 | 5 | 0 | 0 | 0 |
| 8 | 20 | 1 | 3 | 0 | 0 |
| 9 | 22 | 0 | 0 | 0 | 0 |
| 10 | 26 | 0 | 0 | 0 | 0 |
| B Note: Individualized Data of Dental wear. Five-point ordinal grading scale: Grade 0 = no visible wear; Grade 1 = visible enamel wear; Grade 2 = visible wear with dentin exposure and loss of clinical crown height ≤ 1/3; Grade 3 = loss of clinical crown height >1/3 but < 2/3; Grade 4 = loss of clinical crown height ≥ 2/3 [5], with attention to distinguishing it from chemical wear, based on specific criteria [23,24]. Source: data by research (ICA-ABIT). | |||||
References
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; de Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism defined and graded: An international consensus. J. Oral. Rehabil. 2013, 40, 2–4. [Google Scholar] [CrossRef] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Raphael, K.G.; Santiago, V.; Lobbezoo, F. Is bruxism a disorder or a behaviour? Rethinking the international consensus on defining and grading of bruxism. J. Oral Rehabil. 2016, 43, 791–798. [Google Scholar] [CrossRef]
- Manfredini, D.; Arreghini, A.; Lombardo, L.; Visentin, A.; Cerea, S.; Castroflorio, T.; Siciliani, G. Assessment of Anxiety and Coping Features in Bruxers: A Portable Electromyographic and Electrocardiographic Study. J. Oral Facial Pain Headache 2016, 30, 249–254. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Naeije, M. A reliability study of clinical tooth wear measurements. J. Prosthet. Dent. 2001, 86, 597–602. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Lobbezoo, F. Bruxism definition: Past, present, and future—What should a prosthodontist know? J. Prosthet. Dent. 2022, 128, 905–912. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Câmara-Souza, M.B.; Carvalho, A.G.; Figueredo, O.M.C.; Bracci, A.; Manfredini, D.; Rodrigues Garcia, R.C.M. Awake bruxism frequency and psychosocial factors in college preparatory students. Cranio 2023, 41, 178–184. [Google Scholar] [CrossRef]
- Storari, M.; Serri, M.; Aprile, M.; Denotti, G.; Viscuso, D. Bruxism in children: What do we know? Narrative Review of the current evidence. Eur J Paediatr Dent. 2023, 24, 207–210. [Google Scholar] [CrossRef]
- Zieliński, G.; Pająk, A.; Wójcicki, M. Global Prevalence of Sleep Bruxism and Awake Bruxism in Pediatric and Adult Populations: A Systematic Review and Meta-Analysis. J Clin Med. 2024, 13, 4259. [Google Scholar] [CrossRef]
- Friedman Rubin, P.; Erez, A.; Peretz, B.; Birenboim-Wilensky, R.; Winocur, E. Prevalence of bruxism and temporomandibular disorders among orphans in southeast Uganda: A gender and age comparison. Cranio 2018, 36, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Wetselaar, P.; Vermaire, E.J.H.; Lobbezoo, F.; Schuller, A.A. The prevalence of awake bruxism and sleep bruxism in the Dutch adolescent population. J. Oral. Rehabil 2021, 48, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, J.M.D.; Pauletto, P. , Massignan, C., D'Souza, N.; Gonçalves, D.A.G., Flores-Mir, C.; De Luca Canto, G. Prevalence of awake Bruxism: A systematic review. J. Dent. 2023, 138, 104715. [Google Scholar] [CrossRef]
