
Submitted:
27 March 2025
Posted:
28 March 2025
You are already at the latest version
Abstract
Double filtration plasmapheresis (DFPP) is a plasma exchange modality that allows selective clearance of high molecular weight proteins, potentially minimizing albumin loss and the need for volume replacement. Reports concerning DFPP use in dogs are scarce. This study evaluates the quantitative net loss of different plasma proteins fractions in an ex-vivo model using canine blood processed via DFPP. DFPP treatment with INUSpheresis processing 1.5, 2 and 3 plasma volumes (PV) was performed. Plasma proteins fractions were measured in the reservoir blood bag at baseline (pre-treatment) and in the effluent bag at the end of each target PV exchanged to calculate the net loss of selected plasma proteins. At 1.5 PV, net globulin and albumin loss was 41 and 25% respectively. At 3 PV, net globulin and albumin loss was 47 and 40%, respectively. Fibrinogen concentration were unmeasurable low in the reservoir blood bag after processing 1.5 PV. INUSpheresis allows selective plasma proteins removal, with sparing effect on albumin at 1.5 PV. Selectivity is however progressively reduced with incremental target PV. A description of five DFPP treatments in three dogs is additionally presented. Semi-selective protein removal was demonstrated also in-vivo, with a significantly lower percentage reduction of albumin compared to total globulin (P=0.01) and fibrinogen (P=0.007).
Keywords:
INUSpheresis
; extracorporeal apheresis
; immunoglobulin
; double-filtration plasmapheresis
; dog
1. Introduction
Double filtration plasmapheresis (DFPP) is a semi-selective plasma exchange modality that removes high-molecular weight substances including immunoglobulin, immune complexes and toxins, potentially minimizing the loss of albumin and the consequent need for substitution [1,2,3]. In DFPP, the plasma separator is responsible for extracting plasma across the membrane. The second filter is a plasma fractionator, that depending on the pore sizes of the membrane, allows the selective removal of plasma proteins based on their molecular weight. While the large molecular weight components are discarded, small molecular weight proteins including albumin are returned to the patient. In contrast to conventional plasma exchange, the volume of discarded plasma is significantly lower, hence reducing the overall volumes of the replacement fluids required and the risks associated with heterologous plasma transfusions [3].
Due to the efficient removal of immunoglobulins and immune complexes, a large number of immune-mediated diseases can be treated through DFPP, including myasthenia gravis, chronic inflammatory demyelinating polyneuropathy, polymyositis, lupus nephritis, rheumatoid arthritis, prevention of antibody-dependent xenograft rejection, and many other conditions [3,4]. In addition to this, its application in human medicine is also reported in diseases of metabolic origin such as familial hypercholesterolemia or lipoprotein hyperlipoproteinemia, reducing the risk for cardiovascular events and pro-inflammatory processes [4]. Removal of both coagulation and anticoagulation factors with large molecular weight is also expected, requiring coagulation monitoring for the risk of clinical bleeding [1,5].
INUSpheresis® is a specific type of DFPP platform developed for use in humans, that has shown therapeutic potential for the treatment of several metabolic and non-metabolic diseases, neuropathies, as well as for the removal of protein-bound environmental toxins. The pore size of the membrane of the plasma fractionator TKM58® showed a significant reduction in γ-globulin levels in human blood [5].
The aim of the present study is to evaluate ex-vivo the selective net loss of different plasma proteins in canine blood by DFPP treatment with INUSpheresis® and TKM58® processing from 1.5 up to 3 plasma volumes. The net percentage reduction of different plasma proteins was additionally assessed and compared evaluating in-vivo clinical treatments in three dogs.
2. Materials and Methods
2.1. Ex-Vivo Study
This study conducted at the University Veterinary Hospital of XXX assessed the effect of DFPP treatment with INUSpheresis® on canine blood. Canine blood (total volume 1683 ml) was obtained mixing four units of packed red blood cells (803 ml total), and four units of fresh frozen plasma (880 ml total). Packed red blood cells and fresh frozen plasma had been purchased from a commercial veterinary blood bank. Non-fractionated heparin (25000 units; Heparin sodium 5000 I.U./ml) was added to the solution to avoid any risk of clot formation within the reservoir. The commercially available extracorporeal circuit for INUSpheresis® with a standard plasma separator and a TKM58® as plasma fractionator were used for the study. Arterial and venous lines were connected to the canine blood reservoir bag. Normal saline 0.9% was used as the circuit priming solution. The priming volume of the circuit was 250 ml. A continuous DFPP treatment was performed processing incremental volume, respectively 1.5, 2 and 3 target plasma volumes (PV) over 180 minutes. Blood flow was set at 100 ml/min. Plasma filtration fraction across plasma separator was set fixed at 30%. Automatic flushing of the plasma fractionator with 150 ml of normal saline 0.9% were performed at each target PV time point to allow collection of the removed proteins and to eliminate possible fibrin clots within the plasma fractionator. The volume of each flush was accounted as part of the overall effluent volume (Figure 1).
Our reference values were the ones referred to the canine blood reservoir bag at the beginning of the session (baseline, pre-treatment). Blood and plasma samples were collected from the reservoir bag at baseline (pre-treatment), and serially from the effluent bag at each target PV exchange: 1.5, 2 and 3 PV. Samples were processed as follows: heparin whole blood was used to measure hematocrit and total proteins using in-house centrifuge and refractometer. Serum and plasma were obtained after centrifugation (1000 g x 10 min) and stored at -30°C until further analyses. All collected samples from the reservoir and the effluent bag were used for the following evaluations: serum total proteins using the Biuret assay; plasma fibrinogen concentrations using the Clauss method; and serum electrophoresis for the measurement of albumin, α1-globulin, α2-globulin, β1-globulin, β2-globulin and γ-globulin concentrations.
