Submitted:
21 March 2025
Posted:
24 March 2025
You are already at the latest version
Abstract
Endobronchial stenting is crucial in interventional pulmonology and thoracic surgery for managing various medical conditions. Achieving optimal stent fit in the airway remains an evolving discussion in interventional pulmonology, impacting patient outcomes and long-term stent function. Traditional silicone and metallic stents often fail to conform to complex airway anatomy, leading to complications such as migration, granulation, and obstruction. Recent advances in 3D printing have introduced patient-specific stents designed to improve fit and reduce complications. Case reports and small studies suggest that 3D-printed stents can enhance airway patency and symptom relief in select patients. However, challenges remain, including regulatory hurdles, manufacturing time, and real-world scalability. Furthermore, clinical decisions informing their choices remain unclear. Are they the answer to the long-standing limitations of conventional stents, or just one piece of a larger puzzle? As we push the boundaries of technology and patient-specific interventions, the real question may not be whether 3D stents are the solution—but rather, how we continue refining our approach to meet the complexities of airway disease. And perhaps, with advances in smart materials, 4D stents could one day change the conversation entirely. The purpose of this paper is to outline the limitations of pre-manufactured stents and propose detailed design strategies—illustrated with expert case examples—that address diverse clinical challenges in airway stenting. Although this report focuses on design customization, future studies are planned to evaluate radiographic, bronchoscopic, and clinical outcomes after deployment.
Keywords:
airway stent
; bronchoscopy
; three-dimensional printing (3D printing)
; stent sizing
1. Introduction
Airway stents, hollow cylindrical implants made from biocompatible materials such as silicone or metal alloys, have evolved significantly since the introduction of the Dumon silicone stent in the 1990s [1,2,3,4,5]. Recent advancements in stent technology, including custom-designed and biodegradeable 3D-printed stents, have gained prominence [6,7,8,9,10,11,12,13]. Additionally, “active” stents, which incorporate drug elution, antimicrobial coatings, or radiation delivery, are under investigation [14].
Traditional airway stents are available in fixed diameters and lengths, but selecting the appropriate stent size is far more complex than matching lumen dimensions [3,15,16,17,18,19,20]. The decision is influenced by technical, anatomical, and clinical factors, with the underlying indication—whether malignant airway obstruction, post-transplant complications, or benign diseases like tracheobronchomalacia—guiding design parameters and desired outcomes. Stents also vary by region, with differences in availability and regulatory approvals shaping clinical practice [15,16,17,18,19,21]. In the United States, most airway stents are cylindrical, except for a few branched configurations like Y-stents and T-tubes [13,16,22]. Despite their widespread use, airway stents remain prone to complications, including migration, infection, mucus plugging, and granulation, largely due to poor fit—an area that remains inadequately understood but is recognized as critical [5,11,23,24,25,26,27,28,29]. Recent surveys highlight global variability in stent sizing techniques, underscoring the challenge of achieving an optimal fit [15,16,17,18,19,21]. Modifying stent fit features may help mitigate these risks [30,31,32]. However, the complexity of airway disease further complicates stent selection. Pathologies such as cancer, prior airway resections, or lung transplantation can lead to asymmetrical or multifocal involvement, with variations in airway diameter the airway, angulation, and structural integrity [33,34,35,36]. Lung transplantation presents an extreme case, where stenosis, dehiscence, and malacia frequently coexist near the carina and extend into non-anastomotic regions, demanding highly individualized stent solutions.
To address these challenges, patient-specific (PS) implants have been developed in the US and Europe. ³² These custom-designed stents aim to improve fit by accommodating each patient’s unique anatomy and pathology. This study examines the limitations of pre-manufactured stents, the challenges of airway stent sizing, and expert-driven strategies for customization. Although the primary focus is on the design and implementation of 3D-printed PS stents, we also consider the critical post-deployment factors, including radiographic fit, bronchoscopic evaluations, and the “settling phase,” where stents and airways gradually conform to one another. By exploring these factors, we aim to establish a systematic approach for optimizing airway stent fit and improving patient outcomes.
2. Rationale
To better understand stent sizing using patient-specific stent technology, we conducted an observational interview with pulmonologists experienced in designing and utilizing these stents. Our goal was to gain insight into the design-making process behind patient-specific stent design, including the factors influencing customization and the rationale for selecting certain design parameters. This information may serve as a resource that can guide other physicians in designing patient-specific airway stents. However, it is important to acknowledge that clinical outcome data supporting these approaches is currently lacking. Therefore, work should be considered hypothesis-generating, laying the groundwork for future research and validation.
3. Methods
We conducted a semi-structured observational study involving two expert pulmonologists with expertise in 3DPS stent design. See supplemental section for sample questionnaire. The study consisted of:
- A review of nine unique clinical cases in which 3DPS stents were used.
-
In-depth interviews, via email, telephone, and in-person meetings, guided by a pre-defined questionnaire focusing on:Goals of stent designAnatomic limitationsAirway disease characteristicsPrevious treatment challenges
- A subsequent qualitative analysis of the discussions to identify common themes and design strategies. This process was complemented by a detailed description of the software workflow used for stent customization.
