Submitted:
14 March 2025
Posted:
17 March 2025
You are already at the latest version
Abstract
Background: Emergency Departments (ED) are vital within the health system, often representing the first hospital contact for patients who are undifferentiated and may be critically ill. Although advancements in digital technology and increasing use of electronic medical records in health systems have led to the dramatic growth of large data sets, the presence of ED clinical registries in the literature is currently unknown. Objectives: Our scoping review aims to investigate the extent of emergency department clinical registries reported in peer-reviewed literature. Methods: We conducted a scoping review of ED registries in accordance with the PRISMA-ScR checklist. Searches were undertaken in PUBMED, EMBASE and SCOPUS. Studies were included if they described a clinical registry with a focus on the ED. Results: We identified 60 manuscripts with 27 identified as primary registries (6 had a general scope, 21 were condition or population specific). The remaining 33 papers were investigational reports sourced from the iden-tified primary registries. Funding sources were identified for some registries: 3 by re-search grants, 2 by medical colleges, 5 by government organizations or initiatives, 2 by pharmaceutical companies and 3 by research institutes. No funding information was provided in 12 studies. The reported registry periods ranged from 31 days to 4018 days (median 365 days, IQR 181-1309 days). A grey literature search revealed that 6 registries were ongoing. Conclusions: Internationally there appears to be a wide degree of het-erogeneity with primary ED registry publications and secondary publications. Inte-grating ED registries with a learning health system model will enable clinicians to serve their community proactively and with a focus on quality, rather than the current safe-ty-focused approach.
Keywords:
emergency department
; emergency medicine
; registries
; clinical quality registry
; safety
; quality
1. Introduction
Emergency Departments (ED) play a vital role within the health system, often representing the first point of hospital contact for patients who are undifferentiated and may be critically ill [1]. The ED manages a high volume of patients who range in acuity from the critically ill through to the worried well. This places a significant burden on ensuring timely diagnosis and management to avoid potentially avoidable adverse outcomes from care [2]. The ED is therefore a patient care environment that is highly vulnerable to the provision of low-quality care and breaches in patient safety [3]. The exponential growth of ED overcrowding creates further challenges to delivering standardised, high-quality care [4]. A variety of solutions have been developed to try and counter these challenges, including guidelines, policies, and pathways. Despite these best intentions, EDs remain significantly unsafe [5].
In recent years, advancements in digital technology and increasing use of electronic medical records in health systems have led to the dramatic growth in large clinical data sets. Harnessing this data to improve health care has taken on many forms and defined in different ways to include databases, audits and registries. Patient registries can be defined as an organized system that uses observational study methods to collect uniform data (clinical and other) to evaluate specified outcomes for a population defined by a particular disease, condition, or exposure, and that serves a predetermined scientific, clinical, or policy purpose(s) [6].
Clinical quality registries (CQRs) have emerged as a necessary approach to systematically collect, analyse and report information about the care and outcomes being delivered by health service organizations, and serve as a fundamental driver for ongoing improvements in the delivery of safe and high-quality care [7]. Mature CQRs such as the Australian and New Zealand Intensive Care Society Centre for Outcomes and Resources Evaluation (ANZICS CORE) have the capability to also shape health policy, integrate data through linkage projects and inform clinical practice in real-time whilst also providing infrastructure for measuring the translation of evidence into practice [8]. For emerging areas of health care, CQRs have been shown to be a catalyst to create clinical evidence for the development of best practice guidelines such as the Burns Registry of Australia and New Zealand [9]. Since care for many diseases and illnesses as well as the utilization of specific healthcare resources, such as Trauma teams, occur within the ED, the data reflecting the ED phase of care is being collected for these related CQRs. However, given the breadth and varied governance of these CQRs, ED staff often have little input into their methodology, maintenance, analysis and interpretation [2].
Clinical quality registries can be categorised across three broad areas: 1) Procedures, devices or drugs 2) Disease or illness or 3) Specific healthcare resource (table 1) [10]. Although there is no international repository for CQRs, country-level repositories do exist. The National Institutes of Health have a list of 81 registries and the Australian Commission on Safety and Quality in Health Care have developed the Australian Register of Clinical Registries which currently lists 125 CQRs [11,12].
Each CQR category present their own challenges for creating a registry. Potential barriers to constructing an informed ED registry include determining key quality outcome measures. On a more technical level, the volume and heterogeneity of patients and potential data points for collection, rapid turnover, heterogeneous data handling, storage and retrieval, rigorous national and state data privacy laws and institutional and jurisdictional requirements for data sharing agreements pose significant challenges to creating an ED registry [18]. Finally, the financial outlay for the significant infrastructure required to support an ED CQR can be a barrier. The aim of our scoping review is to explore the extent of ED clinical registries described in the peer review literature.
2. Methods
This scoping review was guided by the Joanna Briggs Institute methodology for scoping reviews and in compliance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) recommendations (supp. 1) [19,20]. The search protocol was developed by VT, GB and SP and objectives, search methods, and registry inclusion criteria were prespecified before the commencement of the study. This study did not require approval by an institutional ethical review board as no individual patient data were included and data regarding registries were publicly available. Preregistration of the study protocol was published in Inplasy (INPLASY202440119 - https://inplasy.com/inplasy-2024-4-0119) prior to commencement.
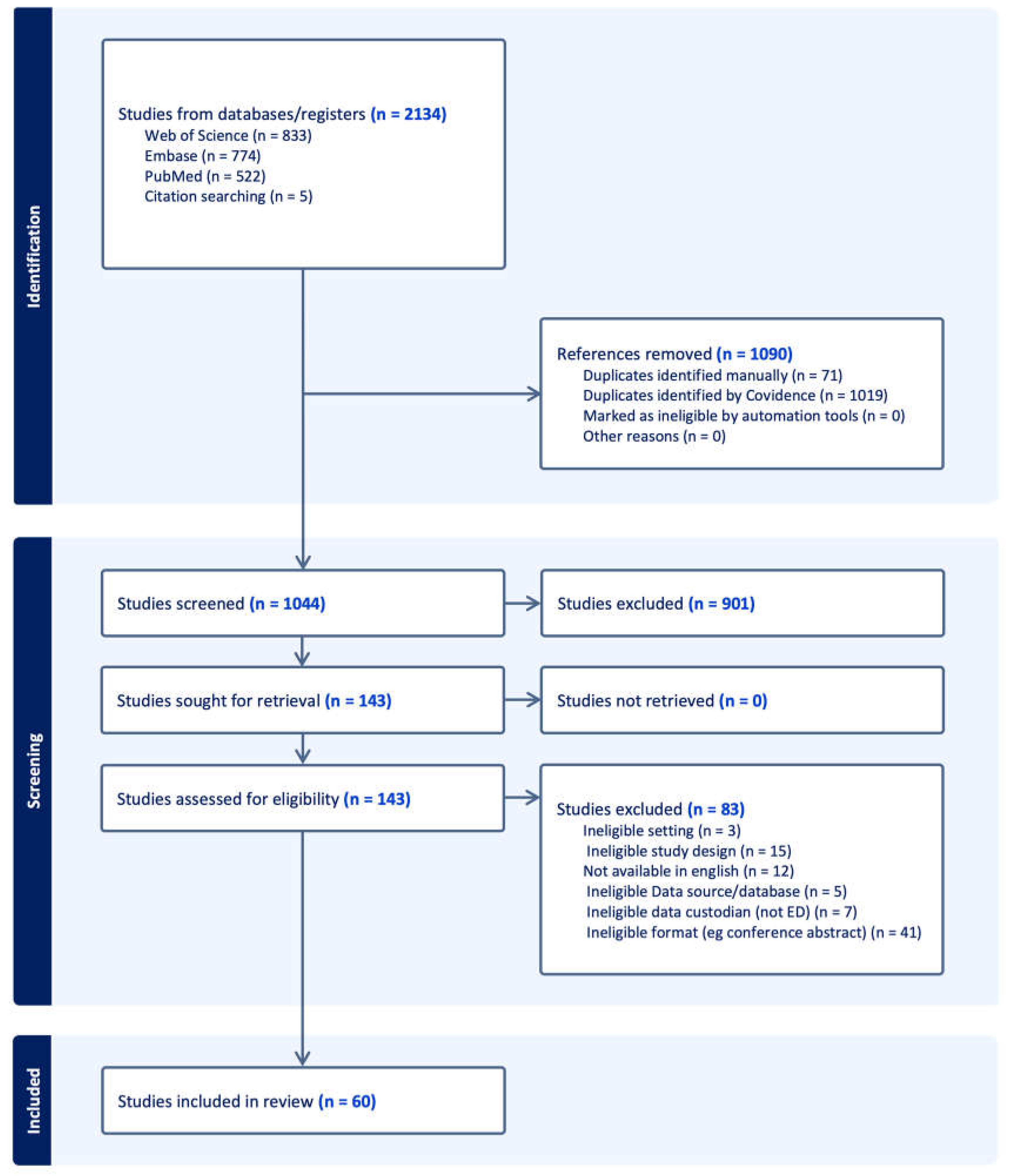
Figure 1.
PRISMA diagram summarizing the search strategy used to identify emergency department clinical quality registries meeting inclusion criteria.
Figure 1.
