Submitted:
20 March 2025
Posted:
21 March 2025
You are already at the latest version
Abstract
Syphilis is a disease caused by Treponema pallidum. It is primarily transmitted sexually or vertically during pregnancy. The origin is twofold, namely it comes from America or Europe. Syphilis was first recorded in human skeleton in the 11th century. However, signs of treponemal disease were observed in osteological material from Pleistocene bear. Hence, it is necessary to study syphilis on bone material to better understand the etiology of the above disease and consequently, introduce preventive measures. Literature review was performed, according to PRISMA statement. Examination of syphilis on skeletal material can be performed at the macroscopic and microscopic level. Those methods refer to the visual assessment of skeletal material, namely the identification of characteristic pathological changes caused by syphilis, such as periostitis, which manifests itself as thickenings on the bone surface, and syphilis nodules (gummata), which are defects in the bones. Most often, these changes are found on long bones such as the tibia, femur and skull. Radiological methods may be used, such as X-ray, computed tomography (CT), Micro-CT (ICT) as well as molecular examination. Summarizing, this review is an overview of the latest methodology regarding syphilis research on skeletal material, thanks to which it can better understand its genesis.
Keywords:
syphilis
; anthropologic diagnostics
; syphilitic bone lesions
1. Introduction
Paleopathology, studying ancient diseases through remains reconstructs past health patterns. It identifies diseases, such as syphilis, Hansen’s disease (leprosy), and tuberculosis via analyzing osteological remains [1]. Genesis of syphilis remains unclear. The most important hypotheses are that it developed in America and came to the Old World with the Columbus expedition or was present on the European continent before [2]. Syphilis played a great role in mankind’s history and persists as a threat to human health. The global incidence of syphilis in 2019 was over 14,000,000. Consequently, paleopathological research on syphilis plays an important role in better understanding the etiology of the above disease and therefore the possibility of faster implementation of preventive measures [3]. Nowadays the methodology for syphilis on bone material includes macroscopic analysis, namely relying on visual examination such as periosteal reactions and caries sicca, which are characteristic of tertiary syphilis for instance by X-ray, Computed tomography (CT), Micro-CT (ICT) [4] Another method is microscopic or histological analysis assures the evaluation of bone remodeling patterns. Molecular techniques rely on polymerase chain reaction (PCR) and ancient DNA (aDNA) analysis, showing direct evidence of Treponema pallidum infection [5]. Recently, it has been postulated that shotgun metagenomics may be another method for detecting syphilis on skeletal materials. This technique focuses on sequencing the genomes of entire microbial communities, without the need to culture them first [6].
Precious information about the past and presence of this disease can be obtained in paleopathological studies. They require diagnostic techniques, which allow distinguishing its marks in human remains. We present a literature review of such methods described in the literature until now. Our objective was to describe techniques used in diagnosing syphilis in paleopathological samples, especially in osseous remains.
2. Materials and Methods
PubMed, Embase, Web of Science, and Google Scholar were browsed using the following search terms:
- syphilis AND differentiation AND anthropology
- syphilis AND molecular AND anthropology
- syphilis AND markers AND anthropology
- syphilis AND imaging AND anthropology
- syphilis AND diagnostics AND anthropology
After the removal of duplicates, there were 125 papers. We included 92 of them, which filled the following criteria:
- The record was an original, peer-reviewed, and published study.
- The full text was available.
- The full text was in English.
- The full text was relevant to the topic of our review: it discusses how described diagnostic methods are being or can be used to detect osteological lesions or molecular marks caused by Treponema pallidum infection in anthropological samples and/or possibilities of differential diagnosis of those lesions.
The results of the review are presented in Figure 1.
3. Results
3.1. Macroscopic Analysis of Bone Lesions
Upon reviewing the selected literature, it becomes evident that macroscopic analysis, also referred to as gross examination, plays a pivotal role in the detection of syphilis in paleopathological research. This method serves as a fundamental approach, enabling researchers to identify skeletal remains likely afflicted by syphilis and to exclude those lacking bone lesions pathognomonic of the disease [1,2,3,7,8,9].
In some studies, stereo microscopes or hand lenses are employed to observe the lesions at low magnification [7,10,11,12]. Additionally, researchers often weigh and measure skeletal material before detailed gross examination to facilitate comparison with unaffected specimens, thereby aiding in diagnosis [1]. Bony alterations, such as pits, cavities, and thickenings, are also measured to provide a more detailed description of the material [12,13,14]. Researchers examine para-articular and articular bony surfaces under raw operating light [11,15] and describe the type and distribution of lesions to conduct accurate diagnoses [8].
Syphilis in paleopathological material is distinguished not only by alterations in bone structure but also by their pattern of occurrence and the specific types of bones affected [16]. Some authors emphasize the significance of reassociating skeletal elements derived from a single individual that became disarticulated post-mortem, as this process aids in understanding lesion distribution in the afflicted remains [16].
Fragmented bones may undergo a process of restoration, enabling the observation of complete or nearly complete specimens [17]. The long bones, such as the tibia, femur, humerus, ulna, and radius, along with the cranium, are the most frequently affected, with the tibia being particularly prone to alteration [3,18,19,20,21] . Indeed, tibial lesions are present in 99% of individuals suffering from treponemal disease [10]. Alterations may also be observed in the clavicles, vertebrae, scapulae, ribs, and sternum [12,18]. Destruction of the frontal bone is considered characteristic of venereal syphilis, as is the involvement of the forearms and the tibia [22,23,24].
Given that syphilis is a systemic disease, the lesions are diffuse and broadly distributed across the skeleton [25]. They are present in 10-20% of individuals [18] and can be categorized as either unremodeled (active) or remodeled lesions [26]. Sclerotic, fibrous periosteal reaction with pitting is an active lesion highly suggestive of venereal syphilis [26]. Hypertrophic periostitis causes fusiform expansion and thickening of the shaft of long bones caused by the formation of subperiosteal new, woven bone over the normal, smooth cortex [26]. Sometimes, new bone appears in the form of raised plaques and spicules, which fuse and create bridges across shallow vascular grooves [27]. The surface of the new bone displays coarse striations and is porous, rugose, containing numerous pits (enlarged vascular foramina) as well as larger depressions with sclerotic bone at their borders (Figure 2a) [1,9,28,29].
In severe cases, the pathological process obliterates physiological bone surface markings [39], while the medullary cavity becomes progressively occluded by bone migration, with cancellous bone transforming into lamellar bone (Figure 2a) [20,22,30]. The latter can only be observed macroscopically at post-depositional breaks, e.g., in the broken-off shaft, illustrating the limitations of gross examination [26,27,30]. Excessive bone formation is also observed at muscle attachment sites [28,29,31].
The foregoing description encapsulates the diagnostic non-gummatous lesions of syphilis [18,23]. Saber shin tibiae and hints of gummatous lesions (reflecting the mixture of bone formation and destruction) are pathognomonic of treponemal infection but are rarely encountered in skeletal remains due to their late onset [18,19]. This also applies to long bone lesions, which primarily affect the diaphyses and do not typically exhibit bilateral characteristics until the disease reaches its tertiary stage [18,25,30,32].
Crania affected by syphilis often display a more lytic nature of lesions [31]. Oval or circular shallow depressions of the outer table of the cranium, most often located on the frontal bone, are characteristic of the disease [27]. These cavities tend to cluster and fuse, forming large, eroded areas [33]. The resulting lytic lesions, combined with irregular, sclerotic bone formed during the healing process, give rise to the characteristic caries sicca of the frontal bone, a hallmark of venereal syphilis (Figure 2b) [28]. This alteration appears as thick nodules separated by deep, stellate depressions, representing a gummatous lesion with a ‘worm-eaten‘ appearance [20,24,29,34,35,36].
Remodeled lesions, in contrast, constitute a healing process, resulting in the deposition of mature, smooth bone [26]. The co-existence of these alterations creates an irregular bone surface, giving the shaft an ‘inflated’ and ’wrinkled’ appearance (Figure 2a) [28,29].
Ernest G. Walker, in his 1983 study, presented an interesting case of syphilitic aortic aneurysm, which manifested as erosion of the sternal end of the right clavicle and the left side of thoracic vertebral bodies, both caused by the pulsatile activity of an aneurysm [37]. Certain authors reported syphilis affecting joints, leading to the destruction of their surface [18].
Furthermore, macroscopic examination aids in differentiating between venereal syphilis and other treponematoses (congenital syphilis, yaws, and bejel, also known as endemic syphilis). While bone lesions occurring in the tertiary stage of venereal syphilis, yaws, and bejel are similar, subtle distinctions exist [8,38]. These differences are most noticeable on the scale of a population and thus are labeled population variations [8,10,27,36]. Here, we aim to underscore the critical importance of geographical, environmental, epidemiological, and historical contexts, which provide indispensable assistance in differentiating between the treponematoses [7,8,26,27,28,29].
Regarding congenital syphilis, dental characteristics play a pivotal role in achieving a definitive diagnosis. Hutchinson’s incisors and Moon’s molars are considered the only dental alterations pathognomonic of the disease [39,40]. Thus, reduced dimensions combined with thinned enamel and occlusal notching of upper permanent incisors make the diagnosis unequivocal [18,41]. Hutchinson himself described them as ’screwdriver’ shaped due to their constricted occlusal surface (Figure 2e) [42]. It should be noted that their characteristic vertical notch is often worn away during life and thus is less visible in skeletal remains. Conversely, in some cases, the notch has not yet formed, and a thin enamel patch occupies its place [39,40,43]. Certain sources also identify a depression on the labial surface of the incisors as characteristic of the disease [40,43]. Apical hypoplasia and notching of the permanent canines are less indicative of the condition and warrant careful consideration [41].
Given inconsistencies in the literature, we would like to clarify the distinction between Moon’s first molars, also referred to as bud molars, and the mulberry molars described by Fournier [10,40,43]. Molars described by Moon are dome-shaped with a narrow occlusal surface and crowded cusps clustered at the center, as presented in Figure 2c [41,44]. In contrast, Fournier’s first molars exhibit a heavily atrophied cusp base and sinuses penetrating the dentine (Figure 2d) [39,41,43]. In both instances, the teeth are reduced in size compared to adjacent molars and show enamel hypoplasia [41,45]. These dental lesions differentiate congenital syphilis from yaws [32].
