
Submitted:
15 March 2025
Posted:
17 March 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Introduction: A top-four-article, March 2024 Google Scholar search of fourteen medical specialties regarding their burnout in COVID-19 redeployment to emergency care found no returns for oncologists. The aim is to investigate oncologist redeployment through a scoping review. Method: Web of Science, Scopus, PubMed, OVID, Google Scholar, and the Cochrane COVID-19 Study Register were searched with the keywords “burnout AND COVID-19 AND emergencies AND oncologists” to determine the resulting redeployment of oncologists to emergency care, the burnout response, and patient outcome. Results: Of the 17,848 search returns using the PRISMA scoping review process, the studies included for assessment were eight reports. The results found that there was a redeployment of oncologists to emergency care defined in various ways, that this redeployment caused oncologist burnout for several reasons, both internally and externally directed, and, together, these reasons negatively affected patient outcomes. Unique to oncologists among the medical specialties was that part of their burnout related to empathy for their patients in their increased risk of mortality and the diminished bond between the doctor and patient. Conclusion: The results of this study can inform oncologists and patients in maintaining the strength of their bond to improve patient outcomes in future pandemics.
Keywords:
oncologists
; burnout
; COVID-19
; emergency care
; redeployment
; patient outcomes
1. Introduction
In March 2024, this author investigated the response of medical specialties regarding redeployment from their usual appointment-based patient care to emergency care resulting from the 2020 [1]-2023 [2] COVID-19 pandemic. Initially, oncologists were among those medical specialties searched by the author through Google Scholar on 31 March. Considering only the top four cited articles returned, this limited search produced no oncologists redeployed to emergency care. The result was a June 2024 publication that did not include oncologists [3].
Pre-COVID-19, burnout in oncologists was recognized as a serious issue [4], with a systematic review and meta-analysis undertaken to investigate the extent of the problem [5]. Since then, COVID-19 increased the burnout in oncologists, reported in several studies [6,7,8,9], while producing different approaches to mitigate such burnout [10,11].
Concerning the redeployment of oncologists to emergency departments during COVID-19, to date, there have been systematic reviews of the redeployment of healthcare providers in general to emergency departments regarding intensive care that might include cancer patients [12] and the effects of COVID-19 on cancer care[13]. Also, there is a scoping review on the impact of COVID-19 on cancer care [14], plus a study of the perceptions of oncology professionals about emergency preparedness during COVID-19 [15]. However, this is the first scoping review on the redeployment of oncologists to emergency departments during COVID-19.
Such an investigation is valuable because of the high and growing [16] volume of patients with advanced cancer who visit emergency departments annually, the complexity of their treatments required, plus their frailty and the acuteness of their illness, requiring the specialized knowledge of oncologists for adequate care management [17]. This need for oncologists is evident, although emergency medical professionals are receiving increasingly specialized training in this regard [16], as significantly, cancer patients are often diagnosed initially from admittance to the emergency department [18]. What is also apparent is the awareness of oncologists that COVID-19 appreciably affected their cancer management [19].
This investigation aims to determine the redeployment of oncologists to emergency care during COVID-19. With a finding of redeployment, consideration is to the type of emergency they experienced and whether these oncologists had a burnout response [20,21,22,23]. The final consideration is the patient outcome from combining the redeployment emergency and the burnout response. Unlike the author's earlier publication [3] with a less extensive search of databases, this work does not additionally examine the coping strategies [24] used by oncologists who experienced burnout from their redeployment. This study has a more limited purview—one best fulfilled by undertaking a scoping review [25].
2. Materials and Methods
The searched databases are as follows: Google Scholar, the four most medically relevant databases (OVID, PubMed, Scopus, and Web of Science), and the Cochrane COVID-19 Study Register. Although questions regard the legitimacy of Google Scholar for academic searches because of its search inconsistency, concurrently, it is noted for its superior range as a database [26,27]. This range provides the reason for including Google Scholar among the searched databases. The search involves the Cochrane COVID-19 Study Register for its relevance regarding COVID-19-related research [28], and it reduces the manual screening workload needed for identifying COVID-19 research studies [29].
Materials were obtained by following the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for scoping reviews [30], providing the flow diagram for the conducted searches and checklist (Supplementary S1). The 24 August 2024 searches were of the keywords “burnout AND COVID-19 AND emergencies AND oncologists”. The order of the searches was Web of Science, Scopus, PubMed, OVID, Google Scholar, and the Cochrane COVID-19 Study Register.
The inclusion criteria are that all keywords must be in the report. The exclusion criteria are no duplicates, not peer-reviewed, and the keywords are not in the publication.
The creation of a Word document followed each search, becoming the supplementary documents of this study. These documents include the keywords, the number of returns, and a color-coded system indicating exclusions made: Red—duplicates, purple—no oncologist, blue—no emergencies, and orange—no burnout.
For Web of Science (Supplementary S2), there were three returns—duplicates of other database searches—either to Google Scholar (in two instances) or to Scopus and PubMed (in one return). Thus, all returns were color-coded red.
The Scopus database search (Supplementary S3) returned four articles. Two were duplicates—one in Web of Science and Pub Med, the other in Google Scholar. These are color-coded red. Another, color-coded purple, did not mention oncologists in the text, although it mentioned oncologists in the references. The last excluded (but first returned) did not discuss emergencies and is color-coded blue.
The PubMed search (Supplementary S4) counted the one reference that was a duplicate of a return from both the Web of Science and Scopus search. The one represents the only return of the five reports included. An exclusion of four followed an investigation finding that none concerned emergencies. Consequently, all of these are color-coded blue.
With 36 returns, the OVID search (Supplementary S5) was the first to return more than a handful of articles. However, only nine of the articles returned are included in the supplementary document because twenty-six lack peer review. There was an immediate report exclusion because the article title demonstrated it was not oncology-related. Of the nine, three are color-coded red—they are duplicates—all of Google Scholar returns. Two are color-coded purple. Although concerning oncology, they did not mention oncologists. Four reports remain included.
