
Submitted:
19 March 2025
Posted:
19 March 2025
You are already at the latest version
Abstract
Tuberculosis poses serious challenges to healthcare personnel as it continues to be highly prevalent in a developing country like India. Several prominent strategies have been adopted to control this contagious infection, but the incidence rate remains high. Many studies have linked fungal infections and tuberculosis, apparently elevating concerns in the TB elimination program. Hence, it is essential to understand the mechanism underlying TB co-infection and pulmonary mycoses to combat the problems caused by these diseases successfully. In addition, differential diagnosis of TB and fungal infections is equally essential to initiate appropriate treatment. In this review, we have documented the findings of TB and fungal diseases individually and as coinfection, focusing on Indian perspectives. Misdiagnosis of fungal diseases as Tuberculosis in many studies elucidates the need for simultaneous diagnosis of both infections for appropriate diagnosis.
Keywords:
Tuberculosis
; fungal
; diagnosis
; therapy
; pathogenesis
; prophylaxis
; mycoses
; infections
1. Introduction
Though preventable and curable, tuberculosis caused by Mycobacterium tuberculosis remains the second leading cause of mortality due to a single infectious agent next to the COVID-19 infection in 2022, WHO Global Tuberculosis Report stated [1] Pulmonary tuberculosis continues to be a serious concern in India and is consecutively enlisted in the top 20 TB high burden countries despite strong measures taken by our health department [2]. Pathogenic fungi cause pulmonary mycoses via inhalation of spores, which disrupt the normal functioning of bronchial and lung tissues, resulting in pulmonary fungal disease. Further, a rapid surge in fungal infection recently is attributed to other pre-existing clinical conditions such as tuberculosis, HIV/AIDS, and substantial use of immunosuppressive drugs which enables these opportunistic fungi to attack the host, who are immunocompromised by the disease listed above [3,4] Commonly, pulmonary fungal infections are caused by Aspergillus, Cryptococcus, Pneumocystis [5], Candida [6], Mucor [7], and endemic fungi which include Blastomyces, Coccidioides and Histoplasma [8].
It’s been reported that people recovering from tuberculosis are prone to pulmonary fungal coinfections and were mostly misdiagnosed as cases of relapsed PTB [9]. However, some clinicians do not pay enough attention to this problem. Another alarming fact is that there is an increase in misdiagnosis of patients with invasive fungal infections, such as tuberculosis, and vice versa, due to similar clinical presentations leading to wrong or delayed treatment of the patients.[10], Therefore, studies on co-infection with PTB and pulmonary fungal infection are needed so that these patients may get treated for antituberculosis or antifungal agents promptly. To attain this, a differential diagnostic algorithm for TB and other fungal infections is required. While tuberculosis diagnostic methods are well designed and implemented in routine programmatic setups, many labs still rely on classical diagnostic tests for fungal infections, such as direct visualization, radiological evidence, and culture, which have very low sensitivity and specificity. In this review, we attempted to compile the Indian studies focusing on fungal infections with special reference to TB coinfection, misdiagnosis, and treatment.
2. Pulmonary Fungal Infections
- A. Pulmonary Aspergillosis
Pulmonary Aspergillosis can be broadly classified into three types based on clinical presentation [11].
1. Allergic Bronchopulmonary Aspergillosis,
2. Chronic Pulmonary Aspergillosis,
3. Invasive Pulmonary Aspergillosis.
2.1. Allergic Bronchopulmonary Aspergillosis (ABPA)
The common aetiological agent of ABPA is reported to be A. fumigatus [12] and is followed by other species such as A. flavus, A. niger, and A. oryzae [13]. The characteristic features of ABPA in conventional CT are bronchiectasis and mucoid opacities in the shape of toothpaste or a finger in a glove [14].
2.2. Invasive Pulmonary Aspergillosis (IPA)
Inhalation of Aspergillus conidia results in IPA, and the subspecies of A. fumigati (A. fumigatus, A. lentulus, and A. udagawae) are involved in this common form of aspergillosis [15]. Other significant species involved in the disease are A. flavus, A. nidulans, A. terreus, and A. niger. Extensive use of corticosteroids in non-neutropenic patients eventually results in invasive aspergillosis. A few symptoms of IPA patients include prolonged fever, nonproductive cough, chest pain, and hemoptysis [16], which are similar to TB, leading to confused CT results [17].
2.3. Chronic Pulmonary Aspergillosis (CPA):
The fungal pathogen causing CPA in most patients is A. fumigatus [18]. Incidentally, it is observed that one in five TB-negative patients after treatment with ATT might suffer from CPA [19]. A study in 2022 reported that the incidence of CPA emerging in PTB patients was estimated to be 363,601 cases and 42,766 deaths - 10.5% of total PTB deaths [20]. In addition, various studies and case reports elucidate the significance of CPA in PTB patients (Table 1). These findings indicate the importance of diagnosing CPA as part of the TB diagnostic algorithm in the program. Other predisposing factors for developing CPA into a serious illness are nontuberculous mycobacterial infections (NTM) and ABPA [21]. CPA is further subdivided into five types based on their colonization and disease development as follows
- Aspergillus nodules,
- Simple Aspergilloma,
- Chronic Cavitary Pulmonary Aspergillosis
- Subacute Invasive Pulmonary Aspergillosis,
- Chronic Fibrosing Pulmonary Aspergillosis
2.4. Aspergillus Nodules
Of the subtypes of CPA, Aspergillus nodules are relatively rare and are characterized by the CT finding of one or more nodules with or without cavities [30]. Minor or no symptoms represent this type of CPA and can only be diagnosed with histological evidence of necrosis severed by the presence of Aspergillus [31].
2.5. Aspergilloma
Simple Aspergilloma is indicated by a single fungal ball with radiological or microbiological evidence of Aspergillus species in immunocompetent individuals. Similar to Aspergillus nodules, this condition also accounts for minor or no symptoms [32].
2.6. Chronic Cavitary Pulmonary Aspergillosis (CCPA)
Complex Aspergilloma, an old surgical term now called CCPA [33], showcases parenchymal disease surrounded by a thick-walled cavity [34]. Contrary to Aspergillus nodules and Aspergilloma, the incidence of CCPA is high, and several reports have been documented for its role in previously treated TB patients. CT image portrays single or multiple cavities with characteristic residues in the lung [35].
2.7. Subacute Invasive Pulmonary Aspergillosis (SAIA)
Occasionally called semi-IPA and chronic necrotizing pulmonary aspergillosis [36], SAIA is similar to CCPA in radiology, with only the distinction of rapid progress in the former condition. Clinical conditions that make the host vulnerable to SAIA are diabetes, malnutrition, corticosteroid use, connective tissue disorders, HIV infection, and COPD [37].
2.8. Chronic Fibrosing Pulmonary Aspergillosis (CFPA)
2.9. Pulmonary Cryptococcosis
Though 30 species of Cryptococcus are identified, C. neoformans and C. gattii are known to cause human infections [39]. Invasive fungal diseases in immunocompromised individuals are known to be caused by C. deneoformans [40], while C. gattii depose infection in immunocompetent individuals [41]. CT findings of pulmonary cryptococcosis (PC) include pulmonary nodules, patchy shadows, ground glass attenuation, interstitial changes, and cavitation. In addition, the left lower lung seems to be involved most frequently in immunocompromised patients and is prone to be misdiagnosed as tuberculosis or tumor [42]. Although not common, studies from various parts of India have been reporting the coinfection of tuberculosis with cryptococcosis, emphasizing routine monitoring (Table 2).
2.10. Pneumocystis Pneumonia
Pneumocystis pneumonia (PCP) is caused by an opportunistic pathogen named Pneumocystis jirovecii [50]. It is an ascomycete fungus that was previously categorized as a protozoan due to its similarity in morphology and drug susceptibility [51] but later as fungi based on RNA analysis [52]. The clinical manifestations of PCP are illustrated by the subacute onset of dyspnoea, nonproductive cough, and low-grade fever [53]. Few studies and case reports have been recorded on Pneumocystis Pneumonia and TB across India (Table 3). This could be due to its coexistence in the HIV population, where one of the diseases gets diagnosed, and by the time the other one is suspected, the patient dies. [54].