- Guimarães, J.K.; Lucietto, T.M.; Scheffel, D.L.S.; Ramos, A.L.; Provenzano, M.G.A. Sleep and Awake Bruxism in Pediatric Patients: A Cross-Sectional Study of Prevalence and Associated Factors. J. Adv. Med. Med. Res. 2024, 36, 109–119. [Google Scholar] [CrossRef]
- Colonna, A.; Bracci, A.; Ahlberg, J.; Câmara-Souza, M.B.; Bucci, R.; Conti, P.C.R.; Dias, R.; Emodi-Perlmam, A.; Favero, R.; Häggmän-Henrikson, B.; Michelotti, A.; Nykänen, L.; Stanisic, N.; Winocur, E.; Lobbezoo, F.; Manfredini, D. Ecological Momentary Assessment of Awake Bruxism Behaviors: A Scoping Review of Findings from Smartphone-Based Studies in Healthy Young Adults. J Clin Med. 2023, 28, 1904. [Google Scholar] [CrossRef]
- Runyan, J.D.; Steinke, E.G. Virtues, ecological momentary assessment/intervention and smartphone technology. Front Psychol. 2015, 6, 6–481. [Google Scholar] [CrossRef]
- Manfredini, D.; Bracci, A.; Djukic, G. BruxApp: the ecological momentary assessment of awake bruxism. Minerva Stomatol. 2016, 65, 252–255. [Google Scholar]
- Manfredini, D.; Ahlberg, J.; Aarab, G.; Bracci, A.; Durham, J.; Ettlin, D.; Gallo, L.M.; Koutris, M.; Wetselaar, P.; Svensson, P.; Lobbezoo, F. Towards a Standardized Tool for the Assessment of Bruxism (STAB)-Overview and general remarks of a multidimensional bruxism evaluation system. J Oral Rehabil. 2020, 47, 549–556. [Google Scholar] [CrossRef]
- Colonna, A.; Lombardo, L.; Siciliani, G.; Bracci, A.; Guarda-Nardini, L.; Djukic, G.; Manfredini, D. Smartphone-based application for EMA assessment of awake bruxism: compliance evaluation in a sample of healthy young adults. Clin Oral Investig. 2020, 24, 1395–1400. [Google Scholar] [CrossRef]
- Emodi-Perlman, A.; Manfredini, D.; Shalev, T.; Yevdayev, I.; Frideman-Rubin, P.; Bracci, A.; Arnias-Winocur, O.; Eli, I. Awake Bruxism-Single-Point Self-Report versus Ecological Momentary Assessment. J. Clin. Med. 2021, 10, 1699. [Google Scholar] [CrossRef]
- Zani, A.; Lobbezoo, F.; Bracci, A.; Djukic, G.; Guarda-Nardini, L.; Favero, R.; Ferrari, M.; Aarab, G.; Manfredini, D. Smartphone-based evaluation of awake bruxism behaviours in a sample of healthy young adults: findings from two University centres. J Oral Rehabil. 2021, 48, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Lobbezoo, F.; Ahlberg, J.; Verhoeff, M.C.; Aarab, G.; Bracci, A.; Koutris, M.; Nykänen, L.; Thymi, M.; Wetselaar, P.; Manfredini, D. The bruxism screener (BruxScreen): Development, pilot testing and face validity. J Oral Rehabil. 2023, 51, 13442. [Google Scholar] [CrossRef]
- Atalay, C.; Ozgunaltay, G. Evaluation of tooth wear and associated risk factors: A matched case-Control study. Niger J Clin Pract. 2018, 21, 1607–1614. [Google Scholar] [CrossRef]
- Schlueter, N.; Luka, B. Erosive tooth wear - a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018, 224, 364–370. [Google Scholar] [CrossRef]
- Likert, R. A Technique for the Measurement of Attitudes. Archives of Psychology 1932, 140, 5. [Google Scholar]
- Ministério da Saúde. Lei nº 8.080; Diário Oficial da União: Brasil, 1990. [Google Scholar]
- Castrillon, E.E.; Ou, K.L.; Wang, K.; Zhang, J.; Zhou, X.; Svensson, P. Sleep bruxism: an updated review of an old problem. Acta Odontol Scand. 2016, 74, 328–334. [Google Scholar] [CrossRef]
