Submitted:
13 March 2025
Posted:
14 March 2025
You are already at the latest version
Abstract
The Department of Veterans Affairs (VA) transportation system plays an important role in ensuring access to transportation services for Veterans, particularly those in rural or underserved areas. However, concerns remain regarding the effectiveness of collaboration among the various VA transportation stakeholders. Persistent transportation challenges hinder Veterans' access to essential healthcare services and resources. Electric, Automated Ride-Sharing Services (ARSS) offer a promising opportunity to enhance transportation access, however their current limitations and the perspectives of VA transportation personnel must be considered. This study explored the current perspectives of the VA transportation system and assessed ARSS as an innovative and sustainable alternative through interviews with eight VA transportation stakeholders representing seven transportation sectors. Findings revealed the VA’s strengths, including personalized service, flexible accommodations, and collaborative care models, but also identified challenges, including limited funding, staff shortages, volunteer constraints, and restrictive eligibility criteria. The introduction of ARSS was identified as an opportunity to alleviate some of these constraints by reallocating human resources and improving access to essential services, although concerns remain regarding ARSS’s ability to accommodate Veterans with disabilities and address rural route complexities. Effective communication strategies and streamlined coordination were key recommendations for improving service delivery and expanding transportation access for Veterans.
Keywords:
autonomous shuttle
; electric vehicles
; shared transport
; sustainable transportation
; veterans
1. Introduction
The VA transportation services are available to approximately 9 million Veterans who are enrolled in the VA healthcare system and require transportation assistance to attend medical appointments at VA facilities or authorized non-VA healthcare providers [1]. The Veterans Transportation Program (VTP) comprises multiple stakeholders, including the Veterans Health Administration (VHA), which offers shuttle services and travel vouchers, and the Veterans Transportation Services (VTS), which assists in scheduling transportation and coordinating specialized services, such as wheelchair-accessible vehicles [2]. Additional programs, such as the Beneficiary Travel Program, reimburse travel expenses, while the Highly Rural Transportation Grants fund initiatives for Veterans in remote areas [3]. The Office of Rural Health (ORH) and Veterans Service Organizations (VSOs) support access through telehealth services and partnerships with local transportation providers [4]. However, challenges remain, including limited availability, regional disparities, and funding constraints, with VHA medical transportation expenses reaching $750 million in FY 2010 [5,6]. Challenges in coordination among stakeholders may result in missed appointments and unreliable services, particularly for rural Veterans or those with disabilities [7]. Addressing these barriers requires policy interventions, enhanced resource allocation, and improved collaboration to ensure equitable transportation access and better healthcare outcomes for Veterans.
The integration of ARSS within the Veterans transportation system presents promising future opportunities. For example, potential benefits may include leveraging the flexibility, efficiency, and cost-effectiveness of ARSS platforms [8] to overcome geographical barriers, reduce transportation costs, and provide Veterans with greater autonomy and convenience in scheduling their travel to VA facilities and community-based services. More specifically, Veterans residing in rural or underserved areas with limited public transportation options could benefit from ARSS by gaining access to reliable transportation services when traditional options are scarce. Additionally, such services have the potential to reduce transportation costs for Veterans, particularly those facing financial constraints, by offering competitive pricing and eliminating the need for vehicle ownership and maintenance [9]. Moreover, ARSS platforms may provide Veterans with greater autonomy and convenience in scheduling their travel to VA facilities and community-based services, allowing for personalized transportation solutions tailored to their specific needs and preferences.
Despite these potential benefits, several drawbacks and limitations of ARSS technology exist currently. First, while these platforms offer convenient and flexible transportation options, they may not yet be suitable for all Veterans, particularly those with special mobility needs or disabilities. Veterans with mobility impairments may require specialized vehicles equipped with wheelchair ramps or other accessibility features, which may not be readily available through ARSS providers [10]. Second, the reliability and availability of ARSS are currently limited due to the technology being in the development and testing phases. Such services are currently operating on fixed routes with restricted speed limits, typically at 10mph [11,12]. As such, the availability of ARSS may be limited to specific areas and times, with service disruptions and delays possible due to technical challenges and testing limitations. In rural or remote areas, ARSS may be particularly challenging, as the technology is still being refined and tested in more urbanized environments [13]. Factors such as weather conditions and road infrastructure may further impact the reliability of ARSS [11,12]. Additionally, concerns about data privacy and security may arise with the use of these platforms, as personal information such as pickup and drop-off locations is often shared with third-party companies [13].
While ARSS offer a promising opportunity to enhance transportation access for Veterans, careful consideration of its current limitations and the perspectives of the VA employees involved in transportation planning and operations is needed for realistic recommendations to the VA transportation system. The purpose of this study is to identify and understand the VA transportation system’s strengths and weaknesses and explore the potential of ARSS as an innovative transportation alternative for Veterans. This research may inform policy decisions, demonstration projects, and resource allocation aimed at enhancing Veterans' access to transportation and improving their overall well-being within the VA healthcare system.
2. Methods
2.1. Ethics
The study obtained approval from the University of Florida's Institutional Review Board (UF IRB-01), the North Florida/South Georgia Veterans Affairs Human Research Protection Office, and the ORH. The study was conducted as part of a VA ORH grant submission for FY23-24 (IRB#: 202202386; Title: Benefits of Autonomous Ride Sharing Services for Florida Veterans). All participants provided their consent by signing IRB- and VA-approved documentation, including the Informed Consent Form (ICF), indicating their agreement to participate in the study.
2.2. Study Design
This study used a generic or “basic” qualitative approach [14] to gain insight into how a particular group of people interpret and give meaning to their experiences, and how people derive meaning from their lives and experiences without being limited by the philosophical assumptions of traditional qualitative methodologies. This approach is flexible and can be used to investigate under-explored phenomena that do not fit neatly into existing methodologies [15].
2.3. Participants
To gain a broader understanding of VA transportation services, this study interviewed a diverse group of stakeholders, including those in leadership, service providers, and representatives from key programs. Leadership provided insights into strategic planning, budgeting, and policy implementation, while service providers shared perspectives on daily operations. Participants included representatives from the VTP, VTS, Facilities Management – Transportation, ORH, and Highly Rural Transportation Grants, offering perspectives on policies, budgeting, strategies, coordination of services and rural transportation efforts. A VSO representative provided insights into Veterans' experiences, access barriers, and operational challenges, while a Veteran Experience Officer contributed insights on stakeholder communication and Veteran satisfaction.
Participants were recruited through purposeful and snowball sampling, leveraging recommendations from key leaders within the ORH, to identify individuals with valuable insights into VA transportation services [16,17,18]. A community-based recruitment strategy involved connectors—trusted individuals who spread awareness—and champions, influential figures passionate about the research topic [19,20]. Eligibility criteria required participants to be actively involved in VA transportation services, proficient in English, and have access to a secure internet connection for Microsoft Teams videoconferencing. Those with less than one year of experience were excluded due to limited knowledge. The study aimed to recruit 9-17 key personnel, with data collection continuing until saturation was reached, ensuring no new themes emerged [21,22,23].
2.4. Procedure
The research team screened participants via phone or email using a pre-determined script to explain the study, interview procedures, eligibility criteria, time commitments, and contact information. Eligible participants received the ICF and a demographic questionnaire by mail. After returning the ICF, they were contacted to schedule their interview via Microsoft Teams. Participants received instructions on accessing Microsoft Teams, and those unfamiliar with the platform were offered a brief training session to ensure ease of use [24]. The research team developed a semi-structured interview guide based on the Strengths, Weaknesses, Opportunities, and Threats (SWOT) framework [25] to identify key factors affecting Veterans' transportation services and the role of ARSS.
The semi-structured interviews were conducted online using VA HIPAA-compliant Microsoft Teams [26]. Online interviews provided scheduling flexibility, convenience, and access to a broader participant pool [27]. Microsoft Teams ensures data security through multi-factor authentication and encryption, making it suitable for VA research. Each interview, lasting 30-60 minutes, was conducted from a VA office in Gainesville, FL. Sessions began with a brief period for technical adjustments before the interviewer formally welcomed the participant and proceeded with the interview. Questions focused on service effectiveness, COVID-19-related barriers, and ARSS opportunities and challenges. A qualitative expert reviewed and refined the guide. Interviews began with an overview of the study, followed by pre-determined prompts that allowed for open discussion [28]. At the end of each session, participants were given the opportunity to share additional insights, and they were thanked for their time.
2.5. Strengths, Weaknesses, Opportunities, and Threats (SWOT) as a Framework
The SWOT analysis, a strategic planning tool used to assess organizational strengths, weaknesses, opportunities, and threats, has been widely applied in various fields, including transportation [25,29]. While this study did not conduct a formal SWOT analysis, the research team used it as a framework to develop the semi-structured interview guide. This ensured a structured yet flexible exploration of transportation services for Veterans. Strengths and weaknesses focused on internal factors such as resources and organizational capabilities, while opportunities and threats addressed external influences specifically related to ARSS. This approach, while structured by the SWOT framework, maintained the inductive principles inherent in the generic qualitative methodology.
2.6. Data Collection and Data Management
Each interview was audio recorded using the VA Microsoft Teams functions. Upon completion of each interview, Microsoft Teams automatically transcribed the recording using Microsoft's speech-to-text technology. Subsequently, the research team promptly initiated the review process of the transcript for accuracy and completeness, cross-checking it against the recording. Transcript accuracy took place concurrently with data collection to ensure early detection and correction of any inaccuracies. The research team took several steps to ensure the security and confidentiality of the data collected from participants. Specifically, participant responses to ICFs, demographic questionnaires, and interview recordings were stored in password-protected systems or locked cabinets in a secured VA research office in compliance with the VA and the University’s information security policies. Additionally, the interview data used for analysis were de-identified to protect the privacy of the participants. Only certain project team members indicated on the IRB had access to the de-identified data for analysis purposes. This ensured that the data was only used for the intended research purposes and that the confidentiality of the participants was maintained throughout the research process.
2.7. Data Analysis
The demographic questionnaire was analyzed using descriptive statistics via RStudio using R 4.3.1 [30]. The semi-structured interviews were recorded, transcribed verbatim, and deidentified for confidentiality. Transcripts were reviewed for accuracy before being analyzed using NVivo software [31]. Two research team members conducted a thematic analysis by allowing categories to emerge inductively from the data [32,33]. The analysis process involved repeated reading for immersion, coding key concepts, and categorizing codes into meaningful groups, typically between 10 and 15 clusters [34]. Coders collaborated to refine the coding scheme, and disagreements were resolved with input from a third researcher. Findings were structured using the socio-ecological model to explore transportation challenges across individual, relational, community, and societal levels. To ensure rigor and trustworthiness, investigator triangulation enhanced credibility by verifying participants' original perspectives through regular discussions on coding, themes, and interpretations [35,36]. An audit trail documented key research decisions, supporting confirmability and transparency throughout data collection, analysis, and reporting [37].