2.11. Pulmonary Blastomycosis
The inhalation of Blastomyces spore results in this fungal infection. The fungal agents involved in Blastomycosis include Blastomyces dermatitidis, B. percursus, and B. emzantsi [59]. Surprisingly, though the lung is the most common site of infection [60], the first human case of this infection was averred in the skin tissue [61]. This extrapulmonary spread could be attributed to a hematogenous initial lung infection [62]. The pulmonary form of the disease is expressed as pneumonia with an insidious course, while chest CT is non-specific, and infection limited to the lungs can mimic M. tuberculosis [63] [64]. One study of Blastomycosis misdiagnosed as TB was reported in the last decade from Kerala, India, in 2019. The patient was on empirical ATT for nearly a year due to an indefinite diagnosis. History of his travel to Chicago, which is endemic for Blastomycosis, stirred suspicion, and he was appropriately diagnosed [65].
2.12. Pulmonary Coccidioidomycosis
Soil inhabiting the arthroconidia of the fungi Coccidioides immitis and Coccidioides posadasii is responsible for pulmonary coccidioidomycosis [66]. The disease is reported rarely in places other than endemic areas [67] and is commonly associated with human and animal middens [68]. Though endemic to deserts in the United States and Central and South America, travel history to these countries has resulted in cases reported from other parts of the world [69]. It has been documented that about 19.5% of Coccidioidomycosis confirmed cases were infected with tuberculosis as well [70]. One case report has been documented so far from India where the diseased individual with a travel history presented with complaints of swelling over the neck and was clinically diagnosed as having tuberculosis. Further diagnosis by fungal stains, fungal culture, and serology confirmed Coccidioides, and a course of fluconazole was used for treatment [71].
2.13. Pulmonary Histoplasmosis
Histoplasma capsulatum, a dimorphic fungus, is accountable for establishing histoplasmosis infection [72]. Disease transmission is reported to be due to inhalation of spores in instances of soil disruption like cave excavation [73]. Chronic histoplasmosis is often characterized by nodule formation, and this clinical condition is termed chronic cavitary pulmonary histoplasmosis (CCPH) [74]. Major clinical features of TB, like radiological findings, pulmonary infiltrates, hilar lymphadenopathy, opacities of the lung, and pleural effusion, are also reported in histoplasmosis [75] [76]. Instances of Histoplasmosis misdiagnosed as TB across India have been recorded in Table 4.
2.14. Pulmonary Candidiasis
Opportunistic candidal infection is caused frequently by Candida albicans, although the incidence of disease by other members of the same genus is also increasing rapidly [81]. Candida, a commensal of the gut microbiome, shapes itself into a pathogen based on antibiotics, severe lapse leading to compromise of the gut integrity, host immune dysfunction, use of central venous catheter, surgery etc. [82]. Diagnosing pulmonary candidiasis is tedious as no specific clinical and radiographic presentations exist. Hence, pulmonary parenchymal invasion through histopathologic examination can be a more reliable method for diagnosis in patients with deep-rooted invasion, though such instances occur rarely. [83]. A systematic review and meta-analysis of different cross-sectional studies by Fishani et al. has established a significantly higher incidence of co-infection of Candidiasis among pulmonary tuberculosis patients in Asia and Africa [84]. Significant correlations between HIV, TB, and Candidiasis that were documented from India are included in Table 5
2.15. Pulmonary Mucormycosis
The order Mucorales includes different genera such as Rhizopus, Mucor, Lichtheimia, Rhizomucor, Cunninghamella, and Apophysomyces spp involved in establishing the invasive fungal infection called mucormycosis [87]. Diabetes mellitus, solid organ transplant, chronic renal failure, hematological malignancy, acute myeloid leukemia, and tuberculosis are the predisposing risk factors for mucormycosis [88]. Clinical features include ground-glass lesions, reverse halo signs, necrosis, lobar and segmental consolidation, and single or multiple lesions [89]. Studies and case reports on mucormycosis documented across India have been described in Table 6.
3. Diagnosis
The Fungal Priority Pathogen List released by WHO in 2022 underscores the need for quick measures to prevent, diagnose, and appropriately treat fungal pathogens [94]. Some of the proven diagnostic tools available for detecting pulmonary mycoses can be broadly categorized into histopathological and culture methods, while radiological, immunological, and molecular techniques are considered for probable diagnosis [95]. Figure 1 shows diagnostic techniques for suspected pulmonary fungal infections in presumed TB patients who have been microbiologically determined to be non-TB patients, with confirmed possibility of bacterial and viral pneumonias ruled out.
3.1. Direct microscopy & Histopathological Examination
Histopathological examination can be carried out by staining methods using Haematoxylin Eosin stain (HE), periodic acid Schiff stain (PAS), or Gomori’s methenamine silver stain (GMS) [96]. An evaluation study carried out to detect fungal infections in post-COVID-19 patients by Baxi et al. from Gujarat compared the efficacies of histopathological, culture, and KOH wet mount methods, of which the histopathological diagnosis by Haematoxylin and Eosin staining was found to be the most sensitive and rapid technique for mycological identification [97]. Another retrospective study from a tertiary care hospital in Jammu & Kashmir stressed the potential misdiagnosis in the microbiological examination as it cannot differentiate between pathogenic fungi and contamination. Further, they suggested that histopathology could be more reliable for fungal diagnosis as it can distinguish between contamination, colonization, or actual infection [98]. Seth et al. from AIIMS New Delhi reviewed the diagnostic progress of fungal infections and concluded that diagnostic tools need to be validated in younger children. They also admitted that histopathological examination remains the gold standard while galactomannan assay or PCR techniques can be employed for pediatric populations [99].
3.2. Radiology
Radiological diagnosis includes the utility of X-rays, CT scans, radiofrequency (MRI), and sound waves (ultrasound) for pathogen identification [100]. High-Resolution Computed Tomography (HRCT), though insensitive, can be utilized as a screening tool initially in highly suspected cases, and an empirical therapy could be started when microbiological diagnosis takes up more time [101]. It has been documented that PJP by Pneumocystis in HIV/AIDS patients can be suspected with radiological evidence. Similarly, lung consolidation, nodules, and masses can be used to suspect cryptococcosis and blastomycosis [102]. Garg et al. from PGIMER, Chandigarh, studied the imaging spectrum of CPA and summarised that a patient's immune status plays a significant role in radiological diagnosis as clinical presentation is often not specific and leads to misdiagnosis [37].
3.3. Culture
Sabouraud’s Dextrose agar or Potato Dextrose agar with certain antibiotics or Brain Heart Infusion agar enriched with blood is generally used for growing fungal pathogens [103]. The culture of clinical specimens is considered more efficient in determining the specific fungal etiological agent if the sample is positive and susceptibility patterns can be determined. A retrospective study by Ghosh et al. from PGIMER stated that around 50% of direct microscopy-confirmed cases of fungal keratitis yielded positive results on culture, with Aspergillus being the predominant among isolated spectrum [104]. When culture is challenging to identify using tease mounts, the slide culture technique has to be used alternately, states the ICMR SOP for Fungal Identification and Detection of Antifungal Resistance, Edition 2 [105].
3.4. Immunology
Serum Galactomannan (GM) testing can be recommended for IPA suspects initially, and they can be subjected to tissue biopsy only when a GM negative result is obtained if there is still high clinical suspicion for IPA. Consequently, false positive serum GM can be avoided with a BAL GM confirmation [106]. Another biomarker, B, D glucan, can identify different fungi in clinical specimens. However, in the case of ABPA, Aspergillus-specific IgG has proven higher sensitivity and specificity than IgE [107] GM and B, D glucan [108]. Point of care identification of Aspergillus in corneal samples was demonstrated by Gunasekaran et al. in Tamil Nadu, using a Lateral flow device for microbial keratitis, and they have achieved prominent results for the same [109]. Other serological assays with significant diagnostic ability for fungal detection include immunodiffusion (ID), counter-immunoelectrophoresis (CIE), enzyme-linked immunosorbent assays (ELISA), complement fixation (CF), radio-immunosorbent assays (RIA) and agglutination assays [110].
3.5. Molecular Diagnosis
Nucleic acid-based molecular diagnostics include PCR, loop-mediated isothermal amplification, nucleic acid sequence-based amplification (NABSA), and rolling circle amplification. Gudisa et al. from PGIMER, Chandigarh, reviewed the evolution of molecular diagnostics for fungal infection over the years and elucidated the significance of RT-PCR, the role of Sanger sequencing, and next-generation sequencing in the detection and speciation of fungal pathogens [111]. A study from North India by Srinivas et al. from Maharashtra evaluated GenoSen’s panfungal RT PCR kit. It depicted the utility of panfungal PCR in a resource-limited country like India [112].
