Submitted:
07 March 2025
Posted:
10 March 2025
You are already at the latest version
Abstract
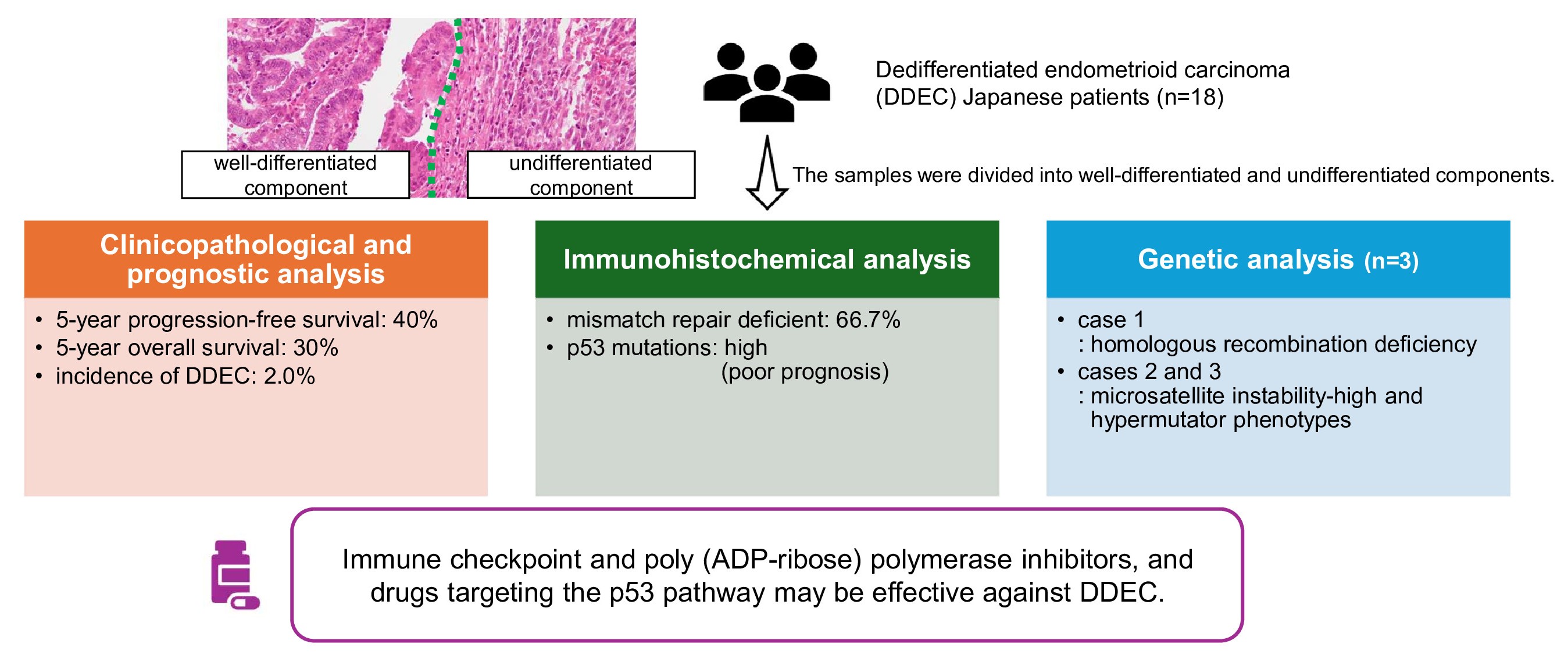
Dedifferentiated endometrioid carcinoma (DDEC) is rare, has a poor prognosis, and the genes responsible for dedifferentiation remain unclear. This study aimed to clarify the characteristics of DDEC in Japanese patients and develop treatment strategies. Eighteen DDEC cases were included; their clinicopathological features and prognoses were analyzed and compared to those of other histological subtypes. The samples were divided into well-differentiated and undifferentiated components; immunostaining and whole-exome sequencing (n = 3 cases) were conducted. The incidence of DDEC was 2.0% among endometrial cancers. The 5-year progression-free survival and the 5-year overall survival for DDEC was approximately 40% and 30%, respectively. Immunohistochemistry showed that 66.7% of patients were mismatch repair deficient. The rate of p53 mutations was higher than that reported in previous studies, and patients with p53 mutations in the undifferentiated components had a poor prognosis. Whole-exome sequencing revealed different gene mutations and mutation signatures between well-differentiated and undifferentiated components. New genetic mutations in undifferentiated regions were uncommon in all three cases. One case (case 1) exhibited homologous recombination deficiency, whereas other two showed microsatellite instability-high and hypermutator phenotypes. Genetic analysis suggests that immune checkpoint and poly (ADP-ribose) polymerase inhibitors, and drugs targeting the p53 pathway may be effective against DDEC.
Keywords:
dedifferentiated endometrioid carcinoma
; endometrial carcinoma
; whole-exome sequencing
; p53
1. Introduction
Dedifferentiated endometrioid carcinoma (DDEC) was first reported in 2006 [1] and was subsequently included in the 2014 World Health Organization (WHO) international classification [2]. Histopathologically, DDEC is characterized by a clear border between low-grade (grades 1 or 2) endometrioid and undifferentiated carcinoma [3]. The incidence of DDEC accounts for approximately 1–9% of all endometrial cancers [4,5]. Well-differentiated component (WC) is located superficially, whereas undifferentiated component (UC) is located deeper, thereby making biopsies prone to diagnostic errors [6]. Furthermore, undifferentiated carcinoma can be misdiagnosed as grade 3 endometrioid carcinoma [7]; therefore, the actual frequency of DDEC may be higher than that previously reported.
The development of new treatment strategies for DDEC is urgently needed owing to its poor prognosis [8,9]. Especially, SWI/SNF-deficient DDEC has a poor prognosis [10], and the loss of E-cadherin and fascin expression is associated with tumor aggressiveness [11]. Recent classifications of endometrial cancer, including The Cancer Genome Atlas (TCGA) and the Proactive Molecular Risk Classifier for Endometrial Cancer (ProMisE) are crucial for guiding postoperative adjuvant therapy and predicting prognosis [12,13,14]. DDEC displays genetic characteristics distinct from typical endometrial cancer, which can vary considerably between cases [15,16]. For example, DDEC rarely expresses hormone receptors even though endometrial cancer is generally hormone-dependent. Deficiencies in mismatch repair (MMR) proteins [17,18] and the SWI/SNF complex [19] are frequently observed in DDEC and associated with prognosis and treatment. Therefore, it may be necessary to evaluate the genomic profile of each patient and use targeted therapies. Exome sequencing of undifferentiated and dedifferentiated carcinomas showed that PTEN mutation was most frequent [15], and another report found somatic mutations in PIK3CA (50%), CTNNB1 (30%), TP53 (30%), FBXW7 (20%) and PPP2R1A (20%) [20].
Although some recent review articles have explored DDEC [21,22], the genetic abnormalities associated with its development and dedifferentiation remain unclear. Furthermore, no studies have specifically focused on Japanese patients. Therefore, this study aimed to characterize DDEC by collecting data from Japanese patients and identifying genetic abnormalities involved in the dedifferentiation process.
2. Results
2.1. Natural Incidence Histology and Clinicopathological Characteristics
The natural incidences of histology between 2011 and 2020 are shown in Table 1. Among the 225 patients, 188 (73.7%) had grade 1 or 2 endometrioid carcinoma, 23 (9.0%) had grade 3 endometrioid carcinoma, and 39 (15.3%) had other carcinomas, including 28 (11.0%) serous carcinoma, six (2.4%) clear cell carcinoma, five (2.0%) mucinous carcinoma, and five (2.0%) DDEC.
The clinicopathological features of DDEC were compared with those of other cancer types (Table 2). No significant differences were observed in age or between DDEC and carcinosarcoma. DDEC exhibited a higher rate of advanced-stage cancers, greater muscle invasion, and a higher rate of lymphovascular space invasion than grade 1/2 endometrioid carcinoma and other carcinomas. Lymphovascular space invasion was not significantly different from grade 3 endometrioid carcinoma. Lymph node metastasis was significantly less frequent in grade 1/2 endometrioid carcinomas than in other cancer types.
2.2. Prognostic Analysis Using the Kaplan–Meier Method
The 5-year PFS and OS rates for DDEC were approximately 40% and 30%, respectively, with a significantly poorer prognosis than grade 1/2 endometrioid carcinoma, grade 3 endometrioid carcinoma, and other carcinomas. No significant differences in prognosis were observed between DDEC and carcinosarcomas (Figure 1A,B).
2.3. Immunohistochemical Findings
Immunohistochemistry was performed on 18 DDEC samples divided into WC and UC. The positive and negative examples for each staining are shown in Figure 2, and the overall staining results are summarized in Figure 3. Epithelial markers such as PAX8, cytokeratin, and epithelial membrane antigen were positive in all WC but significantly negative in UC (p = 0.020, 0.041, 0.041). The proportion of p53 mutations was higher in UC (87.5%) than in WC (68.6%) (p = 0.083). E-cadherin expression was positive in all WC but absent in UC (p = 0.000). Fascin expression was significantly higher in UC than in WC (p = 0.041). The proportion of ARID1A-negative patients was 37.5%. MMR deficiency was observed in 66.7% of cases. Prognostic analysis was conducted separately based on the UC for p53, E-cadherin, fascin, and ARID1A (Figure S1A–H). For example, two cases of wild-type p53 and 14 cases of p53 mutant in UC were compared. The same comparison was made for E-cadherin, fascin, and ARID1A, according to the UC results. The p53 mutant group considerably had a poor prognosis (p = 0.153, 0.178). The prognosis was significantly worse in the E-cadherin-positive group than in the E-cadherin-negative group (p = 0.004, 0.030). There was no significant difference in prognosis depending on the expression of fascin and ARID1A.
