Submitted:
05 March 2025
Posted:
06 March 2025
You are already at the latest version
Abstract
Background/Objectives: Advancements in molecular diagnostics and targeted therapies have significantly transformed the management of non-small cell lung cancer (NSCLC). Rare MET rearrangements, including novel fusions such as HLA-DRB1-MET and HLA-DQB2-MET, represent actionable genetic alterations with critical therapeutic implications. This review synthesizes findings from multiple case reports to highlight the efficacy of MET tyrosine kinase inhibitors (TKIs) in MET-driven oncogenesis. Methods: A systematic review of published case reports and studies on MET rearrangements in NSCLC was conducted. Data were analyzed to assess the clinical outcomes of patients treated with MET TKIs, such as crizotinib and tepotinib. Additionally, our case report demonstrates the utility of comprehensive next-generation sequencing (NGS) in identifying rare MET fusions and guiding personalized treatment strategies.Results: Our case illustrates the potential of NGS in detecting rare MET fusions and achieving durable disease control with crizotinib. Comparative analyses indicate the necessity of individualized treatment approaches, particularly in cases involving central nervous system (CNS) involvement and prior treatment history. The review further emphasizes that MET alterations are more frequently identified in never-smoking female patients, where driver mutation detection rates exceed 60%. Conclusions: Precision oncology plays a pivotal role in addressing rare MET rearrangements in NSCLC. Despite advancements, challenges persist in early identification, therapeutic sequencing, and access to advanced diagnostics. Collaborative efforts among researchers, clinicians, and policymakers are crucial to refining treatment strategies and improving patient outcomes.
Keywords:
1. Introduction
2. Clinical Cases and Therapeutic Insights
2.1. Tepotinib in HLA-DRB1-MET Fusion-Positive NSCLC (Blanc-Durand et al.)
2.2. Crizotinib in HLA-DRB1-MET Fusion-Positive NSCLC (Davies et al.)
2.3. Crizotinib in HLA-DRB1-MET Fusion-Positive NSCLC (Kunte and Stevenson)
2.4. Tepotinib in HLA-DQB2-MET Fusion-Positive NSCLC (Dias e Silva et al.)
2.5. Sequential TKI Therapy in ALK-HLA-DRB1 Fusion-Positive NSCLC (Gao et al.)
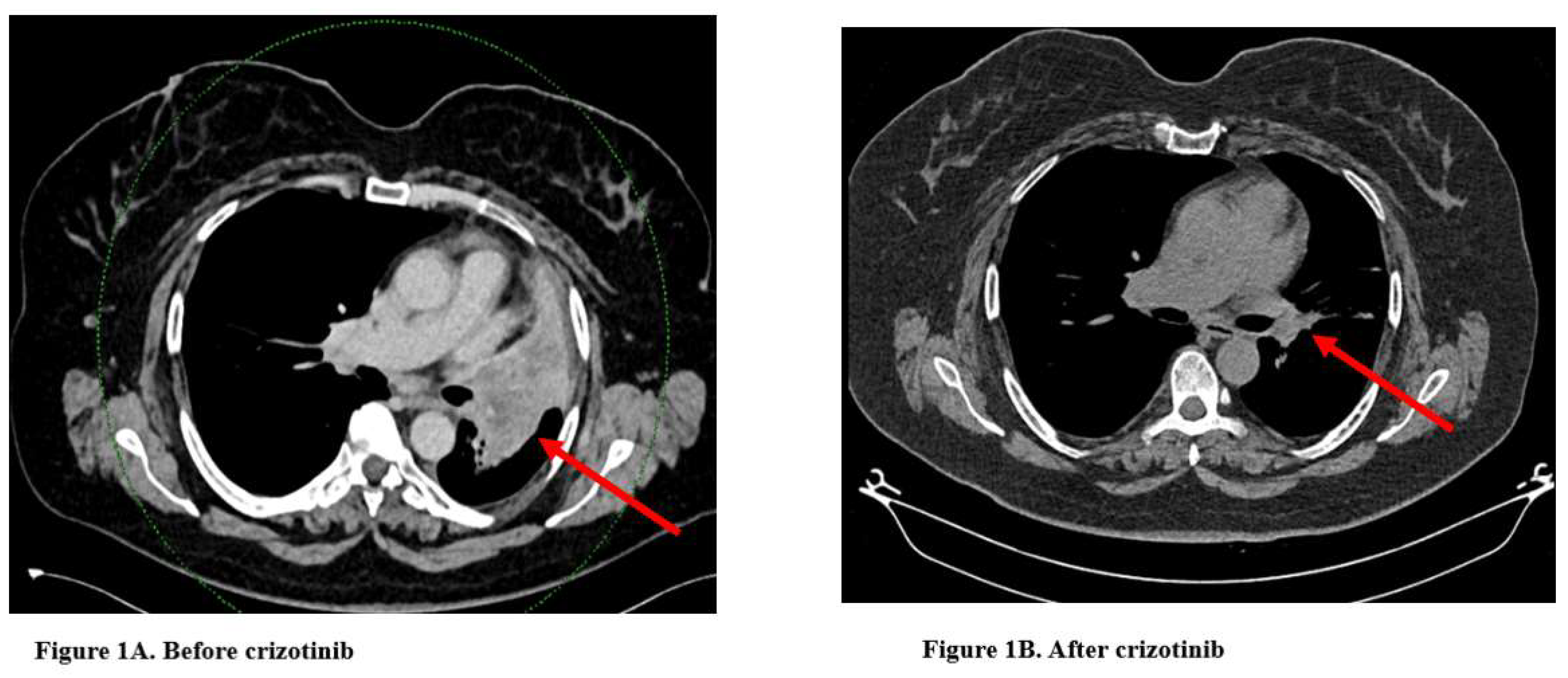
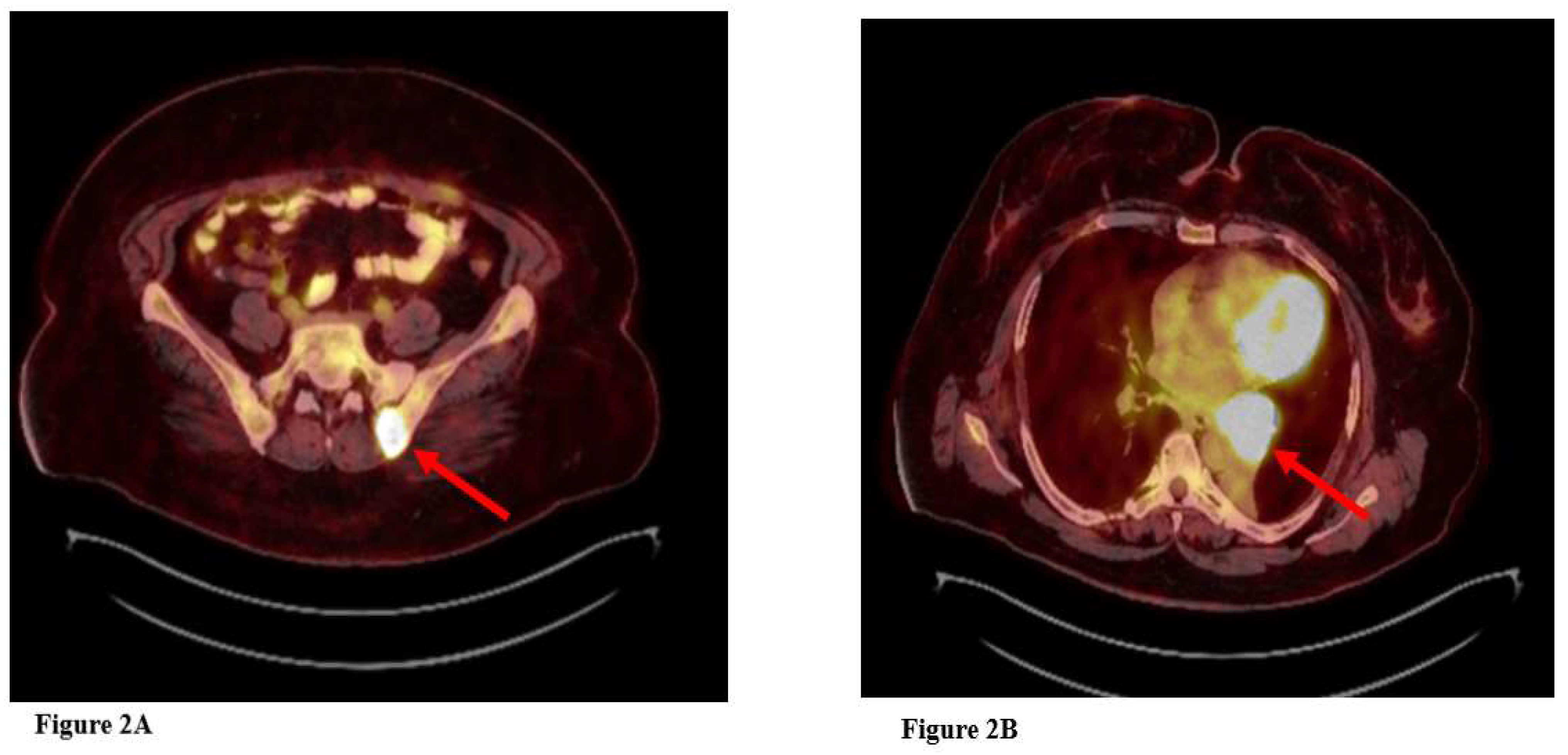
2.6. Crizotinib in HLA-DRB1-MET Fusion-Positive NSCLC: Medipol University Experience (Muğlu et al.)
3. Discussion

| Case | Age Gender |
Smoking Status | Molecular Findings | Treatment | Response | Current Status | PFS / Disease Control Duration |
|---|---|---|---|---|---|---|---|
| Crizotinib in HLA-DRB1-MET Fusion-Positive NSCLC (Davies et al.)[4] | 74 Female |
Never-smoker | HLA-DRB1-MET fusion | Pemetrexed, Carboplatin, Crizotinib (2nd line) |
Complete radiographic response within 6 weeks, maintained for 8 months | Stable with manageable side effects (fatigue, mild hypokalemia) | Crizotinib PFS: 8mo. |
| Tepotinib in HLA-DRB1-MET Fusion-Positive NSCLC (Blanc-Durand et al.)[13] | 41 Female |
Never-smoker | HLA-DRB1-MET fusion | Crizotinib (1st line) Tepotinib (2nd line) Cabozantinib (3rd line) |
Complete intracranial response to tepotinib, sustained control for 9 months | Stable with good tolerance to treatment | Crizotinib PFS: 6mo. Tepotinib PFS: 9mo. Cabozantinib PFS: NR |
| Crizotinib in HLA-DRB1-MET Fusion-Positive NSCLC (Kunte and Stevenson)[14] | 59 Female |
Never-smoker | HLA-DRB1-MET fusion | Curative RT Pembrolizumab Crizotinib (3rd line) |
Complete radiographic response within 4 months | Stable with mild side effects (fatigue, nausea) | Crizotinib PFS: at least 4 months (Ongoing at last follow-up) |