3.6. Metagenomic Next Generation Sequencing (mNGS)
Molecular methods such as mNGS will greatly help diagnosis but require strong validation and standardization for better utility [113]. Moreover, metagenomic next-generation sequencing is a fast-growing diagnostic technique with the subsequent advantage of rapid and broad detection [114]. Different studies have demonstrated the efficiency of the NGS technique in detecting fungal pathogens such as Pneumocystis, Histoplasma, Aspergillus, and Candida [115]
3.7. Matrix Assisted Laser Desorption Ionisation-Time of Flight Mass Spectrometry (MALDI TOF MS)
Ghosh et al. tried to evaluate the utility of MALDI-TOF MS in diagnosing bloodstream yeasts. They also added the need for extensive studies to be carried out to validate the potential of MALDI-TOF as a diagnostic technique for effective patient care and management [116]. Paul et al. standardized the MALDI-TOF method with different protocols and concluded it could be used for routine diagnosis of pathogenic molds [117].
3.8. Antifungal Therapy
Traditional antifungals available for treating pulmonary mycoses were previously limited, but the therapeutic potential has increased substantially with new azole compounds. Further, initiating newer treatment options has established wider options for clinicians to assist in treating fungal infections [118]. Some antifungals and newer biologic agents utilized in treating pulmonary fungal infections are listed in Table 7.
4. Conclusions
This review has summarised distinct studies conducted in India concerning the concrete connection between tuberculosis and pulmonary mycoses. It is worth noting that the incidence of misdiagnosis documented in this review explains the poor clinical suspicion for pulmonary mycosis among TB cases. Hence, we suggest clinical suspicion of pulmonary mycoses among TB cases and ATT non-responders could help in timely prognosis and patient care. Further, it emphasizes the urgent necessity to develop differential diagnostics for TB and pulmonary mycoses, as most of the available tools have been exposed to either cross-reactivity or low specificity.
Conflicts of Interest
All authors declare no conflicts of interest.
References
- “Global Tuberculosis Report 2023.” [Online]. Available: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2023. [Accessed: 28-Aug-2024].
- J. Singh, A. Dinkar, and P. Gupta, “Uncommon manifestations in tuberculosis: An expanding clinical spectrum from North India.,” Int. J. Mycobacteriol., vol. 11, no. 1, pp. 30–37, 2022. [CrossRef]
- A. Bitew and S. Bati, “Profiling of potential pulmonary fungal pathogens and the prevalence of the association between pulmonary tuberculosis and potential fungal pathogens in presumptive tuberculosis patients referred to Saint Peter’s Specialized Tuberculosis Referral Hospital, Addis Ababa, Ethiopia.,” SAGE Open Med., vol. 9, p. 20503121211056164, Nov. 2021. [CrossRef]
- S. Muni et al., “Identification of fungal isolates in patients with pulmonary tuberculosis treated at a tertiary care hospital.,” Cureus, vol. 15, no. 4, p. e37664, Apr. 2023. [CrossRef]
- Z. Li, G. Lu, and G. Meng, “Pathogenic fungal infection in the lung.,” Front. Immunol., vol. 10, p. 1524, Jul. 2019. [CrossRef]
- B. T. Kelly, K. M. Pennington, and A. H. Limper, “Advances in the diagnosis of fungal pneumonias.,” Expert Rev. Respir. Med., vol. 14, no. 7, pp. 703–714, Jul. 2020. [CrossRef]
- X. Yan et al., “Pulmonary Fungal Diseases in Immunocompetent Hosts: A Single-Center Retrospective Analysis of 35 Subjects.,” Mycopathologia, vol. 181, no. 7–8, pp. 513–521, Aug. 2016. [CrossRef]
- A. P. Campbell et al., “Endemic mycoses in children in North America: a review of radiologic findings.,” Pediatr. Radiol., vol. 53, no. 5, pp. 984–1004, May 2023. [CrossRef]
- W. Seo, H. W. Kim, J. S. Kim, and J. Min, “Long term management of people with post-tuberculosis lung disease.,” Korean J. Intern. Med., vol. 39, no. 1, pp. 7–24, Jan. 2024. [CrossRef]
- B. E. Ekeng, A. A. Davies, I. I. Osaigbovo, A. Warris, R. O. Oladele, and D. W. Denning, “Pulmonary and extrapulmonary manifestations of fungal infections misdiagnosed as tuberculosis: the need for prompt diagnosis and management.,” J Fungi (Basel), vol. 8, no. 5, Apr. 2022. [CrossRef]
- A. Kanj, N. Abdallah, and A. O. Soubani, “The spectrum of pulmonary aspergillosis.,” Respir. Med., vol. 141, pp. 121–131, Aug. 2018. [CrossRef]
- R. Agarwal et al., “Allergic bronchopulmonary aspergillosis.,” Indian J. Med. Res., vol. 151, no. 6, pp. 529–549, Jun. 2020. [CrossRef]
- S. Ueki, A. Hebisawa, M. Kitani, K. Asano, and J. S. Neves, “Allergic Bronchopulmonary Aspergillosis-A Luminal Hypereosinophilic Disease With Extracellular Trap Cell Death.,” Front. Immunol., vol. 9, p. 2346, Oct. 2018. [CrossRef]
- P. A. Grenier, A. L. Brun, E. Longchampt, M. Lipski, F. Mellot, and E. Catherinot, “Primary immunodeficiency diseases of adults: a review of pulmonary complication imaging findings.,” Eur. Radiol., vol. 34, no. 6, pp. 4142–4154, Jun. 2024. [CrossRef]
- S. Khan et al., “Distribution of Aspergillus species and risk factors for aspergillosis in mainland China: a systematic review.,” Ther. Adv. Infect. Dis., vol. 11, p. 20499361241252536, Jun. 2024. [CrossRef]
- J. Heylen, Y. Vanbiervliet, J. Maertens, B. Rijnders, and J. Wauters, “Acute invasive pulmonary aspergillosis: clinical presentation and treatment.,” Semin. Respir. Crit. Care Med., vol. 45, no. 1, pp. 69–87, Feb. 2024. [CrossRef]
- S.-H. Kim et al., “Invasive Pulmonary Aspergillosis-mimicking Tuberculosis.,” Clin. Infect. Dis., vol. 61, no. 1, pp. 9–17, Jul. 2015. [CrossRef]
- M. H. van der Torre, H. Shen, R. Rautemaa-Richardson, M. D. Richardson, and L. Novak-Frazer, “Molecular Epidemiology of Aspergillus fumigatus in Chronic Pulmonary Aspergillosis Patients.,” J Fungi (Basel), vol. 7, no. 2, Feb. 2021. [CrossRef]
- C. Kosmidis, “Special issue: chronic pulmonary aspergillosis.,” J Fungi (Basel), vol. 8, no. 7, Jul. 2022. [CrossRef]
- D. W. Denning, D. C. Cole, and A. Ray, “New estimation of the prevalence of chronic pulmonary aspergillosis (CPA) related to pulmonary TB - a revised burden for India.,” IJID Reg., vol. 6, pp. 7–14, Mar. 2023. [CrossRef]
- A. Zarif, A. Thomas, and A. Vayro, “Chronic pulmonary aspergillosis: A brief review.,” Yale J. Biol. Med., vol. 94, no. 4, pp. 673–679, Dec. 2021.