4. Customization Process
The customization process begins with obtaining high-resolution CT scans to reconstruct a detailed 3D model of the patient’s airway, from which precise measurements—such as diameters, lengths, and angles—are extracted and fed into specialized design software. This software defines key stent parameters (including oversizing, tapering, and branch angles), enabling the creation and simulation of a virtual stent model that is refined, finalized, and then manufactured via 3D printing. Finally, after pre-deployment testing, the stent is carefully deployed—adjusted as needed during the procedure—and then monitored with bronchoscopic and radiographic follow-up to confirm its continued fit.
5. Results
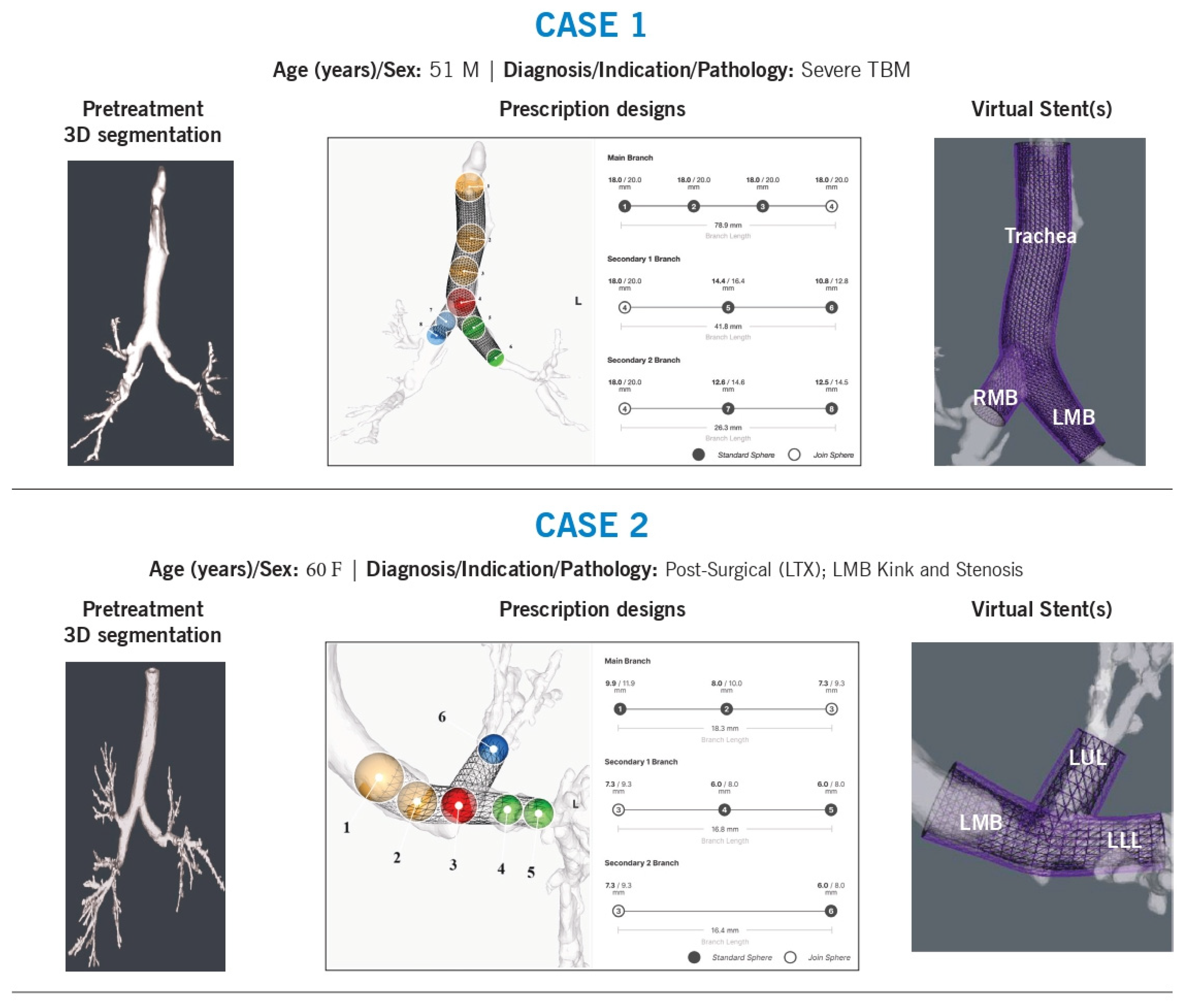
Nine cases were selected for review, each involving a 3DPS stent tailored to complex airway anatomy. These cases were chosen due to diverse pathology and unique anatomical to provide a comprehensive overview of different stent design callenges for different diagnoses, indications, and locations (Figure 1). To understand the decision-making regarding the size and design, the treating physician provided a background and the technical issues associated with the airway and stentingThe primary challenges identified included:
Shape mismatches requiring stent contouring (9/9 cases)
Branching angles requiring custom modification (6/9 cases)
Sizing discrepancies necessitating variable tapering (8/9 cases)
Jailed airway segments requiring fenestrations (1/9 cases)
Migration risk requiring anchoring adjustments (1/9 cases)
Case 1
Background: A 51-year-old man with tracheobronchomalacia underwent multiple 3D-printed patient-specific (3DPS) stent placements to support the trachea, right mainstem, and left mainstem. Prior Y-stents were manually customized by sewing together different sizes to achieve the required shape, angle, and diameter.