| Tepotinib in HLA-DQB2-MET Fusion-Positive NSCLC (Dias e Silva et al.)[15] | 73 Female |
Never-smoker | HLA-DQB2::MET fusion | Pemetrexed, Carboplatin, Pembrolizumab and maintenance pembrolizumab plus pemterexed Tepotinib |
Sustained disease control for over 12 months | Stable, no treatment-related adverse events | Tepotinib PFS: 12 mo. |
| Sequential TKI Therapy in ALK-HLA-DRB1 Fusion-Positive NSCLC (Gao et al.)[16] | 48 Female |
Never-smoker | ALK-HLA-DRB1 fusion | Crizotinib (1st line), Ceritinib (2nd line) |
24 months progression-free survival (crizotinib plus ceritinib) | Stable after sequential TKI therapy | Crizotinib PFS: 6. Mo Ceritinib PFS: 18mo. |
| Crizotinib in HLA-DRB1-MET Fusion-Positive NSCLC: Medipol University Experience (Muğlu et al.) | 59 Female |
Never-smoker | HLA-DRB1-MET fusion | Pemetrexed, Carboplatin, Pembrolizumab, Crizotinib (2nd line) |
Significant tumor regression and symptomatic relief | Ongoing treatment with sustained good response | Crizotinib PFS: at least 5 months (Ongoing at last follow-up) |
|
TKI: Tirozin kinase inhibitor PFS: Progression-free survival NR: Not reached RT:Radiotherapy NSCLC: Non small cell lung cancer | |||||||
4. Conclusion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bade BC, Cruz CSD. Lung cancer 2020: epidemiology, etiology, and prevention. Clinics in chest medicine. 2020;41(1):1-24.
- Salgia R. MET in lung cancer: biomarker selection based on scientific rationale. Molecular cancer therapeutics. 2017;16(4):555-65. [CrossRef]
- Paik PK, Felip E, Veillon R, Sakai H, Cortot AB, Garassino MC, et al. Tepotinib in non–small-cell lung cancer with MET exon 14 skipping mutations. New England Journal of Medicine. 2020;383(10):931-43.