- D. Jha et al., “Chronic pulmonary aspergillosis incidence in newly detected pulmonary tuberculosis cases during follow-up.,” Mycoses, vol. 67, no. 5, p. e13747, May 2024. [CrossRef]
- N. K. Chirumamilla et al., “Innate and adaptive immune responses in subjects with CPA secondary to post-pulmonary tuberculosis lung abnormalities.,” Mycoses, vol. 67, no. 5, p. e13746, May 2024. [CrossRef]
- R. Rajpurohit, P. Wagh, M. Heda, G. Dubey, and P. S. Gujar, “Prevalence of chronic pulmonary aspergillosis in fibrocavitary pulmonary tuberculosis patients.,” J. Family Med. Prim. Care, vol. 12, no. 1, pp. 106–110, Jan. 2023. [CrossRef]
- B. G. Bharath et al., “Diagnostic utility of chest computerized tomography in the diagnosis of recurrence among sputum scarce and sputum negative previously treated pulmonary tuberculosis suspects.,” Lung India, vol. 39, no. 2, pp. 145–151, 2022. [CrossRef]
- I. S. Sehgal et al., “Role of C-Reactive Protein and Erythrocyte Sedimentation Rate in the Diagnosis and Monitoring of Treatment Response in Treatment Naïve Subjects with Chronic Pulmonary Aspergillosis.,” Mycopathologia, vol. 188, no. 5, pp. 705–711, Oct. 2023. [CrossRef]
- R. Lahiri, I. Jhalani, A. Kumar, and A. G. Goswami, “Successful management of delayed postoperative lung collapse secondary to spillage of aspergilloma.,” BMJ Case Rep., vol. 16, no. 7, Jul. 2023. [CrossRef]
- A. Gandotra et al., “Invasive Pulmonary Aspergillosis and Tuberculosis Complicated by Hemophagocytic Lymphohistiocytosis - Sequelae of COVID-19 in a Liver Transplant Recipient.,” J. Clin. Exp. Hepatol., vol. 12, no. 3, pp. 1007–1011, 2022. [CrossRef]
- S. Chaurasia, M. Thimmappa, and S. Chowdhury, “Case Report: Chronic Cavitatory Pulmonary Aspergillosis after COVID-19.,” Am. J. Trop. Med. Hyg., vol. 106, no. 1, pp. 105–107, Nov. 2021. [CrossRef]
- S. Dong, F. Wang, H. Jin, and X. Dai, “Five cases of pulmonary Aspergillus nodules diagnosed at surgery and by pathology in immunocompetent patients, with a literature review.,” Therapeutic Advances in Rare Disease, vol. 5, p. 26330040241252450, May 2024. [CrossRef]
- H. Zhong et al., “Clinical features, diagnostic test performance, and prognosis in different subtypes of chronic pulmonary aspergillosis.,” Front Med (Lausanne), vol. 9, p. 811807, Feb. 2022. [CrossRef]
- R. K. Chakraborty, T. S. Gilotra, E. H. Tobin, and K. M. Baradhi, “Aspergilloma,” in StatPearls, Treasure Island (FL): StatPearls Publishing, 2024.
- F. Lamoth and T. Calandra, “Pulmonary aspergillosis: diagnosis and treatment.,” Eur. Respir. Rev., vol. 31, no. 166, Dec. 2022. [CrossRef]
- A. Pekçolaklar, N. Çıtak, Y. Aksoy, V. Erdoğu, and M. Metin, “Is there any change in disease presentation and surgical outcomes in patients with pulmonary aspergilloma? An evaluation of the time trend.,” Turk Gogus Kalp Damar Cerrahisi Dergisi, vol. 30, no. 2, pp. 241–249, Apr. 2022. [CrossRef]
- A. Uzair, M. Waseem, N. I. Bhatti, Z. Toor, A. Ishaq, and O. Ahmad, “Chronic cavitary pulmonary aspergillosis as a sequela of pulmonary tuberculosis: A case report from Pakistan.,” SAGE Open Med. Case Rep., vol. 12, p. 2050313X241251777, May 2024. [CrossRef]
- I. Izumikawa et al., “Pathogenesis and clinical features of chronic pulmonary aspergillosis - is it possible to distinguish CNPA and CCPA clinically?,” J. Infect. Chemother., vol. 20, no. 3, pp. 208–212, Mar. 2014. [CrossRef]
- M. Garg et al., “Imaging spectrum in chronic pulmonary aspergillosis.,” Am. J. Trop. Med. Hyg., vol. 108, no. 1, pp. 15–21, Jan. 2023. [CrossRef]
- S.-F. Huang, C.-C. Huang, K.-T. Chou, Y.-J. Chan, Y.-Y. Yang, and F.-D. Wang, “Chronic Pulmonary Aspergillosis: Disease Severity Using Image Analysis and Correlation with Systemic Proinflammation and Predictors of Clinical Outcome.,” J Fungi (Basel), vol. 7, no. 10, Oct. 2021. [CrossRef]
- T. Wang, M. Liu, and F. Zhang, “Clinical diagnosis, treatment, and laboratory detection of 50 cases of pulmonary cryptococcosis.,” Comput. Math. Methods Med., vol. 2022, p. 7981472, Jul. 2022. [CrossRef]
- S. E. Kidd, A. Abdolrasouli, and F. Hagen, “Fungal nomenclature: managing change is the name of the game.,” Open Forum Infect. Dis., vol. 10, no. 1, p. ofac559, Jan. 2023. [CrossRef]
- I. J. Kwon-Chung et al., “Cryptococcus neoformans and Cryptococcus gattii, the etiologic agents of cryptococcosis.,” Cold Spring Harb. Perspect. Med., vol. 4, no. 7, p. a019760, Jul. 2014. [CrossRef]
- J. Qu, X. Zhang, Y. Lu, X. Liu, and X. Lv, “Clinical analysis in immunocompetent and immunocompromised patients with pulmonary cryptococcosis in western China.,” Sci. Rep., vol. 10, no. 1, p. 9387, Jun. 2020. [CrossRef]
- P. Meena et al., “Cryptococcosis masquerading as disseminated tuberculosis in a patient on chronic hemodialysis.,” Saudi J. Kidney Dis. Transpl., vol. 30, no. 5, pp. 1179–1183, Oct. 2019. [CrossRef]
- N. Adsul et al., “Thoracic cryptococcal osteomyelitis mimicking tuberculosis: A case report.,” Surg. Neurol. Int., vol. 10, p. 81, May 2019. [CrossRef]
- J. Ismail, M. Chidambaram, J. Sankar, S. Agarwal, and R. Lodha, “Disseminated cryptococcosis presenting as miliary lung shadows in an immunocompetent child.,” J. Trop. Pediatr., vol. 64, no. 5, pp. 434–437, Oct. 2018. [CrossRef]
- S. Jain, V. Mahajan, and A. Kumar, “Unusual case of coexistent pulmonary cryptococcosis and tuberculosis in an immuno-competent host.,” Indian J. Tuberc., vol. 64, no. 3, pp. 228–231, Jul. 2017. [CrossRef]
- S. Pawar et al., “Pulmonary cryptococcoma masquerading as lung cancer.,” J. Assoc. Physicians India, vol. 64, no. 5, pp. 66–68, May 2016.