PRISMA diagram summarizing the search strategy used to identify emergency department clinical quality registries meeting inclusion criteria.
2.1. Eligibility Criteria
2.1.1. Inclusion Criteria
Full-text articles published in English describing ED registries were included. We defined an ED registry as a systematic data collection program (using a database, databank, or register) for monitoring standardised indicators of care quality (including safety) where ED care was the focus. Our inclusion and exclusion criteria only considered registries where the ED led the registry setup and maintenance. By having the ED as the lead department, it ensures that the most appropriate metrics are being measured to answer questions fundamental to the quality of care in the ED. Furthermore, ED staff will have the greatest understanding of the data, its interpretation but most importantly, its limitations [18]. Publications were included from protocol publication through to secondary analysis of registry data. Single-center, multicenter, regional, statewide, national, and multinational registries were also included.
2.1.2. Exclusion Criteria
Publications were excluded if they were developed for epidemiological disease monitoring without collection of clinical care indicators. Publications were also excluded if they were purely for administrative, system monitoring or financial purposes. Publications where the primary locus of care was not in the ED were excluded. Publications that were case reports, case series, narrative reviews, editorials, short communications, case studies or conference abstracts were also excluded. Non-human studies were also excluded.
2.2. Search Strategy
The search strategy (Appendix A) was developed in accordance with the Peer Review of Electronic Search Strategies (PRESS) criteria [21]. The following electronic databases were searched: National Library of Medicine via PubMed, Embase and Web of Science as a minimum requirement to guarantee adequate and efficient coverage [22]. The search period included date of database inception to April 2024.
The results of the database searches were screened using the web-based reviewing platform CovidenceTM (Veritas Health Innovation, Melbourne, Australia). Duplicate studies were removed. Title and abstract screening were performed independently by authors VT & GB where suitability for inclusion was assessed against the eligibility criteria. Following title and abstract screening, identified publications were retrieved and imported to CovidenceTM for full text review. Full text screening of all included publications was performed by authors VT & GB independently. Any disagreement between reviewers during screening of title and abstract or full text were resolved through discussion with a third review author (SP) on the study team.
For publications where it became apparent that they were referencing a registry, a search for the registry occurred using the name of the registry in the PUBMED database to identify the primary publication for that registry.
2.3. Data Extraction and Analysis
Data was extracted from included papers by authors VT and SP. Uncertainties or discrepancies were resolved through discussion with a third review author (GB). The data extraction template included funding source, trial number, type of registry, target demographic, population of interest, start and end dates for the registry, inclusion and exclusion criteria, data sources, collection tools, data entry procedures, number of participants included in the registry, availability of a data dictionary and data sharing arrangements, country of origin, number of participating EDs and ethical approvals.
Registries identified were categorised based on their scope as well as on the sequence in which they were published. For scope, ED registries were described as general if the inclusion criteria included all ED presentations and conditions, or condition or population specific if the data captured was restricted. For studies that identified an ED registry within the search strategy more than once, the oldest paper was considered the primary registry publication and subsequent papers as secondary publications (table 2).
Aims, objectives, results and conclusions were also extracted from publications to understand how registry data is being used. Included studies were not appraised for methodological quality or risk of bias as this is not customary for scoping reviews.
Data analysis included developing summary statistics and frequency counts. SP developed summary tables.
3. Results
3.1. Search Results
The initial literature search identified 2,134 publications (Fig. 1). After removal of 1,090 duplicates, 901 studies were not eligible based on title and abstract screening by two independent reviewers (VT and GB). Of the 143 full-text publications acquired and screened independently by VT and GB, a further 83 publications were excluded due to a variety of reasons described in the PRISMA flow diagram (Fig. 1), such as ineligible format (conference abstract) or ineligible data custodian (not an ED). As a result, 60 studies were eligible for review [23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83].

Table 2.
Count of ED clinical quality registries by type and scope of registry.
| Scope | Primary registry publications 1 | Secondary publications 2 |
|---|---|---|
| General | 6 | 2 |
| Condition or population specific | 21 | 31 |
1 The oldest paper where a registry was identified more than once. 2 Subsequent paper(s) where a registry was identified more than once.
3.2. Characteristics of Primary ED Registry Publications
Our scoping review yielded 27 registries that fit the inclusion criteria for a primary ED registry publications (table 2). Six of these registries were general ED registries. Three registries where specific to the same population, namely pediatrics. The remaining 18 registries were specific to a condition. Airways was the most common condition with 6 registries followed by 2 registries that covered different aspects of venous thromboembolism. The remaining ED registries addressed independenant conditions. The number of EDs involved in each registry varied from 1 to 889 (median 5.5, IQR 1-14). Country representaion included a total of 13 countries with USA the most frequently contributing with 8 registries (2 general, 6 specific) followed by Australia with 5 (1 general, 4 specific), Denmark 2 (2 general, 0 specific), Spain 4 (0 general, 4 specific) and New Zealand 2 (0 general, 2 specific). The reported registry periods ranged from 31 days to 4018 days (median 365 days, IQR 181-1309 days). Following a grey literature search of the 27 primary ED registry publications, 6 were found to be ongoing; 3 general, 2 airway specific and 1 paedatric specific. Distribution of these registries over time is shown in figure 2.
Table 3.
General characteristics of ED clinical quality registries.
| Registry | Date Range | Country/ies | Number of EDs 3 | Condition or population | Funding | Associated studies 2 | |
|---|---|---|---|---|---|---|---|
| Acute Admission Database | Barford, 2012 | 22-09-2009 to 28-02-2010 | Denmark | 1 | General | Hillerød Hospital research grant. | 0 |
| American College of Emergency Physicians Clinical Emergency Data Registry (CEDR) | Venkatesh, 2021 | 2017 1, 5 | USA | 889 | General | American College of Emergency Physicians | 0 |
| Centre des Urgences de Yaoundé (CURY) 4 | Jeong, 2022 | 01-2016 to 06-2018 1 | Africa | 1 | General | Korea International Cooperation Agency | 0 |
| Danish Database for Acute and Emergency Hospital Contacts (DDAEHC) | Lassen, 2016 | Not specified 5 | Denmark | 26 | General | Danish Regions. | 0 |
| Swedish Emergency Registry (SVAR) | Ekelund, 2011 | 01-01-2009 to 30-06-2009 1, 5 | Sweden | 6 | General | Region Skåne, the Stockholm County Council and the Swedish Association of Local Authorities and Regions. | 1 |
| The Registry for Emergency Care (REC) | O’Reilly, 2020 | Not specified | Australia | 1 | General | No funding acknowledged. | 1 |
| Cleveland Clinic Emergency Airway Registry 4 | Phelan, 2010 | 01-07-2005 to 31-03-2007 | USA | 1 | Airway | No funding acknowledged. | 0 |
| Australia and New Zealand Emergency Department Airway Registry (ANZEDAR) | Fogg, 2016 | 01-04-2010 to 30-03-2014 5 | Australia | 1 | Airway | Emergency Care Institute research funding scheme. | 3 |
| Defense Registry for Emergency Airway Management (DREAM) | Mendez, 2021 | 01-2020 to 07-2020 1 | USA | 1 | Airway | No funding acknowledged. | 0 |
| Korean Emergency Airway Management Registry (KEAMR) | Choi, 2021 | 03-2006 to 12-2010 1 | Korea | 13 | Airway | No funding acknowledged. | 2 |
| National Emergency Airway Registry (NEAR) | Brown, 2015 | 01-07-2002 to 31-12-2012 5 | USA, Australia, Canada | 13 | Airway | No funding acknowledged. | 19 |
| South African Emergency Department Airway Registry 4 | Hart, 2020 | 01-09-2015 to 31-10-2016 1 | South Africa | 1 | Airway | No funding acknowledged. | 0 |
| Children's Injury Database (CID) | McCain, 2023 | 2021 1 | USA | 1 | Pediatric | No funding acknowledged. | 0 |
| Nicaragua Pediatric Emergency Registry 4 | Bressan, 2021 | 01-01-2017 to 31-12-2017 1 | Nicaragua | 7 | Pediatric | Regione Lombardia and the Associazione il Bambino Nefropatico | 0 |
| The Pediatric Emergency Care Applied Research Network Registry (PECARN) | Sara, 2018 | 01-2012 to 06-2016 1, 5 | USA | 7 | Pediatric | Agency for Healthcare Research and Quality 6. | 0 |
| Emergency Medicine Pulmonary Embolism in the Real World Registry (EMPORER) | Pollack, 2011 | 01-01-2005 to 29-12-2008 | USA | 22 | Acute pulmonary embolism | GlaxoSmithKline. | 1 |
| Risk Profile of Patients VTED Attended in Spanish Emergency Departments Registry (ESPHERIA) | Jimenez, 2017 | 13-10-2014 to 14-12-2014 1 | Spain | 53 | Venous thromboembolism | Bayer Hispania. | 1 |
| Emergency Atrial Fibrillation Registry of the Catalan Institute of Health (URGFAICS) | Jacob, 2019 | 09-2016 to 02-2017 1 | Spain | 5 | Atrial fibrillation | No funding acknowledged. | 1 |
| Epidemiology of Acute Heart Failure in Emergency Departments Registry (EAHFE) | Llorens, 2015 | 15-03 to 15-05-2007; 01-06 to 30-06-2009;07-11-2011 to 07-01-2012 | Spain | 29 | Heart failure | Partially funded by the Institute of Health. | 2 |
| Acute Epileptic Seizures in the Emergency Department Registry (ACESUR) | Alonso, 2019 | 01-02-2017 to 31-10-2017 | Spain | 18 | Acute epileptic seizures | No funding acknowledged. | 0 |
| Ain Shams University Hospital Trauma Registry 4 | Khalil, 2021 | 01-2017 to 12-2017 | Egypt | 1 | Trauma | Fogarty Institute in USA. | 0 |
| Auckland City Hospital Emergency Department Overdose Database | Theron, 2017 | 2002 to 2004 1 | New Zealand | 1 | Overdose | No funding acknowledged. | 0 |
| Emergency Medicine Events Register (EMER) | Hansen, 2016 | 12-2012 to 02-2015 1 | Australia, New Zealand | 21 | Safety incidents | Australasian College for Emergency Medicine | 0 |
| Procedural Sedation in the Community Emergency Department Registry (ProSCED) | Sacchetti, 2007 | 01-01-2003 to 04-03-2006 1 | USA | 14 | Procedural sedation | No funding acknowledged. | 1 |
| Singapore Head Injury Database 4 | Chong, 2015 | 01-2006 to 06-2014 1 | Singapore | 1 | Pediatric head injury | Pediatrics Academic Clinical Program, Singapore. | 0 |
| The Sepsis Registry 4 | Williams, 2011 | Not specified | Australia | 1 | Sepsis | Queensland Emergency Medicine Research Foundation. | 0 |
| VNICat (NIVCat in English) | Jacob, 2017 | 02-2015 to 03-2015 1 | Spain | 8 | Non-invasive mechanical ventilation | No funding acknowledged. | 1 |
1 No specific day and/or month described in the methodology. 2 Found with the original search strategy. 3 Based on the most recent publication identified in the search strategy. 4 A name for the registry not mentioned in the manuscript. 5 Registry ongoing. 6 The PECARN infrastructure was supported by the Health Resources and Services Administration (HRSA), the Maternal and Child Health Bureau (MCHB), and the Emergency Medical Services for Children (EMSC) Network Development Demonstration Program.
