Submitted:
26 March 2025
Posted:
26 March 2025
You are already at the latest version
Abstract
This study analyzes the comparative performance of ten hospitals in the Kadutu Health Zone in the Democratic Republic of Congo, using the EGIPSS model. The study was carried out in the height of the COVID-19 pandemic in August and September 2021, in a changing global context where health systems are called upon to improve their resilience capacity while remaining high-performing. The study was descriptive and observational, using documentary review, interviews with 85 key informants and participatory observation of the ten hospitals selected on the basis of several criteria including the organization of a complete complementary package of activities assigned to a hospital in the DR Congo. It mainly reveals three facts, namely: (i) university hospitals show the best performance, (ii) adaptive capacity considerably influences the other dimensions of the EGIPSS model and along the way the overall performance of the hospital and (iii) to adapt, hospitals need resources and good management and governance. Adapting hospitals in the Kadutu Health Zone to the changing context requires a holistic approach that combines clinical work with research, investments in infrastructure (often dilapidated and not modern), training, technology and governance. It also involves learning from practices implemented in more efficient hospitals.
Keywords:
EGIPSS model
; Performance
; hospitals
; Kadutu
; Bukavu
; South Kivu
; DR Congo
1. Introduction
Performance is a multidimensional concept that concerns health system managers. Faced with the changing global context of recent years and in particular with the advent of the Covid-19 pandemic, health systems have been called upon to improve their resilience while remaining efficient [1]. At the particular level of hospitals, which are complex adaptive systems [2,3,4], measuring hospital performance fulfills several objectives [5,6]. These include optimal cost management, improving internal hospital management, establishing benchmarking between hospital establishments, putting hospitals under control in order to have visibility on their achievements, putting hospitals in competition and improving patient satisfaction [6]. On the other hand, evaluating performance within the hospital can encounter difficulties linked to the nature of hospital activity, the actors, but also to uncertainty about the tools for this measurement [4].
In practice, there are several performance measurement models [7,8], depending on the definition given to the latter. The literature describes several performance measurement models, some of which are unidimensional [9,10]and others multidimensional [9,11,12]. Studies on hospital performance have demonstrated the interest of considering the concept of performance from a multidimensional perspective [13,14]. One of the integrative models groups the sub-dimensions of performance into four poles that define the four functions of a health system. This is the EGIPSS model (Global and Integrated Evaluation of the Performance of Health Systems) [11]. According to this model, to be efficient (maintain its existence and develop), the hospital, like any organized health system of action, must assume over time four major functions corresponding to four dimensions (or poles) of performance: adaptation to the environment, achievement of goals, production and maintenance of culture and values. Adaptation to the environment is described in terms of acquisition of resources (human, financial and material, including drugs and laboratory reagents), response to the expectations of the population, mobilization of the community, attraction of customers and capacity to innovate. Achievement of goals implies the provision of reference health care with effectiveness, efficiency, even equity to the overall satisfaction of the population. As for production, it is understood as a volume of acts, quality services that the hospital is called upon to provide. Finally, maintaining culture and values represents the organizational climate as well as the different values, including patient and provider satisfaction, compliance with standards and procedures. These four functions have close links called balances or alignments [11].
We were interested in this latter model to measure the performance of ten hospitals in South Kivu, in the East of the Democratic Republic of Congo (DRC), in the Kadutu Health Zone (HZ) . In this unstable region, shaken by conflicts for several decades, hospital structures proliferate, sometimes anarchic, sometimes regulated, offering part or all of the hospital care [15,16]. The objective of this study was to measure the comparative performance of hospital structures in the Kadutu HZ using the EGIPSS model and to draw lessons for managers.
2. Materials and Methods
2.1. Description of the Study Environment
The study was conducted during the COVID-19 pandemic in August and September 2021, in the urban health zone of Kadutu. The health zone is the operational level of the DRC health system, subdivided into two levels of health care. The hospital constitutes the second level of health care and is closely linked to the first level made up of health centers. The hospital thus offers a complementary package of care provided at the health center. In 2020, the Kadutu HZ had 89 health facilities offering hospital care, for a total population estimated at 392,298 inhabitants [17]. It had 549 beds, 38% of which were at the general referral hospital of the health zone ( Ciriri Hospital ) and only 39.5% were used in 2020, compared to 67.1% in 2019, before the pandemic [17]. This low use appears to be linked not only to the proliferation of private structures which do not report their data [15]but also to the effects of the Covid-19 pandemic [18,19]including the resistance of the population to using health structures.
2.2. Operational Framework of the ÉGIPSS Model, Its Components and Their Relationship with the Hospital
EGIPSS is a model developed by Sicotte and his collaborators [11], inspired by Parsons' theory of social action [20]that integrates the essential functions of an organization. It is composed of four main dimensions separated into two axes. A first axis includes the relationship between an open system and its environment (external - internal). On the other side, a second axis takes into account the balance between incoming resources, the use process, transformation and results (means - goals)
Figure 1.
The ÉGIPSS model [11].
Figure 1.
The ÉGIPSS model [11].
