
Submitted:
02 April 2025
Posted:
03 April 2025
You are already at the latest version
Abstract
Background/Objectives: Sacituzumab govitecan (SG) is an antibody-drug conjugate targeting Trop-2, approved for use in metastatic triple-negative breast cancer (mTNBC) and more recently in hormone receptor-positive/HER2-negative (mHRPBC) subtypes. While clinical trials have demonstrated its efficacy, real-world da-ta—especially involving both molecular subtypes—remain scarce. This multicenter, retrospective study aimed to evaluate the real-life effectiveness, safety, and prognostic factors associated with SG treatment in patients with both mTNBC and mHRPBC. Methods: A total of 68 patients treated with SG between 2022 and 2025 were included from multiple oncology centers in Turkey. Patients with mTNBC were required to have received at least one prior chemotherapy line, while mHRPBC patients had received at least two prior chemotherapy lines in addition to hormone therapy. Clinical out-comes—including progression-free survival (PFS), overall survival (OS), and objective response rate (ORR)—were evaluated. Univariate and multivariate analyses were performed to identify factors influencing outcomes. Adverse events (AEs) were also documented and graded according to NCI-CTCAE v5.0. Results: The cohort included 35 (51.5%) mTNBC and 33 (48.5%) mHRPBC patients. The median PFS was 6.1 months, and the median OS was 12.5 months, with no significant differences between subtypes. The ORR was 52.9%, with a complete response observed in 10.3% of patients. Eastern cooperative oncology group performance status (ECOG PS) and liver metastasis were independent predictors of poorer PFS and OS. Prior immunotherapy did not negatively impact SG efficacy. SG was generally well tolerated; the most common AEs were alo-pecia, anemia, neutropenia, and diarrhea. Treatment discontinuation due to AEs was rare (2.9%). Conclusions: SG demonstrated comparable effectiveness and a managea-ble safety profile in real-world patients with both mTNBC and mHRPBC. Importantly, this study provides one of the first real-world datasets evaluating SG in the mHRPBC subgroup, highlighting its potential role beyond clinical trials. These results support SG as a valuable therapeutic option in heavily pretreated patients, warranting further prospective and biomarker-driven studies.
Keywords:
Sacituzumab govitecan
; real-world data
; metastatic breast cancer
; triple-negative breast cancer
; hormone receptor-positive breast cancer
; Trop-2
; antibody-drug conjugate
1. Introduction
Breast cancer remains the most frequently diagnosed malignancy in women worldwide. Despite significant progress in screening methods and systemic treatment options, breast cancer continues to result in substantial clinical challenges, particularly in its advanced stages [1,2].
Metastatic hormone receptor-positive, HER2-negative (mHRPBC) breast cancer constitutes approximately 70% of all cases and is typically managed with endocrine therapies in combination with targeted agents, such as cyclin-dependent kinase 4 and 6 inhibitors (CDK 4/6). However, resistance to hormonal treatments inevitably emerges in many patients, necessitating the use of chemotherapy in later lines. In the metastatic setting, chemotherapy is often associated with limited survival benefits and considerable toxicity, resulting in poor quality of life and a median overall survival(OS) of less than three years for endocrine-resistant cases [3,4,5].
Metastatic triple-negative breast cancer (mTNBC), accounting for 10–15% of all breast cancers, exhibits an aggressive clinical course with a high risk of early metastasis and recurrence, particularly to visceral organs and the central nervous system (CNS). Due to the lack of well-defined molecular targets, systemic chemotherapy has remained the cornerstone of treatment for mTNBC, although outcomes remain suboptimal, with short progression-free survival (PFS) and OS following standard therapies [6,7].
Sacituzumab govitecan (SG) is a novel antibody-drug conjugate that targets the transmembrane glycoprotein Trop-2, which is overexpressed in a wide range of epithelial cancers, including both mTNBC and mHRPBC. SG consists of a humanized anti–Trop-2 monoclonal antibody conjugated to SN-38—the active metabolite of irinotecan—via a hydrolysable linker. This structure allows for targeted delivery of cytotoxic therapy directly into tumor cells and exerts a secondary "bystander effect" on the surrounding tumor microenvironment [8,9,10,11,12].
Following encouraging results from early-phase studies, SG received accelerated approval by the U.S. Food and Drug Administration (FDA) in 2020 for the treatment of patients with mTNBC who had received at least two prior lines of therapy. Its efficacy was later confirmed in the phase III ASCENT trial, which demonstrated significantly improved survival outcomes and response rates compared to standard chemotherapy [13]. More recently, the TROPiCS-02 trial expanded the use of SG to the mHRPBC setting, establishing its benefit over physician’s choice chemotherapy in heavily pretreated, endocrine-resistant patients [14].
While randomized clinical trials have validated the efficacy and safety of SG, real-world data on its use remain relatively limited—particularly among diverse patient populations and across both major Trop-2–expressing subtypes. Observational studies reflecting clinical practice are essential to understanding how SG performs outside of controlled trial settings, especially with respect to tolerability, treatment patterns, and prognostic factors [15,16,17,18,19].
The present multicenter, retrospective study aims to evaluate the real-world effectiveness and safety profile of SG in patients with mTNBC and mHRPBC. By including both molecular subtypes, this analysis seeks to provide a comprehensive overview of clinical outcomes and identify factors associated with treatment response and survival in a real-life clinical setting.
2. Materials and Methods
2.1. Study Design and Population
This retrospective, multicenter study included 68 patients diagnosed with mTNBC and mHRPBC, treated with SG between 2022 and 2025. The study was conducted across several oncology centers, and only female patients aged 18 and above were included. For inclusion in the mTNBC cohort, patients were required to have experienced progression after at least one line of chemotherapy or chemoimmunotherapy, whereas mHRPBC patients were included if they had previously received at least two lines of chemotherapy failed prior to CDK 4/6 inhibitors and other hormonotherapy agents. Patients were excluded if they had received SG as part of a clinical trial, had other primary cancers within the past 5 years (excluding non-metastatic skin cancers), did not provide informed consent, or were male.
2.2. Intervention and Treatment Protocol
Sacituzumab Govitecan was administered at a dose of 10 mg/kg on days 1 and 8 of an every 21-day cycle. In cases of dose reduction, the dosage was decreased to 7.5 mg/kg, followed by 5 mg/kg based on patient tolerance. Concomitant granulocyte-colony stimulating factor (G-CSF) was administered as primary prophylaxis in the majority of patients to mitigate the risk of neutropenia. The treatment continued until disease progression, unacceptable toxicity, or patient decision to discontinue.
2.3. Outcome Measures
The primary study outcomes included PFS and OS. PFS was defined as the time from the initiation of SG treatment to disease progression or death from any cause. OS was also calculated from the initiation of SG treatment to death from any cause. Safety assessments included the incidence and severity of adverse events (AEs), which were classified according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE), version 5.0. Dose reductions and treatment discontinuations due to toxicity were also recorded.
2.4. Statistical Analysis
Statistical analysis was performed using SPSS (version 27). Descriptive statistics were used to summarize the baseline demographic and clinical characteristics of the patients, with categorical variables expressed as frequencies and percentages, and continuous variables as medians with ranges or means with standard deviations.
The primary outcomes, PFS and OS, were estimated using the Kaplan-Meier method. OS was calculated from the initiation of SG treatment to death from any cause. The differences in survival between groups were evaluated using the log-rank test (Mantel-Cox test) for comparing the survival distributions across different subgroups, such as molecular subtype (mTNBC vs mHRPBC), Eastern cooperative oncology group performance status (ECOG PS) (ECOG PS-0 vs ECOG PS-1), and metastatic sites (liver, bone, brain, etc.).
Univariate analysis for PFS and OS was conducted to assess the impact of baseline variables, including molecular subtype, ECOG PS, metastatic sites, previous treatment regimens, and Ki-67 expression, on survival outcomes. Factors identified as significant in the univariate analysis were included in the multivariate Cox regression model to determine independent predictors of survival. Hazard ratios (HR) with 95% confidence intervals (CI) were calculated for each predictor. Additionally, binary logistic regression was performed to evaluate factors associated with treatment response. Variables with significant associations in univariate analysis were included in the logistic regression model. All statistical tests were two-tailed, and a p-value of less than 0.05 was considered statistically significant.
