
Submitted:
25 February 2025
Posted:
25 February 2025
You are already at the latest version
Abstract
Background/Objectives: Influenza infection is associated with cardiovascular mor-bidity and mortality, but effect of influenza vaccination on cardiovascular outcomes is not fully understood. This clinical trial aimed to investigate correlation between car-diovascular outcomes and influenza vaccine (FluVac) in coronary artery diseases (CAD) subjects. Methods: This was a randomized single blinded placebo-controlled trial. Enrolled CAD subjects received 0.5 ml of 2007-2008 trivalent FluVac (15µg he-magglutinin of each of Solomon Islands/3/2006 (H1N1), Wisconsin/67/2005 (H3N2), and Malaysia/2506/2004 (B)). Subjects were followed up at 1 month (hemagglutinin (HA) antibody titers), and at 12 months post-vaccination for evaluation of outcomes (influenza-like episodes, acute coronary syndrome (ACS), myocardial infarction (MI), coronary revascularization, and death). Results: 278 eligible CAD subjects were ran-domized to receive either FluVac (n = 137) or placebo (n = 141) of which consequently 131 and 135 subejcts completed the study. Cardiovascular deaths (3/131 [2.29%] vs. 3/135 [2.22%]) and all-cause deaths (4/131 [3.05%] vs. 4/135 [2.96%]) were similar in both groups. Adverse cardiovascular events, including ACS, MI, and coronary revas-cularization were less frequent in the vaccine group, but did not reach statistical sig-nificance. Magnitude of antibody change and serologic response (≥4-fold HI titer rise) of all three antibodies were significantly higher in the vaccine group compared to the placebo but did not correlate with cardiovascular outcomes in the FluVac group. Con-clusions: Influenza vaccine may improve cardiovascular outcomes, though this im-provement is not correlated with post-vaccination antibody titers. Despite controver-sies, Influenza vaccination is recommended in CAD population. (ClinicalTrials.gov NCT00607178)
Keywords:
Coronary artery disease (CAD)
; Influenza vaccine
; Cardiovascular outcome
; Antibody
1. Introduction
Coronary Artery Disease (CAD) is the leading cause of death with above $400 billion annual direct and indirect costs in the United States [1]. Most individuals who experience a Myocardial Infarction (MI), are reported to have at least one cardiovascular risk factor before the event [2,3]. It is well established that moving toward an ideal cardiovascular health not only prevents cardiovascular adverse events, but also is associated with decrease in heart failure, cancer, depression, and cognitive impairment [4,5].
An association between influenza vaccination and improved cardiovascular mortality has been suggested [6,7,8]; the mechanisms remain unknown [9,10,11]. Several clinical trials have evaluated correlation between influenza vaccination and cardiovascular outcomes; this correlation is also still controversial [12,13,14,15,16].
In the current trial, we evaluated correlation between 2007-2008 influenza vaccine (FluVac) and cardiovascular outcomes in CAD patients. In phase 1 (previously reported), we evaluated antibody (Ab) response to influenza vaccine in CAD patients which was comparable to healthy controls [17]. In phase 2 (current report), we evaluated cardiovascular outcomes 12 months after vaccination in vaccine recipients in comparison with placebo controls. The delay in reporting the result was nothing other than our time limitations.
2. Materials and Methods
2.1. Study Design and Ethics
This randomized, placebo-controlled, single blinded clinical trial (IVCAD) was performed at Shahid Modarres Medical Research Center, Shahid Beheshti University of Medical Sciences, Tehran, Iran. Participants were enrolled from January to August 2008.
IVCAD was conducted following the principles of Declaration of Helsinki and received approval from the ethics committee of Shahid Beheshti University, Tehran, Iran (Study# SBMU-86-03-105-5433A). Before enrollment, all participants provided informed written consent. The trial was registered at clinicaltrials.gov (NCT00607178).
2.2. Participants
Two hundred and seventy-eight (278) CAD subjects enrolled in the trial. Eligible subjects had to be ≥25 years with either stable angina or confirmed coronary artery stenosis by angiography, or recent MI after recovering from acute phase. MI was diagnosed with either pathological finding of an acute MI [18] or changing in biochemical markers (rise and gradual fall (troponin T) or more rapid rise and fall (CK-MB)) of myocardial necrosis with at least one of the following: ischemic symptoms, development of pathologic Q waves or ST segment elevation or depression on the electrocardiogram (ECG), or coronary artery intervention (e.g. coronary angioplasty). We excluded subjects who had any acute disease, unstable angina, chronic kidney or liver diseases, immunosuppression (e.g. transplantation, Human Immunodeficiency Virus (HIV)), confirmed history of active malignancy, inoculation with influenza vaccine or severe influenza infections requiring hospitalization within the past five years, any psychological illness which could interfere with the regular follow up, congestive heart failure (NYHA III/IV and/or Killip class IV [19]), and contraindications of vaccine inoculation (e.g., egg allergy). To check the basic characteristics, a detailed medical history was taken from all subjects, and they underwent a complete echocardiography assessment. Additionally, Angina severity and coronary artery stenosis were assessed using the Seattle Angina Questionnaire (SAQ) [20] and the modified Gensini Score (MGS) [21], respectively. SAQ serves as a reliable tool for assessing coronary artery disease surveillance. It encompasses five key factors: physical limitations, angina stability, angina frequency, treatment satisfaction, and disease perception. These criteria are employed to evaluate clinical changes and cardiovascular outcomes [20]. MGS is a scale used to estimate the degree of stenosis in coronary arteries. This grading system assigns scores to the main vessels and their branches based on the severity of obstruction (<50%, 50–74%, 75–99%, and 100%) observed in coronary angiography. MGS was scored for all subjects by the same cardiologist. By combining individual scores, final scores ranging from 0 to 20 were calculated. Higher scores are indicative of a higher degree of severity in coronary artery disease [21].
