Submitted:
18 March 2025
Posted:
18 March 2025
Read the latest preprint version here
Abstract
Food hypersensitivity remains an understudied and overlooked subject globally. It is characterized by adverse reactions to dietary substances potentially triggered by various mechanisms. Food allergy, a subset of food hypersensitivity, denotes an immune response to food proteins categorized into immunoglobulin IgE-mediated or non-IgE-mediated reactions. Conversely, food intolerance, another facet of food hypersensitivity, refers to non-immunological reactions occurring at typically tolerated doses of food or its components. The main objective of this study is to determine and differentiate the differences, characteristics, and types of food hypersensitivities. We conducted an extensive review encompassing the key studies from 1990 onwards, including prospective studies, nested case-control studies, and meta-analysis. In conclusion, there are big differences between the main characteristics such as symptoms, complications, and treatments between allergies, and food intolerances. Commonly reported trigger foods include cow milk, gluten, eggs, nuts, and seafood.
Keywords:
food hypersensitivity
; food allergy
; food intolerance
; clinical manifestations
; IBS
1. Introduction
Food hypersensitivity is a prevalent condition affecting individuals worldwide, characterized by adverse reactions to specific food components [1]. It encompasses both food allergies and immune-mediated reactions and intolerances (non-immune mediated reactions), which can manifest with a variety of symptoms, ranging from mild discomfort to severe life-threatening reactions [1] such as skin manifestations (rash, dermatitis, rosacea, angioedema), gastrointestinal symptoms (bloating, diarrhea, constipation, gas, reflux, macro and micronutrients malabsorption), and respiratory symptoms (anaphylactic shock, shortness of breath, nasal congestion, rhinorrhea, sneezing, itching of the nose and throat, coughing, and wheezing) [1]. Distinguishing between food allergy and intolerance is crucial for appropriate management and treatment strategies [2] (Figure 1). This systematic review aims to elucidate the differences between food allergies and intolerances, including their epidemiology, pathophysiology, clinical manifestations, diagnostic approaches, and management strategies. By understanding the nuances of these conditions, healthcare professionals can provide better care, treatment, prevention, and nutritional management, and improve the quality of life for individuals suffering from food hypersensitivities.
2. Material and Methods
We conducted research utilizing the Medline database, accessed via its search engine, PubMed. We used the following Medical Subject Headings (MeSH) terms or text words: “Food hypersensitivity” or “food allergies” or “Food intolerances”
Studies included in this review focused on human studies published in English, with publication dates from 1990 onwards. Specifically, we prioritized prospective studies, meta-analyses, systematic reviews, narrative reviews, and nested case-control studies.
Studies excluded: Studies published before 1990, animal studies, non-English language articles
For precision purposes, two researchers reviewed all relevant articles independently to check for any discrepancies and to ensure rigorous data extraction. For each article, we focused on the key study characteristics, including publication year, country of origin, study design, sample size, and participant characteristics.
Details of the study selection process are illustrated in Figure 2
The review is divided into 3 sections, highlighting the 2 main components of Food Hypersensitivity, which are food allergies and food intolerance, with the third part being about the relation of Food Hypersensitivity with IBS and the role of the microbiota.
3. Results
3.1. Food Allergies

Table 1.
Main characteristics of included studies.
| Author | Year | Study Type | Country | Sample Size | Duration of Intervention | Summary of Findings |
|---|---|---|---|---|---|---|
| Vassilopoulou et al. [5] | 2022 | Retrospective, observational, multicenter case-control study | Greece | 96 mothers of infants with and 141 mothers of infants without a history of FPIAP. | From May 2018 to November 2020 | Identified cow milk (83%), eggs (7.3%), wheat (6.4%), and beef (6.4%) as the main triggers for allergic proctocolitis in infants through maternal diet. |
| Ruffner et al. [6] | 2013 | Retrospective chart review | USA | 462 cases identified from the hospital patients | From 2007 until 2012 | FPIES reactions were observed more frequently than previously reported, though their presentation and clinical characteristics remained consistent with earlier findings. Milk- and soy-induced FPIES were prevalent, with 43.5% of patients who reacted to milk also experiencing a reaction to soy. |
| Pinto-Sánchez et al. [7] | 2021 | Prospective study | Canada | prospective study of 50 patients with IBS (ROME III, all subtypes), with and without serologic reactivity to gluten (antigliadin IgG and IgA), and 25 healthy subjects (controls) | Between 2012 and 2016 | Evaluated the effectiveness of a gluten-free diet in achieving mucosal healing for celiac patients. |
| Ford et al. [8] | 2014 | Cross Sectional | Canada | 4224 patients recruited | Between January 2008and December 2014 | Functional bowel disorders (FBDs) showed significant demographic and psychological differences among patients. The Rome III classification system did not clearly distinguish between different FBD subtypes. There was considerable symptom overlap among irritable Bowel syndrome (IBS), functional diarrhea, and chronic idiopathic constipation (CIC). The findings suggest a need for improved diagnostic criteria to differentiate FBDs more effectively. |
| Schink et al. [9] | 2018 | Cross sectional observational study | Germany | 64 participants 8 with histamine intolerance (HIT), 25 with food hypersensitivity (FH), 21 with food allergy and 10 healthy controls (HC) |
12 months | Suggested dietary modifications and DAO supplements for histamine intolerance. |
| Halmos et al. [10] | 2014 | Randomized, controlled, cross-over trial | Australia | 30 patients with IBS and 8 healthy individuals (controls, matched for demographics and diet) |
Between April 2009 and June 2011 | Confirmed the efficacy of the low FODMAP diet in IBS symptom reduction. |
| Nwaru et al. [11] | 2014 | Systematic review and meta-analysis | Europe | Not Applicable | Between 1 January 2000 and 30 September 2012 | Highlighted that early introduction of allergenic foods may reduce the risk of developing IgE-mediated food allergies. |
| West et al. [12] | 2014 | Observational population-based study | UK | 57 million | Between 1990 and 2011 | Found that the incidence of celiac disease is increasing, estimating 19.1 per 100,000 cases annually. |
3.1.1. Definition
A food allergy, categorized under food hypersensitivity, refers to an immunological reaction to food proteins [13]. This reaction can involve immunoglobulin IgE-mediated responses, mixed IgE and non-IgE mediated reactions, or non-IgE-mediated responses [4,5]. IgE-mediated food allergies affect millions worldwide, significantly impacting individuals' daily lives [2] The prevalence of food allergies is estimated to affect 10-25% of the global population, with an upward trend observed over the last two decades [14]. The classification of food allergies is summarized in the Figure 1 [3].
3.1.2. Symptoms
Symptoms may affect various systems including the respiratory tract, the gastrointestinal tract, skin, and the cardiovascular system [16]. Respiratory symptoms encompass sneezing, congestion, rhinorrhea, wheezing, and laryngeal edema [16]. Gastrointestinal manifestations consist of nausea, vomiting, abdominal pain, and diarrhea [16]. Cutaneous presentations may include urticaria, angioedema, flushing, or pruritus [16]. Cardiovascular signs may involve tachycardia, hypotension, or syncope [16]. Typically, symptoms manifest within minutes of food ingestion, although they may delay up to 2 hours [16]. The severity ranges from pruritus alone to anaphylactic shock [16]. The symptoms for each food allergy disorder can be found in Table 2 [7].
3.1.3. IgE-Mediated Food Allergies
Regarding IgE-mediated food allergies, they are categorized as type I hypersensitivity reactions. Symptoms typically manifest rapidly, occurring within minutes to a few hours after ingestion. Diagnosis involves a detailed assessment of clinical symptoms and various testing methods, including oral food challenges, food allergy skin prick testing, and specific food IgE testing [15]. Furthermore, IgE-mediated food allergies are characterized by the immune system's production of IgE antibodies in response to specific food proteins, leading to rapid allergic reactions that can range from mild symptoms to anaphylaxis. Several studies have examined the prevalence and mechanisms of these allergies. A study by Sicherer and Sampson, (2016) highlighted that IgE-mediated food allergies are increasing globally, particularly among children, with common allergens including peanuts, tree nuts, and shellfish [17]. Another study by Savage et al., compared different diagnostic approaches, such as oral food challenges and specific IgE testing, noting that while specific IgE testing is useful, it can sometimes result in false positives, making oral food challenges the gold standard for diagnosis [18]. Furthermore, research by Nwaru et al. emphasized that the early introduction of allergenic foods might reduce the risk of developing IgE-mediated food allergies, a finding that has influenced recent guidelines on allergy prevention [11]. These studies collectively underscore the complexity of diagnosing and managing IgE-mediated food allergies and the need for tailored approaches based on individual patient profiles.
Diagnosis methods
The skin prick test (SPT) serves as a common diagnostic tool for identifying type I hypersensitivity reactions. It involves applying an allergen extract onto the skin, typically on the forearm or back, followed by pricking the skin with a lancet [19]. This minimally invasive test offers the advantage of assessing multiple allergens, including inhalants, foods, drugs, venom, latex, and occupational allergens, within a short timeframe of 15-20 minutes, with a high sensitivity of 95-100% [19].
Skin Prick Testing (SPT) is a widely used method for diagnosing IgE-mediated allergic conditions by exposing the skin to small amounts of suspected allergens and observing for a localized allergic reaction. This method is often compared with other diagnostic approaches like specific IgE (sIgE) testing. A study by Heinzerling et al. found that SPT is highly sensitive, particularly to respiratory allergens such as pollen, mold, and dust mites, and provides rapid results, making it a first-line test in many allergy clinics. However, the study also noted variability in results depending on factors like the allergen extract quality, the technique used, and the patient's skin condition at the time of testing [20].
Another study by Bousquet et al., explored the correlation between SPT results and clinical symptoms and found a strong correlation between positive SPT results and clinical manifestations of allergic rhinitis and asthma, though the strength of the correlation can vary depending on the allergen tested [21].
Despite its advantages, SPT has limitations. For instance, as highlighted by Nelson et al., there can be a risk of false negatives, particularly in cases of recent antihistamine use or improper technique [14]. Additionally, false positives can occur due to irritant reactions rather than true allergic sensitizations [14]. Consequently, while SPT remains a cornerstone in allergy diagnostics, especially in respiratory and food allergies, it is often used in conjunction with sIgE testing and a thorough patient history to confirm diagnoses and guide treatment plans [14]. These studies collectively underscore that while SPT is a valuable and widely used diagnostic tool, its results must be interpreted within the broader clinical context, with consideration given to the method's limitations.
In vitro, total IgE testing measures the overall levels of IgE in the bloodstream and lacks specificity. On the other hand, specific IgE testing targets particular allergens, both food and inhalants, through a blood sample collection from the individual [19]. While specific IgE testing provides high sensitivity and specificity, it requires a longer turnaround time, typically around 10-20 days, to obtain results [22].
Specific IgE (sIgE) testing is a widely used diagnostic tool in allergy testing, designed to detect IgE antibodies specific to particular allergens in a patient’s blood. Numerous studies have compared sIgE testing with other diagnostic methods such as skin prick tests (SPT) and component-resolved diagnostics (CRD). For example, Wood et al. found that sIgE testing is particularly sensitive in detecting sensitization to common allergens like pollen, house dust mites, and pet dander [23]. However, the study noted variability in specificity depending on the allergen and the chosen cutoff values [16]. Another study by Matricardi et al., compared sIgE testing to CRD and concluded that CRD offers a more refined identification of allergen sensitization, particularly in distinguishing primary sensitization from cross-reactivity, which is critical in complex allergy cases [24]. Additionally, a study by Zuberbier et al. underscored that while sIgE testing is a powerful tool for detecting allergic sensitizations, it should not be used in isolation due to the potential for false positives, particularly in individuals with high total IgE levels [25]. This analysis highlighted the importance of interpreting sIgE results within the broader context of a patient’s clinical history and other diagnostic tests. Ewan and Dugue also discussed the possibility of false positives in sIgE testing, especially in patients with elevated total IgE levels, further emphasizing the need for a comprehensive approach to allergy diagnosis [26]. These studies collectively suggest that while sIgE testing is valuable in allergy diagnostics, it should be integrated with other diagnostic methods to achieve the most accurate results.