2.4. Whole-Exome Sequencing
Whole-exome sequencing was performed on well-preserved DDEC tissues from three patients. The three case types are listed in Table 3. The variant positions and allele frequencies are summarized in Table S1. In all three cases, the WC and UC displayed distinct gene mutations. New mutations in the UC were uncommon across the three cases. In case 1, PIK3CA amplification, loss of heterozygosity of MLH1 and PTEN, and uniparental disomy of p53 were observed. Cases 2 and 3 exhibited microsatellite instability (MSI)-high, and high frequencies of nonsynonymous single nucleotide variants, suggesting hypermutator phenotypes. The mutation signatures differed between the WC and UC (Figure 4A,B, Figure S2A–D). The copy number plot of case 1 indicates homologous recombination deficiency (HRD). The copy number plots for cases 2 and 3 were normal (Figure 5A,B, Figure S3A–D).
3. Discussion
To the best of our knowledge, this is the first work to collect data on DDEC in Japan. In this study, DDEC accounted for 2.0% of all uterine cancers, aligning with the findings of previous reports [4,5]. The clinicopathological characteristics of DDEC include a high rate of advanced-stage cancer, muscle layer invasion of more than half of the myometrium, and vascular invasion, all of which are risk factors for recurrence and contribute to a poor prognosis.
Undifferentiated and dedifferentiated endometrioid carcinomas (UDEC) have a 5-year PFS rate of 80% for stage I/II, 29% for stage III, and 10% for stage IV, and a 5-year OS rate of 84% for stage I/II, 38% for stage III, and 12% for stage IV [9]. DDEC also has a worse prognosis than grade 3 endometrioid carcinomas, with a reported 2-year OS of 31.3% for DDEC compared to 82.8% for grade 3 endometrioid carcinoma [23]. In a study involving 443 patients with UDEC, the median OS was 14 months, with a 5-year OS rate of 44% [24]. However, no specific PFS or OS data for DDEC have been published or compared with other cancer types. In this study, DDEC exhibited the poorest prognosis compared with grade 1/2 endometrioid carcinoma, grade 3 endometrioid carcinoma, other carcinomas, and carcinosarcoma. The 5-year PFS for DDEC was approximately 40%, and the 5-year OS was approximately 30%, both of which were significantly worse than those of other cancer types.
Immunohistochemical analysis revealed distinct protein expression patterns between WC and UC of DDEC. The loss of epithelial markers in the UC is a hallmark of DDEC [25]. Furthermore, a high proportion (66.7%) of cases were MMR-deficient. The rate of p53 mutations in DDEC was higher than previously reported [26,27], suggesting that DDEC may resemble Type 2 endometrioid carcinoma [28] or p53-abnormal endometrioid carcinoma according to TCGA molecular classification [12]. This finding may explain the poor prognosis observed in the present study. Prognostic analyses of p53, E-cadherin, fascin, and ARID1A revealed no significant differences between fascin and ARID1A expression, and the E-cadherin results were unexpected. This finding could be attributed to the limited number of DDEC cases in this study. However, cases with p53 mutations in the UC had a poorer prognosis than those who did not. These findings suggest that MMR proteins and p53 may play a role in the dedifferentiation.
Whole-exome sequencing revealed that WC and UC of DDEC exhibit different genetic mutations. Mutation signatures were also distinct between these components. This genetic heterogeneity is reminiscent of dedifferentiated liposarcoma [29], which also presents with mixed genetic profiles, contributing to a poor prognosis. In this study, new genetic mutations in the UC were uncommon across the three cases, making it challenging to identify a single gene responsible for dedifferentiation. Case 1 showed HRD, whereas cases 2 and 3 displayed MSI-high and hypermutator phenotypes, both of which are associated with an increased response to immune checkpoint inhibitors. Furthermore, approximately half of the UC were MMR-deficient and expressed programmed death-ligand 1 (PD-L1), suggesting that DDEC could be a target for immune checkpoint inhibitors [30]. In case 2, mutations in MSH6, ARID1A, and ARID1B were observed in the UC, whereas case 3 exhibited mutations in p53 and POLE. Common mutations in the UC of cases 2 and 3 suggest that MSH6 and ARID1A may be involved in the dedifferentiation mechanism.
Fumarate hydratase (FH) is an enzyme involved in the tricarboxylic acid cycle and is a tumor suppressor gene [31]. FH mutations cause hereditary leiomyomatosis and renal cell carcinoma (HLRCC) [32]. In this study, case 2 exhibited a germline mutation in FH, which was also observed in the somatic mutation in case 3. However, FH mutations in both WC and UC suggest that FH does not play a role in the dedifferentiation process. Furthermore, p53 may be a driver of dedifferentiation [33]. The immunostaining results, particularly the presence of p53 mutations, supported the hypothesis that TP53 dysfunction is involved in dedifferentiation.
Currently, platinum/taxane-based chemotherapy is recommended for DDEC [34]. TCGA molecular classification of UDEC reveals that MMR deficiency occurs in 44.0%, POLE mutations in 12.4%, and p53 abnormalities in 18.6% [35]. The high prevalence of MSI and POLE groups suggests potential responsiveness to immunotherapy. A patient with recurrent DDEC was treated with pembrolizumab and gemcitabine and achieved 15 months of PFS [23]. Another patient with advanced-stage MMR-deficient DDEC was treated with three cycles of maintenance pembrolizumab and experienced over 5 years of PFS [36]. The results of the genetic analysis showed that HRD-related genes had numerous mutations. Poly (ADP-ribose) polymerase (PARP) inhibitors effectively treat HRD [37]. The DUO-E and DUO-O trials are currently underway, and the use of durvalumab and olaparib in maintenance therapy is expected to be effective [38,39]. For DDEC, the DUO-E trial regimen is considered the most appropriate because platinum/taxane-based chemotherapy effectively targets well-differentiated areas, immune checkpoint inhibitors are effective against MSI-high and hypermutator phenotypes, and PARP inhibitors are effective for HRD. APR-246 (Eprenetapopt) targets the p53 pathway [40]. In addition, the combination of adavosertib—a potent antitumor kinase inhibitor—and carboplatin has been used for advanced p53 mutated ovarian cancer in a phase II trial [41]. Targeted drugs for the ARID1A mutation exist, which is common in cases 2 and 3. Aurora A is a therapeutic target in ARID1A-deficient colorectal cancer cells [42]. Alisertib, an aurora A kinase inhibitor, has been investigated for the treatment of several cancers [43].
This study had some limitations. The study design was retrospective, and the number of cases of DDEC was small. In addition, the results of natural incidence histology were based on a single facility, which should be investigated at multiple centers.
4. Materials and Methods
4.1. Study Samples
A retrospective search of the pathology databases of the Seirei Hamamatsu General Hospital, Shimane University, and Shimane Prefectural Central Hospital was conducted between 2000 and 2020. Data from Shimane University from 2011 to 2020 were used to determine the natural incidence of histology. Tumors were histologically classified according to WHO criteria. A total of 273 cases of grade 1–2 endometrioid carcinoma, 41 grade 3 endometrioid carcinoma, 18 DDEC, 34 carcinosarcoma, and 49 other carcinomas (30 serous, 10 clear cell, eight mucinous, and one squamous cell carcinoma) were identified. Five cases of carcinosarcoma and 11 of DDEC were collected from Seirei Hamamatsu General Hospital. Ten cases of carcinosarcoma and two of DDEC were collected from Shimane Prefectural Central Hospital. All the patients were initially treated surgically (modified radical hysterectomy + bilateral salpingo-oophorectomy ± pelvic lymphadenectomy ± para-aortic lymphadenectomy) and adjuvant platinum-based chemotherapy (carboplatin; [AUC5], paclitaxel; 175 mg/m2, or docetaxel; 70 mg/m2). Systematic retroperitoneal lymphadenectomy was conducted in approximately 90% of patients. Postoperative adjuvant chemotherapy was undergone to patients with risk factors for recurrence (e.g., cervical invasion, deep myometrial invasion, lymphovascular space invasion, lymph node metastasis, and positive peritoneal cytology). A total of 415 patients were included in the survival analysis. The follow-up period ranged from 1 to 250 months (median, 60 months).
According to the International Federation of Gynecology and Obstetrics staging criteria (FIGO 2008), the number of DDEC cases in stages I, II, III, and IV were five (27.8%), 0 (0%), nine (50%), and four (22.2%), respectively. Patients’ information was retrospectively acquired from electronic medical records. Samples were collected after obtaining written informed consent from all patients, and the study was approved by the Shimane University Institutional Review Board (IRB No. 20070305-1 and No. 20070305-2, last update, December 8, 2019).