2.3. Randomization, Blinding and Trial Intervention
Eligible subjects were randomized to receive either the influenza vaccine (CAD-FluVac, n = 137) or placebo (CAD-Placebo, n = 141) in a 1:1 ratio using a computer-generated sequence. Participants were blinded to group assignment. The influenza vaccine (FluVac-trivalent influenza vaccine, Solvay Pharma) or placebo was administered as a single 0.5 ml dose into deltoid muscle. The vaccine contained 15µg hemagglutinin of each of the three strains, namely Solomon Islands/3/2006 (H1N1), Wisconsin/67/2005 (H3N2), and Malaysia/2506/2004 (B) according to the World Health Organization guidelines for the anti-influenza vaccination campaign of 2007–2008. Control subjects received one 0.5 ml dose of distilled water into deltoid. All subjects were continued on their standard CAD treatments.
2.4. Antibody Response
Subjects were evaluated before the intervention and at 1 month follow-up for antibody measurements. During the first follow-up visit at one month, Ab titers were measured using hemagglutination inhibition (HI) test [22], which utilized hemagglutinin antigens representing the virus strains contained in the vaccine. The test involved two-fold dilutions of the serum, ranging from 1:10 to 1:1280. Titers lower than 1:10 were recorded as 1:5. The result of antibody response has been published separately [17]. Protective titer or seroconversion was defined as ≥4-fold rise in HI titer.
2.5. Outcomes
Subjects were followed up at 12 months via phone call for outcome evaluation. During this final follow up, subjects were questioned about MI, Acute Coronary Syndrome (ACS), Coronary Artery Bypass Graft surgery (CABG), Percutaneous Intervention (PCI), and number of cold episodes. Additionally, we recorded whether the patient had been reported as deceased (at any time point during the study) through their emergency contact or access to medical record if available and investigated if death was due to cardiovascular cause. Six subjects in each group were lost to follow-up, all due to changes in the contact information of both the subject and their emergency contact.
2.6. Sample Size Estimation and Statistical Analysis
Sample size was estimated to detect a 10% difference in protection rate with an α error of 0.05 and a study power of at least 0.7. Therefore, we aimed to recruit about 300 subjects in the study.
2.7. Analysis
Demographic and clinical characteristics at enrollment were characterized with descriptive statistics (frequency and percentage or mean and standard deviation (SD) for categorical and continuous variables, respectively).
Primary and secondary binary outcomes were compared between randomized arms using logistic regression to estimated odds ratios (OR) and 95% confidence intervals (95%CI). Secondary event count outcomes (acute coronary syndrome and cold episodes) were compared between randomized arm using generalized linear regression with a Poisson distribution, a log-link and an offset for person-months of follow-up to estimate incidence rate ratios (IRR) and 95%CIs.
We utilized Fisher’s Exact Test to determine differences in protective hemagglutination inhibition (HI) titers between the Influvac and Placebo groups at the 1-month follow-up. Kruskal-Wallis tests were used to assess differences in the magnitude of antibody titers between groups. These analyses were repeated at the 12-month follow-up for respondents who received Influvac to examine differences between patients who did and did not experience a cardiovascular event during follow-up.
Statistical significance was determined at α=0.05. All statistical analyses were conducted using R version 4.0.0.
3. Results
3.1. Baseline Characteristics
Between January and August 2008, 278 CAD subjects (mean age 54.73 [SD 15.4], female 33.5%) were enrolled and randomized into CAD-FluVac (n=137) or CAD-Placebo (n=141) group. Six subjects (4%) in each group were lost to follow up (Figure 1).
3.2. 12-Months Outcome
Cardiovascular death was not significantly different between CAD-FluVac and CAD-Placebo groups (3 (2.29%) vs. 3 (2.22%)). Similarly, all-cause mortality did not differ between the two groups (4 (3.05%) vs. 4 (2.96%)). However, ACS, MI, and cardiovascular interventions were less frequent in the CAD-FluVac compared to the CAD-Placebo group but did not reach statistical significance (Figure 2).
Figure 2.
12-months Cardiovascular Outcomes (yes/no) in subjects with CAD, comparison FluVac vs. Placebo group. *At least one outcome (acute coronary syndrome, myocardial infarction, Coronary Artery Bypass Graft (CABG), percutaneous intervention, or death). Analysis: Logistic regression used to estimate incidence rate ratios (IRR) and 95% confidence intervals (95%CI).
Figure 2.
