
Submitted:
03 March 2025
Posted:
04 March 2025
You are already at the latest version
Abstract
Background and Clinical Significance: Cystic Echinococcosis (CE), also known as hydatid disease is a zoonosis in whose life cycle human can be an accidental intermediate host. The liver is the most commonly affected organ, with complications like cyst rupture, hematogenous spread and infection. Imaging techniques such as ultrasound, CT and MRI play a vital role in diagnosing and classifying the disease, facilitating the appropriate therapeutic approach. Treatment options include albendazole for early-stage cysts with more invasive procedures like PAIR, MoCAT and surgery for advanced cases. This article highlights the importance of imaging modalities in diagnosing and therapeutic management of CE. Case Presentation: We report the case of a 23-year-old female patient presented with nausea, fatigue and loss of appetite to the emergency department, who was diagnosed with a giant Echinococcosis lesion. Conclusions: This case highlights the importance of imaging modalities in diagnosing and therapeutic management of CE.
Keywords:
echinococcosis
; hydatid disease
; apparent diffusion coefficient (ADC)
; magnetic resonance imaging (MRI)
; water lily sign
1. Introduction and Clinical Significance
Echinococcosis is a zoonosis that has two basic forms, Alveolar Echinococcosis (AE) caused by Echinococcus multilocularis and Cystic Echinococcosis (CE) caused by Echinococcus granulosus [1]. While AE is a rare form and found solely on northern hemisphere, CE, also known as hydatid disease, is endemic in South America, Eastern and Southern Europe, Russia, the Middle East, Africa and China [2]. The liver is the organ most commonly affected, with an infestation rate ranging from 60% to 75%. Among these cases, the right lobe is involved in 80%, while the left lobe is affected in 20% [3]. Less frequently, other organs such as the lungs (25%), spleen, kidneys and brain may also be involved [4]. There are several potential complications including local manifestations such as rupture as well as the risk of hematogenous spread to other organs [3]. The most used imaging modalities for CE diagnosis are ultrasound (US), computed tomography (CT) and magnetic resonance imaging (MRI) [5].
In this paper we discuss recent implementations in diagnostics and therapy, while presenting a case report of a 23–year-old female patient with Giant Cystic Echinococcosis, who was followed up for 6 months using MR imaging in a tertiary care hospital in Dortmund, Germany.
2. Case Presentation
A 23-year-old female patient presented with nausea, fatigue and loss of appetite to the emergency department for 6-8 weeks. Abdominal examination did not reveal any significant findings. Laboratory blood tests showed elevated AST 62 (U/l), ALT 74 (U/l) and GGT 107 (U/l). Ultrasound of the abdomen discovered a single hypoechoic lesion with sharp margins in Segment IV (Lobus Quadratus) of the liver. The serology for Echinococcosis (IHA and EIA) showed positive values. The patient was admitted to the hospital and further diagnostics were initiated. Liver MRI confirmed a cystic structure with multiple daughter cysts, hypointense on T1 weighted image (T1WI), hyperintense on T2 weighted image (T2WI), with no contrast uptake, no solid components, and no signs of membrane rupture and maximum diameter of 10 cm (craniocaudal) (Figure 1). DWI/ADC mapping further indicated a hydatid cyst, as it showed a peripheral moderate hyperintensity in DWI. Additionally, elevated signals on T2WI in the surrounding liver tissue were found.
The previous findings were highly suspicious of Echinococcosis, and according to World Health Organization Informal Working Groups on Echinococcosis (WHO-IWGE) classified as CE2. The surgical department decided not to opt for a surgical resection due to difficult access to the cyst and therapy with antihelminthic medication albendazole was initiated. Additional diagnostics, including chest CT, did not find any further extrahepatic manifestations of the hydatid disease. Six months later, a second MRI scan to follow-up and control the success of therapy was performed, revealing a decrease of the size cyst from 10 cm in maximal diameter to 8.5 cm. In contrast to the preceding scan, typical T2 hypointense membrane-like structures were observed within the lesion in T2WI. These represented most probably the floating membranes, the typical water-lily sign (Figure 2.). Consecutively, the cyst was classified as WHO-CE3A.