Syphilitic osteochondritis, manifesting as epiphyseal and metaphyseal erosion combined with cortical detachment and paradiaphyseal calcification, is characteristic of congenital syphilis, though it is less common than periostitis [7,15,30]. Periostitis, present in congenital and venereal syphilis as well as in yaws, complicates the differential diagnosis [30,46]. The well-known saber shin deformity, also termed ’pseudo-bowing’ caused by periostitis and subsequent subperiosteal bone formation, occurs more frequently in late congenital syphilis than in venereal syphilis [1], albeit it is also present in yaws and bejel in a less severe form [8,31]. However, only in congenital syphilis does saber shin remodeling progress to the extent capable of obliterating surface striating and rendering the diagnosis by visual examination almost impossible [46]. True bowing of the tibia is exclusive to childhood forms of treponematoses when the disease impacts immature bone, allowing anterior curving of the interosseous crest (Figure 3) [27,43].
As noted previously, the healing process in venereal syphilis leads to the deposition of new, smooth bone, occasionally obscuring all diagnostic markers visible to the naked eye [10]. By contrast, reactive bone remodeling in yaws produces a rugose surface, facilitating differentiation between these treponematoses [3]. George Higoumenakis describes enlargement of the sternal end of the clavicle as highly indicative of late congenital syphilis, which may assist in making a correct diagnosis when the cranium with teeth is not available for examination [47].
The number of bones affected and the localization of lesions are instrumental in distinguishing between the treponematoses (Figure 4) [46]. For instance, tibial lesions in venereal syphilis are often unilateral, contrasting with the bilateral presentation in yaws and bejel [10]. Yaws tends to affect a greater number of bones on average [46]. Additionally, hand and foot lesions are characteristic of yaws, while fibula is most often affected in bejel [8]. Nonetheless, a proper diagnosis cannot be conducted without defining the disease's pattern and prevalence within the examined population and comparing it to populations diagnosed during life, ideally focusing on tibial lesions [10,46,47,48,49].
It is essential to examine the skeletal material for additional pathologies and exclude other potential diseases before making a definitive diagnosis. Macroscopic analysis alone may be insufficient for conducting a differential diagnosis and may require supplementary diagnostic methods [18]. The diffuse nature of syphilitic lesions, coupled with the productive rather than destructive character of bony alterations, distinguishes the disease from pyogenic osteomyelitis [1], which is often noted as highly resembling treponemal infection [28,29]. Moreover, syphilitic lesions usually lack the sequestration diagnostic of pyogenic osteomyelitis [28].
Active cranial lesions are similar to those seen in fungal infections such as cryptococcosis and sporotrichosis, but these primarily affect the vertebrae, ribs, hands, feet, and joints [27,28,32]. Altered teeth seen in congenital syphilis may be difficult to distinguish from so-called mercurial teeth, which occur in patients treated with mercury. Both display a similar atrophied appearance, with enamel loss and dentine exposure [50,51,52]. Notwithstanding their resemblance, mercurial teeth are suggestive of syphilis themselves since mercury was extensively administered to syphilitic patients [45,51,52]. Teeth presenting both lesions characteristic of congenital syphilis and mercurial treatment are referred to as syphilitic-mercurial teeth [45]. Mercury exposure may also cause erosion of the dental alveoli [52,53]. Before conducting a definitive diagnosis, it is crucial to exclude the possibility of mistaking antemortem lesions for taphonomic processes or postmortem damage. Researchers confirm this, for instance, through the examination of specimens at low magnification (c. x40) [10]. This is particularly applicable to osteolytic lesions with destructive character [30], as postmortem erosion resembles crumbling of the external cortex [35]. Only in postmortem erosion do deeper structures of the bone come into sight [35].
A similar approach applies to metastasizing neoplasms, which usually produce lesions penetrating beneath the bone’s outer layer [54]. Lytic lesions of syphilis also resemble those present in tuberculosis (TB). However, TB can be excluded if the subject of concern is the cranium, as it is rarely affected by this disease [13]. Lesions of the ribs are highly suggestive of tuberculosis and should be considered in differential diagnosis [55]. Moreover, distinguishing between bone fractures and old, remodeled lesions presents challenges , albeit it is worth noting that fractures do not exhibit the stellate shape, in the form of which syphilitic lesions sometimes occur [23,36]. Other microorganisms capable of passing the placental barrier must also be considered in differential diagnosis of congenital syphilis, though only a few cause osteological symptoms [30].
It is noteworthy that researchers utilize macroscopic analysis not only as a preliminary screening tool but, in some cases, as a standalone method for definitive diagnosis [9]. The reliance on gross analysis alone varies depending on the study. However, it is crucial to recognize that gross examination is subject to potential biases and should be carefully considered before being used as the sole diagnostic approach for syphilis [20].
There are several limitations associated with diagnosis based on macroscopic examination of syphilitic bone lesions, the primary one being the condition of the skeletal remains themselves. Ideally, the specimens should be complete and well-preserved [33], but in reality, not all bones are in a sufficient condition for a proper examination [14,20,32,56,57].
In the matter of teeth, postmortem exfoliation of the enamel precludes the evaluation of their true width [41]. Additionally, visible bone lesions appear only in individuals who survived long enough for the disease to progress to its tertiary stage, where it can manifest in this specific manner [58]. As a result, skeletal lesions are relatively rare in syphilis [22,53,59].
3.2. Microscopic Analysis of Bone Lesions
The microscopic examination of bone lesions proves to play a pivotal role in the detection and differentiation of syphilis signs in palaeopathological research. It complements the macroscopic identification of the pathology, and by broadening the methodological approach, it potentially provides better diagnoses and assesses the preservation of bone and its constituent parts [10,31,61].
Histological thin sections are taken from visibly apparent pathological areas of the examined skeleton, and if possible, they are later compared with previously excavated and analyzed remains from the researched areas, thus resulting in finding common features and signs [13,57,61].
A microscopic examination aims at finding histological appearances that point to chronic, episodic, osteoclastic, and osteoblastic processes characteristic of syphilis [13,15,57]. It can use histological scales to make it more comprehensible. For example, one of these can be a histological index designed by Millard (2001) that can be used to make a general assessment of bone quality. This index ranks histological bone sections from 0-5, with the bottom values (i.e., 0) signifying no original features identifiable except possibly Haversian systems, to the top values (i.e., 5), where structures are very well-preserved and virtually indistinguishable from modern bone. Over the years, there were set criteria for differentiating and confirming the syphilitic origin of the apparent bone lesions [31]. One of those criteria can be those described by Schultz (1994, 2001, 2003) [10,12,61].
Worth noting is that microscopic examination of syphilitic bones may reveal extensive osteolysis, which was then followed by bone regeneration [13]. The especially vulnerable region is the periosteal cell directly adjacent to the skin. Moreover, the suppressed osteosynthesis on the endosteal side can be caused by treatment using arsenic due to misdiagnosis.
In the histological section, the mosaic structure of the diploe that is typical for this disease can be seen (Schultz, 1994). Numerous broad tangential lamellae can be found, which are partly interrupted by well-developed, relatively large blood vessel sinuses [57].
Another noticeable observation can be the presence of a Maltese cross in the polarized light, as it denotes good preservation of lamellae in osteon structures [15,62]. Subsequently, the diagnostic criteria described by Schultz are used for differentiating venereal syphilis from other specific and nonspecific inflammatory diseases. It states that the periosteal thickening of long bone shafts and the concomitant microscopic changes seen in venereal syphilis are a regular occurrence, most noted when the process of healing and remodeling of compact bone has not yet finished [61].
The primary criterion is the presence of lines or band-like structures called the „Grenzstreifen,” which separate the primary cortical bone from the active periosteal new bone layer laid down during bouts of infection. The next criterion is called the ‘‘Polster,’’ which represents a pillow-like villous proliferation of very dense parallel lamellae found in the highly thickened periosteal layer of cortical bone in the shaft of a long bone, e.g., tibia. There can also be present sinuous resorption lacunae between the original bone surface and the newly calcified layers, which can suggest syphilis but are also found in other nonspecific inflammatory diseases [61,63].
The histological examination may not only show signs of existing pathology, but it can also indicate the age of when the first lesions formed and how long the process has been undergoing. Histological assessment can be based on the number of present fragments of remodeled osteons and the amount of non-osteal vascularization [54,61]. It’s worth noting that the detection of interstitial lamellae, being the remains of earlier generations of lamellae postponed from the periosteal and endosteal side, may confirm the age estimated by the macroscopic analysis [13].
It's important to be aware of the possibility that besides the presence of microscopic signs in the bone section, there can be changes that are not of syphilitic etiology, such as microorganism focal destruction in the form of Wedl canals (described by Hackett, 1981), fungal and microorganism intrusion of unknown origin and additionally, foreign materials, e.g., soil, crystals within lacunae and/or Haversian systems can be visible [61]. Therefore, the lack of good osseous preservation may lead to some difficulties in discerning microscopic structures indicative of syphilis and, in some cases, even make it unattainable by the sole microscopic analysis, which indicates the importance of extending the methodology by other diagnostic means, which allows for an improved diagnosis and better understanding of the disease process Multiple lines of evidence in support of a hypothesis are fundamental in paleopathology [10,31,61].
Some studies are using fluorescent microscopy besides common light microscopy. The use of fluorescence allows us to make visible and measurable compounds in the bone. As an example, it can reveal bone matrix saturation with hydroxyapatite and present inclusions of foreign compounds. Unfortunately, the analysis and interpretation can be disturbed by the presence of minor impurities [10,13,31,61].
3.3. Radiological Examinations
Radiological examinations represent the optimal solution and support for macroscopic examinations. They facilitate enhanced visualization of pathological changes in bones, facilitate differential diagnosis of bone lesions, and enable the exclusion of other bone-related diseases
3.3.1. X-Ray
X-rays are a valuable tool in the diagnosis of infectious diseases such as whooping cough, pneumonia, and syphilis, as detailed in this work. This imaging modality enables the visualization of alterations in the cortical layer of the bone, facilitating a crucial evaluation of disease progression.
In the case of X-ray imaging of the humerus, it was observed that in a patient suffering from syphilis, there was evidence of slight widening, contour irregularities, and lytic changes in the central part of the distal areas [7]. This destructive lesion was observed in the lateral aspect of the metaphysis, where a calcified linear periosteal reaction was also present. Conversely, no radiopaque bands were identified in the metaphysis [15].