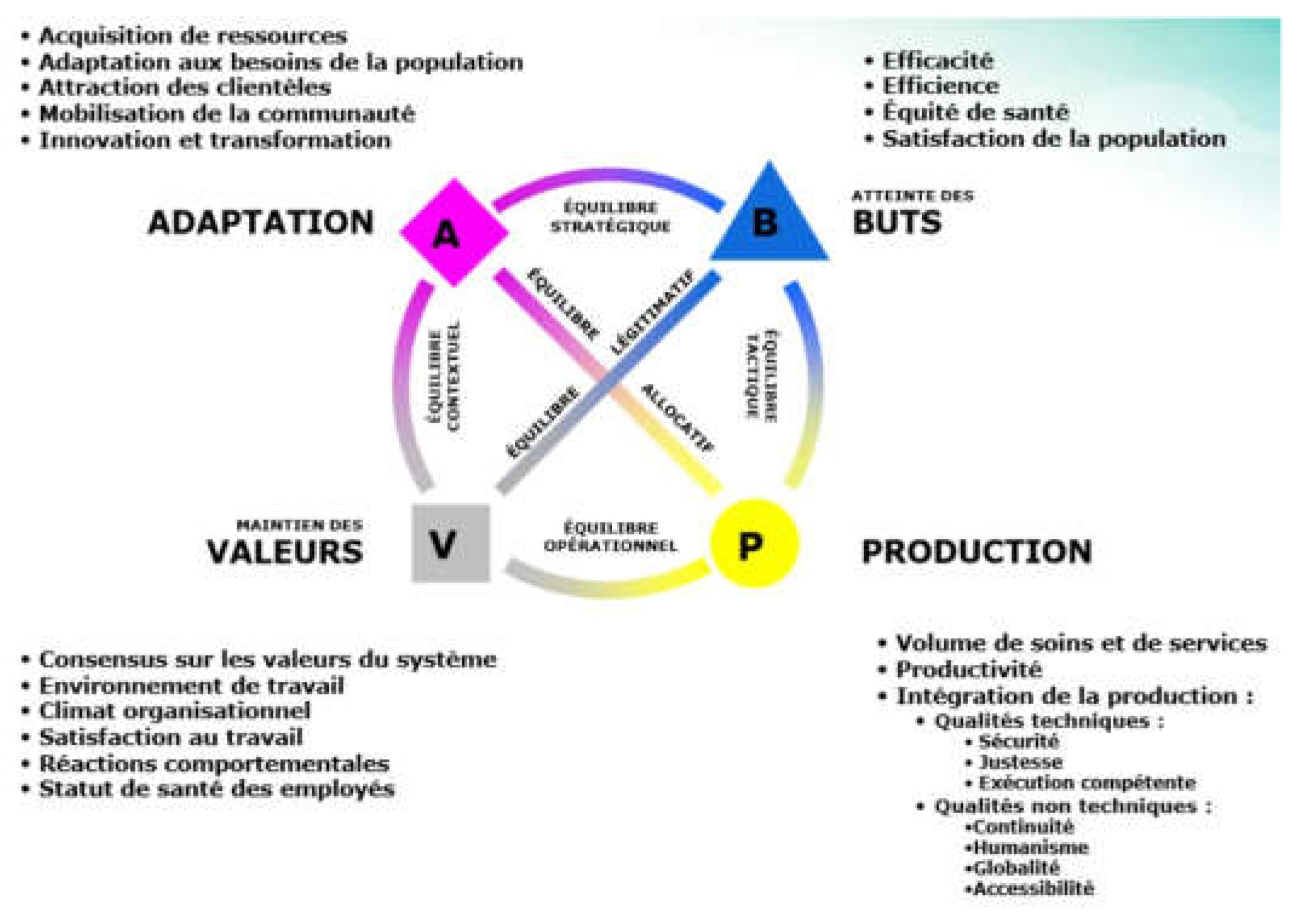
In the EGIPSS model, the functions described by Parsons form the basis of the four functions of performance. The interactions between these four dimensions are called "balances" or "alignments" and are also a fundamental factor to monitor according to the model to maintain a high-performance system. Based on the EGIPSS model, Guisset [5]defined what constitutes a high-performing hospital in a European context. This study draws on the work of Guisset and colleagues to measure the performance of hospitals in the Kadutu HZ. Below we define the components of the model (dimensions and sub-dimensions) and their relationship with a so-called "high-performing" hospital:
Adaptation
• Acquisition of resources (6 items): hospital that obtains public and/or private (NGO) funds, has highly qualified staff (specialists), is associated with groups/associations/mergers, obtains research funds or does research with its funds, has managed to obtain a substantial increase in its total budget, collaborates with other institutions in order to expand its services.
• Local community support (5 items): hospital whose board members are active, whose doctors and other professionals appear in the media, have many volunteers, serve as a reference and whose services are highly regarded by the public.
• Consistency with social values (6 items): Hospital whose board of directors demonstrates accountability, is trusted by other health care providers, consults extensively with the local population, operates within its budget, board members are aware of their responsibilities to payers, and actively seeks to include representatives of the local population.
• Response to population needs (5 items): hospital that adapts its activities in response to the needs of the population, takes sociodemographic data into account, informs the population of changes, has opened certain services and closed others in response to changes in the needs of the population and regularly monitors the evolution of the demographic characteristics of the population it serves.
• Market presence (4 items): hospital that treats a large portion of the population, is considered a reference center (local, provincial, national or international), treats many more patients than competing hospitals and provides services not available elsewhere.
• Innovation and learning (5 items): hospital that has changed its management practices in response to new knowledge, is able to identify the opportune moment to change strategic direction, rewards learning and innovation, demonstrates an interest in research and the production of new technologies and staff members apply research results in their practice.
Achieving goals
• Patient satisfaction (5 items): hospital with loyal patients, patients are very satisfied with the reception and the results of care, treats patients referred by other patients (word of mouth), the patient satisfaction rate is high and receives few complaints from patients about the results of care.