3. Discussion
The life cycle of Echinococcus granulosus involves two hosts: a definitive host, typically a dog (or other carnivores) and an intermediate host, usually a sheep. The adult worm lives in the small intestine of the definitive host, releasing eggs that are excreted in feces. Sheep ingest the eggs while grazing and the larvae (oncospheres) penetrate the intestinal wall, entering the portal circulation and forming cysts in the liver. The cycle is completed when the definitive host consumes the viscera of the infected intermediate host. Humans can become accidental intermediate hosts through contact with infected dogs or consumption of contaminated water or food. In the human liver, cysts grow up to 1 cm in the first 6 months, and 2-3 cm annually thereafter, depending on the host’s immune response [6]. Due to their slow growth they are usually asymptomatic or have unspecific clinical presentation [7].
The natural progression of hepatic hydatid cysts predisposes rupture as a complication in 50 % to 90 % of cases, potentially leading to an anaphylactic reaction. Besides rupturing in the blood stream, more rarely, 0.5 % of the cysts rupture in hollow organs and present with hydatidemesis or hydatidorrhea. In 5 % to 15 % of the cases, it can rupture into the biliary tree and lead to symptoms of biliary obstruction. Furthermore, a cyst can get infected or undergo exophythic growth or transdiaphragmatic involvement with the bare area of the liver being one of the most common pathways. Peritoneal echinococcosis occurs in 13 % of the cases, mostly after surgeries of hepatic diseases [6]. Another complication is a compression or thrombosis of the portal vein [8]. Echinococcosis can act like a tumour and spread hematogenously to every organ, found even in pericard, spinal cord, adrenal glands and muscle [9]. Imaging modalities used for diagnosis are US, CT and MRI [5]. Serology has only a confirmational role after imaging [9].
Because of the difference in growing patterns AE and CE have different imaging findings but have a similar therapy approach. CE has a concentric expansion and AE has a vesicle-to-vesicle growth forming grapes-like clusters with infiltrative nature [2]. CE is the more common type of Echinococcosis [5]. In this paper we will focus on typical imaging findings and therapy plan for CE. Most important differential diagnosis for CE is a cyst with calcification [2]. Ultrasound depicts calcification and is often used as a screening tool because it is not only highly sensitive and specific but also non-invasive, widely available and a cost-efficient mode of investigation [2,10]. The cyst wall typically appears as two echogenic lines with a hypoechogenic fluid layer in between. Simple cysts lack internal structures, but a hydatid cyst may show echogenic foci, known as hydatid sand, that shift to the lowest part of the cyst when the patient is repositioned. This movement creates the snowstorm sign, where the foci appear scattered like a snowstorm, without forming distinct layers [6]. Water lily sign on ultrasound, CT and MRI is used for describing the detachment of the membrane inside the cyst. Depending on the membrane configuration, it can also be observed as a snake sign (also called serpent sign) [11].
CT, with its high sensitivity and specificity, is an effective method for describing rupture, infection, calcification and extrahepatic spread [2,5,6]. On the other hand, MRI is a modality of choice for biliary complications [2]. CT depicts air-fluid levels in case of infection or perforation into hollow viscera. It is a modality of choice in case of peritoneal seeding because it enables the imaging of the whole abdomen [6]. CT is not suitable for staging of the hydatid disease. Furthermore, CT and MR finding that helps to rule out CE is internal enhanced septa [2]. On contrary, specific signs of the disease are daughter cysts and internal detached membrane [12].
In diagnosing CE, MRI is of more value than CT [13]. On MRI, hepatic cysts show homogeneous very low signal intensity on T1WI and homogeneous very high signal intensity on T2WI. Due to their fluid content, there is a notable increase in signal intensity on heavily T2WI, which helps differentiate these cysts from metastatic lesions [14]. No enhancement is observed after the administration of gadolinium contrast. In rare cases of intracystic hemorrhage, when blood products are mixed within the cyst, the signal intensity becomes high, and a fluid-fluid level is seen both on T1WI and T2WI [12]. These features are observed within hydatid cysts as well, although there are differences regarding their histopathological features. A hydatid cyst has three distinct layers; the outer adventitial layer formed by the host liver tissue (pericyst), middle laminated layer derived by parasite and inner germinal layer derived by the parasite [6,13].