The Google Scholar search (Supplementary S6) returned orders of magnitude more than the other searches, with 17,800 returns. Since Google Scholar is a crawler-based search engine, returning the most relevant articles first [26], consideration was to the Google Scholar returns until a page listing ten returns did not include at least one relevant article. This process involved returns from eighteen pages, equaling 180 studies, excluding 17,620 records. Of these, it was clear that 128 did not concern oncologists from the title alone, and two were not in peer-reviewed journals. A manual investigation of the remaining 51 returns found that four were not regarding oncologists and color-coded purple. Of the 41 that did not concern emergencies, color-coded blue, two are the duplicates mentioned from Web of Science and Scopus. The only search that returned reports lacking burnout—they numbered three and are color-coded orange. Most returns were excluded, with only three included. The medically-related databases did not return these three, and this is notable.
The search of the Cochrane COVID-19 Study Register produced no returns. Therefore, there is no supplementary file.
The grouping of the supplementary files regarding the searches is one document: Supplementary S2-S6: Search Results of Each Database Conducted on 24 August 2024 in Order of the Performed Search. The entries provide all details of the searches, including those omitted from following the guidelines for the PRISMA recording process regarding the flow of information.
This study is preregistered at https://doi.org/10.17605/OSF.IO/G9HZU.
3. Results
The search process following PRISMA guidelines [30] is represented in the PRISMA flowchart of Figure 1.
The titles of the eight returned reports in order of their searched return on 24 August 2024 are as follows, from the PubMed search (Supplementary S4): “Burnout, coping and resilience of the cancer care workforce during the SARS-CoV-2: A multinational cross-sectional study” [31] published in 2023. The OVID search (Supplementary S5) returned four reports, one from each of the four years associated with COVID-19. They included “Bio-ethical issues in oncology during the first wave of the COVID-19 epidemic: A qualitative study in a French hospital” [32], “The role of telehealth in oncology care: A qualitative exploration of patient and clinician perspectives” [33], “Victoria (Australia) radiotherapy response to working through the first and second wave of COVID-19: Strategies and staffing” [34], and “Ethical and practical considerations on cancer recommendations during COVID-19 pandemic” [35]. The final group of returns is from the Google Scholar search (Supplementary S6): “Burnout among oncologists, nurses, and radiographers working in oncology patient care during the COVID-19 pandemic” [36] from 2023, “Oncology workload in a tertiary hospital during the COVID-19 pandemic” [37] published in 2022, and “Scientia potentia est: how the Italian world of oncology changes in the COVID-19 pandemic” [38] an Italian publication from 2020 when COVID-19 was particularly severe in that country [39] (see Table 1).
For each report included, the text was examined for three results: (1) the emergency experienced by the oncologists, (2) their burnout response to the emergency, and (3) the outcome for patients contending with the emergency and with the burnout of their oncologist. The results are presented in Table 2.
3.1. Emergency Experienced
The emergency experienced by the oncologists, according to the records returned noted in Table 2, can be grouped by topic. Table 3 provides these groupings in order of their return on the searches performed. The first type of emergency experienced is oncologist-centered and regards a change in the work routine of the oncologists [31,35,38]. That these changes produced an emergency in oncology clarifies that oncologists had not previously prepared for these emergencies during COVID-19, unlike nephrologists [40,41]. The second type of emergency is also oncologist-centered and concerns the increased workload experienced by the oncologists [31,36,37]. Similar to the changes in the work schedules, this change was the first returned emergency from the search and also appeared later in the search process. The emergency following is other-centered, and the detail concerns patients [32]. The emergency is an increase in mortality and decreased survival time. Significantly, only one report considered the emergency to relate to a concern for the patient. The final topic covers the other-centered relationship between the oncologist and the patient [33,34,36]. This topic became evident because of the required use of telehealth during COVID-19—also necessitated in several other medical specialties as a result of the pandemic, including cardiologists [42], dermatologists [43], gastroenterologists [44], and, most successfully, in psychiatrists [45]—which was considered inappropriate for this relationship by both the oncologist and the patient when having to relay bad news, visually inspect the progress of the disease (as with dermatologists [43]), or show empathy.
3.2. Burnout Response
Similar to the emergency experienced, burnout responses by oncologists found in Table 2 are groupable into two topics—oncologist-centered and other-centered in Table 4. The majority of the burnout responses by oncologists [31,34,35,36,37] concerned increasing their burnout regarding escalating personal symptoms associated with burnout [22] that have been found particularly evident in physicians [23]. The other-centered concerns leading to increased burnout in oncologists are of three different types. (1) Those regarding patients, (2) ethical dilemmas stemming from a decrease in quality care, and (3) worries about infecting family members. The evidence is that highly empathetic physicians are the ones who developed pronounced burnout during COVID-19, leading to abandoning the profession [32]. However, unlike oncology nurses [36], abandoning the profession was not an outcome displayed by oncologists concerning the burnout they experienced from empathy for patients during COVID-19. Burnout produced by ethical distress [33] is associated with oncologists, given their role in delivering serious news and end-of-life decision-making—the pandemic produced moral strain, distress, and injury in delivering serious news and end-of-life decision-making [46]. Telehealth decreased the ability of oncologists to provide empathetic care, presenting a form of burnout distinct to oncologists by producing compassion fatigue [47]. Concern for infecting family members [38] was not unique to oncologists and was found most evidently in those physicians specializing in internal medicine [48] and neurology [49]. Early in the pandemic, this worry was reported by all physicians in contact with COVID-19 patients internationally [50].
3.3. Patient Outcome
Grouping the patient outcomes by oncologist-centered and other-centered from Table 2 by topic in Table 5, the detrimental change to the patient’s relationship with their oncologist that was the most significant outcome was a decrease in their level of care [31,35,36,37] to the extent that patients felt the emergency experienced by oncologists and their burnout response put their own life in danger [32]. In a study of oncology patient perceptions of their care during COVID-19, concerns regarding dying from COVID-19 gained one of the most “agreed” and “strongly agreed” responses to questions [51]. The loss of intimate contact with the oncologist [33,34,36] was primarily a result of necessitating telehealth and what patients witnessed as institutional decisions coming between them and their oncologist [38]. During COVID-19, there was an association between feelings of social isolation of oncology patients and a higher incidence of death [51]. Of these concerns, the most numerous regarded what patients saw as the decreased level of care provided, producing oncology patient mistrust in the healthcare system during COVID-19, recognized in a qualitative analysis of patient experiences [52]. Although most patients did not equate this decrease in care to the possibility of their increased mortality, and, in a qualitative study, oncology patients did not see COVID-19 as a barrier to continuing their in-person care [53], noting the decrease in care as the outcome means this decrease might lead to that result. Oncologists anticipated this concern by patients early in the pandemic regarding the possibility of increased litigation resulting from the COVID-19 imposed changes [54,55].