- Saracutu, O.I.; Manfredini, D.; Bracci, A.; Val, M.; Ferrari, M.; Colonna, A. Comparison Between Ecological Momentary Assessment and Self-Report of Awake Bruxism Behaviours in a Group of Healthy Young Adults. J Oral Rehabil. 2025, 52, 289–295. [Google Scholar] [CrossRef]
- Alves, C.L.; Fagundes, D.M.; Soares, P.B.F.; Ferreira, M.C. Knowledge of parents/caregivers about bruxism in children treated at the pediatric dentistry clinic. Sleep Sci. 2019, 12, 185–189. [Google Scholar] [CrossRef]
- Leal, T.R.; de Lima, L.C.M.; Neves, É.T. B.; Arruda, M.J.A.L.L.A.; Perazzo, M.F.; Paiva, S.M.; Serra-Negra, J.M.; Ferreira, F.M.; Granville-Garcia, A.F. Factors associated with awake bruxism according to perceptions of parents/guardians and self-reports of children. Int J Paediatr Dent. 2022, 32, 22–30. [Google Scholar] [CrossRef]
- Bracci, A.; Lobbezoo, F.; Häggman-Henrikson, B.; Colonna, A.; Nykänen, L.; Pollis, M.; Ahlberg, J.; Manfredini, D. International Network For Orofacial Pain And Related Disorders Methodology INfORM. Current Knowledge and Future Perspectives on Awake Bruxism Assessment: Expert Consensus Recommendations. J Clin Med. 2022, 11, 5083. [Google Scholar] [CrossRef]
- Saracutu, O.I.; Manfredini, D.; Bracci, A.; Ferrari Cagidiaco, E.; Ferrari, M.; Colonna, A. Awake bruxism behaviors frequency in a group of healthy young adults with different psychological scores. Cranio. 2024, 7, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bucci, R.; Manfredini, D.; Lenci, F.; Simeon, V.; Bracci, A.; Michelotti, A. Comparison between Ecological Momentary Assessment and Questionnaire for Assessing the Frequency of Waking-Time Non-Functional Oral Behaviours. J. Clin. Med. 2022, 11, 5880. [Google Scholar] [CrossRef] [PubMed]
- Dias, R.; Vaz, R.; Rodrigues, M.J.; Serra-Negra, J.M.; Bracci, A.; Manfredini, D. Utility of Smartphone-based real-time report (Ecological Momentary Assessment) in the assessment and monitoring of awake bruxism: A multiple-week interval study in a Portuguese population of university students. J Oral Rehabil. 2021, 48, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Colonna, A.; Lobbezoo, F.; Bracci, A.; Ferrari, M.; Val, M.; Manfredini, D. Long-Term Study on the Fluctuation of Self-Reported Awake Bruxism in a Cohort of Healthy Young Adults. J Oral Rehabil. 2025, 52, 37–42. [Google Scholar] [CrossRef]
- Asami, K.; Fujisawa, M.; Saito-Murakami, K.; Miura, S.; Fujita, T.; Imamura, Y.; Koyama, S. Assessment of awake bruxism-Combinational analysis of ecological momentary assessment and electromyography. J Prosthodont Res. 2024, 68, 166–171. [Google Scholar] [CrossRef]
- Bracci, A.; Lobbezoo, F.; Colonna, A.; Bender, S.; Conti, P.C.R.; Emodi-Perlman, A.; Häggman-Henrikson, B.; Klasser, G.D.; Michelotti, A.; Lavigne, G.J.; Svensson, P.; Ahlberg, J.; Manfredini, D. Research routes on awake bruxism metrics: Implications of the updated bruxism definition and evaluation strategies. J Oral Rehabil. 2024, 51, 150–161. [Google Scholar] [CrossRef]
- Kwasnicka, D.; Kale, D.; Schneider, V.; Keller, J.; Yeboah-Asiamah Asare, B.; Powell, D.; Naughton, F.; Ten Hoor, G.A.; Verboon, P.; Perski, O. Systematic review of ecological momentary assessment (EMA) studies of five public health-related behaviours: review protocol. BMJ Open. 2021, 11, e046435. [Google Scholar] [CrossRef]
