
Submitted:
01 April 2025
Posted:
02 April 2025
You are already at the latest version
Abstract
Importance. Up to 50% of patients with localized breast cancer (BC) continue to recur after initial treatment for more than 20 years. Recurrent cancer is not curable, and the goal of therapy is the prolongation of life. Many variables, including adrenergic stimuli associated with anxiety and/or depression (anxiety/depression), have been linked to recurrence. Demonstrating this effect in predisposing circumstances could guide investigations of prevention.Objective. This study aims to develop predictive modeling of breast cancer recurrence to identify specific circumstances in which anxiety/depression are associated with breast cancer recurrence.Design, Setting, and Participants. We used the SEER-Medicare dataset linked dataset to investigate women diagnosed with stage I, II, and III breast cancer enrolled at 65 years or older for age eligibility. We collected data on the date of diagnosis, patient-, cancer-, treatment- and adverse events-associated variables, and diagnosis of anxiety and/or depression. We identified recurrence by a documented new diagnosis of recurrent, contralateral, or stage IV BC, new chemo-, bio-, hormone, or radiotherapy outside the 4-month window after completion of initial therapy. We extended four deep learning (DL)-based predictive survival models (Deep-24 Surv and DeepHit. Nnet-survival and Cox-Time) that deal with right-censored time-to-event data and found greater than 95% concordance in each hyperparameter to demonstrate prediction validity. We generated 96 hypothetical patient recurrence curves distributed into categories of stage I or III, White (W), or African American (AA) without or with a diagnosis of anxiety and/or depression.ResultsThe patient's age, race and comorbidities, cancer stage, and hormone status distributions mirrored previously published values. Recurrence rates and time to recurrence were worse in patients who were in the AA group, ER-/PR-, and higher stage. Approximately 36% of the patients had anxiety and/or depression, with higher prevalence in W patients. Time to diagnosis ranged from 23-35 months. Recurrence rates in these patients were 27.9% higher than in patients without these diagnoses, with greater impact in Stage I, ER+/PR+, W, and Hispanic patients. The hypothetical patient recurrent survival curves we generated by DL-based predictive modeling demonstrated wide ranges of predicted recurrence-free survival curves within each grouping, with median survivals varying by more than a decade within each group. There were some long-term survivors in many of the categories, but most patients with the anxiety/depression group had far fewer long-term recurrence-free survival curves than patients without the diagnosis. These results demonstrate the exceptional variability of median predicted survival rates and their modifications by chronic adrenergic stimuli.Conclusions and Relevance.This study demonstrates, for the first time, that the adrenergic stressors anxiety and depression increase the average population recurrence rate of dormant breast cancer in elderly SEER-Medicare patients with stage I, II, and III disease. The predictive impact of population-derived data is limited in individual patients. However, DL-based predictive modeling that accounts for unique circumstance-specific scenarios is able to model individual patient predictive recurrence and generate predicted survival probabilities and responses to psychological stressors with a 95% degree of confidence. The modeling demonstrates the exceptional variability of individual recurrence probabilities and will enable clinical investigation of the impact of variables in specific scenarios.
Keywords:
deep learning
; dormancy
; recurrence
; survival models
; breast cancer
; seer-medicare linked dataset
; anxiety
; depression
1. Introduction
Breast cancer (BC) cells begin to metastasize before primary breast tumors can be detected at the 2-3 millimeter size at the start of angiogenesis and travel to the bone marrow (BM) where they can be found in 27–40% of newly diagnosed patients with localized disease [1,2]. Only one in 105-106 cancer cells that embark on this journey survive the trip to a metastatic site. Furthermore, most of the cells that do reach the BM are killed by active cell death signaling from the hostile microenvironment. Nevertheless, some of these highly resilient cells with tumor-initiating characteristics do survive and are rendered quiescent by signaling initiated by cellular, structural, and soluble components of the bone marrow microenvironment, forming a dormancy niche [3,4,5,6,7,8,9,10,11]. Dormant cells are heterogeneous [12] and survive neoadjuvant or adjuvant systemic therapy [13,14] due to inherent cancer stem cell drug resistance [6,7] and protection endowed by the niche [15,16]. Most of our understanding of the metastatic niche was derived from the bone marrow microenvironment because of its relative ease of access for investigations [17]. However, breast cancer cells also metastasize to other organs, such as the contralateral breast, skin, lungs, liver, and brain, among others, where they can become dormant [17].
Dormant micrometastases can seize opportunities to overcome suppression by a microenvironment potentially weakened by a spectrum of insults suffered over the patient's lifetime and reawaken [17,18]. Indeed, the presence of micrometastases is an independent prognostic indicator for survival in breast cancer patients [1,19]. Once dormant cells reawaken, they are unable to return to dormancy [8] and begin to generate growing metastases. These proliferating cells cause a feed-forward effect, inducing secretory senescence in bone marrow stromal cells in a cell dose-dependent manner [8].
Factors associated with increased risks of recurrence are advanced stage, T-stage, moderate and poorly differentiated grades, negative hormone receptor status and gene expression profile [20,21,22]. Estrogen receptor (ER)-/progesterone receptor (PR)- tumors recur sooner than ER+/PR+ tumors [23]. Their recurrence rate peaks at 2-4 years, with a more than 3-fold greater hazard ratio than that of ER+/PR+ tumors, then declines rapidly and drops below the rate of ER+/PR+ or less aggressive tumors by 8 years [24]. Both continue to recur for more than 25 years [2,19,23,24,25,26,27,28,29]. African American (AA) patients recur sooner and more frequently than White (W) patients due to aggressive cancer molecular features [30,31,32,33,34,35], social [17,35,36,37], treatment [36] and adverse events differences from W patients [38,39,40]. Younger patients recur sooner [41], as they have more aggressive cancer genotypes and more frequent ER-/PR- tumors [17].
These facts suggest that mechanisms of dormancy and recurrence are fundamentally different in cancers with differences in the aggressiveness of their genotypes [24]. This is consistent with the concept that the microenvironment's hold on maintaining dormancy in the ER-/PR- and other genotypically highly aggressive breast cancer cells is not as effective and enduring as that experienced by ER+/PR+ cancers. This is perhaps partly due to the lack of growth inhibition and dormancy induction in ER-/PR- cells by fibroblast growth factor 2 (FGF-2), a key factor in the initiation and maintenance of dormancy of ER+/PR+ BC cells in the bone marrow [3,42]. These data are also consistent with the fact that adjuvant systemic therapy decreases recurrence risk primarily in the first 5 years, but the effects disappear thereafer [24].
Specific factors associated with insults to the dormancy microenvironment have been investigated in preclinical and clinical studies. These include acute or slowly progressive estrogen deprivation [8,43], acute and chronic anxiety, depression and adrenergic stimulation [44], inflammation, including that associated with surgery [45,46,47,48,49,50,51,52,53], obesity [54] and bone marrow adipogenesis [55], hypercoagulable states [56], including ones caused by viral infections [57,58,59], toxins [60,61] and others [17]. Clinical trials have provided support for the use of anti-inflammatory [48,49] and anti-adrenergic drugs [62,63,64,65] for preventing the recurrence of breast cancer. Although limited and preliminary, these investigations provide some intriguing insight into understanding potential mechanisms for recurrence. As in any population-averaged study, broad inclusion and exclusion criteria may mask patient and tumor variables that confound significant observations.
One of our aims in medical oncology is to identify variables that predictably induce a high likelihood of recurrence in specific scenarios generated by cancer variables, patient characteristics, and life events that disrupt the dormancy niche. It is exceptionally difficult to develop clinical trials to generate this genre of data. Some studies have applied machine learning, a subfield of Artificial Intelligence (AI), to predict BC recurrence using tabular data predictors [66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87]. Other BC recurrence prediction studies [83,88] have applied deep learning (DL), another subfield of AI. Machine learning requires feature engineering, and the data scientist has identified what features to include for which model. However, DL infers the features and develops the model based on the inferred features (covariates). Applying DL to large datasets can characterize high-risk, unique circumstances for recurrence based on these variables and point to interventions associated with diminishing the likelihood of recurrence in those specific scenarios.
Predicting the risk of BC recurrence with a high level of accuracy remains an open problem [89]. It is crucial for selecting an effective individualized treatment plan and helping inform patients about their future risks, which may guide their life decisions. Studies have shown that anxiety and depression have adverse effects on recurrence in BC patients [90,91,92,93,94,95,96,97]. In this study, we address the critical question of the role of anxiety and depression in the recurrence of dormant breast cancer, particularly in the elderly population, using the SEER-Medicare dataset, which includes hundreds of thousands of BC patients diagnosed during the period 1991-2015. It is worth noting the significant barriers elderly adults seeking psychiatric treatment faced during this period; these include a lack of readily available mental health services specifically tailored to their needs and referrals from primary care physicians.
To our knowledge, our study is the first to develop DL predictive modeling using longitudinal data for more than 20 years of datasets (SEER-Medicare) with hundreds of thousands of patients and millions of follow-up visits. The SEER-Medicare dataset is available from the National Cancer Institute through a review process. Our DL models take into consideration surgery, radiation, biological, and chemotherapy, which are the mainstays of treatment for breast tumors. In addition, our DL models consider time-fixed covariates recorded at the time of diagnosis, including age, race, marital status, breast cancer stage, tumor grade, laterality, ER, PR, and human epidermal receptor 2 (HER2) status, and comorbidity index. At each patient follow-up visit, our models consider time-varying covariates, including administered treatments, comorbidity index, age, and induced adverse events, including anxiety and depression. Applying DL enabled the capture of complex nonlinear interactions among all these covariates.
2. Methods
2.1. Dataset and Patients
Our study data is the longitudinal SEER-Medicare (S-M) linked dataset [98] obtained through a two-tiered review process under an IRB-exempt review. Medicare files capture fee-for-service claims from hospitals, outpatient facilities, hospice care, home health agencies, prescription drug claims (from 2007), and National Claims History records of physician/supplier bills for claims collected by CMS and from physicians. Each file includes the unique patient ID, service date(s), diagnosis, procedure codes, and reimbursed amount. The cohorts included all female BC beneficiaries ages 65 and older who enrolled in Medicare for age eligibility at 65 years, not disability. The cohorts had equal months of Parts A and B coverage and no managed care coverage. Patients were diagnosed between 1991 and 2015 with Stages I, II, III, or IV as their only primary cancer, i.e., no other malignancy by NCI clinical trials definitions [98], and who also died of cancer between 1991 and 2015. We used the S-M Ccflag file information to compute a patient's comorbidity index (CI) [99]. A patient's Comorbidity index (CI) at a given time was the sum of the weights, based on the C3 comorbidity index [99], specific to this patient's comorbid conditions, as per the Ccflag file, at this time. CI at diagnosis was based on the patient's inpatient and outpatient claims during the full year before diagnosis.
Missing Data. We include patients with valid ID, cancer type, stage, sex, and race. We include a patient visit if it has a valid patient ID, date of diagnosis, and valid diagnosis, procedure, or HCPCS codes.
