Submitted:
13 March 2025
Posted:
14 March 2025
You are already at the latest version
Abstract
Lactic acidosis is a serious metabolic disorder characterized by an accumulation of lactate in the body, which can lead to a severe acid-base imbalance. Metfor-min-associated lactic acidosis is a rare but life-threatening complication of metformin therapy, particularly in the setting of acute kidney injury or other conditions that im-pair lactate clearance. In this case report, we present the remarkable survival of a patient who experienced severe metformin-associated lactic acidosis with a blood pH of 6.8 and a lactate level of 29 mmol/L, which are typically considered incompatible with life.
Keywords:
Lactic acidosis
; Acute kidney injury
; Metformin-intoxication
; Hemodialysis
1. Introduction
Metformin is a first-line pharmacological treatment for type 2 diabetes mellitus (T2DM) due to its efficacy in improving glycemic control, weight neutrality, and low risk of hypoglycemia [3]. It works primarily by inhibiting hepatic gluconeogenesis and improving insulin sensitivity, with most patients tolerating the drug well. However, in rare cases, metformin can lead to a life-threatening condition known as metformin-associated lactic acidosis (MALA). MALA is characterized by severe lactic acidosis, often defined by hyperlactatemia (lactate > 5 mmol/L), profound acidemia (pH < 7.35), and an elevated anion gap [4]. Though rare, MALA carries a high mortality rate, with estimates ranging from 30% to 50% in reported cases [5].
The pathophysiology of MALA is multifaceted and involves the accumulation of metformin in the setting of impaired renal clearance, leading to mitochondrial dysfunction and increased lactate production [6]. Unlike other forms of lactic acidosis, the primary driver in MALA is not tissue hypoxia but rather the inhibition of mitochondrial oxidative phosphorylation and gluconeogenesis, leading to reduced lactate utilization by the liver [7]. This makes MALA distinct from other causes of lactic acidosis, such as sepsis or ischemia, where hypoperfusion and anaerobic metabolism dominate.
Certain risk factors predispose patients to MALA. Acute kidney injury (AKI) or chronic kidney disease (CKD) is one of the most significant risk factors, as metformin is predominantly eliminated renally through glomerular filtration and tubular secretion [8]. Other contributing factors include conditions that increase lactate production or impair its clearance, such as sepsis, hypoxia, heart failure, or hepatic dysfunction[9]. While lactic acidosis is a known complication of critical illness, the presence of metformin exacerbates the metabolic derangements due to its direct effects on mitochondrial function.
Although severe lactic acidosis with pH < 7.0 and lactate > 20 mmol/L is often deemed incompatible with life, there are rare reports of survival with aggressive supportive care [10].
In this report, we detail the extraordinary survival of a patient with MALA who presented with extreme acidemia (pH 6.8) and hyperlactatemia (lactate 29 mmol/L)—values rarely associated with recovery. This case emphasizes the importance of early recognition, a thorough understanding of MALA’s unique pathophysiology, and the need for timely multimodal therapeutic strategies, including renal replacement therapy and hemodynamic stabilization.
2. Case Presentation
A 52-year-old woman with a history of poorly controlled type 2 diabetes mellitus (HbA1c 17%) and hypertension was admitted to the emergency department with complaints of progressive fatigue and generalized weakness over the preceding 48 hours. Her medical history included long-term metformin therapy (2 g/day) for diabetes and antihypertensive treatment with amlodipine. She reported poor adherence to diabetes management and dietary recommendations. On further questioning, she denied recent gastrointestinal symptoms, chest pain, or significant alcohol intake but noted reduced oral intake over the previous days due to malaise.
• Initial Assessment
On admission, the patient appeared lethargic and drowsy. Vital signs revealed hypotension (blood pressure 85/55 mmHg), tachycardia (heart rate 110 beats per minute), tachypnea (respiratory rate 28 breaths per minute), and hypothermia (core body temperature 34°C). Capillary blood glucose testing revealed hypoglycemia (3.2 mmol/L), and clinical examination was notable for cold extremities, delayed capillary refill, and dry mucous membranes, consistent with dehydration and circulatory shock. No focal signs of infection were evident upon physical examination, although a urine dipstick test showed leukocyturia and nitrituria.