However, an X-ray examination of the shaft of the left ulna revealed the presence of a destructive lesion accompanied by an exuberant lamellar periosteal reaction, described as 'onion skin' [15].
Additionally, syphilitic lesions may be identified during the diagnosis of long bones, including the femur and tibia. The photographs illustrate a periosteal reaction that is generalized in nature, as well as zones of extensive obliteration of the medullary cavity that is sclerotic. Additionally, the bones exhibited thickened periosteum and narrowed partially obliterated medullary cavities [33]. In some cases, the outer layers of the femoral cortical bone become detached in their distal region [7].
A radiological examination revealed the presence of a homogeneous spongy network in the hemifrontal region, although some irregular areas were also discernible. The periosteal junction area of the vault on the right hemifrontal and both parietals exhibited extensive new bone formation [30]. Upon examination of the parietal bones, star-shaped, clear areas with surrounding sclerotic bone were observed, which exhibited an identical appearance to the healed lesions in modern cases [35].
3.3.2. CT Imaging
Computed tomography (CT) is a method that provides superior imaging of pathological alterations in the bones in comparison to a conventional X-ray. In the analysis and imaging of bone samples, scanning is conducted in layers. This is employed to reinforce the case for infectious systemic diseases and to visualize alterations in the cortical layer of the bone [64].
In cases of Treponema pallidum infection, the skull CT imaging may reveal evidence of osteolysis and lesions that penetrate the frontal bone, resulting in the formation of serpiginous cavities. Such lesions may subsequently progress to the right orbit, where remodeling of the nasal aperture is evident, as well as the inferior nasal conchae. On CT scans, the lesions are shown as translucencies and thinning in the cortical and diploë bone. The CT scan even revealed a process of already ongoing inflammation within the anterior cranial fossa and the left side of the middle cranial fossa [13].
In some cases indicating a more advanced stage of progression, on the frontal bone, the destructive changes are significantly more severe, exhibiting clustered pitting, erosion of the bone, and marked cavitation. Additionally, nodule formation may occur in some more discrete areas. The aforementioned lesions and their characteristic locations are consistent with those observed in cases of venereal syphilis. This form of syphilis primarily affects the frontal and parietal bones of the neurocranium, where the periosteum adheres closely to the bone surface [65].
It should be noted, however, that the spirochetes do not merely penetrate the aforementioned skull bones; they also invade the occipital bone where a 'worm-eaten' appearance is produced [3,66].
Additionally, alterations resulting from syphilis can be observed in the femurs, as evidenced by computed tomography (CT) imaging, which reveals focal destruction and a cavity. Upon sagittal sectioning, the femurs display extensive cavitations that penetrate deeply into the cortex and regions where the cortex has thickened, resulting in a reduction of the marrow cavity area. Also, in the case of femurs, spirochetes can cause a ‘worm-like’ appearance of the bone with rounded edges [3].
Imaging studies of other bones, for example, the tibia, reveal osteolytic changes in the new bone in the anterior part and a reduction in the density of the original bone. In contrast, a CT scan of the ischium revealed the presence of diffuse lytic structures, initially visible as pitting concentrated on the bone surface [9].
3.3.3. Micro-CT Imaging
Micro-CT (ICT) represents a novel three-dimensional imaging method that facilitates high-resolution imaging of samples. Although this new solution is expensive, it offers a wider range of imaging possibilities due to the use of a focused X-ray beam and a surface detector. This enables the visualization and analysis of defects in bone microarchitecture caused by Treponema pallidum. It can thus be concluded that the method is primarily employed for investigations about the altered mechanical properties of bone [67].
It has been demonstrated in studies that tertiary syphilis is responsible for at least one cranial perforation, which can be identified by comparing macerated skulls with those that are not affected. The majority of these perforations affect the visceral skull, as evidenced by the observation that they are present in up to 80% of the 20 skulls that were analyzed. Conversely, the neurocranium was similarly affected by syphilitic infection in the same study, with 50% of individuals exhibiting evidence of this. Another notable characteristic of the infection is the complete porosity of the bones observed in patients. Additionally, thinning of the cerebral cortex, sclerotic reorganization, and loss of cortex can be observed in the majority of individuals [4]. The use of 3D μ-CT images has revealed a common phenomenon, namely osteolytic destruction of the outer lamina and the formation of cavities within the diploe. Subsequently, the entire cavity may become filled with secondary woven bone. As a consequence of these processes, the outer and inner lamina may undergo thickening (total diameter 10 mm instead of approximately 4 mm), and the area may exhibit a relatively smooth surface. The thickening is visible in the bulging part of the outer lamina and the thinner part of the inner lamina. ICT provides information on the thickening of the beads and their isotropic arrangement. Furthermore, the center of the dipole displays additional indentations of varying dimensions [57]. The non-destructive imaging method has proved invaluable in identifying a wide range of skeletal disorders caused by tertiary syphilis [4].
Nevertheless, this imaging technique also permits the observation of lesions resulting from congenital syphilis. All specimens exhibited the presence of extensive new bone on both the periosteal and intraperitoneal surfaces. Conversely, the separation of growth plates was observed in some long bones [68].
In conclusion, micro-CT imaging offers significant potential for the diagnosis of bone diseases, enabling the performance of a range of studies without the destruction of specimens. This method can make a substantial contribution to the advancement and expansion of knowledge in this field.
3.4. Genetic Techniques
Nine of the included papers concerned the detection of spirochete DNA in fossil material. In all of them, an attempt was made to extract ancient DNA (aDNA) and then multiply it by PCR and detect it. Molecular studies were always accompanied by macroscopic methods and, in some publications, also by radiological methods. The remains came from areas of the US, UK, France, Spain, Hungary, Brazil, Mexico, and Canada, and their ages ranged between the 16th and first half of the 20th century. Skeletons of fetuses, newborns, children, adults, and the elderly were examined. A total of 153 individuals’ bones were examined who were suspected of having syphilis based on macroscopic changes [6,55,56,58,60,69,70,71,72,73].
The extraction of aDNA in the different studies followed a similar pattern. The sources of genetic material were bone fragments from the skull, teeth, ribs, femurs, and fibula. In one study, an unsuccessful attempt was made to extract Treponema pallidum aDNA from dental calculus [6]. It is worth noting the attempt to use LPA to purify genetic material in one study [55].
Detection of aDNA of Treponema pallidum was successful in 5 studies for a total of 9 deceased [56,58,69,71,72]. These included two fetal skeletons, four neonates, and two women whose ages were estimated to be <17 and <18 years. The common feature of the positive cases was a young skeletal age. However, in the same study, other samples subjected to the same procedure and of similar age yielded negative results.
The search for T. pallidum aDNA in historical remains has advantages and limitations. The selection of specific primers (Eco47III) for PCR allows for an unambiguous diagnosis, which is challenging with macroscopic techniques [69]. For the detection of spirochete genetic material, 50 mg of bone dust is sufficient, while a larger fragment is needed for macroscopic evaluation. However, genetic techniques involve the permanent destruction of the collected sample [70]. Although the methods discussed are successful in searching for aDNA of some bacteria, e.g., M. tuberculosis [55], they do not show high efficacy for syphilis and are not part of routine testing. Researchers point out that the reason is a course of syphilis and the biochemical characteristics of the spirochete itself [55].
Treponema pallidum has a sensitive outer membrane [74], in contrast to most Gram-negative bacteria lacking lipopolysaccharide (LPS) [75]. This makes spirochetes susceptible to destruction by detergents, heat, and desiccation [76,77]. Barnes & Thomas (2001) attribute failure in their investigation to weak cell walls [60]. The researchers emphasize that the detection of the aDNA of T. pallidum is due to the focus on those who died of congenital syphilis, as younger patients have significantly more spirochetes in their skeleton [58]. The success of the aDNA Treponema detection to criteria adopted based on epidemiological data and mainly the pathophysiology of the disease, Additional factors affecting the detection of aDNA are temperature or soil type [74,75].
3.5. Detection of Heavy Metals
Four of the included articles involved measuring mercury concentration in bone material and arsenic and lead in one case. In all cases, this method occurred together with macroscopic and radiological techniques. Bones in three of the research studies originate from cemeteries in Poland, and one concerns an anatomical collection from the USA. In total, measurements were carried out on one child skeleton, nine male and eleven female skeletons, dated between the 15th century and the early 20th century. ICP-OES, LA-ICP-MS, and pXRF were used. In only one case there was arsenic level detected that were higher than in remains without signs of syphilis, and in two cases there was found elevated level of mercury [13,78]. The first of them is also the only case of acquired syphilis among those investigated; in the others, a congenital form of the disease was suspected. Mercury was used in the treatment of congenital and acquired syphilis, but because of its toxicity and unclear effectiveness, it was abandoned at the beginning of the XX century. That’s why measuring its concentration may seem an interesting diagnostic technique.