2.5. Ethics Statement
The study was approved by the relevant institutional review boards at each participating center. Ethical approval was granted by the Istanbul Medipol University Ethics Committee (Ethics Committee Decision No: 1209, Date: 28.11.2024). Informed consent was obtained from all participants before the initiation of SG treatment.
3. Results
3.1. Baseline Characteristics
Baseline clinical characteristics of the 68 patients included in the study are summarized in Table 1. The median age was 48 years (range: 29–78). The majority of patients had an ECOG PS of 0 (70.6%) and received prior taxane (94.1%) and anthracycline (79.4%) therapies. De novo metastatic disease was present in 26.5% of patients. In terms of molecular classification, 51.5% had mTNBC, and 48.5% were mHRPBC. HER2 status was predominantly immunohistochemistry (IHC) 0 (70.4%). In the metastatic setting, 42.6% of patients had received three or fewer prior lines of therapy, while 55.9% had received more than three lines. The most frequent sites of metastasis were lymph nodes (85.3%), bone (57.4%), and lung (57.4%), followed by liver (51.5%) and brain (42.6%). Median number of SG cycles was 7 (range: 3–37), and G-CSF support was used in 88.2% of cases.
3.2. Effectiveness
At a median follow-up of 6.8 months (95% CI: 5.4–10.0), the median PFS was 6.1 months (95% CI: 4.83–7.43), and the median mOS was 12.5 months (95% CI: 9.92–15.07) in all cohort (Figure 1 and Figure 2, respectively).
There was no significant difference observed between molecular subgroups, with PFS durations of 6.5 months for mTNBC and 5.76 months for mHRPBC (p = 0.78) (Figure 3). Similarly, no significant difference in PFS was found for the de novo metastasis group (p = 0.63). However, ECOG PS had a significant impact on PFS, with patients in ECOG PS-0 having significantly longer PFS compared to those in ECOG PS-1 (p = 0.004).
Regarding metastatic sites, liver metastasis significantly shortened PFS (p = 0.002). Bone metastasis also had a significant effect on PFS (p = 0.004), whereas no significant difference was observed for lung metastasis (p = 0.088) and brain metastasis (p = 0.253). Similarly, lymph node metastasis did not significantly affect PFS (p = 0.086).
Having received immunotherapy before did not make a significant difference (p = 0.886). There were no significant differences observed between chemotherapy history and treatment types. Taxanes, anthracyclines, carboplatin, and capecitabine did not show any significant impact on PFS. Additionally, factors such as local treatment and the number of chemotherapy lines did not result in significant differences in PFS.
In the analysis of Ki-67 values, no significant difference was observed between patients with Ki-67 ≤20 and those with Ki-67 >20 (p = 0.897). Moreover, no relationship was found between Ki-67 values in the metastatic setting and PFS. Finally, dose reduction due to toxicity and G-CSF use did not have a significant effect on PFS (p = 0.270 and p = 0.097, respectively).
These results highlight several important factors in determining patient prognosis. Specifically, ECOG PS, liver metastasis, and bone metastasis have significant effects on PFS, while treatment types and Ki-67 values do not show a meaningful impact on PFS (Table 2).
The multivariate analysis evaluated independent prognostic factors for PFS. It found that liver metastasis significantly increased the risk of disease progression (p = 0.047, HR = 2.046), with faster disease progression observed in these patients. Similarly, ECOG PS was associated with faster disease progression and shorter PFS (p = 0.050, HR = 1.968). However, bone metastasis and molecular subtype did not show a significant impact on PFS (p = 0.095 and p = 0.348, respectively) (Table 2).
Furthermore, in univariate analysis for OS, molecular subgroups such as mTNBC and mHRPBC did not show a significant difference in OS (p = 0.38), with median OS values of 11.93 months (95% CI: 5.22–18.64 months) for mTNBC and 11.3 months (95% CI: 9.16–25.4 months) for mHRPBC (Figure 4).
In the de novo metastatic cohort, the median OS was 14.73 months (95% CI: 4.23–25.23 months), with no significant difference (p = 0.716). ECOG PS also did not significantly impact OS (p = 0.178).
Regarding metastatic sites, liver metastasis was strongly associated with worse OS (5.96 months, p = 0.001), as were bone and brain metastases with median OS values of 11.93 months (p = 0.008) and 7.13 months (p = 0.02), respectively. Lung metastasis did not significantly affect OS (p = 0.076). Treatment modalities showed varied impacts; carboplatin significantly improved OS (12.30 months, p = 0.04), while other treatments, including immunotherapy and anthracyclines, showed no significant difference (p > 0.05).
The number of chemotherapy lines, treatment discontinuation due to toxicity, and G-CSF use did not show significant effects on OS. Ki-67 expression did not also show a significant difference in OS, either at initial diagnosis or in the metastatic setting (Table 3).
While the multivariate analysis was carried out for OS, liver metastasis was identified as an independent predictor of poorer OS (HR = 3.150, 95% CI: 1.184–8.383, p = 0.022). Bone metastasis showed a trend toward statistical significance (HR = 2.283, 95% CI: 0.927–5.624, p = 0.073). The molecular subtype was also significantly associated with OS, as mTNBC patients had better outcomes compared to mHRPBC patients (HR = 0.467, 95% CI: 0.221–0.987, p = 0.046).
Brain metastasis did not show a significant impact on OS (HR = 1.398, 95% CI: 0.609–3.205, p = 0.429). Overall, liver metastasis and molecular subtype were independent predictors of poorer overall survival (Table 3).
Among the 68 evaluable patients, objective response rate (ORR) was 52.9%, with 7 patients (10.3%) achieving complete response (CR) and 29 patients (42.6%) achieving partial response (PR). Additionally, stable disease (SD) was observed in 14.7% of cases, resulting in a disease control rate (DCR) of 67.6%.
A binary logistic regression analysis was performed to identify factors associated with treatment response. As shown in Figure 5, liver metastasis (Odds Ratio (OR): 6.49, p=0.038) and lung metastasis (OR: 7.59, p=0.013) were significantly associated with a higher likelihood of treatment response, with patients having approximately 6.5- and 7.5-times higher odds of response, respectively. Bone metastasis showed a borderline association (OR: 4.35, p=0.050), suggesting a 4-fold increased likelihood of response. However, lymph node metastasis was associated with a markedly lower likelihood of response (OR: 0.065, p=0.017), indicating a significantly reduced chance of treatment efficacy. Other factors, including de novo disease, molecular subtype, ECOG PS, brain metastasis, and Ki-67 index, were not significantly associated with treatment response (all p-values > 0.05) (Figure 5).
3.3. Safety and Adverse Events
Adverse events (AEs) data are visualized in Figure 6. The most common toxicity was alopecia, reported in 90% of patients. Anemia occurred in 41.7% of patients, with 15% experiencing grade ≥3 severity. Other frequent hematologic toxicities included neutropenia and thrombocytopenia, with a substantial proportion at grade ≥3 severity, highlighting the importance of routine hematologic monitoring and supportive care. Notably, G-CSF was used in 88.2% of patients to manage neutropenia, emphasizing the role of G-CSF in mitigating hematologic toxicity associated with SG treatment.
Among non-hematologic toxicities, nausea and diarrhea were the most common. For patients experiencing grade 2 or higher nausea and vomiting, dexamethasone, 5-hydroxytryptamine 3 receptor agonists (5-HT3), and Neurokinin-1 receptor antagonists (NK-1) inhibitors were routinely administered as part of the antiemetic regimen. Diarrhea was managed with anti-diarrheal agents when patients experienced grade 2 or higher severity, reflecting a proactive approach to managing gastrointestinal toxicity. Fatigue was reported in 21.7% of patients, with a small proportion experiencing higher-grade fatigue. Elevated liver enzymes and febrile neutropenia were infrequent, and did not require treatment interruption.
In terms of treatment modification due to toxicity, dose reduction occurred in 29.4% of patients, and treatment discontinuation due to toxicity was observed in 2.9% of the cohort, which was attributed to treatment-refractory grade 4 thrombocytopenia. These findings underscore the importance of early recognition and management of adverse events, as they can significantly impact treatment continuity and efficacy.