Common allergens and their prevalences according to diagnosis techniques
Food allergies are a growing concern globally, with significant variations in prevalence across different populations and age groups. Studies have consistently identified certain foods as the most common triggers of IgE-mediated allergic reactions, including cow milk, gluten, eggs, wheat, beans, soybean, nuts, and seafood as the primary culprits behind food allergies [27]. A landmark study by Sicherer and Sampson in the United States highlighted that peanut allergy, affecting approximately 1-2% of children, is the most prevalent food allergy in Western countries, with a rising incidence over the past two decades [28]. Another critical review by Gupta et al., explored the burden of food allergies across the globe, noting that while peanut and tree nut allergies are particularly prevalent in Western nations, rice and sesame are more common allergens in Asia and the Middle East, [29]. Moreover, the Australian Health Nuts study emphasized the significant role of environmental and genetic factors in the development of food allergies, with peanut and egg allergies being the most common among Australian children, affecting nearly 10% of infants by the age of one [30]. These studies collectively underscore the importance of geographic and demographic factors in determining the prevalence and types of food allergies, and they highlight the need for region-specific public health strategies to manage and prevent food allergies effectively.
3.1.4. Mixed IgE/Non IgE Mediated Food Allergies
Eosinophilic esophagitis
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated esophageal disease characterized by the infiltration of eosinophils in the esophageal epithelium, leading to symptoms such as dysphagia and food impaction [31]. The rising incidence of EoE has prompted numerous studies aimed at understanding its pathophysiology, prevalence, and treatment options. A pivotal study by Dellon et al., highlighted the increasing prevalence of EoE in both pediatric and adult populations in the United States, noting a significant rise in diagnoses over the past two decades [32]. This study underscored the role of environmental factors, such as food allergens and aeroallergens, in the pathogenesis of EoE [32].
Another key study by Liacouras et al. provided a comprehensive review of diagnostic criteria and treatment guidelines for EoE, emphasizing the importance of dietary management, including elimination diets and the use of proton pump inhibitors (PPIs), in managing the condition [33]. The study compared the effectiveness of different therapeutic approaches, including dietary elimination and pharmacologic treatments, concluding that while both strategies are effective, the choice of the treatment should be individualized based on patient characteristics and preferences [33].
Further research by Hirano et al. explored the long-term outcomes of patients with EoE, revealing that while the disease is chronic and relapsing, early diagnosis and consistent treatment can significantly improve quality of life and reduce the risk of complications such as esophageal strictures) [34]. This study also compared the effectiveness of topical corticosteroids, such as fluticasone and budesonide, with dietary interventions, finding that while corticosteroids are effective in reducing inflammation, dietary changes are crucial in managing symptoms long-term) [34].
Finally, a meta-analysis by Lucendo et al. compared the outcomes of various treatments for EoE, including elimination diets, PPIs, and corticosteroids [35]. The study concluded that while elimination diets are effective in inducing histologic remission, PPIs and corticosteroids also play a vital role, particularly in patients who do not respond to dietary changes [35].
These studies collectively highlight the complex and multifactorial nature of EoE, emphasizing the need for individualized treatment plans that consider both dietary and pharmacologic interventions to manage this chronic condition effectively.
Non IgE mediated food allergies
Non-IgE cell-mediated food allergies pose a greater diagnostic challenge and are categorized into various disorders, including Allergic proctocolitis (AP), Celiac disease/dermatitis herpetiformis, food protein-induced enteropathy (FPE), Heiner syndrome (pulmonary hemosiderosis), food protein-induced enterocolitis syndrome (FPIES), and Cow’s milk (CM) protein-induced iron deficiency anemia [4,5,7].
These allergies are mostly diagnosed during early childhood, except for celiac disease with the main allergens being identified as either wheat, soy and cow milk. [37].
Allergic Proctocolitis
Formerly recognized as allergic colitis, this benign condition primarily affects young children [37]. It is characterized by the presence of bright red blood in the stool (hematochezia), often accompanied by diarrhea, and has been primarily linked to the consumption of cow and soy milk in children [12,13]. Diagnosis of allergic proctocolitis (AP) involves clinical evaluation, laboratory tests, stool examination (fecal calprotectin), endoscopic procedures, and allergy assessments (specific IgE and skin prick testing) [38]. It is marked by mild anemia, elevated eosinophil count (eosinophilia), higher-than-normal total IgE levels, presence of eczema, and hypoalbuminemia [12,13,14]. Treatment typically entails eliminating the offending food trigger, leading to symptom resolution within a maximum of ninety-six hours [37]. According to Elizur et al. the prevalence of AP in young children was 1.6 per 1000 infants [40].
Another study done by Mennini et al. a review study has found that 0.16% of healthy children and 64% of children suffering from blood in stool are in fact suffering from Allergic proctocolitis [41].
Furthermore, Vassilopoulou et al. has found similar results as Mennini et al.[34] in terms of the prevalence of the disease, with cow milk (83%), eggs (7.3%), wheat (6.4%), and beef (6.4%) causing the symptoms of allergic proctocolitis by the ingestion of these food proteins from the mother's diet, which feeds the infant breastfeeding [35].
A 2019 study by Nowak-Węgrzyn et al. provided a comprehensive overview of the condition, emphasizing that while allergic proctocolitis is typically benign and self-limited, occurring in infants within the first few months of life, it requires careful dietary management to avoid complications [42]. This study stressed the importance of eliminating the offending protein from the maternal diet in breastfeeding infants or switching to a hypoallergenic formula for formula-fed infants [5].
A more recent study by Ruffner et al. explored the long-term outcomes of infants diagnosed with allergic proctocolitis, revealing that most children outgrow the condition by the age of one, though a small percentage may develop other atopic conditions later in life. This study highlighted the need for ongoing monitoring, particularly in infants with a family history of atopic diseases [6].
Further research by Caubet et al. emphasized the role of maternal diet during pregnancy and breastfeeding in the prevention and management of allergic proctocolitis, suggesting that maternal dietary restrictions can significantly reduce the incidence and severity of symptoms in infants at risk [43]. This study provided evidence supporting the early identification and elimination of food allergens as a key strategy in managing allergic proctocolitis effectively [43].
These studies collectively highlight the evolving understanding of allergic proctocolitis, emphasizing the importance of personalized dietary management strategies, ongoing monitoring, and the potential benefits of maternal dietary modifications. They underline the significance of early diagnosis and intervention to prevent long-term complications and ensure optimal growth and development in affected infants.
Celiac disease/dermatitis herpetiformis
Celiac disease (CD) is an immune-mediated disorder characterized by a permanent immune response triggered by consuming gluten-containing foods such as wheat, barley, and rye [44]. Classified as an enteropathy, it leads to severe malabsorption of several vitamins (D, B12, B6), minerals (iron), and macronutrients due to the atrophy of intestinal villi, primarily in the duodenum, rendering individuals with CD susceptible to various nutritional deficiencies [17,18]. Most of CD patients are reported to carry haplotype HLA DR3-DQ2 and/or DR4-DQ8, which serves as a susceptibility indicator for predicting celiac disease [47]. Endoscopic duodenal intestinal biopsy is considered the gold standard for diagnosing celiac disease [45]. Serologic testing, including tissue transglutaminase (TTG), endomysia antibody (EMA), deamidated gliadin peptide (DGP), and antigliadin antibodies (AGAs), can help in suspecting CD, with AGAs being less specific and gradually replaced by newer tests like EMA, TTG, and DPG [46]. Treatment involves completely eliminating gluten from the diet for life, which resolves intestinal damage [46], and 1.4% of the global population is estimated to be suffering from celiac disease [48].
According to West et Al., the incidence of celiac disease was estimated to be around 19.1 per 100,000 which has been increasing since the early 2000s [12].
A 2020 study by Lebwohl et al., investigated the global prevalence of celiac disease, finding significant geographical variation, with higher rates in Europe and the United States compared to Asia and Africa [49]. This study underscored the role of genetic predisposition and environmental factors in the development of the disease [49].
In contrast, a 2019 study by Ludvigsson et al. focused on the diagnostic approaches, comparing serological tests such as anti-tissue transglutaminase (tTG) antibodies with biopsy findings [50]. The study emphasized the high sensitivity and specificity of tTG testing, making it a cornerstone in the non-invasive diagnosis of celiac disease, though biopsies remain the gold standard for confirmation [50].
A 2021 systematic review by Pinto-Sánchez et al. evaluated various dietary management strategies, particularly the effectiveness of a strict gluten-free diet (GFD) in achieving mucosal healing and reducing symptoms [7]. The review concluded that while most patients benefit from a GFD, there is a subset of patients with non-responsive celiac disease who may require additional interventions, such as the exclusion of trace gluten or refractory celiac disease therapies [7].
Further research by Rubio-Tapia et al. explored the long-term outcomes of patients with celiac disease, particularly focusing on the risks of complications such as enteropathy-associated T-cell lymphoma (EATL) [51]. This study highlighted the importance of early diagnosis and strict adherence to a GFD to reduce the risk of such severe complications [51].
These studies collectively contribute to a nuanced understanding of celiac disease, highlighting the importance of early and accurate diagnosis, effective management through a strict gluten-free diet, and ongoing monitoring to prevent complications and improve quality of life.
Similarly, Dermatitis herpetiformis (DH) is an autoimmune skin condition characterized by the formation of small blisters or papules, rash, and urticaria, typically appearing on the elbows, knees, and buttocks [52]. DH shares a similar genetic background with CD, with some researchers considering it a subtype of CD [53]. The incidence of DH is decreasing globally, while CD is on the rise, with DH more prevalent in males and CD in females [20,21]. Diagnosis of DH primarily involves examining clinical signs and symptoms and confirming them through direct immunofluorescence examination of perilesional skin, revealing granular immunoglobulin A (IgA) in the papillary dermis [20,21]. Patients with DH may also experience gastrointestinal symptoms and nutritional deficiencies related to CD, which resolve upon complete gluten avoidance [20]. Although adopting a gluten-free diet resolves urticaria and blisters, it may take months to years for skin symptoms to completely clear [20,21].
DH’s incidence is estimated at 0.8 per 100,000 people [22]. The prevalence is thought to be between 11.2 to 75.3 per 100 000 individuals [54]. Another study conducted by Antiga et al. [55] has shown the same prevalence number in the population while additionally showing that the disease is almost absent in African and Asian populations while being frequent in the Caucasian population. This is mainly due to the absence of the human leukocyte haplotypes (HLA) DQ2 and DQ8 from the African and Asian populations and low wheat consumption in these regions [55].
Reunala et al. confirmed that DH is a specific manifestation of celiac disease, with nearly all patients exhibiting some degree of intestinal involvement, even if asymptomatic [56]. This study highlighted the importance of adhering to a strict gluten-free diet (GFD) as the primary treatment for DH, alleviates the skin symptoms and addresses the underlying intestinal inflammation associated with celiac disease [56].
Further research by Mansikka et al., provided insights into the epidemiology of DH, showing that its incidence has decreased over the past few decades, likely due to better recognition and earlier diagnosis of celiac disease [57]. This population-based study from Finland reported a decrease in the prevalence of DH, which the authors attributed to the widespread adoption of gluten-free diets among individuals with celiac disease and the earlier initiation of treatment before the development of skin symptoms [57].
Additionally, Collin et al. examined the long-term outcomes of DH patients, particularly focusing on the risk of associated autoimmune diseases and malignancies [58]. Their findings suggested that while DH patients on a strict GFD had a similar overall mortality risk as the general population, those who did not strictly adhere to the diet had an increased risk of developing other autoimmune conditions, particularly thyroid disease, and certain cancers, such as non-Hodgkin lymphoma [58].
Moreover, a review by Caproni et al. summarized the immunopathogenesis of DH, emphasizing the role of IgA deposits in the skin and the cross-reactivity between epidermal transglutaminase (the autoantigen in DH) and tissue transglutaminase (the autoantigen in celiac disease) [59]. This understanding has informed the diagnostic approaches, with skin biopsies for direct immunofluorescence being the gold standard for diagnosing DH, and serological tests for IgA antibodies used to support the diagnosis of celiac disease [59].