Technical Challenges:
Shape and angulation
Tapering of diameters
Variability in branch sizing, particularly in secondary airways
Intervention & Design Rationale:
The stent length was determined based on the extent of malacia, which originated at the thoracic inlet and extended distally into the left mainstem. The tracheal stent diameter was restricted by a maximum inner diameter of 18 mm. Because the airway had a flattened elliptical shape, diameter estimation required averaging the long and short axes, a challenge that persisted throughout the airway. Beyond the main carina, additional customization was necessary due to significant asymmetry between the right and left mainstem bronchi. The right mainstem was notably larger than the left, requiring precise contouring to ensure the stent closely approximated the medial airway walls while maintaining curvature aligned with native anatomy. Where not limited by maximum diameter specifications, the left mainstem stent wall was intentionally oversized to allow direct luminal interaction, with a 1-mm wall thickness providing additional support and dilation.
To prevent misalignment or excessive airway wall pressure, the stent was designed to follow the natural airway path, avoiding sharp edges or rigid structures that could cause localized stress. This patient-specific approach aimed to optimize airway stabilization while minimizing complications.
Case 2
Background: A 60-year-old lung transplant recipient developed left mainstem stenosis due to a post-anastomotic kink extending beyond the left upper lobe bronchus (LC1).
Technical Challenges:
Shape and angulation
Branch diameter and length
Intervention & Design Rationale:
The left mainstem stenosis and post-transplant kink extended distally into each lobar bronchus. The stent was designed to be long enough to cover the stenotic region while slightly oversized at the narrowest point to prevent restenosis. Proximally, it was tapered to match the native airway before the anastomosis.
To ensure a proper fit beyond the anastomosis, the stent design incorporated rotational adjustments to align lumen size with expected distal airway diameters. At the carina, the positioning of the join-sphere was refined to optimize the angles of each limb. The stent limb lengths were minimized to prevent obstruction of distal branches.
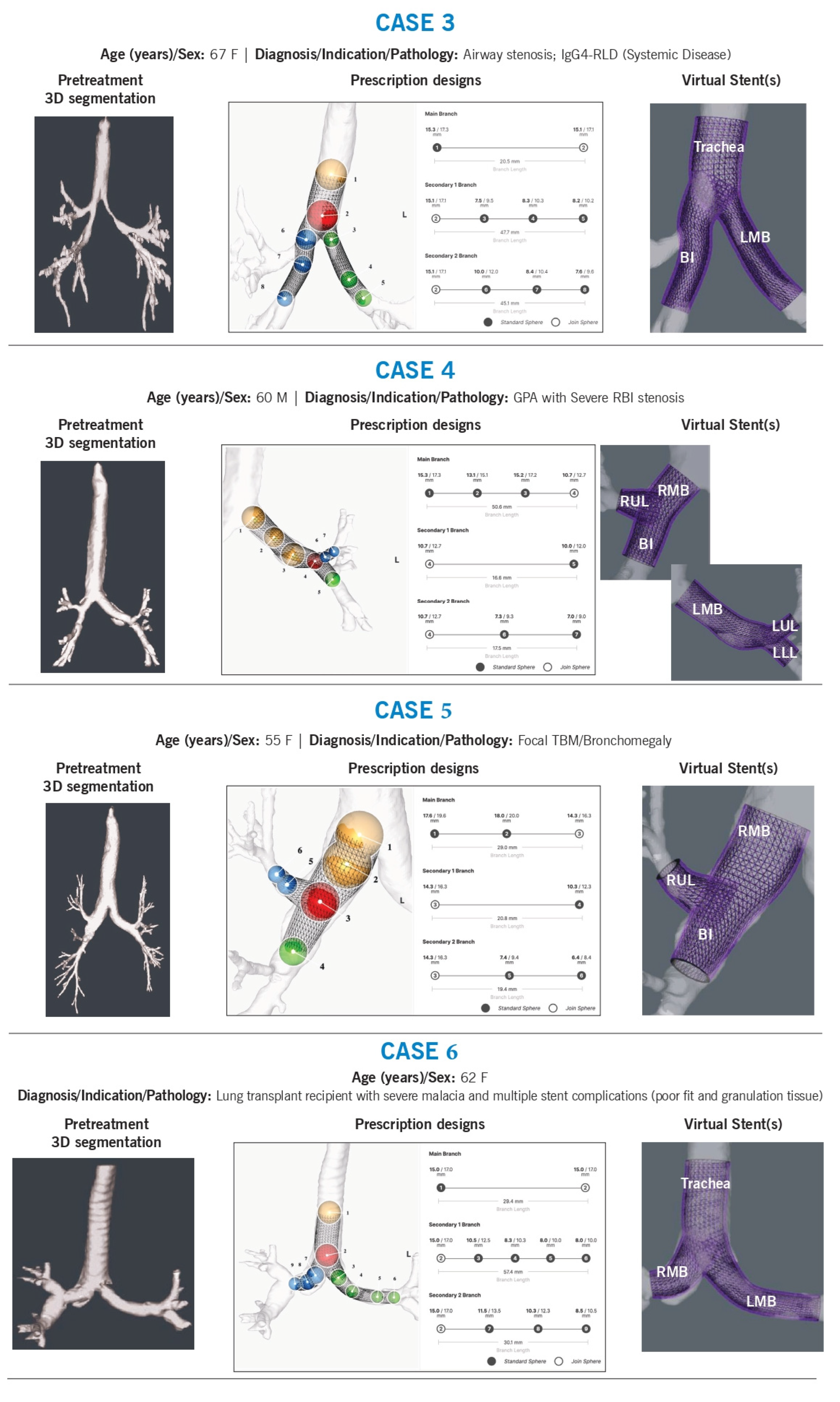
Case 3
Background: A 67-year-old woman with diffuse, multilevel airway stenosis received multiple 3DPS stents for the trachea, right bronchus intermedius (RBI), right lower lobe (RLL), and left mainstem.