Codes and Variables. All files include dates of service and codes for specific diagnoses and procedures using either ICD-9-CM codes or Health Care Procedure Codes (HCPCS. We included all dates and CPT-HCPCS codes for the type of breast and lymph node surgery, of radiation, coded dates, type, body location, and duration, and number of months of adjuvant hormone therapy after the completion of adjuvant chemotherapy and/or biotherapy. We consolidate 141 HCPCS drug J codes: 82 chemotherapy drugs, 49 biotherapy drugs, and 10 hormone therapy drugs used in BC standard-of-care therapy or investigated in clinical trials into 46 categories based on mechanisms of action [40]. We categorized ICD-9 codes of potential AEs into 18 categories representing cancer treatment AEs in the literature [100,101,102,103,104]. These are: 0) no-AEs, 1) infection/fever, 2) neutropenia/leukopenia, 3) thrombocytopenias, 4) anemias, 5) electrolyte abnormalities, 6) liver/gall bladder abnormalities, 7) weakness/malaise/delirium, 8) nausea /vomiting, 9) diarrhea, 10) thrombophilia, 11) pulmonary embolus, 12) edema of any organs 13) skin rashes, 14) weight loss/malnutrition, 15) respiratory symptoms, 16) constipation, 17) mucositis, and 18) neuropathy. We include ICD-9 codes for anxiety (29384, 30000-30029, 3003, 3004) and depression (29013, 29021, 296.1, 296.2, 296.3), in addition to the 18 somatic treatment-associated AEs, and apply them in later life events as risk factors for recurrence [105]. Treatments and AEs. We recorded adjuvant treatment covariates from the time of diagnosis until completion of adjuvant therapy, up to 18-months, to ensure the inclusion of patients receiving Trastuzumab for a year after adjuvant chemotherapy. Covariates include treatment (drug HCPC code) and dates of administration.
2.2. Recurrence
Since the SEER-Medicare data do not explicitly capture recurrence, we inferred the occurrence of recurrence when a new diagnosis of contralateral BC, stage IV BC, new chemo-, bio-, hormone, or radiotherapy outside the 4-month window after completion of adjuvant therapy is recorded. We determined the Time to recurrence, which begins 4 months after completion of adjuvant therapy, to factor in the start of antiestrogens until a recurrence event date. Table 1 shows the details and pseudo-codes of our algorithm to infer recurrence in BC patients.
2.3. Deep Learning Predictive Modeling
Discrete Time-to-Event Data
In our dataset, as in real life, patient follow-up visits occur on a given day with irregular gaps between two consecutive visits. By applying the recurrence algorithm (Table 1), a patient's recurrence status is determined at each visit while the patient is at risk, i.e., has not yet experienced recurrence. Our study has start and end dates; thus, it is right-censored, i.e., some patients are not followed to their recurrence time, resulting in censored time (either the time a patient is lost to follow-up, i.e., time of last visit the patient was seen alive or the study end date). Thus, instead of observing the recurrence at time, , we observe a possibly right-censored event time, is the censoring time.
Our dataset, can be viewed as a set of N patients' history, , where is the patient covariates, is either this patient's recurrence or censoring time, and is the recurrence () or censoring () occurred at time, . This discrete-time framework is used to predict the likelihood of recurrence at each visit. Let be the time to recurrence since diagnosis and and is a covariate vector. We are predicting the probability of a patient experiencing recurrence by time , which is given by An alternative to this probability is the survival function, . Similar to survival analysis, we express the recurrence models in terms of the hazard rate,
Figure 1.
Predictive modeling or recurrence algorithm.
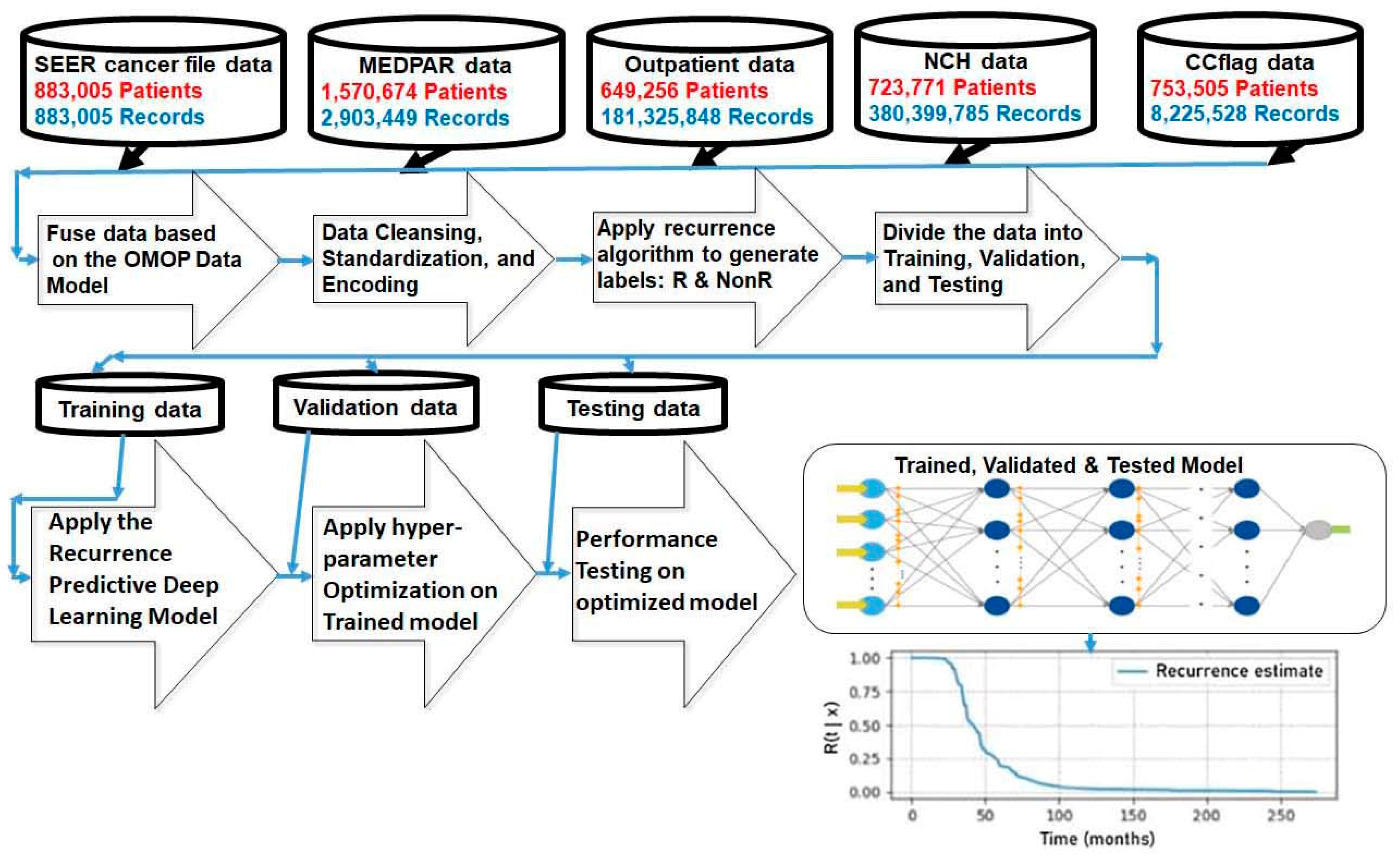
Cancer Patient Recurrence and the Cancer Patient Survival. We build on our work [106,107] by mapping the cancer patient recurrence prediction modeling to the cancer survival prediction modeling. Thus, the time-to-event models are applied by considering the recurrence of a BC patient as the event of interest rather than the patient's survival, as in [106,107].
Experiments
We applied the four predictive models discussed in our prior publications [106,107] when using the patients' time-fixed and time-varying covariates that summarize the patient's history from previous visits.
Performance Metrics. We used the concordance index (C-index) for discriminative evaluation in our recurrence analysis and measured the model's performance using the integrated Brier score (IBS) as a metric of the discrimination and calibration of the model's estimates, as before [106,107].
Model hyperparameters. We applied Amazon SageMaker Python SDK (software development kit), an open-source library, to fine-tune the model by identifying optimal values of the network's hyperparameters [106,107].
The experiments were conducted using five-fold cross-validation using a Bayesian optimization search scheme [108].
Validation. In [106,107] we demonstrated the validation of our implementation of the pycox package [109] using the real-world dataset METABRIC [110] and SUPPORT [111].
To validate our recurrence results, we used the real-world dataset, the Wisconsin Prognosis Breast Cancer (WPBC) dataset [WPBC], obtained from the University of Wisconsin Hospitals and can be found in the UCI Machine Learning Repository [112]. The dataset, which many BC researchers have used [113], consists of 30 features of 196 patients (47 recurrent and 151 non-recurrent). Several studies have shown 93.2% accuracy when using this dataset [113]. This result is aligned with our average and standard deviation of the time-dependent concordance, 0.949 (0.025) when applying five-fold cross-validation.
Features of the WPBC dataset:
Radius of the tumor (ìm); Texture of the tumor; Perimeter of the tumor (ìm); Area of the tumor (ìm2); Smoothness of the tumor; Compactness of the tumor; Concavity; Number of concave points; Symmetry; Fractal dimension; S.E. Radius of the tumor (ìm); S.E. Texture of the tumor; S.E. Perimeter of the tumor (ìm); S.E. Area of the tumor (ìm2); S.E. Smoothness of the tumor; S.E. Compactness of the tumor; S.E. Concavity; S.E. Number of concave points; S.E. Symmetry; S.E. Fractal dimension; M.T.L.V. Radius of the tumor (ìm); M.T.L.V. Texture of the tumor; M.T.L.V. Perimeter of the tumor (ìm); M.T.L.V. Area of the tumor (ìm2); M.T.L.V. Smoothness of the tumor; M.T.L.V. Compactness of the tumor; M.T.L.V. Concavity; M.T.L.V. Number of concave points; M.T.L.V. Symmetry; M.T.L.V. Fractal dimension.
Note, S.E. = Standard Error and M.T.L.V. = Mean of Three Largest Value
3. Results
3.1. Patient Characteristics
The characteristics of all patients in the dataset are outlined in Table 2. and compared to the subset of patients who have registered diagnoses of anxiety and/or depression (anxiety/depression). The patients in the dataset have breast cancers that are approximately 65% ER+/PR+, 3.5% ER-PR-, and 12% ER+/PR-. There are no patients with ER-/PR+ cancers. Approximately 56% of patients have stage I disease, 32% have stage II disease, and 12% have stage III disease. Approximately 88% of patients are W, 7% are AA, and 5% are of other races. About 5% of patients are of Hispanic ethnicity. All of the patients range in age from 73 to 75 years. These are consistent with published data reflecting the S-M population [39].
The comorbidity index of the patients in the dataset at diagnosis was less than 1.0 for all patients in every group. Approximately 36% of all patients were flagged with diagnostic codes for anxiety/depression. The hormone receptor status and stage distributions were not different in the patients with diagnosis of anxiety/depression compared to the general population. W patients were significantly more frequent in the anxiety/depression subpopulation than in the general population, while AA and other race group patients were fewer. The Time from diagnosis to flags for anxiety/depression varied between approximately 23 months to 35 months, with the shortest times noted in stage III and AA patients.
We compared characteristics between non-recurrent and recurrent patients in Table 3. The ages of all subgroups were similar and did not vary between the groups. Comorbidity indices at diagnosis were less than 1.0 in both categories in all subgroups. Approximately 15% of patients were flagged as recurrent, according to our algorithm. Recurrence was substantially higher in ER-PR- patients than in ER+PR+ patients and ER+/PR- patients. ER+/PR- patients recurred at a higher rate than ER+/PR+ patients. Recurrence rates increased substantially with progressive stage, were slightly higher in AA patients than in W patients and less in patients of other races. Recurrence was less in Hispanic patients than in the general population. The Time from diagnosis to recurrence varied from approximately 26 to 46 months, with the short durations noted for ER-/PR-, stage III and AA patients. The comorbidity index at recurrence was consistently higher than recorded at diagnosis in all subgroups.