Celiac disease and DH are nonetheless diseases that can cause many serious health problems if not diagnosed early. Following a lifetime avoidance of gluten is currently the only solution to diseases.
Food protein-induced enteropathy (FPE)
Food protein-induced enteropathy (FPE) is a chronic, non-IgE-mediated gastrointestinal disorder primarily affecting infants, characterized by persistent diarrhea, malabsorption, and failure to thrive due to intolerance to specific dietary proteins, particularly cow’s milk and soy [60]. Comparative studies on FPE and related conditions, such as food protein-induced enterocolitis syndrome (FPIES), have highlighted distinct differences in clinical presentation and progression [60]. Jenkins et al. established cow’s milk as a predominant trigger in FPE, with symptoms typically emerging in the first few months of life [61]. The review of 462 patients with FPE provided insights into the variable prognosis, where some children outgrow the condition, while others continue to experience symptoms into later childhood [6]. Caubet et al. further underscored the challenge of managing FPE in cases of multiple food sensitivities, stressing the need for personalized dietary interventions [62]. Moreover, Fernandes et al. explored the potential for FPE to persist into adulthood, which remains a growing area of interest [63]. These studies suggest that while FPE shares certain clinical characteristics with other non-IgE-mediated disorders, its management requires a more nuanced approach, particularly in children with complex dietary protein intolerances. The evolving body of research advocates continuous monitoring and reevaluation of dietary strategies as children age, ensuring both symptom control and optimal growth and development.
Heiner syndrome (pulmonary hemosiderosis)
Cow milk has been identified as the primary trigger in Heiner syndrome (pulmonary hemosiderosis), a non-IgE-mediated allergy characterized by pulmonary diseases in young infants [64]. This condition is considered rare and often requires time for diagnosis [65]. It typically presents gastrointestinal symptoms, poor growth, anemia, pulmonary hemosiderosis (PH), and symptoms resembling pulmonary infections, which resolve after removing cow milk from the diet [28]. Diagnosis involves clinical evaluation, laboratory tests (cow milk IgE and IgG antibodies), and radiography [66].
Overall, while Heiner syndrome is still relatively under-researched, the available studies underscore the importance of awareness and early intervention to prevent long-term complications in affected children.
Food protein-induced enterocolitis syndrome (FPIES)
Food protein-induced enterocolitis syndrome (FPIES) represents another form of non-IgE-mediated food allergy, characterized by severe delayed gastrointestinal symptoms typically occurring within the first year of life. Symptoms include repeated vomiting, hypotension, blood in the stool, and diarrhea following ingestion of the offending food [67]. Diagnosis of FPIES relies primarily on clinical symptoms, elimination diets, oral food challenges, and assessment of symptom progression in patients [68]. Cow milk is the most common trigger food for this syndrome [3]. According to Katz et al., 0.34% is the current prevalence of the disease in pediatric patients up to 3 years of age with 90% of patients recovering at the age of 3, with the disease being diagnosed in the majority of patients in the 6 first months of life [66].
In Australia, it is estimated that up to 90 patients suffering of FPIES visit allergy clinic for their condition with an estimation of 1 in 10000 Australian infants less than 2 years of age having the disease [69].
A recent study by Ruffner et al. delved into the immune mechanisms underlying FPIES, proposing that T-cell responses may play a pivotal role in its pathogenesis, contrasting the traditional focus on innate immune responses [6]. These studies emphasize the need for tailored approaches in managing FPIES, including individualized elimination diets and careful food reintroduction protocols. Furthermore, the variability in triggers and the immune mechanisms involved suggest that a one-size-fits-all approach may not be adequate.
3.2. Food Intolerances
Food intolerances, another facet of food hypersensitivity, refer to non-immunological reactions triggered by a food or food component typically tolerated in certain doses [70]. It is estimated that up to 20% of the global population experiences food intolerance [33]. However, diagnosing this condition often requires understanding various clinical presentations, including the intensity and timing of symptom onset. Complicating matters further are the diverse modes of action of food intolerance, which may include pharmacological effects (such as with coffee), enzyme deficiencies (like lactose malabsorption), and nonspecific gastrointestinal functioning [33]. Lactose, gluten/wheat, histamine-rich foods, and FODMAPs are among the most commonly implicated triggers for food intolerances [4]. Gastrointestinal symptoms like bloating, gas, diarrhea, abdominal pain, or nausea are typical presentations of food intolerance, with life-threatening reactions being rare [7].
3.2.1. Lactose Intolerance
Lactose intolerance (LI) occurs when individuals with lactose malabsorption (LM) experience symptoms like diarrhea, bloating, nausea, and abdominal pain after consuming lactose-containing foods [71]. It is estimated to affect between 57 to 65 percent of the global population [72]. Lactose, a disaccharide sugar found in most dairy products, is broken down into glucose and galactose by the enzyme lactase [4]. LM is a prerequisite for LI and can stem from various causes, including primary lactase deficiency (a gradual decline in lactase levels as individuals age) [73], secondary lactase deficiency (resulting from intestinal epithelium injury due to conditions like AIDS, chemotherapy, or gastrointestinal infections, which is reversible upon treatment of the underlying cause) [74], congenital lactase deficiency (a rare pediatric genetic disorder characterized by severe symptoms and failure to thrive) [75], and developmental lactase deficiency (occurring in premature infants with immature gastrointestinal systems) [4]. Diagnosis of LM typically relies on non-invasive methods like hydrogen breath tests [76], although other approaches such as genetic testing and enzymatic assays exist, with enzymatic assay measurements in bowel biopsies considered the gold standard [41,47,48]. Treatment options for LM include avoiding lactose-containing foods, using oral lactase enzyme replacements, and incorporating probiotics like Lactobacillus spp., Bifidobacterium longum, or Bifidobacterium into the diet. These probiotics have been demonstrated to stimulate the production of lactase when consumed [4].
A pivotal study by Swallow identified genetic polymorphisms associated with lactase persistence in populations of European descent, shedding light on the evolutionary aspects of lactose tolerance [79]. The study demonstrated that the ability to digest lactose into adulthood is primarily due to genetic mutations that allowed for the persistence of lactase production beyond infancy [79]. This genetic advantage likely provided a nutritional benefit in pastoral societies, where dairy was a major food source [79].
Further exploring dietary management, a study by Shaukat et al. systematically reviewed the efficacy of different interventions for lactose intolerance [80]. The review found that while lactase enzyme supplements can help reduce symptoms, many individuals benefit from gradually introducing small amounts of dairy into their diet to build tolerance [80]. This approach, known as lactose adaptation, takes advantage of the fact that some individuals with lactose intolerance can tolerate up to 12 grams of lactose (the amount in one cup of milk) without significant symptoms [80].
The variation in symptoms and tolerance levels underscores the need for individualized dietary recommendations based on genetic background and symptom severity.
3.2.2. Non-Coeliac Gluten/Wheat Sensitivity (NCGWS)
Non-coeliac gluten/Wheat Sensitivity (NCGWS) refers to individuals sensitive to gluten or wheat but lacking immune serological coeliac antibodies or allergic biomarkers, with a higher prevalence observed among females [81]. The Salerno Experts’ Criteria, relying on exclusion diagnosis, is currently the only reliable diagnostic tool for NCGWS [82]. Manifestations of NCGWS include both intestinal (bloating, diarrhea, constipation, nausea, etc.) and non-intestinal/extraintestinal symptoms (headache, anxiety, weight loss, anemia) [83]. NCGWS shares some similarities and differences with wheat allergy and celiac disease, as summarized in Table 3 [81]. However, the exact mechanism underlying NCGWS remains poorly understood, leading some individuals to be prescribed a gluten-free diet by healthcare practitioners despite negative results on other tests for gluten-containing foods [82].
Several studies have aimed to define the characteristics, prevalence, and management of NCGWS, often highlighting the complexity and controversies surrounding its diagnosis. A 2015 study by Catassi et al. reviewed the diagnostic criteria and noted that while NCGWS shares symptoms with celiac disease, such as bloating, diarrhea, and fatigue, it lacks the serological markers and histological changes seen in celiac disease [82]. The study also highlighted the placebo effect in gluten challenge trials, which complicates the diagnosis further, suggesting that some cases of NCGWS might be due to non-gluten components like FODMAPs [82].
In contrast, a 2016 study by Uhde et al. explored the immunological response in NCGWS patients and found evidence of systemic immune activation in response to gluten, without the intestinal damage typical of celiac disease [84]. This study suggested that NCGWS might involve an innate immune response rather than the adaptive immune response seen in celiac disease [84]. However, the study also acknowledged the heterogeneity of the condition, indicating that different patients might react to different components of wheat, including gluten or other proteins [84].
Further research by Skodje et al. compared the effects of gluten, FODMAPs, and placebo in NCGWS patients and concluded that many individuals who believed they were sensitive to gluten were reacting to FODMAPs, which are poorly absorbed carbohydrates found in wheat and other foods [85]. This study emphasized the importance of a structured dietary approach to diagnose NCGWS, as misdiagnosis could lead to unnecessary dietary restrictions and nutritional deficiencies [85].
These studies highlight the complexities in diagnosing and managing NCGWS, emphasizing that while some individuals may indeed react to gluten, others might be sensitive to other components in wheat or even experience a placebo effect. The variability in immune responses and symptoms underscores the need for personalized approaches in both diagnosis and treatment.
Table 3.
Comparison of prevalence, pathogenic, and diagnostic features of gluten-related disorders.
| Celiac Disease | NCGWS | Wheat Allergy | |
|---|---|---|---|
| Prevalence | 0.5–1.7% | 0.6-10% | 0.5–9% in children |
| Pathogenesis | Autoimmune | Non-specific immune response | IgE mediated response |
| DQ2-DQ8 HLA haplotypes | Positive in 95% cases | Positive in 50% cases | Negative |
| Serological markers | IgA anti-EMA, IgA anti-tTG, IgG anti-DGP, IgA anti-gliadin | IgA/IgG anti-gliadin in 50% cases | specific IgE antibodies against wheat and gliadin |
| Duodenal biopsy * | Marsh I to IV with domination of Marsh III and IV | Marsh 0-II, but according to some experts Marsh III might also be in NCGS | Marsh 0-II |
| Duodenal villi atrophy | Present | Absent | Might be present or absent |
* Marsh classification (histological grading system used to evaluate and classify the degree of intestinal damage, particularly in the small intestine, in individuals with celiac disease or other gluten-sensitive enteropathies [86]).
Non-celiac gluten/wheat sensitivity (NCGWS), IgA anti-EMA (IgA antibodies against endomysium), IgA anti-tTG (IgA antibodies against transglutaminase), IgG anti-DGP (IgG antibodies against deamidated gliadin peptides).
3.2.3. Fructose Intolerance
Hereditary Fructose Intolerance
Hereditary Fructose Intolerance (HFI) is a rare autosomal hereditary disorder characterized by the inability to metabolize fructose directly or indirectly through sucrose or sorbitol, as noted by Singh & Sarma in 2022 [87]. Individuals with fructose intolerance may experience symptoms such as abdominal pain, diarrhea, nausea, and flatulence upon consuming fructose-rich foods like honey, fruits, or vegetables, [88]. The mutation of Aldolase B, the primary enzyme responsible for fructose metabolism in the liver, located on chromosome 9q22.3, is implicated in HFI [87]. Diagnostic criteria for HFI typically involve Benedicts test, glucose dipstick test in urine, and serum carbohydrate-deficient transferrin (CDT), complemented by clinical correlations and sometimes requiring liver biopsies to assess Aldolase B enzyme activity [89]. Treatment for HFI primarily revolves around adopting a diet low in fructose, sucrose, and sorbitol (FSS). In acute cases, patients may require admission to an intensive care unit for intravenous glucose administration to manage metabolic acidosis, and it's crucial for individuals with HFI to avoid medications and vaccines containing sucrose, such as the rotavirus oral vaccine [87].