The fractional extraction of the plasma proteins of interest was calculated comparing the pre-treatment baseline values with those measured in the effluent bag, at each target PV exchanged. The net loss percentage was calculated using the following formula: [(reservoir bag solute concentration at baseline * total volume ml reservoir bag) – (effluent bag solute concentration * total volume ml effluent bag) / (reservoir bag solute concentration at baseline * total volume ml reservoir bag)] * 100.
2.2. Clinical Cases
We evaluated also retrospectively the results of three clinical cases, corresponding to a total of five DFPP treatment sessions performed between June 2024 and January 2025. For each patient, blood and plasma volumes were calculated as follows:
Blood volume (ml) = body weight kg * 0.9
Plasma volume (ml) = blood volume * (1- hematocrit value)
For each patient, pre-treatment and post-treatment concentrations of total proteins, albumin, total globulin, α1-globulin, α2-globulin, β1-globulin, β2-globulin, γ-globulin and fibrinogen were measured during all treatments. Samples were also collected from the effluent bag as part of standard clinical protocol at the end of each treatment.
The net percentage protein reduction was calculated using the following formula: (pre-treatment solute concentration – post-treatment solute concentration) / pre-treatment solute concentration.
The net albumin and total globulin loss expressed in g/kg was calculated as follows: (solute concentration effluent bag * total volume ml effluent bag) / patient body weight kg.
2.3. Statistics
Descriptive statistics were calculated; as data were non-normally distributed, they were expressed as median (min-max). Non-parametric statistics (Mann-Whitney-U test, Kruskal Wallis test with Dunn’s correction for multiple comparisons) were used to compare the net percentage reduction of different plasma proteins. Statistical analyses were performed with commercial software (Prism 10.4.1, GraphPad). Alpha was set a P <0.05.
3. Results
3.1. Ex-Vivo Study
Table 1, Table 2 and Table 3 summarize the laboratory data measured in the canine blood reservoir bag (baseline), as well as those obtained from the effluent bag at 1.5, 2 and 3 PV, respectively.
Baseline total plasma proteins in the reservoir bag were 63,9 gr. The effluent bag had 19.7 gr of total proteins removed at 1.5 PV, 25 gr removed at 2 PV and 27 gr removed at 3 PV. This was equivalent to a net total plasma protein loss percentage of 32% at 1.5 PV, 40% at 2 PV, and 42% at 3 PV.
The amount of albumin in the reservoir bag was 39 gr at baseline. The effluent bag had 9.7 gr of albumin removed at 1.5 PV, 13.6 gr removed at 2 PV, and 15.5 gr removed at 3 PV. This was equivalent to a net albumin loss percentage of 25% at 1.5 PV, 35% at 2 PV and 40% at 3 PV.
The amount of total globulin in the reservoir bag was 24.4 gr. The effluent bag had 10 gr removed at 1.5 PV, and 11.3 gr removed at both 2 PV and 3 PV. This corresponded to a net total globulin loss percentage of 41% at 1.5 PV, 47% at 2 PV and 47% at 3 PV.
The initial amount of γ-globulin in the reservoir bag was 3.2 gr. The effluent bag had 1.6 gr removed at 1.5 PV, and 1.8 gr removed at both 2 PV and 3 PV. This corresponded to a net γ-globulin loss percentage of 50% at 1.5 PV, 57% at 2 PV and 57% at 3 PV.
Baseline plasma fibrinogen in the reservoir bag was 2.2 gr. The effluent bag had 1.1 gr removed at 1.5 PV, 1.5 gr removed at 2 PV, and 1 gr removed at 3 PV. The net plasma fibrinogen loss percentage was 14% at 1.5 PV, 28% at 2 PV and 28% at 3 PV. Notably, fibrinogen concentration in the reservoir bag become unmeasurable low (<0.4 g/l) already after processing 1.5 PV.
3.2. In-Vivo Clinical Treatments
Case 1: A 24.5 kg male intact dog referred to the University Veterinary Hospital XXX for acute immune-mediated hemolytic anemia and glomerulonephritis underwent DFPP with INUSpheresis®. The estimated blood and plasma volumes were 2205 ml and 1725 ml, respectively. Protein percentage reduction was calculated, as previously stated.
A continuous DFPP treatment with INUSpheresis® and TKM58® as plasma fractionator was performed processing 1.7 PV (3000 ml) over 120 minutes. The circuit was primed with packed red blood cells and normal saline. Blood flow was set between 50-110 ml/min. Plasma filtration fraction across plasma separator was set fixed at 30%. Five automatic flushes of the plasma fractionator with 150 ml each of normal saline 0.9% were performed during the session. Net plasma volume removed was 220 ml. Replacement was performed with 220 ml of fresh frozen plasma during the treatment. Lactated Ringer was used as rinse-back at the end of the session.
Pre-treatment proteins values were as follows: total protein 33 g/l, albumin 20.4 g/l, total globulin 12.6 g/l, γ-globulin 2 g/l, fibrinogen 1.1 g/l. Plasma protein concentrations post-treatment were the followings: total protein 15 g/l, albumin 9.8 g/l, total globulin 5.2 g/l, γ-globulin 0.6 g/l, fibrinogen 0.27 g/l. The net percentage reduction was 54% for total proteins, 52% for albumin, 59% for total globulins, 70% for γ-globulins, and for 75% fibrinogen, respectively. The net albumin and total globulin loss was 1.2 g/kg and 0.8 g/kg, respectively.