- S. Sharma, P. Gupta, N. Gupta, A. Lal, D. Behera, and A. Rajwanshi, “Pulmonary infections in immunocompromised patients: the role of image-guided fine needle aspiration cytology.,” Cytopathology, vol. 28, no. 1, pp. 46–54, Feb. 2017. [CrossRef]
- P. Ranjan, M. Jana, S. Krishnan, D. Nath, and R. Sood, “Disseminated cryptococcosis with adrenal and lung involvement in an immunocompetent patient.,” J. Clin. Diagn. Res., vol. 9, no. 4, pp. OD04-5, Apr. 2015. [CrossRef]
- Z. Rafat et al., “The mycological and molecular study of Pneumocystis jiroveci pneumonia among HIV and non-HIV immunocompromised patients hospitalized in pulmonary units in Guilan, Northern Iran.,” Iran. J. Microbiol., vol. 13, no. 4, pp. 518–524, Aug. 2021. [CrossRef]
- H.-Y. Lee, C.-Y. Lu, P.-I. Lee, J.-M. Chen, L.-M. Huang, and L.-Y. Chang, “Pneumocystis jiroveci pneumonia in Taiwan from 2014 to 2017: Clinical manifestations and outcomes between pediatric and adult patients.,” J. Microbiol. Immunol. Infect., vol. 52, no. 6, pp. 983–990, Dec. 2019. [CrossRef]
- A. Apostolopoulou and J. A. Fishman, “The Pathogenesis and Diagnosis of Pneumocystis jiroveci Pneumonia.,” J Fungi (Basel), vol. 8, no. 11, Nov. 2022. [CrossRef]
- I. Bateman, R. Oladele, and J. K. Kolls, “Diagnosing Pneumocystis jirovecii pneumonia: A review of current methods and novel approaches.,” Med. Mycol., vol. 58, no. 8, pp. 1015–1028, Nov. 2020. [CrossRef]
- S. Pandey, S. Ghosh, P. Halder, D. Pal, D. C. Modak, and S. K. Guha, “Pulmonary tuberculosis and pneumocystis jirovecii concurrent pneumonia in HIV infected patients at a resource limited setting in Eastern India: A case series.,” Indian J. Tuberc., vol. 67, no. 3, pp. 378–382, Jul. 2020. [CrossRef]
- J. G, S. Narayanan, S. Kumar, M. Banjade, and M. Bairwa, “Spontaneous pneumothorax, pneumomediastinum, and pneumopericardium in an HIV patient with tuberculosis: A rare trio.,” Cureus, vol. 16, no. 4, p. e58440, Apr. 2024. [CrossRef]
- V. C. Patil and H. V. Patil, “Clinical manifestations and outcome of patients with human immunodeficiency virus infection at tertiary care teaching hospital.,” Indian J. Sex. Transm. Dis., vol. 37, no. 1, pp. 38–45, Jun. 2016. [CrossRef]
- P. Indira, P. M. Kumar, S. Shalini, and K. Vaman, “Opportunistic Infections among People Living with HIV (PLHIV) with Diabetes Mellitus (DM) Attending a Tertiary Care Hospital in Coastal City of South India.,” PLoS ONE, vol. 10, no. 8, p. e0136280, Aug. 2015. [CrossRef]
- K. Ramesh, S. Gandhi, and V. Rao, “Clinical profile of human immunodeficiency virus patients with opportunistic infections: A descriptive case series study.,” Int. J. Appl. Basic Med. Res., vol. 5, no. 2, pp. 119–123, Aug. 2015. [CrossRef]
- F. Bongomin et al., “Invasive fungal diseases in africa: A critical literature review.,” J Fungi (Basel), vol. 8, no. 12, Nov. 2022. [CrossRef]
- A. Goico, J. Henao, and K. Tejada, “Disseminated blastomycosis in a 36-year-old immunocompetent male from Chicago, IL.,” Oxf. Med. Case Reports, vol. 2018, no. 10, p. omy071, Oct. 2018. [CrossRef]
- T. G. Maphanga et al., “Human Blastomycosis in South Africa Caused by Blastomyces percursus and Blastomyces emzantsi sp. nov., 1967 to 2014.,” J. Clin. Microbiol., vol. 58, no. 3, Feb. 2020. [CrossRef]
- F. Bongomin and S. Adetona Fayemiwo, “Epidemiology of fungal diseases in Africa: A review of diagnostic drivers.,” Curr. Med. Mycol., vol. 7, no. 1, pp. 63–70, Mar. 2021. [CrossRef]
- F. C. B. Abdallah et al., “[Pulmonary blastomycosis].,” Pan Afr. Med. J., vol. 36, p. 220, Jul. 2020. [CrossRef]
- I. Wang, Z. Luo, S. Deng, and Q. Li, “A young male with chronic nonproductive cough diagnosed with blastomycosis in China: a case report.,” BMC Pulm. Med., vol. 20, no. 1, p. 189, Jul. 2020. [CrossRef]
- A. Kumar, A. Kunoor, M. Eapen, P. K. Singh, and A. Chowdhary, “Blastomycosis misdiagnosed as tuberculosis, india.,” Emerging Infect. Dis., vol. 25, no. 9, pp. 1776–1777, 2019. [CrossRef]
- R. Cordeiro, S. Moura, D. Castelo-Branco, M. F. Rocha, R. Lima-Neto, and J. J. Sidrim, “Coccidioidomycosis in brazil: historical challenges of a neglected disease.,” J Fungi (Basel), vol. 7, no. 2, Jan. 2021. [CrossRef]
- N. F. Crum, “Coccidioidomycosis: A contemporary review.,” Infect. Dis. Ther., vol. 11, no. 2, pp. 713–742, Apr. 2022. [CrossRef]
- J. W. Taylor and B. M. Barker, “The endozoan, small-mammal reservoir hypothesis and the life cycle of Coccidioides species.,” Med. Mycol., vol. 57, no. Supplement_1, pp. S16–S20, Feb. 2019. [CrossRef]
- R. H. Johnson, R. Sharma, R. Kuran, I. Fong, and A. Heidari, “Coccidioidomycosis: a review.,” J. Investig. Med., vol. 69, no. 2, pp. 316–323, Feb. 2021. [CrossRef]
- A. M. Scott et al., “Examining Miliary Disease Etiology in a Coccidioides-Endemic Center: A Retrospective Cohort Study.,” J Fungi (Basel), vol. 10, no. 1, Dec. 2023. [CrossRef]
- K. Sri, A. Vaithy, S. Kathirvelu, and S. Srinivasan, “Coccidioidomycosis lymphadenopathy: an unusual presentation.,” BMJ Case Rep., vol. 16, no. 7, Jul. 2023. [CrossRef]
- D. H. Caceres and A. Valdes, “Histoplasmosis and Tuberculosis Co-Occurrence in People with Advanced HIV.,” J Fungi (Basel), vol. 5, no. 3, Aug. 2019. [CrossRef]
- M. P. N. Kuate, B. E. Ekeng, R. Kwizera, C. Mandengue, and F. Bongomin, “Histoplasmosis overlapping with HIV and tuberculosis in sub-Saharan Africa: challenges and research priorities.,” Ther. Adv. Infect. Dis., vol. 8, p. 20499361211008676, Apr. 2021. [CrossRef]
- J. Baker, C. Kosmidis, A. Rozaliyani, R. Wahyuningsih, and D. W. Denning, “Chronic Pulmonary Histoplasmosis-A Scoping Literature Review.,” Open Forum Infect. Dis., vol. 7, no. 5, p. ofaa119, May 2020. [CrossRef]
- M. Nacher et al., “A Simple Predictive Score to Distinguish between Disseminated Histoplasmosis and Tuberculosis in Patients with HIV.,” J Fungi (Basel), vol. 8, no. 1, Dec. 2021. [CrossRef]
- A. E. Ekeng, R. O. Oladele, U. E. Emanghe, E. A. Ochang, and T. Y. Mirabeau, “Prevalence of Histoplasmosis and Molecular Characterization of Histoplasma species in Patients with Presumptive Pulmonary Tuberculosis in Calabar, Nigeria.,” Open Forum Infect. Dis., vol. 9, no. 8, p. ofac368, Aug. 2022. [CrossRef]
- M. Agarwal and B. J. Shadrach, “Acute pulmonary histoplasmosis masquerading as miliary tuberculosis in a non-endemic region.,” Adv. Respir. Med., vol. 89, no. 4, pp. 464–465, Jul. 2021. [CrossRef]
- K. Anot, S. Sharma, M. Gupta, and D. Kaur, “Disseminated histoplasmosis and tuberculosis: dual infection in a non-endemic region.,” BMJ Case Rep., vol. 13, no. 8, Aug. 2020. [CrossRef]