A study by Ali et al. identified several mutations in the ALDOB gene responsible for HFI, including the common A149P mutation, which is prevalent in European populations [90]. This research provided insight into the genetic basis of HFI and established the importance of genetic testing for accurate diagnosis [90].
In a more recent study, Tolan reviewed the pathophysiology of HFI and discussed the clinical symptoms that arise due to the accumulation of toxic metabolites, such as fructose-1-phosphate, in the liver, kidneys, and intestines [91]. The study highlighted the importance of early diagnosis and strict dietary management to avoid severe complications like hypoglycemia, liver dysfunction, and failure to thrive in infants [91]. Tolan also discussed the role of genetic counseling for families with a history of HFI and the potential for prenatal diagnosis [91].
These studies underline the genetic complexity of HFI and the critical importance of early diagnosis and dietary management in preventing serious health issues. The advancements in genetic testing have greatly improved the accuracy of HFI diagnosis, enabling better patient outcomes.
Non-Hereditary Fructose Intolerance
Non-Hereditary Fructose Intolerance, or fructose malabsorption (FM), presents as a syndrome where the uptake of fructose in the small intestine is minimal in some individuals, leading to fermentation of unabsorbed fructose in the colon, akin to lactose intolerance and HFI, according [92]. Diagnosis of FM typically involves a specifically designed hydrogen breath test [93]. Treatment options primarily involve the elimination of fructose-containing foods from the diet, with xylose isomerase proposed as an oral treatment to convert fructose to glucose, resulting in a favorable hydrogen breath test in FM patients [94].
A study by Gibson et al. investigated the role of the low FODMAP diet in managing fructose malabsorption [95]. This study highlighted that fructose, along with other fermentable carbohydrates, contribute to symptoms like bloating and diarrhea in susceptible individuals [95]. The low FODMAP diet was shown to be effective in reducing these symptoms, indicating that dietary management is a critical component of treatment for non-hereditary fructose intolerance [95].
Further research by Tuck et al. focused on the diagnostic challenges associated with fructose malabsorption [96]. The study noted that breath hydrogen testing is commonly used to diagnose this condition, but the results can be inconsistent due to variations in individual gut microbiota and other factors [96]. Tuck et al. advocated for a more comprehensive approach to diagnosis, combining dietary history with symptom tracking and possibly genetic testing, although the latter is more relevant to distinguishing between HFI and fructose malabsorption [96].
These studies suggest that non-hereditary fructose intolerance is a complex and multifaceted condition that requires careful dietary management and accurate diagnosis. Unlike HFI, which is caused by a genetic mutation, fructose malabsorption often arises from dietary factors and gut microbiota composition, making individualized treatment plans essential.
3.2.4. Saccharose Intolerance
Saccharose intolerance arises from deficiencies in sucrase-isomaltase enzyme function, caused by congenital sucrase-isomaltase deficiency (CSID) or secondary factors such as celiac disease or Crohn’s disease [94]. Symptoms typically involve gastrointestinal issues such as cramps, bloating, gas, and diarrhea [97]. Diagnosis of saccharose intolerance often involves duodenal endoscopic biopsies or breath tests (hydrogen, C-sucrose) [58]. Treatment may include using sacrosidase enzyme supplementation, which has shown promising results in alleviating symptoms [58].
A 2020 study by Treem et al., published in Journal of Pediatric Gastroenterology and Nutrition, highlighted the various genetic mutations affecting the SI gene and discussed enzyme replacement therapies like sacrosidase as an effective treatment [98]. The study also pointed out the importance of dietary modifications, emphasizing low-sucrose and low-starch diets to manage the symptoms effectively [95]. Furthermore, a study by Robayo-Torres et al. highlighted the importance of genetic screening and enzyme activity testing in diagnosing CSID, emphasizing that many cases remain undiagnosed due to the overlap of symptoms with other gastrointestinal disorders like irritable bowel syndrome (IBS) [99]. This study also pointed to enzyme replacement therapy, particularly with sacrosidase, as an effective treatment option for managing symptoms, alongside dietary modifications that limit sucrose and starch intake [96].
3.2.5. Histamine Intolerance
Histamine Intolerance (HIT) refers to a non-immunological condition believed to result from elevated histamine levels in the blood due to the ingestion of histamine-rich foods, potentially causing adverse effects [100]. Histamine intoxication, on the other hand, occurs following the ingestion of histamine-rich foods, with symptoms ranging from gastrointestinal symptoms to skin reactions, low blood pressure, headaches, and palpitations [101]. Suspected causes of histamine intolerance include a lack of oxidative degradation by diamine oxidase (DAO) activity or reduced levels of methylation by histamine N-methyltransferase (HNMT) [102]. Common symptoms of HIT predominantly affect the gastrointestinal tract, with constipation, diarrhea, abdominal pain, and postprandial fullness being most prevalent [103]. Treatment for HIT typically involves adhering to a low-histamine diet, with antihistamines used to alleviate symptoms [104]. Mast cell stabilizers may also be utilized, although further research is needed to determine their efficacy in HIT [105]. Oral supplementation with exogenous DAO has shown promise in reducing symptoms, but additional studies with larger sample sizes are required to ascertain its effectiveness in HIT patients [106].
Histamine intolerance (HI) is an emerging area of research with various studies examining its prevalence, pathophysiology, and management strategies, that explored the physiological mechanisms of histamine metabolism and its relation to HIT [107]. They emphasize that histamine intolerance results from an imbalance between histamine release and its degradation due to enzyme deficiencies, particularly diamine oxidase (DAO). Another significant contribution is by Schink, et al., who provide insights into diagnostic approaches and clinical management of HIT [9]. They suggested that HIT can be managed through dietary modifications and the use of DAO supplements. These studies underscore the multifaceted nature of HIT and highlight the importance of a comprehensive approach in both diagnosis and management [9].
3.2.6. FODMAP
FODMAPs, or Fermentable Oligo-, Di-, Mono-Saccharides, and Polyols, are short-chain carbohydrates found abundantly in fruits, vegetables, dairy, cereals, and sweeteners [95]. Lactose, fructose, sorbitol, mannitol, fructans, stachyose, and raffinose are all classified as FODMAPs [108]. Consumption of more than 4g of lactose, more than 0.3g of mannitol, sorbitol, galacto-oligosaccharides, or fructans is considered a high FODMAP diet [109]. FODMAPs are poorly digested by intestinal bacteria, leading to the production of short-chain fatty acids (SCFAs) and gas, which can cause symptoms such as abdominal pain, flatulence, diarrhea, and indigestion in susceptible individuals, particularly those with Irritable Bowel Syndrome (IBS) [110]. A low FODMAP diet (LFD) has been shown to effectively reduce symptoms and improve the quality of life in IBS patients [109]. The LFD typically follows a three-phase approach [10]. Phase 1 involves eliminating all FODMAPs from the diet for 4 to 6 weeks. Phase 2 assesses each patient's tolerance to FODMAP subgroups by reintroducing one food at a time over three days. Phase 3, building upon the findings of Phase 2, customizes a long-term FODMAP diet tailored to each patient's tolerance [111]. However, concerns have been raised regarding potential nutritional deficiencies, constipation, eating disorders, and alterations in gut microbiota among individuals on a long-term LFD [111,112,113].
One seminal paper by Gibson et al. in Gastroenterology introduced the low FODMAP diet and demonstrated its effectiveness in reducing IBS symptoms through a controlled trial [95]. Their research provided the foundation for subsequent studies exploring dietary interventions [95]. Another comprehensive review by Halmos et al. supports the low FODMAP diet, showing that it significantly alleviates IBS symptoms compared to a standard diet [10]. This study is crucial for understanding the clinical application of the diet [10]. Additionally, a more recent study by Staudacher et al. confirms the diet's effectiveness across various populations, emphasizing its role in symptom management [115]. These studies emphasize the low FODMAP diet's role in managing IBS and other functional gastrointestinal disorders, providing robust evidence for its clinical use.
3.3. Irritable Bowel Syndrome IBS
Irritable bowel syndrome (IBS) affects approximately 20% of the global population [116]. Its primary symptoms include abdominal pain, bloating, and irregularities in stool form and frequency [117]. Currently, there are no globally recognized biomarkers for diagnosing IBS; instead, diagnostic criteria based on symptoms have been established by the scientific community, known as the Rome IV criteria [118].
Patients are categorized into subtypes based on the Bristol stool form: IBS with constipation (IBS-C), IBS with diarrhea (IBS-D), IBS with mixed stool pattern (IBS-M), and IBS unclassified (IBS-U) [80,81]. IBS is a complex syndrome influenced by multiple factors and often overlaps with various comorbidities, even among its own subtypes [119].
Common gastrointestinal disorders that overlap with IBS include gastroesophageal reflux (GERD), nausea, constipation, diarrhea, heartburn, dyspepsia, and incontinence [83,84]. Non-gastrointestinal syndromes also frequently overlap with IBS [80,81]. These include psychiatric conditions such as depression, anxiety, and somatization, as well as premenstrual syndrome (PMS), overactive bladder, fibromyalgia, eating disorders, and food hypersensitivities (intolerances and allergies) [122].
This overlap has prompted discussion within the scientific community about whether IBS should be considered part of these syndromes rather than as a distinct syndrome on its own [122]. Additionally, IBS and its associated functional gastrointestinal and non-gastrointestinal disorders are now classified under the somatic symptom disorders in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5). This categorization reflects a historical trend where patients with gastrointestinal symptoms treated by psychiatrists often experienced inadequate treatment and care [123].
Numerous risk factors associated with the development of IBS have been identified, including personal factors such as being female and having a low body mass index (BMI) [124].
Psychological factors like anxiety, depression, and low quality of life also increase somatic issues such as diverticulosis, antibiotic use, gastrointestinal infections, and endometriosis, as well as social conditions like a family history of mental illness, childhood socioeconomic status, and marital status [124].
Moreover, many individuals diagnosed with IBS also report food allergies or intolerances, particularly to gluten, dairy (cow milk protein and lactose), and FODMAPs, which can trigger adverse reactions [53,88,89].
The pathophysiology of IBS involves various mechanisms. These include alterations in gut microbiota, changes in the epithelial barrier, immune system responses to food antigens, and bile acids, and interactions within the brain-gut axis, enteric nervous system, and hypothalamus-pituitary-adrenal axis, which are increasingly considered potential biomarkers of IBS [127].
Additionally, psychological factors such as depression, anxiety, and stress contribute to the pathophysiology of IBS by influencing intestinal motility [127].
As mentioned previously, the composition of gut microbiota in patients with IBS varies depending on the subtype of the condition, as detailed in Table [127]. Studies have demonstrated that culturing these microbiota types present in IBS patients, compared to those in individuals without IBS, can lead to lower intestinal motility, induce visceral hypersensitivity, and alter transit time. These findings on microbiota dysbiosis have been recognized by the ROME foundation as seen in Table 4 [127].
Microbiota in the intestine play a role in fermenting certain types of food, particularly in producing short-chain fatty acids (SCFAs) [128]. Elevated production of SCFAs has been associated with gastrointestinal symptoms in IBS [129]. Bacteria such as Roseburia, Blautia, and Veillonella, known for their abundant production of SCFAs, are found in higher numbers in individuals with IBS than in healthy individuals [92]. This increased microbial SCFA production has been linked to T-cell activation, resulting in chronic low-grade inflammation in the intestine and an imbalance between pro- and anti-inflammatory mechanisms in IBS patients [130].
Additionally, Dorea, a prominent gas-producing bacterium in the human gastrointestinal system [131], has been significantly elevated in patients with IBS [132], particularly in those with IBS-C, where its abundance has been associated with increased constipation due to delayed transit [133].