• Laboratory investigations revealed severe metabolic derangements:
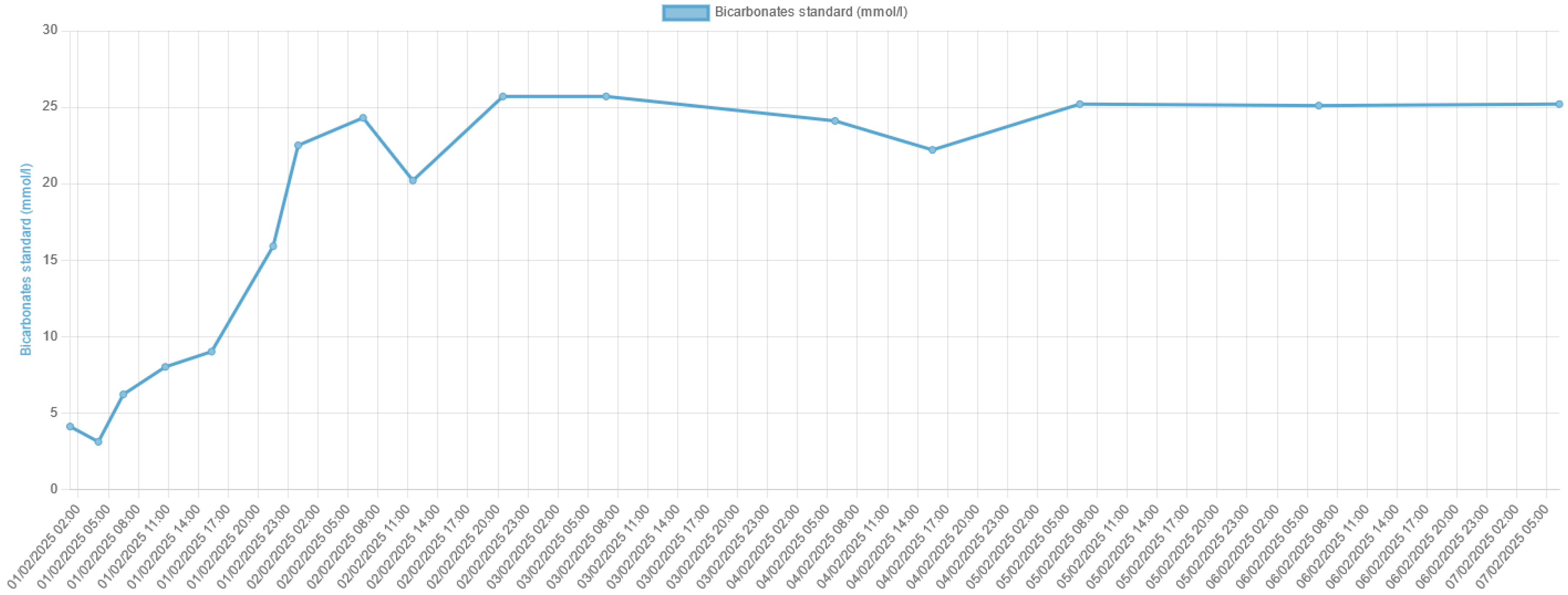
Arterial Blood Gas (ABG): pH 6.78, pCO₂ 19 mmHg, bicarbonate 8.5 mmol/L, base excess -24 mmol/L.
Serum Lactate: 29 mmol/L (reference range: 0.5–2.0 mmol/L).
Electrolytes: Sodium 133 mmol/L, potassium 5.9 mmol/L, chloride 102 mmol/L.
Renal Function: Serum creatinine 3.2 mg/dL (baseline 0.9 mg/dL), blood urea nitrogen (BUN) 58 mg/dL, consistent with acute kidney injury (AKI).
Liver Function Tests: Within normal limits.
Complete Blood Count: Leukocytosis (14,000/μL) with neutrophil predominance, hemoglobin 12.5 g/dL, platelets 210,000/μL.
Other Tests: Normal troponin levels, negative blood cultures initially.
Urine Analysis: Pyuria and bacteriuria, later confirmed as Klebsiella pneumoniae on culture.
The clinical presentation was consistent with severe metabolic acidosis, hyperlactatemia, and AKI in the context of metformin use, strongly suggesting metformin-associated lactic acidosis (MALA). The diagnosis was confirmed by a markedly elevated serum metformin level of 100 µg/mL (normal <10 µg/mL).