- V. Dutta, M. Chopra, U. B. Kovilapu, and G. P. S. Gahlot, “Solitary pulmonary nodule: An interesting clinical mimicry of pulmonary tuberculosis.,” Med. J. Armed Forces India, vol. 75, no. 1, pp. 115–118, Jan. 2019. [CrossRef]
- V. Ramesh, S. Narreddy, S. Gowrishankar, R. Barigala, and S. Nanda, “A challenging case of pyrexia of unknown origin: adrenal histoplasmosis mimicking tuberculosis in a patient with chronic hepatitis C.,” Trop. Doct., vol. 51, no. 4, pp. 621–623, Oct. 2021. [CrossRef]
- M. Astekar, P. S. Bhatiya, and G. V. Sowmya, “Prevalence and characterization of opportunistic candidal infections among patients with pulmonary tuberculosis.,” J. Oral Maxillofac. Pathol., vol. 20, no. 2, pp. 183–189, 2016. [CrossRef]
- A. Azim and A. Ahmed, “Diagnosis and management of invasive fungal diseases in non-neutropenic ICU patients, with focus on candidiasis and aspergillosis: a comprehensive review.,” Front. Cell. Infect. Microbiol., vol. 14, p. 1256158, Mar. 2024. [CrossRef]
- Y. Shweihat, J. Perry, and D. Shah, “Isolated Candida infection of the lung.,” Respir. Med. Case Rep., vol. 16, pp. 18–19, Mar. 2015. [CrossRef]
- M. Hadadi-Fishani, A. Shakerimoghaddam, and A. Khaledi, “Candida coinfection among patients with pulmonary tuberculosis in Asia and Africa; A systematic review and meta-analysis of cross-sectional studies.,” Microb. Pathog., vol. 139, p. 103898, Feb. 2020. [CrossRef]
- R. Khanduri, S. Khanduri, S. Kumar, A. Saini, and A. Kotwal, “Drug-resistant tuberculosis coexisting with invasive candidiasis in an immunocompetent 30-year-old woman: A case report.,” Indian J. Tuberc., vol. 64, no. 3, pp. 232–234, Jul. 2017. [CrossRef]
- A. Kumar, C. Agarwal, A. K. Hooda, A. Ojha, M. Dhillon, and K. V. S. Hari Kumar, “Profile of infections in renal transplant recipients from India.,” J. Family Med. Prim. Care, vol. 5, no. 3, pp. 611–614, 2016. [CrossRef]
- J. Bao et al., “Clinical Manifestations of Pulmonary Mucormycosis in Recipients of Allogeneic Hematopoietic Stem Cell Transplantation: A 21-Case Series Report and Literature Review.,” Can. Respir. J., vol. 2022, p. 1237125, Jun. 2022. [CrossRef]
- H. Prakash and A. Chakrabarti, “Global epidemiology of mucormycosis.,” J. Fungi, vol. 5, no. 1, Mar. 2019. [CrossRef]
- R. Agrawal, A. Yeldandi, H. Savas, N. D. Parekh, P. J. Lombardi, and E. M. Hart, “Pulmonary mucormycosis: risk factors, radiologic findings, and pathologic correlation.,” Radiographics, vol. 40, no. 3, pp. 656–666, Mar. 2020. [CrossRef]
- A. Aggarwal, J. Chander, A. K. Janmeja, and R. Katyal, “Pulmonary tuberculosis and mucormycosis co-infection in a diabetic patient.,” Lung India, vol. 32, no. 1, pp. 53–55, 2015. [CrossRef]
- P. Dube, R. Saroa, and S. Palta, “Coinfections in Intensive Care Unit with pulmonary tuberculosis and mucormycosis: A clinical dilemma.,” Indian J. Crit. Care Med., vol. 20, no. 3, pp. 191–193, Mar. 2016. [CrossRef]
- J. Ramesh, G. Kaur, D. Deepak, and P. Kumar, “Disseminated pulmonary mucormycosis with concomitant tuberculosis infection in a diabetic patient.,” Int. J. Mycobacteriol., vol. 9, no. 1, pp. 95–97, 2020. [CrossRef]
- L. Ramachandran, S. Dewan, V. Kumar, and B. Wankhade, “Mucormycosis causing pulmonary artery aneurysm.,” Respir. Med. Case Rep., vol. 16, pp. 71–73, Jul. 2015. [CrossRef]
- “WHO fungal priority pathogens list to guide research, development and public health action.” [Online]. Available: https://www.who.int/publications/i/item/9789240060241. [Accessed: 05-Oct-2024].
- A. Mendonça, H. Santos, R. Franco-Duarte, and P. Sampaio, “Fungal infections diagnosis - Past, present and future.,” Res. Microbiol., vol. 173, no. 3, p. 103915, 2022. [CrossRef]
- O. A. Cornely et al., “Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium.,” Lancet Infect. Dis., vol. 19, no. 12, pp. e405–e421, Dec. 2019. [CrossRef]
- S. N. Baxi, M. R. Gohil, A. J. Navadiya, M. K. Bapodra, and H. R. Patel, “Comparative evaluation of histopathological analysis, KOH wet mount and fungal culture to diagnose fungal infections in post-COVID patients.,” Indian J. Pathol. Microbiol., vol. 66, no. 3, pp. 540–544, 2023. [CrossRef]
- R. Jandial, M. Choudhary, and K. Singh, “Histomorphological spectrum of fungal infections,” Int. J. Res. Med. Sci., vol. 7, no. 11, p. 4166, Oct. 2019. [CrossRef]
- R. Seth, I. Xess, and M. Jana, “Diagnosis of invasive fungal infections in children.,” Indian Pediatr., vol. 56, no. 3, pp. 229–236, Mar. 2019. [CrossRef]
- A. Vaishnav, G. Gurukiran, O. Ighodaro, and V. Kandi, “Radiological and imaging evidence in the diagnosis and management of microbial infections: an update.,” Cureus, vol. 15, no. 11, p. e48756, Nov. 2023. [CrossRef]
- Z. Ahmad, S. Bagchi, P. Naranje, S. K. Agarwal, and C. J. Das, “Imaging spectrum of pulmonary infections in renal transplant patients.,” Indian J. Radiol. Imaging, vol. 30, no. 3, pp. 273–279, Oct. 2020. [CrossRef]
- S. B. Grover, H. Grover, N. Antil, S. Patra, M. K. Sen, and D. Nair, “Imaging approach to pulmonary infections in the immunocompromised patient.,” Indian J. Radiol. Imaging, vol. 32, no. 1, pp. 81–112, Mar. 2022. [CrossRef]
- P. Ramanan, N. L. Wengenack, and E. S. Theel, “Laboratory diagnostics for fungal infections: A review of current and future diagnostic assays.,” Clin. Chest Med., vol. 38, no. 3, pp. 535–554, May 2017. [CrossRef]
- A. K. Ghosh, A. Gupta, S. M. Rudramurthy, S. Paul, V. K. Hallur, and A. Chakrabarti, “Fungal keratitis in north india: spectrum of agents, risk factors and treatment.,” Mycopathologia, vol. 181, no. 11–12, pp. 843–850, Dec. 2016. [CrossRef]
- www.icmr.gov.in/icmrobject/custom_data/pdf/resource-guidelines/Mycology_SOP_2nd_Ed_2019.pdf.
- C. A. Hage et al., “Microbiological laboratory testing in the diagnosis of fungal infections in pulmonary and critical care practice. an official american thoracic society clinical practice guideline.,” Am. J. Respir. Crit. Care Med., vol. 200, no. 5, pp. 535–550, Sep. 2019. [CrossRef]
- A. Liu et al., “Comparison of diagnostic efficiency of detecting IgG and IgE with immunoassay method in diagnosing ABPA: a meta-analysis.,” BMC Pulm. Med., vol. 23, no. 1, p. 374, Oct. 2023. [CrossRef]
- T. Takazono and K. Izumikawa, “Recent advances in diagnosing chronic pulmonary aspergillosis.,” Front. Microbiol., vol. 9, p. 1810, Aug. 2018. [CrossRef]
- R. Gunasekaran et al., “Rapid Point-of-Care Identification of Aspergillus Species in Microbial Keratitis.,” JAMA Ophthalmol., vol. 141, no. 10, pp. 966–973, Oct. 2023. [CrossRef]
- D. H. Caceres, T. Chiller, and M. D. Lindsley, “Immunodiagnostic assays for the investigation of fungal outbreaks.,” Mycopathologia, vol. 185, no. 5, pp. 867–880, Oct. 2020. [CrossRef]