3.6. Case Reports
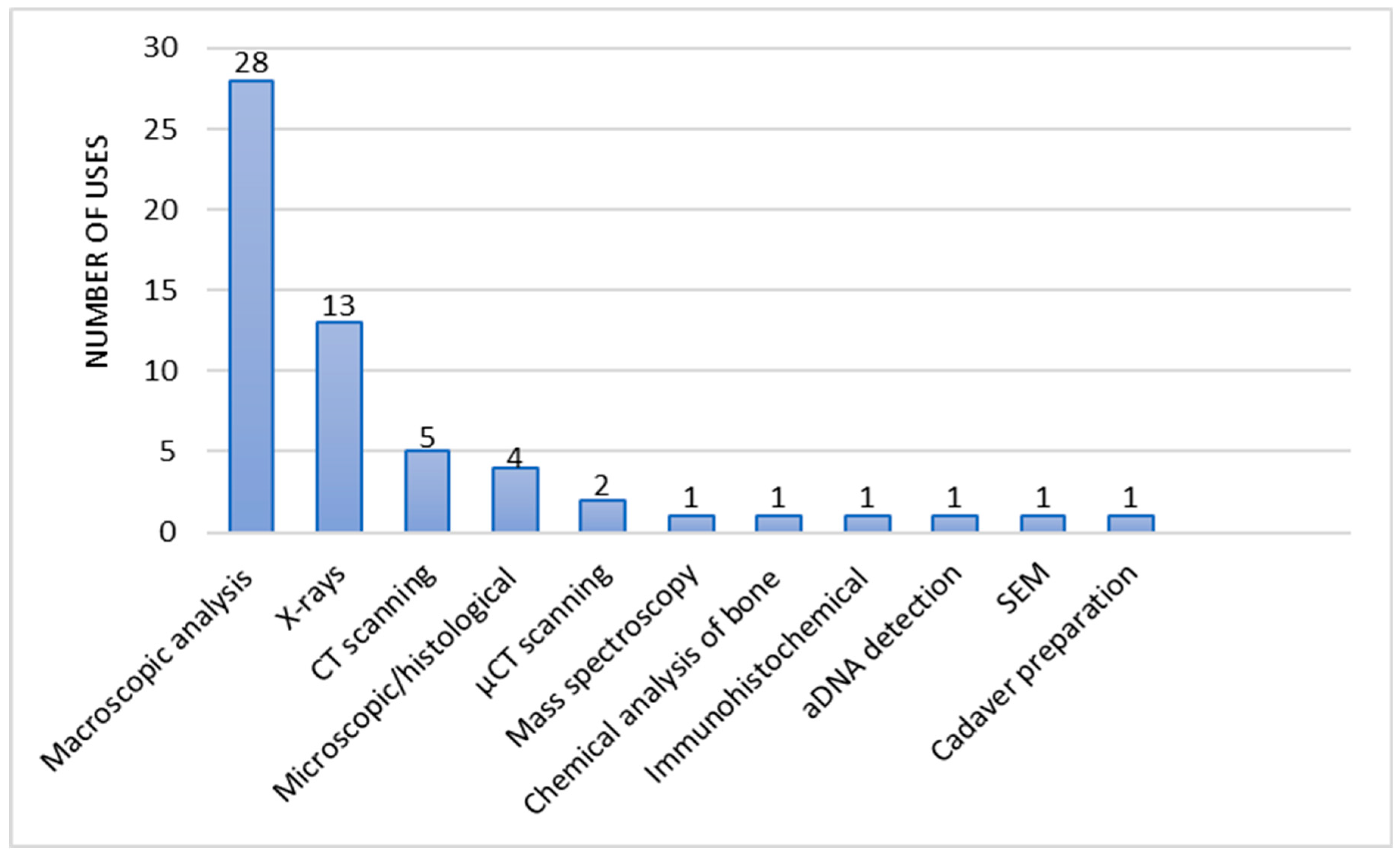
A total of 31 case reports were analyzed in this paper [12,13,15,16,28,30,32,50,51,63,73,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98]. The methods used in the reports consisted of macroscopic analysis of bone lesions, X-rays, CT scanning, microscopic or histological analysis of bone lesions, micro-CT scanning, mass spectroscopy, chemical analysis of the bone composition, immunohistochemical methods, aDNA detection, SEM scanning, and cadaver preparation. Diagnostic methods were identified and assigned to each case report. The methods used were counted for each study, the number of which is shown in Figure 5. The number of uses of each diagnostic method was then calculated and shown in Figure 6.
Among the case reports reviewed, macroscopic analysis of skeletal changes was also, as in the research articles reviewed, the primary method to begin the diagnostic process. In some unequivocal cases of finding pathognomonic lesions, it happened to be the only method needed to diagnose treponemal disease. In numerous of the cases reviewed, the authors diagnosed [2,3,4,7,8,9,22,26] or presumed [31,50,69] congenital syphilis. Hutchinson's incisor, mulberry molar, darkened tooth enamel, and hypoplastic defects found in one specimen provided convincing confirmation of the diagnosis of congenital syphilis [2]. In some cases, radiological examinations were carried out to complement the macroscopic evaluation of bone lesions.
With the help of regular X-ray imaging were observed changes characterizing chronic inflammatory processes such as Harris lines or signs of osteoarthritis [8]. In addition to non-specific changes, it was possible to visualize the Wimberger’s sign, which is typical of the congenital form of syphilis [8,22]. Micro-CT imaging was used to detect lesions of the still hidden permanent dentition in a sub-adult individual [31] CT scanning was the third most frequently chosen diagnostic method. Its use allowed confirmation of initial diagnoses made using macroscopic bone analysis [56] and also allowed the depth of the lesion to be determined [48]. SEM imaging was used to better visualize small lesions on the teeth [26]. Indirect immunofluorescence with human anti-treponema pallidum antibodies revealed syphilis in a Renaissance mummy [61]. The preparation of the cadaver was necessary to expose the subsequently analyzed bone lesions hidden under the mummified tissues in another mummy [4]. DNA analysis helped confirm the diagnosis of syphilis and even pinpoint the pathogen subspecies responsible - Treponema pallidum subsp. Pallidum [70].
4. Discussion
Macroscopic analysis is frequently employed as an initial sorting technique, categorizing skeletal remains by the presence of bone lesions characteristic of treponemal infection before detailed investigation using microscopic, radiological, histological and molecular methods [1,3,4,6,13,22,26,31,48,50,55,56,61,69,70,99]. This ‘top-down’ methodology allows for an overarching perspective on the specimens under examination and the confirmation of macroscopic observations [13,15,61]. Researchers usually distinguish lesions associated with syphilis based on classical literature published in the 19th and 20th centuries authored by pioneering figures in the diagnosis of the disease, such as Hutchinson, Moon, Fournier, Williams and Hackett [9,26,31,41,45,50,65,100,101,102].
Conducting a valid diagnosis requires considerable deduction and logical reasoning from the researcher, particularly since skeletal remains are often incomplete. Consequently, the best results are obtained by integrating macroscopic analysis of the lesions with the epidemiological, historical, and geographical context of the examined population [10]. Despite this innovative approach of differentiating between the treponematoses through the combination of macroscopic examination and population analysis [10], which is highly respected by some authors [36], other researchers still argue that different diagnostic methods may offer greater reliability [20,35,47]. On the contrary, it is essential to recognize that macroscopic analysis allows the examination of rare or highly damaged specimens, which cannot be sectioned and used for microscopic or molecular analysis [40,61,70]. Besides, in certain cases, it remains the only diagnostic method available due to the absence of necessary equipment [103].
Analysis of the histopathological images allows a more comprehensive view of the researched diseases and confirms the diagnosis or negates it, leading on to the other possible etiology. Further expansion of knowledge in the field of microscopic analysis in paleopathology can greatly benefit future research. However, useful newer analysis has shown that some of the „indicative” microscopic signs of syphilis, like Grenzstreifen and Polsters, are present in other diseases such as leprosy or nonspecific inflammatory diseases (e.g., hematogenous osteomyelitis). The difference relies on the manner of production of bone mass - syphilitic structures are laid down gradually, solidly organized as opposed to the rapid, disorganized structures in nonspecific inflammatory diseases [31]. It’s worth noting that the differentiation of syphilis with other treponematoses, yaws, and endemic syphilis can also be difficult based only on those histological signs [10,13,31,61].
The use of computed tomography (CT) scanning as a diagnostic tool for syphilis, particularly at different stages of the disease, serves as a valuable complement to other diagnostic methods. Meanwhile, genetic techniques show promise, especially in diagnosing congenital syphilis and cases involving individuals who died at a young age. Ongoing research in this area may lead to significant advancements. However, it is important to recognize the limitations associated with these approaches.
Syphilis, also known as „Great Imitator,” can be misdiagnosed as either a tumor, tuberculosis, bone inflammations, or leprosy, which could have been treated with arsenic compounds in the past. Arsenic was a far-ranging drug, too, because of its antiseptic, antipyretic, cholagogic, diastolic, calming, and tonic properties. Moreover, it was used as a component of paints or stained glass as well as for leather and wood preservation [76]. It blocks the protein’s sulfhydryl groups, which leads to cell cycle arrest in the S phase and, therefore, to inhibition of bone regeneration [13,15,57,61]. Regarding mercury, it must be noted that in the Middle Ages and Early Modern period, mercury was also used as a laxative as well as a drug for conjunctivitis, corneal irritation, psoriasis, eczema, tinea, skin lesions, and others [77]. Therefore, researchers should take this into consideration while measuring heavy metals concentration in bone material.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
No research data available due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CT | Computed tomography |
| ICT | Micro-computed tomography |
| PCR | Polymerase chain reaction |
| DNA | Deoxyribonucleic acid |
| aDNA | Ancient deoxyribonucleic acid |
| SEM | Scanning electron microscope |
| LPA | Linear polyacrylamide |
| ICP-OES | Inductively coupled plasma optical emission spectroscopy |
| LA-ICP-MS | Laser ablation inductively coupled mass spectrometry |
| pXRF | Portable X-ray fluorescence |
References
- Cole, H.N.; Harkin, J.C.; Kraus, B.S.; Moritz, A.R. Pre-Columbian Osseous Syphilis Skeletal Remains Found at Kinishba and Vandal Cave, Arizona, with Some Comments on Pertinent Literature [Internet]. 1955. Available from: http://archderm.jamanetwork.com/.
- Dabernat, H.; Reis, T.M.; Tarasov, A.Y.; Artyukhov, I.P.; Nikolaev, V.G.; Medvedeva, N.N.; et al. Paleopathology of the population of Krasnoyarsk, central Siberia (Pokrovskiy and Voskresensko-Preobrazhenskiy cemeteries of the 17th- early 20th centuries). Archaeology, Ethnology and Anthropology of Eurasia. 2013, 41, 140–150. [Google Scholar] [CrossRef]
- Hernandez, M.; Hudson, M.J. Diagnosis and evaluation of causative factors for the presence of endemic treponemal disease in a Japanese sub-tropical island population from the Tokugawa period. Int J Paleopathol. 2015, 10, 16–25. [Google Scholar] [CrossRef]
- Fraberger, S.; Dockner, M.; Winter, E.; Pretterklieber, M.; Weber, G.W.; Teschler-Nicola, M.; et al. Micro-CT evaluation of historical human skulls presenting signs of syphilitic infection. Wien Klin Wochenschr. 2021, 133, 602–609. [Google Scholar] [CrossRef]
- Luo, Y.; Xie, Y.; Xiao, Y. Laboratory Diagnostic Tools for Syphilis: Current Status and Future Prospects. Vol. 10, Frontiers in Cellular and Infection Microbiology. Frontiers Media S.A.; 2021.