Case 2: A 45.5 kg male intact dog referred to the University Veterinary Hospital XXX for acute azotemia and glomerulonephritis underwent DFPP with INUSpheresis®. The estimated blood and plasma volumes were 4095 ml and 2839 ml, respectively. A continuous DFPP treatment with INUSpheresis® and TKM58® as plasma fractionator was performed processing 1.5 PV (4200 ml) over 120 minutes. Net plasma volume removed was 600 ml. Replacement was performed with 700 ml of fresh frozen plasma during the treatment. Lactated Ringer was used as rinse-back at the end of the session.
Pre-treatment proteins values were as follows: total protein 50.8 g/l, albumin 19.8 g/l, total globulin 31.0 g/l, γ-globulin 2.2 g/l, fibrinogen 6.1 g/l. Plasma protein concentrations post-treatment were the followings: total protein 31.0 g/l, albumin 16.8 g/l, total globulin 14.8 g/l, γ-globulin 1.6 g/l, fibrinogen 1.5 g/l. The net percentage reduction was 38% for total proteins, 15% for albumin, 52% for total globulins, 27% for γ-globulins, and for 75% fibrinogen, respectively. The net albumin and total globulin loss was 0.9 g/kg and 2 g/kg, respectively.
At 24 hours a second DFPP treatment processing 1.5 PV was again performed. Net plasma volume removed was 120 ml. Replacement was performed with 220 ml of fresh frozen plasma during the treatment. Lactated Ringer was used as rinse-back at the end of the session. Pre-treatment proteins values were as follows: total protein 44 g/l, albumin 20.9 g/l, total globulin 23.2. g/l, γ-globulin 1.9 g/l, fibrinogen 4.6 g/l. Plasma protein concentrations post-treatment were the followings: total protein 23.4 g/l, albumin 14.1 g/l, total globulin 9.3 g/l, γ-globulin 0.8 g/l, fibrinogen 0.6 g/l. The net percentage reduction was 47% for total proteins, 32% for albumin, 60% for total globulins, 58% for γ-globulins, and for 87% fibrinogen, respectively. The net albumin and total globulin loss was 0.6 g/kg and 0.9 g/kg, respectively.
Case 3: A 19.7 kg male intact dog referred to the University Veterinary Hospital XXX for acute immune-mediated hemolytic anemia underwent DFPP with INUSpheresis®. The estimated blood and plasma volumes were 1773 ml and 1008 ml, respectively. A continuous DFPP treatment with INUSpheresis® and TKM58® as plasma fractionator was performed processing 2 PV (2100 ml) over 120 minutes. Net plasma volume removed was 50 ml. Replacement was performed with 220 ml of fresh frozen plasma during the treatment. Lactated Ringer was used as rinse-back at the end of the session.
Pre-treatment proteins values were as follows: total protein 36 g/l, albumin 18.2 g/l, total globulin 17.8. g/l, γ-globulin 1.9 g/l, fibrinogen 3.1 g/l. Plasma protein concentrations post-treatment were the followings: total protein 19 g/l, albumin 11.2 g/l, total globulin 7.8 g/l, γ-globulin 1.2 g/l, fibrinogen 0.4 g/l. The net percentage reduction was 47% for total proteins, 38% for albumin, 56% for total globulins, 37% for γ-globulins, and for 87% fibrinogen, respectively. The net albumin and total globulin loss was 0.5 g/kg and 0.77 g/kg, respectively.
At 24 hours a second DFPP treatment processing 1.5 PV was again performed. Net plasma volume removed was 70 ml. Replacement was performed with 150 ml of fresh frozen plasma during the treatment. Lactated Ringer was used as rinse-back at the end of the session. Pretreatment proteins values were as follows: total protein 29 g/l, albumin 15.7 g/l, total globulin 13.3. g/l, γ-globulin 1.7 g/l, fibrinogen 3 g/l. Plasma protein concentrations post-treatment were the followings: total protein 16 g/l, albumin 10 g/l, total globulin 5.9 g/l, γ-globulin 0.6 g/l, fibrinogen 0.4 g/l. The net percentage reduction was 45% for total proteins, 36% for albumin, 64% for total globulins, 55% for γ-globulins, and for 87% fibrinogen, respectively. The net albumin and total globulin loss was 0.96 g/kg and 1 g/kg, respectively.
The median processed PV in the five treatment sessions described was 1.6. The median values for the net percentage proteins reductions documented for the reported five in-vivo clinical treatments were the following: 36% (15-52) albumin; 56% (52-60) total globulin; 58% (27-70) γ-globulin; 87% (75-87) fibrinogen. The net percentage reduction of albumin resulted significantly lower than the one documented for total globulin (P=0.01) and for fibrinogen (P=0.007) (Figure 2 and 3). No difference was detected in the comparison between the net percentage reduction of total globulin vs. γ-globulin (P=0.9). No difference was detected between the net percentage reduction of albumin vs. γ-globulin (P=0.2).
The median values for the net amount of albumin and globulin loss expressed in g/kg were 0.9 g/kg (0.5-1.2) and 0.9 g/kg (0.8-2), respectively.
4. Discussion
Double filtration plasmapheresis is a recently developed apheretic technique used in human medicine to treat several pathological conditions, but its clinical application in dogs is scarce (1,2,3). There are still knowledge gaps regarding the efficiency of removal of the different plasma components, as well as regarding optimal DFPP protocols in human and veterinary patients [3,7,8].
Our study aimed at measuring the ex-vivo net loss percentage of different plasma proteins in canine blood by continuous DFPP treatment with INUSpheresis® with a TKM58® as plasma fractionator, processing from 1.5 up to 3 plasma volumes.
The results of this study highlight that the removal of plasma proteins by INUSpheresis® is semi-selective, showing a significant sparing effect on albumin, compared to conventional therapeutic plasma exchange at 1.5 PV. Moreover, protein removal seems to be based not only on molecular size, but also on additional factors including adsorption within the filter and dilution by automated flushes.