• Effectiveness (5 items): Hospital that works with other organizations to develop databases to evaluate and monitor performance, has a low rate of unplanned readmissions, has a low percentage of patients who develop complications, evaluates the impact of its care and services, and consistently produces the best possible health outcomes.
• Efficiency (4 items): hospital that presents an excellent cost/quality ratio, systematically produces the best possible health results while controlling costs, reduces its costs by improving the adequacy of care and allocates budgets between services on the basis of their relative cost-effectiveness.
Production
• Productivity (3 items): hospital that manages to reduce costs while maintaining the range of services offered, shares certain services with others in order to achieve economies of scale and whose length of stay is low compared to other similar hospitals.
• Volume of activity (5 items): hospital that treats a large number of patients, has expanded its outpatient services, has increased the range of services offered, has a large number of emergency admissions and allocates new resources to services with increasing patient numbers.
• Quality (5 items): hospital that constantly tries to improve the quality of care, maintains contacts with other institutions to ensure excellent follow-up, where the waiting time for scheduled surgery is short, which makes its services easily accessible to those who need them and which provides excellent care from a technical point of view.
• Coordination of production (5 items): hospital that continually tries to coordinate care with other organizations, has a high degree of coordination between clinical staff and logistics staff, where there is great coordination among professionals, where there is great coordination between care units and where there is good coordination with other care producers.
Culture
• Organizational values (5 items): hospital that regularly reviews and updates its missions and objectives, whose philosophy of care is common to all staff members, which consults its staff, whose organizational objectives have been integrated by everyone, which has established formal mechanisms for discussing and resolving ethical problems.
• Organizational climate (5 items): A hospital whose staff members feel they have the necessary expertise, provides opportunities for managers and staff to improve their leadership skills, is able to create a sense of trust among staff members, whose staff members are aware of the importance of their work, and in which formal channels for conflict resolution have been established and are used by staff members.
2.3. Selection Criteria for Hospital Structures under Study
The mapping of hospital structures in the Kadutu HZ carried out between August 2021 and October 2021 counted a total of 30 structures [16]. Among these structures, 19 offered the complete complementary package of activities (CPA) of care and 11 an incomplete CPA. First, we started by excluding from our sample the hospitals organizing an incomplete CPA. We then refined the selection criteria by applying them to the hospitals selected in the first stage. The hospitals selected in this second stage were those that organized at least the four basic services (pediatrics, gynecology-obstetrics, internal medicine and surgery); had at least one full-time general practitioner, who were functional or stable on their site for at least two years, and held proof of operating authorization issued by the required health authorities. Thus, ten structures were selected for the study, presented in Table 1.
2.4. Type of Study
2.5. Data Collection
A unique data collection tool was developed, based on the dimensions of performance according to the EGIPSS model and the definition of a high-performance hospital according to Guisset. [5], adapted to the Kadutu health zone . This tool sought a total of 73 qualitative elements related to adaptation (31 elements), achievement of goals (14 elements), maintenance of values, culture (10 elements) and production (18 elements). Three data collection techniques were used (see Table 2): (i) the documentary review which concerned several parameters, using national and provincial texts on the provision of hospital care in urban areas (essentially the health development plan of the Kadutu health zone and the collection of national standards on the health zone), various reports from the Provincial Health Division (DPS) on the performance of health facilities and the annual reports of the various hospitals and the Kadutu health zone for the years between 2019 and 2021. This documentary review made it possible on the one hand to identify the hospital structures of the health zone and on the other hand to describe their characteristics; (ii) semi-structured individual interviews with key informants using a pre-established guide. Different key informants were solicited by reasoned choice [21]. These are the head doctor of HZ of Kadutu , the hospital directors, the nursing directors, the members of the management team of HZ of Kadutu , the hospital owners, the representatives of the population and the patients. In total, for all ten structures, 85 key informants were interviewed at a rate of 8 people per hospital (including two patients per hospital drawn at random during the visit), and 5 members of the Management Team of HZ of Kadutu including the head doctor of Health Zone. The interviews were conducted by 4 duly trained investigators who were supervised in the field by one of the researchers in order to ensure the quality of the data collected; (3) the non-participant observations of the ten hospital care structures selected using a data collection grid.
The interviews and observation focused mainly on the acquisition of resources (in particular the availability of qualified human resources), innovation and learning (in this case the new technologies implemented in the hospital and the application of research results in hospital practices), organizational values (mechanisms put in place to implement the missions and achieve the hospital's objectives), quality (in the dimensions of human reception, waiting time before surgery and patient hospitalization conditions) and finally the coordination of production ( the continuous coordination of care with other structures including referral and counter-referral, the level of coordination between clinical staff and logistics staff, coordination within professionals, coordination between care units).
2.6. Data Analysis
The information collected for the 73 items, theoretically representing the attributes of a high-performing hospital, was entered and processed in Excel software and grouped into the 4 dimensions and 14 sub-dimensions. of the EGIPSS model. We conducted a thematic analysis, describing the 4 dimensions (themes) and 14 sub-dimensions (sub-themes) in two stages.
First, a rating of the degree of application of each attribute/item from 0 (no application) to 100 (total application) was carried out and validated with the head of each hospital. Mean scores were calculated for each sub-dimension. Thus, the hospital's performance was considered satisfactory in a sub-dimension when the score was ≥ 75%, it was acceptable when the score was between 50 and 74% and the performance was considered worrying when the score was < 50%.