One pivotal study by Longstreth et al., provides a comprehensive review of IBS epidemiology, diagnostic criteria, and management options, emphasizing the heterogeneity of the disorder and the importance of a tailored treatment approach [134]. Another influential study by Ford et al. examines the efficacy of pharmacological treatments for IBS, including antispasmodics, laxatives, and antidiarrheals, and finds that while some medications are effective, their benefits vary among patients [8]. A more recent randomized controlled trial by Drossman et al. investigates the effectiveness of a novel treatment approach, such as a combination of dietary interventions and pharmacological agents, and showed significant improvement in IBS symptoms compared to traditional therapies [135]. Additionally, a meta-analysis by Lacy et al. provided an overview of the impact of the low FODMAP diet on IBS symptoms, confirming its efficacy in symptom relief and highlighting the need for personalized dietary strategies [136]. Lastly, a review by Quigley et al. explored the role of probiotics and prebiotics in managing IBS, revealing that while some evidence supports their use, more research is needed to establish their effectiveness conclusively [137]. Together, these studies underscored the complexity of IBS and the need for a multifaceted approach to its management.
4. Conclusion
Based on the current review, understanding the key differences between food allergies and intolerances is crucial for effective management and treatment strategies. While both conditions can lead to uncomfortable symptoms, they arise from distinct mechanisms within the body.
Food allergies involve an immune system response to specific proteins in food, often resulting in rapid and potentially life-threatening reactions. On the other hand, food intolerances stem from difficulty digesting certain foods or components, leading to gastrointestinal discomfort or other symptoms. These reactions are typically less severe and do not involve the immune system.
Recognizing the symptoms and triggers of each condition is essential for accurate diagnosis and appropriate management. Food allergies may require strict avoidance of triggering foods and the availability of emergency medication, such as epinephrine, in case of severe reactions. Meanwhile, managing food intolerances often involves identifying and eliminating problematic foods from the diet, as well as considering enzyme supplements or other supportive measures.
Overall, by understanding the nuances between food allergies and intolerances, individuals can take proactive steps to minimize their symptoms and maintain their overall health and well-being. Consulting with healthcare professionals and registered dietitians can provide personalized guidance and support in navigating these dietary challenges.
Author Contributions
G. H., as the principal investigator, developed the idea, performed the literature review, and wrote and edited the manuscript. G.H., Y.S., J.H., M.H, L.S., and N.S. contributed also to the literature review, wrote and edited the manuscript, and acted as lead reviewers. J. H. was responsible for reviewing and editing tables and the figures. All authors participated in the preparation of the manuscript and approved its final version.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gargano D, Appanna R, Santonicola A, De Bartolomeis F, Stellato C, Cianferoni A, Casolaro V, Iovino P. Food Allergy and Intolerance: A Narrative Review on Nutritional Concerns. Nutrients (2021) 13:1638. [CrossRef]
- Tedner SG, Asarnoj A, Thulin H, Westman M, Konradsen JR, Nilsson C. Food allergy and hypersensitivity reactions in children and adults—A review. Journal of Internal Medicine (2022) 291:283–302. [CrossRef]
- Connors L, O’Keefe A, Rosenfield L, Kim H. Non-IgE-mediated food hypersensitivity. Allergy, Asthma & Clinical Immunology (2018) 14:56. [CrossRef]
- Zingone F, Bertin L, Maniero D, Palo M, Lorenzon G, Barberio B, Ciacci C, Savarino EV. Myths and Facts about Food Intolerance: A Narrative Review. Nutrients (2023) 15:4969. [CrossRef]
- Vassilopoulou E, Feketea G, Konstantinou GN, Zekakos Xypolias D, Valianatou M, Petrodimopoulou M, Vourga V, Tasios I, Papadopoulos NG. Food Protein-Induced Allergic Proctocolitis: The Effect of Maternal Diet During Pregnancy and Breastfeeding in a Mediterranean Population. Front Nutr (2022) 9:. [CrossRef]
- Ruffner MA, Ruymann K, Barni S, Cianferoni A, Brown-Whitehorn T, Spergel JM. Food protein-induced enterocolitis syndrome: insights from review of a large referral population. J Allergy Clin Immunol Pract (2013) 1:343–349. [CrossRef]
- Pinto-Sanchez MI, Nardelli A, Borojevic R, De Palma G, Calo NC, McCarville J, Caminero A, Basra D, Mordhorst A, Ignatova E, et al. Gluten-Free Diet Reduces Symptoms, Particularly Diarrhea, in Patients With Irritable Bowel Syndrome and Antigliadin IgG. Clin Gastroenterol Hepatol (2021) 19:2343-2352.e8. [CrossRef]
- Ford AC, Bercik P, Morgan DG, Bolino C, Pintos-Sanchez MI, Moayyedi P. Characteristics of functional bowel disorder patients: a cross-sectional survey using the Rome III criteria. Aliment Pharmacol Ther (2014) 39:312–321. [CrossRef]
- Schink M, Konturek PC, Tietz E, Dieterich W, Pinzer TC, Wirtz S, Neurath MF, Zopf Y. Microbial patterns in patients with histamine intolerance. J Physiol Pharmacol (2018) 69:. [CrossRef]
- Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology (2014) 146:67-75.e5. [CrossRef]
- Nwaru BI, Hickstein L, Panesar SS, Muraro A, Werfel T, Cardona V, Dubois AEJ, Halken S, Hoffmann-Sommergruber K, Poulsen LK, et al. The epidemiology of food allergy in Europe: a systematic review and meta-analysis. Allergy (2014) 69:62–75. [CrossRef]
- West J, Fleming KM, Tata LJ, Card TR, Crooks CJ. Incidence and Prevalence of Celiac Disease and Dermatitis Herpetiformis in the UK Over Two Decades: Population-Based Study. Am J Gastroenterol (2014) 109:757–768. [CrossRef]
- Sicherer SH, Sampson HA. Food allergy: A review and update on epidemiology, pathogenesis, diagnosis, prevention, and management. Journal of Allergy and Clinical Immunology (2018) 141:41–58. [CrossRef]
- Waserman S, Bégin P, Watson W. IgE-mediated food allergy. Allergy, Asthma & Clinical Immunology (2018) 14:55. [CrossRef]
- Anvari S, Miller J, Yeh C-Y, Davis CM. IgE-Mediated Food Allergy. Clinic Rev Allerg Immunol (2019) 57:244–260. [CrossRef]
- Patel BY, Volcheck GW. Food Allergy: Common Causes, Diagnosis, and Treatment. Mayo Clinic Proceedings (2015) 90:1411–1419. [CrossRef]
- Sampson HA, Aceves S, Bock SA, James J, Jones S, Lang D, Nadeau K, Nowak-Wegrzyn A, Oppenheimer J, Perry TT, et al. Food allergy: a practice parameter update-2014. J Allergy Clin Immunol (2014) 134:1016-1025.e43. [CrossRef]
- Savage J, Sicherer S, Wood R. The Natural History of Food Allergy. J Allergy Clin Immunol Pract (2016) 4:196–203; quiz 204. [CrossRef]
- Heinzerling L, Mari A, Bergmann K-C, Bresciani M, Burbach G, Darsow U, Durham S, Fokkens W, Gjomarkaj M, Haahtela T, et al. The skin prick test – European standards. Clin Transl Allergy (2013) 3:3. [CrossRef]
- Heinzerling L, Mari A, Bergmann K-C, Bresciani M, Burbach G, Darsow U, Durham S, Fokkens W, Gjomarkaj M, Haahtela T, et al. The skin prick test – European standards. Clinical and Translational Allergy (2013) 3:3. [CrossRef]
- Bousquet J, Schünemann HJ, Samolinski B, Demoly P, Baena-Cagnani CE, Bachert C, Bonini S, Boulet LP, Bousquet PJ, Brozek JL, et al. Allergic Rhinitis and its Impact on Asthma (ARIA): achievements in 10 years and future needs. J Allergy Clin Immunol (2012) 130:1049–1062. [CrossRef]
- Ansotegui IJ, Melioli G, Canonica GW, Caraballo L, Villa E, Ebisawa M, Passalacqua G, Savi E, Ebo D, Gómez RM, et al. IgE allergy diagnostics and other relevant tests in allergy, a World Allergy Organization position paper. World Allergy Organ J (2020) 13:100080. [CrossRef]
- Wood RA, Kim JS, Lindblad R, Nadeau K, Henning AK, Dawson P, Plaut M, Sampson HA. A randomized, double-blind, placebo-controlled study of omalizumab combined with oral immunotherapy for the treatment of cow’s milk allergy. J Allergy Clin Immunol (2016) 137:1103-1110.e11. [CrossRef]
- Matricardi PM, Kleine-Tebbe J, Hoffmann HJ, Valenta R, Hilger C, Hofmaier S, Aalberse RC, Agache I, Asero R, Ballmer-Weber B, et al. EAACI Molecular Allergology User’s Guide. Pediatr Allergy Immunol (2016) 27 Suppl 23:1–250. [CrossRef]
- Zuberbier T, Aberer W, Asero R, Abdul Latiff AH, Baker D, Ballmer-Weber B, Bernstein JA, Bindslev-Jensen C, Brzoza Z, Buense Bedrikow R, et al. The EAACI/GA2LEN/EDF/WAO guideline for the definition, classification, diagnosis and management of urticaria. Allergy (2018) 73:1393–1414. [CrossRef]
- Ewan PW, Dugué P, Mirakian R, Dixon TA, Harper JN, Nasser SM. BSACI guidelines for the investigation of suspected anaphylaxis during general anaesthesia. Clinical & Experimental Allergy (2010) 40:15–31. [CrossRef]
- Gargano D, Appanna R, Santonicola A, De Bartolomeis F, Stellato C, Cianferoni A, Casolaro V, Iovino P. Food Allergy and Intolerance: A Narrative Review on Nutritional Concerns. Nutrients (2021) 13:1638. [CrossRef]
- Sicherer SH, Sampson HA. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol (2014) 133:291–307; quiz 308. [CrossRef]
- Gupta RS, Warren CM, Smith BM, Jiang J, Blumenstock JA, Davis MM, Schleimer RP, Nadeau KC. Prevalence and Severity of Food Allergies Among US Adults. JAMA Netw Open (2019) 2:e185630. [CrossRef]
- Osborne NJ, Koplin JJ, Martin PE, Gurrin LC, Thiele L, Tang ML, Ponsonby A-L, Dharmage SC, Allen KJ, HealthNuts Study Investigators. The HealthNuts population-based study of paediatric food allergy: validity, safety and acceptability. Clin Exp Allergy (2010) 40:1516–1522. [CrossRef]
- Muir A, Falk GW. Eosinophilic Esophagitis: A Review. JAMA (2021) 326:1310–1318. [CrossRef]
- Dellon ES, Jensen ET, Martin CF, Shaheen NJ, Kappelman MD. Prevalence of eosinophilic esophagitis in the United States. Clin Gastroenterol Hepatol (2014) 12:589-596.e1. [CrossRef]
- Liacouras CA, Furuta GT, Hirano I, Atkins D, Attwood SE, Bonis PA, Burks AW, Chehade M, Collins MH, Dellon ES, et al. Eosinophilic esophagitis: Updated consensus recommendations for children and adults. Journal of Allergy and Clinical Immunology (2011) 128:3-20.e6. [CrossRef]
- Hirano I, Pandolfino JE, Boeckxstaens GE. Functional Lumen Imaging Probe for the Management of Esophageal Disorders: Expert Review From the Clinical Practice Updates Committee of the AGA Institute. Clin Gastroenterol Hepatol (2017) 15:325–334. [CrossRef]
- Lucendo AJ, Arias Á, Molina-Infante J. Efficacy of Proton Pump Inhibitor Drugs for Inducing Clinical and Histologic Remission in Patients With Symptomatic Esophageal Eosinophilia: A Systematic Review and Meta-Analysis. Clin Gastroenterol Hepatol (2016) 14:13-22.e1. [CrossRef]
- Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA, Plaut M, Cooper SF, Fenton MJ, Arshad SH, et al. Guidelines for the Diagnosis and Management of Food Allergy in the United States: Summary of the NIAID-Sponsored Expert Panel Report. Journal of Allergy and Clinical Immunology (2010) 126:1105–1118. [CrossRef]
- Barni S, Mori F, Giovannini M, Liotti L, Mastrorilli C, Pecoraro L, Saretta F, Castagnoli R, Arasi S, Caminiti L, et al. Allergic Proctocolitis: Literature Review and Proposal of a Diagnostic–Therapeutic Algorithm. Life (Basel) (2023) 13:1824. [CrossRef]
- Zubeldia-Varela E, Barker-Tejeda TC, Blanco-Pérez F, Infante S, Zubeldia JM, Pérez-Gordo M. Non-IgE-Mediated Gastrointestinal Food Protein-Induced Allergic Disorders. Clinical Perspectives and Analytical Approaches. Foods (2021) 10:. [CrossRef]
- Martin VM, Virkud YV, Seay H, Hickey A, Ndahayo R, Rosow R, Southwick C, Elkort M, Gupta B, Kramer E, et al. PROSPECTIVE ASSESSMENT OF PEDIATRICIAN-DIAGNOSED FOOD-PROTEIN INDUCED ALLERGIC PROCTOCOLITIS BY GROSS OR OCCULT BLOOD. J Allergy Clin Immunol Pract (2020) 8:1692-1699.e1. [CrossRef]
- Elizur A, Cohen M, Goldberg MR, Rajuan N, Cohen A, Leshno M, Katz Y. Cow’s milk associated rectal bleeding: a population based prospective study. Pediatr Allergy Immunol (2012) 23:766–770. [CrossRef]
- Mennini M, Fiocchi AG, Cafarotti A, Montesano M, Mauro A, Villa MP, Di Nardo G. Food protein-induced allergic proctocolitis in infants: Literature review and proposal of a management protocol. World Allergy Organ J (2020) 13:100471. [CrossRef]
- Nowak-Wegrzyn A, Warren CM, Brown-Whitehorn T, Cianferoni A, Schultz-Matney F, Gupta RS. Food protein-induced enterocolitis syndrome in the US population-based study. J Allergy Clin Immunol (2019) 144:1128–1130. [CrossRef]
- Caubet J-C, Szajewska H, Shamir R, Nowak-Węgrzyn A. Non-IgE-mediated gastrointestinal food allergies in children. Pediatr Allergy Immunol (2017) 28:6–17. doi: le.
