
Submitted:
31 March 2025
Posted:
01 April 2025
You are already at the latest version
Abstract
There are many clinical reasons for tooth extraction due to caries, periodontal disease, trauma, infection or the need to gain space due to orthodontic treatment. This study aimed to radiographically evaluate the preservation of the dental alveolus using platelet-rich fibrin. A total of 17 alveoli without PRF and 19 alveoli with PRF were analyzed, with an initial cephalocaudal height of 10.5 mm in both groups. The dimensional changes of the crest were evaluated using cone beam computed tomography (CBCT) images acquired 30 and 120 days post-extraction. In the cephalocaudal height at 120 days, a difference of 0.99 mm was identified in the alveolar height of both groups. The group with PRF had a greater height reaching an average of 10.30 mm, regarding to the depth measured at 1 mm, 3 mm and 5 mm, no significant differences were identified between both groups at 30 and 120 days, however, it is highlighted that those alveoli with PRF presented a lower bone loss in depth (1,3,5 mm) of 8.06mm, 8.45mm and 9.04mm. PRF filling effectivily preserves the dimensions of the alveolar crest in height, depth and bone tissue quality following extraction.
Keywords:
bone regeneration
; tooth socket
; oral surgery
; platelet-rich fibrin
; CBCT imaging
1. Introduction
There are many clinical reasons for tooth extraction, caries, periodontal disease, trauma, infection or orthodontic treatment.[1] This results in alveolar atrophy in both the horizontal and vertical dimensions due to a combination of soft and hard tissue changes [2]. Tissue resorption is more prominent in the buccal than in the lingual/palatal wall because the buccal bone wall is thinner and the crestal part of the buccal bone is mainly occupied by compact bone, unlike the moderate changes in bone height is approximately 11 to 22% mm, the horizontal reduction approximately 3-4 mm can reach up to 60% of the initial width of the alveolar crest, also the non-molar sites were evaluated clinically with a reduction of 2.7 mm, with respect to the radiographic part is 2.5 mm and 1.7 mm respectively, approximately two thirds of this reduction occurred in the first 3 months after tooth extraction.[3,4]
For this reason in the seventies, Matras et al. described the use of fibrin glue to improve the healing of cutaneous wounds in a rat model[5]. Subsequently, improved versions such as “platelet-fibrinogen-thrombin mixture” and “platelet gelatin foam” were introduced, which offered higher platelet concentrations. Platelet-rich plasma (PRP) was introduced by Marx and Whitman in the late 20th century. Its high concentration of platelets, platelet-derived growth factor (PDGF), transforming growth factor-β (TGF-β) and vascular endothelial growth factor (VEGF) make it a viable material to enhance bone regeneration as an adjunct to bone grafts as well as alveolar wound healing. However, the clinical use of PRP has been limited by its arduous handling, rapid polymerization, and the potential for a host reaction to bovine thrombin[6].
2. Materials and Methods
Experimental study: Single-blind randomized controlled clinical trial of two groups of patients (experimental and control) with the application of PRF.
Analytical study: Identification of the degree of bone regeneration after extraction of the alveoli treated with and without PRF by means of CBCT.
Study universe and patient selection
For the selection of the sample for this study, the G*Power formula, “F” tests, with an ANOVA analysis of repeated measures and an inter-subject determination were used; identifying a total sample size of 36 patient alveoli (17 and 19 per group) with an effect size of 0.25, error of 5% and a confidence of 95%.
Inclusion Criteria
For this study, 10 systematically healthy subjects, between 17 and 38 years old, were selected, who, due to orthodontic indication, require extraction of premolars, two maxillary or two mandibular.
In addition, they could be planning orthognathic surgery, extraction of retained teeth suggesting impaction or third molars that show signs of relationship with the CDI, or any other situation that made it necessary to evaluate available bone tissue or critical anatomy. In general, subjects in which the performance of a CBCT was justified over other imaging routine.
Excluded criteria
Patients with current or past systemic disease that could alter the results of periodontal therapy, as well as patients with insufficient platelet count (less than 200,000 mm3), immunosuppressed patients, pregnancy, lactation and smoking. In addition, patients taking medications interfering with healing were excluded from this study.
The Epidat Info program was used to randomize the alveoli selection , which randomizes the sample:
Experimental group: application of PRF in alveoli after premolar extraction.
Control group: physiological healing of the alveoli after premolar extraction.
A written informed consent was provided with the advantages, disadvantages and objectives of the study. A periodontal clinical record was also filled out to identify the patient's clinical conditions.
PRF preparation
PRF is performed according to the protocol developed and patented by [7], using a PRF Duo centrifuge (Nice, France) and the respective surgical kit. PRF is prepared without biochemical manipulation of the blood. Prior to surgery, after venipuncture, 10 ml of blood was extracted from the antecubital vein, for each alveolus to be treated with biomaterial. The blood was placed in two sterile glass test tubes without additives (10 ml) provided in the kit. Immediately after the sample was taken, the tubes were centrifuged for 12 minutes at 2,700 rpm. The cap was removed from each tube, placed in the tube holder and kept untouched for 5 minutes. The central PRF clot extracted from one tube was taken as a filler. The specific surgical box was used for its manipulation. The PRF clot from the homologous tube was used as a guided tissue regeneration membrane. One clot was placed in the specific container of the surgical box to form the plug of the alveolus, the second clot was placed in the specific base of the surgical box for membrane formation.
Surgical procedure
Both experimental and control sites of the same patient were treated in the same surgical phase. After local anesthesia, an intrasulcular incision was made with a No. 15 scalpel and then the maxillary or mandibular premolars were extracted using an atraumatic technique, according to the patient's orthodontic indication. In the control sites, extractions were performed allowing physiological healing, while in the experimental sites, autologous PRF was placed. Fibrin was partially distributed within the alveolus and, additionally, it was applied as a guided tissue regeneration membrane. To ensure its adequate retention and prevent displacement, 3.0 catgut sutures were used in the alveolar margins, using simple stitches.
The surgical procedures at the test and control sites differed only in the treatment with PRF.
The multidisciplinary team, maxillofacial surgeon, periodontists and maxillofacial imaging specialist performed all the surgeries and the corresponding clinical measurements according to the established protocol.
Postoperative care
Sutures were removed seven days after surgery. Patients were clinically examined 3, 7 and 14 days after surgery, with no changes.
Postoperative measurements
Immediately after tooth extractions, CBCTs were performed using SIRONA equipment. These were repeated 30 and 120 days later, considering the same technical and radiation protection parameters.