We analyzed the differences between recurrence in patients without and with anxiety/depression in Table 4. Patients with anxiety/depression recured at a rate that was 27.9% higher than patients without anxiety/depression flagged in their records and had higher comorbidity indices at recurrence. Patients with ER+/PR+ BC were impacted more by anxiety/depression than patients with ER-PR- BC. Anxiety/depression are associated with higher recurrence in Stage I BC than in Stage II or III BC. Anxiety/depression are associated with higher recurrence, specifically in W patients than in AA or other races. Anxiety/depression are associated with higher recurrence in Hispanic patients.
We note that the Time from diagnosis to recurrence is greater in patients with anxiety/depression than in patients without anxiety/depression. The effect is not seen in stage II and AA patients, where anxiety/and depression have minimal impact on recurrence. The delayed onset of higher rates of recurrence follows the onset of anxiety/depression by several months, consistent with a causal effect of the higher rates by the onset of these symptoms, followed by a wave of recurrence that delays the average of the population, compared to patients without anxiety/depression.
3.2. Predictive Modeling of Recurrence-Free Survival
Our population-based analyses demonstrate significant associations of adrenergic stimuli of anxiety/depression in patients with localized breast cancer. The effect was evident in most broad categories defined by cancer hormone receptor status, cancer stage, patient race, and ethnicity. The effects were more prominent in some categories than others, as noted above. However, the differences are averaged and have significant variability. The broad variability in these rates, as with all previously investigated recurrence hazards, is due to multiple other variables associated with the unique scenarios endowed by the combined effects of each patient, cancer, and treatment history. To improve the predictive model and address this challenge, we applied DL predictive modeling in individual circumstances.
The results in Table 5 demonstrate, for both categories of ER+/PR+ and ER-/PR- in stages I, II, and III, a high prediction accuracy, as shown by the high values of the time-dependent Concordance indices and high-level models' discrimination and calibration as demonstrated by the low values of the integrated Brier Scores.
We generated randomly selected hypothetical patient predictive survival curves to illustrate the impact of anxiety/depression in individual circumstances (Figure 2). We generated these curves in patient groupings with the highest effects on recurrence, which were associated with the interaction of stage, race, anxiety, depression, and analogous comparison groups. The categories we analyzed were W/ER+/PR+ patients in stages I and III and AA/ER-PR- patients in stages I and III. Our DUA with the NCI SEER-Medicare does not allow us to include specific patient-identifying information. Hence, we identify these results as hypothetical patient recurrence-free survival curves.
The first immediately apparent fact is the vastly wide temporal distributions of hypothetical patient-predicted recurrence-free survival curves. The median recurrence-free survival in the 12 curves in the stage I/W/ER+PR+ patient group with no anxiety/depression ranged from 25 months to 260 months. In the group with anxiety/depression, this range was 20 months to 170 months. While these examples were randomly selected from each of the broad race, stage and hormone receptor categories, the individual prediction curves were generated by considering the contribution of many additional patient-, cancer- and treatment-specific variables. They demonstrate that the anxiety/depression groups had far fewer long-term recurrence-free survival curves.
The median survival in stage I/AA/ER-/PR- with no anxiety/depression curves ranged from 20 months to 235 months. In the same group with anxiety/depression, the median recurrence ranged from 25 months to 260 months. The group was peppered with some very long-term recurrence-free hypothetical predicted survival curves in both no anxiety/depression groupings. There were more random short recurrence-free survival curves in the anxiety/depression group, though.
The median survival in the stage III/W/ER+/PR+ with no anxiety/depression curves ranged from 20 months to 185 months, with all but one of the disease-fee predicted survival curves having a median of 100 months or less. The median survival in the stage III/W/ER+/PR+ with anxiety/depression curves ranged from less than 10 months 170 months, with more than half the curves having a median of 75 months.
The median survival in the random hypothetical curves from stage III/AA/ER-/PR- category with either without or with anxiety/depression ranged from 0 months to 1.3 months.
These results demonstrate the exceptional variability of median predicted survival rates and their modifications by chronic adrenergic stimuli of anxiety/depression within established, well-studied population-averaged predictive categories. It helps explain the wide confidence intervals in existing population-based prognostic curves and the need to approach predictive modeling using circumstance-specific scenarios.
4. Discussion
Thousands of studies on variables that can induce, sustain and disrupt dormancy have generated a great deal of data on factors that may contribute to the reawakening of dormant micrometastases. Most of the data are preclinical, but there have been some clinical trials that provided early insight into the role of adrenergic stimuli in the recurrence of breast cancer. [62,63,64,65]. The clinical data is limited and does not provide detail on the patient and cancer variables and their interaction that impacts recurrence.
Our investigations on the S-M population of elderly patients confirmed our previously characterized patient age and racial distributions and the distribution of cancers by hormone receptor status [39]. The comorbidity index of all patients and the subgroups we analyzed was less than 1.0 at the time of diagnosis, reflecting a relatively healthy population of patients diagnosed with localized breast cancer. Since anxiety/depression have been associated with the reawakening of dormant breast cancer, we analyzed the variables associated with it in our patient datasets.
Anxiety, depression, and fear of cancer recurrence are well-documented symptoms in breast cancer patients [114]. In our population, approximately 36% of the patients were diagnosed with anxiety/depression. We found these symptoms more frequently documented in W patients. However, they tended to occur sooner from the time of diagnosis in AA patients than W patients and in patients with stage III disease compared with patients with stage I disease. During the period of 1991-2015 covering the period of the S-M dataset patients in our analysis, elderly adults seeking treatment from psychiatrists faced significant barriers, including a lack of readily available mental health services specifically tailored to their needs, referrals from primary care physicians, and an overreliance on inpatient treatment options, often leading to underdiagnosis and inadequate treatment for mental health issues like anxiety and depression [115]. Our results will provide data for the development of support for such services in the prevention of the recurrence of dormant breast cancer with greater opportunities to provide more comprehensive and personalized care for older patients battling cancer and survivors through tailored interventions [114]. A limitation of using administrative claims data from the S-M to identify patients with depression is the low sensitivity and positive predictive values, under 50%, due to substantial discrepancy between the presence and timing of depression diagnoses in medical claims and inpatient charts [116] and racial differences in reporting claims for depression [117]. Nevertheless, the specificity and negative predictive values are consistently higher than 70% [116,117].
As noted earlier, to overcome the limitation that the S-M data do not explicitly capture recurrence, we inferred a recurrence event when a new diagnosis of contralateral BC, stage IV BC, new chemo-, bio-, hormone, or radiotherapy was recorded outside the 4-month window after completion of adjuvant therapy. This approach still has the limitation that elderly patients diagnosed with recurrent disease often decline diagnostic surgical procedures or systemic therapy, and thus, their recurrence is underdiagnosed [118,119]. Our algorithm identified approximately 15% of the patients in the dataset as recurring during the period of observation. The ages of recurrent and non-recurrent patients were similar, and the higher incidence of recurrence in ER-/PR- tumors, progressive stage, and AA patients mirrored that of published data. However, our data showed a lower rate of recurrence in Hispanic patients. Despite the limitations, the data mirrored well-documented shorter time to recurrence in ER-PR-, stage III, and AA patients.
Even within the sensitivity limitations of the S-M dataset, our data demonstrate, for the first time, that patients with anxiety/depression recur at an average of 27.9% greater rate than patients without these symptoms. Patients with these symptoms also have significantly higher comorbidity indices at recurrence than patients without psychological stress symptoms. The impact of the symptoms is highest in ER+/PR+ BC, stage I, in W, and Hispanic patients. The average time from diagnosis of BC to recurrence is greater, though, in patients with anxiety/depression and follows the onset of these psychiatric symptoms by a few months, suggesting a causal effect. As the hazard ratio for recurrence decreases gradually with years after diagnosis [24], the impact of adrenergic signaling of chronic psychologic stress modifies the subsequent hazard ratio and results in a delayed wave or recurrence that increases the overall rate of recurrence and the population's average time to recurrence after diagnosis
However, when analyzing individual hypothetical patient predictive recurrence-free survival curves, the extreme shortcoming of predictive modeling of averaged populations allocated to a few prognostic groups becomes starkly evident. Median individual survival within a population category can vary by more than a decade. The impact of psychological stress-induced recurrence also varies widely and without explanations available from the few variables of race, stage, and hormone receptor status. There are indeed many variables available from patients and even large databases, but slicing and dicing the population to obtain population-averaged differences with the shrinking n value available for statistical comparisons would suffer from statistical significance. Constructing clinical trials with an unmanageable number of variables would also be untenable due to a variety of limitations. Hence, predictive modeling of individual scenario survival curves provides a unique opportunity to investigate individual variables that can be used to further generate specific hypotheses on the role of relevant variables on the recurrence of dormancy. The exceptionally high concordance indices and their high confidence demonstrate that this approach will be a useful tool when adapted to patient care and designing potential clinical investigations and treatment interventions. Future investigations will expand to additional databases with additional age and insurance parameters profiles to confirm and enhance the predictive modeling to apply more closely to the general population.
5. Conclusions
This study demonstrates, for the first time, that anxiety/depression, psychological stressors that induce chronic adrenergic stimulation, increase the population-averaged rate of recurrence of dormant breast cancer in elderly SEER-Medicare patients with stage I, II, and III localized disease. The impact of these psychological stressors is observed in patient groups with different races, cancers with different hormone receptor status, and different stages. The predictive impact on the recurrence of individual patients is limited due to the effects of averaging multiple covariates that impact recurrence in individuals over population-derived data. To address this challenge, we developed recurrence predictive models that account for patient, cancer, treatment, adverse events, and time-dependent variables, which, when combined, generate a unique, circumstance-specific scenario. The concordance index of the predictive modeling was greater than 95%, with high degrees of confidence. We generated hypothetical patients predicted recurrence-free survival curves and demonstrated that within each race and stage category, the median predicted survival varied by up to more than a decade in individual patients, both in groups without and with anxiety/depression. The data demonstrate that individual patient predictive modeling based on individual unique circumstances can generate predicted survival probabilities and responses to psychological stressors. This approach will enable the investigation of the specific impact of variables in specific scenarios that can generate hypotheses to be tested in directed clinical investigations and therapy.
Institutional Review Board Statement
The study was approved by the Rutgers Institutional Review Board under Exempt Review study number Pro20140000175.
Acknowledgments
This research was funded by 1. Northeast Big Data Innovation Hub, USA, GG014586-02 (RW and NA); 2. 2020 Busch Biomedical Grant Program, USA (RW and NA); 3. AmazonWeb Services Health Equity Initiative ("HEI") Program, USA, CC ADV 00011104 2023 TR (RW and NA). This study used the linked SEER-Medicare database. The interpretation and reporting of these data are the sole responsibility of the authors. The authors acknowledge the efforts of the National Cancer Institute; Information Management Services (IMS), Inc.; and the Surveillance, Epidemiology, and End Results (SEER) Program tumor registries in the creation of the SEER-Medicare database and wish to thank them for their advice and review of the datasets designating the different treatment venues. The collection of cancer incidence data from the California Cancer Registry used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention's (CDC) National Program of Cancer Registries, under cooperative agreement 1NU58DP007156; the National Cancer Institute's Surveillance, Epidemiology and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors.
