
Submitted:
28 March 2025
Posted:
01 April 2025
You are already at the latest version
Abstract
Background/Objectives: Substance use during pregnancy continues to affect maternal and infant health outcomes globally. Applying the Three Delays Framework, this study evaluates the relationship between substance use and maternal health outcomes in Alabama, focusing on prenatal care health barriers. Methods: This study employed a quantitative design using secondary data from the PRAMS Phase 8 survey (2016–2021) provided by the Alabama Department of Public Health. Prenatal care barriers were classified into three domains: delays in seeking, reaching, and receiving care. Advanced statistical techniques were undertaken, including descriptive statistics, logistic regression, and mediation analysis. An item response theory (IRT) model was applied to derive an underlying characteristic for informational barriers (theta_info). This was incorporated into a structural equation model (SEM) to test whether informational barriers mediate the relationship between substance use and maternal health outcomes. Demographic covariates like age, race/ethnicity, income, BMI were included as controls. Results: Logistic regression results showed that systemic barriers (OR = 1.77, p = .047) and informational barriers (OR = 2.42, p < .001) were significantly associated with adverse maternal health outcomes. Structural barriers and substance use had insignificant direct effects. However, mediation analysis and SEM findings revealed that informational barriers significantly mediated the relationship between substance use and maternal health, with approximately 44% of the effect transmitted indirectly through theta_info. Conclusions: These findings emphasize the critical role of prenatal care barriers like systemic and informational barriers in influencing maternal health outcomes in Alabama. Addressing informational deficits can improve prenatal care and perinatal outcomes.
Keywords:
PRAMS
; Three Delays Model
; maternal health
; substance use
; pregnancy
; reproductive health
; infant health
; Alabama
1. Introduction
Substance use during pregnancy presents substantial risks to maternal and neonatal health globally, contributing to adverse birth outcomes, including stillbirth, preterm birth, birth defects, and low birth weight [1]. Inadequate infrastructure challenges have made it difficult to find lasting solutions to a burgeoning public health problem that continues to threaten the social fabric of society, community safety, and the health and well-being of families. Because the burden of disease and disability associated with substance use during pregnancy evolves over a period, understanding and updating our knowledge and strategies on the structural and social drivers of this public health threat must be prioritized to improve outcomes for the population affected.
Even though significant efforts have been made over the past decades to lessen the risks associated with substance use during pregnancy among women of reproductive age, there are still substantial gaps in contextualizing the psychosocial factors that contribute to this problem and how to galvanize community action to address this ongoing health issue [2]. Interestingly, past research has shown that psychosocial and behavioral interventions, like contingency management, motivational support, and cognitive behavioral therapies, are crucial to addressing substance use during pregnancy [3]. Notwithstanding, designing and implementing innovative and sustained strategies that identify at-risk pregnant women early and get them to treatment remains a challenge, underscoring the need for information seeking during the prenatal period.
Geographic factors and cultural nuances can also influence the burden and disability associated with substance use during pregnancy across diverse care settings. The prevailing thought is that culture plays a crucial role in how we behave and communicate, and these intricate nuances affect our beliefs and views on substance and alcohol use [4]. This insight further supports a need to uncover the multidimensions of the interplay and interconnectedness of factors that influence pregnant women afflicted with substance use to seek care, reach care, and receive care. The knowledge gained can guide the development of robust strategies to improve outcomes for those most affected by this public health problem. Notably, opioid use among pregnant women is still deemed a significant public health concern [2], deserving priority attention and policy realignment.
To understand the gravity of this problem, data from 2010 to 2017 shows a 131% increase in opioid-related diagnoses at delivery hospitalization [2,5]. More crucially, opioid use disorder during pregnancy is known to be associated with serious adverse health outcomes, including preterm birth, stillbirth, maternal mortality, and neonatal abstinence syndrome [2]. These adverse health outcomes highlight the urgency and timeliness of this issue, demanding targeted research, implementation of sustained evidence-based practices, program evaluation, and monitoring to ensure improved health gains [4,6]. Given these circumstances, the Three Delays Model was employed in this research to evaluate and understand the complex relationships between substance use and maternal health outcomes and their mediating and moderating effects. This framework has the potential to offer new insights into the latent and observable factors concerning substance use during pregnancy and maternal health outcomes, thereby providing a fuller picture and the context-specific needs to prioritize. Based on the Three Delays Model, the research hypotheses are as follows:
- Higher levels of prenatal care barriers, particularly system-level and informational barriers, would be associated with poorer maternal health outcomes.
- Informational barriers would mediate the relationship between substance use and maternal health.
The Three Delays Model
The Three Delays Model was created to help outline and categorize three groups of factors that may act as barriers to women’s access to maternal health care in resource-constrained settings [7]. This framework has a strong appeal in maternal and infant health research, as it helps us to understand delays in seeking care, delays in reaching healthcare facilities, and delays in receiving adequate and timely care [8,9,10], crystalizing the three domains and their individual and collective impact on barriers to care. In the context of Alabama, this framework provides an approach to assess and comprehend the information needs and decision-making of pregnant women impacted by substance use. This model takes into consideration the speed or timeliness in obtaining care, which can be affected by systemic factors such as transportation issues, difficulty getting an appointment, inadequate knowledge of early signs of pregnancy, financial constraints for services, health insurance needs, and even keeping the pregnancy secret or past unpleasant encounters with healthcare providers. While not an exhaustive list, these factors represent the three main categories under this framework.
Study Materials, Variables, and Operational Definitions
This study utilized a quantitative, cross-sectional design and secondary de-identified data from the Pregnancy Risk Assessment Monitoring System (PRAMS) Phase 8 survey for cohort years 2016–2021. The Alabama Department of Public Health provided the data. PRAMS is administered to women who have recently delivered a live infant and captures maternal behaviors and attitudes during pregnancy and the early postpartum period, typically 2–4 months after birth. The population of interest comprised women who experienced live births in Alabama. The initial PRAMS Phase 8 data set comprised 596 observations. This subset of the original data received from the Alabama Department of Public Health (ADPH) was deliberately selected based on key variables necessary to address the research question, study aims, and the relevance of the Three Delays Model or framework. After excluding cases with missing data on key study variables, a complete case sample of 533 observations was used for analysis.
Table 1 below shows the operational definitions and measurement of the study variables. The primary outcome, maternal health status, was defined and operationalized as a combined measure or composite indicator derived from assessing maternal health status Qn22 as good or poor. Substance use or consumption was evaluated based on smoking during pregnancy, using responses to the Qn42_CigaretteCategory variable, recoded to non-smokers (coded 0) and smokers (coded 1).