4. Discussion
Unlike the limited review results of [3] that found none, this scoping review results in eight reports of oncologists redeployed to emergency care during the COVID-19 pandemic.
Compared with other medical specialties, oncologists were less effective in managing their burnout than nephrologists because they had not developed emergency care procedures before the pandemic [40,41]. Furthermore, unlike psychiatrists [45], they had not found a way to successfully incorporate telehealth into their emergency care to improve patient care. In contrast, their telehealth experience was similar to dermatologists finding this type of contact with patients provided ineffective care [43]. Although, early in the pandemic, oncologists had focused on the increased possibility of augmented litigation resulting from COVID-19, these worries did not appear—as they did for physicians in gastroenterology [56] and physicians specializing in internal medicine [57]. It may be because the litigious environment did not evolve as it did for these other specialties that oncology did not observe mass resignations resulting from the COVID-19 redeployment of these specialists to emergency care.
Oncology has a well-established focus on empathy as patients with cancer experience significant emotional distress to the extent that oncologists aim to reduce patient emotional distress after a consultation [58]. This specialty focus on empathy provides the foundation for identifying a concern for the compromised health of the patient and the reduced intimacy in the doctor/patient relationship as a cause of oncologist burnout [32,33]. Burnout in other specialties did not result from this remarkable patient and relationship empathy [3]. What was similar among oncologists [38] and other specialties [43,49,56,59,60] was their concern about infecting their families due to redeployment to emergency care during COVID-19.
The cherished relationship between patient and oncologist supports why the patient outcome was generally negative regarding the redeployment of oncologists to emergency care, exacerbating their burnout because of a compromised relationship. Patients were unhappy about the effect of oncology burnout on their health [31,35,36,37] and its increasing risk of mortality [32], as well as the breakdown in the patient/oncologist relationship [33,34,36]. This relationship focus for patient outcomes regarding oncologists was not evident for other specialties [3]. What was similar among oncologists [38], gastroenterologists [56], nephrologists [61], obstetricians [62], and plastic surgeons [63] is that patients considered the administrative changes instituted at hospitals to compete with their best interests.
The strengths of this analysis are that (1) evidence has been provided from the most likely databases to contain reports from peer-reviewed sources that redeployment of oncologists to emergency care during COVID-19 was evident during COVID-19, and (2) the analysis following the PRISMA requirements for scoping reviews was of the type to answer the emergency experienced, that burnout was the result, and the patient outcome.
There are several limitations regarding the method selected for the review. In choosing a scoping review, the author did not select to follow a PRISMA systematic review with a meta-analysis. Such systematic reviews answer narrow clinical questions in the PICO (population, intervention, comparison, and outcome) format [64]. As the intent of this examination is not direct guidance of clinical decision-making, the delivery of care, or policy development [65], a systematic review and meta-analysis is inappropriate. The aim instead corresponds with a PRISMA scoping review [65,66]. Ensuring the quality of the included studies with the performance of a risk of bias assessment is therefore not recommended [67]. What this study does as a scoping review is identify and highlight research gaps suggesting further investigation [68].
That one researcher accomplished the work undertaken is another method limitation. As the interpretation of the results might have been affected by misreading the results [69] or an unrecognized cognitive bias [70], documenting all processes is the most effective way to eliminate bias in such circumstances. By providing extensive detail regarding the PRISMA scoping review process undertaken—more than required by [30] — and submitting the results as supplementary documents, other researchers may examine the method and results for veracity.
The paucity of relevant results for several database searches, especially the Cochrane COVID-19 Study Register yielding no results, is an additional limitation. This lack of returns questions the chosen keywords for inclusion, as studies with added depth or contrast to the results might be missing. However, limiting the keywords in this manner eliminated many irrelevant articles [71]. Another limitation regarding the small number of returns is a reduction in the generalizability of the findings [72]. Finally, by including Google Scholar—a supplementary database—as one of the searched databases, the importance of its search results overshadowed those of some of the primary databases (Scopus and Web of Science). The Google Scholar search results were successful because this database is the most comprehensive, explaining it as the number one search engine academics use [26]. Consequently, it is reasonable to select it for this search and that it would provide more returns than some primary databases.
In restricting the consideration to the redeployment of oncologists to emergency care during COVID-19 in a scoping review, this study did not make recommendations regarding coping strategies that may have been effective during the pandemic regarding emergency oncology care. Had this study extended to coping strategies, it might have provided ways to support oncologists in future pandemic situations. Already, there is extensive research on means of burnout reduction in oncologists in [10] and [11]. Furthermore, in the publication that prompted this scoping review [3], the author conducted a substantial analysis of coping strategies for physicians redeployed to emergency care. Duplication of this analysis is unnecessary and not permissible as a scoping review [68].
5. Conclusions
Based on previous research on the redeployment of medical specialties to emergency care during the pandemic, whether there was such redeployment of oncologists from their usual appointment-based care was unknown. This scoping review determined there was a redeployment of oncologists. Additionally, there was an identification of the emergency they encountered. With the recognition of the emergency, the determination was that, for various reasons, this type of redeployment for oncologists always resulted in burnout. Together, their emergency care redeployment and burnout negatively affected patient outcomes. How it affected patient outcome was in some ways similar to other medical specialties, but because of the intimate relationship developed between the oncologist and patient, oncologists were more empathetic towards their patients, and the forced changes to the relationship—usually the result of institutional requirements—intensified oncologists’ burnout and diminished patient outcomes.
The results of this research may help oncologists and their patients recognize the importance of their doctor/patient bond to improve their health and navigate future pandemic situations when the redeployment of oncologists is again to emergency care.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary S1: Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Checklist; Supplementary S2-S6: Search Results of Each Database Conducted on 24 August 2024 in Order of the Performed Search.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Bio Medica Atenei Parmensis 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Rigby, J.; Satija, B. WHO Declares End to COVID Global Health Emergency. Reuters 2023.