3. Results
3.1. Demographics
Eight participants completed the semi-structured interviews, aged between 35 and 56, with 63% being men and 75% identifying as White. All participants were full-time VA employees, with varying levels of experience within the VA transportation system. Half had 1-5 years of experience, one had 6-10 years, and four had over 10 years of experience. Participants were from diverse locations including Florida, Georgia, New York, and Wyoming, though the majority (5 out of 8) were from Florida. Their roles within the transportation system included being a director, analyst, manager, specialist, chief, assistant chief, and coordinator, with expertise in administrative, planning, funding, logistics, operations, and mapping solutions. The participants represented various transportation sectors and departments such as VTP, VTS, Facilities Management – Transportation, ORH, Highly Rural Transportation Grants, Volunteer Transportation Services, and Patient Services.
3.2. Semi-Structured Interview Data
Table 1 illustrates the qualitative themes, subthemes, and their respective operational definitions. A thematic analysis revealed seven major themes and ten subthemes. The seven major themes included: Complex System, Transportation Strengths, Transportation Weaknesses, ARSS Opportunities, ARSS Threats, Communication, and Suggestions for Improvement. Direct quotes from participants are provided throughout the results section below. Complex System had five subthemes: Different modes of transportation, Regulations and policy, Diverse stakeholders, Process of change, and Access to care. Transportation Strengths encompassed four subthemes: North Florida/South Georgia Veterans Health System (NFLSGA) unique, Collaborative approach, Better customer service product, and Drivers working for the VA. Transportation Weaknesses comprised three subthemes: Limited resources, Volunteer transportation limitations, and Eligibility. ARSS Opportunities included two subthemes: Perceived benefits and Suggestions for ARSS deployment. ARSS Threats had three subthemes: ARSS logistics, Serving PWDs, and ARSS adoption. Communication comprised two subthemes: Staff to staff communication, and Veteran and staff communication. Suggestions for improvement included two subthemes: Streamline services and Communication strategies. The themes that emerged from the coding are synopsized as follows.
3.2.1. Complex System
The theme Complex System encompasses five subthemes that highlight the multifaceted nature of the transportation services provided by the VA. Complex System subthemes are: Different modes of transportation, Regulations and policy, Diverse stakeholders, Process of change, and Access to care.
Different modes of transportation. This subtheme involves a variety of transportation options available to Veterans, each tailored to specific needs and eligibility criteria. Special mode transportation caters to wheelchair and stretcher-bound patients, providing door-to-door services for those qualified and eligible.
“So special mode, part of the medical administration service, handles wheelchair and stretcher-bound transport for qualified and eligible individuals. It provides door-to-door service, bringing them from home or a facility to appointments and back…special mode has the secondary option of vending (ID: 1010).”
Volunteer transportation services are primarily for ambulatory Veterans, who can walk and self-assist.
“I can't allow non-ambulatory individuals on the vehicle. We don't have a ramp, lifting device, or any moving equipment, and my volunteers are certainly not medical staff (ID: 1012).”
Uber and Lyft are services available for ambulatory Veterans, offering an alternative to those who do not qualify for other transportation benefits.
“We partnered with Uber on May 10th last year to provide transportation for ambulatory Veterans—those who can walk and self-assist. Before that, they only had mileage reimbursement (ID: 1004).”
Beneficiary Travel is managed by the Medical Administrative Service (MAS). This service provides mileage reimbursement to Veterans who meet specific criteria, such as being service-connected or falling below a certain income threshold.
“Now Veterans qualify for what's called Beneficiary Travel. To qualify, you have to meet certain criteria, you got to be service connected, at least 30% pension, and have an income below $16,500. Not every Veteran qualifies. Ambulatory Veterans, those who can walk and self-assist, previously only received mileage reimbursement, currently 41.5 cents per mile, for travel to and from appointments if eligible (ID: 1004).”
When the demand exceeds internal capacity, trips are outsourced to vendors and contractors, available for special mode only.
“We prioritize special mode trips first. My office assigns drivers to these trips. Everything else is vented out to a contractor. Trips cannot be vended if the individual does not meet special mode criteria (ID: 1006).”
Regulations and policy. This subtheme addresses the regulatory complexities and policy constraints that impact the delivery of transportation services. The numerous and layered regulations governing transportation services create challenges in service delivery and eligibility.
“There are so many regulatory components to transportation and Beneficiary Travel that oftentimes there's more services available than is known. It is not as clear because it is complex because there's so many different layers of the regulations…And there's different requests for adjustments of regulations to open coverage that's going through the congressional process (ID: 1000).”
Additionally, another participant emphasized the stringent adherence required for participation in the VTS program. Accepting VTS funding and resources mandates strict compliance with established protocols, which may not align with the operational realities of certain regions. The participant pointed out that local leadership often adopts a pragmatic approach, prioritizing the immediate transportation needs of Veterans over rigid regulatory adherence. In some instances, VA transportation services operate outside the established system or regulations to ensure effective transportation solutions, demonstrating the importance of flexibility and adaptability in service provision.
“If you join VTS and you sign up 100% and you take their money and you take their vehicles, you have to do everything exactly like they say. That doesn't work for our area. Our leadership is more like do what you gotta do to go out there and bring these folks in and take them home (ID: 1006).”
Diverse stakeholders. This subtheme highlights the range of stakeholders involved in the transportation services, including hospital personnel, social workers, and VA offices. The clinical team, including nurses and physicians, determines and communicates transportation needs for Veterans.
“The clinical inpatient team determines whether a Veteran is ambulatory or requires a wheelchair or stretcher. This information is then communicated to the social worker, who completes a trip ticket specifying the transportation needs—such as requiring oxygen, a stretcher, or a wheelchair—by checking the appropriate box on a form (ID: 1014).”
Social workers facilitate transportation for Veterans who do not qualify for special mode, often handling discharge transportation needs.
“The social work service handles transportation for individuals who do not qualify for special mode, primarily focusing on discharge transportation (ID1010).”
The ORH partners with the VTP to support VTS at rural sites, providing funding and resources to enhance service delivery.
“The Office of Rural Health, we partner with the Veteran Transportation Program to support their VTS program at rural sites. We help provide the funding and the VTS provides vehicle support for the personnel to get them up and running (ID: 1000).”
The Veterans Experience Office handles complaints and ensures service recovery related to transportation.
“Veterans Experience Office, drills down on all transportation complaints and issues. When someone calls patient advocate, they send that complaint out to the service for service recovery, and I get the transportation ones (ID: 1006).”
Overall, the involvement of diverse stakeholders is important for the effective operation and continuous improvement of VA transportation services. Stakeholders interact not only for basic functions such as arranging rides but also at higher levels during planning, evaluation, prioritization of services, problem-solving, and as part of the change process. Participants emphasized the importance of coordinated efforts, data-driven decision-making, and strategic engagement with leadership.
“It comes down to stakeholders sitting down with leadership at the division or facility level and selling the intent. If we think it would be beneficial to station 1-2 drivers at a Community-Based Outpatient Clinic…being able to show based on data what the resource impact would be, both on a dollar side, because then we're not spending funds on 3rd party contractors, vendors, and ambulances, while also increasing access to care for veterans in areas that struggle…being able to sell that point and gain leadership buy in (ID: 1008).”
Process of change. This subtheme involves the ongoing efforts to adapt and improve transportation services in response to emerging needs and challenges.
“We piloted a rural shuttle because everyone said there was a huge need in Levy, Gilchrist, and Dixie County for transportation. We worked on it for six months, meeting with VFW, DAV, and the American Legion and got authorization to launch. We spread the word, advertised, and told people to call if they needed a ride. In six months, we got one call, and it wasn’t even legit. It never really got off the ground. I know there’s a need, but when it comes down to it, it’s hard to… I don’t know, get folks to do it (ID1006).”
Additionally, the integration of services like Uber Health is discussed, though technological barriers such as smartphone requirements pose challenges.
“I do know there's a hiccup using Uber and Lyft because the Veteran needs a smartphone, and that's not always the case with older generations (ID: 1006).”
Access to care. This subtheme emphasizes the critical role of transportation in ensuring Veterans can access necessary medical care, highlighting barriers to access.
“If a Veteran is very poor, has a car that doesn’t work, or lives 3 hours away from a specialty care appointment without a friend or family member to assist, they might not either be eligible for mileage reimbursement or Uber if they're not ambulatory. And that can potentially cause further health concerns for that Veteran if they're not getting the care they need. I would love it if the VA could say every Veteran gets a ride to every appointment, but some of our areas are very rural. Even if the Veteran is eligible for Beneficiary or special mode travel, there might not be a vendor who's available to go to those more rural areas (ID: 1014).”
3.2.2. Transportation Strengths
Participants highlighted several strengths of the VA transportation system, emphasizing unique aspects of the North Florida/South Georgia (NFLSGA) transportation system, a collaborative approach to care, better customer service, and the value of having Veterans as drivers. Transportation Strengths encompassed four subthemes: NFLSGA unique, Collaborative approach, Better customer service product, and Drivers working for the VA.
NFLSGA unique. The NFLSGA transportation system subtheme was repeatedly noted for its distinct capabilities and operational flexibility. Participants emphasized the flexibility of the transportation services offered. This flexibility allows the VA at NFLSGA to accommodate needs that might fall outside their usual support parameters.
“The strength is that North Florida, South Georgia is like no other facility in the planet…and it should be its own service because we're that big (ID: 1006).”
“I can speak to what we provide, and one of our strengths is flexibility in transportation. If a need arises that we wouldn’t typically support, we reassess and find a way to help, considering the long-term impact. For example, if a patient from the Panhandle had surgery in Gainesville and initially had transportation but now needs it for a follow-up appointment, we may classify it as a one-time or until the need is over. We're very flexible here, that's one of the strengths (ID: 1010).”
Collaborative approach. The VA's integrated care model fosters significant collaboration between various departments, enhancing the coordination and quality of care for Veterans. This collaboration includes working with the ORH to support rural transportation programs, integrating with social work services, and maintaining effective communication across different sections to meet diverse needs.
“Because of the integrated nature of VA care, we have a better opportunity through the collaboration between the transportation program and social work to provide better coordinated care, especially in terms of identifying and addressing the social determinants of health (ID: 1002).”
“The Office of Rural Health and the Veteran Transportation Program work really well together. We both recognize how important the other is, and that’s a real strength (ID: 1000).”
Better customer service product. The VA transportation service is noted for its personalized approach, including door-to-door service and close monitoring of transport. This high level of service ensures that Veterans receive tailored transportation, contributing to better overall satisfaction.
“My side of the house provides door-to-door service, offering one-on-one support between the Veteran and VA staff. It is also probably tracked better (ID: 1006).”