12-months Cardiovascular Outcomes (yes/no) in subjects with CAD, comparison FluVac vs. Placebo group. *At least one outcome (acute coronary syndrome, myocardial infarction, Coronary Artery Bypass Graft (CABG), percutaneous intervention, or death). Analysis: Logistic regression used to estimate incidence rate ratios (IRR) and 95% confidence intervals (95%CI).

The number of ACS and cold episodes were also separately analyzed, showing fewer episodes in CAD-FluVac, but did not reach statistical significance (IRR: 0.69 [0.37-1.124], P: 0.22) (Figure 3).
3.3. Antibody Response
The antibody response in the two groups is depicted in Table 3. Protective titer of anti H1N1 antibody was significantly higher in CAD-FluVac vs CAD-Placebo group (53% vs 46%, P-value<0.0001). The magnitude of change and serologic response (≥4-fold HI titer rise) of all three antibodies were significantly higher in the CAD-FluVac group. (Table 3)
We also conducted a subgroup analysis within the CAD-FluVac group to evaluate correlation between antibody titer and cardiovascular outcomes. There was no statistically significant difference in antibody titers between vaccinated participants who had cardiovascular events and those who did not (Table 4).
4. Discussion
Influenza vaccine has been observed to be beneficial in patient with cardiac diseases. The relationship between influenza vaccination and cardiovascular outcome has been reported in multiple observational trials in the past [23,24,25,26,27,28], but few clinical trials have evaluated the correlation. The increased cardiovascular risk after influenza infection can be explained by several mechanisms, including the destabilization of atherosclerotic plaque, increased macrophages in the circulation, proinflammatory molecules like Tumor necrosis factor (TNF)-like weak inducer of apoptosis (TWEAK), and sympathetic activation [3,29,30,31,32,33,34,35,36]. However, it remains controversial whether the influenza vaccine can prevent subsequent cardiovascular events or improve cardiovascular outcomes.
IVCAD was originally designed in 2008 to evaluate this correlation, its data has participated in multiple meta-analysis in 2013, 2015 and most recently 2023 [23,27,28] despite our time limitations to publish it. We have now decided to publish this full report due to continued discussions and remaining controversies in this field since then.
As data shows, IVCAD did not show any statistically significant correlation between influenza vaccination and 12-months cardiovascular/ all-cause mortality. However, influenza vaccination was associated with a 27% reduction in the odds of cardiovascular adverse events (ACS, MI, cardiovascular interventions), although this did not reach statistical significance either.
The results of IVCAD are almost comparable to a recently performed large multicentric placebo-controlled clinical trials conducted by Loeb et al. They enrolled 5,129 heart failure subjects in Asia, Middle east and Africa and did not find any significant improvement in non-fatal MI, non-fatal stroke, heart failure hospitalization, all-cause death and cardiovascular death during a 2.3-year follow-up period in vaccinated group compared to placebo. Interestingly there was a clear reduction in cardiac death, all-cause death and pneumonia only during peak influenza circulation in vaccinated group suggesting benefits [16].
Another trial conducted by Phrommintikul et al. recruited 439 subjects admitted for ACS during 2007-2008 season. The trial reported a significant reduction in major adverse cardiovascular outcomes (death, hospitalization for ACS, heart failure and stroke) at 12-months follow-up after influenza vaccination but did not show any significant improvement in cardiovascular death [15].
Two recent meta-analysis by Gupta et al. [37] and Omidi et al. [38] in 2023, included data from several existing clinical trials. Included trials did not involve similar populations, and some lacked a placebo control group. All these trials concluded that influenza vaccination has protective effects against cardiovascular adverse events and suggested further research to elucidate the precise effects and mechanisms of influenza vaccination on cardiovascular outcomes, while considering vaccination for CAD patients [38].
IVCAD study also did not demonstrate a significant difference in antibody response to influenza vaccine in CAD patients in subpopulations with and without cardiovascular events. To the best of our knowledge there is no other existing parallel data. In a prior publication in IVCAD study population, antibody response in CAD patients was comparable to healthy controls [17]. These results might propose a non-antibody mediated mechanism related to influenza vaccine and its cardioprotective effect. Further evaluation of this correlation is needed in future studies.
There was some limitation with IVCAD study. It had a small sample size, and the results of this study should be interpreted cautiously. Results from IVCAD were similar to other studies showing no statistical significance. In contrast to some more recently designed trials, we did not record the seasonal outcomes, which might have provided more detailed and related cardiovascular outcomes during peak virus circulation. The follow-up period for the current study was 12 months, which is similar to most of the other studies, but a longer follow-up period would have been preferred. Moreover, outcomes were cumulative and could have happened any time after vaccination until 12 months post-vaccination. IVCAD was also a single blinded study (due to technical limitation in design) which is not the preferred methodology in clinical trials and could have impacted its validity.
5. Conclusions
Our study shows that influenza vaccination is associated with lower cardiovascular events in CAD population; however, antibody titer was not correlated with cardiovascular outcomes. This can explain potential non-antibody mediated molecular and cellular immune regulatory pathways for this observation. Further research to investigate other non-antibody immune correlates is recommended to move forward. Based on current existing literature, Influenza vaccination is highly recommended for CAD populations with potential benefit in improving their outcomes, further research, especially large double-blinded controlled clinical trials with longer follow-up period focused on non-antibody mediated correlates, is needed to elucidate the precise effect of vaccination on cardiovascular events and eliminate confounding effects.