DFPP should minimize albumin loss and the subsequent need for substitution fluids, due to the small molecular weight of this protein. Our results show good albumin sparing effect at 1.5 target PV, since for a 50% γ-globulin reduction, the documented net albumin loss was only 25%. Such selective protein removal at 1.5 PV, which represents a conventional target volume of exchange for clinical use of DFPP, highlights the advantage of DFPP compared to conventional therapeutic plasma exchange, where unselective protein removal occurs and the whole volume of plasma extracted has to be fully replaced [3,9]. The albumin sparing reduces substantially the requirement for replacement solutions, minimizing costs and the risks for plasma-transfusion-related complications [3,7,9].
Nonetheless, such selectivity in plasma protein removal decreased with incremental target PV, as net albumin loss reached 40% at 3 PV. The automated saline flushes performed at each target PV time point might have been responsible for the progressive albumin loss alongside incremental PV exchanged, as the volume of the plasma fractionator was removed with each flush instead of being returned to the patient.
Globulin removal was efficiently performed: total globulins and γ-globulins net loss percentage was 41 and 50% at 1.5 target PV, respectively. Globulins are large-size proteins that are directly cleared by the plasma fractionator and subsequently discarded. In humans, a filter-dependent effect on immunoglobulin clearance and protein patterns has been demonstrated following DFPP, with immunoglobulin reduction by 50% using INUSpheresis® with TKM58® [4], similarly to our results. Nonetheless, a decrease in globulin excretion ratio was observed with incremental target PV exchanged, with net γ-globulin removal raising only from 50% at 1.5 PV to 57% at both 2 and 3 target PV. The observed reduction in globulin clearance with increasing PV exchanges can be easily justified with membrane clogging lowering plasma fractionator efficiency. Hence, given the progressive loss of membrane selectivity and reduced globulin clearance with increasing PV exchanges, the use of >1.5 target PV does not seem clinically recommended.
A finding of notice was in regards to fibrinogen concentration. Fibrinogen is a large-size intravascular protein that is expected to be extensively cleared during DFPP treatment [2,6]. Post-treatment ex-vivo fibrinogen concentration was unmeasurable low (<0.4 g/l) already after 1.5 PV exchanged (Table 1). Interestingly, based on the amount of fibrinogen detected in the effluent bag, the net loss fibrinogen percentage directly related to filtration and effluent removal ranged only between 14 to 28% from 1.5 to 3 PV. This highlights the potential role for additional mechanisms contributing to fibrinogen loss other than selected size-based protein removal in the plasma fractionator. In this regard, it is possible that part of the detected fibrinogen loss was due to its adsorption within the plasma fractionator. This seems in accordance with the role of fibrinogen as being directly involved into filter clogging with fibrin clots. Fibrinogen removal after DFPP might positively affect hemostasis in specific conditions where hyperfibrinogenemia and thrombinemia pose patients at risk for hypercoagulation and thrombotic events (e.g. nephrotic syndrome) [9]. Nonetheless, coagulation parameters and transfusion requirements should be closely monitored after apheresis, especially in patients at higher bleeding-risk or if invasive procedures are planned [10]. Previous authors have speculated additional clearance factors in DFPP independent of the protein size alone [8].
The circuit used for INUSpheresis® has a volume of 250 ml. The addition of such volume to the plasma component of the canine reservoir bag (880 ml) used for the ex-vivo study caused roughly 30% dilutional effect on plasma proteins concentration after treatment.
There are some limitations to be acknowledged when interpreting the results of our study. This was an ex-vivo study; hence, generalization of the clinical results is possible only to a limited extent. No proteomic analysis of protein absorption by the plasma fractionator membrane was performed to characterize those more subjected to potential filter adsorption. Moreover, the study relied on a mono-compartment model, hence the role of physiologic proteins redistribution occurring during DFPP treatment in-vivo cannot be assess. However, considering that normal plasma proteins redistribution is a slow process occurring at a rate of 1-3%/h [11,12], our ex-vivo results are likely mirroring those in-vivo.
Given that the aim of the study was to evaluate filter selectivity at incremental PV exchanged, duplicate analyses were not deemed necessary. Finally, the clinical implications of the present results are difficult to predict. For example, although the documented net loss of fibrinogen was significant already after 1.5 PV exchanged, the risk for clinical bleeding or need for blood products transfusions has to be assessed in clinical studies. Similarly, the actual sparing effect of DFPP on the need for plasma substitution in the clinical setting cannot be tested.
Based on the clinical treatments results here presented, DFPP with TKM58® enabled to obtain a differential semi-selective plasma proteins removal also in-vivo. After a median of 1.6 PV processed in the five DFPP sessions described, the median albumin reduction was 36%, resulting significantly lower from the median reduction of total globulin (56%) and the one documented for fibrinogen (87%). The albumin sparing effect was consistent in all clinical treatment. The total albumin loss normalized to body weight averaged 0.9 g/kg, still highlighting the need of possible replacement in case of pre-existing hypoalbuminemia. In this regard, measuring albumin concentration in the effluent bag alongside the discarded plasma volume can be easily used to estimate the amount of post DFPP albumin replacement. Fibrinogen removal was high also in-vivo, requiring close monitoring of coagulation and bleeding risk in the immediate post-treatment period. Interestingly, in the five DFPP sessions analyzed, no difference was documented between total globulin vs. γ-globulin percentage reduction. This might have been due to the low number of treatments analyzed. It might be also possible that globulin removal by TKM58® in canine blood is not selective for the different globulin fraction.