“Many of our Veterans are disabled, and not all disabilities are visible. It's great that we have resources for both seen and unseen disabilities, something not always available to non-Veterans. That’s definitely a strength (ID: 1014).”
Additionally, there is a diversity within the system itself, with availability to staff-operated systems, volunteer-operated systems, and third-party operating systems. This diversity in coverage is considered a strength.
“There is diversity within the system, with staff-operated, volunteer-operated, and third-party-operated systems providing coverage. This variety in transportation options is a strength (ID: 1012).”
Drivers working for the VA. The employment of Veterans as drivers was seen as a significant strength, fostering a strong connection and sense of camaraderie between the drivers and Veteran passengers.
“One of the strengths is that the program is primarily staffed by Veterans. They have a commitment to service and to other Veterans, and because they are Veterans, they have military experience with transportation and logistics and program management, personnel management. It's very unique as it is truly Veteran owned and Veteran operated entity within the VA (ID: 1002).”
This connection was considered inspirational and provided additional comfort to Veterans attending appointments.
“The support of Veterans as drivers, and their components of the service really helps. The frontline drivers really connect with Veterans well. Having worked in a rehab department for 20 years, really was able to appreciate drivers connecting and being the inspiration for a Veteran to get to an appointment or an added comfort for a Veteran to go to their appointment, it’s really impressive and impactful (ID: 1000).”
Moreover, the VA drivers are held to higher standards, which helps ensure a high level of service quality.
“We monitor all training and driver physicals, they're held to a higher standard (ID: 1006).”
3.2.3. Transportation Weaknesses
Participants identified several weaknesses within the VA transportation system, particularly focusing on limited resources and operational challenges. Transportation Weaknesses comprised three subthemes: Limited resources, Volunteer transportation limitations, and Eligibility.
Limited resources. Participants noted significant funding constraints that impact the sustainability and expansion of services. Budget freezes and the high costs associated with outsourcing care to community providers were major concerns. These financial pressures are particularly important given the preference of Veterans to receive care within the VA system, where relationships and understanding of Veterans’ unique needs are stronger.
“We can always use more resources, manpower, vehicles because the demand is crazy. Funding is another, right now we're in a budget crunch, so everything is kind of frozen. The reason why is because we have a community care. So, if I'm a Veteran and can’t get seen within 30 days, then we can outsource it into the community and the VA is on the stick to pay for that. That has become very expensive, just for North Florida, South Georgia, it's a $700 million expensive (ID: 1004).”
Another significant limitation identified by participants is the shortage of staff and drivers within the VA transportation system. This issue exacerbates the operational challenges and strains the ability to provide timely and efficient transportation services to Veterans. The insufficient number of drivers means that each driver must cover a large area, often leading to delays and logistical difficulties. Participants emphasized that the daily schedules are frequently adjusted based on patient appointments, which can be unpredictable and vary widely, further complicating the management of available drivers.
“It's because of staffing. Each morning, my team receives a list of 25 to 35 people from Jacksonville, but we only have two drivers. At best, they can take four to six trips, with three passengers each. And people also have to understand that schedule changes daily. It's driven by patient appointment (ID: 1006).”
“One of the primary weaknesses is staffing. There's a FTE neutral policy and it's because of funding. Because transportation isn’t in the forefront of leaderships’ perspective when thinking the whole health mindset, transportation falls to the wayside. If we can get 25 doctors, that's perfectly fine, but if we can't get the patients to see them, then that's a piece of the pie. Because that's not thought of, transportation does fall to the wayside a lot, and the first thing to take a hit is personnel (ID: 1008).”
Volunteer transportation limitations. The inconsistency of volunteer drivers was frequently cited as a significant challenge. Volunteers, while appreciated, often lack the reliability needed to ensure timely and dependable transportation for Veterans’ appointments.
“The problem with volunteers, they're not consistent. I love every one of them and I wanna volunteer when I retire in a few years, but as far as something like that, you're messing with the patient's appointments (ID: 1006).”
“It is a weakness in the sense that if a volunteer goes on vacation for three months, which happens quite regularly, we don't have a built in backup (ID: 1012).”
Additionally, the limited number of drivers available to cover large areas means that scheduling is often strained, leading to potential delays and logistical difficulties in meeting daily transportation demands. The impact of COVID-19 has further exacerbated this issue, as explained by a participant.
“DAV provides a great product. That's not ran through us. They provide an outstanding shuttle service. It's pretty robust, but after COVID-19 it's gone down. They can't fill the volunteers. Probably average age 60+, and once COVID-19 came through, I think it spooked them. They have a 10-passenger van that would come into Jacksonville, they have two vans. The Jacksonville to Gainesville van would come in loaded every single day, five days a week, and now they don't even have the volunteers to move it every single day anymore. So, there's some holes that are developing within this catchment area (ID: 1010).”
Eligibility. Participants also pointed out that the eligibility criteria for transportation benefits are restrictive, preventing many Veterans from accessing necessary services.
“There’re administrative and clinical criteria that has to be met for Veterans to be eligible for that program, and that can sometimes affect a Veteran's access to care (ID: 1014).”
There is a need for better communication regarding these criteria and potential flexibility to accommodate more Veterans.
“We can do a better job communicating the criteria of what makes a Veteran eligible for certain programs within the VA, specifically regarding transportation (ID: 1014).”
3.2.4. Autonomous Ride-Sharing Services Opportunities
Participants identified several promising opportunities associated with the potential deployment of ARSS within the VA transportation system, focusing on perceived benefits and specific suggestions for effective implementation. ARSS Opportunities included two subthemes: Perceived benefits and Suggestions for ARSS deployment.
Perceived benefits. One major benefit highlighted by participants was the potential for ARSS to expand the pool of available employees who can assist with transportation, thereby alleviating some of the staffing constraints currently faced.
“It would open up the pool of employees that could successfully help with the transportation, so that would be helpful (ID: 1000).”
Additionally, the service offers a consistent and reliable point of access within cities or towns, where Veterans simply need to arrive at a designated stop to begin their journey.
“It would provide a better resource for Veterans to have that consistent point of access in a city or town…all they have to do is show up to one of the stops, get on and away they go (ID: 1008).”
Furthermore, another benefit of ARSS is its potential to assist rural Veterans. For instance, one participant noted that ARSS could provide a standardized, stress-free final leg of the journey for rural Veterans traveling to urban centers for care.
“It would be good if it could help rural Veterans get to their final urban track of their ride to make that standardized and less stressful (ID: 1000).”
Suggestions for ARSS deployment. Participants suggested various deployment strategies to maximize the benefits of ARSS, particularly for short trips and in urban communities.
“On a smaller scale to where it can be within the hospital because we have a lot of Veterans because our campus is so big, where we can have little routes to where they can jump on and jump off. Whether because they are handicap or just because they are running late. We can utilize it into parking, if it's something that can monitor the parking and pick people up. Even something for the employees, not just for the Veterans, to make their jobs easier to get to where they need to and navigate throughout the hospital or campus and even off site at surrounding locations (ID: 1004).”
“Knowing that they can be geofenced it would benefit in metropolitan areas. Autonomous vehicles would be extraordinarily beneficial in a large metropolitan area, because is much easier to maintain. There's a lot more accessible information; cell towers are popping up everywhere (ID: 1008).”
Another participant proposed using ARSS within large, walkable developments designed specifically for Veterans. Such communities could leverage ARSS to facilitate not only medical appointments but also access to grocery shopping, dining, entertainment, physical activities, parks, and other essential services, effectively addressing multiple social determinants of health within a self-contained environment.
“Huge walkable developments, developed communities of Veterans, it would have to still be within the confines of a Veteran community to where this automated system would take folks, not just to medical appointments, but also to things like shopping for groceries, dining, entertainment, physical activity, and parks to address everything in terms of social determinants, get access to food, access to education and medical. And meeting all the other basic needs (ID: 1002).”
3.2.5. Autonomous Ride-Sharing Services Threats
Participants expressed concerns regarding the logistical challenges, limitations of ARSS, particularly in serving people with disabilities (PWDs), and adoption barriers. Autonomous Ride-Sharing Services Threats had three subthemes: ARSS logistics, Serving PWDs, and ARSS adoption.
Autonomous ride-sharing services logistics. One significant logistical threat identified is the variability and complexity of routes in rural areas. Participants noted that rural Veterans often have unique and diverse travel needs, making it difficult to implement a standardized ARSS route. The geographical components and varied road conditions present additional challenges for ARSS deployment in these regions.
“Their trips are so varied; they don't have similar routes to be able to have a shuttle to go back and forth on a standardized route. For it to be a level 4 would have to be close to the VA. For the level 4, it had to be like specific geographical components and rural Veterans have such variety of road conditions, the distance, the terrain… it's gonna be the topography whether impacts distance (ID: 1000).”
Additionally, concerns were raised about the reliance on satellite or tower control for ARSS operations, which might face connectivity issues in rural areas.
“It is being ran on satellites or some kind of tower control and is that going to be an issue in rural areas (ID: 1010).”
“Their primary concern would be safety and connectivity. We have tablets that drivers use that connect via satellite and cell towers for GPS connectivity and connecting with the Vet ride system. Even we encounter connectivity issues where they lose connection with the satellite or cell tower. It’s concerning because we lose some of that trip information. The tablets capture drive time, they capture a plethora of information whenever transporting Veterans. Knowing that we’ve that shortfall and that recurring issue is a concern when it comes to an autonomous vehicle that doesn't have a physical person that can troubleshoot on the fly (ID: 1008).”
Serving PWDs. Another major threat is the ability of ARSS to adequately serve Veterans with disabilities. Participants highlighted that many Veterans rely on wheelchairs, scooters, and other mobility aids, which necessitate accessible vehicles equipped with wheelchair lifts. The absence of a driver in ARSS could significantly impede the ability to assist these Veterans.
“I could see it for fixed routes ambulatory only. But on my fixed routes, all vehicles have wheelchair lifts. So, if you started an autonomous vehicle on that route, well, and the first time someone has a wheelchair, what do you do? You have more folks needing transportation that have a rollator, wheelchair, scooter or power chair than are ambulatory (ID: 1006).”
“I could not right now foresee a vehicle without a person in it in case a Veteran needed assistance because so many times our drivers do that. There’re so many times that they go above and beyond to help a Veteran in need, to get higher level care. I would definitely advocate for somebody being in the vehicle at all times (ID: 1000).”
ARSS adoption. Participants expressed concerns about the adoption of ARSS by Veterans, especially regarding trust and technology acceptance. Veterans might experience anxiety or stress about using a vehicle without a driver, especially given their unique experiences and needs.
“If there's no driver, I think that may cause anxiety or add additional stress for any Veteran, regardless of their age. Our Veterans are very different population, and many have been through very traumatic events. They potentially could be more stressed out if getting into this vehicle and no one’s in here or how they know they're taking me to the right place or how do I know I'm going to be on time for my appointment. I think there are too many unknowns (ID1014).”