Author Contributions
Conceptualization, M.K.; methodology, S.G., S.R., A.S, M.R.; software, E.G.; validation, M.K, M.D.; formal analysis, Y.W.; investigation, S.G., S.R., A.S, M.R.; resources, H.V, M.K.; data curation, M.D., M.K.; writing—original draft preparation, M.D.; writing—review and editing, M.D, S.G.,S.R., A.S, M.R., M.K, Y.W., E.G.; visualization, S.G., S.R., A.S, M.R.; supervision, M.K.; project administration, H.V.; funding acquisition, M.K. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by Shahid Beheshti University of Medical Sciences, Tehran, Iran [SBMU-86-03-105-5433A; AMMC-13861008A].
Institutional Review Board Statement
IVCAD was conducted following the principles of Declaration of Helsinki and received approval from the ethics committee of Shahid Beheshti University, Tehran, Iran (Study# SBMU-86-03-105-5433A). The trial was registered at clinicaltrials.gov (NCT00607178).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study before enrollment.
Data Availability Statement
The data of this study is not publicly available, but it can be requested from the corresponding author.
Acknowledgments
We acknowledge the Johns Hopkins School of Medicine Biostatistics, Epidemiology and Data Management (BEAD) Core for supporting statistical analysis of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ACS | Acute Coronary Syndrome |
| Ab | Antibody |
| BMI | Body Mass Index |
| CAD | Coronary Artery Disease |
| CABG | Coronary Artery Bypass Graft surgery |
| CK-MB | Creatine Kinase-MB |
| MI | Myocardial Infarction |
| FluVac | Influenza Vaccine |
| IHD | Ischemic Heart Diseases |
| IVCAD | Influenza Vaccine and Coronary Artery Disease |
| ECG | Electrocardiogram |
| HI | Hemagglutination Inhibition |
| HIV | Human Immunodeficiency Virus |
| OR | Odds Ratio |
| SAQ | Seattle Angina Questionnaire |
| SD | Standard Deviation |
| MGS | Modified Gensini Score |
| PCI | Percutaneous Intervention |
| TNF | Tumor necrosis factor |
| TWEAK | Tumor Necrosis Factor-like Weak Inducer of Apoptosis |
References
- Johnson NB, Hayes LD, Brown K, et al; Centers for Disease Control and Prevention (CDC). CDC National Health Report: leading causes of morbidity and mortality and associated behavioral risk and protective factors--United States, 2005-2013. MMWR Suppl. 2014;63(4):3-27. 2005-2013. [PubMed]
- Greenland P, Knoll MD, Stamler J, et al. Major risk factors as antecedents of fatal and nonfatal coronary heart disease events. JAMA. 2003;290(7):891-7. [CrossRef] [PubMed]
- Lloyd-Jones DM, Hong Y, Labarthe D, et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association's strategic Impact Goal through 2020 and beyond. Circulation. 2010;121(4):586-613. [CrossRef] [PubMed]
- Younus A, Aneni EC, Spatz ES, et al. A Systematic Review of the Prevalence and Outcomes of Ideal Cardiovascular Health in US and Non-US Populations. Mayo Clin Proc. 2016;91(5):649-70. [CrossRef]
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019 Sep 10;140(11):e596-e646. Epub 2019 Mar 17. Erratum in: Circulation. 2019 Sep 10;140(11):e649-e650. doi: 10.1161/CIR.0000000000000725. Erratum in: Circulation. 2020 Jan 28;141(4):e60. oi: 10.1161/CIR.0000000000000755. Erratum in: Circulation. 2020 Apr 21;141(16):e774. oi: 10.1161/CIR.0000000000000771. PMCID: PMC7734661. [CrossRef] [PubMed]
- Warren-Gash C, Smeeth L, Hayward AC. Influenza as a trigger for acute myocardial infarction or death from cardiovascular disease: a systematic review. Lancet Infect Dis. 2009 Oct;9(10):601-10. [CrossRef] [PubMed]