- Austin, R.M.; Honap, T.P.; Mann, A.E.; Hübner, A.; DeGaglia, C.M.S.; Warinner, C.; et al. Metagenomic and paleopathological analyses of a historic documented collection explore ancient dental calculus as a diagnostic tool. Sci Rep. 2024, 14, 14720. [Google Scholar] [CrossRef] [PubMed]
- Malgosa, A.; Aluja, M.P.; Isidro, A. Pathological Evidence in Newborn Children from the Sixteenth Century in Huelva (Spain). International Journal of Osteoarcbaeology. 1996, 6. [Google Scholar] [CrossRef]
- Rothschild, B.M.; Rothschild, C. Treponemal Disease Revisited: Skeletal Discriminators for Yaws, Bejel, and Venereal Syphilis [Internet]. 1995. Available from: http://cid.oxfordjournals.org/.
- Schwarz, S.; Skytte, L.; Rasmussen, K.L. Pre-Columbian treponemal infection in Denmark?- a paleopathological and archaeometric approach. Herit Sci. 2013, 1. [Google Scholar] [CrossRef]
- Rothschild, B.M.; Calderon, F.L.; Coppa, A.; Rothschild, C. First European Exposure to Syphilis: The Dominican Republic at the Time of Columbian Contact [Internet]. 2000. Available from: http://cid.oxfordjournals.org/.
- Shuler, K.A. Life and death on a Barbadian sugar plantation: Historic and bioarchaeological views of infection and mortality at Newton Plantation. Int J Osteoarchaeol. 2011, 21, 66–81. [Google Scholar] [CrossRef]
- Castro, M.; Pacheco, A.; Kuzmanic, I.; Clarot, A.; Díaz, P. Treponematosis in a pre-Columbian hunter-gatherer male from Antofagasta (1830 ± 20 BP, Northern Coast of Chile). Int J Paleopathol. 2020, 30, 10–16. [Google Scholar] [CrossRef]
- Dabrowski, P.; Kulus, M.J.; Cieslik, A.; Domagala, Z.; Wiglusz, R.J.; Kuropka, P.; et al. A case of syphilis with high bone arsenic concentration from early modern cemetery (Wroclaw, Poland). Open Life Sci. 2019, 14, 427–439. [Google Scholar] [CrossRef]
- Vargová, L.; Vymazalová, K.; Horáčková, L. Evidences of children’s inflammatory diseases, trauma and tumours from the 13th to the 19th centuries in the czech lands. Anthropologie. 2021, 155–170. [Google Scholar] [CrossRef]
- Tomczyk, J.; Mańkowska-Pliszka, H.; Palczewski, P.; Olczak-Kowalczyk, D. Congenital syphilis in the skeleton of a child from Poland (Radom, 18th-19th century AD). Vol. 78, Anthropological Review. Versita; 2015. p. 79–90.
- Marden, K.; Ortner, D.J. A case of treponematosis from pre-Columbian Chaco Canyon, New Mexico. Int J Osteoarchaeol. 2011, 21, 19–31. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Mariotti, V.; Fusari, S.; Gasparini, A.; Bettuzzi, M.; Morigi, M.P.; et al. Syphilis in an Italian medieval jewish community: A bioarchaeological and cultural perspective. Int J Paleopathol. 2020, 30, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Anteric, I.; Basic, Z.; Vilovic, K.; Kolic, K.; Andjelinovic, S. Which theory for the origin of syphilis is true? Journal of Sexual Medicine. 2014, 11, 3112–3118. [Google Scholar] [CrossRef] [PubMed]
- P C Gerszten, E Gerszten, M J Allison. Diseases of the skull in pre-columbian South American mummies. Neurosurgery. 1998, 42. [Google Scholar]
- Walker, D.; Powers, N.; Connell, B.; Redfern, R. Evidence of skeletal treponematosis from the medieval burial ground of St. Mary Spital, London, and implications for the origins of the disease in Europe. Am J Phys Anthropol. 2015, 156, 90–101. [Google Scholar] [CrossRef]
- Somers, J.; Cooper, C.; Alterauge, A.; Lösch, S. A Medieval/Early Modern Alpine Population from Zweisimmen, Switzerland: A Comparative Study of Anthropology and Palaeopathology. Int J Osteoarchaeol. 2017, 27, 958–972. [Google Scholar] [CrossRef]
- El Najjar, M.Y. Human Treponematosis and Tuberculosis: Evidence from the New World. 1979.
- Hackett, C.J. Diagnostic Criteria of Syphilis, Yaws and Treponarid (Treponematoses) and of Some Other Diseases in Dry Bones. Diagnostic Criteria of Syphilis, Yaws and Treponarid (Treponematoses) and of Some Other Diseases in Dry Bones. 1976.
- Williams, H.U. The origin and antiquity of syphilis. The evidence from diseased bones. Arch. Pathol. 1932, 13, 931–83. [Google Scholar]
- Weston, D.A. Investigating the specificity of periosteal reactions in pathology museum specimens. Am J Phys Anthropol. 2008, 137, 48–59. [Google Scholar] [CrossRef]
- Buckley, H.R. Subadult Health and Disease in Prehistoric Tonga, Polynesia. J Phys Anthropol. 2000, 113. [Google Scholar] [CrossRef]
- Mays, S.; Crane-Kramer, G.; Bayliss, A. Two probable cases of treponemal disease of medieval date from England. Am J Phys Anthropol. 2003, 120, 133–143. [Google Scholar] [CrossRef]
- Stirland, A. Pre-Columbian Treponematosis in Medieval Britain. International lournal of Osteoarchaeology. 1991, 1. [Google Scholar] [CrossRef]
- Suzuki, T. Typical Osseous Syphilis in a Medieval Skeletal Remains from Hokkaido. 1984.
- Palfi, G.; Dutour, O.; Borreani, M.; Brun, J.P.; Berato, J. Pre-Columbian Congenital Syphilis from the Late Antiquity in France. Int J Osteoarchaeol. 1992, 2, 245–261. [Google Scholar] [CrossRef]
- Lewis, B. Treponematosis and Lyme Borreliosis Connections: Explanation for Tchefuncte Disease Syndromes? American Journal Of Physical Anthropology. 1994, 93. [Google Scholar] [CrossRef]
- Maryna Steyn, M.H. Pre-Columbian Presence of Treponemal Disease: A Possible Case from Iron Age Southern Africa [Internet]. 1995. Available from: http://www.journals.uchicago.edu/t-and-c.
- Buzhilova, A. Medieval Examples of Syphilis from European Russia. Int. J. Osteoarchaeol. 1999, 9. [Google Scholar] [CrossRef]
- Hackett, C.J. An Introduction to Diagnostic Criteria of Syphilis, Treponarid and Yaws (Treponematoses) in Dry Bones, and Some Implications*. Virchows Arch. A Path. Anat. and ttistol. 1975, 368. [Google Scholar] [CrossRef]
- Mitchell, P.D. Pre-Columbian treponemal disease from 14th century AD Safed, Israel, and implications for the medieval eastern Mediterranean. Am J Phys Anthropol. 2003, 121, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Pineda, C.; Mansilla-Lory, J.; Martínez-Lavín, M.; Leboreiro, I.; Izaguirre, A.; Pijoan, C. Rheumatic diseases in the ancient americas: The skeletal manifestations of treponematoses. Journal of Clinical Rheumatology. 2009, 15, 280–283. [Google Scholar] [CrossRef] [PubMed]
- Walker, E.G. Evidence for Prehistoric Cardiovascular Disease of Syphilitic Origin on the Northern Plains. American Journal Of Physical Anthropology. 1983. [Google Scholar] [CrossRef]
- Rothschild, B.M.; Heathcote, G.M. Characterization of the Skeletal Manifestations of the Treponemal Disease Yaws as a Population Phenomenon Downloaded from [Internet]. Vol. 17, University of Iowa Libraries/Serials Acquisitions. 1993. Available from: http://cid.oxfordjournals.org/.
- Fournier, A. Syphilitic teeth. Dental Cosmos. 1884, 26, 12–25. [Google Scholar]
- Hillson, S.; Grigson, C.; Bond, S. Dental Defects of Congenital Syphilis. 1998.
- Jacobi, K.P.; Cook, D.C.; Corruccini, R.S.; Handler, J.S. Congenital Syphilis in the Past: Slaves at Newton Plantation, Barbados, West lndies. American Journal O F Physical Anthropology. 1992, 89. [Google Scholar] [CrossRef]
- Hutchinson, J. Syphilis. Prepubescent syphilis. 1885.
- Nystrom, K.C. Dental evidence of congenital syphilis in a 19th century cemetery from the mid-hudson valley. Int J Osteoarchaeol. 2011, 21, 371–378. [Google Scholar] [CrossRef]
- Moon, H. On irregular and defective tooth development. Trans Odontol Great Britain. 1877, 9, 223–243. [Google Scholar]
- Ioannou, S.; Hunt, D.; Henneberg, M. Five Cases of Dental Anomalies Attributable to Congenital Syphilis from Early 20th Century American Anatomical Collections. 2017. [Google Scholar]
- Rothschild, B.M.; Rothschild, C. Congenital Syphilis in the Archaeological Record: Diagnostic Insensitivity of Osseous Lesions. 1997.
- Frangos, C.C.; Lavranos, G.M.; Frangos, C.C. Higoumenakis’ sign in the diagnosis of congenital syphilis in anthropological specimens. Med Hypotheses. 2011, 77, 128–131. [Google Scholar] [CrossRef] [PubMed]
- Vargová, L.; Vymazalová, K.; Vargová, L.; Horáčková, L.; Vymazalová, K.; Svoboda, J. Inflammatory changes on skeletons from the 16th to 17th century in Veselí nad Moravou, Czech Republic [Internet]. 2014. Available from: https://www.researchgate.net/publication/309041529.