There might be resistance from older Veterans, who may not be comfortable with new technology.
“We have more older Veterans than younger. We have younger Veterans who might be, oh, this technology is amazing. However, most of our Veterans that do require assistance with transportation are older Veterans and I believe that many of our older Veterans wouldn't be completely comfortable with a level 4-5 autonomous vehicle because they have a lot of older school thinking. Most will prefer to do a paper survey over a computer survey. Many don't still have access to email. Many of our older Veterans don't use my healthy Vet secure messaging, so they're not always thinking that technology is a great thing. Even if it is a great thing, they're not utilizing it. So, our bigger Veteran population that utilizes transportation here would not be on board with a Level 4-5 automated vehicle (ID: 1014).”
Additionally, Veterans who may not have access to a cell phone, including homeless Veterans, might face challenges in accessing and using ARSS.
“I'm sure there's gonna be something where the Vets gotta hit a link and approve it. Because now you're approving transportation for yourself. There's probably something with a manifest, so I'm going to click this link. Not everybody is tech savvy. A lot of the Vets in this area are homeless…so now you're assuming that they have a cell phone (ID1010).”
3.2.6. Communication
Effective communication is essential to the success of the VA transportation system, as it ensures that Veterans and staff are well-informed and coordinated. This theme encompasses communication between Veterans and staff, as well as internal staff communication to facilitate transportation services. Communication comprised two subthemes: Staff to staff communication, and Veteran and staff communication.
Veterans and staff communication. Efforts to inform Veterans about transportation services and eligibility criteria were highlighted by participants. Specifically, participants emphasized the importance of educating both Veterans and VA providers about the transportation services available. While Veterans are often aware that they can access transportation services, they may not always know the best point of contact for scheduling. Ensuring that Veterans are connected to the appropriate person is crucial for providing timely and effective transportation support.
“The transportation program has done a fantastic job at the local level of educating Veterans, providers, and administrative staff that there are transportation services available. Often, it's not an issue that Veterans don't know they can get a ride, they just don't know necessarily the best person to contact to schedule that appointment, and they almost 99% want to speak to a person on the telephone. So, it's more a matter of making sure they are connected to the right person to help them identify what transportation benefits they are eligible for…so we need to make sure that the connection is happening and the benefits are being given to the right Veterans at the right time to make sure they're getting to their appointment (ID: 1002).”
Another participant emphasized the importance of providing clear guidance and criteria for qualifying for transportation services. This includes disseminating information through various channels such as Facebook, websites, flyers, and brochures.
“We try to get the guidance out to the Veterans first to make sure what the criteria is for them to qualify...But once they know we put out guidance on Facebook, all the websites, and even provide literature here in terms of flyers and brochures so that they're aware of it (ID: 1004).”
Despite these efforts, there are still challenges in ensuring effective communication. One participant pointed out that the transportation services they provide are primarily support functions, meaning they rely on internal VA systems and referrals rather than direct outreach to Veterans.
“We don't have a lot of discussions with Veterans. Sometimes they'll sneak through and find our number, but everything that we do is a support, a function. How does anybody find out or get our name? Realistically, it's not out there. The only ones that need to know, know. If Veterans find out, you put them on a carousel, and I don't like doing that. Because they'll call here and be like you need to call this place. And they tell me, oh, I don't feel like getting bounced around, you're like the 5th call, but we don't have the tools in our department to check if they're truly qualified as in VA need (ID: 1010).”
Staff to staff communication. Internal communication among staff was also noted as important, particularly in terms of logistical coordination. Effective communication and collaboration across different sections and regions is needed to ensure that the transportation needs of Veterans are met, regardless of the demand.
“The current strengths I would say, communication probably is one of them. Logistically we communicate, and we collaborate with all the different sections to try to make things happen no matter what the demand is. A lot of it is just real strong communication with the other sites and even outside of our region to make sure we take care of our patients (ID: 1004).”
However, there are notable barriers to effective communication that can impact service delivery. One significant issue is the lack of timely communication between the inpatient team and social workers regarding Veterans' discharge schedules.
“The biggest barrier is sometimes the impatient team doesn't communicate to the social worker when the Veteran's gonna be ready for discharge. So, there might be a last-minute trip that comes in that might need to go six hours, our catchment area is very large and our Veterans come to this facility and our Lake City facility from all over our catchment area. Our catchment area is close to 14 thousand square miles and that's a huge geographical area to cover, 50 counties going into South Georgia, North Florida. So, if they don't tell us in a timely fashion that an escort is needed, sometimes we may have a delay in the discharge because it might be too late in the day to set up a transportation for the same day. That is a barrier (ID: 1014).”
3.2.7. Suggestions for Improvement
Improving the VA transportation system involves addressing various logistical, operational, and communication challenges. Suggestions for improvement included two subthemes: Streamline services and Communication strategies.
Streamline services. One recommendation was to implement the VTS program at all VA facilities to streamline services.
“One thing that would be really helpful is to have the Veteran transportation service program at all facilities because that service is for all Veterans, regardless of their service connection. So, you don't have to be eligible for anything other than that you're a Veteran. So that makes it more streamlined. There's one place to go for the rides and then if there's not enough services to meet the demand, then it would be very clear (ID: 1000).”
Another suggestion focused on consolidating transportation-related departments into a single, centralized unit. Consolidating various departments into a single unit would enhance communication and reduce redundancy. This one-stop shop model would help optimize the care and services provided to Veterans by ensuring all transportation needs are coordinated from one place.
“From a transportation standpoint, I think it would be good because we have separate departments. If we would put it all under one stop shop, so even the communication is good as it is, it can be better because we're in one area. So, I think there's a lot of redundancy that we can minimize that for us to be more optimal in their care and the services that we give (ID: 1004).”
Additionally, by hiring more drivers, the VA could save money compared to contracting out services to vendors. This would also allow for greater control over transportation services, ensuring that Veterans' needs are met more effectively.
“With transportation operations that includes the VA drivers themselves one of the things that helps us save money is it would be more conducive for us to hire more drivers to go take care of the need of the Veteran and have more control versus paying a vendor so much more money under contracts to get that done (ID: 1004).”
Communication strategies. Improving communication about eligibility criteria and available services would help Veterans understand what benefits they qualify for. Public affairs should actively disseminate information about travel reimbursement and ride-share programs to ensure Veterans are well-informed.
“We can do a better job with communicating the criteria of what makes a Veteran eligible for certain programs within the VA, specifically regarding transportation. It would be great if we had better communication in terms of our public affairs sending out information. Did you know that you might be available for travel reimbursement if you meet this criteria? Or did you know that you might be eligible to receive a ride via Uber, Lyft, or ride-share or some other program if you meet this criteria? Most problems revolve around communication or a lack of communication. We could do better with educating and informing veterans of what they might be eligible for (ID: 1014).”
An additional communication strategy included streamlining internal communication by building a communication nucleus where staff can interact directly. This approach would reduce the need for multiple phone calls and emails, leading to quicker decision-making and better service delivery.
“There's a lot of phone calls, emails, teams back and forth which waste time. I think there's a way that you could build a huge communications nucleus and put everybody in the same area where they can just say, hey man, do you know, can you look this up, is this good, and talking across aisles is a lot faster than making multiple phone calls or teams messages (ID: 1010).”
Expanding communication to include third-party services and staff services would ensure seamless coordination when there are gaps in transportation resources. This would help maintain consistent service levels and meet transportation needs effectively.
“We need a broader sense of communication with alternate stakeholders. Being able to communicate with the staff services or third-party services. To be able to say, we have a run of six patients coming out of Jacksonville, I do not have a driver. Here is the manifest, here is the point of contacts and having that level of communication would allow them to kind of encompass on a day that we may fall short (ID: 1012).”
In summary, the qualitative analysis of the VA transportation system reveals a complex interplay of strengths, weaknesses, opportunities, and threats. The qualitative analysis identified seven major themes. These themes—Complex System, Transportation Strengths, Transportation Weaknesses, ARSS Opportunities, ARSS Threats, Communication, and Suggestions for Improvement—offer a comprehensive view of the current state and potential future of VA transportation services. Table 2 includes the seven key themes and their respective take-home messages.
3.3. Findings Related to the Socio-Ecological Model
The qualitative data, organized within the socio-ecological model, presents a detailed view of the various factors influencing the VA transportation services (see Figure 1). This approach encompasses the seven main themes and associated subthemes, along with additional findings. The socio-ecological model captures the layered and interconnected influences at the individual, relational, community, and societal levels.
The individual level focuses on factors such as knowledge, perceptions, and experiences that influence the use of transportation services. Themes that fall under this level include Interviewee-related factors (perspectives of ideal transportation system, background/role, ARSS perspectives and knowledge), Veteran experiences (how individual access to transportation affects their ability to receive timely medical care), Veterans satisfaction (satisfaction levels with transportation services provided), and Transportation eligibility (how criteria affects access). These themes reflect the importance of understanding individual perspectives and experiences to improve service delivery. For instance, one participant described how they started using Uber for ambulatory Veterans. However, they encountered challenges with driver availability in certain areas, particularly in the North catchment area of NFLSGA region. This led to missed appointments, sometimes resulting in a six-month wait for the next available slot (ID: 1004). This indicates the need for a system that meets Veterans' expectations and needs, with clear transportation eligibility criteria to enhance accessibility for more Veterans.
The relational level examines the role of communication and interpersonal connections in influencing Veterans' access to and satisfaction with transportation services. Themes that fall under the relational level include VA drivers (Veterans serving Veterans), and Communication (staff to staff communication, and staff to Veteran communication). The involvement of Veterans as drivers or support staff fosters trust and satisfaction, creating a more relatable and supportive transportation experience. Effective communication is important for ensuring Veterans understand and utilize transportation services properly. Participants highlighted the importance of clear and efficient communication in enhancing service delivery and ensuring Veterans receive the support they need. For instance, one group has been working on a project with stakeholders from the VTS to develop a decision support tool. This tool is designed to help clinicians and administrators identify eligibility criteria, match them with Veterans' needs, and track these interactions within EPRS for better care coordination (ID: 1002).
The community level focuses on transportation organization, logistics, capacity, planning and evaluation processes, stakeholder collaboration, and specific challenges faced in different community settings. This level encompasses how community infrastructure, local policies, and community-specific needs and resources impact the VA transportation. Themes include VA transportation system goals, Different modes of transportation, Stakeholders, Physical environmental factors, Facility leadership, NFLSGA transportation system, System capacity, Logistics (drivers, vehicles, routes), VA transportation planning process, Evaluation process, Collaborative approach, Volunteer transportation limitations, Suggestions for improvement, and Suggestion for ARSS deployment. For example, one of the VA transportation system goals is to increase access to care by fostering stakeholder collaboration and understanding Veterans' needs (ID: 1010). However, achieving this goal requires careful assessment of each case to avoid setting unrealistic expectations and ensuring that transportation solutions are sustainable. In terms of physical environmental factors, one participant highlighted the challenges of workforce recruitment and retention in rural areas, identifying the difficulty of keeping drivers within the program (ID: 1002).