4. Discussion
4.1. Real-World Effectiveness Compared to Clinical Trials
This retrospective, multicenter real-world study provides important insights into the clinical effectiveness and safety of SG in patients with both mTNBC and mHRPBC, treated in routine clinical practice in Turkey. Our findings confirm and extend the clinical trial data by demonstrating that SG retains its efficacy and manageable safety profile in real-world populations, including those typically underrepresented in randomized controlled trials [20,21].
In our cohort, median PFS and OS were 6.1 months and 12.5 months, respectively, aligning well with pivotal trial outcomes. For example, the ASCENT study reported a median PFS of 5.6 months and OS of 12.1 months in pretreated mTNBC patients [13], while TROPiCS-02 demonstrated a median PFS of 5.5 months and OS of 14.4 months in mHRPBC patients [14]. The EVER-132-002 trial focusing on Asian patients also confirmed these outcomes, with a median OS of 21.0 months in the SG arm [22]. Notably, our real-world population included both subtypes and showed comparable or even slightly superior outcomes, highlighting the robustness of SG across different biological subtypes and clinical settings.
A particularly novel contribution of our study is the inclusion of mHRPBC patients, for whom real-world data are remarkably sparse. To our knowledge, this is the first real-life cohorts to systematically evaluate SG in both mTNBC and mHRPBC populations. Despite the growing body of evidence supporting SG in mHRPBC disease from trials such as TROPiCS-02 and EVER-132-002, there remains a significant gap in observational literature. Previously published real-world studies have almost exclusively focused on mTNBC, leaving a critical evidence gap for mHRPBC patients [16,23].
In our study, 33 patients (48.5% of the cohort) had mHRPBCand had previously received endocrine therapy and at least two lines of chemotherapy. In this subgroup, the median PFS was 6.1 months, and the median OS was 12.5 months, which are consistent with the outcomes reported in the TROPiCS-02 trial (median PFS 5.5 months, OS 14.4 months) [14]. These real-world findings support the therapeutic role of SG in chemotherapy-pretreated mHRPBC patients and demonstrate comparable effectiveness to clinical trial populations.
Our findings are further supported by the EVER-132-002 study, which reported a favorable safety and efficacy profile of SG in Asian mHRPBC patients [22]. However, no real-world studies to date have provided detailed clinical outcomes for this subgroup, particularly in a multicenter, Turkish clinical setting. Therefore, the current analysis significantly contributes to the literature by providing rare, real-life data on SG use in mHRPBC, reinforcing its place in treatment sequencing for endocrine-resistant disease. for informing treatment strategies in endocrine-resistant, chemotherapy-pretreated mHRPBC.
Our analysis identified two major clinical parameters—ECOG PS ≥1 and the presence of liver metastases—as independent predictors of shorter PFS and OS. These findings were consistent with multiple prior real-world studies and clinical trial subgroup analyses that have associated poor ECOG PS and visceral involvement with inferior treatment outcomes [24,25,26]. In our multivariate model, patients with ECOG PS ≥1 experienced significantly reduced OS, suggesting that functional status remains a critical determinant in SG efficacy and patient selection.
Liver metastases, in particular, were a consistent marker of poor prognosis in our study, mirroring findings from both the ASCENT trial and a meta-analysis by [25], which highlighted diminished SG benefit in patients with hepatic involvement. This is further supported by the Italian and Polish real-world cohorts, where patients with liver metastases also showed worse clinical outcomes [16,23].
Intriguingly, despite their association with worse survival, liver and lung metastases in our cohort were independently associated with higher ORR. This seemingly paradoxical finding may reflect initial tumor burden reduction before progression or enhanced drug delivery in highly perfused organs. It is also possible that such patients benefit from early disease control but eventually succumb to aggressive tumor biology or resistance mechanisms. Further molecular and pharmacokinetic studies are needed to explore this observation.
Another notable subgroup within our population was patients with CNS metastases. While SG is not formally indicated for active brain metastases, emerging data—including our findings—suggest that SG may offer clinical benefit in selected patients with stable or previously treated CNS disease. In our analysis, brain metastases were not significantly associated with worse PFS or OS, which is in line with the CNS subgroup analyses from Grinda et al. and the German cohort, both indicating that intracranial progression can remain controlled in selected patients receiving SG [17,18].
In addition to these subgroups, a relevant clinical consideration is the impact of prior immunotherapy exposure. A subset of our patients—primarily in the mTNBC cohort—had received immune checkpoint inhibitors (ICIs) before initiating SG. Our data suggest that prior ICIs use did not adversely affect outcomes with SG, consistent with observations from the ASCENT trial, where clinical benefit was maintained irrespective of prior ICIs exposure [13]. Furthermore, emerging real-world evidence supports the continued efficacy of SG following immunotherapy failure, highlighting its utility as a viable treatment option in later lines of therapy. This is particularly relevant in Programmed death-ligand 1 (PD-L1) -positive mTNBC, where ICIs are commonly used in earlier treatment lines [23,27,28]. These subgroup insights contribute important granularity to real-world treatment planning and highlight the potential of SG to remain effective in heavily pretreated and immunotherapy-experienced populations.
Together, these subgroup analyses contribute important granularity to patient selection in the real-world setting. They also highlight the need for further biomarker-guided stratification to identify individuals who derive the most benefit from SG, especially in heavily pretreated and clinically diverse populations.
Our ORR was 52.9%, with a CR rate of 10.3%, exceeding those reported in most prior real-world studies. For instance, the Italian multicenter cohort reported an ORR of 33.3% [23], while a large US cohort showed 27.8% [19]. These encouraging results may be attributed to differences in baseline characteristics, disease burden, treatment adherence, or supportive care measures, including high G-CSF utilization in our population.
4.2. Safety and Tolerability Profile
In our study, SG was generally well tolerated, with AEs consistent with those reported in clinical trials and prior real-world studies. The most frequently observed AEs included alopecia (64.7%), anemia (52.9%), neutropenia (50%), and diarrhea (38.2%). Grade ≥3 hematologic toxicities, especially neutropenia, were observed in a substantial proportion of patients but were successfully managed with G-CSF, which was administered to 88.2% of patients. Only 2.9% of patients discontinued treatment due to AEs, and no new safety signals emerged.
These results support the established safety profile of SG as seen in the ASCENT [13] and TROPiCS-02 [14] trials. Furthermore, they are consistent with findings from other real-world analyses. For instance, the Italian multicenter study reported anemia (66.6%), neutropenia (59.6%), and diarrhea (38.6%) as the most common toxicities, with treatment discontinuation due to AEs in 5.3% of patients [23]. Similarly, the German [17] and Polish [16] cohorts reported comparable safety profiles, suggesting that the toxicity of SG is predictable and can be effectively mitigated with supportive care.
A recent meta-analysis also reinforced these observations, concluding that although SG is associated with a higher incidence of grade 3–4 neutropenia and anemia compared to standard chemotherapy, it does not significantly increase the risk of treatment discontinuation. Importantly, our low discontinuation rate—despite a heavily pretreated and clinically diverse population—underscores the tolerability of SG in routine practice [25].
Given the high rate of G-CSF usage in our cohort, the role of proactive supportive care should not be underestimated. Early recognition and management of hematologic toxicity are essential to maintaining dose intensity and prolonging treatment benefit. Our findings reinforce the importance of preemptive strategies to minimize interruptions or discontinuations due to toxicity.
4.3. Limitations
This study has several limitations, some of which are related to contextual and regulatory factors specific to the study setting. First, its retrospective design may introduce bias in data collection and interpretation. Second, the relatively small sample size may limit the statistical power, particularly for subgroup analyses. Third, the study did not include biomarker analyses such as Trop-2 expression, which may provide additional predictive information. Fourth, treatment selection and supportive care measures were not standardized across centers. Additionally, the relatively low number of patients included in the study was influenced by access-related limitations. At the time this study was initiated, SG was not reimbursed by national health authorities for patients with mHRPBC metastatic breast cancer in Turkey. Even among mTNBC patients, reimbursement was restricted to those who had received at least two prior chemotherapy regimens in the metastatic setting. These reimbursement constraints likely delayed treatment initiation and limited broader access to SG, thereby reducing patient enrollment and potentially affecting the generalizability of the findings.