4.2. Immunohistochemistry
Immunohistochemistry was performed on 18 DDEC samples, and the expression of PAX8, cytokeratin, epithelial membrane antigen, p53, E-cadherin, fascin, ARID1A, and MMR proteins (MLH1, PMS2, MSH2, and MSH6) was evaluated. These markers were selected based on previous studies indicating their prognostic relevance in DDEC [10,11]. Detailed antibody information is provided in Table 4. Staining procedures followed the manufacturer's instructions [44,45,46], and evaluations were conducted by two researchers (H.H. and M.N.) using a double-blind method.
4.3. DNA Extraction
Next-generation sequencing was performed on three DDEC samples [47,48]. For total DNA isolation, DNA was extracted from formalin-fixed, paraffin-embedded tissues as previously mentioned [48]. WC and UC were separately collected using macroscopic hematoxylin and eosin staining, and normal tissue was used as a control.
4.4. Statistical Analyses
Statistical analyses were conducted using SPSS software (version 19.0; IBM Corporation, Armonk, NY, USA). Kaplan–Meier curves and log-rank tests were used to compare the progression-free survival (PFS) and overall survival (OS). PFS was calculated from the first day of treatment to the date of recurrence or last follow-up, whereas OS was defined from the first day of treatment to the date of death or last follow-up. Chi-square tests were used to compare clinicopathological characteristics across different histological types. Paired sample t-tests were used to compare the immunostaining results of the WC and UC. Statistical significance was set at p < 0.05.
5. Conclusions
This study presents the first accumulation of data on DDEC in the Japanese population and provides valuable insights into its characteristics. Genetic analysis revealed that approximately one-third of the cases exhibited HRD, whereas two-thirds showed MSI-high and hypermutator phenotypes, suggesting that immune checkpoint and PARP inhibitors may be effective treatments for DDEC. Additionally, the high prevalence of p53 mutations detected by immunohistochemistry supports the use of drugs that target the p53 pathway. However, larger surveys are needed in the future to verify our hypothesis. Future studies will create organoid and xenograft [49] of DDEC to use as models for chemosensitivity tests and genotype-matched therapy.
Supplementary Materials
Table S1: Actionable variants in dedifferentiated endometrioid carcinoma. Figure S1: Kaplan-Meier analysis of progression-free survival and overall survival. Figure S2: Mutation signatures. Figure S3: Copy number alteration plot.
Author Contributions
H.H.; Writing, S.R., M.I., H.Y., K.K., T.I., H.K., S.N., and K.S.; Investigation, M.N., R.S., and Y.O.; Formal analysis, K.N. and S.K.; Supervision.
Funding
This research was funded by JSPS KAKENHI (grant numbers 21K09472).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the collection of tumor tissues has been approved by the Shimane University Institutional Review Board (IRB No. 20070305-1 and No. 20070305-2, approval date: Mar 5, 2007, last update, Dec 8, 2019).
Informed Consent Statement
Written consent was obtained from all patients for the procedure and participation in the study after an adequate explanation was provided.
Data Availability Statement
The data that support the findings of this study are available from the corresponding authors (K.N.) (S.K.) upon reasonable request.
Acknowledgments
We would like to thank Editage (www.editage.jp) for English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Silva, E.G.; Deavers, M.T.; Bodurka, D.C.; Malpica, A. Association of low-grade endometrioid carcinoma of the uterus and ovary with undifferentiated carcinoma: a new type of dedifferentiated carcinoma? Int J Gynecol Pathol. 2006, 25, 52–58. [Google Scholar] [CrossRef]
- Zaino, R.; Carinelli, S.G.; Eng, C.; Kurman, R.J.; Carcangiu, M.L.; Herrington, C.S.; Young, R.H. WHO Classification of tumours of Female Reproductive Organs: World Health Organization Classification of Tumours. 4th ed. IARC Press; Lyon, France; 2014.
- Cree, I.A.; White, V.A.; Indave, B.I.; Lokuhetty, D. Revising the WHO classification: female genital tract tumours. Histopathology. 2020, 76, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.G.; Deavers, M.T.; Malpica, A. Undifferentiated carcinoma of the endometrium: a review. Pathology. 2007, 39, 134–138. [Google Scholar] [CrossRef]
- AlHilli, M.; Elson, P.; Rybicki, L.; Amarnath, S.; Yang, B.; Michener, C.M.; Rose, P.G. Undifferentiated endometrial carcinoma: a National Cancer Database analysis of prognostic factors and treatment outcomes. Int J Gynecol Cancer. 2019, 29, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Tafe, L.J.; Garg, K.; Chew, I.; Tornos, C.; Soslow, R.A. Endometrial and ovarian carcinomas with undifferentiated components: clinically aggressive and frequently underrecognized neoplasms. Mod Pathol. 2010, 23, 781–789. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, C. Clinicopathologic and Immunohistochemical characterization of dedifferentiated endometrioid adenocarcinoma. Appl Immunohistochem Mol Morphol. 2016, 24, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Altrabulsi, B.; Malpica, A.; Deavers, M.T.; Bodurka, D.C.; Broaddus, R.; Silva, E.G. Undifferentiated carcinoma of the endometrium. Am J Surg Pathol. 2005, 29, 1316–1321. [Google Scholar] [CrossRef]
- Hamilton, S.N.; Tinker, A.V.; Kwon, J.; Lim, P.; Kong, I.; Sihra, S.; Koebel, M.; Lee, C.H. Treatment and outcomes in undifferentiated and dedifferentiated endometrial carcinoma. J Gynecol Oncol. 2022, 33, e25. [Google Scholar] [CrossRef]
- Tessier-Cloutier, B.; Coatham, M.; Carey, M.; Nelson, G.S.; Hamilton, S.; Lum, A.; Soslow, R.A.; Stewart, C.J.; Postovit, L.M.; Köbel, M.; Lee, C.H. SWI/SNF-deficiency defines highly aggressive undifferentiated endometrial carcinoma. J Pathol Clin Res. 2021, 7, 144–153. [Google Scholar] [CrossRef]
- Onder, S.; Taskin, O.C.; Sen, F.; Topuz, S.; Kucucuk, S.; Sozen, H.; Ilhan, R.; Tuzlali, S.; Yavuz, E. High expression of SALL4 and fascin, and loss of E-cadherin expression in undifferentiated/dedifferentiated carcinomas of the endometrium: An immunohistochemical and clinicopathologic study. Medicine (Baltimore). 2017, 96, e6248. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth C, Schultz N, Cherniack AD, Akbani R, Liu Y, Shen H, Robertson AG, Pashtan I, Shen R, Benz CC, Yau C, Laird PW, Ding L, Zhang W, Mills GB, Kucherlapati R, Mardis ER, Levine DA. Integrated genomic characterization of endometrial carcinoma. Integrated genomic characterization of endometrial carcinoma. Nature. 497, 67–73. [CrossRef]