The societal level encompasses broad factors such as policies, federal funding, and organizational structures that shape the availability, quality, and accessibility of transportation services. Themes include Importance of transportation, Social determinants of health, Innovation (including concerns and technology access), Regulations and policies, No one-size-fits-all approach, Return on investment, Limited resources (federal funding), VA organization structure (in-house care vs. care in the community), Impact of COVID-19 , Suggestion for improvement, ARSS threats, and ARSS benefits. One participant emphasized the importance of transportation in meeting the social determinants of health for Veterans, noting that it contributes significantly to Veterans' health and well-being by ensuring they can attend primary care, specialty care, and mental health appointments, thereby preventing poor health outcomes (ID: 1002). Others noted how COVID-19 reduced the availability of DAV volunteer drivers (often older drivers), even after the pandemic, which has led to missed appointments for many Veterans and an increase in expenditures (ID: 1006 and 1004). Suggestions for improvement appeared at both the community and societal levels. Suggestions at the community level included adding more drivers, streamlining services (creating a one-stop shop and eliminating redundancy), covering more rides, and transporting more Veterans. At the societal level, improvements involved adjusting regulations, bringing Veterans' care back to VA facilities, and securing increased federal funding for transportation programs.
The levels of the socio-ecological model are interconnected, with changes at one level affecting outcomes at another. For instance, individual experiences (Individual Level) can influence communication (Relationship Level), which in turn can impact community logistics and stakeholder involvement (Community Level), ultimately shaped by federal policies and funding (Societal Level). Three main examples are illustrated below:
Impact of delays in care on Veterans' health and the need for improved stakeholder collaboration and communication. Transportation delays have a profound impact on Veterans' health, with effects observable across multiple levels of the socio-ecological model. At the individual level, participants reported that transportation delays are particularly detrimental to Veterans who lack reliable transportation and live far from medical facilities, which may exacerbate existing health conditions due to missed or delayed care (ID: 1006, 1004, 1014). Confusion over eligibility criteria further limits access to services and may lead to gaps in care (ID: 1014). At the relational level, effective communication is important for coordinating timely transportation, yet breakdowns in coordination prolong delays. Clear guidance on eligibility, shared through multiple channels, may mitigate these issues (ID: 1004). At the community level, the availability and reliability of transportation options play a significant role in either mitigating or exacerbating delays. This is particularly critical in rural areas where transportation infrastructure may be lacking. Stakeholders, including social workers, transportation coordinators, and leadership, must work together to develop tools and processes that improve service delivery, such as the decision support tool for identifying eligibility criteria and matching them with Veterans' needs (ID: 1002). At the societal level, policies and funding allocations are needed to create a robust transportation system capable of meeting Veterans' needs. Overall, by enhancing communication and coordination at the relational level, improving transportation infrastructure and planning at the community level, and securing robust policies and funding at the societal level, the VA can better support Veterans' access to timely medical care (individual level).
Veterans satisfaction and interactions with VA Drivers. Veterans' satisfaction and trust in VA transportation services are significantly influenced by the personal connections and understanding exhibited by VA drivers. At the individual and relational levels, Veterans often express a preference for VA drivers over contractors due to their deeper personal connections and familiarity with their specific needs (ID: 1010, 1006, 1008). Veterans often feel more comfortable and understood when transported by another Veteran who shares similar experiences, fostering a sense of trust and enhancing their overall satisfaction with the transportation services (ID: 1000, 1002, 1006, 1008). At the community level, ensuring that VA drivers are well-trained, adequately compensated, and available to meet the transportation needs of Veterans is important to maintaining customer satisfaction. At the societal level, policies and funding should prioritize hiring and training Veterans as drivers to sustain Veterans’ trust and satisfaction. By prioritizing the employment of VA drivers and ensuring they are well-trained and supported, both at the community and societal levels, the VA can maintain high satisfaction levels and trust among Veterans.
Addressing system capacity and exploring ARSS opportunities in VA transportation. Addressing system capacity and integrating ARSS in VA transportation is important for improving service efficiency. At the community level, a shortage of drivers significantly impacts the ability to meet demand (ID: 1000, 1002, 1004, 1006, 1008, 1010, 1012). Challenges such as workforce recruitment and retention, particularly in rural areas, indicate the need for consolidating transportation-related departments into a centralized unit to enhance communication and reduce redundancy (ID: 1002, 1004). At the societal level, government funding and policies play a key role in resource allocation to ensure adequate staffing and vehicle procurement. Additionally, leveraging ARSS may alleviate staffing constraints and enhance transportation capacity, especially in urban areas where potential reliable access points may help streamline services (ID: 1008, 1004). However, ARSS faces challenges in rural areas due to complex routes, connectivity issues, and limited accessibility for Veterans with disabilities. To address these concerns, shuttle attendants, such as social workers, could assist passengers and foster trust among Veterans resistant to new technology. Deployment should focus on short trips and urban communities where infrastructure supports ARSS, with potential applications for shuttle services within hospital campuses and large VA facilities to enhance intra-campus mobility.
4. Discussion
The research team conducted semi-structured interviews with eight VA transportation stakeholders to understand the strengths and weaknesses of the current system and to explore future plans for ARSS. Participants were full-time employees with extensive experience in the VA transportation system. This ensured that the insights gathered were well-informed by years of practical engagement. However, the relatively small sample size may not encompass the full diversity of experiences and viewpoints present within the VA transportation workforce. Geographically, the participants were spread across diverse locations, including Florida, Georgia, New York, and Wyoming, although a significant majority (five out of eight) were based in Florida. The concentration in Florida might have skewed the findings towards issues and solutions more pertinent to that state, potentially overlooking those from other regions. The participants held a range of roles within the transportation system, encompassing a wide array of responsibilities. This indicates the multifaceted nature of the VA transportation system and the collaborative efforts required to manage it effectively. Participants represented various transportation sectors and departments, which helped capture a broad view of the transportation system's operational landscape and the interconnectedness of its various components.
The Complex System theme identifies the multifaceted nature of the VA transportation services, shaped by diverse transportation modes, regulatory constraints, various stakeholders, ongoing processes of change, and access to care. This complexity aligns with current literature which identify challenges in providing transportation services to Veterans due to varying needs, such as medical conditions, geographical location, socio-economic status, and systemic constraints including regulatory policies and resource limitations [38,39]. The subtheme, Different modes of transportation, reveals the tailored services available to Veterans based on their specific needs and eligibility. This variety, while beneficial, also reflects the challenges of coordinating multiple services, as supported by participant responses. Regulations and policy also emerged as significant factors influencing the delivery of transportation services. The study identified the complexities and rigidities of the regulatory environment, which often hinder the flexibility needed to address local transportation needs. Diverse stakeholders, including hospital personnel and social workers, play an important role in service coordination. Process of change reflects ongoing adaptations, such as rural shuttles and Uber Health, though barriers like low uptake and technological challenges persist. Ultimately, access to care remains a key issue, with eligibility restrictions and vendor limitations exacerbating transportation-related healthcare barriers. This aligns with existing studies that identify transportation as a significant barrier to healthcare access for Veterans, particularly those in rural areas [40,41].
The Transportation Strengths theme identifies key advantages of the VA transportation system, including flexibility, collaboration, superior customer service, and the benefits of employing Veterans as drivers. The NFLSGA region exemplifies adaptability by accommodating unique transportation needs, such as follow-up transport for surgery patients from distant areas, aligning with calls for personalized healthcare transportation solutions [39]. Collaboration between VA transportation and social work services, along with partnerships like those with the ORH, enhances coordinated care and helps bridge service gaps in rural areas, a strategy that has been shown to be effective in improving access to care in underserved regions [42]. The VA's personalized, door-to-door service and diverse transportation options—ranging from staff-operated to volunteer and third-party systems—enhance service flexibility, particularly for Veterans with disabilities that require special attention. Employing Veterans as drivers fosters camaraderie and empathy, improving service quality and patient satisfaction [43]. Additionally, holding VA drivers to higher standards ensures consistent service quality, making Veteran drivers a valuable asset in creating a supportive transportation environment.
The Transportation Weaknesses theme identified challenges within the VA transportation system, including limited resources, volunteer transportation limitations, and restrictive eligibility criteria. Limited resources emerged as a barrier, with participants highlighting funding constraints and staffing shortages that impact service sustainability and expansion. These issues are exacerbated by the high costs associated with outsourcing care to community providers, which diverts funds that could otherwise enhance the in-house transportation capabilities. The financial pressures are particularly concerning given Veterans' preference for receiving care within the VA system, where relationships and understanding of their unique needs are stronger. This aligns with existing literature, which cites funding limitations as a major hurdle in the delivery of transportation services [43]. Volunteer transportation limitations were another significant weakness identified. Participants noted the inconsistency and unreliability of volunteer drivers, which affects the dependability of transportation for Veterans' appointments. The COVID-19 pandemic has further strained this system, reducing the availability of volunteers. While volunteers provide a valuable service, their unreliability compared to paid staff poses a persistent challenge. Additionally, the restrictive eligibility criteria for transportation benefits were identified as a barrier. Participants pointed out that these criteria prevent many Veterans from accessing necessary services. Thus, the need for better communication regarding these criteria and potential flexibility to accommodate more Veterans underscores the importance of education and adaptability in service provision [40].
The ARSS Opportunities theme identify the potential benefits and deployment strategies of ARSS within the VA transportation system. Participants identified ARSS as a solution to alleviate staffing shortages by expanding the pool of available employees for transportation. ARSS may streamline transportation logistics by providing consistent and reliable access points in cities, with shorter delay times, less variation in expected delays per trip, and reduced vehicle miles traveled [44]. For rural Veterans, ARSS may offer a standardized, stress-free final leg to urban centers for care [42,45]. By reducing the stress and uncertainty associated with long-distance travel, ARSS may enhance the overall transportation experience for rural Veterans. Deployment strategies include using ARSS for short trips, hospital campus mobility, and metropolitan areas where existing infrastructure supports geofenced Level 4 autonomy [46,47]. Additionally, deploying ARSS within Veteran communities may support transportation for medical appointments, grocery shopping, and recreational activities, addressing multiple social determinants of health.
