
Submitted:
14 March 2025
Posted:
18 March 2025
You are already at the latest version
Abstract
Objective: To enhance the awareness of the diverse manifestations of head and neck tuberculosis (HNTB) and the diagnostic hurdles it poses. Study Design: To analyze the presentation and clinical characteristics of HNTB cases. The diagnosis in all cases was established through histopathological examination of infected tissue in conjunction with medical history, TB-SPOT and other complementary TB investigations. Follow-up time 1 to 10 years. Setting: Peking Union Medical College Hospital. Methods: This retrospective study examined the clinical profiles of 60 patients diagnosed with HNTB at a tertiary university institution between 2013 and 2023.The cohort consisted of 29 men and 31 women aged 12 to 80 years (mean 43.95±16.98 years). Results: HNTB predominantly manifested in the larynx (27 cases, 45.0%), with most cases presenting with diffuse ulcerated or proliferative lesions. Notably, six patients exhibited irregular lesions on the unilateral vocal cords, mimicking early stage glottic carcinoma. The second most common localisation was in the cervical lymph nodes (20 cases, 33.33%), including cases such as retropharyngeal lymph node tuberculosis and tracheoesophageal groove lymph node tuberculosis. Conclusion: Clinicians should always consider HNTB in the differential diagnosis of lesions in this region. Given the oligobacterial nature of this disease and the absence of pulmonary involvement in the majority of cases, histopathological biopsy should be performed in cases of high suspicion. Early detection and treatment are of paramount importance to optimise therapeutic outcomes and improve the quality of life of patients.
Keywords:
Tuberculosis
; extra pulmonary
; head and neck
; laryngeal tuberculosis
; cervical lymphadenopathy
1. Introduction
Tuberculosis (TB) remains a formidable global health challenge, claiming nearly twice as many lives as AIDS [1]. According to a report by the World Health Organization (WHO), in 2022, there were an estimated 10.6 million new TB cases worldwide, resulting in approximately 1.30 million deaths [1]. Factors predisposing individuals to TB include socioeconomic disparities, malnutrition, immunosuppression (such as HIV infection), diabetes, smoking, alcoholism, among others [2].
Extrapulmonary tuberculosis (EPTB) accounts for about one-fifth of all TB cases, affecting primarily the lymph nodes, pleura, genitourinary system, bones and joints, and gastrointestinal tract [3]. And head and neck tuberculosis (HNTB) constitutes approximately 10% of TB patients [4]. HNTB can manifest in various organs within the head and neck region, including the lymph nodes, larynx, middle ear, oral cavity, and pharynx [5]. Given that the symptoms of HNTB often resemble those of tumors or inflammatory conditions, and systemic manifestations are typically absent, diagnosing HNTB is often challenging. Recognition of HNTB usually occurs only after ineffective anti-inflammatory treatment, biopsy, or even surgical intervention [4,6,7,8]. Consequently, there has been no reduction in the frequency of late-stage diagnoses of HNTB in recent years [9]. A comprehensive evaluation, including a thorough patient history, assessment of exposure to TB, physical examination, fine needle aspiration cytology (FNAC), and biopsy, is essential for achieving an early and accurate diagnosis [10,11,12,13,14].
This study seeks to analyze the presentation and clinical characteristics of HNTB cases diagnosed at our institution, aiming to enhance awareness of the diverse manifestations of HNTB and the diagnostic hurdles it poses.
2. Materials and Methods
This retrospective study analyzed 60 patients diagnosed with HNTB at Peking Union Medical College Hospital (PUMCH) between 2013 and 2023. Demographic data including patients’ sex, age, site of origin, clinical presentation, results of tuberculosis-specific enzyme-linked immunospot assay (TB-SPOT), next-generation sequencing (NGS) findings, TB history, comorbidities (such as HIV, diabetes, autoimmune diseases, tumors, etc.), and imaging features of the lesion and chest were collected and reviewed. Radiological and histopathological findings were also evaluated. The diagnosis in all cases was established through histopathological examination of infected tissue in conjunction with medical history, TB-SPOT and other complementary TB investigations. For comprehensive diagnosis and treatment [15], all patients were referred to one of the two specialized tuberculosis centers in Beijing. This study received approval from the Ethics Committee of PUMCH, and written consent was obtained from the patient presented in this paper.
3. Results
The patient characteristics are summarized in Table 1. Among the 60 patients diagnosed with HNTB, there were 29 males and 31 females, with ages ranging from 12 to 80 years (mean 43.95±16.98 years). The age range for men was 12 to 80 years (mean 41.14±17.49 years), and for women, it was 13 to 79 years (mean 46.58±16.33 years). The male to female ratio was 0.94:1. Laryngeal TB was the most frequently observed localization in the head and neck region, accounting for 27 (45.00%) cases. Many of these cases exhibited extensive lesions involving multiple parts of the larynx (Figure 1). In Figure 1, A and B illustrate supraglottic involvement. C shows bilateral glottic and subglottic lesions. D, E and F show multiple lesions on the base of the tongue, lateral pharyngeal wall and supraglottic area in a single case. G and H show multiple scars resulting from antituberculosis treatment. However, six patients presented with unilateral vocal cord involvement, resembling early-stage glottic carcinoma (Figure 2). The second most common localization was cervical lymph nodes, with 20 (33.33%) cases. Most cases of cervical lymph node TB involved the lateral cervical lymph nodes (Figure 3). In our series, two cases stood out due to special cervical lymph node involvement. They are detailed in the typical case description below. Pharyngeal TB was diagnosed in 7 (11.67%) cases (Figure 1). Additionally, there were 3 (5.00%) cases of salivary gland TB, including 2 (3.33%) cases involving the parotid gland and 1 (1.67%) case involving the submandibular gland. Furthermore, there were 3 (5.00%) cases of multiple involvement, with two cases involving the oropharynx and larynx, and one involving the nasopharynx, oropharynx, hypopharynx, and larynx. One of these cases presented with laryngeal stenosis and second-degree dyspnoea, which resolved after antituberculosis treatment.