- Lebwohl B, Rubio-Tapia A. Epidemiology, Presentation, and Diagnosis of Celiac Disease. Gastroenterology (2021) 160:63–75. [CrossRef]
- Al-Toma A, Volta U, Auricchio R, Castillejo G, Sanders DS, Cellier C, Mulder CJ, Lundin KEA. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United European Gastroenterol J (2019) 7:583–613. [CrossRef]
- Alkalay MJ. Nutrition in Patients with Lactose Malabsorption, Celiac Disease, and Related Disorders. Nutrients (2021) 14:2. [CrossRef]
- Hadithi M, von Blomberg BME, Crusius JBA, Bloemena E, Kostense PJ, Meijer JWR, Mulder CJJ, Stehouwer CDA, Peña AS. Accuracy of Serologic Tests and HLA-DQ Typing for Diagnosing Celiac Disease. Ann Intern Med (2007) 147:294–302. [CrossRef]
- Singh P, Arora A, Strand TA, Leffler DA, Catassi C, Green PH, Kelly CP, Ahuja V, Makharia GK. Global Prevalence of Celiac Disease: Systematic Review and Meta-analysis. Clinical Gastroenterology and Hepatology (2018) 16:823-836.e2. [CrossRef]
- Lebwohl B, Rubio-Tapia A. Epidemiology, Presentation, and Diagnosis of Celiac Disease. Gastroenterology (2021) 160:63–75. [CrossRef]
- Ludvigsson JF, Murray JA. Epidemiology of Celiac Disease. Gastroenterol Clin North Am (2019) 48:1–18. [CrossRef]
- Rubio-Tapia A, Hill ID, Semrad C, Kelly CP, Greer KB, Limketkai BN, Lebwohl B. American College of Gastroenterology Guidelines Update: Diagnosis and Management of Celiac Disease. Official journal of the American College of Gastroenterology | ACG (2023) 118:59. [CrossRef]
- SALMI T, HERVONEN K. Current Concepts of Dermatitis Herpetiformis. Acta Derm Venereol (2020) 100:5664. [CrossRef]
- Collin P, Salmi TT, Hervonen K, Kaukinen K, Reunala T. Dermatitis herpetiformis: a cutaneous manifestation of coeliac disease. Annals of Medicine (2017) 49:23–31. [CrossRef]
- Nguyen CN, Kim S-J. Dermatitis Herpetiformis: An Update on Diagnosis, Disease Monitoring, and Management. Medicina (Kaunas) (2021) 57:843. [CrossRef]
- Antiga E, Maglie R, Quintarelli L, Verdelli A, Bonciani D, Bonciolini V, Caproni M. Dermatitis Herpetiformis: Novel Perspectives. Front Immunol (2019) 10:1290. [CrossRef]
- Reunala T, Hervonen K, Salmi T. Dermatitis Herpetiformis: An Update on Diagnosis and Management. Am J Clin Dermatol (2021) 22:329–338. [CrossRef]
- Mansikka E, Hervonen K, Kaukinen K, Collin P, Huhtala H, Reunala T, Salmi T. Prognosis of Dermatitis Herpetiformis Patients with and without Villous Atrophy at Diagnosis. Nutrients (2018) 10:641. [CrossRef]
- Collin P, Salmi TT, Hervonen K, Kaukinen K, Reunala T. Dermatitis herpetiformis: a cutaneous manifestation of coeliac disease. Ann Med (2017) 49:23–31. [CrossRef]
- Caproni M, Antiga E, Melani L, Fabbri P, Italian Group for Cutaneous Immunopathology. Guidelines for the diagnosis and treatment of dermatitis herpetiformis. J Eur Acad Dermatol Venereol (2009) 23:633–638. [CrossRef]
- Feuille E, Nowak-Węgrzyn A. Food Protein-Induced Enterocolitis Syndrome, Allergic Proctocolitis, and Enteropathy. Curr Allergy Asthma Rep (2015) 15:50. [CrossRef]
- Jenkins HR, Pincott JR, Soothill JF, Milla PJ, Harries JT. Food allergy: the major cause of infantile colitis. Arch Dis Child (1984) 59:326–329.
- Caubet JC, Ford LS, Sickles L, Järvinen KM, Sicherer SH, Sampson HA, Nowak-Węgrzyn A. Clinical features and resolution of food protein-induced enterocolitis syndrome: 10-year experience. J Allergy Clin Immunol (2014) 134:382–389. [CrossRef]
- Fernandes BN, Boyle RJ, Gore C, Simpson A, Custovic A. Food protein-induced enterocolitis syndrome can occur in adults. J Allergy Clin Immunol (2012) 130:1199–1200. [CrossRef]
- Koc AS, Sucu A, Celik U. A different clinical presentation of Heiner syndrome: The case of diffuse alveolar hemorrhage causing massive hemoptysis and hematemesis. Respir Med Case Rep (2019) 26:206–208. [CrossRef]
- Arasi S, Mastrorilli C, Pecoraro L, Giovannini M, Mori F, Barni S, Caminiti L, Castagnoli R, Liotti L, Saretta F, et al. Heiner Syndrome and Milk Hypersensitivity: An Updated Overview on the Current Evidence. Nutrients (2021) 13:1710. [CrossRef]
- Lee JY, Park M, Jung JH, Kim SY, Kim YH, Hahn SM, Kim S, Lee M-J, Shim HS, Sohn MH, et al. Children with Heiner Syndrome: A Single-Center Experience. Children (Basel) (2021) 8:1110. [CrossRef]
- Calvani M, Anania C, Bianchi A, D’Auria E, Cardinale F, Votto M, Martelli A, Tosca M, Chiappini E, Brambilla I, et al. Update on Food protein-induced enterocolitis syndrome (FPIES). Acta Biomed (2021) 92:e2021518. [CrossRef]
- Nowak-Węgrzyn A, Chehade M, Groetch ME, Spergel JM, Wood RA, Allen K, Atkins D, Bahna S, Barad AV, Berin C, et al. International consensus guidelines for the diagnosis and management of food protein–induced enterocolitis syndrome: Executive summary—Workgroup Report of the Adverse Reactions to Foods Committee, American Academy of Allergy, Asthma & Immunology. Journal of Allergy and Clinical Immunology (2017) 139:1111-1126.e4. [CrossRef]
- Mehr S, Frith K, Campbell DE. Epidemiology of food protein-induced enterocolitis syndrome. Curr Opin Allergy Clin Immunol (2014) 14:208–216. [CrossRef]
- Tuck CJ, Biesiekierski JR, Schmid-Grendelmeier P, Pohl D. Food Intolerances. Nutrients (2019) 11:1684. [CrossRef]
- Misselwitz B, Butter M, Verbeke K, Fox MR. Update on lactose malabsorption and intolerance: pathogenesis, diagnosis and clinical management. Gut (2019) 68:2080–2091. [CrossRef]
- Catanzaro R, Sciuto M, Marotta F. Lactose intolerance: An update on its pathogenesis, diagnosis, and treatment. Nutrition Research (2021) 89:23–34. [CrossRef]
- Bayless TM, Brown E, Paige DM. Lactase Non-persistence and Lactose Intolerance. Curr Gastroenterol Rep (2017) 19:23. [CrossRef]
- Deng Y, Misselwitz B, Dai N, Fox M. Lactose Intolerance in Adults: Biological Mechanism and Dietary Management. Nutrients (2015) 7:8020–8035. [CrossRef]
- Enattah NS, Sahi T, Savilahti E, Terwilliger JD, Peltonen L, Järvelä I. Identification of a variant associated with adult-type hypolactasia. Nat Genet (2002) 30:233–237. [CrossRef]
- Simrén M, Stotzer P. Use and abuse of hydrogen breath tests. Gut (2006) 55:297–303. [CrossRef]
- Simrén M, Barbara G, Flint HJ, Spiegel BMR, Spiller RC, Vanner S, Verdu EF, Whorwell PJ, Zoetendal EG. Intestinal microbiota in functional bowel disorders: a Rome foundation report. Gut (2013) 62:159–176. [CrossRef]
- Jo IH, Paik C-N, Kim Y-J, Lee JM, Choi SY, Hong KP. Lactase Deficiency Diagnosed by Endoscopic Biopsy-based Method is Associated With Positivity to Glucose Breath Test. J Neurogastroenterol Motil (2023) 29:85–93. [CrossRef]
- Swallow DM. Genetics of lactase persistence and lactose intolerance. Annu Rev Genet (2003) 37:197–219. [CrossRef]
- Shaukat A, Levitt MD, Taylor BC, MacDonald R, Shamliyan TA, Kane RL, Wilt TJ. Systematic review: effective management strategies for lactose intolerance. Ann Intern Med (2010) 152:797–803. [CrossRef]
- Roszkowska A, Pawlicka M, Mroczek A, Bałabuszek K, Nieradko-Iwanicka B. Non-Celiac Gluten Sensitivity: A Review. Medicina (Kaunas) (2019) 55:222. [CrossRef]
- Catassi C, Elli L, Bonaz B, Bouma G, Carroccio A, Castillejo G, Cellier C, Cristofori F, de Magistris L, Dolinsek J, et al. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria. Nutrients (2015) 7:4966–4977. [CrossRef]