The retrospective nature of our clinical analysis prevented the standardization of the DFPP procedure. In this regard, the plasma volume processed, as well as the volume of discarded plasma were variable, and mainly affected by the number of automated flushes imposed by the machine. This can also have affected the amount of protein recovery in the effluent after treatments. The replacement volume varied based on hemodynamic stability and bleeding tendencies of enrolled patients. Finally, the number of described sessions is low to allow meaningful statistical analysis and to reach definitive clinical conclusions.
In conclusion, INUSpheresis® allows an effective and selective plasma proteins removal in canine blood. Particularly at 1.5 target PV, large-size proteins are efficiently removed through selective plasma filtration, while albumin loss is reduced compared to conventional therapeutic plasma exchange. Both selectivity and efficiency of globulin removal are progressively reduced with increasing plasma volumes exchanged, pointing out the clinical advantage of DFPP mainly when conventional target PV are processed. Other mechanisms including adsorption within the filter and circuit dilution play an additional role in further net protein loss after treatments. DFPP seems to promote a semi-selective protein removal also in-vivo in dogs. The need for substitution fluids, as well as the clinical consequences of albumin and fibrinogen loss in dogs undergoing DFPP treatment have to be addressed in future clinical studies.
Author Contributions
Conceptualization, A.V.; methodology, A.V., R.T., C.I., L.N.; formal analysis, A.V., R.T., C.I., L.N.; investigation, A.V., R.T., C.I., L.N.; resources, A.V., C.I.; data curation, A.V., R.T., C.I.; writing—original draft preparation, R.T., C.I.; writing—review and editing, A.V., R.T., C.I., L.N..; visualization, A.V.; supervision, A.V.; project administration, A.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were not required for this study. Data reported for the in-vivo treatments were routinely collected for prescribed diagnostic and monitoring purposes and subsequently made available for this study.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| DFPP | Double filtration plasmapheresis |
| PV | Plasma volumes |
References
- Perondi, F.; Brovida, C.; Ceccherini, G.; Guidi, G.; Lippi, I. Double filtration plasmapheresis in the treatment of hyperprotinemia in dogs affected by Leishmania infantum. J Vet Sci. 2018, 19, 472-476. [CrossRef]
- Lin, S.; Yeh, J.;Le, C.; Chiu, H. Clearance of Fibrinogen and von Willebrand Factor in Serial Double-Filtration Plasmapheresis. J Clin Apher. 2003, 18, 67-70. [CrossRef]
- Hirano, R.; Namazuda, K.; Hirata, N. Double filtration plasmapheresis: Review of current clinical applications. Ther Apher Dial. 2021, 25, 145-151. [CrossRef]
- Scholkmann, F.; Tsenkova, R. Changes in Water Properties in Human Tissue after Double Filtration Plasmapheresis—A Case Study. Molecules 2022, 27:3947. [CrossRef]
- Yin, X.; Takov, K.; Straube, R. et al. Precision medicine approach for cardiometabolic risk factors in therapeutic apheresis. Horm Metab Res. 2022, 54, 238-249. [CrossRef]
- Pan, Y.S.; Huang, T.; Lin, Y.C. et al. The effects of double-filtration plasmapheresis on coagulation profiles and the risk of bleeding. J Formos Med Assoc. 2024, 123, 899-903. [CrossRef]
- Jagdish, K.; Jacob, S.; Varughese, S. et al. Effect of Double Filtration Plasmapheresis on Various Plasma Components and Patient Safety: A Prospective Observational Cohort Study. Indian J Nephrol. 2017, 27, 377-383. [CrossRef]
- Xu, X.; Liu, X.; Liu, A. et al. Proteomic analysis of the rest filtered protein after double filtration plasmapheresis. Int J Clin Exp Med. 2018, 11, 9715-9721.
- Daga Ruiz, D.; Fonseca San Miguel, F.; Gonzàles de Molina, F.J. et al. Plasmapheresis and other extracorporeal filtration techniques in critical patients. Med Intensiva 2017, 41, 174-187.
- Kolesnyk, M.O., Lapchyns’ka, I.; Dudar, O.; Velychko, M.B. The effect of therapeutic plasmapheresis on the hemostatic system of patients with chronic glomerulonephritis and the nephrotic syndrome. Lik Sprava 1993, 2, 79-81.
- Marlu, R.; Bennani, H.N.; Seyve, L. et al. Comparison of three modalities of plasmapheresis on coagulation: Centrifugal, single-membrane filtration, and double-filtration plasmapheresis. J Clin Apher 2021, 36, 408-419. [CrossRef]
- Noiri, E.; Hanafusa, N. The concise manual of apheresis therapy. Springer, Japan, 2014; pp. 141- 152.
Figure 1.
The extracorporeal circulation circuit of double filtration plasmapheresis.