- Nash, C. Burnout in Medical Specialists Redeployed to Emergency Care during the COVID-19 Pandemic. Emergency Care and Medicine 2024, 1, 176–192. [Google Scholar] [CrossRef]
- Murali, K.; Banerjee, S. Burnout in Oncologists Is a Serious Issue: What Can We Do about It? Cancer Treatment Reviews 2018, 68, 55–61. [Google Scholar] [CrossRef]
- Yates, M.; Samuel, V. Burnout in Oncologists and Associated Factors: A Systematic Literature Review and Meta-analysis. Eur J Cancer Care 2019, 28. [Google Scholar] [CrossRef]
- Sipos, D.; Kunstár, O.; Kovács, A.; Petőné Csima, M. Burnout among Oncologists, Nurses, and Radiographers Working in Oncology Patient Care during the COVID-19 Pandemic. Radiography 2023, 29, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Granek, L.; Nakash, O. Oncology Healthcare Professionals’ Mental Health during the COVID-19 Pandemic. Current Oncology 2022, 29, 4054–4067. [Google Scholar] [CrossRef]
- Hlubocky, F.J.; Back, A.L.; Shanafelt, T.D.; Gallagher, C.M.; Burke, J.M.; Kamal, A.H.; Paice, J.A.; Page, R.D.; Spence, R.; McGinnis, M.; et al. Occupational and Personal Consequences of the COVID-19 Pandemic on US Oncologist Burnout and Well-Being: A Study From the ASCO Clinician Well-Being Task Force. JCO Oncology Practice 2021, 17, e427–e438. [Google Scholar] [CrossRef]
- Hlubocky, F.J.; Symington, B.E.; McFarland, D.C.; Gallagher, C.M.; Dragnev, K.H.; Burke, J.M.; Lee, R.T.; El-Jawahri, A.; Popp, B.; Rosenberg, A.R.; et al. Impact of the COVID-19 Pandemic on Oncologist Burnout, Emotional Well-Being, and Moral Distress: Considerations for the Cancer Organization’s Response for Readiness, Mitigation, and Resilience. JCO Oncology Practice 2021, 17, 365–374. [Google Scholar] [CrossRef]
- Jiménez-Labaig, P.; Pacheco-Barcia, V.; Cebrià, A.; Gálvez, F.; Obispo, B.; Páez, D.; Quílez, A.; Quintanar, T.; Ramchandani, A.; Remon, J.; et al. Identifying and Preventing Burnout in Young Oncologists, an Overwhelming Challenge in the COVID-19 Era: A Study of the Spanish Society of Medical Oncology (SEOM). ESMO Open 2021, 6, 100215. [Google Scholar] [CrossRef]
- Budisavljevic, A.; Kelemenic-Drazin, R.; Silovski, T.; Plestina, S.; Plavetic, N.D. Correlation between Psychological Resilience and Burnout Syndrome in Oncologists amid the Covid-19 Pandemic. Support Care Cancer 2023, 31, 207. [Google Scholar] [CrossRef] [PubMed]
- Clark, S.E.; Chisnall, G.; Vindrola-Padros, C. A Systematic Review of De-Escalation Strategies for Redeployed Staff and Repurposed Facilities in COVID-19 Intensive Care Units (ICUs) during the Pandemic. eClinicalMedicine 2022, 44, 101286. [Google Scholar] [CrossRef]
- Alom, S.; Chiu, C.M.; Jha, A.; Lai, S.H.D.; Yau, T.H.L.; Harky, A. The Effects of COVID-19 on Cancer Care Provision: A Systematic Review. Cancer Control 2021, 28, 1073274821997425. [Google Scholar] [CrossRef] [PubMed]
- Powis, M.; Milley-Daigle, C.; Hack, S.; Alibhai, S.; Singh, S.; Krzyzanowska, M.K. Impact of the Early Phase of the COVID Pandemic on Cancer Treatment Delivery and the Quality of Cancer Care: A Scoping Review and Conceptual Model. International Journal for Quality in Health Care 2021, 33, mzab088. [Google Scholar] [CrossRef] [PubMed]
- Marshall, V.K.; Chavez, M.; Mason, T.M.; Martinez-Tyson, D. Emergency Preparedness during the COVID-19 Pandemic: Perceptions of Oncology Professionals and Implications for Nursing Management from a Qualitative Study. J Nurs Manag 2021, 29, 1375–1384. [Google Scholar] [CrossRef] [PubMed]
- Bischof, J.J.; Caterino, J.M.; Creditt, A.B.; Wattana, M.K.; Pettit, N.R. The Current State of Acute Oncology Training for Emergency Physicians: A Narrative Review. Emerg Cancer Care 2022, 1, 2. [Google Scholar] [CrossRef]
- Gould Rothberg, B.E.; Quest, T.E.; Yeung, S.J.; Pelosof, L.C.; Gerber, D.E.; Seltzer, J.A.; Bischof, J.J.; Thomas, C.R.; Akhter, N.; Mamtani, M.; et al. Oncologic Emergencies and Urgencies: A Comprehensive Review. CA A Cancer J Clinicians 2022, 72, 570–593. [Google Scholar] [CrossRef] [PubMed]
- Gri, N.; Longhitano, Y.; Zanza, C.; Monticone, V.; Fuschi, D.; Piccioni, A.; Bellou, A.; Esposito, C.; Ceresa, I.F.; Savioli, G. Acute Oncologic Complications: Clinical–Therapeutic Management in Critical Care and Emergency Departments. Current Oncology 2023, 30, 7315–7334. [Google Scholar] [CrossRef] [PubMed]
- Brugel, M.; Carlier, C.; Essner, C.; Debreuve-Theresette, A.; Beck, M.-F.; Merrouche, Y.; Bouché, O. Dramatic Changes in Oncology Care Pathways During the COVID-19 Pandemic: The French ONCOCARE-COV Study. The Oncologist 2021, 26, e338–e341. [Google Scholar] [CrossRef]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi, R.S. Burnout among Healthcare Providers of COVID-19; a Systematic Review of Epidemiology and Recommendations : Burnout in Healthcare Providers. Archives of Academic Emergency Medicine 2020, 9, e7. [Google Scholar] [CrossRef]
- Freudenberger, H.J. Staff Burn-Out. Journal of Social Issues 1974, 30, 159–165. [Google Scholar] [CrossRef]
- World Health Organization Burn-out an “Occupational Phenomenon”: International Classification of Diseases 2019.