All acquisitions were performed with a FOV of 8 x 8 cm. Voxel size of 0.2 mm. Exposure parameters were 16 seconds, 30.89 mAs and 120 kVp.
Reconstruction, visualization and measurement were performed with Sidexis 4.0 software and analyses by a maxillofacial imager external to the ECA.
Post-surgical measurement points
Using the method proposed by [8], the measurement of each empty alveolus was performed in height (cephalic – caudal) and vestibule – palatal depth.
Depth of the vestibular and palatal/lingual bone plates
The total thickness of the alveolus was measured from the vestibular to the palatal bone plate divided into three points, located at 1, 3 and 5 mm below the highest point of the vestibular cortex, perpendicular to the vertical reference line, located in the center of the alveolus from the bottom to the bone cortex (caudal or cephalic), according to the maxilla or mandible (Figure 1).
The width of the alveolus was measured at 1.3 and 5 mm from the vestibular and palatal or lingual bone cortex, which were identified as RW - 1, RW - 3 and RW - 5 respectively in both the initial and final CBCT (Figure 2).
Alveolar process height
To identify the height, a horizontal line was drawn at the bottom of the alveolus, two lines parallel to the bone tables according to the cortex, which were called BH for the vestibular table and LH for the palatal or lingual table. Finally, a horizontal line was drawn between the aforementioned bone tables to identify the limit of the alveolar process. This procedure was performed in the initial and final CBCT.
Quality of the newly formed bone tissue
To identify the quality of bone tissue, the gray scale was used through the Hounsfield Units (HU), a CBCT tool for determining the type of bone tissue, which uses a scale from -1093 to 3000, with the bone being between 500 and 2000 according to the degree of calcification of the bone surface. The limits of the alveolus were marked by drawing a horizontal line (B1) between the apices of the adjacent teeth and another horizontal line (L1) between the cusps of the teeth mentioned above. Point A was identified at the bottom of the alveolus, using line B1 and point B, located 4 mm from B1, as a base, for which a vertical line was identified in the middle area of the alveolus between the limits determined by lines B1 and L1, identification carried out according to the method proposed by [9].
Post-surgical measurements were carried out 30 and 120 days after the atraumatic extraction of the teeth, using the same parameters previously mentioned for the different visualization moments of the CBCT. The data obtained in this research were recorded in an Excel 2018 table for data collection, which includes height, depth at 1,3,5 mm and bone tissue quality in Hounsfield units, both at 30 and 120 days after PRF placement.
Data analysis
The analysis of the results was carried out in the statistical application Jasp 0.18.1.0., the results are presented using measures of central tendency and dispersion, the t-student test was performed for independent samples for comparisons between groups and the Wilcoxon test for related samples (before and after). Additionally, to establish the effect between groups, the ANOVA RM test was applied.
3. Results
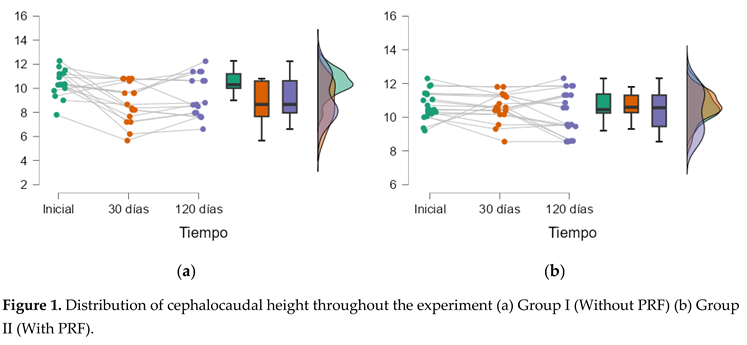
At the beginning of the experiment, the cephalocaudal height of the alveoli of both groups was approximately 10.5 mm, with no significant differences (p<0.05), which made the experiment feasible. 30 days after the extraction of the pieces, a significant difference (p <0.05) was identified between both groups; Group II (Alveolus with PRF) measured 1.79 mm more than Group I (Alveolus without PRF). On the other hand, at 120 days, a difference of 0.99 mm was identified in the height of the alveoli of both groups, however, it was not significant. Group II exhibited the greatest height, averaging 10.30 mm. Regarding the depth measured at 1 mm, 3 mm and 5 mm, no significant differences were identified between both groups at 30 and 120 days, however, it is noted that those alveoli with PRF (Group II) had a depth (1 mm) of 8.06 mm (SD = 1.78 mm), depth (3 mm) of 8.45 mm (SD = 1.67 mm) and depth (5 mm) of 9.04 mm (SD = 1.65 m). Details in (Figure 2) (Table 1).
In order to deepen the understanding of the behavior of cephalocaudal height, in the following diagrams it can be seen that, in Group I from t = 0, a pronounced decrease was observed to 8.82 mm (SD = 1.68) on average at 30 days (SD = 1.68) and subsequently an increase to 9.31 mm (SD = 1.73) at 120 days; with a progressive increase in the dispersion of data. In Group II, with reference to t = 0, at 30 days it presented a slight decrease to 10.61 mm (SD = 0.85) and finally at 120 days a slight decrease with an average of 10.30 mm (SD = 0.96), as can be seen in the graph, the dispersion of data of similar cephalocaudal height is preserved, which implies no changes over time with respect to their means.
Intra-group tests determined significant effects only with the intervention of time and the interaction of time with group (time * group), in height and depth at 1 mm, while, in depth at 3 mm and 5 mm, statistical significance was given only in the interaction of time and group (time * group). Time alone explained the behavior of 7.4% of the response of the height of the alveolus, while the combination of time and group explained 4.6%, on the other hand, the interaction of time and group explained between 2% and 6% of the depth changes at 3 mm and 5 mm.
In the tests between groups, it was identified that the height was explained by the group membership in 12.5%, while the depths were not affected.

Table 4.
Analysis between groups.
| Variable | Analysis | Sum of squares | Degrees of freedom | Root mean square | F | p | η² |
|---|---|---|---|---|---|---|---|
| Height | Group | 27.85 | 1 | 27.850 | 9.800 | 0.004 | 0.125 |
| Residuals | 96.62 | 34 | 2.842 | ||||
| Depth 1mm | Group | 0.36 | 1 | 0.362 | 0.071 | 0.791 | 0.002 |
| Residuals | 172.50 | 34 | 5.073 | ||||
| Depth 3mm | Group | 0.47 | 1 | 0.468 | 0.107 | 0.745 | 0.003 |
| Residuals | 148.11 | 34 | 4.356 | ||||
| Depth 5mm | Group | 3.42 | 1 | 3.422 | 0.663 | 0.421 | 0.016 |
| Residuals | 175.46 | 34 | 5.161 |
Note: F= ANOVA, p= statistical significance, η²= Eta squared.