References
- Braun, S.; Pantel, K.; Muller, P.; Janni, W.; Hepp, F.; Kentenich, C.R.; Gastroph, S.; Wischnik, A.; Dimpfl, T.; Kindermann, G.; et al. Cytokeratin-positive cells in the bone marrow and survival of patients with stage I, II, or III breast cancer. New. Engl. J. Med. 2000, 342, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Hartkopf, A.D.; Brucker, S.Y.; Taran, F.A.; Harbeck, N.; von Au, A.; Naume, B.; Pierga, J.Y.; Hoffmann, O.; Beckmann, M.W.; Rydén, L.; et al. Disseminated tumour cells from the bone marrow of early breast cancer patients: Results from an international pooled analysis. Eur. J. Cancer 2021, 154, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Korah, R.; Boots, M.; Wieder, R. Integrin α5β1 promotes survival of growth-arrested breast cancer cells: An in vitro paradigm for breast cancer dormancy in bone marrow. Cancer Research 2004, 64, 4514–4522. [Google Scholar] [CrossRef] [PubMed]
- Najmi, S.; Korah, R.; Chandra, R.; Abdellatif, M.; Wieder, R. Flavopiridol blocks integrin-mediated survival in dormant breast cancer cells. Clinical Cancer Research 2005, 11, 2038–2046. [Google Scholar] [CrossRef]
- Barrios, J.; Wieder, R. Dual FGF-2 and intergrin α5β1 signaling mediate GRAF-induced RhoA inactivation in a model of breast cancer dormancy. Cancer Microenvironment 2009, 2, 33–47. [Google Scholar] [CrossRef]
- Klein, C.A. Parallel progression of primary tumours and metastases. Nat. Rev. Cancer 2009, 9, 302–312Car19. [Google Scholar] [CrossRef]
- Huang, Z.; Wu, T.; Liu, A.Y.; Ouyang, G. Differentiation and transdifferentiation potentials of cancer stem cells. Oncotarget 2015, 6, 39550–39563. [Google Scholar] [CrossRef]
- Tivari, S.; Lu, H.; Dasgupta, T.; De Lorenzo, M.S.; Wieder, R. Reawakening of dormant estrogen-dependent human breast cancer cells by bone marrow stroma secretory senescence. Cell Communication and Signaling 2018, 16, 48. [Google Scholar] [CrossRef]
- Nobre, A.R.; Risson, E.; Singh, D.K.; di Martino, J.; Cheung, J.F.; Wang, J.; Johnson, J.; Russnes, H.G.; Bravo-Cordero, J.J.; Birbrair, A.; et al. Bone Marrow NG2+/Nestin+ mesenchymal stem cells drive DTC dormancy via TGFβ2. Nat. Cancer 2021, 2, 327–339. [Google Scholar] [CrossRef]
- Wieder, R. Bone marrow stoma co-cultivation model of breast cancer dormancy. Methods in Molecular Biology 2024, 2811, 55–67. [Google Scholar] [CrossRef]
- Sreekumar, A.; Lu, M.; Choudhury, B.; Pan, T.C.; Pant, D.K.; Lawrence-Paul, M.R.; Sterner, C.J.; Belka, G.K.; Toriumi, T.; Benz, B.A.; Escobar-Aguirre, M.; Marino, F.E.; Esko, J.D.; Chodosh, L.A. B3GALT6 promotes dormant breast cancer cell survival and recurrence by enabling heparan sulfate-mediated FGF signaling. Cancer Cell. 2024, 42, 52–69. [Google Scholar] [CrossRef] [PubMed]
- Fluegen, G.; Avivar-Valderas, A.; Wang, Y.; Padgen, M.R.; Williams, J.K.; Nobre, A.R.; Calvo, V.; Cheung, J.F.; Bravo-Cordero, J.J.; Entenberg, D.; et al. Phenotypic heterogeneity of disseminated tumour cells is preset by primary tumour hypoxic microenvironments. Nat. Cell Biol. 2017, 19, 120–132. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.; Kentenich, C.; Janni, W.; Hepp, F.; de Waal, J.; Willegroth, F.; Sommer, H.; Pantel, K. Lack of an effect of adjuvant chemotherapy on the elimination of single dormant tumor cells in bone marrow of high risk breast cancer patients. J. Clin. Onc. 2000, 18, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Naumov, G.N.; Townson, J.L.; MacDonald, I.C.; Wilson, S.M.; Bramwell, V.H.; Groom, A.C.; Chambers, A.F. Ineffectiveness of doxorubicin treatment on solitary dormant mammary carcinoma cells or late-developing metastases. Breast Cancer Res. Treat. 2003, 82, 199–206. [Google Scholar]
- Carlson, P.; Dasgupta, A.; Grzelak, C.A.; Kim, J.; Barrett, A.; Coleman, I.M.; Shor, R.E.; Goddard, E.T.; Dai, J.; Schweitzer, E.M.; et al. Targeting the perivascular niche sensitizes disseminated tumour cells to chemotherapy. Nat. Cell Biol. 2019, 21, 238–250. [Google Scholar] [CrossRef]
- Hughes, R.; Chen, X.; Cowley, N.; Ottewell, P.D.; Hawkins, R.J.; Hunter, K.D.; Hobbs, J.K.; Brown, N.J.; Holen, I. Osteoblast-derived paracrine and juxtacrine signals protect disseminated breast cancer cells from stress. Cancers 2021, 13, 6. [Google Scholar] [CrossRef]
- Wieder, R. Awakening of Dormant Breast Cancer Cells in the Bone Marrow. Cancers 2023, 15, 3021. [Google Scholar] [CrossRef]
- Wieder, R. Insurgent micrometastases: Sleeper cells and harboring the enemy. J. Surgical Oncology 2005, 89, 207–210. [Google Scholar] [CrossRef]
- Braun, S.; Vogl, F.D.; Naume, B.; Janni, W.; Osborne, M.P.; Coombes, R.C.; Schlimok, G.; Diel, I.J.; Gerber, B.; Gebauer, G.; et al. A pooled analysis of bone marrow micrometastasis in breast cancer. N. Engl. J. Med. 2005, 353, 793–802. [Google Scholar] [CrossRef]
- Fan, C.; Oh, D.S.; Wessels, L.; Weigelt, B.; Nuyten, D.S.; Nobel, A.B.; van't Veer, L.J.; Perou, C.M. Concordance among gene-expression-based predictors for breast cancer. N. Engl. J. Med. 2006, 355, 560–569. [Google Scholar] [CrossRef]
- Cheng, L.; Swartz, M.D.; Zhao, H.; Kapadia, A.S.; Lai, D.; Rowan, P.J.; Buchholz, T.A.; Giordano, S.H. Hazard of recurrence among women after primary breast cancer treatment--a 10-year follow-up using data from SEER-Medicare. Cancer Epidemiol Biomarkers Prev. 2012, 21, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.Z.; Wang, L.; Hu, X.; Shao, Z.M. Effect of tumor size on breast cancer-specific survival stratified by joint hormone receptor status in a SEER population-based study. Oncotarget. 2015, 6, 22985–22995. [Google Scholar] [CrossRef]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: Clinical features and patterns of recurrence. Clin. Cancer Res. 2007, 13, 4429–4434. [Google Scholar] [CrossRef]
- Jatoi, I.; Anderson, W.F.; Jeong, J.H.; Redmond, C.K. Breast cancer adjuvant therapy: Time to consider its time-dependent effects. J. Clin. Oncol. 2011, 29, 2301–2304. [Google Scholar] [CrossRef] [PubMed]
- Naume, B.; Synnestvedt, M.; Falk, R.S.; Wiedswang, G.; Weyde, K.; Risberg, T.; Kersten, C.; Mjaaland, I.; Vindi, L.; Sommer, H.H.; et al. Clinical outcome with correlation to disseminated tumor cell (DTC) status after DTC-guided secondary adjuvant treatment with docetaxel in early breast cancer. J. Clin. Oncol. 2014, 32, 3848–3857. [Google Scholar] [CrossRef]
- Colleoni, M.; Sun, Z.; Price, K.N.; Karlsson, P.; Forbes, J.F.; Thürlimann, B.; Gianni, L.; Castiglione, M.; Gelber, R.D.; Coates, A.S.; et al. Annual Hazard Rates of Recurrence for Breast Cancer During 24 Years of Follow-Up: Results from the International Breast Cancer Study Group Trials I to V. J. Clin. Oncol. 2016, 34, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Borgen, E.; Rypdal, M.C.; Sosa, M.S.; Renolen, A.; Schlichting, E.; Lonning, P.E.; Synnestvedt, M.; Aguirre-Ghiso, J.A.; Naume, B. NR2F1 stratifies dormant disseminated tumor cells in breast cancer patients. Breast Cancer Res. 2018, 20, 120. [Google Scholar] [CrossRef]
- Klein, C.A. Cancer progression and the invisible phase of metastatic colonization. Nat. Rev. Cancer 2020, 20, 681–694. [Google Scholar] [CrossRef]
- Bushnell, G.G.; Deshmukh, A.P.; den Hollander, P.; Luo, M.; Soundararajan, R.; Jia, D.; Levine, H.; Mani, S.A.; Wicha, M.S. ; Breast cancer dormancy: Need for clinically relevant models to address current gaps in knowledge. NPJ Breast Cancer. 2021, 7, 66. [Google Scholar] [CrossRef]
- Martini, R.; Newman, L.; Davis, M. Breast cancer disparities in outcomes; unmasking biological determinants associated with racial and genetic diversity. Clin. Exp. Metastasis 2022, 39, 7–14. [Google Scholar] [CrossRef]
- Joshi, S.; Garlapati, C.; Aneja, R. Epigenetic determinants of racial disparity in breast cancer: Looking beyond genetic alterations. Cancers 2022, 14, 1903. [Google Scholar] [CrossRef] [PubMed]
- Jiagge, E.; Chitale, D.; Newman, L.A. Triple-negative breast cancer, stem cells, and African ancestry. Am. J. Pathol. 2018, 188, 271–279. [Google Scholar] [CrossRef]
- Zhang, H.; Barner, J.C.; Moczygemba, L.R.; Rascati, K.L.; Park, C.; Kodali, D. Comparing survival outcomes between neoadjuvant and adjuvant chemotherapy within breast cancer subtypes and stages among older women: A SEER-Medicare analysis. Breast Cancer 2023, 30, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Wieder, R. Fibroblasts as turned agents in cancer progression. Cancers 2023, 15, 24. [Google Scholar] [CrossRef]
- Prakash, O.; Hossain, F.; Danos, D.; Lassak, A.; Scribner, R.; Miele, L. Racial disparities in triple negative breast cancer: A review of the role of biologic and non-biologic factors. Front. Public Health 2020, 8, 576964. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.C.; Wheeler, S.B.; Reeder-Hayes, K. Racial/ethnic and socioeconomic disparities in endocrine therapy adherence in breast cancer: A systematic review. Am. J. Public Health 2015, 105 (Suppl. S3), e4–e15. [Google Scholar] [CrossRef]
- Daly, B.; Olopade, O.I. A perfect storm: How tumor biology, genomics, and health care delivery patterns collide to create a racial survival disparity in breast cancer and proposed interventions for change. CA Cancer J Clin. 2015, 65, 221–238. [Google Scholar] [CrossRef]
- Russo, A.; Autelitano, M.; Bisanti, L. Re: Frequency and cost of chemotherapy-related serious adverse effects in a population sample of women with breast cancer. J. Natl. Cancer Inst. 2006, 98, 1826–1827. [Google Scholar] [CrossRef]