- Smeeth L, Thomas SL, Hall AJ, at al. Risk of myocardial infarction and stroke after acute infection or vaccination. N Engl J Med. 2004 Dec 16;351(25):2611-8. [CrossRef] [PubMed]
- Kwong JC, Schwartz KL, Campitelli MA, et al. Acute Myocardial Infarction after Laboratory-Confirmed Influenza Infection. N Engl J Med. 2018 Jan 25;378(4):345-353. [CrossRef] [PubMed]
- Musher DM, Abers MS, Corrales-Medina VF. Acute Infection and Myocardial Infarction. N Engl J Med. 2019 Jan 10;380(2):171-176. [CrossRef] [PubMed]
- Kaynar AM, Yende S, Zhu L, et al. Effects of intra-abdominal sepsis on atherosclerosis in mice. Crit Care. 2014 Sep 3;18(5):469. [CrossRef] [PubMed] [PubMed Central]
- Madjid M, Vela D, Khalili-Tabrizi H, at al. Systemic infections cause exaggerated local inflammation in atherosclerotic coronary arteries: clues to the triggering effect of acute infections on acute coronary syndromes. Tex Heart Inst J. 2007;34(1):11-8. [PubMed] [PubMed Central]
- Fröbert O, Götberg M, Erlinge D, et al. Influenza Vaccination After Myocardial Infarction: A Randomized, Double-Blind, Placebo-Controlled, Multicenter Trial. Circulation. 2021 Nov 2;144(18):1476-1484. Epub 2021 Aug 30. [CrossRef] [PubMed]
- Ciszewski A, Bilinska ZT, Brydak LB, et al. Influenza vaccination in secondary prevention from coronary ischaemic events in coronary artery disease: FLUCAD study. Eur Heart J 2008;29:1350–1358. [CrossRef] [PubMed]
- Ciszewski A, Bilinska ZT, Brydak LB, et al. Influenza vaccination in secondary prevention from coronary ischaemic events in coronary artery disease: FLUCAD study. Eur Heart J. 2008 Jun;29(11):1350-8. Epub 2008 Jan 10. [CrossRef] [PubMed]
- Phrommintikul A, Kuanprasert S, Wongcharoen W, et al. Influenza vaccination reduces cardiovascular events in patients with acute coronary syndrome. Eur Heart J. 2011 Jul;32(14):1730-5. Epub 2011 Feb 2. [CrossRef] [PubMed]
- Loeb M, Roy A, Dokainish H, et al. Influenza Vaccine to Prevent Adverse Vascular Events investigators. Influenza vaccine to reduce adverse vascular events in patients with heart failure: a multinational randomised, double-blind, placebo-controlled trial. Lancet Glob Health. 2022 Dec;10(12):e1835-e1844. Erratum in: Lancet Glob Health. 2023 Feb;11(2):e196. doi: 10.1016/S2214-109X(22)00517-4. [CrossRef] [PubMed]
- Keshtkar-Jahromi M, Vakili H, Rahnavardi M, et al. Antibody response to influenza immunization in coronary artery disease patients: a controlled trial. Vaccine. 2009 Dec 10;28(1):110-3. Epub 2009 Oct 9. [CrossRef] [PubMed]
- Alpert JS, Thygesen K, Antman E, at al. Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. 2000 Sep;36(3):959-69. Erratum in: J Am Coll Cardiol 2001 Mar 1;37(3):973. [CrossRef] [PubMed]
- Killip T 3rd, Kimball JT. Treatment of myocardial infarction in a coronary care unit. A two year experience with 250 patients. Am J Cardiol. 1967 Oct;20(4):457-64. [CrossRef] [PubMed]
- Spertus JA, Winder JA, Dewhurst TA et al. Development and evaluation of the Seattle Angina Questionnaire: a new functional status measure for coronary artery disease. J Am Coll Cardiol. 1995 Feb;25(2):333-41. [CrossRef] [PubMed]
- Gensini, GG. A more meaningful scoring system for determining the severity of coronary heart disease. Am J Cardiol. 1983 Feb;51(3):606. [CrossRef] [PubMed]
- WHO Collaborating Center for Influenza, Biological Products Division: The Hemagglutination Inhibition Test for Influenza Viruses. Version 31 revised, DHEW, PHS, CDC. Atlanta, GA, USA, Center for Infectious Disease, 1981;1–21.