3.3. Funding for Primary ED Registry Publications
For registries where funding was acknowledged, 3 were funded by research grants, 2 by medical colleges, 5 by government organisations or initatives, 2 by pharmaceutical companies and 3 by research institutes. For registries identified as ongoing (figure 2), sources of funding were identified as medical college for 1 registry, government organisation or initaitive for 3 registries, research grants for 1 registry and no funding acknoweldged for 1 registry. Twelve of the 27 primary ED registry publications did not acknowledge any funding for the registries described. The funding amount was not described for any of the studies.
3.4. Aims, Results and Conclusion in Primary ED Registry Publications with a General Scope
Aims, results and conclusions for primary ED registry publications with a general scope provided insight into the breadth of each manuscript (table 4). Three publications focused on registry methodology, feasability and evaluation, while 2 described its use for performance measurements and one described its use for measuring the quality of clinical care.
For publications that focused on registry methdology, feasbility and evaluation, 2 concluded that creating a registry and evaluating a pilot project was feasible, with the other describing methdology without acknowledging feasability. One paper also described a desire to expand the dataset to include non-ED metrics, another described the potential for use in quality improvement and the last described expansion to additional EDs.
Lassen et al was the only general primary ED registry publication that described the evaluation of quality of clinical care. Notably this registry included specicific outcomes and process health care quality indicators. Performance measures in the ED are often represented by time-based targets including length of time in the ED and time awaiting medical review. Two general ED registries described the use of a registry to inform these performance measures, although one paper was simply the protocol.
3.5. Aims, Results and Conclusion in Primary ED Registry Publications Specific for a Condition or Population
Aims, results and conclusions for primary ED registry publications specific for a condition or population provided insight into the scope of each manuscript (supp. 2). Unlike general scope primary ED registry publications, condition specific primary ED registry publications focused on clinical quality including evaluating or benchmarking against standards. The only population specific registries were for pediatrics and these were similar to general scope primary ED registry publications focusing on registry methodology, feasability and evaluation.
3.6. Aims, Results and Conclusion in Secondary Publications
Of the 27 primary ED registry publications, 16 did not have a secondary study (table 3). Of those that did have secondary publications, the median number of studies was 1 (IQR 1-2). Two general ED registries each had 1 secondary publication while 24 secondary publications were identified for all airway specific registries with the NEAR registry accompanied by 19 assocaited studies (table 3).
Aims, results and conclusions for secondary publications were similar to their primary ED registry publications (supp. 3). Secondary publications with a focus on specific conditions reported on clinical quality through a variety of means. Including benchmarking and describing trends in practice. Secondary publications with a general scope reported on performance indicators in the form of time-based performance.
4. Discussion
Emergency Departments are often tasked with managing a high proportion of undifferentiated patients who range from the critically ill through to the worried well [2]. This combination of undifferentiated and unwell patients places a significant burden on ensuring timely diagnosis and management to avoid significant adverse outcomes from care [2]. Clinical registries are focused on the quality of health care within specific clinical domains by systematically analyzing health-related data for an eligible population and serves as an efficient approach to the assessment of quality care in the ED setting [7]. This scoping review sought to understand the current use of ED registries.
4.1. Emergency Department Registries Reported in the Literature
Our review identified 27 primary ED registry publications, representing a diverse range of focuses and geographical representations. Notably, most registries were condition-specific, with airway being by far the most common condition studied (33.3% of all condition-specific primary ED registry publications). This may represent the fact that airway management in the ED setting is of critical importance [84]. It may also be that there are more reproducible clinical quality measures within the process of airway management in this setting [84]. The reality is likely to be multifactorial but suggests that airway registries may be more feasible at a local level and therefore individual EDs or networks of EDs could consider establishing or contributing to an ED airway registry to pilot the creation of a registry in the ED. This process would assist in understanding the technical requirements as well as local ethical, governance and data sharing requirements prior to embarking on a larger registry.
Whereas condition or population specific ED registries offer an easier approach to understanding the infrastructure needs for local registry set up and maintenance, general ED registries serve a broader purpose given the general nature of emergency medicine as a specialty and the need to interrogate many aspects of this heterogenous patient population. The difference between condition or population specific registries and general registries is therefore vastly different and requires a significantly higher investment both financially and administratively. All the general ED registries included in our search strategy utilized a largely administrative data set. This appears to be the most practical approach for developing general ED registries although has its limitations in terms of largely performance data in the form of time-based targets. A natural evolution should involve the inclusion of clinical data to shift the analysis to clinical care and patient centred outcomes. How clinical data is linked to administrative data and what clinical data should be prioritised for capture are all considerations that will require further research or consensus [18].
4.2. Emergency Department Registry Scope
The analysis of primary ED registry publications specific to conditions or populations revealed distinct trends and focuses compared to general scope primary ED registry publications. Condition-specific registries predominantly emphasized clinical quality, often through evaluation and benchmarking against established standards. This focus on clinical quality underscores the importance of these registries in enhancing patient care and outcomes by providing a framework for continuous improvement and adherence to best practices.
In contrast, the only population-specific registries identified were those targeting paediatric populations. These registries shared similarities with general scope primary ED registry publications, particularly in their emphasis on registry methodology, feasibility, and evaluation. This alignment suggests that while the target population may differ, the foundational principles guiding the development and implementation of these registries remain consistent.
Our scoping review describes a largely heterogenous set of ED registries. As a result of this, quality indicators were not well described. To enhance the selection of quality indicators, it would be advantageous to adopt a stakeholder-driven approach. This approach should prioritize the values of patients and communities, as well as the actionable improvement priorities identified by healthcare providers. Additionally, there should be a greater emphasis on measuring distinct and discernible processes of care [85].
4.3. Temporal Scope of Emergency Department Registries
Most registries were time-limited, with a median duration of one year (0.05-3.59 years). A grey search of all primary ED registry publications recognized 6 of these registries as ongoing, 3 of which are general ED registries. This time limitation may exist for a variety of reasons. It may reflect the challenges associated with sustaining long-term registry efforts, including funding, data collection, and maintenance. A more plausible explanation is that researchers using the term registry interchangeably with traditional data collection tools for audit or research and databases that do not meet the criteria of a registry [6].
4.4. Funding source for Emergency Department Registries
Health economic studies have demonstrated that relatively small injections of funding to supplement existing efforts at creating and maintaining a clinical registry is likely to be highly cost effective [86,87]. The funding sources described for the registries identified was varied, ranging from hospital-based funding to government organizations and pharmaceutical companies. Nearly half of the registries did not acknowledge any funding, which raises questions about the sustainability and potential biases in the data collection processes. For the registries that did report funding, government organizations and research institutes were the most common sources.
None of the studies reported amount of funding provided for either registry related costs or study related costs. Future studies should aim to provide more transparency in funding to better understand the resources required for developing, maintaining and interrogating registry data.