Technical Challenges:
Size, shape, and angulation
Tapering
Airway preservation (avoiding luminal obstruction or “jailed airway segments”)
Intervention & Design Rationale:
The patient had a significantly distorted main carina with an acute angle due to prior upper tracheal resection. Disease extended distally into the left mainstem and right bronchus intermedius, beyond the right upper lobe level.
To accommodate stenotic regions, the stents were oversized by approximately 2 mm, allowing for planned balloon dilation before implantation. The right mainstem stent was contoured along the medial wall and extended past the right upper lobe, with a fenestration designed to maintain ventilation. The tapered design and strategic sizing ensured adequate luminal patency while minimizing airway obstruction. The stent design also accommodated the abnormal main carina by ensuring precise contouring to prevent migration.
Case 4
Background: A 60-year-old man with granulomatosis with polyangiitis (GPA) had recurrent granulation tissue formation despite prior commercial stents. This was a complex case with mixed airway disease and several years of stent complications.
Technical Challenges:
Size, shape, and angulation
Intervention & Design Rationale:
Left Mainstem:
The left airway presented with significant malacia in a curved mainstem, potentially exacerbated by prior stents. The proximal stent was designed to match airway volume, while the distal portion was oversized (by 2–4 mm) to accommodate known strictures at the secondary carina. The sphere at the carina was positioned to extend into both the left upper and lower lobes while avoiding excessive distal airway oversizing. The stent met a minimum branch length of 15 mm but was excess length was intended to be trimmed before implantation.
Right mainstem:
A stent was designed to replace a previously customized hourglass stent, addressing a GPA-related stricture at the right bronchus intermedius (RBI) orifice. Minimal oversizing (<1 mm) was used in the right mainstem. The right upper lobe limb was slightly tapered and oversized by 1 mm, with precise angulation to ensure central placement. The RBI stent was contoured to restore near-normal luminal dimensions, with a slight distal taper to reduce granulation tissue formation. The stent was positioned 1–2 mm above the right middle lobe (RML) and RB6 orifice.
Case 5
Background: A 55-year-old woman with bronchomegaly at RC1 was managed for right mainstem malacia.
Technical Challenges:
Size, and shape
Intervention & Design Rationale:
The patient had focal right-sided malacia with recurrent infections. Previous stents were intentionally oversized to prevent migration but may have contributed to airway dilation over time. The airway stent was designed to match, rather than significantly oversize, the right mainstem. It tapered distally into the right bronchus intermedius (RBI) and right upper lobe to ensure proper fit. Given the short segmental anatomy of the right upper lobe, the stent was centered but extended through the segmental trifurcation, with the intention of trimming the stent prior to implantation, to maintain ventilation into segmental bronchi. The RBI stent was extended to the mid-RBI, ensuring adequate coverage of the malacic region.
Case 6
Background: A 62-year-old lung transplant recipient with non-anastomotic airway complications, received an airway stent treating the trachea, right mainstem, and left mainstem. She had a history of severe malacia and multiple prior stent failures due to poor fit and granulation tissue formation.
Technical Challenges:
Shape adaptation of abnormal airway anatomy
Intervention & Design Rationale:
The patient exhibited severe distal tracheal malacia, along with combined stenosis and malacia of both mainstem bronchi. The left mainstem bronchus had an almost horizontal orientation, while the right mainstem anastomosis was highly curved. The stent was designed to conform to these unique airway angles, with distal limbs extending just beyond both anastomoses to ensure proper support while preventing migration and airway obstruction.