Prenatal care barriers were classified according to the Three Delays Model and divided into three categories. Structural barriers included financial constraints and work or school conflicts, measured by an aggregated score of Qn21b_Money and Qn21f_WorkSchool. Informational obstacles or barriers implied a lack of awareness and knowledge regarding prenatal care modeled as an underlying trait (theta_info) derived from an IRT analysis of Qn21i_Unaware, Qn21j_Secret, and Qn21k_NoPNC items. System barriers captured difficulties experienced by respondents in navigating the healthcare system, operationalized as a composite score of Qn21a_Appoint and Qn21d_HealthPlan. In addition, demographic variables such as Age Group, Race/Ethnicity, Income Category, and BMI Category served as control variables.
Factors that influence substance use during pregnancy among women of reproductive age are multifaceted [11,12,13]. Finding sustainable solutions to this intractable public health crisis requires the application of an appropriate theoretical framework and an unyielding resource commitment. The socio-ecological model of health and the health belief model (HBM) offers valuable insights into understanding this ongoing public health issue [14,15], as they capture the subtle nuances that contribute to this public health crisis by revealing influences at the individual, interpersonal, community, organizational, and societal levels. However, this study selected the Three Delays Framework because it aligns more closely with the objective of this research. This framework provides additional context for understanding and addressing the health system and community-based challenges that women encounter during pregnancy when seeking prenatal care health services [7]. Accordingly, this study aims to examine the association between substance use during pregnancy and maternal health outcomes, identify specific barriers, and recommend targeted interventions for improved outcomes.
2. Methods and Statistical Analysis
Descriptive statistics were generated to summarize sample characteristics and variable distributions. Exploratory techniques, including multidimensional scaling (MDS) and hierarchical clustering, were performed to ascertain the grouping of prenatal care barrier items. Internal consistency was evaluated using Cronbach’s alpha and McDonald’s omega. Given the low reliability estimates for the composite measures [omega totals of 0.11 for Delay Seeking, 0.07 for Delay Reaching, and 0.14 for Delay Receiving], an IRT model was employed to derive the latent trait for informational barriers (theta_info). The inferential analyses included logistic regression to examine associations among substance use, prenatal care barrier constructs, and maternal health outcomes while controlling for demographic covariates. The logistic regression model was specified as:
logit[P(Y
= poor)] = β₀ + β₁(smoker_status) + β₂(structural_barriers_new) +
β₃(system_barriers_new) + β₄(theta_info) + β₅(Age_Group) + β₆(Race/Ethnicity)
+ β₇(Qn79_IncomeCategory) + β₈(BMI_Category).
Mediation analyses, utilizing bootstrapping (1,000 simulations), were employed to evaluate whether informational barriers mediated the relationship between substance use and maternal health. A structural equation model (SEM) was estimated using the WLSMV estimator in lavaan, with maternal health status treated as an ordered categorical variable. Multi-level covariates were converted to numeric form for model inclusion, and model fit was evaluated using indices such as the Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), and Root Mean Square Error of Approximation (RMSEA). All analyses were performed in R version 4.4 using packages including dplyr, tidyr, psych, mediation, and lavaan.
3. Results
Table 2 below shows the frequencies and percentages for the key study variables. For example, 53.8% of respondents were classified as having good maternal health, while 46.2% had poor maternal health. In addition, 60.2% were categorized as non-smokers, and 39.8% were smokers. The table also displays the distributions for individual Qn21 items, income categories, BMI, age groups, and race/ethnicity.
To visually assess the underlying grouping structure for each of the items, a multidimensional scaling (MDS) plot was employed. As shown in Figure 1, the items clustered in a two-dimensional space, revealing several groupings that may correspond to distinct barriers. Items associated with financial or scheduling constraints, like Qn21b_Money and Qn21a_Appoint, appeared in one region, while items reflecting knowledge or secrecy barriers, like Qn21i_Unaware and Qn21j_Secret, appeared in another. These patterns provide initial evidence that these items may capture multiple underlying dimensions of prenatal care barriers, aligning partially with the Three Delays Model.
To determine whether different types of delays (seeking, reaching, and receiving care) have a significant relationship with maternal health status, bivariate analyses using chi-square tests were employed. The bivariate analyses revealed that the Delay Seeking factor was significantly associated with maternal health status (χ²(3) = 23.11, p < .001), while the Delay Reaching (χ²(1) = 2.59, p = 0.462) and Delay Receiving (χ²(1) = 4.42, p = 0.229) factors were not. These results show that, at the bivariate level, only variations in Delay Seeking are significantly related to differences in maternal health outcomes.
Expanding on these initial findings, a logistic regression model was employed to assess associations among substance use, prenatal care barrier constructs, and maternal health outcomes while controlling for demographic covariates. As shown in Table 3, system-level barriers (OR = 1.77, p = .046) and informational barriers, as measured by the IRT-derived latent trait (theta_info; OR = 2.42, p < .001), were significantly associated with adverse maternal health outcomes. However, structural barriers and substance use did not show significant direct effects.
These results suggest that, among the prenatal care barriers examined, system-level barriers or obstacles and informational barriers, as measured by the IRT-derived latent trait, are the most robust predictors of maternal health outcomes. Specifically, higher levels of system barriers increase the odds of poor maternal health by 77%, and a one-unit increase in informational barriers is associated with a 142% increase in the odds of poor health. Although substance use showed a trend toward significance, its association was not statistically robust after adjusting for other factors. Together, these findings underscore the importance of addressing systemic and informational barriers in interventions to improve maternal health outcomes.
A hierarchical clustering analysis was performed to identify distinct groups of prenatal care barriers. This method shows how specific barriers cluster together, offering insights into their relationships and guiding targeted perinatal interventions. Figure 2 depicts the hierarchical clustering dendrogram for the Qn21 items, which were hypothesized as representing different domains of prenatal care barriers. Several notable clusters emerged.
For example, Qn21b_Money and Qn21f_WorkSchool are grouped, showing a potential overlap in financial and work-related constraints. Likewise, Qn21g_MedicaidCard, Qn21e_Busy, and Qn21i_Unaware formed another cluster, revealing a set of logistical or knowledge-related barriers or issues. Conversely, Qn21j_Secret and Qn21k_NoPNC appeared as a distinct pair, potentially capturing personal or privacy concerns associated with pregnant women not seeking prenatal care.
These groupings largely align with the patterns observed in the Multidimensional Scaling (MDS) analysis shown in Figure 1. However, the dendrogram does not wholly separate the items into three discrete clusters corresponding to the Three Delays Model. Instead, the results suggest that some barriers, like money and work constraints, may cut across multiple theoretical domains. Composite scores for each cluster were created to understand their relationship to maternal health outcomes. Further steps involve refining these item groupings and examining how they relate to maternal health outcomes.