- Wieder, R.; Adam, N. Racial Disparities in Breast Cancer Treatments and Adverse Events in the SEER-Medicare Data. Cancers 2023, 15, 4333. [Google Scholar] [CrossRef]
- Adam, N.; Wieder, R. Temporal Association Rule Mining: Race-Based Patterns of Treatment-Adverse Events in Breast Cancer Patients Using SEER–Medicare Dataset. Biomedicines. 2024, 12, 1213. [Google Scholar] [CrossRef]
- Geurts, Y.M.; Witteveen, A.; Bretveld, R.; Poortmans, P.M.; Sonke, G.S.; Strobbe, L.J.A.; Siesling, S. Patterns and predictors of first and subsequent recurrence in women with early breast cancer. Breast Cancer Res Treat. 2017, 165, 709–720. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sreekumar, A.; Lu, M.; Choudhury, B.; Pan, T.C.; Pant, D.K.; Lawrence-Paul, M.R.; Sterner, C.J.; Belka, G.K.; Toriumi, T.; Benz, B.A.; Escobar-Aguirre, M.; Marino, F.E.; Esko, J.D.; Chodosh, L.A. B3GALT6 promotes dormant breast cancer cell survival and recurrence by enabling heparan sulfate-mediated FGF signaling. Cancer Cell. 2024, 42, 52–69. [Google Scholar] [CrossRef]
- Roy, R.; Yang, J.; Shimura, T.; Merritt, L.; Alluin, J.; Man, E.; Daisy, C.; Aldakhlallah, R.; Dillon, D.; Pories, S.; Chodosh, L.A.; Moses, M.A. Escape from breast tumor dormancy: The convergence of obesity and menopause. Proc Natl Acad Sci USA 2022, 119, e2204758119. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, N.; Zhong, L.; Wang, S.; Zheng, Y.; Yang, B.; Zhang, J.; Lin, Y.; Wang, Z. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: A systematic review and meta-analysis of 282,203 patients. Mol. Psychiatry 2020, 25, 3186–3197. [Google Scholar] [CrossRef]
- Forget, P.; Vandenhende, J.; Berliere, M.; Machiels, J.P.; Nussbaum, B.; Legrand, C.; DeKock, M. Do intraoperative analgesics influence breast cancer recurrence after mastectomy? A retrospective analysis. Anesth. Analg. 2010, 110, 1630–1635. [Google Scholar] [CrossRef]
- Retsky, M.; Rogers, R.; Demicheli, R.; Hrushesky, W.J.; Gukas, I.; Vaidya, J.S.; Baum, M.; Forget, P.; Dekock, M.; Pachmann, K. Nsaid analgesic ketorolac used perioperatively may suppress early breast cancer relapse: Particular relevance to triple negative subgroup. Breast Cancer Research & Treatment 2012, 134, 881–888. [Google Scholar]
- Hanin, L.; Pavlova, L. A quantitative insight into metastatic relapse of breast cancer. J. Theor. Biol. 2016, 394, 172–181. [Google Scholar] [CrossRef]
- Shaashua, L.; Shabat-Simon, M.; Haldar, R.; Matzner, P.; Zmora, O.; Shabtai, M.; Sharon, E.; Allweis, T.; Barshack, I.; Hayman, L.; et al. Perioperative Cox-2 and beta-adrenergic blockade improves metastatic biomarkers in breast cancer patients in a phase-ii randomized trial. Clin. Cancer Res. 2017, 23, 4651–4661. [Google Scholar] [CrossRef]
- Haldar, R.; Ricon-Becker, I.; Radin, A.; Gutman, M.; Cole, S.W.; Zmora, O.; Ben-Eliyahu, S. Perioperative cox2 and beta-adrenergic blockade improves biomarkers of tumor metastasis, immunity, and inflammation in colorectal cancer: A randomized controlled trial. Cancer 2020, 126, 3991–4001. [Google Scholar] [CrossRef]
- De Cock, J.M.; Shibue, T.; Dongre, A.; Keckesova, Z.; Reinhardt, F.; Weinberg, R.A. Inflammation triggers zeb1-dependent escape from tumor latency. Cancer Res. 2016, 76, 6778–6784. [Google Scholar] [CrossRef]
- Walker, N.D.; Elias, M.; Guiro, K.; Bhatia, R.; Greco, S.J.; Bryan, M.; Gergues, M.; Sandiford, O.A.; Ponzio, N.M.; Leibovich, S.J.; et al. Exosomes from differentially activated macrophages influence dormancy or resurgence of breast cancer cells within bone marrow stroma. Cell Death Dis. 2019, 10, 59. [Google Scholar] [CrossRef]
- Ricon, I.; Hanalis-Miller, T.; Haldar, R.; Jacoby, R.; Ben-Eliyahu, S. Perioperative biobehavioral interventions to prevent cancer recurrence through combined inhibition of beta-adrenergic and cyclooxygenase 2 signaling. Cancer 2019, 125, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Zhang, L.; Dong, Y.; Tian, Z.; Chen, Y.; Dong, S. Tumour dormancy in inflammatory microenvironment: A promising therapeutic strategy for cancer-related bone metastasis. Cell Mol Life Sci. 2020, 77, 5149–5169. [Google Scholar] [CrossRef] [PubMed]
- Ecker, B.L.; Lee, J.Y.; Sterner, C.J.; Solomon, A.C.; Pant, D.K.; Shen, F.; Peraza, J.; Vaught, L.; Mahendra, S.; Belka, G.K.; Pan, T.C.; Schmitz, K.H.; Chodosh, L.A. Impact of obesity on breast cancer recurrence and minimal residual disease. Breast Cancer Res. 2019, 21, 41. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bowers, E.; Singer, K. Obesity-induced inflammation: The impact of the hematopoietic stem cell niche. Jci Insight. 2021, 6, 145295. [Google Scholar] [CrossRef]
- Karpatkin, S. Does hypercoagulability awaken dormant tumor cells in the host? J. Thromb. Haemost. 2004, 2, 2103–2106. [Google Scholar] [CrossRef]
- Fogarty, H.; Townsend, L.; Morrin, H.; Ahmad, A.; Comerford, C.; Karampini, E.; Englert, H.; Byrne, M.; Bergin, C.; O'Sullivan, J.M.; et al. Persistent endotheliopathy in the pathogenesis of long covid syndrome. J. Thromb. Haemost. 2021, 19, 2546–2553. [Google Scholar] [CrossRef]
- Takatsuka, H.; Wakae, T.; Mori, A.; Okada, M.; Fujimori, Y.; Takemoto, Y.; Okamoto, T.; Kanamaru, A.; Kakishita, E. Endothelial damage caused by cytomegalovirus and human herpesvirus-6. Bone Marrow Transplant. 2003, 31, 475–479. [Google Scholar] [CrossRef]
- Hyakutake, M.T.; Steinberg, E.; Disla, E.; Heller, M. Concomitant infection with epstein-barr virus and cytomegalovirus infection leading to portal vein thrombosis. J. Emerg. Med. 2019, 57, e49–e51. [Google Scholar] [CrossRef]
- Kampeerawipakorn, O.; Navasumrit, P.; Settachan, D.; Promvijit, J.; Hunsonti, P.; Parnlob, V.; Nakngam, N.; Choonvisase, S.; Chotikapukana, P.; Chanchaeamsai, S.; et al. Health risk evaluation in a population exposed to chemical releases from a petrochemical complex in Thailand. Environ. Res. 2017, 152, 207–213. [Google Scholar] [CrossRef]
- Jaguin, M.; Fardel, O.; Lecureur, V. Exposure to diesel exhaust particle extracts (DEPe) impairs some polarization markers and functions of human macrophages through activation of AhR and Nrf2. PLoS ONE 2015, 10, e0116560. [Google Scholar] [CrossRef]
- Montoya, A.; Amaya, C.N.; Belmont, A.; Diab, N.; Trevino, R.; Villanueva, G.; Nahleh, Z. Use of non-selective beta-blockers is associated with decreased tumor proliferative indices in early stage breast cancer. . Oncotarget 2017, 8, 6446–6460. [Google Scholar] [CrossRef] [PubMed]
- Montoya, A.; Varela-Ramirez, A.; Dickerson, E.; Pasquier, E.; Torabi, A.; Aguilera, R.; Bryan, B. The beta adrenergic receptor antagonist propranolol alters mitogenic and apoptotic signaling in late stage breast cancer. . Biomedical Journal 2019, 42, 155–165. [Google Scholar] [CrossRef]
- Liu, Y.; Sun, J.; Wu, T.; Lu, X.; Du, Y.; Duan, H.; Tian, J. Effects of serum from breast cancer surgery patients receiving perioperative dexmedetomidine on breast cancer cell malignancy: A prospective randomized controlled trial. . Cancer Medicine 2019, 8, 7603–7612. [Google Scholar] [CrossRef] [PubMed]
- Hiller, J.G.; Cole, S.W.; Crone, E.M.; Byrne, D.J.; Shackleford, D.M.; Pang, J.B.; Henderson, M.A.; Nightingale, S.S.; Ho, K.M.; Myles, P.S.; Fox, S.; Riedel, B.; Sloan, E.K. Preoperative β-Blockade with Propranolol Reduces Biomarkers of Metastasis in Breast Cancer: A Phase II Randomized Trial. Clin Cancer Res. 2020, 26, 1803–1811. [Google Scholar] [CrossRef]
- El Haji, H.; Souadka, A.; Patel, B.N.; Sbihi, N.; Ramasamy, G.; Patel, B.K.; Ghogho, M.; Banerjee, I. Evolution of breast cancer recurrence risk prediction: A systematic review of statistical and machine learning–based models. JCO Clinical Cancer Informatics 2023, 7, p.e2300049. [Google Scholar] [CrossRef] [PubMed]
- Lauritzen, A.D.; Berg, T.; Jensen, M.B.; Lillholm, M.; Knoop, A. Identifying recurrent breast cancer patients in national health registries using machine learning. Acta Oncologica. 2023, 62, 350–357. [Google Scholar] [CrossRef]
- Sittenfeld, S.M.C.; Zabor, E.C.; Hamilton, S.N.; et al. A multi-institutional prediction model to estimate the risk of recurrence and mortality after mastectomy for T1-2N1 breast cancer. Cancer 2022, 128, 3057–3066, © 2023 by American Society of Clinical Oncology. [Google Scholar] [CrossRef]
- Lou, S.J.; Hou, M.F.; Chang, H.T.; Chiu, C.C.; Lee, H.H.; Yeh, S.C.; Shi, H.Y. Machine learning algorithms to predict recurrence within 10 years after breast cancer surgery: A prospective cohort study. Cancers 2020, 12, 3817. [Google Scholar] [CrossRef]
- Wang, C.; Xu, Y.; Lin, Y.; et al. Comparison of CTS5 risk model and 21-gene recurrence score assay in large-scale breast cancer population and combination of CTS5 and recurrence score to develop a novel nomogram for prognosis prediction. Breast 2022, 63, 61–70. [Google Scholar] [CrossRef]
- Rudloff, U.; Jacks, L.M.; Goldberg, J.I.; et al. Nomogram for predicting the risk of local recurrence after breast-conserving surgery for ductal carcinoma in situ. J Clin Oncol 2010, 28, 3762–3769. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Kim, K.S.; Lee, J.E.; et al. Development of novel breast cancer recurrence prediction model using support vector machine. J Breast Cancer 2012, 15, 230–238. [Google Scholar] [CrossRef] [PubMed]
- Mohebian, M.R.; Marateb, H.R.; Mansourian, M.; et al. A hybrid computer-aided-diagnosis system for prediction of breast cancer recurrence (HPBCR) using optimized ensemble learning. Comput Struct Biotechnol J 2016, 15, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.; Kim, K.S.; Park, R.W. Nomogram of naive Bayesian model for recurrence prediction of breast cancer. Healthc Inform Res 2016, 22, 89–94. [Google Scholar] [CrossRef]