Then, a description of the performance by dimension of the EGIPSS model was carried out from qualitative, triangulated information from interviews, documentary review and observation.
The comparison between the hospitals studied was established, identifying on the one hand the best performing hospitals in the 14 sub-dimensions and on the other hand the sub-dimensions requiring improvement in order to re-establish a dynamic balance between the 4 dimensions of the EGIPSS model, a guarantee of hospital performance necessary for patient satisfaction.
2.7. Ethical Considerations
The research protocol was approved by the Kadutu HZ management team, which authorized data collection. A prior informed consent form, guaranteeing anonymity and free participation, was completed by each of the identified structures and key informants.
3. Results
Table 3 gives the overall performance score of the different hospitals considering the rating made for the four dimensions of the EGIPSS model.

| Performance Level | Satisfying | Acceptable | Worrying | |||||||
| STRUCTURES | PGRHB | GRH CIRIRI | CLIN OUB | GRH KADUTU | HC NYAMUGO | POLY.RED CROSS | POLY BERNA | HC ISTM | HC SAINT VINCENT | MC FOND MAROY |
| ADAPTATION | 78 | 61 | 59 | 53 | 47 | 42 | 41 | 40 | 40 | 36 |
| Resource acquisition (%) | 60 | 43 | 45 | 32 | 28 | 27 | 30 | 28 | 22 | 18 |
| Local community support (%) | 78 | 66 | 68 | 56 | 48 | 42 | 36 | 40 | 46 | 40 |
| Consistency with social values (%) | 85 | 67 | 68 | 67 | 65 | 62 | 62 | 62 | 58 | 48 |
| Response to population needs (%) | 78 | 50 | 58 | 46 | 50 | 28 | 38 | 26 | 24 | 26 |
| Market presence (%) | 88 | 75 | 35 | 55 | 48 | 55 | 38 | 45 | 48 | 48 |
| Innovation and learning (%) | 80 | 64 | 82 | 62 | 40 | 40 | 40 | 38 | 40 | 34 |
| ACHIEVEMENT OF OBJECTIVES | 78 | 69 | 65 | 64 | 63 | 60 | 60 | 59 | 60 | 56 |
| Patient satisfaction (%) | 82 | 80 | 72 | 72 | 68 | 70 | 76 | 62 | 66 | 62 |
| Efficiency (%) | 74 | 68 | 58 | 66 | 60 | 62 | 56 | 70 | 60 | 52 |
| Efficiency (%) | 78 | 60 | 65 | 55 | 60 | 48 | 48 | 45 | 53 | 55 |
| PRODUCTION | 85 | 75 | 73 | 66 | 57 | 55 | 55 | 54 | 53 | 48 |
| Activity volume (%) | 86 | 76 | 70 | 76 | 54 | 46 | 46 | 46 | 50 | 42 |
| Quality (%) | 83 | 78 | 80 | 68 | 60 | 65 | 64 | 67 | 62 | 50 |
| Production coordination (%) | 86 | 72 | 70 | 54 | 58 | 54 | 54 | 48 | 48 | 52 |
| CULTURE/VALUES | 85 | 82 | 71 | 67 | 62 | 61 | 57 | 55 | 54 | 53 |
| Organizational values (%) | 86 | 82 | 76 | 74 | 64 | 60 | 62 | 62 | 56 | 56 |
| Organizational climate (%) | 84 | 82 | 66 | 60 | 60 | 62 | 52 | 48 | 52 | 50 |
| OVERALL AVERAGE | 82 | 72 | 67 | 63 | 57 | 55 | 53 | 52 | 52 | 48 |
3.1. Adaptation
Only one hospital structure (PGRHB) out of ten, or 10%, has a satisfactory level of performance in adaptation to the urban context. Three others (30%) have an adaptation performance level considered acceptable (GRH CIRIRI, CLINIQUES OUB and GRH KADUTU). On the other hand, 60% of the structures display a worrying performance (CH NYAMUGO, POLYCLINIQUE CROIX ROUGE, POLYCLIQUE BERNA, HC ISTM BUKAVU, CH SAINT VINCENT and CH MAROY).
The HPGR of BUKAVU naturally stands out from other hospital structures in the Kadutu HZ due to the specificities conferred on it by its status as a tertiary level structure with an acquisition of considerable resources supported by other partner organizations (including the International Committee of the Red Cross or Doctors Without Borders), specific equipment, highly qualified personnel engaged in operational research and regularly appearing in the media. It organizes services not available elsewhere (MRI, Hemodialysis, Neonatology).
The University Clinics of the Official University of BUKAVU (OUB), a public structure supposed to be of tertiary level, has a team of highly qualified and diversified professionals (professors, specialists, general practitioners, nurses and other paramedical). The structure is specialized and demonstrates an interest in research, organizes the continuous training of staff, facilitates providers to access scholarships, rewards research and innovation by promotion in grades.
The GRH CIRIRI is a denominational structure managed by the Diocesan Bureau of Medical Works (BDOM) Bukavu. It has sufficiently qualified staff including specialists, general practitioners, caregivers and paramedical staff. Following the arrival of specialists and new services, it has increased its budget. It is a reference structure within the Kadutu HZ and takes care of patients from other HZ, with good attendance in outpatient and hospitalization, whose services are highly regarded by the public.