Following the hierarchical clustering analysis, the complex relationships between prenatal care barriers, substance use, and maternal health outcomes were further evaluated through mediation analysis. This approach allowed for an assessment of the indirect effects of informational barriers on the observed associations. The mediation analyses using 1,000 bootstrap simulations were performed to test whether informational barriers mediated the relationship between substance use and maternal health. Table 4 summarizes these findings.
The average causal mediation effect (ACME) was statistically significant (Estimate = 0.03, 95% CI [0.01, 0.05], p = .006), indicating that informational barriers significantly mediate the relationship between substance use and maternal health. The average direct effect (ADE) was not statistically significant (Estimate = –0.08, 95% CI [–0.16, 0.00], p = .056), and the total effect was non-significant (p = .232). The proportion mediated was –0.44. The negative value suggests that the mediated (indirect) effect operates in the opposite direction of the direct effect, a pattern that may indicate a suppression effect. In essence, while substance use tends to reduce the odds of poor maternal health (although not significantly so), the pathway through informational barriers contributes an effect in the opposite direction. These findings highlight the complex interplay of factors influencing maternal health outcomes and strengthen the importance of informational barriers in this relationship.
To expand on and confirm the findings from the logistic regression and mediation analyses, a structural equation model (SEM) was estimated. This thorough approach allows for the simultaneous examination of multiple relationships among the variables, providing a robust framework to understand the complex dynamics influencing maternal health outcomes. Table 5 reports the parameter estimates from a structural equation model testing whether informational barriers (measured by the IRT-derived latent trait, θ) mediate the relationship between substance use (smoker_status) and maternal health status (good vs. poor), controlling for structural and system barriers and demographic covariates.
The mediator equation revealed that smoker_status significantly predicted θ (a = 0.143, SE = 0.058, 95% CI [0.029, 0.257], p = .014). In the outcome equation, θ significantly predicted maternal health status (d = 0.530, SE = 0.079, 95% CI [0.375, 0.685], p < .001). However, the direct effect of smoker_status on maternal health (c′ = –0.199, SE = 0.111, 95% CI [–0.417, 0.019], p = .072) did not reach conventional significance.
The estimated indirect effect (a*d = 0.076, SE = 0.032, 95% CI [0.013, 0.139], p = .018) was statistically significant, indicating that informational barriers partially mediate the association between substance use and maternal health. The total effect was also non-significant (–0.123, p = .269). These results suggest that while the direct effect of substance use on maternal health is weak, a significant portion of the effect is transmitted indirectly through informational barriers.
To illustrate the discriminative properties of the informational barriers’ items, Figure 3 shows the item characteristic curves. For example, the item characteristic curves (ICCs) for Qn21i_Unaware, Qn21j_Secret, and Qn21k_NoPNC under a two-parameter logistic (2PL) IRT model. Qn21i_Unaware demonstrates a relatively flat slope, reflecting low discrimination. In contrast, Qn21j_Secret shows a sharply decreasing curve, consistent with its high negative loading and strong discrimination. Qn21k_NoPNC also depicts a steep slope, revealing moderate-to-high discrimination. These patterns suggest that Qn21j_Secret and Qn21k_NoPNC are particularly effective at distinguishing respondents across the latent trait of informational barriers, whereas Qn21i_Unaware contributes less to differentiating individuals. Despite the limited discrimination of Qn21i_Unaware, the items collectively capture a meaningful latent construct of informational barriers to prenatal care. These curves visually demonstrate how each item differentiates between various levels of the latent trait, further emphasizing the significance of informational barriers in understanding maternal health outcomes.
4. Discussion
This cross-sectional study is among the few that have examined the association between substance use during pregnancy and maternal health outcomes in Alabama using the Three Delays Model. While this framework has been extensively employed in maternal health research [7,8,9,10,16], its application to substance use during pregnancy remains limited. This study contributes to the literature by examining the association between substance use and maternal health outcomes through the lens of this framework, emphasizing the mediating role of informational barriers.
Barriers to prenatal care were conceptualized and categorized into three domains: structural barriers, informational barriers, and system barriers. The analysis showed that system-level barriers and informational barriers were significantly associated with adverse or poor maternal health outcomes [11,15,17,18,19,20]. In contrast, structural barriers and substance use (smoker_status) did not exhibit significant direct effects, as observed in this study.
Additionally, mediation analyses demonstrated that informational barriers, which were operationalized as an IRT-derived latent trait (theta_info), significantly mediated the relationship between substance use and maternal health outcomes, with approximately 44 percent of the effect transmitted indirectly. Likewise, the structural equation model (SEM) corroborated these findings, showing excellent model fit and robust parameter estimates. The methodological robustness of combining IRT and SEM is supported or validated by past research [21,22].
4.1. Implications for Theory and Practice
The study findings highlight the utility of the Three Delays Model in understanding prenatal care barriers and how they impact maternal and perinatal outcomes. For instance, the significant effects of system-level and informational barriers suggest that pregnant women experiencing substance use disorders face challenges related to navigating the healthcare system. Deficits in awareness about and access to prenatal health services and other community resources and informational needs during the perinatal period critically continue to impact maternal health outcomes.
Research has shown that low maternal health literacy significantly affects maternal and child health outcomes, including access to essential care and health services [23]. Likewise, language barriers and health communication anxiety among linguistic minorities exacerbate healthcare disparities and limit access to appropriate services [24]. Cultural norms and health-seeking behaviors also shape the utilization of healthcare services, particularly in diverse or rural settings [25]. Developing culturally tailored health education materials and initiatives has been shown to reduce disparities and improve outcomes in vulnerable populations [26]. Alabama could benefit from such efforts by investing in telehealth and mobile clinic initiatives. The mediating role of informational barriers implies that, even when substance use may not directly compromise maternal health, the lack of information or awareness about prenatal care can exacerbate adverse outcomes.
These results extend previous research by underscoring the complex interplay of behavioral and systemic factors.
In practical terms, the findings suggest that interventions aimed at improving maternal health in Alabama should prioritize enhancing the accessibility and quality of information about prenatal care and other community support services for those in need during the prenatal and postpartum periods. Referral and case management services should complement other public health evidence-based practices to sustain health gains. Addressing systemic issues like appointment scheduling and service availability should be prioritized in healthcare planning and policy development.