- Wu, X.; Ye, Y.; Barcenas, C.H.; et al. Personalized prognostic prediction models for breast cancer recurrence and survival incorporating multidimensional data. J Natl Cancer Inst 2016, 109, djw314. [Google Scholar]
- Vazifehdan, M.; Moattar, M.H.; Jalali, M. A hybrid Bayesian network and tensor factorization approach for missing value imputation to improve breast cancer recurrence prediction. J King Saud Univ Comput Inf Sci 2018, 31, 175–184. [Google Scholar] [CrossRef]
- Yoo, S.H.; Kim, T.-Y.; Kim, M.; et al. Development of a nomogram to predict the recurrence score of 21-gene prediction assay in hormone receptor–positive early breast cancer. Clin Breast Cancer 2019, 20, 98–107.e1. [Google Scholar] [CrossRef]
- Gu, D.; Su, K.; Zhao, H. A case-based ensemble learning system for explainable breast cancer recurrence prediction. Artif Intell Med 2020, 107, 101858. [Google Scholar] [CrossRef]
- Wang, H.; Li, Y.; Khan, S.A.; et al. Prediction of breast cancer distant recurrence using natural language processing and knowledge-guided convolutional neural network. Artif Intell Med 2020, 110, 101977. [Google Scholar] [CrossRef]
- Baltres, A.; Al Masry, Z.; Zemouri, R.; et al. Prediction of Oncotype DX recurrence score using deep multi-layer perceptrons in estrogen receptor-positive, HER2-negative breast cancer. Breast Cancer 2020, 27, 1007–1016. [Google Scholar] [CrossRef]
- Alwohaibi, M.; Alzaqebah, M.; Alotaibi, N.M.; et al. A hybrid multi-stage learning technique based on brain storming opti- mization algorithm for breast cancer recurrence prediction. J King Saud Univ—Comput Inf Sci 2021, 34, 5192–5203. [Google Scholar] [CrossRef]
- Dawngliani, M.S.; Chandrasekaran, N.; Lalmawipuii, R.; et al. Breast cancer recurrence prediction model using voting technique. In International Conference on Mobile Computing and Sustainable Informatics. EAI/Springer Innovations in Communication and Computing; Raj, J.S., Ed.; Springer: Cham, Switzerland, 2021; pp. 17–28. [Google Scholar]
- Kim, J.-Y.; Lee, Y.S.; Yu, J.; et al. Deep learning-based prediction model for breast cancer recurrence using adjuvant breast cancer cohort in tertiary cancer center registry. Front Oncol 2021, 11, 596364. [Google Scholar] [CrossRef]
- Phan, N.N.; Hsu, C.-Y.; Huang, C.-C.; et al. Prediction of breast cancer recurrence using a deep convolutional neural network without region-of-interest labeling. Front Oncol 2021, 11, 734015. [Google Scholar] [CrossRef]
- Osako, T.; Matsuura, M.; Yotsumoto, D.; et al. A prediction model for early systemic recurrence in breast cancer using a molecular diagnostic analysis of sentinel lymph nodes: A large-scale, multicenter cohort study. Cancer 2022, 128, 1913–1920. [Google Scholar] [CrossRef] [PubMed]
- Xin, L.; Wu, Q.; Zhan, C.; et al. Multicenter study of the clinicopathological features and recurrence risk prediction model of early-stage breast cancer with low-positive human epidermal growth factor receptor 2 expression in China (Chinese Society of Breast Surgery 021). Chin Med J 2022, 135, 697–706. [Google Scholar] [CrossRef] [PubMed]
- Koume, M.; Seguin, L.; Bouhnik, A.D.; Urena, R. Predicting Fear of Breast Cancer Recurrence from Healthcare Reimbursement Data using Deep Learning. In 2024 IEEE 37th International Symposium on Computer-Based Medical Systems (CBMS) (pp. 57–60). IEEE.
- Mazo, C.; Aura, C.; Rahman, A.; Gallagher, W.M.; Mooney, C. Application of artificial intelligence techniques to predict risk of recurrence of breast cancer: A systematic review. Journal of Personalized Medicine. 2022, 12, 1496. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, N.; Zhong, L.; Wang, S.; Zheng, Y.; Yang, B.; Zhang, J.; Lin, Y.; Wang, Z. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: A systematic review and meta-analysis of 282,203 patients. Molecular psychiatry. 2020, 25, 3186–3197. [Google Scholar] [CrossRef]
- Yang, Y.; Sun, H.; Luo, X.; Li, W.; Yang, F.; Xu, W.; Ding, K.; Zhou, J.; Liu, W.; Garg, S.; Jackson, T. Network connectivity between fear of cancer recurrence, anxiety, and depression in breast cancer patients. Journal of affective disorders. 2022, 309, 358–367. [Google Scholar] [CrossRef]
- Lopes, C.; Lopes-Conceição, L.; Fontes, F.; Ferreira, A.; Pereira, S.; Lunet, N.; Araújo, N. Prevalence and persistence of anxiety and depression over five years since breast cancer diagnosis—The NEON-BC prospective study. Current oncology. 2022, 29, 2141–2153. [Google Scholar] [CrossRef]
- Maheu, C.; Singh, M.; Tock, W.L.; Eyrenci, A.; Galica, J.; Hébert, M.; Frati, F.; Estapé, T. Fear of cancer recurrence, health anxiety, worry, and uncertainty: A scoping review about their conceptualization and measurement within breast cancer survivorship research. Frontiers in psychology. 2021, 12, 644932. [Google Scholar] [CrossRef]
- Lyu, M.M.; Siah, R.C.; Lam, A.S.; Cheng, K.K. The effect of psychological interventions on fear of cancer recurrence in breast cancer survivors: A systematic review and meta-analysis. Journal of Advanced Nursing. 2022, 78, 3069–3082. [Google Scholar] [CrossRef]
- Oh, H.M.; Son, C.G. The risk of psychological stress on cancer recurrence: A systematic review. Cancers. 2021, 13, 5816. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.; Dunn, L.B.; Phoenix, B.; Paul, S.M.; Hamolsky, D.; Levine, J.D.; Miaskowski, C. Co-occurrence of anxiety and depressive symptoms following breast cancer surgery and its impact on quality of life. European Journal of Oncology Nursing. 2016, 20, 97–105. [Google Scholar] [CrossRef]
- McGinty, H.L.; Small, B.J.; Laronga, C.; Jacobsen, P.B. Predictors and patterns of fear of cancer recurrence in breast cancer survivors. Health Psychology. 2016, 35, 1. [Google Scholar] [CrossRef] [PubMed]
- Enewold, L.; Parsons, H.; Zhao, L.; Bott, D.; Rivera, D.R.; Barrett, M.J.; Virnig, B.A.; Warren, J.L. Updated overview of the SEER-Medicare data: Enhanced content and applications. JNCI Monographs. 2020, 2020, 3–13. [Google Scholar]
- Sarfati, D.; Gurney, J.; Stanley, J.; Salmond, C.; Crampton, P.; Dennett, E.; Koea, J.; Pearce, N. Cancer-specific administrative data–based comorbidity indices provided valid alternative to Charlson and National Cancer Institute Indices. J. Clinical Epidemiology. 2014, 67, 586–595. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Barner, J.C.; Moczygemba, L.R.; Rascati, K.L.; Park, C.; Kodali, D. Comparing survival outcomes between neoadjuvant and adjuvant chemotherapy within breast cancer subtypes and stages among older women: A SEER-Medicare analysis. Breast Cancer. 2023, 01441-w. [Google Scholar] [CrossRef]
- Du, X.L.; Osborne, C.; Goodwin, J.S. Population-based assessment of hospitalizations for toxicity from chemotherapy in older women with breast cancer. J. Clinical Oncology. 2002, 20, 4636–4642. [Google Scholar] [CrossRef]
- Russo, A.; Autelitano, M.; Bisanti, L. Re: Frequency and cost of chemotherapy-related serious adverse effects in a population sample of women with breast cancer. J. National Cancer Institute. 2006, 98, 1826–1827. [Google Scholar] [CrossRef]
- Hassett, M.J.; O'Malley, A.J.; Pakes, J.R.; Newhouse, J.P.; Earle, C.C. Frequency and cost of chemotherapy-related serious adverse effects in a population sample of women with breast cancer. J. National Cancer Institute. 2006, 98, 1108–1117. [Google Scholar] [CrossRef]
- Rashid, N.; Koh, H.A.; Baca, H.C.; Li, Z.; Malecha, S.; Abidoye, O.; Masaquel, A. Clinical impact of chemotherapy-related adverse events in patients with metastatic breast cancer in an integrated health care system. J. Managed Care & Specialty Pharmacy. 2015, 21, 863–871. [Google Scholar]
- Groenvold, M.; Petersen, M.A.; Idler, E.; Bjorner, J.B.; Fayers, P.M.; Mouridsen, H.T. Psychological distress and fatigue predicted recurrence and survival in primary breast cancer patients. Breast Cancer Res Treat. 2007, 105, 209–219. [Google Scholar] [CrossRef] [PubMed]
- Adam, N.; Wieder, R. AI Survival Prediction Modeling: The Importance of Considering Treatments and Changes in Health Status Over Time. Cancers. 2024, 16, 3527. [Google Scholar] [CrossRef] [PubMed]
- Adam, N.; Wieder, R. Predictive Modeling of Long-Term Survivors with Stage IV Breast Cancer Using the SEER-Medicare Dataset. Cancers. 2024, 16, 4033. [Google Scholar] [CrossRef] [PubMed]
- Snoek, J.; Larochelle, H.; Adams, R.P. Practical bayesian optimization of machine learning algorithms. Advances in neural information processing systems. 2012, 25. [Google Scholar]
- Kvamme, H.; Borgan, Ø.; Scheel, I. Time-to-event prediction with neural networks and Cox regression. Journal of Machine Learning Research. 2019, 20, 1–30. [Google Scholar]
- Mucaki, E.J.; Baranova, K.; Pham, H.Q.; Rezaeian, I.; Angelov, D.; Ngom, A.; Rueda, L.; Rogan, P.K. the Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) Study by Biochemically-inspired Machine Learning [version 3; referees: 2.
- Connors, A.F.; Dawson, N.V.; Desbiens, N.A.; Fulkerson, W.J.; Goldman, L.; Knaus, W.A.; Lynn, J.; Oye, R.K.; Bergner, M.; Damiano, A.; Hakim, R. A controlled trial to improve care for seriously iII hospitalized patients: The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). JAMA 1995, 274, 1591–1598. [Google Scholar] [CrossRef]
- WPBC Breast Cancer Wisconsin (Prognostic) Data Set," archive.ics.uci.edu. Available online: https://archive.ics.uci.edu/.