4.4. Clinical Implications
In conclusion, this study demonstrates that SG is an effective and safe treatment option for patients with mTNBC and mHRPBC breast cancer in routine clinical settings. Importantly, our analysis highlights the paucity of real-world data in the mHRPBC subgroup, positioning our findings as a critical contribution to the literature. These results support the integration of SG into treatment algorithms for both subtypes, particularly in patients with endocrine resistance and high disease burden. Further prospective and biomarker-driven studies are warranted to validate these observations and guide optimal patient selection, sequencing strategies, and supportive care planning.
5. Conclusions
This multicenter, retrospective real-world study provides compelling evidence that SG is an effective and well-tolerated treatment option for patients with both mTNBC and mHRPBC, including those heavily pretreated and with poor prognostic features. Our findings confirm and extend previous clinical trial results, demonstrating comparable PFS and OS outcomes in a real-life population that is typically underrepresented in randomized trials.
Importantly, this study adds novel real-world data for the mHRPBC subgroup, which remains underexplored in the existing literature. Clinical outcomes for these patients mirrored those observed in phase III trials, reinforcing the role of SG in endocrine-resistant, chemotherapy-exposed mHRPBC. In addition, we identified ECOG PS and liver metastasis as independent predictors of inferior survival outcomes, underscoring the importance of baseline functional and disease burden assessments when considering SG therapy.
Furthermore, the safety profile of SG was manageable, with toxicity patterns aligning with previous reports and a low rate of treatment discontinuation, partly attributable to high rates of proactive G-CSF use and supportive care.
In summary, our results support the incorporation of SG into real-world treatment algorithms for both mTNBC and mHRPBC. Future prospective studies with larger cohorts and biomarker-driven stratification are warranted to refine patient selection and optimize treatment outcomes. Additionally, addressing access and reimbursement barriers will be essential to ensuring broader implementation of SG in routine clinical practice.
Author Contributions
Conceptualization, H.M., M.H.Y., B.K., G.B., A.B., Ö.FÖ. ; methodology, H.M., Ö.M.C., T.K., G.B., software, H.M., B.K., B.O.U.,F.S., U.D., validation, H.M. Ö.F.Ö., M.H.Y. formal analysis, H.M., K.H., A.B., investigation, H.M.; resources, H.M., A.B; data curation, H.M., K.H., M.H.Y, Ö.M.C., T.K.,U.D., B.O.U., G.B., F.S..; Initial manuscript drafting was carried out by H.M. and A.B.; H.M. was responsible for manuscript revision and editing; data visualization was performed by H.M.; supervision was led by A.B.; project coordination and oversight were managed by H.M. and A.B.; All authors have read and agreed to the published version of the manuscript.
Funding
None.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Istanbul Medipol University Clinical Research Ethics Committee (Ethics Committee Decision No: 1209, Date: 28.11.2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data of this study is available from the corresponding author upon a reasonable request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jallah JK, Dweh TJ, Anjankar A, Palma O. A review of the advancements in targeted therapies for breast cancer. Cureus. 2023;15(10). [CrossRef]
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2021;71(3):209-49. [CrossRef]
- Cuyún Carter G, Mohanty M, Stenger K, Morato Guimaraes C, Singuru S, Basa P, et al. Prognostic factors in hormone receptor-positive/human epidermal growth factor receptor 2-negative (HR+/HER2–) advanced breast cancer: a systematic literature review. Cancer Management and Research. 2021:6537-66.
- Gradishar WJ, Moran MS, Abraham J, Abramson V, Aft R, Agnese D, et al. NCCN Guidelines® insights: breast cancer, version 4.2023: featured updates to the NCCN guidelines. Journal of the National Comprehensive Cancer Network. 2023;21(6):594-608.
- Gennari A, André F, Barrios C, Cortes J, de Azambuja E, DeMichele A, et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer☆. Annals of oncology. 2021;32(12):1475-95.
- Li CH, Karantza V, Aktan G, Lala M. Current treatment landscape for patients with locally recurrent inoperable or metastatic triple-negative breast cancer: a systematic literature review. Breast cancer research. 2019;21:1-14. [CrossRef]
- Diana A, Franzese E, Centonze S, Carlino F, Della Corte CM, Ventriglia J, et al. Triple-negative breast cancers: systematic review of the literature on molecular and clinical features with a focus on treatment with innovative drugs. Current oncology reports. 2018;20:1-11. [CrossRef]
- Nardin S, Del Mastro L. Sacituzumab Govitecan in HR-positive HER2-negative metastatic breast cancer. Annals of Translational Medicine. 2023;11(5):228. [CrossRef]
- Goldenberg DM, Cardillo TM, Govindan SV, Rossi EA, Sharkey RM. Trop-2 is a novel target for solid cancer therapy with sacituzumab govitecan (IMMU-132), an antibody-drug conjugate (ADC). Oncotarget. 2015;6(26):22496. [CrossRef]
- Goldenberg DM, Sharkey RM. Sacituzumab govitecan, a novel, third-generation, antibody-drug conjugate (ADC) for cancer therapy. Expert opinion on biological therapy. 2020;20(8):871-85. [CrossRef]
- Nagayama A, Vidula N, Ellisen L, Bardia A. Novel antibody–drug conjugates for triple negative breast cancer. Therapeutic advances in medical oncology. 2020;12:1758835920915980. [CrossRef]
- Goldenberg DM, Stein R, Sharkey RM. The emergence of trophoblast cell-surface antigen 2 (TROP-2) as a novel cancer target. Oncotarget. 2018;9(48):28989. [CrossRef]
- Bardia A, Rugo HS, Tolaney SM, Loirat D, Punie K, Oliveira M, et al. Final results from the randomized phase III ASCENT clinical trial in metastatic triple-negative breast cancer and association of outcomes by human epidermal growth factor receptor 2 and trophoblast cell surface antigen 2 expression. Journal of Clinical Oncology. 2024;42(15):1738-44. [CrossRef]
- Rugo HS, Bardia A, Marmé F, Cortés J, Schmid P, Loirat D, et al. Overall survival with sacituzumab govitecan in hormone receptor-positive and human epidermal growth factor receptor 2-negative metastatic breast cancer (TROPiCS-02): a randomised, open-label, multicentre, phase 3 trial. The Lancet. 2023;402(10411):1423-33. [CrossRef]
- Spring LM, Nakajima E, Hutchinson J, Viscosi E, Blouin G, Weekes C, et al. Sacituzumab govitecan for metastatic triple-negative breast cancer: clinical overview and management of potential toxicities. The Oncologist. 2021;26(10):827-34. [CrossRef]
- Püsküllüoğlu M, Pieniążek M, Las-Jankowska M, Streb J, Ziobro M, Pacholczak-Madej R, et al. Sacituzumab govitecan for second and subsequent line palliative treatment of patients with triple-negative breast cancer: a Polish real-world multicenter cohort study. Oncology and Therapy. 2024;12(4):787-801. [CrossRef]
- Reinisch M, Bruzas S, Spoenlein J, Shenoy S, Traut A, Harrach H, et al. Safety and effectiveness of sacituzumab govitecan in patients with metastatic triple-negative breast cancer in real-world settings: first observations from an interdisciplinary breast cancer centre in Germany. Therapeutic Advances in Medical Oncology. 2023;15:17588359231200454. [CrossRef]
- Grinda T, Morganti S, Hsu L, Yoo T-K, Kusmick RJ, Aizer AA, et al. Real-World outcomes with sacituzumab govitecan among breast cancer patients with central nervous system metastases. NPJ Breast Cancer. 2025;11(1):22. [CrossRef]
- Kalinsky K, Spring L, Yam C, Bhave MA, Ntalla I, Lai C, et al. Real-world use patterns, effectiveness, and tolerability of sacituzumab govitecan for second-line and later-line treatment of metastatic triple-negative breast cancer in the United States. Breast Cancer Research and Treatment. 2024;208(1):203-14. [CrossRef]
- Kang C. Sacituzumab Govitecan: A Review in Unresectable or Metastatic HR+/HER2− Breast Cancer. Targeted Oncology. 2024;19(2):289-96.