4.2. Study Limitations
Despite its strengths, this study has a few limitations that merit discussion. First, its cross-sectional design limits causal interpretations, as the associations identified do not necessarily imply causation. Second, the reliance on self-reported data from the PRAMS Phase 8 data set introduces the possibility of response bias, as participants may underreport or overreport behaviors and experiences. While this limitation is inherent to survey-based research, it is essential to interpret the findings with caution.
Third, the study findings are specific to Alabama and cannot be generalized to other states or regions. The design of PRAMS, including its implementation of state-specific core questions and sampling methodologies, inherently limits comparability across states. This methodological nuance highlights the importance of situating the findings within the context of Alabama’s unique demographic, socioeconomic, and healthcare characteristics. Lastly, the low reliability of some composite measures necessitated the use of advanced statistical techniques, such as item response theory (IRT), to derive latent traits. Although these methods address reliability concerns, they may obscure nuances within individual items. Future research should consider qualitative approaches or longitudinal designs to provide a deeper understanding of these prenatal care barriers and their influence on maternal health outcomes.
5. Conclusions
Altogether, this study demonstrates that system-level and informational barriers significantly influence maternal health outcomes among women who experience substance use during pregnancy. Addressing these barriers through policy changes, tailored interventions, and enhanced access to resources could improve prenatal care utilization and, consequently, lead to better maternal and infant health outcomes.
Author Contributions
JKD: Conceptualization, methodology, data curation, formal analysis, visualization, validation, writing (original draft, review, editing), and project administration.
Funding
Please add: This study did not receive funding from government, commercial, or non-profit organizations.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. It utilized de-identified, anonymized data, and new approval was unnecessary or not applicable. The PRAMS Phase 8 dataset was approved previously for use by Auburn University IRB under protocol number 24-831, with an approval date of July 11, 2024.
Informed Consent Statement
Informed consent was not required for this research study.
Data Availability Statement
Due to the existing data use agreement with the state of Alabama, the entire dataset cannot be shared. However, data supporting the study findings can be made available upon reasonable request.
Acknowledgments
Special thanks to the Alabama PRAMS Work Group and the Centers for Disease Control and Prevention for providing quantitative data for this study.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACME | Average Causal Mediation Effect |
| ADE | Average Direct Effect |
| ADPH | Alabama Department of Public Health |
| BMI | Body Mass Index |
| CFI | Comparative Fit Index |
| CI | Confidence Interval |
| IRB | Institutional Review Board |
| IRT | Item Response Theory |
| MDS | Multidimensional Scaling |
| PNC | Prenatal Care |
| PRAMS | Pregnancy Risk Assessment Monitoring System |
| Qn21a | Alabama PRAMS Phase 8 Questionnaire #21a |
| Qn21b | Alabama PRAMS Phase 8 Questionnaire #21b |
| Qn21e | Alabama PRAMS Phase 8 Questionnaire #21e |
| Qn21f | Alabama PRAMS Phase 8 Questionnaire #21f |
| Qn21g | Alabama PRAMS Phase 8 Questionnaire #21g |
| Qn21i | Alabama PRAMS Phase 8 Questionnaire #21i |
| Qn21j | Alabama PRAMS Phase 8 Questionnaire #21j |
| Qn21k | Alabama PRAMS Phase 8 Questionnaire #21k |
| RMSEA | Root Mean Square Error of Approximation |
| SE | Standard Error |
| SEM | Structural Equation Model |
| TLI | Tucker-Lewis Index |
References
- National Institute on Drug Abuse. Substance Use While Pregnant and Breastfeeding [Internet]. National Institute on Drug Abuse. 2020. Available from: https://nida.nih.gov/publications/research-reports/substance-use-in-women/substance-use-while-pregnant-breastfeeding.
- CDC. Substance Use During Pregnancy [Internet]. Maternal Infant Health. 2024. Available from: https://www.cdc.gov/maternal-infant-health/pregnancy-substance-abuse/index.html.
- Brandon AR. Psychosocial Interventions for Substance Use During Pregnancy. The Journal of Perinatal & Neonatal Nursing 2014, 28, 169–77.
- Des Marais S. Cultural Differences in Substance Use [Internet]. Psych Central. 2022. Available from: https://psychcentral.com/addictions/cultural-context-and-influences-on-substance-abuse.
- Hirai AH, Ko JY, Owens PL, Stocks C, Patrick SW. Neonatal Abstinence Syndrome and Maternal Opioid-Related Diagnoses in the US, 2010-2017. JAMA 2021, 325, 146. [CrossRef] [PubMed]
- Le C, Coombs S. Substance Use Disorder Hurts Moms & Babies [Internet]. National Partnership for Women & Families. 2021. Available from: https://nationalpartnership.org/report/substance-use-disorder-hurts-moms-and-babies/.
- Thaddeus S, Maine D. Too far to walk: Maternal mortality in context. Social Science & Medicine 1994, 38, 1091–110.
- Keating EM, Sakita F, Mmbaga BT, Amiri I, Getrude Nkini, Rent S, et al. Three delays model applied to pediatric injury care seeking in Northern Tanzania: A mixed methods study. PLOS Global Public Health. PLOS Global Public Health 2022, 2, e0000657–7. [CrossRef] [PubMed]
- Elisa Garcia Gomez, Kitiezo Aggrey Igunza, Madewell ZJ, Akelo V, Onyango D, Shams El Arifeen, et al. Identifying delays in healthcare seeking and provision: The Three Delays-in-Healthcare and mortality among infants and children aged 1–59 months. PLOS global public health 2024, 4, e0002494–4. [CrossRef] [PubMed]
- Knight HE, Self A, Kennedy SH. Why Are Women Dying When They Reach Hospital on Time? A Systematic Review of the “Third Delay.” Young RC, editor. PLoS ONE 2013, 8, e63846.
- Wilson CA, Finch E, Kerr C, Shakespeare J. Alcohol, smoking, and other substance use in the perinatal period. BMJ [Internet]. 2020 May 11;369:m1627. Available from: https://www.bmj.com/content/369/bmj.m1627.
- Pomar EG, Berryhill J, Bhattacharyya S. Evaluating maternal drug use disparities, risk factors and outcomes in Northeast Arkansas: a pre, during, and post-COVID-19 pandemic analysis. BMC Public Health 2025, 25.
- M. Pielage, Hanan El Marroun, Odendaal HJ, Willemsen SP, Manon, Eric A.P. Steegers, et al. Alcohol exposure before and during pregnancy is associated with reduced fetal growth: the Safe Passage Study. BMC Medicine 2023, 21.
- Glanz K, Rimer B, Viswanath K. Health Behavior: Theory, Research, and Practice, 5th ed.; John Wiley & Sons; 2015.