• Clinical Course and Management
The patient was admitted to the intensive care unit (ICU) for further management. Given the severity of her presentation, a multimodal therapeutic approach was initiated:
- Hemodynamic Stabilization:
Aggressive fluid resuscitation with isotonic crystalloids was initiated to correct hypovolemia and improve tissue perfusion.
Norepinephrine infusion was started to address distributive shock, with doses titrated up to 5.64 µg/kg/min to maintain a mean arterial pressure >65 mmHg.
- Renal Replacement Therapy (RRT):
Early and prolonged intermittent hemodialysis was initiated within 6 hours of ICU admission, with a total duration of 20 hours. This therapy aimed to remove accumulated metformin, correct acidemia, and improve lactate clearance. Dialysis fluid was bicarbonate-buffered to help restore metabolic balance.
- Empirical Antibiotic Therapy:
Broad-spectrum antibiotics (piperacillin-tazobactam and amikacin) were administered to treat the suspected urinary tract infection. This was later adjusted based on culture results confirming Klebsiella pneumoniae sensitivity.
- Additional Supportive Measures:
Hypoglycemia was managed with continuous dextrose infusion until stabilization of blood glucose levels.
Electrolyte imbalances were closely monitored and corrected (including hyperkalemia).
• Outcome and Follow-Up
Despite the severity of her metabolic derangements (pH 6.78 and lactate 29 mmol/L), the patient showed remarkable improvement within 48 hours. Key milestones in her recovery included:
Progressive hemodynamic stabilization with down-titration of norepinephrine.
Resolution of metabolic acidosis with normalization of lactate levels and pH.
By day 3, vasopressor support was discontinued, and renal function began to recover.
Figures illustrating the biological progression mirrored the clinical improvement:
Figure 1.
Time Course of Arterial pH Recovery During Management of Severe Acidemia.
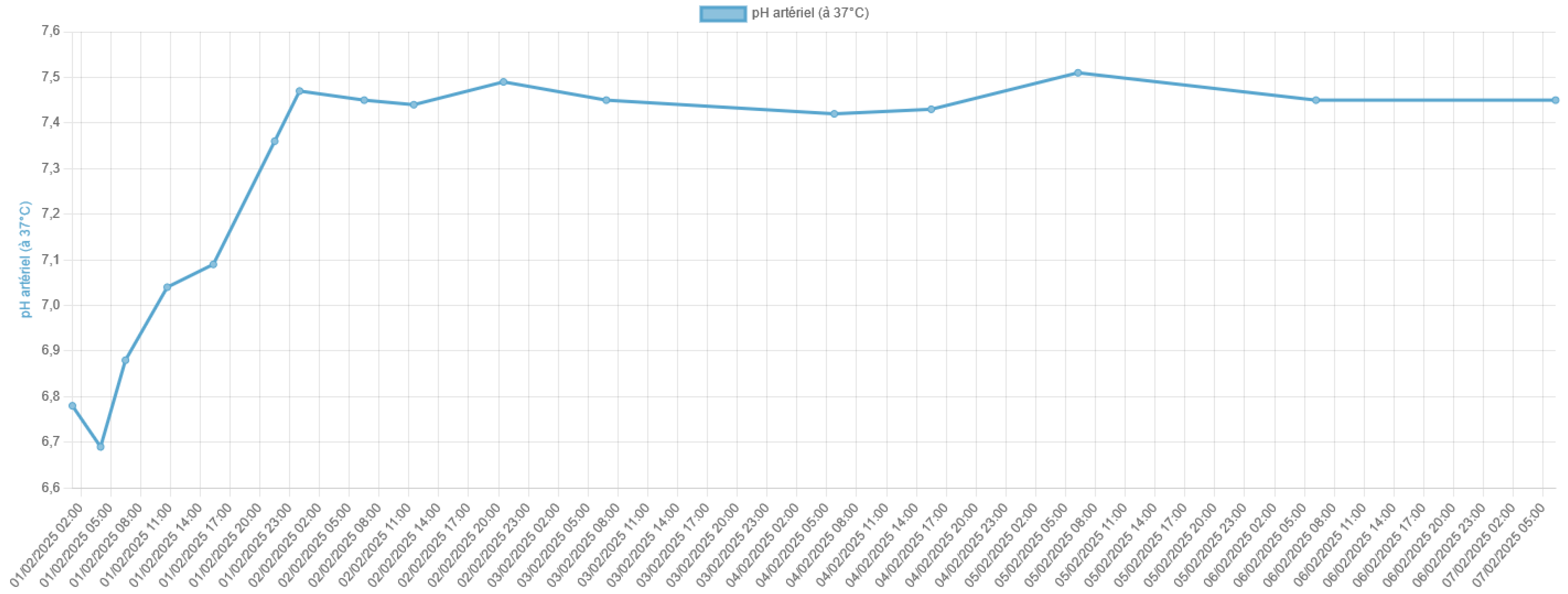
Figure 2.