- Rothschild, B.M.; Rothschild, C.; Doran, G. Virgin Texas: Treponematosis-Associated Periosteal Reaction 6 Millenia in the Past. Advances in Anthropology. 2011, 01, 15–18. [Google Scholar] [CrossRef]
- Radu, C.; Soficaru, A.D. Dental developmental defects in a subadult from 16th–19th centuries Bucharest, Romania. Int J Paleopathol. 2016, 15, 33–38. [Google Scholar] [CrossRef]
- Ioannou, S.; Henneberg, M.; Henneberg, R.J.; Anson, T. Diagnosis of Mercurial Teeth in a Possible Case of Congenital Syphilis and Tuberculosis in a 19th Century Child Skeleton. Journal of Anthropology. 2015, 2015, 1–11. [Google Scholar] [CrossRef]
- Zuckerman, M.K. More harm than healing? Investigating the iatrogenic effects of mercury treatment on acquired syphilis in post-medieval London. Open Archaeology. 2016, 2, 42–55. [Google Scholar] [CrossRef]
- Ioannou, S.; Henneberg, M. Dental signs attributed to congenital syphilis and its treatments in the Hamann-Todd Skeletal Collection. Anthropological Review. 2017, 80, 449–465. [Google Scholar] [CrossRef]
- Zhou, Y.; Gao, G.; Zhang, X.; Gao, B.; Duan, C.; Zhu, H.; et al. Identifying treponemal disease in early East Asia. American Journal of Biological Anthropology. 2022, 178, 530–543. [Google Scholar] [CrossRef]
- Jäger, H.Y.; Maixner, F.; Pap, I.; Szikossy, I.; Pálfi, G.; Zink, A.R. Metagenomic analysis reveals mixed Mycobacterium tuberculosis infection in a 18th century Hungarian midwife. Tuberculosis. 2022, 137. [Google Scholar] [CrossRef] [PubMed]
- Schuenemann, V.J.; Kumar Lankapalli, A.; Barquera, R.; Nelson, E.A.; Iraíz Hernández, D.; Acuña Alonzo, V.; et al. Historic Treponema pallidum genomes from Colonial Mexico retrieved from archaeological remains. PLoS Negl Trop Dis. 2018, 12. [Google Scholar] [CrossRef] [PubMed]
- Rühli, F.J.; Kuhn, G.; Evison, R.; Müller, R.; Schultz, M. Diagnostic value of micro-CT in comparison with histology in the qualitative assessment of historical human skull bone pathologies. Am J Phys Anthropol. 2007, 133, 1099–1111. [Google Scholar] [CrossRef]
- Guedes, L.; Dias, O.; Neto, J.; Ribeiro Da Silva, L.D.P.; Mendonça De Souza, S.M.F.; Iñiguez, A.M. First Paleogenetic Evidence of Probable Syphilis and Treponematoses Cases in the Brazilian Colonial Period. Biomed Res Int. 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, S.; Henneberg, R.J.; Henneberg, M. Presence of dental signs of congenital syphilis in pre-modern specimens. Vol. 85, Archives of Oral Biology. Elsevier Ltd; 2018. p. 192–200.
- Barnes, I.; Thomas, M.G. Evaluating bacterial pathogen DNA preservation in museum osteological collections. Proceedings of the Royal Society B: Biological Sciences. 2006, 273, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Von Hunnius, T.E.; Roberts, C.A.; Boylston, A.; Saunders, S.R. Histological identification of syphilis in pre-Columbian England. Am J Phys Anthropol. 2006, 129, 559–566. [Google Scholar] [CrossRef]
- Rothschild, B.; Jellema, L. Periosteal reaction recognition and specificity assessed by surface microscopy. Int J Osteoarchaeol. 2020, 30, 355–361. [Google Scholar] [CrossRef]
- Mansilia, J.; Pijoan, C.M. Brief Communication: A Case of Congenital Syphilis During the Colonial Period in Mexico City. American Journal Of Physical Anthropology. 1995, 97. [Google Scholar]
- Andreu-Arasa, V.C.; Chapman, M.N.; Kuno, H.; Fujita, A.; Sakai, O. Craniofacial manifestations of systemic disorders: CT and MR imaging findings and imaging approach. Radiographics. 2018, 38, 890–911. [Google Scholar] [CrossRef]
- Biehler-Gomez, L.; Mattia, M.; Sala, C.; Giordano, G.; Di Candia, D.; Messina, C.; et al. Mercury poisoning in two patients with tertiary syphilis from the Ca’ Granda hospital (17th-century Milan). Archaeometry. 2022, 64, 500–510. [Google Scholar] [CrossRef]
- Sarhan, M.S.; Wurst, C.; Tzankov, A.; Bircher, A.J.; Wittig, H.; Briellmann, T.; et al. A nontuberculous mycobacterium could solve the mystery of the lady from the Franciscan church in Basel, Switzerland. BMC Biol. 2023, 21. [Google Scholar] [CrossRef] [PubMed]
- Mirzaali, M.J.; Schwiedrzik, J.J.; Thaiwichai, S.; Best, J.P.; Michler, J.; Zysset, P.K.; et al. Mechanical properties of cortical bone and their relationships with age, gender, composition and microindentation properties in the elderly. Bone. 2016, 93, 196–211. [Google Scholar] [CrossRef] [PubMed]
- Cole, G.; Waldron, T.; Shelmerdine, S.; Hutchinson, C.; McHugh, K.; Calder, A.; et al. The skeletal effects of congenital syphilis: The case of Parrot’s bones. Med Hist. 2020, 64, 467–477. [Google Scholar] [CrossRef]
- Montiel, R.; Solórzano, E.; Díaz, N.; Álvarez-Sandoval, B.A.; González-Ruiz, M.; Cañadas, M.P.; et al. Neonate human remains: A window of opportunity to the molecular study of ancient syphilis. PLoS One. 2012, 7. [Google Scholar] [CrossRef] [PubMed]
- von Hunnius, T.E.; Yang, D.; Eng, B.; Waye, J.S.; Saunders, S.R. Digging deeper into the limits of ancient DNA research on syphilis. J Archaeol Sci. 2007, 34, 2091–2100. [Google Scholar] [CrossRef]
- Meffray, A.; Perrin, M.; Richier, A.; Schmitt, A.; Ardagna, Y.; Biagini, P. Molecular detection of Treponema Pallidum subspecies Pallidum in 150-year-old foetal remains, southeastern France. J Med Microbiol. 2019, 68, 761–769. [Google Scholar] [CrossRef]
- Giffin, K.; Lankapalli, A.K.; Sabin, S.; Spyrou, M.A.; Posth, C.; Kozakaitė, J.; et al. A treponemal genome from an historic plague victim supports a recent emergence of yaws and its presence in 15th century Europe. Sci Rep. 2020, 10. [Google Scholar] [CrossRef]
- Kolman, C.J.; Centurion-Lara, A.; Lukehart, S.A.; Owsley, D.W.; Tuross, N. Identification of Treponema pallidum Subspecies pallidum in a 200-Year-Old Skeletal Specimen [Internet]. 1999. Available from: http://jid.oxfordjournals.org/.
- Pääbo, S.; Poinar, H.; Serre, D.; Jaenicke-Després, V.; Hebler, J.; Rohland, N.; et al. Genetic analyses from ancient DNA. Annual Review of Genetics. 2004, 38, 645–679. [Google Scholar] [CrossRef]
- Höss, M.; Jaruga, P.; Zastawny, T.H.; Dizdaroglu, M.; Pääbo, S. DNA damage and DNA sequence retrieval from ancient tissues. Vol. 24, Nucleic Acids Research. Oxford University Press; 1996.
- Kulik-Kupka, K.; Koszowska, A.; Brończyk-Puzoń, A.; Nowak, J.; Gwizdek, K.; Zubelewicz-Szkodzińska, B. Arsen – trucizna czy lek? Vol. 67, Medycyna Pracy. Nofer Institute of Occupational Medicine; 2016. p. 89–96.
- Kłys, M. Z rtęcią (i...) przez stulecia. 2010. [Google Scholar]
- Kepa, M.; Kozłowski, T.; Szostek, K.; Drozd, A.; Walas, S.; Mrowiec, H.; et al. Analysis of mercury levels in historical bone material from syphilitic subjects - Pilot studies (short report). Anthropologischer Anzeiger. 2012, 69, 367–377. [Google Scholar] [CrossRef]
- Erdal, Y.S. A pre-Columbian case of congenital syphilis from anatolia (Nicaea, 13th century AD). Int J Osteoarchaeol. 2006, 16, 16–33. [Google Scholar] [CrossRef]
- Ioannou, S.; Henneberg, M. A Rare Case of Congenital Syphilis and a Supernumerary Fourth Molar in an Early 20th Century African American Woman. Vol. 29. 2016. [CrossRef]
- Henkel, J.S.; Davis, J.; Farley, N. Anatomical and biochemical evidence for Treponema pallidum in a 19th to early twentieth century skeletal cadaver. Forensic Sci Med Pathol. 2020, 16, 557–561. [Google Scholar] [CrossRef]
- Mendonça De Souza/ + S, Codinha, S.; Cunha, E. The girl from the Church of the Sacrament: a case of congenital syphilis in XVIII century Lisbon. Mem Inst Oswaldo Cruz, Rio de Janeiro. 2006, 101.
- Patel, R.; Mitchell, P.D. The Search for Rosa Pike: Congenital Syphilis in 1880s London. Archaeopress; 2007.
- Gaul, J.S.; Grossschmidt, K.; Gusenbauer, C.; Kanz, F. A probable case of congenital syphilis from pre-Columbian Austria. Anthropologischer Anzeiger. 2015, 72, 451–472. [Google Scholar] [CrossRef]
- Gaul, J.S.; Grossschmidt, K. A probable case of congenital syphilis from 18th century Vienna. Int J Paleopathol. 2014, 6, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Fornaciari, A.; Gaeta, R.; Minozzi, S.; Giuffra, V. Syphilis in Maria Salviati (1499–1543), Wife of Giovanni de’ Medici of the Black Bands. Emerg Infect Dis. 2020, 26, 1274–1282. [Google Scholar] [CrossRef]
- Lopez, B.; Lopez-Garcia, J.M.; Costilla, S.; Garcia-Vazquez, E.; Dopico, E.; Pardiñas, A.F. Treponemal disease in the old world? Integrated palaeopathological assessment of a 9th-11th century skeleton from north-central Spain. Anthropological Science. 2017, 125, 101–114. [Google Scholar] [CrossRef]
- Gino Fornaciari. Renaissance mummies in Italy. 1999.
- Mario Šlaus, Mn. A Case of Venereal Syphilis in the Modern Age Horizon of Graves near the Church of St. Lawrence in Crkvar. 2007.