3.1. Typical Cases
3.1.1. Case 1
A 30-year-old man with a one-month history of foreign body sensation in the throat presented to another hospital. MRI results indicated a “parapharyngeal mass with suspected infection,” leading to antibiotic treatment and preparation for surgical resection. Subsequently, he visited the PUMCH clinic. Laryngoscopy revealed a smooth prominence at the level of the nasopharynx (Figure 4A), while enhanced CT imaging of the neck displayed a possible lymph node abscess in the right retropharyngeal space (Figure 4C). Needle aspiration was performed under fiberoptic laryngoscopy, yielding 7 ml of yellowish viscous fluid. The aspirated pus tested positive for acid-fast bacilli (AFB). Throughout the disease course, the patient did not present with fever, cough, sputum, night sweats, or any other complaints. Sputum smear and culture results were negative. After six weeks of receiving a four-drug combination therapy for TB (isoniazid, rifampicin, pyrazinamide, and ethambutol hydrochloride), fiberoptic laryngoscopy and cervical CT were reviewed, revealing the disappearance of the pharyngeal bulge and lymph node abscess (Figure 4B, 4D). Routine antituberculosis treatment was discontinued after six months, and the patient underwent a two-year follow-up without experiencing recurrence.
3.1.2. Case 2
A 47-year-old woman with a one-month history of dysphagia presented to the PUMCH for the first time. Enhanced cervical and thoracic CT scans showed thickening of the upper oesophageal wall with significant enhancement, accompanied by surrounding enlarged lymph nodes (white arrowhead in Figure 5A). Multiple white lesions were found in the oesophagus during a gastroscopy at another medical facility (Figure 5B), and biopsy pathology confirmed the presence of mycobacterial hyphae and spores. Five days before her emergency visit to PUMCH, the patient developed fever and became unable to ingest water and food. Emergency chest CT scan showed thickening of the upper and middle oesophageal wall with low density nodular lesions on both sides of the tracheoesophageal groove with annular enhancement (blue arrowhead in Figure 5C). Notably, the patient did not report cough, sputum, or night sweats. With an 8-year medical history of thymoma and myasthenia gravis, and current treatment comprising oral brompheniramine 60mg q6h and Medrol 48mg qd, the patient underwent a multidisciplinary consultation. A potential diagnosis of a peritracheal space abscess due to esophageal perforation was considered, prompting an emergency abscess drainage procedure. Intraoperatively, rigid esophagoscopy confirmed esophageal perforation, and approximately 15 ml of pus was drained from the left side of the cervical root surrounding the esophagus through an open neck incision. The drained pus tested positive for AFB. Despite consistently negative sputum smear and culture results, a diagnosis of mycotic esophagitis with mediastinal lymph node TB abscess was established. Mycotic esophagitis resolved after two weeks of antifungal treatment (fluconazole 200mg), while the lymph node abscess disappeared following two months of antituberculosis treatment. However, complete healing of the esophageal perforation occurred only after 8 months of antituberculosis treatment (blue arrowhead in Figure 5D).
4. Discussion
The male-to-female ratio observed in our study was 0.94. According to the WHO annual report, TB infection tends to affect more men than women in the general population [1]. Additionally, EPTB cases have been reported to be predominantly male [16,17,18]. Interestingly, a systematic review of HNTB revealed a higher incidence among females [19], consistent with our findings. This suggests that HNTB may be more prevalent in females compared to pulmonary TB and EPTB at other sites. Therefore, the identification of nonspecific head and neck lesions in female patients warrants greater attention to exclude TB.
In our study, the larynx emerges as the most common site for HNTB, followed closely by the lymph nodes, with proportions not significantly different from that of the larynx. Most studies have indicated that cervical lymph nodes are the most frequently affected site in HNTB [19,20,21]. However, some reports indicates that the larynx may be equally or more involved in HNTB compared to cervical lymph nodes, or that these two entities exhibit a similar ratio [9,12]. This suggests that both the larynx and cervical lymph nodes are prominent sites for HNTB. The larynx, alongside the trachea and lungs, constitutes the respiratory system. Etiologically, laryngeal TB is predominantly caused by respiratory transmission of pulmonary TB, whereas cervical lymph node TB is more likely caused by bloodstream transmission. In this case group, the incidence of laryngeal tuberculosis coexisting with pulmonary tuberculosis was notably higher than that of lymph node TB. This observation supports the hypothesis that the transmission routes differ between these two manifestations.
According to the latest WHO global report, TB has shown an upward trend in recent years, often associated with a high prevalence of HIV infection and other immunosuppressive conditions [1]. A prior study conducted at our center recorded 10 cases of laryngeal TB diagnosed over a 14-year period from 1996 to 2010 [22]. However, the current study revealed a substantial increase, with 27 cases of laryngeal TB identified over the past decade, indicating a rising overall trend in cases. Among the 60 patients included in our study, 8 cases(11.33%) had concomitant autoimmune diseases (8.33%), diabetes mellitus (1.67%), or tumors (3.33%). Therefore, individuals with immunosuppressive conditions should be particularly vigilant regarding the possibility of TB. Comprehensive evaluation, including a thorough medical history, physical examination, and appropriate ancillary tests, is crucial for timely diagnosis and management.
Systemic symptoms such as cough, fever, or night sweats were reported in only 20% of patients with HNTB in the literature [23], with clinical examinations often yielding negative results. In our series, typical systemic symptoms were present in only 17 (28.33%) patients. The presentation of HNTB varies depending on the site of onset, with the pharynx commonly presenting as a non-healing ulcer or mass, mimicking malignancy [7]. Notably, solitary hyperplastic or ulcerative lesions should prompt vigilance during consultation. In the cases of unilateral vocal cord hyperplastic lesions depicted in Figure 2, the initial clinical diagnosis was vocal cord cancer. It was only during intraoperative frozen sections that granuloma with necrosis was suggested, leading to further investigation for TB. TB of cervical lymph nodes typically manifests as painless neck masses and may, in some cases, be associated with deep cervical space abscesses [24,25]. The former can be misdiagnosed as malignancy or metastatic cancer, while the latter may be mistaken for a common infection. Imaging studies, such as ultrasound and CT, aid in distinguishing the location, size, and number of HNTB lesions. Given that most HNTB patients present to surgeons, FNAC serves as a cost-effective diagnostic tool for painless masses, with excisional biopsy considered when other tests and FNAC fail to confirm the diagnosis. Biopsy demonstrates higher sensitivity (84-100%) than FNAC (9-90%) and better differentiation between tumor and tuberculosis [26,27]. Excisional biopsy helps avoid underdiagnosis, especially in cases of TB-tumor coexistence, which has been reported in previous studies involving laryngeal, oropharyngeal, and cervical lymph node TB [9,12,23,28,29]. In our series, two patients with HNTB had concomitant tumors at other sites. Diagnosis was confirmed by biopsy in 61.67% of patients, while in the remaining cases, diagnosis was based on history and complementary findings from TB investigations.