4.5. ED Registries as a Catalyst for Further Publications
The examination of secondary publications reveals the impact and scope of these registries. Of the 27 primary ED registry publications analyzed, 16 did not have any secondary publications, highlighting a potential area for future research and exploration. Some non-ED registries such as the Australian Trauma Registry have been successful with more abundant reporting with over 14 secondary publications since the registry started in 2012 [88]. One hypothesis includes the lack of ongoing funding to support such endeavours. For those registries with secondary publications, the median number of studies was relatively low, with a median of 1 (IQR 1-2). This finding suggests that while some registries are actively contributing to the research landscape, there is significant room for expansion and the barriers for these should be explored.
Interestingly, the NEAR registry, an airway-specific registry, stood out with 19 secondary publications, indicating a robust research output and a strong focus on airway management within the ED context. This contrasts with the general ED registries, which had fewer secondary publications. The secondary publications for condition-specific registries primarily reported on clinical quality through various means, including benchmarking and trend analysis.
4.6. ED Registries as a Catalyst for Quality –A Piece of the Learning Health System Puzzle?
Registries themselves serve as a rich source of data and on its own serves no other purpose. It is up to organizations and clinicians to utilize this data to deliver these quality initiatives. Although quality and safety are often used in the same phrase, the current driver for enhancing care prioritizes the delivery of safe (rather than quality) care. In the context of resource poor services, the result of this focus is a system that is reactive without the opportunity or resources to focus on quality. Learning health systems (LHSs) have emerged as a popular concept to bring focus back on quality through a standardized framework [89]. The Institute of Medicine coined the term Learning Health System (LHS) in 2007, describing it as a health system where “science, informatics, incentives, and culture are aligned for continuous improvement and innovation, with best practices seamlessly embedded in the care process, patients and families active participants in all elements, and new knowledge captured as an integral by-product of the care experience” [89]. Although there is debate around a specific definition for an LHS, a review of bibliometric trends for LHSs found a large degree of convergence describing LHSs as ‘achieving healthcare quality improvement by using big data and embedding data analysis and intelligent decision-making into routine care delivery processes’ [90]. A fundamental requirement for this system to work, and indeed any quality improvement strategy, relies on the availability of data relevant to the quality being evaluated. The appeal of registries in the ED setting is that quality can be truly assessed on a broad level compared with current ad hoc strategies that realistically result in no evaluation and thereof limited understanding of the true quality of care being delivered.
5. Limitations
There are several limitations to this review. The search strategy used terms in English. Our search strategy was limited to publications and therefore excludes registries that were operationalised without any publications (eg local quality improvement or annual reports not published in the peer review literature). We retrospectively searched the grey literature where a registry that fulfilled the inclusion criteria was identified but was not the primary paper. One example of this is the World Health Organization’s clinical registry tool, a web-based platform for aggregation and analysis of case-based data from emergency care visits [91]. Most health service quality improvement projects and evaluations are contained within the service itself and therefore initiatives generated from registry data is not able to be quantified unless published in the peer review literature.
Some countries adopted a whole of health system approach for clinical quality registries based around innovative implementation of health information management technology. Emergency Department subsets of these large registries were excluded from our search strategy as they were not considered a feasible approach for many clinicians and clinician researchers considering developing and implementing an ED registry.
6. Conclusions
The use of clinical registries for quality improvement and research has grown significantly and will continue to do so with advancements in information technology. Whilst many registries are used to evaluate and enhance the quality of care provided, the chaotic nature of EDs has been overlooked. From our scoping review, internationally there appears to be a lack of published registries and secondary publications. Of those that do exist, ED based airway registries have been the most abundant and can potentially serve as a ‘pilot’ registry for departments to understand capacity and capability for managing and using registry data. The development of general ED registries offers the potential to assess the quality of care provided. Integrating these registries with a learning health system model will enable clinicians to serve their community proactively and with a focus on quality, rather than the current reactive and safety-focused approach.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist.; Table S2: Aims, results and conclusion of primary ED registry publications specific for a condition or population.; Table S3: Aims, results and conclusion of studies secondary publications (both general scope and specific for a condition or population).
Author Contributions
Conceptualization, V.T.; methodology, V.T., S.P. and G.B.; formal analysis, V.T., S.P.; investigation, V.T., S.P. and G.B; resources, V.T., S.P. and G.B; data curation, V.T., S.P. and G.B; writing—original draft preparation, V.T.; writing—review and editing, V.T., S.P. and G.B; visualization, V.T.; supervision, V.T.; project administration, G.B.; funding acquisition, V.T., S.P. and G.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research and the APC was funded by the Medical Research Future Fund (MRFF), grant number MRF2018041.
Institutional Review Board Statement
Ethical review and approval was not sought as they are not applicable for scoping reviews.
Informed Consent Statement
Patient consent is not required for scoping reviews.
Data Availability Statement
The original contributions presented in the study are included in the publication/supplementary material, further inquiries can be directed to the corresponding author/s.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A. Search Strategy
The following electronic databases were searched: National Library of Medicine via PubMed, Embase and Web of Science as a minimum requirement to guarantee adequate and efficient coverage (Table A1) [22]. The search period included date of database inception to April 2024. For all databases, only publications in English and where full text was available were included.
For the National Library of Medicine, the PubMed Central search field query entered was: (((registry[Title]) OR register[Title]) OR database[Title]) AND emergency[Title]. For embase, we used emtree terms ; ‘registry’ or ‘register’ or ‘database’ combined with the MeSH terms referring to ‘emergency ward’ or ‘emergency medicine’ or ‘emergency care’. For the Web of Science we searched in “All Databases”, “All” collections, document type ‘article’, language English, . We used the search terms: (((SO=(emergency)) AND SO=(registry)) OR SO=(register)) OR SO=(database).
Medical Subject Headings (MeSH), ‘registries’ or ‘database’ AND ‘emergency medicine’ or ‘emergency room visits’ or ‘emergency medical service’ or ‘evidence based emergency medicine’.
Table A1.
Detailed search strategy for PubMed, Embase and Web of Science.
| Search Query | ||
|---|---|---|
| All databases | Full text available; English language | |
| PubMed | ((Emergency [Title]) AND (Registry [Title] OR Register[Title] OR Database[Title])) | |
| Embase | ((Emergency.ti.) AND (Registry.ti. OR Register.ti. OR Database.ti.)) | |
| Web of Science | (TI=(Emergency) AND (TI=(Registry) OR TI=(Register) OR TI=(Database))) |
References
- Trzeciak, S.; Rivers, E.P. Emergency department overcrowding in the United States: an emerging threat to patient safety and public health. Emerg Med J 2003, 20, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Tran, V.; Barrington, G.; Page, S. The Tasmanian Emergency Care Outcomes Registry (TECOR) Protocol. Emerg Care Med 2024, 1, 153–164. [Google Scholar] [CrossRef]
- Schneider, S.M.; Gardner, A.F.; Weiss, L.D.; Wood, J.P.; Ybarra, M.; Beck, D.M.; Stauffer, A.R.; Wilkerson, D.; Brabson, T.; Jennings, A.; et al. The future of emergency medicine. J Emerg Nurs 2010, 36, 330–335. [Google Scholar] [CrossRef]
- Sprivulis, P.C.; Da Silva, J.-A.; Jacobs, I.G.; Frazer, A.R.L.; Jelinek, G.A. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. MJA 2006, 184, 616–616. [Google Scholar] [CrossRef]
- Ramlakhan, S.; Qayyum, H.; Burke, D.; Brown, R. The safety of emergency medicine. Emerg Med J 2016, 33, 293–299. [Google Scholar] [CrossRef]
- Gliklich, R.E.; Dreyer, N.A.; Leavy, M.B. AHRQ Methods for Effective Health Care. In Registries for Evaluating Patient Outcomes: A User's Guide, Gliklich, R.E., Dreyer, N.A., Leavy, M.B., Eds.; Agency for Healthcare Research and Quality (US): Rockville (MD), 2014. [Google Scholar]
- Evans, S.M.; Scott, I.A.; Johnson, N.P.; Cameron, P.A.; McNeil, J.J. Development of clinical-quality registries in Australia: the way forward. Med J Aust 2011, 194, 360–363. [Google Scholar] [CrossRef]
- Secombe, P.; Millar, J.; Litton, E.; Chavan, S.; Hensman, T.; Hart, G.K.; Slater, A.; Herkes, R.; Huckson, S.; Pilcher, D.V. Thirty years of ANZICS CORE: A clinical quality success story. Crit Care Resusc 2023, 25, 43–46. [Google Scholar] [CrossRef]
- Gong, J.; Singer, Y.; Cleland, H.; Wood, F.; Cameron, P.; Tracy, L.M.; Gabbe, B.J. Driving improved burns care and patient outcomes through clinical registry data: A review of quality indicators in the Burns Registry of Australia and New Zealand. Burns 2021, 47, 14–24. [Google Scholar] [CrossRef]
- Australian Commission On Safety And Quality In Health Care. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/australian-framework-national-clinical-quality-registries-2024 (accessed on 6 March 2025).
- Australian Commission On Safety And Quality In Health Care. Australian Register of Clinical Registries. Available online: https://www.safetyandquality.gov.au/publications-and-resources/australian-register-clinical-registries (accessed on 27 March 2024).
- National Institutes of Health. List of Registries. Available online: https://www.nih.gov/health-information/nih-clinical-research-trials-you/list-registries (accessed on December 11, 2024).