Finally, the post hoc analysis of each of the groups can be seen in Table 5. Significant differences were identified in the group without PRF (Group I) in height between the start and 30 days (-1.63 mm), as well as in depth (3 mm) from 30 to 120 days (-0.630 mm), and at 5 millimeters from 30 to 120 days (+ 0.8 mm).
In Group II (alveoli with PRF) a significant change was evident between the start and 30 days after extraction in height (-0.115 m) however, between 30 and 120 days no significant differences were evident (p > 0.05), likewise the depth at 1 mm and 3 mm evaluated, revealed significant differences of decreases of 0.968 mm and 0.933 mm respectively.
4. Discussion
The application of PRF, although showing benefits in the preservation of the alveolar ridge, seems to be influenced by patient-specific factors. Although the PRF membrane can promote bone regeneration in situ, by enhancing the body's natural response to bone loss after extraction, its ability to stimulate osteogenesis is limited by the quantity and variety of cytokines released. In the present RCT, when analyzing the height variable in the experimental group and comparing it with the control group at 30 days post-extraction, a statistically significant loss of 0.92 mm was observed. This reduction suggests minimal alveolar atrophy, which is favorable, consistent with studies by [10,11,12] who reported an average bone loss of 0.9 and 1.00 mm. However, these findings differ from the results obtained by [13,14,15,16] who documented a considerably greater alveolar atrophy, between 1.8- and 5.0-mm. Result variability may stem from differences in the PRF application methodology, patient characteristics and other external factors.
When analyzing the height variable at 120 days post-extraction compared to day 30, a loss of 0.84 mm was observed, which was statistically significant. This finding agrees with the study by [17] who documented statistically significant changes at 120 days, reporting a reduction of 1.80 ± 0.07 mm (p < 0.001). Similarly,[15] indicated a statistical significance in the maintenance of the alveolar process in the long term, with a loss of 1.8 ± 2.1 mm (p < 0.005). However,[18] found no significant differences in the control group at 120 days, with an average loss of only 0.10 mm when comparing the alveolus treated with and without PRF. The findings indicate that PRF can accelerate the bone healing process, promoting early mineralization that begins around day fourteen and extends to 120 days. The sustained release of growth factors associated with PRF contributes to a higher quality of the newly formed bone, while minimizing bone resorption caused by inflammatory processes inherent to masticatory processes. [16] mention that the use of PRF in general can stimulate bone regeneration in situ without waiting for a normal response from the body, however due to the minimum number of cytokines in PRF, the bone regeneration effect is limited and cannot maintain the shape of the alveolar crest after extraction, without generating significant statistics at 1, 2, 4, 6 and 8 weeks, finding a difference between the control and experimental groups of 0.63 mm; while in the RCT applied in this research it yields different results in which an effect of the time variable between subjects and the experimental group of 4.46% can be seen, which identifies a significant change in height of 1.04 mm between the two groups (experimental and control). Regarding the variable of the degree of bone regeneration in width at a depth of 1 mm, [12] identified a resorption in the width of the alveolar process of 0.57 mm at 120 days post-extraction, which agrees with the values obtained in this study and supports the use of PRF in preserving the width of the alveolar ridge (0.18 mm). These findings are also aligned with the observations of [19,20], who also demonstrated positive results in the preservation of the alveolar ridge by PRF. However, [21] reported a greater reduction in the width of the alveolar ridge of 1.4 mm in the same time interval, results that also agree with [22], who documented a loss of 0.9 mm, as well as with other studies [11,13,23,24]. These data suggest that although PRF promotes bone preservation, the effects on alveolar crest width may vary depending on additional factors.
The results of this investigation on the use of PRF in bone regeneration at a depth of 3 mm show a loss in the width of the alveolar ridge of between 0.89 and 0.97 mm, results consistent with the studies of [10,11,13,25] This reduction was significant when comparing the control group with the experimental group, suggesting a greater effectiveness of PRF in preserving the alveolar ridge. A possible explanation for these findings could be the ability of PRF to resist external forces, which contributes to its structural stability at the application site. In addition, the sustained release of growth factors for up to 180 days post-extraction. [26] These findings confirm the usefulness of PRF in alveolar preservation procedures and demonstrate its significant contribution in minimizing postoperative bone loss, in line with previous studies, such as those mentioned above. When evaluating bone regeneration in terms of alveolar width over time (30 and 120 days) and depth (1, 3 and 5 mm), a statistically significant decrease of 0.44 mm was observed, which is in agreement with the results of [19,20] who reported promising results in alveolar ridge preservation after single tooth extractions. [21] reported a mean reduction of 1.4 mm (23%) at 1 mm below the crest and 5.0 mm (51%) at 5 mm, in the experimental group. [22] observed an average variation between 0.9 and 2.2 mm in ridge width in the control and experimental groups respectively, at 1, 3 and 5 mm below the crest. The results of this investigation are in line with other studies, such as those of [11,13,23,24] that have also demonstrated the benefits of PRF in reducing alveolar bone loss. However, it has been identified that the results are highly dependent on the PRF application technique, as suggested by several authors [21,24]. The variability of the techniques could influence the stability of the results obtained, which highlights the need for standardization in the use of PRF for alveolar preservation.
In a study by [27] the dimensional changes of the alveolar process were evaluated four months after extraction and PRF placement, using CBCT and a method similar to that of this RCT. The results showed a decrease in the width of the alveolar process of -1.38, -0.82 and -0.43 mm at depths of 1, 3 and 5 mm, respectively. Furthermore, a 1.1% gain in bone height was observed. [28] reported a 63% gain in alveolar process height at seven months post-extraction, suggesting a similar pattern of bone regeneration. From a clinical standpoint, the most significant changes in ridge dimension after tooth extraction were observed in the height of the buccal bone plate and the width of the alveolar process at 1 mm. The findings of this investigation are consistent with these studies, showing an average height loss of -1.04 mm when comparing the control site with the experimental site. In terms of depth, the reduction was -0.44 mm at 1 mm, -1.02 mm at 3 mm, and -0.46 mm at 5 mm. This supports the use of PRF as an effective resource to preserve alveolar bone structure after tooth extraction.
Other studies by [9] that identified the height and width of the alveolar process six months after extraction and placement of PRF, showed statistically significant differences in the maintenance of the depth of the alveolus since in the experimental group (PRF) it was 1.49 mm and in the control group it was 1.85 mm, being consistent with this research. The use of PRF causes the growth factors that remain at the highest point for up to fourteen days to help the cells differentiate more quickly and generate new bone, leading to less alveolar atrophy. After this period these factors begin to decrease rapidly, thus decreasing the formation of bone tissue.