- Carroccio A, Mansueto P, Iacono G, Soresi M, D’Alcamo A, Cavataio F, Brusca I, Florena AM, Ambrosiano G, Seidita A, et al. Non-Celiac Wheat Sensitivity Diagnosed by Double-Blind Placebo-Controlled Challenge: Exploring a New Clinical Entity. Official journal of the American College of Gastroenterology | ACG (2012) 107:1898. [CrossRef]
- Uhde M, Ajamian M, Caio G, De Giorgio R, Indart A, Green PH, Verna EC, Volta U, Alaedini A. Intestinal cell damage and systemic immune activation in individuals reporting sensitivity to wheat in the absence of coeliac disease. Gut (2016) 65:1930–1937. [CrossRef]
- Skodje GI, Sarna VK, Minelle IH, Rolfsen KL, Muir JG, Gibson PR, Veierød MB, Henriksen C, Lundin KEA. Fructan, Rather Than Gluten, Induces Symptoms in Patients With Self-Reported Non-Celiac Gluten Sensitivity. Gastroenterology (2018) 154:529-539.e2. [CrossRef]
- Ensari A, Marsh MN. Diagnosing celiac disease: A critical overview. Turk J Gastroenterol (2019) 30:389–397. [CrossRef]
- Singh SK, Sarma MS. Hereditary fructose intolerance: A comprehensive review. World J Clin Pediatr (2022) 11:321–329. [CrossRef]
- Debray F-G, Seyssel K, Fadeur M, Tappy L, Paquot N, Tran C. Effect of a high fructose diet on metabolic parameters in carriers for hereditary fructose intolerance. Clinical Nutrition (2021) 40:4246–4254. [CrossRef]
- Adamowicz M, Płoski R, Rokicki D, Morava E, Giżewska M, Mierzewska H, Pollak A, Lefeber DJ, Wevers RA, Pronicka E. Transferrin hypoglycosylation in hereditary fructose intolerance: Using the clues and avoiding the pitfalls. Journal of Inherited Metabolic Disease (2007) 30:407. [CrossRef]
- Ali M, Rellos P, Cox TM. Hereditary fructose intolerance. J Med Genet (1998) 35:353–365. [CrossRef]
- Tolan DR, Brooks CC. Molecular analysis of common aldolase B alleles for hereditary fructose intolerance in North Americans. Biochem Med Metab Biol (1992) 48:19–25. [CrossRef]
- Ebert K, Witt H. Fructose malabsorption. Mol Cell Pediatr (2016) 3:10. [CrossRef]
- Hammer HF, Fox MR, Keller J, Salvatore S, Basilisco G, Hammer J, Lopetuso L, Benninga M, Borrelli O, Dumitrascu D, et al. European guideline on indications, performance, and clinical impact of hydrogen and methane breath tests in adult and pediatric patients: European Association for Gastroenterology, Endoscopy and Nutrition, European Society of Neurogastroenterology and Motility, and European Society for Paediatric Gastroenterology Hepatology and Nutrition consensus. United European Gastroenterol J (2021) 10:15–40. [CrossRef]
- Komericki P, Akkilic-Materna M, Strimitzer T, Weyermair K, Hammer HF, Aberer W. Oral xylose isomerase decreases breath hydrogen excretion and improves gastrointestinal symptoms in fructose malabsorption – a double-blind, placebo-controlled study. Alimentary Pharmacology & Therapeutics (2012) 36:980–987. [CrossRef]
- Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. Journal of Gastroenterology and Hepatology (2010) 25:252–258. [CrossRef]
- Tuck CJ, Biesiekierski JR, Schmid-Grendelmeier P, Pohl D. Food Intolerances. Nutrients (2019) 11:1684. [CrossRef]
- Frissora CL, Rao SSC. Sucrose intolerance in adults with common functional gastrointestinal symptoms. Proc (Bayl Univ Med Cent) (2022) 35:790–793. [CrossRef]
- Treem WR, McAdams L, Stanford L, Kastoff G, Justinich C, Hyams J. Sacrosidase therapy for congenital sucrase-isomaltase deficiency. J Pediatr Gastroenterol Nutr (1999) 28:137–142. [CrossRef]
- Robayo-Torres CC, Opekun AR, Quezada-Calvillo R, Villa X, Smith EO, Navarrete M, Baker SS, Nichols BL. 13C-breath tests for sucrose digestion in congenital sucrase isomaltase-deficient and sacrosidase-supplemented patients. J Pediatr Gastroenterol Nutr (2009) 48:412–418. [CrossRef]
- Latorre-Moratalla ML, Comas-Basté O, Bover-Cid S, Vidal-Carou MC. Tyramine and histamine risk assessment related to consumption of dry fermented sausages by the Spanish population. Food and Chemical Toxicology (2017) 99:78–85. [CrossRef]
- Comas-Basté O, Sánchez-Pérez S, Veciana-Nogués MT, Latorre-Moratalla M, Vidal-Carou M del C. Histamine Intolerance: The Current State of the Art. Biomolecules (2020) 10:1181. [CrossRef]
- Schwelberger HG, Feurle J, Houen G. Mapping of the binding sites of human diamine oxidase (DAO) monoclonal antibodies. Inflamm Res (2018) 67:245–253. [CrossRef]
- Schnedl WJ, Lackner S, Enko D, Schenk M, Holasek SJ, Mangge H. Evaluation of symptoms and symptom combinations in histamine intolerance. Intest Res (2019) 17:427–433. [CrossRef]
- Reese I, Ballmer-Weber B, Beyer K, Dölle-Bierke S, Kleine-Tebbe J, Klimek L, Lämmel S, Lepp U, Saloga J, Schäfer C, et al. Guideline on management of suspected adverse reactions to ingested histamine: Guideline of the German Society for Allergology and Clinical Immunology (DGAKI), the Society for Pediatric Allergology and Environmental Medicine (GPA), the Medical Association of German Allergologists (AeDA) as well as the Swiss Society for Allergology and Immunology (SGAI) and the Austrian Society for Allergology and Immunology (ÖGAI). Allergologie Select (2021) 5:305. [CrossRef]
- Hasler WL, Grabauskas G, Singh P, Owyang C. Mast cell mediation of visceral sensation and permeability in irritable bowel syndrome. Neurogastroenterol Motil (2022) 34:e14339. [CrossRef]
- Schnedl WJ, Schenk M, Lackner S, Enko D, Mangge H, Forster F. Diamine oxidase supplementation improves symptoms in patients with histamine intolerance. Food Sci Biotechnol (2019) 28:1779–1784. [CrossRef]
- Maintz L, Novak N. Histamine and histamine intolerance. Am J Clin Nutr (2007) 85:1185–1196. [CrossRef]
- Ispiryan L, Zannini E, Arendt EK. FODMAP modulation as a dietary therapy for IBS: Scientific and market perspective. Comprehensive Reviews in Food Science and Food Safety (2022) 21:1491–1516. [CrossRef]
- Morariu I-D, Avasilcai L, Vieriu M, Lupu VV, Morariu B-A, Lupu A, Morariu P-C, Pop O-L, Starcea IM, Trandafir L. Effects of a Low-FODMAP Diet on Irritable Bowel Syndrome in Both Children and Adults—A Narrative Review. Nutrients (2023) 15:2295. [CrossRef]
- Lenhart A, Chey WD. A Systematic Review of the Effects of Polyols on Gastrointestinal Health and Irritable Bowel Syndrome. Adv Nutr (2017) 8:587–596. [CrossRef]
- Sultan N, Varney JE, Halmos EP, Biesiekierski JR, Yao CK, Muir JG, Gibson PR, Tuck CJ. How to Implement the 3-Phase FODMAP Diet Into Gastroenterological Practice. J Neurogastroenterol Motil (2022) 28:343–356. [CrossRef]
- Bellini M, Tonarelli S, Nagy AG, Pancetti A, Costa F, Ricchiuti A, de Bortoli N, Mosca M, Marchi S, Rossi A. Low FODMAP Diet: Evidence, Doubts, and Hopes. Nutrients (2020) 12:148. [CrossRef]
- Gwioździk W, Krupa-Kotara K, Całyniuk B, Helisz P, Grajek M, Głogowska-Ligus J. Traditional, Vegetarian, or Low FODMAP Diets and Their Relation to Symptoms of Eating Disorders: A Cross-Sectional Study among Young Women in Poland. Nutrients (2022) 14:4125. [CrossRef]
- So D, Loughman A, Staudacher HM. Effects of a low FODMAP diet on the colonic microbiome in irritable bowel syndrome: a systematic review with meta-analysis. Am J Clin Nutr (2022) 116:943–952. [CrossRef]
- Staudacher HM, Lomer MCE, Farquharson FM, Louis P, Fava F, Franciosi E, Scholz M, Tuohy KM, Lindsay JO, Irving PM, et al. A Diet Low in FODMAPs Reduces Symptoms in Patients With Irritable Bowel Syndrome and A Probiotic Restores Bifidobacterium Species: A Randomized Controlled Trial. Gastroenterology (2017) 153:936–947. [CrossRef]