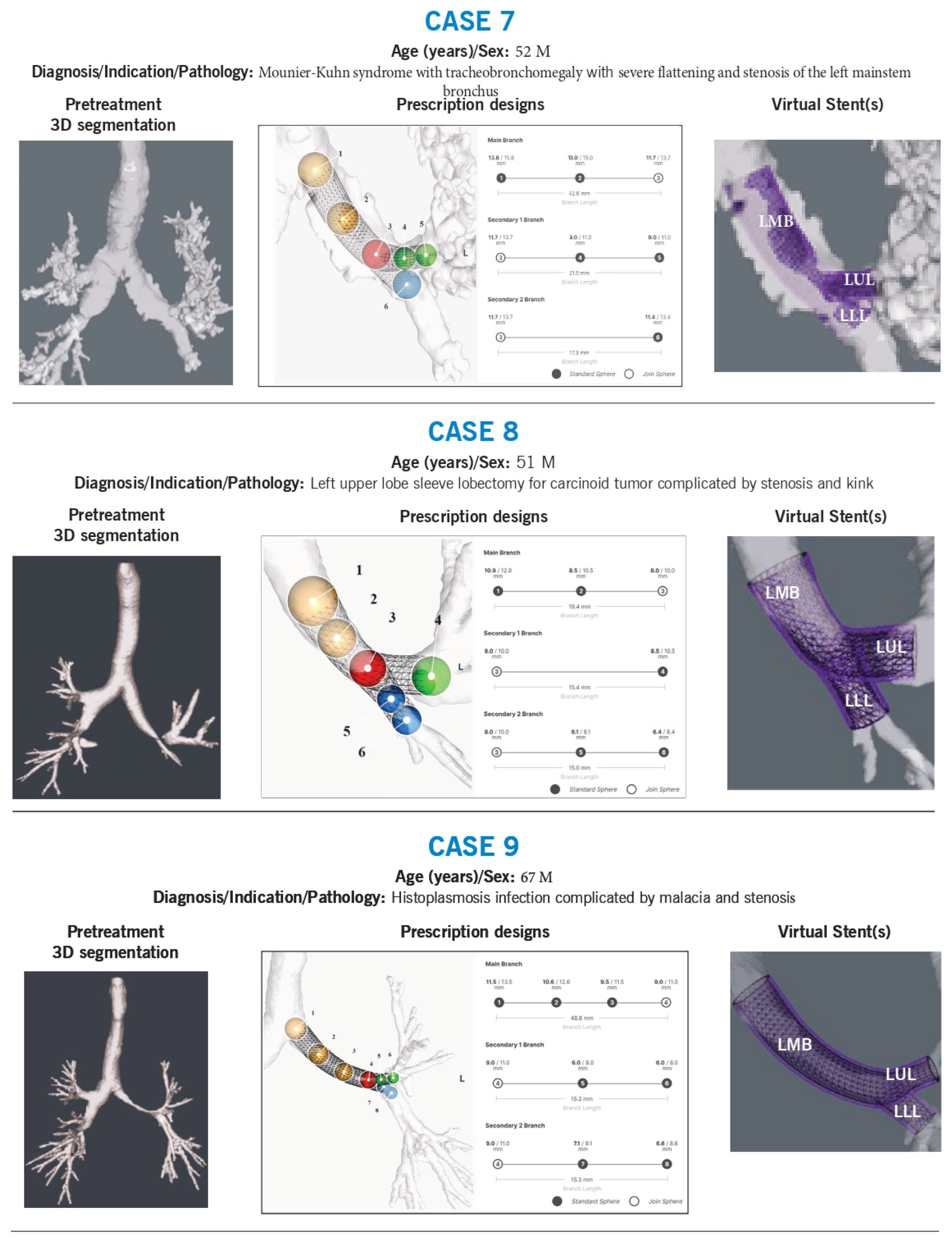
Case 7
Background: A 52-year-old man with Mounier-Kuhn syndrome and tracheobronchomegaly had severe flattening and stenosis of the left mainstem bronchus. Multiple prior stent placements were complicated by proximal migration.
Technical Challenges:
Size, and shape adaption
Stent migration risk
Intervention & Design Rationale:
The patient’s airways were markedly dilated, characteristic of Mounier-Kuhn syndrome. The left mainstem bronchus was particularly flattened (1 mm × 30 mm). Stent sizing was based on previous CT measurements and the fit of prior silicone stents (up to 16 mm). The stent was shaped to match the left mainstem morphology, with left upper and lower lobe limbs contoured for both stenting and anchoring, reducing the risk of migration.
Case 8
Background: A 51-year-old man with a history of left upper lobe sleeve lobectomy for carcinoid tumor developed a stenotic kink in the left mainstem.
Technical Challenges:
Size, shape, and angulation
Intervention & Design Rationale:
The left lower lobe exhibited stenosis at the sleeve anastomosis, with a non-anatomical airway conformation. Previous stenting attempts had failed. The new stent was designed with an outer diameter approximating the unaffected left mainstem (~12 mm) to maintain luminal integrity. The left lower lobe received two branches, one into the superior segment and another into the basilar bronchus, with dimensions based on preoperative CT measurements. The stent design evolved with subsequent placements to optimize fit and function.
Case 9
Background: A 67-year-old man with severe left mainstem and left upper lobe malacia due to histoplasmosis underwent multiple airway stent placements.
Technical Challenges:
Size, shape, length, and branch point alignment
Intervention & Design Rationale:
The first stent was designed using a 3D airway reconstruction in the setting of malacia but failed to fit properly in the left upper lobe and was removed. The second stent was modeled using a pre-malacia CT scan, ensuring anatomic precision and a superior fit, effectively restoring airway patency.