The mineral density of bone tissue identifies the biological activity of osteoblasts; therefore, today the use of CBCT based on the gray scale (Hounsfield Units) helps to assess this parameter; However, for the evaluation of bone density using this method, calibration of the equipment is necessary before its application, which is a limitation in its use [29].
According to this parameter, it has been reported that the correlation of bone quality using Uh is stronger in the absence of bone grafts, especially xenograft, which decreases the capacity of CBCT to identify bone density, [30] however, in this research the material is resorbable without affecting the assessment of bone density.
Regarding the variable quality (density) of the newly formed bone tissue evaluated by Uh through CBCT studies carried out by [11,13,31,32] identified that the healing of the bone tissue had a better score on the experimental side with density values of 163.9 Uh compared to the control side of 159.3 Uh with a statistical significance of p = 0.015, evaluated at 30 days post-extraction, being consistent with the results obtained in this investigation where the authors obtained a bone quality between 190 to 282 Uh, being a possible response to this result since the PRF being a biomaterial obtained from the same patient, the platelets and white blood cells are trapped in a three-dimensional fibrin structure and slowly release several growth factors, favoring the gradual formation of new blood vessels, regulating the immune system, capturing circulating stem cells and helping bone regeneration [33].
[34] investigated how growth factors present in PRF, such as PDGF and TGF-β, contribute to bone regeneration; their studies showed that PRF, having a high concentration of these factors, favors the activity of osteoblasts, promoting the regeneration and healing of bone tissue, through proliferation, differentiation and formation of bone tissue.
Several studies have demonstrated the usefulness of CBCT to identify the degree of bone regeneration through PRF in established periods of time and with appropriate methods such as in the identification of the degree of bone mineralization;[35] in an in vitro study they investigated the mean value of the Uh of the CBCT, according to their evaluation the bone density of the jaws presents a positive correlation between the parameters mentioned above, especially in the edentulous regions where there is no other recognizable hyperdense structure except the cancellous bone. This justifies the possibility of using Uh in the maxillary bones; According to this parameter used in this research, the quality of the bone tissue is greatly improved from day 30 to 120 with a wide intraclass correlation of 0.75. In agreement with the studies of [9] who evaluated six months post-extraction and placement of PRF showing statistically significant differences (p = 0.0097) in the values of the Uh being higher for the experimental group (PRF) with a value of 308.16 ± 128.51, while in the control group (without PRF) of 279.4 ± 136.23: as in other studies, [36,37,38,39,40] justifying the reason for this result since the PRF by containing active growth factors at the beginning of healing, allows the formation of bone structures, as well as the rapid mineralization of bone tissue, being important the maintenance of growth factors in the alveolus for a long time to improve bone quality.
In this investigation, the correlation between the variables of height and depth at 30 days showed a strong relationship (rs=0.83), which is in agreement with the findings of [19,41]. who also observed a strong correlation between these dimensions after the application of PRF. These authors concluded that PRF is effective in maintaining the alveolar ridge, conserving both height and depth over time. However, other studies, such as those of [15,16,42]. did not find a significant relationship between height and depth, since their findings indicate that, although PRF contributes to preserving the width of the alveolar ridge, the same effect is not always achieved in height, which is significantly reduced in some cases.
The correlation between the variables of height, depth and quality of the newly formed bone tissue, evaluated at 30 and 120 days, was investigated by [17] who identified a significant relationship between these variables (p<0.001), particularly at 16 weeks post-extraction, which agrees with the results obtained by the authors of this research. However, this finding contrasts with recent research by [9,15,43] who do not report a consistent correlation between height, depth and quality of bone tissue. In their studies, they observed a considerable variability in bone density, suggesting that the quality of the newly formed tissue is not uniformly related to the post-surgical alveolar dimensions.
The present study generally identified a statistically significant difference between the control and experimental groups, concluding that PRF is effective in reducing alveolar bone resorption in height, depth and quality of bone tissue, promoting bone regeneration in the post-extraction alveolus. This finding was consistent with previous clinical studies by [16,44,45].
5. Conclusions
Despite the limitations of this research, it can be concluded that the use of post-extraction PRF preserves the dental alveolus of premolars for orthodontic indications in height and depth, stimulating a greater number of cell proliferation, improving healing at 30 and 120 days.
Author Contributions
All authors contributed to the development of the randomized controlled trial, conceptualization: M, M, B.; controlled trial, statistics, JC.; methodology, EF.; writing-review, RAR and J, D, C, T.; supervision, D, M and J, U.; project administration, fundraising.
Funding
This research did not receive external funding.
Data Availability Statement
The data presented in this study are available from the corresponding author upon request.
Acknowledgments
Thanks to the Catholic University of Cuenca
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- Abdulkarim, H. H. , Zeng, R., Pazdernik, V. K., & Davis, J. M. (2021). Effect of Bone Graft on the Correlation between Clinical Bone Quality and CBCT-determined Bone Density: A Pilot Study. Journal of Contemporary Dental Practice, 22(7), 756–762. [CrossRef]
- Ahmed, N. , Gopalakrishna, V., Shetty, A., Nagraj, V., Imran, M., & Kumar, P. (2019). Efficacy of PRF vs PRF + biodegradable collagen plug in post-extraction preservation of socket. Journal of Contemporary Dental Practice, 20(11), 1323–1328. [CrossRef]
- Alzahrani, A. A. , Murriky, A., & Shafik, S. (2017). Influence of platelet rich fibrin on post-extraction socket healing: A clinical and radiographic study. Saudi Dental Journal, 29(4), 149–155. [CrossRef]
- Anwandter, A. , Bohmann, S., Nally, M., Castro, A. B., Quirynen, M., & Pinto, N. (2016). Dimensional changes of the post extraction alveolar ridge, preserved with Leukocyte- and Platelet Rich Fibrin: A clinical pilot study. Journal of Dentistry, 52, 23–29. [CrossRef]
- Canellas, J. V. dos S., da Costa, R. C., Breves, R. C., de Oliveira, G. P., Figueredo, C. M. da S., Fischer, R. G., Thole, A. A., Medeiros, P. J. D. A., & Ritto, F. G. (2020a). Tomographic and histomorphometric evaluation of socket healing after tooth extraction using leukocyte- and platelet-rich fibrin: A randomized, single-blind, controlled clinical trial. Journal of Cranio-Maxillofacial Surgery, 48(1), 24–32. [CrossRef]
- Simon BI, Von Hagen S, Deasy MJ, Faldu M, Resnansky D. Changes in Alveolar Bone Height and Width Following Ridge Augmentation Using Bone Graft and Membranes. Journal of Periodontology. 2000 Nov 1;71(11):1774–91.