- Abu-Rustum, N.; Yashar, C.; Arend, R.; Barber, E.; Bradley, K.; Brooks, R.; Campos, S.M.; Chino, J.; Chon, H.S.; Chu, C.; Crispens, M.A.; Damast, S.; Fisher, C.M.; Frederick, P.; Gaffney, D.K.; Giuntoli, R.; Han, E.; Holmes, J.; Howitt, B.E.; Lea, J.; Mariani, A.; Mutch, D.; Nagel, C.; Nekhlyudov, L.; Podoll, M.; Salani, R.; Schorge, J.; Siedel, J.; Sisodia, R.; Soliman, P.; Ueda, S.; Urban, R.; Wethington, S.L.; Wyse, E.; Zanotti, K.; McMillian, N.R.; Aggarwal, S. Uterine Neoplasms, Version 1.2023, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2023, 21, 181–209. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; Fotopoulou, C.; Gonzalez Martin, A.; Lax, S.; Lorusso, D.; Marth, C.; Morice, P.; Nout, R.A.; O'Donnell, D.; Querleu, D.; Raspollini, M.R.; Sehouli, J.; Sturdza, A.; Taylor, A.; Westermann, A.; Wimberger, P.; Colombo, N. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int J Gynecol Cancer. 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Rosa-Rosa, J.M.; Leskelä, S.; Cristóbal-Lana, E.; Santón, A.; López-García, M.Á.; Muñoz, G.; Pérez-Mies, B.; Biscuola, M.; Prat, J.; Esther, O.; Soslow, R.A.; Matias-Guiu, X.; Palacios, J. Molecular genetic heterogeneity in undifferentiated endometrial carcinomas. Mod Pathol. 2016, 29, 1390–1398. [Google Scholar] [CrossRef] [PubMed]
- Taira, Y.; Shimoji, Y.; Arakaki, Y.; Nakamoto, T.; Kudaka, W.; Aoki, Y. Comprehensive genomic profiling for therapeutic decision and identification of gene mutation in uterine endometrial dedifferentiated carcinoma. Case Rep Oncol. 2022, 15, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Hacking, S.; Jin, C.; Komforti, M.; Liang, S.; Nasim, M. MMR deficient undifferentiated/dedifferentiated endometrial carcinomas showing significant programmed death ligand-1 expression (sp 142) with potential therapeutic implications. Pathol Res Pract. 2019, 215, 152552. [Google Scholar] [CrossRef]
- Kaur, R.; Mehta, J.; Borges, A.M. Role of SMARCA4 (BRG1) and SMARCB1 (INI1) in dedifferentiated endometrial carcinoma with paradoxical aberrant expression of MMR in the well-differentiated component: A case report and review of the literature. Int J Surg Pathol. 2021, 29, 571–577. [Google Scholar] [CrossRef]
- Strehl, J.D.; Wachter, D.L.; Fiedler, J.; Heimerl, E.; Beckmann, M.W.; Hartmann, A.; Agaimy, A. Pattern of SMARCB1 (INI1) and SMARCA4 (BRG1) in poorly differentiated endometrioid adenocarcinoma of the uterus: analysis of a series with emphasis on a novel SMARCA4-deficient dedifferentiated rhabdoid variant. Ann Diagn Pathol. 2015, 19, 198–202. [Google Scholar] [CrossRef]
- Kuhn, E.; Ayhan, A.; Bahadirli-Talbott, A.; Zhao, C.; Shih, I.e.M. Molecular characterization of undifferentiated carcinoma associated with endometrioid carcinoma. Am J Surg Pathol. 2014, 38, 660–665. [Google Scholar] [CrossRef]
- Tung, H.J.; Wu, R.C.; Lin, C.Y.; Lai, C.H. Rare subtype of endometrial cancer: Undifferentiated/dedifferentiated endometrial carcinoma, from genetic aspects to clinical practice. Int J Mol Sci. 2022, 23, 3794. [Google Scholar] [CrossRef]
- Giordano, G.; Ferioli, E.; Guareschi, D.; Tafuni, A. Dedifferentiated endometrial carcinoma: A rare aggressive neoplasm-clinical, morphological and immunohistochemical features. Cancers (Basel) 2023, 15, 5155. [Google Scholar] [CrossRef] [PubMed]
- Goh, C.; Farah, B.L.; Ho, W.Y.; Wong, S.L.; Goh, C.H.R.; Chew, S.H.; Nadarajah, R.; Lim, Y.K.; Ho, T.H. Dedifferentiated endometrioid adenocarcinoma of the uterus: A case series and review of literature. Gynecol Oncol Rep. 2020, 32, 100538. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.; Wu, H.; Cao, J.; Li, Y.; Cheng, W.; Luo, C. Analysis of prognostic factors and cancer-specific survival in patients with undifferentiated and dedifferentiated endometrial carcinoma undergoing various postoperative adjuvant therapies. Cancer Manag Res. 2024, 16, 559–573. [Google Scholar] [CrossRef]
- Murali, R.; Davidson, B.; Fadare, O.; Carlson, J.A.; Crum, C.P.; Gilks, C.B.; Irving, J.A.; Malpica, A.; Matias-Guiu, X.; McCluggage, W.G.; Mittal, K.; Oliva, E.; Parkash, V.; Rutgers, J.K.L.; Staats, P.N.; Stewart, C.J.R.; Tornos, C.; Soslow, R.A. High-grade endometrial carcinomas: Morphologic and immunohistochemical features, diagnostic challenges and recommendations. Int J Gynecol Pathol. 2019, 38, S40–S63. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Liu, Y.; Liu, X.; Du, J.; Wang, Y.; Yang, J.; Li, Y.; Liu, C. Clinicopathological significance of multiple molecular features in undifferentiated and dedifferentiated endometrial carcinomas. Pathology. 2021, 53, 179–186. [Google Scholar] [CrossRef]
- Espinosa, I.; Lee, C.H.; D'Angelo, E.; Palacios, J.; Prat, J. Undifferentiated and dedifferentiated endometrial carcinomas with POLE exonuclease domain mutations have a favorable prognosis. Am J Surg Pathol. 2017, 41, 1121–1128. [Google Scholar] [CrossRef]
- Setiawan, V.W.; Yang, H.P.; Pike, M.C.; McCann, S.E.; Yu, H.; Xiang, Y.B.; Wolk, A.; Wentzensen, N.; Weiss, N.S.; Webb, P.M.; et al. Type I and II endometrial cancers: have they different risk factors? J Clin Oncol. 2013, 31, 2607–2618. [Google Scholar] [CrossRef]
- Hirata, M.; Asano, N.; Katayama, K.; Yoshida, A.; Tsuda, Y.; Sekimizu, M.; Mitani, S.; Kobayashi, E.; Komiyama, M.; Fujimoto, H.; Goto, T.; Iwamoto, Y.; Naka, N.; Iwata, S.; Nishida, Y.; Hiruma, T.; Hiraga, H.; Kawano, H.; Motoi, T.; Oda, Y.; Matsubara, D.; Fujita, M.; Shibata, T.; Nakagawa, H.; Nakayama, R.; Kondo, T.; Imoto, S.; Miyano, S.; Kawai, A.; Yamaguchi, R.; Ichikawa, H.; Matsuda, K. Integrated exome and RNA sequencing of dedifferentiated liposarcoma. Nat Commun. 2019, 10, 5683. [Google Scholar] [CrossRef]
- Ono, R.; Nakayama, K.; Nakamura, K.; Yamashita, H.; Ishibashi, T.; Ishikawa, M.; Minamoto, T.; Razia, S.; Ishikawa, N.; Otsuki, Y.; Nakayama, S.; Onuma, H.; Kurioka, H.; Kyo, S. Dedifferentiated endometrial carcinoma could be a target for immune checkpoint inhibitors (anti PD-1/PD-L1 antibodies). Int J Mol Sci. 2019, 20, 3744. [Google Scholar] [CrossRef]
- Valcarcel-Jimenez, L.; Frezza, C. Fumarate hydratase (FH) and cancer: a paradigm of oncometabolism. Br J Cancer. 2023, 129, 1546–1557. [Google Scholar] [CrossRef]