Hospital structures in the last category generally have problems with the resources needed to meet the needs and demand for services and health care. They do not organize operational research but apply therapeutic protocols for care resulting from research by other institutions or the Ministry of Health. They operate with a low budget and do not benefit sufficiently from funds from donations from the public and organizations to support their operations. The medical staff of most of these structures have little or no involvement in the media. They do not take into account demographic data in their planning or the involvement of the community in decision-making.
3.2. Achieving Goals
Only one structure, the PGRHB has a satisfactory performance for this dimension. All other structures have an acceptable performance.
The PGRHB periodically conducts satisfaction surveys, with an average patient satisfaction rate of 80% in 2020 and 2021. It receives support from performance evaluation organizations such as the ICRC, WHO, and MSF and enjoys autonomy in diagnostic equipment and materials.
OUB University Clinics, in addition to satisfaction surveys, collect data from suggestion boxes to assess the level of appreciation of services and benefits by clients. They work with partner organizations to develop databases to assess and monitor performance. GRH CIRIRI also receives technical support from BDOM to periodically assess the performance of services and operations in general.
Furthermore, the other structures do not benefit from permanent technical support from partner organizations to evaluate and support the performance of the services and care offered to clients. This generally limits the effectiveness and efficiency of the services to achieve the objectives of each of them. These structures record low use of services, the vast majority of whose clients come from the health areas in which they are implemented. They even request certain paraclinical examinations elsewhere to confirm the diagnosis and schedule interventions, and this prolongs the waiting time of clients. The patient satisfaction study is not conducted in the majority of these structures.
3.3. Production
The study shows that 30% of the hospital structures in the urban HZ of Kadutu have a satisfactory performance for the "Production" dimension (PGRHB, CLINIQUES OUB and GRH CIRIRI); 60% have an acceptable performance (CH NYAMUGO, CH SAINT VINCENT, GRH KADUTU, CH ISTM BUKAVU, the POLYCLINIQUES CROIX ROUGE and BERNA) and 10% have a worrying performance, the MC MAROY.
The structures with satisfactory performance are those that admit a large number of patients in the emergency and intensive care departments, are a reference structure, have a short length of hospital stay (with the exception of PGRHB and OUB clinics which record more reference cases with chronic pathologies or having dragged on in the therapeutic itinerary). They organize services that are not available elsewhere such as neonatology and maintain contacts with other institutions, allocate additional resources to the services according to their use to maximize revenue. They regularly strengthen the capacities of the staff through in-service training, specialization and operational research. These structures have developed different services and have a short waiting time for scheduled surgery.
Furthermore, the underperformance in the other category of structures (Acceptable Production) is due to the lack of certain services such as emergency and intensive care, the lack or obsolescence of diagnostic equipment, and the fact that they do not share services with other institutions. Relatively high healthcare costs were also noted in structures with underperformance. At MC FONDATION MAROY, for example, most patients are followed up on an outpatient basis by general practitioners, the waiting time for scheduled surgery is long, due to the lack of a permanent surgeon.
3.4. Culture / Values
For this dimension, 30% of hospital structures have a satisfactory performance (HPGR BUKAVU, CLINIQUES OUB and GRH CIRIRI) and the other structures have an acceptable performance. The performances are recorded in the structures where formal mechanisms for discussion and resolution of conflicts, management of ethical problems (ethics committee, complaints management committee, the union, etc.) have been set up and are functioning. The integration of organizational objectives by the members, the common philosophy of care for all staff members (the protocols of care displayed, applied and discussed in medical staff meetings), the consultation of staff by the steering committee (maintenance of good communication between managers and providers) before any decision were also assessed.
Poor performance was noted in structures that do not provide staff training or opportunities to improve management team members' skills in leadership, conflict management and ethical issues.
4. Discussion
The present study aimed to measure the comparative performance of hospital structures in the Kadutu HZ using the EGIPSS model, with a view to drawing lessons for their improvement. The study mainly reveals three facts namely: (i) university hospitals have the best performances, (ii) adaptability significantly influences the other dimensions of the EGIPSS model and along the way the overall performance of the hospital and (iii) to adapt, hospitals need resources and good management and governance.
4.1. Combining Clinical Care with Research and Teaching Improves Hospital Performance
The Bukavu Provincial General Reference Hospital attached to the Catholic University of Bukavu and the Bukavu Clinic attached to the Official University of Bukavu have better performances in the different dimensions of the EGIPSS model. The teaching and research component found in university hospitals allows them to incorporate the latest medical discoveries and technologies into their clinical practices. Collaboration between clinicians and researchers leads to more effective treatments, the introduction of new therapeutic approaches and better patient care [22,23,24]. Another fundamental aspect of university hospitals is their role in medical education. They train future doctors, nurses, researchers, and other health professionals, which allows for the continuous dissemination of best practices and current knowledge. This continuing education helps to maintain a high level of clinical skills and quality of care in the institution [25,26]. These hospitals also have access to rare and complex specialists as well as advanced infrastructure and technologies, which are not yet found in other hospitals in the Kadutu HZ .
University hospitals are typically subject to rigorous quality standards, due to their involvement in research and teaching. These standards ensure continuous monitoring and evaluation of clinical performance, which allows for rapid correction of failures, optimization of processes, and improvement of patient safety. Due to their academic nature, these hospitals are often well connected to international research and exchange networks, allowing them to benefit from the latest advances and share their own innovations. This international openness allows them to attract talent, collaborate on large-scale research projects, and maintain a leading position in certain medical fields [26]. In addition, university hospitals often benefit from greater public and/or private funding than other types of hospitals, particularly for research, education, and the acquisition of cutting-edge technologies. [24,26]. Adequate budget and institutional support help maintain a high level of quality of care and invest in innovation.