While ARSS offer potential benefits, their implementation faces threats, including logistical challenges, limitations in serving PWDs, and adoption barriers. In rural areas, complex routes and diverse travel needs make standardizing ARSS difficult, compounded by infrastructure limitations and varied road conditions [46]. Concerns about satellite or tower connectivity further threaten AV reliability in less urbanized regions. However, as improving rural internet connectivity remains a political and economic priority, these challenges may diminish over time [48]. Serving PWDs poses a significant challenge for ARSS, as participants expressed concerns about the lack of human assistance for Veterans using wheelchairs, scooters, and other mobility aids. The absence of a driver could hinder accessibility, aligning with literature identifying the need for human support in transportation for PWDs [49]. Ensuring vehicles are equipped with necessary modifications, such as wheelchair lifts, remains a key concern. Concerns about ARSS adoption were also prevalent among participants, particularly regarding trust and technology acceptance. Veterans may experience anxiety or stress about using a driverless vehicle, which could hinder the adoption of ARSS. This finding is supported by studies that show older adults and PWDs having less positive attitudes toward and acceptance of AVs compared to younger individuals [50,51]. To potentially solve this problem, participants strongly recommended the presence of a shuttle assistant to help PWDs and improve users' feelings of safety, trust, and overall satisfaction. Lastly, equity concerns arise for Veterans without cell phone access, including homeless Veterans, reflecting broader challenges in digital inclusion and technology access [52].
The Communication theme identifies the important role of effective communication in the VA transportation system, both between Veterans and staff and among internal staff. While Veterans may be aware of transportation services, they often struggle to identify the correct point of contact for scheduling. Ensuring clear connections to the appropriate personnel is important for providing timely and effective transportation support [53]. Participants emphasized the need for clear guidance on transportation service eligibility through multiple communication channels, which aligns with best practices in public health communication [54]. In fact, overreliance on internal VA systems and referrals rather than direct outreach can make Veterans feel like they are being bounced between departments. Thus, streamlining communication strategies and expanding outreach efforts may help ensure Veterans are fully aware of available transportation services and eligibility criteria. Internally, delays in communication between inpatient teams and social workers regarding discharge schedules lead to last-minute trip requests that are difficult to accommodate, particularly in large service areas like NFLSGA. Strengthening collaboration and addressing communication barriers are important for improving service delivery and ensuring timely transportation support.
The Suggestions for Improvement theme addressed logistical, operational, and communication challenges within the VA transportation system. Participants recommended implementing the VTS program at all VA facilities to create a uniform service accessible to all Veterans, simplifying access and ensuring consistency. Another key suggestion was consolidating transportation-related departments into a centralized unit. The current decentralized approach leads to inconsistencies [43], and a "one-stop shop" model could improve communication, reduce redundancy, and enhance service delivery for Veterans. Participants recommended hiring more drivers instead of relying on contracted services to reduce costs and improve control over transportation. With VHA medical transportation expenses rising—$750 million spent on Beneficiary Travel in FY 2010—cost-effectiveness is a growing concern [43]. Enhancing communication about eligibility criteria and available services was also suggested, with public affairs playing a key role in disseminating information on travel reimbursement and ride-share programs. Streamlining internal communication through a centralized hub could reduce redundant calls and emails, leading to faster decision-making. Additionally, expanding communication to third-party vendors and VA transportation departments would improve coordination and address gaps in transportation resources.
The qualitative data, organized within the socio-ecological model, provides a comprehensive view of the factors influencing VA transportation services at individual, relational, community, and societal levels. The interconnections between the levels of the socio-ecological model show the complexity of the VA transportation system and indicate the necessity for a holistic approach to service improvement. Relational aspects, such as communication and trust between Veterans and staff, directly influence individual experiences with transportation. Communication also affects community-level logistics and stakeholder involvement, which are ultimately influenced by broader societal factors like policies and funding. For instance, the need for clear communication about transportation eligibility and services is important at the individual level but requires effective relational-level strategies to ensure Veterans are informed. Addressing transportation challenges requires coordinated efforts across all socio-ecological model levels, ensuring that individual needs are met through effective communication, robust community logistics, and supportive societal policies. This holistic approach is necessary for improving Veterans' access to timely and reliable transportation services, ultimately enhancing their overall satisfaction and health outcomes.
5. Conclusions
This study explored key VA transportation stakeholders' perceptions through semi-structured interviews, identifying strengths and weaknesses of the VA transportation system, as well as the opportunities and threats of the potential implementation of ARSS. Using the socio-ecological model, the study identified factors across individual, relational, community, and societal levels that influence Veterans' transportation access. Strengths included personalized service, flexibility, Veteran drivers, and collaborative care, while challenges such as funding constraints, staff shortages, volunteer limitations, and restrictive eligibility criteria were identified. ARSS presents opportunities to alleviate some of these issues, particularly by freeing up human resources and addressing social determinants of health in urban areas, though logistical complexities and accessibility for Veterans with disabilities remain concerns. Suggestions for improvement included streamlining and consolidating transportation-related departments, hiring more drivers, and enhancing communication strategies to ensure Veterans are well-informed and connected to appropriate services. These findings provide an overview of the VA transportation system's current state, indicating areas for improvement and offering recommendations for leveraging the identified opportunities. By addressing the weaknesses and capitalizing on the strengths and opportunities, the VA may enhance its transportation services to better meet Veterans' needs. This study offers insights for VA decision-makers, transportation planners, and industry partners to advocate for policy adjustments and collaborative efforts to optimize service delivery.
5.1. Limitations, Strengths, and Future Directions
Some participants may have been hesitant to respond due to concerns about professional implications; however, confidentiality was assured, and open-ended questions allowed discretion in answering [28]. An inherent bias of participants may be present, as those who agreed to participate might have had more positive attitudes and perceptions towards AVs. The absence of representatives from the Beneficiary Travel Program and Veterans Transportation and Community Living Initiative may have limited insights into these programs. Additionally, the geographic concentration of participants in Florida may have skewed findings toward state-specific issues. The small sample size may have limited the diversity of perspectives, and the study could have benefitted from additional interviews, particularly with representatives from the aforementioned programs that were not included.
A key strength of this study is the knowledge and experience of participants in VA transportation, representing various roles, sectors, and departments. The semi-structured interview format enabled in-depth discussions, while Zoom facilitated participation across six areas in four states. These qualitative insights, although limited to the geographic regions as previously stated, may provide initial guidance for decision-makers and stakeholders seeking to enhance transportation services for Veterans. Future research may focus on understanding the barriers to implementing transportation solutions for Veterans, particularly in rural areas where funding limitations and staffing shortages persist. Exploring strategies to enhance coordination among VA transportation stakeholders, streamline services, and improve communication about eligibility criteria will be important in reducing inefficiencies and increasing service accessibility. The development and evaluation of decision support tools, such as those designed to assist clinicians and administrators in matching Veterans' needs with appropriate transportation options, may be considered to improve care coordination.
Additionally, the integration of ARSS presents an initial promising avenue for addressing transportation gaps, particularly in underserved areas. Our research team piloted an AS in a rural area to evaluate its benefits and effectiveness. Strengths and opportunities identified in the pilot suggest that AS deployment warrants further consideration, especially for first-mile–last-mile service. Weaknesses and threats were noted, some are being addressed in the next generation of the AS, including a redesigned chassis for improved on-road performance, enhanced accessibility and comfort features, and operational refinements such as routine foliage trimming and optimized satellite antenna placement to improve communication. A longer, stable deployment may further enhance these elements while providing additional insights into feasibility and scalability. Pilot testing within VA facilities, rural communities, and urban settings may provide insights into feasibility, scalability, and effectiveness in reducing transportation-related healthcare barriers. Furthermore, strengthening collaboration between VA transportation programs and social work services may enhance efforts to address the social determinants of health, ultimately improving Veterans’ access to essential services and overall well-being.
Author Contributions
Conceptualization, S.C. and I.W.; methodology, I.W.; validation, N.S.; formal analysis, I.W. and S.W.; investigation, I.W.; resources, S.C.; data curation, I.W.; writing—original draft preparation, I.W.; writing—review and editing, S.C., S.W., and N.S.; visualization, I.W. and S.W.; supervision, S.C.; project administration, I.W.; funding acquisition, S.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the VA Office of Rural Health, project number P0213747.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding authors.
Acknowledgments
The research acknowledges the support provided by the University of Florida's Institute for Driving, Activity, Participation, & Technology. Additionally, the collaboration and resources of the North Florida/South Georgia Veterans Health System, the Malcom Randall VA Medical Center, and the Gainesville Office of Rural Health were pivotal to the successful execution of this study.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- US Department of Veterans Affairs. About the department: Veterans health care. 2025. Available online: https://department.va.gov/about/#:~:text=VA's%20Veterans%20Health%20Administration%20is:million%20enrolled%20Veterans%20each%20year (accessed on 28 February 2025).
- US Department of Veterans Affairs. Veterans Health Administration: About VHA. 2025. Available online: https://www.va.gov/health/aboutvha.asp (accessed on 28 February 2025).
- US Department of Veterans Affairs. Highly Rural Transportation Grants [Fact Sheet]. 2022. Available online: https://www.va.gov/HEALTHBENEFITS/resources/publications/IB10-761_VA_HRTG_factsheet.pdf (accessed on 28 February 2025).
- US Department of Veterans Affairs. Veterans Transportation Service (VTS). 2019. Available online: https://www.va.gov/healthbenefits/vtp/veterans_transportation_service.asp (accessed on 28 February 2025).
- Burkhardt, J. E., Rubino, J. M., & Yum, J. Improving Mobility for Veterans; Transportation Research Board, 2011. https://nap.nationalacademies.org/catalog/14507.
- Brownley, J., Welch, P., & Stabenow, D. Brownley, Welch, and Stabenow introduce legislation to increase travel reimbursement for veterans [Press Release]. 2023. Available online: https://juliabrownley.house.gov/brownley-welch-and-stabenow-introduce-legislation-to-increase-travel-reimbursement-for-veterans/ (accessed on 28 February 2025).
- Hussey, P.S., Ringel, J.S., Ahluwalia, S., Price, R.A., Buttorff, C., Concannon, T.W., Lovejoy, S.L., Martsolf, G.R., Rudin, R.S., Schultz, D. and Sloss, E.M. Resources and capabilities of the Department of Veterans Affairs to provide timely and accessible care to veterans. Rand Health Quarterly 2016, 5(4), 14. https://pmc.ncbi.nlm.nih.gov/articles/PMC5158229/.