MR imaging clearly visualizes pericyst, matrix and daughter cysts. The pericyst appears as a hypointense rim on both T1WI and T2WI due to its fibrous structure and the presence of calcifications. This is a specific feature of hydatid cysts, called the rim sign, mostly better visualized on T2WI [5]. The matrix represents hydatid fluid containing membranes of broken daughter vesicles, scolices, and hydatid sand [6]. The hydatid matrix appears hypointense on T1WI and significantly hyperintense on T2WI. When daughter cysts are present, they are typically more hypointense than the matrix on T2WI, as observed in our case report [14] (Figure 1).
If the membrane is separated it can shift with movement, resembling a water lily floating on the surface of a pond, previously described as water lily sign, which was seen in our case report as well [15] (Figure 2.). Diffusion weighted imaging (DWI) is an MRI technique that allows quantitative and non-invasive measurement of water molecule diffusion in biological tissues. DWI enables to calculate apparent diffusion coefficients using different b-values. B-value measures the degree of diffusion weighting applied [16]. Inan et al. and Yalcinoz et al. found significant difference between hydatid cysts type CE 1 and CE 2 and simple cyst based on significantly lower mean ADCs of hydatid cysts [16,17]. On contrary, Konukoglu et al. did not find any significant difference between these two entities in ADC comparing all stages of hydatid cyst and simple cysts [18]. Distinction between simple cysts and hydatid cysts (CE 1 and CE 2) can be identified using ADC measurements at b600 and b1000 values. Both simple and hydatid cysts (CE 1 and CE 2) appear isointense on DWI with b1000, but simple cysts exhibit a peripheral moderate hyperintensity when compared to hydatid cysts [17].
4. Conclusions
The main focus of this paper is to highlight the crucial role of imaging modalities in the classification of echinococcosis, which is essential for making informed therapeutic decisions; taking into consideration the limited predictive value of serology for CE.
Due to globalization, echinococcosis is no longer confined only to tropical regions, stretching the need for heightened awareness and inclusion of this disease in differential diagnoses.
MRI with DWI/ADC mapping is a specific and sensitive tool, not only for diagnosing hydatid cyst in its earliest stage, but for establishing and surveilling a therapy plan. In contrary, in low-setting environment, where the disease is endemic, not all diagnostic tools are available which makes the diagnostic more challenging.
Application and continuous development of clear guidlines, accessible tailored therapeutical approach and establishment of a multidisciplinary team where it is possible, are essential for effectively managing this disease and preventing its spread.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to its retrospective model and the informed consent obtained from the participant as part of the standard care in the University Hospital.
Informed Consent Statement
Informed consent was obtained from the patient for his data and images to be used in this study and published in this journal. The patients understood that their anonymity would be preserved, and no identifiable information would be disclosed.
Conflicts of Interest
None of the authors have any conflicts of interest to declare.