- Modin D, Lassen MCH, Claggett B, et al. Influenza vaccination and cardiovascular events in patients with ischaemic heart disease and heart failure: A meta-analysis. Eur J Heart Fail. 2023 Sep;25(9):1685-1692. Epub 2023 Jul 5. [CrossRef] [PubMed]
- Modin D, Jørgensen ME, Gislason G, et al. Influenza Vaccine in Heart Failure. Circulation. 2019 Jan 29;139(5):575-586. [CrossRef] [PubMed]
- Kaya H, Beton O, Acar G, et al. Influence of influenza vaccination on recurrent hospitalization in patients with heart failure. Herz. 2017 May;42(3):307-315. English. Epub 2016 Jul 26. [CrossRef] [PubMed]
- Naghavi M, Barlas Z, Siadaty S, at al. Association of influenza vaccination and reduced risk of recurrent myocardial infarction. Circulation. 2000 Dec 19;102(25):3039-45. [CrossRef] [PubMed]
- Udell JA, Zawi R, Bhatt DL, et al. Association between influenza vaccination and cardiovascular outcomes in high-risk patients: a meta-analysis. JAMA. 2013 Oct 23;310(16):1711-20. [CrossRef] [PubMed]
- 28. Clar C, Oseni Z, Flowers N, at al. Influenza vaccines for preventing cardiovascular disease. Cochrane Database Syst Rev. 2015 May 5;2015(5):CD005050. [CrossRef] [PubMed] [PubMed Central]
- Conti, CR. Vascular events responsible for thrombotic occlusion of a blood vessel. Clin Cardiol. 1993 Nov;16(11):761-2. [CrossRef] [PubMed]
- Hebsur S, Vakil E, Oetgen WJ, at al. Influenza and coronary artery disease: exploring a clinical association with myocardial infarction and analyzing the utility of vaccination in prevention of myocardial infarction. Rev Cardiovasc Med. 2014;15(2):168-75. [CrossRef] [PubMed]
- Kinlay S, Ganz P. Role of endothelial dysfunction in coronary artery disease and implications for therapy. Am J Cardiol. 1997 Nov 6;80(9A):11I-16I. [CrossRef] [PubMed]
- Tomiyama H, Yamashina A. Vascular Dysfunction: A Key Player in Chronic Cardio-renal Syndrome. Intern Med. 2015;54(12):1465-72. Epub 2015 Jun 15. [CrossRef] [PubMed]
- Marti CN, Georgiopoulou VV, Kalogeropoulos AP. Acute heart failure: patient characteristics and pathophysiology. Curr Heart Fail Rep. 2013 Dec;10(4):427-33. [CrossRef] [PubMed] [PubMed Central]
- Davies MJ. The composition of coronary-artery plaques. N Engl J Med. 1997 May 1;336(18):1312-4. [CrossRef] [PubMed]
- Chan NN, Colhoun HM, Vallance P. Cardiovascular risk factors as determinants of endothelium-dependent and endothelium-independent vascular reactivity in the general population. J Am Coll Cardiol. 2001 Dec;38(7):1814-20. [CrossRef] [PubMed]
- Keshtkar-Jahromi M, Ouyang M, Keshtkarjahromi M, et al. Effect of influenza vaccine on tumor necrosis factor-like weak inducer of apoptosis (TWEAK) in older adults. Vaccine. 2018 Apr 12;36(16):2220-2225. [CrossRef] [PubMed] [PubMed Central]
- Gupta R, Quy R, Lin M, et al. Role of Influenza Vaccination in Cardiovascular Disease: Systematic Review and Meta-Analysis. Cardiol Rev. 2024 Sep-Oct 01;32(5):423-428. Epub 2023 May 9. [CrossRef] [PubMed]
- Omidi F, Zangiabadian M, Shahidi Bonjar AH, at al. Influenza vaccination and major cardiovascular risk: a systematic review and meta-analysis of clinical trials studies. Sci Rep. 2023 Nov 19;13(1):20235. [CrossRef] [PubMed] [PubMed Central]
Figure 1.
Study Flow Diagram. *Screen failures were due to exclusion criteria. CAD: coronary artery disease, 12m: 12-months, FU: follow up.
Figure 1.
Study Flow Diagram. *Screen failures were due to exclusion criteria. CAD: coronary artery disease, 12m: 12-months, FU: follow up.
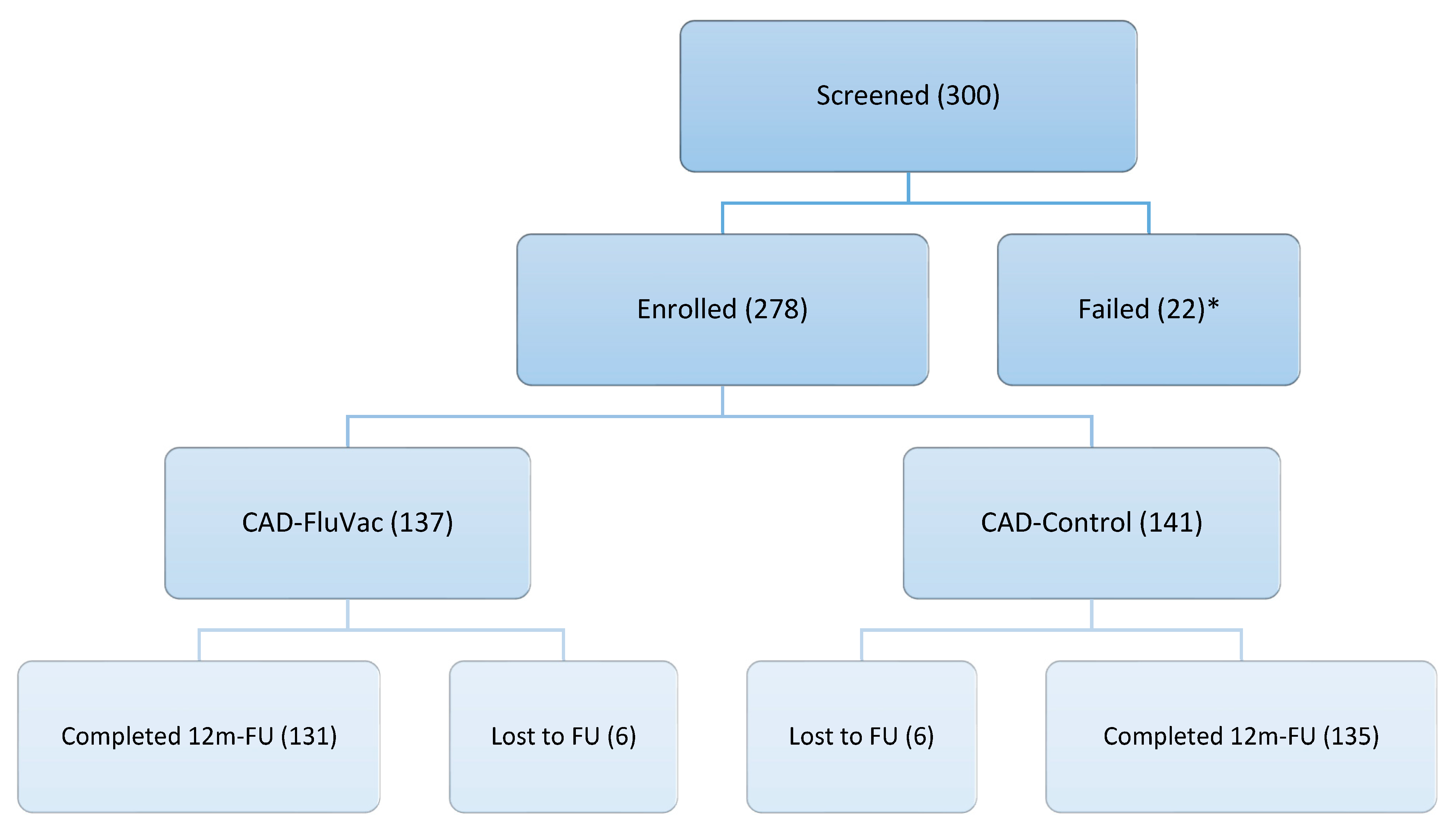
Figure 3.