- Shen, Y., Zhang, H., & Zhao, J. Integrating shared autonomous vehicle in public transportation system: A supply-side simulation of the first-mile service in Singapore. Transportation Research Part A: Policy and Practice 2018, 113, 125-136. [CrossRef]
- Whitmore, A., Samaras, C., Hendrickson, C.T., Matthews, H.S. and Wong-Parodi, G. Integrating public transportation and shared autonomous mobility for equitable transit coverage: A cost-efficiency analysis. Transportation Research Interdisciplinary Perspectives 2022, 14, 100571. [CrossRef]
- Hwangbo, S.W., Stetten, N.E., Wandenkolk, I.C., Li, Y. and Classen, S. Lived experiences of people with and without disabilities across the lifespan on autonomous shuttles. Future Transportation 2024, 4(1), 27-45. [CrossRef]
- Classen, S., Wandenkolk, I.C., Mason, J., Stetten, N., Hwangbo, S.W. and LeBeau, K. Promoting veteran-centric transportation options through exposure to autonomous shuttles. Safety 2023, 9(4), 77. [CrossRef]
- Kim, H., & Doerzaph, Z. Road user attitudes toward automated shuttle operation: Pre and post-deployment surveys. Proceedings of the Human Factors and Ergonomics Society Annual Meeting 2022, 66(1), 315-319. [CrossRef]
- Benyahya, M., Kechagia, S., Collen, A., & Nijdam, N. A. The interface of privacy and data security in automated city shuttles: The GDPR analysis. Applied Sciences 2022, 12(9), 4413. [CrossRef]
- Tisdell, E. J., Merriam, S. B., & Stuckey-Peyrot, H. L. Qualitative research: A guide to design and implementation. Lohn Wiley & Sons, San Francisco, CA, 2025.
- Kahlke, R.M. Generic qualitative approaches: Pitfalls and benefits of methodological mixology. International Journal of Qualitative Methods 2014, 13(1), 37-52. [CrossRef]
- Portney, L. G., & Watkins, M. P. Foundations of clinical research: Applications to practice. Pearson/Prentice Hall, Upper Saddle River, NJ, 2009.
- Patton, M.Q. Qualitative research & evaluation methods. Sage, 2002.
- Goodman, L.A. Snowball sampling. The Annals of Mathematical Statistics 1961, 32(1), 148-170. https://www.jstor.org/stable/2237615.
- MacDougall, C., & Fudge, E. Planning and recruiting the sample for focus groups and in-depth interviews. Qualitative Health Research 2001, 11(1), 117-126. [CrossRef]
- Cornwall, A., & Jewkes, R. What is participatory research? Social Science & Medicine 1995, 41(12), 1667-1676. [CrossRef]
- Glaser, B., & Strauss, A. Discovery of grounded theory: Strategies for qualitative research. Routledge, NY, 1967. [CrossRef]
- Saunders, B., Sim, J., Kingstone, T., Baker, S., Waterfield, J., Bartlam, B., Burroughs, H. and Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Quality & Quantity 2018, 52, 1893-1907. [CrossRef]
- Hennink, M. and Kaiser, B.N. Sample sizes for saturation in qualitative research: A systematic review of empirical tests. Social Science & Medicine 2022, 114523. [CrossRef]
- Archibald, M.M., Ambagtsheer, R.C., Casey, M.G. and Lawless, M. Using zoom videoconferencing for qualitative data collection: Perceptions and experiences of researchers and participants. International Journal of Qualitative Methods 2019, 18. [CrossRef]
- Gurl, E. SWOT analysis: A theoretical review. Journal of International Social Research 2017, 10(51), 994-1006. [CrossRef]
- Microsoft. Security and Compliance for Microsoft Teams. 2025. Available online: https://www.safeguardcyber.com/platform/channels-we-protect/ms-teams?gclid=CjwKCAjw__ihBhADEiwAXEazJg21St8fe43jrZFOLif7IxSFdC-oHHQvLoLixVcuuTJp0edXqrQmEBoCibgQAvD_BwE (accessed on 28 February 2025).
- Thunberg, S. and Arnell, L. Pioneering the use of technologies in qualitative research–A research review of the use of digital interviews. International Journal of Social Research Methodology 2022, 25(6), 757-768. [CrossRef]
- Taylor, R.R. Kielhofner's research in occupational therapy: Methods of inquiry for enhancing practice. FA Davis, 2017.
- Parekh, T., Kumar, B.V., Maheswar, R., Sivakumar, P., Surendiran, B. and Aileni, R.M. Intelligent transportation system in smart city: A SWOT analysis. In Challenges and Solutions for Sustainable Smart City Development, Springer, 2021. [CrossRef]
- R Core Team. R: A language and environment for statistical computing. 2023. Available online: https://www.R-project.org/.
- QSR International Pty Ltd. NVivo qualitative data analysis software (Version 12) [Computer Software]. 2018.
- Braun, V. and Clarke, V. Using thematic analysis in psychology. Qualitative Research in Psychology 2006, 3(2), 77-101. [CrossRef]
- Kondracki, N.L., Wellman, N.S. and Amundson, D.R. Content analysis: Review of methods and their applications in nutrition education. Journal of Nutrition Education and Behavior 2002, 34(4), 224-230. [CrossRef]
- Morse, J.M. and Field, P.A. Nursing research: The application of qualitative approaches. Nelson Thornes, 1995.
- Krefting, L. Rigor in qualitative research: The assessment of trustworthiness. The American Journal of Occupational Therapy 1991, 45(3), 214-222. [CrossRef]
- Knafl, K.A. and Breitmaye, B.J. Triangulation in qualitative research: Issues of conceptual clarity and purpose. In Qualitative Nursing Research: A Contemporary Dialogue, JM Morse, Aspen, Rockville, MD, 1991.
- Miles, M.B. and Huberman, A.M. Qualitative data analysis: An expanded sourcebook. Sage, 1994.
- Buzza, C., Ono, S.S., Turvey, C., Wittrock, S., Noble, M., Reddy, G., Kaboli, P.J. and Reisinger, H.S. Distance is relative: Unpacking a principal barrier in rural healthcare. Journal of General Internal Medicine 2011, 26, 648-654. [CrossRef]
- Syed, S.T., Gerber, B.S. and Sharp, L.K. Traveling towards disease: Transportation barriers to health care access. Journal of Community Health 2013, 38, 976-993. [CrossRef]
- Washington, D.L., Bean-Mayberry, B., Riopelle, D. and Yano, E.M. Access to care for women veterans: Delayed healthcare and unmet need. Journal of General Internal Medicine 2011, 26, 655-661. [CrossRef]
- Zullig, L.L., Jackson, G.L., Provenzale, D., Griffin, J.M., Phelan, S. and Van Ryn, M. Transportation—A vehicle or roadblock to cancer care for VA patients with colorectal cancer? Clinical Colorectal Cancer 2012, 11(1), 60-65. [CrossRef]
- US Department of Veterans Affairs. Office of Rural Health: Rural Veterans. 2024. Available online: https://www.ruralhealth.va.gov/aboutus/ruralvets.asp (accessed on 28 February 2025).
- Burkhardt, J.E., Rubino, J.M. and Yum, J. Improving Mobility for Veterans. Transportation Research Board, 2011. https://nap.nationalacademies.org/catalog/14507.
- Zhang, W., Guhathakurta, S., Fang, J. and Zhang, G. The performance and benefits of a shared autonomous vehicles based dynamic ridesharing system: An agent-based simulation approach. In Transportation Research Board 94th Annual Meeting, 2015.
- Schlüter, J., Bossert, A., Rössy, P. and Kersting, M. Impact assessment of autonomous demand responsive transport as a link between urban and rural areas. Research in Transportation Business & Management 2021, 39, 100613. [CrossRef]
- Prioleau, D., Dames, P., Alikhademi, K. and Gilbert, J.E. Autonomous vehicles in rural communities: Is it feasible? IEEE Technology and Society Magazine 2021, 40(3), 28-30. [CrossRef]
- Mohiuddin, H. Planning for the first and last mile: A review of practices at selected transit agencies in the United States. Sustainability 2021, 13(4), 2222. [CrossRef]
- Carney, C., Johnson-Kaiser, T. and Ahmad, O. Automated Vehicles in Rural America: What’s the Holdup? Transportation Research Board 2023, 347, 8-12. https://www.trb.org/Publications/Blurbs/183152.aspx.
- Bezyak, J.L., Sabella, S.A. and Gattis, R.H. Public transportation: An investigation of barriers for people with disabilities. Journal of Disability Policy Studies 2017, 28(1), 52-60. [CrossRef]
- Bennett, R., Vijaygopal, R. and Kottasz, R. Attitudes towards autonomous vehicles among people with physical disabilities. Transportation Research Part A: Policy and Practice 2019, 127, 1-17. [CrossRef]
- Dicianno, B.E., Sivakanthan, S., Sundaram, S.A., Satpute, S., Kulich, H., Powers, E., Deepak, N., Russell, R., Cooper, R. and Cooper, R.A. Systematic review: Automated vehicles and services for people with disabilities. Neuroscience Letters 2021, 761, 136103. [CrossRef]
- Dianin, A., Ravazzoli, E. and Hauger, G. Implications of autonomous vehicles for accessibility and transport equity: A framework based on literature. Sustainability 2021, 13(8), 4448. [CrossRef]
- Cacace, S., Smith, E., Desmarais, S. and Alders, E. Locale matters: Regional needs of US military service members and veterans. Military Behavioral Health 2022, 10(3), 221-234. [CrossRef]
- Parvanta, C., Nelson, D.E. and Harner, R.N. Public health communication: Critical tools and strategies. Jones & Bartlett Learning, 2017.
Figure 1.
Summary of qualitative data organized by the socio-ecological model levels.