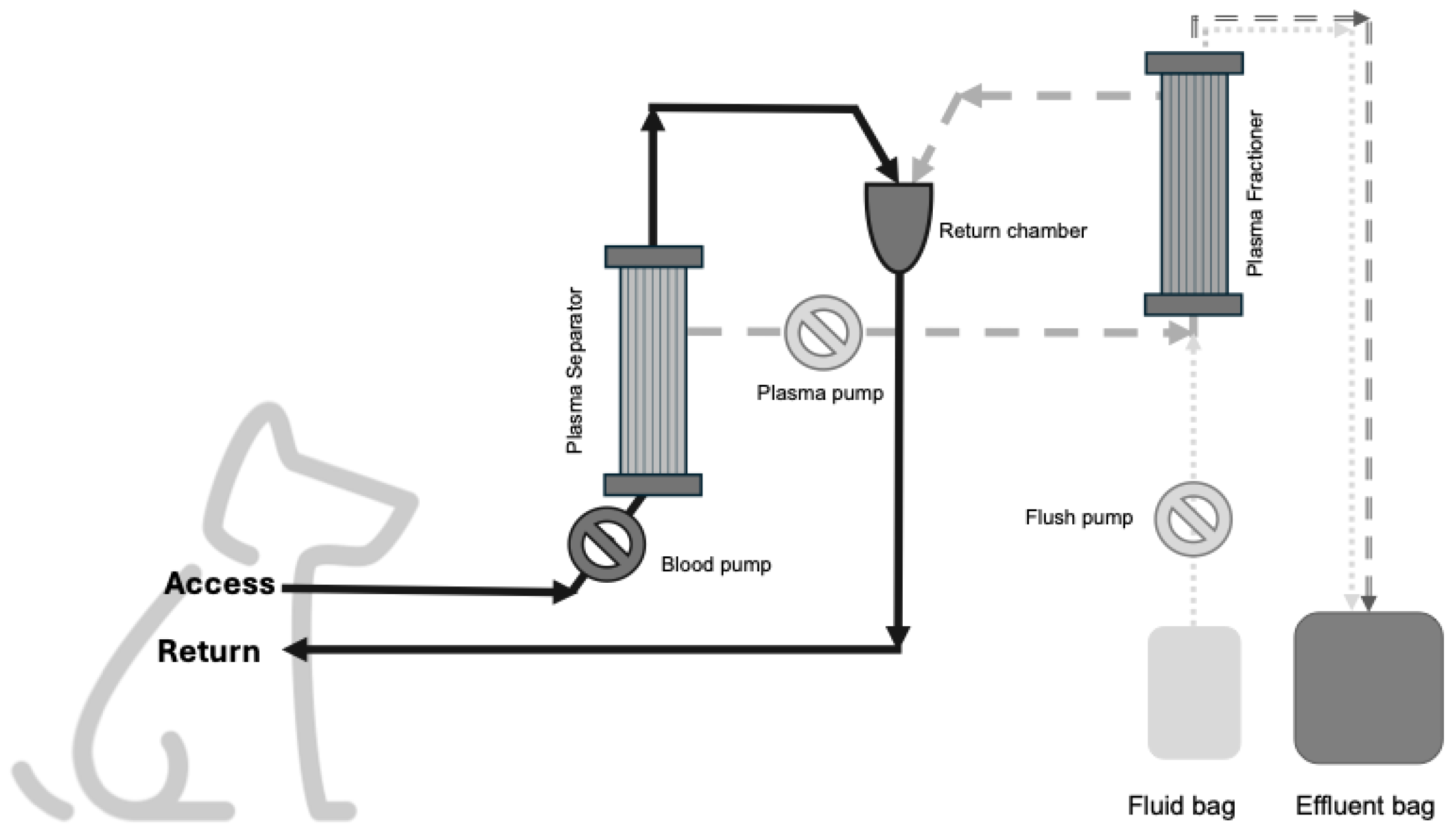
Figure 2.
Box and whisker plot comparison of the median net percentage protein reduction of albumin vs. total globulin from five double filtration plasmapheresis sessions in three dogs. The central line represents the median, the boxes represent the interquartile range and the whiskers represent the minimum and maximum values. Albumin net percentage reduction resulted significantly lower compared to globulin net percentage reduction (P=0.01) by Mann-Whitney U test.
Figure 2.
Box and whisker plot comparison of the median net percentage protein reduction of albumin vs. total globulin from five double filtration plasmapheresis sessions in three dogs. The central line represents the median, the boxes represent the interquartile range and the whiskers represent the minimum and maximum values. Albumin net percentage reduction resulted significantly lower compared to globulin net percentage reduction (P=0.01) by Mann-Whitney U test.
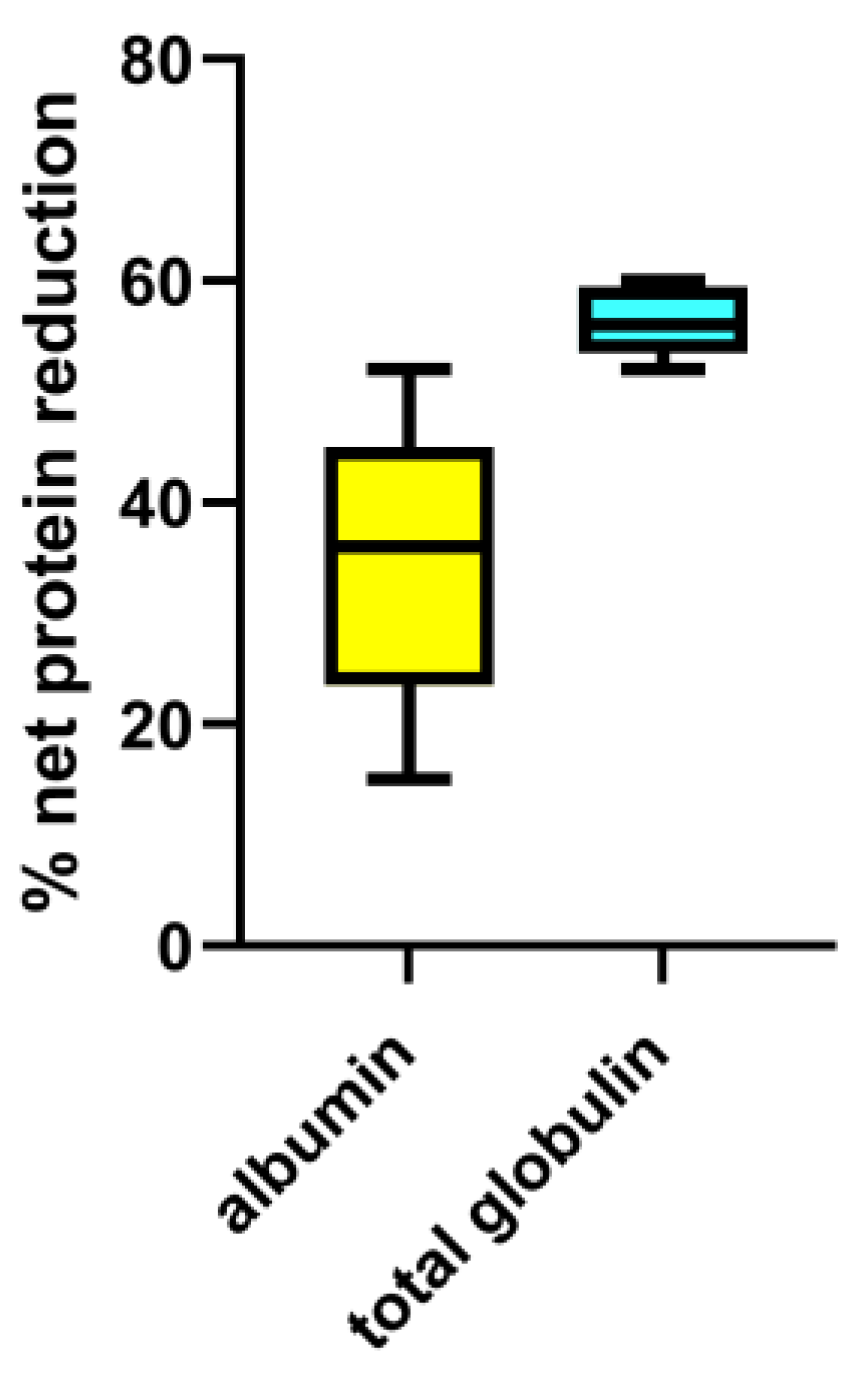