Currently, culture of Mycobacterium tuberculosis (MTB) remains the gold standard for TB diagnosis. However, it can take up to 4-6 weeks and its sensitivity varies depending on the host and site of infection [2]. The Tuberculin Skin Test (TST) is the oldest and most commonly used test in clinical settings, but its positivity rate is only around 53%, and it’s even lower in patients with localized primary TB foci [23]. Serum interferon-gamma release assays (IGRAs), such as QFT-TB and TB-SPOT, offer higher specificity and better positive and negative predictive values compared to TST [30,31]. IGRAs can distinguish between BCG-vaccinated and non-vaccinated individuals more accurately than TST, and they are particularly useful in immunosuppressed patients. And they have the capability to differentiate cases not infected with MTB. TB-SPOT, for instance, has shown a sensitivity of 90.3% and a specificity of 92.3% [32]. In this study, TB-SPOT was conducted in 53.3% of patients, with a sensitivity of 87.5%. Although AFB Ziehl-Neelsen stains are commonly used in clinical practice, their sensitivity ranges from 27-60% due to the selective scarcity of bacilli in tissue [33]. Moreover, a positive result does not conclusively confirm a diagnosis of TB. Polymerase chain reaction (PCR) has a sensitivity of 45-75% and a specificity of 97.3-100% for cervical lymph node needle aspiration specimens [21]. Gene Xpert MTB/RIF can confirm TB diagnosis within 2 hours with a sensitivity of 89% in smear-positive patients and 67% in smear-negative patients [34]. Diagnostic chemotherapy may be administered to patients with similar clinical symptoms but inconclusive test results. Confirmation of TB diagnosis is based on a favorable response to initial TB chemotherapy. Additionally, next-generation nucleic acid amplification tests (NAATs), microscopy, and blood tests are being explored to fulfill the need for sensitive, low-cost, high-throughput TB screening methods.
Among the cases examined, one instance of retropharyngeal lymph node suppurative TB was identified, representing a unique finding not previously reported in the literature. Existing studies have suggested that retropharyngeal TB abscesses typically result from the spread of cervical tuberculosis [35,36]. Notably, the reported abscesses were predominantly midline, and patients typically had a history of cervical TB supporting this conclusion. However, our case diverged from this pattern, as the retropharyngeal abscess was located exclusively on the right side, without crossing the midline. Additionally, solid tissue adjacent to the abscess indicated suppurative changes within the lymph node, with another enlarged retropharyngeal lymph node adjacent to it. Remarkably, this patient had no history of cervical tuberculosis, leading us to conclude that the TB infection solely involved the retropharyngeal lymph nodes. Another exceptional case in our study involved both fungal esophagitis and cervical lymph node TB within the tracheoesophageal sulcus. Unfortunately, during the disease course, the patient developed esophageal perforation. Based on her medical history, we attributed the cause of the perforation to esophageal wall damage resulting from an esophageal biopsy. Moreover, the patient’s immunocompromised state due to high-dose glucocorticoid therapy likely contributed to the perforation due to local inflammation at the biopsy site. The presence of tuberculous lymph node abscesses adjacent to the perforation led to the formation of a minimal fistula between the perforated esophagus and the abscess. Initially, we suspected that the abscesses were a consequence of esophageal perforation until TB diagnosis was confirmed via smear and culture. Due to the TB infection, the fistula did not heal completely, and the patient resumed oral feeding only after 8 months of antituberculosis treatment.
This study presents several limitations. Firstly, it is a single-center retrospective study, inherently prone to bias in the epidemiology and distribution of sites affected by HNTB. Over the 10-year study period, diagnostic techniques have significantly evolved, leading to some variation in diagnostic approaches across cases, contributing to heterogeneity within the cohort. Additionally, the relatively small number of cases limits the assessment of TB risk in individuals with autoimmune diseases or comorbidities such as diabetes and tumors. Despite these constraints, this study stands out as one of the few with a relatively large sample size focusing on HNTB. It offers valuable insights into the diagnosis and management of HNTB, with some rare cases providing crucial clinical guidance for head and neck surgeons.
5. Conclusion
HNTB can affect various organs in the head and neck region, with TB of the larynx and cervical lymph nodes being the most common. However, clinical practice often sees HNTB misdiagnosed as malignancy or a common infection. Given its oligobacterial nature and the absence of pulmonary involvement in most cases, a biopsy for histopathologic examination should be performed in highly suspected cases. However, in instances where a biopsy might cause a natural luminal fistula, a minimally invasive approach to obtain the specimen is preferable to avoid the potential decrease in the patient’s quality of life associated with a prolonged fistula. Early diagnosis and treatment of HNTB can significantly improve patient quality of life, reduce the risk of disease transmission, and safeguard healthcare providers. Given the lengthy culture time required for MTB, clinical diagnosis should be supplemented with pathology, IGRAs, TSTs, sputum smear, and other diagnostic measures. Diagnostic antituberculosis therapy can be initiated in highly suspected cases to expedite treatment and minimize disease progression.
Funding
National High Level Hospital Clinical Research Funding (2022-PUMCH-B-094);Science & Technology Fundamental Resources Investigation Program (Grant No.2022FY100800); CAMS Innovation Fund for Medical Sciences (CIFMS) (2021-I2M-1-023), (2023-I2M-C&T-B-005).
Conflicts of Interest
None.
References
- WHO global tuberculosis report 2023. https://www.who.int/publications/i/item/9789240083851.
- Gambhir S, Ravina M, Rangan K, et al. Imaging in extrapulmonary tuberculosis. Int J Infect Dis 2017; 56: 237-47.
- Sandgren, A.; Hollo, V.; van der Werf, M.J. Extrapulmonary tuberculosis in the European Union and European Economic Area, 2002 to 2011. Eurosurveillance 2013, 18, 20431. [Google Scholar] [CrossRef] [PubMed]
- Brucoli, M.; Borello, G.; Boffano, P.; Benech, A. Tuberculous neck lymphadenopathy: A diagnostic challenge. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Das S, Das D, Bhuyan UT, Saikia N. Head and Neck Tuberculosis: Scenario in a Tertiary Care Hospital of North Eastern India. J Clin Diagn Res 2016; 10(1): MC04-7.