Lactate Clearance Over Time in Severe Metformin-Associated Lactic Acidosis.
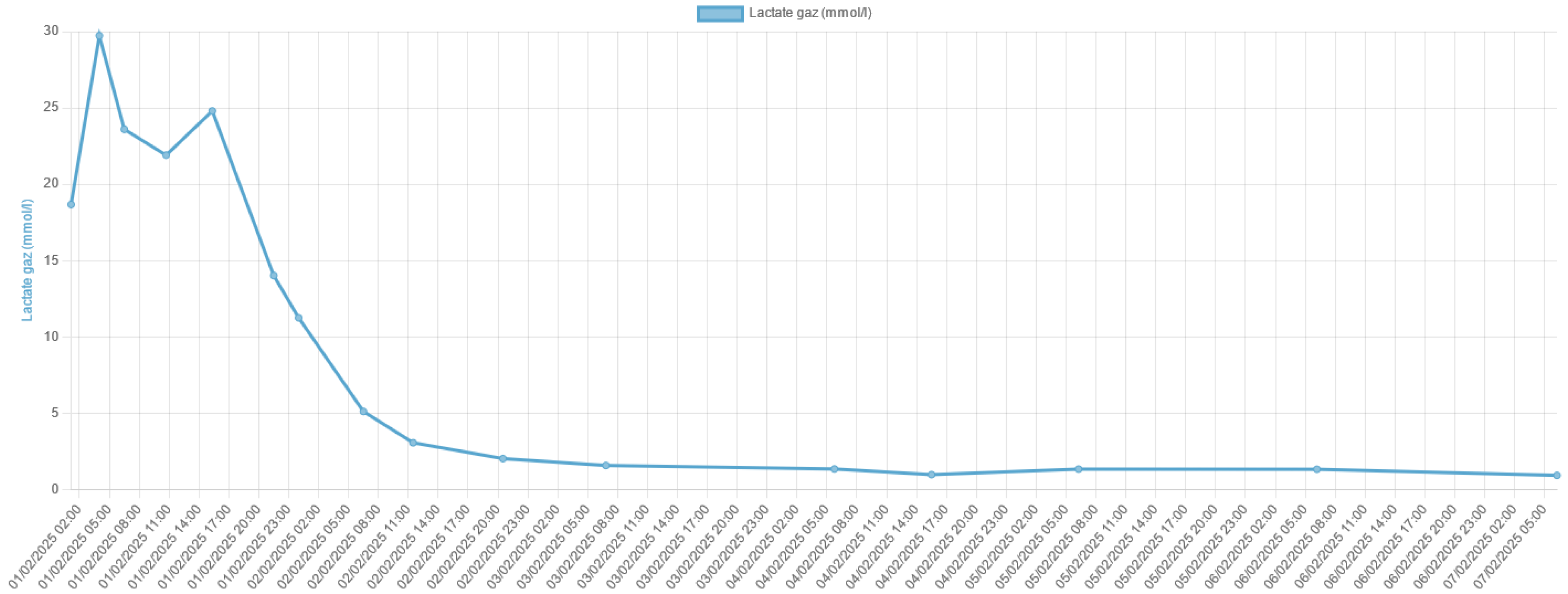
Figure 3.
Improvement in Standard Bicarbonate Levels Following Multimodal Therapy.
The patient was successfully weaned off mechanical support and discharged from the ICU on day 5. Her serum creatinine levels returned to baseline within 10 days, and she remained hemodynamically stable. Metformin therapy was permanently discontinued, and she was transitioned to insulin regimen. She was counseled on the importance of glycemic control, adherence to treatment, and regular follow-up.