- Castaño-Granada, M. C. , Arismendi-Echavarria, J. A., Pérez-Cano, M. I., Gómez-Yali, A. J., & Sanchez-Gómez, S. (2023). Comparative tomographic and histological investigation of two biomaterials for preservation of the alveolar ridge. Uniciencia, 37(1). [CrossRef]
- Castro, A. B. , Van Dessel, J., Temmerman, A., Jacobs, R., & Quirynen, M. (2021). Effect of different platelet-rich fibrin matrices for ridge preservation in multiple tooth extractions: A split-mouth randomized controlled clinical trial. Journal of Clinical Periodontology, 48(7), 984–995. [CrossRef]
- Choukroun, J. , & Ghanaati, S. (2018). Reduction of relative centrifugation force within injectable platelet-rich-fibrin (PRF) concentrates advances patients’ own inflammatory cells, platelets and growth factors: the first introduction to the low speed centrifugation concept. European Journal of Trauma and Emergency Surgery, 44(1), 87–95. [CrossRef]
- Clark, D. , Rajendran, Y., Paydar, S., Ho, S., Cox, D., Ryder, M., Dollard, J., & Kao, R. T. (2018). Advanced platelet-rich fibrin and freeze-dried bone allograft for ridge preservation: A randomized controlled clinical trial. Journal of Periodontology, 89(4), 379–387. [CrossRef]
- Dimofte, A.-M. , Agop Forna, D., Costan, V.-V., & Popescu, E. (n.d.). THE VALUE OF PLATELET RICH FIBRIN IN BONE REGENERATION FOLLOWING TOOTH EXTRACTION. In Romanian Journal of Oral Rehabilitation (Vol. 9, Issue 3).
- Dutta, S. , Passi, D., Singh, P., Sharma, S., Singh, M., & Srivastava, D. (2016). A randomized comparative prospective study of platelet-rich plasma, platelet-rich fibrin, and hydroxyapatite as a graft material for mandibular third molar extraction socket healing. National Journal of Maxillofacial Surgery, 7(1), 45. [CrossRef]
- Eelen, G., De Zeeuw, P., Treps, L., Harjes, U., Wong, B. W., & Carmeliet, P. (2018). ENDOTHELIAL CELL METABOLISM. Endothelial Cell Metabolism. Physiol Rev, 98, 3–58. [CrossRef]
- Fickl, S., Zuhr, O., Wachtel, H., Stappert, C. F. J., Stein, J. M., & Hürzeler, M. B. (2008). Dimensional changes of the alveolar ridge contour after different socket preservation techniques. Journal of Clinical Periodontology, 35(10), 906–913. [CrossRef]
- Gupta, N. , & Agarwal, S. (2021). Advanced–PRF: Clinical evaluation in impacted mandibular third molar sockets. Journal of Stomatology, Oral and Maxillofacial Surgery, 122(1), 43–49. [CrossRef]
- Gürbüzer, B. , Pikdöken, L., Tunali, M., Urhan, M., Küçükodaci, Z., & Ercan, F. (2010). Scintigraphic Evaluation of Osteoblastic Activity in Extraction Sockets Treated With Platelet-Rich Fibrin. Journal of Oral and Maxillofacial Surgery, 68(5), 980–989. [CrossRef]
- Guzmán Castillo, G. F. , Paltas Miranda, M. E., Benenaula Bojorque, J. A., Núñez Barragán, K. I., & Simbaña García, D. V. (2017). Gingival and bone tissue healing in lower third molar surgeries. Comparative study between use of platelet rich fibrin versus physiological healing. Revista Odontológica Mexicana, 21(2), e112–e118. [CrossRef]
- Hauser, F. , Gaydarov, N., Badoud, I., Vazquez, L., Bernard, J. P., & Ammann, P. (2013). Clinical and histological evaluation of postextraction platelet-rich fibrin socket filling: A prospective randomized controlled study. Implant Dentistry, 22(3), 295–303. [CrossRef]
- He, L. , Lin, Y., Hu, X., Zhang, Y., & Wu, H. (2009). A comparative study of platelet-rich fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology, 108(5), 707–713. [CrossRef]
- Hoaglin, D. R. , & Lines, G. K. (2013). Prevention of localized osteitis in mandibular third-molar sites using platelet-rich fibrin. In International Journal of Dentistry (Vol. 2013). [CrossRef]
- Kapse, S. , Surana, S., Satish, M., Hussain, S. E., Vyas, S., & Thakur, D. (2019). Autologous platelet-rich fibrin: can it secure a better healing? Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, 127(1), 8–18. [CrossRef]
- Kattimani, V. S. , Lingamaneni, K. P., Kreedapathi, G. E., & Kattappagari, K. K. (2019). Socket preservation using eggshell-derived nanohydroxyapatite with platelet-rich fibrin as a barrier membrane: A new technique. Journal of the Korean Association of Oral and Maxillofacial Surgeons, 45(6), 332–342. [CrossRef]
- Kim, D.-G. (2014). Can Dental Cone Beam Computed Tomography Assess Bone Mineral Density? Journal of Bone Metabolism, 21(2), 117. [CrossRef]
- Kumar, Y. R. , Mohanty, S., Verma, M., Kaur, R. R., Bhatia, P., Kumar, V. R., & Chaudhary, Z. (2016). Platelet-rich fibrin: The benefits. British Journal of Oral and Maxillofacial Surgery, 54(1), 57–61. [CrossRef]
- Mazor, Z. , Horowitz, R., Prasad, H., & Kotsakis, G. (2019). Healing Dynamics Following Alveolar Ridge Preservation with Autologous Tooth Structure. The International Journal of Periodontics & Restorative Dentistry, 39(5), 697–702. [CrossRef]
- Nemtoi, A. , Sirghe, A., Nemtoi, A., & Haba, D. (2018). The Effect of a Plasma With Platelet-rich Fibrin in Bone Regeneration and on Rate of Orthodontic Tooth Movement in Adolescents. In REV.CHIM.(Bucharest)♦ (Vol. 69, Issue 12). 372. Available online: http://www.revistadechimie.ro3727.