- Bozan, N.; Sakin, Y.F.; Parlak, M.; Bozkuş, F. Suppurative Cervical Tuberculous Lymphadenitis Mimicking a Metastatic Neck Mass. J. Craniofacial Surg. 2016, 27, e565–e567. [Google Scholar] [CrossRef] [PubMed]
- Mocanu, A.-I.; Mocanu, H.; Moldovan, C.; Soare, I.; Niculet, E.; Tatu, A.L.; Vasile, C.I.; Diculencu, D.; A Postolache, P.; Nechifor, A. Some Manifestations of Tuberculosis in Otorhinolaryngology – Case Series and a Short Review of Related Data from South-Eastern Europe. Infect. Drug Resist. 2022, ume 15, 2753–2762. [Google Scholar] [CrossRef]
- Sheikh, S.; Pallagatti, S.; Gupta, D.; Mittal, A. Tuberculous osteomyelitis of mandibular condyle: a diagnostic dilemma. Dentomaxillofacial Radiol. 2012, 41, 169–174. [Google Scholar] [CrossRef]
- Pajor, A.M.; Józefowicz-Korczyńska, M.; Korzeniewska-Koseła, M.; Kwiatkowska, S. A Clinic-Epidemiological Study of Head and Neck Tuberculosis—A Single-Center Experience. Adv. Respir. Med. 2016, 84, 324–330. [Google Scholar] [CrossRef]
- Balikci, H.H.; Gurdal, M.M.; Ozkul, M.H.; Karakas, M.; Uvacin, O.; Kara, N.; Alp, A.; Ozbay, I. Neck masses: diagnostic analysis of 630 cases in Turkish population. Eur. Arch. Oto-Rhino-Laryngology 2013, 270, 2953–2958. [Google Scholar] [CrossRef]
- Lee J, Fernandes R. Neck masses: evaluation and diagnostic approach. Oral Maxillofac Surg Clin North Am 2008; 20(3): 321-37.
- Pang, P.; Duan, W.; Liu, S.; Bai, S.; Ma, Y.; Li, R.; Liu, F.; Sun, C. Clinical study of tuberculosis in the head and neck region—11 years’ experience and a review of the literature. Emerg. Microbes Infect. 2018, 7, 1–10. [Google Scholar] [CrossRef]
- Vaid, S.; Lee, Y.; Rawat, S.; Luthra, A.; Shah, D.; Ahuja, A. Tuberculosis in the head and neck — a forgotten differential diagnosis. Clin. Radiol. 2010, 65, 73–81. [Google Scholar] [CrossRef]
- Yashveer, J.K.; Kirti, Y.K. Presentations and Challenges in Tuberculosis of Head and Neck Region. Indian J. Otolaryngol. Head Neck Surg. 2016, 68, 270–274. [Google Scholar] [CrossRef]
- Cheng, L.; Chen, J.; Fu, Q.; He, S.; Li, H.; Liu, Z.; Tan, G.; Tao, Z.; Wang, D.; Wen, W.; et al. Chinese Society of Allergy Guidelines for Diagnosis and Treatment of Allergic Rhinitis. Allergy, Asthma Immunol. Res. 2018, 10, 300–353. [Google Scholar] [CrossRef] [PubMed]
- Ranzani, O.T.; Rodrigues, L.C.; Waldman, E.A.; Carvalho, C.R.R. Estimating the impact of tuberculosis anatomical classification on treatment outcomes: A patient and surveillance perspective analysis. PLOS ONE 2017, 12, e0187585. [Google Scholar] [CrossRef] [PubMed]
- Sama, J.; Chida, N.; Polan, R.; Nuzzo, J.; Page, K.; Shah, M. High proportion of extrapulmonary tuberculosis in a low prevalence setting: a retrospective cohort study. Public Health 2016, 138, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Leeds, I.L.; Magee, M.J.; Kurbatova, E.V.; del Rio, C.; Blumberg, H.M.; Leonard, M.K.; Kraft, C.S. Site of Extrapulmonary Tuberculosis is Associated with HIV Infection. Clin. Infect. Dis. 2012, 55, 75–81. [Google Scholar] [CrossRef]
- Qian, X.; Albers, A.E.; Nguyen, D.T.; Dong, Y.; Zhang, Y.; Schreiber, F.; Sinikovic, B.; Bi, X.; Graviss, E.A. Head and neck tuberculosis: Literature review and meta-analysis. Tuberculosis 2019, 116, S78–S88. [Google Scholar] [CrossRef]
- Oishi, M.; Okamoto, S.; Teranishi, Y.; Yokota, C.; Takano, S.; Iguchi, H. Clinical Study of Extrapulmonary Head and Neck Tuberculosis: A Single-Institute 10-year Experience. Int. Arch. Otorhinolaryngol. 2016, 20, 030–033. [Google Scholar] [CrossRef]
- Chiesa Estomba CM, Betances Reinoso FA, Rivera Schmitz T, Ossa Echeverri CC, Gonzalez Cortes MJ, Santidrian Hidalgo C. Head and neck tuberculosis: 6-year retrospective study. Acta Otorrinolaringol Esp 2016; 67(1): 9-14.
- Zhu XL Chen XW, Yang H, etc. Clinical Manifestations and Differential Diagnosis of Laryngeal Tuberculosis. Basic and Clinical Medicine 2011; 31(5): 586-90.
- Bruzgielewicz, A.; Rzepakowska, A.; Osuch-Wójcikewicz, E.; Niemczyk, K.; Chmielewski, R. Tuberculosis of the head and neck – epidemiological and clinical presentation. Arch. Med Sci. 2014, 6, 1160–1166. [Google Scholar] [CrossRef]
- Deveci HS, Kule M, Kule ZA, Habesoglu TE. Diagnostic challenges in cervical tuberculous lymphadenitis: A review. North Clin Istanb 2016; 3(2): 150-5.