The culture of university hospitals generally encourages continuous improvement of processes, integrating feedback from patients, healthcare professionals and researchers [24]. This allows weaknesses to be identified and solutions to be implemented to improve the efficiency and quality of care. Finally, the organization of care in a university hospital often places particular emphasis on patient-centered care, thanks to diverse teams that collaborate to provide holistic and personalized care. Taking into account the psychological, social and medical needs of patients, such as those with HIV [27] or chronic diseases [28], as well as communication with them, can improve their experience and, ultimately, their health outcomes [28].
4.2. Adaptability Significantly Influences Other Dimensions of the EGIPSS Model and Along the Way the Overall Performance of the Hospital
Adaptability in a hospital, as in any complex organization, is a crucial factor that impacts other organizational dimensions, such as human resources management, innovation, quality of care, and even the relationship with patients [29]. This adaptation concerns both the constantly evolving needs of patients and technological advances, human resources management, health crisis management, or the changing economic and regulatory environment. Patient needs are constantly evolving, whether due to the aging of the population, the emergence of new pathologies, or increasing expectations for quality care. A hospital that is able to adapt quickly to these changes (for example, by developing new services, integrating advanced technologies, or changing its practices) can better meet patient expectations and remain efficient [30]. Regarding technological advances, they are essential in the hospital sector to improve the accuracy of diagnoses, the effectiveness of treatments, and the management of medical data through the electronic medical record [31,32]. The hospitals analyzed in our study are however not able to quickly adopt new technologies, such as artificial intelligence, surgical robotics, or telemedicine in order to increase their clinical efficiency. The integration of innovative technologies allows to reduce costs, increase productivity and free up time for medical staff. Also, the use of advanced technologies allows for faster and more accurate diagnoses, contributing to better patient care. As for human resources management, it is a key dimension of hospital performance. In a context of shortage of qualified labor as in DR Congo [33,34,35], hospitals must demonstrate a great capacity for adaptation to maintain a motivated and efficient team. This requires effective management of recruitment, continuing training, and retention strategies.
Hospitals’ adaptation to health crises, such as the COVID-19 outbreak, or to other unforeseen situations (natural disasters, drug shortages, etc.) including their ability to quickly reorganize services, implement emergency protocols, and manage the massive influx of patients in times of crisis inspires confidence among patients and the public, which is a guarantee of their long-term performance. Finally, hospitals operate in a dynamic regulatory and economic environment, with increasing budgetary constraints and higher social expectations. The ability to adapt to these changes (for example, by optimizing costs without sacrificing quality of care or by complying with new security and data management standards) is a key element of long-term performance.
Kadutu HZ hospitals presents unique challenges due to the socio-economic, cultural and environmental context, as well as resource limitations. However, these challenges can become levers for innovation and performance. By leveraging strong governance, effective human resource management, adapted technologies, resilient infrastructure, and close collaboration with the community and partners, hospitals can not only overcome challenges but also excel in a complex and dynamic environment. This also requires a long-term commitment to ensure the sustainability and performance of the health system [36,37].
4.3. To Adapt, Hospitals Need Resources and Good Management and Governance
In the context of the DR Congo, as in many African countries, hospitals face complex challenges in adapting to changes in health, whether related to demographic, technological, epidemic or social developments. Access to resources is essential for them to strengthen them in order to better meet the needs of populations and multiple contemporary challenges. These challenges include improving and modernizing infrastructure, permanent access to electricity, water supply, training and education of staff, retention of medical staff, digitalization of health care, supply of medicines and medical equipment, disease prevention, response to epidemics and pandemics involving dedicated infrastructure, trained crisis management teams and strengthened partnerships with international organizations [38,39]. Resources are also needed to support the universal health coverage system advocated in the DR Congo and equity of access to care [40]. To address these challenges, public-private partnerships (including for technological innovation, infrastructure financing and staff training) [41]and international cooperation, including partnerships with global organizations such as WHO or local NGOs, are crucial to fill gaps in financing, crisis management and technology transfer. Finally, hospital management and governance need to be strengthened. Effective and transparent hospital management, including good strategic planning, regular audits, anti-corruption and improved human and financial resource management, is essential for effective care [3].
4.4. Limitations of the Study
The main limitation of this study is the impossibility of measuring the variation of balances between the dimensions of the EGIPSS model because the data were collected, not in a recurring manner over several years but in a transversal manner, at a given moment in the life of the hospitals.
5. Conclusions
The measurement of hospital performance in the Kadutu HZ according to the EGIPSS model focused on attributes of the 4 dimensions of the model, without being able to analyze the alignments between the dimensions, due to lack of longitudinal data. The comparative study of hospitals essentially demonstrates that combining clinical care with research and teaching contributes to improving the overall performance of a hospital, that the capacity for adaptation considerably influences the other dimensions of the EGIPSS model and along the way the overall performance of the hospital and that to adapt, hospitals need resources and good management and governance. Adapting hospitals in the Kadutu HZ to change requires a holistic approach that combines investments in infrastructure (often outdated and not modern), training, technology and governance. It also involves learning from practices implemented in more efficient hospitals.
Author Contributions
“Conceptualization, H.K. and S.M.L.; methodology, H.K” and I.B.; software, I.B.; validation, All authors; formal analysis, H.K. and I.B..; investigation, I.B.; resources, X.X.; data curation, X.X.; writing—original draft preparation, I.B. and H.K..; writing—review and editing, H.K. and I.B.; visualization, S.M.L and S.K. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
“The authors declare no conflicts of interest.”