- Brostolin, M.R.; Souza, T.M.F. de. A docência na educação infantil: pontos e contrapontos de uma educação inclusiva. Cad CEDES 2023, 43, 52–62. [Google Scholar] [CrossRef]
- Poluha, R.L.; Macário, H.S.; Câmara-Souza, M.B.; De la Torre Canales, G.; Ernberg, M.; Stuginski-Barbosa, J. Benefits of the combination of digital and analogic tools as a strategy to control possible awake bruxism: A randomised clinical trial. J Oral Rehabil. 2024, 51, 917–923. [Google Scholar] [CrossRef]
- Martins, I.M.; Vale, M.P.; Alonso, L.S.; Abreu, L.G.; Tourino, L.F.P.G.; Serra-Negra, J.M.C. Association Between Probable Awake Bruxism and School Bullying in Children and Adolescents: A Case-Control Study. Pediatr Dent. 2022, 44, 284–289. [Google Scholar]
- Lavigne, G.J.; Rompré, P.H.; Montplaisir, J.Y. Sleep bruxism: validity of clinical research diagnostic criteria in a controlled polysomnographic study. J Dent Res. 1996, 75, 546–552. [Google Scholar] [CrossRef] [PubMed]
- Giudice, M.; Marra, A.; Barba, A.; Passariello, N.; D'Onofrio, F. Hypertrophy of the masseter: a rare case associated with hypertrophic cardiomyopathy. Minerva stomatol 1992, 41, 535–542. [Google Scholar] [PubMed]
- Prado, I.M.; Abreu, L.G.; Pordeus, I.A.; Amin, M.; Paiva, S.M.; Serra-Negra, J.M. Diagnosis and prevalence of probable awake and sleep bruxism in adolescents: an exploratory analysis. Braz Dent J. 2023, 34, 9–24. [Google Scholar] [CrossRef] [PubMed]
- Nykänen, L.; Manfredini, D.; Lobbezoo, F.; Kämppi, A.; Bracci, A.; Ahlberg, J. Assessment of awake bruxism by a novel bruxism screener and ecological momentary assessment among patients with masticatory muscle myalgia and healthy controls. J Oral Rehabil. 2024, 51, 162–169. [Google Scholar] [CrossRef]
- Hilgenberg-Sydney, P.B.; Lorenzon, A.L.; Pimentel, G.; Petterle, R.R.; Bonotto, D. Probable awake bruxism - prevalence and associated factors: a cross-sectional study. Dental Press J Orthod. 2022, 27, e2220298. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Aarab, G.; Bender, S.; Bracci, A.; Cistulli, P.A.; Conti, P.C.; De Leeuw, R.; Durham, J.; Emodi-Perlman, A.; Ettlin, D.; Gallo, L.M.; Häggman-Henrikson, B.; Hublin, C.; Kato, T.; Klasser, G.; Koutris, M.; Lavigne, G.J.; Paesani, D.; Peroz, I.; Svensson, P.; Wetselaar, P.; Lobbezoo, F. Standardised Tool for the Assessment of Bruxism. J Oral Rehabil. 2024, 51, 29–58. [Google Scholar] [CrossRef]
- Manfredini, D.; Lobbezoo, F. Sleep bruxism and temporomandibular disorders: A scoping review of the literature. J Dent. 2021, 111, 103711. [Google Scholar] [CrossRef]
- Colonna, A.; Noveri, L.; Ferrari, M.; Bracci, A.; Manfredini, D. Electromyographic Assessment of Masseter Muscle Activity: A Proposal for a 24 h Recording Device with Preliminary Data. J Clin Med. 2022, 12, 247. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Jacobs, R.; De Laat, A.; Aarab, G.; Wetselaar, P.; Manfredini, D. Kauwen op bruxisme. Diagnostiek, beeldvorming, epidemiologie en oorzaken [Chewing on bruxism. Diagnosis, imaging, epidemiology and aetiology]. Ned Tijdschr Tandheelkd. 2017, 124, 309–316. [Google Scholar] [CrossRef]