- W DeClue R, Fisher MD, Gooden K, Walker MS, Le TK. Real-world outcomes in metastatic HR+/HER2-, HER2+ and triple negative breast cancer after start of first-line therapy. Future Oncology. 2023;19(13):909-23. [CrossRef]
- Xu B, Wang S, Yan M, Sohn J, Li W, Tang J, et al. Sacituzumab govitecan in HR+ HER2− metastatic breast cancer: the randomized phase 3 EVER-132-002 trial. Nature Medicine. 2024;30(12):3709-16. [CrossRef]
- Caputo R, Buono G, Piezzo M, Martinelli C, Cianniello D, Rizzo A, et al. Sacituzumab Govitecan for the treatment of advanced triple negative breast cancer patients: a multi-center real-world analysis. Frontiers in oncology. 2024;14:1362641. [CrossRef]
- Alaklabi S, Roy AM, Zagami P, Chakraborty A, Held N, Elijah J, et al. Real-World Clinical Outcomes With Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. JCO Oncology Practice. 2024:OP. 24.00242. [CrossRef]
- Rizzo A, Rinaldi L, Massafra R, Cusmai A, Guven DC, Forgia DL, et al. Sacituzumab govitecan vs. chemotherapy for metastatic breast cancer: a meta-analysis on safety outcomes. Future Oncology. 2024;20(20):1427-34. [CrossRef]
- Hanna D, Merrick S, Ghose A, Devlin MJ, Yang DD, Phillips E, et al. Real world study of sacituzumab govitecan in metastatic triple-negative breast cancer in the United Kingdom. British Journal of Cancer. 2024;130(12):1916-20. [CrossRef]
- Sathe AG, Diderichsen PM, Fauchet F, Phan SC, Girish S, Othman AA. Exposure-Response Analyses of Sacituzumab Govitecan Efficacy and Safety in Patients With Metastatic Triple-Negative Breast Cancer. Clin Pharmacol Ther. 2025;117(2):570-8. [CrossRef]
- Yang Y, Li H, Yang W, Shi Y. Improving efficacy of TNBC immunotherapy: based on analysis and subtyping of immune microenvironment. Frontiers in immunology. 2024;15:1441667. [CrossRef]
Figure 1.
Progression-free survival.
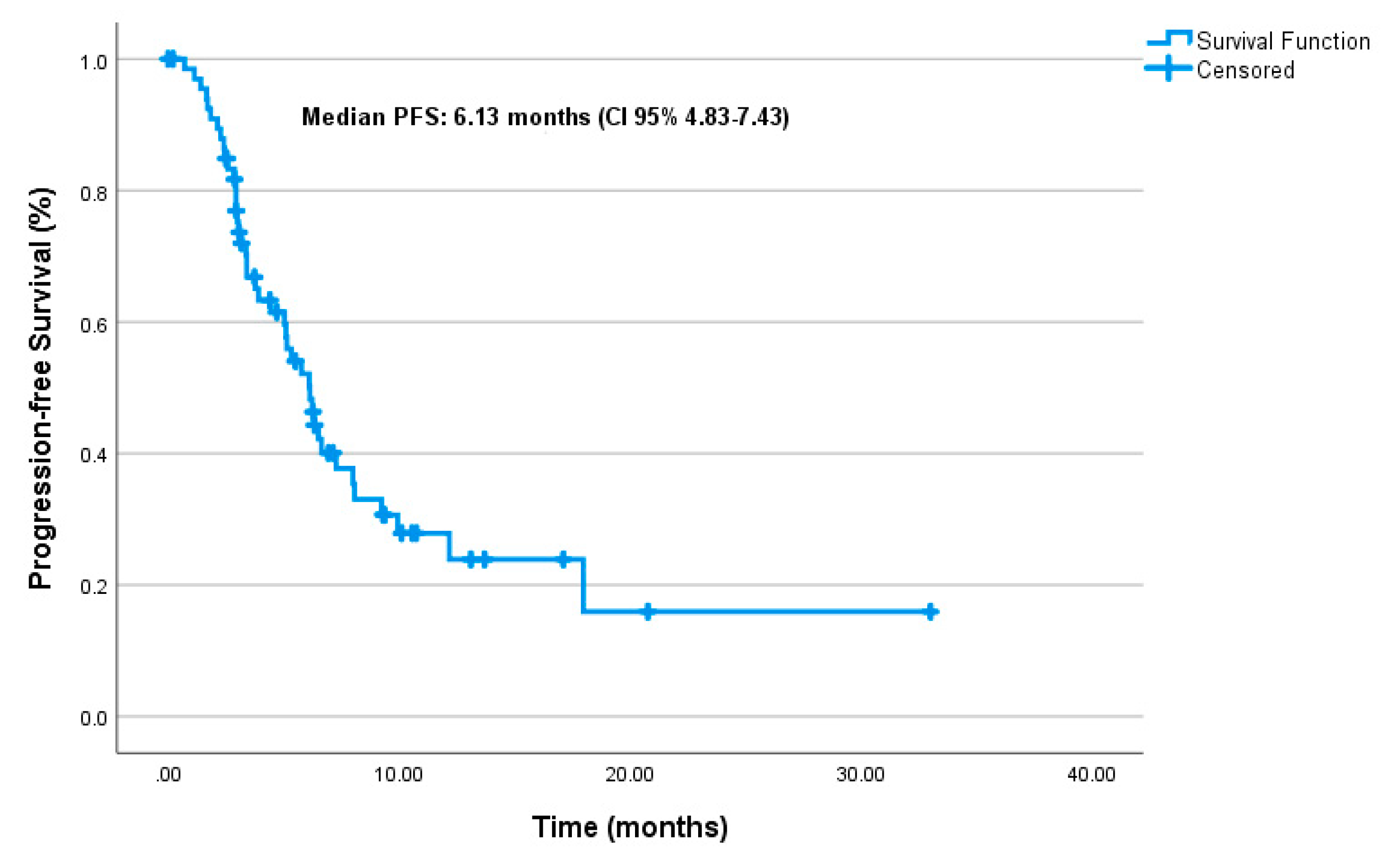
Figure 2.
Overall survival.
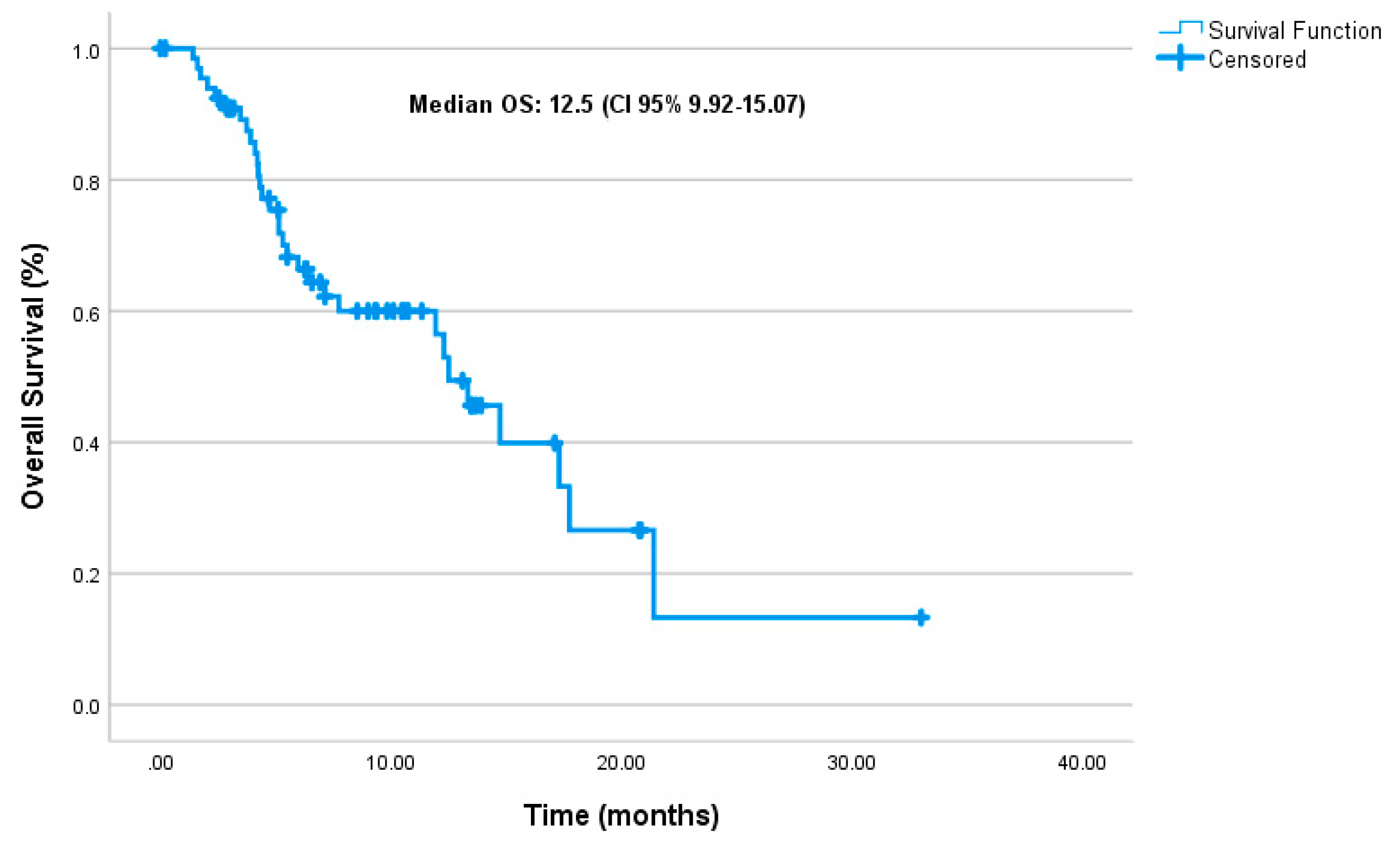
Figure 3.