References
- Saulnier, D.D., et al., Re-evaluating our knowledge of health system resilience during COVID-19: lessons from the first two years of the pandemic. International Journal of Health Policy and Management, 2023. 12. [CrossRef]
- Karemere Bimana, H., Gouvernance hospitalière adaptative en contexte changeant: étude des hôpitaux de Bunia, Logo et Katana en République démocratique du Congo. 2013, UCL-Université Catholique de Louvain.
- Karemere, H., et al., Gouvernance des hôpitaux de référence en République démocratique du Congo: synthèse critique interprétative de la littérature. Médecine et Santé Tropicales, 2013. 23(4): p. 397-402.
- Alvarez, F. Le contrôle de gestion en milieu hospitalier: une réponse à l'émergence de risques organisationnels. in XXIème congrès de l'Association Française de Comptabilité. 2000.
- Guisset, A.-L., et al., Définition de la performance hospitalière: une enquête auprès des divers acteurs stratégiques au sein des hôpitaux. Sciences sociales et santé, 2002. 20(2): p. 65-104.
- BERRADA, H. and A. MARGHICH, PERFORMANCE HOSPITALIERE: ETAT DE L’ART. Revue du contrôle, de la comptabilité et de l’audit, 2023. 7(1).
- Kaplan, R.S. and D.P. Norton, The balanced scorecard: measures that drive performance. Vol. 70. 2005: Harvard business review Boston, MA.
- Kruk, M.E. and L.P. Freedman, Assessing health system performance in developing countries: a review of the literature. Health policy, 2008. 85(3): p. 263-276. [CrossRef]
- LAHBIB, A. and A. SAID, La performance hospitalière: approches et modèles de définitions. Revue Internationale du Chercheur, 2022. 3(4).
- DIAKITE, O., et al., Proposition d’un modèle explicatif de la performance organisationnelle par les facteurs individuels dans les Centres Hospitaliers Universitaires du Mali. Revue Internationale des Sciences de Gestion, 2022. 5(1).
- Sicotte, C., et al., A conceptual framework for the analysis of health care organizations' performance. Health services management research, 1998. 11(1): p. 24-41. [CrossRef]
- Papanicolas, I., et al., Health system performance assessment: a framework for policy analysis. 2022.
- Contandriopoulos, A.-P., La gouvernance dans le domaine de la santé: une régulation orientée par la performance. Santé publique, 2008. 20(2): p. 191-199.
- Karemere, H., et al., Analysis of hospital performance from the point of view of sanitary standards: study of Bagira General Referral Hospital in DR Congo. Journal of Hospital Management and Health Policy, 2020. 4. [CrossRef]
- Sivyavugha, S.K., et al., Proliferation of hospital facilities in the Ibanda Health Zone in the Democratic Republic of Congo: Determinants and perceptions of health stakeholders. International Journal of Innovation and Applied Studies, 2024. 43(1): p. 28-38.
- Batumike, I., et al., Analysis of hospital care provision in the urban health zones of Bukavu, DR Congo. International Journal of Innovation and Applied Studies, 2024. 43(1): p. 70-81.
- HZ-Kadutu, Rapport annuel 2021. Ministère de la santé de la RD Congo, 2021.
- JANDARME, F. and P. BALUNGU, Vécu psychosocial au sein des familles victimes du confinement dû à la Covid-19 dans la ville de Bukavu, au Sud-Kivu en République Démocratique du Congo. Éducation et développement, 2020(24): p. 19-19.
- Kajiramugabi, F.M., et al., Impact de la COVID-19 sur les services de prévention du VIH et de prise en charge des personnes vivant avec le VIH dans la ville de Bukavu: une étude mixte séquentielle explicative. Science of Nursing and Health Practices, 2023. 6(2): p. 16-32. [CrossRef]
- Sciulli, D. and D. Gerstein, Social theory and Talcott Parsons in the 1980s. Annual Review of Sociology, 1985: p. 369-387. [CrossRef]
- Beaud, J.-P., L’échantillonnage. Recherche sociale: de la problématique à la collecte des données, 2009. 5: p. 169-198.
- De Roten, Y., Évaluation ou dévaluation? Quelques malentendus entre chercheurs et cliniciens sur la recherche empirique. Psychothérapies, 2021. 41(4): p. 209-217.
- Porro, B. and K. Lamore, Vers un décloisonnement de la recherche en psycho-oncologie: quid de la formation des jeunes chercheurs? 2022. [CrossRef]
- Peixoto, M.G.M., M.A. Musetti, and M.C.A. Mendonça, Multivariate analysis techniques applied for the performance measurement of Federal University Hospitals of Brazil. Computers & Industrial Engineering, 2018. 126: p. 16-29. [CrossRef]
- De Melo, G.A., et al., Performance measurement of Brazilian federal university hospitals: an overview of the public health care services through principal component analysis. Journal of Health Organization and Management, 2024. 38(3): p. 351-371.
- Li, H., et al., Tianjin Medical University General Hospital. Obstetrics, Gynecology and Reproduction, 2025. 18(6): p. 925—930. [CrossRef]
- Slama, L., et al., L'observance thérapeutique au cours de l'infection VIH, une approche multidisciplinaire. Médecine et maladies infectieuses, 2006. 36(1): p. 16-26.