6. Discussion
Currently available stents are designed primarily in a single linear plane, which is suitable for short-segment stenosis but inadequate for complex airway pathologies. Metallic stents offer flexibility but may exert uneven pressure on the airway, while stock Y-stents can accommodate extrinsic compression without significant carinal distortion. However, many airway diseases result in multifocal or extensive involvement, leading to occlusion, distortion, and a combination of stenosis and malacia of varying lengths and diameters. Disease affecting the carina further complicates stent angulation and transitions between different lumen diameters and shapes. Thus, contouring a stent to the airway’s abnormal morphology while strategically adding volume to optimize airflow and reduce mechanical stress is crucial for improving its function and durability.
Since airway diseases are often non-linear, particularly at the carina, more adaptable solutions are required. Silicone stents allow further modifications, including shortening or creating side holes for branch access, enhancing their adaptability. These stents also possess specific mechanical properties such as durometer, modulus, hoop strength, and tear resistance that influence clinical outcomes; however, these parameters remain poorly understood and underutilized in clinical practice. Each stent on the market has some variability in these characteristics, and while experienced bronchoscopists may consider these properties during selection, the lack of standardized data limits evidence-based decision-making regarding optimal stent choice.
Proper stent sizing is crucial, as undersizing can lead to poor airflow, mucus buildup, and migration, whereas oversizing may cause airway trauma, rupture, or undue pressure on surrounding structures. Optimal selection involves placing a slightly oversized stent that maintains luminal patency while generating sufficient friction to resist migration. Diameter selection is typically guided by CT imaging, direct visualization, or sizing tools such as balloons or rigid bronchoscopes with known diameters to get a “feel” for the lesion [5,6,20]. Endoscopic sizing tools are also available to assist in ensuring appropriate fit [9,18,19].
The required stent length depends on disease extent and anatomical constraints; however, longer stents may impair mucociliary function and increase the risk of mucus occlusion. While metallic stents have fixed lengths due to prepacking and mesh integrity concerns, silicone stents can be trimmed and shaped intraoperatively to accommodate patient-specific needs [37].
Achieving optimal stent fit requires more than simply matching diameter and length; clinical judgement is essential to contour a prosthesis that provides adequate support while minimizing adverse tissue interactions. Advances in computational modeling offer promising avenues for stent customization by enabling precise volumetric adjustments tailored to complex airway morphologies.
Stent Deployment and Procedural Considerations
Stent deployment remains a critical aspect of the overall success of airway stenting. Standard rigid bronchoscopy tools, designed for linear, pre-manufactured stents, may not be well suited for unique contours of patient-specific designs. Regarding stent delivery, metal stents are preloaded for ease of placement, often utilizing guidewires or flexible bronchoscopic instruments that do not require rigid bronchoscopy. This makes them advantageous in certain scenarios. In contrast, silicone stents require manual loading and deployment, often necessating post-deployment adjustments or even removal and repositioning. Unlike metal stents, silicone stents can be reloaded, modified, or replaced, offering greater flexibility in complex cases.
From our experience, meticulous pre-procedural planning—incorporating 3D airway reconstructions before and after stent insertion—helps anticipate challenges and optimize fit. Intra operative stent trimming was required in several cases, highlighting the need for more flexible deployment systems that can accommodate customized stents. Future research should focus on developing dedicated deployment kits for 3D-printed stents and systematically evaluating post-deployment “settling” phase through serial imaging and bronchoscopic follow up.
Implications for 3DPS Stents and Future Directions
Our case series highlights that optimal stent fitting involves more than simply matching diameter and length—it requires a detailed understanding of the patient’s airway pathology and the dynamic interplay between the stent and airway structures. By leveraging 3D printing, we can tailor stent contours to provide targeted airway support while minimizing adverse tissue interactions. However, future investigations must systematically assess post-deployment outcomes, including the ‘settling’ phase, to determine whether these design principles translate into improved clinical performance. Respiration and coughing further influence stent positioning and function, necessitating ongoing assessment to validate these design strategies. This study emphasizes the importance of the design process, and the clinical decision making involved, while acknowledging that the final fit requires continuous evaluation.
Limitations
This study has notable limitations. As all cases involved Y-stents, we were unable to assess design-related factors influencing migration, which is typically less concerning with this configuration. Additionally, material properties were not extensively analyzed. The current stent model features a single wall thickness and base material, meaning its mechanical properties—such as softness (flexibility) and hoop strengh—are dictated primarily by diameter rather than intentional design variations. Furthermore, clinical outcomes were beyond the scope of this study, preventing meaningful evaluation of potential complications. The dynamic interaction between the stent and airway, particularly the post deployment settling phase, was not captured in our current analysis. Future work will integrate serial radiographic and bronchoscopic follow-up to better quantify stent fit and function.
Ongoing studies, including those registered under NCT03111888, aim to correlate stent parameters with objective oiutcomes such as migration, mucus clearance, and respiratory function. Although our current study focuses on design methodology, we recognize that the ultimate test of a stent’s efficacy lies in its clinical performance. Whether these advancements truly address the challenge of stent fit will require further post-deployment analysis in prospective studies.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, SAMPLE QUESTIONNAIRE USED.