- Etkin, C.D.; Springer, B.D. The American Joint Replacement Registry—the first 5 years. Arthroplasty Today 2017, 3, 67–69. [Google Scholar] [CrossRef]
- Gómez-Bueno, M.; Pérez de la Sota, E.; Forteza Gil, A.; Ortiz-Berbel, D.; Castrodeza, J.; García-Cosío Carmena, M.D.; Barge-Caballero, E.; Rangel Sousa, D.; Díaz Molina, B.; Manrique Antón, R.; et al. Durable ventricular assist device in Spain (2007-2020). First report of the REGALAD registry. Rev Esp Cardiol (Engl Ed) 2023, 76, 227–237. [Google Scholar] [CrossRef]
- Wennergren, D.; Ekholm, C.; Sandelin, A.; Möller, M. The Swedish fracture register: 103,000 fractures registered. BMC Musculoskelet Disord 2015, 16. [Google Scholar] [CrossRef]
- Cadilhac, D.A.; Kim, J.; Lannin, N.A.; Kapral, M.K.; Schwamm, L.H.; Dennis, M.S.; Norrving, B.; Meretoja, A. National stroke registries for monitoring and improving the quality of hospital care: A systematic review. Int. J. Stroke 2015, 11, 28–40. [Google Scholar] [CrossRef]
- Cameron, P.A.; Fitzgerald, M.C.; Curtis, K.; McKie, E.; Gabbe, B.; Earnest, A.; Christey, G.; Clarke, C.; Crozier, J.; Dinh, M.; et al. Over view of major traumatic injury in Australia––Implications for trauma system design. Injury 2020, 51, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Craig, S.; O'Reilly, G.M.; Egerton-Warburton, D.; Jones, P.; Than, M.P.; Tran, V.; Taniar, D.; Moore, K.; Alvandi, A.; Tuxen-Vu, J.; et al. Making the most of what we have: What does the future hold for Emergency Department data? Emerg Med Australas 2024, 36, 795–798. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiology 2016, 75, 40–46. [Google Scholar] [CrossRef]
- Bramer, W.M.; Rethlefsen, M.L.; Kleijnen, J.; Franco, O.H. Optimal database combinations for literature searches in systematic reviews: a prospective exploratory study. Syst Rev 2017, 6. [Google Scholar] [CrossRef]
- Williams, J.M.; Greenslade, J.H.; McKenzie, J.V.; Chu, K.H.; Brown, A.; Paterson, D.; Lipman, J. A prospective registry of emergency department patients admitted with infection. BMC Infect Dis 2011, 11, 27. [Google Scholar] [CrossRef]
- Venkatesh, A.; Ravi, S.; Rothenberg, C.; Kinsman, J.; Sun, J.; Goyal, P.; Augustine, J.; Epstein, S.K. Fair Play: Application of Normalized Scoring to Emergency Department Throughput Quality Measures in a National Registry. Ann Emerg Med 2021, 77, 501–510. [Google Scholar] [CrossRef]
- Van Oeveren, L.; Donner, J.; Fantegrossi, A.; Mohr, N.M.; Brown, C.A., 3rd. Telemedicine-Assisted Intubation in Rural Emergency Departments: A National Emergency Airway Registry Study. Telemed J E Health 2017, 23, 290–297. [Google Scholar] [CrossRef]
- Trent, S.A.; Kaji, A.H.; Carlson, J.N.; McCormick, T.; Haukoos, J.S.; Brown, C.A., 3rd. Video Laryngoscopy Is Associated With First-Pass Success in Emergency Department Intubations for Trauma Patients: A Propensity Score Matched Analysis of the National Emergency Airway Registry. Ann Emerg Med 2021, 78, 708–719. [Google Scholar] [CrossRef] [PubMed]
- Theron, L.; Jansen, K.; Miles, J. Benzylpiperizine-based party pills' impact on the Auckland City Hospital Emergency Department Overdose Database (2002-2004) compared with ecstasy (MDMA or methylene dioxymethamphetamine), gamma hydroxybutyrate (GHB), amphetamines, cocaine, and alcohol. N Z Med J 2007, 120, U2416. [Google Scholar] [PubMed]
- Stoecklein, H.H.; Kelly, C.; Kaji, A.H.; Fantegrossi, A.; Carlson, M.; Fix, M.L.; Madsen, T.; Walls, R.M.; Brown, C.A., 3rd. Multicenter Comparison of Nonsupine Versus Supine Positioning During Intubation in the Emergency Department: A National Emergency Airway Registry (NEAR) Study. Acad Emerg Med 2019, 26, 1144–1151. [Google Scholar] [CrossRef]
- Sandefur, B.J.; Liu, X.W.; Kaji, A.H.; Campbell, R.L.; Driver, B.E.; Walls, R.M.; Carlson, J.N.; Brown, C.A., 3rd. Emergency Department Intubations in Patients With Angioedema: A Report from the National Emergency Airway Registry. J Emerg Med 2021, 61, 481–488. [Google Scholar] [CrossRef]
- Sacchetti, A.; Senula, G.; Strickland, J.; Dubin, R. Procedural sedation in the community emergency department: initial results of the ProSCED registry. Acad Emerg Med 2007, 14, 41–46. [Google Scholar] [CrossRef]
- Sacchetti, A.; Stander, E.; Ferguson, N.; Maniar, G.; Valko, P. Pediatric Procedural Sedation in the Community Emergency Department: results from the ProSCED registry. Pediatr Emerg Care 2007, 23, 218–222. [Google Scholar] [CrossRef]
- Ruderman, B.T.; Mali, M.; Kaji, A.H.; Kilgo, R.; Watts, S.; Wells, R.; Limkakeng, A.T.; Borawski, J.B.; Fantegrossi, A.E.; Walls, R.M.; et al. Direct vs Video Laryngoscopy for Difficult Airway Patients in the Emergency Department: A National Emergency Airway Registry Study. West J Emerg Med 2022, 23, 706–715. [Google Scholar] [CrossRef]
- Pollack, C.V.; Schreiber, D.; Goldhaber, S.Z.; Slattery, D.; Fanikos, J.; O'Neil, B.J.; Thompson, J.R.; Hiestand, B.; Briese, B.A.; Pendleton, R.C.; et al. Clinical characteristics, management, and outcomes of patients diagnosed with acute pulmonary embolism in the emergency department: initial report of EMPEROR (Multicenter Emergency Medicine Pulmonary Embolism in the Real World Registry). J Am Coll Cardiol 2011, 57, 700–706. [Google Scholar] [CrossRef]
- Phelan, M.P.; Glauser, J.; Yuen, H.W.; Sturges-Smith, E.; Schrump, S.E. Airway registry: a performance improvement surveillance project of emergency department airway management. Am J Med Qual 2010, 25, 346–350. [Google Scholar] [CrossRef]
- Pediat Emergency Care Appl, R.; Davies, S.J.D.; Grundmeier, R.W.; Campos, D.A.; Hayes, K.L.; Bell, J.; Alessandrini, E.A.; Bajaj, L.; Chamberlain, J.M.; Gorelick, M.H.; et al. The Pediatric Emergency Care Applied Research Network Registry: A Multicentre Electronic Health Record Registry of Pediatric Emergency Care. Appl Clin Inform 2018, 9, 366–376. [Google Scholar] [CrossRef]
- Pallin, D.J.; Dwyer, R.C.; Walls, R.M.; Brown, C.A., 3rd. Techniques and Trends, Success Rates, and Adverse Events in Emergency Department Pediatric Intubations: A Report From the National Emergency Airway Registry. Ann Emerg Med 2016, 67, 610–615.e611. [Google Scholar] [CrossRef] [PubMed]
- Otto, R.; Blaschke, S.; Schirrmeister, W.; Drynda, S.; Walcher, F.; Greiner, F. Length of stay as quality indicator in emergency departments: analysis of determinants in the German Emergency Department Data Registry (AKTIN registry). Intern Emerg Med 2022, 17, 1199–1209. [Google Scholar] [CrossRef] [PubMed]
- Offenbacher, J.; Nikolla, D.A.; Carlson, J.N.; Smith, S.W.; Genes, N.; Boatright, D.H.; Brown, C.A., 3rd. Incidence of rescue surgical airways after attempted orotracheal intubation in the emergency department: A National Emergency Airway Registry (NEAR) Study. Am J Emerg Med 2023, 68, 22–27. [Google Scholar] [CrossRef]
- O'Reilly, G.M.; Mitchell, R.D.; Mitra, B.; Noonan, M.P.; Hiller, R.; Brichko, L.; Luckhoff, C.; Paton, A.; Smit, V.; Cameron, P.A. Impact of patient isolation on emergency department length of stay: A retrospective cohort study using the Registry for Emergency Care. Emerg Med Australas 2020, 32, 1034–1039. [Google Scholar] [CrossRef]
- Nikolla, D.A.; Offenbacher, J.; Smith, S.W.; Genes, N.G.; Herrera, O.A.; Carlson, J.N.; Brown, C.A., 3rd. First-Attempt Success Between Anatomically and Physiologically Difficult Airways in the National Emergency Airway Registry. Anesth Analg 2024. [Google Scholar] [CrossRef]