Abbreviations
The following abbreviations are used in this manuscript:
| ADC | Apparent diffusion coefficient |
| AE | Alveolar echinococcosis |
| CE | Cystic echinococcosis |
| CT | Computed tomography |
| DWI | Diffusion weighted imaging |
| MoCAT | Modified catheterization technique |
| MRI | Magnetic resonance imaging |
| PAIR | Puncture-Aspiration of cyst contents-Injection of protoscolecidal agents |
| T1WI | T1 weighted image |
| T2WI | T2 weighted image |
| US | Ultrasound |
References
- Gatti, M.; Maino, C.; Tore, D.; Carisio, A.; Darvizeh, F.; Tricarico, E.; Inchingolo, R.; Ippolito, D.; Faletti, R. Benign focal liver lesions: The role of magnetic resonance imaging. World J. Hepatol. 2022, 14, 923–943. [Google Scholar] [CrossRef] [PubMed]
- Calame, P.; Weck, M.; Busse-Cote, A.; Brumpt, E.; Richou, C.; Turco, C.; Doussot, A.; Bresson-Hadni, S.; Delabrousse, E. Role of the radiologist in the diagnosis and management of the two forms of hepatic echinococcosis. Insights into Imaging 2022, 13, 1–20. [Google Scholar] [CrossRef]
- Alexiou; Alexiou, K. ; Mitsos, S.; Fotopoulos, A.; Karanikas, I.; Tavernaraki, K.; Konstantinidis, F.; Antonopoulos, P.; Ekonomou, N. Complications of Hydatid Cysts of the Liver: Spiral Computed Tomography Findings. Gastroenterol. Res. 2012, 5, 139–143. [Google Scholar] [CrossRef]
- Jallali, M.; Chaouch, M.A.; Zenati, H.; Ben Hassine, H.; Saad, J.; Noomen, F. Primary isolated hydatid cyst of the spleen: A case report. Int. J. Surg. Case Rep. 2024, 117, 109552. [Google Scholar] [CrossRef] [PubMed]
- Marrone, G.; Crino', F.; Caruso, S.; Mamone, G.; Carollo, V.; Milazzo, M.; Gruttadauria, S.; Luca, A.; Gridelli, B. Multidisciplinary imaging of liver hydatidosis. World J. Gastroenterol. 2012, 18, 1438–47. [Google Scholar] [CrossRef]
- Pedrosa, I.; Saíz, A.; Arrazola, J.; Ferreirós, J.; Pedrosa, C.S. Hydatid Disease: Radiologic and Pathologic Features and Complications. RadioGraphics 2000, 20, 795–817. [Google Scholar] [CrossRef] [PubMed]
- Sutihar, A.; Lamichhane, D.; JanakyRaman, G.; Arafin, M.; Shrestha, R.J.; Pandey, N.; Yadav, A.; Uprety, S. Giant Calcified Hepatic Hydatid Cyst: A Case Report. Cureus 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Tesemma, A.; Adane, M.; Bekele, K.; Debebe, B.; Rosso, E.; Zenbaba, D.; Gomora, D.; Beressa, G. Giant pedunculated liver hydatid cyst causing inferior vena cava syndrome: a case report. J. Med Case Rep. 2024, 18, 1–4. [Google Scholar] [CrossRef]
- Srinivas, M.R.; Deepashri, B.; Lakshmeesha, M.T. Imaging Spectrum of Hydatid Disease: Usual and Unusual Locations. Pol. J. Radiol. 2016, 81, 190–205. [Google Scholar] [CrossRef]
- World Health Organization. Neglected tropical diseases in the context of the Sustainable Development Goals. WHO-HTM-NTD-NZD-2017.01. Geneva: World Health Organization; 2017. Available from: https://www.who.int/publications/i/item/WHO-HTM-NTD-NZD-2017.
- Farrar J, Hotez PJ, Junghanss T, Kang G, Lalloo D, White NJ, Garcia PJ. Manson's Tropical Diseases. 24th ed. London: Elsevier; 2023. ISBN: 9780702079597.