- Tabur, A.; Elkefi, S.; Emhan, A.; Mengenci, C.; Bez, Y.; Asan, O. Anxiety, Burnout and Depression, Psychological Well-Being as Predictor of Healthcare Professionals’ Turnover during the COVID-19 Pandemic: Study in a Pandemic Hospital. Healthcare 2022, 10, 525. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, 1984; ISBN 978-0-8261-4191-0. [Google Scholar]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med Res Methodol 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Gusenbauer, M.; Haddaway, N.R. Which Academic Search Systems Are Suitable for Systematic Reviews or Meta-analyses? Evaluating Retrieval Qualities of Google Scholar, PubMed, and 26 Other Resources. Research Synthesis Methods 2020, 11, 181–217. [Google Scholar] [CrossRef]
- Gusenbauer, M. Google Scholar to Overshadow Them All? Comparing the Sizes of 12 Academic Search Engines and Bibliographic Databases. Scientometrics 2019, 118, 177–214. [Google Scholar] [CrossRef]
- Metzendorf, M.; Featherstone, R.M. Evaluation of the Comprehensiveness, Accuracy and Currency of the Cochrane COVID -19 Study Register for Supporting Rapid Evidence Synthesis Production. Research Synthesis Methods 2021, 12, 607–617. [Google Scholar] [CrossRef]
- Shemilt, I.; Noel-Storr, A.; Thomas, J.; Featherstone, R.; Mavergames, C. Machine Learning Reduced Workload for the Cochrane COVID-19 Study Register: Development and Evaluation of the Cochrane COVID-19 Study Classifier. Syst Rev 2022, 11, 15. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, n71. [Google Scholar] [CrossRef]
- Cloconi, C.; Economou, M.; Charalambous, A. Burnout, Coping and Resilience of the Cancer Care Workforce during the SARS-CoV-2: A Multinational Cross-Sectional Study. European Journal of Oncology Nursing 2023, 63, 102204. [Google Scholar] [CrossRef]
- Stoeklé, H.; Ladrat, L.; Landrin, T.; Beuzeboc, P.; Hervé, C. Bio-ethical Issues in Oncology during the First Wave of the COVID-19 Epidemic: A Qualitative Study in a French Hospital. Evaluation Clinical Practice 2023, 29, 925–933. [Google Scholar] [CrossRef]
- Aung, E.; Pasanen, L.; LeGautier, R.; McLachlan, S.; Collins, A.; Philip, J. The Role of Telehealth in Oncology Care: A Qualitative Exploration of Patient and Clinician Perspectives. European J Cancer Care 2022, 31. [Google Scholar] [CrossRef]
- Rykers, K.; Tacey, M.; Bowes, J.; Brown, K.; Yuen, E.; Wilson, C.; Khor, R.; Foroudi, F. Victoria (Australia) Radiotherapy Response to Working through the First and Second Wave of COVID-19: Strategies and Staffing. J Med Imag Rad Onc 2021, 65, 374–383. [Google Scholar] [CrossRef]
- Melidis, C.; Vantsos, M. [Comment] Ethical and Practical Considerations on Cancer Recommendations during COVID-19 Pandemic. mol clin onc 2020. [Google Scholar] [CrossRef]
- Sipos, D.; Kunstár, O.; Kovács, A.; Petőné Csima, M. Burnout among Oncologists, Nurses, and Radiographers Working in Oncology Patient Care during the COVID-19 Pandemic. Radiography 2023, 29, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.; Yang, V.; Han, S.; Zhuang, Q.; Zhou, S.; Mathur, S.; Kang, M.L.; Ngeow, J.; Yap, S.P.; Tham, C.K. Oncology Workload in a Tertiary Hospital during the COVID-19 Pandemic. Proceedings of Singapore Healthcare 2022, 31, 201010582110511. [Google Scholar] [CrossRef]
- Ballatore, Z.; Bastianelli, L.; Merloni, F.; Ranallo, N.; Cantini, L.; Marcantognini, G.; Berardi, R. Scientia Potentia Est: How the Italian World of Oncology Changes in the COVID-19 Pandemic. JCO Global Oncology 2020, 1017–1023. [Google Scholar] [CrossRef]
- De Natale, G.; Ricciardi, V.; De Luca, G.; De Natale, D.; Di Meglio, G.; Ferragamo, A.; Marchitelli, V.; Piccolo, A.; Scala, A.; Somma, R.; et al. The COVID-19 Infection in Italy: A Statistical Study of an Abnormally Severe Disease. JCM 2020, 9, 1564. [Google Scholar] [CrossRef]
- Pawłowicz-Szlarska, E.; Forycka, J.; Harendarz, K.; Stanisławska, M.; Makówka, A.; Nowicki, M. Organizational Support, Training and Equipment Are Key Determinants of Burnout among Dialysis Healthcare Professionals during the COVID-19 Pandemic. J Nephrol 2022, 35, 2077–2086. [Google Scholar] [CrossRef]
- Nair, D.; Brereton, L.; Hoge, C.; Plantinga, L.C.; Agrawal, V.; Soman, S.S.; Choi, M.J.; Jaar, B.G.; Soman, S.; Jaar, B.; et al. Burnout Among Nephrologists in the United States: A Survey Study. Kidney Medicine 2022, 4, 100407. [Google Scholar] [CrossRef]