- Chhabra, B.; Vyas, P.; Gupta, P.; Sharma, P.; Sharma, K. Incidence, Diagnosis and Treatment of Otorhinolaryngological, Head and Neck Tuberculosis: A Prospective Clinical Study. Int. Arch. Otorhinolaryngol. 2023, 27, e630. [Google Scholar] [CrossRef]
- Fontanilla, J.-M.; Barnes, A.; von Reyn, C.F. Current Diagnosis and Management of Peripheral Tuberculous Lymphadenitis. Clin. Infect. Dis. 2011, 53, 555–562. [Google Scholar] [CrossRef]
- Tachibana, T.; Ogawara, Y.; Matsuyama, Y.; Abe, I.; Orita, Y.; Nishizaki, K.; Fujisawa, M.; Nakada, M.; Sato, Y.; Uesaka, K. Factors that make it difficult to diagnose cervical tuberculous lymphadenitis. J. Infect. Chemother. 2013, 19, 1015–1020. [Google Scholar] [CrossRef]
- Prasad, K.C.; Sreedharan, S.; Chakravarthy, Y.; Prasad, S.C. Tuberculosis in the head and neck: experience in India. J. Laryngol. Otol. 2007, 121, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Sriram, R.; Bhojwani, K.M. Manifestations of Tuberculosis in Otorhinolaryngology Practice: A Retrospective Study Conducted in a Coastal City of South India. Indian J. Otolaryngol. Head Neck Surg. 2017, 69, 210–215. [Google Scholar] [CrossRef] [PubMed]
- Steingart, K.R.; Schiller, I.; Horne, D.J.; Pai, M.; Boehme, C.C.; Dendukuri, N.; Sohn, H.; A Kloda, L. Xpert® MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst. Rev. 2015, 2014. [Google Scholar] [CrossRef]
- Walusimbi, S.; Bwanga, F.; De Costa, A.; Haile, M.; Joloba, M.; Hoffner, S. Meta-analysis to compare the accuracy of GeneXpert, MODS and the WHO 2007 algorithm for diagnosis of smear-negative pulmonary tuberculosis. BMC Infect. Dis. 2013, 13, 507. [Google Scholar] [CrossRef]
- Fei B, Wu Z, Min K, Zhang J, Ding C, Wu H. Interferon-gamma release assay in the diagnosis of laryngeal tuberculosis. Acta Otolaryngol 2014; 134(3): 314-7.
- Neville B DD, Allen C et al. Soft tissue tumors. In: Neville B, Damm D, Allen C et al, eds. Oral and Maxillofacial Pathology, 2nd edition. 2002: W.B. Saunders: Philadelphia, pp. 458–61.
- Dheda K, Barry CE, 3rd, Maartens G. Tuberculosis. Lancet 2016; 387(10024): 1211-26.
- Lubben B, Tombach B, Rudack C. [Tubercular spondylitis with retropharyngeal abscess]. HNO 2004; 52(9): 820-3.
- Kosmidou, P.; Kosmidou, A.; Angelis, S.; Dimitriadou, P.P.; Filippou, D. Atypical Retropharyngeal Abscess of Tuberculosis: Diagnostic Reasoning, Management, and Treatment. Cureus 2020, 12, e9124. [Google Scholar] [CrossRef]
Figure 1.
Typical lesions of TB in the larynx and pharynx.
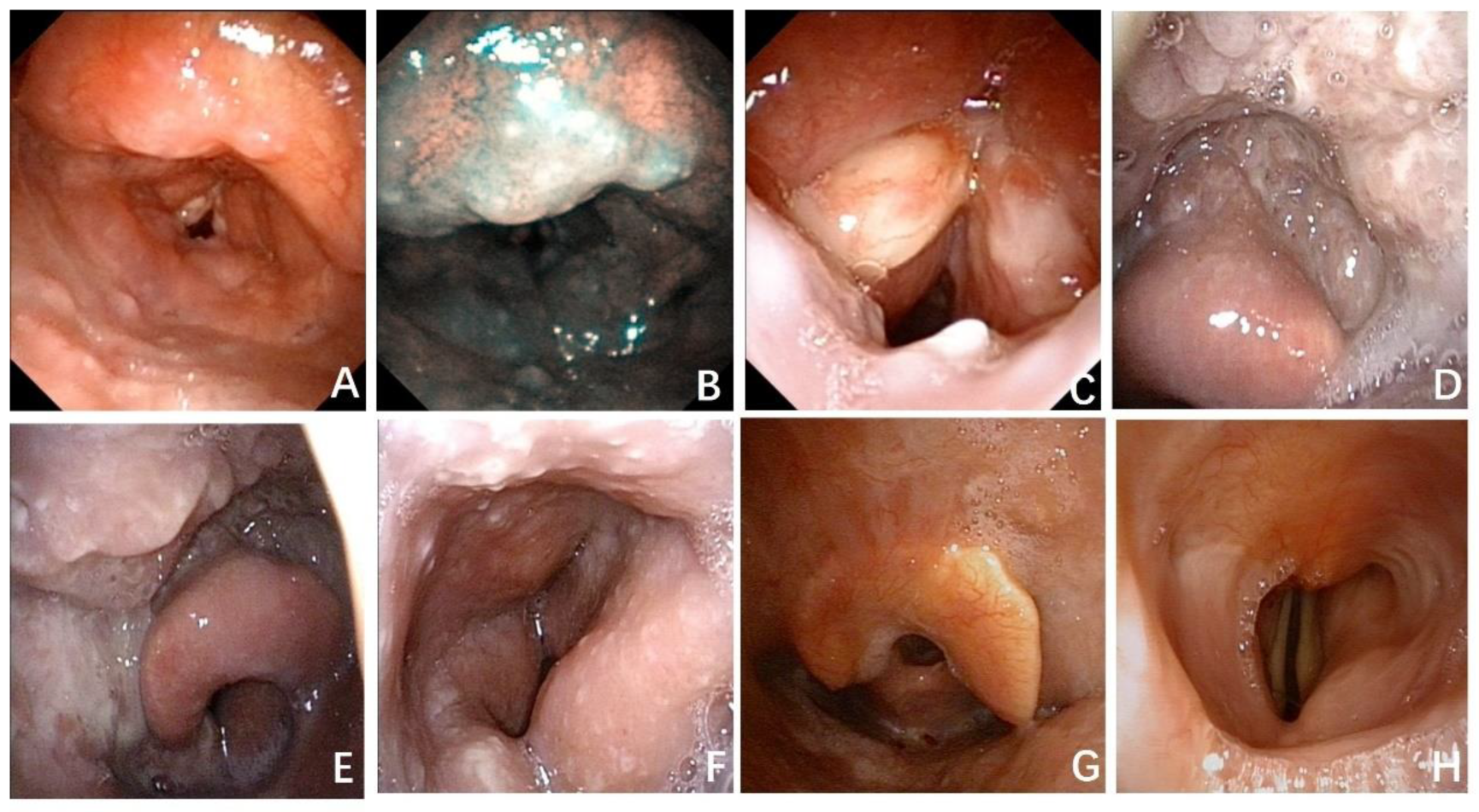
Figure 2.