This case highlights the potential for survival in MALA, even in the presence of extreme acidemia and hyperlactatemia, when aggressive and timely interventions are implemented.
3. Discussion
Pathophysiology of Metformin-Associated Lactic Acidosis (MALA)
Metformin-associated lactic acidosis (MALA) is a rare but severe complication of metformin therapy, characterized by the accumulation of lactate and profound acidemia. Its pathophysiology involves a complex interplay of mitochondrial dysfunction, impaired lactate clearance, and predisposing clinical conditions.
Mitochondrial Dysfunction Induced by Metformin
Metformin primarily acts by inhibiting hepatic gluconeogenesis through suppression of mitochondrial respiratory chain complex I. This inhibition reduces ATP production and shifts cellular metabolism toward anaerobic glycolysis, resulting in increased production of lactate [11]. Under normal circumstances, lactate is utilized by the liver for gluconeogenesis. However, metformin's suppression of gluconeogenesis leads to reduced lactate consumption, further contributing to its accumulation.
Figure 4.
Molecular Mechanisms of Metformin-Induced Inhibition of Hepatic Glucose Output [11].
Figure 4.
Molecular Mechanisms of Metformin-Induced Inhibition of Hepatic Glucose Output [11].
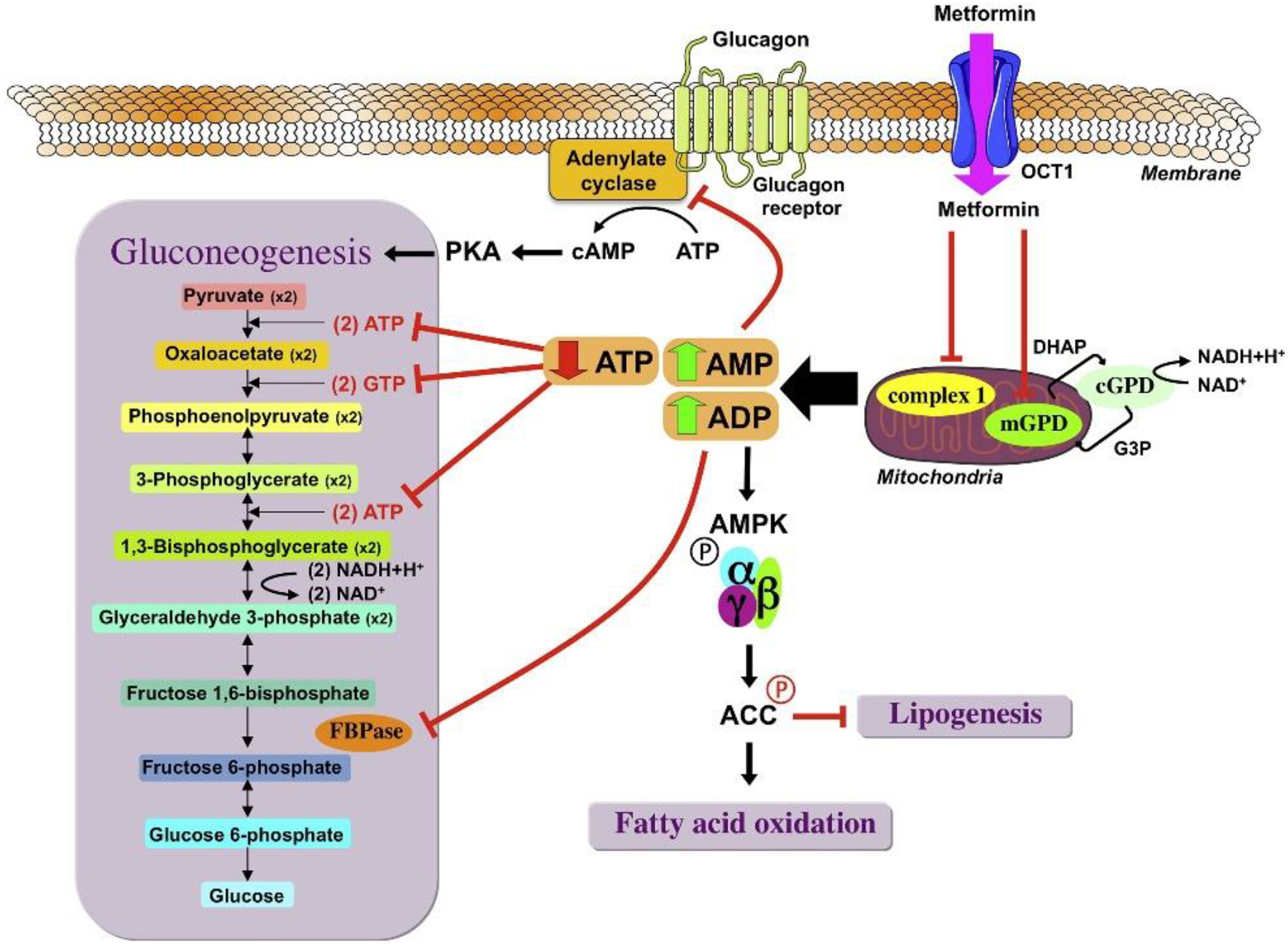
Additionally, at high plasma concentrations, metformin directly impairs mitochondrial oxidative phosphorylation, exacerbating lactate production and reducing the cell’s ability to buffer acidemia. This mechanism is particularly pronounced in the liver and skeletal muscle, where mitochondrial energy demands are high [6].