Progression-free survival by molecular subgroups.
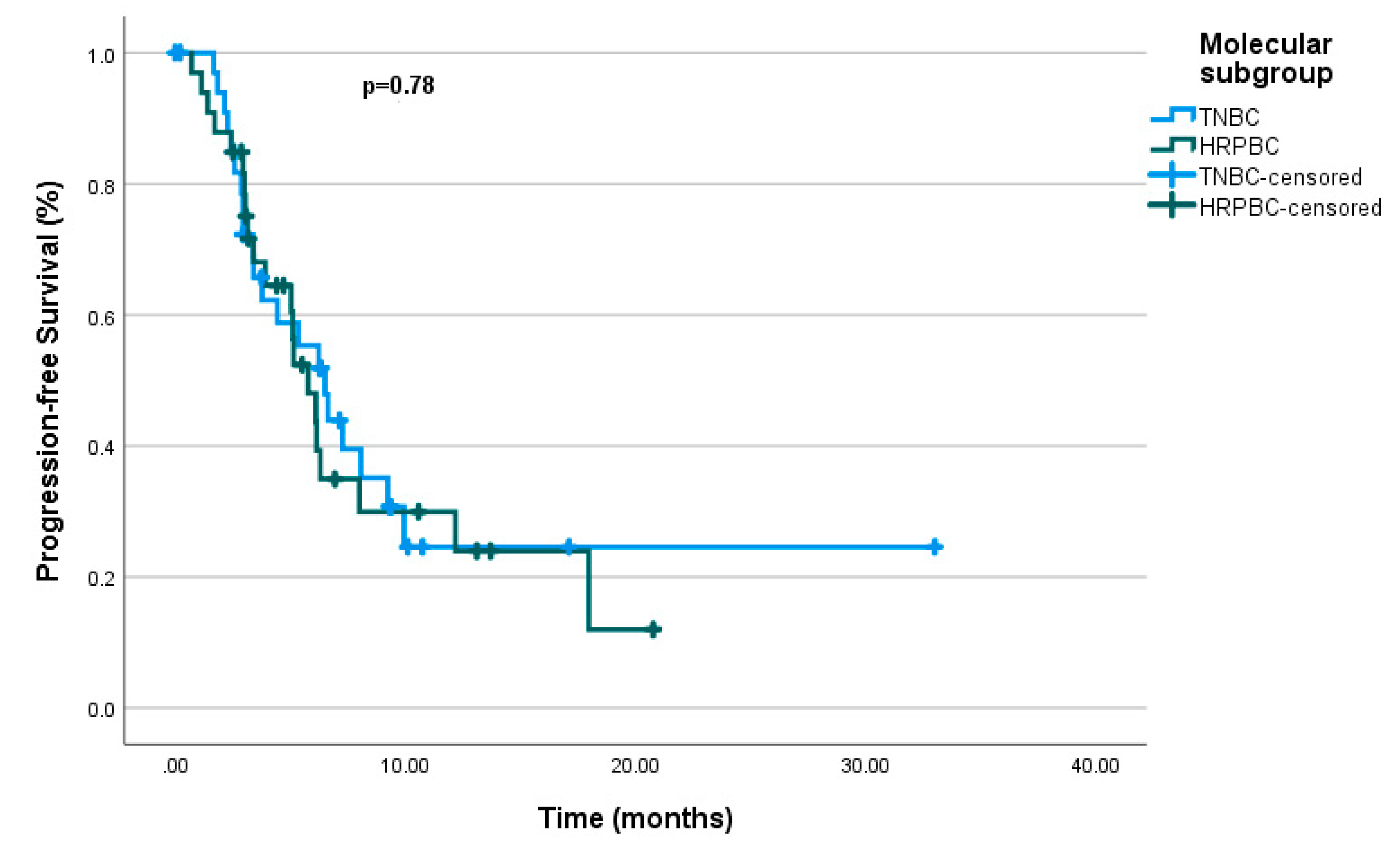
Figure 4.
Overall survival by molecular subgroups..
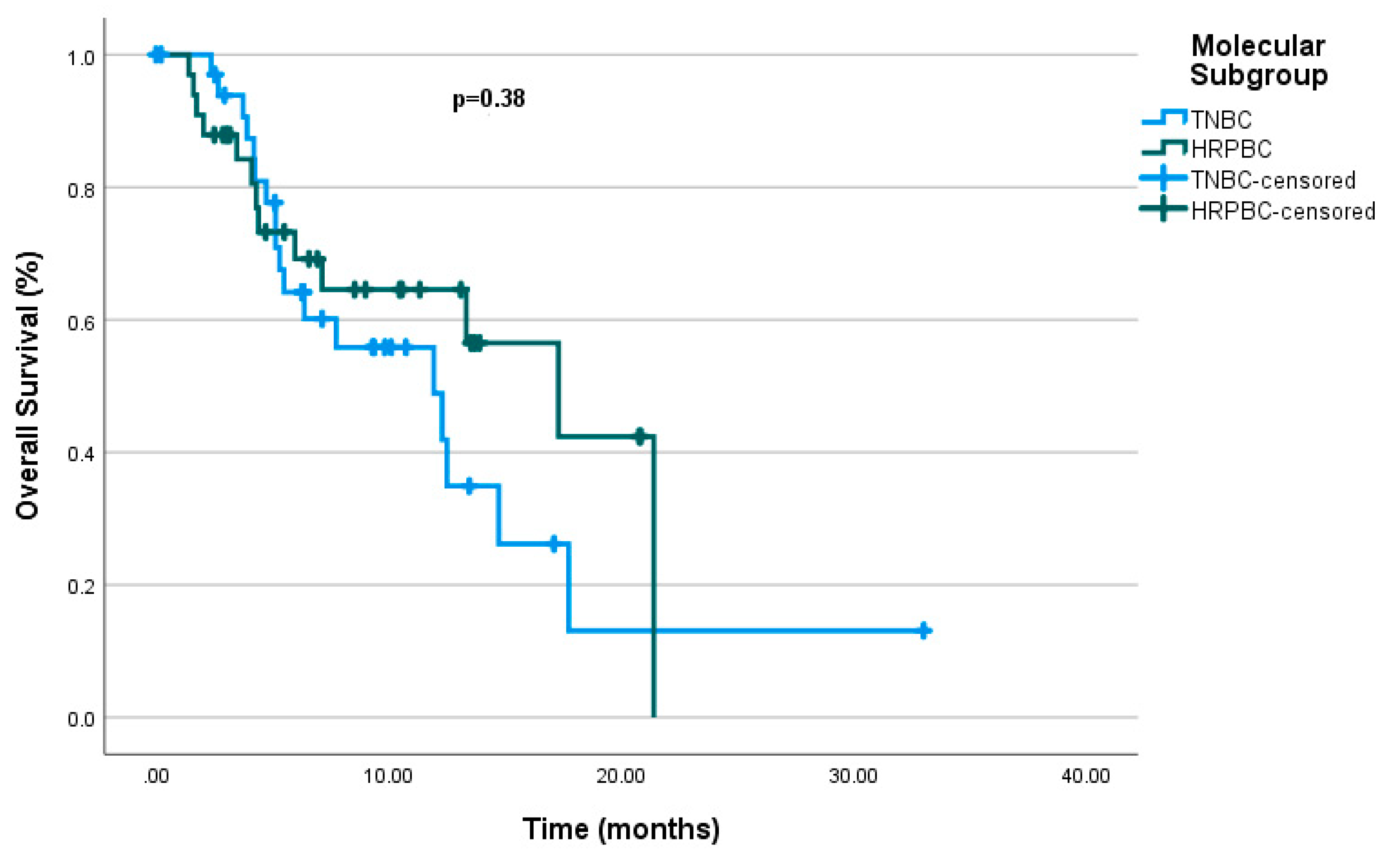
Figure 5.