Two cases of unilateral vocal cord tuberculosis observed by electron laryngoscopy. The lesions resemble malignancy (A, C). The scar on the right vocal cord is healing after anti-tuberculosis treatment (B, D).
Figure 2.
Two cases of unilateral vocal cord tuberculosis observed by electron laryngoscopy. The lesions resemble malignancy (A, C). The scar on the right vocal cord is healing after anti-tuberculosis treatment (B, D).
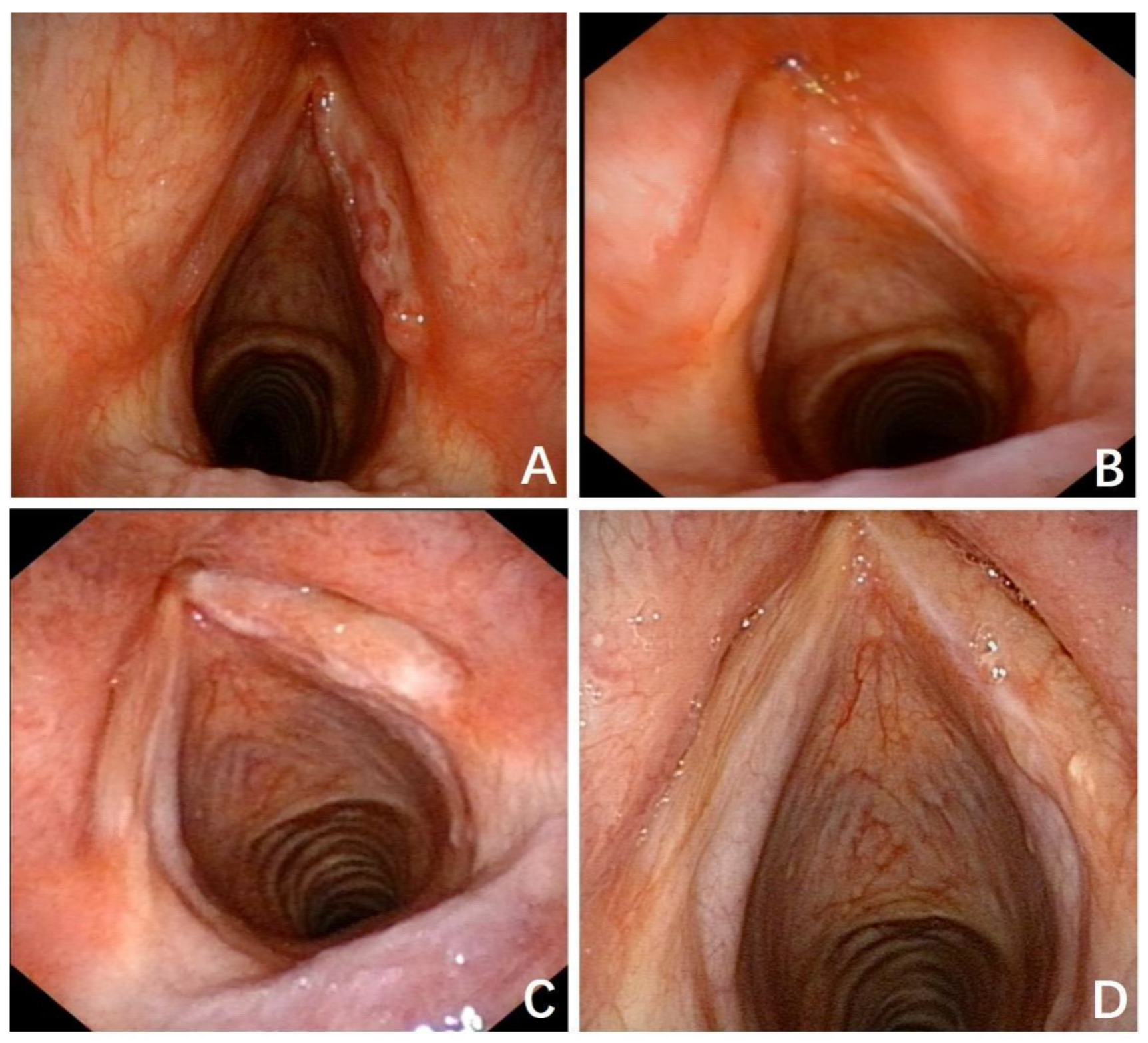
Figure 3.
Typical cervical lymph node TB is depicted on CT, showcasing bilateral multiple lymphadenopathy. A provides a coronal view, while B offers a horizontal view. The blue arrows indicate the affected lymph nodes.
Figure 3.
Typical cervical lymph node TB is depicted on CT, showcasing bilateral multiple lymphadenopathy. A provides a coronal view, while B offers a horizontal view. The blue arrows indicate the affected lymph nodes.