- Jalali MS, Botticelli M, Hwang RC, Koh HK, McHugh RK. The opioid crisis: A contextual, social-ecological framework. Health Research Policy and Systems [Internet]. 2020 Aug 6;18(1):1–9. Available from: https://health-policy-systems.biomedcentral.com/articles/10.1186/s12961-020-00596-8.
- Save the Children. Applying the Three Delays Model: Improving access to care for newborns with danger signs [Internet]. 2013. Available from: https://www.healthynewbornnetwork.org/hnn-content/uploads/Applying-the-three-delays-model_Final.pdf.
- CDC. Polysubstance Use During Pregnancy [Internet]. Pregnancy. 2024. Available from: https://www.cdc.gov/pregnancy/during/polysubstance-use.html.
- Office USGA. Maternal Health: HHS Should Improve Assessment of Efforts to Address Worsening Outcomes | U.S. GAO [Internet]. www.gao.gov. 2024. Available from: https://www.gao.gov/products/gao-24-106271.
- Office on Women’s Health. Maternal Health | Office on Women’s Health [Internet]. OASH | Office on Women’s Health. 2022. Available from: https://womenshealth.gov/maternalhealth.
- World Health Organization. Maternal Health [Internet]. Who.int. World Health Organization; 2019. Available from: https://www.who.int/health-topics/maternal-health#tab=tab_1.
- Blanchin M, Guilleux A, Hardouin JB, Sébille V. Comparison of structural equation modelling, item response theory and Rasch measurement theory-based methods for response shift detection at item level: A simulation study. Statistical Methods in Medical Research 2019, 29, 096228021988457.
- Lu IRR, Thomas DR, Zumbo BD. Embedding IRT in Structural Equation Models: A Comparison With Regression Based on IRT Scores. Structural Equation Modeling: A Multidisciplinary Journal 2005, 12, 263–77. [CrossRef]
- Phommachanh S, Essink DR, Wright PE, Broerse JEW, Mayxay M. Maternal health literacy on mother and child health care: A community cluster survey in two southern provinces in Laos. Fischer F, editor. PLOS ONE 2021, 16, e0244181.
- Zhao Y, Segalowitz N, Voloshyn A, Chamoux E, Ryder AG. Language barriers to healthcare for linguistic minorities: The case of second language-specific health communication anxiety. Health Communication 2019, 36, 1–13.
- Yadav R, Zaman K, Mishra A, Reddy MM, Shankar P, Yadav P, et al. Health Seeking Behaviour and Healthcare Utilization in a Rural Cohort of North India. Healthcare 2022, 10, 757. [CrossRef] [PubMed]
- Harvey I, O’Brien M. Addressing Health Disparities Through Patient Education: The Development of Culturally-Tailored Health Education Materials at Puentes de Salud. Journal of Community Health Nursing 2011, 28, 181–9. [CrossRef] [PubMed]
Figure 1.
Multidimensional scaling of Qn21 items. Note: Distances represent the dissimilarity among items (1 – |correlation|). Items closer together in the two- dimensional space share stronger correlations, suggesting they may reflect similar underlying barriers to prenatal care.
Figure 1.
Multidimensional scaling of Qn21 items. Note: Distances represent the dissimilarity among items (1 – |correlation|). Items closer together in the two- dimensional space share stronger correlations, suggesting they may reflect similar underlying barriers to prenatal care.
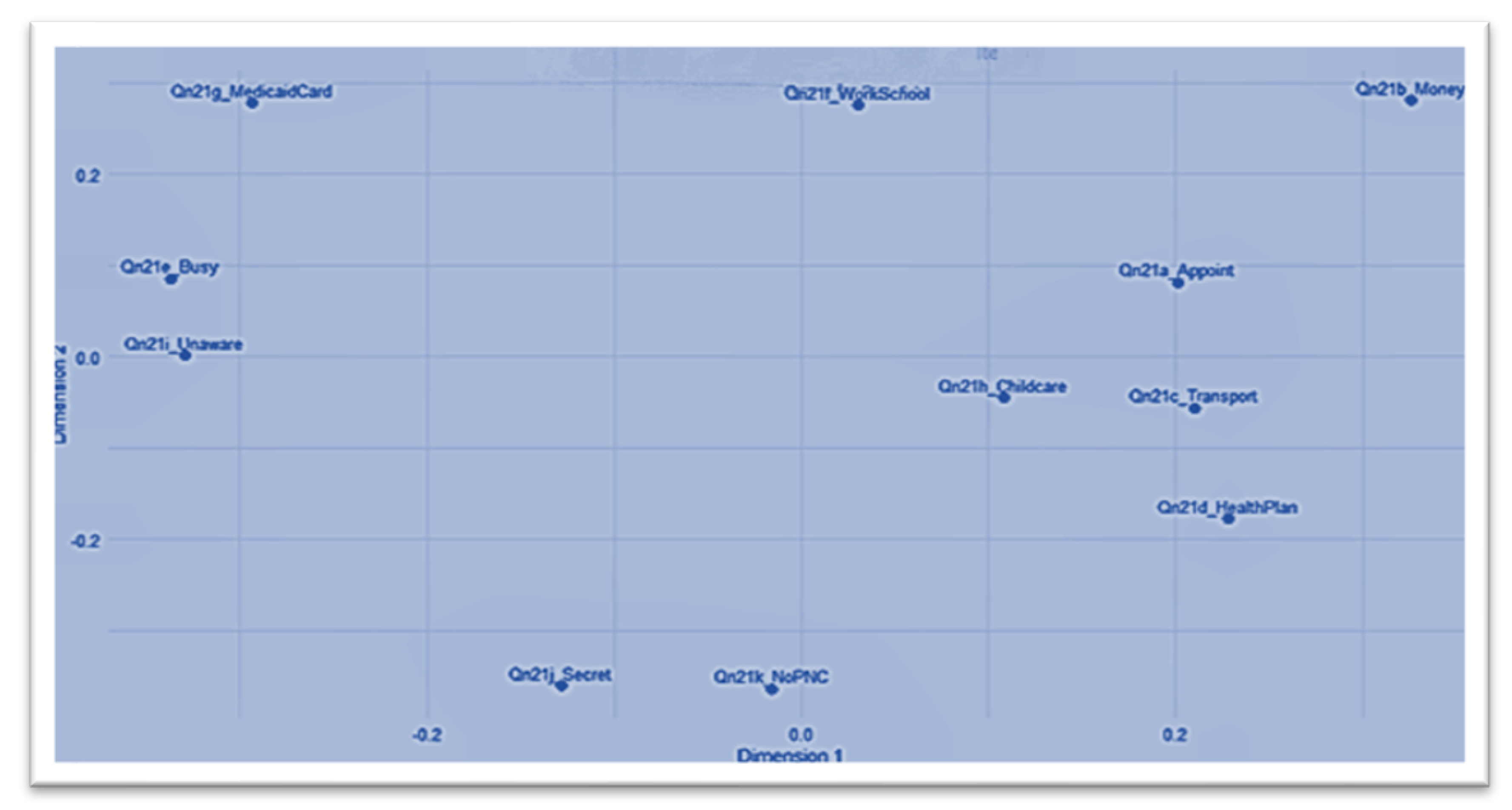
Figure 2.