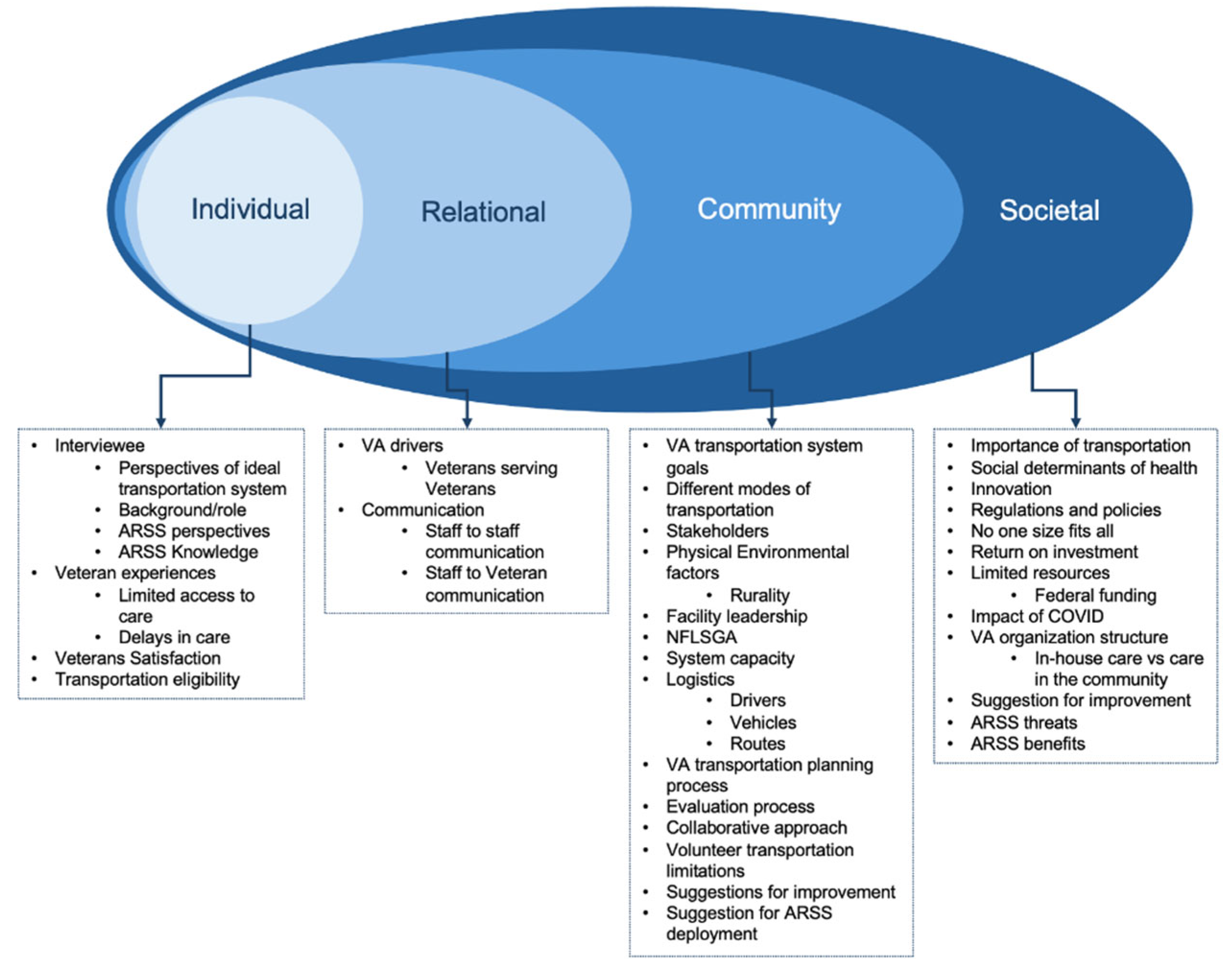

Table 1.
Main qualitative themes and subthemes and respective operational definitions.
| Themes/Subthemes | Operational Definitions of Themes and Subthemes |
| Complex System | The VA transportation system consists of multiple interconnected components, including the various modes of transportation, regulatory frameworks, diverse stakeholders, processes of change, and access to care. Each element contributes to the system’s complexity and functionality. |
| Different modes of transportation | Includes special mode transport for wheelchair and stretcher-bound patients, Uber/Lyft and volunteer services for ambulatory Veterans, and Beneficiary Travel for travel reimbursement. MAS outsources to vendors for trips to Veterans that are special mode. Each mode of transportation addresses different needs. |
| Regulations and policy | The regulatory structure is complex, involving multiple layers of rules and guidelines that influence funding, programs, and standard operating procedures for day-to-day operations. This complexity often leads to challenges in service provision, requiring flexibility and adaptation by transportation services. |
| Diverse stakeholders | The system involves Veterans, caregivers, healthcare personnel, the ORH, the Veterans Experience Office, and community partners such as the Disabled American Veterans (DAV). Stakeholders have a unique role in determining transportation needs, organizing services, managing complaints and working toward service improvements. |
| Process of change | The VA is integrating new technologies and piloting new services to improve accessibility. Challenges include technology reliance, coordination issues, and engagement difficulties. Efforts focus on identifying transportation deserts, expanding resources, and overcoming barriers to enhance service provision. |
| Access to care | Reliable transportation impacts Veterans' health outcomes by providing access to primary, specialty, and mental health services. High outsourcing costs emphasize the need to bring care back to VA facilities. Strict eligibility criteria and limited service availability pose significant barriers, especially in rural areas. |
| Transportation Strengths | Strengths include the NFLSGA unique ability to provide a wide range of flexible and adaptive transportation services. Strong collaboration between various transportation departments and external contractors. Personalized, high-quality services facilitated by trained and dedicated drivers, many of whom are Veterans themselves. |
| NFLSGA unique | NFLSGA is unique due to its geographic reach and the range of services it offers. It is flexible and adaptable and transport those who may not qualify under Beneficiary Travel criteria. The integration of services under one umbrella allows NFLSGA to cater to a wide array of needs, making it distinct from other facilities. |
| Collaborative approach | Collaborative efforts with various stakeholders such as social workers, nurses, and external contractors. This integrated approach ensures coordinated care and addresses the social determinants of health by working closely with all stakeholders involved in Veterans' healthcare. |
| Better customer service product | The VA transportation services are tailored to Veterans' needs, providing door-to-door service, better tracking, and higher safety standards. This personalized approach enhances Veterans overall experience. |
| Drivers working for the VA | The employment of Veterans as drivers, who share a unique bond and understanding with their passengers. This Veteran-to-Veteran interaction provides comfort and encouragement to Veterans. The high training standards and commitment to service further enhance the reliability and quality of the transportation provided. |
| Transportation Weaknesses | Limited resources, such as insufficient funding, manpower, and vehicles. Reliance on volunteer transportation presents challenges, including inconsistency, and restrictions on the types of patients that can be transported. Strict eligibility criteria further complicate access to transportation services. |
| Limited resources | Insufficient manpower, vehicles, and funding to meet the transportation demands of Veterans. This impacts the ability to provide timely and effective transportation services, as highlighted by the constraints of staffing and vehicle availability due to budget cuts and funding limitations. |
| Volunteer transportation limitations | Challenges in relying on volunteers for transportation services, including inconsistency of volunteer availability, lack of medical training, and restrictions on the types of patients they can transport. |
| Eligibility | Strict criteria that Veterans must meet to qualify for certain transportation services. The criteria often exclude Veterans who do not meet specific administrative or clinical requirements, thereby limiting their access to transportation services and impacting their access to healthcare. |
| ARSS Opportunities | Potential advantages and strategic recommendations for deploying ARSS. Perceived benefits include increased efficiency, resource reallocation, and improved accessibility for underserved populations. Suggestions for deployment include its integration in urban areas and hospital campuses. |
| Perceived benefits | Perceived benefits include the potential for increased efficiency and resource allocation within transportation services. By automating aspects of transportation, human resources can potentially be reallocated to other tasks. ARSS may improve accessibility for Veterans by providing consistent and reliable transportation options. |
| Suggestions for ARSS deployment | Implementing fixed routes, focusing on short trips, and providing transportation services in small communities. Serving able and ambulatory Veterans and deployment in urban areas as a last leg of trip. Incorporating ARSS in hospital campuses and parking lots may benefit both Veterans and employees. |
| ARSS Threats | The ARSS threats are the potential challenges and barriers that could impede the effective implementation and operation of ARSS. These threats encompass logistical, accessibility, and adoption issues. |
| ARSS logistics | Limited application for rural Veterans due to varied trips and geographical components. Funding limitations, connectivity issues, road conditions, operation constraints and the suitability of vehicles for different terrains and weather conditions, and limited reach due to reliance on fixed routes. |
| Serving PWDs | Serving PWDs in the context of ARSS involves ensuring that these services are accessible and accommodating to individuals with mobility challenges. This includes having personnel available to assist, which may be challenging with AVs that lack onboard staff to help with wheelchairs, scooters, or other assistive devices. |
| ARSS adoption | Factors influencing adoption include trust in the technology, comfort levels with driverless vehicles, and the perceived reliability of these services. This is particularly challenging for older Veterans, those living in rural areas, homeless Veterans and those with no access to technology or limited technological proficiency. |
| Communication | Encompasses the methods and effectiveness of information exchange between staff members and between staff and Veterans. It involves ensuring that all parties are informed about transportation options, eligibility criteria, scheduling processes, and service availability. |
| Staff to staff communication | Effective communication is important for coordinating transportation for Veterans. Challenges include timely communication between inpatient teams and social workers, which can delay discharges. Regular and structured communication among departments is needed to ensure smooth operations and timely transportation services. |
| Veteran and staff communication | Clear communication between Veterans and VA staff ensures Veterans are aware of the transportation services available to them and understand the eligibility criteria. This involves disseminating information through various channels and ensuring Veterans are connected to the right personnel for scheduling transportation. |
| Suggestions for Improvement | Streamline services by integrating departments under a unified system. The focus is on reducing redundancy, improving coordination, and ensuring that Veterans have better access to transportation options through clear eligibility criteria and efficient scheduling processes. |
| Streamline services | Consolidate departments and services under a unified system to reduce redundancy and improve efficiency. By centralizing services, the VA can enhance coordination, reduce operational delays, and better manage resources. This also includes hiring more drivers and transportation staff and reducing reliance on external vendors. |
| Communication strategies | Enhancing communication strategies includes improving internal communication within the VA and external communication with Veterans. Developing a centralized communication hub and utilizing public affairs to disseminate information about transportation eligibility and services can improve awareness and access. |
Table 2.
Key themes and respective take-home messages.
| Theme | Subthemes | Take-Home Messages |
| Complex System | Different modes of transportation, Regulations and policy, Diverse stakeholders, Process of change, Access to care | The VA transportation system is multifaceted, involving a variety of transportation options, regulatory challenges, diverse stakeholders, ongoing changes, and access to care issues. Flexibility and adaptability are important in addressing these complexities. |
| Transportation Strengths | NFLSGA unique, Collaborative approach, Better customer service product, Drivers working for the VA | Strengths include the unique aspects of the NFLSGA system due to its geographical size and transportation flexibility; a collaborative care model; personalized customer service; and the employment of Veterans as drivers, enhancing satisfaction and service quality. |
| Transportation Weaknesses | Limited resources, Volunteer transportation limitations, Eligibility | Weaknesses include funding constraints, a shortage of staff and drivers, inconsistency and reliability issues with volunteer drivers, and restrictive eligibility criteria. Addressing staffing shortages and budget constraints is essential for improving service delivery. |
| ARSS Opportunities |
Perceived benefits, Suggestions for ARSS deployment | ARSS may expand the pool of transportation employees, provide reliable access points in urban areas, and assist rural Veterans by standardizing and easing final leg journeys. ARSS may alleviate staffing constraints and offer a reliable solution for short trips. |
| ARSS Threats | ARSS logistics, Serving PWDs, ARSS adoption | Threats include logistical challenges in rural areas, connectivity and safety issues, the ability to serve Veterans with disabilities, and adoption barriers due to trust and technology acceptance issues. Threats need to be addressed to support ARSS implementation. |
| Communication | Staff to staff communication, Veteran and staff communication | Effective communication between Veterans and staff, as well as among staff members, is important for ensuring awareness and coordination of transportation services. Improving communication strategies can enhance service delivery and Veteran satisfaction. |
| Suggestions for Improvement | Streamline services, Communication strategies | Streamline services by implementing the VTS program at all facilities or consolidating departments into a centralized unit to reduce redundancy and improve efficiency. Hire more drivers and enhance communication about eligibility criteria. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