12-months Cardiovascular Outcomes (numerical) in subjects with CAD, comparison FluVac vs. Placebo group. Analysis: Generalized linear regression with a poisson distribution, log-link and an offset for person-months of follow-up used to estimate incidence rate ratios (IRR) and 95% confidence intervals (95%CI).
Figure 3.
12-months Cardiovascular Outcomes (numerical) in subjects with CAD, comparison FluVac vs. Placebo group. Analysis: Generalized linear regression with a poisson distribution, log-link and an offset for person-months of follow-up used to estimate incidence rate ratios (IRR) and 95% confidence intervals (95%CI).


Table 1.
Demographic features and background history in participants.
| All(n=278) | CAD-FluVac(n=137) | CAD-Placebo(n=141) | |
| Mean age, mean years(SD) | 54.73 (9.08) | 54.53 (9.21) | 54.93 (8.98) |
| Female n (%) | 93 (33.5) | 45 (32.8) | 48 (34.0) |
| Mean BMI mean (SD) | 27.69 (4.47) | 27.63 (4.48) | 27.75 (4.48) |
| Background diseases (History) | |||
| Diabetes mellitus n (%) | 75 (27.0) | 35 (25.5) | 40 (28.4) |
| Hypertension n (%) | 231 (83.1) | 115 (83.9) | 116 (82.3) |
| Hyperlipidemia n (%) | 155 (55.8) | 77 (56.2) | 78 (55.3) |
| Daily aspirin n (%) | 254 (91.4) | 128 (93.4) | 126 (89.4) |
| Daily multivitamin n (%) | 15 (5.4) | 9 (6.6) | 6 (4.3) |
| Smoking history, pack/year(SD) | 10.66 (21.11) | 10.04 (20.65) | 11.26 (21.61) |
| Exercise* n (%) | 138 (49.8) | 72 (52.6) | 66 (47.1) |
| Family history of IHD n (%) | 133 (47.8) | 61 (44.5) | 72 (51.1) |
*Exercise was defined as minimum of 15 minutes physical activity including walking daily for at least 4 days per week. BMI: body mass index, IHD: ischemic heart disease,.
Table 2.
Baseline cardiologic features in participants.
| All (n=278) | CAD-FluVac (n=137) | CAD-Placebo (n=141) | |
| Echocardiography findings | |||
| Estimated EF mean (SD) | 52.81 (10.09) | 52.55 (10.46) | 53.07 (9.78) |
| LV systolic dysfunction n (%) | 32 (17.8) | 17 (19.3) | 15 (16.3) |
| LV diastolic dysfunction n (%) | 75 (41.7) | 35 (39.8) | 40 (43.5) |
| Septal wall akinesia n (%) | 76 (42.2) | 36 (40.9) | 40 (43.5) |
| Myocardial aneurysm n (%) | 4 (2.2) | 2 (2.3) | 2 (2.2) |
| Heart Valve abnormalities n (%) | 55 (30.6) | 21 (23.9) | 34 (37.0) |
|
Angina severity, (SAQ) Physical limitation mean (SD) Angina stability mean (SD) Angina frequency mean (SD) Treatment satisfaction mean (SD) Disease perception mean (SD) |
|||
| 71.81 (22.69) | 71.00 (25.24) | 72.58 (20.04) | |
| 37.26 (30.86) | 36.52 (31.16) | 37.98 (30.67) | |
| 66.27 (21.93) | 65.33 (21.78) | 67.16 (22.11) | |
| 75.52 (20.35) | 74.69 (21.37) | 76.32 (19.37) | |
| 56.63 (26.41) | 54.86 (26.44) | 58.33 (26.37) | |
| Gensini Score mean (SD) | 8.74 (5.34) | 7.97 (5.03) | 9.50 (5.54) |
|
CAD management PCI n (%) CABG n (%) Medical n (%) |
|||
| 105 (37.8) | 47 (34.3) | 58 (41.1) | |
| 46 (16.5) | 21 (15.3) | 25 (17.7) | |
| 270 (97.1) | 131 (95.6) | 139 (98.6) |
EF: Ejection Fraction, LV: Left Ventricle, SAQ: Seattle Angina Questionnaire, CAD: Coronary Artery Disease, PCI: Percutaneous Intervention, CABG: Coronary Artery Bypass Graft.