Hierarchical clustering dendrogram of Qn21 items. Note: The dendrogram was created using an average linkage method and a dissimilarity matrix derived from 1−∣r∣. Items that fuse at lower heights share stronger correlations, showing they measure similar or overlapping barriers to prenatal care.
Figure 2.
Hierarchical clustering dendrogram of Qn21 items. Note: The dendrogram was created using an average linkage method and a dissimilarity matrix derived from 1−∣r∣. Items that fuse at lower heights share stronger correlations, showing they measure similar or overlapping barriers to prenatal care.
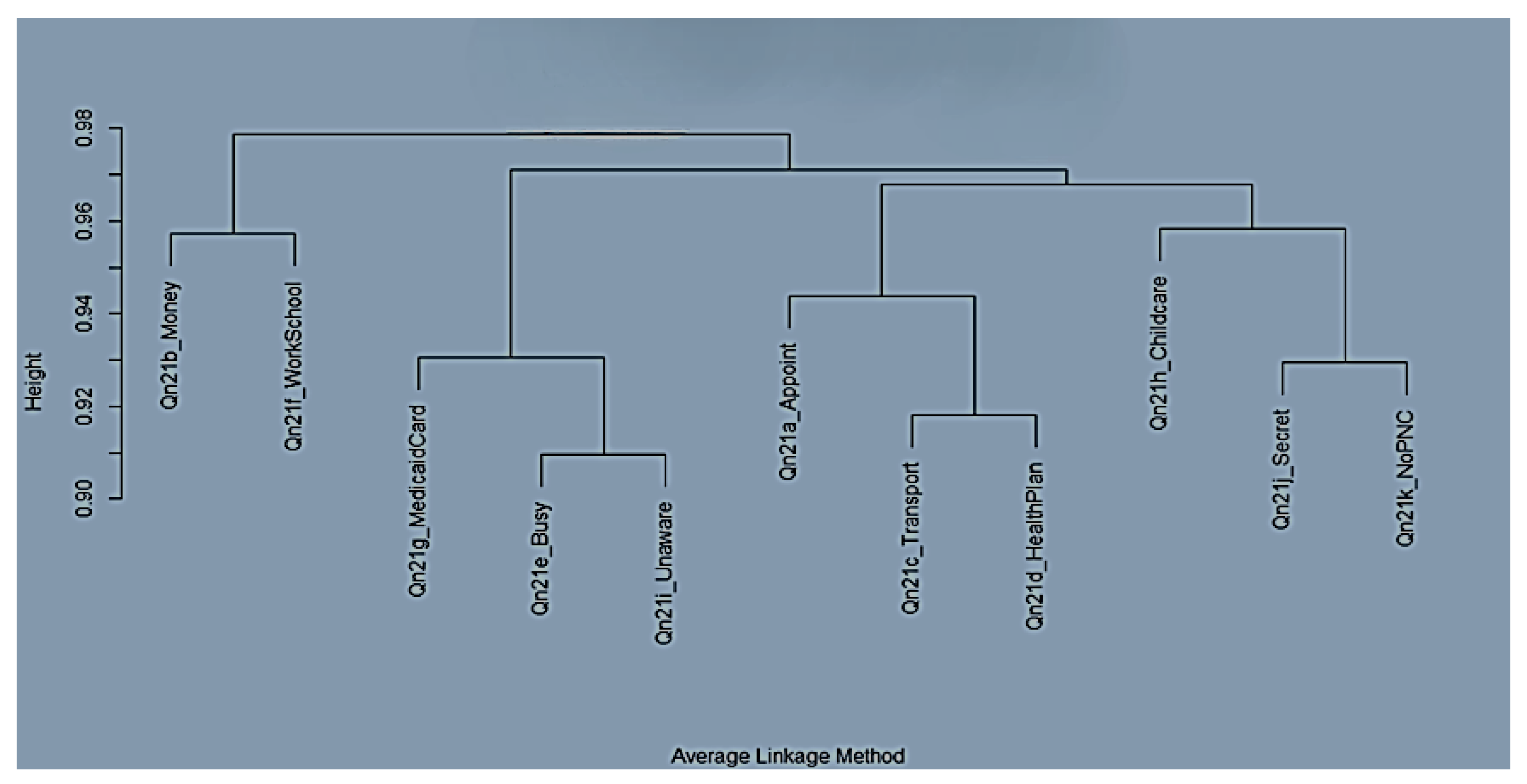
Figure 3.
Item characteristics curves for informational barriers.