- R. Gudisa, R. Harchand, and S. M. Rudramurthy, “Nucleic-Acid-Based Molecular Fungal Diagnostics: A Way to a Better Future.,” Diagnostics (Basel), vol. 14, no. 5, Feb. 2024. [CrossRef]
- S. Srinivas, P. Kumari, and D. K. Gupta, “Utility of Panfungal PCR in the diagnosis of invasive fungal infections in febrile neutropenia.,” J. Family Med. Prim. Care, vol. 10, no. 7, pp. 2533–2540, Jul. 2021. [CrossRef]
- V. Poplin, C. Smith, D. Milsap, L. Zabel, and N. C. Bahr, “Diagnosis of pulmonary infections due to endemic fungi.,” Diagnostics (Basel), vol. 11, no. 5, May 2021. [CrossRef]
- Y. Liu, W. Wu, Y. Xiao, H. Zou, S. Hao, and Y. Jiang, “Application of metagenomic next-generation sequencing and targeted metagenomic next-generation sequencing in diagnosing pulmonary infections in immunocompetent and immunocompromised patients.,” Front. Cell. Infect. Microbiol., vol. 14, p. 1439472, Aug. 2024. [CrossRef]
- S. Naik et al., “Utilizing Next-Generation Sequencing: Advancements in the Diagnosis of Fungal Infections.,” Diagnostics (Basel), vol. 14, no. 15, Aug. 2024. [CrossRef]
- A. K. Ghosh et al., “Matrix-assisted laser desorption ionization time-of-flight mass spectrometry for the rapid identification of yeasts causing bloodstream infections.,” Clin. Microbiol. Infect., vol. 21, no. 4, pp. 372–378, Apr. 2015. [CrossRef]
- S. Paul, P. Singh, S. M. Rudramurthy, A. Chakrabarti, and A. K. Ghosh, “Matrix-assisted laser desorption/ionization-time of flight mass spectrometry: protocol standardization and database expansion for rapid identification of clinically important molds.,” Future Microbiol., vol. 12, pp. 1457–1466, Dec. 2017. [CrossRef]
- M. Roy, S. Karhana, M. Shamsuzzaman, and M. A. Khan, “Recent drug development and treatments for fungal infections.,” Braz. J. Microbiol, vol. 54, no. 3, pp. 1695–1716, Sep. 2023. [CrossRef]
- L. Guo et al., “Clinical Characteristics and the Prognostic Impact of Acute Kidney Injury in Critically Ill Patients with Invasive Pulmonary Aspergillosis in the Intensive Care Unit: A Retrospective, Single-Center Study.,” Kidney Dis (Basel), vol. 10, no. 4, pp. 262–273, Aug. 2024. [CrossRef]
- R. Agarwal et al., “Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses.,” Eur. Respir. J., vol. 63, no. 4, Apr. 2024. [CrossRef]
- M. Aruanno, E. Glampedakis, and F. Lamoth, “Echinocandins for the Treatment of Invasive Aspergillosis: from Laboratory to Bedside.,” Antimicrob. Agents Chemother., vol. 63, no. 8, Aug. 2019. [CrossRef]
- Q. Li, D. Wen, Y. Chen, L. Yang, J. Li, and S. Luo, “Early respiratory interventional therapy combined with antifungal agent for endobronchial cryptococcosis: A case report and literature review.,” Medicine (Baltimore), vol. 103, no. 12, p. e37455, Mar. 2024. [CrossRef]
- K. Przywara, R. Adamski, M. Książczyk, J. Suchodolski, and M. Cal, “3-bromopyruvate induces morphological alteration and may initiate programmed cell death in Cryptococcus neoformans cells.,” Arch. Microbiol., vol. 206, no. 4, p. 153, Mar. 2024. [CrossRef]
- T. Kitazawa et al., “Efficacies of atovaquone, pentamidine, and trimethoprim/sulfamethoxazole for the prevention of Pneumocystis jirovecii pneumonia in patients with connective tissue diseases.,” J. Infect. Chemother., vol. 25, no. 5, pp. 351–354, May 2019. [CrossRef]
- J.-A. Tabanor and S. Lakshminarayanan, “Do patients on biologic drugs for rheumatic disease need PCP prophylaxis?,” Cleve. Clin. J. Med., vol. 86, no. 7, pp. 449–453, Jul. 2019. [CrossRef]
- G. R. Thompson et al., “Global guideline for the diagnosis and management of the endemic mycoses: an initiative of the European Confederation of Medical Mycology in cooperation with the International Society for Human and Animal Mycology.,” Lancet Infect. Dis., vol. 21, no. 12, pp. e364–e374, Dec. 2021. [CrossRef]
Figure 1.
Diagnostic tools for fungal infections in patients with pulmonary diseases.
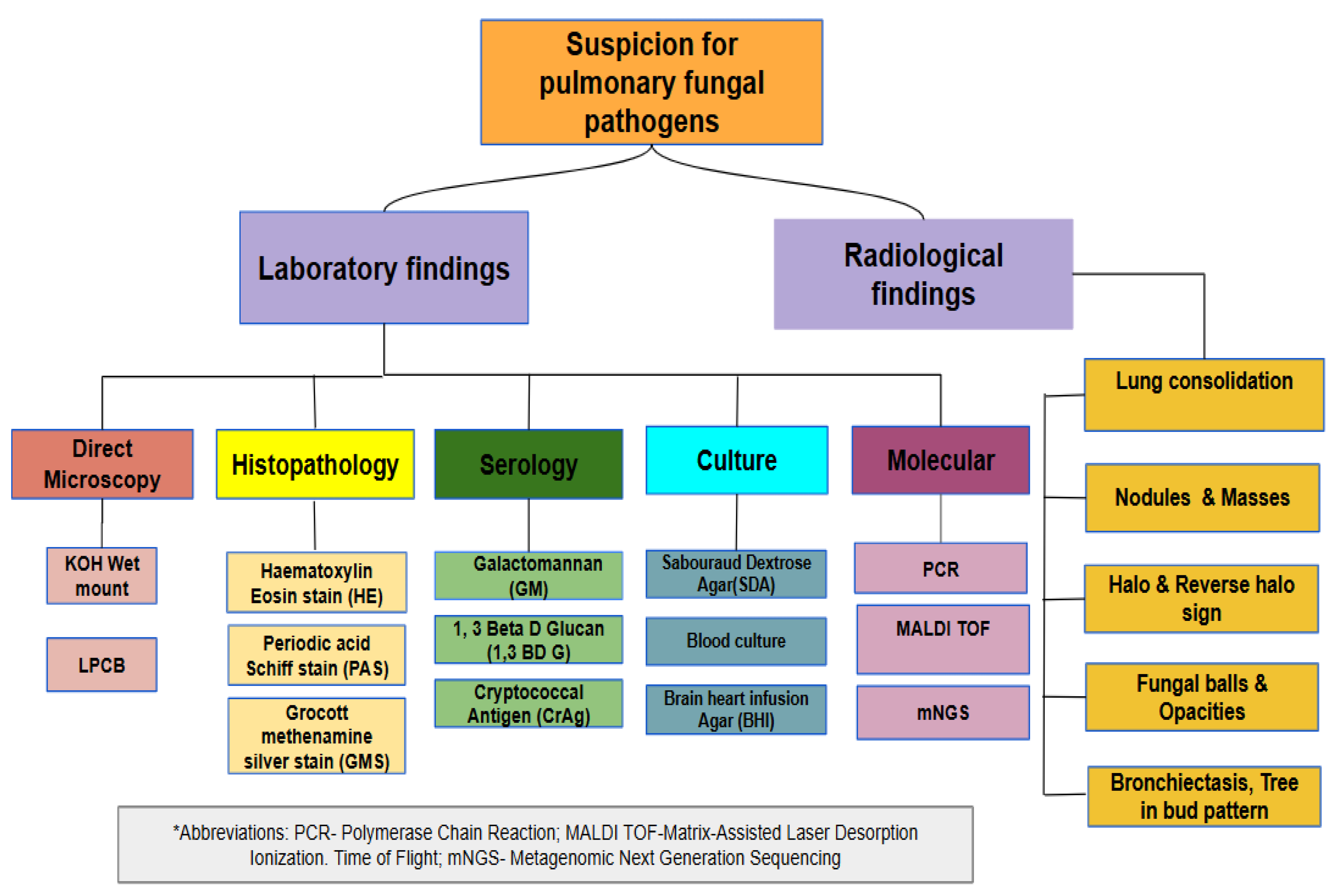

Table 1.
Recent studies on Aspergillosis with or without TB across India.
| Type of Aspergillosis | Reported State & Year | Type of Study | Study population | Number of isolates | Salient Findings | Reference |
|---|---|---|---|---|---|---|
| Chronic Pulmonary Aspergillosis | New Delhi 2024 | Prospective | 255- Recruited 158- Completed follow up | 11.1% were positive at baseline, and 27.5% were positive at the end of ATT | CPA may arise after anti-tubercular treatment or be present at the time of diagnosis in patients with newly diagnosed tuberculosis. | Jha et al. [22]. |
| Chronic Pulmonary Aspergillosis | Chandigarh 2024 | Prospective | 111- Of which 53 were control | 52.25%- Proven CPA | Compared to controls, those with CPA related to PTLA exhibit reduced Th-1 response and decreased neutrophil oxidative burst. | Chirumamilla et al [23] |
| Chronic Pulmonary Aspergillosis | Maharashtra 2023 | Cross-sectional/Observational | 42 | 9.5% | Serological diagnosis is necessary for detecting CPA in patients with or without TB due to similar clinical features. | Rajpurohit et al [24] |
| Chronic Pulmonary Aspergillosis | New Delhi 2022 | Prospective-Observational | 130 | 24.2% | While a differential diagnosis is needed for CPA and TB, the mediastinal necrotic lymph node is the proper CT finding for differentiating between recurrent TB and post-TB sequelae. | Bharath et al. [25] |
| Chronic Pulmonary Aspergillosis | India 2022 |
Estimation Analysis | - | - | Comprehensive estimation of total CPA burden in pulmonary TB patients | Denning et al. [20] |
| Chronic Pulmonary Aspergillosis | Chandigarh 2023 | Retrospective | 434 subjects and 20 disease controls - | - | The significance of Erythrocyte Sedimentation rate (ESR) and C-reactive protein (CRP) in CPA diagnosis among Post Tuberculosis Lung Disease PTLD has been established by this study. | Sehgal et al [26] |
| Aspergilloma | Uttarakhand 2023 | Case Report | - | 1 | This Case was reported after a decade of undergoing ATT where, unusually, Aspergilloma was found as a mass in the intrabronchial region instead of a lung cavity. | Lahiri et al [27] [59] |
| Invasive Pulmonary Aspergillosis | Chandigarh 2022 | Case Report | - | 1 | Sequelae of COVID-19 complicated by TB and IPA | Gandotra et al. [28] |
| Chronic Cavitary Pulmonary Aspergillosis | Karnataka 2022 | Case Report | - | 1 | About 20 years ago, a patient had tuberculosis and aspergilloma. COVID-19 had reactivated latent aspergilloma, and the condition developed into CCPA, a more severe form of aspergillosis. | Chaurasia et al [29] |
Table 2.