- DeVellis, R.F. Classical test theory. Med Care. 2006, 44 (Suppl 3), S50–S59. [Google Scholar] [CrossRef]
- Pasquali, L. Psicometria. Rev esc enferm USP [Internet] 2009, 43, 992–999. [Google Scholar] [CrossRef]
- De Vet, H.; Terwee, C.; Mokkink, L.; Knol, D. Measurement in Medicine: A Practical Guide, 1 ed.; Cambridge University Press: Cambridge, Brazil, 2011; pp. 1–338. [Google Scholar]
- Manfredini, D.; Ahlberg, J.; Wetselaar, P.; Svensson, P.; Lobbezoo, F. The bruxism construct: From cut-off points to a continuum spectrum. J Oral Rehabil. 2019, 46, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Neuert, C.E.; Kunz, T.; Gummer, T. An empirical evaluation of probing questions investigating question comprehensibility in web surveys. Int. J. Soc. Res. 2024, 2024, 1–12. [Google Scholar] [CrossRef]
- de Souza, A.C.; Alexandre, N.M.C.; Guirardello, E. de B. Propriedades psicométricas na avaliação de instrumentos: avaliação da confiabilidade e da validade. Epidemiol. Serv. Saúde 2017, 26, 649–659. [Google Scholar] [CrossRef]
- Winocur, E.; Messer, T.; Eli, I.; Emodi-Perlman, A.; Kedem, R.; Reiter, S.; Friedman-Rubin, P. Awake and Sleep Bruxism Among Israeli Adolescents. Front. Neurol. 2019, 10, 443. [Google Scholar] [CrossRef]
- Marceliano, C.R.V.; Gavião, M.B.D. Possible sleep bruxism and biological rhythm in school children. Clin Oral Investig. 2023, 27, 2979–2992. [Google Scholar] [CrossRef]
- Bracci, A.; Djukic, G.; Favero, L.; Salmaso, L.; Guarda-Nardini, L.; Manfredini, D. Frequency of awake bruxism behaviours in the natural environment. A 7-day, multiple-point observation of real-time report in healthy young adults. J Oral Rehabil. 2018, 45, 423–429. [Google Scholar] [CrossRef]
- Goldstein, R.E.; Auclair, C.W. The clinical management of awake bruxism. J Am Dent Assoc. 2017, 148, 387–391. [Google Scholar] [CrossRef]
- Zani, A.; Lobbezoo, F.; Bracci, A.; Ahlberg, J.; Manfredini, D. Ecological Momentary Assessment and Intervention Principles for the Study of Awake Bruxism Behaviors, Part 1: General Principles and Preliminary Data on Healthy Young Italian Adults. Front Neurol. 2019, 10, 169. [Google Scholar] [CrossRef]
- Walentek, N.P.; Schäfer, R.; Bergmann, N.; Franken, M.; Ommerborn, M.A. Relationship between Sleep Bruxism Determined by Non-Instrumental and Instrumental Approaches and Psychometric Variables. Int J Environ Res Public Health. 2024, 21, 543. [Google Scholar] [CrossRef]

Table 1.
Scoring and interpretation of ABIT items.
| Item | Scores | Cutoff Values | Clinical Interpretation Possibilities | AB Spectrum |
|---|---|---|---|---|
| R1 | 0 a 4 | Greater than or equal to 1* | Possible | 12 |
| SR | 0 a 4 | Greater than or equal to 1* | Possible | 12 |
| R2 | 0 a 4 | Greater than or equal to 1* | Possible | 12 |
| ICA | 0 a 6 | Greater than or equal to 1* | Probable | 6 |
| ECA | 0 a 2 | Greater than or equal to 1* | Probable | 2 |
| EMA | 0 a 42 | Greater than or equal to 4 days with paintings |
Possible corroborated by EMA Probable corroborated by EMA |
42 |
| 96 |
1Note: Score R1, R2 and SR: Likert Scala of 5 points. *value 1 is only considered valid if another.Item scores higher than 0. **value 1 is only valid if ECA and ICA are above 0.
Table 2.
Test and Retest Results for ABIT Items.