Factors associated with treatment response.
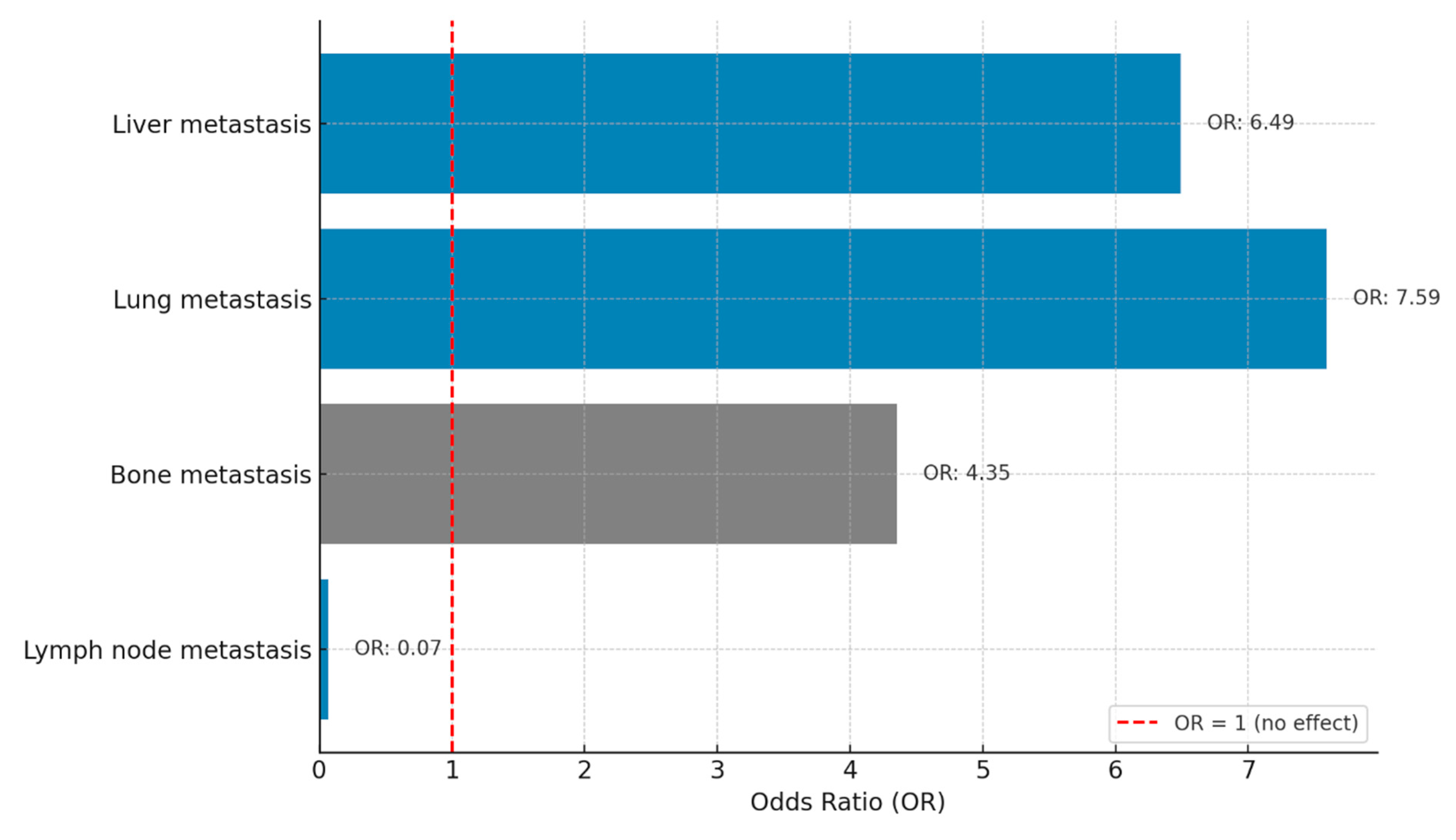
Figure 6.
Adverse events.
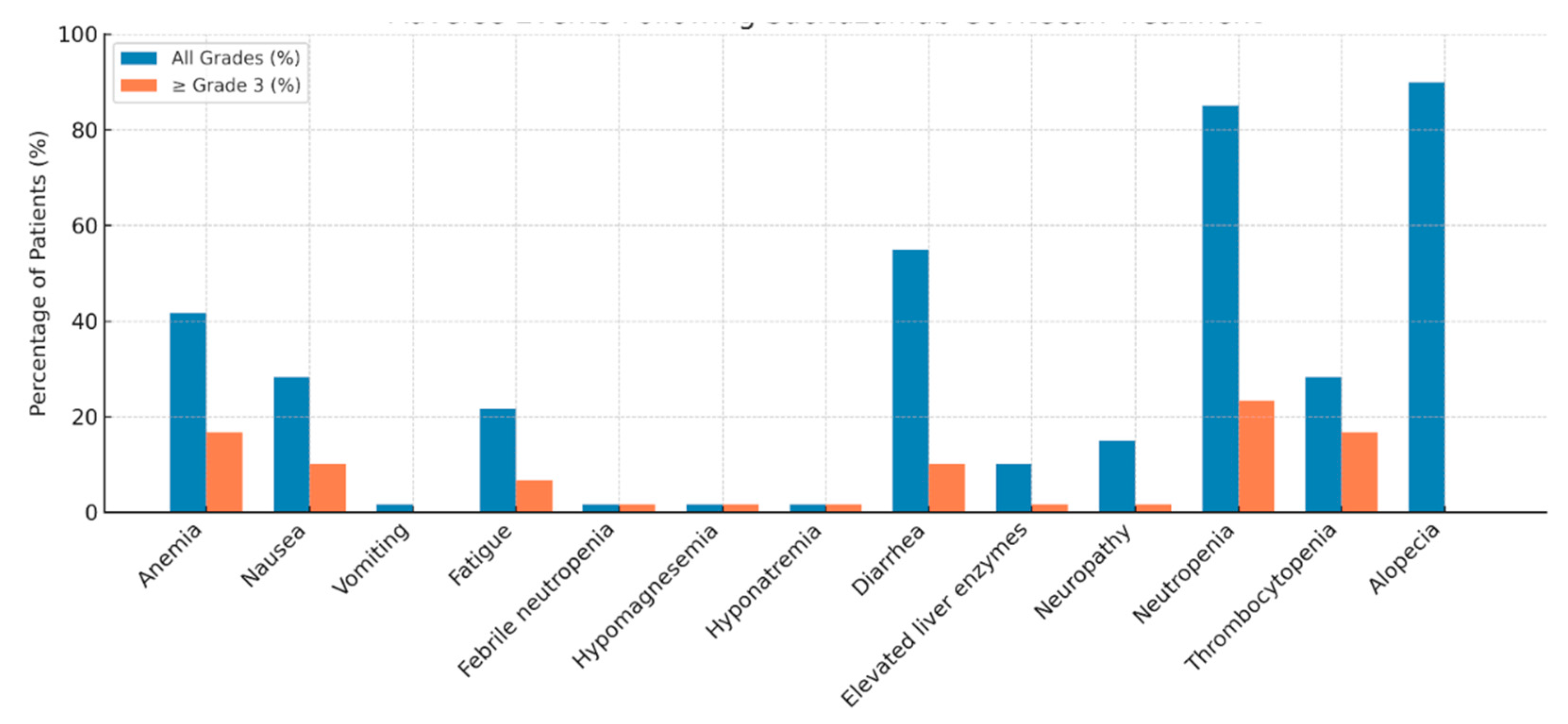

Table 1.