- Levesque 1, J., et al., Barrières et éléments facilitant l’implantation de modèles intégrés de prévention et de gestion des maladies chroniques. Pratiques et organisation des soins, 2009(4): p. 251-265.
- Boeker, W. and J. Goodstein, Organizational performance and adaptation: Effects of environment and performance on changes in board composition. Academy of Management journal, 1991. 34(4): p. 805-826. [CrossRef]
- Tagne, A.G.F., et al., Appréciation de la performance hospitalière des hôpitaux publics au Cameroun: une perception du personnel de santé. Journal of Academic Finance, 2020. 11(2): p. 331-344.
- Kehili, H., et al., Le Dossier Électronique médical à l’EHUO: Une avancée cruciale pour les soins de santé. 2024.
- Collet, L., ParKourS 2024: intégration des innovations numériques dans le parcours de soins du patient et mise en place dans les établissements hospitaliers. Innovations & Thérapeutiques en Oncologie, 2024. 10(5): p. 342-344. [CrossRef]
- Dorier, E. and E. Morand, " Accessibilité aux services de soins en situation post conflit, République du Congo. Bulletin de l'Association de géographes français, 2012. 2012: p. pp 289-312.
- Tete, B., et al., Connaissances et attitudes des médecins sur le syndrome d’apnées-hypopnées obstructives du sommeil à Kinshasa-République Démocratique du Congo. Médecine du Sommeil, 2022. 19(3): p. 182-189.
- Mulinganya, V., et al., Temps d’attente prolongés aux services de consultation médicale: enjeux et perspectives pour des hôpitaux de Bukavu en République Démocratique du Congo. The Pan African Medical Journal, 2018. 29.
- Ghioua, K. and H.E. Tebbouche, Labellisation de la durabilité des équipements sanitaires en Algerie: Cas de l’hôpital Bachir Mentourie d’El-Milia-Jijel. 2020, Université de Jijel.
- De Witte, L. and L. Decaux, " Importance de la durabilité dans les hôpitaux belges à l'horizon 2030: comment améliorer la durabilité tout en maintenant la qualité des soins?
- Tchouaket, E., et al., An Analysis of the Social Impacts of a Health System Strengthening Program Based on Purchasing Health Services. Journal of Epidemiology and Global Health, 2023. 13(4): p. 751-773. [CrossRef]
- Karemere, H., et al., Analyzing Katana referral hospital as a complex adaptive system: agents, interactions and adaptation to a changing environment. Conflict and health, 2015. 9: p. 1-10. [CrossRef]
- Baganda, B.M., S.L. Makali, and H. Karemere, Analyse des coûts des soins de santé chez les enfants de moins de 5 ans dans la Zone de santé de Bagira et implications pour la couverture sanitaire universelle. International Journal of Innovation and Applied Studies, 2024. 43(1): p. 14-27.
- Dumez, H. and A. Jeunemaître, Combinaison harmonieuse des vertus du public et du privé, ou mélange des genres? Les partenariats public/privé, nouveaux venus du management public. Politiques et management public, 2003. 21(4): p. 1-14.
Table 1.
Hospitals under study.
| No. | HA* | HA Population | Selected hospital structures |
|---|---|---|---|
| 1 | BINAME | 32361 | |
| 2 | BUHOLO2 | 28197 | |
| 3 | CECA MWEZE | 29030 | |
| 4 | CIMPUNDA | 29904 | |
| 5 | CIRIRI 1 | 59628 | GRH CIRIRI |
| 6 | CIRIRI2 | 14786 | |
| 7 | UNEF | 23515 | GRH Kadutu |
| MC Red Cross | |||
| 8 | LURHUMA | 19068 | HC ISTM Bukavu |
| 9 | MARIA | 71543 | OUB Clinic |
| PGRHB | |||
| Maroy Foundation Medical Center | |||
| 10 | NEEMA | 20932 | HC Saint Vincent |
| 11 | NYAMUGO | 26059 | Nyamugo Hospital Center |
| 12 | NYAMULAGIRA | 22736 | Berna Polyclinic |
| 13 | UZIMA | 14537 | |
| TOTAL HZ | 392296 |
*HA= Health area (geographic subdivisions of the HZ which include at least one functional health center). GRH = General Reference Hospital; HC = hospital center; MC = Medical Center; OUB = Official University of Bukavu; PGRHB = Provincial General Reference Hospital of Bukavu; CBCA = Baptist Community of Central Africa; ISTM = Higher Institute of Medical Techniques
Table 2.
Data collection technique for each parameter.
| Settings | Number of items | Data collection technique |
|---|---|---|
| Adaptation | ||
| Adaptation of resources | 6 | Documentary review, interviews, observation |
| Local Community Support | 5 | Interviews |
| Consistency with social values | 6 | Interviews |
| Responses to the needs of the population | 5 | Documentary review, interviews |
| Market presence | 4 | Documentary review, interviews |
| Innovation and learning | 5 | Documentary review, interviews, observation |
| Achieving goals | ||
| Patient satisfaction | 5 | Interviews |
| Efficiency | 5 | Documentary review, interviews |
| Efficiency | 4 | Documentary review, interviews |
| Culture (maintaining values) | ||
| Organizational values | 5 | Documentary review, interviews, observation |
| Organizational climate | 5 | Interviews |
| Production | ||
| Productivity | 3 | Documentary review, interviews |
| Volume of activity | 5 | Documentary review, interviews |
| Quality | 5 | Interviews, observation |
| Production coordination | 5 | Interviews, observation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