The Role of Renal Dysfunction
Metformin is predominantly cleared by the kidneys through glomerular filtration and active tubular secretion. In the setting of acute kidney injury (AKI) or chronic kidney disease, reduced clearance of metformin leads to its accumulation, amplifying its inhibitory effects on mitochondrial respiration [8].
Furthermore, renal dysfunction impairs lactate clearance, as the kidneys contribute up to 30% of lactate metabolism under normal conditions [12]. This dual impairment—metformin accumulation and reduced lactate metabolism—creates a vicious cycle that accelerates the development of severe lactic acidosis.
Acidosis and the Impact on Cellular Function
The profound acidemia observed in MALA (pH < 7.0) has significant physiological effects:
Hemodynamic instability: Acidosis impairs myocardial contractility and systemic vascular tone, contributing to distributive and cardiogenic shock [13]. This exacerbates tissue hypoperfusion and further promotes anaerobic metabolism and lactate production.
Intracellular dysfunction: A low intracellular pH disrupts enzymatic activity and ion gradients, compounding mitochondrial dysfunction and impairing cellular recovery mechanisms.
Triggers and Predisposing Factors
While metformin alone rarely causes lactic acidosis, precipitating factors such as AKI, sepsis, or hypoxia are almost always involved. In this case, the urinary tract infection with Klebsiella pneumoniae likely contributed to systemic inflammation and sepsis-related hypoperfusion, further increasing lactate production. The patient’s poorly controlled type 2 diabetes (HbA1c 17%) may have also predisposed her to metabolic stress and reduced lactate clearance.
Reframing the Lactate Threshold in MALA
Although lactate levels >20 mmol/L and pH <6.8 are traditionally considered incompatible with life, MALA appears to have a unique pathophysiology compared to other forms of lactic acidosis, such as those seen in sepsis or ischemia. In MALA, the predominant mechanism is impaired lactate clearance and mitochondrial dysfunction, rather than overwhelming lactate production secondary to tissue hypoxia. This distinction may partly explain the potential for survival in extreme cases, provided aggressive supportive therapy is initiated promptly [5].
Role of Renal Replacement Therapy
Renal replacement therapy (RRT) plays a dual role in the management of MALA:
Metformin elimination: Hemodialysis effectively removes metformin due to its low molecular weight and lack of protein binding.
Lactate and acid-base correction: RRT helps to normalize lactate levels and correct acidemia by buffering the extracellular environment. While lactate itself is not directly removed by hemodialysis, the improvement in metabolic homeostasis and hemodynamics indirectly reduces lactate production.
Clinical Implications and Lessons
This case demonstrates the critical interplay between mitochondrial dysfunction, renal impairment, and acid-base imbalance in MALA. Early recognition and aggressive intervention are paramount to interrupt the pathological cascade. The patient's recovery highlights the importance of:
Early initiation of renal replacement therapy to address metformin accumulation and acidemia.
Hemodynamic stabilization with vasopressors to restore tissue perfusion and mitigate anaerobic metabolism.
Identification and treatment of precipitating factors, such as infections, to prevent further lactate accumulation.