Recent studies on Cryptococcosis with or without TB across India.
| Reported State/ Year | Type of Study | Study Population | Number of isolates | Site of infection | Salient Findings | Reference |
|---|---|---|---|---|---|---|
| New Delhi 2019 | Case Report | - | 1 | Lung | Initially treated for TB due to misdiagnosis but later diagnosed as Cryptococcosis. | Meena et al. [43] |
| New Delhi 2019 | Case Report | - | 1 | Thoracic spine | Empirically treated for TB before being diagnosed with Cryptococcus Osteomyelitis and was treated with voriconazole for 8 weeks. | Adsul et al. [44] |
| New Delhi 2018 | Case Report | - | 1 | Lung and CNS | Disseminated Cryptococcosis mimicking TB- Reported in an immunocompetent child | Ismail et al [45] |
| New Delhi 2016 | Case Report | - | 1 | Lung | The co-existence of Pulmonary Cryptococcosis and tuberculosis was reported. Treated with fluconazole and anti-tubercular therapy | Jain et al [46], [47] |
| New Delhi 2016 | Case Report | - | 1 | Lung | They had a history of TB, a right lower lobe mass similar to a lung tumor, but was eventually diagnosed as Cryptococcoma through CT and histopathological examination. | Pawar et al [47] |
| Chandigarh 2017 | Retrospective | 42 | 2 | Lung | This introspects the significance of Fine Needle Aspiration Cytology(FNAC) as a rapid method of diagnosis in immunocompromised patients. | Sharma et al. [48] |
| New Delhi 2015 | Case Report | - | 1 | Lung / Adrenal gland | A 65-year-old adult male with no history of TB was reportedly diagnosed with Cryptococcosis mimicking TB. Still, CT findings indicated that the abnormality was due to the fungal pathogen Cryptococcus spp. | Ranjan et al [49] |
Table 3.
Recent studies on Pneumocystis pneumonia with or without TB across India.
| Reported State/ Year | Type of Study | Study Population | Number of isolates | Site of infection | Salient Findings | Reference |
|---|---|---|---|---|---|---|
| Uttarakhand 2024 | Case Report | - | 1 | Lung | HIV, Pneumothorax, and TB- A rare coexistence of three pathogens | Jithesh et al. [55] |
| Maharashtra 2016 | Retrospective | 111- HIV Patients | 3(5.76%) | Lung | Of the respiratory manifestations in HIV seropositive subjects, TB is the most common. Pneumocystis was also recorded in 3 patients. | Patil et al. [56] |
| Karnataka 2015 | Prospective | 74 PLHIV -People living with HIV (37 with diabetes mellitus (DM) and 37 without DM) | 5% among DM and 18% among those without DM | Lung | EP-TB was diagnosed among 22% of the study population, while the study also recognized the significance of Pneumocystis infection | Indhira et al [57] |
| Karnataka 2015 | Descriptive | 164- HIV population | 16% | Lung | Among opportunistic infections, 50% were reported as TB in this study. | Ramesh et al [58] |
Table 4.
Recent studies on Histoplasmosis with or without TB across India.
| Reported Year | Type of Study | Study Population | Number of isolates | Site of infection | Salient Findings | Reference |
|---|---|---|---|---|---|---|
| Rajasthan 2021 | Case Report | - | 1 | Lung | Pulmonary histoplasmosis misdiagnosed as miliary tuberculosis | Agarwal et al [77] |
| Chandigarh 2020 | Case Report | - | 1 | Skin, Lung | Disseminated TB and histoplasmosis co-infection was reported in a 50-year-old male. | Anot et al [78] |
| New Delhi 2019 | Case Report | - | 1 | Lung | A 59-year-old female with a history of cutaneous TB was presented with manifestations such as fever and dry cough. Multi Drug Resistant-TB was suspected due to substantial evidence from CT images. Eventually a PET scan was performed which revealed soft tissue nodule, histopathological examination suggested the presence of H. capsulatum. | Dutta et al [79] |
| Telangana 2018 | Case Report | - | 1 | Adrenal gland, lung | Hepatitis C confirmed, case with fever, treated for four months with ATT for suspected TB but was finally diagnosed as Histoplasmosis which mimics TB in clinical manifestations. | Ramesh et al [80] |
Table 5.
Recent studies on Candidiasis with or without TB across India.
| Reported State/ Year | Type of Study | Study Population | Number of isolates | Site of infection | Salient Findings | Reference |
|---|---|---|---|---|---|---|
| Uttarakhand 2016 | Case Report | - | 1 | Lung | Coexistence of drug-resistant tuberculosis with invasive candidiasis | Khanduri et al [85] |
| Rajasthan2016 | Prevalence Study | 60 confirmed Pulmonary TB patients | 33 | Lung | Prevalence of candidal presence in sputum samples among pulmonary tuberculosis patients was reported using SDA and ChromAgar cultures. | Astekar et al [81] |
| Maharashtra 2016 | Prospective observational Study | 45- Renal transplant recipients (RTR) | 7 | - | Among renal transplant recipients, TB with candidiasis and CMV with TB was found in 7 patients | Kumar et al [86] |
| Karnataka2015 | Descriptive Study | 164- HIV positive patients | 80 | Lung | This study reported that TB and candidiasis were most frequently occurring opportunistic infections among HIV patients which were concreted by several other studies from India. | Ramesh et al [58] |
Table 6.
Recent case reports on Mucormycosis with or without TB across India.
| State | Year | Site of infection | Salient Findings | Reference |
|---|---|---|---|---|
| Chandigarh2015 | 2015 | Lung | Coinfection of Tuberculosis and mucormycosis in a diabetic patient was reported. | Aggarwal et al [90] |
| Puducherry 2016 | 2016 | Lung | Pulmonary TB with mucormycosis co-infection was demonstrated in a diabetic patient admitted to the intensive care Unit. | Dube et al [91] |
| New Delhi2020 | 2020 | Lung | Disseminated pulmonary mucormycosis and tuberculosis co-infection in a diabetic patient was reported. | Ramesh et al [92] |
| Uttar Pradesh2015 | 2015 | Lung | Pulmonary artery aneurysm, a rare condition, and its association with pulmonary mucormycosis was reported. | Ramachandran et al [93] |
Table 7.
Antifungal and biologic agents used for treatment of pulmonary mycoses.
| Pulmonary Mycosis | Antifungal Agents | Biological Agents |
|---|---|---|
| Aspergillosis | Voriconazole, Amphotericin B, Caspofungin, Posaconazole [119] | Omalizumab, Mepolizumab, Benralizumab, Dupilumab, Tezepelumab [120] , Echinocandins [121] |
| Cryptococcosis | Fluconazole, Amphotericin B, Amphotericin B with flucytosine [122] | 3-Bromopyruvate - Anticancer agent with excellent fungicidal activity [123] |
| Pneumocystis pneumonia | Trimethoprim-sulfamethoxazole, pentamidine, & Atovaquone [124] | Adalimumab, Certolizumab, Etanercept, Golimumab, Infliximab- these anti-tumor necrosis factor alpha agents used for Rheumatoid arthritis patients have been involved in Pneumocystis development [125] |
| Endemic mycoses | Itraconazole, Fluconazole, Voriconazole, Posaconazole, Isavuconazole and Corticosteroids [126]. | Promising research is currently underway to develop biological agents for the treatment of endemic mycoses. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