- Yang, L.; Harper, A.; Imm, K.R.; Grubb RL 3rd Kim, E.H.; Colditz, G.A.; Wolin, K.Y.; Kibel, A.S.; Sutcliffe, S. Hereditary leiomyomatosis and renal cell cancer: a syndrome associated with an aggressive form of inherited renal cancer. J Urol. 2007, 177, 2074–2079. [Google Scholar] [CrossRef]
- Kanno, K.; Nakayama, K.; Razia, S.; Islam, S.H.; Farzana, Z.U.; Sonia, S.B.; Sasamori, H.; Yamashita, H.; Ishibashi, T.; Ishikawa, M.; Imamura, K.; Ishikawa, N.; Kyo, S. Molecular analysis of high-grade serous ovarian carcinoma exhibiting low-grade serous carcinoma and serous borderline tumor. Curr Issues Mol Biol. 2024, 46, 9376–9385. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) for Endometrial Carcinoma V.3.2024.
- Travaglino, A.; Raffone, A.; Mascolo, M.; Guida, M.; Insabato, L.; Zannoni, G.F.; Zullo, F. TCGA molecular subgroups in endometrial undifferentiated/dedifferentiated carcinoma. Pathol Oncol Res. 2020, 26, s12253–s019. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.M.; Rushton, T.; Nsiah, F.; Stone, R.L.; Beavis, A.L.; Gaillard, S.L.; Dobi, A.; Fader, A.N. Long-term disease-free survival with chemotherapy and pembrolizumab in a patient with unmeasurable, advanced stage dedifferentiated endometrial carcinoma. Gynecol Oncol Rep. 2024, 53, 101380. [Google Scholar] [CrossRef]
- O'Malley, D.M.; Krivak, T.C.; Kabil, N.; Munley, J.; Moore, K.N. PARP inhibitors in ovarian cancer: A review. Target Oncol. 2023, 18, 471–503. [Google Scholar] [CrossRef]
- Westin, S.N.; Moore, K.; Chon, H.S.; Lee, J.Y.; Thomes Pepin, J.; Sundborg, M.; Shai, A.; de la Garza, J.; Nishio, S.; Gold, M.A.; et al. Durvalumab plus carboplatin/paclitaxel followed by maintenance durvalumab with or without olaparib as first-line treatment for advanced endometrial cancer: The Phase III DUO-E Trial. J Clin Oncol. 2024, 42, 283–299. [Google Scholar] [CrossRef]
- Harter, P.; Trillsch, F.; Okamoto, A.; Reuss, A.; Kim, J.-W.; Rubio Pérez, M.J.; Vardar, M.A.; Scambia, G.; Trédan, O.; Nyvang, G.; Colombo, N.; Chudecka-Głaz, A.; Grimm, C.; e Lheureux, S.; Van Nieuwenhuysen, E.; Heitz, F.; Wenham, R.M.; Ushijima, K.; Day, E.; Aghajanian, C. Durvalumab with paclitaxel/carboplatin (PC) and bevacizumab (bev), followed by maintenance durvalumab, bev, and olaparib in patients (pts) with newly diagnosed advanced ovarian cancer (AOC) without a tumor BRCA1/2 mutation (non-tBRCAm): results from the randomized, placebo (pbo)-controlled phase III DUO-O trial. J Clin Oncol. 2023, 41, abstr LBA5506. [Google Scholar]
- Sallman, D.A.; DeZern, A.E.; Garcia-Manero, G.; Steensma, D.P.; Roboz, G.J.; Sekeres, M.A.; Cluzeau, T.; Sweet, K.L.; McLemore, A.; McGraw, K.L.; Puskas, J.; Zhang, L.; Yao, J.; Mo, Q.; Nardelli, L.; Al Ali, N.H.; Padron, E.; Korbel, G.; Attar, E.C.; Kantarjian, H.M.; Lancet, J.E.; Fenaux, P.; List, A.F.; Komrokji, R.S. Eprenetapopt (APR-246) and azacitidine in TP53-mutant myelodysplastic syndromes. J Clin Oncol. 2021, 39, 1584–1594. [Google Scholar] [CrossRef] [PubMed]
- Embaby, A.; Kutzera, J.; Geenen, J.J.; Pluim, D.; Hofland, I.; Sanders, J.; Lopez-Yurda, M.; Beijnen, J.H.; Huitema, A.D.R.; Witteveen, P.O.; Steeghs, N.; van Haaften, G.; van Vugt, M.A.T.M.; de Ridder, J.; Opdam, F.L. WEE1 inhibitor adavosertib in combination with carboplatin in advanced TP53 mutated ovarian cancer: A biomarker-enriched phase II study. Gynecol Oncol. 2023, 174, 239–246. [Google Scholar] [CrossRef]
- Wu, C.; Lyu, J.; Yang, E.J.; Liu, Y.; Zhang, B.; Shim, J.S. Targeting AURKA-CDC25C axis to induce synthetic lethality in ARID1A-deficient colorectal cancer cells. Nat Commun. 2018, 9, 3212. [Google Scholar] [CrossRef]
- Liewer, S.; Huddleston, A. Alisertib: a review of pharmacokinetics, efficacy and toxicity in patients with hematologic malignancies and solid tumors. Expert Opin Investig Drugs. 2018, 27, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, K.; Takebayashi, Y.; Nakayama, S.; Hata, K.; Fujiwaki, R.; Fukumoto, M.; Miyazaki, K. Prognostic value of overexpression of p53 in human ovarian carcinoma patients receiving cisplatin. Cancer Lett. 2003, 192, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Katagiri, A.; Nakayama, K.; Rahman, M.T.; Rahman, M.; Katagiri, H.; Nakayama, N.; Ishikawa, M.; Ishibashi, T.; Iida, K.; Kobayashi, H.; Otsuki, Y.; Nakayama, S.; Miyazaki, K. Loss of ARID1A expression is related to shorter progression-free survival and chemoresistance in ovarian clear cell carcinoma. Mod Pathol. 2012, 25, 282–288. [Google Scholar] [CrossRef]
- Yamashita, H.; Nakayama, K.; Ishikawa, M.; Nakamura, K.; Ishibashi, T.; Sanuki, K.; Ono, R.; Sasamori, H.; Minamoto, T.; Iida, K.; Sultana, R.; Ishikawa, N.; Kyo, S. Microsatellite instability is a biomarker for immune checkpoint inhibitors in endometrial cancer. Oncotarget. 2017, 9, 5652–5664. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Aimono, E.; Tanishima, S.; Imai, M.; Nagatsuma, A.K.; Hayashi, H.; Yoshimura, Y.; Nakayama, K.; Kyo, S.; Nishihara, H. Intratumoral genomic heterogeneity may hinder precision medicine strategies in patients with serous ovarian carcinoma. Diagnostics (Basel) 2020, 10, 200. [Google Scholar] [CrossRef]
- Kurose, S.; Nakayama, K.; Razia, S.; Ishikawa, M.; Ishibashi, T.; Yamashita, H.; Sato, S.; Sakiyama, A.; Yoshioka, S.; Kobayashi, M.; Nakayama, S.; Otuski, Y.; Ishikawa, N.; Kyo, S. Whole-exome sequencing of rare site endometriosis-associated cancer. Diseases 2021, 9, 14. [Google Scholar] [CrossRef]
- Lin, C.Y.; Wu, R.C.; Huang, C.Y.; Lai, C.H.; Chao, A.S.; Li, H.P.; Tsai, C.L.; Kuek, E.J.; Hsu, C.L.; Chao, A. A patient-derived xenograft model of dedifferentiated endometrial carcinoma: A proof-of-concept study for the identification of new molecularly informed treatment approaches. Cancers (Basel). 2021, 13, 5962. [Google Scholar] [CrossRef]
Figure 1.
Kaplan–Meier analysis of progression-free survival (A) and overall survival (B). G1/G2, grade 1 and 2 endometrioid carcinoma; G3, grade 3 endometrioid carcinoma; others, other carcinomas; DDEC, dedifferentiated endometrioid carcinoma.
Figure 1.
Kaplan–Meier analysis of progression-free survival (A) and overall survival (B). G1/G2, grade 1 and 2 endometrioid carcinoma; G3, grade 3 endometrioid carcinoma; others, other carcinomas; DDEC, dedifferentiated endometrioid carcinoma.
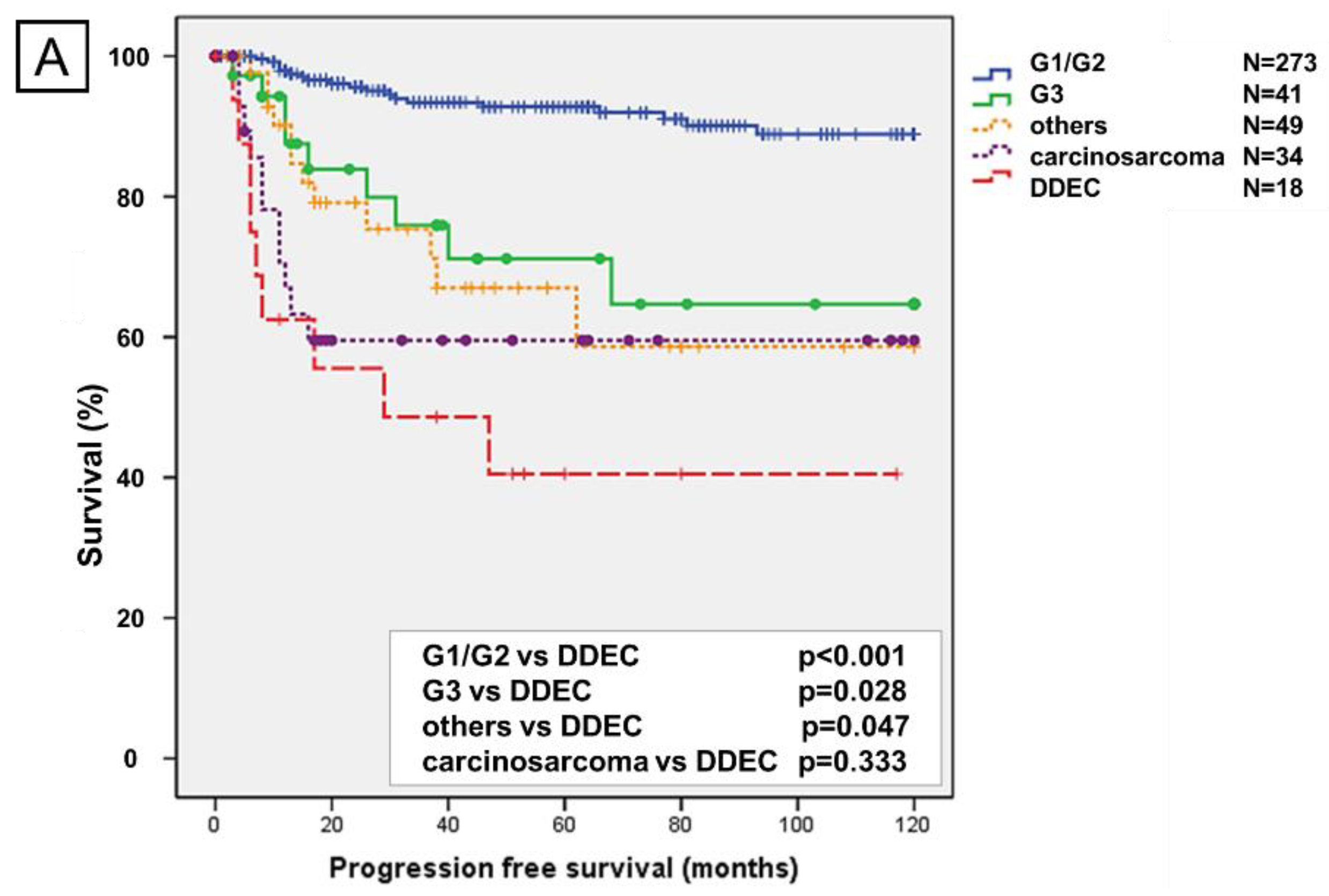
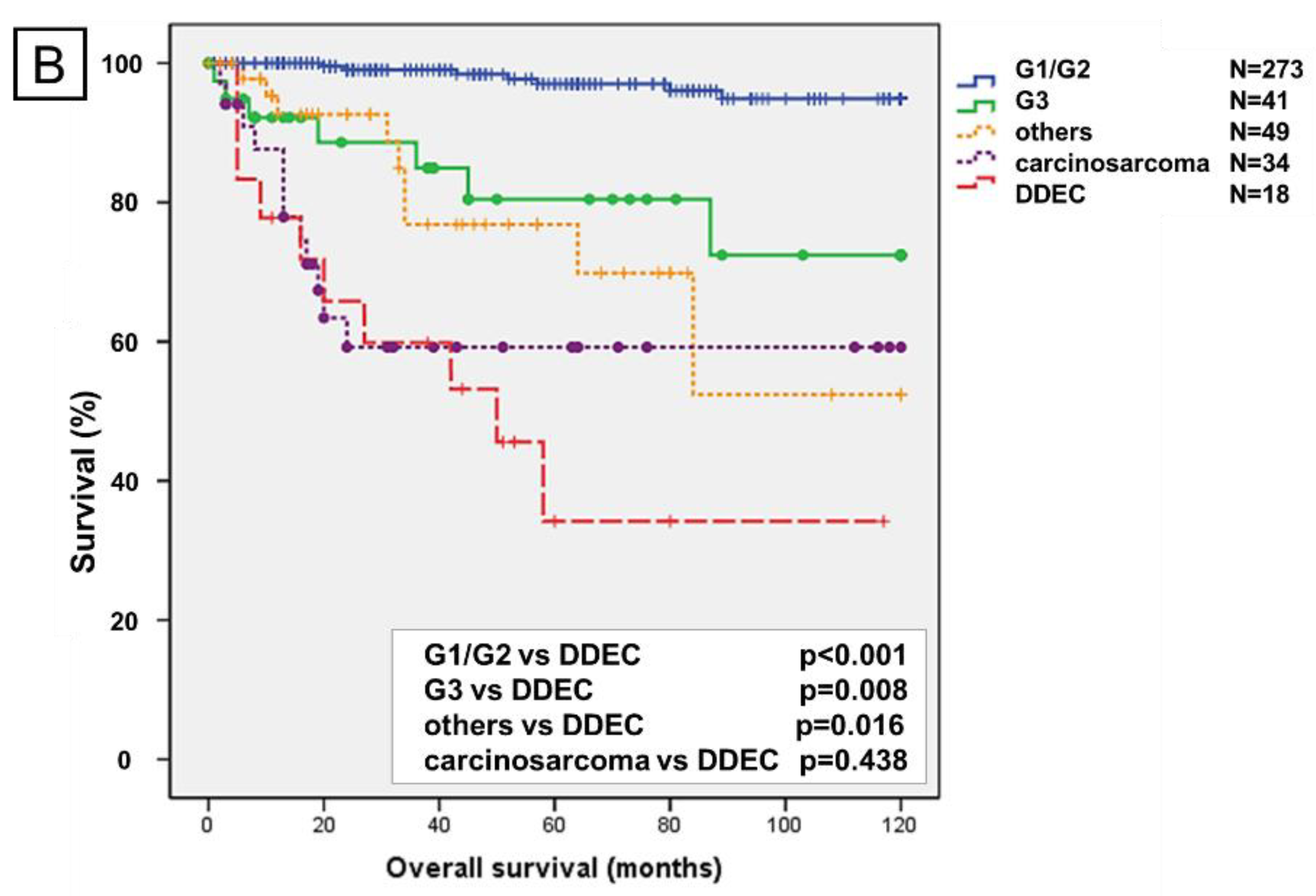
Figure 2.