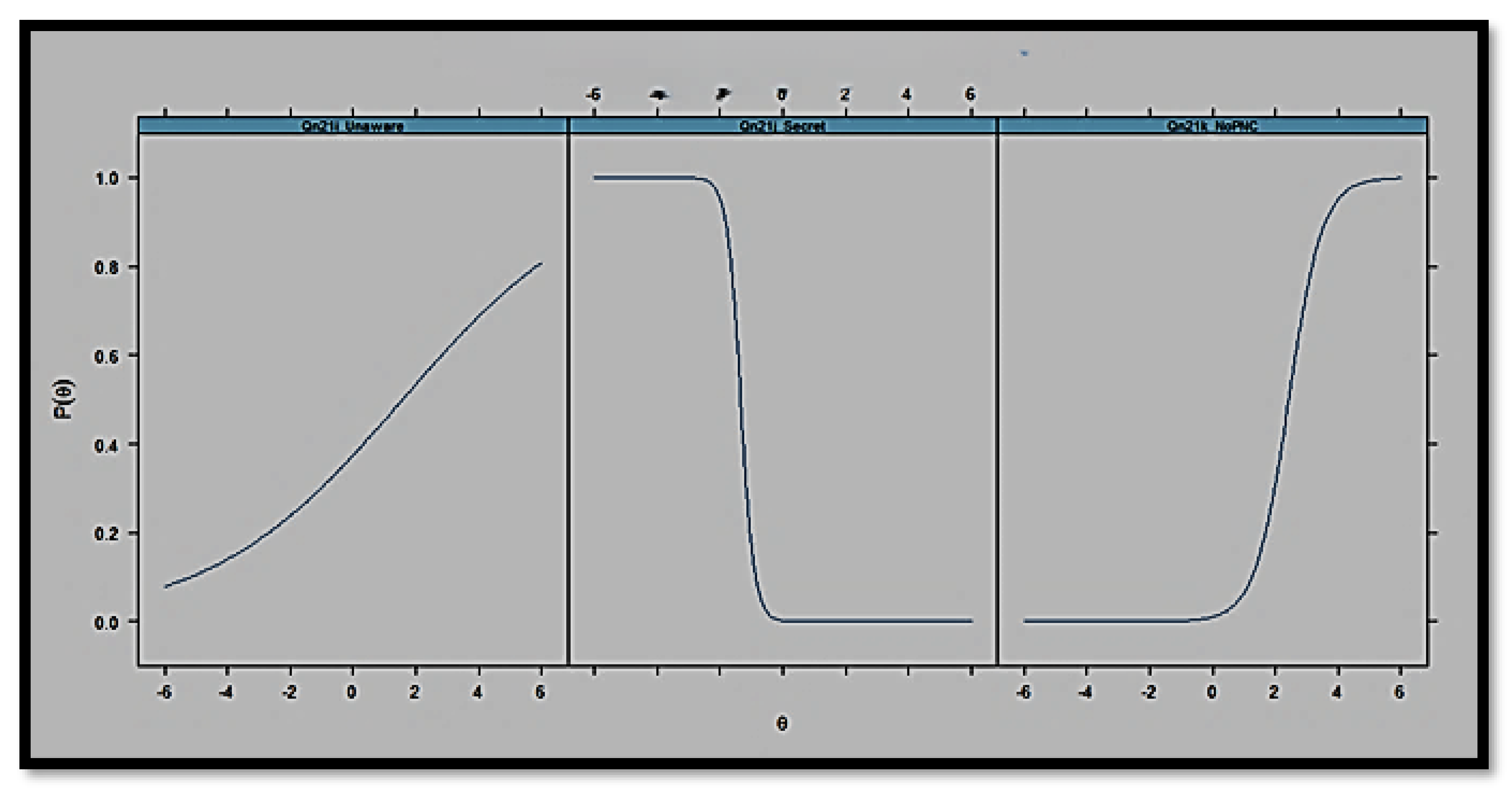

Table 1.
Operational definitions and measurement of study variables.
| Variable | Operational Definition | Coding/Measurement | Data Source |
|---|---|---|---|
| Maternal Health Status | Refers to overall maternal health and operationalized as good vs. poor | The composite variable from Qn22 items is coded as 1 = good and 2 = poor | ADPH PRAMS Phase 8 data set (2016–2021) |
| Substance Use | This refers to pregnant women’s smoking behavior during pregnancy | The binary variable from Qn42_CigaretteCategory is coded as 0 = non-smoker and 1 = smoker | ADPH PRAMS Phase 8 data set (2016–2021) |
| Structural Barriers | This refers to the financial constraints and work/school conflicts experienced when accessing care | The composite score of Qn21b_Money and Qn21f_WorkSchool | ADPH PRAMS Phase 8 data set (2016–2021) |
| Informational Barriers | This refers to deficits in awareness or information regarding prenatal care | This is the IRT-derived latent trait (theta_info) from Qn21i_Unaware, Qn21j_Secret, and Qn21k_NoPNC | ADPH PRAMS Phase 8 data set (2016–2021) |
| System Barriers | This refers to barriers related to navigating the healthcare system | This is the composite score of Qn21a_Appoint and Qn21d_HealthPlan | ADPH PRAMS Phase 8 data set (2016–2021) |
| Age Group | This refers to the age category of the respondent | This is a categorical variable, grouped as 15–19, 20–24, and above | ADPH PRAMS Phase 8 data set (2016–2021) |
| Race/Ethnicity | This refers to the self-reported race and ethnicity of respondents | This is a categorical variable coded as 1 = Non-Hispanic White, 2 = Non-Hispanic Black, and 3 = Hispanic | ADPH PRAMS Phase 8 data set (2016–2021) |
| Qn79_Income Category | This refers to the household income level reported by respondents (Qn79 items) | This is a categorical variable, with income categories ranging from $0 to $16,000, $16,001 to $20,000, $20,001 to $24,000, $24,001 to $28,000, and above | ADPH PRAMS Phase 8 data set (2016–2021) |
| BMI Category | This refers to the body mass index (BMI) classification provided by the Alabama Department of Public Health (ADPH) | This is a categorical variable, coded as 1 = Healthy Weight, 2 = Overweight, and 3 = Obesity | ADPH PRAMS Phase 8 data set (2016–2021) |
Note: The maternal health outcome is derived from Qn22 items, while substance use is based on Qn42_CigaretteCategory. Prenatal care barriers are grouped into structural, informational, and system domains in accordance with the Three Delays Model.
Table 2.
Descriptive statistics for key study variables.
| Variable | Category | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Maternal Health Status | Good (1) Poor (2) |
287 246 |
53.8 46.2 |
| Substance Use | Non-smoker Smoker |
321 212 |
60.2 39.8 |
| Qn21a_Appoint | 0 1 |
304 229 |
57.0 43.0 |
| Qn21b_Money | 0 1 |
356 177 |
66.8 33.2 |
| Qn21c_Transport | 0 1 |
468 65 |
87.8 12.2 |
| Qn21d_HealthPlan | 0 1 |
403 130 |
75.6 24.4 |
| Qn21e_Busy | 0 1 |
441 92 |
82.7 17.3 |
| Qn21f_WorkSchool | 0 1 |
482 51 |
90.4 9.6 |
| Qn21g_MedicaidCard | 0 1 |
387 146 |
72.6 27.4 |
| Qn21h_Childcare | 0 1 |
500 33 |
93.8 6.2 |
| Qn21i_Unaware | 0 1 |
371 162 |
69.6 30.4 |
| Qn21j_Secret | 0 1 |
480 53 |
90.1 9.9 |
| Qn21k_NoPNC | 0 1 |
512 21 |
96.1 3.9 |
| Qn79_IncomeCategory |
$0 to $16,000 $16,001 to $20,000 $20,001 to $24,000 $24,001 to $28,000 $28,001 to $32,000 $32,001 to $40,000 $40,001 to $48,000 $48,001 to $57,000 $57,001 to $60,000 $60,001 to $73,000 $73,001 to $85,000 $85,001 or more |
123 65 37 25 37 28 21 28 15 25 24 105 |
23.1 12.2 6.9 4.7 6.9 5.3 3.9 5.3 2.8 4.7 4.5 19.7 |
| BMI_Category | Healthy Weight Obesity Weight Overweight Weight Underweight Weight |
226 180 117 10 |
42.4 33.8 22.0 1.9 |
| Age_Group | 15–19 20–24 25–29 30–34 35–39 40 or older |
35 136 163 130 60 9 |
6.6 25.5 30.6 24.4 11.3 1.7 |
| Race_Ethnicity | Non-Hispanic White Non-Hispanic Black Hispanic Origin |
290 184 59 |
54.4 34.5 11.1 |
Note: Percentages are based on the complete-case sample (N = 533).