- Sadler, D.; DeCara, J.M.; Herrmann, J.; Arnold, A.; Ghosh, A.K.; Abdel-Qadir, H.; Yang, E.H.; Szmit, S.; Akhter, N.; Leja, M.; et al. Perspectives on the COVID-19 Pandemic Impact on Cardio-Oncology: Results from the COVID-19 International Collaborative Network Survey. Cardio-Oncology 2020, 6, 28. [Google Scholar] [CrossRef]
- Helm, M.F.; Kimball, A.B.; Butt, M.; Stuckey, H.; Costigan, H.; Shinkai, K.; Nagler, A.R. Challenges for Dermatologists during the COVID-19 Pandemic: A Qualitative Study. International Journal of Women’s Dermatology 2022, 8, e013. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.-J. Psychosocio-Economic Impacts of COVID-19 on Gastroenterology and Endoscopy Practice. Gastroenterology Report 2021, 9, 205–211. [Google Scholar] [CrossRef]
- Yellowlees, P. Impact of COVID-19 on Mental Health Care Practitioners. Psychiatric Clinics of North America 2022, 45, 109–121. [Google Scholar] [CrossRef]
- Hlubocky, F.J.; Symington, B.E.; McFarland, D.C.; Gallagher, C.M.; Dragnev, K.H.; Burke, J.M.; Lee, R.T.; El-Jawahri, A.; Popp, B.; Rosenberg, A.R.; et al. Impact of the COVID-19 Pandemic on Oncologist Burnout, Emotional Well-Being, and Moral Distress: Considerations for the Cancer Organization’s Response for Readiness, Mitigation, and Resilience. JCO Oncology Practice 2021, 17, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Hlubocky, F.J.; Shanafelt, T.D.; Back, A.L.; Paice, J.A.; Tetzlaff, E.D.; Friese, C.R.; Kamal, A.H.; McFarland, D.C.; Lyckholm, L.; Gallagher, C.M.; et al. Creating a Blueprint of Well-Being in Oncology: An Approach for Addressing Burnout From ASCO’s Clinician Well-Being Taskforce. American Society of Clinical Oncology Educational Book 2021, e339–e353. [Google Scholar] [CrossRef]
- Elhadi, M.; Msherghi, A.; Elgzairi, M.; Alhashimi, A.; Bouhuwaish, A.; Biala, M.; Abuelmeda, S.; Khel, S.; Khaled, A.; Alsoufi, A.; et al. Burnout Syndrome Among Hospital Healthcare Workers During the COVID-19 Pandemic and Civil War: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 579563. [Google Scholar] [CrossRef]
- Kristoffersen, E.S.; Winsvold, B.S.; Sandset, E.C.; Storstein, A.M.; Faiz, K.W. Experiences, Distress and Burden among Neurologists in Norway during the COVID-19 Pandemic. PLoS ONE 2021, 16, e0246567. [Google Scholar] [CrossRef]
- Adams, J.G.; Walls, R.M. Supporting the Health Care Workforce During the COVID-19 Global Epidemic. JAMA 2020, 323, 1439. [Google Scholar] [CrossRef]
- Ludwigson, A.; Huynh, V.; Myers, S.; Hampanda, K.; Christian, N.; Ahrendt, G.; Romandetti, K.; Tevis, S. Patient Perceptions of Changes in Breast Cancer Care and Well-Being During COVID-19: A Mixed Methods Study. Ann Surg Oncol 2022, 29, 1649–1657. [Google Scholar] [CrossRef]
- Adams, A.; Heinert, S.; Sanchez, L.; Karasz, A.; Ramos, M.E.; Sarkar, S.; Rapkin, B.; In, H. A Qualitative Analysis of Patients’ Experiences with an Emergency Department Diagnosis of Gastrointestinal Cancer. Academic Emergency Medicine 2023, 30, 1201–1209. [Google Scholar] [CrossRef]
- Gotlib Conn, L.; Tahmasebi, H.; Meti, N.; Wright, F.C.; Thawer, A.; Cheung, M.; Singh, S. Cancer Treatment During COVID-19: A Qualitative Analysis of Patient-Perceived Risks and Experiences with Virtual Care. Journal of Patient Experience 2021, 8, 23743735211039328. [Google Scholar] [CrossRef]
- Gebbia, V.; Bordonaro, R.; Blasi, L.; Piazza, D.; Pellegrino, A.; Iacono, C.; Spada, M.; Tralongo, P.; Firenze, A. Liability of Clinical Oncologists and the COVID-19 Emergency: Between Hopes and Concerns. Journal of Cancer Policy 2020, 25, 100234. [Google Scholar] [CrossRef] [PubMed]
- Barranco, R.; Messina, C.; Bonsignore, A.; Cattrini, C.; Ventura, F. Medical Liability in Cancer Care During COVID-19 Pandemic: Heroes or Guilty? Front. Public Health 2020, 8, 602988. [Google Scholar] [CrossRef]
- Lacy, B.E.; Cangemi, D.J.; Burke, C.A. Burnout in Gastrointestinal Providers. Am J Gastroenterol 2024. [Google Scholar] [CrossRef]