Author Contributions
Conceptualization, T.R.G and R.K.; methodology, T.G.; software, A.B.; validation, T.G., R.K. and A.B.; data curation, P.N and C.Y.; writing—original draft preparation, P.N.; writing—review and editing, P.N., C.Y., A.B., R.K., TRG. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study because it does not involve direct human subject research requiring intervention, interaction, or access to identifiable private information. The study is based on retrospective analysis of airway-related data without patient-identifiable information, ensuring compliance with privacy and confidentiality regulations. Additionally, the interviews conducted with physicians focused on their expert opinions and clinical experiences rather than patient-specific data, classifying the study as non-human subject research. According to institutional and national ethical guidelines, studies that do not involve identifiable patient data or pose risks to human participants may be exempt from formal review.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
All data is available in the manuscript with no new data available elsewhere.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| 3DPS | Three-Dimensional Patient-Specific |
| CT | Computed Tomography |
| EDAC | Evidence-Based Data Acquisition and Critical Appraisal |
| GPA | Granulomatosis with Polyangiitis |
| LC1 | Left Upper Lobe Bronchus |
| PS | Patient-Specific |
| RBI | Right Bronchus Intermedius |
| RLL | Right Lower Lobe |
| RML | Right Middle Lobe |
| ILD | Interstitial Lung Disease |
| NCT | National Clinical Trial |
| Y-stent | Y-shaped Stent |
References
- Dumon, J.F. A Dedicated Tracheobronchial Stent. Chest. 1990, 97, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Jung HS, Chae G, Kim JH, Park CY, Lim S, Park SE, et al. The mechanical characteristics and performance evaluation of a newly developed silicone airway stent (GINA stent). Sci Rep. 2021, 11.
- Guibert N, Didier A, Moreno B, Lepage B, Leyx P, Plat G, et al. Treatment of complex airway stenoses using patient-specific 3D-engineered stents: a proof-of-concept study. Thorax. 2019, 74, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Palo, M.; Holländer, J.; Suominen, J.; Yliruusi, J.; Sandler, N. Expert Review of Medical Devices 3D printed drug delivery devices: perspectives and technical challenges 3D printed drug delivery devices: perspectives and technical challenges. 2017. [Google Scholar]
- Folch, E.; Keyes, C. Airway stents. Ann Cardiothorac Surg. 2018, 7, 273. [Google Scholar] [CrossRef] [PubMed]
- Facciolongo N, Piro R, Menzella F, Lusuardi M, Salio M, Agli LL, et al. Training and practice in bronchoscopy a national survey in Italy. Monaldi Arch Chest Dis. 2013, 79, 128–133. [Google Scholar]
- Sethi, S.; Gildea, T.R.; Almeida, F.A.; Cicenia, J.C.; Machuzak, M.S. Clinical Success Stenting Distal Bronchi for “Lobar Salvage” in Bronchial Stenosis. J Bronchology Interv Pulmonol. 2018, 25, 9–16. [Google Scholar] [CrossRef]
- Fruchter O, Raouf BA El, Rosengarten D, Kramer MR. Long-term Outcome of Short Metallic Stents for Lobar Airway Stenosis. J Bronchology Interv Pulmonol. 2017, 24, 211–215. [Google Scholar] [CrossRef]
- Miyazawa T, Miyazu Y, Iwamoto Y, Ishida A, Kanoh K, Sumiyoshi H, et al. Stenting at the flow-limiting segment in tracheobronchial stenosis due to lung cancer. Am J Respir Crit Care Med. 2004, 169, 1096–1102. [Google Scholar] [CrossRef]
- Tian, S.; Huang, H.; Hu, Z.; Dong, Y.; Bai, C. A narrative review of progress in airway stents. J Thorac Dis. 2022, 14, 1674–1683. [Google Scholar] [CrossRef]
- Guibert N, DIdier A, Moreno B, Mhanna L, Brouchet L, Plat G, et al. Treatment of post-transplant complex airway stenosis with a three-dimensional, computer-assisted customized airway stent. Am J Respir Crit Care Med. 2017, 195, e31–3. [Google Scholar] [CrossRef]
- Leon, C.A.; Inaty, H.; Urbas, A.; Grafmeyer, K.; Machuzak, M.; Sethi, S.; et al. EARLYOUTCOMESWITH, 3.D.P.R.I.N.T.I.N.G.A.N.D.A.I.R.W.A.Y.S.T.E.N.T.S. Chest. 2019, 156, A199–200. [Google Scholar] [CrossRef]
- Aravena, C.; Gildea, T.R. Patient-specific airway stent using three-dimensional printing: a review. Ann Transl Med. 2022. [Google Scholar] [CrossRef]
- Guibert, N.; Saka, H.; Dutau, H. Airway stenting: Technological advancements and its role in interventional pulmonology. Respirology. 2020, 25, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Guibert N, Mhanna L, Didier A, Moreno B, Leyx P, Plat G, et al. Integration of 3D printing and additive manufacturing in the interventional pulmonologist’s toolbox. Respir Med. 2018, 134, 139–142. [Google Scholar] [CrossRef]