- Miró, Ò.; Martínez, G.; Masip, J.; Gil, V.; Martín-Sánchez, F.J.; Llorens, P.; Herrero-Puente, P.; Sánchez, C.; Richard, F.; Lucas-Invernón, J.; et al. Effects on short term outcome of non-invasive ventilation use in the emergency department to treat patients with acute heart failure: A propensity score-based analysis of the EAHFE Registry. Eur J Intern Med 2018, 53, 45–51. [Google Scholar] [CrossRef]
- Miró, Ò.; Llorens, P.; Freund, Y.; Davison, B.; Takagi, K.; Herrero-Puente, P.; Jacob, J.; Martín-Sánchez, F.J.; Gil, V.; Rosselló, X.; et al. Early intravenous nitroglycerin use in prehospital setting and in the emergency department to treat patients with acute heart failure: Insights from the EAHFE Spanish registry. Int J Cardiol 2021, 344, 127–134. [Google Scholar] [CrossRef]
- Mendez, J.; Escandon, M.; Tapia, A.D.; Davis, W.T.; April, M.D.; Maddry, J.K.; Couperus, K.; Hu, J.S.; Chin, E.; Schauer, S.G. Development of the Defense Registry for Emergency Airway Management (DREAM). Med J (Ft Sam Houst Tex) 2021, 93–97. [Google Scholar]
- McCain, J.E.; Bridgmon, A.E.; King, W.D.; Monroe, K. Children's injury database: development of an injury surveillance system in a pediatric emergency department. Inj Epidemiol 2023, 10, 40. [Google Scholar] [CrossRef]
- Llorens, P.; Escoda, R.; Miró, Ò.; Herrero-Puente, P.; Martín-Sánchez, F.J.; Jacob, J.; Garrido, J.M.; Pérez-Durá, M.J.; Gil, C.; Fuentes, M.; et al. Characteristics and clinical course of patients with acute heart failure and the therapeutic measures applied in Spanish emergency departments: based on the EAHFE registry (Epidemiology of Acute Heart Failure in Emergency Departments). Emergencias 2015, 27, 11–22. [Google Scholar] [PubMed]
- Lin, B.W.; Schreiber, D.H.; Liu, G.; Briese, B.; Hiestand, B.; Slattery, D.; Kline, J.A.; Goldhaber, S.Z.; Pollack, C.V. Therapy and outcomes in massive pulmonary embolism from the Emergency Medicine Pulmonary Embolism in the Real World Registry. Am J Emerg Med 2012, 30, 1774–1781. [Google Scholar] [CrossRef] [PubMed]
- Lembersky, O.; Golz, D.; Kramer, C.; Fantegrossi, A.; Carlson, J.N.; Walls, R.M.; Brown, C.A., 3rd. Factors associated with post-intubation sedation after emergency department intubation: A Report from The National Emergency Airway Registry. Am J Emerg Med 2020, 38, 466–470. [Google Scholar] [CrossRef]
- Lassen, A.T.; Jørgensen, H.; Jørsboe, H.B.; Odby, A.; Brabrand, M.; Steinmetz, J.; Mackenhauer, J.; Kirkegaard, H.; Christiansen, C.F. The Danish database for acute and emergency hospital contacts. Clin Epidemiol 2016, 8, 469–474. [Google Scholar] [CrossRef]
- Kunzler, N.M.; Cole, J.B.; Driver, B.E.; Carlson, J.; April, M.; Brown, C.A., 3rd. Risk of peri-intubation adverse events during emergency department intubation of overdose patients: a national emergency airway registry (near) analysis. Clin Toxicol (Phila) 2022, 60, 1293–1298. [Google Scholar] [CrossRef]
- Kim, H.; Kim, S.; You, J.S.; Choi, H.J.; Chung, H.S. The clinical effectiveness of simulation based airway management education using the Korean emergency airway registry. Signa Vitae 2017, 13, 56–60. [Google Scholar] [CrossRef]
- Khalil, A.A.; El-Setouhy, M.; Hirshon, J.M.; El-Shinawi, M. Developing a trauma registry for the emergency department of a tertiary care hospital in Egypt: a step toward success. Egypt J Surg 2021, 40, 649–655. [Google Scholar] [CrossRef]
- Kaisler, M.C.; Hyde, R.J.; Sandefur, B.J.; Kaji, A.H.; Campbell, R.L.; Driver, B.E.; Brown, C.A., 3rd. Awake intubations in the emergency department: A report from the National Emergency Airway Registry. Am J Emerg Med 2021, 49, 48–51. [Google Scholar] [CrossRef]
- Jimenez, S.; Ruiz-Artacho, P.; Merlo, M.; Suero, C.; Antolin, A.; Casal, J.R.; Sanchez, M.; Ortega-Duarte, A.; Genis, M.; Piñera, P. Risk profile, management, and outcomes of patients with venous thromboembolism attended in Spanish Emergency Departments: The ESPHERIA registry. Medicine (Baltimore) 2017, 96, e8796. [Google Scholar] [CrossRef]
- Jeong, J.; Kim, Y.J.; Kong, S.Y.; Shin, S.D.; Ro, Y.S.; Wi, D.H.; Kim, S.C.; Sun, K.M.; Kim, S.; Kang, S.B.; et al. Monitoring of characteristics of the patients visiting an emergency center in Cameroon through the development of hospital patient database. Afr J Emerg Med 2022, 12, 77–84. [Google Scholar] [CrossRef]
- Jacob, J.; Cabello, I.; Yuguero, O.; Alexis Guzmán, J.; Arranz Betegón, M.; Abadías, M.J.; Francés Artigas, P.; Santos, J.; Esquerrà, A.; Mòdol, J.M. Emergency Atrial Fibrillation Registry of the Catalan Institute of Health (URGFAICS): analysis by type of atrial fibrillation and revisits within 30 days. Emergencias 2019, 31, 99–106. [Google Scholar] [PubMed]
- Hart, J.C.; Goldstein, L.N. Analysis of the airway registry from an academic emergency department in South Africa. S Afr Med J 2020, 110, 484–490. [Google Scholar] [CrossRef] [PubMed]
- Hansen, K.; Schultz, T.; Crock, C.; Deakin, A.; Runciman, W.; Gosbell, A. The Emergency Medicine Events Register: An analysis of the first 150 incidents entered into a novel, online incident reporting registry. Emerg Med Australas 2016, 28, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Grp, A.; Alonso, C.F.; Avilés, R.A.; López, M.L.; Martínez, F.G.; Ferrer, M.F.; Bañeres, B.G.; Najera, D.; Loaiza, J.E.G.; García, L.B.Z.; et al. Differences in emergency department care of adults with a first epileptic seizure versus a recurrent seizure: a study of the ACESUR (Acute Epileptic Seizures in the Emergency Department) registry. Emergencias 2019, 31, 91–98. [Google Scholar]
- Garcia, S.I.; Sandefur, B.J.; Campbell, R.L.; Driver, B.E.; April, M.D.; Carlson, J.N.; Walls, R.M.; Brown, C.A., 3rd. First-Attempt Intubation Success Among Emergency Medicine Trainees by Laryngoscopic Device and Training Year: A National Emergency Airway Registry Study. Ann Emerg Med 2023, 81, 649–657. [Google Scholar] [CrossRef]
- Fogg, T.; Alkhouri, H.; Vassiliadis, J. The Royal North Shore Hospital Emergency Department airway registry: Closing the audit loop. Emerg Med Australas 2016, 28, 27–33. [Google Scholar] [CrossRef]
- Ferguson, I.; Alkhouri, H.; Fogg, T.; Aneman, A. Ketamine use for rapid sequence intubation in Australian and New Zealand emergency departments from 2010 to 2015: A registry study. Emerg Med Australas 2019, 31, 205–210. [Google Scholar] [CrossRef]
- Chong, S.L.; Barbier, S.; Liu, N.; Ong, G.Y.; Ng, K.C.; Ong, M.E. Predictors for moderate to severe paediatric head injury derived from a surveillance registry in the emergency department. Injury 2015, 46, 1270–1274. [Google Scholar] [CrossRef]
- Choi, H.J.; Je, S.M.; Kim, J.H.; Kim, E. The factors associated with successful paediatric endotracheal intubation on the first attempt in emergency departments: a 13-emergency-department registry study. Resuscitation 2012, 83, 1363–1368. [Google Scholar] [CrossRef]
- Choi, D.; Park, J.W.; Kwak, Y.H.; Kim, D.K.; Jung, J.Y.; Lee, J.H.; Jung, J.H.; Suh, D.; Lee, H.N.; Lee, E.J.; et al. Comparison of age-adjusted shock indices as predictors of injury severity in paediatric trauma patients immediately after emergency department triage: A report from the Korean multicentre registry. Injury 2024, 55, 111108. [Google Scholar] [CrossRef]
- Cho, J.; Cho, Y.S.; You, J.S.; Lee, H.S.; Kim, H.; Chung, H.S. Current status of emergency airway management for elderly patients in Korea: Multicentre study using the Korean Emergency Airway Management Registry. Emerg Med Australas 2013, 25, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Chan, G.W.H.; Chai, C.Y.; Teo, J.S.Y.; Tjio, C.K.E.; Chua, M.T.; Brown, I.C. Emergency airway management in a Singapore centre: A registry study. Ann Acad Med Singap 2021, 50, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Carriel Mancilla, J.; Jiménez Hernández, S.; Martín-Sánchez, F.J.; Jiménez, D.; Fuentes Ferrer, M.; Ruiz-Artacho, P. Clinical characteristics and course in emergency department patients with chronic obstructive pulmonary disease and symptomatic acute venous thromboembolic disease: secondary analysis of the ESPHERIA registry. Emergencias 2020, 32, 40–44. [Google Scholar] [PubMed]