Baseline characteristics.
| Variable | Value |
| Age (median, range) | 48(29-78) |
|
De novo metastasis Molecular classification |
18(26.5%) |
| mTNBC mHRPBC |
35(51.5%) 33(48.5%) |
|
Her2 Status Her2 0 Her2 +1 Her2 +2 (FISH negative) |
52(76.4%) 10(14.7%) 6(8.8%) |
|
ECOG PS 0 1 Metastatic Sites Liver Lung |
48(70.6%) 20(29.4%) 35(51.5%) 39(57.4%) |
| Brain | 29(42.6%) |
| Bone | 39(57.4%) |
| Lymph Node |
58(85.3%) |
| Prior Immunotherapy | 22(32.4%) |
| Dose reduction due to Toxicity | 20(29.4%) |
| Treatment discontinuation due to toxicity | 2(2.9%) |
|
Prior Chemotherapy Agents Taxane Anthracycline Carboplatin Capecitabine |
64(94.1%) 54(79.4%) 48(70.6%) 53(77.9%) |
| Local Treatment | 60(88.2%) |
|
Prior Lines of Therapy in Metastatic Set ≤3 lines >3 lines |
29(42.6%) 38(55.9%) |
| Number of SG Cycles (median, range) | 7(3-37) |
| G-CSF use with SG | 60(88.2%) |
mTNBC: Metastatic triple negative breast cancer, mHRPBC: Metastatic hormone reseptore positive/ Human epidermal growth factor receptor 2 negative breast cancer, ECOG PS: Eastern cooperative oncology group performance status, IHC: Immunohistochemistry, FISH: Fluorescence in situ hybridization, SG: Sacituzumab gavitecan, G-CSF: Granulocyte colony-stimulating factor.
Table 2.
Univariate and multivariate analysis for progression-free survival.
| Variable | mPFS (months) | 95% CI | p-value | HR(95% CI) | p-value |
|---|---|---|---|---|---|
| Molecular subgroup 0.78 | 0.733 (0.384-1.401) |
0.348 | |||
| mTNBC | 6.5 | (4.45 – 8.54) | |||
| mHRPBC | 5.76 | (4.28 – 7.24) | |||
| De novo met | 5.13 | (1.97 – 8.28) | 0.63 | ||
| ECOG PS 0.004 | 1.968 (0.999-3.875) |
0.050 | |||
| ECOG PS-0 | 7.26 | (5.32 – 9.21) | |||
| ECOG PS-1 | 3.76 | (2.26 – 5.27) | |||
| Metastatic site | |||||
| Liver | 4.43 | (2.74 – 6.12) | 0.002 | 2.046 (1.008-4.151 |
0.047 |
| Lung | 3.9 | (2.30 – 7.76) | 0.088 | ||
| Brain | 5.03 | (2.74 – 6.12) | 0.253 | ||
| Bone | 5.03 | (3.18 – 6.88) | 0.004 | 1.873 (0.896-3.913) |
0.095 |
| Lymph nodes | 6.5 | (4.07 – 8.92) | 0.086 | ||
| Prior ICIs | 6.30 | (2.31 – 10.28) | 0.886 | ||
| Prior chemotherapy | |||||
| Taxane | 6.13 | (4.86 – 7.40) | 0.692 | ||
| Antracycline | 6.13 | (4.79 – 7.47) | 0.717 | ||
| Carboplatin | 6.23 | (4.62 – 7.84) | 0.762 | ||
| Capecitabine | 6.13 | (4.94 – 7.32) | 0.703 | ||
| Local treatment | 6.13 | (4.90 – 7.36) | 0.929 | ||
| No. of chemotherapy lines | |||||
| ≤3 lines chemotherapy | 5.33 | (2.89 – 7.76) | 0.796 | ||
| >3 lines chemotherapy | 6.23 | (5.32 – 7.14) | 0.836 | ||
| Dose reduction due to Toxicity | 3.13 | (0.13 – 6.13) | 0.270 | ||
| G-CSF Use with SG | - | - | 0.097 | ||
| At diagnosis Ki-67≤20 | 6.13 | (4.55 – 7.71) | 0.897 | ||
| At diagnosis Ki-67>20 | 5.76 | (4.27 – 7.25) | 0.897 | ||
| Metastatic setting Ki-67≤20 | 6.13 | (3.46 – 8.80) | 1 | ||
| Metastatic setting Ki-67>20 | 6.23 | (4.67 – 7.79) | 1 | ||
mTNBC: Metastatic triple negative breast cancer, mHRPBC: Metastatic hormone reseptore positive/ Human epidermal growth factor receptor 2 negative breast cancer, ECOG PS: Eastern cooperative oncology group performance status, G-CSF: Granulocyte colony-stimulating factor, ICIs: Immune check point inhibitors, HR: Hazard ratio, CI: Confidence interval.
Table 3.
Univariate and multivariate analysis for overall survival.
| Variable | mOS (months) | 95% CI | p-value | HR(95% CI) | p-value |
|---|---|---|---|---|---|
| Molecular subgroup 0.380 | 0.467 (0.221-0.987) |
0.046 | |||
| mTNBC | 11.93 | (5.22 – 18.64) | |||
| mHRPBC | 11.3 | (9.16 – 25.4) | |||
| De novo met | 14.73 | (4.23 – 25.23) | 0.716 | ||
| ECOG-PS 0.178 | |||||
| ECOG-0 | 14.73 | (10.52-18.94) | |||
| ECOG-1 | 13.33 | (2.56-24.10) | |||
| Metastatic site | |||||
| Liver | 5.96 | (2.79-9.14) | 0.001 | 3.15 (1.184-8.383) |
0.022 |
| Lung | 7.13 | (3.65-14.78) | 0.076 | ||
| Brain | 7.13 | (1.07-13.18) | 0.02 | 1.398 (0.609-3.205 |
0.429 |
| Bone | 11.93 | (4.98-18.88) | 0.008 | 2.283 (0.927-5.624) |
0.073 |
| Lymph nodes | 12.5 | (10.72-14.27) | 0.884 | ||
| Prior ICIs | 12.5 | (10.31-14.68) | 0.963 | ||
| Prior chemotherapy | |||||
| Taxane | - | - | 0.293 | ||
| Antracycline | 13.33 | (4.56-22.10) | 0.963 | ||
| Carboplatin | 12.30 | (4.71-19.88) | 0.04 | ||
| Capecitabine | 12.50 | (9.95-15.04) | 0.613 | ||
| Local treatment | 12.50 | (10.75-14.24) | 0.673 | ||
| No. of chemotherapy lines | |||||
| ≤3 lines chemotherapy | 14.73 | (4.99-24.47) | 0.745 | ||
| >3 lines chemotherapy | 12.30 | (5.81-18.79) | 0.724 | ||
| G-CSF use with SG | 13.33 | (6.96-19.69) | 0.724 | ||
| At diagnosis Ki-67 0.460 | |||||
| Ki-67≤ 20% | 14.73 | (4.85-22.63) | |||
| Ki-67>20% | 12.30 | (6.02-18.57) | |||
| Metastatic setting Ki-67 0.184 | |||||
| Ki-67≤20% | 14.73 | (2.81-30.21) | |||
| Ki-67>20% | 12.50 | (10.82 -14.17) | |||
mTNBC: Metastatic triple negative breast cancer, mHRPBC: Metastatic hormone reseptore positive/ Human epidermal growth factor receptor 2 negative breast cancer, ECOG PS: Eastern cooperative oncology group performance status, G-CSF: Granulocyte colony-stimulating factor, ICIs: Immune check point inhibitors, HR: Hazard ratio, CI: Confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