| Stage | Participant | Clinic Score |
Score R1 | Score R2 | Score SR | EMA | Score ABIT |
Spectrum AB | SB |
|---|---|---|---|---|---|---|---|---|---|
| T | 1 | 1 | 3 | 4 | 3 | 13 | 24 | Possible AB corroborated by EMA | Yes |
| T | 2 | 0 | 0 | Null | 0 | 0 | 0 | No AB | No |
| T | 3 | 0 | 0 | 0 | 0 | 0 | 0 | No AB | Yes |
| T | 4 | 2 | 3 | 4 | 5 | 7 | 21 | Possible AB corroborated by EMA | No |
| T | 5 | 0 | 0 | 0 | Null | <4 | 0 | No AB | No |
| T | 6 | 0 | 0 | 0 | 0 | <4 | 0 | No AB | No |
| T | 7 | 0 | 2 | 3 | 4 | <4 | 9 | Possible AB | Yes |
| T | 8 | 0 | 0 | 0 | Null | <4 | 0 | No AB | No |
| T | 9 | 0 | 4 | 4 | 8 | 12 | 28 | Possible AB corroborated by EMA | DK |
| T | 10 | 0 | 0 | 0 | Null | <4 | 0 | No AB | No |
| T | 1 | 1 | 3 | 4 | 3 | 13 | 24 | Possible AB corroborated by EMA | |
| R | 1 | 4 | 5 | 4 | 8 | 22 | Possible AB corroborated by EMA | ||
| T | 4 | 2 | 3 | 4 | 5 | 7 | 21 | Possible AB corroborated by EMA | |
| R | 2 | 3 | 5 | 6 | 5 | 21 | Possible AB corroborated by EMA | ||
| T | 6 | 0 | 0 | 0 | 0 | <4 | 0 | No AB | |
| R | 0 | 0 | 0 | 0 | 0 | 0 | No AB | ||
| T | 8 | 0 | 0 | 0 | Null | <4 | 0 | No AB | |
| R | 0 | 0 | 0 | 0 | 0 | 0 | No AB | ||
| T | 10 | 0 | 0 | 0 | Null | <4 | 0 | No AB | |
| R | 0 | 0 | 0 | Null | <4 | 0 | No AB |
2Note: Score R1, R2 and SR: Likert Scale of 5 points. *value 1 is only considered valid if another item scores higher than 0. **value 1 is only valid if ECA and ICA are above 0.
Table 3.
Number of times each condition was indicated in the Test and Retest.
| Stage | AB Behavior | Parent´s Relats R1 |
Parent´s Relats R2 |
Child´s SR |
Total |
|---|---|---|---|---|---|
| Test | Teeth Griding | 1 | 0 | 4 | 5 |
| Retest | Teeth Griding | 0 | 0 | 3 | 3 |
| Test | Teeth Clenching | 1 | 5 | 5 | 11 |
| Retest | Teeth Clenching | 2 | 2 | 3 | 7 |
| Test | Mandible Bracing/Thrusting | 3 | 4 | 3 | 10 |
| Retest | Mandible Bracing/Thrusting | 2 | 2 | 1 | 5 |
3 Note: List of behaviors that characterize AB: Griding|Clenching|Mandible Bracing/Thrusting.
Table 4.
EMA Report of 7 days and average paintings per child in Test and Retest.
| Stage | Participant | D1 | D2 | D3 | D4 | D5 | D6 | D7 | Mean |
|---|---|---|---|---|---|---|---|---|---|
| Test | 1 | 1 | 2 | 1 | 3 | 3 | 2 | 1 | 1,85 |
| Test | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Test | 3 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Test | 4 | 2 | 1 | 0 | 0 | 1 | 1 | 2 | 1,00 |
| Test | 5 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0.14 |
| Test | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0,14 |
| Test | 7 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0.14 |
| Test | 8 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0,28 |
| Test | 9 | 2 | 2 | 0 | 1 | 2 | 2 | 3 | 1,71 |
| Test | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0,14 |
| Test versus retest | |||||||||
| Test | 1 | 1 | 2 | 1 | 3 | 3 | 2 | 1 | 1,85 |
| Retest | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 2 | 1 |
| Test | 4 | 2 | 1 | 0 | 0 | 1 | 1 | 2 | 1 |
| Retest | 4 | 1 | 0 | 2 | 1 | 0 | 0 | 1 | 0,71 |
| Test | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0,14 |
| Retest | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Test | 8 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 0,14 |
| Retest | 8 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Test | 10 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0,14 |
| Retest | 10 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0,14 |
4 Abbreviations: D1, Day one; D2, Day two; D3, Day three; D4; Day four; D5, Day five; D6, Day six; D7, Day seven.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