- Niedzielska, I. , Ciapiński, D., Bak, M., & Niedzielski, D. (2022). The Assessment of the Usefulness of Platelet-Rich Fibrin in the Healing Process Bone Resorption. Coatings, 12(2). [CrossRef]
- of Oral, P. , & Radiology, M. (2017). In vitro Evaluation of the Relationship between Gray Scales in Digital Intraoral Radiographs and Hounsfield Units in CT Scans. In J Biomed Phys Eng (Vol. 7, Issue 3). www.jbpe.
- Peck, M. T. , Marnewick, J., & Stephen, L. (2011). Alveolar Ridge Preservation Using Leukocyte and Platelet-Rich Fibrin: A Report of a Case. Case Reports in Dentistry, 2011, 1–5. [CrossRef]
- Pohl, S. , Binderman, I., & Tomac, J. (2020a). Maintenance of alveolar ridge dimensions utilizing an extracted tooth dentin particulate autograft and platelet-rich fibrin: A retrospective radiographic cone-beam computed tomography study. Materials, 13(5). [CrossRef]
- Ratajczak, J. , Vangansewinkel, T., Gervois, P., Merckx, G., Hilkens, P., Quirynen, M., Lambrichts, I., & Bronckaers, A. (2018). Angiogenic Properties of ‘Leukocyte- and Platelet-Rich Fibrin.’ Scientific Reports, 8(1). [CrossRef]
- Revathy, Ns. , Kannan, R., Karthik, R., Kumar, M. S., Munshi, M. I., & Vijay, R. (2018). Comparative study on alveolar bone healing in postextraction socket versus healing aided with autologous platelet-rich fibrin following surgical removal of bilateral mandibular impacted third molar tooth: A radiographic evaluation. National Journal of Maxillofacial Surgery, 9(2), 140. [CrossRef]
- Shiezadeh, F. , Taher, M., Shooshtari, Z., Arab, H. R., & Shafieian, R. (2023). Using Platelet-Rich Fibrin in Combination With Allograft Bone Particles Can Induce Bone Formation in Maxillary Sinus Augmentation. Journal of Oral and Maxillofacial Surgery, 81(7), 904–912. [CrossRef]
- Srinivas, B. , Das, P., Rana, M. M., Qureshi, A. Q., Vaidya, K. C., & Raziuddin, S. J. A. (2018c). Wound healing and bone regeneration in postextraction sockets with and without platelet-rich fibrin. Annals of Maxillofacial Surgery, 8(1), 28–34. [CrossRef]
- Strauss, F. J. , Nasirzade, J., Kargarpoor, Z., Stähli, A., & Gruber, R. (2020). Effect of platelet-rich fibrin on cell proliferation, migration, differentiation, inflammation, and osteoclastogenesis: a systematic review of in vitro studies. In Clinical Oral Investigations (Vol. 24, Issue 2, pp. 569–584). Springer. [CrossRef]
- Suttapreyasri, S. , & Leepong, N. (2013). Influence of platelet-rich fibrin on alveolar ridge preservation. Journal of Craniofacial Surgery, 24(4), 1088–1094. [CrossRef]
- Temmerman, A. , Vandessel, J., Castro, A., Jacobs, R., Teughels, W., Pinto, N., & Quirynen, M. (2016). The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: a split-mouth, randomized, controlled clinical trial. Journal of Clinical Periodontology, 43(11), 990–999. [CrossRef]
- Ucer, C. , & Khan, R. S. (2023). Extraction Socket Augmentation with Autologous Platelet-Rich Fibrin (PRF): The Rationale for Socket Augmentation. In Dentistry Journal (Vol. 11, Issue 8). Multidisciplinary Digital Publishing Institute (MDPI). [CrossRef]
- Yuan, Y. , Xu, B., Yang, J., & Wu, M. (2024). Effects of platelet-rich fibrin on post-extraction wound healing and wound pain: A meta-analysis. International Wound Journal, 21(2). [CrossRef]
- Zhang, Y. , Ruan, Z., Shen, M., Tan, L., Huang, W., Wang, L., & Huang, Y. (2018). Clinical effect of platelet-rich fibrin on the preservation of the alveolar ridge following tooth extraction. Experimental and Therapeutic Medicine, 15(3), 2277–2286. [CrossRef]
Figure 1.
Cross sections of CBCT 30 days post-extraction. a: Height, depth 1, 3, 5 mm measurements of alveolar ridge piece 4.4 with PRF; b: Alveolar ridge measurements piece 3.4 without PRF; c: Bone quality in Uh piece 4.4 with PRF; d: Bone quality in Uh piece 3.4 without PRF.
Figure 1.
Cross sections of CBCT 30 days post-extraction. a: Height, depth 1, 3, 5 mm measurements of alveolar ridge piece 4.4 with PRF; b: Alveolar ridge measurements piece 3.4 without PRF; c: Bone quality in Uh piece 4.4 with PRF; d: Bone quality in Uh piece 3.4 without PRF.