- Carriel Mancilla, J.; Jiménez Hernández, S.; Martín-Sánchez, F.J.; Jiménez, D.; Lecumberri, R.; Alonso Valle, H.; Beddar Chaib, F.; Ruiz-Artacho, P. Profiles of patients with venous thromboembolic disease in the emergency department and their medium-term prognosis: data from the ESPHERIA registry. Emergencias 2021, 33, 107–114. [Google Scholar]
- Cabello, I.; Jacob, J.; Arranz, M.; Yuguero, O.; Guzman, J.; Moreno-Pena, A.; Frances, P.; Santos, J.; Esquerrà, A.; Mòdol, J.M. Impact of emergency department management of atrial fibrillation with amiodarone on length of stay. A propensity score analysis based on the URGFAICS registry. Eur J Emerg Med 2020, 27, 429–435. [Google Scholar] [CrossRef]
- Brown, C.A., 3rd; Kaji, A.H.; Fantegrossi, A.; Carlson, J.N.; April, M.D.; Kilgo, R.W.; Walls, R.M. Video Laryngoscopy Compared to Augmented Direct Laryngoscopy in Adult Emergency Department Tracheal Intubations: A National Emergency Airway Registry (NEAR) Study. Acad Emerg Med 2020, 27, 100–108. [Google Scholar] [CrossRef]
- Bressan, S.; Da Dalt, L.; Chamorro, M.; Abarca, R.; Azzolina, D.; Gregori, D.; Sereni, F.; Montini, G.; Tognoni, G. Paediatric emergencies and related mortality in Nicaragua: results from a multi-site paediatric emergency registry. Emerg Med J 2021, 38, 338–344. [Google Scholar] [CrossRef]
- Bennett, S.; Alkhouri, H.; Badge, H.; Long, E.; Chan, T.; Vassiliadis, J.; Fogg, T. Bed tilt and ramp positions are associated with increased first-pass success of adult endotracheal intubation in the emergency department: A registry study. Emerg Med Australas 2023, 35, 983–990. [Google Scholar] [CrossRef]
- Beauchet, O.; Cooper-Brown, L.A.; Lubov, J.; Allali, G.; Afilalo, M.; Launay, C.P. “Emergency Room Evaluation and Recommendations” (ER2) Tool for the Screening of Older Emergency Department Visitors With Major Neurocognitive Disorders: Results From the ER2 Database. Front Neurol 2022, 12. [Google Scholar] [CrossRef]
- Barfod, C.; Lauritzen, M.M.; Danker, J.K.; Sölétormos, G.; Berlac, P.A.; Lippert, F.; Lundstrøm, L.H.; Antonsen, K.; Lange, K.H. The formation and design of the 'Acute Admission Database'- a database including a prospective, observational cohort of 6279 patients triaged in the emergency department in a larger Danish hospital. Scand J Trauma Resusc Emerg Med 2012, 20, 29. [Google Scholar] [CrossRef]
- Balls, A.; LoVecchio, F.; Kroeger, A.; Stapczynski, J.S.; Mulrow, M.; Drachman, D. Ultrasound guidance for central venous catheter placement: results from the Central Line Emergency Access Registry Database. Am J Emerg Med 2010, 28, 561–567. [Google Scholar] [CrossRef] [PubMed]
- Arranz, M.; Jacob, J.; Sancho-Ramoneda, M.; Lopez, À.; Navarro-Sáez, M.C.; Cousiño-Chao, J.R.; López-Altimiras, X.; López, I.V.F.; García-Trallero, O.; German, A.; et al. Characteristics of prolonged noninvasive ventilation in emergency departments and impact upon effectiveness. Analysis of the VNICat registry. Med Intensiva (Engl Ed) 2021, 45, 477–484. [Google Scholar] [CrossRef] [PubMed]
- April, M.D.; Schauer, S.G.; Brown Rd, C.A.; Ng, P.C.; Fernandez, J.; Fantegrossi, A.E.; Maddry, J.K.; Summers, S.; Sessions, D.J.; Barnwell, R.M.; et al. A 12-month descriptive analysis of emergency intubations at Brooke Army Medical Center: a National Emergency Airway Registry study. US Army Med Dep J 2017, 98–104. [Google Scholar]
- April, M.D.; Driver, B.; Schauer, S.G.; Carlson, J.N.; Bridwell, R.E.; Long, B.; Stang, J.; Farah, S.; De Lorenzo, R.A.; Brown, C.A., 3rd. Extraglottic device use is rare during emergency airway management: A National Emergency Airway Registry (NEAR) study. Am J Emerg Med 2023, 72, 95–100. [Google Scholar] [CrossRef]
- April, M.D.; Arana, A.; Schauer, S.G.; Davis, W.T.; Oliver, J.J.; Fantegrossi, A.; Summers, S.M.; Maddry, J.K.; Walls, R.M.; Brown, C.A., 3rd. Ketamine Versus Etomidate and Peri-intubation Hypotension: A National Emergency Airway Registry Study. Acad Emerg Med 2020, 27, 1106–1115. [Google Scholar] [CrossRef]
- April, M.D.; Arana, A.; Reynolds, J.C.; Carlson, J.N.; Davis, W.T.; Schauer, S.G.; Oliver, J.J.; Summers, S.M.; Long, B.; Walls, R.M.; et al. Peri-intubation cardiac arrest in the Emergency Department: A National Emergency Airway Registry (NEAR) study. Resuscitation 2021, 162, 403–411. [Google Scholar] [CrossRef]
- April, M.D.; Arana, A.; Pallin, D.J.; Schauer, S.G.; Fantegrossi, A.; Fernandez, J.; Maddry, J.K.; Summers, S.M.; Antonacci, M.A.; Brown, C.A., 3rd. Emergency Department Intubation Success With Succinylcholine Versus Rocuronium: A National Emergency Airway Registry Study. Ann Emerg Med 2018, 72, 645–653. [Google Scholar] [CrossRef]
- Alkhouri, H.; Richards, C.; Miers, J.; Fogg, T.; McCarthy, S. Case series and review of emergency front-of-neck surgical airways from The Australian and New Zealand Emergency Department Airway Registry. EMA 2021, 33, 499–507. [Google Scholar] [CrossRef]
- Af Ugglas, B.; Lindmarker, P.; Ekelund, U.; Djärv, T.; Holzmann, M.J. Emergency department crowding and mortality in 14 Swedish emergency departments, a cohort study leveraging the Swedish Emergency Registry (SVAR). PLoS One 2021, 16, e0247881. [Google Scholar] [CrossRef]
- Alkhouri, H.; Vassiliadis, J.; Murray, M.; Mackenzie, J.; Tzannes, A.; McCarthy, S.; Fogg, T. Emergency airway management in Australian and New Zealand emergency departments: A multicentre descriptive study of 3710 emergency intubations. EMA 2017, 29, 499–508. [Google Scholar] [CrossRef]
- Jawad, I.; Rashan, S.; Sigera, C.; Salluh, J.; Dondorp, A.M.; Haniffa, R.; Beane, A. A scoping review of registry captured indicators for evaluating quality of critical care in ICU. J Intensive Care 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Australian Commission On Safety And Quality In Health Care. Economic evaluation of clinical quality registries, Final report. Available online: https://www.safetyandquality.gov.au/sites/default/files/migrated/Economic-evaluation-of-clinical-quality-registries-Final-report-Nov-2016.
- Lee, P.; Chin, K.; Liew, D.; Stub, D.; Brennan, A.L.; Lefkovits, J.; Zomer, E. Economic evaluation of clinical quality registries: a systematic review. BMJ Open 2019, 9, e030984. [Google Scholar] [CrossRef] [PubMed]
- Palmer, C.S.; Davey, T.M.; Mok, M.T.; McClure, R.J.; Farrow, N.C.; Gruen, R.L.; Pollard, C.W. Standardising trauma monitoring: the development of a minimum dataset for trauma registries in Australia and New Zealand. Injury 2013, 44, 834–841. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Roundtable on Evidence-Based Medicine. The Learning Healthcare System: Workshop Summary; Olsen, L., Aisner, D., McGinnis, J.M., Eds.; National Academies Press (US) Copyright © 2007, National Academy of Sciences.: Washington (DC), 2007. [Google Scholar]
- Pomare, C.; Mahmoud, Z.; Vedovi, A.; Ellis, L.A.; Knaggs, G.; Smith, C.L.; Zurynski, Y.; Braithwaite, J. Learning health systems: A review of key topic areas and bibliometric trends. LHS 2022, 6, e10265. [Google Scholar] [CrossRef]
- World Health Organization. Available online: https://www.who.int/publications/m/item/who-clinical-registry (accessed on 5 March 2025).
Figure 2.
Timeframes for primary ED registry publications.