- Oka P, Parr H, Barberio B, Black CJ, Savarino EV, Ford AC. Global prevalence of irritable bowel syndrome according to Rome III or IV criteria: a systematic review and meta-analysis. The Lancet Gastroenterology & Hepatology (2020) 5:908–917. [CrossRef]
- Lacy BE, Mearin F, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R. Bowel Disorders. Gastroenterology (2016) 150:1393-1407.e5. [CrossRef]
- Ford AC, Sperber AD, Corsetti M, Camilleri M. Irritable bowel syndrome. The Lancet (2020) 396:1675–1688. [CrossRef]
- Ford AC, Forman D, Bailey AG, Axon ATR, Moayyedi P. Irritable bowel syndrome: a 10-yr natural history of symptoms and factors that influence consultation behavior. Am J Gastroenterol (2008) 103:1229–1239; quiz 1240. [CrossRef]
- Yarandi SS, Nasseri-Moghaddam S, Mostajabi P, Malekzadeh R. Overlapping gastroesophageal reflux disease and irritable bowel syndrome: Increased dysfunctional symptoms. World J Gastroenterol (2010) 16:1232–1238. [CrossRef]
- Ford AC, Moayyedi P, Lacy BE, Lembo AJ, Saito YA, Schiller LR, Soffer EE, Spiegel BMR, Quigley EMM, Task Force on the Management of Functional Bowel Disorders. American College of Gastroenterology monograph on the management of irritable bowel syndrome and chronic idiopathic constipation. Am J Gastroenterol (2014) 109 Suppl 1:S2-26; quiz S27. [CrossRef]
- Matheis A, Martens U, Kruse J, Enck P. Irritable bowel syndrome and chronic pelvic pain: A singular or two different clinical syndrome? World J Gastroenterol (2007) 13:3446–3455. [CrossRef]
- Barsky AJ. Assessing the New DSM-5 Diagnosis of Somatic Symptom Disorder. Psychosom Med (2016) 78:2–4. [CrossRef]
- Koloski NA, Jones M, Weltman M, Kalantar J, Bone C, Gowryshankar A, Walker MM, Talley NJ. Identification of early environmental risk factors for irritable bowel syndrome and dyspepsia. Neurogastroenterol Motil (2015) 27:1317–1325. [CrossRef]
- Biesiekierski JR, Peters SL, Newnham ED, Rosella O, Muir JG, Gibson PR. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology (2013) 145:320-328.e1–3. [CrossRef]
- Czaja-Bulsa G. Non coeliac gluten sensitivity - A new disease with gluten intolerance. Clin Nutr (2015) 34:189–194. [CrossRef]
- Enck P, Aziz Q, Barbara G, Farmer AD, Fukudo S, Mayer EA, Niesler B, Quigley EMM, Rajilić-Stojanović M, Schemann M, et al. Irritable bowel syndrome. Nat Rev Dis Primers (2016) 2:16014. [CrossRef]
- Hamer HM, Jonkers D, Venema K, Vanhoutvin S, Troost FJ, Brummer R-J. Review article: the role of butyrate on colonic function. Aliment Pharmacol Ther (2008) 27:104–119. [CrossRef]
- Rajilić-Stojanović M, de Vos WM. The first 1000 cultured species of the human gastrointestinal microbiota. FEMS Microbiol Rev (2014) 38:996–1047. [CrossRef]
- Spiller RC. Inflammation as a basis for functional GI disorders. Best Pract Res Clin Gastroenterol (2004) 18:641–661. [CrossRef]
- Pimentel M, Gunsalus R, Rao S, Zhang H. Methanogens in Human Health and Disease. Am J Gastroenterol (2012) 1:28–33. [CrossRef]
- Rajilić-Stojanović M, Biagi E, Heilig HGHJ, Kajander K, Kekkonen RA, Tims S, de Vos WM. Global and deep molecular analysis of microbiota signatures in fecal samples from patients with irritable bowel syndrome. Gastroenterology (2011) 141:1792–1801. [CrossRef]
- Attaluri A, Jackson M, Paulson J, Rao SS. Methanogenic flora is associated with altered colonic transit but not stool characteristics in constipation without IBS. Am J Gastroenterol (2010) 105:10.1038/ajg.2009.655. [CrossRef]
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology (2006) 130:1480–1491. [CrossRef]
- Drossman DA, Tack J, Ford AC, Szigethy E, Törnblom H, Van Oudenhove L. Neuromodulators for Functional Gastrointestinal Disorders (Disorders of Gut-Brain Interaction): A Rome Foundation Working Team Report. Gastroenterology (2018) 154:1140-1171.e1. [CrossRef]
- Lacy BE, Mearin F, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R. Bowel Disorders. Gastroenterology (2016) 150:1393-1407.e5. [CrossRef]
- Quigley EMM. Prebiotics and Probiotics in Digestive Health. Clin Gastroenterol Hepatol (2019) 17:333–344. [CrossRef]
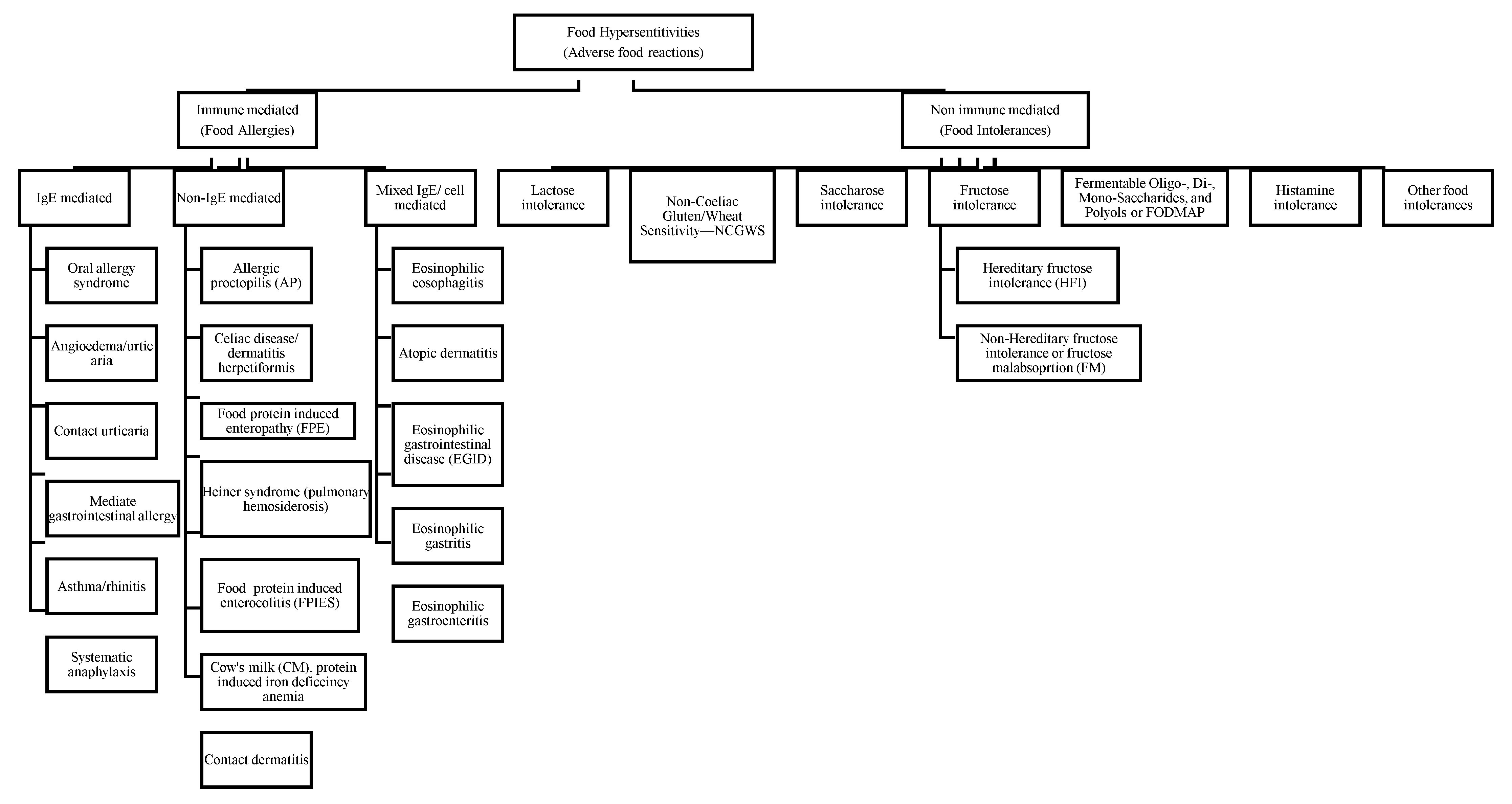
Figure 2.
Flowchart of study selection.
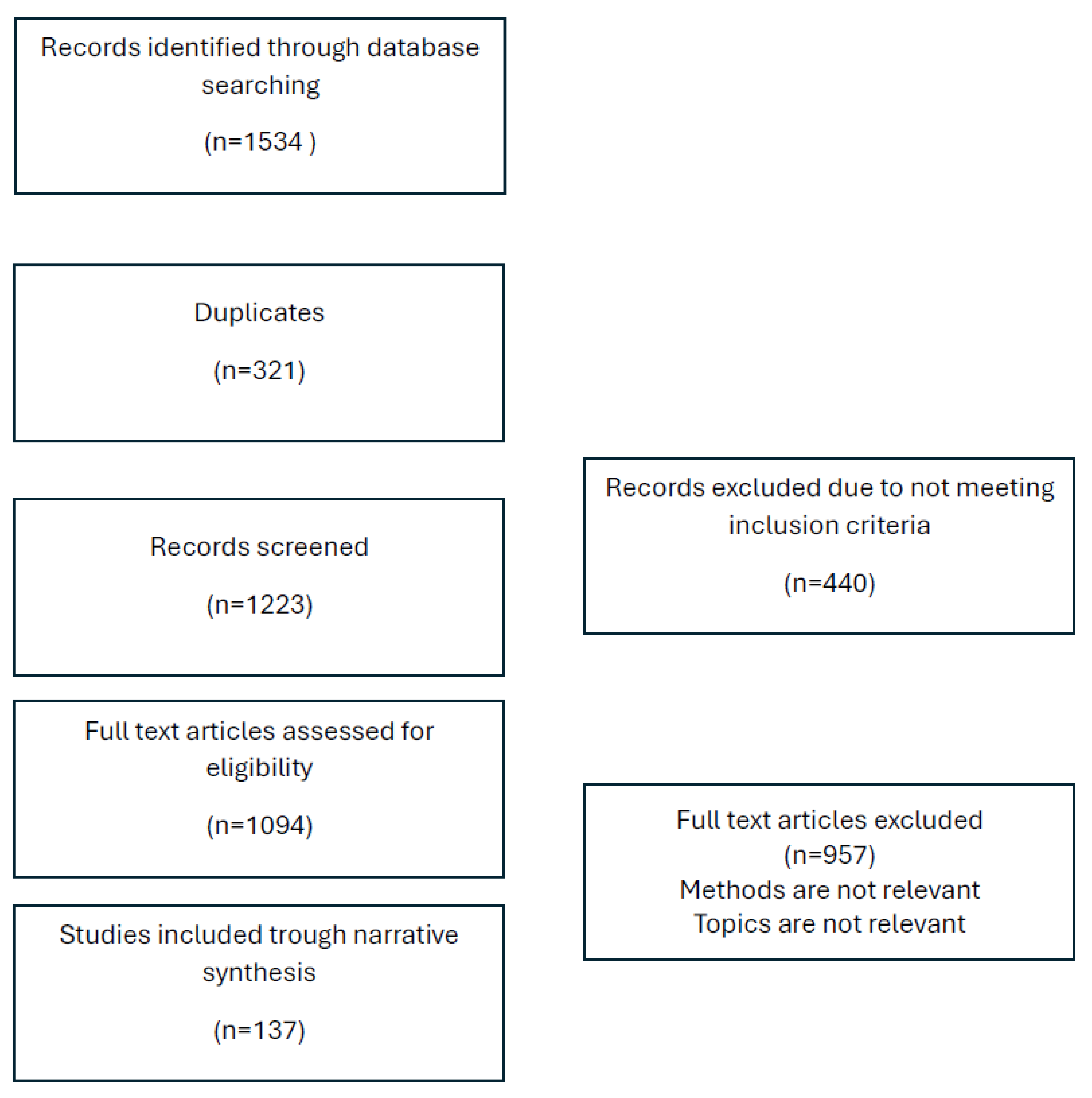
Table 2.
Food allergies disorders and main features.
| Pathology | Disorder | Key features | Most common causal foods |
|---|---|---|---|
| IgE-mediated (acute onset) | Acute urticaria/angioedema | Food commonly causes acute (20%) but rarely chronic urticaria | Cow milk, gluten, eggs, wheat, beans, soybean, nuts, and seafood |
| Contact urticaria | Direct skin contact results in lesions. Histamine release, in rare cases, can cause urticaria. (I change the sentence) (nonimmunologic) |
Multiple | |
| Anaphylaxis | Rapidly progressive, multiple organs system reactions can include cardiovascular collapse | Any but more commonly peanut, Tree nuts, shellfish, fish, milk, and egg | |
| Food-associated, exercise-induced anaphylaxis | Food triggers anaphylaxis only if ingestion is followed temporally by exercise | Wheat, shellfish, and celery are most often described | |
| Oral allergy syndrome (pollen-associated food allergy syndrome) | Pruritus and mild edema are confined to the oral cavity and uncommonly progress beyond the mouth (w7%) and rarely to anaphylaxis (1% to 2%). It might increase after the pollen season. | Raw fruit/vegetables; cooked forms tolerated; examples of relationships: birch (apple, peach, pear, carrot), ragweed (melons) | |
| Immediate gastrointestinal hypersensitivity | Immediate vomiting, pain | Cow milk, gluten, eggs, wheat, beans, soybean, nuts, and seafood | |
| Combined IgE and cell-mediated (delayed onset/chronic) | Atopic dermatitis | Associated with food allergy in 35% of children with moderate-to-severe rash | Major allergens, particularly egg, milk |
| Eosinophilic esophagitis | Symptoms might include feeding disorders, reflux symptoms, vomiting, dysphagia, and food impaction. | Multiple | |
| Eosinophilic gastroenteritis | Vary on site(s)/degree of eosinophilic inflammation; might include ascites, weight loss, edema, obstruction | Multiple | |
| Cell-mediated (delayed onset/chronic) | Food protein-induced enterocolitis syndrome Cow’s milk, soy, rice, oat, meat | Primarily affects infants; chronic exposure: emesis, diarrhea, poor growth, lethargy; re-exposure after restriction: emesis, diarrhea, hypotension (15%) 2 hours after ingestion | Cow’s milk, soy, rice, oat, meat |
| Food protein induced allergic proctocolitis | Mucus-laden, bloody stools in infants Milk (through breast-feeding) | Milk (through breast-feeding) | |
| Allergic contact dermatitis | Often occupational because of chemical moieties, oleoresins. Systemic contact dermatitis is a rare variant because of ingestion | Spices, fruits, vegetables | |
| Heiner syndrome | Pulmonary infiltrates, failure to thrive, iron deficiency anemia | Cow’s milk |
Table 4.
Dysbiosis in IBS.
|
Microbiota species increased in IBS -Enterobacteriaceae -Veillonella -Streptococcus* -Dorea -Blautia -Roseburia -Ruminococcus -Methanobrevibacter‡ |
|
Microbiota species decreased in IBS -Bifidobacterium -Collinsella -Streptococcus‡ -Faecalibacterium -Christensenellaceae -Clostridiales -Methanobrevibacter§ |
IBS, irritable bowel syndrome. *IBS with diarrhea. ‡IBS with constipation. §Mixed-type IBS. [127].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