Table 3.
Logistic regression results predicting maternal health status.
| Predictor | OR | Std. Error | z value | p | 95% CI |
| (Intercept) | 0.753 | 0.448 | -0.631 | 0.528 | [0.310, - 1.812] |
| Smoker_statussmoker | 0.698 | 0.192 | -1.870 | 0.061 | [0.478, - 1.015] |
| Structural_barriers_new | 1.077 | 0.329 | 0.225 | 0.821 | [0.564,- 2.056] |
| System_barriers_new | 1.766 | 0.286 | 1.986 | 0.046 | [1.009, - 3.108] |
| Theta_info | 2.422 | 0.186 | 4.745 | < .001 | [1.710, - 3.568] |
| Age_Group20-24 | 0.953 | 0.408 | -0.117 | 0.906 | [0.428, -2.144] |
| Age_Group25-29 | 1.090 | 0.400 | 0.215 | 0.829 | [0.498, - 2.409] |
| Age_Group30-34 | 1.017 | 0.412 | 0.041 | 0.967 | [0.453, - 2.302] |
| Age_Group35-39 | 0.772 | 0.462 | -0.560 | 0.575 | [0.311, - 1.918] |
| Age_Group40 or older | 1.767 | 0.793 | 0.718 | 0.473 | [0.374, -8.960] |
| Race_EthnicityNon-Hispanic Black | 1.278 | 0.200 | 1.225 | 0.220 | [0.863, -1.894] |
| Race_EthnicityHispanic Origin | 1.258 | 0.301 | 0.764 | 0.445 | [0.696, -2.274] |
| Qn79_IncomeCategory16,001to20,000 | 0.692 | 0.329 | -1.118 | 0.263 | [0.361,- 1.315] |
| Qn79_IncomeCategory20,001 to24,000 | 0.964 | 0.392 | -0.093 | 0.926 | [0.445, - 2.087] |
| Qn79_IncomeCategory24,001to28,000 | 0.726 | 0.476 | -0.672 | 0.501 | [0.280, - 1.833] |
| Qn79_IncomeCategory28,001to32,000 | 0.890 | 0.400 | -0.292 | 0.770 | [0.405, - 1.951] |
| Qn79_IncomeCategory32,001to40,000 | 1.105 | 0.441 | 0.226 | 0.821 | [0.463, -2.640] |
| Qn79_IncomeCategory40,001to48,000 | 1.201 | 0.505 | 0.362 | 0.717 | [0.442, - 3.266] |
| Qn79_IncomeCategory48,001to57,000 | 0.830 | 0.439 | -0.425 | 0.671 | [0.347, -1.962] |
| Qn79_IncomeCategory57,001to60,000 | 0.7287383 | 0.590 | -0.540 | 0.590 | [0.220, -2.289] |
| Qn79_IncomeCategory60,001to73,000 | 1.040 | 0.458 | 0.082 | 0.935 | [0.419, - 2.560] |
| Qn79_IncomeCategory73,001to85,000 | 0.874 | 0.470 | -0.287 | 0.774 | [0.343, -2.200] |
| Qn79_IncomeCategory$85,001 or more | 0.883 | 0.280 | -0.443 | 0.660 | [0.509, - 1.529] |
| BMI_CategoryObesity Weight | 1.071 | 0.213 | 0.324 | 0.746 | [0.706, - 1.627] |
| BMI_CategoryOverweight Weight | 1.074 | 0.242 | 0.295 | 0.768 | [0.668, -1.726] |
| BMI_CategoryUnderweight Weight | 0.786 | 0.690 | -0.350 | 0.728 | [0.187, - 3.020] |
Note. Odds ratios (OR) are exponentiated coefficients from the logistic regression analysis predicting maternal health status (good vs. poor). System barriers (system_barriers_new) and the latent trait for informational barriers (θ, derived from the 2PL IRT model) were statistically significant predictors (p < .05). Smoker status did not reach statistical significance (p = .061), and neither structural barriers nor the demographic covariates were significantly associated with maternal health outcomes.
Table 4.
Bootstrapped mediation analysis of informational barriers as a mediator between substance use and maternal health.
Table 4.
Bootstrapped mediation analysis of informational barriers as a mediator between substance use and maternal health.
| Effect | Estimate | 95% CI | p-value |
|---|---|---|---|
| ACME (Average) | 0.03 | [0.01, 0.05] | .006 *** |
| ADE (Average) | -0.08 | [-0.16, 0.00] | .056 |
| Total Effect | -0.05 | [-0.13, 0.04] | .232 |
| Prop. Mediated (Average) | -0.44 | [-4.62, 4.34] | .238 |
Note. ACME = Average Causal Mediation Effect; ADE = Average Direct Effect. Asterisks indicate significance levels: *** p < .001.
Table 5.
Structural equation model parameter estimates and fit indices.
| Parameter | Estimate | Std. Error | z-value | p-value | 95% CI |
|---|---|---|---|---|---|
| Mediator Equation | |||||
| Smoker_status (a) | 0.143 | 0.058 | 2.453 | .014 | [0.029, 0.257] |
| Outcome Equation | |||||
| Theta_info (d) | 0.530 | 0.079 | 6.683 | < .001 | [0.375, 0.685] |
| Smoker_status (c′) | –0.199 | 0.111 | –1.797 | .072 | [–0.417, 0.019] |
| Defined Effects | |||||
| Indirect Effect (a*d) | 0.076 | 0.032 | 2.363 | .018 | [0.013, 0.139] |
| Total Effect | –0.123 | 0.112 | –1.106 | .269 | [–0.343, 0.097] |
Note. Confidence intervals are computed as Estimate ± 1.96 × Std. Error. ACME = Average Causal Mediation Effect (indirect effect); ADE = Average Direct Effect. In this model, substance use (smoker_status) significantly predicts informational barriers (a), and informational barriers significantly predict maternal health (d), yielding a significant indirect effect.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