- Pati, A.; Panigrahi, A.; Parhi, M.; Giri, J.; Qin, H.; Mallik, S.; Pattanayak, S.R.; Agrawal, U.K. Performance assessment of hybrid machine learning approaches for breast cancer and recurrence prediction. PLoS ONE. 2024, 19, e0304768. [Google Scholar] [CrossRef]
- Yang, Y.; Sun, H.; Luo, X.; Li, W.; Yang, F.; Xu, W.; Ding, K.; Zhou, J.; Liu, W.; Garg, S.; Jackson, T. Network connectivity between fear of cancer recurrence, anxiety, and depression in breast cancer patients. Journal of affective disorders. 2022, 309, 358–367. [Google Scholar] [CrossRef]
- Lavingia, R.; Jones, K.; Asghar-Ali, A.A. A systematic review of barriers faced by older adults in seeking and accessing mental health care. Journal of Psychiatric Practice 2020, 26, 367–382. [Google Scholar] [CrossRef]
- Noyes, K.; Liu, H.; Lyness, J.M.; Friedman, B. Medicare beneficiaries with depression: Comparing diagnoses in claims data with the results of screening. Psychiatr Serv. 2011, 62, 1159–1166. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.; Jayadevappa, R.; Zee, J.; Zivin, K.; Bogner, H.R.; Raue, P.J.; Bruce, M.L.; Reynolds CF3rd Gallo, J.J. Concordance Between Clinical Diagnosis and Medicare Claims of Depression Among Older Primary Care Patients. Am J Geriatr Psychiatry. 2015, 23, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Hassett, M.J.; Ritzwoller, D.P.; Taback, N.; Carroll, N.; Cronin, A.M.; Ting, G.V.; Schrag, D.; Warren, J.L.; Hornbrook, M.C.; Weeks, J.C. Validating billing/encounter codes as indicators of lung, colorectal, breast, and prostate cancer recurrence using 2 large contemporary cohorts. Med Care. 2014, 52, e65–e73. [Google Scholar] [CrossRef] [PubMed]
- Warren, J.L.; Mariotto, A.; Melbert, D.; Schrag, D.; Doria-Rose, P.; Penson, D.; Yabroff, K.R. Sensitivity of Medicare Claims to Identify Cancer Recurrence in Elderly Colorectal and Breast Cancer Patients. Med Care. 2016, 54, e47–e54. [Google Scholar] [CrossRef]
Figure 2.
Hypothetical patient predicted recurrence-free survival curves for 12 random scenarios from Stage I W/ER+PR+ or AA/ER-PR- categories and Stage III W/ER+PR+ or AA/ER-PR- categories withour or with anxiety/depression. No patient details are provided; our DUA with the NCI SEER-Medicare does not allow us to include specific patient identifying information.
Figure 2.
Hypothetical patient predicted recurrence-free survival curves for 12 random scenarios from Stage I W/ER+PR+ or AA/ER-PR- categories and Stage III W/ER+PR+ or AA/ER-PR- categories withour or with anxiety/depression. No patient details are provided; our DUA with the NCI SEER-Medicare does not allow us to include specific patient identifying information.
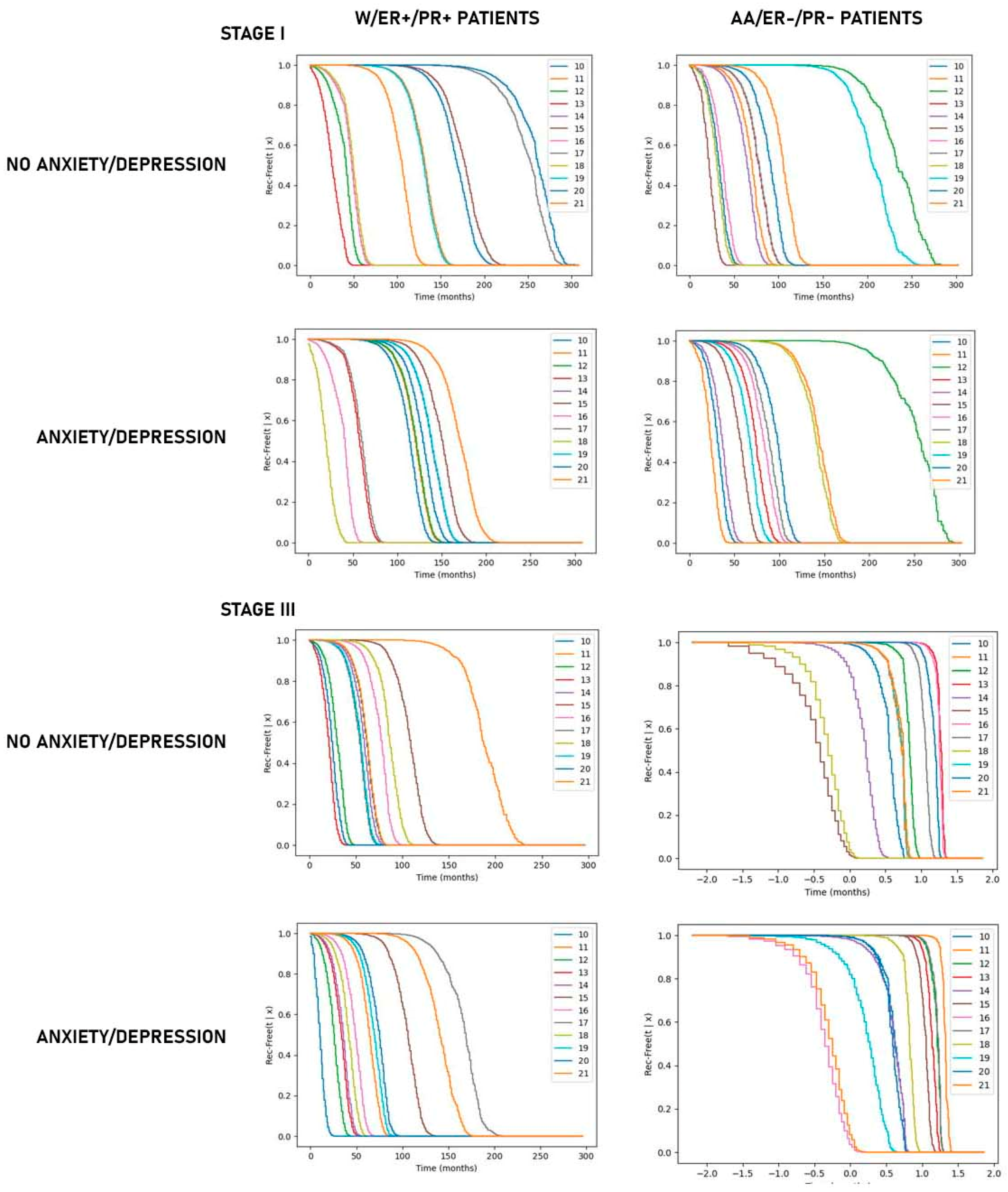

Table 1.
Algorithm 1: Patient's Recurrence.
| Algorithm 1: ALGORITHM TO INFER PATIENT'S RECURRENCE | |||||
|---|---|---|---|---|---|
|
Input:Window_after_completion_of_adjuvant_therapy=4 Month 2nd_Mal_Neop_BC_dx=19881 SRG=["8511","8512","850","8519","8520","8521","8522","8523","8525","8591","860d1", "8533","8534", "8535","8536","4022","4023","4029","403","4050","4051","8541","8542","8543","8544","8545","8546","8547","8548] PR=["9221","9222","9223","9224","9225","9226","9227","9228","9229","9230","9231","9232","9233","9239","9241"] TR=["G9829","1","2","3","4","5","6","7","8","9","10","11","12","13","14","15","16","17","18","19","20", "21","22", "23","24","25","26","27","28","29","30","31","32","33","34","35","36","37","38","39","40","41","42","43","44","45","46"] |
|||||
|
Output:For Each Patient: Infer her/his Rec_flag and the corresponding Rec_Date |
|||||
|
1 2 |
Initialization: New_Chem_Hor_Bio_Rad_List=[], Mal_Neop_List=[], New_Contralat_List=[], No_Rec_Date←“2050-01-01” |
||||
| 3 | For Each Patient | ||||
|
4 5 6 7 8 9 10 |
Rec_flag← 0, Rec_Date← No_Rec_Date Identify: Date_1st_Chem, Date_1st Hor, Date_1st Bio, Date_1st Rad, Date_1st_Sur, Date_1st_Course_Tr Date_Init_Adj_Therapy←Max{Date_1st_Chem, Date_1st Hor, Date_1st Bio, Date_1st Rad, Date_1st_Sur, Date_1st_Course_Tr } Order visits in ascending order of Visit_Date |
||||
| 11 | For Each Visit | ||||
| 12 | For Each Entry within this Visit | ||||
|
13 14 |
If ( (Visit_Date-Date_Init_Adj_Therapy) >=4mon) And (Sur OR Bio OR Hor OR Rad) |
||||
| 15 | Rec_flag← 1 | ||||
|
16 17 |
Rec_Date ← VisitDate Break |
||||
| 18 | If (Rec_flag = 1) | ||||
|
19 20 21 |
Append this Patient to New_Chem_Hor_Bio_Rad_List Rec_flag ← 0, Rec_Date ← No_Rec_Date |
||||
| 22 | For Each Visit | ||||
| 23 | For Each Entry within this Visit | ||||
| 24 | If (dx_code=2nd_Mal_Neop_BC_dx) | ||||
| 25 | Rec_flag← 1 | ||||
| 26 | If ( (Rec_flag =1 & (Visit_Date < Rec_Date) ) | ||||
| 27 | Rec_Date← Visit_Date | ||||
| 28 | If (Rec_flag = 1) | ||||
|
29 30 31 |
Append this Patient to Mal_Neop_List Rec_flag ← 0, Rec_Date ← No_Rec_Date |
||||
| 32 | For Each of the Ten Recorded Diagnoses | ||||
| 33 | If Diagnosis =1 | ||||
|
34 35 36 |
Prev_Laterality=Current_Laterality Rec_flag← 0 Date_of_Prev_diagnosis ← No_Rec_Date |
||||
|
37 38 |
If ( ((Current_Laterality).isin(2,4,5,9)) & (Prev_Laterality)=1)) OR ((Current_Laterality).isin(1,4,5,9)) & (Prev_Laterality)=2)) ) |
||||
|
39 40 |
Rec_flag1← 1 If (Date_of_this_Diagnosis < Date_of_Prev_Diagnosis) |
||||
| 41 | Rec_Date← Date_of_this_Diagnosis | ||||
| 42 | Date_of_Prev_Diagnosis← Date_of_this_Diagnosis | ||||
| 43 | If (Rec_flag = 1) | ||||
|
44 45 46 |
Append this Patient to New_Contralat_List Rec_flag← 0, Rec_Date← No_Rec_Date |
||||
| 47 | If (patient isin New_Chem_Hor_Bio_Rad_List OR isin Mal_Neop_List OR isin New_Contralat_List)) | ||||
|
48 49 50 |
Rec_flag← 0, Rec_Date← Min{Patient’s Rec_Date in New_Chem_Hor_Bio_Rad_List, Patient’s Rec_Date in Mal_Neop_List, Patient’s Rec_Date in New_Contralat_List} |
||||
Table 2.