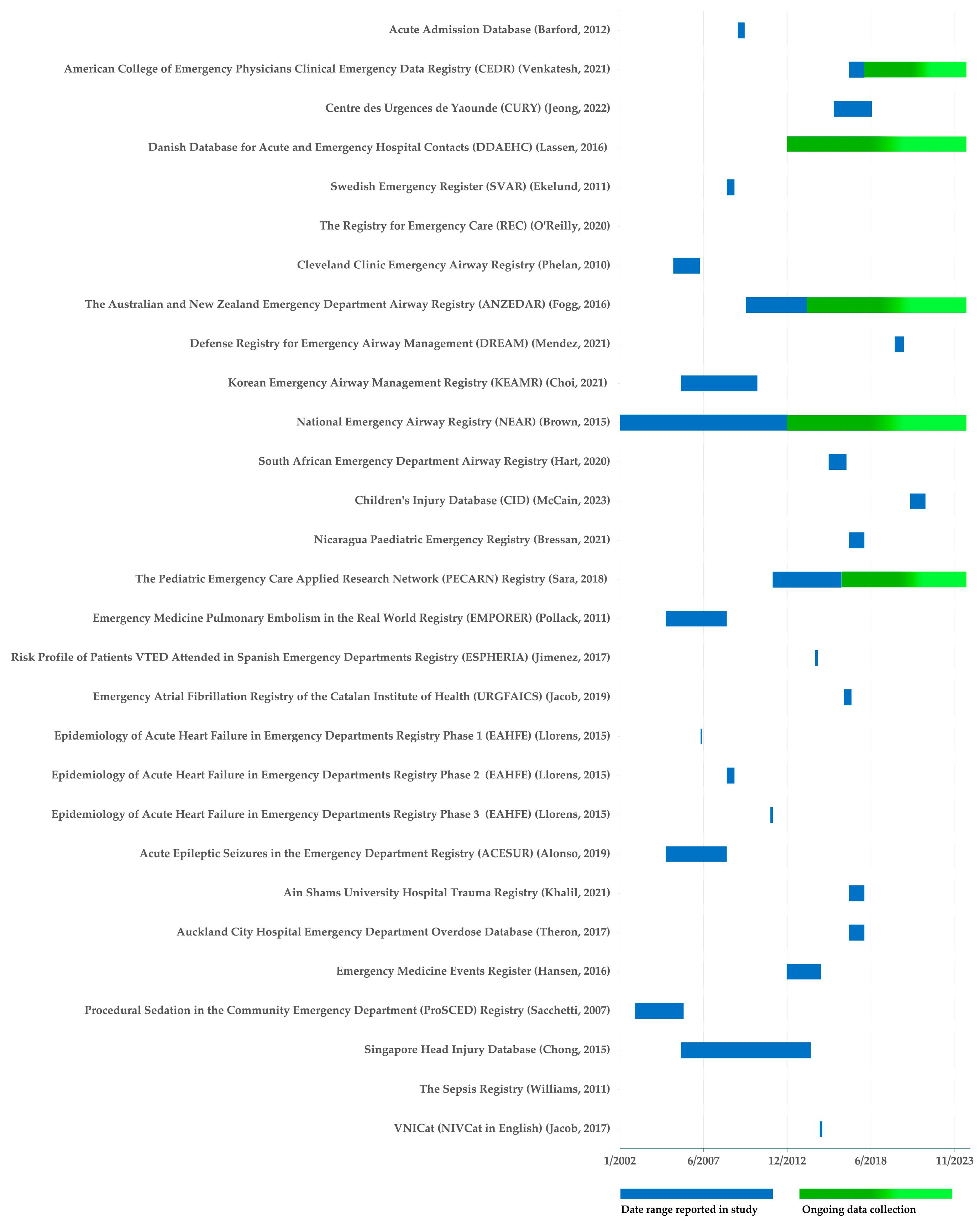
Table 1.
Categories and examples of clinical quality registries .
| Category | Scope | Clinical quality registry example |
|---|---|---|
| Procedure, device or drug | Joint replacement | The American Joint Replacement Registry [13] |
| Ventricular Assisted Device | The Spanish Registry of durable ventricular assist devices [14] | |
| Disease or illness | Hip fracture | The Swedish Fracture Register [15] |
| Stroke | The Australian Stroke Clinical Registry [16] | |
| Specific healthcare resource | Trauma | The Australian Trauma Registry [17] |
| Intensive Care | The Australian and New Zealand Intensive Care Society Centre for Outcomes and Resources Evaluation [8] |
Table 4.
Aims, results and conclusion of primary ED registry publications.
| Registry | Aim | Results | Conclusion | |
|---|---|---|---|---|
| Acute Admission Database | Barford, 2012 | The objective of this article is to 1) describe the formation and design of the ‘Acute Admission Database’ and 2) characterize the cohort included. | In primary triage, patients were categorized as red (4.4%), orange (25.2%), yellow (38.7%) and green (31.7%). Abnormal vital signs were present at admission in 25% of the patients, most often temperature (10.5%), saturation of peripheral oxygen (9.2%), Glasgow Coma Score (6.6%) and respiratory rate (4.8%). A venous acid-base status was obtained in 43% of all patients. The majority (78%) had a pH within the normal range (7.35-7.45), 15% had acidosis (pH < 7.35) and 7% had alkalosis (pH > 7.45). Median length of stay was 2 days (range 1-123). The proportion of patients admitted to Intensive Care Unit was 1.6% (95% CI 1.2-2.0), 1.8% (95% CI 1.5-2.2) died within 7 days, and 4.2% (95% CI 3.7-4.7) died within 28 days after admission. | Despite challenges of data registration, we succeeded in creating a database of adequate size and data quality. Future studies will focus on the association between patient status at admission and patient outcome, e.g. admission to Intensive Care Unit or in-hospital mortality. |
| American College of Emergency Physicians Clinical Emergency Data Registry (CEDR) | Venkatesh, 2021 | To develop a volume-adjusted ED throughput quality measure to balance variation at the ED group level. | We found marked differences in the classification of ED throughput performance between scoring approaches. The weighted standardized score (z score) approach resulted in the least skewed and most uniform distribution across the majority of ED types, with a kurtosis of 12.91 for taxpayer identification numbers composed of 1 ED, 2.58 for those with multiple EDs without any supercenter, and 3.56 for those with multiple EDs with at least 1 supercenter, all lower than comparable scoring methods. The plurality and simple average scoring approaches appeared to disproportionally penalize ED groups that staff a single ED or multiple large-volume EDs. | Application of a weighted standardized (z score) approach to ED throughput measurement resulted in a more balanced variation between different ED group types and reduced distortions in the length-of-stay measurement among ED groups staffing high-volume EDs. This approach may be a more accurate and acceptable method of profiling ED group throughput pay-for-performance programs. |
| Centre des Urgences de Yaoundé (CURY) 4 | Jeong, 2022 | This paper describes the methods of CURY patient data collection and the characteristics of the patients visited CURY from January 2016 to June 2018. | During the study period, a total of 18,875 patients’ data were collected (44.5% women, median age of 36). Of the total patients, 2.4% had chest pain, 2.7% had stroke, 1.9% had sepsis/septic shock, and 1.6% had multiple trauma. About 6.0% patients received operation and majority of patients were discharged either normally (48.2%) or with continuity of care (26.3%). About 5.0% of patients were transferred to other hospital and 5.2% of patients were dead. | This study serves to broaden understanding of the emergency patients in Yaoundé, Cameroon. The hospital patient database for emergency patients can be further used as a basis for providing improved quality of medical care and effective communication tool among the medical staffs. |
| Danish Database for Acute and Emergency Hospital Contacts (DDAEHC) | Lassen, 2016 | The aim of the Danish database for acute and emergency hospital contacts (DDAEHC) is to monitor the quality of care for all unplanned hospital contacts in Denmark (acute and emergency contacts). | The DDAEHC also includes age, sex, Charlson Comorbidity Index conditions, civil status, residency, and discharge diagnoses. The DDAEHC expects to include 1.7 million acute and emergency contacts per year. | The DDAEHC is a new database established by the Danish Regions including all acute and emergency hospital contacts in Denmark. The database includes specific outcome and process health care quality indicators as well as demographic and other basic information with the purpose to be used for enhancement of quality of acute care. |
| Swedish Emergency Registry (SVAR) | Ekelund, 2011 | To assess the feasibility of collecting selected quality of care data from six different Swedish EDs using automated data capture as a basis for a national quality of care registry, and to present some first results regarding throughput times and patient presentation times. | All EDs provided throughput times and patient presentation data without significant problems. In all EDs, Monday was the busiest day and the fewest patients presented on Saturday. All EDs had a large increase in patient inflow before noon with a slow decline over the rest of the 24 h, and this peak and decline was especially pronounced in elderly patients. The average LOS was 4 h of which 2 h was spent waiting for the first physician. These throughput times showed a considerable diurnal variation in all EDs, with the longest times occurring 6-7am and in the late afternoon. | These results demonstrate the feasibility of collecting benchmarking data on quality of care targets within Swedish EM, and form the basis for ANSWER, A National SWedish Emergency Registry. |
| The Registry for Emergency Care | O’Reilly, 2020 | The first objective of the REC Project is to determine the impact of patient isolation and IPC processes on ED length of stay for adult patients. | Clinical tools will be generated to inform emergency care, both during and beyond the COVID-19 pandemic. | The REC Project will support ED clinicians in the emergency care of all patients. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