Table 3.
Pre-and Post-vaccination Ab titer (Month 1) in subjects with CAD, FluVac vs. Placebo group.
Table 3.
Pre-and Post-vaccination Ab titer (Month 1) in subjects with CAD, FluVac vs. Placebo group.
| Outcome | CAD-Placebo (n=137) | CAD-FluVac (n=141) | P-value |
| Antibody A (Solomon Islands/3/2006 (H1N1)) | |||
| Protective (≥1:40) pre-vaccination, n (%) | 80 (47.62%) | 88 (52.38) | 0.12 |
| Protective (≥1:40) post-vaccination, n (%) | 109 (46.98%) | 123 (53.02%) | <0.0001 |
| Magnitude of change*, ×fold, mean (SD) | 16.30 (66.65) | 57.92 (159.81) | <0.0001 |
| Serologic response (≥4-fold rise), n (%) | 50 (35.46%) | 91 (64.54%) | <0.0001 |
| Antibody B (Wisconsin/67/2005 (H3N2)) | |||
| Protective (≥1:40) pre-vaccination, n (%) | 113 (49.34%) | 116 (50.66%) | 0.10 |
| Protective (≥1:40) post-vaccination, n (%) | 126 (50.20%) | 125 (49.80%) | 0.14 |
| Magnitude of change, ×fold, mean (SD) | 6.41 (21.59) | 28.48 (114.76) | <0.0001 |
| Serologic response (≥4-fold rise), n (%) | 33 (28.45%) | 83 (71.55%) | <0.0001 |
| Antibody C (Malaysia/2506/2004) | |||
| Protective (≥1:40) pre-vaccination, n (%) | 116 (49.79%) | 117 (50.21%) | 0.18 |
| Protective (≥1:40) post-vaccination, n (%) | 135 (51.72%) | 126 (48.27%) | 0.24 |
| Magnitude of change, ×fold, mean (SD) | 6.60 (28.18) | 12.45 (56.60) | <0.0001 |
| Serologic response (≥4-fold rise), n (%) | 64 (39.26%) | 100 (60.98%) | <0.0001 |
*after/before, CAD: Coronary Artery Disease, IQR: InterQuartile Range. Analysis: Fisher’s Exact Test used for protective level of antibody and serologic response and Kruskal-Wallis Test used for magnitude of change.
Table 4.
Correlation between Antibody Response and 12-months Cardiovascular events in CAD-FluVac subjects.
Table 4.
Correlation between Antibody Response and 12-months Cardiovascular events in CAD-FluVac subjects.
| Outcome (n) | CAD-FluVac (n=137) | P-value | |
| CV event*(n=34) | No CV event (n=103) | ||
| Antibody A (Solomon Islands/3/2006 (H1N1)) | |||
| Protective (≥1:40) Pre-vaccination, n (%) | 25 (75.76%) | 63 (66.32%) | 0.39 |
| Protective (≥1:40) Post-vaccination, n (%) | 33 (97.06%) | 90 (94.74%) | 0.33 |
| Magnitude of change, ×fold, mean (SD) | 97.61 (213.17) | 44.14 (135.25) | 0.65 |
| Serologic response (≥4-fold rise), n (%) | 24 (70.59%) | 67 (65.05%) | 1 |
| Antibody B (Wisconsin/67/2005 (H3N2)) | |||
| Protective (≥1:40) Pre-vaccination, n (%) | 29 (87.88%) | 87 (91.58%) | 0.50 |
| Protective (≥1:40) Post-vaccination, n (%) | 32 (96.97%) | 93 (97.89%) | 1 |
| Magnitude of change, ×fold, mean (SD) | 33.09 (122.06) | 26.87 (112.74) | 0.90 |
| Serologic response (≥4-fold rise), n (%) | 22 (66.67%) | 61 (64.21%) | 0.84 |
| Antibody C (Malaysia/2506/2004) | |||
| Protective (≥1:40) Pre-vaccination, n (%) | 29 (87.88%) | 88 (92.63%) | 0.47 |
| Protective (≥1:40) Post-vaccination, n (%) | 33 (100.00%) | 93 (97.89%) | 1 |
| Magnitude of change, ×fold, mean (SD) | 9.27 (14.79) | 13.55 (65.18) | 0.56 |
| Serologic response (≥4-fold rise), n (%) | 26 (76.47%) | 74 (71.84%) | 1 |
*CV events: Cardiovascular death, Acute Coronary Syndrome, Myocardial Infarction, Coronary Artery Bypass Graft or Percutaneous Intervention. CAD: Coronary Artery Disease, IQR: InterQuartile Range. Analysis: Fisher’s Exact Test used for protective level of antibody and serologic response and Kruskal-Wallis Test used for magnitude of change.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