- Precetti, S.; Gandon, Y.; Vilgrain, V. ing of cystic liver diseases. J. Radiol. 2007, 88, 1061–1072. [Google Scholar] [CrossRef] [PubMed]
- Wen, H.; Vuitton, L.; Tuxun, T.; Li, J.; Vuitton, D.A.; Zhang, W.; McManus, D.P. Echinococcosis: Advances in the 21st Century. Clin. Microbiol. Rev. 2019, 32, e00075–18. [Google Scholar] [CrossRef] [PubMed]
- Mortelé, K.J.; Ros, P.R. Cystic Focal Liver Lesions in the Adult: Differential CT and MR Imaging Features. RadioGraphics 2001, 21, 895–910. [Google Scholar] [CrossRef] [PubMed]
- Grocholski, S.; Agabawi, S.; Kadkhoda, K.; Hammond, G. Echinococcus granulosus hydatid cyst in rural Manitoba, Canada: Case report and review of the literature. IDCases 2019, 18, e00632. [Google Scholar] [CrossRef] [PubMed]
- Inan, N.; Arslan, A.; Akansel, G.; Anik, Y.; Sarisoy, H.T.; Ciftci, E.; Demirci, A. Diffusion-Weighted Imaging in the Differential Diagnosis of Simple and Hydatid Cysts of the Liver. Am. J. Roentgenol. 2007, 189, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Yalcinoz, K.; Ikizceli, T.; Kahveci, S.; Karahan, O.I. Diffusion-weighted MRI and FLAIR sequence for differentiation of hydatid cysts and simple cysts in the liver. Eur. J. Radiol. Open 2021, 8, 100355. [Google Scholar] [CrossRef] [PubMed]
- Konukoglu, O.; Tahtabasi, M.; Boyaci, F.N.; Karakas, E. The role of diffusion-weighted imaging in the differential diagnosis of liver lesions. Central Asian J. Med Hypotheses Ethic- 2024, 5, 13–23. [Google Scholar] [CrossRef]
- Djuric-Stefanovic, A.; Cvejic, S.; Mijovic, K.; Ostojic, S. Rosette sign. Abdom. Imaging 2022, 47, 2560–2561. [Google Scholar] [CrossRef] [PubMed]