- Rissech, C.; Roberts, C.; Tomás-Batlle, X.; Tomás-Gimeno, X.; Fuller, B.; Fernandez, P.L.; et al. A Roman Skeleton with Possible Treponematosis in the North-East of the Iberian Peninsula: A Morphological and Radiological Study. Int J Osteoarchaeol. 2013, 23, 651–663. [Google Scholar] [CrossRef]
- Cole, G.; Waldron, T. Apple Down 152: A putative case of syphilis from sixth century AD Anglo-Saxon England. Am J Phys Anthropol. 2011, 144, 72–79. [Google Scholar] [CrossRef]
- Carlos Pineda JCSFMML. Radiographs of an Ancient Mortuary Bundle Support Theory for the NewWorld Origin of Syphilis. 1998.
- Célia Lopes MLPALS. Syphilis and cirrhosis: a lethal combination in a XIX century individual identified from the Medical Schools Collection at the University of Coimbra (Portugal). 2010.
- Woo, E.J.; Kim, J.H.; Lee, W.J.; Cho, H.; Pak, S. Syphilitic infection in a pre-modern population from South Korea (19th century AD). Anthropological Science. 2019, 127, 55–63. [Google Scholar] [CrossRef]
- Castro, M.M.; Benavente, M.A.; Ortega, J.; Acuña, R.; Montero, C.; Thomas, C.; et al. Thoracic aortic aneurysm in a pre-Columbian (210 BC) inhabitant of Northern Chile: Implications for the origins of syphilis. Int J Paleopathol. 2016, 13, 20–26. [Google Scholar] [CrossRef]
- Klaus, H.D.; Ortner, D.J. Treponemal infection in Peru’s Early Colonial period: A case of complex lesion patterning and unusual funerary treatment. Int J Paleopathol. 2014, 4, 25–36. [Google Scholar] [CrossRef]
- Salesse, K.; Kaupová, S.; Brůžek, J.; Kuželka, V.; Velemínský, P. An isotopic case study of individuals with syphilis from the pathological-anatomical reference collection of the national museum in Prague (Czech Republic, 19th century A.D.). Int J Paleopathol. 2019, 25, 46–55. [Google Scholar] [CrossRef]
- Szczepanek, A.; Walocha, J.; Kochan, P. Cases of late syphilis documented at the cemetery of noblemen residents of the Knights of the Holy Sepulchre poorhouse (XVII-XVIII centuries) on Stradom in Cracow, Poland. World J Med Images. 2019, 5. [Google Scholar]
- Assis, S.; Casimiro, S.; Cardoso, F.A. A possible case of acquired syphilis at the former Royal Hospital of All-Saints (RHAS) in Lisbon, Portugal (18th century): A comparative methodological approach to differential diagnosis. Anthropologischer Anzeiger. 2015, 72, 427–449. [Google Scholar] [CrossRef] [PubMed]
- Radu, C.; Andreica, L.; Constantinescu, M.; Soficaru, A. Multiple Cases with Probable Treponemal Infection from 16th to 19th Centuries Romania. Int J Osteoarchaeol. 2015, 26, 563–573. [Google Scholar] [CrossRef]
- Zuckerman, M.K. The “Poxed” and the “Pure”: A Bioarchaeological Investigation of Community and Marginalization Relative to Infection with Acquired Syphilis in Post-Medieval London. Archeological Papers of the American Anthropological Association. 2017, 28, 91–103. [Google Scholar] [CrossRef]
- Gladykowska - Rzeczycka, J. J. , Kwiatkowska, B., Nowakowski, D., Trnka, J. Treponematosis in a 14 th century skeleton from Wroclaw, Poland. Journal of Paleopathology 2003, 15, 187–193. [Google Scholar]
- Suzuki, T.; Matsushita, T.; Han, K. On the possible case of treponematosis from the Bronze Age in China. Anthropological Science. 2005, 113, 253–258. [Google Scholar] [CrossRef]
Figure 1.
The procedure of includindg and excluding articles in review.
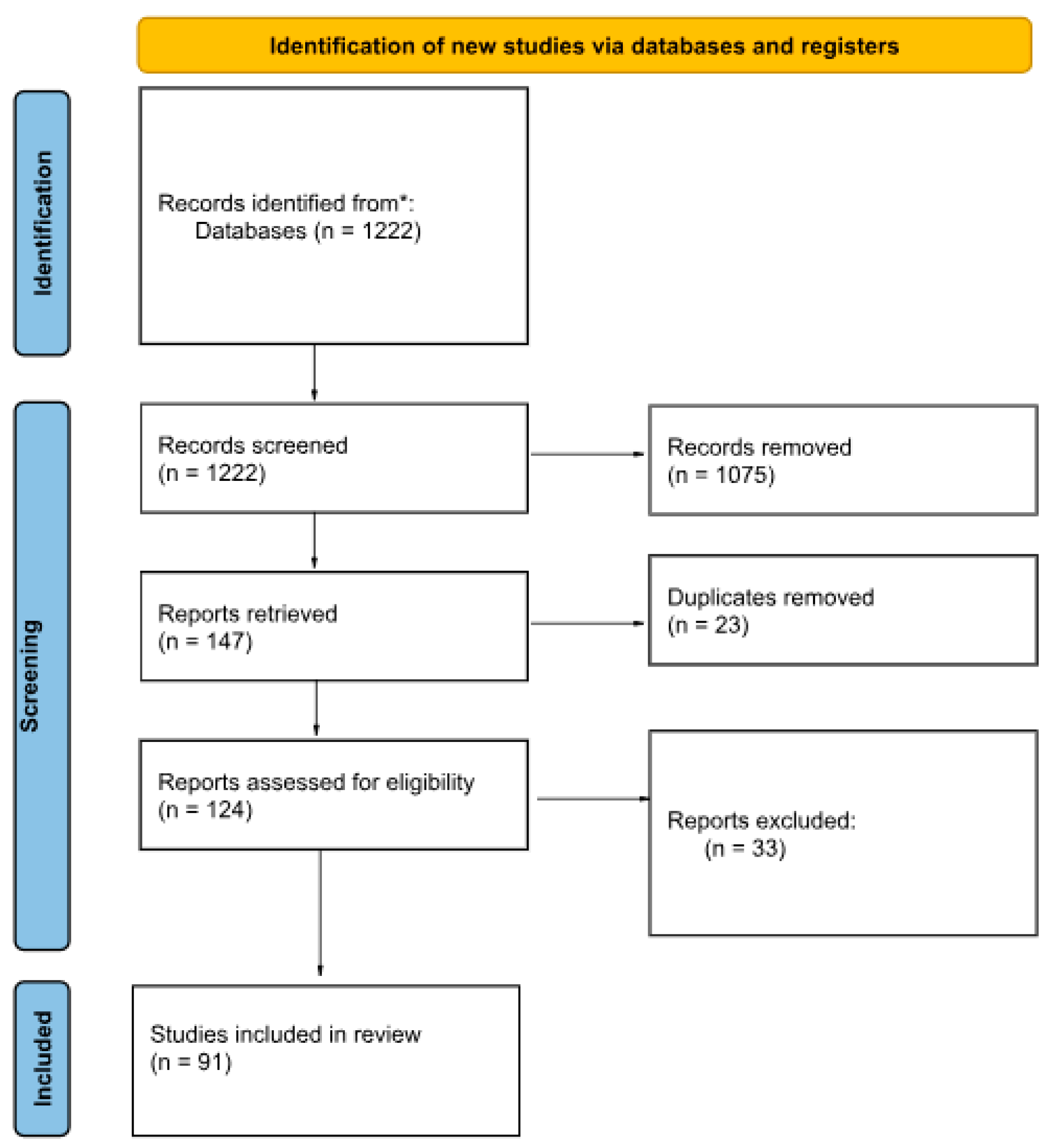
Figure 2.
(a) 1. Irregular surface of bone due to remodelling of lesions. 2,4,5. Porosity of syphilitic bone. 3. Formation of lamellar bone in medullar cavity. 6,7. Pathological sclerosis of bone on its’ borders. (b) Caries sicca of the frontal bone. (c) Dome-shaped molar with a narrow occlusal surface and crowded cusps clustered at the center (d) Molar with penetrating sinuses and atrophied cusps. (e) Hutchinson’s incisor.
Figure 2.
(a) 1. Irregular surface of bone due to remodelling of lesions. 2,4,5. Porosity of syphilitic bone. 3. Formation of lamellar bone in medullar cavity. 6,7. Pathological sclerosis of bone on its’ borders. (b) Caries sicca of the frontal bone. (c) Dome-shaped molar with a narrow occlusal surface and crowded cusps clustered at the center (d) Molar with penetrating sinuses and atrophied cusps. (e) Hutchinson’s incisor.