Patient characteristics – all patients and patient subgroup with anxiety/depression.
| All Patients | All patients with Anxiety/Depression | |||||||
|---|---|---|---|---|---|---|---|---|
| Number (%) | Age + SD | Comorbidity at Dx + SD | Number (%) | p (chi sq) | Age + SD | Comorbidity at Dx + SD | Mos, Dx-Dep/anx Avg+ SD |
|
| Total Patients | 239,288 (100) | 75.2 + 7.2 | 0.6 + 1.5 | 86,745 (100) (36.3% of all) | 75.4 + 7.0 | 0.7 + 1.7 | 31.4 + 48.0 | |
| ER+/PR+ | 154,730 (64.7) | 75.1 + 7.1 | 0.7 + 1.5 | 55,681 (64.2) | n.s. | 75.3 + 7.0 | 0.8 + 1.7 | 29.9 + 46.6 |
| ER+/PR- | 29,278 (12.2) | 75.6 + 7.3 | 0.6 + 1.5 | 10,775 (12.4) | 75.7 + 7.1 | 0.7 + 1.6 | 31.8 + 47.6 | |
| ER-/PR- | 32,400 (13.5) | 74.8 + 7.2 | 0.6 + 1.5 | 11,505 (13.3) | 75.0 + 7.1 | 0.7 + 1.7 | 28.3 + 46.3 | |
| Stage I | 134,598 (56.2) | 74.7 + 6.8 | 0.6 + 1.4 | 49,628 (57.2) | n.s. | 75.0 + 6.7 | 0.7 + 1.6 | 34.5 + 50.2 |
| Stage II | 76,928 (32.1) | 75.8 + 7.6 | 0.7 + 1.6 | 28,098 (32.4) | 76.0 + 7.4 | 0.8 + 1.8 | 28.8 + 46.0 | |
| Stage III | 27,762 (11.6) | 76.0 + 7.7 | 0.6 + 1.6 | 9,019 (10.4) | 76.1 + 7.5 | 0.8 + 1.7 | 22.8 + 39.8 | |
| Race–W | 210,108 (87.8) | 75.3 + 7.2 | 0.6 + 1.5 | 79,239 (91.3) | p = 0 | 75.5 + 7.0 | 0.7 + 1.6 | 31.7 + 48.2 |
| Race–AA | 16,887 (7.1) | 74.8 + 7.2 | 0.8 + 1.7 | 4,781 (5.5) | 75.3 + 7.2 | 1.0 + 2.0 | 27.4 + 44.4 | |
| Race–Other | 12,293 (5.1) | 73.7 + 6.7 | 0.7 + 1.5 | 2,725 (3.1) | 74.2 + 6.6 | 0.9 + 1.8 | 31.3 + 48.3 | |
| Hispanic | 12,603 (5.3) | 4,486 (5.2) | p=0 | |||||
n.s. – not significant at p=0.05.
Table 3.
Non-recurrent and recurrent patients.
| Non-Recurrent Patients | Recurrent Patients | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Number (%) | Age + SD | Comorb. at Dx + SD | Number (%) | p (chi sq.) | Age + SD | Comorb. at Dx + SD | Mos, Dx-Recr + SD | Comorb. at recur. + SD | |
| Total Patients | 202,339 (100) (84.6% of all) | 75.2 + 7.2 | 0.6 + 1.5 | 36,949 (100) (15.4% of all) | 74.6 + 6.9 | 0.5 + 1.4 | 37.5 + 44.6 | 2.9 + 3.5 | |
| ER+/PR+ | 133,560 (66.0) | 75.2 + 7.2 | 0.7 + 1.6 | 21,170 (57.3) | p = 0 | 74.5 + 6.8 | 0.6 + 1.4 | 39.7 + 45.6 | 3.2 + 3.5 |
| ER+/PR- | 24,280 (12.0) | 75.7 + 7.3 | 0.6 + 1.5 | 4,998 (13.5) | 75.0 + 7.0 | 0.5 + 1.4 | 36.2 + 41.5 | 3.0 + 3.5 | |
| ER-/PR- | 25,762 (12.7) | 74.9 + 7.3 | 0.6 + 1.5 | 6,638 (18.0) | 74.2 + 6.8 | 0.5 + 1.3 | 28.6 + 37.6 | 2.6 + 3.3 | |
| Stage I | 120,231 (59.4) | 74.7 + 6.8 | 0.6 + 1.4 | 14,367 (38.9) | p = 0 | 74.4 + 6.6 | 0.5 + 1.4 | 46.0 + 50.3 | 3.3 + 3.6 |
| Stage II | 63,363 (31.3) | 76.0 + 7.6 | 0.7 + 1.6 | 13,565 (36.7) | 74.6 + 7.0 | 0.5 + 1.4 | 36.1 + 42.9 | 2.9 + 3.5 | |
| Stage III | 18,745 (9.3) | 76.6 + 7.9 | 0.6 + 1.5 | 9,017 (24.4) | 74.7 + 7.1 | 0.5 + 1.3 | 26.2 + 33.6 | 2.3 + 3.3 | |
| Race–W | 177,554 (87.8) | 75.4 + 7.3 | 0.6 + 1.5 | 32,554 (88.1) | p = 0 | 74.7 + 6.9 | 0.5 + 1.3 | 38.4 + 45.3 | 2.9 + 3.5 |
| Race–AA | 14,189 (7.0) | 74.9 + 7.3 | 0.9 + 1.8 | 2,698 (7.3) | 73.9 + 6.9 | 0.5 + 1.4 | 28.6 + 35.8 | 2.9 + 3.6 | |
| Race–Other | 10,596 (5.2) | 73.8 + 6.7 | 0.0 + 0.3 | 1,697 (4.6) | 73.1 + 6.5 | 0.6 + 1.4 | 35.3 + 43.0 | 3.1 + 3.4 | |
| Hispanic | 10,789 (5.3) | 1,814 (4.9) | p = 0 | ||||||
Table 4.
Recurrent patients - Impact of anxiety/depression on recurrence.
| Recurrent patients without anxiety/depression | Recurrent patients with anxiety/depression | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number (%) | Age + SD | Mos, Dx- Recr + (SD) | Comorb. at recur. + SD | Number (%) | p (chi sq.) | Age + SD | Mos, Dx-Recr + (SD) p (t-test) |
Comorb.at recur. + SD p (t-test) |
Mos, Dx-Dep /Anx + SD |
|
| Tot. Pts. |
21,412 (100) 14.0% of pts. without anx/dep | 74.5 + 7.0 | 36.3 + 43.6 | 2.4 + 3.1 | 15,537 (100) 17.9% of pts with anx/dep | p= 0 | 74.6 + 6.7 | 39.3 + 46.0 p=0 |
3.6 + 3.8 p=0 |
32.9 + 48.8 |
| ER+/PR+ | 12,101 (56.5) | 74.5 + 7.0 | 38.6 + 44.8 | 2.7 + 3.2 | 9,069 (58.4) | p=0 | 746 + 6.7 | 41.1 + 46.6 p=0 |
3.9 + 3.9 p=0 |
32.7 + 48.0 |
| ER+/PR- | 2,875 (13.4) | 75.1 + 7.1 | 34.9 + 40.1 | 2.5 + 3.1 | 2,123 (13.7) | 74.9 + 7.0 | 38.0 + 43.2 p=0.009 |
3.7 + 3.8 p= |
32.4 + 48.2 | |
| ER-/PR- | 3,976 (18.6) | 74.0 + 6.9 | 27.9 + 37.2 | 2.0 + 2.9 | 2,662 (17.1) | 74.4 + 6.8 | 29.8 + 38.3 p=0.044 |
3.3 + 3.7 p=0 |
25.6 + 42.6 | |
| Stage I | 7,900 (36.9) | 74.4 + 6.7 | 44.6 + 49.4 | 2.8 + 3.2 | 6,467 (41.6) | p=0 | 74.4 + 6.5 | 47.8 + 51.3 p=0 |
3.9.+ 3.9 p=0 |
38.0 + 53.1 |
| Stage II | 7,737 (36.1) | 74.6 + 7.1 | 36.0 + 42.5 | 2.4 + 3.1 | 5,828 (37.5) | 74.7 + 6.9 | 36.2 + 43.3 n.s. |
3.6 + 3.8 p=0 |
32.0 + 48.8 | |
| Stage III | 5,775 (27.0) | 74.6 + 7.2 | 25.3 + 32.8 | 1.8 + 2.8 | 3,242 (20.9) | 74.9 + 7.0 | 27.7 + 34.9 p=0.001 |
3.2 + 3.7 p=0 |
24.3 + 38.8 | |
| Race–W | 18,399 (85.9) | 74.7 + 7.0 | 37.3 + 44.4 | 2.4 + 3.1 | 14,155 (91.1) | p=0 | 74.7 + 6.8 | 39.9 + 46.4 p=0 |
3.6 + 3.8 p=0 |
32.9 + 48.8 |
| Race–AA | 1,799 (8.4) | 73.8 + 7.0 | 27.8 + 35.6 | 2.4 + 3.2 | 899 (5.8) | 74.2 + 6.7 | 30.2 + 36.1 n.s. |
3.9.+ 4.0 p=0 |
30.6 + 46.5 | |
| Race–Oth | 1,214 (5.7) | 73.0 + 6.5 | 34.0 + 41.4 | 2.8 + 3.2 | 583 (3.1) | 73.5 + 6.4 | 38.4 + 46.8 p=0.044 |
3.8 + 3.8 p=0 |
35.9 + 51.9 | |
| Hispanic | 957 (4.5) | 857 (5.5) | p=0 | |||||||
n.s.= not significant.
Table 5.
Concordance indices.
| Model | ER+/PR+ | ER-PR- | ||
|---|---|---|---|---|
| Time-dependent Concordance (C-Index) Avg. + SD | Integrated Brier Score (IBS) Avg. + SD | Time-dependent Concordance (C-Index) Avg. + SD | Integrated Brier Score (IBS) Avg. + SD | |
| Stage I | ||||
| CoxTime | 0.989 + 0.001 | 0.031 + 0.007 | 0.983 + 0.001 | 0.028 + 0.007 |
| DeepHit | 0.983 + 0.001 | 0.036 + 0.003 | 0.972 + 0.004 | 0.018 + 0.004 |
| DeepSurv | 0.987 + 0.001 | 0.027 + 0.001 | 0.984 + 0.001 | 0.024 + 0.001 |
|
Nnet-Survival (Logistic Hazard) |
0.982 + 0.001 | 0.026 + 0.001 | 0.969 + 0.001 | 0.055 + 0.002 |
| Stage II | ||||
| CoxTime | 0.981 + 0.001 | 0.056 + 0.022 | 0.972 + 0.001 | 0.055 + 0.018 |
| DeepHit | 0.981 + 0.001 | 0.009 + 0.001 | 0.970 + 0.001 | 0.021 + 0.002 |
| DeepSurv | 0.970 + 0.001 | 0.052 + 0.002 | 0.967 + 0.006 | 0.035 + 0.006 |
|
Nnet-Survival (Logistic Hazard) |
0.982 + 0.001 | 0.026 + 0.001 | 0.966 + 0.001 | 0.045 + 0.003 |
| Stage III | ||||
| CoxTime | 0.968 + 0.001 | 0.024 + 0.009 | 0.955 + 0.002 | 0.028 + 0.025 |
| DeepHit | 0.948 + 0.002 | 0.012 + 0.001 | 0.945 + 0.001 | 0.091 + 0.002 |
| DeepSurv | 0.972 + 0.002 | 0.019 + 0.001 | 0.961 + 0.001 | 0.021 + 0.001 |
|
Nnet-Survival (Logistic Hazard) |
0.965 + 0.002 | 0.039 + 0.002 | 0.928 + 0.003 | 0.030 + 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