- Brunetti, E.; Kern, P.; Vuitton, D.A.; Writing Panel for the WHO-IWGE. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010, 114, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Akhan, O.; Gumus, B.; Akinci, D.; Karcaaltincaba, M.; Ozmen, M. Diagnosis and Percutaneous Treatment of Soft-Tissue Hydatid Cysts. Cardiovasc. Interv. Radiol. 2007, 30, 419–425. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Axial T2W MRI, hypointense daughter cysts.
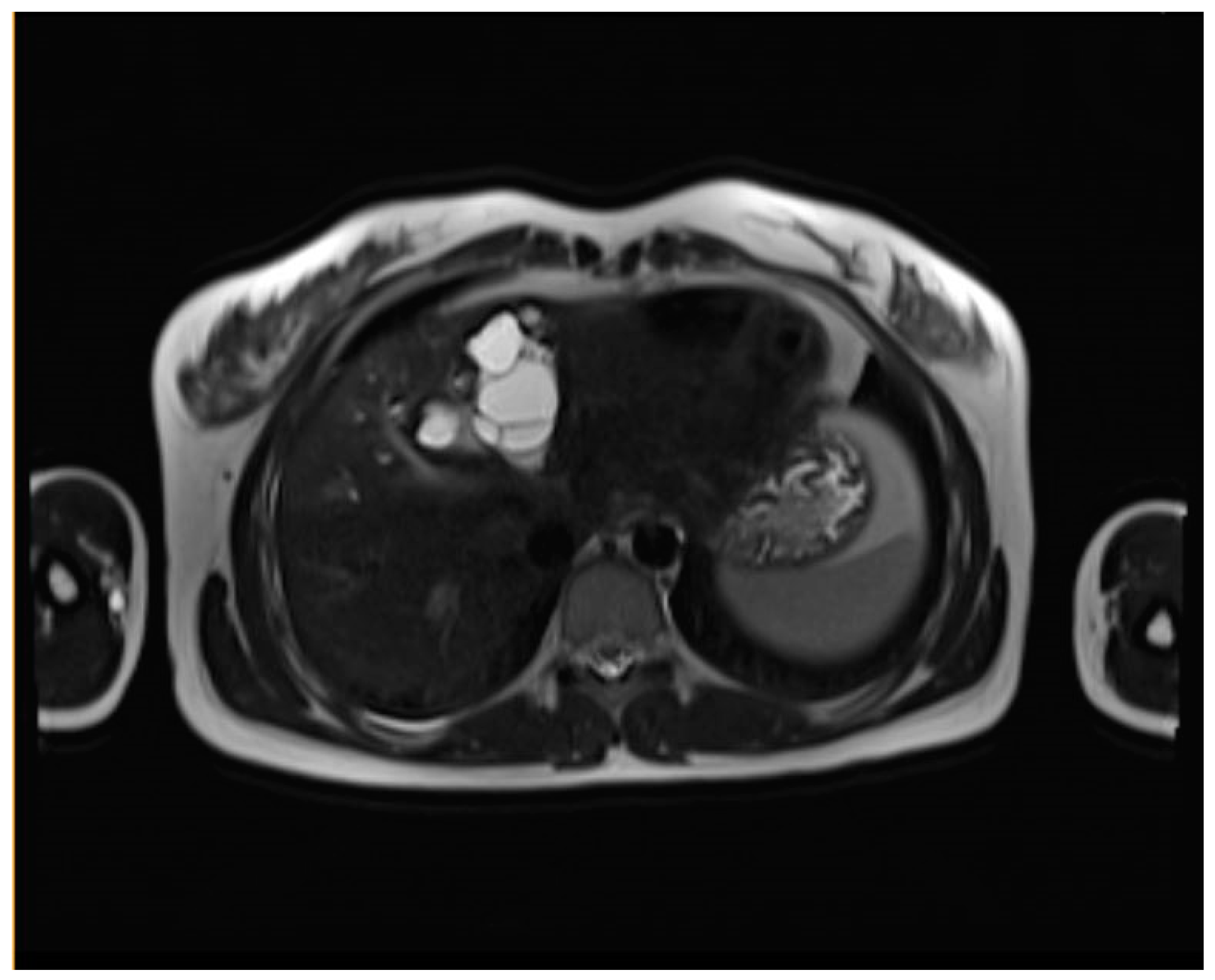
Figure 2.
Axial T2W MRI, water lily sign after medical treatment.
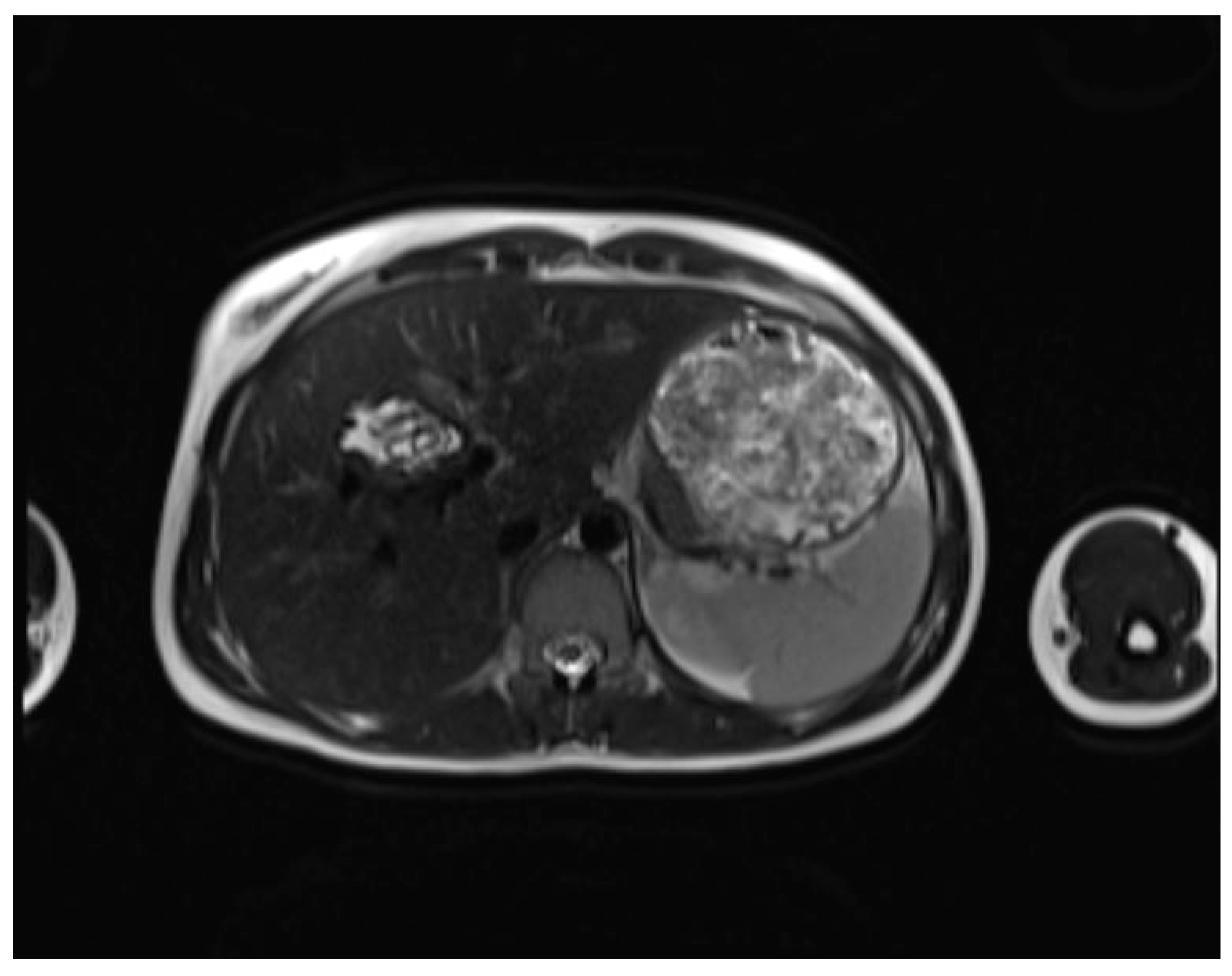

Table 1.
WHO-IWGE-Classification, the MRI and US appearance (4, 12, 19). CE1: Active stage with fluid-filled cyst and peripheral capsule. CE2: Active stage with daughter cysts visible. CE3: Transitional stage, with CE3A showing the water lily sign (detached laminated membranes) and CE3B showing daughter cysts within a solid matrix. CE4: Inactive stage, often with calcifications and heterogeneous content. Complications like rupture can alter the imaging appearance. CE5: Completely calcified cyst, hypointense on MRI with no residual cystic structures.
Table 1.
WHO-IWGE-Classification, the MRI and US appearance (4, 12, 19). CE1: Active stage with fluid-filled cyst and peripheral capsule. CE2: Active stage with daughter cysts visible. CE3: Transitional stage, with CE3A showing the water lily sign (detached laminated membranes) and CE3B showing daughter cysts within a solid matrix. CE4: Inactive stage, often with calcifications and heterogeneous content. Complications like rupture can alter the imaging appearance. CE5: Completely calcified cyst, hypointense on MRI with no residual cystic structures.
| WHO-IWGE staging | MRI | US |
|---|---|---|