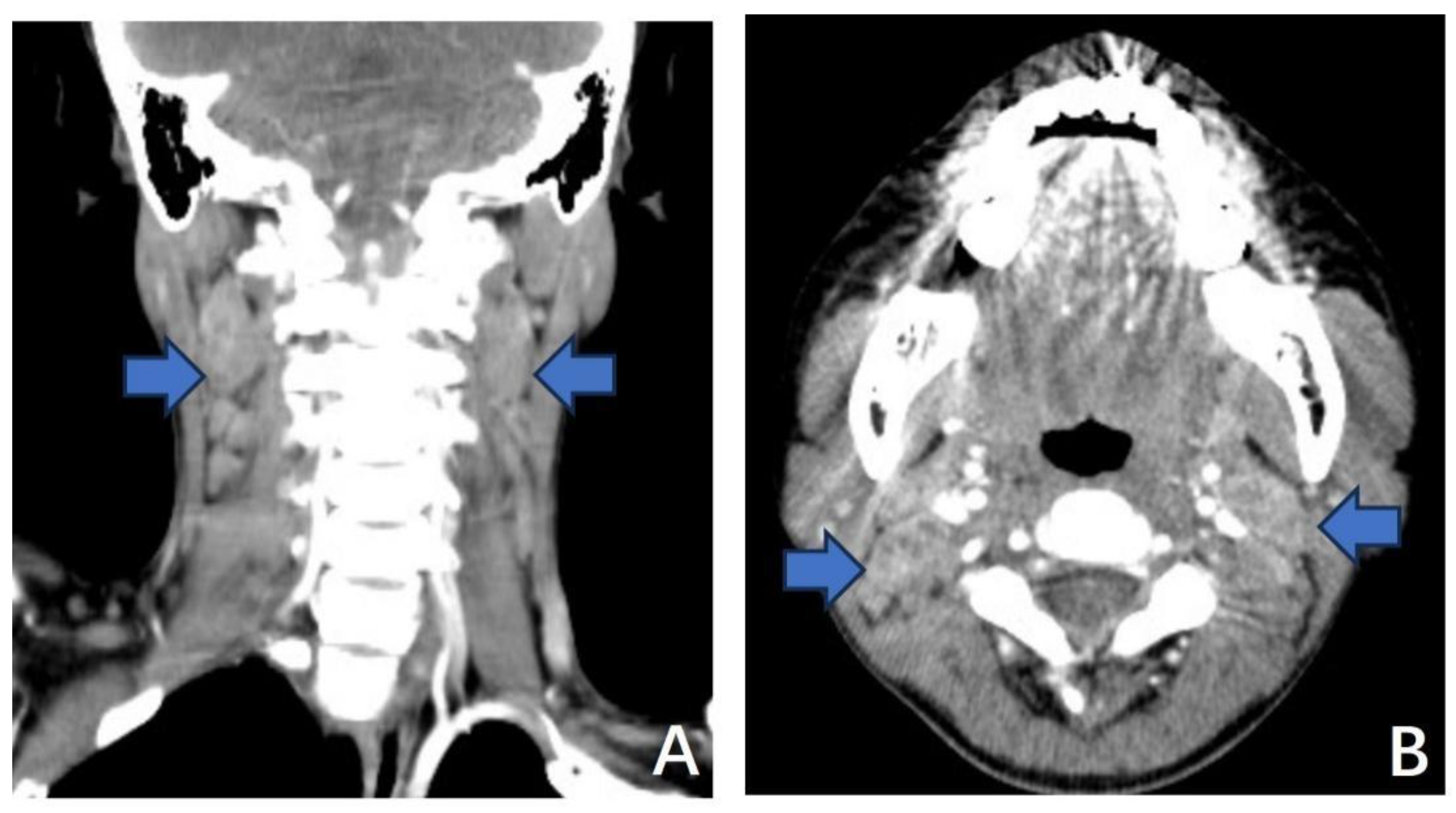
Figure 4.
Tuberculous retropharyngeal lymph node infection mimics retropharyngeal abscess. Nasopharyngeal bulge by laryngoscopy and an enlarged lymph node with pus (A,C). Lymph node and nasopharyngeal conditions improved with anti-tuberculosis medication(B, D).
Figure 4.
Tuberculous retropharyngeal lymph node infection mimics retropharyngeal abscess. Nasopharyngeal bulge by laryngoscopy and an enlarged lymph node with pus (A,C). Lymph node and nasopharyngeal conditions improved with anti-tuberculosis medication(B, D).
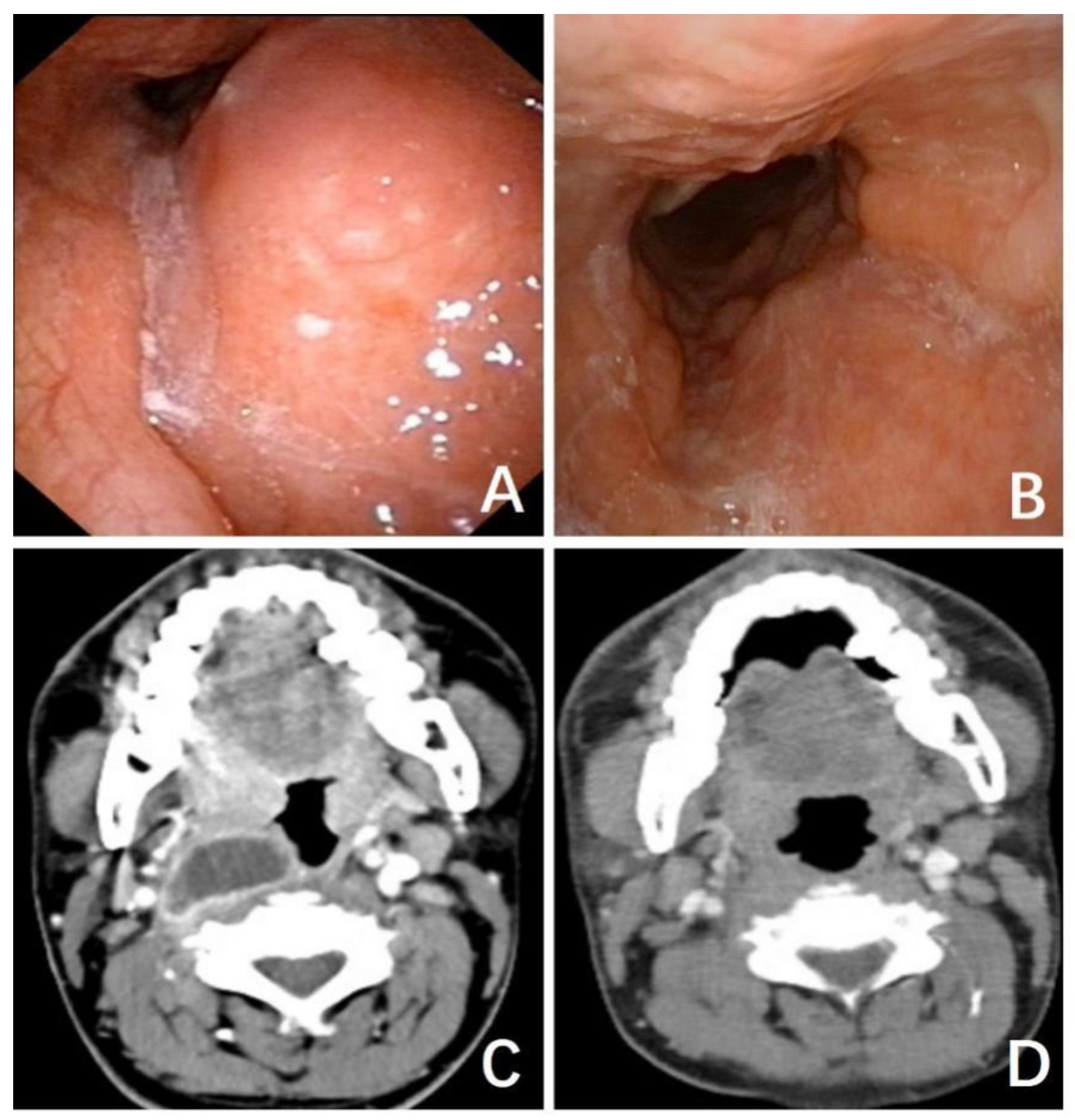
Figure 5.