Figure 3.
Box and whisker plot comparison of the median net percentage protein reduction of albumin vs. fibrinogen from five double filtration plasmapheresis sessions in three dogs. The central line represents the median, the boxes represent the interquartile range and the whiskers represent the minimum and maximum values. Albumin net percentage reduction resulted significantly lower compared to fibrinogen net percentage reduction (P=0.01) by Mann-Whitney U test.
Figure 3.
Box and whisker plot comparison of the median net percentage protein reduction of albumin vs. fibrinogen from five double filtration plasmapheresis sessions in three dogs. The central line represents the median, the boxes represent the interquartile range and the whiskers represent the minimum and maximum values. Albumin net percentage reduction resulted significantly lower compared to fibrinogen net percentage reduction (P=0.01) by Mann-Whitney U test.
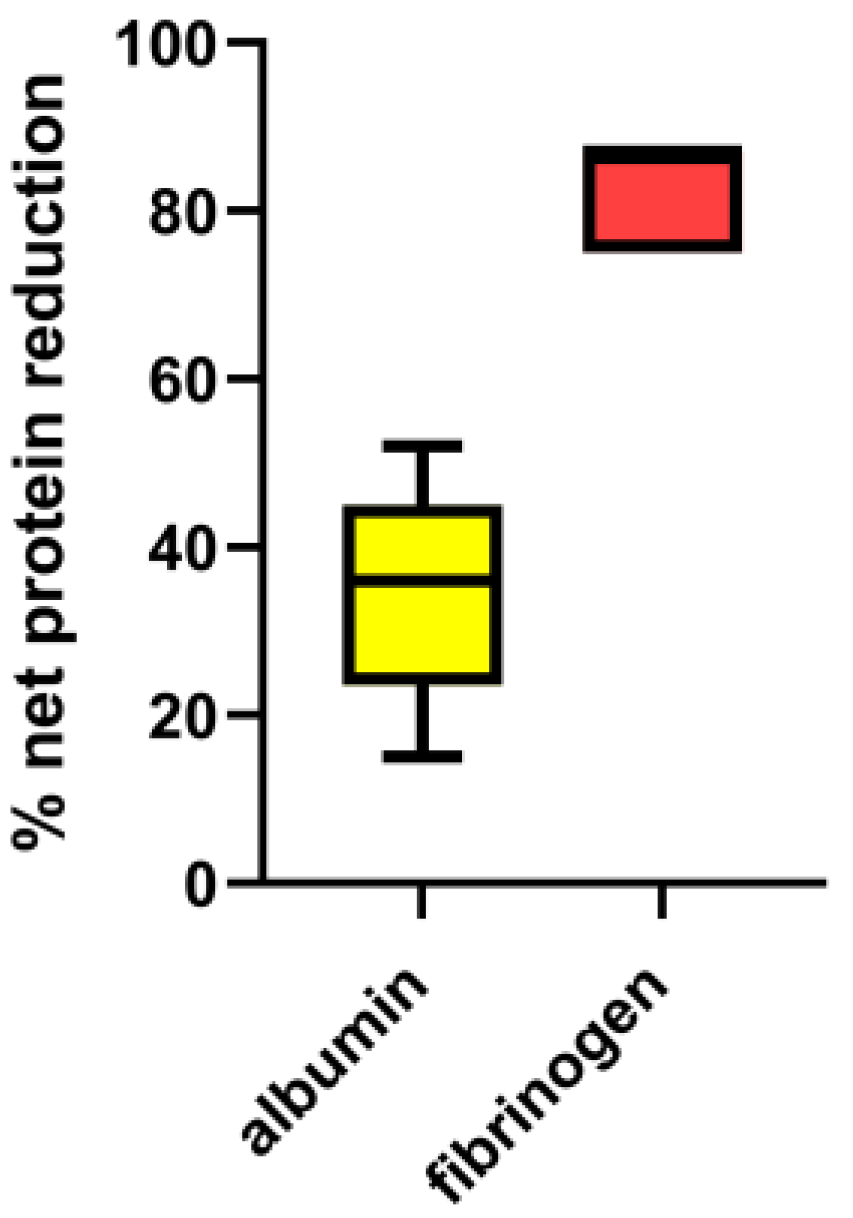

Table 1.