Immunohistochemical findings. (A) Hematoxylin and eosin staining showing WC and UC from case 9. (B) PAX8: expression in the WC and loss of expression in the UC in case 7. (C) Cytokeratin: expression in the WC and loss of expression in the UC in case 9. (D) Epithelial membrane antigen: expression in the WC and loss of expression in the UC in case 9. (E1) p53: wild-type expression in the WC and UC in case 9. (E2) p53: overexpression in the WC and UC in case 7. (F) E-cadherin: expression in the WC and loss of expression in the UC in case 7. (G) Fascin: loss of expression in the WC and expression in the UC in case 9. (H) ARID1A: expression in the WC and loss of expression in the UC in case 9. WC, well-differentiated component; UC, undifferentiated component.
Figure 2.
Immunohistochemical findings. (A) Hematoxylin and eosin staining showing WC and UC from case 9. (B) PAX8: expression in the WC and loss of expression in the UC in case 7. (C) Cytokeratin: expression in the WC and loss of expression in the UC in case 9. (D) Epithelial membrane antigen: expression in the WC and loss of expression in the UC in case 9. (E1) p53: wild-type expression in the WC and UC in case 9. (E2) p53: overexpression in the WC and UC in case 7. (F) E-cadherin: expression in the WC and loss of expression in the UC in case 7. (G) Fascin: loss of expression in the WC and expression in the UC in case 9. (H) ARID1A: expression in the WC and loss of expression in the UC in case 9. WC, well-differentiated component; UC, undifferentiated component.
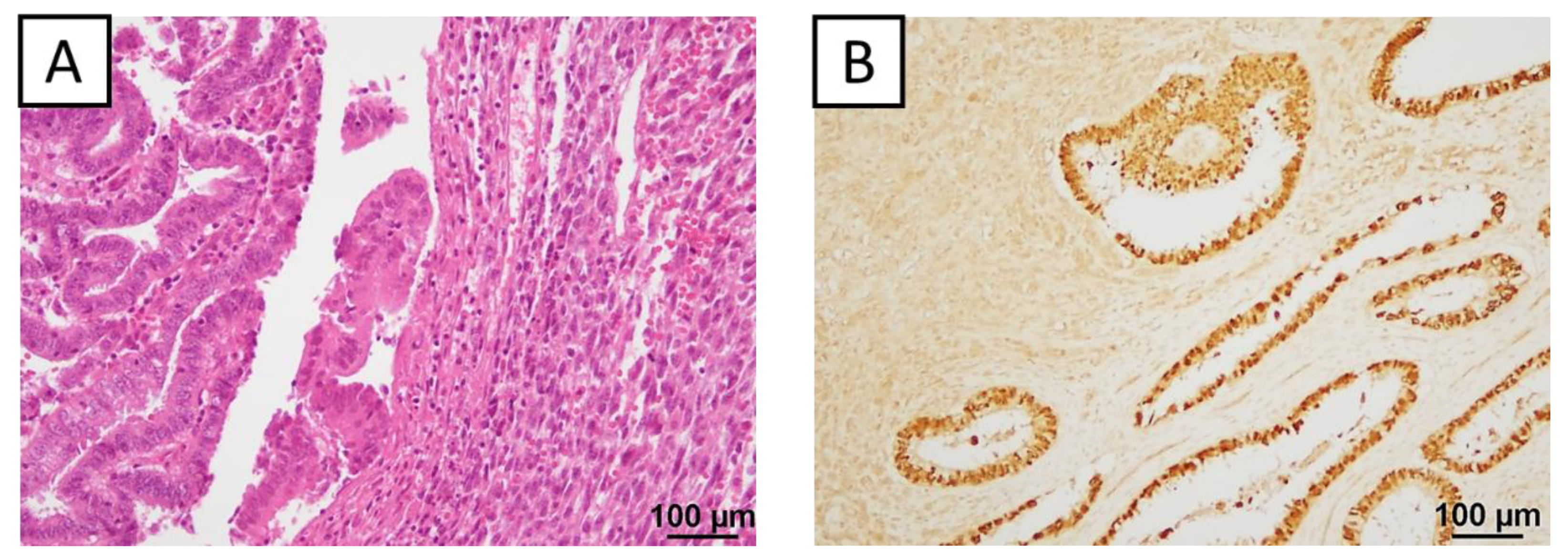
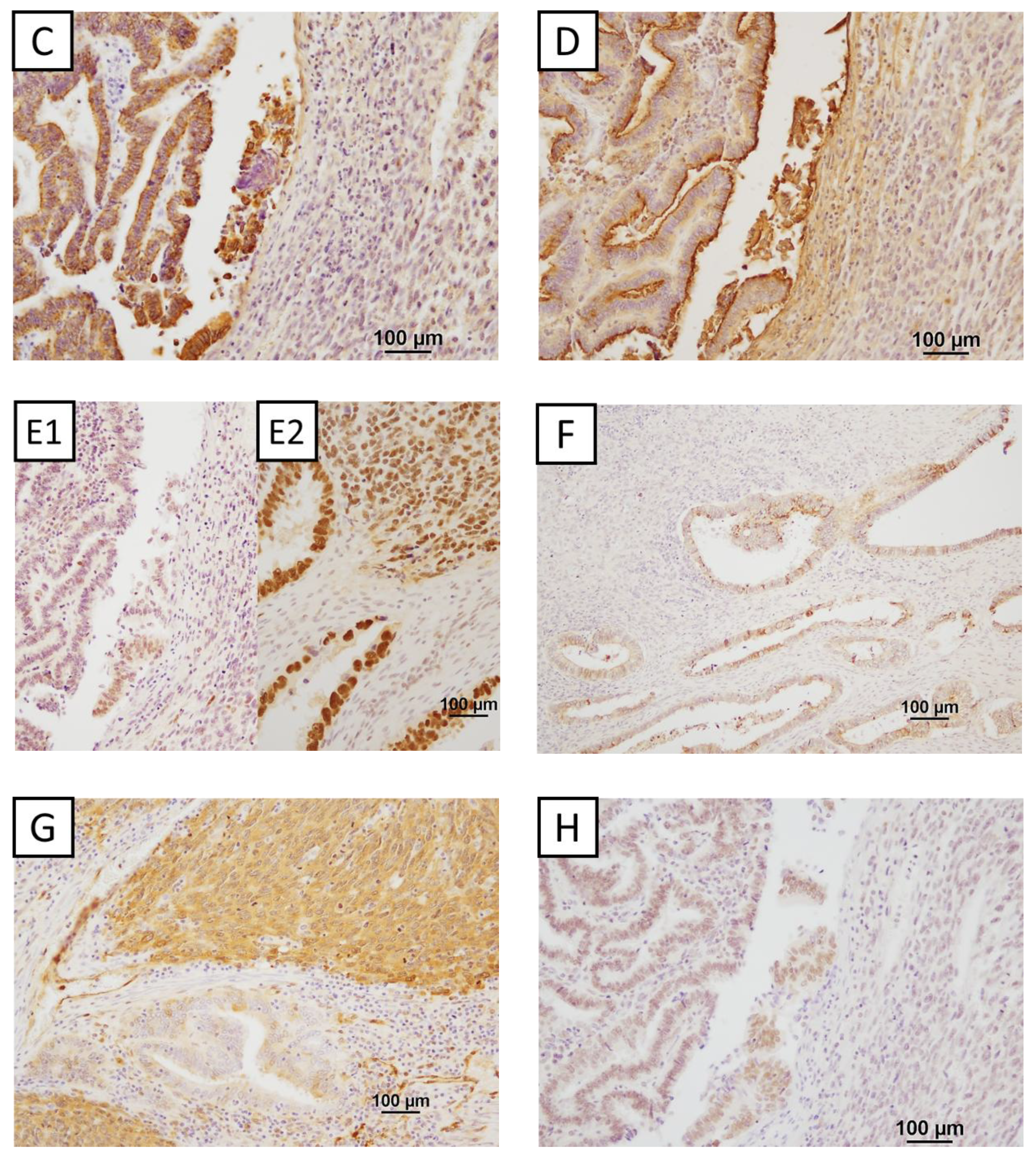
Figure 3.