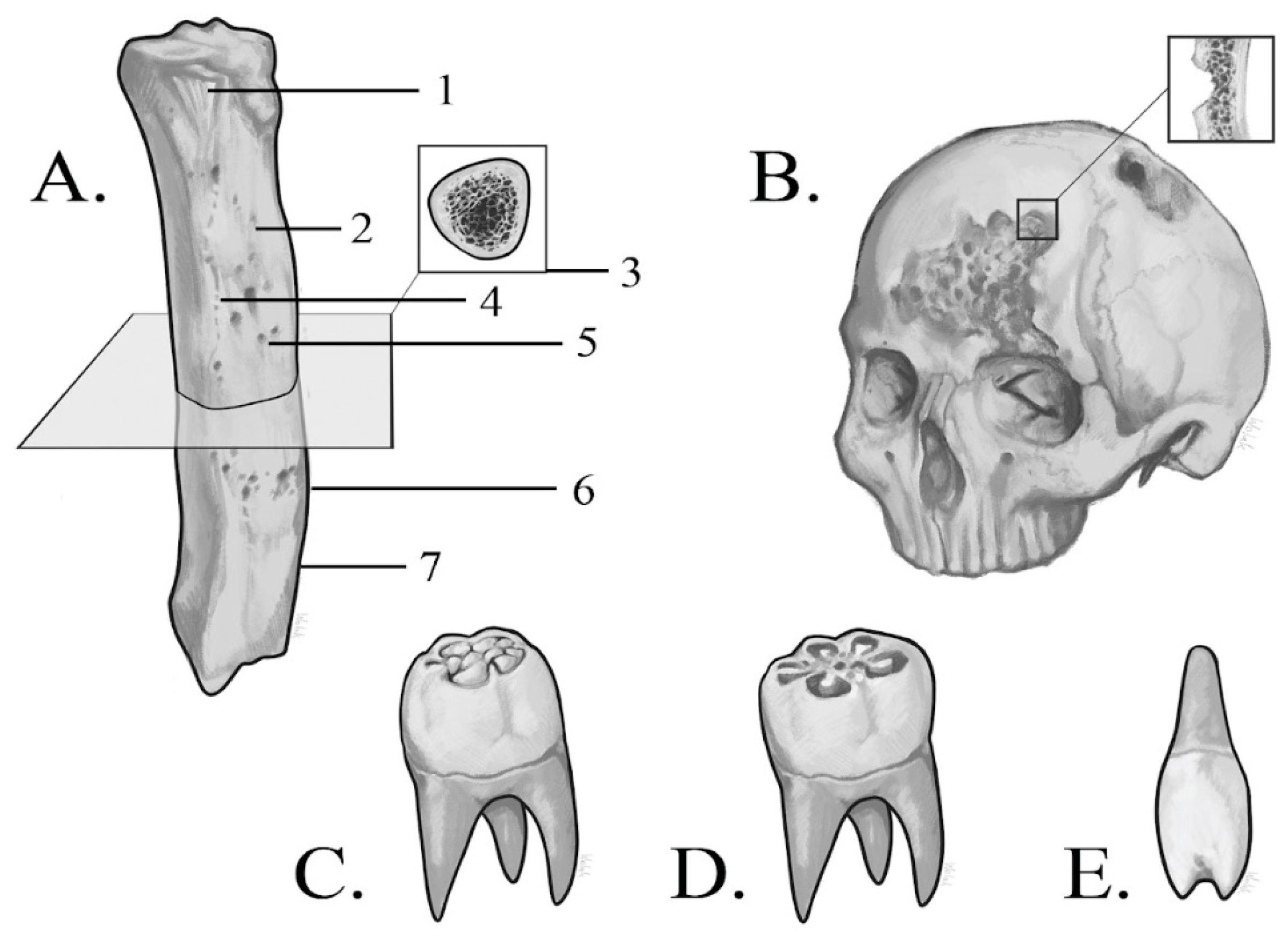
Figure 3.
Syphilitic shin deformity in immature (a) and mature bone (b).

Figure 4.
Differences in localization of skeletal lesions in various treponematoses. Number of altered bones marked.
Figure 4.
Differences in localization of skeletal lesions in various treponematoses. Number of altered bones marked.
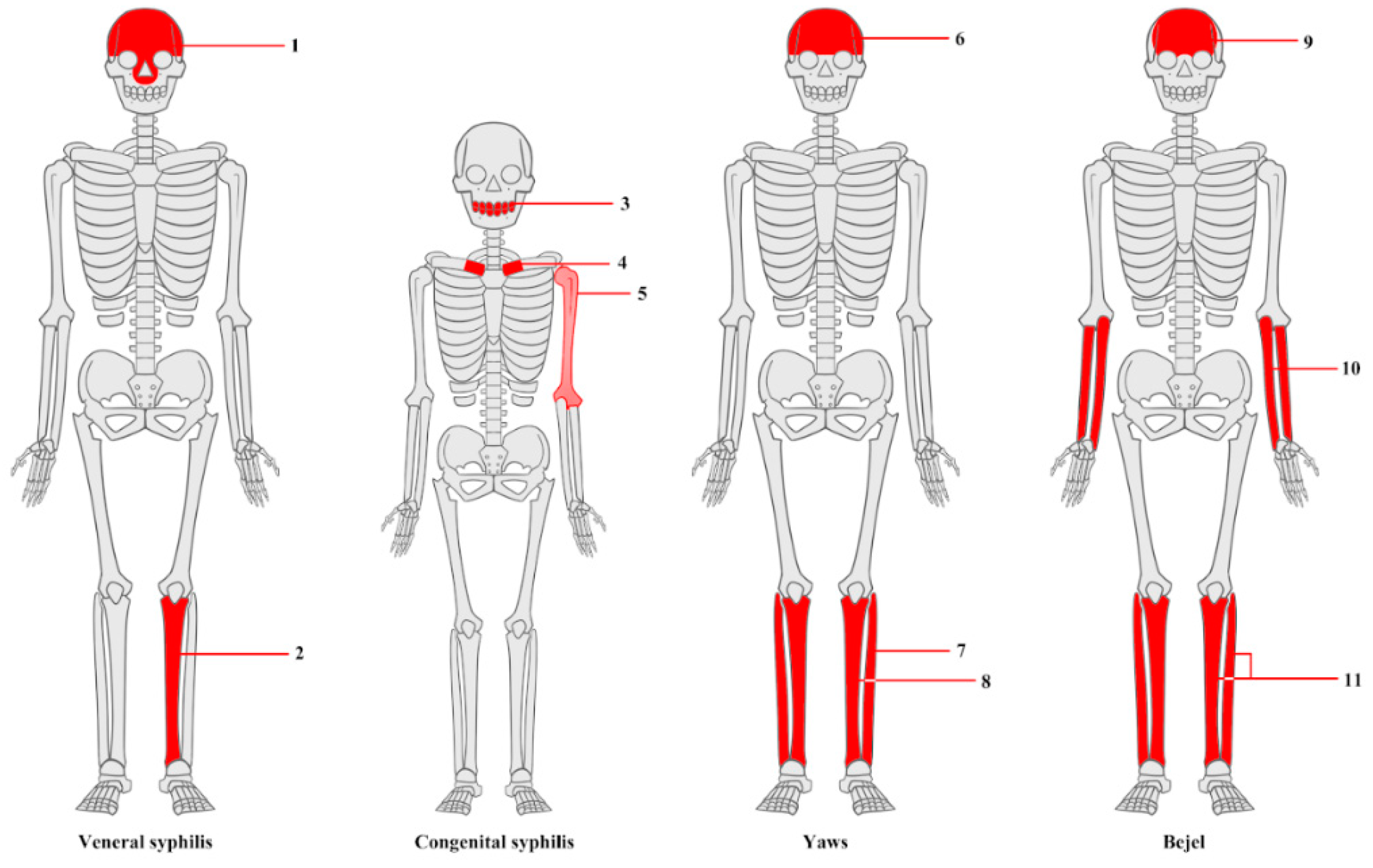
Figure 5.
Diagram presenting number of studies where various numbers of diagnostic methods were used.
Figure 5.
Diagram presenting number of studies where various numbers of diagnostic methods were used.
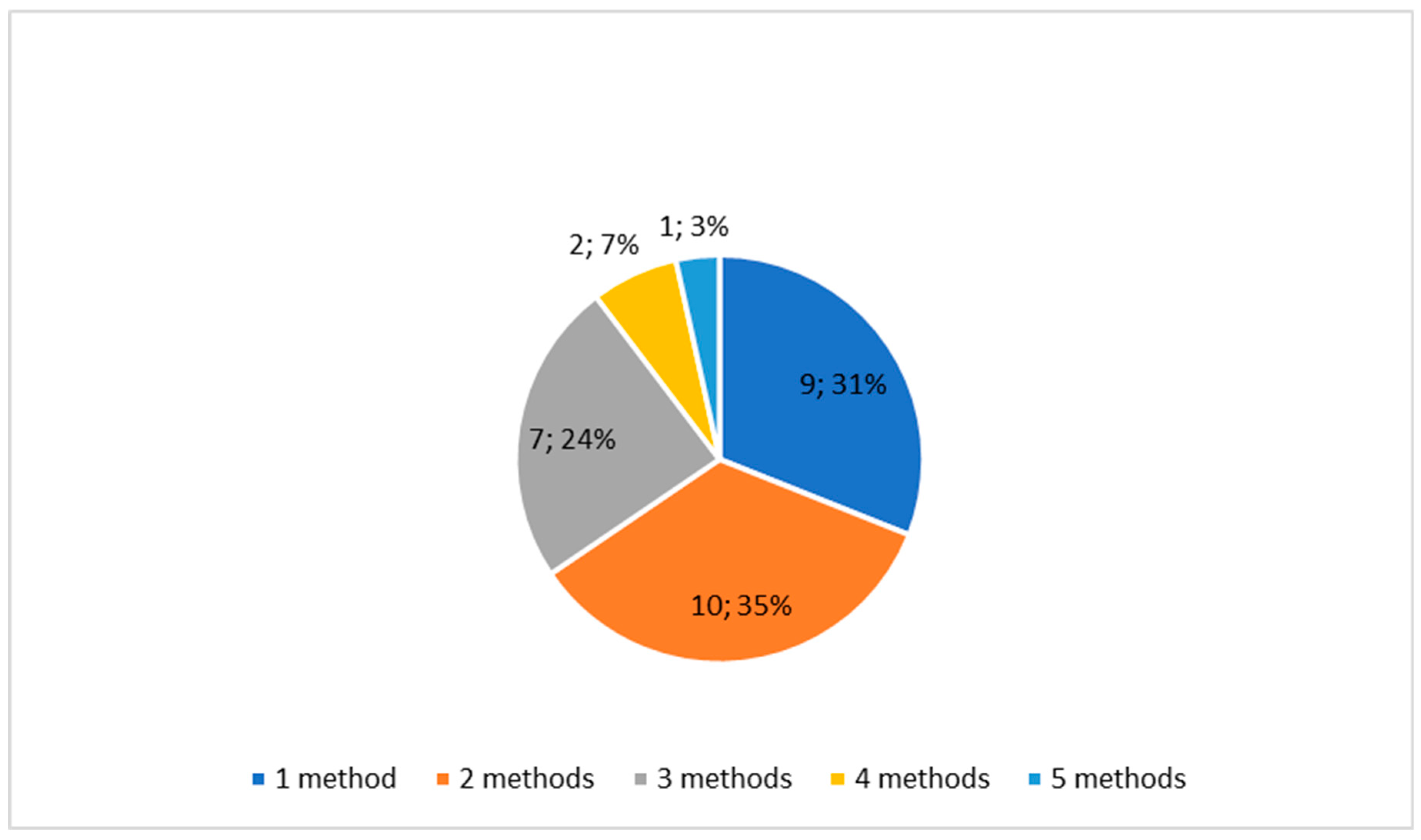
Figure 6.
The number of uses of each diagnostic method.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