| CE1 (Simple cyst) | Well-defined, unilocular cyst with a peripheral capsule, hypointense on T2WI, possible rim sign. Hyperintense hydatid matrix on DWI and ADC. | Unilocular anechoic cyst with possible rim sign and internal echoes (hydatid sand, snowflake sign) seen after repositioning. |
| CE2 (Cyst with daughter cysts and matrix) | Multicystic mass with septa (wheel-spoke pattern), daughter cysts are hypointense or isointense compared to the mother cyst on both T1WI and T2WI. | Well-defined cyst with multiple internal septations and daughter cysts, described as honeycomb or rosette appearance. |
| CE3A (Transitional) | Detachment of laminated membranes, with a floating water lily sign or serpent sign. Daughter cysts may be visible in the matrix. | Internal floating membranes or detached laminated membranes (water lily sign). |
| CE3B (Transitional; daughter cysts within solid matrix) | Solid matrix with visible daughter cysts; signal intensity varies depending on the proteinaceous content of the cyst. | Similar to CE3A, but daughter cysts are present within a solid matrix, often with calcification. |
| CE4 (Complicated or inactive cyst) | Heterogeneous mass with hypointense and hyperintense areas, often partially or completely calcified. Inactive stage. May show signs of complication like rupture (biliary communication) or infection. | Cyst with heterogeneous hypoechoic and hyperechoic contents, resembling a ball of wool; absence of daughter cysts. |
| CE5 (Completely calcified cyst) | Complete calcification, appearing as hypointense on all MRI sequences due to lack of fluid. No residual daughter cysts. | Completely calcified cyst with no internal structures. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