Summary of immunohistochemical findings. WC, well-differentiated component; UC, undifferentiated component; CK, cytokeratin; EMA, epithelial membrane antigen; N/A, not performed. Positive results are indicated in red, and negative results are indicated in white (for p53, wild-type is blue, mutant is white).
Figure 3.
Summary of immunohistochemical findings. WC, well-differentiated component; UC, undifferentiated component; CK, cytokeratin; EMA, epithelial membrane antigen; N/A, not performed. Positive results are indicated in red, and negative results are indicated in white (for p53, wild-type is blue, mutant is white).
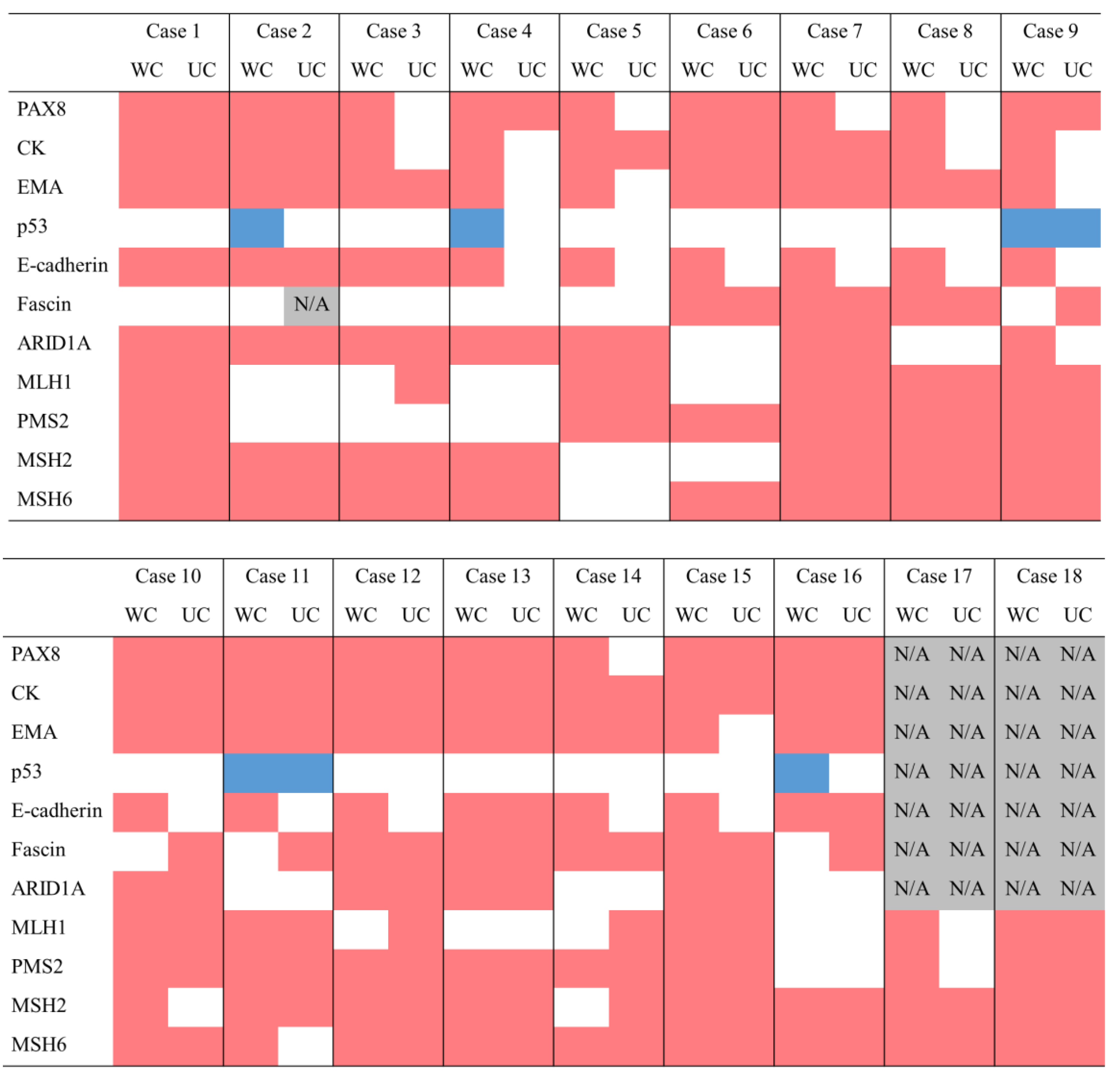
Figure 4.
Mutation signatures. (A) Signature 2 exhibits the highest similarity with the mutation profile of the WC in case 1. (B) Signature 30 exhibits the highest similarity with the mutation profile of the UC in case 1. WC, well-differentiated component; UC, undifferentiated component.
Figure 4.
Mutation signatures. (A) Signature 2 exhibits the highest similarity with the mutation profile of the WC in case 1. (B) Signature 30 exhibits the highest similarity with the mutation profile of the UC in case 1. WC, well-differentiated component; UC, undifferentiated component.
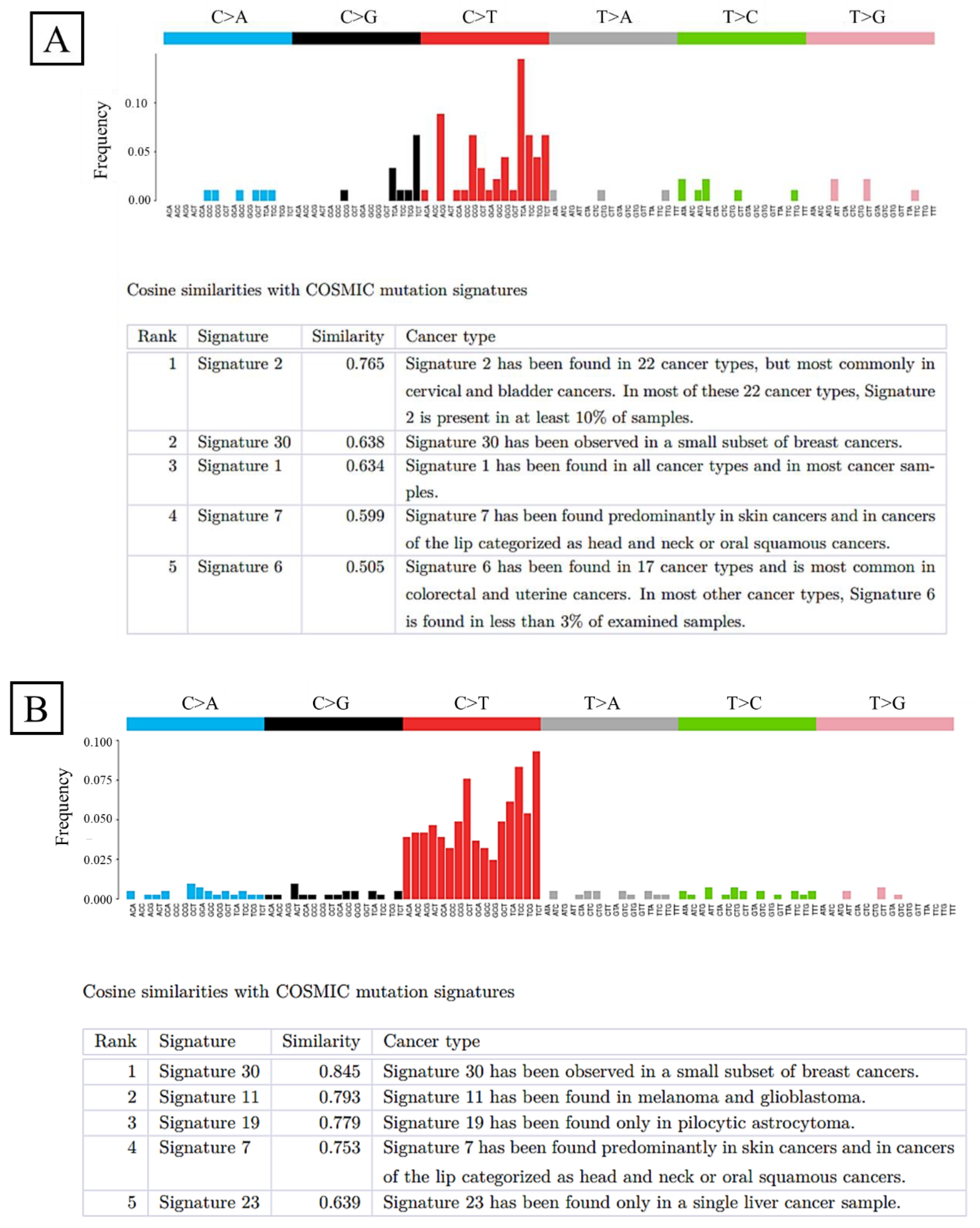
Figure 5.