- Hu, H.; Zhang, J.; Wu, F.; Chen, E. Application of the Montgomery T-tube in subglottic tracheal benign stenosis. J Thorac Dis. 2018, 10, 3070. [Google Scholar] [CrossRef] [PubMed]
- Mathew, R.; Hibare, K.; Dalar, L.; Roy, W.E. Tracheobronchial stent sizing and deployment practices airway stenting practices around the world: a survey study. J Thorac Dis. 2020, 12, 5495–5504. [Google Scholar] [CrossRef]
- Nobuyama, S.; Sato, T.; Handa, H.; Nishine, H.; Inoue, T.; Mineshita, M.; et al. Comparison of Airway Measurements for Tracheobronchial Stenosis Between Stereoscopic Bronchoscope, M.D.-C.T. J Bronchology Interv Pulmonol. 2017, 24, 296–302. [Google Scholar] [CrossRef]
- Hayashi, A.; Takanashi, S.; Tsushima, T.; Denpoya, J.; Okumura, K.; Hirota, K. New method for quantitative assessment of airway calibre using a stereovision fibreoptic bronchoscope. Br J Anaesth. 2012, 108, 512–516. [Google Scholar] [CrossRef]
- Cheng GZ, Folch E, Wilson A, Brik R, Garcia N, Estepar RSJ, et al. 3D Printing and Personalized Airway Stents. Pulm Ther. 2017, 3, 59–66. [Google Scholar] [CrossRef]
- Begnaud, A.; Connett, J.E.; Harwood, E.M.; Jantz, M.A.; Mehta, H.J. Measuring central airway obstruction. What do bronchoscopists do? Ann Am Thorac Soc. 2015, 12, 85–90. [Google Scholar] [CrossRef]
- Cheng GZ, Folch E, Brik R, Gangadharan S, Mallur P, Wilson JH, et al. Three-dimensional modeled T-tube design and insertion in a patient with tracheal dehiscence. Chest. 2015, 148, e106–8. [Google Scholar]
- Ost DE, Ernst A, Grosu HB, Lei X, Diaz-Mendoza J, Slade M, et al. Complications following therapeutic bronchoscopy for malignant central airway obstruction: Results of the AQuIRE registry. Chest. 2015, 148, 450–471. [Google Scholar]
- Dutau H, Breen D, Bugalho A, Dalar L, Daniels J, Dooms C, et al. Current Practice of Airway Stenting in the Adult Population in Europe: A Survey of the European Association of Bronchology and Interventional Pulmonology (EABIP). Respiration. 2018, 95, 44–54. [Google Scholar]
- Gildea, T.R.; Young, B.P.; Machuzak, M.S. Application of 3D printing for patient-specific silicone stents: 1-year follow-up on 2 patients. Respiration. 2018, 96, 488–494. [Google Scholar]
- Shan Q, Huang W, Shang M, Wang Z, Xia N, Xue Q, et al. Customization of stent design for treating malignant airway stenosis with the aid of three-dimensional printing. Quant Imaging Med Surg. 2021, 11, 1437. [Google Scholar]
- Shan Q, Huang W, Wang Z, Xue Q, Shi Z, Zhou J, et al. Preliminary Experience With a Novel Metallic Segmented Transcordal Stent Modified With Three-Dimensional Printing for Inoperable Malignant Laryngotracheal Stenosis. Front Oncol. 2021, 11.
- Tjahjono, R.; Chin, R.Y.K.; Flynn, P. Tracheobronchial stents in palliative care: A case series and literature review. BMJ Support Palliat Care. 2018, 8, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Cheng GZ, Folch E, Brik R, Gangadharan S, Mallur P, Wilson JH, et al. Three-dimensional modeled T-tube design and insertion in a patient with tracheal dehiscence. Chest. 2015, 148, e106–8. [Google Scholar]
- Fortin, M.; Dutau, H. Airway stents. ERS Monograph. 2017, 2017, 236–251. [Google Scholar]
- Gildea, T.R.; Young, B.P.; Machuzak, M.S. Application of 3D printing for patient-specific silicone stents: 1-year follow-up on 2 patients. Respiration. 2018, 96, 488–494. [Google Scholar] [CrossRef]
- Jung HS, Chae G, Kim JH, Park CY, Lim S, Park SE, et al. The mechanical characteristics and performance evaluation of a newly developed silicone airway stent (GINA stent). Sci Rep. 2021, 11, 7958. [Google Scholar]
- Felice C Di, Sethi S. Lung transplant anastomotic airway complications and bronchoscopic management. Current Challenges in Thoracic Surgery. 2022, 4, 8–8. [Google Scholar]
- Machuzak, M.; Santacruz, J.F.; Gildea, T.; Murthy, S.C. Airway complications after lung transplantation. Thorac Surg Clin. 2015, 25, 55–75. [Google Scholar] [PubMed]
- Murthy, S.C.; Gildea, T.R.; MacHuzak, M.S. Anastomotic airway complications after lung transplantation. Curr Opin Organ Transplant. 2010, 15, 582–587. [Google Scholar]
- Santacruz, J.F.; Mehta, A.C. Airway complications and management after lung transplantation: ischemia, dehiscence, and stenosis. Proc Am Thorac Soc. 2009, 6, 79–93. [Google Scholar]
- Breen, D.P.; Dutau, H. On-site customization of silicone stents: towards optimal palliation of complex airway conditions. Respiration. 2009, 77, 447–453. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