- Buran, F.; Altın, Z. Burnout among Physicians Working in a Pandemic Hospital during the COVID-19 Pandemic. Legal Medicine 2021, 51, 101881. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.J.; Dubey, M.; Hall, J.A.; Catzen, H.Z.; Blanch-Hartigan, D.; Schwartz, R. What Is Empathy? Oncology Patient Perspectives on Empathic Clinician Behaviors. Cancer 2021, 127, 4258–4265. [Google Scholar] [CrossRef]
- Mavrogenis, A.F.; Scarlat, M.M. Stress, Anxiety, and Burnout of Orthopaedic Surgeons in COVID-19 Pandemic. International Orthopaedics (SICOT) 2022, 46, 931–935. [Google Scholar] [CrossRef]
- Macía-Rodríguez, C.; Alejandre De Oña, Á.; Martín-Iglesias, D.; Barrera-López, L.; Pérez-Sanz, M.T.; Moreno-Diaz, J.; González-Munera, A. Burn-out Syndrome in Spanish Internists during the COVID-19 Outbreak and Associated Factors: A Cross-Sectional Survey. BMJ Open 2021, 11, e042966. [Google Scholar] [CrossRef]
- Selvaskandan, H.; Nimmo, A.; Savino, M.; Afuwape, S.; Brand, S.; Graham-Brown, M.; Medcalf, J.; Cockwell, P.; Beckwith, H. Burnout and Long COVID among the UK Nephrology Workforce: Results from a National Survey Investigating the Impact of COVID-19 on Working Lives. Clinical Kidney Journal 2022, 15, 517–526. [Google Scholar] [CrossRef]
- Del Piccolo, L.; Donisi, V.; Raffaelli, R.; Garzon, S.; Perlini, C.; Rimondini, M.; Uccella, S.; Cromi, A.; Ghezzi, F.; Ginami, M.; et al. The Psychological Impact of COVID-19 on Healthcare Providers in Obstetrics: A Cross-Sectional Survey Study. Front. Psychol. 2021, 12, 632999. [Google Scholar] [CrossRef]
- MacKenzie, E.L.; Poore, S.O. Slowing the Spread and Minimizing the Impact of COVID-19: Lessons from the Past and Recommendations for the Plastic Surgeon. Plastic & Reconstructive Surgery 2020, 146, 681–689. [Google Scholar] [CrossRef]
- Smith, S.A.; Duncan, A.A. Systematic and Scoping Reviews: A Comparison and Overview. Seminars in Vascular Surgery 2022, 35, 464–469. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med Res Methodol 2018, 18, 143. [Google Scholar] [CrossRef]
- Munn, Z.; Pollock, D.; Khalil, H.; Alexander, L.; Mclnerney, P.; Godfrey, C.M.; Peters, M.; Tricco, A.C. What Are Scoping Reviews? Providing a Formal Definition of Scoping Reviews as a Type of Evidence Synthesis. JBI Evidence Synthesis 2022, 20, 950–952. [Google Scholar] [CrossRef]
- Khalil, H.; Peters, M.Dj.; Tricco, A.C.; Pollock, D.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Munn, Z. Conducting High Quality Scoping Reviews-Challenges and Solutions. Journal of Clinical Epidemiology 2021, 130, 156–160. [Google Scholar] [CrossRef]
- Peters, M.D.J.; Godfrey, C.; McInerney, P.; Khalil, H.; Larsen, P.; Marnie, C.; Pollock, D.; Tricco, A.C.; Munn, Z. Best Practice Guidance and Reporting Items for the Development of Scoping Review Protocols. JBI Evidence Synthesis 2022, 20, 953–968. [Google Scholar] [CrossRef]
- Poerwandari, E.K. Minimizing Bias and Maximizing the Potential Strengths of Autoethnography as a Narrative Research. Jpn Psychol Res 2021, 63, 310–323. [Google Scholar] [CrossRef]
- Neal, T.M.S.; Lienert, P.; Denne, E.; Singh, J.P. A General Model of Cognitive Bias in Human Judgment and Systematic Review Specific to Forensic Mental Health. Law and Human Behavior 2022, 46, 99–120. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Shaffril, H.A.; Samsuddin, S.F.; Abu Samah, A. The ABC of Systematic Literature Review: The Basic Methodological Guidance for Beginners. Qual Quant 2021, 55, 1319–1346. [Google Scholar] [CrossRef]
- Barrett, C.B.; Ghezzi-Kopel, K.; Hoddinott, J.; Homami, N.; Tennant, E.; Upton, J.; Wu, T. A Scoping Review of the Development Resilience Literature: Theory, Methods and Evidence. World Development 2021, 146, 105612. [Google Scholar] [CrossRef]
Figure 1.
The PRISMA Flow of Information Chart for scoping reviews [30] of a search of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” on 24 August 2024, of Web of Science, Scopus, PubMed, OVID, Google Scholar databases, and the Cochrane COVID-19 Study Register listed in order of the most results to the least.
Figure 1.
The PRISMA Flow of Information Chart for scoping reviews [30] of a search of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” on 24 August 2024, of Web of Science, Scopus, PubMed, OVID, Google Scholar databases, and the Cochrane COVID-19 Study Register listed in order of the most results to the least.
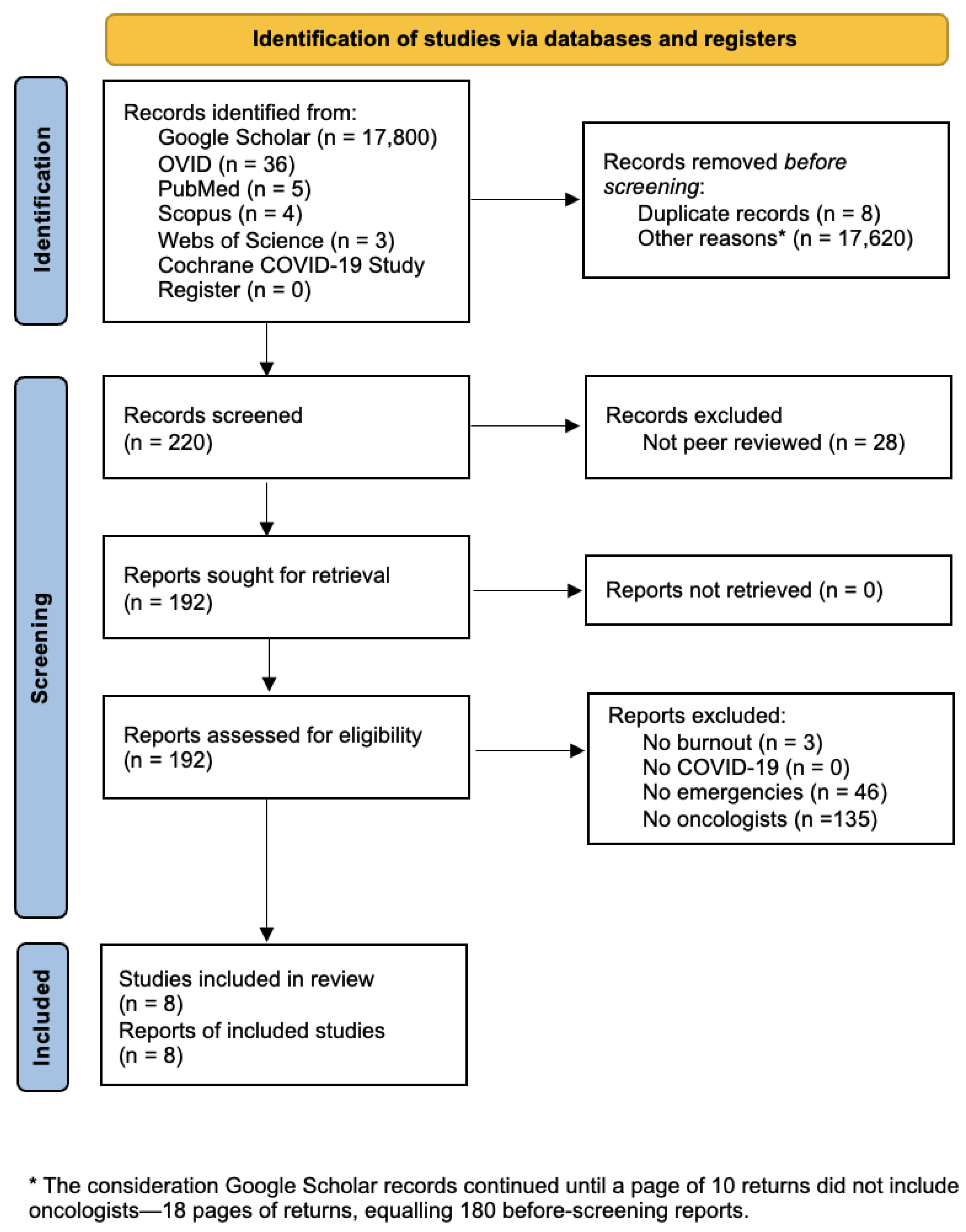

Table 1.