Copy number alteration plot. The horizontal axis represents the chromosome location, and the vertical axis represents the gene copy number. (A) CNA plot of the WC in case 1.(B) CNA plot of the UC in case 1. CN, copy number; CNA, copy number alteration; VAF, variant allele frequency; WC, well-differentiated component; UC, undifferentiated component.
Figure 5.
Copy number alteration plot. The horizontal axis represents the chromosome location, and the vertical axis represents the gene copy number. (A) CNA plot of the WC in case 1.(B) CNA plot of the UC in case 1. CN, copy number; CNA, copy number alteration; VAF, variant allele frequency; WC, well-differentiated component; UC, undifferentiated component.
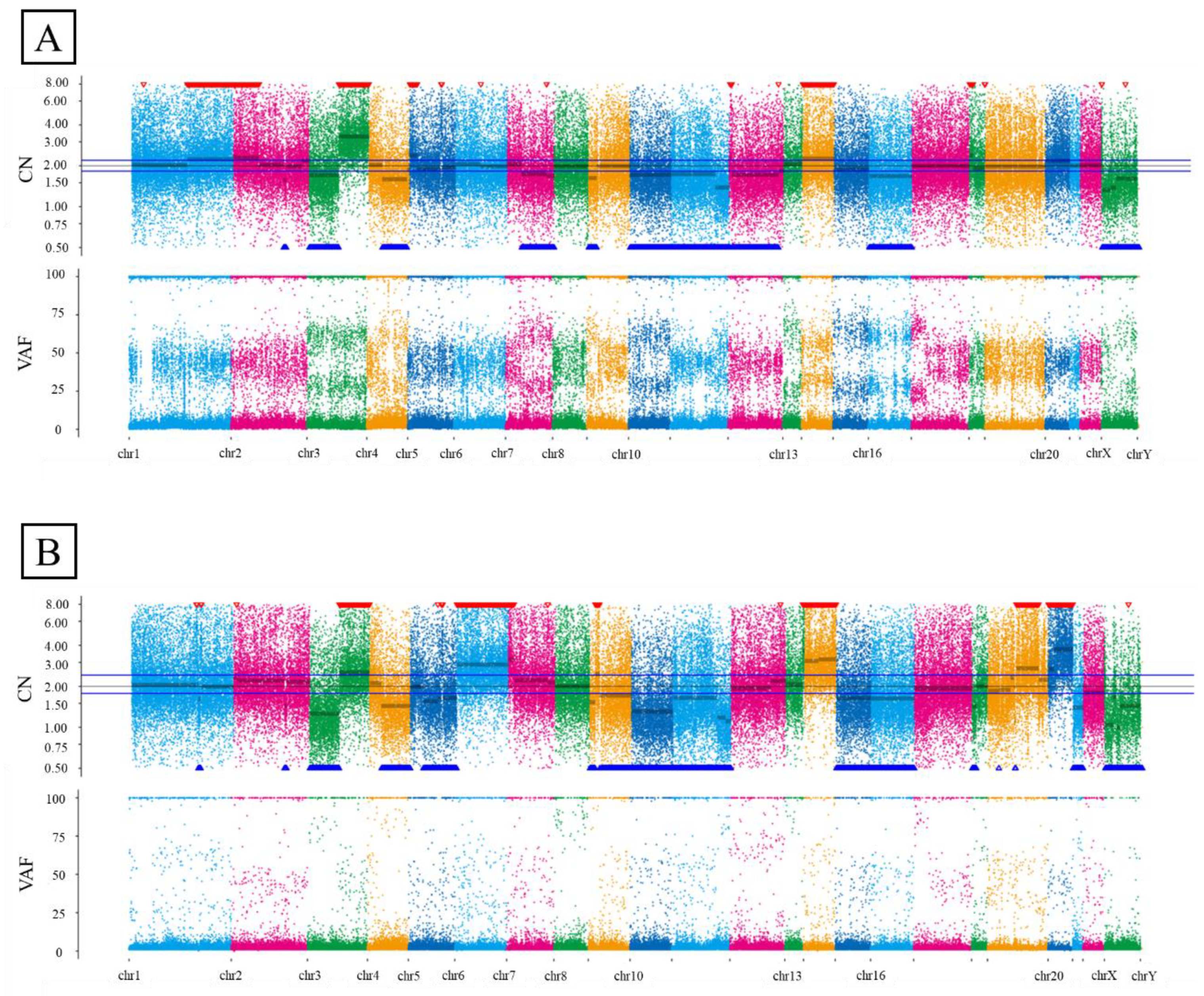

Table 1.
Natural incidence histology of endometrial cancer.
| Histology | Number of Patients (n = 255) | Percentage (%) |
|---|---|---|
| Endometrioid carcinoma G1/G2 | 188 | 73.7 |
| Endometrioid carcinoma G3 | 23 | 9.0 |
| Others | 39 | 15.3 |
| Serous carcinoma | 28 | 11.0 |
| Clear cell carcinoma | 6 | 2.4 |
| Mucinous carcinoma | 5 | 2.0 |
| Dedifferentiated endometrioid carcinoma | 5 | 2.0 |
Table 2.
Clinicopathological characteristics of each histological type.
| Characteristic | G1/G2 | p-value | G3 | p-value | Others | p-value | Carcino sarcoma |
p-value | DDEC | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (%) | 0.554 | 0.931 | 0.102 | 0.053 | |||||||
| <60 | 156 (57) | 20 (49) | 14 (29) | 8 (24) | 9 (50) | ||||||
| ≧60 | 117 (43) | 21 (51) | 35 (71) | 26 (76) | 9 (50) | ||||||
| FIGO Stage (%) | <0.01 | 0.011 | 0.024 | 0.236 | |||||||
| Ⅰ, Ⅱ | 236 (87) | 27 (66) | 30 (61) | 16 (48) | 5 (28) | ||||||
| Ⅲ, Ⅳ | 36 (13) | 14 (34) | 19 (39) | 17 (52) | 13 (72) | ||||||
| Muscle invasion (%) | <0.01 | 0.032 | <0.01 | 0.055 | |||||||
| <50% | 195 (72) | 17 (42.5) | 28 (61) | 6 (46) | 2 (12.5) | ||||||
| ≧50% | 77 (28) | 23 (57.5) | 18 (39) | 7 (54) | 14 (87.5) | ||||||
| LVSI (%) | <0.01 | 0.244 | 0.036 | 0.317 | |||||||
| Yes | 105 (39) | 29 (74) | 27 (59) | 12 (100) | 14 (87.5) | ||||||
| No | 162 (61) | 10 (26) | 19 (41) | 0 (0) | 2 (12.5) | ||||||
| Pelvic/Para aortic lymph metastasis (%) |
<0.01 | 0.297 | 0.213 | 0.170 | |||||||
| Yes | 26 (10) | 12 (29) | 13 (27) | 9 (69) | 7 (44) | ||||||
| No | 247 (90) | 29 (71) | 35 (73) | 4 (31) | 9 (56) | ||||||
G1/G2, endometrioid carcinoma grade 1 and grade 2; G3, endometrioid carcinoma grade 3; Others, other carcinomas; DDEC, dedifferentiated endometrioid carcinoma; LVSI, lymphovascular space invasion.
Table 3.
The three case types of whole-exome sequencing.
| WC | UC | |||
| type | type | |||
| Case1 | LOH high | 21.57% | LOH high | 22.371% |
| Case2 | TMB high | 227 | TMB high | 1927 |
| MSI high | 30.25% | MSI high | 36.38% | |
| Case3 | TMB high | 1099 | TMB high | 15105 |
| MSI high | 28.88% | |||
WC, well-differentiated component; UC, undifferentiated component; LOH, loss of heterozygosity; TMB, tumor mutation burden; MSI, microsatellite instability. The unit of tumor mutation burden is nonsynonymous mutation.
Table 4.
Details of immunohistochemical procedure.
| Antibody | Producer | Dilution |
|---|---|---|
| PAX8 | Proteintech (10336-1-AP) | 1:500 |
| CK | Santa Cruz Biotechnology (sc-8018) | 1:50 |
| EMA | Thermo Fisher Scientific (MA1-06503) | 1:100 |
| p53 | Dako (M7001) | 1:50 |
| E-cadherin | abcam (ab15148) | 1:50 |
| Fascin | Thermo Fisher Scientific (MAF-11483) | 1:200 |
| ARID1A | Santa Cruz Biotechnology (sc-32761) | 1:100 |
| MLH1 | Dako (M3640) | 1:50 |
| PMS2 | Dako (M3647) | 1:40 |
| MSH2 | Dako (M3639) | 1:50 |
| MSH6 | Dako (M3646) | 1:50 |
CK, cytokeratin; EMA, epithelial membrane antigen.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