4. Conclusions
Metformin-associated lactic acidosis (MALA) is a rare but life-threatening condition with a complex pathophysiology involving mitochondrial dysfunction, impaired lactate clearance, and contributing factors such as renal impairment or sepsis. This case demonstrates that survival is possible even in the presence of extreme acidemia (pH 6.8) and hyperlactatemia (lactate 29 mmol/L)—values traditionally considered incompatible with life—when aggressive and timely multimodal interventions are implemented.
Early recognition of MALA, combined with targeted therapeutic strategies such as renal replacement therapy, hemodynamic stabilization, and correction of precipitating factors, is critical for improving patient outcomes. This case underscores the importance of understanding the unique mechanisms of MALA to guide effective management and highlights the resilience of physiological systems when supported by prompt, comprehensive care.
Author Contributions
The main author is KORTLI, with the manuscript reviewed by GHALAYINI and AMATHIEU.
Funding
Not received.
Institutional Review Board Statement
Ethics approval and consent to participate. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The Ethics Committee of the Gonesse General Hospital approved this study.
Informed Consent Statement
Written informed consent was obtained from the patient for publication of this study and accompanying images.
Data Availability Statement
No datasets were generated or analyzed during the current study.
Acknowledgments
We are grateful to the patient who kindly consented to the presentation of this case in this paper.
Conflicts of Interest
The authors declare no competing interests.
References
- Montagnani A, Nardi R. Lactic acidosis, hyperlactatemia and sepsis. Ital J Med. 15 déc 2016;10(4):282-8.
- Nnodum BN, Oduah E, Albert D, Pettus M. Ketogenic Diet-Induced Severe Ketoacidosis in a Lactating Woman: A Case Report and Review of the Literature. [cité 26 févr 2025]; Disponible sur. Available online: https://onlinelibrary.wiley.com/doi/10.1155/2019/1214208.
- Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes - PubMed [Internet]. [cité 28 févr 2025]. Disponible sur. Available online: https://pubmed.ncbi.nlm.nih.gov/25538310/.
- Metformin and lactic acidosis in diabetic humans - Lalau - 2000 - Diabetes, Obesity and Metabolism - Wiley Online Library [Internet]. [cité 28 févr 2025]. Disponible sur. Available online: https://dom-pubs.onlinelibrary.wiley.com/doi/abs/10.1046/j.1463-1326.2000.00053.x?sid=nlm%3Apubmed.
- Seidowsky A, Nseir S, Houdret N, Fourrier F. Metformin-associated lactic acidosis: A prognostic and therapeutic study*: Crit Care Med. juill 2009;37(7):2191-6.
- The criteria for metformin-associated lactic acidosis: the quality of reporting in a large pharmacovigilance database - Kajbaf - 2013 - Diabetic Medicine - Wiley Online Library [Internet]. [cité 28 févr 2025]. Disponible sur. Available online: https://onlinelibrary.wiley.com/doi/abs/10.1111/dme.12017.
- El-Mir MY, Nogueira V, Fontaine E, Avéret N, Rigoulet M, Leverve X. Dimethylbiguanide inhibits cell respiration via an indirect effect targeted on the respiratory chain complex I. J Biol Chem. 7 janv 2000;275(1):223-8.
- Davidson MB, Peters AL. An overview of metformin in the treatment of type 2 diabetes mellitus. Am J Med. janv 1997;102(1):99-110.
- Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and Therapeutic Approach to Elevated Lactate Levels. Mayo Clin Proc. 1 oct 2013;88(10):1127-40.
- Lalau JD, Kajbaf F, Bennis Y, Hurtel-Lemaire AS, Belpaire F, De Broe ME. Metformin Treatment in Patients With Type 2 Diabetes and Chronic Kidney Disease Stages 3A, 3B, or 4. Diabetes Care. 5 janv 2018;41(3):547-53.
- Foretz M, Guigas B, Bertrand L, Pollak M, Viollet B. Metformin: From Mechanisms of Action to Therapies. Cell Metab. 2 déc 2014;20(6):953-66.
- Bench-to-bedside review: Lactate and the kidney | Critical Care | Full Text [Internet]. [cité 28 févr 2025]. Disponible sur. Available online: https://ccforum.biomedcentral.com/articles/10.1186/cc1518.
- Kraut JA, Madias NE. Lactic Acidosis. N Engl J Med. 11 déc 2014;371(24):2309-19.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