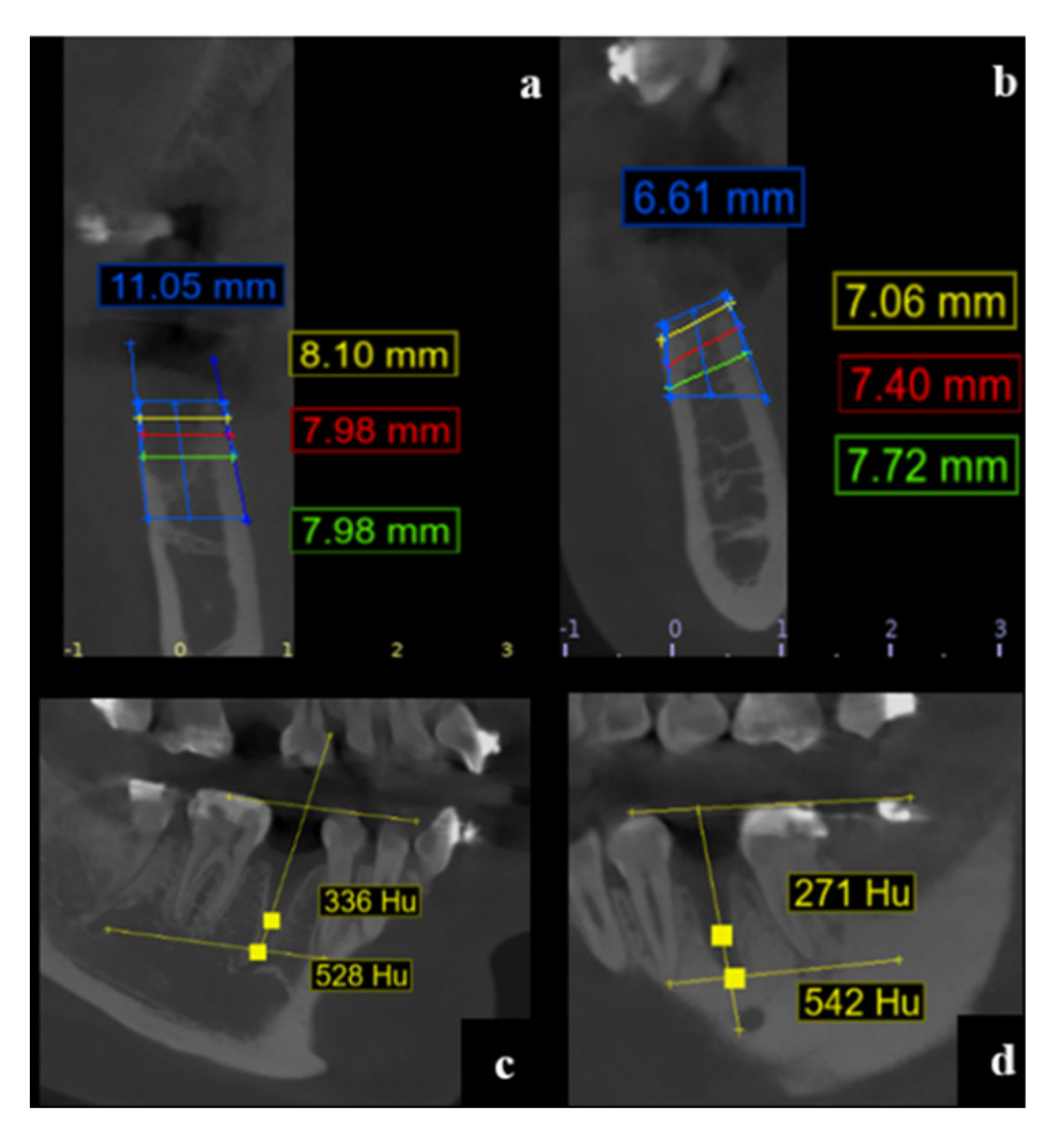
Figure 2.
Cross sections of CBCT 120 days post-extraction. a: Height, depth 1, 3, 5 mm measurements of alveolar ridge piece 4.4 with PRF; b: Alveolar ridge measurements piece 3.4 without PRF; c: Bone quality in Uh piece 4.4 with PRF; d: Bone quality in Uh piece 3.4 with PRF.
Figure 2.
Cross sections of CBCT 120 days post-extraction. a: Height, depth 1, 3, 5 mm measurements of alveolar ridge piece 4.4 with PRF; b: Alveolar ridge measurements piece 3.4 without PRF; c: Bone quality in Uh piece 4.4 with PRF; d: Bone quality in Uh piece 3.4 with PRF.
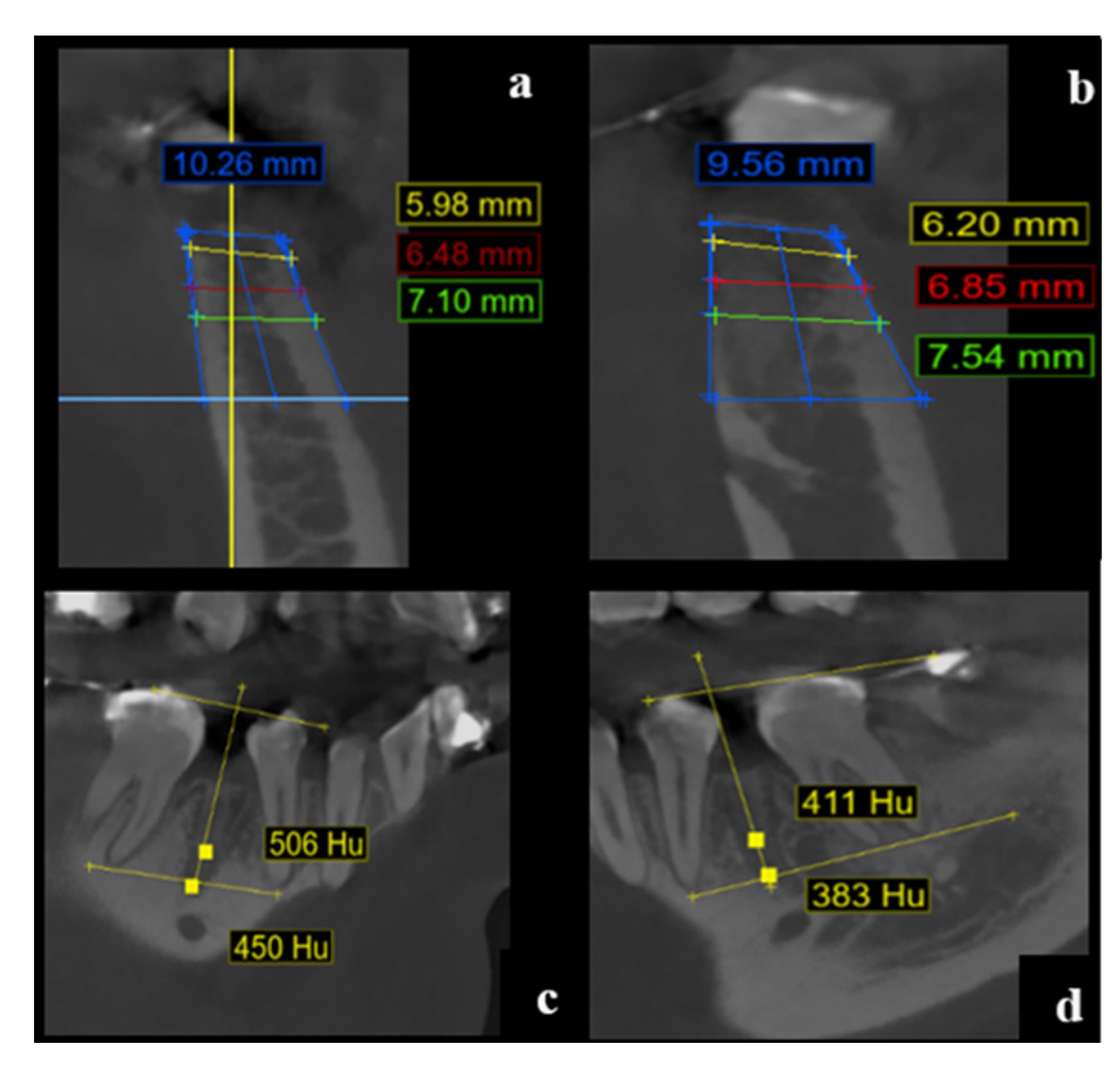
Table 1.