A patient presented with mycotic esophagitis and bilateral tracheoesophageal sulcus lymph node TB.
Figure 5.
A patient presented with mycotic esophagitis and bilateral tracheoesophageal sulcus lymph node TB.
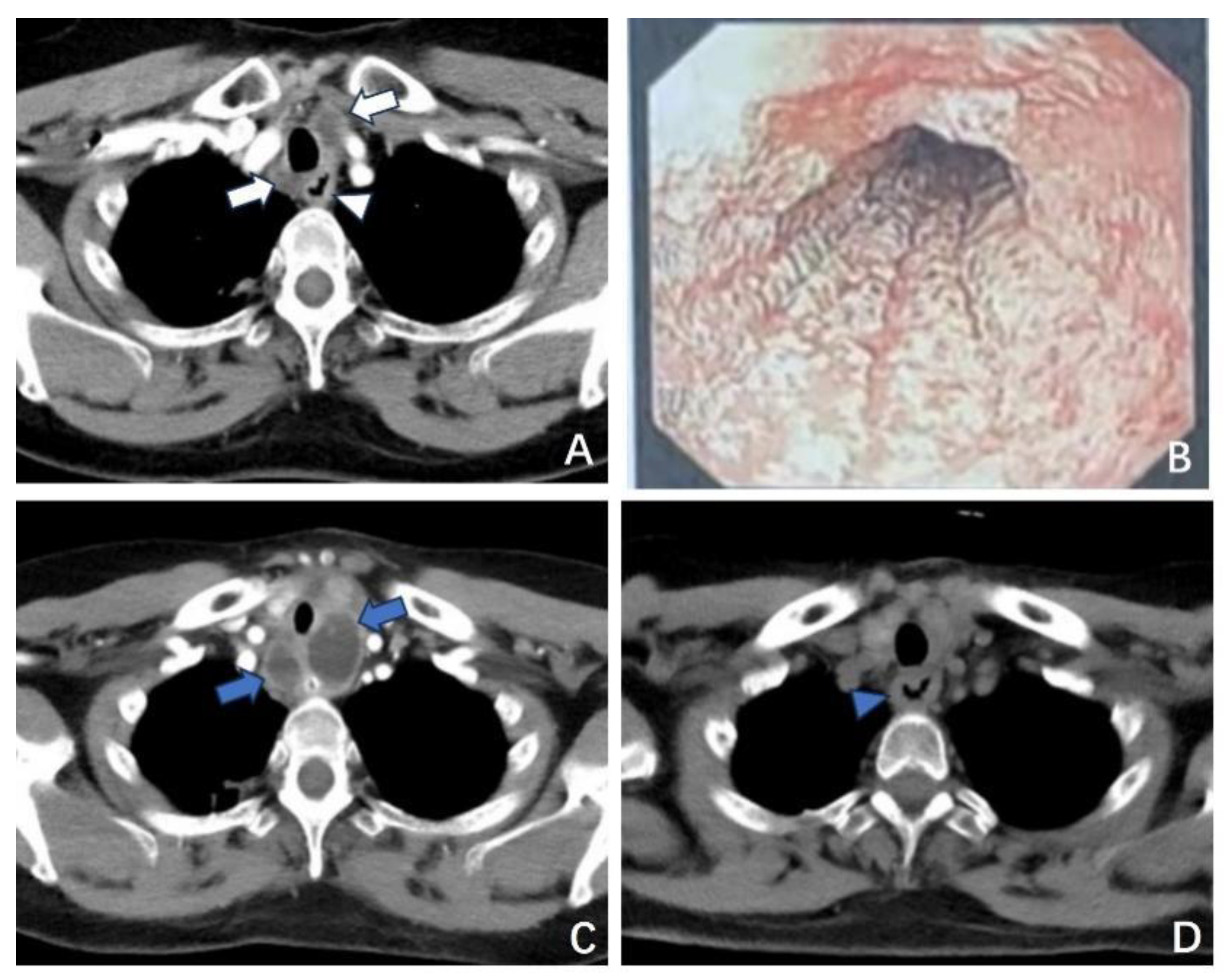

Table 1.
Patient characteristics.
| Site of Lesion | Total | % | |||||
|---|---|---|---|---|---|---|---|
| Larynx | Lymph node | Pharynx | Salivary | Multiple Sites | |||
| Total | 27(45.00%) | 20(33.33%) | 7(11.67%) | 3(5.00%) | 3(5.00%) | 60 | 100 |
| Sex | |||||||
| Male | 16 | 8 | 4 | 1 | 0 | 29 | 48.33 |
| Female | 11 | 12 | 3 | 2 | 3 | 31 | 51.67 |
| Age, yrs | |||||||
| <18 | 0 | 1 | 1 | 0 | 0 | 2 | 3.33 |
| 18-60 | 24 | 14 | 4 | 3 | 2 | 47 | 78,33 |
| >60 | 3 | 5 | 2 | 0 | 1 | 11 | 18.33 |
| Typical systemic symptoms | 4 | 10 | 3 | 0 | 0 | 17 | 28.33 |
| Comorbidities | 2 | 3 | 2 | 0 | 1 | 8 | 13.33 |
| Autoimmune diseases | 1 | 1 | 2 | 0 | 1 | 5 | 8.33 |
| Diabetes | 0 | 1 | 0 | 0 | 0 | 1 | 1.67 |
| Tumor | 1 | 1 | 0 | 0 | 0 | 2 | 3.33 |
| TB-spot | |||||||
| positive | 11 | 10 | 5 | 0 | 2 | 28 | 46.67 |
| negative | 2 | 1 | 0 | 1 | 0 | 4 | 6.67 |
| unidentified | 14 | 9 | 2 | 2 | 1 | 28 | 46.67 |
| Confirmed by biopsy | 12 | 16 | 4 | 3 | 2 | 37 | 61.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