Citation number, report title, and year of publication of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar listed in order of their return.
Table 1.
Citation number, report title, and year of publication of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar listed in order of their return.
| Citation # | Report Title | Database | Year |
| [31] | Burnout, coping and resilience of the cancer care workforce during the SARS-CoV-2: A multinational cross-sectional study | PubMed | 2023 |
| [32] | Bio-ethical issues in oncology during the first wave of the COVID-19 epidemic: A qualitative study in a French hospital | OVID | 2023 |
| [33] | The role of telehealth in oncology care: A qualitative exploration of patient and clinician perspectives | OVID | 2022 |
| [34] | Victoria (Australia) radiotherapy response to working through the first and second wave of COVID-19: Strategies and staffing | OVID | 2021 |
| [35] | [Comment] Ethical and practical considerations on cancer recommendations during COVID-19 pandemic | OVID | 2020 |
| [36] | Burnout among oncologists, nurses, and radiographers working in oncology patient care during the COVID-19 pandemic. Radiography | Google Scholar | 2023 |
| [37] | Oncology workload in a tertiary hospital during the COVID-19 pandemic | Google Scholar | 2022 |
| [38] | Scientia potentia est: how the Italian world of oncology changes in the COVID-19 pandemic | Google Scholar | 2020 |
Table 2.
Citation number, report title, and year of publication of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar listed in order of their return.
Table 2.
Citation number, report title, and year of publication of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar listed in order of their return.
| # | Emergency Experienced | Burnout Response | Patient Outcome |
| [31] | Delay of critical surgeries, suspension or reduction of chemotherapy treatments and change of chemotherapy regimens, increased workload | There were increased levels of burnout, posttraumatic stress, anxiety, and depression, 35% of oncologists raising to 49% at follow up | 66% of oncologists reported an inability to perform their job effectively for patients in comparison with pre-COVID-19 |
| [32] | Patients have high COVID-19-associated mortality rates and decreased survival | Increased concern for patients is viewed as part of the increase in burnout | Prohibition of infected patient family visits implicated in increasing patient mortality |
| [33] | Inability to meet with patients in person, telehealth required for meetings | Experienced ethical distress over their poor performances in breaking bad news on telehealth | Faced decreased intimacy and familiarity previously formed from care pre-COVID-19 |
| [34] | Remote working strategies expanded, and additional telehealth supports were quickly adopted | Over half of the respondents indicated that they often or always felt worn out at the end of the working day | Contact of 90% of new and returning patient clinic reviews was by Internet video or telephone |
| [35] | Reduced number of treatment sessions than initially presented to patients with distinctions based on age criteria and level of emergency | More stressful working conditions than usual, resulting in augmented fatigue and less patience—additional accidents a possibility | Distressed cancer patients—feel they are being put aside and neglected by their oncologist, despite an increased mortality risk |
| [36] | Contending with COVID-19 in association with on-call duties and inappropriate communication techniques | Increased depersonalization and emotional exhaustion, particularly for males and those working more than 50h per week | Mishandling of patient emotions by their oncologists became overwhelming for patients during the pandemic’s progression |
| [37] | The proportion of emergency department admissions to medical oncology increased | The risk of fatigue resulting from the increased workload, leading to poor personal health | A decrease in elective admissions, postponement of non-essential clinic appointments |
| [38] | Required to redefine clinical organization and patient management | Very high perception of risk and concern of infectious danger for their family members | Clash between treatment for patients with cancer and COVID-19 management requirements |
Table 3.
Citation number, report title, and year of publication of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar.
Table 3.
Citation number, report title, and year of publication of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar.
| Citation # | Topic | Topic Details |
| [31,35,38] | Oncologist-centered | Delay of critical surgeries, suspension or reduction of chemotherapy treatments, and change of chemotherapy regimens |
| [31,36,37] | Oncologist-centered | Increased workload |
| [32] | Other-centered | Patients have high COVID-19-associated mortality rates, decreased survival |
| [33,34,36] | Other-centered | Inability to meet with patients in person, telehealth required for meetings |
Table 4.
Citation number of included records and the burnout response by oncologists grouped by topic and topic details of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar.
Table 4.
Citation number of included records and the burnout response by oncologists grouped by topic and topic details of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar.
| Citation # | Topic | Topic Details |
| [31,34,35,36,37] | Oncologist-centered | Posttraumatic stress, anxiety, depression, and fatigue |
| [32] | Other-centered | Increased concern for patients’ health |
| [33] | Other-centered | Ethical distress for requiring telehealth |
| [38] | Other-centered | Concern for family members |
Table 5.
Citation number of included records and the patient outcome of the emergency experienced by oncologists with their burnout response grouped by topic and topic details of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar.
Table 5.
Citation number of included records and the patient outcome of the emergency experienced by oncologists with their burnout response grouped by topic and topic details of included articles returned on 24 August 2024 regarding searches of the keywords “burnout AND COVID-19 AND emergencies AND oncologists” for three databases: PubMed, OVID, and Google Scholar.
| Citation # | Topic | Topic Details |
| [31,35,36,37] | Oncologist-centered | Poor care from the oncologist |
| [32] | Oncologist-centered | Increased risk of mortality from oncologist burnout |
| [33,34,36] | Oncologist-centered | Loss of intimate contact with oncologist |
| [38] | Other-centered | Patient concerns contrasted with institutional decisions |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