- Davies KD, Ng TL, Estrada-Bernal A, Le AT, Ennever PR, Camidge DR, et al. Dramatic response to crizotinib in a patient with lung cancer positive for an HLA-DRB1-MET gene fusion. JCO precision oncology. 2017;1. [CrossRef]
- Stransky N, Cerami E, Schalm S, Kim JL, Lengauer C. The landscape of kinase fusions in cancer. Nature communications. 2014;5(1):4846. [CrossRef]
- Recurrent MET fusion genes represent a drug target in pediatric glioblastoma. Nature medicine. 2016;22(11):1314-20.
- Zehir A, Benayed R, Shah RH, Syed A, Middha S, Kim HR, et al. Mutational landscape of metastatic cancer revealed from prospective clinical sequencing of 10,000 patients. Nature medicine. 2017;23(6):703-13.
- Santarpia M, Massafra M, Gebbia V, D’Aquino A, Garipoli C, Altavilla G, et al. A narrative review of MET inhibitors in non-small cell lung cancer with MET exon 14 skipping mutations. Translational lung cancer research. 2021;10(3):1536. [CrossRef]
- Plenker D, Bertrand M, de Langen AJ, Riedel R, Lorenz C, Scheel AH, et al. Structural alterations of MET trigger response to MET kinase inhibition in lung adenocarcinoma patients. Clinical Cancer Research. 2018;24(6):1337-43.
- Yu H, Ahn M-J, Kim S-W, Cho BC, Sequist L, Orlov S, et al. TATTON phase Ib expansion cohort: osimertinib plus savolitinib for patients (pts) with EGFR-mutant, MET-amplified NSCLC after progression on prior first/second-generation epidermal growth factor receptor (EGFR) tyrosine kinase inhibitor (TKI). CANCER RESEARCH. 2019;79(13).
- Wolf J, Seto T, Han J-Y, Reguart N, Garon EB, Groen HJ, et al. Capmatinib (INC280) in METΔex14-mutated advanced non-small cell lung cancer (NSCLC): Efficacy data from the phase II GEOMETRY mono-1 study. American Society of Clinical Oncology; 2019.
- Reungwetwattana T, Liang Y, Zhu V, Ou S-HI. The race to target MET exon 14 skipping alterations in non-small cell lung cancer: the why, the how, the who, the unknown, and the inevitable. Lung cancer. 2017;103:27-37. [CrossRef]
- Blanc-Durand F, Alameddine R, Iafrate AJ, Tran-Thanh D, Lo YC, Blais N, et al. Tepotinib Efficacy in a Patient with Non-Small Cell Lung Cancer with Brain Metastasis Harboring an HLA-DRB1-MET Gene Fusion. The Oncologist. 2020;25(11):916-20. [CrossRef]
- Kunte S, Stevenson J. A case of HLA-DRB1-MET rearranged lung adenocarcinoma with rapid response to crizotinib. Clinical Lung Cancer. 2021;22(3):e298-e300. [CrossRef]
- e Silva DD, Mambetsariev I, Fricke J, Babikian R, Dingal ST, Mazdisnian F, et al. A novel HLA-DQB2:: MET gene fusion variant in lung adenocarcinoma with prolonged response to tepotinib: a case report. Translational Lung Cancer Research. 2024;13(5):1163. [CrossRef]
- Gao P, Tang K, Hao Y, Li W, Lv X, Li D, et al. Case Report: Patient With Lung Adenocarcinoma With ALK-HLA-DRB1 Rearrangement Shows Impressive Progression-Free Survival After Sequential Crizotinib and Ceritinib Treatment. Frontiers in Oncology. 2022;12:762338. [CrossRef]
- Awad MM. Impaired c-Met receptor degradation mediated by MET Exon 14 mutations in non–small-cell lung cancer. Journal of Clinical Oncology. 2016;34(8):879-81. [CrossRef]
- Ettinger D, Wood D. NCCN Guidelines Version 3.2020 Non-Small Cell Lung Cancer. National Comprehensive Cancer Network. 2020:1-244.
- Paik PK, Veillon R, Cortot AB, Felip E, Sakai H, Mazieres J, et al. Phase II study of tepotinib in NSCLC patients with MET ex14 mutations. American Society of Clinical Oncology; 2019.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