Serum total proteins, albumin, total and γ-globulins and plasma fibrinogen concentrations during a 180-min-session of double filtration plasmapheresis in a canine blood reservoir bag and in the effluent bag at 1.5, 2 and 3 target plasma volumes.
Table 1.
Serum total proteins, albumin, total and γ-globulins and plasma fibrinogen concentrations during a 180-min-session of double filtration plasmapheresis in a canine blood reservoir bag and in the effluent bag at 1.5, 2 and 3 target plasma volumes.
| PV processed | Total proteins (g/l) | Albumin (g/l) | Total globulins (g/l) | γ-globulins (g/l) | Fibrinogen (g/l) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| RB | EF | RB | EF | RB | EF | RB | EF | RB | EF | |
| Baseline | 38 | n.a. | 23.2 | n.a. | 14.5 | n.a. | 1.9 | n.a. | 1.3 | n.a. |
| 1.5 PV | 16 | 79 | 11.2 | 38.6 | 5.2 | 40.3 | 0.7 | 6.2 | < 0.4 | 1.1 |
| 2 PV | 11 | 61 | 7.5 | 33.3 | 3.8 | 27.6 | 0.5 | 4.3 | < 0.4 | 1.5 |
| 3 PV | 9 | 44 | 5.6 | 25.2 | 3.1 | 18.4 | 0.5 | 3.0 | <0.4 | 1.0 |
1 PV, plasma volume; RB, reservoir bag; EF, effluent bag; n.a., not applicable.
Table 2.
Serum electrophoresis for different globulin fractions: α1-globulin, α2-globulin, β1-globulin, β2-globulin and γ-globulin concentrations during a 180-min-session of double filtration plasmapheresis in a canine blood reservoir bag and in the effluent bag at 1.5, 2 and 3 target plasma volumes.
Table 2.
Serum electrophoresis for different globulin fractions: α1-globulin, α2-globulin, β1-globulin, β2-globulin and γ-globulin concentrations during a 180-min-session of double filtration plasmapheresis in a canine blood reservoir bag and in the effluent bag at 1.5, 2 and 3 target plasma volumes.
| PV processed | α1-globulin (g/l) | α2-globulin (g/l) | β1-globulin (g/l) | β2-globulin (g/l) | γ-globulin (g/l) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| RB | EF | RB | EF | RB | EF | RB | EF | RB | EF | |
| Baseline | 1.7 | n.a. | 4.4 | n.a. | 2.8 | n.a. | 3.7 | n.a. | 1.9 | n.a. |
| 1.5 PV | 0.9 | 2.5 | 1.3 | 15.8 | 1.0 | 7.0 | 1.3 | 8.8 | 0.7 | 6.2 |
| 2 PV | 0.6 | 2.4 | 0.9 | 10.1 | 1.0 | 4.7 | 0.8 | 6.1 | 0.5 | 4.3 |
| 3 PV | 0.4 | 1.9 | 0.8 | 6.1 | 0.8 | 3.0 | 0.6 | 4.4 | 0.5 | 3.0 |
1 PV, plasma volume; RB, reservoir bag; EF, effluent bag; n.a., not applicable.
Table 3.
Total amount in grams (gr) of serum total protein, albumin, fibrinogen, total globulins and γ-globulin concentrations in a canine blood reservoir bag and in the effluent bag at 1.5, 2 and 3 target plasma volumes and net percentage loss (%) during a 180-min-session of double filtration plasmapheresis.
Table 3.
Total amount in grams (gr) of serum total protein, albumin, fibrinogen, total globulins and γ-globulin concentrations in a canine blood reservoir bag and in the effluent bag at 1.5, 2 and 3 target plasma volumes and net percentage loss (%) during a 180-min-session of double filtration plasmapheresis.
| PV processed | Total protein | Net protein loss (%) | Total albumin | Net albumin loss (%) | Total globulin | Net total globulin loss (%) | γ-globulin | Net γ-globulin loss (%) | Fibrinogen | Net fibrinogen loss (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RB | EF | RB | EB | RB | EB | RB | EB | RB | EF | ||||||
| Baseline | 63.9 | n.a. | n.a. | 39 | n.a. | n.a. | 24.4 | n.a. | n.a. | 3.2 | n.a. | n.a. | 2.2 | n.a. | n.a. |
| 1.5 PV | n.a. | 20 | 32 | n.a. | 9.7 | 25 | n.a. | 10 | 41 | n.a. | 1.6 | 50 | n.a. | 1.1 | 14 |
| 2 PV | n.a. | 25 | 40 | n.a. | 13.7 | 35 | n.a. | 11.3 | 47 | n.a. | 1.8 | 57 | n.a. | 1.5 | 28 |
| 3 PV | n.a. | 27 | 42 | n.a. | 15.5 | 40 | n.a. | 11.3 | 47 | n.a. | 1.8 | 57 | n.a. | 1.0 | 28 |
* Total amount in grams of the different serum protein fractions was calculated as follow = [(solute concentration in reservoir/effluent (g/l) * total volume (l) reservoir/effluent bag)]. Net percentage loss of the different serum protein fractions was calculated as follow = [(reservoir bag solute concentration at baseline * total volume ml reservoir bag) – (effluent bag solute concentration * total volume ml effluent bag) / (reservoir bag solute concentration at baseline * total volume ml reservoir bag)] * 100. PV, plasma volume; RB; reservoir bag; EF, effluent bag; n.a., not applicable.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