Note: Group I = Alveolus without PRF; Group II = Alveolus with PRF; N = Absolute frequency of observations; M = Mean; SD = Standard deviation; CV = Coefficient of variation; Diff = Difference in means; CI (95%) = 95% confidence interval; t = Student t test for independent samples; p = statistical significance.
Table 1.
Note: Group I = Alveolus without PRF; Group II = Alveolus with PRF; N = Absolute frequency of observations; M = Mean; SD = Standard deviation; CV = Coefficient of variation; Diff = Difference in means; CI (95%) = 95% confidence interval; t = Student t test for independent samples; p = statistical significance.
| Variable | Time | Group | N | M | DE | CV | Averages | t | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Dif | IC (95%) | |||||||||
| Height | Initial | Group I | 17 | 10,45 | 1,10 | 0,11 | -0.28 | ICI= -0.324 ICS= 0.382 | -0.853 | 0.399 |
| Group II | 19 | 10,72 | 0,84 | 0,08 | ||||||
| 30 days | Group I | 17 | 8,82 | 1,68 | 0,19 | -1.79 | ICI= -2.674 ICS= -0.901 |
-4.099 | < .001 | |
| Group II | 19 | 10,61 | 0,85 | 0,08 | ||||||
| 120 days | Group I | 17 | 9,31 | 1,73 | 0,19 | -0.99 | ICI= -2.015ICS= 0.040 | -1.953 | 0.059 | |
| Group II | 19 | 10,30 | 1,29 | 0,13 | ||||||
| Depth 1mm | 30 days | Group I | 17 | 8,40 | 1,84 | 0,22 | -0.63 | ICI= -1.705 ICS= 0.453 | -1.179 | 0.247 |
| Group II | 19 | 9,02 | 1,33 | 0,15 | ||||||
| 120 days | Group I | 17 | 8,40 | 1,92 | 0,23 | 0.34 | ICI= -0.912 ICS= 1.596 | 0.554 | 0.583 | |
| Group II | 19 | 8,06 | 1,78 | 0,22 | ||||||
| Depth 3mm | 30 days | Group I | 17 | 8,76 | 1,69 | 0,19 | -0.62 | ICI= -1.626 ICS= 0.385 | -1.254 | 0.218 |
| Group II | 19 | 9,38 | 1,27 | 0,14 | ||||||
| 120 days | Group I | 17 | 9,39 | 1,69 | 0,18 | 0.94 | ICI= -0.195 ICS= 2.082 | 1.684 | 0.101 | |
| Group II | 19 | 8,45 | 1,67 | 0,20 | ||||||
| Depth 5mm | 30 days | Group I | 17 | 9,19 | 1,78 | 0,19 | -0.07 | ICI= -1.174 ICS= 1.029 |
-0.133 | 0.895 |
| Group II | 19 | 9,26 | 1,47 | 0,16 | ||||||
| 120 days | Group I | 17 | 9,99 | 1,93 | 0,19 | 0.95 | ICI= -0.266 ICS= 2.157 | 1.586 | 0.122 | |
| Group II | 19 | 9,04 | 1,65 | 0,18 | ||||||
Table 3.
Intragroup analysis.
| Variable | Analysis | Sum of squares | Degrees of freedom | Root mean square | F | p | η² |
|---|---|---|---|---|---|---|---|
| Height | Time | 16.45 | 2 | 8.224 | 7.840 | < .001 | 0.074 |
| Time ✻ Group | 10.26 | 2 | 5.132 | 4.892 | 0.010 | 0.046 | |
| Residuals | 71.33 | 68 | 1.049 | ||||
| Depth 1mm | Time | 4.21 | 1 | 4.212 | 4.840 | 0.035 | 0.020 |
| Time ✻ Group | 4.20 | 1 | 4.202 | 4.828 | 0.035 | 0.020 | |
| Residuals | 29.59 | 34 | 0.870 | ||||
| Depth 3mm | Time | 0.41 | 1 | 0.412 | 0.627 | 0.434 | 0.002 |
| Time ✻ Group | 10.98 | 1 | 10.977 | 16.693 | < .001 | 0.060 | |
| Residuals | 22.36 | 34 | 0.658 | ||||
| Depth 5mm | Time | 1.52 | 1 | 1.520 | 2.284 | 0.140 | 0.007 |
| Time ✻ Group | 4.65 | 1 | 4.648 | 6.985 | 0.012 | 0.022 | |
| Residuals | 22.63 | 34 | 0.665 |
Note: F= ANOVA, p= statistical significance, η²= Eta squared.
Table 5.
Post hoc tests, changes by group.
| Group | Variable | Measurement 1 | Measurement 2 | Difroot mean square | W | z | p | IC root mean square differences (95%) |
|---|---|---|---|---|---|---|---|---|
| Group I | Height | Start | 30 days | -1,626 | 13.65 | 2.840 | 0.005 | ICI= 0.550 ICS=2.610 |
| 30 days | 120 days | 0,491 | 4.30 | -1.586 | 0.118 | ICI= -1.100 ICS= 0.090 |
||
| Depth | 30 days (1 mm) |
120 days (1 mm) |
0,000 | 6.80 | -0.402 | 0.705 | ICI= -0.755 ICS=0.755 | |
| 30 days (3 mm) |
120 days (3 mm) |
-0,630 | 2.70 | -2.343 | 0.020 | ICI= -1.280ICS=-0.090 | ||
| 30 days (5 mm) |
120 days (5 mm) |
0,800 | 2.10 | -2.627 | 0.009 | ICI= -1.355ICS=-0.465 | ||
| Group II | Height | Start | 30 days | -0,115 | 15.40 | 2.374 | 0.019 | ICI=0.055 ICS= 0.435 |
| 30 days | 120 days | -0,310 | 9.20 | 0.734 | 0.477 | ICI= -0.300 ICS=0.970 | ||
| Depth | 30 days (1 mm) |
120 days (1 mm) |
-0,968 | 16.20 | 2.696 | 0.007 | ICI=0.190 ICS=1.560 | |
| 30 days (3 mm) |
120 days (3 mm) |
-0,933 | 16.70 | 2.897 | 0.004 | ICI=0.340 ICS=1.420 | ||
| 30 days (5 mm) |
120 days (5 mm) |
-0,218 | 9.90 | 0.161 | 0.888 | ICI= -0.480 ICS=0.900 |
Note: Note: Group I= Alveolus without PRF; Group II= Alveolus with PRF; Dif means= Difference in means; p= statistical significance; W= Wilcoxon test z= z value, CI= 95% confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



